Embed Size (px)
Citation preview

Journal de Mycologie Médicale (2015) 25, 101—107
Available online at
ScienceDirectwww.sciencedirect.com
ORIGINAL ARTICLE/ARTICLE ORIGINAL
Aspergillus species as emerging causative
agents of onychomycosis Aspergillus spp. agents emergents responsables d’onychomycoseS. Nouripour-Sisakht a, H. Mirhendi a,*, M.R. Shidfar a,B. Ahmadi a, A. Rezaei-Matehkolaei b, M. Geramishoar a,F. Zarei a, N. Jalalizand a
aDepartment of Medical Parasitology and Mycology, School of Public Health, National Institute of HealthResearch, Tehran University of Medical Sciences, Tehran, IranbDepartment of Medical Mycology, School of Medicine, Infectious and Tropical Diseases Research Center,Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Received 2 November 2014; received in revised form 19 December 2014; accepted 30 December 2014Available online 2 February 2015
KEYWORDSAspergillus;Aspergillus flavus;Onychomycosis
* Corresponding author.E-mail address: [email protected]
http://dx.doi.org/10.1016/j.mycmed.1156-5233/# 2015 Elsevier Masson SA
SummaryBackground. — Onychomycosis is a common nail infection caused by dermatophytes, non-dermatophyte molds (NDM), and yeasts. Aspergillus species are emerging as increasing causesof toenail onychomycosis. The purpose of this study was species delineation of Aspergillus spp.isolated from patients with onychomycosis.Methods. — During a period of one year (2012—2013), nail samples were collected from patientsclinically suspected of onychomycosis and subjected to microscopic examination and culture.Species identification was performed based on macro- and micro-morphology of colonies. Forprecise species identification, PCR-amplification and sequencing of the beta-tubulin genefollowed by BLAST queries were performed where required.Results. — A total of 463/2,292 (20.2%) tested nails were diagnosed with onychomycosis. Amongthe positive specimens, 154 cases (33.2%) were identified as saprophytic NDM onychomycosis,135 (29.2%) of which were attributable to Aspergillus. Aspergillus species isolated from theinfected nails included Aspergillus flavus (77.3%, n = 119), Aspergillus niger (n = 4), Aspergillustubingensis (n = 4), Aspergillus terreus (n = 3), Aspergillus sydowii (n = 2), Aspergillus spp.(n = 2), and Aspergillus candidus (n = 1). Among the patients diagnosed with onychomycosisdue to Aspergillus (average patient age, 47.4 years), 40 had fingernail and 95 toenail involve-ment. The large toenails were most commonly affected.
.ir (H. Mirhendi).
2014.12.001S. All rights reserved.

102 S. Nouripour-Sisakht et al.
Conclusions. — This study identified a markedly high occurrence of A. flavus, and this fungusappears to be an emerging cause of saprophytic onychomycosis in Iran. The study moreoverhighlights the necessity of differentiating between dermatophytic and non-dermatophytic nailinfections for informed decisions on appropriate therapy.# 2015 Elsevier Masson SAS. All rights reserved.
MOTS CLÉSAspergillus ;Aspergillus flavus ;Onychomycose
Resume
Contexte. — L’onychomycose est une infection commune de l’ongle causée par des dermato-phytes, des moisissures non-dermatophytes (NDM), et des levures. Des espèces d’Aspergillusdeviennent la cause de plus en plus fréquente d’onychomycose. Le but de cette étude était lacaractérisation des espèces d’Aspergillus isolées chez des patients avec onychomycose.Methodes. — Pendant une période d’un an (2012—2013), les échantillons d’ongles ont étéprélevés chez des patients cliniquement suspects d’onychomycose et soumis à un examenmicroscopique et culture. L’identification des espèces a été effectuée par l’examen macro- etmicroscopique des colonies. Pour l’identification précise de l’espèce, l’amplification par PCRet le séquençage du gène de la bêta-tubuline suivi d’une analyse de BLAST ont été effectuésle cas échéant.Resultats. — Un total de 463/2292 (20,2 %) ongles testés ont été diagnostiqués avec uneonychomycose. Parmi les échantillons positifs, 154 cas (33,2 %) ont été identifiés commeonychomycose à saprophytes NDM, 135 (29,2 %) étaient attribuables à Aspergillus. Les espècesd’Aspergillus isolées des ongles infectés étaient les suivantes: Aspergillus flavus (77,3 %,n = 119), Aspergillus niger (n = 4), Aspergillus tubingensis (n = 4), Aspergillus terreus (n = 3),Aspergillus sydowii (n = 2), Aspergillus spp. (n = 2), et Aspergillus candidus (n = 1). Parmi lespatients diagnostiqués avec l’onychomycose causée par Aspergillus (âge moyen des patients,47,4 années), 40 concernaient un ongle de doigt et 95 un ongle d’orteil. Les ongles d’orteil dupouce ont été plus souvent infectés.Conclusions. — Cette étude a identifié une prévalence nettement élevée d’Aspergillus flavus.Cette moisissure semble être une cause émergente d’onychomycose saprophyte en Iran. L’étudesouligne en outre la nécessité de différenciation entre les infections des ongles dermatophyteset non dermatophytes pour rendre possible un choix éclairé de traitement approprié.# 2015 Elsevier Masson SAS. Tous droits réservés.
