Embed Size (px)
Citation preview
Assessing Scheduled Support
of Medical Equipment
North Central Biomedical Association Seminar
September 5, 2008Tim Ritter Senior
Project Engineer.
Who is ECRI Institute?
Nonprofit, international health services research agency Seeking to promote the highest standards of safety, quality and
cost effectiveness in healthcare since 1968Resources include
Membership-based access to Web resources, databases, research reports, guides, directories
Consultation services and special projects Information used by
Hospitals, health systems, health plans, and insurers Government agencies, legal and regulatory professionals
©2008 ECRI Institute
Alternative Presentation Titles . . .
To PM or Not to PM . . .How Often is Enough?Recommendations or Requirements?
© 2008 ECRI.©2008 ECRI Institute

© 2008 ECRI.
How safe is “safe”?
©2008 ECRI Institute
In the Beginning . . .
Emergency Care Research Institute – 1968“1,200 US hospital electrocutions/yr” – 1969
5,000/yr according to Ralph Nader by 1971The electrical safety “scare” gives birth to clinical engineeringHealth Devices Volume 1 Number 1 addresses
the isolated power controversyMonthly inspections of defibrillatorsQuarterly inspections of monitors
© 2008 ECRI.©2008 ECRI Institute
In the Beginning . . .
Technology was not reliable and possibly dangerousVacuum tubesHigh leakage currentsMetal chassis with minimal fluid protectionAnalog metersHeated stylus recordersLousy batteriesReusable pressure transducers© 2008 ECRI.
©2008 ECRI Institute
© 2008 ECRI.
Over the Past 40 YearsTechnology has become more reliable
Better designed and frequently double insulated
Devices have self diagnostics and error/event logs
Significant failures rarely identified during inspections
The need for preventive maintenance is declining
ECRI Institute has no evidence of injury or death attributable to neglected inspection or preventive maintenance
©2008 ECRI Institute
© 2008 ECRI.
Initial Observations
Many “PM” programs are outdated ─ electrical safety and equipment risk levels are overemphasized
Manufacturer recommendations ─ the same for all units under all operating conditions
Risk managers and regulatory agencies frequently interpret those recommendations to be requirements
©2008 ECRI Institute
© 2008 ECRI.
Initial Observations
Equipment management is essentially risk management.
Nothing can be 100% safe or 100% reliable!
Inspect something today and it can fail tomorrow . . .
©2008 ECRI Institute
What is Scheduled Support?
Inspection – verification of performance and safetyPreventive maintenance – periodic procedures to minimize
risk of failure and to ensure continued proper operation “PM” is frequently used incorrectly to mean inspection
Scheduled support = inspection and/or preventive maintenance
Relatively few devices require true preventive maintenanceThe focus of this presentation: Scheduled Inspections
© 2008 ECRI.©2008 ECRI Institute
© 2008 ECRI.
What reasons are given for
performing scheduled support?
To reduce the risk of injury (to patients, staff, visitors)To reduce the risk of significant adverse impact on patient care
(e.g., due to downtime)To comply with codes, standards, and regulations
©2008 ECRI Institute
Initial Questions for Any Technology
Is there value in performing inspections?If so, do what? How often?How to determine, document and update the decision?Are manufacturer recommendations for performance
verifications justified?
© 2008 ECRI.©2008 ECRI Institute
What is Risk?
Risk
“ Combination of the probability of occurrence of harm and the severity of that harm.”
ANSI/AAMI/ISO 14971:2000
© 2008 ECRI.©2008 ECRI Institute

Assessing Equipment Risk
High-risk devices Medium-risk devices Low-risk devices
© 2008 ECRI.©2008 ECRI Institute
© 2008 ECRI.
High-risk devices
Life-support, key resuscitation, critical monitoring and other likely devices whose failure or misuse is reasonably likely to seriously injure patients or staff
Ventilators
Defibrillators
Anesthesia units
Patient lifts
©2008 ECRI Institute
© 2008 ECRI.
Medium-risk devices
Devices, including many diagnostic instruments, whose misuse, failure or absence (e.g. out of service with no replacement available) would have a significant impact on patient care, but would not be likely to cause direct serious injury
Clinical laboratory equipment
Ultrasound scanners
Electrocardiographs
©2008 ECRI Institute
© 2008 ECRI.
Low-risk devices
Devices whose failure or misuse is unlikely to result in serious consequences
Ophthalmoscopes
Electronic thermometers
Cast cutters
©2008 ECRI Institute
© 2008 ECRI.
