Embed Size (px)
Citation preview

Approaching Personalized Oncology as a Clinician and Researcher
Where are we now, and how can we
take it further? Andrew Poklepovic MD Massey Cancer Center
Hematology, Oncology, and PalliaCve Care Associate Member
Developmental TherapeuCcs Program

Personalized Cancer Care Goals and DefiniCons
• Individualized care for each paCent
• Treatments prescribed based upon the unique nature of that person’s cancer – with the goal to maximize responses, improve survival, and improve the ability to cure
• Avoiding treatments that are likely to be ineffecCve
• AdjusCng doses of medicaCons to accommodate each person’s own metabolism

The origins of personalized care • Breast Cancer
• Estrogen Receptor (ER) /Progesterone Receptor (PR) – ~80% of breast cancers – Tamoxifen FDA approved in 1977 following studies showing benefits in advanced disease, but
not unCl over a decade later did the idea that ER was associated with response was confirmed.
– Anastrozole (Arimidex) Letrozole (Femara) Exemestane (Aromasin) Fulvestrant (Faslodex)
• HER2 – GeneCc amplificaCon (more copies of the gene than there should be) in 15-‐20% of breast cancers. – Trastuzumab (HercepCn) –
• Approved 1998 for stage IV breast cancer, the first anCbody specifically targeCng a cancer related protein
• Approved in 2006 for adjuvant treatment of breast cancer with the intent for improving cure rates – LapaCnib (Tykerb) – 2007 stage IV breast cancer – Pertuzumab (Perjeta) 2012 stage IV breast cancer – Trastuzumab-‐emtansine (Kadcyla) 2013 stage IV breast cancer – Pertuzumab (Perjeta) 2014 – approved for stage I-‐III breast cancer prior to surgery
• Triple NegaCve: ER, PR, and HER2 negaCve. – No targeted therapy idenCfied to date.

Breast Cancer • Oncotype DX
• Or…Do I need Chemo?
• FDA approved genomic test for early stage ER+ breast cancer.
• AddiConal studies to determine its role in lymph node posiCve (more advanced) disease

Taking it further than ER/PR/HER2 or Oncotype
• Complete Gene Sequencing of 510 breast tumors – over 30,000 mutaCons found • 4 major sub-‐classes of breast cancer, with variability within each sub-‐class.

Lung cancer • SCLC v. NSCLC
• EGFR MutaCon – EGFR aka HER1 – the first “kinase” discovered, 1978 – Its acCvated role in mutaCons was idenCfied much later.
• EGFR
• ALK/EML4 Fusion MutaCon – First idenCfied in 2007 in a single paCent in Japan, now known to affect ~5% of all lung cancer paCents (70,000 worldwide)
• Others being idenCfied

EGFR • Epidermal • Growth • Factor • Receptor
• When mutated, sends a conCnuous signal into the cell. “The Broken Switch”
• The cancer cell may be dependent on this broken signal for cell survival – so when that signal is interrupted (targeted by the drug), the cell dies.
EGFR

TargeCng the mutant EGFR with erloCnib
• ErloCnib superior to chemotherapy in EGFR mutated lung cancer
• Chemotherapy superior to erloCnib in EGFR non-‐mutated (wildtype) cancer. = chemotherapy
= EGFR targeted therapy
Garassino et al. Lancet 2013 Zhou et al. Lancet 2011

Open Access At: hqp://cancergrace.org/lung/2010/10/10/overview-‐of-‐molecular-‐markers-‐in-‐lung-‐cancer/

Targeted ALK therapy is beqer than chemotherapy
• A second agent, ceriCnib, (Zykadia) was FDA approved in 2014, arer showing a substanCal number of paCents who had experienced progression on crizoCnib obtaining a response from ceriCnib.
• CeriCnib is 20x more potent than crizoCnib, and is acCve against the most common mutaCons in ALK that develop in response to crizoCnib
Shaw et al. NEJM 2013

Lung Cancer MutaConal Landscape • MutaConal rates within a
lung cancer are 10x greater in smokers than nonsmokers
• Carcinogens – ie tobacco smoke -‐ lead to mutaCons
• Different mutaCons tend to show up in cancers in smokers vs. nonsmokers

The KIT example
• Kit is another protein that, when mutated, leads to uncontrolled cancer growth (similar concept to EGFR). – Kit mutated cancers are generally not responsive to chemotherapy.
– MulCple newer “targeted therapies” can inhibit mutated Kit.

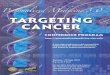
Kit mutaCons common in rare cancer GastrointesCnal Stromal Tumor (GIST)
0
20
40
60
80
Median OS (months) Median OS (months)
Pre-‐Imatinib Era
Imatinib
Kit Exon 11 (imatinib)
Kit Exon 9 (imatinib)
ImaCnib is the standard of care for advanced, unresectable or metastaCc GIST. It has improved median overall survival from 18 to 57 months, vastly changing the outlook for paCents with this disease. Targeted therapy with a logical biologic target changed the course of this disease.
Poklepovic et al, GastrointensCnal stromal tumor: imaCnib and beyond. InTech 2012 open access

• TargeCng KIT requires understanding what drug fits in the pocket to turn it off.

The KIT protein
ImaCnib

KIT in other cancers
• GIST – 85-‐90% of a rare disease • Melanoma 5% – up to 35% of mucosal melanoma, a rare subtype of melanoma
• Rare with unclear frequencies (usually 1-‐3%) – Acute Myelogenous Leukemia – Clear cell sarcoma – Seminoma – Mastocytosis – Lung Cancer

PaCent Example
• Mucosal melanoma paCent – MulCple sites of disease in the mouth and throat. – Surgically removed, but likely residual disease
• KIT exon 11 mutaCon posiCve. – Same as dominant mutaCon in the GIST group.

