Embed Size (px)
Citation preview

ARDS Guidelines
Dr. George John,
Critical Care,
Christian Medical College,
Vellore

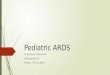
Causative Factors in ARDS
PRIMARY INJURY
HOST RESPONSE
CONSEQUENCES OF THERAPY

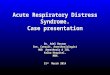
SPECTRUM OF LUNG “INJURY”
Cardiogenic pulmonary
oedema
ALI ARDS
Altered Starling’s Forces
P/F RATIO 200 - 300 P/F RATIO < 200

Pulmonary Changes
• Alveolar Flooding
• Interstitial inflammation
• Atelectasis
Early Exudative Phase < 1 week
Late Fibro Proliferative Phase > 1 week

Guidelines
• Oxygenation
• Ventilation
• Position
• Fluid management
• Miscellaneous

Oxygenation
Lowest FiO2
- to keep PaO2 55 – 80mm Hg
Increase Alveolar Recruitment = degree of penetration of gas into poorly / nonaerated lung regions
- PEEP - recruitment manoeuver- inverse ratio ventilation
Prone positioning ( “proning” )NO (Nitric Oxide)

The Pressure Profile
Peak Pressure
Plateau Pressure
Mean Pressure
PEEP

VentilationVENTILATIONVolume Control mode; I:E ratio 1:1 – 1:3
- Tidal Volume 6ml / kg- Plateau Pressure < 30cm H2O - High rate if CO2 high – up to 35 / minute
Measures to decrease CO2 production (sedation, decrease temperature) Permissive hypercapnoeaIf pH < 7.30 – use HCO3 infusionOther techniques:?Tracheal gas insufflation (TGI) / Expiratory washout (EWO)
(use humidified gas only)? Pressure Control Mode with pressure = 30
- many with less pressure needed for ventilation in the study - study done with VC mode

Position“PRONING”
• Ventilation in the prone position improves oxygenation but most clinical studies have not shown that prone ventilation improves outcome. In a study of paediatric patients (2 weeks to 18 years of age) with acute lung injury, prone positioning did not significantly reduce ventilator-free days or improve clinical outcome.
• However, in a study published in 2006, prolonged prone positioning (at least 20 hours a day) in patients greater than 18 years of age showed that it was safe and may reduce mortality.

Fluid ManagementLiberal versus Conservative
Conservative strategy: maintain a low target filling pressure (CVP of less than 4mm Hg or PAOPof less than 8 mm Hg)
versusLiberal strategy: maintain higher filling pressure CVP 10 – 14mm Hg orPAOP 14-18mm Hg. This was achieved by a combination of bolus fluidadministration, use of frusemide or dobutamine, depending on theperfusion, urine output , measured filling pressures and cardiac output (if available).
Result:There was no significant difference in mortality (25.5% in the conservative group vs.
28.4% in the liberal group). However, the conservative strategy improved the oxygenation index, lung injury score, increased the number of ventilator free days and days not spent in ICU. The conservative strategy did not increase the incidence or prevalence of shock during the study. In addition, the conservative strategy did not increase the use of dialysis during the first 60 days.

Monitoring
• In a landmark study published in 2006, the use of PA catheter guided therapy did not improve organ function or survival as compared to CVC guided therapy. The PA catheter was associated with more complications (twice as many catheter related complications, predominantly arrhythmias) than CVC guided therapy.

Cardiovascular
• Haemoglobin 8 – 10 g%
• Maintain Cardiac Output
Judicious fluids
Use inotropes as needed

Other Modalities• SteroidsEarlier study:
Evidence that use of steroids after the first week of ARDS improves prognosis significantly.
In 2006: No benefit in the use of methylprednisolone after the first week of ARDS. Use of sterods after 14 days of ARDS was associated with increased mortality at 60 days. This was in spite of the steroid therapy and improving ventilator free shock free days during the first 28 days. Methyprednisolone did not increase infectious complications but was associated with a higher rate of neuromuscular weakness.
• Nitric OxideNo benefit• Beta agonists:The beta agonist lung injury trial (BALTI) has shown that treatment withintravenous albutamol (15ug / kg / hr) reduces extravascular lung water (EVLW)in patients with ALI / ARDS with a reduction in plateau pressures at Day 7.The effect on EVLW started at 48 hours. Patients receiving intravenoussalbutamol had a higher incidence ofsupraventricular arrhythmias these were notsustained as the dose of salbutamol was modified in these patients. There wasno improvement in mortality with the use of salbutamol – however the study wasnot Powered to detect a difference in mortality.

