Embed Size (px)
Citation preview

This article was downloaded by: [University of Colorado at Boulder Libraries]On: 19 December 2014, At: 12:16Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Population Studies: A Journal of DemographyPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/rpst20
Assessing the impact of in utero exposure to famineon fecundity: Evidence from the 1959–61 famine inChinaShige Songa
a Queens College of The City University of New YorkPublished online: 15 Mar 2013.
To cite this article: Shige Song (2013) Assessing the impact of in utero exposure to famine on fecundity:Evidence from the 1959–61 famine in China, Population Studies: A Journal of Demography, 67:3, 293-308, DOI:10.1080/00324728.2013.774045
To link to this article: http://dx.doi.org/10.1080/00324728.2013.774045
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) containedin the publications on our platform. However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose ofthe Content. Any opinions and views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be reliedupon and should be independently verified with primary sources of information. Taylor and Francis shallnot be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and otherliabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Assessing the impact of in utero exposure to famine onfecundity: Evidence from the 1959�61 famine in China
Shige SongQueens College of The City University of New York
This study identifies a significant increase in sterility among rural, but not urban, Chinese women who were
conceived and born during the 1959�61 famine that resulted from the Great Leap Forward. Applied to data
from two large-scale, nationally representative, sample surveys of Chinese women of childbearing age
conducted in 1997 and 2001 by the State Family Planning Commission, difference-in-differences analysis
revealed that exposure to the famine while in the womb caused an increase in the risk of sterility amongst
the adult women surveyed of 1.1 per cent. This is a substantial increase given that the overall prevalence of
primary and permanent sterility is only slightly over 1 per cent in China. These findings support the
hypothesis that a woman exposed to acute malnutrition while in the womb may experience a long-term
negative impact on her reproductive system, which could result in permanently impaired fecundity.
Keywords: developmental origins of health and disease; fecundity; female sterility; mixture model; long-
term survivor; China; famine; difference-in-differences analysis
[Submitted April 2011; Final version accepted July 2012]
Introduction
When food consumption falls below a critical mini-
mum level, women stop ovulating and thus cannot
conceive; when food levels rise once again ovulation
is restored, explaining why acute malnutrition may
temporarily decrease fecundity. Recent progress in
the search for the foetal, or developmental, origins
of health and disease suggests that famine may also
have a long-term impact on fecundity by affecting
the in utero development of the organs responsible
for the production and regulation of reproductive
hormones (Lumey and Stein 1997; Gluckman et al.
2005; Gardner et al. 2009). If this is indeed the case,
then the demographic consequences of famine are
likely to be substantially greater than has previously
been believed.
Evidence for the proposed long-term impact of
famine exposure on human fecundity is limited and
inconsistent. There are only three relevant studies,
all of which were of the effects of the major famine
resulting from the German occupation of the Neth-
erlands during the Second World War: the ‘Hunger
Winter’ of 1944�45 (Stein 1975). Using hospital
records and interview data on 700 Dutch women
born between 1944 and 1946, Lumey and Stein
(1997) reported that girls exposed in utero to the
Dutch famine were not significantly different from
girls not exposed in this way in age at menarche, age
at the birth of first child, number of births, or the
proportion of who remained childless. In contrast, a
second study based on the Dutch famine, albeit with
a smaller sample of 473 women, reported that
women exposed to the famine while in the womb
went on to begin childbearing at a younger age, to
have more children, to have more twin births, and to
be less likely to remain childless than women who
were not exposed (Painter et al. 2008). A third study
based on the Dutch famine reached conclusions
different from each of the other two. Examining data
from 7,941 women born in 1932�41, Elias et al.
(2005) showed that women exposed to severe famine
during childhood, rather than in utero, grew up to
experience a significantly decreased chance of bear-
ing a first or second child, and, for medical reasons,
an increased chance of having no children or fewer
than desired.
This paper reports results from a study that uses
high-quality survey data in conjunction with the
difference-in-differences method to identify the
long-term effect on the fecundity of women exposed,
while in the womb, to China’s 1959�61 famine. The
Population Studies, 2013
Vol. 67, No. 3, 293�308, http://dx.doi.org/10.1080/00324728.2013.774045
# 2013 Population Investigation Committee
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

famine was the result of a political campaign (the
‘Great Leap Forward’) to modernize the country’s
agrarian economy (Dikotter 2010). The plan of the
paper is as follows. I first review the demographic
literature on human fecundity, paying special atten-
tion to issues of measurement and estimation. In
light of this literature, I then discuss some of the
shared weaknesses of the Dutch famine studies and
assess how these weaknesses may have influenced
their findings. Next, I describe the empirical context
of the current study and the data, variables, and
identification and estimation strategy used. Finally, I
present the statistical results and discuss their policy
relevance.
Measuring fecundity: a demographic approach
Fecundity and fertility
Fecundity and fertility are closely related to each
other. Fecundity refers to the biological capacity to
reproduce, whereas fertility refers to the number of
offspring actually produced. Because fecundity is not
directly observable, demographers have to infer
fecundity from attained fertility. The total number
of children borne by a woman can be treated as a
proxy measure of her fecundity only among popula-
tions with natural fertility, where there is no contra-
ceptive use. There are almost no contemporary
populations that practise natural fertility, and there-
fore the number of children each woman bears
seldom reflects her biological capacity to reproduce.
In some special cases, however, even in contempor-
ary populations, it is possible to infer the two key
aspects of fecundity, fecundability and sterility, from
the time between marriage and first birth, or from
the lack of any child.
Fecundity, fecundability, and sterility
Fecundability refers to the monthly probability of
conceiving amongst women who are in a susceptible
state and who do not practise any form of contra-
ception. In populations with natural fertility, it is
possible to estimate fecundability using information
on birth intervals. In most contemporary popula-
tions, however, the widespread use of highly effec-
tive contraceptive methods severely distorts the
biological pace of childbearing, making estimates
of fecundability that are based on birth intervals a
less reliable indicator of fecundity. In addition,
estimates of fecundability may be influenced by
heterogeneity in fertility-related behaviours, such
as the frequency of sexual intercourse (Dunson
and Zhou 2000).
Sterility, also known as ‘permanent’, ‘complete’,
and ‘primary’ sterility (Wood 1994, pp. 443�4), refers
to an irreversible biological state that lasts through-
out a woman’s entire reproductive period. Child-
lessness is a reasonable proxy measure of it. When
data on contraceptive use or frequency of sexual
intercourse are lacking, the prevalence of sterility,
which is primarily influenced by biological factors,
may be considered a more reliable measure of
fecundity than fecundability (Weinstein and Stark
1994; Wood 1994). The only non-biological factor
that must be taken into account when estimating the
prevalence of sterility is the extent of a preference
for voluntary childlessness within a population, since
childlessness by choice cannot be taken to indicate
sterility.
In the demographic literature the estimation of
fecundability and sterility have been largely treated
as two separate issues (Trussell and Wilson 1985;
Kallan and Udry 1986; Larsen and Menken 1989;
Weinstein et al. 1990; Larsen and Vaupel 1993).
However, during the past 20 years demographers
have begun to realize that these two closely related
aspects of fecundity should be analysed jointly
because they each introduce additional information
about the other (Wood 1994). A number of statis-
tical procedures, each with different underlying
behavioural assumptions and varying degrees of
sophistication, have been proposed to estimate
sterility and fecundability simultaneously using in-
formation on birth intervals (Heckman and Walker
1990; Larsen and Vaupel 1993; Wood 1994; Dunson
and Zhou 2000).
Lessons from the Dutch famine studies
The cohort of women born in the Netherlands
during the 1944�45 Dutch famine can hardly be
described as a natural-fertility population. When
these women reached childbearing age in the 1960s,
the vast majority of them would use highly effective
contraceptive measures (Moors 1978; Leridon 1981).
As a result, the number of children borne by each of
these women depended heavily on choice and could
not be used as an indicator of fecundity (although
see Lumey and Stein 1997; Painter et al. 2008). Since
it is impossible to obtain reliable estimates of
fecundability from birth-interval information with-
out knowing the exact timing of contraceptive use,
the high level of contraceptive use amongst the
294 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

