Embed Size (px)
Citation preview

CLINICAL REVIEW
Approach to Syncope
WILLIAM T. BRANCH, JR., MD*
SYNCOPE is def ined a s transient loss of conscious- ness accompanied by loss of postural tone and fol- lowed by spontaneous recovery. As a clinical prob- lem, it spans severa l spec ia l t ies - - cardiology, neurology, and psychiatry - - and hence is best eva lua ted by a physic ian with broad training and background in internal medicine. The most com- mon type, vasovaga l syncope, is a lmost a lways self-limited. For pat ients eva lua ted with transient losses of consciousness in an emergency room or hospital setting, however, rates of mortali ty or ma- jor morbidity within one year were 7.4 to 14%. 1-3 Available diagnost ic tests to identify those at high- es t r isk a r e i m p r e c i s e a n d e x p e n s i v e . The approach, therefore, is problematic. Nevertheless, the clinician facing a pat ient with syncope must make decisions regarding the extent of clinical and laboratory evaluat ion.
This review descr ibes the differential diagno- sis and provides an ana lys i s of the approach to pat ients with syncope. The most important s tep in the evaluat ion is to elicit a deta i led "moment-by- moment" description of the event, its setting and sequelae . Further evaluat ion depends on this his- tory, together with the physical examinat ion, the electrocardiogram (ECG), and, if indicated, blood counts, glucose, electrolytes and other tests per- formed during the initial visit. Pat ients with syn- cope or presyncope are s epa ra t ed from those with vertigo, "giddiness," confusional states, and other categories of symptoms. In many ca se s of syncope a specific pathogenet ic mechanism can be identi- fied during the initial evaluat ion. Examples in- clude post- tussive syncope, seizures, aortic steno- sis, and orthostatic hypotension. The approach to the remaining pat ients depends on an a s se s smen t of their risk. Such an assessment , d i scussed later, should take into account age and pas t history a s well a s features of the spell(s) in question.
Table 1 lists the types of syncope identified in more than 1,000 pat ients with transient losses of consciousness.L 3-5 In ~- 90% of cases, syncope re- sulted from dec reased cerebral peffusion caused by a decline in blood pressure due to loss of vascu-
*Associate Professor of Medicine at the Brigham and Women's Hospi- tal, Harvard Medical School, Boston, Massachusetts.
Address correspondence and reprint requests to Dr. Branch: Brigham and Women's Hospital, 75 Francis Street, Boston, MA 02115.
lar tone, interruption of normal cardiac rhythm, or decreased cardiac output. The remaining pat ients include - 10% in whom consc iousness was al tered by a seizure, metabol ic imbalance, local ischemia, or other factors affecting the central nervous sys- tem. A psychiatric disorder (hysteria) a l tered re- spons iveness of a few patients.
DIFFERENTIAL DIAGNOSIS
Vasovagal Syncope
Vasovagal syncope, a l so termed vasodepres- sor syncope or s imple fainting spells, is the most common type of syncope in medical outpatients. L 4 These fainting spells share the common mechan- ism of transient i nadequacy of cerebral perfusion due to inappropriate vasodi la ta t ion with pooling of blood in the extremities. They share common char- acterist ics of be ing brief, usua l ly without adverse consequences , and usua l ly occurring while the pa- tient is s tanding, somet imes while sitting, and rarely if ever while recumbent . Diagnostic clues are provided by the setting, the onset, the patient 's appearance , and the recovery (Table 2).
Vasovagal syncope often follows a stressful event . E x a m p l e s inc lude rece iv ing b a d news , donating blood, having a venipuncture, or making a stressful presentat ion. Other spells, which are sometimes dis t inguished from stress induced vaso- vagal syncope and termed vasodepressor spel ls or temporary orthostatic hypotension, 4 are related to prolonged s tanding or a s suming the upright pos- ture. Typical se t t ings inc lude wai t ing in lines, s tanding in warm crowded rooms, or ar is ing from bed to empty a full b ladder . Predisposing factors include large meals , warm baths, and pregnancy, as well a s malnutrition, fatigue, and physical de- conditioning. The Valsa lva maneuver performed during prolonged s tanding or with defecat ion can also produce syncope, a s can intense visceral pain, such as the pain of g lossopharyngea l neuralgia . Hypervent i la t ion induces per iphera l vasodi la ta - tion and thus may predispose to this type of syn- cope.
Characterist ic premonitory symptoms precede vasovaga l syncope by severa l minutes. Weakness , nausea , diaphoresis , general ized warmth or numb- ness, and, finally, the sensat ion of an impending
49

5 0 Branch, APPROACH TO SYNCOPE
TABLE 1
Types of Syncope in Four Series of Patients
Type of Syncope
Wayne, 19614 Silverstein et al., 1982 s Day et al., 19821 Kapoor et al., 19833
Patients Encountered Patients Admitted to in EW with Patients Hospitalized
All Patients Medical ICU Transiently Altered or seen in EW with Syncope with Syncope Consciousness or as Outpatients
(n = 510) (n = 108) (n = 198) (n = 204)
Vasovagal or vasodepressor 298 (58%) 1 (1%) 57 (2996) 24 (12%)
Cardiovascular 58 (11%) 42 (39%) 17 (8.6%) 53 (26%) Heart block or bradyarrhythmias 17 2 2 5 Carotid sinus sensitivity 15 - - - - 1 Aortic stenosis 9 4 4 5 Supraventricular tachycardia 8 - - 1 3 Atrial fibrillation - - 6 - - - - Ventdcu]ar tachycardia or dysrhythmia - - 13 4 20 Sick sinus syndrome - - 4 3 12 Pacemaker failure - - 4 - - 1 Angina pectoris 4 - - 1 - - Myocardial infarction 3 6 - - 2 Pulmonary hypertension 2 - - - - 1 Pulmonary embolism - - 3 1 1 Dissecting aneurysm - - - - - - 1 Subclavian steal - - - - - - 2 Mitral stenosis - - - - 1 - -
Neurologic 54 (10.6%) 9 (8.3%) 76 (38%) 12 (5.9%) Generalized seizures 26 5* 30 3 Other types o f seizures - - - - 15 - - Metabolic disorders or drug toxicity w/o seizures - - 4 21 6 t Cerebrovascular disease (TIAs) 24 - - 2 3 Migraine 2 - - 3 - - Hypertensive encephalopathy . . . . Multiple sclerosis - - - - 1 - - Brain tumors/metastases - - - - 4 - -
Postmicturition 17 (33%) - - 2 (1%) - -
Post-tussive 13 (2.5%) 1 (1%) - - - -
Post-pain (trigeminal neuralgia) - - - - - - 1 (0.5%)
Orthostatic hypotension 28 (5.5%) 4 (3.7%) 7 (3.5%) 14 (6.8%)
Hyperventilation 15 (2.996) - - 5 (2.5%) - -
HystericaVpsychogenic 4 (0.8%) _~t 9 (4.5%) 1 (0.5%)
Unknown cause 23 (4.5%)§ 51 (47%) 25 (13%) 97 (48%)
* Type of seizure not specified. t All drug-related, no metabolic disorders. $ Psychogenic included in vasovagal category. § Percentages classified as unknown range f rom 4.5% to 48%, in part according to the stringency of the criteria necessary to classify the syncope as having
another cause.
