Arrhythmias in Children: Assessment and Management Robert H. Pass, MD Director, Pediatric Cardiac...
59
Arrhythmias in Children: Assessment and Management Robert H. Pass, MD Director, Pediatric Cardiac Electrophysiology Montefiore Medical Center – Albert Einstein College of Medicine
Arrhythmias in Children: Assessment and Management Robert H. Pass, MD Director, Pediatric Cardiac Electrophysiology Montefiore Medical Center – Albert
Arrhythmias in Children: Assessment and Management Robert H.
Pass, MD Director, Pediatric Cardiac Electrophysiology Montefiore
Medical Center Albert Einstein College of Medicine
Slide 3
Pediatric Arrhythmia Management Bradycardia (Boring) vs.
Tachycardias (Exciting) Disorders of Automaticity Disorders of
Reentry
Slide 4
Pediatric Arrhythmia Management Normal Cardiac Conduction
System Electrical Anatomic Substrate
Slide 5
Bradyarrhythmias Sinus Node Dysfunction: Rare in patients with
structurally normal hearts Commonly seen following palliative
congenital heart surgery: Acutely: AV Canal Repairs Sinus Venosus
ASD repair Chronically: Mustard/Senning Repair of DTGA Fontan
Palliation of Single Ventricular hearts
Slide 6
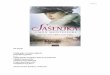
Bradyarrhythmias Mustard Procedure for D-Transposition of the
Great Arteries
Slide 7
Bradyarrhythmias 75% of all DTGA patients undergoing Mustard at
Columbia not in sinus rhythm at follow-up
Bradyarrhythmias Clinical Examples 7 year old with history of
severe cold symptoms, lethargy, dyspnea and echocardiogram
demonstrated severe ventricular dysfunction
Slide 11
Bradyarrhythmias Clinical Examples 8 year old referred to
cardiology for evaluation of heart murmur
Slide 12
Bradyarrhythmias Treatment: - Treat underlying problem - If
postoperative CHB or due to irreversible cause, pacemaker
implantation
Slide 13
Bradyarrhythmias 9 Months old30 Months old Transvenous
Pacemaker in Infant Loop technique ( from Spotnitz et al. Annals of
Thoracic Surgery, 1991 )
Slide 14
Tachyarrhythmias Disorders of Automaticity VS. Disorders of
Reentry
Slide 15
Tachyarrhythmias - Automatic Common characteristics of
automatic arrhythmias include: - heat up / cool down - No abrupt
onset or offset - Cannot be DC cardioverted - Very catecholamine
sensitive
Slide 16
Tachyarrhythmias - Automatic Clinical Examples of Automatic
Tachyarrhythmias: - Sinus tachycardia - Ectopic atrial tachycardia
(EAT) - Junctional Ectopic Tachycardia (JET) - Some types of
VT
Slide 17
Tachyarrhythmias Disorders of automaticity: Whatever is fastest
in the heart wins In automatic arrhythmias, an area of myocardium
with calcium channel cells fires at a rate that is faster than the
sinus node and therefore controls the rhythm
Slide 18
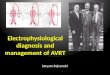
Tachyarrhythmias - Automatic Clinical Example: 14 year old girl
seen by pediatrician who heard irregular heart beat and obtained
ECG; recent history of fainting without palpitations;
Echocardiogram demonstrated severely depressed function
Slide 19
Tachyarrhythmias - Automatic EAT Ectopic Atrial Tachycardia
Atrial ectopy from a single area of atrial myocardium other than
sinus node Commonly results in ventricular dysfunction
Slide 20
Tachyarrhythmias - Automatic Clinical Example 5 mo s/p
Tetralogy of Fallot repair postoperative hour 4 JET !!!!!!!