Dutch population casts doubt on the relevance of
any estimated cohort differences in fecundability
based on birth-interval information.
In addition, none of the studies based on the
1944�45 Dutch famine attempted to exclude from
their analyses those women who were voluntarily
childless, although they comprised up to a quarter of
the cohort born during the famine (Den Bandt
1980). Such a high percentage of voluntarily child-
less individuals in the study populations could easily
have biased the results on cohort differences in
sterility in unexpected ways.
Finally, none of the studies of the Dutch famine
controlled for age at marriage which, although the
relationship is not yet well understood, has been
shown to be an important correlate of childlessness
in historical populations (Trussell and Wilson 1985;
Menken et al. 1986).
In summary, none of the studies of the Dutch
famine were able to achieve an adequate measure of
women’s fecundity. It is therefore necessary to treat
with caution the conclusions drawn from these
studies about the long-term effect of famine expo-
sure on women’s fecundity.
The current study
The Great Leap Forward, the 1959�61 famine,and urban�rural differences in famine severity
A number of studies have detailed the causes and
magnitude of the 1959�61 famine in China (Ashton
et al. 1984; Peng 1987; Kung and Lin 2003), and
these indicate that the famine affected most parts of
the country, causing approximately 30 million excess
deaths and an additional 33 million foetal losses,
making it one of the most disastrous events in
human history. The famine was much more severe
in rural areas than in urban ones. Although reliable
data on changes in daily calorie intake during the
famine are not available, indirect estimates have
suggested that grain availability declined much more
dramatically in rural areas, exacerbating a pre-
existing urban�rural difference in grain availability
per head and pushing the daily calorie intake of
many rural residents below subsistence level (Peng
1987; Lin and Yang 2000). In contrast, the effects on
the urban population were far less severe; starvation
rarely occurred in the cities.
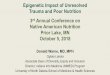
Figure 1 shows the annual crude mortality rates
for the populations of urban and rural China from
1956 to1964 (State Statistical Bureau 1991; Lin and
Yang 2000). Among the urban population there is no
sign of a major increase in mortality during the three
famine years 1959, 1960, and 1961. Indeed, in 1959
and 1961 the rate of mortality in urban areas was not
much higher than the rate in rural areas during non-
famine years. Furthermore, amongst the urban
population the rate of mortality in the peak famine
year, 1961, was lower than the rate of mortality in
rural areas in either 1959 or 1961, and much lower
than the peak rate of rural famine mortality in 1960.
The Chinese population recovered quickly however.
In 1962, immediately after the famine ended, the
national mortality rate returned to its pre-famine
level and the country’s fertility rate, which had fallen
markedly during the famine, rose well beyond its
pre-famine level and subsequently remained high for
several years (Peng 1987).
An important reason for the urban�rural differ-
ence in famine severity was the different treatment
meted out to urban and rural residents by China’s
socialist system. Whereas urban residents were
granted legal rights to food security through a
system of food rationing, rural residents, who
produced and supplied the food, were legally bound,
under the coercive quotas imposed by the national
food-procurement system, to surrender their pro-
duce (Lin and Yang 2000). In years of poor harvest,
such as 1959, 1960, and 1961, peasants and their
families had little food remaining after they had
fulfilled quotas. The extreme measures used by the
state to extract ‘surplus’ food from the peasants left
the latter with no choice but to comply, although
resistance and conflicts were not uncommon (Walker
1984; Dikotter 2010). The different impact which the
famine had on urban and rural areas, as depicted in
Figure 1, contributes crucially to the information
30
25
20
15
10
51956 1958 1960 1962 1964
Year
Urban population Rural population
Mor
talit
y ra
te (
per
thou
sand
)
Figure 1 Annual crude mortality rates per 1,000
population for the urban and rural populations of
China; 1956�64Source: Statistical Yearbook of China 1991 (State Statis-tical Bureau 1991, pp. 79�80).
Long-term effect of famine on fecundity 295
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

needed to identify and estimate the long-term effect
of famine exposure on women’s fecundity.
The famine resulting from the Great Leap For-
ward has been used to study both short-term and
long-term effects of exposure in utero to acute
malnutrition. The outcomes include the following:
involuntary foetal loss suffered by the mothers (Cai
and Wang 2005); a reduced propensity to have male
offspring (Song 2012); and changes in mortality
(Song 2010) and disability among children born
during the famine (Mu and Zhang 2010). As a
source of data on the effects of famine, China’s
famine differs strikingly from the Dutch example
owing to the unusually long duration of the former,
the extent to which it affected the population, and
the significant spatial variations in the severity of its
impact. Previous studies have shown that the Chi-
nese famine provides an opportunity to investigate
outcomes on which the studies based on the Dutch
famine failed to provide consistent results (Song
2012).
The one-child policy and changing fertilitypatterns in China
When the cohorts of Chinese women born during
the 1959�61 famine entered their childbearing years
in the early 1980s, China was in the process of
changing from a ‘later, longer, fewer’ family plan-
ning policy to a more rigid policy of ‘one child per
couple’. Whereas the earlier policy had encouraged
couples to marry late, to have no more than two
children, and to have long birth intervals, the new
policy prohibited couples from having more than
one birth, while at the same time relaxing the
regulations about late marriage and long birth
intervals. In 1980 a new marriage law made the
legal minimum age at marriage 20 for women and 22
for men; both considerably lower than the de facto
local standards of the 1970s (Song 2004).
These policy changes, combined with other con-
temporaneous social and economic changes, such as
a shift away from arranged marriage and increased
intimacy and sexual activity between spouses, as well
as a rapid increase in formal education for both men
and women, led to a secular decline in both the age
at marriage and the age at first birth (Wang and
Yang 1996; Hong 2006). Clearly, these demographic
changes were policy-induced and had nothing to do
with the 1959�61 famine. Although the ‘later, longer,
fewer’ policy in the 1970s and the ‘one-child policy’
that was adopted in the early 1980s both aimed to
prevent people from having ‘too many’ children,
under neither policy was having one child consid-
ered to be having ‘too many’. According to Scharp-
ing (2003, pp. 215�6), a long-standing feature of life
in rural China is that virtually all women desire to
have children. In addition, although the use of
contraceptives has been widespread in China since
the 1980s, few Chinese women practise contracep-
tion before the birth of their first child, particularly
in rural areas (Choe and Tsuya 1991; Short et al.
2000). Women who do not proceed to have at least
one child are therefore highly likely to be involun-
tarily childless and suffering from primary sterility.
Thus, in the unique historical context of Chinese
society over the past half century, neither the
‘number children borne’ nor birth spacing can
reliably be used to describe cohort trends in wo-
men’s fecundity. Being much less sensitive to
changes in policy, society, or the economy, women’s
sterility, as measured by involuntary childlessness,
can, in contrast, be used to capture famine-induced
changes in fecundity.
Research hypothesis
Table 1 summarizes the in utero famine exposure
status of six selected birth cohorts of Chinese women
and the hypothesized effect on their fecundity in
adulthood. Of the six birth cohorts considered, the
Table 1 Windows of in utero exposure to the 1959�61 famine in China by birth cohort and the expected effects onfecundity by rural and urban residence
Expected effect on female fecundity
Birth cohort Prenatal famine exposure Rural women Urban women
1957�58 No exposure No effect No effect1959 Partial exposure, late Some damaging effect Weak to no effect1960�61 Full exposure Full damaging effect Weak to no effect1962 Partial exposure, early Some damaging effect Weak to no effect1963�64 No exposure No effect No effect1965�66 No exposure No effect No effect
296 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

