Embed Size (px)
Citation preview

Argon Laser Destruction of Anterior Chamber Implantation Cysts JOEL SUGAR, MD, LEE M. JAMPOL, MD, MORTON F. GOLDBERG, MD
Abstract: Five patients with anterior chamber implantation cysts underwent argon laser therapy. Three cysts were eradicated and one shrunk to a small stable remnant within 1 to 5 treatment sessions. One cyst re-formed repeatedly, prompting iridocyclectomy. Follow-up ranged from 3 to 38 months. [Key words: anterior chamber cysts, argon laser, epithelial implantation cysts.] Ophthalmology 91:1040-1044, 1984
Implantation of epithelium into the anterior chamber leading to the formation of cysts can cause ultimate ocular destruction through the development of glaucoma and intraocular inflammation. L'Esperance1 has described the use of the argon laser as a means of destroying anterior chamber implantation cysts. Few other reports have followed. 2 We describe our technical approach and results with five patients undergoing argon laser photocoagulation of anterior chamber implantation cysts.
MATERIALS AND METHODS
Five patients with anterior chamber implantation cysts were treated with argon laser photocoagulation. The photocoagulation was carried out under topical anesthesia at the slit lamp. Argon laser photocoagulation was applied using an Abraham contact lens, no contact lens, or in some cases a gonioscopy (1 mirror) lens to apply treatment posterior to the iris plane. Initially, therapy was given to normal tissue along the margins of the cyst. Shrinkage of this tissue resulted in a gradual shrinkage of the cyst. In three instances no obvious rupture of the cyst was noted. With additional shrinkage of the cyst, direct treatment was applied to pigmented portions of the anterior or posterior cyst wall. An
From the University of Illinois Eye and Ear Infirmary, Chicago.
Presented at the Eighty-eighth Annual Meeting of the American Academy of Ophthalmology, Chicago, Illinois, October 30-November 3, 1983.
Supported in part by National Institutes of Health grant EY01792.
Reprint Requests to Joel Sugar, MD, 1855 W. Taylor, Chicago, IL 60612.
1040
attempt was made to treat all portions of the cyst wall including the posterior wall. Whitening of the tissue was apparent in most areas of application of energy. When the cyst had collapsed to a solid-appearing vestige, intense treatment was then applied to this residual tissue, whether the cyst was pigmented or not. In most instances, several treatment sessions were required to cause complete collapse and apparent destruction of the cyst. Patients were seen at 1-week intervals and treatment was repeated if the cysts were persistent.
CASE REPORTS
Case 1. A 70-year-old woman underwent an apparently uncomplicated left intracapsular lens extraction at age 61 with resulting 20/20 acuity. Four years later, an iris cyst and decreasing vision were noted. When first seen by us in 1979, her best corrected vision had dropped in the left eye to 20/ 200. On slit-lamp examination (Fig 1), a bilobed cyst 8 mm horizontally by 4 mm vertically was present on the anterior iris surface. Superiorly, the cyst was in contact with the cornea, and superior corneal edema encroached on the visual axis. The posterior wall of the cyst was in contact with the pigmented posterior leaf of the iris. On April 24, 1979, treatment was carried out with 1-second burns, 500-micron spot size, and 7 50 milliwatts. During the procedure the anterior cyst wall ruptured. Two weeks later, the cyst appeared completely collapsed. Two months later, the cyst had re-formed and treatment was repeated with 121 burns of 0.5- to 1.0-second duration, 500- to 1000-micron spot size, and 700 milliwatts. The cyst was noted to shrink during the treatment but did not appear to rupture. Over the ensuing month, the corneal edema gradually resolved and visual acuity returned to 20/30. A small remnant of the cyst recurred in the region of the angle but has

SUGAR, et al • ARGON TREATMENT OF CYSTS
Fig 1. Top left, case 1: before laser treatment. Corneal edema involves superior two-thirds of cornea. Fig 2. Top right, case 1: cyst remnant remains, edema is gone. Fig 3. Center left, case 2: cyst present on anterior iris. Fig 4. Center right, case 2: 6 months post argon laser. No cyst remnants are present. Fig 5. Bottom left, case 3: large cyst arising from the posterior cornea. Fig 6. Bottom right, case 3: cyst absent.
not changed (Fig 2), and the patient's vision was 20/25 when last seen in August 1982.
