-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
1/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Are psychoeducational smoking cessationinterventions for
coronary heart disease patientseffective? Meta-analysis of
interventions
M. Huttunen-Lenz1*, F. Song1 and F. Poland2
1School of Allied Health Professions, School of Medicine, Health
Policy and Practice,University of East Anglia, Norwich, UK
2School of Allied Health Professions, University of East Anglia,
Norwich, UK
Purpose. This systematic review aimed to assess the
effectiveness of psychoeduca-tional smoking cessation interventions
for coronary heart disease (CHD) patients; and
to examine behaviour change techniques used in interventions and
their suitability to
change behavioural determinants.
Methods. Multiple bibliographic databases and references of
retrieved articles were
searched for relevant randomized controlled studies. One
reviewer extracted and a
second reviewer checked data from included trials. Random
effects meta-analyses were
conducted to estimate pooled relative risks for smoking
cessation and mortality
outcomes. Behaviour change techniques used and their suitability
to change behavioural
determinants were evaluated using a framework by Michie,
Johnston, Francis,
Hardeman, and Eccles.
Results. A total of 14 studies were included. Psychoeducational
interventions
statistically significantly increased point prevalent (RR 1.44,
95% CI, 1.201.73) and
continuous (RR 1.51, 95% CI, 1.181.93) smoking cessation, and
statistically non-
significantly decreased total mortality (RR 0.73, 95% CI,
0.461.15). Included studiesused a mixture of theories in
intervention planning. Despite superficial differences,
interventions appear to deploy similar behaviour change
techniques, targeted mainly at
motivation and goals, beliefs about capacity, knowledge, and
skills.
Conclusions. Psychoeducational smoking cessation interventions
appear effective
for patients with CHD. Although questions remain about what
characteristics
distinguish an effective intervention, analysis indicates
similarities between the
behaviour change techniques used in such interventions.
Alongside well-established medical, pharmacological, and
surgical interventions forcoronary heart disease (CHD), patients
are also often encouraged to modify their
* Correspondence should be addressed to M. Huttunen-Lenz, Queens
Building, University of East Anglia, Norwich NR4 7TJ,UK (e-mail:
[email protected]).
The
British
Psychological
Society
749
British Journal of Health Psychology (2010), 15, 749777
q 2010 The British Psychological Society
www.bpsjournals.co.uk
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
2/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
existing behavioural risk factors such as smoking, lack of
exercise, and diet (Isles et al.,2002; NSF-CHD, 2000). However, as
changing longstanding habits can be difficult,
psychoeducational interventions have been developed to help in
modifying behaviouralrisk factors, but evidence of the
effectiveness of such interventions is mixed(Dusseldorp, van
Elderen, Maes, Meulman, & Kraaij, 1999; Godin, 1989; Isles et
al.,2002; Moore, 1997; Mullen, Mains, & Velez, 1992; NSF-CHD,
2000; Rees, Bennett, West,Davey Smith, & Ebrahim, 2004;
Sebregts, Falger, & Bar, 2000). One of factors whichcontributes
to contradictions in the body of review evidence appears to be a
current
lack of consensus in defining a psychoeducational intervention
(e.g., Rees et al., 2004).This makes it more difficult for
clinicians to confidently offer practical advice andguidance in
planning such interventions.
While a wide range of interventions has been included in earlier
reviews of
psychoeducational interventions, these have often omitted
smoking cessation-onlyinterventions. When the effectiveness of
smoking cessation is considered (Critchley &Capewell, 2003),
these interventions can form an important, though specialized, part
ofthe secondary prevention and rehabilitation of CHD patients
(Isles et al., 2002).Available review evidence suggests that
behaviour modification interventions can beeffective in increasing
smoking cessation for hospitalized patients in general
(Rigotti,Munafo, & Stead, 2007), and for CHD patients (Van
Berkel, Boersma, Roos-Hesselink,Erdman, & Simoons, 1999). These
reviews, however, have included studies with mixedparticipant
populations (Rigotti et al., 2007) and mixed intervention aims (Van
Berkel
et al., 1999). Furthermore, available evidence is unclear about
identifying thecharacteristics of an effective smoking cessation
intervention (Van Berkel et al., 1999), which means that only
limited use can be made of the review evidence to develop
practical applications.Michie, Johnston, Francis, Hardeman, and
Eccles (2008) suggest that while including
theory may be useful in the design of behaviour change
interventions, theory by itselfoffers only limited guidance for
designing interventions. Building on their previouswork, which
identified theoretical constructs that can be used to explain
behaviourchange (Michie & Abraham, 2004), Michie et al. (2008)
developed a comprehensive listof behaviour change techniques and a
framework of how they link to theoreticalconstructs to be used in
intervention planning. Michie and Abraham (2004), identify 11key
behavioural constructs, or determinants, namely:
social/professional role and
identity; knowledge; skills; beliefs about capabilities; beliefs
about consequences;motivation and goals; environmental context and
resources; social influences; emotion;action planning; and
motivation, attention and decision processes that can be used
toexplain behaviour. Behavioural determinants may be influenced by
behaviour changetechniques, 137 of which are listed by Michie et
al. (2008). Using an initial set of 35behaviour change techniques,
researchers independently evaluated techniquessuitability to change
each of the behavioural determinants. Depending on the
achievedconsensus, behaviour change techniques were rated as agreed
use, agreed non-use,disagreement, and uncertain. Agreed use and
agreed non-use referred to the
agreement by Michie et al. (2008) on the suitability or
non-suitability of a technique toinfluence a behavioural
determinant; disagreement meant that this technique hadevaluated
both suitable and unsuitable, while uncertain refers to
evaluatorsuncertainty about the techniques effectiveness. Michie et
al. (2008) intended this
framework to help effective intervention planning by making
explicit which behaviourchange techniques are considered effective
to change which behavioural determinants.While this framework was
initially intended to be used for intervention planning, we
750 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
3/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
suggest that it may be applied retrospectively to interventions
in meta-analysis, to clarifyintervention features and
mechanisms.
As a part of a review of research on psychoeducational cardiac
rehabilitationinterventions, the present paper reports findings
from our meta-analysis of randomizedtrials of non-pharmacological
psychoeducational smoking cessation interventions inCHD patients.
We also report our findings from applying the framework by Michie
et al.(2008) in retrospectively evaluating behaviour determinants
targeted in the studies andtechniques used to change smoking
behaviour. We will also discuss issues associated
with difficulties in evaluating psychoeducational interventions
and related problemsthat arose in this meta-analysis.
Methods
Identification of studies
We initially searched the Cochrane Controlled Trials Register,
PsycINFO, MEDLINE,CINAHL, and Dissertations and Abstracts
International databases from the 1970s
onwards to locate any studies that evaluated effectiveness of
psychoeducational cardiacrehabilitation interventions using a
comparison group design. The search termsincluded words such as
myocardial ischemia, rehabilitation, lifestyle, and RCT(randomized
controlled trial) (see Table 1 for the MEDLINE search strategy). We
also
checked reference lists of previous reviews and retrieved any
relevant studies.
Study selection
From initially identified references for research on
psychoeducational cardiacrehabilitation interventions, we selected
randomized controlled studies of non-pharmacological interventions
for smoking cessation among patients with CHD. For astudy to be
included, it needed to be written in the English language, to
provide data onpoint prevalent smoking cessation, continuous
smoking cessation, or mortality as anoutcome and to have a minimum
of 6 months follow-up period. While only studieswritten in English
were selected for full text review, we recorded the number of
studiesexcluded because of the language restriction. One reviewer
selected studies for full-text
review based on titles and abstracts and in unclear cases, the
opinion of a second
reviewer was sought.
Data extraction
Using data extraction sheetsdesignedfor this review, onereviewer
extracted anda secondreviewer checked thedata. Data that
wecollectedfrom theprimary studies included studydesign,
intervention and patient characteristics, point prevalent (number
of non-smokers
at the point of measurement), continuous smoking cessation
(number of participants notsmoking during the whole length of
follow-up period), and mortality. We contacted allstudy authors
after data extraction to request any additional data not published
in thearticles. We then included in the analyses, any data obtained
from the authors.
Assessment of study quality We assessed the methodological
quality of the included studies, covering therandomization process,
the intervention and participant description, blinding, outcome
Smoking cessation for CHD patients 751
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
4/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
verification, and completeness of follow-up. We decided not to
rank studies based onthe quality assessment, but recorded
weaknesses in the study methodology using thepre-set assessment
criteria.
