Embed Size (px)
Citation preview
Approach to pediatric retinal
disease Ghanbari MD
1391:12:10
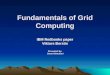
LCA
Infant with normal fundus and low vision• LCA• Stationary night blindness• Achromatopsia • Immue retinopathy
Development of the Retina
• The retina develops over a relatively long period of time beginning from the early gestational period through the first years of life.
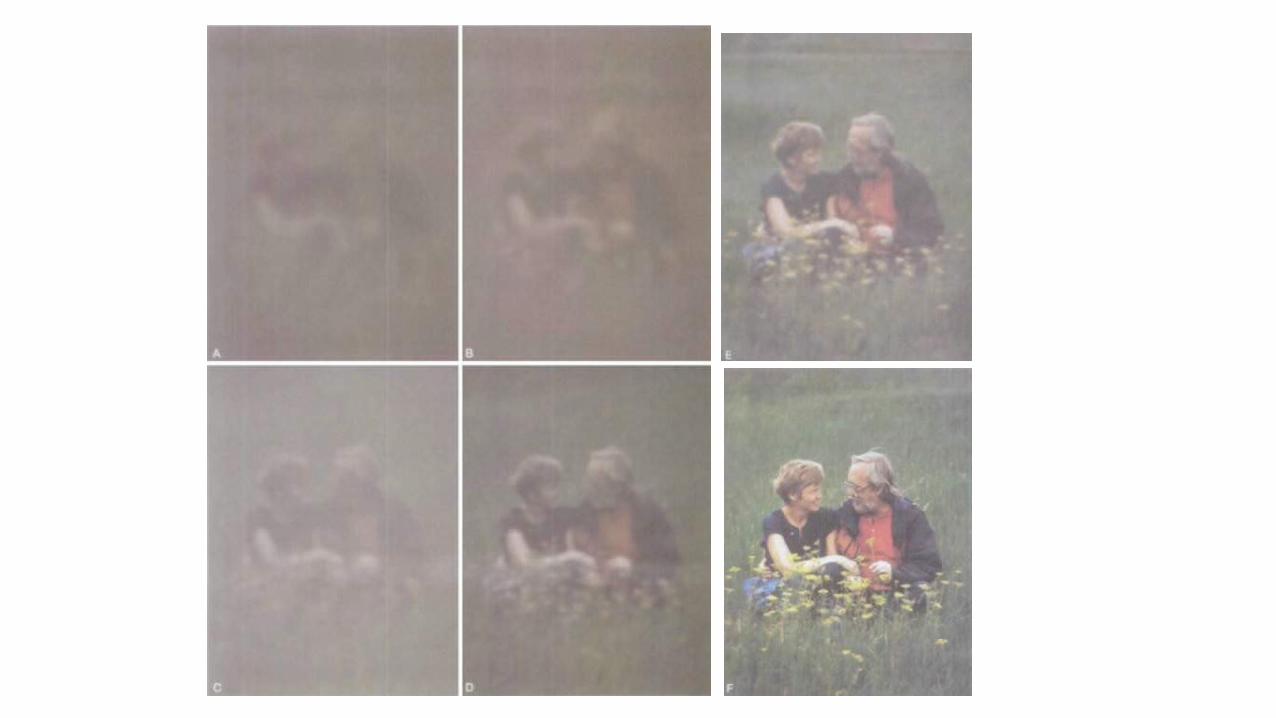
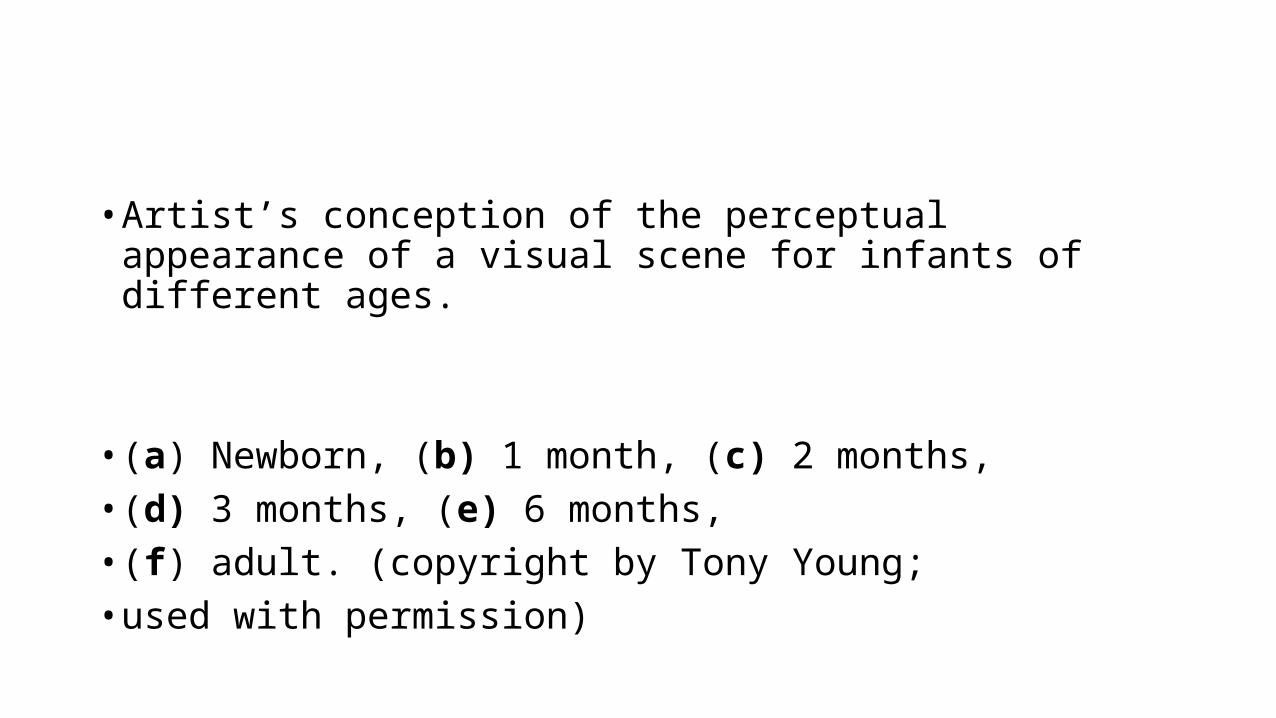
• Artist’s conception of the perceptual appearance of a visual scene for infants of different ages.
