Embed Size (px)
Citation preview
Are Esophageal Pressure Measurements Important in ClinicalDecision-Making in Mechanically Ventilated Patients?
Daniel S Talmor MD MPH and Henry E Fessler MD
IntroductionPro: Esophageal Pressure Measurements Are Important in Clinical Deci-
sion Making in Mechanically Ventilated PatientsPleural and Transpulmonary Pressures During Mechanical VentilationEsophageal Pressure as a Surrogate for Pleural PressureClinical Observations Using Esophageal Pressure
Con: Esophageal Pressure Measurements Have Not Been Shown to BeImportant in Clinical Decision Making in Mechanically VentilatedPatients
Esophageal Pressure Measurement: Sources of ErrorUsing Esophageal Pressure to Guide Ventilator Management in ALI/
ARDSSummary
Low-tidal-volume ventilation strategies are clearly beneficial in patients with acute lung injury andacute respiratory distress syndrome, but the optimal level of applied positive end-expiratory pres-sure (PEEP) is uncertain. In patients with high pleural pressure on conventional ventilator settings,under-inflation may lead to atelectasis, hypoxemia, and exacerbation of lung injury through “at-electrauma.” In such patients, raising PEEP to maintain a positive transpulmonary pressure mightimprove aeration and oxygenation without causing over-distention. Conversely, in patients with lowpleural pressure, maintaining a low PEEP would keep transpulmonary pressure low, avoidingover-distention and consequent “volutrauma.” Thus, the currently recommended strategy of settingPEEP without regard to transpulmonary pressure is predicted to benefit some patients whileharming others. Recently the use of esophageal manometry to identify the optimal ventilatorsettings, avoiding both under-inflation and over-inflation, was proposed. This method shows prom-ise but awaits larger clinical trials to assess its impact on clinical outcomes. Key words. esophagealmanometry; mechanical ventilation; acute lung injury; ALI; acute respiratory distress syndrome; ARDS;positive end-expiratory pressure; PEEP; pleural pressure; transpulmonary pressure. [Respir Care 2010;55(2):162–172. © 2010 Daedalus Enterprises]
Daniel S Talmor MD MPH is affiliated with the Department of Anes-thesia, Critical Care, and Pain Management, Beth Israel Deaconess Med-ical Center, and Harvard School of Medicine. Boston, Massachusetts.Henry E Fessler MD is affiliated with the Department of Pulmonary andCritical Care Medicine, Johns Hopkins School of Medicine. Baltimore,Maryland.
Drs Talmor and Fessler presented a version of this paper at the 44th
RESPIRATORY CARE Journal Conference, “Respiratory Care Controver-sies II,” held March 13-15, 2009, in Cancun, Mexico.
The authors have disclosed no conflicts of interest.
Correspondence: Daniel S Talmor MD MPH, Department of Anesthesiaand Critical Care, Beth Israel Deaconess Medical Center, 1 DeaconessRoad, Boston MA 02446. E-mail: [email protected].
162 RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2

Introduction
Esophageal pressure (Pes) has been measured in man forover 50 years.1,2 More recently it has been proposed as asurrogate for pleural pressure. This would allow the cal-culation of transpulmonary pressure and provide a meansto guide the management of mechanically ventilated pa-tients. Although it has been used to measure work of breath-ing and to guide weaning,3 we will limit our comments tothe management of acute respiratory distress syndrome(ARDS) and acute lung injury (ALI). Improvements inventilator management have reduced the high mortalityand morbidity associated with ARDS. It is known fromdecades of animal experimentation that mechanical venti-lation can cause ventilator-induced lung injury (VILI) fromlung over-distention at end-inspiration, and from repetitiveairway opening and closing.4
VILI can be reduced by limiting tidal volume (VT) andend-inspiratory plateau pressure (Pplat), which reducesARDS mortality.5 Consequently, small VT and lower Pplat
have become the standard of care for such patients. Duringspontaneous inspiration to total lung capacity, transpulmo-nary pressure (airway pressure [Paw] minus pleural pres-sure) is approximately 25–30 cm H2O, which correspondsto a Pplat of 30–35 cm H2O in a patient with normal chestwall compliance. Animal studies showed little lung in-flammation or injury when mechanical ventilation of nor-mal lungs remained below 30–35 cm H2O.6 Although ALIand ARDS lungs are mechanically heterogeneous, restrict-ing Pplat to � 30–35 cm H2O avoids injurious over-dis-tention of even the most normal regions.7-9
Attempts have also been made to mitigate the injuriouseffects of repetitive airway opening and closure by ma-nipulating PEEP. Higher PEEP prevents lung regions fromclosing during expiration and allows ventilation of otherlung regions that might otherwise remain atelectaticthroughout the respiratory cycle. Unfortunately, severallarge randomized clinical trials found no survival advan-tage from managing ARDS with higher PEEP.10-12 Severalexplanations have been suggested for that disappointingresult. Unless accompanied by further VT reduction, higherPEEP may increase lung stretch at peak inspiration, so onesource of injury may be traded for another. In addition, theresponse to increased PEEP is heterogeneous. Some indi-viduals effectively recruit lung, whereas others may over-distend lung that was already recruited. The best way to setPEEP, to optimally balance recruitment and distention ineach patient, remains elusive.
Based on these concepts, the use of Pes to set PEEP ishypothetically very attractive. Pes is often quite elevated inpatients with ARDS. Thoracic-wall compliance may bereduced and Pes elevated due to body habitus, abdominaldistention, edema, or other mechanical abnormalities. Thecalculated transpulmonary pressure is often a negative value
at end-expiration.13 This is presumed to reflect closed air-ways. In the presence of closed airways and flooded oratelectatic lung, the Paw measured proximally (the set PEEP)may underestimate alveolar pressure, resulting in a nega-tive calculated transpulmonary pressure. Raising PEEPuntil transpulmonary pressure becomes positive at end-expiration could assure that airways remain open. Further-more, the same chest wall factors that elevate Pes at end-expiration also elevate Pes at end-inspiration. Pplat mayreach 35 cm H2O or more when transpulmonary pressureis in fact much lower than it would be in a patient withnormal chest wall mechanics. Measuring Pes and calculat-ing transpulmonary pressure directly would allow PEEP tobe increased while assuring that transpulmonary pressureat end-inspiration still remains in a safe range.
As theoretically appealing as this approach may be, ev-idence for its effectiveness is only beginning to emerge.There are concerns about the accuracy of Pes measure-ments in patients with ALI/ARDS, and the relevance ofthe Pes as a reflection of the relevant pressure on the pleurasurface. Ventilator management using Pes measurement toset PEEP while limiting peak transpulmonary pressure im-proves oxygenation.14 We will review the concepts anddata supporting and refuting this approach.
Pro: Esophageal Pressure MeasurementsAre Important in Clinical Decision Making
in Mechanically Ventilated Patients
Pleural and Transpulmonary Pressures DuringMechanical Ventilation
Clinicians manage mechanical ventilation to preventVILI by monitoring and controlling airway pressures. Forexample, PEEP is set to control Paw at end-expiration, andend-inspiratory Pplat is monitored to minimize the risk ofover-distention. This is a reasonable strategy to the extentthat pleural pressure is predictable or restricted to a narrowrange, but pleural pressure ranges widely and unpredict-ably in patients with ARDS, due to factors such as obesityand abdominal fluid accumulation, which influence themechanical behavior of the chest wall. A wide pleuralpressure range among individuals could affect the lunginflation produced by mechanical ventilation. For exam-ple, a seemingly high PEEP of 18 cm H2O could still betoo low in a patient with a pleural pressure of 20 cm H2O,allowing repetitive collapse of air spaces with each expi-ration, or it could be too high in a patient with a pleuralpressure of 5 cm H2O, over-distending the lungs at end-inflation. Because Paw reflects the sum of pressures acrossthe lung and chest wall, the portion of the applied pressureinflating the lung (transpulmonary pressure) could varywidely, depending on chest wall characteristics.15
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2 163

One cause of elevated pleural pressure is obesity, whichis known to cause restrictive chest wall physiology andlow lung volumes indicative of high pleural pressure. Morecommonly, elevated pleural pressure can result from re-suscitation with large fluid volumes and the resulting edemaof the intrathoracic and intra-abdominal tissues. In pigs,Mutoh and colleagues found that intravascular volume in-fusion produced abdominal distention, lung volume re-striction, chest wall stiffening, increased pleural pressure,and decreased chest wall and lung compliance.16 Similareffects were produced by increasing the intra-abdominalpressure by inflating an abdominal balloon. Malbrain et alestimated the prevalence of intra-abdominal hypertensionfrom bladder pressure in 97 critically ill patients admittedto medical and surgical intensive care units.17 Bladder pres-sure, which approximates intra-abdominal pressure,
18 wasnormal in only 41% of patients, whereas 58% of the pa-tients had intra-abdominal hypertension, defined as blad-der pressure of 16–27 cm H2O. Eight percent of the sub-jects had bladder pressure over 27 cm H2O, indicatingabdominal compartment syndrome. In passively ventilatedpatients, intra-abdominal pressure is transmitted to the pleu-ral space, so these findings suggest that pleural pressurealso differs widely among such patients. The abdominalpressure range in these patients spans nearly the entirerange of PEEP values that would ordinarily be used formechanical ventilation in ALI/ARDS.
