Embed Size (px)
Citation preview

J Neurosurg: Pediatrics / Volume 9 / January 2012
J Neurosurg Pediatrics 9:000–000, 2012
11
Arteriovenous malformations are one of the major causes of stroke in children.1,4–6 Because intrace-rebral hemorrhage is the most devastating as well
as the most common clinical presentation (46%–87%) in children with AVMs, there is a strong interest in establish-ing treatment strategies that could prevent or reduce both the initial hemorrhage and possible rebleeding.7,9,11,14,15,17
Aneurysms separate and distinct from the circle of Willis are commonly found located adjacent to or within AVMs, and are typically classified as either arterial, in-tranidal, or venous in location.21,22 The nature of these
AVM-associated aneurysms has been partially investi-gated in adults.3,18,19,24,25 Although the data are mixed, the preponderance of data suggests that the presence of an aneurysm may be an independent risk factor for hemor-rhage in adults with AVMs.12,13,16,19,22,24,26 For this reason, most adults with ruptured AVMs undergo prompt cere-bral angiography with endovascular treatment of AVM-associated aneurysms. In children, however, conventional cerebral angiography and treatment are often performed in a delayed fashion, in part because the nature of AVM-associated aneurysms is generally unknown. Because pe-
J Neurosurg Pediatrics 9:11–16, 2012
Arteriovenous malformation–associated aneurysms in the pediatric population
Clinical article
RichaRd c. E. andERson, M.d., MichaEl M. McdowEll, B.s., chRistophER p. KEllnER, M.d., GEoffREy appElBooM, M.d., saMuEl s. BRucE, B.a., ivan s. KotchEtKov, B.a., RaqEEB haquE, M.d., nEil a. fEldstEin, M.d., E. sandER connolly JR., M.d., RoBERt a. soloMon, M.d., philip M. MEyERs, M.d., and sEan d. lavinE, M.d.Columbia University, Department of Neurological Surgery, New York, New York
Object. Conventional cerebral angiography and treatment for ruptured arteriovenous malformations (AVMs) in children are often performed in a delayed fashion. In adults, current literature suggests that AVM-associated aneu-rysms may be more likely to hemorrhage than isolated AVMs, which often leads to earlier angiography and endo-vascular treatment of associated aneurysms. The nature of AVM-associated aneurysms in the pediatric population is virtually unknown. In this report, the authors investigate the relationship of associated aneurysms in a large group of children with AVMs.
Methods. Seventy-seven pediatric patients (≤ 21 years old) with AVMs were treated at the Columbia University Medical Center between 1991 and 2010. Medical records and imaging studies were retrospectively reviewed, and associated aneurysms were classified as arterial, intranidal, or venous in location. Clinical presentation and outcome variables were compared between children with and without AVM-associated aneurysms.
Results. A total of 30 AVM-associated aneurysms were found in 22 children (29% incidence). Eleven were arte-rial, 9 intranidal, and 10 were venous in location. There was no significant difference in the rate of hemorrhage (p = 0.91) between children with isolated AVMs (35 of 55 [64%]) and children with AVM-associated aneurysms (13 of 22 [59%]). However, of the 11 children with AVM-associated aneurysms in an arterial location, 10 presented with hemorrhage (91%). An association with hemorrhage was significant in univariate analysis (p = 0.045) but not in multivariate analysis (p = 0.37).
Conclusions. Associated aneurysms are present in nearly a third of children with AVMs, and when arterially located, are more likely to present with hemorrhage. These data suggest that early angiography with endovascular treatment of arterial-based aneurysms in children with AVMs may be indicated. (http://thejns.org/doi/abs/10.3171//2011.10.PEDS11181)
KEy woRds • arteriovenous malformation • aneurysm • angiography • intracerebral hemorrhage • vascular disorders
11
Abbreviations used in this paper: AVM = arteriovenous mal-formation; GCS = Glasgow Coma Scale; mRS = modified Rankin scale.
This article contains some figures that are displayed in color on line but in black and white in the print edition.

R. C. E. Anderson et al.
12 J Neurosurg: Pediatrics / Volume 9 / January 2012
diatric and adult aneurysms may have different causes, extrapolation of data from adult studies may not be appli-cable.2,8,20 In this study, we examined a large single-center experience to determine the incidence and behavior of AVM-associated aneurysms in children with AVMs.
