Embed Size (px)
Citation preview
Approach to Massive HemorrhageYulia Lin, MD, FRCPC, CTBSDivision Head, Transfusion Medicine, Sunnybrook HSCAssociate Professor, University of Toronto
Educational Objectives
We will focus on the following aspects of massive hemorrhage:1. When to activate the massive hemorrhage
protocol (MHP)2. Which blood products should be given3. Which adjunctive therapies should be given4. When to stop the MHP
Introduction to Massive Hemorrhage Protocols
Provide state-of-the-art care to achieve best possible outcomes
• Streamline complex logistics of rapid blood delivery• High quality, standardized care• Facilitates communication• Reduce cognitive burden during resuscitation• Tracking metrics for continuous QI
Goals of the Massive Hemorrhage Protocol
Callum et al. CMAJ Open; DOI:10.9788/cmajo.20190042
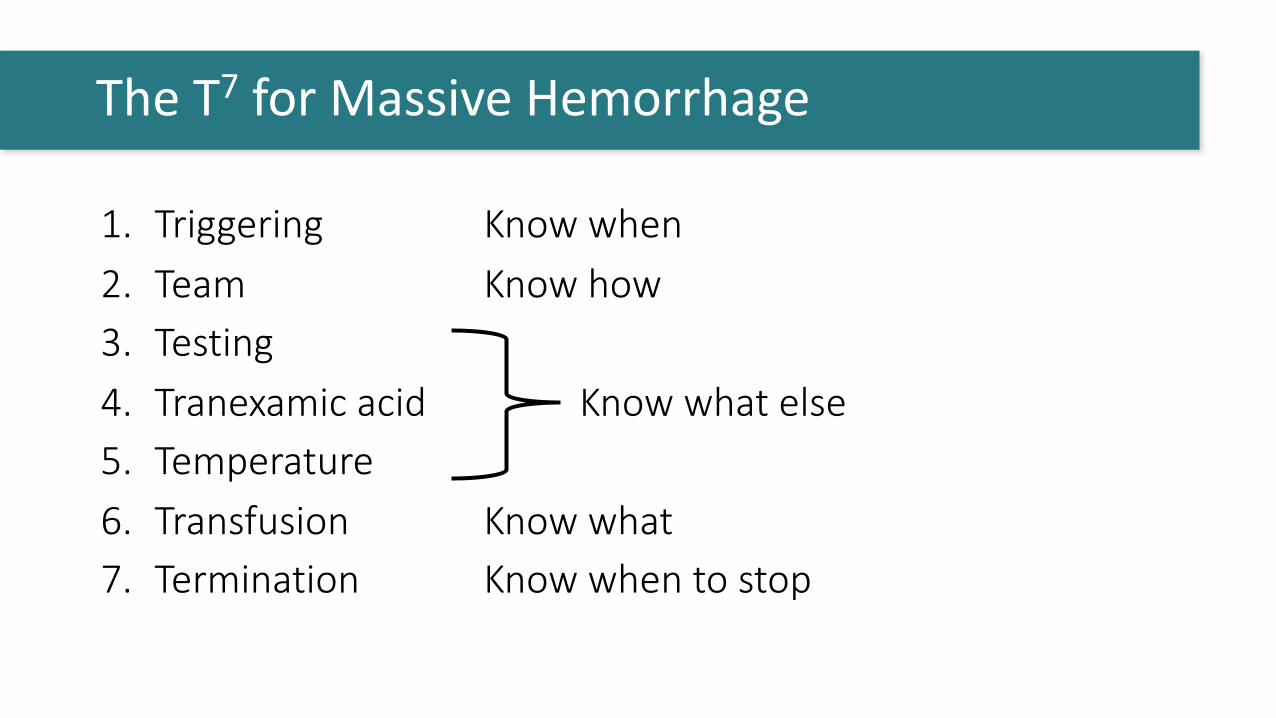
1. Triggering Know when2. Team Know how3. Testing4. Tranexamic acid Know what else5. Temperature6. Transfusion Know what7. Termination Know when to stop
The T7 for Massive Hemorrhage

1. Triggering the MHP
Minimize UndertriageHemorrhagic shock
Accept some OvertriageUnnecessary transfusion
Fluid overloadTransfusion complications
Blood WastageResource mobilization
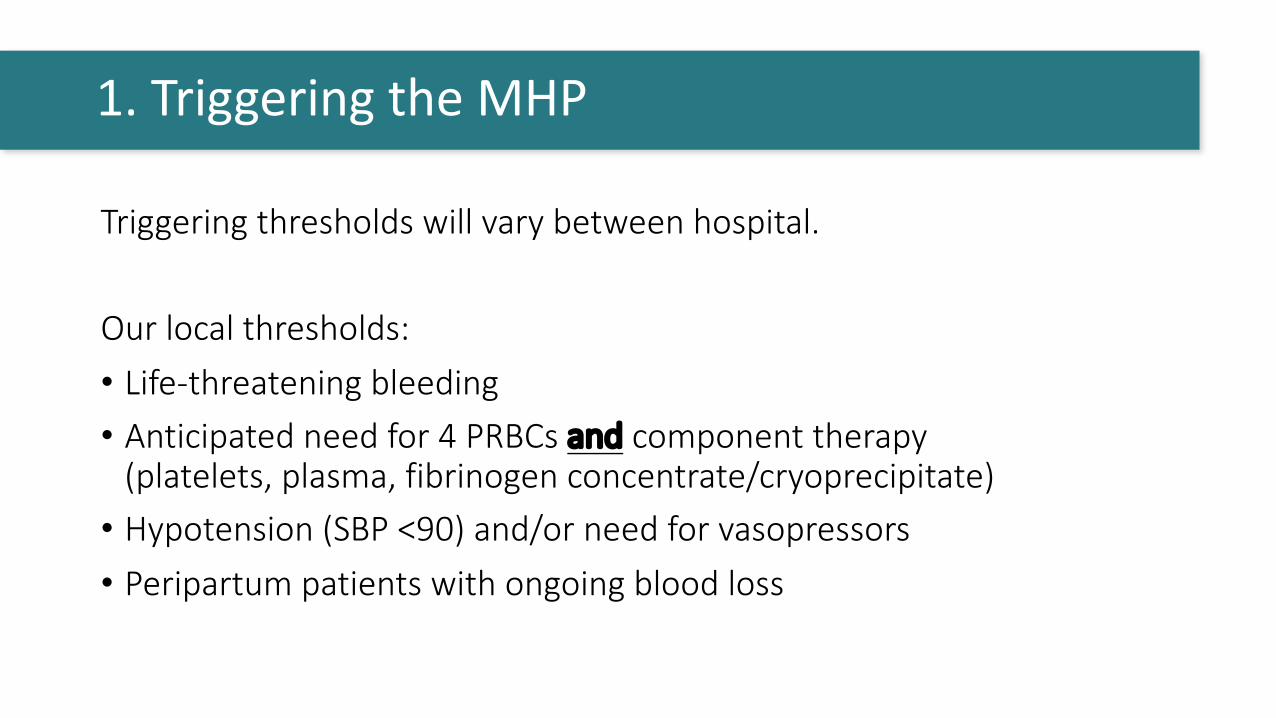
Triggering thresholds will vary between hospital.