Defining versus Predicting
Risk level definitions don’t predict probability or nature of device or system failure
High risk devices should be and usually are very reliable
Risk level should be used for prioritizing the completion of scheduled inspections
©2008 ECRI Institute
Case Study: Infusion Pumps
They are usually considered to be high-risk devicesThey have mechanical parts and are used for many yearsA comparatively high number of adverse incidents are
associated with pumps
© 2008 ECRI.
©2008 ECRI Institute
© 2008 ECRI.
Why pumps may not require periodic testing! Flow accuracy does not significantly deteriorate over time (5-10 years)
No reports of insidious or preventable failures
When they do fail, they fail “safe” (stop and alarm rather than over- or under-infusing)
Event logs show primary cause of adverse incidents is
operator error
Survey: some have stopped scheduling inspection or gone to every other year; some inspect a small sample
©2008 ECRI Institute
© 2008 ECRI.
Inspecting Infusion Pumps: How Often Is Enough?
“Many hospitals have a large number of general-purpose infusion pumps in their inventory. Therefore, the frequency at which these facilities schedule routine inspection of these pumps can have a major impact on their workforce utilization and costs. . .ECRI believes that, for most pumps in most facilities, inspection need not be scheduled for more than once a year, and that in many cases even this frequency is unnecessary.” (Health Devices 1998)
©2008 ECRI Institute
© 2008 ECRI.
Low-risk devices
If failure of a device is unlikely to result in serious consequences...
then there is little value in inspecting low risk devices
Some exceptions: ultrasound therapy units and warming cabinets
©2008 ECRI Institute
© 2008 ECRI.
Joint Commission
OK not to schedule IPM – but document decisionOK for different schedules for same device based on
differences in use (hospital versus ambulance defibs)Hospitals may modify manufacturer protocols based on
service experience Support decisions with records that identify issues related
to failure and misuse
©2008 ECRI Institute
© 2008 ECRI.
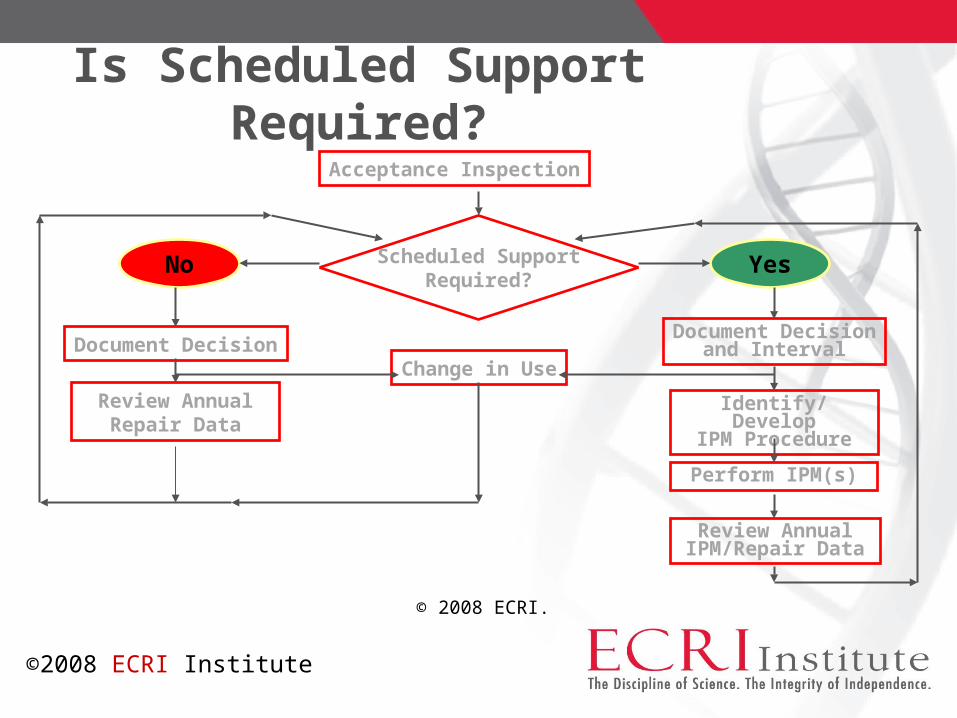
Is Scheduled Support Required? Acceptance Inspection
Scheduled SupportRequired?
No Yes
Document DecisionChange in Use
Document Decisionand Interval
Identify/DevelopIPM Procedure
Perform IPM(s)
Review AnnualIPM/Repair Data
Review AnnualRepair Data
©2008 ECRI Institute
© 2008 ECRI.