Although the first successful trial of low-VT ventilationfor ALI/ARDS used high PEEP,19 and a later trial foundthat lung-protective ventilation with higher PEEP reducesthe release of pro-inflammatory cytokines,20 subsequenttrials have not confirmed a survival benefit from higherPEEP,10-12,21 and the protective role of PEEP in preventingVILI remains in doubt.22 Why is it that higher PEEP,which was protective in numerous animal experiments,has been of equivocal benefit in clinical trials of ventilatorstrategies for ALI/ARDS? One possible explanation is thatthe end-inspiratory Pplat and PEEP specified in the clinicalprotocols do not reflect transpulmonary pressure, the ac-tual inflating pressure of the lung. Estimating pleural pres-sure to calculate transpulmonary pressure may allow bettercontrol of both end-inspiratory and end-expiratory lungvolume, and thereby reduce VILI caused by over-disten-tion or atelectrauma.
Esophageal Pressure as a Surrogate for PleuralPressure
It is not feasible to directly measure pleural pressure inhumans. However, pleural pressure has long been esti-mated in upright subjects by measuring Pes with a balloon-tipped catheter. It is well accepted that the respiratorychanges in Pes are representative of changes in pleuralpressure applied to the lung surface.23 Furthermore, Pes
is considered representative of an effective pleural pres-sure surrounding the lung, such that the difference be-tween Paw and Pes is a valid estimate of transpulmonarypressure.23
By contrast, in mechanically ventilated supine patientswith ALI/ARDS, Pes is rarely used to estimate pleuralpressure. Although several investigators have reported thechanges in Pes with changes in lung volume to characterizelung compliance, they did not report the baseline value ofPes. There are several reasons why baseline Pes values inmechanically ventilated patients are often ignored. First,studies in normal subjects have shown that Pes at a givenlung volume is higher in the supine position than the up-right posture.1,2,24,25 Lung compliance also appears to bereduced in the supine position,2,24-26 a finding attributed tocompression of the esophagus by the mediastinal con-tents.1,2,25,26 Lesser changes in Pes have been observedupon changing from supine to prone or lateral positions.1,25
These postural effects complicate the interpretation of Pes
even in healthy subjects, when supine.The properly positioned esophageal balloon catheter sits
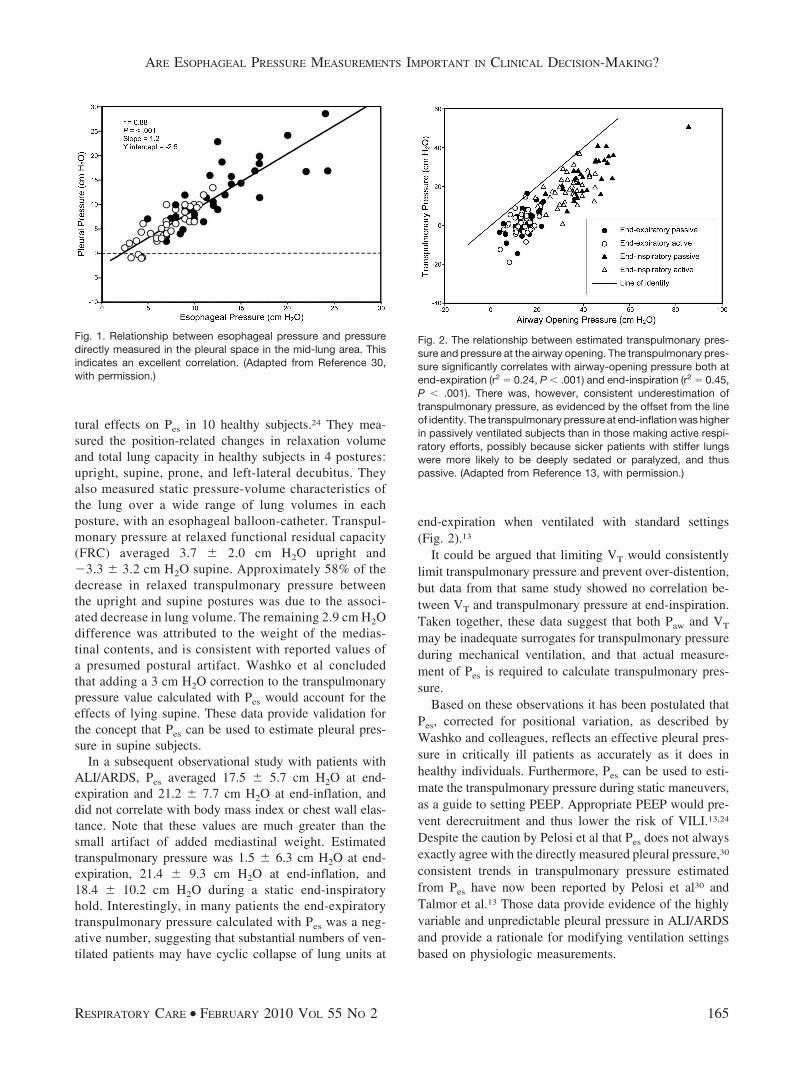
at approximately the midpoint of the lung’s gravitationalplane in both the upright and supine positions. In the nor-mal individual, the Pes therefore reflects pressure at mid-lung height, somewhat underestimating pressure surround-ing the dependent lung and overestimating that surroundingthe non-dependent lung. In ALI/ARDS the lung tissue ismore dense, increasing the gravitational gradient in pleuralpressure.27 Thus, the mid-thoracic Pes may differ morefrom the pleural pressure in the most dependent and non-dependent lung regions. Furthermore, diseased lungs areoften mechanically inhomogeneous and less deformable,increasing inter-regional differences in pleural pressure dueto shape change.28 These considerations have led to a wide-spread assumption that Pes is not a useful measure of lungsurface pressure in such patients, and that it should not beused to estimate transpulmonary pressure.28 However, thishypothesis has not actually been tested. To the contrary, ina canine model of ARDS, Pelosi et al29 demonstrated thatthe actual value of Pes accurately estimated the pleuralpressure within the mid-lung zone (Fig. 1). Optimizingmechanical ventilation to transpulmonary pressure in thismid-lung region may be a more appropriate strategy thanone that relies on measurement of Paw alone. Moreover,optimizing inflating pressures to the mid-lung may preventover-distention of the upper, non-dependent portions ofaerated lung while preventing collapse of the lower, de-pendent portions.
Concern has been raised that artifacts induced by themediastinal contents make Pes an unreliable estimate ofpleural pressure in supine patients with ALI.28 Washkoet al characterized the magnitude and variability of pos-
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
164 RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2
tural effects on Pes in 10 healthy subjects.24 They mea-sured the position-related changes in relaxation volumeand total lung capacity in healthy subjects in 4 postures:upright, supine, prone, and left-lateral decubitus. Theyalso measured static pressure-volume characteristics ofthe lung over a wide range of lung volumes in eachposture, with an esophageal balloon-catheter. Transpul-monary pressure at relaxed functional residual capacity(FRC) averaged 3.7 � 2.0 cm H2O upright and�3.3 � 3.2 cm H2O supine. Approximately 58% of thedecrease in relaxed transpulmonary pressure betweenthe upright and supine postures was due to the associ-ated decrease in lung volume. The remaining 2.9 cm H2Odifference was attributed to the weight of the medias-tinal contents, and is consistent with reported values ofa presumed postural artifact. Washko et al concludedthat adding a 3 cm H2O correction to the transpulmonarypressure value calculated with Pes would account for theeffects of lying supine. These data provide validation forthe concept that Pes can be used to estimate pleural pres-sure in supine subjects.
In a subsequent observational study with patients withALI/ARDS, Pes averaged 17.5 � 5.7 cm H2O at end-expiration and 21.2 � 7.7 cm H2O at end-inflation, anddid not correlate with body mass index or chest wall elas-tance. Note that these values are much greater than thesmall artifact of added mediastinal weight. Estimatedtranspulmonary pressure was 1.5 � 6.3 cm H2O at end-expiration, 21.4 � 9.3 cm H2O at end-inflation, and18.4 � 10.2 cm H2O during a static end-inspiratoryhold. Interestingly, in many patients the end-expiratorytranspulmonary pressure calculated with Pes was a neg-ative number, suggesting that substantial numbers of ven-tilated patients may have cyclic collapse of lung units at
end-expiration when ventilated with standard settings(Fig. 2).13
It could be argued that limiting VT would consistentlylimit transpulmonary pressure and prevent over-distention,but data from that same study showed no correlation be-tween VT and transpulmonary pressure at end-inspiration.Taken together, these data suggest that both Paw and VT
may be inadequate surrogates for transpulmonary pressureduring mechanical ventilation, and that actual measure-ment of Pes is required to calculate transpulmonary pres-sure.
