-
8/13/2019 artif cell 24515305
1/19
Comparison of Treatment Modalities for
Hemorrhagic Shock
Anthony T. W. Cheung, Patricia L. (Duong) To, Danielle M.
Chan,
Sahana Ramanujam, and Michelle A. Barbosa
Department of Medical Pathology and Laboratory
Medicine,University of California, Davis School of
Medicine,Sacramento, CA, USA
Peter C. Y. Chen
Department of Bioengineering, University of California,San
Diego, La Jolla, CA, USA
Bernd Driessen
Department of Clinical Studies, University of Pennsylvania
School of Veterinary Medicine, Kennett Square,PA, USA
The research was partially funded by NIH grant (HL67432) awarded
toATWC, a UC Davis Professional Development Award to ATWC, a UC
DavisSchool of Medicine Faculty Research Award to ATWC, a UC Davis
School ofMedicine Robert Stowell (MD=PhD) Scholarship Award to
PLDT, a UC Davis
Hugh Edmondson Summer Research Fellowship to PLDT, and a
HowardHughes Medical Institute (S.H.A.R.P.) Research Fellowship to
PLDT.The subject materials in this manuscript have been presented,
in parts, in a
poster=discussion session in a workshop session lecture at the
9th InternationalSymposium on Blood Substitutes (Tokyo, Japan), a
lecture at the 23rd Meetingof the European Society for
Microcirculation (Lisbon, Portugal), a lecture atthe 05 Asian
Conference on the Microcirculation (Tokyo, Japan), and a lectureat
the 10th International Symposium on Blood Substitutes (Providence,
RI,USA). In addition, parts of this article have been published in
the symposiumproceedings of these international meetings.
The assistance of Cindy Her and Erin Lee, in the preparation of
this manu-script, is very much appreciated.Address correspondence
to Dr Anthony T W Cheung Professor and Vice
Artificial Cells, Blood Substitutes, and Biotechnology, 35:
173190, 2007
CopyrightQ Informa Healthcare
ISSN: 1073-1199 print/1532-4184 online
DOI: 10.1080/10731190601188257
-
8/13/2019 artif cell 24515305
2/19
Jonathan S. Jahr
Department of Anesthesiology, University of California,
Los Angeles David Geffen School of Medicine, Los Angeles,
CA, and Department of Anesthesiology, Charles Drew
University of Medicine and Science, Los Angeles, CA, USA
Robert A. Gunther
Department of Surgery, University of California,
Davis School of Medicine, Sacramento, CA, USA
Abstract: Allogeneic blood resuscitation is the treatment of
choice for hemor-rhagic shock. When blood is unavailable, plasma
expanders, including crystal-
loids, colloids, and blood substitutes, may be used. Another
treatment modality
is vasopressin, a vasoconstrictor administered to redistribute
blood flow, increase
venous return, and maintain adequate cardiac output. While much
information
exists on systemic function and oxygenation characteristics
following treatment
with these resuscitants, data on their effects on the
microcirculation and corre-
lation of real-time microvascular changes with changes in
systemic function
and oxygenation in the same animal are lacking. In this study,
real-time microvas-
cular changes during hemorrhagic shock treatment were correlated
with systemic
function and oxygenation changes in a canine hemorrhagic shock
model (5055%
total blood loss with a MAP of 4550 mmHg as a clinical
criterion). Following
splenectomy and hemorrhage, the dogs were assigned to five
resuscitation groups:
autologous=shed blood, hemoglobin-based oxygen
carrier=Oxyglobin1, crystalloid=saline, colloid=Hespan1 (6%
hetastarch), and vasopressin. Systemic functionand oxygenation
changes were continuously monitored and periodically mea-
sured (during various phases of the study) using standard
operating room proto-
cols. Computer-assisted intravital video-microscopy was used to
objectively
analyze and quantify real-time microvascular changes (diameter,
red-cell velocity)
in the conjunctival microcirculation. Measurements were made
during pre-hemor-
rhagic (baseline), post-hemorrhagic (pre-resuscitation), and
post-resuscitation
phases of the study. Pre-hemorrhagic microvascular variables
were similar in all
dogs (venular diameter 42 4 mm, red-cell velocity 0.55 0.5
mm=sec). Alldogs showed significant (P< 0.05) post-hemorrhagic
microvascular changes:20% decrease in venular diameter and 30%
increase in red-cell velocity,
indicative of sympathetic effects arising from substantial blood
loss. Microvascu-
lar changes correlated with post-hemorrhagic systemic function
and oxygenation
changes. All resuscitation modalities except vasopressin
restored microvascularand systemic function changes close to
pre-hemorrhagic values. However,
only autologous blood restored oxygenation changes to
pre-hemorrhagic levels
174 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
3/19
an important role in pre-hospital=en route treatment for
hemorrhagic shock.Vasopressin treatment resulted in inadvertent
detrimental outcome without the
intended benefit.
