Embed Size (px)
Citation preview

ARE YOU READY FOR ICD-10-CM?
PALMETTO HEALTH
Carolyn Todd Mahon, PhD, MSN-NP, MBAMedical Business Institute
Dallas, Texas
DISCLOSURE
I have no relevant financial relationships with any commercial
interests related to the content
of this activity –
Carolyn Todd Mahon, PhD, MSN-NP, MBAMedical Business Institute
Dallas, Texas
DISCLAIMER
• While all information in this document is believed to be correct at the time of writing, this document is for educational purposes only and does not purport to provide legal advice. All models, methodologies and guidelines are undergoing continuous improvement and modification by NHIC, Corp. and the Centers for Medicare & Medicaid Services (CMS). The most current edition of the information contained in this release can be found on the NHIC, Corp. web site at www.medicarenhic.comand the CMS web site at www.cms.gov.

ICD-10-CM WHERE DO I START?
1. Overview
2. Structure and Use
3. Actions and Timeline
4. Tools and Resource
4
ICD-10-CM OVERVIEW
• ICD is one of the code sets used in medical billing along with others such as CPT
• The ICD system is the code set for identifying diagnoses to support services and/or procedures (identified by the CPT code sets) rendered by healthcare providers
• ICD-10-CM is the abbreviation for the International Classification of Diseases, Tenth Revision, Clinical Modification
OVERVIEW OF ICD-10-CM
• No longer October 1, 2013 but a future date to be announced by HHS, medical coding in U.S. health care settings will change from ICD-9 to ICD-10. The transition will require business and systems changes throughout the health care industry. Everyone who is covered by the Health Insurance Portability and Accountability Act (HIPAA) must make the transition, not just those who submit Medicare or Medicaid claims.
OVERVIEW OF ICD-10
• On January 1, 2012, standards for electronic health transactions change to Version 5010. Version 5010 accommodates the ICD-10 code structure. This change occurs before the ICD-10 implementation date to allow adequate testing and implementation time.
What’s In IT For You?
• Benefits– Claims Acknowledgement– 5010 is more specific about required data– Supports new ICD-10 codes– 5010 contains significant improvements
for the reporting of clinical data– 5010 supports increased use of EDI
between covered entities– 5010 supports E-Health initiatives now
and in the future
5010 Changes
Some 5010 changes• Prohibits use of P.O. Boxaddresses for billing provider(different from pay to address)• Expands size of diagnosis codefield• Expansion of the number ofdiagnosis codes to 12• Immediate assignment of a claimnumber allows easier follow-up
WHEN DOES ICD-10 ACTUALLY HAPPEN?
• A date to be announced by HHS• “I believe we are looking at a minimum of 1
year. They will need to announce a delay from October 1, 2013 to at least October 1, 2014 because of CMS fiscal planning calendars.”
When the new compliance date is set it will still be true that if you are not ready, your claims will not be paid. Preparing now can help you avoid potential reimbursement issues
History of ICD-9-CM
• World Health Organization (WHO) developed ICD-9 for use worldwide– The National Center for Health Statistics
developed clinical modification (ICD-9-CM) Implemented in 1979 in U.S.
– Expanded number of diagnosis codes– Developed procedure coding system– DESIGNED TO LAST 10 YEARS
WHAT IS ICD-10?
• 1990 –Endorsed by World Health Assembly (diagnosis only)
• 1994 –Release of full ICD-10 by WHO • HIPAA Mandate- 1996• 2002 (October) –ICD-10 published in 42
languages (including 6 official WHO languages)
• January 1, 1999 –U.S. implemented for mortality (death certificates)
WHY ARE WE MOVING TO ICD-10?
• ICD-9-CM is Outdated– 30 years old –technology has changed– Many categories full– Not descriptive enough
WHY ARE WE MOVING TO ICD-10?
– Reimbursement–would enhance accurate payment for services rendered
– Quality–would facilitate evaluation of medical processes and outcomes
– What Characteristics Are Needed in a Coding System?
• Flexible enough to quickly incorporate emerging diagnoses and procedures
• Exact enough to identify diagnoses and procedures precisely
ICD-9-CM is too old to be either of these
Reimbursement and Quality Problems With ICD-9-CM
• Example – Fracture of wrist– Patient fractures left wrist.
» A month later, fractures right wrist» ICD-9-CM does not identify left versus right –
requires additional documentation– ICD-10 CM describes
» Left versus right» Initial encounter, subsequent encounter» Routine healing, delayed healing, nonunion, or
malunion
Reimbursement and Quality Problems With ICD-9-CM
Ex: Ovary - ICD-9= 1 code vs. ICD-10= 4 codes• ICD-10-CM describes Left versus right • Initial encounter, subsequent encounter
Reimbursement and Quality Problems With ICD-9-CM
Example –combination defibrillator pacemaker device
– Codes for this device are not in the cardiovascular chapter of ICD-9-CM with other defibrillator and pacemaker devices
– Coders and researchers have trouble finding these codes with this type of erratic code assignment
– ICD-10-PCS provides distinct codes for all these types of devices, in an orderly manner that is easy to find
ICD-10
1. ICD Structure and Use
2. Actions and Timeline
3. Tools and Resource
18
Structural Differences –ICD-9-CM Diagnoses
• ICD-9 HAS TWO VOLUMES• ICD-9-CM has 3 –5 digits• Chapters 1 –17: all characters are numeric• Supplemental chapters: first digit is alpha (E or
V), remainder are numeric
– Examples: 496 Chronic airway obstruction not elsewhere classified (NEC)
– 511.9 Unspecified pleural effusion– V02.61 Hepatitis B carrier
Structural Differences –ICD-9/10-CM Diagnoses
ICD-10-CM – diagnosis coding• Change in structure and volume• ICD-9-CM 2010 - 14,315 codes• ICD-10-CM 2010 – 69,099 codes• Both code sets currently beingupdated• Added specificity & added complexity• Electronic “crosswalk” created andfree from CMS
Structural Differences ICD-10-CM Diagnoses
• ICD-10 HAS THREE VOLUMES• ICD-10-CM has 3 –7 digits
• •Digit 1 is alpha (A –Z, not case sensitive)
• •Digit 2 is numeric
• •Digit 3-7 is ALPHA (not case sensitive) or NUMERIC
– A69.20 Lyme disease, unspecified– O9A.311 Physical abuse complicating pregnancy, first trimester– S42.001A Fracture of unspecified part of right clavicle, initial
encounter for closed fracture
ICD-10-CM Tabular List
1. Certain Infectious and Parasitic Diseases
2. Neoplasms
3. Diseases of the Blood and Blood-forming Organs and Certain Disorders Involving the Immune Mechanism
4. Endocrine, Nutritional, and Metabolic Diseases
5. Mental and Behavioral Disorders
6. Diseases of the Nervous System
7. Diseases of the Eye and Adnexa
8. Diseases of the Ear and Mastoid Process
9. Diseases of the Circulatory System
10. Diseases of the Respiratory System
ICD-10-CM Tabular List
11. Diseases of the Digestive System12. Diseases of the Skin and Subcutaneous System13. Diseases of the Musculoskeletal System and Connective Tissue14. Diseases of the Genitourinary System15. Pregnancy, Childbirth and the Puerperium16. Certain Conditions Originating in the Perinatal Period17. Congenital Malformations, Deformations and Chromosomal
Abnormalities18. Symptoms, Signs and Abnormal Clinical and Laboratory Findings,
not elsewhere classifiable19. Injury, Poisonings, and Certain Other Consequences of External
Causes20. External Causes of Morbidity21. Factors Influencing Health Status and Contact with Health
Services
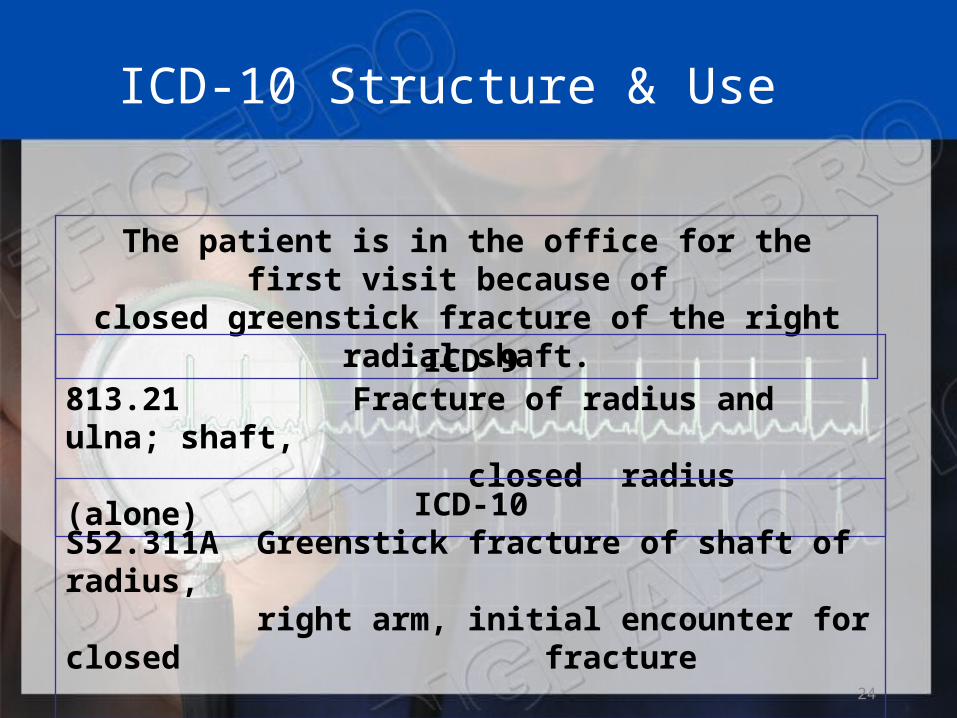
ICD-10 Structure & Use
24
The patient is in the office for the first visit because of
closed greenstick fracture of the right radial shaft.ICD-9
813.21 Fracture of radius and ulna; shaft, closed radius (alone)
ICD-10S52.311A Greenstick fracture of shaft of radius, right arm, initial encounter for closed fracture
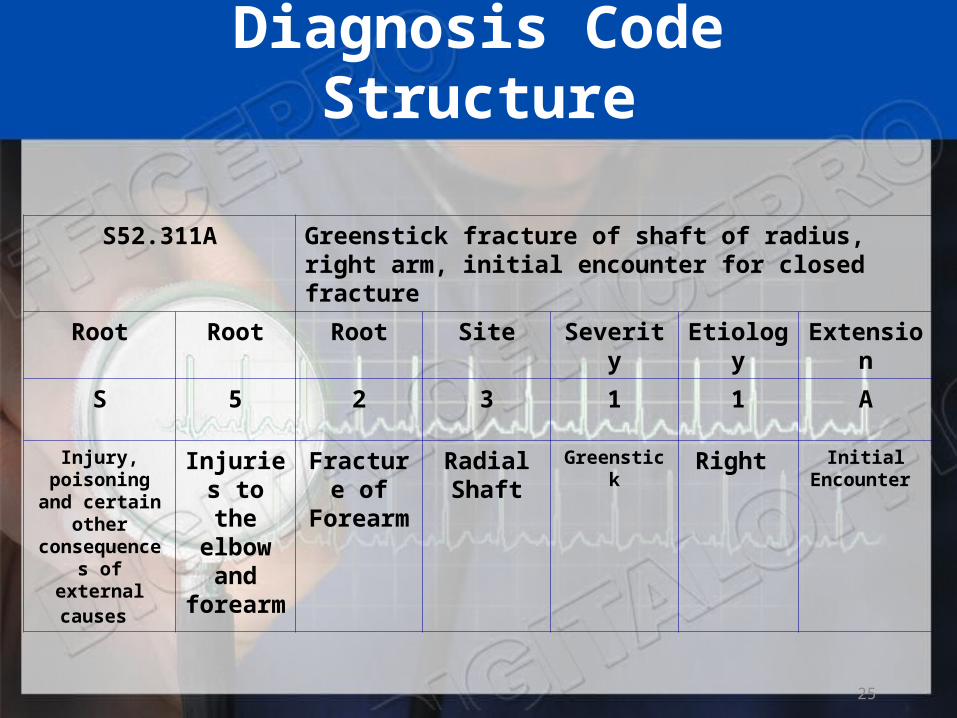
Diagnosis Code Structure
S52.311A Greenstick fracture of shaft of radius, right arm, initial encounter for closed fracture
Root Root Root Site Severity Etiology Extension
S 5 2 3 1 1 A
Injury, poisoning and certain other
consequences of external
causes
Injuries to the elbow and
forearm
Fracture of
Forearm
Radial Shaft
Greenstick Right Initial Encounter
25
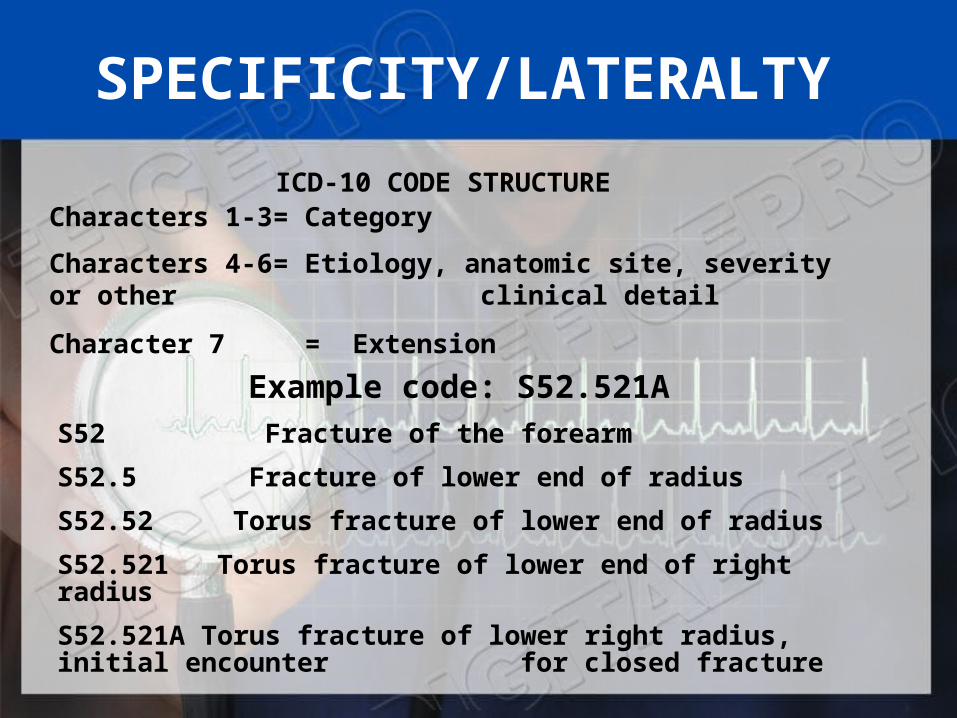
SPECIFICITY/LATERALTY
ICD-10 CODE STRUCTURECharacters 1-3= Category
Characters 4-6= Etiology, anatomic site, severity or other clinical detail
Character 7 = Extension
Example code: S52.521A
S52 Fracture of the forearm
S52.5 Fracture of lower end of radius
S52.52 Torus fracture of lower end of radius
S52.521 Torus fracture of lower end of right radius
S52.521A Torus fracture of lower right radius, initial encounter for closed fracture
Code extensions (seventh character)
• Code extensions (seventh character) have been added for injuries and external causes to identify the encounter: initial, subsequent, or sequela. The extensions are:
• A Initial encounter • D Subsequent encounter • S Sequelae • For example, ICD-10-CM code S31.623A, Laceration
with foreign body of abdominal wall, right lower quadrant with penetration into peritoneal cavity, initial encounter, shows an extension used with a laceration code. Note that in ICD-10-CM, the entire code description is written out.
Code extensions(seventh character)
• Fracture codes require a seventh character that identifies if the fracture is open or closed for an initial encounter or if a subsequent encounter is for routine healing, delayed healing, nonunion, malunion, or sequelae. The fracture extensions are:
• A Initial encounter for closed fracture • B Initial encounter for open fracture • D Subsequent encounter for fracture with routine healing • G Subsequent encounter for fracture with delayed healing • K Subsequent encounter for fracture with nonunion • P Subsequent encounter for fracture with malunion • S Sequelae • An example is code S42.321A, Displaced transverse fracture of
shaft of humerus, right arm, initial encounter for closed fracture.
Diabetes mellitus
• Diabetes mellitus codes are expanded to include the classification of the diabetes and the manifestation. The category for diabetes mellitus has been updated to reflect the current clinical classification of diabetes and is no longer classified as controlled/uncontrolled:
• E08.22, Diabetes mellitus due to an underlying condition with diabetic chronic kidney disease
• E09.52, Drug or chemical induced diabetes mellitus with diabetic peripheral angiopathy with gangrene
• E10.11, Type 1 diabetes mellitus with ketoacidosis with coma
• E11.41, Type 2 diabetes mellitus with diabetic mononeuropathy
Complications of foreign body
• ICD-10-CM provides 50 different codes for “complications of foreign body accidently left in body following a procedure,” compared to only one code in ICD-9-CM. Examples include:
• T81.535, Perforation due to foreign body accidently left in body following heart catheterization
• T81.530, Perforation due to foreign body accidently left in body following surgical operation
• T81.524, Obstruction due to foreign body accidently left in body following endoscopic examination
• T81.516, Adhesions due to foreign body accidently left in body following aspiration, puncture or other catheterization
MAPPING WITH GEMS• What are the General Equivalence Mappings?• The GEMs are a tool that can be used to convert data from
ICD-9-CM to ICD-10-CM and PCS• and vice versa. Mapping from ICD-10-CM and PCS codes back
to ICD-9-CM codes is referred to• as backward mapping. Mapping from ICD-9-CM codes to ICD-
10-CM and PCS codes is referred to• as forward mapping. The GEMs are a comprehensive
translation dictionary that can be used to• accurately and effectively translate any ICD-9-CM-based data,
including data for: ➤ Tracking quality; ➤ Recording morbidity/mortality; ➤ Calculating reimbursement; or ➤ Converting any ICD-9-CM-based application to
ICD-10-CM/PCS. (CDC)
MAPPING WITH GEMs
• The GEMs are complete in their description of all the mapping possibilities as well as when there are new concepts in ICD-10 that are not found in ICD-9-CM. All ICD-9-CM codes and all ICD-10-CM/PCS codes are included in the collective GEMs:
➤ All ICD-10-CM codes are in the ICD-10-CM to ICD-9-CM GEM;
➤ All ICD-9-CM Diagnosis Codes are in the ICD-9- CM to ICD-10-CM GEM;
Why Do We Need the General Equivalence
Mappings?• ICD-10 is much more specific:
– For diagnoses, there are 14,025 ICD-9-CM codes and 68,069 ICD-10-CM codes; and
– For procedures, there are 3,824 ICD-9-CM codes and 72,589 ICD-10-PCS codes (in the 2009 versions of ICD-9-CM, ICD-10-CM, and ICD-10-PCS).
Why Do We Need the General Equivalence
Mappings? Cont’dOne ICD-9-CM Diagnosis Code is represented by
multiple ICD-10-CM codes: 82002 Fracture of midcervical section of femur, closed– From S72031A
• Displaced midcervical fracture of right femur, initial encounter for closed fracture
– From S72031G • Displaced midcervical fracture of right femur, subsequent
encounter for closed fracture with delayed healing
– From S72032A• Displaced midcervical fracture of left femur, initial encounter
for closed fracture
– From S72032G• Displaced midcervical fracture of left femur, subsequent
encounter for closed fracture with delayed healing
– And other codes from the GEMs
Why Do We Need the General Equivalence
Mappings? Cont’d• One ICD-10-CM Diagnosis Code is
represented by multiple ICD-9-CM Codes:– E11341 Type 2 diabetes mellitus with severe
nonproliferative diabetic retinopathy with macular edema
• To ICD-9 Cluster:– 250.50 Diabetes with ophthalmic
manisfestations, type II or specified type, not stated as uncontrolled
– 362.06 Severe nonproliferative diabetic retinopathy
– 362.07 Diabetic macular edema
Why Do We Need the General Equivalence
Mappings? Cont’d ➤ A few ICD-10-CM codes have no predecessor ICD-9-CM codes:– T500x6A Under dosing of mineral corticoids and their
antagonists, initial encounter– T501x6A Under dosing of loop [high-ceiling] diuretics,
initial encounter– T502x6A Under dosing of carbonic-anhydrase inhibitors,
benzothiadiazides and other diuretics, initial encounter– T503x6A Under dosing of electrolytic, caloric and water-
balance agents, initial encounter– T504x6A Under dosing of drugs affecting uric acid
metabolism, initial encounter– And others found in the GEMs

How are the GEM Files Formatted?• Here is an example from the ICD-10-CM diagnosis
mapping: ➤ ICD-10-CM Source system code is on the left side;
➤ ICD-9-CM Target system code is in the middle; and
➤ Flags are on the right.
ICD-10 CM Source Code
T1500xA
T1500xA
T1500xD
T1500xD
T1500xS
ICD-9 CM Target Code
9300
E914
9300
E914
908.5
Flags
10111
10112
10111
10112
10000
How are the GEM Files Formatted?
• T1500xA Foreign body in cornea, unspecified eye, initial encounter
– To ICD-9 cluster:• 9300 Corneal foreign body• E914 Foreign body accidentally entering eye and
adnexa
• T1500xD Foreign body in cornea, unspecified eye, subsequent encounter– To ICD-9 cluster:
• 9300 Corneal foreign body• E914 Foreign body accidentally entering eye and
adnexa• T1500xS Foreign body in cornea, unspecified
eye, sequela– To 908.5 Late effect of foreign body in orifice
How are the GEM Files Formatted?
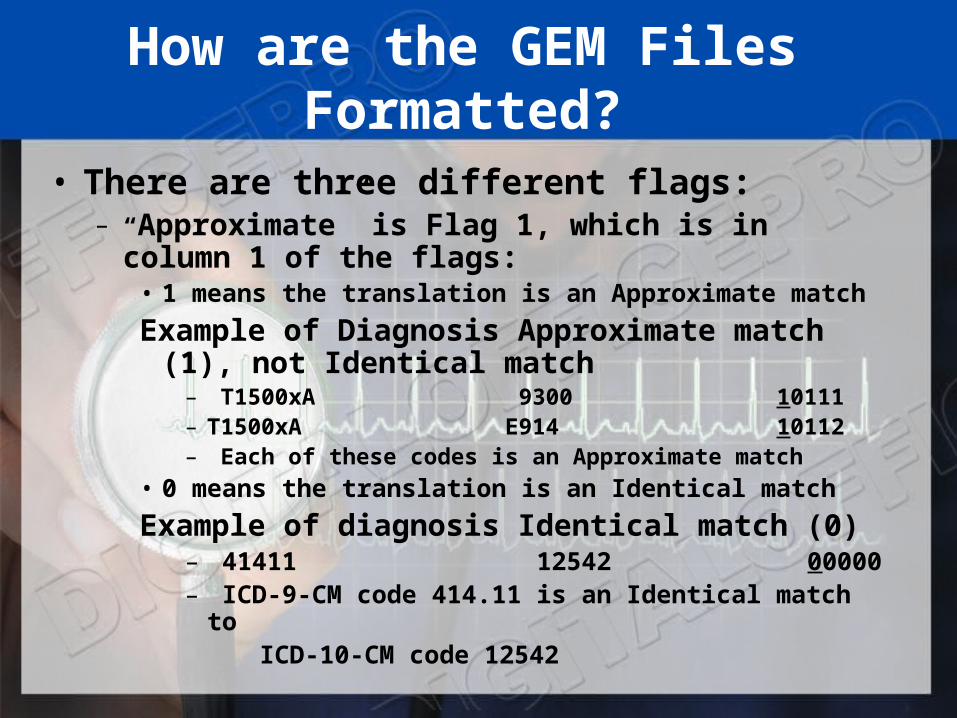
• There are three different flags:– “Approximate” is Flag 1, which is in column 1 of
the flags:• 1 means the translation is an Approximate match
Example of Diagnosis Approximate match (1), not Identical match
– T1500xA 9300 10111– T1500xA E914 10112– Each of these codes is an Approximate match
• 0 means the translation is an Identical match
Example of diagnosis Identical match (0)– 41411 12542 00000– ICD-9-CM code 414.11 is an Identical match to ICD-10-CM code 12542
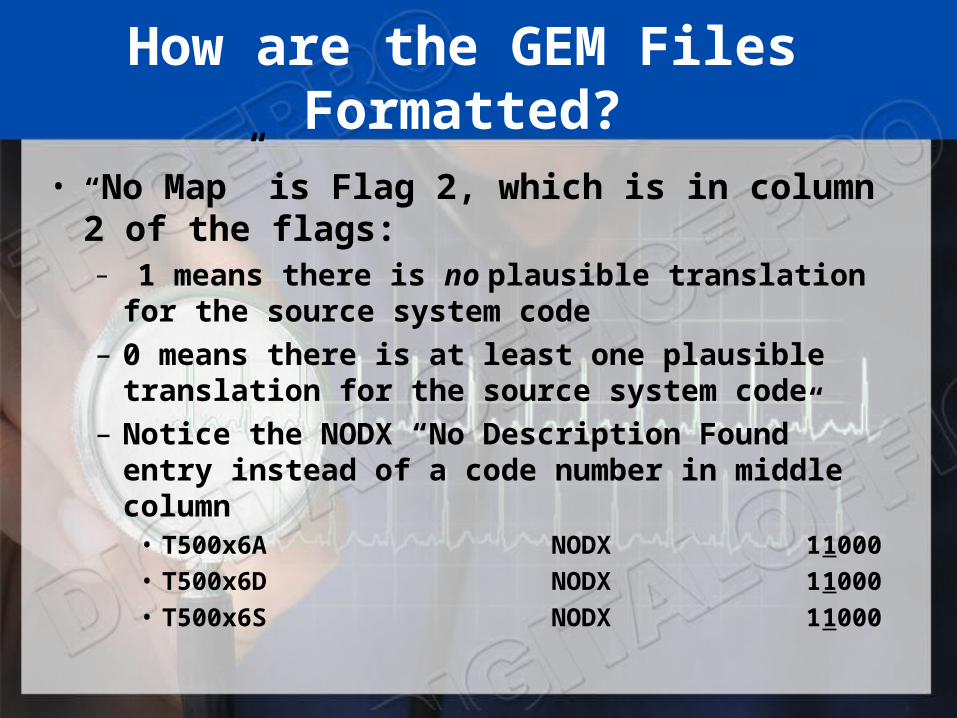
How are the GEM Files Formatted?
• “No Map” is Flag 2, which is in column 2 of the flags:– 1 means there is no plausible translation for the
source system code– 0 means there is at least one plausible translation
for the source system code– Notice the NODX “No Description Found” entry
instead of a code number in middle column• T500x6A NODX 11000• T500x6D NODX 11000• T500x6S NODX 11000
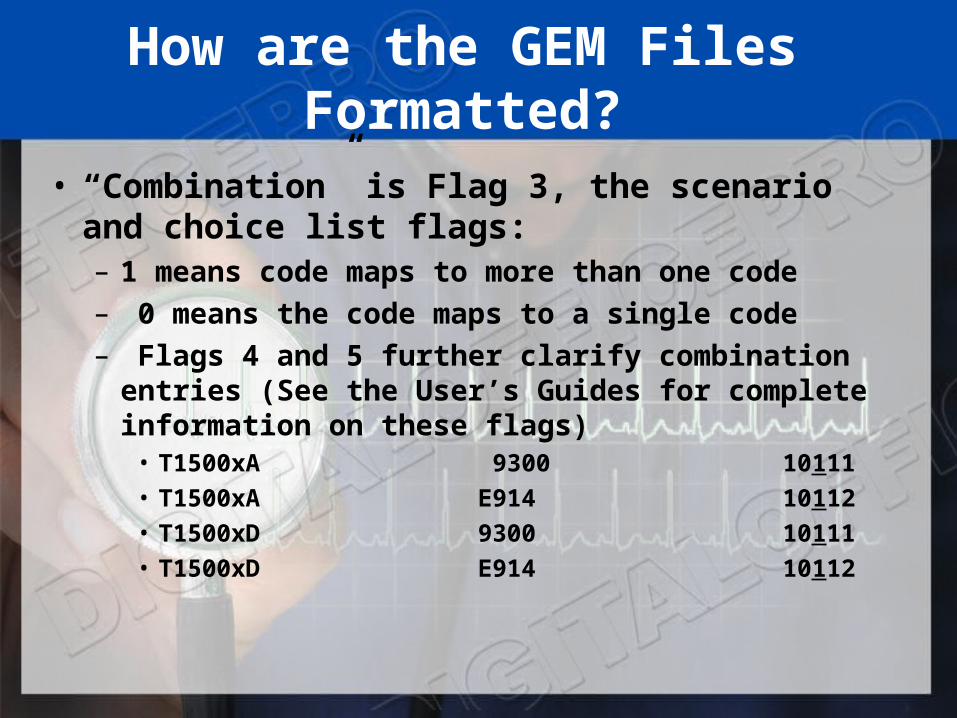
How are the GEM Files Formatted?
• “Combination” is Flag 3, the scenario and choice list flags:– 1 means code maps to more than one code– 0 means the code maps to a single code– Flags 4 and 5 further clarify combination entries
(See the User’s Guides for complete information on these flags)
• T1500xA 9300 10111• T1500xA E914 10112• T1500xD 9300 10111• T1500xD E914 10112
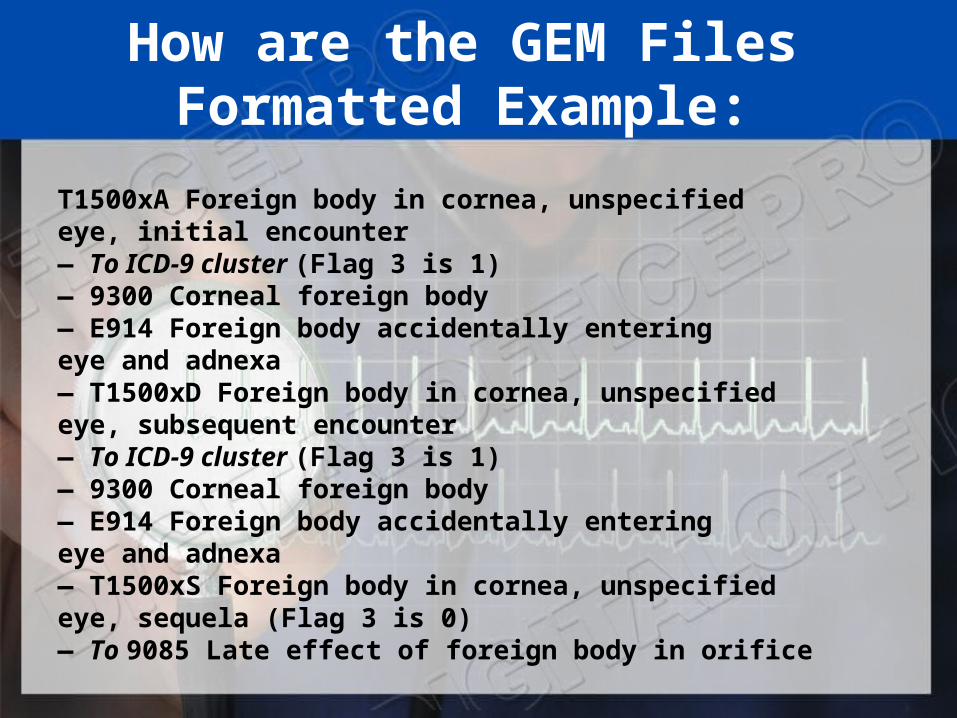
How are the GEM Files Formatted Example:
T1500xA Foreign body in cornea, unspecifiedeye, initial encounter— To ICD-9 cluster (Flag 3 is 1)— 9300 Corneal foreign body— E914 Foreign body accidentally enteringeye and adnexa— T1500xD Foreign body in cornea, unspecifiedeye, subsequent encounter— To ICD-9 cluster (Flag 3 is 1)— 9300 Corneal foreign body— E914 Foreign body accidentally enteringeye and adnexa— T1500xS Foreign body in cornea, unspecifiedeye, sequela (Flag 3 is 0)— To 9085 Late effect of foreign body in orifice
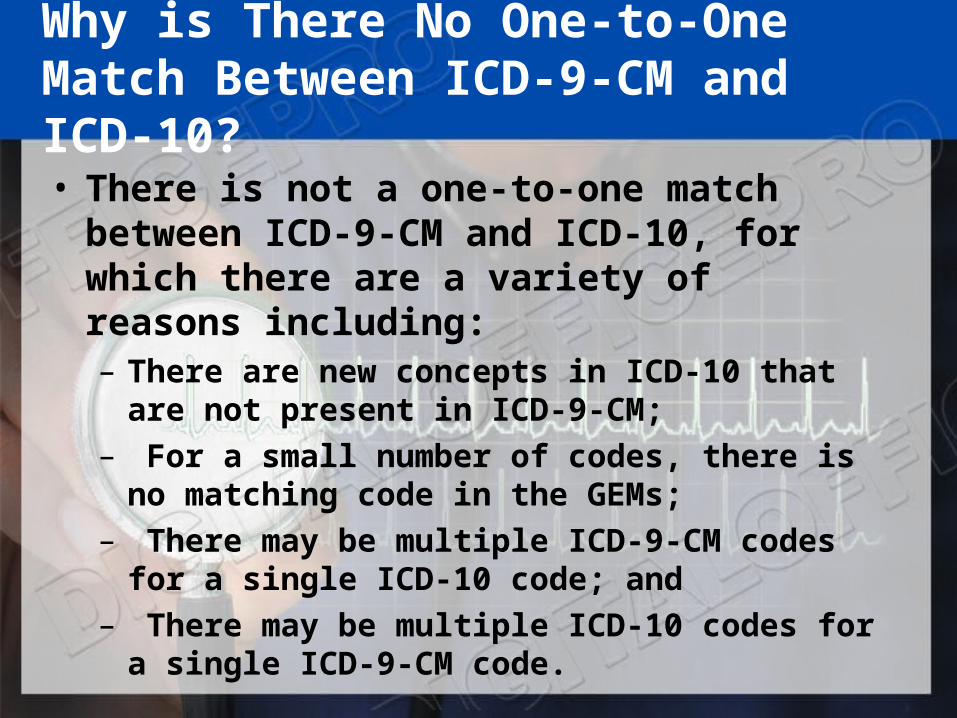
Why is There No One-to-One Match Between ICD-9-CM and ICD-10?• There is not a one-to-one match between
ICD-9-CM and ICD-10, for which there are a variety of reasons including:– There are new concepts in ICD-10 that are not
present in ICD-9-CM;– For a small number of codes, there is no
matching code in the GEMs;– There may be multiple ICD-9-CM codes for a
single ICD-10 code; and– There may be multiple ICD-10 codes for a single
ICD-9-CM code.

Action Overview
• ICD-10 Awareness• Budget Strategy • Business Assessment• Internal System assessment• External (Vendor) System assessment• Implementation• Education• Testing • Maintenance and Ongoing Support
44
WHERE DO I START?
• Learn about the structure, organization and unique features of ICD-10-CM all provider types
• Understand system impact and 5010
• Identify areas of strength/weakness in medical terminology and medical record documentation
ICD-10 Preparedness
46
• Provide information on ICD usage and format
• Identify why you need ICD-10• Determine what needs to be done• Identify who needs to be involved• Discuss a time line for maximum benefit• Collect needed tools and resources

Benefits and Challenges
• Mandatory• Will cost – time and money • Learning something different• Documentation requirements• Improve business practices• Improve reporting• Reduce costs• Increase efficiency• Improve timely claim processing
47
Education
Who should receive ICD-10-CM training in your office?
• Coders• System users• Business users• Management• Physicians
48
CODER EDUCATION??
• Plan to provide intensive coder training approximately 6-9 months prior to implementation –allocating 16 hours of ICD-10-CM training will likely be adequate for most coders
• Providers should have at least 4-6 hours of ICD-10-CM training
• Other staff receiving training will determine number of hours by individual practice needs
Business Impact Assessment
• Operational processes
• Reports
• Procedures
• Charge Master or Super bills
• Pre-authorizations
• Coding changes
50
Business Impact Assessment
• Budget impact
• Cash flow
• Contract revisions
• Fee schedule changes/revisions
• Pay for performance initiatives
• Productivity losses
51
Internal System Implementation
• Data structure differences • Field structure• Programs• Maintain both ICD-9 and ICD-10 data• Implement and test systems changes.
52
External System Impact Assessment
• Vendor Readiness• Vendor Timeline• Interfaces• Cost • System changes/upgrades • Testing
53
HOW DOES THIS HELP YOU?
• Improved ability to measure health care services• Decreased need to include supporting
documentation with claims• Updated medical terminology and classification of
diseases• Codes allow comparison of mortality and morbidity
data• Better data for:
– Measuring care furnished to patients– Processing claims– Making clinical decisions– Tracking public health issues– Conducting research http://www.cms.gov/ICD10/05a_ProviderResources.asp#TopOfPage

LET’S REVIEW
• Basic Steps to Prepare for Version 5010/ICD-10
• Begin preparing now for the ICD-10 transition to make sure you are ready by the compliance deadline. The following quick checklist will assist you with preliminary planning steps.
LET’S REVIEW
• Identify your current systems and work processes that use ICD-9 codes. This could include clinical documentation, encounter forms/superbills, practice management system, electronic health record system, contracts, and public health and quality reporting protocols. It is likely that wherever ICD-9 codes now appear, ICD-10 codes will take their place.
LET’S REVIEW
• Talk with your practice management system vendor about accommodations for both Version 5010 and ICD-10 codes. Contact your vendor and ask what updates they are planning to your practice management system for both Version 5010 and ICD-10, and when they expect to have it ready to install. Check your contract to see if upgrades are included as part of your agreement. If you are in the process of making a practice management or related system purchase, ask if it is Version 5010 and ICD-10 ready.
LET’S REVIEW
• Discuss implementation plans with all your clearinghouses, billing services, and payers to ensure a smooth transition. Be proactive, don't wait. Contact your payers, clearinghouse, billing service with whom you conduct business, ask about their plans for the Version 5010 and ICD-10 compliance, and when they will be ready to test their systems for both transitions
LET’S REVIEW
• Talk with your payers about how ICD-10 implementation might affect your contracts. Because ICD-10 codes are much more specific than ICD-9 codes, payers may modify terms of contracts, payment schedules, or reimbursement.
LET’S REVIEW
• Identify potential changes to work flow and business processes. Consider changes to existing processes including clinical documentation, encounter forms, and quality and public health reporting.
LET’S REVIEW
• Assess staff training needs. Identify the staff in your office who code, or have a need to know the new codes. There are a wide variety of training opportunities and materials available through professional associations, online courses, webinars, and onsite training. If you have a small practice, think about teaming up with other local providers. You might be able, for example, to provide training for a staff person from one practice, who can in turn train staff members in other practices. MBI recommends that training take place approximately 6 months prior to the compliance date
LET’S REVIEW
• Budget for time and costs related to ICD-10 implementation, including expenses for system changes, resource materials, and training. Assess the costs of any necessary software updates, reprinting of super bills, training and related expenses.
THANK YOU VERY MUCH!





