MethodsStudy Population
We performed a retrospective review of patients ≤ 21 years old who presented to Columbia University/Morgan Stanley Children’s Hospital of New York between 1991 and 2010 with the diagnosis of a cerebral AVM. Hospital records, office charts, and radiographic imaging studies were reviewed. All patients underwent conventional cere-bral angiography. Patients with other cerebrovascular le-sions including dural fistulas, circle of Willis aneurysms, and vein of Galen malformations were excluded. Patients who did not undergo any form of subsequent treatment of the AVM were excluded. All imaging studies were re-viewed by an attending neurosurgeon, an endovascular neurosurgeon (S.D.L.), and an interventional neuroradi-ologist (P.M.M.).
Outcome AssessmentPatients were divided into 2 groups: those with iso-
lated AVMs and those with AVM-associated aneurysms. Aneurysms were defined as saccular dilations of the lu-men of a blood vessel with characteristic delayed filling relative to nearby regions. In patients with AVM-associat-ed aneurysms, the aneurysm location was subdivided into arterial, intranidal, or venous (Fig. 1). Clinical and radio-graphic data were collected to determine the pediatric ad-justed GCS score on presentation, presence or absence of intracranial hemorrhage, and the Spetzler-Martin grade of each lesion. Outcomes were measured by comparing mRS scores at admission, discharge, and latest follow-up. The time from radiographic diagnosis to initial emboliza-tion, resection, or radiation of the aneurysm and AVM was compared between groups.
TreatmentIn this study, children presenting with AVM-associ-
ated hemorrhage underwent urgent cerebral angiography when medically stable. If any AVM-associated arterial or intranidal aneurysms were identified, and the bleed pattern or aneurysm morphology was suspicious for the aneurysm
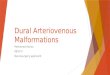
Fig. 1. Representative angiograms from patients with AVM-associated aneurysms. A: Anteroposterior projection demon-strating a parietal AVM arising from the middle cerebral artery vasculature and a concurrent intranidal aneurysm (arrow). B: Oblique view demonstrating a parietal AVM arising from the middle cerebral artery vasculature with a venous aneurysm (ar-row). C: Lateral view demonstrating an occipital AVM arising from the posterior cerebral artery vasculature with an arterial aneurysm (arrow).

J Neurosurg: Pediatrics / Volume 9 / January 2012
Aneurysms and arteriovenous malformations in children
13
to be the likely source of the hemorrhage, endovascular treatment of the aneurysms was performed at that time. Embolization for venous aneurysms was not performed. Treatment of the AVM nidus was performed in a delayed fashion using a combination of endovascular staged em-bolization, open surgical excision, or stereotactic radio-surgery. Patients with isolated or unruptured AVMs were treated in a delayed fashion using similar modalities.
Statistical AnalysisUnivariate analyses were conducted to determine
associations of clinical, radiographic, and demographic variables with the presence of AVM-associated aneurysm and incidence of AVM hemorrhage. The Fisher exact test, chi-squared test, t-test, Wilcoxon signed-rank test, and Mann-Whitney U-test were used as appropriate. All variables with a univariate association of p < 0.02 were entered in a logistic regression model to predict AVM hemorrhage. All statistical analyses were performed us-ing SPSS version 18.
ResultsStudy Population
Seventy-seven children with cerebral AVMs were treated during the study period. The mean age was 13.4 years, with 38 boys (49%) and 39 girls (51%). Eleven (14%) children were treated with surgical excision alone, 16 (21%) by radiosurgery alone, 43 (56%) with endovas-cular occlusion followed by surgical excision, 4 (5%) with endovascular occlusion followed by radiosurgery, 2 (3%) by radiosurgery and excision, and 1 (1%) using only em-bolization. There were no cases of patients presenting with hemorrhage who did not receive subsequent treat-ment for the AVM.
Association Between AVM-Associated Aneurysms, Hemorrhage, and Outcome
A total of 30 aneurysms were found in 22 patients (29% of cases). Eleven were arterial (37%), 9 intranidal (30%), and 10 venous (33%) in location (Table 1). Multiple aneurysms were present in 7 cases (32% of patients). When patients were divided into those with or without AVM-as-sociated aneurysms, there was no significant difference in the mean age of patients, sex, or location of AVM.
When AVM size, venous drainage, and eloquence were examined to determine Spetzler-Martin grades, no significant differences were found between children with isolated AVMs and those with AVM-associated aneurysms
(Tables 2 and 3). There was a significant finding regarding a larger nidus size in AVM patients with associated aneu-rysms (p = 0.019).