Statistical methods
We collected study results data from all available follow-up
time points, but used data atthe longest follow-up, in the main
analyses. Relative risk was used as the outcomestatistic to
calculate effectiveness of the interventions. We calculated
relative risk forthree outcomes: point prevalent, continuous
smoking cessation, and total mortality.Point prevalent smoking
cessationdescribes the number of participants not smoking at
the measurement point regardless of their previous smoking
status, while continuoussmoking cessation describes the number of
participants not smoking during the wholelength of the study
follow-up. Studies differed in how they reported participants
lost
Table 1. MEDLINE search strategy
Limit: English language
1. Myocardial ischemia (medical subject heading (MESH) term,
focus, all subheadings)
2. Coronary ADJ3 (adjacent) disease
3. Isch$ ADJ3 disease
4. Cardiovascular disease
5. Myocard$ infarct$
6. Heart attack
7. Heart infarct$8. Angina
9. Coronary artery bypass (MESH, focus, all subheadings)
10. Coronary ADJ3 bypass
11. CABG (Coronary artery bypass graft)
12. PTCA (Percutaneous transluminal coronary angioplasty)
13. Coronary ADJ3 angioplasty
14. Coronary ADJ3 angiograph$
15. Rehabilitation (MESH, focus, all subheadings)
16. Rehabilit$
17. Psychoeducat$
18. Psychoeducat$
19. Health educat$
20. Lifestyle
21. Life ADJ1 style22. Counselling
23. Counselling
24. Health ADJ3 advice
25. Health ADJ1 behav$
26. Cognitive ADJ1 behav$
27. Behav ADJ3 change
28. Behav$ ADJ3 risk
29. Control group
30. Trial
31. Randomized controlled trial
32. RCT
33. Comparison group
752 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
5/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
to follow-up. To avoid overestimating intervention
effectiveness, we calculated relativerisk so that cases lost to
follow-up and deaths were considered as negative outcomes,
i.e., as continuing to smoke. We report the results of the
intention-to-treat analysis inthis paper.
For smoking cessation outcomes, a relative risk of larger than
one indicated apositive outcome, i.e., that the intervention was
successful in increasing smokingabstinence. Relative risk for
mortality was calculated so that a value of smaller than
oneindicated lower mortality in the intervention group. We carried
out sensitivity analyses
to investigate any outlying studies, effects of including two
studies which methods ofrandomization was not optimal (Burt et al.,
1974; Johnson, Budz, Mackay, & Miller,1999), effects of
including one study where we were uncertain about the diagnosis
ofsome study participants (Mohiuddin et al., 2007), and effects of
including one study
which had both these methodological problems (Bolman, de Vries,
& van Breukelen,2002a). RevMan (2008) computer program was used
to conduct random effectsmeta-analyses and to graphically present
the data. We used Peters method to testfunnel plot asymmetry, which
is a regression analysis of association betweentreatment effect and
a variable based on sample size (Peters, Sutton, Jones, Abrams,
&Rushton, 2006).
Subgroup analyses ( post hoc ) were used to investigate possible
causes ofheterogeneity in meta-analysis. In the first subgroup
analysis, we investigated theeffects of use of pharmacotherapy in
the intervention, firstly with all studies that offered
pharmacotherapy and then with the studies that offered
pharmacotherapy only for theintervention group. For
pharmacotherapy, we refer to use of bupropion or
nicotinereplacement therapy (NRT). The second subgroup analysis
investigated effects of
studies explicitly using a theory in intervention planning. For
this analysis, we dividedstudies between those that explicitly
specified a theoretical model and those that didnot. In the latter
group, we included those studies that mentioned behaviour
changetechniques. The third subgroup analysis looked at the effects
of intervention intensity, in which we classified the interventions
as intensive, less intensive, or could beintensive interventions.
The intensity of could be intensive interventions wasdependent on
participants response to the initial intervention, with the
interventioninput increased for those participants who failed to
stop smoking or who struggled withstopping altogether after the
initial intervention. Finally, we investigated the effect of
follow-up time to intervention effectiveness. For this analysis,
we used three data points:up to 6, 12, and 24 months onwards. We
conducted statistical tests of interactionbetween independent
subgroups (Altman & Bland, 2003).
Evaluation of behavioural determinants and behaviour change
techniques
Applying the framework described by Michie et al. (2008) to
interventions investigatedin studies, we estimated which
behavioural determinants were targeted by theinterventions and
which behaviour change techniques appeared to have been used
tochange the behavioural determinants. We conducted the evaluation
process bycomparing the description of the intervention with the
framework of Michie et al.(2008). For example, if the intervention
description stated that health care professionalsadvised
participants about the health consequences of smoking cessation,
we
considered that the targeted behavioural determinant was
knowledge and thebehaviour change technique was behavioural
information. Finally, based onrecommendations by Michie et al.
(2008), we evaluated the suitability of behaviour
Smoking cessation for CHD patients 753
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
6/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
change techniques in relation to targeted behavioural
determinants. In this review, theterm agreed technique is used to
refer to any technique considered effective by Michie
et al. (2008).
Investigation of process variables
We also investigated process variables reported in the studies.
Process variables arecommonly termed mediating variables that can
help describe the process through
which, here, change in smoking behaviour happens.
Results
The initial search for psychoeducational cardiac rehabilitation
interventions identified8,026 citations, of which 249 were
potentially eligible studies and 178 of these appearedto be
randomized controlled trials. Twenty of the randomized controlled
studies were
identified as potentially eligible smoking cessation studies. We
included 11 relevanttrials after scrutinizing the full text
articles, and added three additional studies afterinspection of
references of retrieved studies and previous reviews. In two cases,
thesame study has two published articles (Bolman, de Vries, &
van Breukelen, 2002a,b;Ockene et al., 1992; Rosal et al., 1998). A
major cause for the study exclusion was
inclusion of participants with other diagnoses than CHD, which
included peripheral vascular disease, cardiopulmonary disease,
chronic obstructive pulmonary disease,arrhythmias, and
hypertension. Based on the abstracts, we did not identify any of
thearticles not written in English as potentially eligible
studies.
Main characteristics of the included studies are summarized in
Table 2 anddescriptions of psychoeducational interventions used in
these studies are presented inTable 3. Studies included 1,792
participants in the intervention condition and 1,766
participants in the control condition, ranging from 87 to 789
participants recruited perstudy. All the interventions were
initiated in the hospital, and all apart from Hajek,Taylor, and
Mills (2002) included some form of home follow-up after hospital
discharge.Only one study did not include women among participants,
although women were inminority in each study. Studies differed in
how far they required motivation to stopsmoking as well in the
availability of nicotine replacement products. A range of
approaches were also taken to defining smoking status, so that
some studies recruitedonly current smokers (smoking just before the
hospital admission), whereas others alsorecruited recent
quitters.
Quality of included studies
The results of quality assessment are summarized in Table 4. The
randomization methodwas clearly appropriate in 8 of the 14 included
studies. Two studies were cluster-randomized trials (Bolman et al.,
2002a,b; Johnson, 1999). One trial allocated patientsaccording to
the day of admission (Burt et al., 1974); and the method of
patientallocation was unclear in three studies (Mohiuddin et al.,
2007; Ockene et al., 1992;Rigotti et al., 1994). Only six studies
had adequate concealment of allocation. Trial
participants were generally comparable at the baseline. The
descriptions ofinterventions and inclusion criteria were
appropriate in all included studies.Participants, intervention
provider and outcome assessors were not blinded, except
754 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
7/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
2.
Maincharacteristicsoftheincludedtria
ls
Study
Setting,country
Interventiontheoryand
intensity
Samplesize
(intervention/control)
Diagnosis,smokingstatusbefore
admission
Age,male(%)
Bolman
etal.
(2002a,b
)
Hospitalandout-patient
clinic,T
heNetherlands
Sociallearningtheory,
attitudesocialinfluence
efficacy(ASE)model;less
intensive
388/4
01
MI,anginapectoris,other.
Smokinginthe7daysbefore
admission
Mean57(11),
male(78%)
Burtetal.(1974)
Hospitalandout-patient
clinicandcommunity,
UK
Notspecified;intensive
125/98
MI.SmokingatthetimeofMI
attack
Notspecified,
male(100%)
Dornelasetal.
(2000)
Hospitalandcommunity,
USA
Transtheoreticalmodel,
MartlattGordonsrelapse
preventiontechniques;
lessintensive
54/46
AcuteMI.Smokingduringthe
monthbeforeadmission
From27to83,
male(77)
Feeney
etal.
(2001)
Hospitalandout-patient
clinic,Australia
Notspecified;couldbe
intensive
96/1
02
AcuteMI.Smokingorusing
tobaccoproductsduringthe
weekbeforeadmission
Meanage:53.9
(11),
male(64%)
Hajeketal.(2002)
Hospital,U
K
Notspecified;less
intensive
274/2
66
MI,CABG.Currentorrecent
smokers;notsmokingsince
admission;motivatedtostop
smoking
Under76,mean
age:56(10),
male(77%)
Johnsonetal.
(1999)
Hospitalandcommunity,
Canada
Stagesofchange;less
intensive
50/52
Medicaland/orsurgicalcardia
c
diagnosis.Self-reportedsmok
ers
inthecontemplationstageto
stopsmoking
Over19,meanage:
55(13),male(75%)
Mohiud
dinetal.
(2007)
Hospitalandcommunity,
USA
Stagesofchange(author
inf.);intensive
109/1
00
Acutecoronarysyndrome,
de-compensatedheartfailure.
Dailysmokersforatleast5ye
ars
Aged3075years,
meanage:55(11),
male(63%)
Smoking cessation for CHD patients 755
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
8/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
2.