Based on these observations it has been postulated thatPes, corrected for positional variation, as described byWashko and colleagues, reflects an effective pleural pres-sure in critically ill patients as accurately as it does inhealthy individuals. Furthermore, Pes can be used to esti-mate the transpulmonary pressure during static maneuvers,as a guide to setting PEEP. Appropriate PEEP would pre-vent derecruitment and thus lower the risk of VILI.13,24
Despite the caution by Pelosi et al that Pes does not alwaysexactly agree with the directly measured pleural pressure,30
consistent trends in transpulmonary pressure estimatedfrom Pes have now been reported by Pelosi et al30 andTalmor et al.13 Those data provide evidence of the highlyvariable and unpredictable pleural pressure in ALI/ARDSand provide a rationale for modifying ventilation settingsbased on physiologic measurements.
Fig. 1. Relationship between esophageal pressure and pressuredirectly measured in the pleural space in the mid-lung area. Thisindicates an excellent correlation. (Adapted from Reference 30,with permission.)
Fig. 2. The relationship between estimated transpulmonary pres-sure and pressure at the airway opening. The transpulmonary pres-sure significantly correlates with airway-opening pressure both atend-expiration (r2 � 0.24, P � .001) and end-inspiration (r2 � 0.45,P � .001). There was, however, consistent underestimation oftranspulmonary pressure, as evidenced by the offset from the lineof identity. The transpulmonary pressure at end-inflation was higherin passively ventilated subjects than in those making active respi-ratory efforts, possibly because sicker patients with stiffer lungswere more likely to be deeply sedated or paralyzed, and thuspassive. (Adapted from Reference 13, with permission.)
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2 165
Clinical Observations Using Esophageal Pressure
A phase-2 randomized controlled trial of mechanicalventilation directed by Pes, compared to ventilation basedon the ARDS Network protocol,14 used oxygenation as theprimary outcome and was terminated early because of over-whelming effect, after enrolling 61 patients. There were nounexpected study-related adverse events in either group.The ratio of PaO2
to fraction of inspired oxygen (FIO2) at
72 hours was 88 mm Hg higher in the intervention group(95% CI 78.1–98.3, P � .002), and this improvement wasevident at 24, 48, and 72 hours (P � .001 via repeated-measures analysis). Respiratory-system compliance wasalso significantly improved in the intervention group(P � .002 via repeated-measures analysis at 24, 48, and72 h). In the intervention group there was also a trendtoward lower 28-day and 6-month mortality.13 Though Pplat
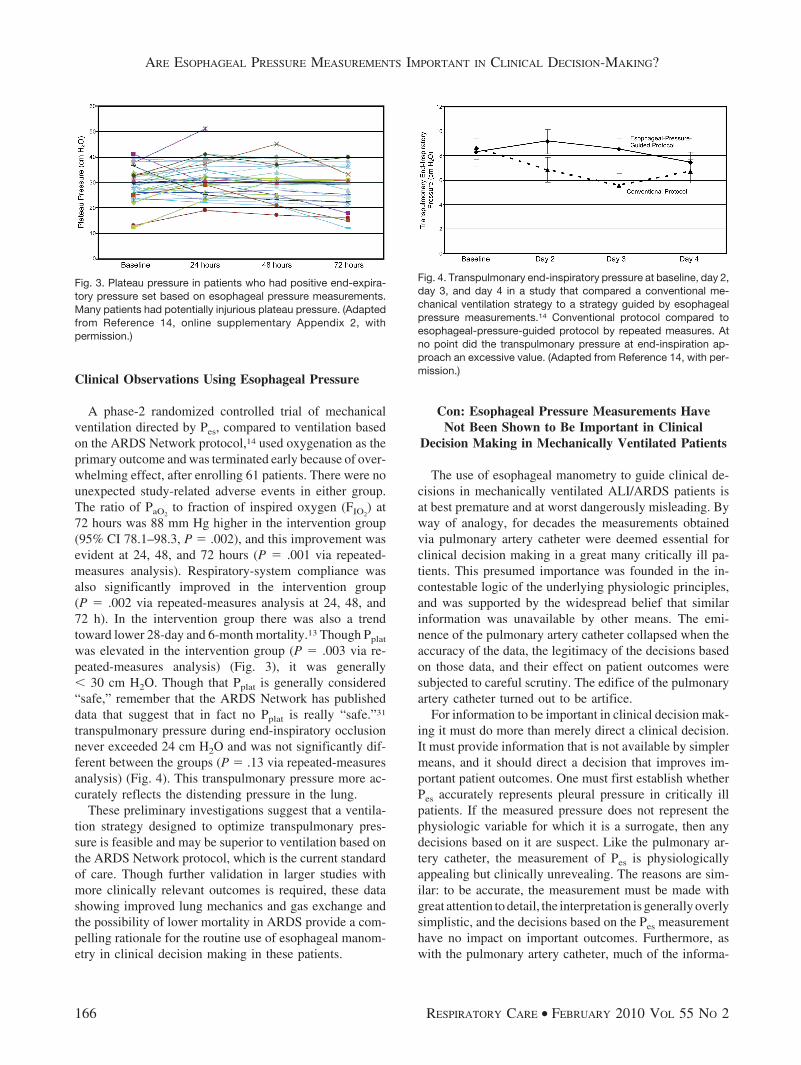
was elevated in the intervention group (P � .003 via re-peated-measures analysis) (Fig. 3), it was generally� 30 cm H2O. Though that Pplat is generally considered“safe,” remember that the ARDS Network has publisheddata that suggest that in fact no Pplat is really “safe.”31
transpulmonary pressure during end-inspiratory occlusionnever exceeded 24 cm H2O and was not significantly dif-ferent between the groups (P � .13 via repeated-measuresanalysis) (Fig. 4). This transpulmonary pressure more ac-curately reflects the distending pressure in the lung.
These preliminary investigations suggest that a ventila-tion strategy designed to optimize transpulmonary pres-sure is feasible and may be superior to ventilation based onthe ARDS Network protocol, which is the current standardof care. Though further validation in larger studies withmore clinically relevant outcomes is required, these datashowing improved lung mechanics and gas exchange andthe possibility of lower mortality in ARDS provide a com-pelling rationale for the routine use of esophageal manom-etry in clinical decision making in these patients.
Con: Esophageal Pressure Measurements HaveNot Been Shown to Be Important in Clinical
Decision Making in Mechanically Ventilated Patients
The use of esophageal manometry to guide clinical de-cisions in mechanically ventilated ALI/ARDS patients isat best premature and at worst dangerously misleading. Byway of analogy, for decades the measurements obtainedvia pulmonary artery catheter were deemed essential forclinical decision making in a great many critically ill pa-tients. This presumed importance was founded in the in-contestable logic of the underlying physiologic principles,and was supported by the widespread belief that similarinformation was unavailable by other means. The emi-nence of the pulmonary artery catheter collapsed when theaccuracy of the data, the legitimacy of the decisions basedon those data, and their effect on patient outcomes weresubjected to careful scrutiny. The edifice of the pulmonaryartery catheter turned out to be artifice.
For information to be important in clinical decision mak-ing it must do more than merely direct a clinical decision.It must provide information that is not available by simplermeans, and it should direct a decision that improves im-portant patient outcomes. One must first establish whetherPes accurately represents pleural pressure in critically illpatients. If the measured pressure does not represent thephysiologic variable for which it is a surrogate, then anydecisions based on it are suspect. Like the pulmonary ar-tery catheter, the measurement of Pes is physiologicallyappealing but clinically unrevealing. The reasons are sim-ilar: to be accurate, the measurement must be made withgreat attention to detail, the interpretation is generally overlysimplistic, and the decisions based on the Pes measurementhave no impact on important outcomes. Furthermore, aswith the pulmonary artery catheter, much of the informa-
Fig. 3. Plateau pressure in patients who had positive end-expira-tory pressure set based on esophageal pressure measurements.Many patients had potentially injurious plateau pressure. (Adaptedfrom Reference 14, online supplementary Appendix 2, withpermission.)
Fig. 4. Transpulmonary end-inspiratory pressure at baseline, day 2,day 3, and day 4 in a study that compared a conventional me-chanical ventilation strategy to a strategy guided by esophagealpressure measurements.14 Conventional protocol compared toesophageal-pressure-guided protocol by repeated measures. Atno point did the transpulmonary pressure at end-inspiration ap-proach an excessive value. (Adapted from Reference 14, with per-mission.)
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
166 RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2

tion sought by measurement of Pes can be inferred fromother, less invasive means. In the case of setting PEEP inmechanically ventilated ALI/ARDS patients, the decisionsdirected by using Pes appear to be diametrically opposite tothose directed by other physiologic data.