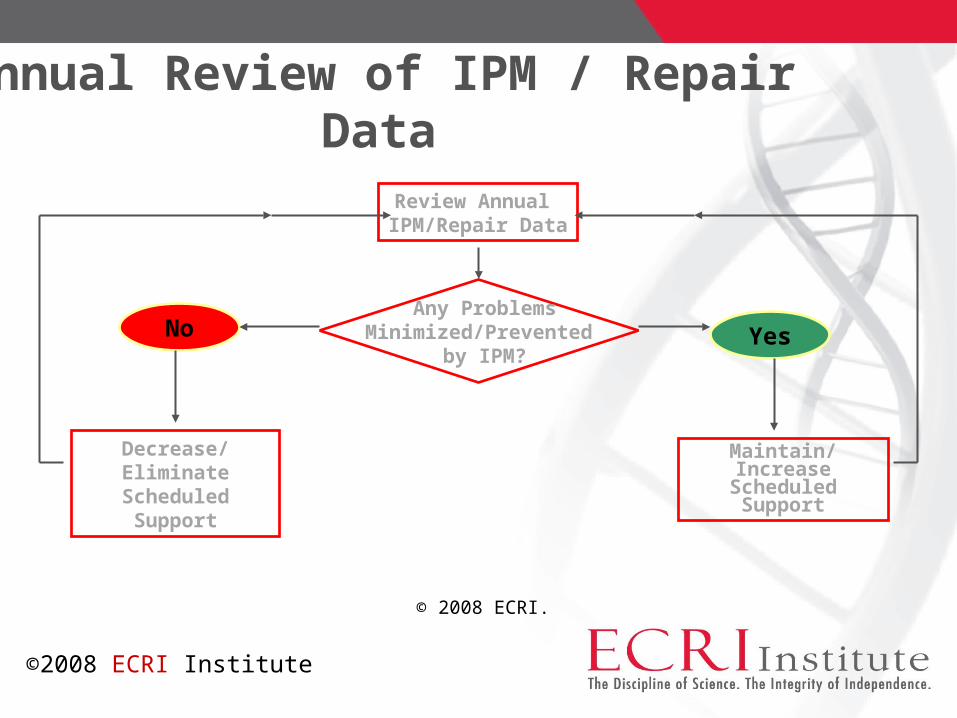
Annual Review of IPM / Repair Data
Review Annual IPM/Repair Data
Any Problems Minimized/Prevented
by IPM?No Yes
Maintain/IncreaseScheduled Support
Decrease/EliminateScheduled Support
©2008 ECRI Institute
Determining and Documenting Scheduled Support Decisions
Need to switch emphasis from equipment “risk level” to failure mode analysis
Need to identify differences in use/environmentNeed to document these issues have been considered
© 2008 ECRI.
©2008 ECRI Institute
Numeric/Formulaic Assessment Tools
These tools tend to emphasize failure effects and ignore failure mode data
Can these tools produce an objective determination?Can they produce consistent results?
© 2008 ECRI.
©2008 ECRI Institute
Hypothetical Scheduled Support Assessment Scheme
Consequence of Failure (1–4)
multiplied by
Likelihood of Failure (1–4) =
“Risk” Score© 2008 ECRI.
©2008 ECRI Institute
Hypothetical Scheduled Support Assessment Scheme
Risk Score ≥8: device is likely to need inspection
How can factoring 2 subjective decisions identifying a worst case failure resultestimating the likelihood of such a failure
produce an objective, definitive determination???© 2008 ECRI.
©2008 ECRI Institute
© 2008 ECRI.©2008 ECRI Institute
© 2008 ECRI.©2008 ECRI Institute
© 2008 ECRI.©2008 ECRI Institute
© 2008 ECRI.
An Interesting Study
Global Failure Rate: A Promising Medical Equipment Management Outcome Benchmark
Journal of Clinical Engineering July/September 2006
Binseng Wang et al. present failure data from three independent service organizations
Data is presented as Failures/Device/Year
Failure = # completed repair work orders
©2008 ECRI Institute
© 2008 ECRI.
What is a Failure?
“The device doesn’t operate”
“Repair or calibration had to be performed”
“Equivalent to a work order”
“Shouldn’t include cosmetic repairs”
“Shouldn’t include work orders for user abuse or error”
©2008 ECRI Institute
© 2008 ECRI.
Failure: Proposed Definition
“The condition of not meeting intended function or safety requirements and or a breach of physical integrity.
A failure is corrected by repair and/or calibration.” A Universal Medical Technology Service Nomenclature
Health Devices - June 2007
©2008 ECRI Institute
© 2008 ECRI.
Definition Challenges
It may be difficult to determine when user abuse or user error is the cause of a failure.