KIT exon 11 mutated melanoma • Clinical trial evidence of
significant effect in a melanoma paCent when targeCng known KIT mutaCon with a drug with acCvity against that specific mutaCon.
• The drug is not FDA approved, however. I have had mixed success, at Cmes unable to get insurance coverage for imaCnib
• Only opCon was a research trial, at least 5 states away.
JCO 2011

Other cancers with similar problems
• BRAF mutaCon = 40-‐50% melanoma
• BRAF mutaCon – <1-‐3% of lung cancer
• BRAF mutaCon – never previously reported in case of small cell neuroendocrine carcinoma of the intesCne-‐ an already exceedingly rare tumor.
• BRAF mutaCon – present in GIST in very low frequencies of non KIT mutated cancer (1-‐2%)

How do you design the trial?
• In unselected paCents (not chosen based upon EGFR status), therapy against the EGFR was no beqer than a sugar pill. – This trial led the FDA to revoke approval for this agent in the US in 2005.

How do you design the trial? • Be wary of trying to hit a home run in a big ballpark. Low frequency
events will be lost in the noise of the high frequency events. • Development of companion biomarkers or targets is easier in concept
than in pracCce.

How are we trying to do this? • In Glioblastoma (GBM) a rare and
deadly brain tumor, there are very few treatment opCons.
• MCC 14816 looks at triple therapy in paCents who have progressed on primary treatment.
• In the lab, the presence of PDGFR was associated with the greatest tumor cell kill
• Only 30% of GBM has the PDGFR
• Our trial is tesCng first in all GBM, if no posiCve result, shrink the ballpark and only include PDGFR+ GBM
Perc
enta
ge c
ell d
eath
0
20
40
60
80
SO
R 1
SO
R 2
GBM5, 24h GBM5, 48h
**
**
Figure 3
VE
H
SO
R 3
VEH
SO
R 6
VAL (1) VEH VAL (1)
SO
R 1
SO
R 2
VE
H
SO
R 3
SO
R 6
SO
R 1
SO
R 2
VE
H
SO
R 3
SO
R 6
SO
R 1
SO
R 2
VE
H
SO
R 3
SO
R 6
PDGFR +
PDGFR -‐

How else are we trying to do this? NCI Match Trial
• A naConal trial that will idenCfy paCents enCrely upon their mutaConal profile, not the type of cancer that they have.
– PaCents with the “same” type of cancer (lung or breast), could get totally different treatments. • EGFR mutaCon paCent gets EGFR targeCng drug • KIT mutaCon paCent gets KIT targeCng drug
– Opens up opportuniCes for paCents with rare cancers, where disease specific (breast cancer) trials would leave them with few opCons.

NCI Match Trial • Will open to accrual naConwide in 2015
• One master protocol with ~25 subprotocols – Goal is to ulCmately develop FDA approvals based upon mutaCons
within a cancer, not what the cancer looks like under a microscope.
• PaCents get a biopsy for the trial, and the tumor is sequenced. – Assignment to a trial arm is preset based upon mutaCons idenCfied.
– Can end up in more than one arm over Cme if mulCple mutaCons are idenCfied
– 25% of the total trial will be made up of rare cancers

• BRAF mutaCon = 40-‐50% melanoma – BRAF treatments are now FDA approved in melanoma
• BRAF mutaCon – <1-‐3% of lung cancer – BRAF therapy would be available in the MATCH Trial
• BRAF mutaCon – never previously reported in case of small cell neuroendocrine carcinoma of the intesCne-‐ an already exceedingly rare tumor. – BRAF therapy would be available in the MATCH Trial
• BRAF mutaCon – present in GIST in very low frequencies of non KIT
mutated cancer (1-‐2%) – BRAF therapy would be available in the MATCH Trial
NCI Match Trial

How do you help? • Support the funding for development of, and ulCmately
reimbursement of, geneCc tesCng of paCent tumors. – SupporCng the tests that will find the targets the drugs can be used on, or developed for.
– In late 2014, a geneCc tesCng company, FoundaCon Medicine, reported that some insurance companies were going to start covering their geneCc tesCng.
– The NCI is building a repository of tumor informaCon, to find the rare events that can generate new treatment ideas. • Also idenCfy gene signatures in paCents in which a treatment was remarkably successful, to generate new ideas. – This is called “The ExcepConal Responders” program.

How do you help? • Support the idea that there are scienCfic reasons for using drugs in
personalized cancer care. Not every drug will work for everybody, and it may be that most drugs will work really well for only a few people in many cancers.
• Insurance coverage should support logical use of known targeted drugs against the mutaCons they are acCve on, once at least some efficacy is shown. – The cost is generally not substanCally different from an approved standard
therapy. – FDA approval combining a mutaCon requirement (melanoma with BRAF
mutaCon to get vemurafenib) but also histology (melanoma, not small cell cancer), can make it hard to get therapy for individual paCents with rare diseases or low frequency mutaCons. • It can be traumaCc for a paCent to know that they have a rare disease, with a druggable
target, but no ready access to the drug. • This may be addressed with the MATCH trial
• Tell your friends and others not to be afraid of clinical trials for cancer. Tomorrow’s treatments are being invesCgated today

Thank You Please help to conCnue the fight,
as you have been doing.
It makes a difference, every day.