1957�58 cohort were born before the famine and
experienced the famine as young children. Both the
1963�64 and 1965�66 cohorts were born after the
famine and thus were not exposed to its pernicious
effects. The 1959 and the 1962 cohorts were only
partially exposed to the famine in utero, although at
different gestational ages. Finally, the 1960�61 co-
hort were exposed to the famine from the moment
of conception to birth
To make the cohort comparison as sharp and
informative as possible, the main statistical analysis
of the current study focused primarily on the
contrast between the following three cohorts: the
pre-famine cohort (1957�58), the famine cohort
(1960�61), and the post-famine cohort (1963�64).
According to hypotheses about the foetal origins of
health and disease, only the period spent in the
womb is vital for the development of the woman’s
reproductive system and it was therefore hypothe-
sized that individuals from the 1960�61 rural cohort
would have significantly reduced fecundity. This was
because they had been exposed to the famine
throughout their gestation and would have been
most affected by the acute malnutrition suffered by
their mothers during the famine. It was further
hypothesized that members of the 1963�64 rural
cohort would exhibit ‘normal’ levels of fecundity
during their own childbearing years because they
were not exposed to the famine in utero. Finally, it
was assumed that women of the 1957�58 rural
cohort would also have more or less normal levels
of fecundity because they had been exposed to the
famine during early childhood rather than in the
womb. Cohort variations in fecundity were expected
to be much weaker among the urban population
because annual differences in exposure to the
famine were much less marked in urban areas.
Research design
Data and sample
The analyses undertaken in the current study were
based on data from the two most recent, nationally
representative, sample surveys conducted by China’s
State Family Planning Commission: the 1997
National Population and Reproductive Health
Survey and the 2001 National Family Planning and
Reproductive Health Survey. The sampling plans
and questionnaires used in both surveys were very
similar. The questionnaires collected pregnancy
and birth-history information from women of child-
bearing age residing in family households across all
31 of China’s provinces. The 1997 survey interviewed
15,000 women and the 2001 survey 39,586. The
surveys provided good population coverage and
the data collected are considered to be of high
quality (Zhang and Zhao 2006; Chen et al. 2007;
Song and Burgard 2011).
Two outcome variables were extracted from the
retrospective birth histories and these were then
used to estimate fecundability and sterility jointly.
The variables were ‘ever had a child’, a binary
variable indicating whether or not a respondent
had ever given birth and ‘time to first birth’, a
continuous variable measuring, for each woman who
had ever given birth, the interval, in years, between
her first marriage and first birth.
Most existing studies define a woman as sterile if
she has not given birth after 2 years of marriage
(Collins et al. 1983; Fang et al. 1993). Some studies
have adopted a more rigid definition, classifying a
woman as sterile only if she has not given birth after
7 years of marriage (Larsen 2000; Liu et al. 2004).
For the current study, women aged 33�40 in the 1997
survey and women aged 37�44 in the 2001 survey
were selected for analysis. Because rural women had
married, on average, in their early 20s and urban
women in their mid-20s (see Table 3), a woman who
had not given birth by the time of the surveys had
therefore been ‘at risk’ of having a child for
considerably more than 7 years, so the definition of
sterility used in the current analysis was particularly
rigorous.
Table 2 compares the estimated prevalence of
sterility amongst the women sampled from the 1997
and 2001 surveys, using each of the three definitions
of sterility given above: no child born after 2 years of
marriage, no child born after 7 years of marriage,
and no child born by 1997 or 2001. The estimates
calculated using the last of these definitions were
assumed to indicate the true prevalence of primary
sterility. When the 2-year cut-off was applied to the
1997 and 2001 data, the true prevalence of women’s
sterility was vastly overestimated. When the 7-year
cut-off was applied, the true prevalence was again
overestimated but by a much smaller margin. The
estimates for the three cohorts derived from the
1997 survey data were largely consistent with those
derived for the same cohorts from the 2001 survey
data. When the 7-year cut-off was applied to the data
in the two surveys, approximately 1.8 per cent of
women were estimated to be sterile. This was a
similar magnitude to the 1.3 per cent rate estimated
for China by earlier studies using the same definition
of sterility (Liu et al. 2004). However, both these
rates are lower than comparable estimates for other
Long-term effect of famine on fecundity 297
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

societies where 2.1�4 per cent of women were
considered to be sterile (Bongaarts 1980; Wrigley
1997; Larsen 2000). The reasons for the lower
prevalence of sterility in China is not yet well
understood, but may be related to Chinese culture,
which is strongly pro-natalist, and actively en-
courages childless women to seek fertility treatment.
However, the aim of the current research was not to
estimate the prevalence of women’s sterility in
China, but to identify differences in the levels of
sterility between birth cohorts, and between urban
and rural populations. Thus unless the*so far
unexplained*‘Chinese factor’ had a differential
impact in urban and rural areas or across birth
cohorts, which is considered most unlikely, it will
have little influence on either the analysis or the
central findings.
The key independent variables of interest in the
analysis were women’s birth cohort and urban vs.
rural residence. As described above, Chinese women
born between 1957 and 1966, and surveyed in either
1997 or 2001, were classified into six birth cohorts: a
1957�58 cohort (pre-famine, no in utero exposure to
the 1959�61 famine); a 1959 cohort (partial exposure
in utero at late gestational age); a 1960�61 cohort
(full exposure; whole time in utero spent exposed to
famine conditions); a 1962 cohort (partial exposure
in utero at early gestational age); and a 1963�64 and
a 1965�66 cohort (both post-famine, no exposure).
All six cohorts were included in an exploratory
analysis (see Table 2) and a sensitivity test (see
Table 5) but the main analysis was conducted using
only the 1957�58, 1969�61, and 1963�64 cohorts (see
Tables 3 and 4). ‘Urban�rural residence’ was taken
to be a binary variable indicating where the respon-
dent was living at the time they were surveyed; if
they lived in a rural area they were given the code
‘1’, if in an urban area they were given the code ‘0’.
Although it is possible that some women had
changed their place of residence between the time
of their birth and the time they were interviewed,
the impact of such changes on key findings about the
effect of in utero famine exposure on fecundity is
largely predictable and likely to be small in scale. In
China the flow of migration was nearly always from
rural to urban areas. Because women born in rural
areas were most severely affected by the 1959�61
famine, the presence of a fraction of rural-born
women in the urban sample drawn from the 1997
and 2001 surveys may mean that the effects of the
famine were somewhat overestimated for the urban
sample but not for the rural sample. If so, the
difference-in-differences estimate of the famine
effect was more conservative than was truly
the case.
A number of control variables were included in
the analysis. ‘Age at marriage’, which is a known
correlate of both fecundability and sterility (Trussell
and Wilson 1985; Menken et al. 1986), was included
as a continuous variable. ‘Education’ was taken to be
a four-category ordinal variable, derived from the six
categories used in the surveys. The four categories
were: no schooling, primary school, junior high
school, and senior high school education and above.
Women’s education is an important socio-economic
indicator, widely used in population and health
studies in less developed countries where data on
other socio-economic indicators, such as household
income or occupation, are unreliable or unavailable
(Desai and Alva 1998). In addition, women’s educa-
tion can be used to measure self-efficacy, as women
with higher education are assumed to be more
capable of utilizing modern health services and
pursuing health-enhancing activities (Caldwell
Table 2 Estimated prevalence of sterility (per 100 women) among Chinese women when different definitions of sterilityare used; 19971 and 20012 surveys
1997 Survey1 2001 Survey2
BirthNo child after
2 yearsNo child after
7 yearsNo childby time
No child after2 years
No child after 7years
No childby time
cohort of marriage of marriage of survey N of marriage of marriage of survey N
1957�58 16.44 1.74 0.93 864 17.20 1.72 0.97 2,2621959 15.44 1.40 1.05 285 15.97 1.60 1.35 8141960�61 17.13 1.96 1.31 613 17.24 2.63 1.59 1,6361962 15.91 1.52 0.57 528 16.92 1.21 0.78 1,4071963�64 17.11 1.56 1.23 1,216 15.21 2.01 1.03 3,2871965�66 16.12 2.33 2.05 1,073 14.24 1.67 1.00 3,110Overall 16.51 1.81 1.29 4,579 15.84 1.84 1.08 12,516
Source: 11997 National Population and Reproductive Health Survey and 22001 National Family Planning and ReproductiveHealth Survey.
298 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