Keywords: Blood substitutes; Hemorrhagic shock; Oxygenation;
Real-timemicrocirculation; Systemic function
INTRODUCTION
Hemorrhagic shock, when not properly managed or treated in a
timelymanner, can lead to irreversible damage and fatality.
Therefore, appropriatemanagement and treatment of hemorrhagic shock
are crucial modalities thatcan serve to prevent deleterious
outcomes. Pre-hospitalen routetreat-ment, which on the average is
conducted within 12 hours after blood loss,normally consists of
resuscitations using non-oxygen carrying plasma expan-ders
(crystalloid or colloid solution) or catecholamines, including
epineph-rine and norepinephrine [15]. These treatments are designed
to increasecardiac output so as to maintain mean arterial pressure
(MAP), by redistri-buting blood flow and increasing venous return,
until arrival at the hospitalfor allogeneic blood resuscitation or
other definitive intervention.
In the past few years, hemoglobin-based oxygen carriers
(HBOC)have been used as resuscitants in experimental trials to
treat hemorrhagicshock [1,68]. The HBOC were designed to be very
similar to allogeneicblood in oxygen-carrying and hemodynamic
properties, with the intentthat they could serve literally as
oxygen-carrying blood substitutes. Afew HBOC have been tested in
animal models and are now in clinicaltrials in South Africa and
Europe. One of the HBOC, Oxyglobin1, hasbeen approved by the Food
and Drug Administration (FDA) for canine
use in the United States.Recently, it has been suggested that
treatment using vasopressinthe
most potent naturally occurring vasoconstrictor knowncould
ade-quately and alternatively serve to redistribute blood flow and,
therefore,may be a more effective treatment modality than
conventional plasmaexpanders or catecholamines [35,9]. Clinical
reports have indicated thatin cases where fluid (plasma expander)
or catecholamine resuscitationswere futile, alternative treatment
with vasopressin led to successful out-comes [1012]. Several animal
studies have shown that vasopressin treat-
ment provided hemodynamic stabilization (monitored via MAP)
duringthe pre-hospital phase of shock studies, while fluid- or
catecholamine-
Comparison of Treatment Modalities 175
-
8/13/2019 artif cell 24515305
4/19
critical pre-hospital phase of hemorrhagic shock treatment by
redistribut-ing blood flow to improve cardiac output and maintain
MAP.
HBOC and vasopressin resuscitations, therefore, are
modalitiesthat have great potential to manage and treat hemorrhagic
shock in apre-hospital setting, in addition to the availability of
crystalloid(s) and col-loid(s), which have been used for decades,
albeit with variable outcomes.
The goal of this study was to compare the different treatment
modal-ities available for pre-hospital use, including an
oxygen-carrying blood sub-stitute=HBOC (Oxyglobin1), a
non-oxygen-carrying crystalloid (saline), anon-oxygen-carrying
colloid (Hespan1), and a potent vasoconstrictor(vasopressin), using
autologous=shed bloodthe gold standard for thetreatment of
hemorrhagic shockas positive control. The experimentalprotocol was
designed to longitudinally and simultaneously measure sys-temic
functions, oxygenation characteristics, and microvascular
activitiesin pre-hemorrhagic (baseline), post-hemorrhagic
(pre-resuscitation) andpost-resuscitation phases of the study for
data correlation (in the sameanimal), efficacy comparison, and
critical outcome evaluation.