Slide 21
Tachyarrhythmias - Automatic Clinical Example: 15 year old with
history of VT noncompliant with medication ER 1999
Slide 22
Tachyarrhythmias - Reentry Reentry - represents 90% of SVT in
pediatric populations 3 Major Requirements: 1.2 pathways connected
proximally and distally 2.Unidirectional block in one pathway 3.A
zone of slow conduction
Slide 23
Tachyarrhythmias - Reentry Reentry General Characteristics:
1.Rhythm can be initiated and terminated with appropriately timed
premature beats. 2.Abrupt onset and termination. 3.Successful
termination (at least temporarily) with DC cardioversion
Tachyarrhythmias - Reentry Accessory pathway tachycardia is
most common etiology of tachycardia in children More common in
males Typical route is from atria to ventricles via AV node and
retrograde via accessory pathway Orthodromic Reentrant Tachycardia
(ORT)
Slide 26
Tachyarrhythmias - Reentry Clinical example : 15 year old boy
with history of Ebsteins anomaly and intermittent palpitations
TachycardiaSinus Rhythm
Slide 27
Tachyarrhythmias - Reentry Peak age for occurrence of SVT/ORT
is first 2 months of age 40% of first episodes occur this early in
life Frequency decreases over first year of life 2/3 of infants no
longer have clinical tachycardia at age 1 year and 1/3 have no
evidence of accessory pathway conduction at one year by formal
transesophageal testing
Slide 28
Tachyarrhythmias - Reentry Other peaks for tachycardia
recurrence are 5-8 years and 10-15 years ~ 40% of patients with
tachycardia as young infants will recur some time in life Reasons
for this finding unclear
Slide 29
Tachyarrhythmias - Reentry WPW Paradigm of ORT First described
in 1930 Short PR interval, bundle branch block on resting surface
ECG and intermittent tachycardia Presence of delta wave ventricular
preexcitation Risk of sudden death ~ 1.5/1000 pt. years
Slide 30
Tachyarrhythmias - Reentry Clinical example: 15 year old boy
with insignificant past medical history seen in ER with
palpitations and dizziness
Slide 31
Tachyarrythmias - Reentry Acute therapy was administered :
Slide 32
Tachyarrhythmias - Reentry ECG s/p DC Cardioversion Wolff
Parkinson White Syndrome!
Slide 33
Tachyarrhythmias - WPW Mechanism of arrhythmia is preexcited
atrial fibrillation Most common cause of sudden death in WPW
Slide 34
Tachyarrhythmias - WPW WPW Key points: 1.Risk of death is not
from SVT/ORT but instead from rapidly conducted A fib (rare in
infants). 2.Digoxin/Verapamil are contraindicated in older
patients. 3.Parent education about identifying tachycardia
critical.
Slide 35
Tachyarrhythmias - Reentry 16 year old with palpitations and
dizziness 10 years s/p Fontan palliation for tricuspid atresia
Slide 36
Tachyarrhythmias - Reentry Intraatrial Reentrant Tachycardia
(IART): -Common problem affecting 12.5-26% of patients with
repaired/palliated CHD at intermediate and long-term follow-up
-Particular problem among Fontan patients
Slide 37
Tachyarrhythmias - Reentry IART is virtually universal
following Fontan (from Fishberger et al. JTCVS, 1997)
Slide 38
Tachyarrhythmias - Reentry Typical IART reentrant loop due to
scarring in postoperative children
Slide 39
Tachyarrhythmias Summary of Mechanisms Level of
HeartAutomaticityReentry SA NodeSinus tachycardia SA node reentry
Atrial muscleEAT/MATAflutter/Afib AV NodeJETAVNRT AV
reciprocatingNAWPW/ Concealed AP VentriclesVT/VFVT
Slide 40
Tachyarrhythmias - Treatment Chronic/Definitive therapy: Drug
therapy in general, for most forms of SVT, drugs are effective Most
commonly used agents: Digoxin Sotalol Procainamide Amiodarone
Betablockers Flecainide Verapamil
Slide 41
Tachyarrhythmias Drug Therapy Acute therapy: IV adenosine
causes transient AV nodal blockade Particularly useful for AV
reciprocating tachycardias such as ORT or AVNRT (2 most common SVTs