1994; Ross and Wu 1995; Desai and Alva 1998; Song
and Burgard 2011). Ethnicity was measured as a
binary variable, members of the Han ethnic majority
being coded ‘1’ and the non-Han ethnic minority
being coded ‘0’.
In Table 3, data from the 1997 and 2001 surveys
have been combined to produce descriptive statistics
for women drawn from the three birth cohorts of the
main study sample, cross-classified by place of
residence.
Statistical models of fecundity: joint estimationof sterility and fecundability
When estimating women’s sterility from birth-his-
tory information, the problem of right censoring was
encountered. Women in the cohorts being studied
were aged 33�40 at the time of the 1997 survey and
37�44 when the 2001 survey was taken. At such ages,
most Chinese women would have stopped giving
birth, but would not yet have lost their biological
capacity to reproduce (Lavely 1986). Data derived
from the two surveys indicate whether each woman
had given birth to a child by the time she was
surveyed, but not whether she went on to have a
birth thereafter. Older cohorts in the sample would
therefore almost certainly show a lower level of
childlessness than their younger counterparts, not
because they were less likely to be sterile, but
because they have had more time to bear a child.
It is possible to truncate the period in which the
older cohorts are being observed in order to achieve
better comparability, but this strategy is not optimal
because valuable information that can be used to
achieve more precise effect estimates is discarded.
Hazard models can be used to handle right-
censored data, but conventional hazard models do
not make a clear distinction between the probability
of an event occurring and the timing of its occur-
rence. If a subset of the population under observa-
tion has never been ‘at risk’ of experiencing a
particular event, conventional hazard models are
no longer sufficient. For this study it was hypothe-
sized that within the sample population there was a
subgroup of women who were not ‘at risk’ of giving
birth because they were biologically sterile, and
in utero exposure to famine potentially increased a
woman’s risk of being in the ‘sterile’ subgroup. The
analytical task was to identify the effect of in utero
famine exposure on adult sterility by comparing the
relative prevalence of sterility across cohorts and
between urban and rural populations. To obtain
unbiased estimates of the prevalence of sterility, it
is crucial to control adequately for differential
exposure to the risk of having a child by imposing
certain parametric assumptions on the baseline
hazard function of ‘time from marriage to first
birth’. In the literature a parallel argument is often
encountered: that because sterile women are not at
risk of giving birth, their presence must be ade-
quately controlled for in order to obtain unbiased
estimates of fecundability (Heckman and Walker
1990; Wood 1994; Dunson and Zhou 2000).
Table 3 Combined descriptive statistics of selected Chinese women interviewed in the 19971 and 20012 surveys
Rural Urban
1957�58 1960�61 1963�64 1957�58 1960�61 1963�64(N�2,264) (N�1,545) (N�3,353) (N�862) (N�704) (N�1,150)
For everybody in the sample
% who had never given birth 0.75 1.55 0.84 1.51 1.42 1.83% belonging to the non-Han ethnic minority 8.66 10.36 9.81 5.68 5.97 7.04
Education% with no schooling 39.84 26.21 19.09 5.22 2.56 1.91% who attended primary school only 31.67 33.98 34.66 10.56 8.66 7.74% who attended junior high 21.69 27.44 39.70 34.80 26.85 37.74% who attended senior high or above 6.80 12.36 6.56 49.42 61.93 52.61
Age at first marriage 22.10 21.81 21.45 24.07 23.71 23.40(2.41) (2.39) (2.41) (2.69) (2.77) (2.73)
For those who had given birth
Average age at first birth (years) 23.65 23.32 22.90 25.66 25.38 24.98(2.53) (2.50) (2.48) (2.85) (2.98) (2.86)
Average length of first birth interval (years) 1.57 1.52 1.47 1.63 1.71 1.63(1.14) (1.12) (1.01) (1.25) (1.42) (1.47)
Note: Standard deviation given in parentheses.Sources: 1 and 2 as for Table 2; the figures from the two surveys have been combined.
Long-term effect of famine on fecundity 299
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

A mixture cure fraction model, also known as a
‘cure model’, a ‘long-term survivor model’, a ‘split-
population model’, or a ‘mover-stayer’ model (Fare-
well 1982; Schmidt and Witte 1989; Maller and Zhou
1996) was used to jointly estimate both a probability
model that predicted sterility status and a parametric
hazard model that predicted the monthly probability
of conception for those who were not sterile.
Following Sposto (2002) and Lambert et al. (2010),
the survival function of a cure model can be defined
as
SðtÞ ¼ pþ ð1� pÞð1� FðtÞÞ (1)
where p represents the fraction of sterile women
within a population and F(t) denotes a statistical
distribution function for the time from marriage to
first birth. The hazard function for the model can be
written as
hðtÞ ¼ ð1� pÞf ðtÞSðtÞ
(2)
where f(t) is the density function of F(t). Following
Wood (1994), a log-normal distribution for F(t) was
chosen because ‘time from marriage to first birth’ is
known to have an inverse J-shaped hazard function:
FðtÞ ¼ Uðlog½kt�cÞ (3)
where F(�) denotes the standard normal distribution
function.
Covariates can be introduced into both the
sterility probability model p and the log-normal
hazard model h(t). For a binary dependent variable
such as sterility, a logit link function has commonly
been used to introduce covariates, and the coeffi-
cients can be interpreted as an odds ratio:
logpðxÞ
1� pðxÞ¼aþbX: (4)
Probit, complementary log�log, and even linear
link functions can also be used. Using a linear link
function with a binary dependent variable*com-
monly known as a ‘linear probability model’*has
the important advantage that the interpretation of
its coefficients, including those for the interaction
terms, is similar to that of a linear regression model.
This makes it much easier to construct the differ-
ence-in-differences effect estimates from the statis-
tical results. While linear probability models have
some weaknesses, such as the assumption that errors
are normally distributed, these can be handled by
bootstrapping the standard errors or confidence
intervals (Mooney et al. 1993).
When using a log-normal hazard model, covari-
ates can be introduced to predict either the scale
parameter l, the shape parameter g or both.
Following Sposto (2002) and De Angelis et al.
(1999), in the main analysis the shape parameter
was held constant and only the scale parameter was
allowed to vary with covariates:
logðkÞ¼aþbXþl (5)
in which m follows a standard normal distribution
with mean value of zero and a fixed standard
deviation. Because the log-normal model is not a
member of the proportional hazard model family, its
coefficients are interpreted as a time ratio, rather
than a hazard ratio. Thus, one unit increase in the
covariate X produces exp(b) units of change in the
time it takes for an event to occur, the ‘time-to-
event’. If the time ratio of a covariate is lower than
one, then that covariate accelerates the process
under observation; if higher than one then the
covariate is acting to slow down the occurrence of
the event of interest.
More technical details of the mixture cure model,
including the derivation of the model likelihood
function and numerical maximization strategy, can
be found in Sposto (2002) and Lambert et al. (2010).
The current analysis employed user-contributed
mixture analysis modules in Stata to implement the
above procedures (Lambert 2007).
Obtaining difference-in-differences estimates ofthe effect of in utero famine exposure onwomen’s sterility in adulthood
The most commonly used strategy for identifying the
effect of famine exposure is to compare the outcome
of interest between an observed famine cohort and
non-famine cohorts, but, as Chen and Zhou (2007)
and Huang et al. (2010a) have indicated, such an
estimated difference between the two types of
cohort may include both a famine effect and a
residual cohort effect that is unrelated to famine.
These authors suggest that a difference-in-differ-
ences strategy should be used to remove the residual
cohort effect in order to obtain a more reliable
estimate of the famine effect.
Let Ci denote the birth cohort of the ith woman in
the sample; Ci�1 if she was exposed to the famine
while in the womb, otherwise Ci�0. Let Ri denote
the place of residence of the ith woman; Ri�1 if she
was living in a rural area, otherwise Ri�0. A
difference-in-differences estimate of the effect of in
utero famine exposure on adult sterility can be
300 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