MATERIALS AND METHODS
Animals
Fifteen dogs (healthy adult, male or female, 3035 kg) were
studied in a12-month period. They were prepared, instrumented,
splenectomized,hemorrhaged (to attain a MAP of 4550 mmHg as a
clinical criterion;equivalent to 5055% blood loss), and
resuscitated as performed inpreviously reported studies [1315]. The
dogs were randomly assigned tofive resuscitation groups
(autologous=shed blood, n3; Oxyglobin1,
n3; saline, n3; Hespan1, n3; vasopressin, n3) as briefly
describedin Methods. A schematic flow-chart of the study is shown
in Figure 1.
Resuscitants
Autologous=shed blood was anti-coagulated blood from the same
dogcollected during hemorrhaging for use as positive resuscitation
control.
Oxyglobin1 (Hemoglobin Glutamer-200 [Bovine]; Biopure
Corpor-
ation, Cambridge, MA) was an oxygen-carrying blood substitute
thathas been approved by the FDA for canine use in the United
States.
176 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
5/19
Hespan1 (6% hetastarch; Abbott Laboratories, Chicago, IL) was
anon-oxygen-carrying colloid solution that has been commonly used
asa plasma expander.
Arginine Vasopressin (Vasopressin injection USP; AVP;
AmericanRegent Laboratories, Shirley, NY) was a potent
vasoconstrictor com-monly used in the hospital with the intent to
redistribute blood flow.
Animal Preparation and Instrumentation
A total of 15 healthy, adult mongrel dogs were used within a
12-monthperiod. Approval (Animal Welfare Assurance #A-343301) by
the Uni-versity of California, Davis Animal Care and Use Committee
wasobtained for this study. The experimental protocol used in this
studywas in compliance with the Guide for the Care of Laboratory
Animals
(National Institutes of Health Publication #8623, revised
1985).Each dog was premedicated with IM oxymorphone (0.02 mg=kg)
and
Figure 1. Schematic flow-chart of the study.
Comparison of Treatment Modalities 177
-
8/13/2019 artif cell 24515305
6/19
instrumentation period and during the administration of drugs.
Anesthe-sia was induced with IV propofol (24 mg=kg) and diazepam
(0.5 mg=kg),followed by orotracheal intubation. Anesthesia was
maintained followinga balanced protocol, using isoflurane and
fentanyl to minimize potentialconfounding hemodynamic effects
[16,17]. During animal preparationand instrumentation, isoflurane
in oxygen was delivered at an end-tidalconcentration of 0.81.2%,
and fentanyl infused at a rate of 0.7 mg=kg=minfollowing an initial
bolus of fentanyl (10 mg=kg). The dog was mechani-cally ventilated
with an anesthesia ventilator (Model 2000; HallowellEMC,
Pittsfield, MA) using tidal volumes (VT) of 1520 mL=kg and a
res-piratory rate of 912 breaths per minute to ensure an arterial
partial pres-sure of carbon dioxide (PaCO2) in the range of 3545
torr (4.66.0 kPa).End-tidal partial pressure of CO2 (PETCO2),
end-tidal concentration ofisoflurane (ISOET), and inspired O2
concentration (FiO2) were continu-ously monitored using a Datex
airway gas monitor (Datex 254; Helsinki,Finland).
Each dog was instrumented initially in dorsal recumbency and
thenplaced on its side. Further monitoring included continuous
recordingof the electrocardiogram (ECG; Monitor Model 78353B,
Hewlett Pack-ard, Andover, MA) and arterial O2saturation (SaO2;
Model N-180 pulseoximeter, Nellcor Inc., Hayward, CA). Further
instrumentation includedplacement of catheters into the dogs
femoral artery for arterial bloodwithdrawal, and determinations of
systemic arterial pressures using mem-brane transducers (Model
1290A, Hewlett Packard, Watham, MA). An8-fr balloon-tipped
flow-directed thermodilution pulmonary arterialcatheter (OptiQ2,
Abbott Laboratories, Chicago, IL) was also insertedvia the jugular
vein and floated into the pulmonary artery under directmonitoring
of pressure traces for measurements of central venous pres-sure
(CVP), pulmonary occlusion pressure (POP), mean arterial
pressure
(MAP), systolic arterial pressure (SAP), diastolic arterial
pressure (DAP),mean pulmonary arterial pressure (MPAP), core body
temperature andcardiac output (CO). The pulmonary arterial catheter
was connected to acardiac output computer (Critical Care System
QVUE, Oximetrix 3,Abbott Laboratories, Chicago, IL) for continuous
CO monitoring.Cardiac output was also assessed by thermodilution in
triplicate using10 mL of saline at room temperature. Body
temperature was maintainedbetween 3839C by means of a heating pad
and circulating warm airblanket (Bair Hugger1 Model 505, Augustine
Medical Inc., Eden, MN).