(Continued)
Study
Setting,country
Interventiontheoryand
intensity
Samplesize
(intervention/control)
Diagnosis,smokingstatusbefore
admission
Age,male(%)
Ockeneetal.
(1992)
andRosal
etal.(1
998)
Hospitalandout-patient
clinicandcommunity,
USA
Behavioural
multicomponent
approach;couldbe
intensive
135/1
32
Patientswithoneormore
arteriographicalcoronaryartery
lesions.Smokingatleast5
cigarettes/dayanytimeduring
the
last2monthsbeforeadmission
Aged3075years,
meanage:53,
male(75%)
Quist-P
aulsenand
Gallefoss(2003)
Hospitalandcommunity,
Norway
Feararousal;couldbe
intensive
118/1
22
MI,CABG,unstableAngina.D
aily
smokersuntilstartofthepres
ent
coronarysymptoms
Under76,
meanage:57(9),
male(75%)
Reidet
al.(2003)
Hospitalandcommunity,
Canda
Transtheoreticalmodel
(authorinf.);lessintensive
126/1
28
PTCA,M
I,CABG.Fiveormore
cigarettesperdayduringthe
monthbeforeadmission.
Motivationtoquitwasinquired
Over18,meanage:
54(9),male(80%)
Reid,Pipe,
Quinlan,andOda
(2007)
Hospitalandcommunity,
Canada
Notspecified;couldbe
intensive
50/50
CHD.Fiveormorecigarettes
perday
Over18,meanage:
54(9),male(67%)
Rigotti,McKool,
andShiffman
(1994)
Hospitalandcommunity,
USA
Notspecified;less
intensive
44/43
CABG.Smokedoneormore
packsofcigarettesin6months
beforeadmission
Meanage:59(8),
male(77%)
Smitha
ndBurgess
(2009)
Hospitalandcommunity,
Canada
MarlattandGordons
relapsepreventionmodel;
intensive
137/1
39
MI,CABG.Smokinginthemo
nth
beforetheadmission
Over18,meanage:
54(10),male(83%)
Taylor,Houston-
Miller,Killen,and
DeBusk(1990)
Hospital,out-patient
clinicandcommunity,
USA
Sociallearningtheory;
couldbeintensive
86/87
AcuteMI.Smokingduringthe
last
6monthsbeforeadmission
Under70,mean
age:58(9),male
(86%)
Note.M
l,Myocardialinfarction.
756 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
9/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
3.
Descriptionofexperimentalandcontro
linterventions
Study
Interventiontheory
Experimentalgroup
Controlgroup
Bolman
etal.
(2002a,b
)
Sociallearningtheory,A
SE
model,theoriesofrelapse
prevention,t
hestageof
changetheory,and
motivationalinterview
strategies
Cardiologistprovidedstopsmokingadvice,w
hichwas
followedby1530standardizedind
ividualcounselling
andprovisionofself-helpmaterialbyanurse.
Counsellingwastailoredtopatientsstageofchangeand
includedassessmentofsmokingbeh
aviour,motivationto
quit,consequencesofquitting,barr
ierstoquitting,and
encouragementtosetadateforqu
itting.Aftercarewas
providedbycardiologistatthefirstout-patient
appointment,whichaddressedvariousaspectsof
smoking.PatientsGPwasinformed
oftheintervention
andaskedtonotesmokingbehavio
ur
Usualcare,nospecialstressonsmoking
cessation
Pharmacotherapynotoffered
Pharmacotherapynotoffered
Burtetal.(1974)
Notspecified(harmfuleffec
ts
ofsmoking)
Aconsultantexplainedeffectsofsm
okingandadvised
patientstostopsmoking.Participantswereinformedthat
smokingcessationwaslikelytoreduceoccurrenceof
anotherMI.Ifparticipantsfailedtostopsmoking,further
advicewasprovidedandreinforced
byleafletsandadvice
booklet.Afterdischargeparticipantswerefollowedina
clinicandsmokingcessationadvice
wasextendedto
familymembers.Communitynurse
visitedathomeand
gaveadviceregardingsmokingandotherriskfactors
Participantsrece
ivedstandardhospital
advice(unclearaboutdetails),without
follow-upathos
pital.Acommunitynurse
visitedpatientsa
thomeoneormoreyears
latertoseekinformationonsmoking
Pharmacotherapynotoffered
Pharmacotherapynotoffered
Dornelasetal.
(2000)
Transtheoreticalmodel,
motivationalintervention,
andMartlattGordons
relapsepreventiontechniques
(copingskillstraining);
dependingonthestageof
change
A20minbedsidesmokingcessationcounsellingby
psychologistwhoevaluatedparticipantscurrentstageof
changeandbasedthecounsellingcontextonthatstage.
Afterdischargeparticipantswerecontactedby
telephoneafterweeks1,4,8,12,16
,20,and29.Bedside
andtelephonecounsellingcombinedaspectsof
motivationalinterviewingandrelap
seprevention
Participantsrece
ivedashortintervention
lastingabout10minfromapsychologist.
Interventioncon
sistedverbalandwritten
recommendationtowatchanon-line
educationalvideowhileinhospital.
Participantswerealsoreferredtolocal
AmericanHeart
orLungAssociations
smokingcessatio
nresources
Pharmacotherapynotoffered
Pharmacotherapynotoffered
Smoking cessation for CHD patients 757
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
10/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
3.
(Continued)
Study
Interventiontheory
Experimentalgroup
Controlgroup
Feeney
etal.
(2001)
Notspecified
Relapseprevention:coping
skillstraining(self-efficacy,
Bandurassocialcognitive
theory1986)
StanfordHeartAttackStayingFreep
rogramme.
Participantswereadvisedonsmokin
gcessationand
medicalimplicationsofcessation.Participantsreceiveda
manual,whichidentifiedhigh-riskrelapsesituationsand
exercisestomanagethesesituations.
Audiotapesreviewed
programmesmainpointsandprovidedprogressivemuscle
relaxation.Afterdischargetelephonecontactwasinitiated
weeklyfor4weeksandat2,3,6,and12monthswith
additionalsupportandadvicegivenwhennecessary
Participantsrece
ivedusualcareoffering
verbalandwrittenadviceaboutsmoking
cessation.Includ
edaneducationalvideo
whileinhospital,andreviewbyanalcohol
anddrugassessm
entunit(ADAU)nurse.
Participantswerealsoofferedout-patient
counsellingandfollow-upbyADAUclinic
at3,6,and12m
onthintervals
Pharmacotherapy:informedthatNRTavailable
outsideofhospital.NouseofNRTreported
Pharmacotherapy:informedthat
NRTavailable
outsideofhospital.No
useofNRTreported
Hajeketal.
(2002)
Notspecified(multiple
components,including
informationabouthealth
benefitsofquitting;buddy
support;andself-efficacy)
Participantsweregivenabookletaboutsmokingand
cardiacrecoveryandcarbonmonoxidereadingwas
recorded.T
hebookletchallengedbeliefsthatsmoking
reducesstressandadvisedonrelapseprevention.A
quiz-testedparticipantsknowledge
ofthebooklet,
whichwasalsodiscussedwithanu
rse.Participants
signedadeclarationandastickero
ntheirnotes
remindedstaffofsmokingcessationattempt
Participantsweregivenbothverbaladvice
tostopsmoking
andBritishHeart
Foundationbookletsmokingandyourheart
Pharmacotherapynotoffered.
Veryfew
appearedtohaveusedNRT
Pharmacotherapynotoffered.Very
fewappeared
tohaveusedNRT
Johnsonetal.
(1999)
Stagesofchange;problem
solving,reinforcingthe
patientsself-efficacy
Participantsreceivedabookletandwereshownavideo
abouteffectsofsmoking,importance
ofsmokingcessation,
cessationprocess,andsmokingtrigg
ers.Thevideo
encourageddiscussionofsmokinghabitsandtosetaquit
date.Onthesecondvisit,smokingcessationskillswere
reviewedinavideoandparticipants
developedasmoking
cessationplanandstrategiestomanagesmokingtriggers.
Sixtelephonecontactsduringthefir
st3monthsafter
dischargeencouragedandreinforcedcessationefforts
Participantsinthecontrolgroupreceived
routinecare,wh
ichincludedstopsmoking
advice,butnotasystematicintervention
Pharmacotherapynotoffered
Pharmacotherapynotoffered
758 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
11/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
3.
(Continued)
Study
Interventiontheory
Experimentalgroup
Controlgroup
Mohiud
dinetal.
(2007)
Multiplecomponents:
relaxationtraining,
contingencycontracting,
socialsupport,copingskills,
stimuluscontrol,andnicotine
fading
Priortodischargeallparticipantsreceivedastandardized
counselling(30min)andself-helpm
aterialonsmoking
cessation
Priortodischargeallparticipantsreceived
astandardizedcounselling(30min)and
self-helpmateria
lonsmokingcessation
Participantsintheinterventiongroupwereaskedto
meetatobaccocessation(60min)weeklyfor3months
insmallgroupsorindividually.Counsellingincluded
relaxationtraining,contingencycontracting,social
support,copingskills,stimuluscontrol,nicotinefading,
andriskfactormodificationsuchasdietandexercise
Noadditionalinterventionprovidedinthe
controlgroup
Pharmacotherapyoffered,usedby75%
Pharmacotherapynotformally
offered;17%reporteduseofNRTor
bupropion
Ockeneetal.