TABLE 2
Differentiating Vasovagal Syncope from Seizure f rom Cardiac Syncope
Vasovagal Syncope Seizure Cardiac Syncope
Onset Prodromal weakness, nausea, di- Sudden onset, or brief aura: deja vu, aphoresis, lasting seconds to minutes olfactory, gustatory, visual, etc.
Typical settings
Occurrence Appearance Residiuum
Emotional upse~ prolonged standing, uncomfortable surroundings, or on f i rst arising with full bladder Only when upright Pallor, weak pulse Rapid recovery but may recur on standing, occasional br ief donic move- ments, or urinary incontinence
Any setting, including sleep, some- times blinking lights, monotonous music Any position Cyanosis, stertorous breathing Prolonged recovery wi th postictal state, Todd's paresis
Sudden onset 4s or preceded by cardiac symptoms: chest tightness, dyspnea, di- aphoresis, palpitations Any setting, often without warning
Any position Pallor, variable pulse Recovery may be rapid or prolonged: i f cardiac arrest: seizure-like activity, signs o f cerebral hypoxia
Tables reproduced by permission from Branch WT, ed., Office practice o f medicine, Philadelphia, W. B. Saunders.
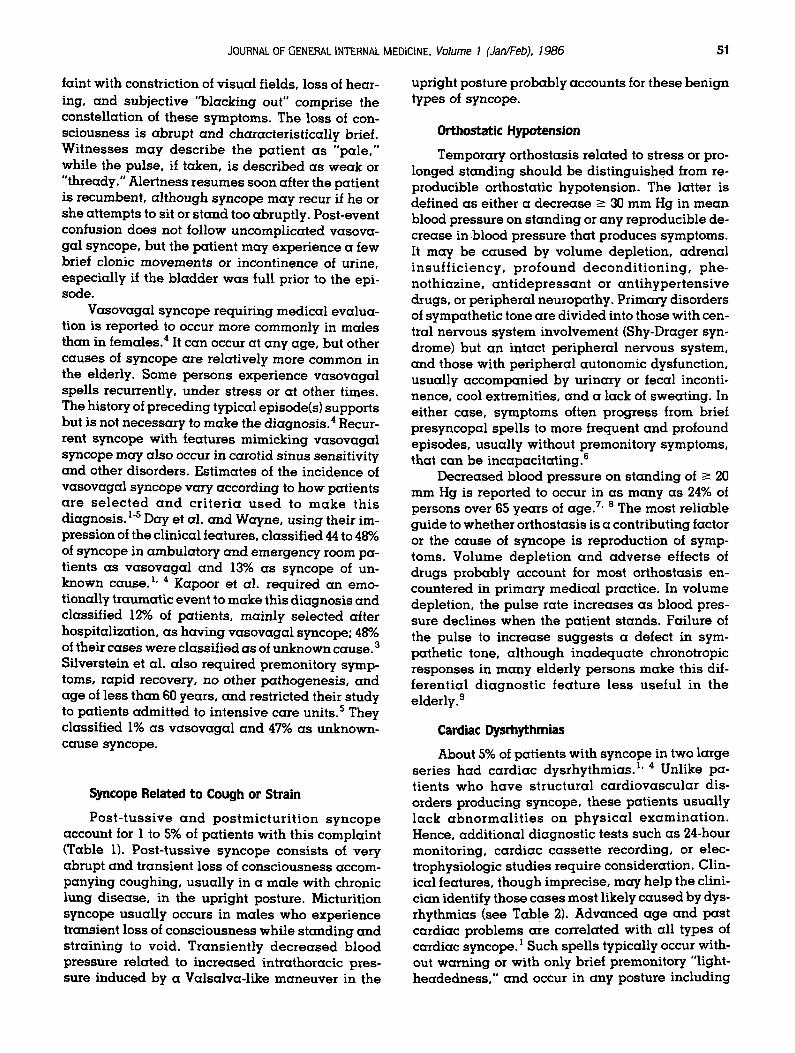
JOURNAL OF GENERAL INTERNAL MEDICINE. Volume I (Jan~Feb). 1986 ]51
faint with constriction of visual fields, loss of hear- ing, and subject ive "blacking out" comprise the constellation of these symptoms. The loss of con- sc iousness is abrupt and character is t ical ly brief. Wi tne s se s may desc r ibe the pa t ient a s "pale ," while the pulse, if taken, is descr ibed as weak or "thready." Alertness r esumes soon after the patient is recumbent, a l though syncope may recur if he or she at tempts to sit or s tand too abruptly. Post-event confusion does not follow uncomplicated vasova- gal syncope, but the pat ient may exper ience a few brief clonic movements or incontinence of urine, especia l ly if the b ladder w a s full prior to the epi- sode.
Vasovagal syncope requiring medical evalua- tion is reported to occur more commonly in males than in females, 4 It can occur at any age, but other causes of syncope are relat ively more common in the elderly. Some persons exper ience vasovaga l spel ls recurrently, under s tress or at other times. The history of preceding typical episode(s) supports but is not necessa ry to make the diagnosis . 4 Recur- rent syncope with features mimicking vasovaga l syncope may a lso occur in carotid sinus sensit ivity and other disorders. Est imates of the incidence of vasovaga l syncope vary according to how pat ients a r e s e l e c t e d a n d c r i t e r i a u s e d to m a k e th i s diagnosis. 1-5 Day et al. and Wayne, using their im- pression of the clinical features, c lassif ied 44 to 48% of syncope in ambula tory and emergency room pa- tients as va sovaga l and 13% as syncope of un- known cause. l ' 4 Kapoor et al. required an emo- tionally t raumatic event to make this d iagnosis and classified 12% of patients, mainly se lec ted after hospitalization, as having vasovaga l syncope; 48% of their cases were classif ied as of unknown cause. 3 Silverstein et al, a lso required premonitory symp- toms, rapid recovery, no other pathogenesis , and age of less than 60 years, and restricted their s tudy to pat ients admit ted to intensive care units. 5 They classif ied 1% as vasovaga l and 47% as unknown- cause syncope.
Syncope Related to Cough or Strain
P o s t - t u s s i v e a n d p o s t m i c t u r i t i o n s y n c o p e account for 1 to 5% of pat ients with this complaint (Table 1). Pos t - tuss ive syncope consis ts of very abrupt and transient loss of consc iousness accom- panying coughing, usual ly in a male with chronic lung disease , in the upright posture. Micturition syncope usual ly occurs in males who experience transient loss of consc iousness while s tanding and s t ra in ing to void. Trans ien t ly d e c r e a s e d b lood pressure re la ted to increased intrathoracic pres- sure induced by a Valsalva-l ike maneuver in the
upright posture probably accounts for these benign types of syncope.