After preparation and instrumentation, the dog was
splenectomizedfollowing a midline laparotomy to prevent release of
sequestered blood
178 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
7/19
Measurement of Systemic Variables
A bioengineering station, which was designed to monitor and
studyhemorrhagic shock and treatment modalities in large animals in
an oper-ation room setting, was established for this study in our
laboratory at UCDavis. The bioengineering station was capable of
measuring numeroussystemic function and oxygenation variables. Of
interest to this study,the measured variables included ECG, MAP,
SAP, DAP, MPAP, POP,CVP, heart rate (HR), stroke volume index
(SVI), and CO. Arterialand mixed-venous heparinized blood samples
were collected intermit-tently (whenever appropriate) from the
femoral artery and the rightatrium, respectively. Immediately after
collection, blood samples weresealed and stored on ice.
Subsequently, arterial and mixed-venous totalhemoglobin (aHbtotal;
vHbtotal), arterial plasma hemoglobin (aHbplasma)and methemoglobin
(Met-Hb) concentrations, and arterial and mixed-venous O2
saturation (SaO2; SvO2) were measured, using a co-oximeter(Model
482, Instrumentation Laboratories, Lexington, MA). Arterialand
mixed-venous O2 content (CaO2; CvO2) were directly measured
intriplicate, using an oxygen-specific electrode (LEXO2CON-K,
HospexFiberoptics, Chestnut Hill, MA). Mean tissue oxygenation
(MtO2) wasmeasured by an oxygen-measuring microprobe inserted
percutaneouslyinto the quadriceps femoris muscle of the thigh,
using the OxyFloTM=OxyLite2 microprobe technology (Oxford
Instruments; Oxford, UK).Arterial and mixed-venous lactate
(lactatea; lactatev) concentrations weredetermined in duplicate by
means of a lactate analyzer (Model 1500, YSIInc., Yellow Springs,
OH). Arterial and mixed-venous pH (pHa; pHv) andpartial pressures
of O2(PaO2; PvO2) and CO2(PaCO2; PvCO2) were ana-lyzed with a blood
gas analyzer (Rapidlab Model 248, Bayer CorporationDiagnostics
Division, Norwood, MA). Blood gas values were corrected
for the body temperature of the animal at the time of sampling.
Arterialand mixed venous standard base excesses (SBEa; SBEv) and
bicarbonatelevels (aHCO3; vHCO3) were computed by the blood gas
analyzer. Othervariables, including body surface area (BSA in m2),
systemic vascularresistance (SVR), etc., were calculated using
standard equations.
Computer-Assisted Intravital Microscope (CAIM)
The CAIM system was anchored along the front edge of the
operatingtable for non-invasive videotaping of the real-time
conjunctival microcir-
Comparison of Treatment Modalities 179
-
8/13/2019 artif cell 24515305
8/19
the bioengineering station, it has been substantially redesigned
and modi-fied to study the microcirculation in the bulbar
conjunctiva of the dog sothat real-time microvascular changes in
the conjunctival microcirculationcould be videotaped simultaneously
with the measurements of systemicfunctions and oxygenation in the
same animal for critical correlation(see Figure 2). CAIM was
macro-optic based and has an opticalmagnification of 4.5 and an
on-screen magnification of 125. The
180 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
9/19
optical magnification of CAIM was fixed because of its macro
design;this non-changeable magnification was important as it
assured that allmicrovascular measurements made in various phases
of the experimen-tation were quantified on the same basis without a
magnification vari-able. An anti-red (#58 Wratten green filter)
fiber-optic light sourcewas used to illuminate the conjunctival
microcirculation and to enhancevessel visualization. The angle and
level of the front element of CAIMwere adjusted to provide the
flattest possible surface for focusing.A COHU video camera (Model
2622-100; 1/2-inch monochrome CCD-format, San Diego, CA) was used
to non-invasively videotape the real-time conjunctival
microcirculation via a high-resolution video-recorder.Focus of CAIM
was centered on the microcirculation in the bulbar con-
junctiva of the left eye of the dog. The microvascular
activities werevideotaped and subsequently analyzed via
computer-assisted imageanalysis for microvascular morphometry and
dynamics using in-housedeveloped imaging software VASCAN and VASVEL
[1315,1822].The imaging software can objectively quantify over 20
parameters ofmicrovascular characteristics. However, only venular
diameter (morpho-metric) and red-cell velocity (dynamic)
characteristics, which we considerrelevant based on previous
investigations, were objectively quantified andreported in this
study [1315]. Most conjunctival vessels have uniqueshapes and forms
and were easily recognizable. In this study, the vesselsof interest
were identified and relocated for time-dependent videotaping.During
various phases of the experimentation, the same vessels were
relo-cated and restudied so that relevant measurements (e.g.,
vessel diameterand red-cell velocity) were made for longitudinal
comparison, with eachvessel serving as its own reference control
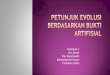
(see Figures 3 and 4).
Figure 3. A series of three images showing the same location in
the conjunctival
microcirculation of a dog during pre-hemorrhagic (basline),
post-hemorrhagicand post-resuscitation phases of the experiment in
the autologous=shed bloodstudy Because of the unique shape and form
of the vessels under observation
Comparison of Treatment Modalities 181
-
8/13/2019 artif cell 24515305
10/19
Canine Hemorrhagic Shock Model
Each dog was allowed to stabilize after the splenectomy. The
amount ofsequestered blood in the spleen from each dog was measured
andincluded in the computation of total blood loss (5055%). At the
endof a 60-min stabilization period, pre-hemorrhagic (baseline)
measure-ments on systemic function and oxygenation were made
(pre-hemorrha-gic phase). In addition, videotape sequences were
made via CAIM onthe conjunctival microcirculation simultaneously.
Immediately after thebaseline measurements were made, 5055% of the
blood volume ofthe dog (based on body weight and the amount of
sequestered bloodin the spleen measured after splenectomy) was
withdrawn from the lateralsaphenous and femoral veinsat an overall
hemorrhage rate of 3236mL=kg=hruntil a MAP of 4550 mmHg was
achieved (normally45 min). The method of attaining a MAP of 4550
mmHg as a clinical
criterion was used to ensure the induction of acute but
non-lethalhypovolemia and hemorrhagic shock. Within the
post-hemorrhagic1-hr acclimatization period to induce hemorrhagic
shock, small amountsof blood were withdrawn if needed (whenever MAP
increased to over50 mmHg) to maintain a MAP of 50 mmHg (within a
4550 mmHgrange). Shed blood was collected, anticoagulated and used
in autologousblood resuscitation to serve as control. In similar
manner to pre-hemorrhagic (baseline) measurements, post-hemorrhagic
measurementsand videotape sequences were made (post-hemorrhagic
phase). At the
end of post-hemorrhagic measurements, the dogs were randomly
assignedto one of the five resuscitation groups: autologous=shed
blood (resusci-
Figure 4. A series of three images showing the same location in
the conjunctivalmicrocirculation of a dog during pre-hemorrhagic
(basline), post-hemorrhagicand post-resuscitation phases of the
experiment in the crystalloid=saline study.
Again, the same vessels were identified and relocated for
longitudinal evaluations.Magnification 125on-screen.
182 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
11/19
vasopressin (resuscitated at a loading bolus dose of 0.4 IU=kg
followedby 4.8 IU=kg=hr for one hour). Systemic function and
oxygenationmeasurements were again made at the completion of the
resuscitationprocess (post-resuscitation phase). Videotape
sequences were also madesimultaneously.
Statistics
All results were averaged and reported as mean SD. Analysis of
vari-ance, students t-test and post hoc Bonferroni corrections were
usedwhenever appropriate. A 0.05 significance level was used in
this study.P values smaller than 0.01 (e.g., P 0.000045 or P 5.793
104) werepresented as P
-
8/13/2019 artif cell 24515305
12/19
different extents and did not return to pre-hemorrhagic values,
withHespan1 being most effective and Oxyglobin1 being least
effective.