in children) IV verapamil also causes AV nodal blockade Not as
commonly used due to potent negative inotropy also shown to be
associated with cardiovascular collapse in infants
Slide 42
Tachyarrhythmias Drug Therapy Chronic Therapy: (Infancy)
Digoxin Useful antiarrhythmic agent in infants Causes AV nodal
slowing and reduces atrial ectopy Dosing from 8-14 mcg/kg/day
divided bid Beta Blockers Useful alternative antiarrhythmic agent
in infants Causes AV nodal slowing and reduces atrial ectopy
Commonly used agent is Inderal Associated with low blood glucose
levels D sticks must be monitored initially
Slide 43
Arrhythmias Drug Therapy Chronic Therapy Children and
Adolescents: Beta blockade effective about 60-75% Low side effect
profile Calcium channel blockers similar efficacy Low side effect
profile (e.g. Verapamil) Digoxin not as effective in older patients
as in infancy and thus not typically used in this age range
Slide 44
Arrhythmias Drug Therapy Chronic Therapy When the SIMPLE STUFF
doesnt work: Sotalol Class III agent Potent beta blocker High
incidence of proarrhythmia (~ 10%) Significantly more effective
than simple agents Flecainide Class Ib agent Very effective ? High
incidence of proarrhythmia (CAST study)
Slide 45
Arrhythmias Drug Therapy Amiodarone Class III agent (all 4
Vaughn Williams classification effects) Very effective agent Very
long half life (~ 45 days) Low incidence of proarrhythmia High side
effect profile PulmonaryLiverThyroidSkin EyeGI tract
Slide 46
Tachyarrhythmias - Therapy Drugs are not a free ride - Side
effects (cardiac and non-cardiac) - Proarrhythmia - Not always
efficacious - Compliance -? Lifelong usage - For WPW, may not
reduce risk of sudden death
Slide 47
Tachyarrhythmias - Therapy Drug therapy for IART stinks -%
freedom from recurrence of IART on various antiarrhythmic agents in
patients s/p CHD surgery from Weindling et al. Unpublished
abstract
Slide 48
Tachyarrhythmias - Therapy Radiofrequency Catheter Ablation
(RFCA) Advantages: Potentially Definitive therapy Drug use often
not required following procedure
Tachyarrhythmias - Therapy Simplified example of successful
ablation of left sided EAT focus in 5 year old
Slide 51
Slide 52
Tachyarrhythmias - Therapy DiagnosisSuccess (%) WPW94 Concealed
AP99 PJRT95 EAT100 Mahaim100 AVNRT83 Totals90 RFCA Success Rates
are quite high ! (Boston Childrens Data J Peds 1997) Data from
Childrens Hospital at Montefiore for past 3 years overall success
rate ~ 94%
Slide 53
Tachyarrhythmias - Therapy Risks associated with RFCA: Normal
cath risks: bleeding, stroke, infection Serious complications
(death, ventricular dysfunction, CVA, cardiac perforation) Occurred
1.2% of time in Tanel, Boston Childrens Study (1997)
Slide 54
Tachyarrhythmias - Therapy Angiogram of Fontan GIGANTIC RA so
much ground to cover
Slide 55
Tachyarrhythmias - Therapy Data for standard RFCA of IART have
been generally poor using standard techniques ~ 50% arrhythmia free
at 2 years follow-up In light of these findings, interest in newer
mapping techniques are growing
Tachyarrhythmias New Mapping Strategies Electroanatomical
Mapping Non Contact Endocardial Solutions 9 French Balloon
Catheter
Slide 58
Tachyarrhythmias Newer Therapies Newer Chilli catheters
allowing larger and deeper radiofrequency lesions for IART in
Fontan patients
Slide 59
Cryoablation Smaller reversible lesions
Slide 60
Tachyarrhythmias New Directions Refining of newer mapping
strategies for better understanding of scar anatomy and its
relationship to IART Newer surgical approaches to congenital
surgery to reduce rates of IART or to treat it (cryosurgery) New
catheter design to lower cath-related risks of RFCA (e.g.
Cryocatheters) Use of low fluoroscopy protocols and 3 D
electroanatomical mapping techniques to reduce exposure to ionizing
radiation