constructed by taking the second difference between
the cohort difference and the urban�rural difference
in sterility risk:
d ¼fP½Ci ¼ 1;Ri ¼ 1� � P½Ci ¼ 1;Ri ¼ 0�g� fP½Ci ¼ 0;Ri ¼ 1� � P½Ci ¼ 0;Ri ¼ 0�g:
(6)
This is equivalent to including Ci, Ri and their
interaction term in the logistic regression for sterility
in equation (4):
logpðxÞ
1� pðxÞ¼ aþ b1Ci þ b2Ri þ b3Ci � Ri: (7)
As Puhani (2008) has demonstrated, owing to the
non-linear nature of the logit link used above, the
difference-in-differences estimate of the famine
effect is a monotonic nonlinear transformation of
b3, the statistical significance of which can be
assessed using numerical methods. The interpreta-
tion can be greatly simplified by estimating an
equivalent linear probability model:
pðxÞ ¼ aþ b1Ci þ b2Ri þ b3Ci � Ri (8)
in which b3 represents the difference-in-differences
estimate of the famine effect. The statistical signifi-
cance and confidence intervals of which can be
assessed in the same manner as those of a linear
regression model.
Analysis
The analysis was conducted in three steps. First,
descriptive statistics of the study sample were
calculated. Then a series of cure fraction models,
which jointly estimated sterility and fecundability,
were estimated and compared. Finally, the differ-
ence-in-differences estimates of the famine effect on
fecundity were constructed based on the best-fit
model.
Descriptive analysis
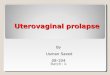
Figure 2 shows the observed pattern of women’s
sterility, defined as having no child between first
marriage and the survey interview, for single-year
birth cohorts in both rural and urban areas of China.
For rural women, the impact of in utero famine
exposure on sterility is clear. The proportion of
sterile rural women rose between the 1958 and the
1959 cohort before reaching its peak level in the
1960 cohort. The proportion of sterile women
declined in the 1961 birth cohort and fell to its
lowest level in the 1962 cohort. Although both the
1959 and the 1962 rural cohorts were exposed to
famine conditions for part of their time in the womb,
they show dramatically different patterns of sterility
in their adult years. These patterns suggest that
either exposure to famine during early gestation had
a different effect from exposure later in gestation,
something which has not been previously reported in
the literature, or that random sampling errors were
present. In contrast, it is more difficult to identify a
cohort pattern in sterility amongst urban women
owing to the considerable year-to-year fluctuations
observed.
Did in utero famine exposure influence thefecundity of adult women differently in urbanand rural areas?
Table 4 reports results from four mixture cure
models that estimated both women’s sterility and
fecundability. For each model, the output has been
divided into two panels: Panel A shows the results of
a logistic regression predicting sterility status, while
controlling for right censoring; Panel B shows a log-
normal accelerated-failure-time hazard model that
estimated the fecundability of those who were not
sterile. The model selection was based on AIC and
BIC (Raftery 1995; Aitkin 1996), the two widely
used measures of relative goodness of fit of statis-
tical models. For both measures, a smaller value
indicates a better fit to the data.
Model 1 included birth cohort, urban�rural resi-
dence, and year of survey as variables in both the
2.5
2.0
1.5
1.0
0.5
01950 1953 1959 1965 1968
Birth cohort19621956
Urban women Rural women
Lev
el o
f st
erili
ty (
per
hund
red)
Figure 2 Trends in sterility amongst rural and
urban Chinese women, by year of birth; 1951�67,
as reported in the 1997 and 2001 surveysNote: Sterility is defined as no childbirth between firstmarriage and the time of the survey.Source: As for Table 2.
Long-term effect of famine on fecundity 301
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

Table 4 Results from four joint sterility and fecundability models (mixture logit�log-normal cure fraction model) forwomen from the 1957�58, 1960�61, and 1963�64 birth cohorts interviewed in the 19971 and 20012 surveys
Model 1 Model 2 Model 3 Model 4
Panel A: sterility model (odds ratios)Year of survey
1997 � � � �2001 1.01 1.01 0.87 0.87
[0.65, 1.57] [0.65, 1.57] [0.57, 1.34] [0.57, 1.34]Birth cohort
1957�58 0.88 0.89 0.68 0.68[0.42, 1.84] [0.43, 1.84] [0.33, 1.39] [0.33, 1.40]
1960�61 0.77 0.77 0.65 0.65[0.34, 1.74] [0.34, 1.74] [0.29, 1.46] [0.29, 1.45]
1963�64 � � � �Rural residence 0.45* 0.45* 0.78 0.81
[0.24, 0.83] [0.24, 0.83] [0.40, 1.53] [0.45, 1.49]Interaction effect
1957�58�rural residence 1.14 1.14 1.17 1.20[0.44, 2.99] [0.44, 2.98] [0.45, 3.03] [0.47, 3.09]
1960�61�rural residence 2.72* 2.72* 2.78* 2.81*[1.02, 7.31] [1.02, 7.31] [1.04, 7.40] [1.06, 7.46]
Age at first marriage 1.34*** 1.33***[1.26, 1.42] [1.26, 1.41]
EducationNo schooling 1.24
[0.67, 2.29]Primary school � �Junior high school 1.09
[0.63, 1.88]Senior high school and above 0.98
[0.51, 1.88]Han ethnic majority 1.17
[0.56, 2.44]Panel B: fecundability model (time ratios)Year of survey
1997 � � � �2001 0.76*** 0.76*** 0.77*** 0.77***
[0.75, 0.78] [0.75, 0.78] [0.75, 0.79] [0.75, 0.79]Birth cohort
1957�58 1.04*** 1.02 1.05*** 1.05***[1.02, 1.06] [0.97, 1.06] [1.02, 1.07] [1.02, 1.07]
1960�61 1.03* 1.05* 1.03* 1.03*[1.01, 1.06] [1.01, 1.10] [1.01, 1.06] [1.01, 1.06]
1963�64 � � � �Rural residence 0.95*** 0.95*** 0.93*** 0.93***
[0.93, 0.97] [0.92, 0.98] [0.91, 0.96] [0.91, 0.96]Interaction effect
1957�58�rural residence 1.03[0.98, 1.08]
1960�61�rural residence 0.97[0.92, 1.03]
Age at first marriage 0.98*** 0.98***[0.98, 0.98] [0.98, 0.98]
EducationNo schooling 1.04** 1.04**
[1.01, 1.07] [1.01, 1.07]Primary school � �
Junior high school 0.99 0.99[0.96, 1.01] [0.96, 1.01]
Senior high school and above 1.07*** 1.07***[1.04, 1.11] [1.04, 1.11]
302 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