Case 2. A 44-year-old woman underwent penetrating keratoplasty in her right eye in April 1981 for keratoconus. Recovery was uneventful. In April of 1982, visual acuity was 20/25 with +0.50 +3.25 X 155° and a small cyst was noted on the anterior iris surface at 2 o'clock. Over the ensuing 6 months, the cyst enlarged to 2.6 mm in diameter (Fig 3), and on October 4, 1982 this was treated with 76 argon laser burns of 100-micron spot size, 0.2 seconds duration, 200 milliwatts
power through the Abraham lens. The cyst immediately collapsed and has not recurred in 12 months follow-up (Fig 4).
Case 3. A 22-year-old man sustained a left corneal laceration on July 5, 1982. This was surgically repaired with a resultant visual acuity of 20/30. However, 5 months later a cyst was noted in the anterior chamber adherent to the cornea but not adherent to the iris (Fig 5). There was a great deal of pigment lining the posterior wall of the cyst. On December 21, 1982, 90 burns of 0.2 seconds duration, 500-micron spot size, 300 milliwatts were used to directly treat the lesion and the
1041

OPHTHALMOLOGY • SEPTEMBER 1984 • VOLUME 91 • NUMBER 9
surrounding area. One week later, 70 additional burns were placed on the cyst because it had not changed in size. These were 225 micron in spot size, 600 to 750 milliwatts power, and 0.3 seconds duration. During the procedure the cyst was noted to shrink and on the subsequent visits the cyst has not been visible (Fig 6). When last seen on August 24, 1983, the visual acuity was 20/25 and there was no cyst evident.
Case 4. A 14-year-old boy was struck in his left eye with a pencil in February of 1982. He was seen by his ophthalmologist and a corneal laceration at the superior limbus was surgically repaired. Marked vitritis followed but cleared and acuity returned to normal. Six months later, an iris implantation cyst was noted and he was referred for our evaluation. When seen by us on August 30, 1982, his visual acuity was 20/25 in his
1042
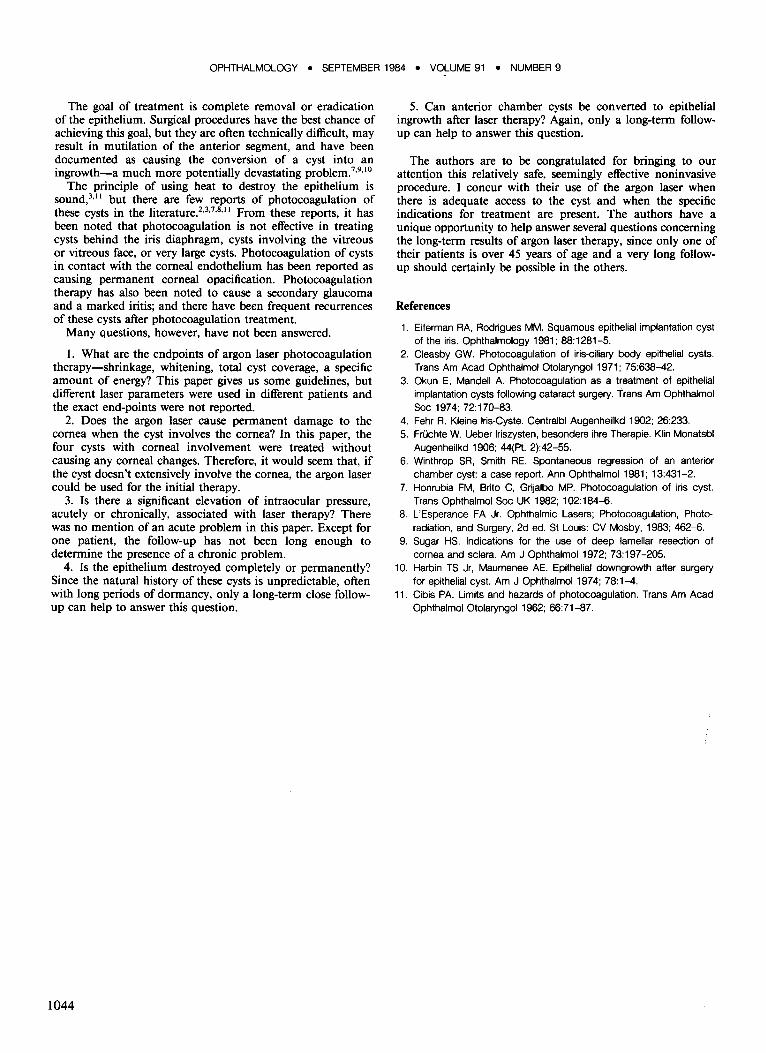
Fig 7. Top left, case 4: enlarging cyst. Fig 8. Top right, case 4: cyst no longer evident after repeated treatments. Fig 9. Center left, case 5: large cyst involving the angle and deeply imbedded in the iris. Fig 10. Center right, case 5: apparent regression of cyst after treatment. Fig 11. Bottom, case 5: recurrent cyst evident posterior to the iris.