Overall, 48 (62%) of 77 children presented with hem-orrhage. A number of factors had a univariate association with presence of hemorrhage, including arterial-based an-eurysm presence (p = 0.045), age (p = 0.018), symptomatic discovery (p < 0.001), admission GCS score (p < 0.001), and admission mRS score (p < 0.001; Table 4). Only ad-mission mRS score remained significant after multivari-ate analysis (p = 0.028), with age possessing a strong trend toward significance (p = 0.082).
When children with isolated AVMs (35 of 55 [64%]) were compared with children with AVM-associated aneu-rysms (13 of 22 [59%]), there was no significant difference in the rate of hemorrhage (p = 0.91; Table 2). However, of the 11 children with AVM-associated aneurysms in an ar-terial location, 10 presented with hemorrhage (91%). In 7 of the 10 cases, the location of the bleed and morphology of the aneurysm suggested that the aneurysm bled. There was a significantly higher initial hemorrhage rate with arterial aneurysms than those in children with isolated AVMs (35 of 55 [64%]; p = 0.023) or those with aneurysms only in other locations (3 of 11 [27%]; p = 0.001). When multivari-ate logistic regression analysis was performed, however, the association between an arterial-based aneurysm and hemorrhage did not reach statistical significance as an in-dependent risk factor for hemorrhage (p = 0.37).
There was no significant difference in initial GCS score between children with isolated AVMs and those with AVM-associated aneurysms (mean 13.9 for both
TABLE 1: Location of AVM-associated aneurysms and risk of hemorrhage
Aneurysms No. of Cases No. (%) w/ Hemorrhage
arterial 11 10 (91)venous 10 4 (40)intranidal 9 3 (33)multiple 7 3 (43)
TABLE 2: Univariate analysis results of AVM subgroups
Factor AVM OnlyAVM &
Aneurysmp
Value
no. of cases 55 22age ± SD (yrs) 13.63 ± 5.35 12.73 ± 5.881 0.515lt-sided AVM 33 (60%) 12 (55%) 0.661AVM location 0.561 lobar 41 (75%) 15 (68%) deep 9 (16%) 3 (14%) infratentorial 5 (9%) 4 (18%)female 29 (53%) 9 (41%) 0.349symptomatic discovery 46 (84%) 21 (95%) 0.265drainage (deep component) 24 (44%) 10 (45%) 0.913eloquent 38 (69%) 17 (77%) 0.833nidus size (3–6 cm) 11 (20%) 9 (41%) 0.019*mean Spetzler-Martin grade II (II–III) III (II–III) 0.169hemorrhage 35 (64%) 13 (59%) 0.911admission GCS score (range) 13.9 (13–15) 13.9 (13.5–15) 0.405mean mRS score (range) discharge 1 (0–1) 2 (1–2) 0.027* admission 1 (1–2) 2 (1–3) 0.100 most recent 0 (0–1) 0 (0–2) 0.179 change 1.36 (1–1) 1.39 (0–2) 0.928
* Significant in the univariate analysis.

R. C. E. Anderson et al.
14 J Neurosurg: Pediatrics / Volume 9 / January 2012
groups; p = 0.405; Table 2). When clinical status was compared (using mRS score) there was no significant dif-ference between the two groups at presentation and most recent follow-up, although there was a significant differ-ence at discharge (p = 0.027; Table 2). The overall cohort showed improvement in clinical status from admission to most recent follow-up (p = 0.005). Children with both iso-lated AVMs and AVM-associated aneurysms had equiva-lent clinical improvement over time (average mRS score improvement 1.36 and 1.39, respectively; p > 0.9; Table 2).
Association Between Hemorrhage, Time Until Treatment, and Aneurysm Presence
In patients with an AVM only, the average time be-tween diagnosis and initiation of treatment was 56 days. However, in children with AVM and concurrent aneu-rysms, there was a mean time of 8 days between diagno-sis and treatment (p < 0.001). In patients who presented with hemorrhage who were found to harbor arterial aneu-rysms that were believed to be the cause of hemorrhage, the average time from diagnosis to treatment was 2.4
days. In this series, there were no patients who suffered from hemorrhage after presentation or treatment but prior to complete obliteration of the AVM.
DiscussionIn this study we have shown that nearly one-third of
children with AVMs harbor associated aneurysms. Fur-thermore, the presence of an AVM-associated aneurysm in an arterial location is strongly associated with hemor-rhage in children. To the best of our knowledge, this is the largest study to report the overall incidence of AVM-associated aneurysms in children as well as their associa-tion with hemorrhage.