sterility and fecundability equations and the inter-
action between urban�rural residence and birth
cohort in the sterility equation. Model 2 added
interaction terms between birth cohort and urban�rural residence to the fecundability equation.
Although AIC does not show a strong preference
between the two models, BIC clearly suggests that
Model 1 fits the data better than Model 2, indicating
that in utero famine exposure status affected sterility
amongst women in rural areas differently from those
in urban areas, but that there was no differential
effect on fecundability. The inclusion of additional
control variables such as age at marriage, level of
education, and ethnicity in Model 3 resulted in an
even better fit to the data, as suggested by both AIC
and BIC. Careful inspection of Model 3 reveals that
the effects of education and ethnicity are significant
in the fecundability equation (Panel B) but not in
the sterility equation (Panel A). By excluding
education and ethnicity from the sterility equation
in Model 4, the fit of the model was further
improved, according to both the AIC and BIC,
making Model 4 the best-fit model.
The foregoing model comparison exercise sug-
gests that exposure to the 1959�61 famine while in
the womb had a differential influence on the sterility,
but not the fecundability, of adult women in urban
and rural areas of China.
The biological nature of the relationship betweenin utero famine exposure and sterility inadulthood
In the best-fit model, Model 4, neither education nor
ethnicity has a statistically significant effect on
sterility, and statistically significant urban�rural
differences in sterility are only present in the famine
cohorts but not in the non-famine cohorts because
women in rural areas were exposed to much more
severe famine-induced acute malnutrition than wo-
men in urban areas.
A key assumption underlying this research was
that the childlessness observed among the Chinese
women in the two survey populations was caused by
biology, not by choice. Such an assumption typically
does not hold for late twentieth or twenty-first-
century populations because of their widespread use
of highly effective contraceptive measures. How-
ever, it is possible to identify particular populations,
such as the Hutterites (Larsen and Vaupel 1993) or
the Amish (Wood et al. 1994), who have very low
levels of contraceptive use and voluntary childless-
ness, and it is possible, as previously discussed, that
because of their unique cultural heritage the Chinese
population, even in recent years, may resemble the
Amish and the Hutterite populations in that all
couples desire to have at least one child. It is crucial,
when using observed childlessness as an indicator of
sterility, that such a universal desire can be assumed
amongst the study population. Were this assumption
not valid, and some of the childlessness observed
was the result of choice, the prevalence of child-
lessness would be influenced by socio-economic
factors, with a clear relationship being discernible
between the relevant socio-economic factors and the
level of observed childlessness (Bloom and Pebley
1982). The fact that no such relationship is present in
the four models reported in Table 4 suggests that the
assumption that the observed levels of childlessness
were the result of biology, rather than of choice, was
a valid one.
The effect of ‘age at marriage’ on sterility war-
rants further discussion. Inclusion of age at first
marriage in Models 3 and 4 shows a strong and
positive effect on sterility (Panel A). However, one
should not jump to the conclusion, based on the
statistically significant coefficients of ‘age at mar-
riage’, that late marriage caused an increase in the
risk of sterility. As previously discussed, the model
relationship could have been produced by several
different mechanisms and additional research is
needed to reach a more solid understanding of the
factors at play. The inclusion of age at marriage in
Table 4 (Continued)
Model 1 Model 2 Model 3 Model 4
Han ethnic majority 0.91*** 0.01***[0.88, 0.94] [0.99, 0.94]
AIC 68,733.8 68,733.6 68,502.9 68,495.7BIC 68,827.3 68,841.5 68,668.5 68,632.4N 9,878
*pB0.05, **pB0.01, ***pB0.001.Note: 95 per cent confidence intervals in square brackets.Source: 1 and 2 as for Table 2.
Long-term effect of famine on fecundity 303
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

Models 3 and 4 changed the influence of the ‘rural
residence’ variable from statistically significant in
Model 2 to non-significant in Models 3 and 4,
suggesting that the observed urban�rural difference
in the level of sterility was largely attributable to the
difference in the timing of marriage between urban
and rural areas (see Table 2). For the purposes of the
present study, it should be noted that controlling for
‘age at marriage’ has little impact on the key
coefficients.
Fecundability was influenced by both social andbiological factors
In contrast to the sterility results, variables repre-
senting educational attainment, ethnicity, place of
residence, birth cohort, and age at marriage all
demonstrate significant effects on fecundability
(Panel B), supporting the claim that fecundability
has both biological and behavioural components.
The frequency of sexual intercourse is a particularly
important behavioural factor (Weinstein and Stark
1994) but, because it is virtually impossible to
control for the frequency of intercourse in social
surveys, some of its effect on fecundability is
attributed to more general socio-economic factors.
The estimated cohort difference in fecundability
should not, therefore, be interpreted as a result of
famine exposure.
Model 4 shows a secular trend toward a shorter
interval between marriage and first birth developed
in both the urban and rural populations. This pattern
is consistent with other studies of China (Wang and
Yang 1996; Hong 2006) and is likely to have been
driven by the changes in marriage patterns, family
structure, and state family planning policy taking
place over the second half of the twentieth century.
Constructing the difference-in-differencesestimate of the in utero famine effect on women’ssterility
Although it is possible to extract the difference-in-
differences estimate of the in utero famine effect on
women’s sterility in adulthood directly from the
nonlinear probability models reported in Table 4 (Ai
and Norton 2003; Zelner 2009), linear probability
models provide much more straightforward alter-
natives. Table 5 reports such difference-in-differ-
ences estimates obtained from the best-fit linear
probability model, as well as their 95 per cent
confidence intervals.
To offer a more complete picture of the relation-
ship between in utero famine exposure and sterility
in adulthood, the new model included the 1959,
1962, and 1965�66 birth cohorts in addition to the
three birth cohorts represented in Table 4. Both the
1959 and 1962 birth cohorts experienced partial
exposure to the famine while in the womb, but the
1965�66 cohort, like the 1963�64 cohort, were
conceived after the famine was over. As Table 5
shows, five of the six difference-in-differences coef-
ficients are positive and only one of them (1962�rural residence) is negative. Among the five positive
coefficients, four have a 95 per cent confidence
interval including zero and only one (1960�61�rural residence) has a 95 per cent confidence interval
excluding zero. The only negative coefficient also
has a 95 per cent confidence interval including zero.
Based on these results it was concluded that,
compared to their counterparts who were not
exposed to the famine, female foetuses that spent
the whole of their period of gestation under famine
conditions faced an increased risk of experiencing
sterility as an adult of approximately 0.011 (i.e., an
increase of 1.1 sterile cases per 100 women), an
effect which is statistically significant. As previously
discussed, the presence of some rural-born women in
the urban sample means that the estimated differ-
ence-in-differences estimate reported in Table 5 is
likely to be biased downward. The true effect of in
utero famine exposure on sterility may, therefore, be
greater than 0.011. It was also concluded that being
exposed to famine in early childhood or for only part
of the 9 months of gestation, did not have a
statistically significant effect on sterility in adult-
hood.
The fact that the interaction term between the
1965�66 cohort and rural residence is not significant
increases confidence in the difference-in-differences
results. It provides additional evidence that in the
absence of famine conditions there was no real
urban�rural difference in women’s sterility.
Discussion
Using data from two large, nationally representative
surveys conducted in China in 1997 and 2001, this
study has shown that in utero exposure to the 1959�61 famine had a permanently damaging effect on
women’s fecundity. More specifically, exposure to
the famine while in the womb increased the risk of
women being sterile by 1.1 per cent. Given that
primary and permanent sterility is a rare phenom-
enon with an overall population prevalence only
304 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

slightly higher than 1 per cent in China (Liu et al.
2004), this is a substantial and important effect.
The unique strength of the present study comes
from the use of data from two large surveys of a
population in which the desire for at least one child
is universal (Scharping 2003), in combination with
the use of a difference-in-differences identification
strategy and mixture cure models, which can simul-
taneously model sterility and fecundability. The
significance of the findings is two-fold. First, by
showing the presence of a permanently damaging
effect of in utero exposure to famine on fecundity, an
important gap in our understanding of the develop-
mental origins of health and disease has been
bridged. Secondly, the results demonstrate the re-
levance and usefulness of the developmental origins
framework when seeking a better understanding of
population phenomena.
It may be pertinent to ask in the context of the
1959�61 famine whether, and to what extent, the
results of the analyses may have been influenced by
differential selection through mortality, fertility, or
both, since the members of the birth cohorts from
the famine years who survived to be interviewed in
1997 or 2001 constituted only a fraction of the
original cohorts. Selection effects in the context of
famine have been shown to be important in shaping
the subsequently observed cohort patterns of child
and adolescent mortality and of schizophrenia (Song
et al. 2009; Huang et al. 2010b; Song 2010). The
results shown above indicate that the famine cohort
had a higher sterility risk than both the pre-famine
and the post-famine cohorts. This suggests two
possibilities. The first is that the estimated differ-
ence-in-differences effect of in utero famine expo-
sure represents the lower bound of the true effect
because the famine survivors were more likely to
have been genetically well endowed and therefore to
have had higher-than-average reproductive perfor-
mance over their adult years. The second possibility
is that the estimated difference-in-differences coeffi-
cient represents the true effect of in utero exposure
to famine, in which case the factors that influenced a
woman’s reproductive function later in life were
unrelated to those determining her chance of
surviving the famine. In either case, the key finding
that in utero famine exposure increases the like-
lihood of sterility in adulthood remains valid.
Sterility, as defined in the present study, is a rare
phenomenon within a population. Despite the sta-
tistically significant coefficients reported in Tables 4
and 5, some reservations remain concerning the
substantive importance of such findings. After all,
a famine-induced increase in sterility of 1.1 per cent
is unlikely to change the population dynamics in
China significantly, so why are the findings impor-
tant?
Menken and Larsen (1994) provided the best
answer to this question. They argued that under-
standing the potential impact on population dy-
namics is the fourth most important reason to
study sterility. Their three most important reasons
were: the need to understand the effects of sterility
on the lives of affected individuals; the need to
estimate the prevalence of sterility within popula-
tions so that appropriate public health intervention
can be implemented; and the need to understand the
risk factors and causes with which sterility is
associated. The findings of the present study shed
light on all four areas of enquiry.
In many societies sterility and the resulting
involuntary childlessness cause women to be stigma-
tized, resulting in a great deal of pain and harm
(Miall 1985; Whiteford and Gonzalez 1995). Because
sterility does not have a clearly defined aetiology,
apart from those cases resulting from sexually
transmitted diseases, it is often viewed as the woman’s
fault, a punishment for her sins and wrongdoings.
The stigma is particularly great in societies with
strong pro-natalist cultures, such as China. The
Table 5 Difference-in-differences estimates of the effect of in utero exposure to the 1959�61 famine on the risk of sterilityin adulthood: results from the joint linear probability�log-normal cure fraction model using data combined from the 19971
and 20012 surveys
Cohort�place of residence Effect on the probability of sterility 95 per cent confidence intervals
1957�58�rural residence 0.0013 [�0.0088, 0.0114]1959�rural residence 0.0072 [�0.0072, 0.0247]1960�61�rural residence 0.0109 [0.0006, 0.0248]1962�rural residence �0.0055 [�0.0198, 0.0073]1963�64�rural residence � �1965�66�rural residence 0.0040 [�0.0065, 0.0175]Observations 17,095
Note: The 95 per cent confidence intervals were calculated using the bootstrap method.Source: 1 and 2 as for Table 2.
Long-term effect of famine on fecundity 305
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