Orthostatic Hypotension
Temporary orthostasis related to stress or pro- longed s tanding should be dis t inguished from re- producible orthostatic hypotension. The latter is defined as either a dec rease -~ 30 mm Hg in mean blood pressure on s tanding or any reproducible de- crease in blood pressure that produces symptoms. It may be c a u s e d by volume depletion, adrena l i n s u f f i c i e n c y , p r o f o u n d d e c o n d i t i o n i n g , phe- nothiazine, a n t i d e p r e s s a n t or an t ihype r t ens ive drugs, or per ipheral neuropathy. Primary disorders of sympathet ic tone are divided into those with cen- tral nervous sys tem involvement (Shy-Drager syn- drome) but an intact per ipheral nervous system, and those with per ipheral autonomic dysfunction, usual ly accompan ied by urinary or fecal inconti- nence, cool extremities, and a lack of sweating. In either case, symptoms often progress from brief presyncopal spel ls to more frequent and profound episodes, usual ly without premonitory symptoms, that can be incapacitat ing, e
Decreased blood pressure on s tanding of > 20 mm Hg is reported to occur in as many as 24% of persons over 65 years of age. 7' 8 The most rel iable guide to whether orthostasis is a contributing factor or the cause of syncope is reproduction of symp- toms. Volume dep le t ion and adve r se effects of
d r u g s probably account for most or thostasis en- countered in pr imary medical practice. In volume depletion, the pulse rate increases as blood pres- sure decl ines when the pat ient s tands. Failure of the pulse to increase sugges t s a defect in sym- pathetic tone, a l though inadequa te chronotropic responses in many elderly persons make this dif- fe ren t ia l d i a g n o s t i c f ea tu re l ess use fu l in the elderly. 9
Cardiac Dysrhythmias
About 5% of pat ients with syncope in two large ser ies had card iac dysrhythmias . 1' 4 Unlike pa- t ients who h a v e s t ruc tura l c a rd iovascu l a r dis- orders producing syncope, these pat ients usual ly l ack a b n o r m a l i t i e s on p h y s i c a l e x a m i n a t i o n . Hence, addi t ional diagnost ic tests such as 24-hour monitoring, cardiac casse t t e recording, or elec- trophysiologic s tudies require consideration. Clin- ical features, though imprecise, may help the clini- cian identify those cases most likely caused by dys- rhythmias (see Table 2). Advanced age and pas t cardiac problems are correlated with all types of cardiac syncope. 1 Such spel ls typically occur with- out warning or with only brief premonitory "light- headedness , " and occur in any posture including

52. Branch, APPROACH TO SYNCOPE
recumbency. They may occur at any time or in any setting. A "cluster" of spel ls may occur, so that several ep isodes of presyncope or syncope in the days to weeks before the pat ient seeks treatment sugges t this d iagnosis . The spell, if c aused by asystole or cardiac arrest, may be unusual ly pro- longed or severe.
Sup raven t r i cu l a r t a c h y c a r d i a s , ven t r i cu la r tachycardia, and bradyar rhythmias of all types are about equal ly common as causes of syncope. 1° In particular, elderly persons may faint at the onset of a brief run of supraventr icular tachycardia at ra tes that would be tolerated by younger persons. 10 Sus- ta ined palpi ta t ions prior to a spell may sugges t syncope re la ted to a prolonged s inus pause follow- •ng s p o n t a n e o u s reve r s ion of supraven t r i cu la r tachycardia to s inus rhythm. This may occur in the sick sinus syndrome, a l though most pat ients with that syndrome exper ience symptoms re la ted to spontaneously occurring prolonged sinus p a u s e s (~ 3 seconds duration) or profound sinus bradycar- dia (rates -< 45 bpm). 11 Complete heart block is usual ly followed by a 10- to 90-second "warm-up" period prior to restoration of cerebral blood flow by idioventricular rhythmiC; hence, most pat ients re- cover spontaneous ly from a spell, though only 50% su rv ive for one y e a r w i t h o u t a p a c e m a k e r . 13 Although - 90% of these individuals have some sign of heart block (right bundle branch block, LAH, RBBB with LAH or LPH, or left bundle branch block) or surface electrocardiograms, ~4 such findings in an asymptornatic person represent only - 1% per year risk of developing complete heart block.~5
Structural and Other Recognizable Cardiovascular Disorders
In the four large series, 1' 3-5 aortic stenosis, a n g i n a pectoris , and myocard ia l infarction ac- counted for the majority of cases of cardiac syncope that were due to disorders that could be recognized from features evident at presentat ion. Angina pec- toris or myocardia l infarction should certainly be considered if chest discomfort or dyspnea precedes syncope. These cases may otherwise mimic vaso- vaga l syncope since weakness , d iaphores is and n a u s e a may precede the loss of consciousness . Chest discomfort and dyspnea are a lso reported prior to syncope in many cases of aortic stenosis . 4 Although benign causes of syncope are far more common than cardiac syncope in persons under 30, structural disorders accounted for 28 of 29 cases of sudden dea th in young athletes . 16 Hypertrophic cardiomyopathy (14 cases) was most common, fol- lowed by concentric ventr icular hypertrophy (5), anomalous origin of the left coronary artery (3), pre- mature coronary artery d i s ease (3), ruptured aorta
assoc ia ted with Marfan's syndrome (2), and hypo- plastic coronary artery (1). Syncope during or im- mediate ly following physica l exertion a lways sug- ges ts a cardiac disorder. Heart murmurs, if present, should be carefully categorized according to loca- tion, character and radiation, as well as responses to Valsalva and other maneuvers .
The prolonged Q-T syndrome is a rare but rec- ogn izab le and t r e a t a b l e disorder , pr imar i ly of young persons, who may present with loss of con- sc iousness . This condition is heredi tary in deaf mutes but may occur sporadical ly in apparent ly heal thy individuals. Mitral va lve prolapse may be present . Abnormal i t ies on sur face ECGs range from unequivocal Q-T prolongation with T-wave inversion to borderl ine prolongation of the Q-T in- terval (normal rate-corrected Q-T -< 0.44 sec). Some cases are characterized by a slow pulse rate at rest that fails to increase a s expected with exercise, during which the Q-T interval, initially borderline, may become prolonged, or by alternation of the T wave.17 This and other cardiac causes of syncope should be s u s p e c t e d in the appa ren t ly hea l thy young person if there is a family history of sudden death, if the spell occurred during or immedia te ly after extreme physical or emotional exertion, or if the spell (cardiac arrest) includes unusual ly pro- longed unconsc iousness , cyanosis , incontinence and/or multiple seizure-like movements .
Prolongation of the Q-T interval is a lso associ- a ted with electrolyte disorders and drugs, includ- ing quinidine, procainamide, phenothiazines, and tricyclic an t i dep re s san t s , a s well a s other dis- orders. Pat ients may develop spontaneous ly occur- ring ventricular tachycardia with changing elec- trical polarity, rapid rate, and frequent deteriora- t ion into v e n t r i c u l a r f ib r i l l a t ion ( t o r s a d e s de pointes), m This should be suspec ted when pat ients on any of the drugs l isted above exper ience presyn- copal or syncopal spells.
Syncope was the present ing complaint of 13% of a series of pat ients with pulmonary embolism. 18 Several had syncope during a bowel movement, probably re la ted to d iminished pulmonary blood flow during straining in an a l ready compromised patient. In general , loss of consc iousness implies a major or re la t ive ly m a s s i v e e m b o l u s and thus should be assoc ia ted with the history of dyspnea , weakness , pleur isy or hernoptysis, a long with elec- t rocardiographic abnormal i t ies and/or abnormal arterial blood gases .