Introduction
Aspergillus species are ubiquitous environmental moldsfrequently isolated from soil, air, water, and vegetation.They cause a wide range of diseases in humans, includinginvasive or allergic aspergillosis, aspergilloma, sinusitis,otomycosis, onychomycosis, and keratitis [4,29,31]. Ony-chomycosis is a common infection of the nail with worldwidedistribution caused by dermatophytes, yeasts, and somespecies of non-dermatophyte molds (NDM) [25,36]. It repre-sents 30% of superficial fungal infections and 50% of all naildisorders [28]. The incidence of onychomycosis due to non-dermatophyte (saprophytic) molds is increasing [11,33,37].Factors contributing to this increase are damage of thenail surface during nail grinding or manicuring, use of artifi-cial nails, advanced age, peripheral vascular diseases, dia-betes, smoking and regular swimming [22,28]. Saprophyticonychomycosis can be caused by various fungi, includingScopulariopsis brevicaulis, Aspergillus spp., Fusarium spp.,Acremonium spp., and Scytalidium spp. [6,7,10,16,18,28,37]. Some epidemiological studies indicate that Asper-gillus is an emerging cause of toenail onychomycosis, andafter Scopulariopsis it is the most common cause of non-dermatophyte mold onychomycosis [13]. Over the recentyears, onychomycosis caused by different Aspergillusspecies is increasing, evidenced by case reports and
epidemiological studies [2,25,26,39]. While identificationof unknown Aspergillus isolates would be important toclinicians for informed therapeutic decisions, prognosis,and epidemiological purposes [5], many closely relatedAspergillus species are identified using morphologicalcriteria only in diagnostic laboratories. Therefore, in thisstudy, our aims were to determine the prevalence of Asper-gillus species isolated from patients with mycotic nailinfections in Tehran, Iran, as well as to carry out precisemolecular species delineation of rare aspergilli. This studycould potentially herald the beginning of a suite of mole-cular epidemiological studies of superficial fungal naildiseases in Iran.
Materials and methods
Clinical samples
Over a period of one year (2012 to 2013), clinical specimens(nail scrapings) were collected from patients referred totwo medical mycology laboratories in Tehran. The sampleswere taken from deep cuttings of the affected nail alongthe part bordering the healthy part of the nail. One partof each collected nail fragment was examined by potassiumhydroxide (KOH 20%) preparation for the presence of fungal

Table 2 Frequency of non-dermatophyte molds identifiedas the causative agents of onychomycosis in this study.Frequence des moisissures non-dermatophytes identifieescomme agents responsables d’onychomycose.
Non-dermatophyte mold species Number (%)
A. flavus 119 (77.3)A. niger 4 (2.6)A. tubingensis 4 (2.6)A. terreus 3 (2)A. sydowii 2 (1.3)A. candidus 1 (0.7)Aspergillus spp. 2 (1.3)Fusarium spp. 9 (5.8)Cladosporium spp. 2 (1.3)Scopulariopsis 4 (2.6)Penicillium 2 (1.3)Chrysosporium 1 (0.7)Trichoderma 1 (0.7)
Total 154 (100)
[(Figure_1)TD$FIG]
Onychomycosis due to Aspergillus 103
elements, and another part was cultured onto Sabourauddextrose agar (Difco, Detroit, MI, USA) with chloramphenicolby inoculation of three nail fragments onto the agar plate andincubation for up to four weeks at 25—28 8C. Diagnosis ofNDM Aspergillus onychomycosis was made based on dystro-phic nail appearance, microscopy-confirmed presence offungal elements characteristic of saprophytes in KOH pre-parations, lack of dermatophyte or yeast colonies in culture,and growth of identical Aspergillus colonies in all triplicateculture inoculums. Samples having characteristic saprophy-tic hyphal elements observed by direct microscopy andsignificant growth of Aspergillus in culture were consideredfor species identification based on macro-/microscopic cri-teria of colonies including slide cultures.
PCR identification of Aspergillus species: For moleculartests, about 10—20 cubic millimeters of the fresh colonieswere added to 200 mL distilled water in a 1.5 mL tube. Twohundred microliters of glass beads (0.5 millimeter in dia-meter) were added, shaked or vortexed rigorously forabout 5 min, centrifuged at 8000 rpm for 1 min, afterwhich 200 mL of the supernatant was submitted to DNAextraction by a commercial kit (GeneAll, Korea) accordingto the instructions of the manufacturer. A 1-mL aliquot oftemplate DNA, 0.4 mM of each forward Bt2a (50-GGT AACCAA ATC GGT GCT GCT TTC-30) and reverse Bt2b (50-ACCCTC AGT GTA GTG ACC CTT GGC-30) primer [14], 12.5 mL ofpremix (Amplicon, Denmark), and enough water to pro-duce a final volume of a 25 mL were used for PCR amplifi-cation of the beta tubulin gene, using the following PCRconditions: Initial denaturation for 5 min at 94 8C, follo-wed by 35 cycles of amplification, consisting of denatura-tion for 30 sec at 94 8C, annealing for 30 sec at 58 8C, andextension for 1 min at 72 8C, followed by an ultimateextension step at 72 8C for 10 min. PCR products wereelectrophoresed on a 1.2% agarose gel containing0.5 mg/mL ethidium bromide for about one hour in TBE(Tris 0.09 M, Boric acid 0.09 M, EDTA 2 mM) buffer. PCRproducts were purified using a purification kit (Bioneer,Korea) and sequenced bidirectionally using the forwardand reverse primers employed in the PCR. Each sequencechromatogram was analyzed and confirmed manually,using the Geneious software (http://www.geneious.com). Final species delineation was based on comparisonof the sequences with relevant reference sequence inGenBank, using the BLASTn algorithm (http://blast.ncbi.nlm.nih.gov/Blast) and/or considering the micro/macro-morphology of the cultures.
Table 1 Frequency distribution of onychomycosis by cau-sative agent and infection location.Distribution de frequence de l’onychomycose par agentcausal et localisation de l’infection.
Fungi Yeasts Dermatophytes NDM Total
Fingernail 154 12 45 211Toenail 23 120 109 252Total
(percent)177(38.2%)
132(28.5%)
154(33.2%)
463(100%)
NDM: non-dermatophyte mold.
Results
Among the 2292 nail samples, a total of 463 (20.2%) werediagnosed with onychomycosis. Details on clinical sites ofinfection and causative fungal agent are summarized inTable 1. Among the positive specimens, 154 (33.2%) caseswere identified as NDM onychomycosis. Direct microscopicexamination showed irregular saprophytic septate hyphaeassociated with single or grouped conidia in a few samples.Table 2 displays NDMs isolated from nails with onychomy-cosis in our study. The causative agents in 135/154cases of NDM onychomycosis (29.2% of the total number
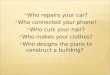
Figure 1 Agarose gel electrophoresis of amplified beta tubulingene from Aspergillus species isolated from nails infected withA. niger (lanes 1 and 2), A. tubingensis (lane 3), A. flavus (lanes 4and 5), A. terreus (lane 6), A. candidus (lane 7), and A. sydowii(lane 8). Lane M represents a 100 bp molecular size marker.L’electrophorese en gel d’agarose du gene de la tubuline beta,amplifie a partir de l’espece Aspergillus isolee a partir d’onglesinfectes par A. niger (pistes 1 et 2), A. tubingensis (piste 3), A.flavus (pistes 4 et 5), A. terreus (piste 6), A. candidus (piste 7),et A. sydowii (piste 8). Piste M represente un marqueur detaille moleculaire : 100pb, et la piste NC represente le controlenegatif.

104 S. Nouripour-Sisakht et al.
of onychomycosis cases) were diagnosed as Aspergillus spp.Among these, only four cases had a negative direct smear;however, because of dystrophic nail features and growth ofidentical Aspergillus in all triplicate culture inoculums,these four cases were considered as onychomycosis. A totalof 35 Aspergillus isolates, including 15 non-flavus species,were subjected to sequence analysis of the beta tubulingene, the most commonly used target for molecular speciesidentification of Aspergillus. Amplification of the betatubulin gene by the primer set Bt2a/Bt2b yielded singlebands of approximately 550 bp on agarose gel electropho-resis (Fig. 1). The most common Aspergillus species isolatedfrom NDM onychomycosis was Aspergillus flavus (77.3%,n = 119), followed in prevalence by A. niger (2.6%, n = 4),Aspergillus tubingensis (2.6%, n = 4), Aspergillus terreus(2%, n = 3), Aspergillus sydowii (1.3%, n = 2), Aspergilluscandidus (0.7%, n = 1), and Aspergillus spp. (1.3%, n = 2).Examples of microscopic features characteristic of eachspecies of Aspergillus isolated in the study are shown inFig. 2. The number of Aspergillus isolates in fingernail and
[(Figure_2)TD$FIG]
Figure 2 Microscopic pictures of Aspergillus species isolated fromA. tubingensis. D and E. A. candidus (E: large vesicle; D: small vesicle)Images microscopiques des especes d’Aspergillus isolees a partir destubingensis. D et E. A. candidus (E : grande vesicule ; D : petite ve
toenail lesions were 40 (29.62%) and 95 (70.38%), respecti-vely. Two patients had a mixed infection of Candida andAspergillus (one patient had A. niger and the other hadA. flavus). The youngest patient was 19 years old, and theoldest was 87 years old — both of them with their toenailsaffected— and the overall mean patient age was 47.4 years.Various clinical forms of onychomycosis due to Aspergillusspecies, including distal subungual onychomycosis, lateralsubungual onychomycosis, distal and lateral subungual ony-chomycosis, and total dystrophic onychomycosis were seenand the examples are shown in Fig. 3.
Discussion
Recently we have experienced a high number of onychomy-cosis due to NDM — particularly Aspergillus species — in ourlaboratory. The occurrence of 135 cases of Aspergillus nailinfection in one year at the two medical mycology labora-tories in Tehran is remarkable, and together with previous
cases of onychomycosis in the study A: A. flavus. B. A. niger. C.. F and G. A. sydowii (F: diminutive conidial head). H. A. terreus.cas d’onychomycose dans l’etude. A. A. flavus. B. A. niger. C. A.sicule). F et G. A. sydowii (F : tete conidiale). H. A. terreus.

[(Figure_3)TD$FIG]
Figure 3 Examples of nails affected by different species of Aspergillus. A to F. A. flavus. G and H. A. niger. I. A. tubingensis. J.A. sydowii. K. A. candidus. L. A. terreus (A, B, E and L distal and lateral subungual onychomycosis, C, F, H and K lateral subungualonychomycosis, M distal subungual onychomycosis, and D and I total dystrophic onychomycosis).Exemples d’ongles infectes par differentes especes d’Aspergillus. A a F. A. flavus. G et H. A. niger. I. A. tubingensis. J. A. sydowii. K. A.candidus. L. A. terreus (A, B, E, et L : onychomycose sous-ungueale distolaterale ; C, F, H, et K : onychomycose sous-unguealelaterale ; M : onychomycose sous-ungueale distale ; D et I : onychomycose totale dystrophique).
Onychomycosis due to Aspergillus 105
studies on onychomycosis in Tehran and in some other partsof the country, our data suggest that Aspergillus spp., mainlyA. flavus, are somewhat commonly involved in NDM onycho-mycosis in Iran [8,10,18,27].
Unlike almost all studies performed in Iran, in our survey,the frequency of onychomycosis due to yeasts and NDMsexceeds the frequency of nail infections caused by derma-tophytes [18]. This high occurrence was similar to that ofScherer et al. who found a shift from dermatophytes tosaprophytes as agents of nail infections [33]. A number ofrisk factors may contribute to this situation, of which‘‘change of lifestyle’’ may be the most logical explanation,including improvement in the level of hygiene, aging commu-nities, and a decrease in the risk of contracting infectionssuch as tinea unguium. Concordant with this fact, the mostrecent epidemiological survey of dermatophytosis in Iranshowed a decrease in the frequency of nail infection bydermatophytes [1]. Instead, the phenomenon of aging ledto an increase in some disorders such as peripheral vasculardisease of nails, diabetes, repeated nail trauma, and immunefunction disorders, which are all noted to be risk factors of
nail infections by molds [6,23]. The high frequency of nailinfections due to A. flavus can be attributed to the fact thatthis species is the most frequent Aspergillus isolated fromthe environment in Iran [9] and this species is one of thecommon pathogenic fungi to humans [19].
Although our study is not a comprehensive epidemiologi-cal survey and we did not test all NDMs delivered to ourlaboratory, these random data demonstrate an increasingoccurrence of onychomycosis due to non-dermatophytesmolds, especially Aspergillus species. The prevalence ofNDMs isolated from nail infections in various parts of theworld range between 1.49 and 33.5% [6,28,29,38]. Accordingto the data in the present survey, the overall prevalence ofNDM onychomycosis is 33.2% with Aspergillus spp. being themost common cause of NDM onychomycosis. This result issimilar to those reported by Hilmioglupolat et al. [20],Hwang et al. [22], and Zaini et al. [37]; however, our resultsdiffer from those reported in some other studies, for exam-ple Bonifaz et al. [6] and Khosravi et al. [24], who reportedScopulariopsis brevicaulis and Tosti et al. [35] who reportedFusarium spp. as the principal etiologic agents. The most

106 S. Nouripour-Sisakht et al.
common species of Aspergillus identified in our study was A.flavus, which is different to what was reported by Ng et al.[29], Gupta et al. [15], and Shokohi et al. [34], who found A.niger, A. sydowii, and A. terreus to be the most commonagents, respectively. In the present investigation, A. fumi-gatus, the infamous cause of invasive Aspergillus worldwide,was not isolated from any of the patients, but in somestudies, this species was isolated from nail infections[3,13,29,37]. The Aspergillus species most frequently isola-ted from nail infections are Aspergillus fumigatus, Aspergil-lus tamarii, Aspergillus niger, and A. flavus [6], while byapplication of molecular techniques several rare Aspergillusspecies have been identified from nail infections, includingA. terreus, A. alliaceus, A. ochraceus, A. versicolor, A.sydowii, A. candidus, and A. nomius [13,39]. In the presentstudy, some uncommon Aspergillus species, including A.sydowii, A. tubingensis, and A. candidus, were isolatedand identified by beta tubulin sequencing. To our knowledge,onychomycosis due to A. tubingensis and A. sydowii are herereported from Iran for the first time.
Morphological features are insufficient for precise iden-tification of Aspergillus species. For example in SectionNigri, A. brasiliensis, A. acidus, A. awamori, A. niger, andA. tubingensis have similar morphological characteristics,and sequencing of a suitable DNA target is essential fordifferentiation of such closely related species [21,30,32],In our study, all black aspergilli were initially reported asA. niger based on morphology, but after sequence analysis ofbeta tubulin genes it was revealed that half of isolates werein fact A. tubingensis.
In this study, toenail onychomycosis represented 70.38%of all cases of Aspergillus onychomycosis, which is similar tothe results reported by Hilmioglupolat et al. (67%) [20] andGianni et al. (67%) [12], but lower than those reported byBonifaz et al. (96%) [6], Tosti et al. (89.7%) [35], Hwang et al.(84.7%) [22], and higher than the results by Zaini et al.(54.3%) [37] and Hashemi et al. (33.7%) [18]. Bonifazet al. reported that 50.0% of the onychomycosis patientshad predisposing factors such as peripheral vascular disease;however, our patients were not significantly associated withpredisposing disease or risk factor, except for being elderly[6] The presence of a black area in nails infected with A.niger is common [25]; likewise, onychomycosis due to A.niger and A. tubingensis were usually associated with blackpigmentation in affected nails investigated in the presentstudy (Fig. 3).
The drug choice for treatment of onychomycosis is asso-ciated with causative agent, the number of nail involved andthe risks and benefits of different treatments [17]. The invitro activity of terbinafine is more effective than itracona-zole against different Aspergillus species, however thera-peutic choices are very scarce [11].