Our local thresholds:• Life-threatening bleeding• Anticipated need for 4 PRBCs and component therapy
(platelets, plasma, fibrinogen concentrate/cryoprecipitate)• Hypotension (SBP <90) and/or need for vasopressors• Peripartum patients with ongoing blood loss
1. Triggering the MHP
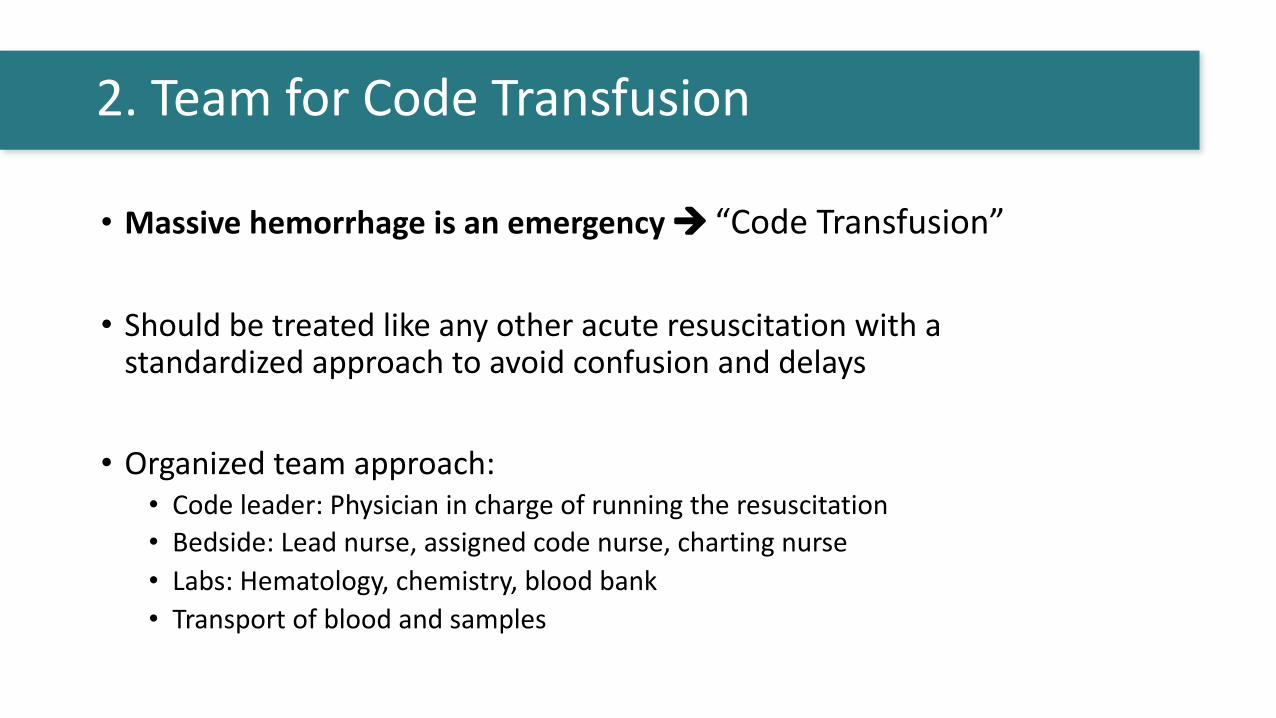
• Massive hemorrhage is an emergency à “Code Transfusion”
• Should be treated like any other acute resuscitation with a standardized approach to avoid confusion and delays
• Organized team approach:• Code leader: Physician in charge of running the resuscitation• Bedside: Lead nurse, assigned code nurse, charting nurse• Labs: Hematology, chemistry, blood bank • Transport of blood and samples
2. Team for Code Transfusion
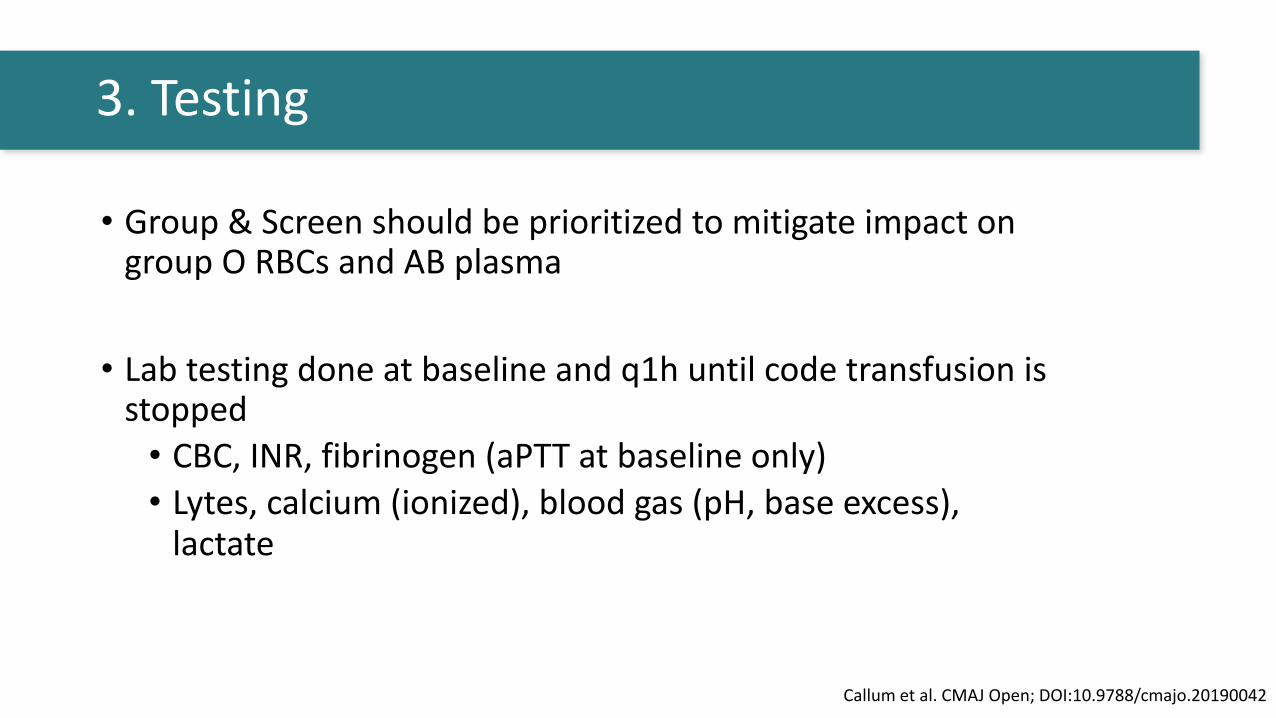
• Group & Screen should be prioritized to mitigate impact on group O RBCs and AB plasma
• Lab testing done at baseline and q1h until code transfusion is stopped • CBC, INR, fibrinogen (aPTT at baseline only)• Lytes, calcium (ionized), blood gas (pH, base excess),
lactate
3. Testing
Callum et al. CMAJ Open; DOI:10.9788/cmajo.20190042
• Uncrossmatched blood: Group O RBCs and Group AB plasma • O RhD positive: males, postmenopausal females• O RhD negative (4% of donor supply): reserved for
females of childbearing age • AB plasma (4% of donor supply): always short supply