Esophageal Pressure Measurement: Sources of Error
Pes measurement technique was studied in detail in the1950s and 1960s, when measurements were being appliedto studies of normal lung mechanics. Open-ended cathe-ters, filled with either fluid or air, are unsuitable, becausethe surface forces at air-fluid interfaces within the esoph-agus or catheter distort the measured pressure. Because theradii of curvature at these interfaces are small and the fluidgenerally has high surface tension, the errors can be sub-stantial when small pressures are being measured.
To avoid these surface force errors, Pes is measured withan air-filled catheter terminating in a thin balloon. Thestandard balloon is 10 cm long, and the catheter has mul-tiple side holes within the balloon. If the balloon containsa volume below its unstressed volume, it will have nopressure gradient across its wall, so the pressure within theballoon will equal the pressure within the esophagus. Withtoo little air volume the positive pressure in the esophaguswill compress the remaining gas and empty the balloon.The measured pressure will then underestimate the Pes.Too much air volume will distend the local region of theesophagus, or even the balloon, and the measured pressurewill overestimate the pressure in the empty esophagus.
The technique has been standardized as follows. Afterthe balloon-tipped catheter is positioned (see below), it isopened to the air while the subject bears down to raisepleural pressure and empty the balloon. The subject re-laxes, 5 mL of air are injected into the balloon, and 4.5 mLare removed. This ensures that the balloon is not twistedaround the catheter and compartmentalized, and leaves avolume of air that will minimally distort the measured Pes.The residual bubble will flow to wherever the pressurewithin the balloon is lowest.1
Pressure within the esophagus varies considerably be-tween the gastroesophageal junction and the thoracic in-let.1 Some of this reflects the hydrostatic gradient of pleu-ral pressure from non-dependent to dependent regions.However, much of the variability of Pes is due to localdifferences in Pes, which are unrelated to the pleural pres-sure. They are therefore considered artifacts, which mustbe minimized by proper positioning of the balloon. Thegoal is for the Pes to represent the average pressure on thelung surface. Optimal positioning of the balloon has beenstudied by comparing the change in Paw to the change inPes as the subject makes gentle expulsive or inspiratoryefforts against an occluded airway.32 Since the airway isoccluded, transpulmonary pressure will not change. Paw
and Pes will not be equal (their difference is transpulmo-nary pressure), but they should change equally during theseoccluded efforts, so the ratio of �Pes to �Paw should benear unity. This criterion is generally met in the lowerthird of the esophagus, approximately 10 cm above thegastroesophageal junction.1 Note, however, that all of theseinvestigations were performed with upright and coopera-tive subjects.
Furthermore, this method of optimal positioning indi-cates only that changes in Pes may accurately track changesin pleural pressure. It does not indicate that Pes is accurate.Changes in pressure and volume are all that are necessaryto measure lung or chest wall compliance, when compli-ance is calculated as a slope, but an accurate Pes is essen-tial to calculate a specific transpulmonary pressure.
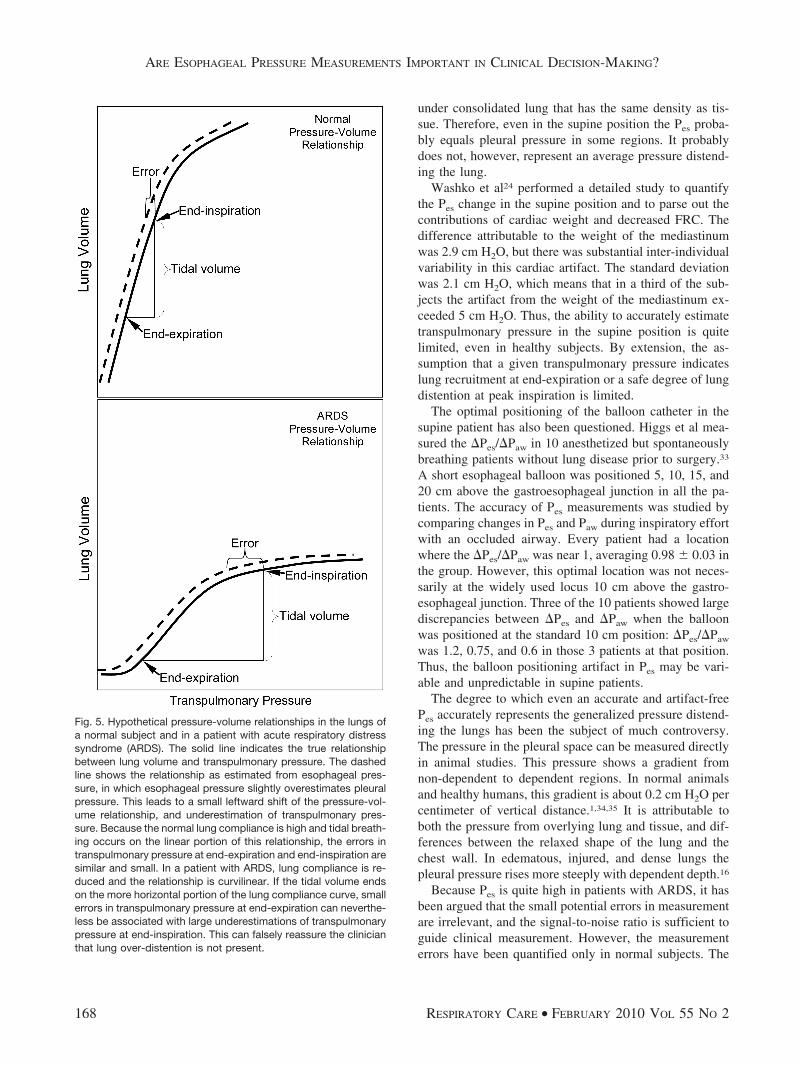
Consider the effect of a small error in Pes measured atend-expiration in a normal subject (Fig. 5A). A slight over-estimation of Pes (for example, from having a little toomuch air in the balloon) will cause a slight underestima-tion of transpulmonary pressure at any volume. This canbe represented as a leftward shift of the lung pressure-volume relationship. Since the normal VT of a normalsubject occurs on a linear portion of this pressure-volumerelationship, the small underestimate of transpulmonarypressure at end-expiration will be of similar magnitude atend-inspiration. But in the highly non-linear lung pressure-volume relationship in a patient with ARDS (Fig. 5B),depending on the shape and position of the lung pressure-volume relationship, a small underestimation of transpul-monary pressure at end-expiration may cause a large un-derestimate at end-inspiration. Stated differently, the effectof balloon volume on measured pressure is greater at highlung volume, even in normal subjects.1 This artifact wouldprovide false reassurance about the degree of lung disten-tion at peak inspiration.
Another source of Pes error is attributable to patientpositioning. Most of the seminal studies of lung mechanicshave been performed in upright subjects. In the supineposition the heart rests almost directly over the esophagealballoon catheter, so the measured pressure reflects the addedweight of the mediastinum. In addition, FRC is lower inthe supine position, which raises pleural pressure. Severalstudies have documented a Pes increase of 5–7 mm Hgupon recumbence.2,24,25 This has been dismissed as an ar-tifact, and the general assumption is that Pes cannot beused to estimate pleural pressure in supine patients. How-ever, defining this effect as an artifact is itself somewhatartifactual. If an upright patient exhaled to a lower lungvolume, pleural pressure would be higher, as defined bythe pressure-volume mechanics of the thorax, so the con-tribution of decreased FRC in the supine position to in-creased Pes is not an artifact. Furthermore, the pressurebeneath the heart in the esophagus may be similar to thepressure beneath the heart in the nearby pleural space, or
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2 167
under consolidated lung that has the same density as tis-sue. Therefore, even in the supine position the Pes proba-bly equals pleural pressure in some regions. It probablydoes not, however, represent an average pressure distend-ing the lung.
Washko et al24 performed a detailed study to quantifythe Pes change in the supine position and to parse out thecontributions of cardiac weight and decreased FRC. Thedifference attributable to the weight of the mediastinumwas 2.9 cm H2O, but there was substantial inter-individualvariability in this cardiac artifact. The standard deviationwas 2.1 cm H2O, which means that in a third of the sub-jects the artifact from the weight of the mediastinum ex-ceeded 5 cm H2O. Thus, the ability to accurately estimatetranspulmonary pressure in the supine position is quitelimited, even in healthy subjects. By extension, the as-sumption that a given transpulmonary pressure indicateslung recruitment at end-expiration or a safe degree of lungdistention at peak inspiration is limited.