Similarly, environmental conditions (e.g., temperature, electrostatic discharge, line voltage spikes) beyond manufacturer specifications would ideally be excluded but are often not easily identified.
©2008 ECRI Institute
© 2008 ECRI.
Failure Data: Key Questions for Optimizing Scheduled Support Activities
Review findings from inspections and repairs: were any failures not detected by users? were any failures preventable? were any failures due to user abuse?
©2008 ECRI Institute
© 2008 ECRI.
Sources of Information/EvidenceInternal
Maintenance management system – Failure Data!
Use/environment considerations
External
Equipment manufacturers
Official bodies (FDA, Health Canada)
Independent bodies (ECRI Institute)
Other equipment users
©2008 ECRI Institute
Assessing the Need for Inspection
Start with manufacturer recommendations but consider that they were developed:
before reliability data was available for the device in every type of facility, anywhere over its expected life
(i.e., a worst-case use scenario) And, manufacturers sell . . .
service contracts!
© 2008 ECRI.
©2008 ECRI Institute
© 2008 ECRI.
Assessing the Need for Inspection
Consider manufacturer recommendations but also equipment service experience and the use environment
Determine appropriate inspection procedure and inspection interval
Eliminate unnecessary inspections particularly on low-risk devices
De-emphasize electrical safety testing
©2008 ECRI Institute
Another Look at Risk
“ Combination of the probability of occurrence of harm and the severity of that harm.”
In terms of scheduled support, the probability of occurrence of harm translates to . . .
quantifying the probability and types of equipment failure
© 2008 ECRI.©2008 ECRI Institute
© 2008 ECRI.
Assessing the Need for Inspection
Document decisions on a support assessment formPresent conclusions to hospital’s safety/quality committee
for approvalModify inspection intervals based on failure data from
ongoing repairs and changes in device use
©2008 ECRI Institute
© 2008 ECRI.
Failure Data: The Key to Scheduled Support
Failure data is needed to assess the value of scheduled support
Determine and track any failures - that were not/would not have been recognized by clinicians
- that could have been prevented
Step 1: Collect and analyze CMMS data
Step 2: Compare it to data from other service groups
©2008 ECRI Institute
© 2008 ECRI.
Strategies for Change
Process needs to become driven by relevant failure data ─ start by reviewing experience with pumps and monitors