present research has demonstrated for the first time
that of the 15 million women born in the rural areas
of China in 1960 and 1961, 110,000 were rendered
sterile by exposure to the 1959�61 famine while in
the womb. These 110,000 rural women have lived
their lives in the shadow of the famine.
The effects will follow them into old age because
the one-child policy, in combination with the pre-
dominantly family-based support system in rural
China, means that it will become increasingly
difficult to obtain adequate old-age support even
for those who have children (Wang 2011) and
virtually impossible for those who do not.
It should be acknowledged that this study has a
number of limitations and weaknesses. One is that
the lack of individual-level measures of famine-
induced malnutrition makes it difficult to attribute
the estimated effects directly to the causal influence
of in utero malnutrition. After all, acute malnutrition
is not the only adverse event that occurs during
famine; infectious disease and heightened stress may
have similar effects. While infectious disease is not
thought to have been widespread during or after
China’s 1959�61 famine because the state closely
monitored their incidence even during the famine
(Dikotter 2010), the lack of food would certainly
have caused heightened anxiety and stress, but there
are no direct measures of these factors. It can
therefore be said only that in utero famine exposure
increased the risk of sterility in women; the extent to
which this was a result of malnutrition of the foetus
in the womb, or of heightened maternal stress could
not be determined. Another piece of useful informa-
tion that is missing from the data is information on
women’s birth weight and length. Such measures can
be used as individual-level proxies for the famine-
induced malnutrition (as opposed to birth cohort
and urban�rural residence used in this study) to
obtain more fine-grained results. To the best of my
knowledge, none of the existing data sources have
the above-mentioned information and new data
collection efforts are necessary.
Notes
1 Shige Song is at Queens College and CUNY Institute
for Demographic Research, The City University of New
York, 65�30 Kissena Blvd., Queen’s, NY 11367, USA.
E-mail: [email protected]
2 An earlier version of this paper was presented at the
2010 annual meeting of the Population Association of
America.
References
Ai, C. and E. C. Norton. 2003. Interaction terms in logit
and probit models, Economics Letters 80(1): 123�129.
Aitkin, M. 1996. A general maximum likelihood analysis
of overdispersion in generalized linear models, Statistics
and Computing 6(3): 251�262.
Ashton, B., K. Hill, A. Piazza, and R. Zeitz. 1984. Famine
in China, 1958�61, Population and Development
Review 10(4): 613�645.
Bloom, D. E. and A. R. Pebley. 1982. Voluntary child-
lessness: a review of the evidence and implications,
Population Research and Policy Review 1(3): 203�224.
Bongaarts, J. 1980. Malnutrition and fecundity, Studies in
Family Planning 11(12): 401�406.
Cai, Y. and F. Wang. 2005. Famine, social disruption, and
involuntary fetal loss: evidence from Chinese survey
data, Demography 42(2): 301�322.
Caldwell, J. C. 1994. How is greater maternal education
translated into lower child mortality, Health Transition
Review 4(2): 224�229.
Chen, J., Z. Xie, and H. Liu. 2007. Son preference, use of
maternal health care, and infant mortality in rural
China, 1989�2000, Population Studies 61(2): 161�183.
Chen, Y. and L. A. Zhou. 2007. The long-term health and
economic consequences of the 1959�1961 famine in
China, Journal of Health Economics 26(4): 659�681.
Choe, M. K. and N. O. Tsuya. 1991. Why do Chinese
women practice contraception? The case of rural
Jilin Province, Studies in Family Planning 22(1):
39�51.
Collins, J. A., W. Wrixon, L. B. Janes, and E. H. Wilson.
1983. Treatment-independent pregnancy among infer-
tile couples, New England Journal of Medicine 309(20):
1201�1206.
De Angelis, R., R. Capocaccia, T. Hakulinen, B. Soderman,
and A. Verdecchia. 1999. Mixture models for cancer
survival analysis: application to population-based data
with covariates, Statistics in Medicine 18(4): 441�454.
Den Bandt, M. L. 1980. Voluntary childlessness in the
Netherlands, Journal of Family and Economic Issues
3(3): 329�349.
Desai, S. and S. Alva. 1998. Maternal education and child
health: is there a strong causal relationship?,
Demography 35(1): 71�81.
Dikotter, F. 2010. Mao’s Great Famine: The History of
China’s Most Devastating Catastrophe, 1958�1962. New
York: Walker.
Dunson, D. B. and H. Zhou. 2000. A Bayesian model for
fecundability and sterility, Journal of the American
Statistical Association 95(452): 1054�1062.
Elias, S. G., P. A. H. van Noord, P. H. M. Peeters, I. den
Tonkelaar, and D. E. Grobbee. 2005. Childhood ex-
posure to the 1944�1945 Dutch Famine and subsequent
306 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