Shed blood resuscitation restored post-hemorrhagic
microvascularchanges to pre-hemorrhagic values. Oxyglobin1, saline,
and Hespan1
Figure 5. Post-hemorrhagic and post-resuscitation changes in
venular diametersinduced by the five resuscitation treatment
modalities.
184 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
13/19
resuscitations, similar to the effect of shed blood, also
restored post-hemorrhagic microvascular changes close to
pre-hemorrhagic values(see Figures 5 and 6). However, vasopressin
treatment resulted in furtherdecreases in venular diameter (50%) as
well as red-cell velocity (70%)(see Figures 57).
Shed blood resuscitation restored post-hemorrhagic
oxygenation(CaO2 and CvO2) changes to pre-hemorrhagic (baseline)
values. How-ever, Oxyglobin1, saline, Hespan1, and vasopressin
resuscitations did
Figure 7. A series of two images showing the same location in
the conjunctivalmicrocirculation of a dog during post-hemorrhagic
and post-resuscitation phasesof the experiment in the vasopressin
study. Again, the same vessels were identifiedand relocated for
longitudinal evaluations. Note the extensive
vasoconstrictionarising from the vasopressin infusion.
Magnification 125on-screen.
Comparison of Treatment Modalities 185
-
8/13/2019 artif cell 24515305
14/19
not have any effect in restoring these post-hemorrhagic
oxygenationchanges (see Figures 8 and 9). The unexpected result
that Oxyglobin1,an oxygen carrier, did not restore oxygenation
changes led to the sus-picion that standard blood sample based
oxygenation measurementsmay not adequately measure tissue
oxygenation levels. To investigate this
Figure 9. Post-hemorrhagic and post-resuscitation changes in
venous oxygencontent (CvO2).
186 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
15/19
possibility, the OxyfloTM=OxyliteTM microprobe technology was
used tomeasure tissue level oxygenation levels in the same animals.
The resultsconfirmed that, of all the resuscitants used in this
study, only shed bloodrestored oxygenation at the tissue level to
pre-hemorrhagic values. Inaddition, it was also shown that
vasopressin resuscitation led to a furtherdecrease in tissue
oxygenation (see Figure 10).
DISCUSSION
Allogeneic blood resuscitation is the treatment of choice for
hemorrhagicshock. However, in situations when blood is not
available (e.g., battle-field or rural area injury), crystalloids,
colloids, artificial blood substi-tutes, or vasoactive agents have
been used. The goal of this study wasto evaluate the efficacy of
these resuscitants in the pre-hospital treatmentof hemorrhagic
shock, with special emphasis on studying their effects onthe
microcirculation, the raison detre of the vasculature [1]. Few
studieshave focused on the real-time microcirculation in large
animals due to alack of relevant technologies and appropriate
non-invasive research sites.In addition, rarely have real-time
microvascular changes been simul-taneously studied and correlated
with systemic function and oxygenationchanges in the same animal.
The availability of CAIM provided a meansfor non-invasive
evaluation of the effects of different resuscitants on thereal-time
microcirculation. In addition, the large size of the dog allowedfor
extensive measurements of systemic function, blood chemistry,
andoxygenation changes to correlate with changes in microvascular
para-meters. This study represents the first of its kind in which
systemic func-tions, oxygenation, blood chemistry, and
microvascular characteristicswere measured in the same animal
simultaneously. In addition, the results
can serve as a benchmark for testing treatment modalities for
hemorrha-gic shock, and in the future development of artificial
blood substitutes.
In order to adequately evaluate the efficacy of different
resuscitants,a suitable hemorrhagic shock model (substantially
modified from theWiggers model [23]) was adapted in our laboratory
in which the dogswere maintained for a 1-hr acclimatization period
following hemorrha-ging to ensure the development of hemorrhagic
shock for this study. Thismodel may serve as a testing platform for
future hemorrhagic shock andresuscitation studies.
In this study, only shed blood resuscitation restored
post-hemorrhagicsystemic function and oxygenation changes to
pre-hemorrhagic levels.
