Embed Size (px)
DESCRIPTION
Assessment and treatment of severe personality disorders in adolescence. ISSPD Congress 2007 The Hague, September 19 Joost Hutsebaut, Kirsten Catthoor, and Dineke Feenstra. What do you know about personality disorders in adolescence??? Let’s start with a little quiz…. Thesis 1. - PowerPoint PPT Presentation
Citation preview

Assessment and treatment of severe personality disorders in
adolescence
ISSPD Congress 2007
The Hague, September 19
Joost Hutsebaut, Kirsten Catthoor, and Dineke Feenstra

What do you know about personality disorders in
adolescence???
Let’s start with a little quiz…

Thesis 1
• In DSM-IV-TR (2000), age is no criterion for the diagnosis of personality disorders.
• In other words, clinicians are allowed to give a diagnosis of PD to a minus 18-years old.

Multiple choice 1
• A. True in all cases
• B. True in all cases except for the diagnosis of antisocial PD
• C. Only true for the borderline PD
• D. Not true

Answer 1
• The correct answer is B.
• DSM-IV-TR p. 687
• There is no age criterion for the diagnosis of PD in DSM-IV-TR, except for the antisocial PD.

Thesis 2
• The prevalence of borderline PD in adults and adolescents is about the same.

Multiple choice 2
• A. Not true, the prevalence of borderline PD is higher in adults.
• B. Not true, the prevalence of borderline PD is higher in adolescents.
• C. True
• D. There is no information on this.

Answer 2
• The correct answer is C.
• There is empirical evidence that the prevalence of borderline PD is (more or less) the same in adults and adolescents in as well a community as a clinical sample.
• 14.4% of ‘community’ adolescents can be diagnosed with a PD.

Thesis 3
• The diagnosis of BPD in adolescence predicts more axis 1 and axis 2 disorders in early adulthood.

Multiple choice 3
• A. True.
• B. Only true for axis 1, not for axis 2.
• C. Only true for axis 2, not for axis 1.
• D. Not true.

Answer 3
• The correct answer is A: the diagnosis of PD in adolescence predicts as well axis 1 as axis 2 disorders in early adulthood.
• Axis 1 disorders are a highly sensitive marker for the seriousness of the PD.

Thesis 4
• What is the most specific feature of a borderline PD in adolescence?

Multiple choice 4
• A. Impulsivity.
• B. Instability of affect.
• C. Identity confusion.
• D. Suicidal ideation and gestures.

Answer 4
• The correct answer is B.
• The most typical feature of borderline PD in adolescents is instability of affect, in adults it is impulsivity.

Thesis 5
• 4 to 20% of adult patients in an inpatient setting self mutilates. What is the percentage of self injurious behavior in adolescents in an inpatient treatment setting?

Multiple choice 5
• A. Less than adults, 5 to 10%.
• B. The same as adults, 10 to 20%.
• C. A little more than adults, 25-40%.
• D. Much more than adults, 40-60%.

Answer 5
• The correct answer is D.
• 90% of all self injurious behavior happens in adolescence.

Case Study
(Because of privacy reasons this information has been omitted)

Psychotherapy in PD adolescents?
• Review of 25 empirically supported psychotherapies in adolescents (Weisz and Hawley, 2002)– 14 effective– 7 ‘adult’ models, 6 ‘child’ models– 1 ‘adolescent’ model
• Review of 34 studies of CBT in adolescents (Holmbeck et al., 2003)– 9 (26%) involved developmental issues– 1 studied a developmental factor as moderator of outcome
• PD in adolescence? – No RCT’s– No age-specific treatment guidelines– Few treatment manuals (Bleiberg, 2001), Miller et al (2007),
Freeman and Reinecke (2007)

Psychotherapy in PD adolescents?
• Conclusion– No evidence based adolescence-oriented
psychotherapy models for PD– Almost no well developed treatment manuals– No age-specific practice guidelines (APA etc)
• Challenging!

What are our objectives today?• Proposal of practice guidelines for the assessment and
treatment of severe PD in adolescents (mainly cluster B)– Pragmatically: how to design a concrete treatment
trajectory– Systematically: from intake to follow-up– Not restricted to one theoretical frame
• Based on: – Literature and evidence based results of research on
PD in adults– Available literature on (treatment of) PD in
adolescence – Literature on developmental psycho(patho)logy in
adolescence – Our clinical experiences with PD adolescents

Structure of the workshop
• Assessment of PD in adolescence– Empirical research on PD in adolescence– Assessment of PD in adolescence and indication for
treatment setting
• Designing a flexible treatment trajectory– Preparation phase– Integrative, adolescence-specific, treatment, including
psychotherapy, system therapy and pharmacotherapy– Relapse prevention and follow-up

Structure of the workshop
• Assessment of PD in adolescence– Empirical research on PD in adolescence– Assessment of PD in adolescence and indication for
treatment setting
• Designing a flexible treatment trajectory– Preparation phase– