Embed Size (px)
Citation preview

Approaches and planning inApproaches and planning inskull base surgeryg y
Alexis Bozorg Grayeli, Michel Kalamarides,g y , ,Didier Bouccara, Françoise Cyna-Gorse &
Olivier SterkersOlivier SterkersOtoneurosurgery and Radiology DepartmentsHôpital Beaujon Université Paris 7 FranceHôpital Beaujon, Université Paris 7, France
1960 19801960-1980:Rationalizing the skull base approaches
Willi H Middl i l f d• William House : Middle cranial fossa andtranslabyrinthine approaches
Re introduction of already described approaches– Re introduction of already described approaches– Microdrill
Surgical anatomy– Surgical anatomy– Mortality reduction from 20% to less than 5%
House WF, Laryngoscope, 1961, 71:1363House WF, Archives Otolaryngol, 1964, 80:752
House WF Luetje CM In: Acoustic tumors 1979House WF, Luetje CM, In: Acoustic tumors, 1979

1960-1980:1960 1980:Rationalizing the skull base approaches
Ugo Fisch : Infratemporal aproachesUgo Fisch : Infratemporal aproachesExtradural aproaches of the lateral cranial baseFisch U, In: Microsurgery. Applied to Neurosurgery, 1969
Fisch U, Mattox D, In: Microsurgery of the skull base, 1988
A B CA B C
1960-1980:1960 1980:Rationalizing the skull base approaches
• Retrosigmoid approach : – Otogical principals added to aOtogical principals added to a
« neurosurgical approach »– Hearing preservation especially in NF2Brémond G, Garcin M, Magnan J. Cahiers d’ORL, 1974Sterkers JM, Corlieu P, Hamann FK, Sterkers O. Ann Oto
Laryng, 1980
• Transotic and transcochlear approaches :approaches :– Particular situationsHouse WF, Hitselberger W. Archives Otolaryngol, 1976Jenkins HA, Fisch U. Am J Otol, 1980

Surgical objectives
Zero mortality and morbidity Total tumor removalFacial and caudal nerve preservationHearing preservationHearing preservation
Planning and pre operativePlanning and pre operativework-upwork up
Evaluating the pre opertive deficitsAssessing the size, the location and the agressiveness of the lesiong

Preop symptomes and tumor locationPreop symptomes and tumor location
A H d hPetroclival : SNHL, VII, V
Apex : Headaches
Estachian tube: Serous Otitis media
Labyrinthe and middle ear:
CPA: Retrococh SNHL, vertigo
Labyrinthe and middle ear:vertigo, mixed HL
Endolymphatic sac: Fluctuating
Foramen lacerum: aspiration
y p gSNHL, vertigos
Foramen lacerum: aspiration,hoarsness, SNHL
Clinical preop deficits
• Interrogation• Otoscopy• Otoneurological examination:Otoneurological examination:
– VII : Facial motricity, ShirmerV : Blink reflex– V : Blink reflex
– Cerebellar syndrome C d l l l l d– Caudal nerves: velar palsy, vocal cordeand pharyngeal mobility, stroboscopy

Audiovestibular examinationAudiovestibular examination
ImagingImaging
CT• CT scan:– Overlaping slices or spiral acquisition
B i d ith t t t i j ti– Bone window without contrast injection– Axial and coronal views
Study of Bony structures– Study of Bony structures• MRI:
T1 without (lipomes) and with gadolinium injection– T1 without (lipomes) and with gadolinium injection– T2 (acousticofacial bundle in CPA)
Diffusion (B1000 cholesteatoma)– Diffusion (B1000, cholesteatoma)– Angio MRI

I iImagingAngiography:Angiography:
Hypervascularized lesions (paragangliomas, some meningiomas)g )Tumor pedicules (embolisation ?)Willis polygoneygCarotid occlusion testEmbolisation 24-48 h before surgery
Octreoscan® (indium In-111 pentetreotide) : paragangliomasBone scan and et thoraco abdominal CT scanBone scan and et thoraco-abdominal CT scan:metastases and malignant lesions
Evaluating the tumor locationEvaluating the tumor location
SupralabyrinthineApical Infralabyrinthine
R t l b i thiTranslabyrinthine RetrolabyrinthineTranslabyrinthine

Supralabyrinthine ApexInfralabyrinthineSupralabyrinthine pInfralabyrinthine
Translabyrinthine Retrolabyrinthine Cervicomastoid
Paragangliomas:g gFisch classification
Intracranial:
• De (extradural):- De1 < 2 cmDe1 < 2 cm- De2 > 2 cm
C2C3
• Di (intradural):- Di1 < 2 cm
Di2 > 2BC1C2C3C4- Di2 > 2 cm

Tumor extension following cell tracts
Post. supra-labyrinthine
Translabyrinthine
Post. supra labyrinthine
Ant supra-labyrinthine
Precochlear
Anterior infra-labyrinthine
Posterior infra-labyrinthine
Evaluating the tumor type and aggressiveness
TOP FIVECholesteatomaCholesterin granulomaP liParagangliomaSchwannomaMeningioma

Imaging of cholesteatomaImaging of cholesteatoma
CT scan:Lytic and convex edgesIn density similar to CSF
MRI:Hyposignal on T1Hyposignal on T1Variable signal on T2Not enhaced after godoliniumNot enhaced after godoliniumHypersignal on diffusion

B 1000
Imaging of cholestrin granuloma
Benign cyctic lesionsCT scan:
Round and regular marginsRound and regular marginsIn density similar to brain
MRI:Hypersignal on T1 and T2ype s g a o a dVariable homogeneity

Imaging of paraganglioma
CT-scan:F b iFuzzy bone erosion
IRM:H i l T1Hyposignal on T1Hypersignal on T2 (variable)Pepper and salt image: vessel voids andPepper and salt image: vessel voids andhemorrhage hypersignal Intense enhancementIntense enhancement
Angiography: highly vascularised OctreoscanOctreoscan

Imaging of the temporal bone Swartz JD Harnsberger HR Thieme

Imaging of schwannomas
• CT-scan:L t d– Located on a nerve
– Regular enlargement of nerve foramenBone erosion with regular margins– Bone erosion with regular margins
• MRI:Hyposignal on T1– Hyposignal on T1
– Isosignal on T2– Cystic components in large lesions– Cystic components in large lesions– Enhancement after contrast– « Bell clapper » forme« Bell clapper » forme

Imaging of meningiomes
CT-scan:HyperostosisBone erosionBone erosion
MRI:Intermediate signal on T1variable signal on T2Thinckening and enhancement of dura

Location can indicate pathologyp gy
CholesteatomaCholesteatoma,Cholesterin granuloma Meningioma
F i l h
SchwannomaMeningioma
Facial schwannomaCholesteatomaCholestrin granuloma
Endolymphatic sac tumorMeningiomaHistiocytosis X
Foramen lacerum: ParagangiomaCaudal nerve schwannomaCaudal nerve schwannoma
Evaluating nerve location andEvaluating nerve location andinvolvement
MRI 3D reconstructionMRI T2 with multiplanar reconstruction MRI 3D reconstructionSuperior view
p

P ti t fPreoperative assessment ofvascularisationvascularisation
Tumor vesselsArteriesVenous drainage: sigmoid sinus hypoplasia, Labbé vein
Computer assisted navigation
More user-friendlyM iMore precise
Useful in retrosigmoid: locatin of the posterior semicircular canal
Useful in MCF approachpp

L t l k ll b hLateral skull base approaches
Enlarged middle cranial fossa
Transotic
Transcochlear
Translabyrinthine
Transotic
Retrolabyrinthine
Translabyrinthine
Retrosigmoid
I t ll tiInstallation

Intra operative monitoring
Facial :Improves the quality and the
reliability of dissectionAccelerates learning curveAccelerates learning curve
Hraring:No impact on hearingNo impact on hearing
preservation
C d lCaudal nerves: :In large VS and paragangliomas
Translabyrinthine approachTranslabyrinthine approach
Lateral cranial base approach trough the posterior labyrinth
Indications:Indications:
Translabyrinthine and large CPA lesions
Lesions invading the fundus of IAMo
Class C or D hearing

Transotic approachTransotic approach
Anterior extension of the translabyrinthine approachtranslabyrinthine approach
Indications:
Translabyrinthine and largeTranslabyrinthine and largeCPA lesions extending anteriorly
Lesions invading theLesions invading thefundus of IAM and cochlea
Class C or D hearing

Transotic approachTransotic approach
E L t l R t d lE. Lescanne et al., Rapport de laSociété Française d’ORL, 2001
T hl hTranscochlear approach
Posterior rerouting of the facial nervefacial nerve
Indications:
Apical lesions with class C or D hearingor D hearing
Lesions located anterior to the IAM

Retrosigmoid approachRetrosigmoid approachIndications:
Mid-size CPA lesionsClass A or B hearingClass A or B hearingFundus free of tumorCan be combined to mastoid-retrolabyrinthine
Drilling the posteriorIncisionaspect of IAM
3 cm23 cmcraniotomy
Retrosigmoid approach
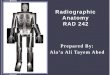
Middle cranial fossa approachMiddle cranial fossa approachIndications:d cat o s
Supralabyrinthine lesionsIAM or small CPA lesions notIAM or small CPA lesions not
involving the fundusClass A or B hearing
Vertical incision � from tragus upward� from tragus upward� < 1 cm from helix insertion
Bone flap: 3 x 3 cm
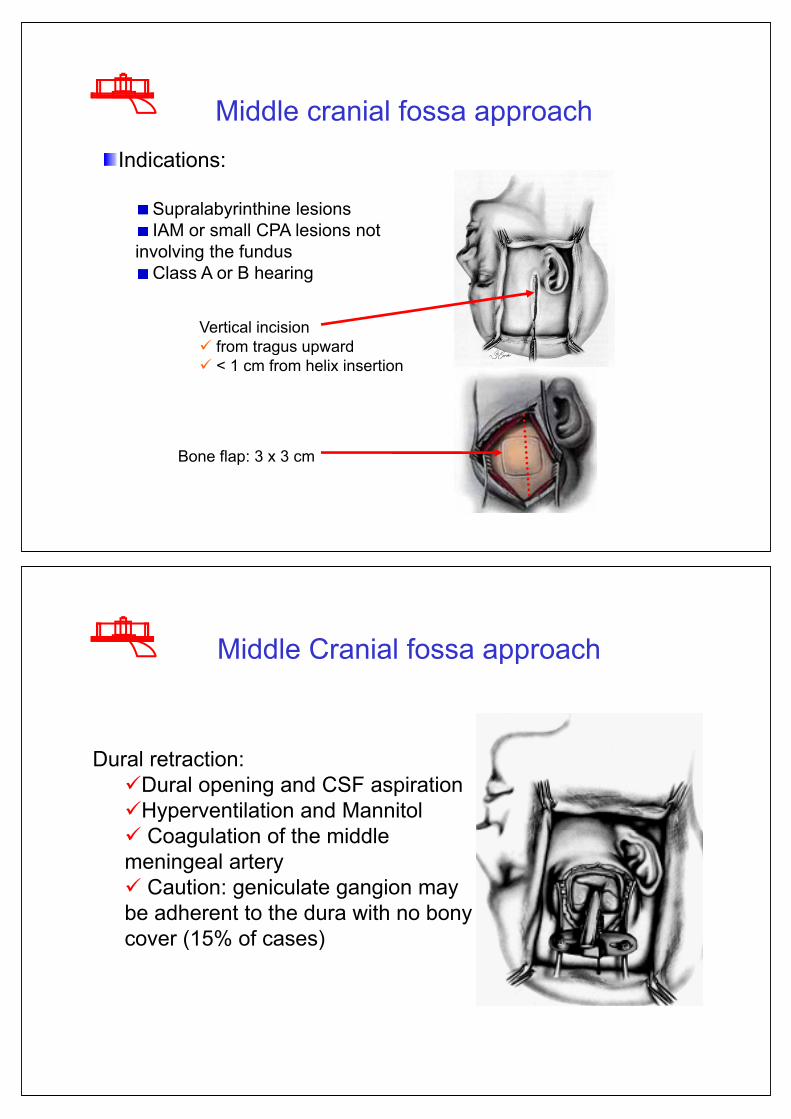
Middle Cranial fossa approachMiddle Cranial fossa approach
Dural retraction:�Dural opening and CSF aspiration�Hyperventilation and Mannitol� C l ti f th iddl� Coagulation of the middlemeningeal artery� Caution: geniculate gangion may� Caution: geniculate gangion maybe adherent to the dura with no bony cover (15% of cases)

Middle Cranial fossa approachMiddle Cranial fossa approach
Front
Middle cranial fossaMiddle cranial fossa
� Identification of MAI:
E i i tEminancia arcuata
Greater petrosal nerveGreater petrosal nerve
� MAI on the bisecting line
�Measuring the depth from the24 mm 27 mm
�Measuring the depth from theinternal diploe

Infratemporal approachesIndications:
Paragangliomas other aggressive tumors:
A: Foramen lacerum and C1
A B C
A: Foramen lacerum and C1segment of carotid
B: Petrous apex and C2 tsegment
C: Rhinopharynx, petroclival junction, cavernous sinus
Can be combined translabyrinthine approach
Type A Type B anterior rerouting of facial nerve
ypTrijeminal sacrifice

Type C Condylar section and trijeminal sacrificeCondylar section and trijeminal sacrifice
Preoperative deficits and signsGeneral status
Imaging
Apical Infralabyrinthine Supralabyrinthine Retrolabyrinthine Translabyrinthine
Hearing
+ - + - + -+ -
SP TO STP SP TOTORLTO SP ou TOSP TO STPor ITA
SP TOTORLTO SP ou TO
ComplicationsComplications
• Keratitis• Keratitis• CSF leak
I f ti i t i i iti• Infectious: respiratory, urinary, meningitis• Pulmonary embolism• CPA hematoma• Stroke, lateral sinus thrombophlebitisp• Carotid artery dissection and hemorrage
(paragangliomas)(p g g )
Immeiate postoperative careImmeiate postoperative care• ICU for 24 – 48 h• No systematic antibiotics• Prevention of phlebitis• Prevention of phlebitis• Eye care• Prevention of cough and constipation (CSF hypertension)
• Early facial and vestibular rehabilitationy• In case of caudal nerve deficit:
– Speech therapistSpeech therapist– Nasogastric tube or gastrostomy– Tracheotomy– Tracheotomy

Late postoperative careLate postoperative care
• Ophtalmological follow-up and facial h i thphysiotherapy
• Facial nerve rehabilitation: eyelid surgery,y g y,muscular transposition, 7-12 anastomosisVestibular rehabilitation• Vestibular rehabilitation
• Hearing rehabilitation (BAHA)g ( )
C l iConclusions
Imaging and otoneurological explorations are essential in the preoperative work-up.p p p
Transpetrous approaches are the safest approaches to lateral skull base lesions and can be t il d t i di id ltailored to individual cases.
Facial and caudal nerve are mandatory. Auditory monitoring remains difficultmonitoring remains difficult.
Computer assisted surgery improves the quality of tumor resection in selected cases.