“Imitators”
• Acute Interstitial Pneumonia (AIP)
• Acute Eosinophilic Pneumonia
• Acute BOOP
• DAH
• Acute HP

Suspecting “ Imitators”
• Common features: fever, cough, myalgia, raised WBC, CRP, LDH
• Distinguishing features: BAL, Lung Biopsy, Response to steroids and prognosis (in some)

Possible Approach• Early BAL – infectious agents, differential WBC count• Serological tests for autoimmune disease, CK (polymyositis)• Haematocrit – serial• Ferritin (increased in adult Still’s)• Renal function• Urine microscopy• Lung biopsy – if BAL is inconclusive, after considering risk vs.
benefit. Specially important in DAH (vasculitis induced) ; necessary for immunofluorecent staing for ABMA.
• The suggestion to start all these patients initially on steroids for 3 days till the BAL results / other tests are available is controversial and needs to be evaluated in a RCT.

References - 11. Bernard GR et al. The American European Consensus Conference on ARDS. Am J Respir Crit
Care Med 1994; 149: 818 – 8242. Meduri et al. Corticosteroid rescue treatment of progressive fibroproliferation in late ARDS.
Patterns of response and predictors of outcome. Chest 1994; 105: 1516 – 15273. Meduri GU et al. Effect of prolonged methylprednisoloine therapy in unresolving acute respiratory
distress syndrome. A randomized controlled trial. JAMA 1998; 280: 159 – 1654. Brun-Buisson C and Brochard L. Corticosteroid therapy in acute respiratory distress syndrome.
Better late than never? JAMA 1998; 280: 182 – 1835. Cook D et al. A comparison of Sucralfate and Ranitidine for the prevention of upper gastrointestinal
bleeding in patients requiring mechanical ventilation. N Engl J Med 1998; 338: 791 - 79 6. Amato MBP et al. Effect of protective ventilation strategy on mortality in the acute respiratory
distress syndrome. N Engl J Med 1998; 338: 347 - 3547. Stewart TE et al. Evaluation of a ventilation strategy to prevent barotrauma in patients at high risk
for acute respiratory distress syndrome. N Engl J Med 1998: 338: 355 – 3618. Richecoeur J et al. Respiratory washout versus optimisation of mechanical ventilation during
permissive hypercapnoea in patients with severe acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999; 160: 77 - 85
9. The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N Engl J Med 2000; 342: 1301 – 1308
10. Gattinoni L et al. Effect of prone positioning on the survival of patients with acute respiratory failure. N Engl J Med 2001; 345: 568 – 573
11. Nuckton T et al. Pulmonary dead space fraction as a risk factor for death in the acute respiratory distress syndrome. N Engl J Med 2002; 346: 1281 – 1286
12. New Management strategies in ARDS. Editor Levy MM. Critical Care Clinics, January 2002 13. Jindal SK et al. Adult respiratory distress syndrome in the tropics. Clin Chest Med 2002; 23: 445 –
455

References - 213. Kopp R et al. Evidence based medicine in the therapy of the acute respiratory distress
syndrome. Intensive Care Medicine 2002; 28: 244 – 24514. The ARDS Clinical Trials Network. Effects of recruitment manoeuvers in patients with
acute lung injury and acute respiratory distress syndrome ventilated with high positive end expiratory pressure. Crit. Care Med. 2003; 31: 2592 – 2597
15. Marini JJ. Are recruiting maneuvers needed when ventilating acute respiratory distress syndrome? Crit. Care Med. 2003; 31: 2701 – 2702
16. Barbas CSV. Lung recruitment menoeuvers in acute respiratory distress syndrome and facilitating resolution. Crit. Care Med. 2003; 31 (Suppl): S265 – S271
17. Marini J & Gattinoni L. Ventilatory management of acute respiratory distress syndrome: a consensus of two Crit. Care Med 2004; 32: 250 – 255
18. The Margaux IV Conference on Critical Illness: Acute Lung Injury – Understanding the mechanisms of injury and repair. Crit. Care Med. 2003; 31 (Suppl): S183 – S342
19. Schwarz MI et al. “Imitators” of the ARDS. Implications for diagnosis and treatment. Chest 2004; 125: 1530- 1535
20. Mancebo J et al. A multicenter trial of prolonged prone ventilation in severe acute respiratory distress syndrome. Am J Respir Crit Care Med. 2006; 173: 1233 – 1239
21. Barrett NA & Kam PCA. Transfusion-related lung injury: a literature review. Anaesthesia 2006; 61: 777 – 785
22. ARDS Clinical Trials Network. Pulmonary Artery versus Central Venous Catheter to guide treatment of Acute Lung Injury. The New Engl. J Med. 2006; 354: 2213 - 2224
23. ARDS CLINICAL Trials Network. Comparison of two fluid management strategies in Acute Lung Injury. The New Engl J Med. 2006; 354: 2564 – 2575
24. Rivers EP. Fluid Management Strategies in Acute Lung Injury – Liberal or Conservative or both? The New Engl J Med. 2006; 354: 2598 – 2600