The optimal positioning of the balloon catheter in thesupine patient has also been questioned. Higgs et al mea-sured the �Pes/�Paw in 10 anesthetized but spontaneouslybreathing patients without lung disease prior to surgery.33
A short esophageal balloon was positioned 5, 10, 15, and20 cm above the gastroesophageal junction in all the pa-tients. The accuracy of Pes measurements was studied bycomparing changes in Pes and Paw during inspiratory effortwith an occluded airway. Every patient had a locationwhere the �Pes/�Paw was near 1, averaging 0.98 � 0.03 inthe group. However, this optimal location was not neces-sarily at the widely used locus 10 cm above the gastro-esophageal junction. Three of the 10 patients showed largediscrepancies between �Pes and �Paw when the balloonwas positioned at the standard 10 cm position: �Pes/�Paw
was 1.2, 0.75, and 0.6 in those 3 patients at that position.Thus, the balloon positioning artifact in Pes may be vari-able and unpredictable in supine patients.
The degree to which even an accurate and artifact-freePes accurately represents the generalized pressure distend-ing the lungs has been the subject of much controversy.The pressure in the pleural space can be measured directlyin animal studies. This pressure shows a gradient fromnon-dependent to dependent regions. In normal animalsand healthy humans, this gradient is about 0.2 cm H2O percentimeter of vertical distance.1,34,35 It is attributable toboth the pressure from overlying lung and tissue, and dif-ferences between the relaxed shape of the lung and thechest wall. In edematous, injured, and dense lungs thepleural pressure rises more steeply with dependent depth.16
Because Pes is quite high in patients with ARDS, it hasbeen argued that the small potential errors in measurementare irrelevant, and the signal-to-noise ratio is sufficient toguide clinical measurement. However, the measurementerrors have been quantified only in normal subjects. The
Fig. 5. Hypothetical pressure-volume relationships in the lungs ofa normal subject and in a patient with acute respiratory distresssyndrome (ARDS). The solid line indicates the true relationshipbetween lung volume and transpulmonary pressure. The dashedline shows the relationship as estimated from esophageal pres-sure, in which esophageal pressure slightly overestimates pleuralpressure. This leads to a small leftward shift of the pressure-vol-ume relationship, and underestimation of transpulmonary pres-sure. Because the normal lung compliance is high and tidal breath-ing occurs on the linear portion of this relationship, the errors intranspulmonary pressure at end-expiration and end-inspiration aresimilar and small. In a patient with ARDS, lung compliance is re-duced and the relationship is curvilinear. If the tidal volume endson the more horizontal portion of the lung compliance curve, smallerrors in transpulmonary pressure at end-expiration can neverthe-less be associated with large underestimations of transpulmonarypressure at end-inspiration. This can falsely reassure the clinicianthat lung over-distention is not present.
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
168 RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2

same characteristics that increase Pes in ARDS patientscan also increase the error, and it would be an error oflogic to assume otherwise.
The topography of pleural pressure in critically ill pa-tients is unknown. However, when regional lung mechan-ics are not uniform, it is likely that regional pleural pres-sure is also quite variable. In animals in which expansionof one lung or lobe is prevented by bronchial occlusion,the pleural pressure change in the occluded region is lessthan over other lung regions during lung inflation.36 Sim-ilar inferences have been made in non-critically-ill patientswith obstructive or restrictive disease, in whom a lobe isoccluded and used as a tonometer to estimate the change inpressure surrounding it when the rest of the lung is inflat-ed.37 Patients with ALI typically have very heterogeneousand asymmetric lung disease. Some flooded or atelectaticlung regions fail to inflate with inspiration. The range ofcardiac volume encountered is much larger than normal,pleural effusions are common, and pleural fibrosis andpneumothoraces are often present. There is little rationaleand no data to support the assumption that the measure-ment of Pes in such patients bears the same relationship toaverage pleural pressure as in upright healthy subjects.Moreover, the exaggerated change in pleural pressure withgravitational height in ARDS ensures that, in regions be-low the level of the esophageal balloon, the airways willhave a substantially higher pleural pressure, and in regionsabove the balloon pleural pressure will be substantiallylower. Even if PEEP were titrated to optimize lung volumeat the level of the esophagus, lung regions elsewhere wouldbe under-inflated or over-inflated.
Thus, with meticulous technique, an esophageal ballooncatheter can measure the pressure in the esophagus, whichin an upright normal subject represents an average pres-sure on the surface of the lung. In the supine normal sub-ject the pressure is elevated to an individually variableamount by the weight of the mediastinal contents. Thoughit probably corresponds to the pressure at some parts of thelung surface, it may no longer reflect an average surfacepressure. In critically ill patients the relationship betweenthe measured Pes and the average pleural pressure is un-known. However, extrapolating from healthy subjects, it isupon that unknown relationship that clinical decisions havebeen based.
Using Esophageal Pressure to Guide VentilatorManagement in ALI/ARDS
This approach has been tested in one study,14 reviewedabove, which found that setting PEEP based on standard-ized transpulmonary pressure/FIO2
tables, compared to thestandardized PEEP/FIO2
tables used in the ARDS Networktrials, led to PEEP being increased in almost all patients inthat arm. As would be expected on higher PEEP, oxygen-
ation improved in the group managed with transpulmonarypressure data. Transpulmonary pressure at end-inspirationremained below a safe limit in all patients in that group.There was no significant difference in 28-day or 180-daymortality.
Because that investigation was designed to show greaterimprovements in oxygenation in the patients managed us-ing transpulmonary pressure data, it concluded early as apositive study. However, this does not validate Pes as “im-portant in clinical decision making.” The higher PEEPused was entirely predictable, based on the prior knowl-edge that transpulmonary pressure would be negative atend-expiration in most patients.13 That higher PEEP wouldimprove oxygenation was likewise predictable from pre-vious experience.10-12 It remains uncertain whether lunginjury was ameliorated or important outcomes improvedby transpulmonary-pressure-based PEEP. About half thepatients randomized to the transpulmonary-pressuregroup, after PEEP was adjusted, had Pplat � 30 cm H2O.Some had Pplat � 40 cm H2O (see Fig. 3). Since pleuralpressure is heterogeneous in ARDS patients, the “safe”transpulmonary pressure in the regions near where Pes
was measured provide no assurance that injurious over-distention was avoided in other lung regions. The bestthat can be concluded is that in the lung regions wherePes happens to have equaled pleural pressure, end-ex-piratory collapse and end-inspiratory over-distentionmay have been avoided. The improved oxygenation doesnot help reveal the optimal balance between recruitmentand distention.
We may therefore dismiss the use of transpulmonarypressure, on the basis that it does not provide accurateinformation upon which to base clinical decisions, andbecause the decisions can be made based on simpler, lessinvasive methods. A protocol-based approach that individ-ualizes PEEP based on lung recruitability was studied byGrasso et al.38 They based their PEEP decisions on theconcavity of the pressure-time plot of Paw during constant-flow inflation. Those data are available on any mechanicalventilator with a graphical interface. They calculated aquantitative “stress index” from the shape of the pressure-time relationship, but the index can be interpreted quali-tatively as follows: when the plot was concave up (accel-erating increase in pressure as inflation proceeds), theyreasoned that the lung was over-distended and PEEP shouldbe reduced. If the plot was concave down, lung inflationwas recruiting lung regions and the PEEP was safe. In 15patients ventilated per the ARDS Network PEEP/FIO2
ta-ble, they found that the majority of patients were on toomuch PEEP (Fig. 6). This is precisely opposite of whatwas suggested by the measurement of transpulmonary pres-sure.14 Moreover, reducing the PEEP until the stress index
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2 169
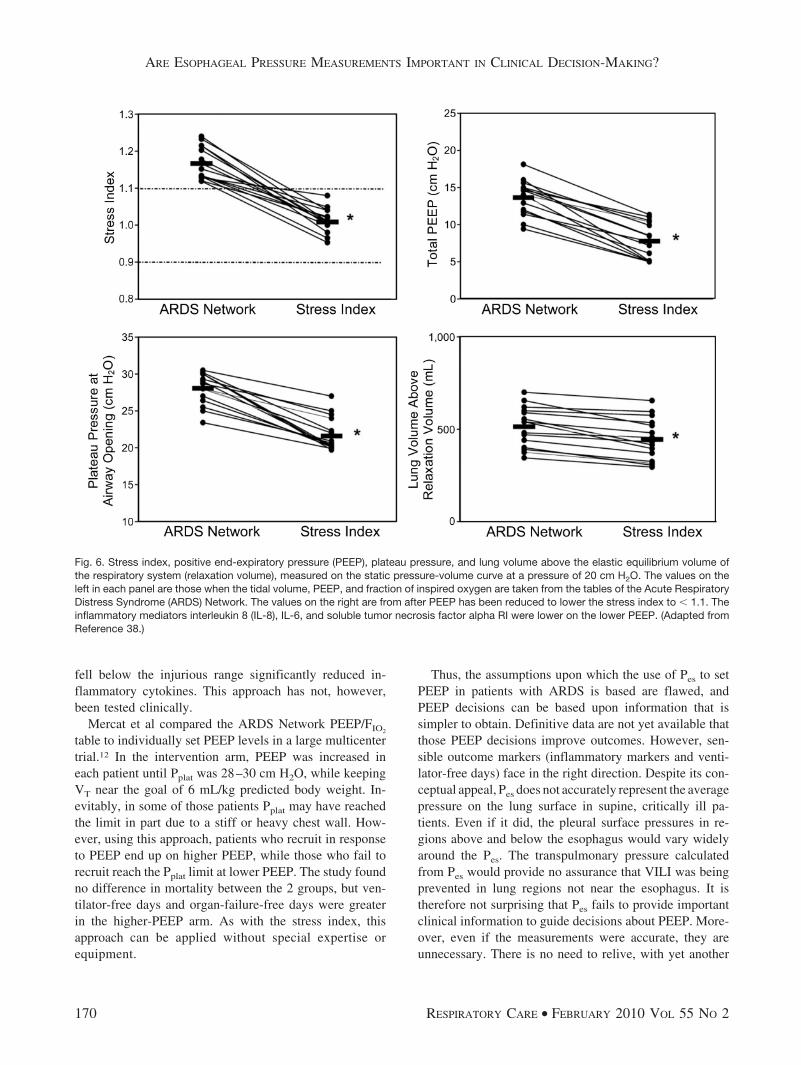
fell below the injurious range significantly reduced in-flammatory cytokines. This approach has not, however,been tested clinically.