(1992)
and
Rosale
tal.
(1998)
Behaviouralmulticomponen
t
approach:including
motivationalsupport,
behaviouralself-managemen
t
strategies,relaxation,and
scopingskillstraining
Allreceivedstandardizedinitial(10
15min)adviceto
stopsmoking,includingareviewofhealthrisksof
smokingandthebenefitsofquitting,andalistof
communitytreatmentprogrammes
Allreceivedstan
dardizedinitial(1015
min)advicetostopsmoking,includinga
reviewofhealth
risksofsmokingandthe
benefitsofquitting,andalistofcommunity
treatmentprogrammes
Participantsintheinterventiongroupreceiveda30-min
in-patientcounsellingsession,anindividualout-patient
counsellingvisit,andfollow-upcounsellingtelephone
calls.Participantsalsoreceivedinte
rventionmanual,
relaxationtapes,maintenancetraining,andself-help
material
Noadditionalinterventionprovidedinthe
controlgroup
Pharmacotherapynotoffered
Pharmacotherapynotoffered
Quist-P
aulsen
(2003)
Feararousal;relapse
preventioncopingskills
Participantswereofferedgroupsessionswithanurse,
withavideoshownandabookletab
outCHDandadvice
aboutquitsmoking
Participantswereofferedgroupsessions
withanurse,withavideoshownanda
bookletaboutC
HDandadviceaboutquit
smoking
Participantsintheinterventiongrou
preceivedaspecially
producedbookletabouthealthben
efitsofquitting
smoking,informationaboutsmokin
gcessation,relapse
prevention,nicotinereplacementproducts,highrisk
Noadditionalinterventionprovided
Smoking cessation for CHD patients 759
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
12/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
3.
(Continued)
Study
Interventiontheory
Experimentalgroup
Controlgroup
relapsesituations,andactionplans.Participantswere
toldinafeararousalmessagethatiftheycontinued
smokingtheywerelikelytohaveanotherheartattack.
Spouseswhosmokedwerealsoaskedtoquit.Telephone
contactwasinitiatedafterdischarge
andparticipantshad
consultationinout-patientclinic
Pharmacotherapy:useofNRT
recommendedfor
thosewithstrongwithdrawalu
rges,usedby36%
Pharmacotherapynotexplicitly
offered,but28%reportedusingNRT
Reidet
al.(2003)
Positivereinforcement,
problemsolving,andsocial
support
Allreceivedbriefbedside,510minindividual
counsellingbyanursecounsellor;andaself-helpbooklet
andinformationonadditionalsuppo
rtfromprimarycare
physiciansprovided
Allreceivedbrie
fbedside,510min
individualcounsellingbyanursecounsellor;
andaself-helpbookletandinformationon
additionalsuppo
rtfromprimarycare
physiciansprovided
Afterhospitaldischarge,participant
sinthestepped-care
groupreceivedthree20-minface-to-facecounselling
sessionswithanurse-counsellorover8weeks.I
f
participantsreportedabstinenceth
eyreceivedpositive
feedbackandwereremindedabouttherelapse
preventioninformationinthebook
let.Ifparticipants
reportedsmoking,counsellingwas
startedandNRT
madeavailable
Noadditionalinterventionprovided
Pharmacotherapy:NRTprovid
edfor4weeks
afterrelapse(26.2%relapsedafterinitialsmoking
cessation)
Pharmacotherapynotoffered.Six
reportedusingNRTandfour
bupropion
Reidet
al.(2007)
Notspecified(self-efficacy,
socialsupport,problem
solving,anddevelopmentof
copingstrategies)
Allreceivedstandardusualcare,includedpersonalized
advicetostopsmokingandNRTif
necessary,brief
bedsidecounsellingbyanurse-counsellor,self-help
guide,andinformationaboutout-pa
tientandcommunity
smokingcessationprogrammes
Allreceivedstan
dardusualcare,included
personalizedadv
icetostopsmokingand
NRTifnecessary,briefbedsidecounselling
byanurse-counsellor,self-helpguide,and
informationaboutout-patientand
communitysmokingcessationprogrammes
760 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
13/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
3.
(Continued)
Study
Interventiontheory
Experimentalgroup
Controlgroup
Participantsinthetreatmentgroup
receivedinteractive
voiceresponsivetelephony(IVR)in
tervention.A
fter
dischargeanautomatedtelephonysystemcontacted
participantsondays3,14,and30p
ost-discharge.Calls
inquiredsmokingstatusandassessedriskofrelapse.
Thoseparticipantsthatreportedeitherrelapsewith
willingnesstofurthersmokingcessationattemptorlow
confidencetostaysmokefree,wereflaggedintheIVR
systemsoftware.Nurse-specialistc
ontactedthese
participantstoofferadditionalassistance.A
dditional
interventionsincludeduptothree
20-mincounselling
sessionsover8week-periodcouns
ellor-ledtelephone
sessions,encouragement,helpinid
entifyingsituations
thatwereunderminingtheirconfidenceandpossible
solutions,andaccesstopharmacot
herapy
Noadditionaltreatmentsprovided
Pharmacotherapy:NRTofferedinhospitaland
afterrelapse.Usedby70%inh
ospitalandby14%
afterdischarge
Pharmacotherapy:accesstoNRT
duringhospita
lizationifrequired.
NRTwasused
by58%inhospitaland
by14.3%durin
gfollow-up
Rigotti
etal.
(1994)
Behaviouralandcognitive
methods
BasedontheAmericanLungAssociationsInControl
programme,theinterventionwasa
standardized
counsellingprogramme,whichincludededited
videotape,patientmanual,andthre
e20-minsessionsto
individualpatientsbyaresearchnurse.Familymembers
werealsoencouragedtoparticipate.Within2weeksof
dischargeparticipantswerecontactedbytelephoneto
offersupportandshortcounselling
Participantsrece
ivedstandardpost-
operativecare;includingbriefadvicenotto
smokeaspartofagrouplecture
Pharmacotherapynotoffered
Pharmacotherapynotoffered
Smitha
nd
Burgess(2009)
MarlattandGordonsrelapse
preventionmodel
Nursereviewedtwopamphletswiththepatients,w
hich
containedinformationabouthowt
oquitandwhereto
findhelp.Nurseplacedanotetop
atientschartsto
remindtheirphysicianstodeliverscriptednon-smoking
messageatbedside
Nursereviewed
twopamphletswiththe
patients,w
hichcontainedinformation
abouthowtoquitandwheretofindhelp.
Nurseplacedanotetopatientschartsto
remindtheirphysicianstodeliverscripted
non-smokingme
ssageatbedside
Smoking cessation for CHD patients 761
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
14/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
3.
(Continued)
Study
Interventiontheory
Experimentalgroup
Controlgroup
Intheinterventiongroupparticipantsreceivedbedside
counselling(4560min)andeducationalmaterialsto
takehome(video,workbook,audiotape),andseven
telephonecounsellingsessions(at2
,7,1
4,21,3
0,45,6
0
daysafterdischarge).E
ducationconsistedpersonalised
riskassociatedwithsmoking,benefitsofquitting,and
helptodevelopstrategiestostaysm
okefree.Telephone
counsellingfocusedonrelapseprev
entionbydeveloping
cognitive,behavioural,andsocialsu
pportstrategiesfor
situationsidentifiedashighrisksitu
ations
Pharmacotherapynotpartof
intervention,butavailableif
requested,use
dby34%
Pharmacotherapynotpartofintervention,but
availableifrequested,usedby
34%
Tayloretal.
(1990)
Sociallearningtheory,relapse
preventioncopingskills
training
Anursecounsellorreviewedbenefitsofsmoking
cessation,providedamanualandaudiotapesfor
identifyinghighriskrelapsesituations,andprovided
exercisestocopewiththesesituations.A
fterdischarge
telephonecontactwasinitiatedtomonitorrelapseand
offersupportandadvicefor4mon
ths.Out-patient
appointmentwasofferedwhennee
ded.NRTwas
availableandpatientssignedacontracttoquitsmoking
Participantsrece
ivednospecificsmoking
cessationhelp,b
utwerefreetoattend
hospitalsstopsmokingclasses
Pharmacotherapy:NRTavailab
leforstrong
withdrawalurges
Pharmacotherapynotoffered
762 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
15/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table4.
Assessmentofstudyqualityofincluded
trials
Study
Random
allocation
method
Allocation
concealed
?Trialarms
similarat
baseline?
Interventions
clearly
described?
Inclusion
eligibility
criteriaset?
O
utcome
assessor
blind?
Intervention
provider
blind?
Participants
blind?
Cessation
verified?
Total
drop-out
rate(%)
Follow-up
(months)
Bolman
etal.