An AVM-associated aneurysm was found in 29% of children with AVMs in this study. The majority of aneu-rysms were arterial in location (37%), with a similar per-centage of intranidal (30%) and venous (33%) locations. The presence of an aneurysm could not be predicted based on patient age, sex, or location of the AVM. The Spetzler-Martin scale and its components were also not found to be associated with the presence or absence of aneurysms within this cohort. These findings are similar to inci-dences reported in adult studies but substantially higher than prior reports suggesting a lower incidence (around 9%) of aneurysms in children.20,22 A much smaller study10 recently reported a 16.7% incidence of associated arte-rial and intranidal aneurysms in pediatric patients with AVMs, which is more comparable to patients within this study presenting with these particular types of aneurysm (23%). Possible explanations for such differences from older publications may be the larger size of this study or
TABLE 3: Comparison of Spetzler-Martin grades in the AVM groups
Spetzler-Martin Grade No. w/ AVM Only (%) No. w/ AVM & Aneurysm (%)
I 10 (18) 2 (9)II 21 (38) 8 (36)III 21 (38) 8 (36)IV 3 (5) 4 (18)
TABLE 4: Univariate and multivariate analysis of factors associated with hemorrhage
p ValueFactor Hemorrhage No Hemorrhage Univariate Multivariate
no. of patients 48 29age ± SD (yrs) 12.31 ± 5.85 15.14 ± 4.35 0.018 0.082lt-sided AVM 26 (54%) 19 (66%) 0.327AVM location 0.561 lobar 36 (75%) 20 (69%) deep 5 (10%) 7 (24%) infratentorial 7 (15%) 2 (7%)female 26 (54%) 12 (41%) 0.277symptomatic discovery 47 (98%) 20 (69%) <0.001 0.094drainage (deep component) 23 (48%) 11 (38%) 0.393eloquent 34 (71%) 20 (69%) 0.862nidus size (3–6 cm) 10 (21%) 10 (35%) 0.186 0.217arterial aneurysm 10 (21%) 1 (3%) 0.045 0.368admission GCS score 13 (12.25–15) 15 (15–15) <0.001 0.276mean Spetzler-Martin grade (range) 2 (2–3) 3 (2–3) 0.798mean mRS score discharge 1 (0–2) 1 (0–1) 0.089 admission 2 (1–3) 1 (0.25–1) <0.001 0.028 most recent 0 (0–2) 0 (0–0) 0.057 change 1 (1–2) 1 (0–1) 0.004

J Neurosurg: Pediatrics / Volume 9 / January 2012
Aneurysms and arteriovenous malformations in children
15
the more sophisticated and detailed angiographic images currently available with biplane digital subtraction angi-ography compared with single-plane manual subtraction angiography in older studies.
Sixty-two percent of patients in this study presented with hemorrhage. This high level of hemorrhage on pre-sentation is consistent with other recent studies focusing on pediatric AVMs.6,9–11,14,15,17,26 Overall, the presence of an AVM-associated aneurysm was not associated with a significant difference in the incidence of hemorrhage. This is probably because AVM-associated aneurysms in only venous and intranidal locations (48% of patients) did not appear to be associated with hemorrhage when separated from arterial aneurysms for additional statisti-cal analysis. However, there was an association between AVM-associated aneurysms in an arterial location with hemorrhage. Seven of the 10 patients with arterial-based aneurysms had radiographic evidence highly suggestive that the aneurysm was the source of the hemorrhage. This is in agreement with some studies in adult patients with AVMs, where the presence of an aneurysm has been shown to be an independent risk factor for hemorrhage.3 In this study, the association between an arterial-based aneurysm and hemorrhage reached statistical significance on univariate analysis (p = 0.045). However, multivariate logistic regression analysis demonstrated a trend, but did not reach statistical significance, as an independent risk factor for hemorrhage (p = 0.37). The most likely expla-nation for this difference is that despite the large size of our study, the overall low incidence of arterial-based an-eurysms led to insufficient power to convey the statisti-cally significant additional risk of concurrent arterial an-eurysms and AVMs. From our clinical experience in both children and adults, we believe that arterial aneurysms present an increased risk of hemorrhage in the pediatric population, and as such should be treated in the acute set-ting. Our hypothesis is that the flow dynamics of an AVM with an arterially based aneurysm are altered enough to affect the transmural pressure and lead to an increased risk of rupture, possibly due to the higher flow rate and pressure on the arterial side of an AVM compared with an intranidal location or the venous side.