Carotid Sinus Sensitivity
This form of cardiac syncope occurs almost ex- clusively in the aged and usual ly in those with

JOURNAL OF GENERAL INTERNAL MEDICINE, Volume I (Jan~Feb). 1986
under ly ing hype r t ens ion or a therosclerot ic dis- ease . Loss of consc iousnes s m a y result from a period of asystole, a drop in blood pressure, or both. Spells typically are brief and abrupt if induced by slowing of the pulse (cardioinhibitory type) but may be preceded by weakness , sweat iness , and other autonomic symptoms if related to dec reased blood pressure (vasodepressor type). 4 Twenty-four-hour monitoring in the cardioinhibi tory type revea l s s inus pauses similar to those seen in the sick s inus syndrome.
A posit ive test for carotid s inus sensit ivity con- sists of > 3 seconds of asystole, falls in diastolic and systolic blood pressures of -> 50 mm Hg, or symptoms assoc ia ted with lesser s lowing of the pulse (at least 30%) or decl ines in blood pressure (-> 30 mm Hg). False-posi t ive and fa lse-negat ive tests are reported, part icularly in the elderly, 9' 20, 21 so that test results must be correlated with the history of symptoms. Massage should be done by applying light pressure very briefly over the carotid sinus, only af ter a s c e r t a i n i n g that ca rd iac rhythm is stable, that digitalis toxicity is not present, and that the carotids are pa lpab le and without bruits. The need for caution in performing carotid sinus mas- sage is emphas ized by a report of prolonged asys- tole during test ing in 26% of pat ients with carotid sinus sensitivity. 22
Seizures
Even if a sudden loss of consciousness is tran- sient and unwi tnessed , 23 the d iagnos is of seizure, ins tead of syncope, can still be made from the clin- ical features (Table 2). Loss of consciousness typi- cally occurs without warning. When an aura pre- cedes the seizure it consists of a localized neurolog- ic occurrence, e.g., an olfactory sensat ion, a com- plex visual or audi tory phenomenon, or a "sinking" feeling, and not of the general ized weakness and other premonitory symptoms that often precede fainting. Seizures occur in any posture and at any time, including during sleep. They may be induced by bl inking lights, loud noises , o r monotonous music, but not typically by prolonged s tanding or events assoc ia ted with s imple fainting. The pa- tient's eyes may turn upward or to one side, and wi tnesses may descr ibe a "bounding" pulse, deep stertorous breathing, and cyanosis rather than pal- lor. Fecal as well as ur inary incontinence occurs. Postictal confusion is the most specific feature of seizures and, if documented, excludes the diagno- sis of s imple fainting. Occurrence of an aura or of transient neurologic s igns after convulsions indi- cates the initially part ial na ture of the seizure and is of localizing value.
Transient Cerebral lschemic Attacks (TIAs)
Most TIAs are abrupt in onset and persist for less than 10 minutes. 24 As a rule, they produce focal neurologic deficits rather than al terat ions of con- sciousness. Except for the associa t ion of cardiac arrhythmias with cerebral emboli, t ransient focal neurologic deficits induced by arrhythmias are un- usual, even in pat ients with underlying carotid or ver tebrobasi lar occlusive d isease . 25' 2s There are some situations, however, in which cerebrovascu- lar d i s e a s e may lead to a l tered consciousness . Such condi t ions inc lude b i l a t e ra l ex t r ac ran ia l carot id occ lus ive d i sease , "migra ine syncope ," p o s s i b l y i n d u c e d by v e r t e b r o b a s i l a r a r t e r i a l spasm, and akinetic fainting spel ls of the aged, possibly resulting from transient bra ins tem ische- mia. In some cases , a transient ischemic a t tack may resemble a seizure. Incoherence and confu- sion are prominent manifestat ions. 4 The d iagnos is of these cases may be suspec ted because of accom- panying vertigo, ataxia, al terat ion of vision, and other focal deficits either preceding or following the event, as well as b e c a u s e of the first occurrence of such a spell in an elderly person or someone with underlying atherosclerosis .
Metabolic and Drug-induced Alterations of Consciousness
Hypoglycemia and other metabol ic or drug- induced disorders lead to prolonged al terat ions of consciousness falling into the categories of confu- sion, delirium and coma. Thus, Day's series of 198 emergency room pat ients in whom syncope may have been part of a picture of a l tered consciousness included two pat ients with hypoglycemia, two with hypoca lcemia , and one with hyponat remia . 1 In contrast, Kapoor et al., who excluded all pat ients with coma, shock, cardiac arrest, or seizure, re- p o r t e d no m e t a b o l i c d e r a n g e m e n t s c a u s i n g syncope. 3 Mild or react ive hypoglycemia can be differentiated from syncope by its g radual onset of palpitations, anxiety, sweat ing, and hunger sensa- tions, only rarely progress ing to actual loss of con- sciousness, and by its relat ionship to meals.
Hysteria
Hysterical pat ients may appea r unrespons ive but will not have fainted. Their waxing and waning unrespons iveness genera l ly persis ts much longer than brief syncope. Blood pressure and pulse are unaffected. Prolonged complex partial seizures can a l so p roduce u n r e s p o n s i v e n e s s with una l t e r ed blood pressure and pulse, but in such cases, the e lec t roencepha logram (EEG) is abnormal at the time the pat ient is symptomatic.
54 Branch, APPROACH TO SYNCOPE
DIAGNOSTIC TESTS
The history and physica l examinat ion estab- l ished a d iagnosis in 74% of the 198 cases reported by Day et al.~ Even in pat ients requiring hospital- ization to invest igate the cause of syncope, history and physical examinat ion were reported to estab- lish the d iagnos is in 38%. s
Neurologic Tests
Of 231 pat ients in three series the EEG was impor tant in e s t a b l i s h i n g the d i agnos i s for 22 (9.5%). ~'3 All of these pat ients were a l ready sus- pected of having a seizure disorder or central ner- vous system lesion b a s e d on the description of the spell or the presence of focal neurologic abnormali- ties on examination.~3 Since even s leep-depr ived EEGs of pe r sons with se izures can be normal, whereas abnormal EEGs of persons without known seizures are not rare, it should be emphas ized that the d iagnosis of a seizure should be made from the history.2~ The EEG provides confirmatory evidence.