• Aim to switch to group specific ASAP• Remember “O negative” is not matched for other RBC
antibodies
Until testing available: Uncrossmatched Blood
Urgent Reversal of Anticoagulants
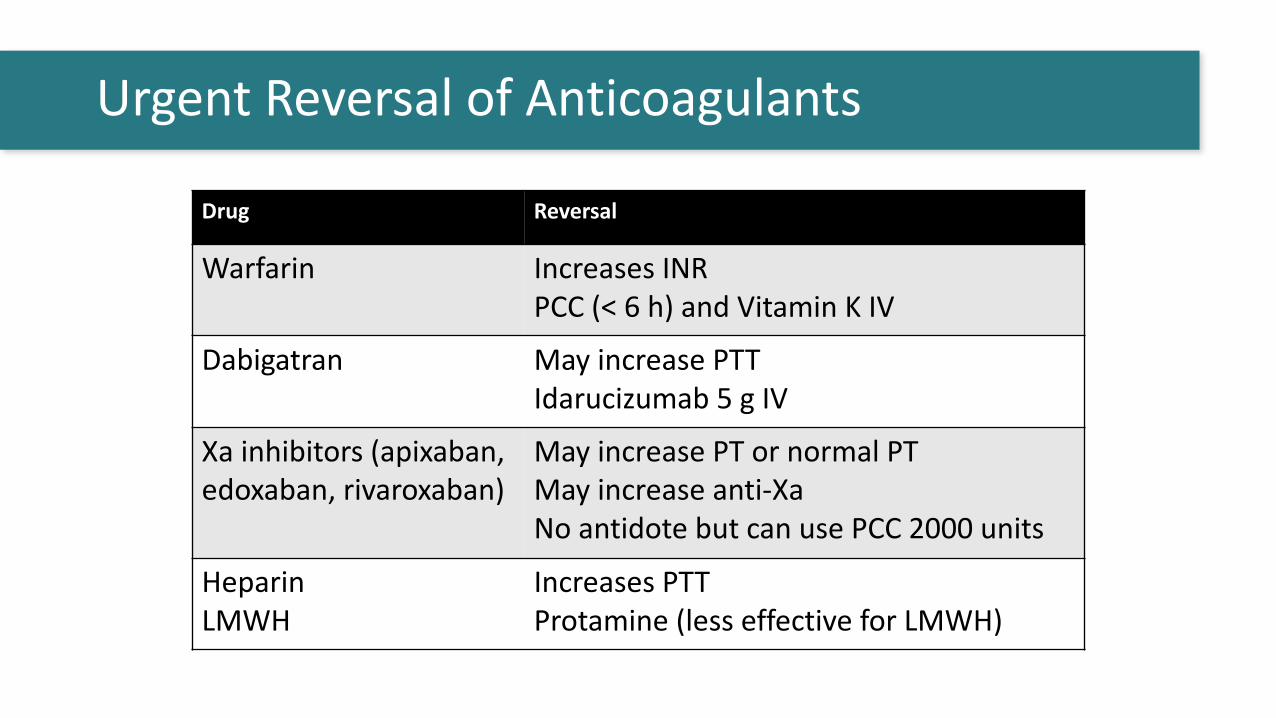
Drug Reversal
Warfarin Increases INRPCC (< 6 h) and Vitamin K IV
Dabigatran May increase PTTIdarucizumab 5 g IV
Xa inhibitors (apixaban, edoxaban, rivaroxaban)
May increase PT or normal PTMay increase anti-XaNo antidote but can use PCC 2000 units
HeparinLMWH
Increases PTTProtamine (less effective for LMWH)
• Tranexamic acid can improve coagulopathy and there is evidence of survival benefit in some populations
• Tranexamic acid should be given as soon as possible à Target within 1 hour (less than 3 hours) of injury for trauma patients or within 3 hours of MHP activation for other patients
• Give 1g IV bolus + 1g IV over 8 h (alternative: 2 gm IV bolus)
4. Tranexamic Acid
Callum et al. CMAJ Open; DOI:10.9788/cmajo.20190042
• Why is this important?• Poorly monitored during pre-hospital and pre-OR phase• Often hypothermic (T< 36oC) in the trauma setting• Temp <34°C associated with an increase in mortality• Each 1°C increases blood loss by 16% and the risk of transfusion by 22%• Pts feel better when they are warmer
• Measure at baseline then at least Q30mins during MHP • Target temperature ≥ 36oC
5. Temperature