Regarding clinical status, our data confirm prior studies that demonstrate that children with AVMs over-all improve clinically over time.23 Comparison of clinical status at initial presentation, discharge, and most recent follow-up all suggested that while children with AVM-associated aneurysms have worse neurological status at discharge, there was no significant difference between children with isolated AVMs and those with AVM-asso-ciated aneurysms at long-term follow-up.
Contrary to many other pediatric centers, our clini-cal practice for the past 2 decades has been to perform urgent cerebral angiography in children with suspected AVMs to identify and potentially treat AVM-associated aneurysms. We have done this because of our hypothesis that AVM-associated aneurysms have a higher risk of rehemorrhage than isolated AVMs. The purpose of this paper was not to discuss indications or compare treatment strategies for children with AVMs. Rather, we intended only to determine if our clinical approach was supported
by data. The limitations of this paper are those inherent to a retrospective review and that because of the absence of a control group, our data do not allow us to make any conclusions regarding whether early treatment of AVM-associated aneurysms actually reduces the incidence of initial or recurrent hemorrhage.
ConclusionsAssociated aneurysms are present in nearly one-third
of children with AVMs. When they are arterially located, they may be more likely to present with hemorrhage than if intranidal or venous in location, or if no aneurysm is present. These data suggest that early angiography with endovascular treatment of arterial-based aneurysms in children with AVMs may be indicated.
Disclosure
Dr. Lavine is a consultant for Codman Neurovascular.Author contributions to the study and manuscript preparation
include the following. Conception and design: Anderson, Kellner, Appelboom, Kotchetkov, Haque, Feldstein, Connolly, Meyers. Acquisition of data: Anderson, McDowell, Kellner, Appelboom, Bruce, Kotchetkov, Haque, Feldstein, Connolly, Meyers. Analysis and interpretation of data: Anderson, McDowell, Kellner, Appelboom, Bruce, Kotchetkov, Haque, Feldstein, Connolly, Meyers, Lavine. Drafting the article: Anderson, McDowell, Kellner, Appelboom, Bruce, Kotchetkov, Haque, Feldstein, Solomon, Meyers, Lavine. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final ver-sion of the manuscript on behalf of all authors: Anderson. Statistical analysis: Anderson, McDowell, Kellner, Bruce, Feldstein, Connolly, Solomon, Meyers, Lavine. Administrative/technical/material sup-port: Anderson, Feldstein, Connolly, Solomon, Meyers, Lavine. Study supervision: Anderson, Feldstein, Solomon, Meyers, Lavine.
References
1. Blom I, De Schryver EL, Kappelle LJ, Rinkel GJ, Jennekens-Schinkel A, Peters AC: Prognosis of haemorrhagic stroke in childhood: a long-term follow-up study. Dev Med Child Neu-rol 45:233–239, 2003
2. Broderick J, Talbot GT, Prenger E, Leach A, Brott T: Stroke in children within a major metropolitan area: the surprising importance of intracerebral hemorrhage. J Child Neurol 8:250–255, 1993
3. Cunha e Sa MJ, Stein BM, Solomon RA, McCormick PC: The treatment of associated intracranial aneurysms and arteriove-nous malformations. J Neurosurg 77:853–859, 1992
4. Earley CJ, Kittner SJ, Feeser BR, Gardner J, Epstein A, Woz-niak MA, et al: Stroke in children and sickle-cell disease: Bal-timore-Washington Cooperative Young Stroke Study. Neurol-ogy 51:169–176, 1998
5. Eeg-Olofsson O, Ringheim Y: Stroke in children. Clinical char-acteristics and prognosis. Acta Paediatr Scand 72:391–395, 1983
6. Fullerton HJ, Achrol AS, Johnston SC, McCulloch CE, Hi-gashida RT, Lawton MT, et al: Long-term hemorrhage risk in children versus adults with brain arteriovenous malforma-tions. Stroke 36:2099–2104, 2005
7. Fullerton HJ, Wu YW, Sidney S, Johnston SC: Recurrent hem-orrhagic stroke in children: a population-based cohort study. Stroke 38:2658–2662, 2007
8. Hetts SW, Narvid J, Sanai N, Lawton MT, Gupta N, Fullerton HJ, et al: Intracranial aneurysms in childhood: 27-year single-institution experience. AJNR Am J Neuroradiol 30:1315–1324, 2009