Mercat et al compared the ARDS Network PEEP/FIO2
table to individually set PEEP levels in a large multicentertrial.12 In the intervention arm, PEEP was increased ineach patient until Pplat was 28–30 cm H2O, while keepingVT near the goal of 6 mL/kg predicted body weight. In-evitably, in some of those patients Pplat may have reachedthe limit in part due to a stiff or heavy chest wall. How-ever, using this approach, patients who recruit in responseto PEEP end up on higher PEEP, while those who fail torecruit reach the Pplat limit at lower PEEP. The study foundno difference in mortality between the 2 groups, but ven-tilator-free days and organ-failure-free days were greaterin the higher-PEEP arm. As with the stress index, thisapproach can be applied without special expertise orequipment.
Thus, the assumptions upon which the use of Pes to setPEEP in patients with ARDS is based are flawed, andPEEP decisions can be based upon information that issimpler to obtain. Definitive data are not yet available thatthose PEEP decisions improve outcomes. However, sen-sible outcome markers (inflammatory markers and venti-lator-free days) face in the right direction. Despite its con-ceptual appeal, Pes does not accurately represent the averagepressure on the lung surface in supine, critically ill pa-tients. Even if it did, the pleural surface pressures in re-gions above and below the esophagus would vary widelyaround the Pes. The transpulmonary pressure calculatedfrom Pes would provide no assurance that VILI was beingprevented in lung regions not near the esophagus. It istherefore not surprising that Pes fails to provide importantclinical information to guide decisions about PEEP. More-over, even if the measurements were accurate, they areunnecessary. There is no need to relive, with yet another
Fig. 6. Stress index, positive end-expiratory pressure (PEEP), plateau pressure, and lung volume above the elastic equilibrium volume ofthe respiratory system (relaxation volume), measured on the static pressure-volume curve at a pressure of 20 cm H2O. The values on theleft in each panel are those when the tidal volume, PEEP, and fraction of inspired oxygen are taken from the tables of the Acute RespiratoryDistress Syndrome (ARDS) Network. The values on the right are from after PEEP has been reduced to lower the stress index to � 1.1. Theinflammatory mediators interleukin 8 (IL-8), IL-6, and soluble tumor necrosis factor alpha RI were lower on the lower PEEP. (Adapted fromReference 38.)
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
170 RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2

physiologic variable, the folly of our 30-year infatuationwith the pulmonary artery catheter.
Summary
In patients with ALI/ARDS, pleural pressure in somelung regions is substantially higher than in upright normalsubjects. Basing ventilator settings on a maximum allow-able Paw of 30–35 cm H2O may leave large portions of thelung under-inflated and at risk of VILI from repetitiveairway opening and closing. It is logical that estimatingpleural pressure from Pes and setting PEEP to achieve atarget transpulmonary pressure may allow higher PEEP inmany patients without over-distending lung regions thatare already recruited. However, there may also be irreduc-ible errors in the measurement of pleural pressure in su-pine patients with lung disease. In addition to potentialartifacts, pleural pressure varies greatly from non-depen-dent to dependent regions in injured lungs. Nevertheless,PEEP that yields a safe transpulmonary pressure rangeduring tidal breathing, based on Pes measurements, mayunder-inflate or over-inflate lung regions at a distance fromthe esophagus. Pilot studies have shown that ventilatorsettings based on transpulmonary pressure generally yieldhigher PEEP and better oxygenation than the PEEP/FIO2
tables of the ARDS Network trials. Whether that yieldsbetter clinical outcomes will have to await larger clinicaltrials.
REFERENCES
1. Milic-Emili J, Mead J, Turner JM, Glauser EM. Improved techniquefor estimating pleural pressure from esophageal balloons. J ApplPhysiol 1964;19(2):207-211.
2. Mead J, Gaensler EA. Esophageal and pleural pressures in man,upright and supine. J Appl Physiol 1959;14(1):81-83.
3. Jubran A, Grant BJ, Laghi F, Parthasarathy S, Tobin MJ. Weaningprediction: esophageal pressure monitoring complements readinesstesting. Am J Respir Crit Care Med 2005;171(11):1252-1259.
4. Slutsky AS. Lung injury caused by mechanical ventilation. Chest1999;116(1 Suppl):9S-15S.
5. The Acute Respiratory Distress Syndrome Network. Ventilation withlower tidal volumes as compared with traditional tidal volumes foracute lung injury and the acute respiratory distress syndrome. N EnglJ Med 2000;342(18):1301-1308.
6. Dreyfuss D, Saumon G. Ventilator-induced lung injury: lessons fromexperimental studies. Am J Respir Crit Care Med 1998;157(1):294-323.
7. Puybasset L, Cluzel P, Chao N, Slutsky AS, Coriat P, Rouby JJ. Acomputed tomography scan assessment of regional lung volume inacute lung injury. The CT Scan ARDS Study Group. Am J RespirCrit Care Med 1998;158(5 Pt 1):1644-1655.
8. Vieira SR, Puybasset L, Richecoeur J, et al. A lung computed to-mographic assessment of positive end-expiratory pressure-inducedlung overdistension. Am J Respir Crit Care Med 1998;158(5 Pt1):1571-1577.
9. Gattinoni L, Pesenti A, Avalli L, Rossi F, Bombino M. Pressure-volume curve of total respiratory system in acute respiratory failure.
Computed tomographic scan study. Am Rev Respir Dis 1987;136(3):730-736.
10. Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A,Ancukiewicz M, et al. Higher versus lower positive end-expiratorypressures in patients with the acute respiratory distress syndrome.N Engl J Med 2004;351(4):327-336.
11. Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, CooperDJ, et al. Ventilation strategy using low tidal volumes, recruitmentmaneuvers, and high positive end-expiratory pressure for acute lunginjury and acute respiratory distress syndrome: a randomized con-trolled trial. JAMA 2008;299(6):637-645.
12. Mercat A, Richard JC, Vielle B, Jaber S, Osman D, Diehl JL, et al.Positive end-expiratory pressure setting in adults with acute lunginjury and acute respiratory distress syndrome: a randomized con-trolled trial. JAMA 2008;299(6):646-655.
13. Talmor D, Sarge T, O’Donnell CR, Ritz R, Malhotra A, Lisbon A,Loring SH. Esophageal and transpulmonary pressures in acute re-spiratory failure. Crit Care Med 2006;34(5):1389-1394.
14. Talmor D, Sarge T, Malhotra A, O’Donnell CR, Ritz R, Lisbon A,et al. Mechanical ventilation guided by esophageal pressure in acutelung injury. N Engl J Med 2008;359(20):2095-2104.
15. Gattinoni L, Vagginelli F, Chiumello D, Taccone P, Carlesso E.Physiologic rationale for ventilator setting in acute lung injury/acuterespiratory distress syndrome patients. Crit Care Med 2003;31(4Suppl):S300-S304.
16. Mutoh T, Lamm WJ, Embree LJ, Hildebrandt J, Albert RK. Volumeinfusion produces abdominal distension, lung compression, and chestwall stiffening in pigs. J Appl Physiol 1992;72(2):575-582.
17. Malbrain ML, Chiumello D, Pelosi P, Wilmer A, Brienza N, Mal-cangi V, et al. Prevalence of intra-abdominal hypertension in criti-cally ill patients: a multicentre epidemiological study. Intensive CareMed 2004;30(5):822-829.
18. Fusco MA, Martin RS, Chang MC. Estimation of intra-abdominalpressure by bladder pressure measurement: validity and methodol-ogy. J Trauma 2001;50(2):297-302.
19. Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP,Lorenzi-Filho G, et al. Effect of a protective-ventilation strategy onmortality in the acute respiratory distress syndrome. N Engl J MedFeb 5 1998;338(6):347-354.