left eye. On slit-lamp examination there was slight vascularization along the superior limbus to a horizontal corneal scar and an area of marked corneal thinning. Behind this, a cyst extended into the iris. It measured 2.0 mm vertically by 2.4 mm horizontally. Intraocular pressure by applanation was 11 mmHg, and on gonioscopy the ciliary body and iris processes were not involved. No therapy was carried out. On December 12, 1982, the patient returned, complaining that his pupil had become distorted. Vision was unchanged but the cyst had markedly enlarged (Fig 7). Treatment was carried out at that time using the argon laser with 37 burns of 0.2 seconds duration, 500 micron spot size, 300 milliwatts. The cyst was smaller 1 week later and 135 additional burns were placed around and on the lesion. These were 0.2 seconds in duration,
SUGAR, et at • ARGON TREATMENT OF CYSTS
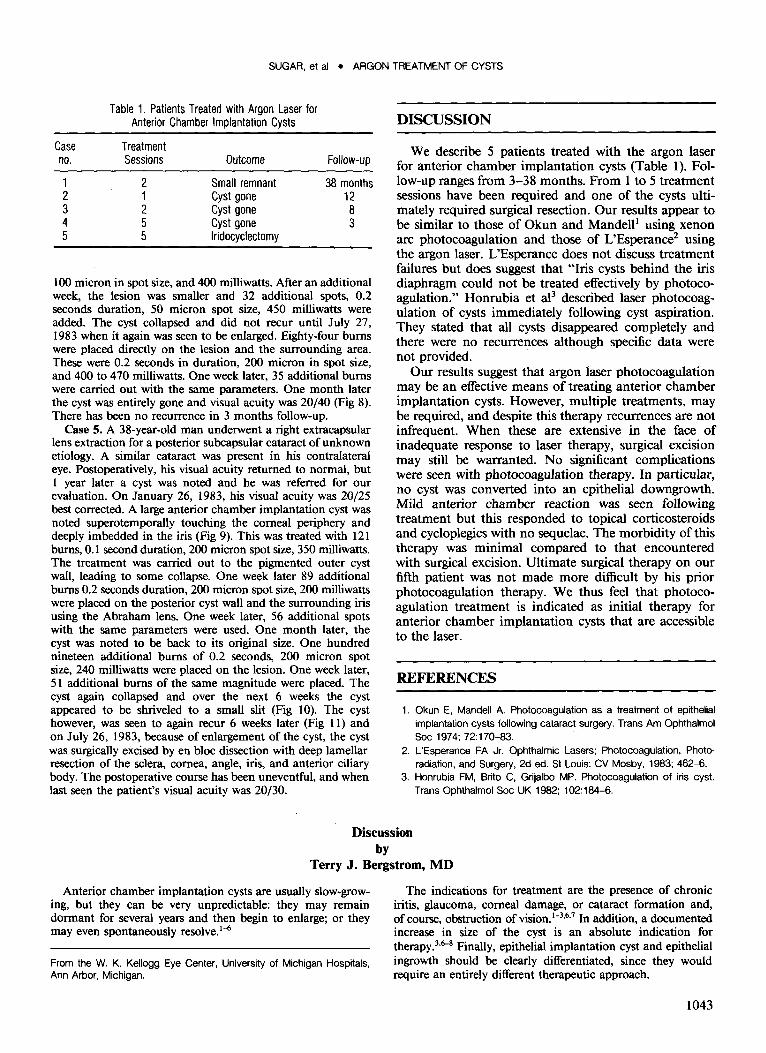
Table 1. Patients Treated with Argon Laser for Anterior Chamber Implantation Cysts
Case Treatment no. Sessions Outcome Follow-up
1 2 Small remnant 38 months 2 1 Cyst gone 12 3 2 Cyst gone 8 4 5 Cyst gone 3 5 5 Iridocyclectomy
l 00 micron in spot size, and 400 milliwatts. After an additional week, the lesion was smaller and 32 additional spots, 0.2 seconds duration, 50 micron spot size, 450 milliwatts were added. The cyst collapsed and did not recur until July 27, 1983 when it again was seen to be enlarged. Eighty-four burns were placed directly on the lesion and the surrounding area. These were 0.2 seconds in duration, 200 micron in spot size, and 400 to 470 milliwatts. One week later, 35 additional burns were carried out with the same parameters. One month later the cyst was entirely gone and visual acuity was 20/40 (Fig 8). There has been no recurrence in 3 months follow-up.