Alam A et al. Injury 2018;49:117-123Reynolds BR et al. J Trauma. 2012;73:486-91
Rajagopalan S et al. Anesthesiology 2008;108:71-77Kober A et al. Mayo Clin Proc. 2001;76(4):369-75.
• Emergency uncrossmatched components (O RBCs, AB FP)• Start with immediate RBC transfusion, then 2RBC:1 plasma ratio• Switch to lab guided as soon as lab results are back
• Targets during MHP:• Hb > 80 g/L (RBC)• INR < 1.8 (plasma)• Fibrinogen > 1.5 g/L (fibrinogen concentrate or cryoprecipitate) • Platelets > 50 x 109/L (platelets)• Ionized Ca2+ > 1.15 mmol/L
6. Transfusion
Callum et al. CMAJ Open; DOI:10.9788/cmajo.20190042
• Once bleeding source control attained and transfusion slowed call to cancel the MHP
• Return coolers and unused blood to blood bank• Return blood as received (e.g. RBCs in cooler, Do not put
platelets in coolers)• Blood Bank will cease preparing more units (e.g. thawing
plasma)• Resources redirected back to other patients
7. Terminating the MHP
Callum et al. CMAJ Open; DOI:10.9788/cmajo.20190042

• At earliest opportunity, inform patient and/or substitute decision maker about MHP• Discuss risks of massive transfusion
• Common: fever, rash, TACO, hyperkalemia• Uncommon: TRALI• Potential risks (eg. RBC alloimmunization in women of child-bearing
potential)
• Women of child-bearing potential should undergo G&S at 6 weeks and/or 6 months after transfusion for RBC antibodies