Computer ized axial tomography of the head (CT scanning) r evea led a pr imary or metas ta t ic bra in tumor or other d iagnos t ic abnormal i ty in seven of 20 cases (35%) of pat ients present ing with syncope whose histories sugges ted a seizure dis- order, or in whom examina t ion r e v e a l e d focal neurologic abnormalities.~ Without such a history or finding, CT scanning provided a d iagnosis of syncope in none of 121 patients. ~-3 Skull films, lum- bar punctures, and cerebral angiography were a lso universal ly unrewarding in the absence of such a history or finding. 2
Cardiac Testing
The surface ECG es tab l i shed the d iagnosis in 16 (4.5%) of 335 cases reported. L 3 Other cardiac t e s t s s u c h a s e c h o c a r d i o g r a p h y a n d c a r d i a c catheterization were diagnost ic only when pat ients were s u s p e c t e d on c l in ical g r o u n d s of hav ing valvular or ischemic heart d isease . The chief ques- tion in syncope, however, is whether to perform cardiac monitoring and/or electrophysiologic test- ing. Monitoring y ie lded a specific d iagnosis not previously es tab l i shed in 40 (14%) of 227 reported cases . ~-3 However , dys rhy thmias not u l t imate ly accepted a s an explanat ion for syncope were found in -50% of these cases . ~' 2 In another series, a mean recording time of 68 hours was required to es tabl i sh a d iagnosis by correlating syncopal symptoms with complex dysrhythmias . 1° In that ser ies a s well as others, no correlation of symptoms with frequent atrial or ventricular premature contractures and/or couplets was revealed.~°" z9 Even ep isodes of ven-
tricular and supraventr icular tachycardia most fre- quently were asymptomat ic . 2g
Intracardiac electrophysiologic s tudies (EPS) induced ventricular tachycardia in 20 (35%) of 57 pat ients with recurrent syncope of suspec ted car- diac etiology but previously negat ive evaluat ions that had included prolonged monitoring and exer- cise testing. 3~' 32 Eighteen of the 20 pat ients had recurrence of the ep i sodes after ant iarrhythmic therapy. In addition, EPS identified five pat ients with sinus node dysfunction, two with prolonged HV intervals, one with increased atrioventricular (AV) nodal refractoriness, one with infraHis block during pacing, and one with atrial flutter induced by atrial stimulation. 3~' 32 In contrast, of 35 pat ients selected after a single ep i sode of unexpla ined syn- cope, none had ventricular tachycard ia induced by EPS, the findings being limited to induced SVT or p r o l o n g e d s i n u s n o d e r e c o v e r y t ime in s ix patients. ~ Whereas it is genera l ly be l ieved that induction of sus ta ined or nonsus ta ined ventricular tachycardia occurs in only a very small proportion of normal subjects 31 and, therefore, usual ly repre- sents a posit ive finding in pat ients be ing s tudied for symptoms, 3 the signif icance of other findings uncovered during EPS is less certain. EPS es tab- l ished the d iagnosis in only three (13%) of 23 cases se lected for s tudy in Kapoor's series, which in- cluded all pat ients present ing with syncope. 3
Casse t t e recording and te lephone monitoring are ava i lab le at some institutions. These systems, which require activation by the patient, record car- diac rhythm, usua l ly for 30 seconds. They a l low observat ion of the pat ient for a prolonged period and are present ly cheaper than 24-hour monitoring at our institution. The pat ient must have sufficient warning prior to the spell and be sufficiently coop- erative to trigger the casse t te or dial the te lephone system.
DIAGNOSTIC APPROACH
The first s tep in es tabl i sh ing the d iagnosis is to ascer ta in that p resyncope or syncope is in fact the chief complaint. These must be dis t inguished from vertigo, best descr ibed as the illusory sense of mo- tion. Several other categories of symptoms can be recognized. Disequil ibrium is perhaps best defined as imbalance. Like vertigo, it usual ly is related to a neurologic condition, such as parkinsonism, cere- bel lar a taxia , or mult iple sensory deficits, e.g., ca ta rac ts p lus d imin ished posi t ional sensat ion. The terms " l igh theadedness" or "giddiness" are more difficult to categorize. These symptoms most commonly reflect hyperventi lat ion; the patient may descr ibe them as similar to the sensa t ion of mild alcoholic intoxication or to being slightly off ba-

JOURNAL OF GENERAL INTERNAL MEDICINE, Volume I (Jan/Feb), 1986 55
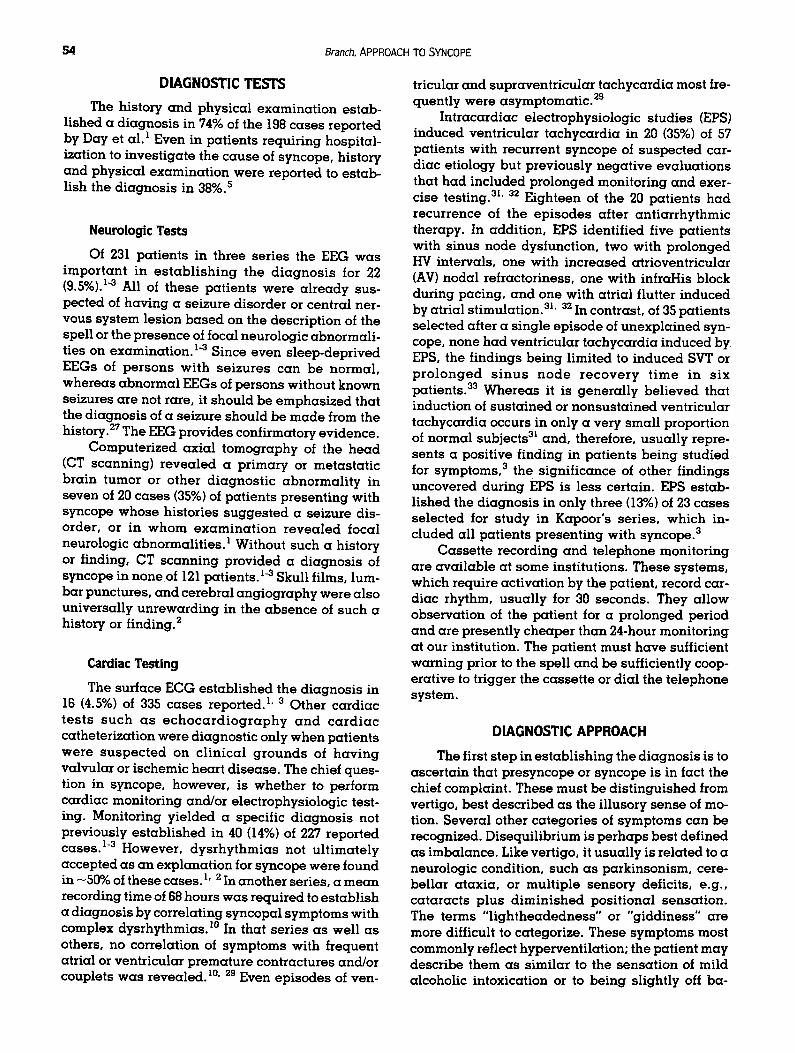
FIGURE 1. General guidelines for an approach to patients with syncope. (Reproduced by permission, from Branch WT, ed., Office practice of medicine, Philadelphia: W. B. Saunders.)
I A L L PATIENTS I
Diagnosis 8uspawcted by history:
SOitores
metobelic disorders/drag toxicity
transient ischemic attacks
postmi¢furot~on syncope
post* tuusive syncope post I ~ n syncopo
hyper venti lation- induced
hysterio
synCOpe related to myoCordioI inforctk)n or ong i~ pectOris
pulmonary emlH)llsm
dissecting onour yam
Oiognosis 8vlH~cted by complete physical ( including nouroloqlic ) eneminotk)n :
¢Orotid sinus sensitivity
aortic stenouil, IHSS, other structural cordlo¢ abnormalities
pulmOnory hypertension
sukClovion stool primary or.metastatic brain tumor
orthoetot~ hypofoneioa
Diagnostic or Thoropeut!c,,,.Considetations
• [ [G0 CT icon, ontieeizure medication
• blood glucose, electrolytes, BUN, ca lc ium.ar ter ia l blood 90USS, drug levels
• noninvasive l is t ing or cerebral ongiogrophy, ontiplotelet or anticoagulant therapy
• reproduce symptoms by voluntary hyperventi lot ion
• psychotherapy
• [ C G. exercise testing, hospitalization
• Iupg scanning Or bi lateral venogrophy • c h i l i f i lm. angiogrophy or chest CT scanning
with contrast
• carotid sinus lasting in clearly and those with unClOr lying otherosclero$is
• echOcOrdiogrom
u chest fi lm
• heed CT se:onning • CBC, BUN, electrolytes, adrenal testing, treating with
pressure i tockiogs, mineJrolocorticoids, sympothomimet ic agents "r
RqH~linin9 pOthlnts : ]
Chief ly : vOsovogat vs unkc'~own us suspected cardiac syncope
Hqlh I~ish :
OIl with suSpocted ¢OrdiO¢ syncope:
mcivstOra of spoils. without wornin 9
or syncope in recumbency
~r • compl icated" hypol i¢ spell
of spells accompanied by polpi totwns. chest pain dyspn44, end/or abnormal (CG
Intermediate Risk : bow Risk :
not suspected cardiac syncope oge ~ 30 years bet post history cardiac disease with no post h is tory
or or suspected cardiac syncope age Z 30 but ~ 70 o r with unknown syncoge oge ~.. 7 o
or with suspected v o c o q o l syncope age ~ "tO
lance without moving or fall ing in a s ingle direc- tion. Unlike vertigo, "giddiness" usual ly does not start or stop abruptly, and is not reproduced by the Barany or other posit ional maneuvers . Unlike pre- syncope, it is not perceived as "blacking out" or fainting, and it usual ly persists, somet imes inter- mittently, for many minutes to hours. Exact repro- duction of this sensat ion by voluntary hyperventila- tion provides the best diagnost ic maneuver.
Once it is es tabl i shed that a patient has syn- cope or presyncope, the first step is to identify the pathogenes i s if poss ib le from the history, physical examination, and routine tests. An ECG is general- ly obtained. Drug levels, electrolytes, and other tests may be obtained at the initial visit when pro- longed confusion or other alteration of conscious- ness sugges t s a metabol ic or drug-induced dis- order. Many types of syncope , inc luding post-
tuss ive , postmictur i t ion , and those c a u s e d by structural cardiovascular abnormalit ies and sei- zures, can be recognized, and their treatment, if indicated, can be initiated at the first visit (see Fig. 1). Thirty to 53% of patients in two relatively un- selected series were in these categories. L 4
Patients who do not fall into these categories may be classified, on the bas i s of clinical data, as having v a s o v a g a l syncope, syncope of unknown cause, or cardiac syncope due to dysrhythmias. In approaching these patients, the clinician will prob- ably consider one of three diagnost ic strategies: clinical follow up without further testing; obtaining a s ingle 24-hour monitoring; or prolonged monitor- ing plus consideration of addit ional tests such as exercise testing, EPS, and cassette recording.
As sugges ted by Day et al. , l the most rational choice of a diagnost ic strategy probably depends

$6 Branch, APPROACH TO SYNCOPE
upon a careful assessment of risk. It is a s sumed that vasovagal syncope carries a good prognosis. Conversely, death occurred within a year in 18.5 to 30% of p a t i e n t s wi th c a r d i a c s y n c o p e in two series.S, s Thus, pat ients with any feature of cardiac syncope (Fig. 1) are considered to be at high risk. By definition, the remaining patients have only brief losses of consciousness, with onset of symptoms in the upright or sitting posture, followed by rapid recovery. Although there is no "gold s tandard" for identifying vasovagal syncope, spells with these characteristics that also occur in a typical sett ing or in associat ion with typical premonitory symptoms of vasovagal syncope should probably be consid- ered to have this diagnosis . Lacking such a sett ing or premonitory symptoms, syncope is considered to be of unknown cause.
Prolonged monitoring, perhaps during hospi- ta l izat ion, a p p e a r s i nd i ca t ed for pa t i en t s sus- pected of having cardiac syncope due to dysrhyth- mias, i.e., the high-risk group (Fig. 1). If syncope is recurrent and a cardiac pathogenet ic mechanism remains strongly suspec ted but cannot be con- firmed by prolonged monitoring, then EPS, casset te recording, and/or other tests are also indicated.
It seems possible to identify a group of patients at low risk by considering age and past history in addit ion to clinical features (Fig. 1). Those under the age of - 70 years with features of vasovagal syncope and no past history of cardiac disease, along with those under the age of - 30 years with syncope of unknown cause and no past history of cardiac disease, are probably at low risk. Support for this conclusion exists in the da ta of Day et al. Roughly 50% of their 198 patients were in these categories, and they accounted for only - 1% of poor outcomes per year and no poor outcomes caused by dysrhythmias. 1 The most reasonable di- agnostic strategy for such patients is probably clin- ical follow up without further testing. Assuming a cost of - $300 for three 24-hour monitorings, and assuming, despite the inherent diagnostic impreci- sion, that three studies would yield an accurate diagnosis, the cost of making a single diagnosis by monitoring pat ients at 1% risk of cardiac syncope would be - $30,000. This cost would be reduced to $3,000 per diagnosis if, without excluding patients with this problem, the clinician could select for prolonged monitoring pat ients who have an inci- dence of cardiac syncope as high as 10%.
There remains a group of pat ients who are probably best cons idered at intermediate risk. Although the criteria are somewhat arbitrary, it seems best to include in this group all patients not at high risk who are above the age of - 70 years, and those at any age with a past history of cardiac disease. Patients with syncope of unknown cause
who are between - 30 and - 70 years of age may also be included in this group. The ass ignment of intermediate risk to pat ients with syncope of un- known cause more than 30 years old cannot be based on da ta (Day et al. 's intermediate-risk group with 16% poor outcomes included syncope caused by neurologic and metabolic disorders as well as syncope of unknown causel), but is based on the judgment that vasovaga l syncope can usual ly be recognized clinically, and that da ta are lacking to show that pat ients > 30 years of age with unknown syncope are at low risk. It seems most reasonable to suggest that the approach to patients in this group be individualized. For example, exercise testing may be the first test indicated when an older person has syncope that is preceded by weakness and di- aphoresis, where the first priority may be to distin- guish vasovagal from ang ina pectoris-related syn- cope. In other cases, only especial ly careful clinical follow up may be warranted. For many patients at intermediate risk, however, obtaining a single 24- hour monitoring seems appropriate. This estab- lishes a noncardiac diagnosis if symptoms recur during regular sinus rhythm. Finding complex dys- rhythmias without symptoms is difficult to assess, but may be an indication for more frequent follow- up visits and/or addi t ional monitoring. Recurrent but infrequent spells preceded by warning symp- toms may indicate use of a casset te or telephone- recording system.
THERAPEUTIC ISSUES
Antiarrhythmic Therapy In general, ant iarrhythmic therapy is not indi-
cated for pat ients with syncope until a cardiac etiol- ogy is es tabl ished by correlating symptoms with dysrhythmias demonstra ted by monitoring. Clini- cians may be tempted at t imes to prescribe a "trial" of an t ia r rhythmic therapy. If spells occur infre- quently, such " t r ia ls" are difficult to interpret, whereas the relationship of frequently occurring spells to dysrhythmias can be determined by more pro longed moni tor ing or by casse t t e recording without resorting to a "trial." There are addit ional reasons to avoid ant iarrhythmic therapy in the ab- sence of an es tabl ished diagnosis. Procainamide, quinidine, and disopyramide commonly produce side effects and, therefore, are difficult to mainta in as long-term therapy. 34" 3s This was il lustrated in one study in which procainamide had to be discon- t inued within six months in 50% of pat ients because of side effects. 35 The efficacy of antiarrhythmic ther- apy to prevent sus ta ined arrhythmias is also diffi- cult to assess, since a single 24-hour monitoring showing increased or decreased numbers of ex-
JOURNAL OF GENERAL INTERNAL MEDICINE. Volume I (Jan/Feb), 1986 57
trasystoles is often misleading in this regard. 36 Of more concern are the hazards of antiarrhythmic therapy. In a careful study of patients referred for treatment for serious ventricular arrhythmias, a fourfold increase in ventricular extrasystoles, a tenfold increase in repetitive forms, and/or first- time production of sustained ventricular tachycar- dia followed adminis t ra t ion of antiarrhythmic agents in 5.9 to 15.8% of patients (drugs and inci- dences of exacerbated arrhythmias were: quini- dine 15.4%, proca inamide 9.1%, d isopyramide 5.9%, propranolol 14.6%, metoprolol 7.1%, aprin- dine 11.3%, mexiletine 7.6%, tocainide 15.8%, pin- dolol 14.6%37).
The patients in this study were undoubtedly predisposed to ventricular dysrhythmias by their underlying heart disease and, hence, may have been more likely to suffer provocation of such dys- rhythmias than the average patient receiving anti- arrhythmic therapy. In other settings, such as treat- ment of sustained atrial fibrillation, atrial flutter, or supraventricular tachycardia with digoxin, beta- blockers, or quinidine, antiarrhythmic therapy may be less hazardous. Although treatment should al- ways be initiated cautiously, prolonged hospi- talization to assess its initial efficacy may not be necessary. Treatment of complex ventricular dys- rhythmias is more problematic. Survivors of acute myocardial infarction have a higher incidence of sudden death when complex ventricular dysrhyth- mias accompany an ejection fraction of less than 40%. 38 Clinicians are certainly more inclined to treat complex ventricular dysrhythmias under this circumstance or, at least, in the presence of clini- cally active ischemic heart disease. Beta-blockers are well known to prolong survival in the year fol- lowing myocardial infarction. No randomized trial, however, has proved that survival is enhanced in any group of patients because of antiarrhythmic therapy, per se. There are uncontrolled studies in- dicating reduction of symptoms of patients with the p ro longed Q-T synd rome t r ea t ed with be ta - blockers, 17 syncope caused by supraventricular tachycardia, 1° recurrent syncope, who had ven- tricular tachycardia induced by EPS, 31' 33 and life- threatening ventricular dysrhythmias, treated with empir ica l ly se l ec t ed effect ive ant iar rhythmic drugs. 39 When syncope is possibly but not proved to be caused by ventricular dysrhythmias, and there is no other reason to treat, it seems generally best to withhold antiarrhythmic therapy until prolonged monitoring and/or other studies clarify the rela- tionship of the dysrhythmias to symptoms. Treat- ment can then be instituted under controlled cir- cumstances, allowing selection of the empirically determined optimal antiarrhythmic program for each patient.
Pacemaker Implantation
Pacemaker implantation carries a small risk and requires prolonged follow up and, thus, is usually indicated only when heart block or symp- tomatic bradycardia or sinus pauses are demon- s t rable by monitoring. Recurrent syncope was terminated by pacemaker implantation in some cases in which heart block was suspected but its infrequent occurrence prohibited documentation by monitoring.4° Cassette recording and EPS to pro- voke heart block during rapid atrial pacing or other maneuvers offer alternative methods to establish the diagnosis before resorting to pacemaker ther- apy. Pacemakers do prolong survival of patients with comple te heart block. 13 Avai lab le data , however, demonstrate the need for careful clinical evaluation to exclude other causes of syncope in patients suspected to have heart block. Even those with bifascicular block on surface ECG are more likely to have syncope because of factors other than heart block, e.g., seizures or orthostasis.15" 41 Like- wise, after pacemaker implantation, patients with sick sinus syndrome frequently continue to experi- ence "dizziness" related to comorbid conditions such as ischemic heart d isease and congestive heart failure. 42 Such patients usually succumb to their comorbid conditions, so that pacing has not clearly been shown to prolong their lives. 42" 43
Other Management Issues
Even benign types of syncope represent a se- rious threat to elderly persons because of the dan- ger of hip fractures and other injuries produced by falling. Multiple factors frequently are related to loss of consciousness in the elderly. 9 For example, orthostatic hypotension occurs in many otherwise normal aged persons; many are on drugs with anti- cholinergic properties that also induce orthostasis; subclinical coronary artery disease, aortic steno- sis, chronic lung disease, and cardiac conduction a b n o r m a l i t i e s a re f r equen t ly present , whi le baroreceptor responses are often sluggish in the elderly. 9 Establishing the relationship between dysrhythmias and syncope is particularly prob- lematic in the elderly. Monitoring of seemingly healthy persons 75 years of age or older revealed sinus bradycardia in 10%, atrial fibrillation in 11%, ventricular irritability in 42%, and nonsustained ventricular tachycardia in 4%.44 None of these dys- rhythmias correlated with symptoms. Thus, it is difficult to distinguish contributing factors from in- cidental findings in elderly persons with syncope. Predisposing factors that coexist with syncope should be corrected whenever possible. It may be necessary to decrease doses of antihypertensive and other medications, to correct underlying ane-

58 Branch, APPROACH TO SYNCOPE
mia, dehydration or infection, or to refer the patient to a physical therapist for training in using a cane or walker. Advice to avoid standing too quickly often needs reiteration. A home visit to remove "throw rugs" and rearrange furniture to avert trip- ping may be useful. Primary orthostasis can be lessened by wearing support stockings or s leeping with the head of the bed elevated on blocks, as wel l as by eliminating diuretic therapy if it is not essen- tial. When the exact cause of syncope is not estab- l ished initially, a period of observation with correc- tion of identif ied predispos ing factors is often appropriate. When symptoms recur in such pa- tients, careful review of all clinical features often leads to the diagnosis .
REFERENCES 1. Day SC, Cook EF, Funkenstein H, Goldman L. Evaluation and outcome of
emergency room patients with transient loss of consciousness. Am J Med 1982;/5:15-23
2. Kapoor WN, Karpf M, Maher Y, et al. Syncope of unknown origin. The need for a more cost effective approach to his diagnostic evaluation. JAMA 1982.24"7.2687-91
3. Kapoor WN, K,3rpf M, Wieand S, et al. Prospective evaluation and followup of patients with syncope. N Engl J Med 1983.309:197-204
4. Wayne HH. Syncope. Physiological considerations and analysis of the clinic characteristics in 510 patients. Am J Med 1961 '30:418-38
5. Silverstein MD, Singer DE, Mulley AG. et aL Patients with syncope admitted to medical intensive care units. JAMA 1982"248:1185-89
6. Zeigler MG, Lake CR, Kopin IJ. The sympathetic nervous system defect in primary orthostatic hypotension. N Engl J Med 1977-296.293-7
7. Caird FI, Andrews GR, Kennedy RD. Effect of posture on blood pressure in the elderly. Br Heart J 1973.35:527-30
8. MacLennan W J, Hall MRP, Timothy JI. Postural hypotension in old age: is it a disorder of the nervous system or of blood vessels? Age Aging 1980;9.25-32
9. Lipsitz LA. Syncope in the elderly. Ann Intern Med 1983;99:92-105 10. Van Durme JP. Tachyarrhythmias and transient cerebral Jschemic
attacks. Am Heart J 1975;89:538-40 11. Sauerwein HP, Roos JC, Becket AE, et aL The sick sinus syndrome. Acta
Med Scand 1976;199:467-73 12. Pomerantz B, O'Rourke RA. The Stokes-Adams syndrome. Am J Med
1969;46:941-60 13. Edhags O, Swahn A. Prognosis of patients with complete heart b~ock or
arrhythmia syncope who are not treated with pacemakers. Acta Med Scand 1976-200:457-63
14. Lasser RP, Haft JI, Fdedberg CK. Relationship of right bundle branch block and marked left axis deviation (with left parietal or peal-infarction) to complete heart block and syncope. Circulation 1968'37:429-3,7
15. McAnulty JH, Rahimtoola SH, Murphey E, et aL Natural history of "high risk" bundle branch block. Final report of a prospective study. N Engl J Med 1982.30"7:137-43
16. Maron B J, Roberts WC, McAIlister HA, et aL Sudden death in young athletes. Circulation 1980~2.218-29
17. Thames MD, Alpert JS, Dalen JE. Syncope in patients with pulmonary embolism. JAMA 1977-238.2509-11
18. Schwartz P J, Pedti M, Malianti A. The long Q-T syndrome. Am J Cardio] 19/5;89'378-90
19. Karen A, Tzivoni D, Garish D, et at. Etiology, warning signs and therapy of torsade de points: a study of 10 patients. Circulation 1981 ,~:}4:1167- 74
20. SmJddy J, Lewis HD Jr, Dunn M. The effect of carotid massage in older men. J Gerontol 1972.~7"209-11
21. Mankikar GD, Clark ANG. Cardiac effects of carotid sinus massage in old age. Age Aging 19/5;4:86-94
22. Trout HH, Brown LL, Thompson JE. Carotid sinus syndrome: treatment by carotid sinus denervation. Ann Surg 1979;189:575-80
23. Hughes JR, Drechman DA. Dizziness, epilepsy and the EEG. Dis Nerv Sys 19?7.38:431-5
24. Pessin MS, Dunean GW, Mohr JP, et aL Clinical and angiographic features of carotid transient ischemic attacks. N Engl J Meal 1977-296"358-62
25. Walter PF, Reid SD Jr, Winger NK. Transient cerebral ischemia due to arrbythmia. Ann Intern Meal 1970;72:471-4
26. Reed RL, Siekert RG, Meddeth J. Rarity of transient focal cerebral iscbemia in cardiac dysrhythmia. JAMA 1973-223:893-5
27. Mansan CA: Factors related to the occurrence of typical paroxysmal abnormalities of the EEG records in epileptic patients. Epilepsia 1 gTO; 11.361 -
28. Clark P[, Glasser SP, SPOto E, etaL Arrhythmias detected by ambulatory monitoring. Lack of correlation with symptoms of dizziness and syn- cope. Chest 1980;77:722-5
29. Zeldis SM, Levine B J, Michelson EL, et aL Cardiovascular complaints: correlation with cardiac arrhythmias on 24 hour electrocardiographic monitoring. Chest 1980;78:456-62
30. Morady F, Scheinman MM, Hess DS, etal. Electrophysiologic testing in the management of survivors of out-of-hospital cardiac arrest. Am J Cardiol 1983;51:85-89
31. Hess DS, Morady F. Scheinman MM. Electrophysiologic testing in the evaluation of patients with syncope of undetermined origin. Am J Cardiol 1983;50:1309-15
32. DiMarco JP, Garan H, Harthorne JW, et al. Intracardiac electrophysio- logic techniques in recurring syncope of unknown cause. Ann Intern Med 1982;95:542-8
33. Gulamhusein S, Naccarelli GV, Ko FT. et al. Value and limitations of clinical electrophysiologic study in assessment of patients with unex- plained syncope. Am J Med 1982;73:700-5
34. Warnowicz MA, Denes P. Chronic ventricular arrhythmias: comparative drug effectiveness and toxicity. Progr Cardiovesc Dis 1980-23-225-36
35. Kosowski BD, Taylor J, Lown B, et at. Long term use of procainamide following acute myocardial infarction. Circulation 1975;47:1204-10
36. Morganroth J, Michelson EL, Horowitz LN, et al. Limitations of routine long-term electrocardiographic monitoring to assess ventricular ectopic frequency. Circulation 1978;58:408-14
37. Velebit V, Poddd P, l.own B. Aggravation or provocation of ventdcular arrhythmias by antiarrhythmic drugs. Circulation 1982,~5:886-94
38. Schulze RA, Strauss HW, Pitt B. Sudden death in the year following myocardial infarction. Relation to ventricular premature contractions in the late hospital phase and left ventdcular ejection fraction. Am J Med 1977,~Z:192-99
39. Lown B. Sudden cardiac death: the major challenge confronting contem- porary cardiology. Am J Cardiol 1979;43"313-28
40. deBooo DP, Wadow CP, Hyman NM. Cardiac rhythm abnormalities in patients presenting with transient non-focal neurological symptoms: a diagnostic grey area. Br Med J 1982.284:1437-9
41. Dhingra RC, Denes P, Wu D, et aL Syncope in patients with chronic bifescicular block Significance. causative mechanisms, and clinical im- plications. Ann [ntern Med 1974;81.302-6
42. Wohl A J, Laborde J, Atkins JM, etaL Prognosis of patients permanently paced for sick sinus syndrome. Arch Intern Med 19"76;136:406-8
43. Gann D, Tolentino A, Samet P. Electrophysiologic evaluation of elderly patients with sinus bradycardia; a long-term follow-up study. Ann Intern Med 19"79;~.2A-9
44. Carom A J, Evans KE, Ward DE, et al. The rhythm of the heart in active elderly subjects. Am Heart J 1980;~:598-603
45. Martin GJ, Adams SL Martin HG, et aL Prospective evaluation of syncope. Ann Emerg Med 1984;13:499-504.
DEMENTIA IN THE ELDERLY
Although accurate prevalence rates are difficult to determine, as many as 10-15 per cent of persons over age 65 may have cognitive impairment. In our next issue Eric B. Larson, Bernard Lo, and Mark E. Will iams emphas ize thorough, careful, and compass ionate care. Watch for the March/April Clini- cal Review, "Evaluation and Care of Elderly Patients with Dementia."