female reproductive function, Human Reproduction
20(9): 2483�2488.
Fang, K., Q. Deng, and E. Gao. 1993. Analysis of infertility
rate among firstly married Chinese women during
1976�1985, Reproduction and Contraception 4(2):
148�155.
Farewell, V. T. 1982. The use of mixture models for the
analysis of survival data with long-term survivors,
Biometrics 38(4): 1041�1046.
Gardner, D. S., S. E. Ozanne, and K. D. Sinclair. 2009.
Effect of the early-life nutritional environment on
fecundity and fertility of mammals, Philosophical
Transactions of the Royal Society B: Biological Sciences
364(1534): 3419�3427.
Gluckman, P. D., M. A. Hanson, H. G. Spencer, and P.
Bateson. 2005. Environmental influences during devel-
opment and their later consequences for health and
disease: implications for the interpretation of empirical
studies, Proceedings of the Royal Society B: Biological
Sciences 272(1564): 671�677.
Heckman, J. J. and J. R. Walker. 1990. Estimating
fecundability from data on waiting times to first
conception, Journal of the American Statistical
Association 85(410): 283�294.
Hong, Y. 2006. Marital decision-making and the timing of
first birth in rural China before the 1990s, Population
Studies 60(3): 329�341.
Huang, C., Z. Li, K. M. Venkat Narayan, D. F. Williamson,
and R. Martorell. 2010a. Bigger babies born to women
survivors of the 1959�1961 Chinese famine: a puzzle
due to survival selection?, Journal of Developmental
Origins of Health and Disease 1(6): 412�418.
Huang, C., Z. Li, M. Wang, and R. Martorell. 2010b. Early
life exposure to the 1959�1961 Chinese famine has
long-term health consequences, Journal of Nutrition
140(10): 1874�1878.
Kallan, J. and J. R. Udry. 1986. The determinants of
effective fecundability based on the first birth interval,
Demography 23(1): 53�66.
Kung, J. K. and J. Y. Lin. 2003. The causes of China’s Great
Leap Famine, 1959�1961, Economic Development and
Cultural Change 52(1): 51�73.
Lambert, P. C. 2007. Modeling of the cure fraction in
survival studies, Stata Journal 7(3): 351�375.
Lambert, P. C., P. W. Dickman, C. L. Weston, and J. R.
Thompson. 2010. Estimating the cure fraction in
population-based cancer studies by using finite mixture
models, Journal of the Royal Statistical Society: Series C
(Applied Statistics) 59(1): 35�55.
Larsen, U. and J. Menken. 1989. Measuring sterility from
incomplete birth histories, Demography 26(2): 185�201.
Larsen, U. and J. W. Vaupel. 1993. Hutterite fecundability
by age and parity: strategies for frailty modeling of
event histories, Demography 30(1): 81�102.
Larsen, U. 2000. Primary and secondary infertility in sub-
Saharan Africa, International Journal of Epidemiology
29(2): 285�291.
Lavely, W. R. 1986. Age patterns of Chinese marital
fertility, 1950�1981, Demography 23(3): 419�434.
Leridon, H. 1981. Fertility and contraception in 12
developed countries, International Family Planning
Perspectives 7(2): 70�78.
Lin, J. Y. and D. T. Yang. 2000. Food availability,
entitlements and the Chinese famine of 1959�61, The
Economic Journal 110(460): 136�158.
Liu, J., U. Larsen, and G. Wyshak. 2004. Prevalence of
primary infertility in China: in-depth analysis of
infertility differentials in three minority province/
autonomous regions, Journal of Biosocial Science
37(1): 55�74.
Lumey, L. H. and A. D. Stein. 1997. In utero exposure to
famine and subsequent fertility: the Dutch Famine
Birth Cohort Study, American Journal of Public Health
87(12): 1962�1966.
Maller, R. A. and X. Zhou. 1996. Survival Analysis with
Long-Term Survivors. New York: Wiley.
Menken, J., J. Trussell, and U. Larsen. 1986. Age and
infertility, Science 233(4771): 1389�1394.
Menken, J. and U. Larsen. 1994. Estimating the incidence
and prevalence and analyzing the correlates of inferti-
lity and sterility, Annals of the New York Academy of
Sciences 709(1): 249�265.
Miall, C. E. 1985. The stigma of involuntary childlessness,
Social Problems 33(4): 268�282.
Mooney, C. Z., R. D. Duval, and R. Duval. 1993.
Bootstrapping: A Nonparametric Approach to Statistical
Inference. Newbury Park, CA: Sage.
Moors, H. G. 1978. The Netherlands Survey on Fertility
and Parenthood Motivation, 1975: a summary of
findings, in International Statistical Institute/Word Ferti-
lity Survey. Voorburg, the Netherlands.
Mu, R. and X. Zhang. 2010. Why does the Great Chinese
Famine affect the male and female survivors differ-
ently? Mortality selection versus son preference,
Economics & Human Biology 9(1): 92�105.
Painter, R. C., R. G. J. Westendorp, S. R. de Rooij, C.
Osmond, D. J. P. Barker, and T. J. Roseboom. 2008.
Increased reproductive success of women after prenatal
undernutrition, Human Reproduction 23(11): 2591�2595.
Peng, X. 1987. Demographic consequences of the Great
Leap Forward in China’s provinces, Population and
Development Review 13(4): 639�670.
Puhani, P. A. 2008. The treatment effect, the cross
difference, and the interaction term in nonlinear ‘differ-
ence-in-differences’ models, IZA Discussion Papers.
Raftery, A. E. 1995. Bayesian model selection in social
research, Sociological Methodology 25: 111�164.
Long-term effect of famine on fecundity 307
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014

Ross, C. E. and C. Wu. 1995. The links between education
and health, American Sociological Review 60(5): 719�745.
Scharping, T. 2003. Birth Control in China 1949�2000:
Population Policy and Demographic Development. New
York: Routledge.
Schmidt, P. and A. D. Witte. 1989. Predicting criminal
recidivism using ‘split population’ survival time models,
Journal of Econometrics 40(1): 141�159.
Short, S. E., L. Ma, and W. Yu. 2000. Birth planning and
sterilization in China, Population Studies 54(3): 279�291.
Song, S. 2004. Marriage Formation in Contemporary China.
Los Angeles: University of California, Los Angeles.
Song, S., W. Wang, and P. Hu. 2009. Famine, death, and
madness: schizophrenia in early adulthood after pre-
natal exposure to the Chinese Great Leap Forward
Famine, Social Science & Medicine 68(7): 1315�1321.
Song, S. 2010. Mortality consequences of the 1959�1961
Great Leap Forward Famine in China: debilitation,
selection, and mortality crossovers, Social Science &
Medicine 71(3): 551�558.
Song, S. and S. A. Burgard. 2011. Dynamics of inequality:
mother’s education and infant mortality in China,
1970�2001, Journal of Health and Social Behavior
52(3): 349�364.
Song, S. 2012. Does famine influence sex ratio at birth?
Evidence from the 1959�1961 Great Leap Forward
Famine in China, Proceedings of the Royal Society B:
Biological Sciences 279(1739): 2883�2890.
Sposto, R. 2002. Cure model analysis in cancer: an
application to data from the Children’s Cancer Group,
Statistics in Medicine 21(2): 293�312.
State Statistical Bureau. 1991. Statistical Yearbook of
China 1991. Beijing: State Statistical Press.
Stein, Z. 1975. Famine and Human Development: The
Dutch Hunger Winter of 1944�1945. New York: Oxford
University Press.
Trussell, J. and C. Wilson. 1985. Sterility in a population
with natural fertility, Population Studies 39(2): 269�286.
Walker, K. R. 1984. Food Grain Procurement and Con-
sumption in China. New York: Cambridge University
Press.
Wang, F. and Q. Yang. 1996. Age at marriage and the first
birth interval: the emerging change in sexual behavior
among young couples in China, Population and Devel-
opment Review 22(2): 299�320.
Wang, F. 2011. The future of a demographic overachiever:
long-term implications of the demographic transition in
China, Population and Development Review 37(s1):
173�190.
Weinstein, M., J. W. Wood, M. A. Stoto, and D. D.
Greenfield. 1990. Components of age-specific fecund-
ability, Population Studies 44(3): 447�467.
Weinstein, M. and M. Stark. 1994. Behavioral and
biological determinants of fecundability, Annals of the
New York Academy of Sciences*Paper Edition 709:
128�144.
Whiteford, L. M. and L. Gonzalez. 1995. Stigma: the
hidden burden of infertility, Social Science & Medicine
40(1): 27�36.
Wood, J. W. 1994. Dynamics of Human Reproduction:
Biology, Biometry, Demography. New York: Aldine.
Wood, J. W., D. J. Holman, A. I. Yashin, R. J. Peterson, M.
Weinstein, and M. C. Chang. 1994. A multistate model
of fecundability and sterility, Demography 31(3): 403�
426.
Wrigley, E. A. 1997. English Population History from
Family Reconstitution, 1580�1837. New York: Cam-
bridge University Press.
Zelner, B. A. 2009. Using simulation to interpret results
from logit, probit, and other nonlinear models, Strategic
Management Journal 30(12): 1335�1348.
Zhang, G. and Z. Zhao. 2006. Reexamining China’s
fertility puzzle: data collection and quality over the
last two decades, Population and Development Review
32(2): 293�321.
308 Shige Song
Dow
nloa
ded
by [
Uni
vers
ity o
f C
olor
ado
at B
ould
er L
ibra
ries
] at
12:
16 1
9 D
ecem
ber
2014