R. C. E. Anderson et al.
16 J Neurosurg: Pediatrics / Volume 9 / January 2012
9. Hladky JP, Lejeune JP, Blond S, Pruvo JP, Dhellemmes P: Ce-rebral arteriovenous malformations in children: report on 62 cases. Childs Nerv Syst 10:328–333, 1994
10. Hoffman C, Riina HA, Stieg P, Allen B, Gobin YP, Santil-lan A, et al: Associated aneurysms in pediatric arteriovenous malformations and the implications for treatment. Neurosur-gery 69:315–322, 2011
11. Hofmeister C, Stapf C, Hartmann A, Sciacca RR, Mansmann U, terBrugge K, et al: Demographic, morphological, and clini-cal characteristics of 1289 patients with brain arteriovenous malformation. Stroke 31:1307–1310, 2000
12. Jordan LC, Johnston SC, Wu YW, Sidney S, Fullerton HJ: The importance of cerebral aneurysms in childhood hemorrhagic stroke: a population-based study. Stroke 40:400–405, 2009
13. Kim EJ, Halim AX, Dowd CF, Lawton MT, Singh V, Bennett J, et al: The relationship of coexisting extranidal aneurysms to intracranial hemorrhage in patients harboring brain arteriove-nous malformations. Neurosurgery 54:1349–1358, 2004
14. Klimo P Jr, Rao G, Brockmeyer D: Pediatric arteriovenous malformations: a 15-year experience with an emphasis on re-sidual and recurrent lesions. Childs Nerv Syst 23:31–37, 2007
15. Kondziolka D, Humphreys RP, Hoffman HJ, Hendrick EB, Drake JM: Arteriovenous malformations of the brain in chil-dren: a forty year experience. Can J Neurol Sci 19:40–45, 1992
16. Laakso A, Dashti R, Juvela S, Niemelä M, Hernesniemi J: Natural history of arteriovenous malformations: presentation, risk of hemorrhage and mortality. Acta Neurochir Suppl 107: 65–69, 2010
17. Maher CO, Scott RM: Linear vein-based arteriovenous mal-formations in children. Clinical article. J Neurosurg Pediatr 4:12–16, 2009
18. Meisel HJ, Mansmann U, Alvarez H, Rodesch G, Brock M, Lasjaunias P: Cerebral arteriovenous malformations and as-sociated aneurysms: analysis of 305 cases from a series of 662 patients. Neurosurgery 46:793–802, 2000
19. Miyasaka K, Wolpert SM, Prager RJ: The association of ce-rebral aneurysms, infundibula, and intracranial arteriovenous malformations. Stroke 13:196–203, 1982
20. Niazi TN, Klimo P Jr, Anderson RC, Raffel C: Diagnosis and management of arteriovenous malformations in children. Neu-rosurg Clin N Am 21:443–456, 2010
21. Okamoto S, Handa H, Hashimoto N: Location of intracranial aneurysms associated with cerebral arteriovenous malforma-tion: statistical analysis. Surg Neurol 22:335–340, 1984
22. Redekop G, TerBrugge K, Montanera W, Willinsky R: Arte-rial aneurysms associated with cerebral arteriovenous malfor-mations: classification, incidence, and risk of hemorrhage. J Neurosurg 89:539–546, 1998
23. Sanchez-Mejia RO, Chennupati SK, Gupta N, Fullerton H, Young WL, Lawton MT: Superior outcomes in children com-pared with adults after microsurgical resection of brain arte-riovenous malformations. J Neurosurg 105 (2 Suppl):82–87, 2006
24. Stapf C, Mohr JP, Pile-Spellman J, Sciacca RR, Hartmann A, Schumacher HC, et al: Concurrent arterial aneurysms in brain arteriovenous malformations with haemorrhagic presentation. J Neurol Neurosurg Psychiatry 73:294–298, 2002
25. Thompson RC, Steinberg GK, Levy RP, Marks MP: The man-agement of patients with arteriovenous malformations and as-sociated intracranial aneurysms. Neurosurgery 43:202–212, 1998
26. Turjman F, Massoud TF, Viñuela F, Sayre JW, Guglielmi G, Duckwiler G: Correlation of the angioarchitectural features of cerebral arteriovenous malformations with clinical presenta-tion of hemorrhage. Neurosurgery 37:856–862, 1995
Manuscript submitted May 4, 2011.Accepted October 10, 2011.Please include this information when citing this paper: DOI:
10.3171/2011.10.PEDS11181. Address correspondence to: Richard C. E. Anderson, M.D., The
Neurological Institute, 710 West 168th Street, Room 213, New York, New York 10032. email: [email protected].