Adopt the proposed definition for failureCollect data for each model to share/compare with other groups ECRI Institute will be facilitating a model-specific failure database When in doubt, perform inspections on a sample
©2008 ECRI Institute
© 2008 ECRI.
Strategies for Change
Lobby manufacturers to be more flexible with maintenance recommendations ( . . .“or in accord with hospital experience”) Request scheduled support requirements in equipment RFPsForward replies of excessive requirements to ECRI InstituteEducate governmental agencies and accreditation groups by demonstrating relevant failure data
©2008 ECRI Institute
What is Benchmarking?
The continuous, systematic search for, and implementation of better practices that lead to improved performance (www.idcon.com)
The process of comparing business practices and performance levels . . . to gain new insights and to identify opportunities for making improvements (Cohen et. al. 1995)
Benchmarking and Clinical Engineering
Indicators or metrics – numbers that represent level of performance of significant CE activities Annual service cost/device Average response time Multiple indicators for contrasting cost with service quality
Indicators or metrics – numbers that characterize equipment performance Failure rate Downtime
Evolution of a Product
Health Devices Inspection and Preventive Maintenance System™
becomes BiomedicalBenchmark™
Key new feature: Support Assessment database
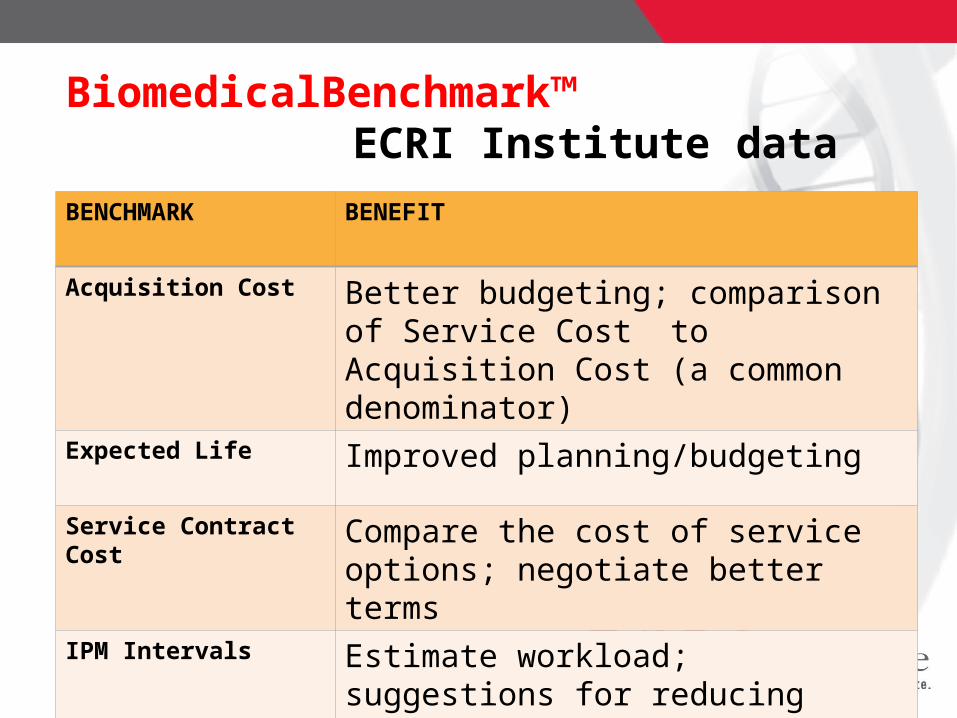
BiomedicalBenchmark™ECRI Institute data
BENCHMARK BENEFIT
Acquisition Cost Better budgeting; comparison of Service Cost to Acquisition Cost (a common denominator)
Expected Life Improved planning/budgeting
Service Contract Cost Compare the cost of service options; negotiate better terms
IPM Intervals Estimate workload; suggestions for reducing inspection frequency
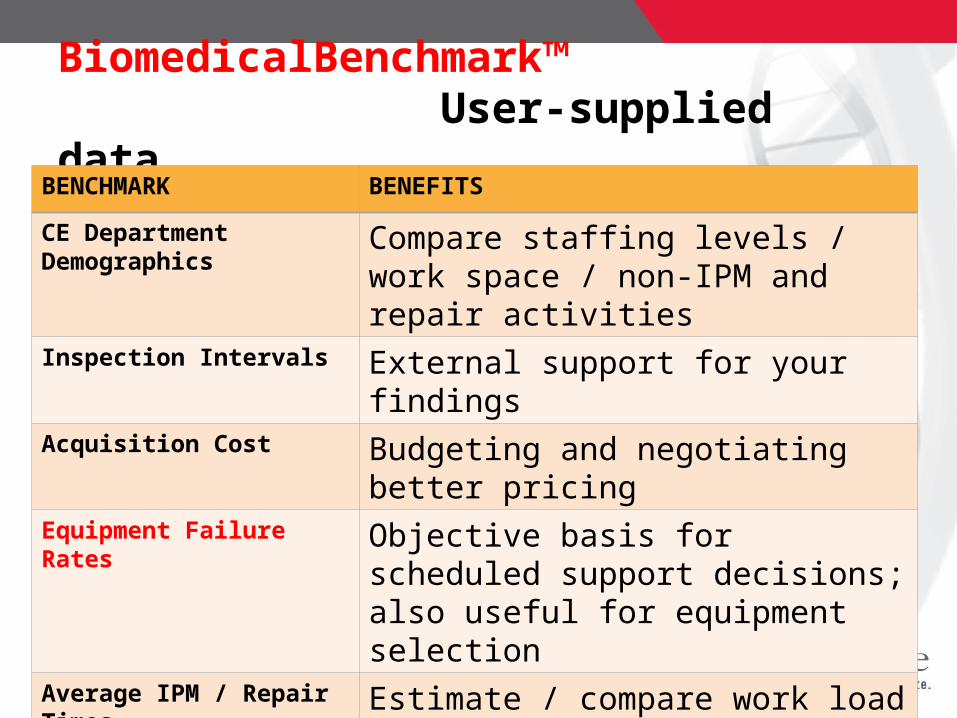
BiomedicalBenchmark™User-supplied data
BENCHMARK BENEFITS
CE Department Demographics Compare staffing levels / work space / non-IPM and repair activities
Inspection Intervals External support for your findingsAcquisition Cost Budgeting and negotiating better pricingEquipment Failure Rates Objective basis for scheduled support
decisions; also useful for equipment selectionAverage IPM / Repair Times Estimate / compare work load by modelModel-specific IPM Procedures Reduce time to develop new procedures
© 2008 ECRI.
Questions / Comments?
[email protected] 610-825-6000 x5168 ECRI Institute Web site: www.ecri.org [email protected]
©2008 ECRI Institute


![1350 ritter[1]](https://img.pdfslide.net/doc/110x75/558a55ded8b42a88468b458c/1350-ritter1.jpg)