Comparison of Treatment Modalities 187
-
8/13/2019 artif cell 24515305
16/19
at a rate of 30mL=kg=hr. However, Oxyglobin1 was administered at
aslower rate (10 mL=kg=hr) as recommended by the manufacturer to
pre-vent excessive circulatory hemoglobin overload. This
significantly slowerrate of administration, which replenished less
blood volume comparedwith the standard protocol, may account for
the failure of Oxyglobin1
to restore CO and HR to baseline values. While it was expected
that saline,Hespan1, and vasopressin resuscitations would not
restore oxygenationcharacteristics due to their non-oxygen carrying
capability, it was surpris-ing that oxygen-carrying Oxyglobin1 did
not restore oxygenation (CaO2and CvO2) characteristics. To address
the possibility that blood-samplebased measurements of oxygenation
characteristics may not be reflectiveof tissue level oxygenation,
the OxyFloTM=OxyLiteTM microprobe tech-nology was used to obtain
measurements of oxygenation at the tissue level.The results
indicated that only shed blood resuscitation restored
tissueoxygenation to pre-hemorrhagic values and that, indeed, the
oxygen-carrying Oxyglobin1 was not effective in improving blood
oxygenation.In addition, it was also convincingly shown that
vasopressin treatmentresulted in a further decrease in tissue
oxygenation (see Figure 10).
In this longitudinal study when efficacy studies were made to
mimicpre-hospital treatment of hemorrhagic shock, autologous=shed
blood,Oxyglobin1, crystalloid (saline), and colloid (Hespan1)
resuscitations wereeffective in restoring MAP from a
post-hemorrhagic value of 4550 mmHgto a close-to-baseline
(pre-hemorrhagic) level of 95100 mmHg immedi-ately after completion
of resuscitation. However, follow-up studies toevaluate the effects
of these resuscitants 34 hrs after resuscitation areneeded to show
their long-term efficacies in the treatment of
hemorrhagicshock.
Vasopressin treatment, instead of achieving the intended goal
ofredistributing blood flow to improve CO and maintain MAP,
resulted
in detrimental effects, including extensive peripheral
vasoconstriction,which led to a cessation of blood flow,
significant reduction in red-cellvelocity, significant
disappearance of capillaries and arterioles, andsignificant
decreases in tissue oxygenation. These results indicate
thatvasopressin may not be an appropriate choice as a resuscitant
for thetreatment of hemorrhagic shock.
REFERENCES
1. Intaglietta, M. (1999). Microcirculatory basis for the design
of artificial blood.Microcir 6: 247258
188 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
17/19
3. Voelckel, W.G., Lurie, K.G., Lindner, K.H., Zielinski, T.,
McKnite, S.,Krismer, A.C., Wenzel, V. (2000). Vaspressin improves
survival after cardiac
arrest in hypovolemic shock. Anesth. Analges. 91: 627634.4.
Raedler, C., Voelckel, W.G., Wenzel V., Krismer, A.C.,
Schmittinger, C.A.,
Herff, H., Mayr, V.D., Stadlbauer, K.H., Lindner, K.H.,
Konigsrainer, A.(2004). Treatment of uncontrolled hemorrhagic shock
after liver trauma:fatal effects of fluid resuscitation versus
improved outcome after vasopressin.Anesth. Analges. 98:
17591766.
5. Stadlbauer, K.H., Wagner-Berger, H.G., Wenzel, V., Voelckel,
W.G.,Krismer, A.C., Klima, G., Rheinberger, K., Pehlaner, S., Mayr,
V.D.,Lindner, K.H. (2003). Survival with full neurologic recovery
after prolongedcardiopulmonary resuscitation with a combination of
vasopressin andepinephrine in pigs. Anesth. Analges. 96:
17431749.
6. Klein, H.G. (1995). Oxygen carriers and transfusion
medicine.Art. Cell BloodSubstit. Immobil. Biotech. 22: 123135.
7. Klein, H.G. (2000). The prospects of red-cell substitutes
(Editorial).N. Engl.J. Med. 342: 838843.
8. Tsai, A.G. (2001). Influence of cell-free Hb on local tissue
perfusion andoxygenation in acute anemia after isovolemic
hemodilution. Transfus. Med.41: 12901298.
9. Voelckel, W.G., Raedler, C., Wenzel, V., Lindner, K.H.,
Krismer, A.C.,Schmittinger, C.A., Herff, H., Rheinberger, K.,
Konigsrainer, A. (2003).Arginine vasopressin, but not epinephrine,
improves survival in uncon-trolled hemorrhagic shock after liver
trauma in pigs. Crit. Care Med. 31:12861287.