7. Terminating the MHP
Callum et al. CMAJ Open; DOI:10.9788/cmajo.20190042

Additional ICU Management Considerations
• Enable rapid administration of blood products:• IV access: Preference is for large bore peripheral IVs (14 or 16G) or
cordis central venous catheter• Pressure bags or rapid infusers (blood warmer)
• Arterial line for continuous blood pressure monitoring and to facilitate frequent bloodwork
• Warming devices: • Fluid warmers• Warming blankets
Supportive Measures
• Consequences of high volume resuscitation:• Transfusion-associated circulatory overload (TACO)• Third-spacing and abdominal compartment syndrome• Limb compartment syndrome
• Electrolyte abnormalities:• Hypocalcaemia (citrate in blood products)• Hyperkalemia• Hypomagnesemia
• Metabolic acidosis: Often multifactorial à hypoperfusion, hepatic and/or renal dysfunction
Monitor For and Treat Complications
Patients frequently require mechanical ventilation and
hemodynamic support while undergoing massive
resuscitation
MHP T7 Summary
1. Triggering Know when and how to activate MHP2. Team Know team member roles3. Testing G&S done, bloodwork Q1H minimum4. Tranexamic acid Give early (<3 hours)5. Temperature Monitored and kept above 36oC6. Transfusion Minimize over/under transfusion7. Termination Avoid blood/resource wastage





