(2002a,b
)
Randomselectionand
assignmentof
hospitals,seven
randomlyassigned,
fourself-selected
condition
No
Somediff.Yes
Yes
No
No
No
No
28
12
Burt(19
74)
Bythedayof
admission
No
Unclear
Yes
Yes
No
No
No
No
0
.12
Dornela
s(2000)
Drawnfrom
envelopes
No
Yes
Yes
Yes
No
No
No
No
20
12
Feeney(2001)
Sealedenvelopes
Yes
Yes
Yes
Yes
No
No
No
Bioch.
66
12
Hajek(2
002)
Seriallynumbered,
opaque,sealed
envelopes
Yes
Yes
Yes
Yes
No
No
No
Bioch.
11
12
Johnson
(1999)
Byadmissionunit
(clusterRCT)
No
Somediff.Yes
Yes
No
No
No
No
14
6
Mohiuddin(2007)
UCwithoutblock
assignment
No
Somediff.Yes
Yes
No
No
No
Bioch.
4
24
Ockene
(1992)
andRos
al(1998)
UC
No
Yes
Yes
Yes
No
No
No
Bioch.
40
60
Quist-Paulen
(2003)
Seriallynumbered,
sealedenvelopes
Yes
Somediff.Yes
Yes
No
No
No
Bioch.
9
12
Reid(20
03)
Usingarandom
numberstable,
stratifiedbyreason
foradmission
UC
Yes
Yes
Yes
No
No
No
Bioch.a
sampleo
nly
(N25)
15
12
Reid(20
07)
Thirdparty,computer
generatedlist
Yes
Yes
Yes
Yes
No
No
No
No
16
12
Rigotti(1994)
UC
No
Yes
Yes
Yes
No
No
No
Bioch.
24
66
Smoking cessation for CHD patients 763
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
16/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table4
.(Continued)
Study
Random
allocation
method
Allocation
concealed
?Trialarms
similarat
baseline?
Interventions
clearly
described?
Inclusion
eligibility
criteriaset?
O
utcome
as
sessor
blind?
Intervention
provider
blind?
Participants
blind?
Cessation
verified?
Total
drop-out
rate(%)
Follow-up
(months)
Smith(2
009)
Envelopescontaining
computer-generated
random-number,
randompermuted
blocksof10,stratified
byacuteMIand
CABG
Yes
Yes
Yes
Yes
Ye
s
No
No
Proxy
11
12
Taylor(1990)
Serialnumbered,
sealedenvelopes,
openedbyatrial
coordinator
Yes
Yes
Yes
Yes
No
No
No
Bioch.
25
12
Note.U
C,Unclear.
764 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
17/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
the trial by Smith and Burgess (2009) in which outcome assessor
was blinded. Smokingcessation was verified in nine studies
biologically or by proxy confirmation. Reported
drop-outs during the follow-up (including deaths) ranged from 0
to 66%.
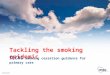
Point prevalent smoking cessation
Thirteen included studies provided sufficient data on point
prevalent smoking cessation
(Figure 1). Heterogeneity between studies was statistically
significant (p , :0001;
I2
73%). The combined effect size indicated that in comparison to
controlinterventions, psychoeducational interventions were
associated with a higher rate ofpoint prevalent smoking cessation
(RR 1.44, 95% CI, 1.201.73). For this outcome, weconducted one
sensitivity analysis by excluding four studies: Bolman et al.
(2002a), Burtet al. (1974), Johnson et al. (1999), and Mohiuddin et
al. (2007). The heterogeneitybetween studies remained statistically
significant (I2 60%), as did the pooled relativerisk (RR 1.28, 95%
CI, 1.071.52).
Continuous smoking cessation
Again, there is statistically significant heterogeneity across
studies (Figure 2). Thepooled relative risk for the 10 studies that
reported this outcome indicated thatpsychoeducational interventions
were more effective in increasing continuous smoking
cessation than interventions in the control group (RR 1.51, 95%
CI, 1.181.93). For thisoutcome, we performed two sensitivity
analyses: first excluding Bolman et al. (2002a)and Mohiuddin et al.
(2007), and then excluding Feeney et al. (2001). The results
ofthese sensitivity analyses were similar to the result of the main
analysis using all included
studies.
Total mortality
Heterogeneity across 10 studies that reported total mortality
was not statistically
significant (Figure 3). Pooled relative risk indicated a
tendency for a lower total mortality
Study or subgroup
Bolman 2002
Burt 1974
Dornelas 2000
Hajek 2002
Johnson 1999
Mohiuddin 2007
Quist-Paulsen 2003
Reid 2003
Reid 2007
Rigotti 1994
Rosal 1998
Smith 2009
Taylor 1990
Total (95% CI)
Total events
Heterogeneity: Tau2 = 0.07; Chi2 = 44.92, df = 12 (P<
0.0001); I2 = 73%
Test for overall effect: Z = 3.97 (P< 0.0001)
164
79
28
99
23
43
57
49
23
25
47
73
51
761
388
125
54
274
50
109
118
126
50
44
135
137
86
1696
124
27
16
108
16
9
44
46
17
23
37
48
26
541
401
98
46
266
52
100
122
128
50
43
132
139
87
1664
Events Total Events Total Weight
10.1%
8.0%
6.4%
9.8%
6.0%
4.5%
8.6%
8.4%
6.2%
7.6%
7.8%
8.9%
7.7%
100.0%
1.37 (1.13, 1.65)
2.29 (1.62, 3.25)
1.49 (0.93, 2.39)
0.89 (0.72, 1.10)
1.50 (0.90, 2.48)
4.38 (2.25, 8.53)
1.34 (0.99, 1.81)
1.08 (0.79, 1.49)
1.35 (0.83, 2.21)
1.06 (0.73, 1.55)
1.24 (0.87, 1.78)
1.54 (1.17, 2.04)
1.98 (1.38, 2.86)
1.44 (1.20, 1.73)
Treatment Control Risk ratioM-H, random, 95% CI
Risk ratioM-H, random, 95% CI
0.2 0.5 1 2 5
Favours control Favours treatment
Figure 1. Point prevalent smoking cessation outcome comparing
effectiveness of psychoeducational
smoking cessation intervention to control condition.
Smoking cessation for CHD patients 765
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
18/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
in the psychological intervention group, although the difference
was not statisticallysignificant (RR 0.73, 95% CI, 0.461.15). After
excluding the studies by Bolman et al.
(2002a) and Mohiuddin et al. (2007), there were no substantial
changes in result (RR0.58, 95% CI, 0.281.18).
Peters method was used to statistically test funnel plot
asymmetry (funnel plots notshown). Tests for the point prevalent
(p
:
38), continuous (p :
51) smoking cessationand total mortality (p :76) suggested that
the funnel plots were not statisticallysignificantly asymmetric,
indicating that studies with smaller sample size are
notsignificantly associated with greater treatment effects. The
results of funnel plot testingshould be interpreted with caution
because of the small number of studies included.
Subgroup analyses
The results of the subgroup analyses are summarized in Figure 4.
Studies that providedpharmacotherapy for smoking withdrawal
symptoms, either nicotine replacement
Study or Subgroup
Bolman 2002
Dornelas 2000
Feeney 2001
Hajek 2002
Mohiuddin 2007
Quist-Paulsen 2003
Rigotti 1994
Rosal 1998
Smith 2009
Taylor 1990
Total (95% CI)
Total events
Heterogeneity: Tau2 = 0.11; Chi2 = 41.07, df = 9 (P<
0.00001); I2 = 78%
Test for overall effect: Z = 3.24 (P= 0.001)
Events
146
23
31
94
36
54
19
40
77
55
575
Total
388
54
96
274
109
118
44
135
137
86
1441
Events
98
12
1
102
9
40
19
31
54
29
395
Total
401
46
102
266
100
122
43
132
139
87
1438
Weight
13.4%
8.3%
1.4%
13.2%
7.1%
11.9%
9.6%
10.7%
12.8%
11.7%
100.0%
1.54 (1.24, 1.91)
1.63 (0.92, 2.91)
32.94 (4.59, 236.59)
0.89 (0.72, 1.12)
3.67 (1.86, 7.23)
1.40 (1.01, 1.92)
0.98 (0.61, 1.57)
1.26 (0.84, 1.89)
1.45 (1.12, 1.87)
1.92 (1.37, 2.69)
1.51 (1.18, 1.93)
Treatment Control Risk ratio
M-H, random, 95% CI
Risk ratio
M-H, random, 95% CI
0.1 0.2 0.5 1 2 5 10Favours control Favours treatment
Figure 2. Continuous smoking cessation outcome comparing
effectiveness of psychoeducational
intervention to control condition.