10. Haas, T., Voelckel, W.G., Wiedermann, F., Wenzel, V.,
Lindner, K.H.(2004). Successful resuscitation of a traumatic
cardiac victim in hemorrhagicshock with vasopressin: a case report
and brief review of the literature.Trauma57: 177179.
11. Forrest, P. (2001). Vasopressin and shock.Anaesth. Intensive
Care19: 463472.12. Morales, D., Madigan, J., Cullinane S., Chen,
J., Heath, M., Oz, M., Oliver,
J.A., Landry, D.W. (1999). Reversal by vasopressin of
intractable hypoten-sion in the late phase of hemorrhagic shock.
Circ. 100: 226229.13. Cheung, A.T.W., Jahr, J.S., Driessen, B.,
Duong, P.L., Chan, M.S., Lurie, F.,
Golkaryeh, M.S., Kullar, R.K., Gunther, R.A. (2001). The effects
ofhemoglobin-based oxygen-carrier Hemoglobin glutamer-200 (bovine)
on themicrocirculation in a canine hypovolemia model: a noninvasive
computer-assisted intravital microscopy study. Anesth. Analges. 93:
832838.
14. Cheung, A.T.W., Driessen, B., Jahr, J.S., Duong, P.L.,
Ramanujam, S.,Chen, P.C.Y., Gunther, R.A. (2004). Blood substitute
resuscitation as a treat-ment modality for moderate hypovolemia.
Art. Cell Blood Substit. Biotech.
32: 189207.15. Cheung, A.T.W., Duong, P.L., Driessen, B., Chen,
P.C.Y., Jahr, J.S.,
Gunther R A (2006) Systemic function oxygenation and
microvascular
Comparison of Treatment Modalities 189
-
8/13/2019 artif cell 24515305
18/19
16. Ilkiw, J.E. (1999). Balanced anesthetic techniques in dogs
and cats. Clin.Techniq. in Small Animal Prac. 114: 2733.
17. Lemmens, H.J.M. (1995). Pharmacokinetik-pharmacodynamic
relationshipsfor opioids in balanced anesthesia. Clin. Pharmacol.
29: 231242.
18. Cheung, A.T.W., Perez R.V., Chen, P.C.Y. (1999). Improvement
in diabeticmicroangiopathy after successful simultaneous
pancreas-kidney transplan-tation: a computer-assisted intravital
microscopy study on the conjunctivalmicrocirculation. Transpl. 68:
927932.
19. Cheung, A.T.W., Ramanujam, S., Greer, D.A., Kumagai, L.,
Aoki, T.T.(2001). Microvascular complications in the bulbar
conjunctiva of type 2diabetes mellitus (T2DM) patients.Endocrine
Prac. 7: 358363.
20. Cheung, A.T.W., Harmatz, P., Wun, T., Chen, P.C.Y., Larkin,
E.C.,Adams, R.J., Vinchinsky, E.P. (2001). Correlation of abnormal
intracranialvessel velocity (measured by transcranial Doppler
ultrasonography) withabnormal conjunctival vessel velocity
(measured by computer-assisted intra-vital microscopy) in sickle
cell disease. Blood 97: 34013404.
21. Cheung, A.T.W., Price, A.R., Duong, P.L., Ramanujam, S.,Gut,
J.,Larkin, E.C.,Chen, P.C.Y., Wilson, D.M. (2002). Microvascular
abnormalities in pediatricdiabetic patients.Microvas. Res.63:
252258.
22. Cheung, A.T.W., Chen, P.C.Y., Larkin, E.C., Duong, P.L.,
Ramanujam, S.,Tablin, F., Wun, T. (2002). Microvascular
abnormalities in sickle cell disease:a computer-assisted intravital
microscopy study.Blood99: 39994005.
23. Wiggers, H.C., Ingram, R.C., Dille, J. (1945).
Hemorrhagic-hypotensionshock in locally anesthetized dogs. Am. J.
Physiol. 143:126133.
190 A. T. W. Cheung et al.
-
8/13/2019 artif cell 24515305
19/19