20. Ranieri VM, Suter PM, Tortorella C, De Tullio R, Dayer JM, BrienzaA, et al. Effect of mechanical ventilation on inflammatory mediatorsin patients with acute respiratory distress syndrome: a randomizedcontrolled trial. JAMA 1999;282(1):54-61.
21. Villar J, Kacmarek RM, Perez-Mendez L, Aguirre-Jaime A. A highpositive end-expiratory pressure, low tidal volume ventilatory strat-egy improves outcome in persistent acute respiratory distress syn-drome: a randomized, controlled trial. Crit Care Med 2006;34(5):1311-1318.
22. Gattinoni L, Caironi P, Carlesso E. How to ventilate patients withacute lung injury and acute respiratory distress syndrome. Curr OpinCrit Care 2005;11(1):69-76.
23. Agostoni E, Hyatt RE. Static behavior of the respiratory system. In:Macklem PT, Mead J, editors. Handbook of Physiology, volume 3,part 1. American Physiological Society; 1986:113-130.
24. Washko GR, O’Donnell CR, Loring SH. Volume-related and vol-ume-independent effects of posture on esophageal and transpulmo-nary pressures in healthy subjects. J Appl Physiol Mar 2006;100(3):753-758.
25. Ferris BG, Mead J, Frank NR. Effect of body position on esophagealpressure and measurement of pulmonary compliance. J Appl Physiol1959;14(4):521-524.
26. Knowles J, Hong K, Rahn H. Possible errors using esophageal bal-loon in determination of pressure-volume characteristics of the lungand thoracic cage. J Appl Physiol 1959;14(4):525-530.
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2 171

27. Pelosi P, D’Andrea L, Vitale G, Pesenti A, Gattinoni L. Verticalgradient of regional lung inflation in adult respiratory distress syn-drome. Am J Respir Crit Care Med 1994;149(1):8-13.
28. de Chazal I, Hubmayr RD. Novel aspects of pulmonary mechanics inintensive care. Br J Anaesth 2003;91(1):81-91.
29. Pelosi P, Chiumello D, Calvi E, Taccone P, Bottino N, Panigada M,et al. Effects of different continuous positive airway pressure devicesand periodic hyperinflations on respiratory function. Crit Care Med2001;29(9):1683-1689.
30. Pelosi P, Goldner M, McKibben A, Adams A, Eccher G, Caironi P, etal. Recruitment and derecruitment during acute respiratory failure: anexperimental study. Am J Respir Crit Care Med 2001;164(1):122-130.
31. Hager DN, Brower RG. Customizing lung-protective mechanicalventilation strategies. Crit Care Med 2006;34(5):1554-1555.
32. Baydur A, Behrakis PK, Zin WA, Jaeger M, Milic-Emili J. A simplemethod for assessing the validity of the esophageal balloon tech-nique. Am Rev Respir Dis 1982;126(5):788-791.
33. Higgs BD, Behrakis PK, Bevan DR, Milic-Emili J. Measurement ofpleural pressure with esophageal balloon in anesthetized humans.Anesthesiology 1983;59(4):340-343.
34. Glazier JB, Hughes JM, Maloney JE, West JB. Vertical gradient ofalveolar size in lungs of dogs frozen intact. J Appl Physiol 1967;23(5):694-705.
35. Proctor DF, Caldini P, Permutt S. The pressure surrounding thelungs. Respir Physiol 1968;5(1):130-144.
36. Hubmayr RD, Margulies SS. Effects of unilateral hyperinflation onthe interpulmonary distribution of pleural pressure. J Appl Physiol1992;73(4):1650-1654.
37. Martin CJ, Young AC, Ishikawa K. Regional lung mechanics inpulmonary disease. J Clin Invest 1965;44:906-913.
38. Grasso S, Stripoli T, De Michele M, Bruno F, Moschetta M, An-gelelli G, et al. ARDSNet ventilatory protocol and alveolar hyper-inflation: role of positive end-expiratory pressure. Am J Respir CritCare Med Oct 15 2007;176(8):761-767.
Discussion
MacIntyre: I think we have to givethe Fessler/Talmor team the award formost entertaining presentations.
Dan, I was struck by Gordon Ber-nard’s editorial1 on your paper2 that sug-gested that if you had used the high-PEEP/FIO2
table from the ARDSNetwork’s ALVEOLI [Assessment ofLow Tidal Volume and Elevated End-Expiratory Volume to Obviate Lung In-jury] trial,3 you might have seen some-thing very similar. He argued that theALVEOLI results, which found higherPaO2
/FIO2ratios, also found that plateau
pressure went up, but not quite as muchas the increase inPEEP,whichsuggestedimproved compliance. Is the esophagealtechnique you described just a morecomplicated way of instituting theARDS Network high-PEEP strategy?
1. Bernard GR. PEEP guided by esophagealpressure: any added value? N Engl J Med2008;359(20):2166-2168.
2. Talmor D, Sarge T, Malhotra A, O’DonnellCR, Ritz R, Lisbon A, et al. Mechanicalventilation guided by esophageal pressurein acute lung injury. N Engl J Med 2008;259(20):2095-2104.
3. ARDS Clinical Trials Network. Higher ver-sus lower positive end-expiratory pressuresin patients with the acute respiratory distresssyndrome. N Engl J Med 2004;351:327-336.
Talmor: I need to rebut Hank here.We never said that esophageal pres-sure reflects pleural pressure acrossthe entire lung. The only time it’s ever
actually been compared, in dogs withALI, it reflected pleural pressure inthe mid-lung portion. So that clearlyrequires further validation, and Vilarin Spain is doing a similar validationstudy in humans.
As to whether the stress index givesequivalent information, well, maybe.Obtaining the stress index is not as easyas it looks in Grasso’s paper.1 He pre-sents the very clearest tracings in hispaper, but in clinical practice these areoften difficult to interpret. Secondly, thestress index has never been validated ina clinical trial. There are devices on themarket to measure esophageal pressure,so I am happy to tell you that Hopkinswill be able to buy a few when theystart using this technique.
About your question: did we justrepeat the ALVEOLI high-PEEP trial?I don’t think so. The PEEPs we ap-plied were higher than those in AL-VEOLI, and we titrated PEEP to thepatient’s individual respiratory physi-ology rather than basing it on a one-size-fits-all sliding scale. Now, step-ping backwards, the only way we’reever going to know this is with a largertrial with multiple centers, to see howgeneralizable is this technique. Butsome pre-clinical investigation defi-nitely needs to be done: we need astudy showing some kind of imaging,and we need to validate the correla-tion between pleural pressure andesophageal pressure in humans.There’s a lot more work to do before
I’d say that esophageal pressure mea-surements are the way to go in ARDS.However, the question at hand is, doesit add valuable information? I still be-lieve it stands to reason that there maybe valuable information here.
1. Grasso S, Stripoli T, De Michele M,Bruno F, Moschetta M, Angelelli G, et al.ARDSNet ventilatory protocol and alveo-lar hyperinflation: role of positive end-ex-piratory pressure. Am J Respir Crit CareMed Oct 15 2007;176(8):761-767.
Epstein: Let’s say you do anotherclinical trial and it looks positive—although I would wonder about an evenmore aggressive PEEP strategy in thecontrol arm, because there is a differ-ence between what you found and whatALVEOLI and the other trials found—about a 4 cm H2O difference in PEEP.The question is widespread applica-tion. We can’t even get people to turndown the tidal volume, and now we’regoing to ask them to place a specialcatheter that requires special exper-tise?
What I haven’t heard about is themaintenance of these catheters. I’veplaced hundreds of esophageal cathe-ters in spontaneously breathing pa-tients, but not in patients on ventila-tors, and the catheter is in for just ashort period. These catheters move alot, so to keep one in would require alot of maintenance work. Is this reallyfeasible for general clinical use?
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
172 RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2

Talmor: Let me answer that on ahigher philosophical level, and thenon a lower practical level. We alwaysseem to think that we have to designour trials and our interventions forsome hypothetical intensivist whodoesn’t have any expertise with theintervention. Most intensivists and re-spiratory therapists I meet are reallyinterested in doing what’s best for theirpatients. If we present a compellingargument, I believe they’ll buy it.
At the practical level, at Beth IsraelDeaconess Medical Center, I wouldsay that, after a few years of work,more than 70% of the respiratory ther-apists can place the balloon and makeconsistent measurements. We have agreat respiratory therapy director, RayRitz, who was integral to this trial,and he’s worked hard with his people.I would say that placing an esopha-geal balloon and making measure-ments is no more difficult than plac-ing a central line or many of the otherthings we do. If the clinical usefulnessis proven, I believe that people will adoptthe technique and use it. In a multi-cen-ter trial we always consider the abilityof other centers to get up and runningwith it.