Study or Subgroup
Bolman 2002
Feeney 2001
Mohiuddin 2007
Ockene 1992
Quist-Paulsen 2003
Reid 2003
Reid 2007
Rigotti 1994
Smith 2009
Taylor 1990
Total (95% CI)
Total events
Heterogeneity: Tau2 = 0.07; Chi2 = 10.23, df = 9 (P= 0.33); I2 =
12%
Test for overall effect: Z = 1.36 (P= 0.18)
Events
14
4
3
2
3
1
0
8
2
2
39
Total
388
96
109
135
118
126
50
44
137
86
1289
Events
11
5
12
9
2
1
1
8
2
5
56
Total
401
102
100
132
122
128
50
43
139
87
1304
Weight
24.7%
11.1%
11.9%
8.3%
6.2%
2.7%
2.0%
20.4%
5.2%
7.4%
100.0%
1.32 (0.60, 2.86)
0.85 (0.24, 3.07)
0.23 (0.07, 0.79)
0.22 (0.05, 0.99)
1.55 (0.26, 9.12)
1.02 (0.06, 16.06)
0.33 (0.01, 7.99)
0.98 (0.40, 2.37)
1.01 (0.14, 7.10)
0.40 (0.08, 2.03)
0.73 (0.46, 1.15)
Treatment Control Risk ratio
M-H, random, 95% CI
Risk ratio
M-H, random, 95% CI
0.01 0.1 1 10 100Favours treatment Favours control
Figure 3. Total mortality outcome comparing effectiveness of
psychoeducational intervention to
control condition.
766 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
19/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
therapy (NRT) or bupropion, to the intervention group only or
for all participantstended to report greater treatment effects than
those studies that did not offer
pharmacotherapy (Figure 4). However, the differences between
these subgroups werestatistically non-significant. A test for
subgroup differences indicated that there was nostatistically
significant difference in smoking cessation results between studies
that
reported or did not report using theory in intervention planning
(Figure 4).We judged interventions to be intensive in three
studies, could-be-intensive in five
studies, and less intensive interventions in six studies.
Analysis for subgroupdifferences suggested that compared to less
intensive interventions intensiveinterventions were statistically
significantly associated with increased smokingabstinence (Figure
4). We did not find statistically significant differences between
the
intensive and the could-be-intensive interventions or between
the could-be-intensive and less intensive interventions, although
there was a tendency for themore intensive interventions to be
associated with larger treatment effects.
Follow-up data for smoking cessation suggested that in
comparison to controlinterventions, psychoeducational interventions
were effective at 6 months and12 months. Non-significant results at
2460 months for point prevalent cessation, andat 6 months and 2460
months for continuous cessation may be explained by thesmall number
of studies that provided relevant data for the analyses (Figure
4).
Investigation of process variables
Studies appeared to report predictor variables rather than
process variables and we
encountered difficulties in distinguishing when process
variables as opposed topredictor variables had been investigated.
Five of the studies appeared to be identifyingprocess variables,
but we questioned whether some of these were more appropriately
0 1 2 3 4 0 2 4 6
Pharmac. offered to all
To treat group only
Not offered
Theory group
No theory group
Intensive treatment
Could be intensive
Less intensive
Follow-up 6 mon
Follow-up 12 mon
Follow-up 24-60 mon
Point prevalent Continuous
1 3 5
Figure 4. Results of subgroup or sensitivity analyses relative
risk (95% CI) of psychoeducational
intervention to control condition.
Smoking cessation for CHD patients 767
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
20/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
identified as predictor variables. However, we identified the
following variables aspotential process variables: stage of change,
i.e., readiness to quit smoking, though there
was no interaction with intervention group (Ockene et al.,
1992); self-efficacy(Dornelas, Sampson, Gray, Waters, &
Thompson, 2000; Reid et al., 2003); signingcommitment to stop
smoking; and adherence of intervention participants to
procedures(Hajeket al., 2002). We also identified some
contradictions. For instance, Johnson et al.(1999) did not find any
difference in self-efficacy between the intervention and
controlgroup even though the intervention was designed to improve
self-efficacy.
Behavioural determinants and behaviour change techniques
All interventions appeared to target multiple behavioural
determinants and while weestimated that majority of interventions
aimed influence smoking behaviour through
beliefs about capabilities, knowledge, and skills, in our
estimation all interventionstargeted participants motivation and
goals (Tables 5 and 6). Fewer interventions aimedto modify smoking
behaviour through social influences, beliefs about consequences
of
continuing smoking, action planning, or emotions. We did not
assess any of theinterventions influencing smoking behaviour
explicitly through social or professionalrole and identity, memory
attention and decision processes, or environmental contextand
recourses. While it seemed to us very likely that all interventions
targeted attentionand decision processes at some level, this proved
to be hard to evaluate and was not
considered in the analysis. In addition, we found it difficult
to decide between actionplanning and skills, and decided to record
action planning only when this was explicitlymentioned in an
intervention. However, it cannot be assumed that elements of
actionplanning were not present in interventions where this was not
made explicit (Table 5).
We estimate that 14 different behaviour change techniques were
used in theinterventions. The most commonly used were: standard,
monitoring, behaviouralinformation, relapse prevention, and
planning. Less commonly used were: socialsupport, personalized
message, feedback, and relaxation. The least-used behaviourchange
techniques were: contract, fear arousal, verbal persuasion, coping
strategies,motivational interviewing, and buddy systems (Table
5).
Evaluation of techniques suitability
While only a limited number of behaviour change techniques were
used, everyintervention used at least one technique recognized by
Michie et al. (2008) as
influencing targeted behavioural determinants. We noted, though,
that some behaviourchange techniques used in interventions were not
recognized as effective in influencingbehavioural determinants by
Michie et al. (2008). For example, several trials
investigated relapse prevention, considered ineffective by
Michie et al. (2008). Studies,however, tended not only to mention
relapse prevention, but also to specify its differentelements
(Tables 5 and 6).
Effect of explicit use of theory in intervention planning
Our findings suggested that interventions have deployed diverse
theories inintervention planning (Tables 2 and 6). We judged the
behavioural determinants
targeted in the interventions to be compatible with assumptions
of the differenttheories. Studies that did not include a
theoretical model in intervention planningappeared to use similar
behavioural determinants to those studies that included theory
768 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
21/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table
5.
Targetedbehaviouraldeterminantsand
techniquesusedtoinfluencebehaviouraldeterminants
Techniq
uesused
Behaviouraldeterminantsnum
berofstudiesused(andusefulness)
Motivarionand
goals
Beliefsabout
capabilities
Beliefsabout
consequences
Knowledge
Skills
Social
influences
Emotion
Action
planning
Standard
14(Ok)
12(No)
5(Dis)
11(Un)
12(Ok)
7(No)
1(No)
2(Ok)
Relapse
prevention
8(Un)
7(Un)
3(No)
7(No)
7(No)
4(No)
1(No)
2(Un)
Monito
ring
13(Un)
11(Un)
5(Un)
10(No)
11(Ok)
6(Un)
1(No)
2(Un)
Contra
ct
2(Ok)
2(No)
1(No)
2(Ok)
2(No)
2(Dis)
1(Ok)
Planning
11(No)
10(No)
4(No)
9(No)
11(Un)
6(No)
1(Un)
2(Ok)
Feararousal
2(Ok)
2(Ok)
2(Ok)
2(No)
1(No)
1(Dis)
Behavio
uralinformation
11(Ok)
9(Un)
5(Ok)
11(Ok)
10(No)
5(No)
1(No)
2(Dis)
Verbalpersuasion
1(Ok)
1(Ok)
1(Un)
1(Un)
Coping
strategies
1(No)
1(Ok)
1(No)
1(Dis)
Motivationalinterview
2(Ok)
2(Ok)
1(Dis)
1(No)
1(No)
Relaxation
3(No)
3(No)
1(No)
3(No)
3(No)
1(No)
1(No)
Socials
upport
8(Ok)
7(Ok)
3(No)
6(No)
7(No)
6(Ok)
1(Un)
Personalizedmessage
8(Un)
7(Un)
3(Un)
7(Dis)
7(No)
4(No)
1(Un)
Feedback
3(Un)
2(Ok)
2(Ok)
3(No)
3(Dis)
1(No)
1(No)
1(Un)
Note.U
sefulnessoftechniqueswasbasedonMic
hieetal.(2008);Ok,agreeduse;Un,uncertain;Dis,disagreement;No,agreednon-use.
Smoking cessation for CHD patients 769
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
22/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table6
.Targetedbehaviouraldeterminantsandusedbehaviourchangetechniquesbythestudiesandbehaviuorchangetechniquessuitabilitytoinfluencebehaviouraldeterminants
Behavioural
determinants
targeted,
Either
givenor
estimated
from
available
information,
Michieetal.