Case 5. A 38-year-old man underwent a right extracapsular lens extraction for a posterior subcapsular cataract of unknown etiology. A similar cataract was present in his contralateral eye. Postoperatively, his visual acuity returned to normal, but l year later a cyst was noted and he was referred for our evaluation. On January 26, 1983, his visual acuity was 20/25 best corrected. A large anterior chamber implantation cyst was noted superotemporally touching the corneal periphery and deeply imbedded in the iris (Fig 9). This was treated with 121 burns, 0.1 second duration, 200 micron spot size, 350 milliwatts. The treatment was carried out to the pigmented outer cyst wall, leading to some collapse. One week later 89 additional bums 0.2 seconds duration, 200 micron spot size, 200 milliwatts were placed on the posterior cyst wall and the surrounding iris using the Abraham lens. One week later, 56 additional spots with the same parameters were used. One month later, the cyst was noted to be back to its original size. One hundred nineteen additional burns of 0.2 seconds, 200 micron spot size, 240 milliwatts were placed on the lesion. One week later, 51 additional burns of the same magnitude were placed. The cyst again collapsed and over the next 6 weeks the cyst appeared to be shriveled to a small slit (Fig 10). The cyst however, was seen to again recur 6 weeks later (Fig ll) and on July 26, 1983, because of enlargement of the cyst, the cyst was surgically excised by en bloc dissection with deep lamellar resection of the sclera, cornea, angle, iris, and anterior ciliary body. The postoperative course has been uneventful, and when last seen the patient's visual acuity was 20/30.
DISCUSSION
We describe 5 patients treated with the argon laser for anterior chamber implantation cysts (Table 1). Follow-up ranges from 3-38 months. From 1 to 5 treatment sessions have been required and one of the cysts ultimately required surgical resection. Our results appear to be similar to those of Okun and Mandell1 using xenon arc photocoagulation and those of L'Esperance2 using the argon laser. L'Esperance does not discuss treatment failures but does suggest that "Iris cysts behind the iris diaphragm could not be treated effectively by photocoagulation." Honrubia et al3 described laser photocoagulation of cysts immediately following cyst aspiration. They stated that all cysts disappeared completely and there were no recurrences although specific data were not provided.
Our results suggest that argon laser photocoagulation may be an effective means of treating anterior chamber implantation cysts. However, multiple treatments, may be required, and despite this therapy recurrences are not infrequent. When these are extensive in the face of inadequate response to laser therapy, surgical excision may still be warranted. No significant complications were seen with photocoagulation therapy. In particular, no cyst was converted into an epithelial downgrowth. Mild anterior chamber reaction was seen following treatment but this responded to topical corticosteroids and cycloplegics with no sequelae. The morbidity of this therapy was minimal compared to that encountered with surgical excision. Ultimate surgical therapy on our fifth patient was not made more difficult by his prior photocoagulation therapy. We thus feel that photocoagulation treatment is indicated as initial therapy for anterior chamber implantation cysts that are accessible to the laser.
REFERENCES
1. Okun E, Mandell A. Photocoagulation as a treatment of epithelial implantation cysts following cataract surgery. Trans Am Ophthalmol Soc 1974; 72:170-83.
2. L'Esperance FA Jr. Ophthalmic Lasers; Photocoagulation, Photoradiation, and Surgery, 2d ed. StLouis: CV Mosby, 1983; 462-6.
3. Honrubia FM, Brito C, Grijalbo MP. Photocoagulation of iris cyst. Trans Ophthalmol Soc UK 1982; 102:184-6.
Discussion by
Terry J. Bergstrom, MD
Anterior chamber implantation cysts are usually slow-growing, but they can be very unpredictable: they may remain dormant for several years and then begin to enlarge; or they may even spontaneously resolve. 1
-6
From theW. K. Kellogg Eye Center, University of Michigan Hospitals, Ann Arbor, Michigan.
The indications for treatment are the presence of chronic iritis, glaucoma, corneal damage, or cataract formation and, of course, obstruction of vision. 1
-3
•6
•7 In addition, a documented
increase in size of the cyst is an absolute indication for therapy.3
•6-8 Finally, epithelial implantation cyst and epithelial
ingrowth should be clearly differentiated, since they would require an entirely different therapeutic approach.
1043
OPHTHALMOLOGY • SEPTEMBER 1984 • VOLUME 91 • NUMBER 9
The goal of treatment is complete removal or eradication of the epithelium. Surgical procedures have the best chance of achieving this goal, but they are often technically difficult, may result in mutilation of the anterior segment, and have been documented as causing the conversion of a cyst into an ingrowth-a much more potentially devastating problem.7
•9
·10
The principle of using heat to destroy the epithelium is sound,3
•11 but there are few reports of photocoagulation of
these cysts in the literature.2•3
•7
•8
•11 From these reports, it has
been noted that photocoagulation is not effective in treating cysts behind the iris diaphragm, cysts involving the vitreous or vitreous face, or very large cysts. Photocoagulation of cysts in contact with the corneal endothelium has been reported as causing permanent corneal opacification. Photocoagulation therapy has also been noted to cause a secondary glaucoma and a marked iritis; and there have been frequent recurrences of these cysts after photocoagulation treatment.
Many questions, however, have not been answered.
1. What are the endpoints of argon laser photocoagulation therapy-shrinkage, whitening, total cyst coverage, a specific amount of energy? This paper gives us some guidelines, but different laser parameters were used in different patients and the exact end-points were not reported.
2. Does the argon laser cause permanent damage to the cornea when the cyst involves the cornea? In this paper, the four cysts with corneal involvement were treated without causing any corneal changes. Therefore, it would seem that, if the cyst doesn't extensively involve the cornea, the argon laser could be used for the initial therapy.
3. Is there a significant elevation of intraocular pressure, acutely or chronically, associated with laser therapy? There was no mention of an acute problem in this paper. Except for one patient, the follow-up has not been long enough to determine the presence of a chronic problem.
4. Is the epithelium destroyed completely or permanently? Since the natural history of these cysts is unpredictable, often with long periods of dormancy, only a long-term close followup can help to answer this question.
1044
5. Can anterior chamber cysts be converted to epithelial ingrowth after laser therapy? Again, only a long-term followup can help to answer this question.
The authors are to be congratulated for bringing to our attention this relatively safe, seemingly effective noninvasive procedure. I concur with their use of the argon laser when there is adequate access to the cyst and when the specific indications for treatment are present. The authors have a unique opportunity to help answer several questions concerning the long-term results of argon laser therapy, since only one of their patients is over 45 years of age and a very long followup should certainly be possible in the others.
References
1. Eilerman RA, Rodrigues MM. Squamous epithelial implantation cyst of the iris. Ophthalmology 1981; 88:1281-5.
2. Cleasby GW. Photocoagulation of iris-ciliary body epithelial cysts. Trans Am Acad Ophthalmol Otolaryngol 1971; 75:638-42.
3. Okun E, Mandell A. Photocoagulation as a treatment of epithelial implantation cysts following cataract surgery. Trans Am Ophthalmol Soc 1974; 72:170-83.
4. Fehr R. Kleine lris-Cyste. Centralbl Augenheilkd 1902; 26:233. 5. FrUchte W. Ueber lriszysten, besonders ihre Therapie. Klin Monatsbl
Augenheilkd 1906; 44(Pt. 2):42-55. 6. Winthrop SR, Smith RE. Spontaneous regression of an anterior
chamber cyst: a case report. Ann Ophthalmol 1981; 13:431-2. 7. Honrubia FM, Brito C, Grijalbo MP. Photocoagulation of iris cyst.
Trans Ophthalmol Soc UK 1982; 102:184-6. 8. L'Esperance FA Jr. Ophthalmic Lasers; Photocoagulation, Photo
radiation, and Surgery, 2d ed. StLouis: CV Mosby, 1983; 462-6. 9. Sugar HS. Indications for the use of deep lamellar resection of
cornea and sclera. Am J Ophthalmol 1972; 73:197-205. 10. Harbin TS Jr, Maumenee AE. Epithelial downgrowth after surgery
for epithelial cyst. Am J Ophthalmol 1974; 78:1-4. 11. Cibis PA. Limits and hazards of photocoagulation. Trans Am Acad
Ophthalmol Otolaryngol1962; 66:71-87.