Gay: Neil, I go along with your sug-gestion of why not just use the higher-PEEP table? But I would add one morething. I’d always thought of it as amore appropriate treatment for patientswith so-called non-pulmonary ARDSpatients, with whom you might getaway with higher PEEP. Wouldn’t youthen have a better opportunity to justuse that higher PEEP if you confinedit to that patient population?
Talmor: I’d argue that patients withso-called non-pulmonary ARDS arethe ones in whom you really want toknow the chest wall component andto titrate based on that, so I would sayno. The point is to individualize thetherapy. It’s a major misunderstand-ing of our paper to say that it was ahigh-PEEP versus low-PEEP trial. It
wasn’t. It’s about individualizing tothe patient’s physiology, based on cer-tain assumptions; the name of the gamefor us is individualization.
I’ve been doing this for 9 years, andwe can still get fooled: you’re sure you’llhave to increase the PEEP in a certainpatient, but then you place the balloonand it shows you that you don’t, or viceversa. Consider intra-abdominal hyper-tension in a medical patient; you see theskinniest medical patient with a soft ab-domen, but they require a higher PEEPbased on our method.
Fessler: Dan, the positioning of theesophageal balloon is somewhat prob-lematic, and was even in your study.In some patients you couldn’t pass itinto the stomach, and so you positionedit somewhat arbitrarily. If you movethe balloon several centimeters up theesophagus, how much does that changethe Pes measurement?
Talmor: That is a misinterpretationof the paper. In some patients it wasdifficult to pass it below the loweresophageal junction, so we couldn’tmeasure gastric pressure, but we couldand did optimally place the balloonby looking at cardiac oscillations,which is the way to do it. In sponta-neously breathing patients you’d lookat an occlusion test and things likethat, but you can’t do that in patientswho aren’t making spontaneous res-pirations. And the balloon seems tostay put unless someone pulls it, and afew centimeters up or down does notseem to make a big difference.
Gentile: I’ve placed several hundredof these over the years, for variousreasons, and the most useful one is anasogastric tube with a balloon on it,which doesn’t add any extra lines ortubes to the patient. You put it in dur-ing intubation, and it seems to be morehelpful than having to put another tubein after the nasogastric and Dobhofftubes are in.
Talmor: Is the nasogastric tube withthe integrated esophageal balloon pro-prietary to one ventilator company?
Siobal: That was a BiCore product.A couple years ago, Alex Adams pub-lished an abstract1 of a study in whichhe took a regular nasogastric tube, po-sitioned it in the esophagus, and thenattached a manometer to the bedsidemonitor, and it correlated with theesophageal balloon measurements.
What about lateral decubitus posi-tioning? Does it improve the measure-ment accuracy? We also occasionallyfind esophageal balloon measurementsuseful in morbidly obese patients,where you want to show the intensivecare team that we need to keep thispatient on PEEP of 20 cm H2O and dospontaneous breathing trials from highPEEP so we can wean them of the ven-tilator without the lungs collapsing.
1. Adams A, Shapiro R, Armaganides A. Apotential for monitoring esophageal pres-sure with open-ended, fluid-filled, or air-filled catheters (abstract). Respir Care2001;46(10):1108.
Talmor: We haven’t used nasogas-tric tubes the way you described, butwe have looked at the relationship be-tween gastric pressure and esophagealpressure, and they correlate prettynicely, so there’s a possibility that wemay be able to titrate PEEP based ongastric pressure. We haven’t tried dif-ferent body positions. Your point aboutobese patients is really good; whenwe do the measurements, we find thatthe chest wall compliance in obese pa-tients is normal. Then we need to lookat the absolute pressures and titratePEEP based on those baseline pres-sures rather than looking at the chestwall compliance, which can often bequite good in these patients. These pa-tients definitely benefit from this.
Branson: I’ve placed a lot of thesetoo. When the nasogastric tube is po-sitioned optimally for esophageal pres-sure measurement, it’s not positionedoptimally to empty the stomach, so you
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2 173

can get into a push-and-pull with thenurses—literally, with them putting itwhere they need it, and me trying to putit where I need it. I know you can placeit and a therapist can place it, but howoften does it become displaced and howoften do you have to reposition it? Assomebody who works in a trauma in-tensive care unit, where things changequickly, I think the ARDS Network ta-ble doesn’t provide the ability to deliverthe necessary PEEP.
MacIntyre: Use the higher table,Rich!
Branson: Oftentimes we are look-ing at lung mechanics and not reallyworrying so much about oxygenation.Dan’s ideas have a lot of interest inthe group I work with.
Talmor: One thing that I hope wasclear in the paper is that we usuallymade these measurements only once aday. We found that after optimally re-cruiting the lung that one time, thepatients usually became stable, at leastfrom a respiratory standpoint. If thepatient’s situation changed, and ofcourse there are unstable trauma pa-tients where that could easily happen,we would make the measurementsmore often. It’s not something you’remeasuring every half hour, and youhave to make sure it’s in the right placebefore you make the measurements.
With regard to the other tubes inthe esophagus, we’ve found no mea-surement artifact with either a Dob-hoff tube or a regular nasogastric tube.The times we’ve run into trouble iswhen there are 2 tubes down there andthe esophageal balloon gets in the mid-dle between the 2 tubes, and becauseof the very low inflation volume theballoon might not be touching the sidesof the esophagus and that throws yourmeasurements off. So a surgical pa-tient with a nasogastric tube and an-other tube down into the jejunum orsomething is a problem.
Sessler: To me, the individualiza-tion is really attractive, and I liked
that about the Mercat et al1 study, butI think there was an over-inflationproblem in the patients with milderALI. Your individualized approach re-quires more work, Dan. Is Mercat’stechnique another way of modifyingPEEP based on individual patient char-acteristics?
Also, was there a difference in ratesof air leak? You didn’t present any-thing on air leaks.
1. Mercat A, Richard, JC, Vielle B, Jaber S,Osman D, Diehl JL, et al; Expiratory Pres-sure (Express) Study Group. Positive end-expiratory pressure setting in adults withacute lung injury and acute respiratory dis-tress syndrome: a randomized controlledtrial. JAMA 2008;299(6):646-655.
Talmor: There were no incidents ofair leak in any patients in either group.
I’m not sure I fully understand theMercat study. By limiting the PEEPto a plateau pressure of 28 cm H2O,you’re actually giving your sickest,least compliant patients the leastPEEP, which is not something Iwould do, and it doesn’t sound likeRich would either. By increasingtheir PEEP in the sickest patientsyou’re very quickly going to get to aplateau pressure of 28 cm H2O, whilethe least sick patients are going toget the most PEEP. That is very dif-ferent from my practice, so I can’tsay I really understand that study.
I’m postulating now, but I think partof their rationale was a strong beliefamong many French intensivists thata plateau pressure of greater than28 cm H2O can lead to right-ventric-ular failure. We’re very different fromthe Mercat study, and I wouldn’t rec-ommend using that as an alternative. Itmay be better, but I wouldn’t use it asan alternative; they are completely dif-ferent strategies.
Hess: Dan, the question, as you sug-gested, is, “Well, maybe gastric pres-sure is as good as esophageal pres-sure?” If that’s the case, then why notuse bladder pressure? That’s a wholelot easier to measure and most all these
patients already have a Foley catheter.Another comment I would make is, ifwe’re going to individualize the PEEPto lung mechanics, I would considerthe stress index. I’m intrigued by thestress index, and I’ve been looking atit in the intensive care unit. I haven’tbeen doing the curve fitting and cal-culating the b-coefficient, but I cantell you that if you look for it, you cansee the curve change as you changethe PEEP and tidal volume.
Talmor: We have looked at bladderpressure and gastric pressure, andthere’s a similar correlation; bladderpressure may be useful as well. Oneof the problems with bladder pressureis that by the time the signal gets downto the bladder, you lose the respira-tory variation. So you’re essentiallyleft with one number, it’s kind of aflat tracing, as opposed to the gastricpressure, where you still see respira-tory variation. In terms of the stressindex, this is anecdotal, but we com-pared our measurements to the stressindex and they seemed to show signalin the same direction. I think there’s aformal study going on comparing ourmeasurements to the stress index.
MacIntyre: Hank, you mentionedusing esophageal pressure to predictthe outcome of a spontaneous breath-ing trial. That’s different than whatwe’ve been talking about, but I don’tunderstand why we need all these pre-dictors for spontaneous breathing tri-als. Why not just do it?
Epstein: Agreed.
Fessler: I think all three of us areon the same page.
MacIntyre: I spend a lot of timereviewing papers for Dean and othereditors, and paper after paper after pa-per keeps trying to find ways of pre-dicting the outcome of a spontaneousbreathing trial. It befuddles me. Justdo the trial.
ARE ESOPHAGEAL PRESSURE MEASUREMENTS IMPORTANT IN CLINICAL DECISION-MAKING?
174 RESPIRATORY CARE • FEBRUARY 2010 VOL 55 NO 2