(2008)
Studiesthat
targetgiven
behavioural
determinant
(onlyfirst
author
listed)
Techniqueusedintheintervention
anditsappropriatenesstoinfluenceontargetedbehaviouraldeterminant,Eithergivenintheinterventiondescriptionorestimatedfromavailable
information.TechniquesandtheirappropriatenessaccordingtoMichieetal.(2008)
Standard
Relapse
prevention
Monito
ring
Contract
Planning
Fear
arousal
Behavioural
information
Verbal
persuasion
Coping
strategies
Motivational
interview
RelaxationS
ocial
s
upport
Personalized
message
Feedback
Motivatio
n
andgoals
Bolman
Ok
Un
Dis
Ok
Ok
Un
Burt
Ok
Un
Ok
Ok
Ok
Ok
Dornelas
Ok
Un
Un
Ok
Feeney
Ok
Un
Un
Dis
Ok
No
Hajek
Ok
Un
Ok
Dis
Ok
Un
Johnson
Ok
Un
Dis
Ok
Ok
Un
Un
Mohiuddin
Ok
Un
Dis
Ok
No
No
Ok
Un
Ockeneand
Rosal
Ok
Un
Un
Ok
Un
Quist-
Paulsen
Ok
Un
Un
Dis
Ok
Ok
Un
Reid03
Ok
Un
Un
Dis
Ok
Ok
Un
Reid07
Ok
Un
Dis
Ok
Un
Rigotti
Ok
Un
Dis
Ok
Smith
Ok
Un
Un
Dis
Ok
Ok
Un
Taylor
Ok
Un
Un
Ok
Dis
Ok
No
Ok
Un
Beliefsab
out
capabilities
Bolman
No
Un
No
Un
Ok
Un
Dornelas
No
Un
Un
Ok
Feeney
No
Un
Un
No
Un
No
Hajek
No
Un
No
No
Un
Ok
Johnson
No
Un
No
Un
Ok
Un
Ok
Mohiuddin
No
Un
No
Un
Ok
No
Ok
Un
Ockeneand
Rosal
No
Un
Un
Un
Un
Reid03
No
Un
Un
No
Un
Ok
Un
Reid07
No
Un
No
Ok
Un
Rigotti
No
Un
No
Ok
Smith
No
Un
Un
No
Un
Ok
Un
Taylor
No
Un
Un
No
No
Un
No
Ok
Un
770 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
23/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table6
.(Continued)
Behavioural
determinants
targeted,
Either
givenor
estimated
from
available
information,
Michieetal.
(2008)
Studiesthat
targetgiven
behavioural
determinant
(onlyfirst
author
listed)
Techniqueusedintheintervention
anditsappropriatenesstoinfluenceontargetedbehaviouraldeterminant,Eithergivenintheinterventiondescriptionorestimatedfromavailable
information.TechniquesandtheirappropriatenessaccordingtoMichieetal.(2008)
Standard
Relapse
prevention
Monito
ring
Contract
Planning
Fear
arousal
Behavioural
information
Verbal
persuasion
Coping
strategies
Motivational
interview
RelaxationS
ocial
s
upport
Personalized
message
Feedback
Beliefsab
out
conseque
nces
Bolman
Dis
Un
No
Ok
Dis
Un
Burt
Dis
Un
Ok
Ok
Ok
No
Quist-
Paulsen
Dis
No
Un
No
Ok
Ok
Ok
Smith
Dis
No
Un
No
Ok
No
Un
Taylor
Dis
No
Un
No
No
Ok
No
No
Un
Ok
Knowledge
Bolman
Un
No
No
Ok
No
Dis
Burt
Un
No
Ok
Ok
Un
No
Feeney
Un
No
No
No
Ok
No
Hajek
Un
No
Ok
No
Ok
No
Johnson
Un
No
No
Ok
No
Dis
No
Mohiuddin
Un
No
No
Ok
No
No
No
Dis
Ockeneand
Rosal
Un
No
No
Ok
Dis
Quist-
Paulsen
Un
No
No
No
Ok
Ok
No
Reid03
Un
No
No
No
Ok
No
Dis
Smith
Un
No
No
No
Ok
No
Dis
Taylor
Un
No
No
Ok
No
Ok
No
No
Dis
Skills
Bolman
Ok
Ok
Un
No
No
No
Feeney
Ok
No
Ok
Un
No
No
No
Hajek
Ok
No
No
Un
No
Dis
Johnson
Ok
Ok
Un
No
No
No
Dis
Mohiuddin
Ok
Ok
Un
No
Dis
No
No
No
Ockeneand
Rosal
Ok
No
Ok
No
No
Quist-
Paulsen
Ok
No
Ok
Un
No
No
Dis
Reid03
Ok
No
Ok
Un
No
No
No
Smoking cessation for CHD patients 771
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
24/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
Table6
.(Continued)
Behavioural
determinants
targeted,
Either
givenor
estimated
from
available
information,
Michieetal.
(2008)
Studiesthat
targetgiven
behavioural
determinant
(onlyfirst
author
listed)
Techniqueusedintheintervention
anditsappropriatenesstoinfluenceontargetedbehaviouraldeterminant,Eithergivenintheinterventiondescriptionorestimatedfromavailable
information.TechniquesandtheirappropriatenessaccordingtoMichieetal.(2008)
Standard
Relapse
prevention
Monito
ring
Contract
Planning
Fear
arousal
Behavioural
information
Verbal
persuasion
Coping
strategies
Motivational
interview
RelaxationS
ocial
s
upport
Personalized
message
Feedback
Reid07
Ok
Ok
Un
No
No
Rigotti
Ok
Ok
Un
No
Smith
Ok
No
Ok
Un
No
No
No
Taylor
Ok
No
Ok
No
Un
No
No
No
No
Social
influences
Burt
No
Un
No
Un
Ok
Hajek
No
No
Dis
No
No
No
Reid03
No
No
Un
No
No
Ok
No
Reid07
No
Un
No
Ok
No
Rigotti
No
Un
No
Ok
Smith
No
No
Un
No
No
Ok
No
Taylor
No
No
Un
Dis
No
No
No
Ok
No
Emotion
Quist-
Paulsen
No
No
No
Un
No
No
No
Action
planning
Quist-
Paulsen
Ok
Un
Un
Ok
Dis
Dis
Un
Taylor
Ok
Un
Un
Ok
Ok
Dis
No
Un
Un
Note.O
k,techniqueappropriatetochangebehaviouraltargetaccordingtoMichieetal.(2008);Un,un
certthereisuncertaintyabouttechniqueseffectiveness/appropriatenessto
changebehaviouraldeterminantaccordingtoMichieet
al.(2008);No,techniquenotappropriatetochangebehaviouraldeterminantaccordingtoMichieetal.(2008);Dis,disagree
thereis
disagreementabouttechniquesappropriateto
changebehaviouraldeterminantaccordingtoM
ichieetal.(2008);,interventiondidnotuse
thistechnique;buddysystem
(Hajeketal.)notincludedinthelistasthereisnoinformationavailableinMichieetal.(2008)aboutte
chniquesappropriatenessoreffectiveness.
772 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
25/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
in intervention planning. We noted, however, some differences in
behaviour changetechniques used. It appeared that those studies
that explicitly included theory in
intervention planning, used diverse techniques more frequently
and to a greater extentthan studies in the group not deploying
theory. Intervention intensity, on the otherhand, did not appear to
exert any marked influence on targeted behaviouraldeterminants or
behaviour change techniques.
Discussion
Results of our meta-analysis suggested that psychoeducational
smoking cessationinterventions for CHD patients are effective.
Psychoeducational interventionssignificantly increased rates of
smoking cessation, and statistically non-significantlyreduced total
mortality. While our results are in line with the findings of
previousreviews and meta-analyses (e.g., Rigotti et al., 2007; Van
Berkel et al., 1999), our reviewconcentrated on CHD patients and
psychoeducational interventions. In addition, wetested an
innovative approach to investigating intervention mechanisms.
We found that analysing and interpreting the results posed
certain challenges. Apart
from the total mortality rate, analysis showed high levels of
unexplained variationbetween the studies, which could not be
accounted for by chance. Methodologicalappraisal and sensitivity
analysis suggested that methodological diversity between the
studies could not alone account for the variation found. To
further explore, the possiblecauses of heterogeneity for point
prevalent and continuous smoking cessation, we didunplanned post
hoc subgroup analysis. However, the results of the subgroup
analysesshould be treated with caution as the number of studies
included in some subgroupswere very small.
The effectiveness of pharmacotherapy in smoking cessation is
well established
(Stead, Perera, Bullen, Mant, & Lancaster, 2008; Woolacott
et al., 2002). We usedpost hocanalyses to investigate the effects
of pharmacotherapy, intervention theory andintensity, and length of
follow-up to intervention outcomes. Similarly to Rigotti et al.
(2007), we found that adding pharmacotherapy to
psychoeducational intervention didnot cause statistically
significant improvement in rates of smoking cessation comparedto
psychoeducational intervention alone.
As theories of behaviour change can guide intervention planning
by making itexplicit how the desired behaviour change can be
achieved, we tested whether explicitinclusion of theory in
intervention planning influences the effectiveness of
theintervention. However, we did not find any statistically
significant difference betweengroups that explicitly mentioned
theory in intervention planning and those that did notreport using
any theory. We do not view this result as suggesting that using a
theory in
intervention planning would be wasted effort. On the contrary,
this result highlights theimportance of examining actual theories
or mechanisms underlying interventions,rather than simply
considering whether theories are explicitly stated or not.
Thisconsideration also highlights the increased need for
practitioners and researchers whoare involved in intervention
planning and report writing to report, not only
interventionprocedures, but also how they suggest that the
intervention causes the desired change.