In conclusion, accurate identification of Aspergillus spe-cies, which are increasing causes of onychomycosis, is neces-sary for clarifying the microbial and clinical epidemiologyaspects of various causative agents of nail infections. Asmorphological criteria are insufficient for identification ofuncommon Aspergillus species, molecular methods could bea suitable complementary approach to compensate for thislimitation. In this study, we report a high occurrence ofA. flavus as an emerging cause of saprophytic onychomycosisin Iran.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
Acknowledgements
This work was financially supported by Tehran University ofMedical Sciences (TUMS) Tehran, Iran, grant No. 92-01-27-21704.
References
[1] Abastabar M, et al. A molecular epidemiological survey ofclinically important dermatophytes in iran based on specificRFLP profiles of beta-tubulin gene. Iran J Public Health 2013;42:1049—57.
[2] Ahmadi B, et al. A case of onychomycosis caused by Aspergilluscandidus. Med Mycol Cas Rep 2011;1:45—8.
[3] Asadi MA, Dehghani R, Sharif MR. Epidemiologic study of ony-chomycosis and tinea pedis in Kashan, Iran. Jundishapur JMicrobiol 2007;2:61—4.
[4] Balajee S, et al. Aspergillus species identification in the clinicalsetting. Stud Mycol 2007;59:39—46.
[5] Balajee SA. Aspergillus terreus complex. Med Mycol 2009;47:S42—6.
[6] Bonifaz A, Cruz-Aguilar P, Ponce RM. Onychomycosis by molds.Report of 78 cases. Eur J Dermatol 2007;17:70—2.
[7] Bontems O, Hauser P, Monod M. Evaluation of a polymerasechain reaction-restriction fragment length polymorphism assayfor dermatophyte and nondermatophyte identification in ony-chomycosis. Br J Dermatol 2009;161:791—6.
[8] Chadeganipour M, Nilipour S, Ahmadi G. Study of onychomy-cosis in Isfahan, Iran. Mycoses 2010;53:153—7.
[9] Diba K, Mirhendi H, Kordbacheh P, Rezaie S. Development ofRFLP-PCR method for the identification of medically importantAspergillus species using single restriction enzyme MwoI. Braz JMicrobiol 2014;45:503—7.
[10] Falahati M, Ghasemi Z, Farideh Z, Assadi M, Ahmadi F. Iden-tification of the etiological agents of onychomycosis in Tehran(2011-2012). Life Sci J 2012;9:5469—72.
[11] Fernandez MS, Rojas FD, Cattana ME, Sosa M, Mangiaterra ML,Giusiano GE. Aspergillus terreus complex: an emergent oppor-tunistic agent of onychomycosis. Mycoses 2013;56:477—81.
[12] Gianni C, Cerri A, Crosti C. Non-dermatophytic onychomycosis.An understimated entity? A study of 51 cases Nicht-Dermato-phyten-Onychomykose: Eine unterschätzte Krankheit? Eine Stu-die von 51 Fällen. Mycoses 2000;43:29—33.
[13] Gianni C, Romano C. Clinical and histological aspects of toenailonychomycosis caused by Aspergillus spp.: 34 cases treatedwith weekly intermittent terbinafine. J Dermatol 2004;209:104—10.
[14] Glass NL, Donaldson GC. Development of primer sets designedfor use with the PCR to amplify conserved genes fromfilamentous ascomycetes. Appl Environ Microbiol 1995;61:1323—30.
[15] Gupta AK, Cooper EA, MacDonald P, Summerbell RC. Utility ofinoculum counting (Walshe and English criteria) in clinicaldiagnosis of onychomycosis caused by nondermatophyticfilamentous fungi. J Clin Microbiol 2001;39:2115—21.
[16] Gupta AK, Drummond-Main C, Cooper EA, Brintnell W, PiracciniBM, Tosti A. Systematic review of nondermatophyte moldonychomycosis: diagnosis, clinical types, epidemiology, andtreatment. J Am Acad Dermatol 2012;66:494—502.

Onychomycosis due to Aspergillus 107
[17] Gupta AK, Paquet M, Simpson FC. Therapies for the treatmentof onychomycosis. Clin Dermatol 2013;31:544—54.
[18] Hashemi S, Gerami M, Zibafar E, Daei M, Moazeni M, NasrollahiA. Onychomycosis in Tehran: mycological study of 504 patients.Mycoses 2010;53:251—5.
[19] Hedayati MT, Pasqualotto AC, Warn PA, Bowyer P, Denning DW.Aspergillus flavus: human pathogen, allergen and mycotoxinproducer. Microbiology 2007;153:1677—92.
[20] Hilmioglu-Polat S, Metin D, Inci R, Dereli T, K½l½nc I, Tümbay E.Non-dermatophytic molds as agents of onychomycosis in Izmir,Turkey— a prospective study. Mycopathologia 2005;160:125—8.
[21] Howard SJ, Harrison E, Bowyer P, Varga J, Denning DW. Crypticspecies and azole resistance in the Aspergillus niger complex.Antimicrob Agents Chemother 2011;55:4802—9.
[22] Hwang SM, Suh MK, Ha GY. Onychomycosis due to nonderma-tophytic molds. Ann Dermatol 2012;24:175—80.
[23] Kaur R, Kashyap B, Bhalla P. Onychomycosis-epidemiology,diagnosis and management. Indian J Med Microbiol 2008;26:108—16.
[24] Khosravi AR, Mansouri P. Onychomycosis in Tehran, Iran: pre-vailing fungi and treatment with itraconazole. Mycopathologia2001;150:9—13.
[25] Kim DM, Suh MK, Ha GY, Sohng SH. Fingernail onychomycosisdue to Aspergillus niger. Ann Dermatol 2012;24:459—63.
[26] Kristensen L, Stenderup J, Otkjaer A. Onychomycosis due toAspergillus tamarii in a 3-year-old boy. Acta Derm Venereol2005;85:261—2.
[27] Mikaeili A, Karimi I. The incidence of onychomycosis infectionamong patients referred to hospitals in Kermanshah Province,Western Iran. Iran J Public Health 2013;42:320—5.
[28] Moreno G, Arenas R. Other fungi causing onychomycosis. ClinDermatol 2010;28:160—3.
[29] Ng KP, Saw TL, Madasamy M, Soo Hoo T. Onychomycosis inMalaysia. Mycopathologia 1999;147:29—32.
[30] Perrone G, Stea G, Epifani F, Varga J, Frisvad JC, Samson RA.Aspergillus niger contains the cryptic phylogenetic speciesA. awamori. Fungal Biol 2011;115:1138—50.
[31] Pfaller MA, Diekema DJ. Epidemiology of invasive mycoses inNorth America. Crit Rev Microbiol 2010;36:1—53.
[32] Samson RA, Houbraken J, Kuijpers AF, Frank JM, Frisvad JC.New ochratoxin A or sclerotium producing species in Aspergillussection Nigri. Stud Mycol 2004;50:45—61.
[33] Scherer WP, McCreary JP, Hayes WW. The diagnosis of ony-chomycosis in a geriatric population. A study of 450 cases inSouth Florida. J Am Podiatr Med Assoc 2001;91:456—64.
[34] Shokohi T, Hajheidari Z, Haghani E, Khalilian A, Aghili S, Miahi S.The study of 101 cases of onychomycosis and associate factorsin patients referred to Boali Sina Hospital and Toba dermato-logy outpatient clinics in Sari. J Mazandaran Univ Med Sci2009;18:33—43.
[35] Tosti A, Piraccini BM, Lorenzi S. Onychomycosis caused by non-dermatophytic molds: clinical features and response to treat-ment of 59 cases. J Am Acad Dermatol 2000;42:217—24.
[36] Welsh O, Vera-Cabrera L, Welsh E. Onychomycosis. Clin Der-matol 2010;28:151—9.
[37] Zaini F, Mahmoudi M, Mehbod A, Kordbacheh P, Safara M.Fungal nail infections in Tehran, Iran. Iran J Public Health2009;38:46—53.
[38] Zomorodian K, Emami M, Tarazoei B, Saadat F. Study andidentification of the etiological agents of onychomycosis inTehran, capital of Iran. Iran J Public Health 2002;31:100—4.
[39] Zotti M, Machetti M, Persi A, Barabino G, dParodi A. Onycho-mycosis: first case due to Aspergillus nomius. Acta Derm Vene-reol 2011;91:591—2.