• (a) Newborn, (b) 1 month, (c) 2 months, • (d) 3 months, (e) 6 months,• (f) adult. (copyright by Tony Young;• used with permission)
Electroretinographic Testing in Infants and Children
• ERG can be recorded as in preterm infants
Retinopathy of Prematurity (ROP) • Signs and symptoms:• Retinopathy of prematurity (ROP) affects low-birth-weight
premature infants and can lead to blindness; the incidence of ROP has increased, as smaller and younger babies are surviving.
ROP Risk factors:
• Birth before 32 weeks' gestation, especially before 30 weeks• Birth weight of less than 1500 g, especially less than 1250 g• Possible risk factors include:• Supplemental oxygen, • Hypoxemia, • Hypercarbia, • Concurrent illness.
Treatment of ROP
• Cryotherapy• Laser surgery • Scleral buckling • Vitrectomy• Anti-VEGF
Treatment may also be initiated for the following retinal findings:
• Zone 1 ROP - Any stage, with plus disease• Zone 1 ROP - Stage 3, with no plus disease• Zone 2 ROP - Stage 2 or 3, with plus disease
• Treatment should generally be accomplished, when possible, within 72 hours of determination of treatable disease to minimize the risk of retinal detachment.
• An Updated Study of the Use of Bevacizumab in the Treatment of Patients with Prethreshold Retinopathy of Prematurity in Taiwan.
• FAMILIAL EXUDATIVE VITREORETINOPATHY
)
• Persistent Hyperplastic Primary Vitreous (PHPV
A Language for Retinoblastoma:Guidelines and Standard Operating Procedures
• Retinoblastoma is the most common primary malignant intraocular tumor in children.
International Classification for Intraocular Retinoblastoma
• Group A
• Small tumors (3 mm across or less) that are confined to the retina and are not near important structures such as the optic disk (where the optic nerve enters the retina) or the foveola (the center of vision).
• Group B
• All other tumors (either larger than 3 mm or small but close to the optic disk or foveola) that are still confined to the retina.
• Group C
• Well-defined tumors with small amounts of spread under the retina (subretinal seeding) or into the gelatinous material that fills the eye (vitreous seeding).
• Group D
• Large or poorly defined tumors with widespread vitreous or subretinal seeding. The retina may have become detached from the back of the eye.
• Group E
• The tumor is very large, extends near the front of the eye, is bleeding or causing glaucoma (high pressure inside the eye), or has other features that mean there is almost no chance the eye can be saved.
• Shields et al analyzed 249 eyes with retinoblastoma treated with intravenous chemoreduction and found that success was: achieved in of
• Group A 100%, • Group B 93%, • Group C 90%,• Group D 47% eyes. • A later study identified treatment success with intra-arterial
chemotherapy (IAC) in 100% of group C and D eyes, and 33% of group E eyes.
High-Risk Retinoblastoma Based onInternational Classification ofRetinoblastoma: Analysis of 519Enucleated Eyes
• On the basis of the ICRB, 17% of group D and 24% of group E eyes are at increased risk for metastatic disease. In this study, 8% of patients developed metastasis. There was no metastasis in any patient classified with non–high-risk retinoblastoma.
پوزش عرض ضمن
باالی حجم در LECTUERبدلیل نمیباشد پذیر امکان اسالیدها ادامهآموزشی مرکز بصری و سمعی واحد به لطفا ادامه به نیاز صورت
تلفن شماره با یا و مراجعه فیض داخلی 03114476010درمانیتماس حاصل نمائید 392
با تشکر