We found, similarly to Rigotti et al. (2007), that there was a
significant difference in
rates of smoking cessation between intensive and less-intensive
interventions. Whilerecognizing the methodological problems
associated with classifying the interventionsinto the reported
subgroups, results suggest that less-intensive interventions may
not
Smoking cessation for CHD patients 773
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
26/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
have been able to offer enough support especially for those
participants that werestruggling to maintain cessation. While
intensive interventions are likely to require more
resources, especially in terms of health care professionals
time, they may not beapplicable to every situation. It is also
worth noting that we considered only two studiesas intensive, and
that regardless of studies intensity and in contrast to
controltreatments, most of the studies included some form of
supportive contact afterdischarge from hospital. Consistent with
our findings, Rigotti et al. (2007) concludedthat high-intensity
interventions that begin during hospitalization and provide at
least
1 months supportive follow-up after discharge do increase
smoking cessation amongparticipants. At the present, the cumulative
evidence for hospitalized patients suggeststhat a successful
smoking cessation intervention should consist of substantial
in-patientintervention followed by supportive contact after
discharge from hospital.
Our estimates of smoking abstinence at different time points
show that the effects ofpsychological interventions were evident up
to 24 months. Results from the differentfollow-up points should
nevertheless be interpreted with caution, as the small number
oftrials or patients included in the analyses may have led to wide
or statistically non-significant confidenceintervals at certaintime
points, rather than measuring interventionineffectiveness as such.
Collecting reliable long-term follow-up data for this kind
ofpsychoeducational intervention is challenging, as it is difficult
to evaluate influence ofmany possible confounding factors that may
have influenced the results, such as adviceand support received
from other sources by the control group participants.
We did not find evidence of systematic testing of process
variables, and in many casesit was problematic to decide whether an
identified variable should be considered as apredictor or a process
variable, as in many cases, such as with self-efficacy, a
variable
could have both functions. While we judged that five studies did
investigate process variables, there was not enough information
available to reliably identify processesunderlying successful
smoking cessation.
While our statistical analyses offered only limited information
about interventionmechanisms and features, our qualitative
assessment of behavioural determinants andbehaviour change
techniques using the framework provided by Michie et al.
(2008)suggested considerable similarities between the
interventions. Those interventionsincluded in this review, tended
to emphasize individuals responsibility for theirsmoking and aimed
to improve smoking cessation via participants knowledge,
skills,
and beliefs about their capabilities to stop smoking and
continuing abstinence.Considering the available pool of (137)
behaviour change techniques listed by Michieet al. (2008),
interventions were found to deploy a rather more limited number
oftechniques, all relatively straightforward to apply in practice,
to deliver to high numbersof people, and requiring limited staff
training. Our analyses do not permit us tocomment on whether the
limited pool of behaviour change techniques in use reflectstheir
comparative practicability or effectiveness. Analysing behavioural
determinantsand behaviour change techniques, however, raises
practical considerations. As the poolof techniques deployed in
interventions was limited, we must consider whether the
results of the meta-analysis are only generalizable to smoking
cessation interventionsthat use similar techniques than
interventions in this review. As this is the first attemptto
analyse retrospectively behavioural determinants and behaviour
change techniquesin interventions, we should be cautious in
interpreting the evidence. What our results
do indicate, however, is that relatively straightforward
behaviour change techniques thatare also comparatively easy to
apply in practice can be effective in changing smokingbehaviour.
What separated interventions from each others in this review, was
not so
774 M. Huttunen-Lenz et al.
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
27/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
much the behaviour change techniques used or the behavioural
determinants targetedbut how behaviour change techniques were
combined and applied in practice.
Michie et al. (2008) argue that not all behaviour change
techniques are effective inchanging behavioural determinants. We
evaluated the effectiveness of behaviour changetechniques in
influencing behavioural determinants in the interventions, based on
theexpert opinion of Michie et al. (2008). Interestingly, these
findings suggested that somecommonly used intervention techniques
such as relapse prevention and personalizedmessages may not be
effective. Also, although most interventions used at least one
agreed technique to influence-targeted behavioural determinants,
interventionsinvestigated in some trials, for example Feeney et al.
(2001), did not appear to usesuch agreed techniques for all
targeted behavioural determinants. While these findingsare
tentative and open to debate, they nevertheless highlight the need
for intervention
planners to make explicit what different intervention components
are aiming toachieve.
Although we found our approach to meta-analysis useful and
informative, weencountered considerable difficulties when
retrospectively evaluating behaviouraldeterminants. It was
especially difficult to differentiate between skills and
actionplanning, and to identify memory attention and decision
processes. Part of theproblem here undoubtedly relates to the
limited space available for the reporting of anyintervention and
the usual practice of providing a description of the
interventionunaccompanied by even brief explanation of the
intervention rationale, i.e., why or how
the desired behaviour change should be achieved.Some of the
included studies had not been considered in other meta-analyses
as
randomized controlled trials (Burt et al., 1974; Johnson et al.,
1999), but performed
sensitivity analyses showed that inclusion of these studies did
not essentially change theresults. Although we did include
unpublished data from the authors, data analyses werealso carried
out using conservative methods to guard against overestimation of
anytreatment effect. The large between-study variation also raised
questions about theappropriateness of meta-analysis, but we felt
that the observed heterogeneity was animportant part of the
results, indicating the complexity of the interventions included
inthe review.
Although the retrospective evaluation of interventions entails
some problems, it mayoffer the potential to improve the
understanding of interventions included in the review.
However, various problems confronted us while using the study by
Michie et al. (2008) within our own process of evaluation, as when
we found the descriptions of somebehaviour change techniques to be
confusing or inadequate. Michie et al. (2008) hadalso constructed a
consensus table of the suitability of behaviour change techniques
toinfluence behavioural determinants. For us, however, it appeared
that many of the 35behaviour change techniques included in the
consensus table were actuallycombinations of originally listed
techniques within a new composite description,making any subsequent
evaluation process more rather than less complex. Anotherdifficulty
with taking this approach was that assessing the suitability of
techniques was
based on expert opinion, rather than on empirical evidence.
Conclusions
Psychoeducational smoking cessation interventions are associated
with increased ratesof smoking cessation. The results of post hoc
subgroup analyses suggested thatintervention intensity was
associated with intervention effectiveness. Meta-analysis
Smoking cessation for CHD patients 775
-
8/6/2019 Are Psycho Educational Smoking Cessation
Interventions
28/30
Copyright The British Psychological SocietyReproduction in any
form (including the internet) is prohibited without prior
permission from the Society
indicated a high level of heterogeneity and interventions
appeared to be very differentfrom each other. However, the
examination of behavioural determinants and behaviour
change techniques suggested less than expected variation in the
interventiontechniques used. Results of the meta-analyses may only
be generalizable to smokingcessation interventions that use similar
techniques to interventions in this review.
References
Altman, D., & Bland, J. (2003). Interaction revisited: The
difference between two estimates.
British Medical Journal, 326, 219.
Bolman, C., de Vries, H., & van Breukelen, G. (2002a). A
minimal-contact intervention for cardiac
inpatients: Long-term effects on smoking cessation. Preventive
Medicine, 35, 181192.
Bolman, C.,de Vries, H.,& vanBreukelen,G. (2002b).
Evaluation of nurse managed minimal contact
smoking cessation intervention for cardiac patients. Health
Education Research, 17, 99116.
Burt, A., Thornley, P., Illingworth, D., White, P., Shaw, T. R.,
& Turner, R. (1974). Stopping smoking
after myocardial infarction. Lancet, 1, 304306.
Critchley, J. A., & Capewell, S. (2003). Smoking cessation
for the secondary prevention of
coronary heart disease. Cochrane Database of Systematic Reviews,
Issue 4. Art. No.:
CD003041. doi:10.1002/14651858.CD003041.pub2
Dornelas, E. A., Sampson, R. A., Gray, J. F., Waters, D., &
Thompson, P. D. (2000). A randomized
controlled trial of smoking cessation counseling after
myocardial infarction. Preventive
Medicine, 30, 261268.Dusseldorp, E., van Elderen, T., Maes, S.,
Meulman, J., & Kraaij, V. (1999). A meta-analysis of
psychoeducational programs for coronary heart disease patients.
Health Psychology, 18,
506519.
Feeney, G., McPherson, A., Connor, J., McAlister, A., Young, M.,
& Garrahy, P. (2001). Randomized
controlled trial of two cigarette quit programmes in coronary
care patients after acute
myocardial infarction. Internal Medicine Journal, 31,
470475.
Godin, G. (1989). The effectiveness of interventions in
modifying behavioural risk factors of
individuals with coronary heart disease. Journal of
Cardiopulmonary Rehabilitation, 9,
223236.
Hajek, P., Taylor, T., & Mills, P. (2002). Brief
intervention during hospital admission to help patients
to give up smoking after myocardial infarction and bypass
surgery: Randomised controlled
trial. British Medical Journal (Clinical research ed.), 324,
8789.
Isles, C., Armstrong, G., Begg, A., Bowbeer, J., Breslin, A.,
Brown, A., Baker, C. (2002). Cardiac
rehabilitation a national clinical guideline. Edinburgh:
Scottish Intercollegiate GuidelinesNetwork (SIGN).
Johnson, J. L., Budz, B., Mackay, M., & Miller, M. (1999).
Evaluation of a nurse-delivered smoking
cessation intervention for hospitalized patients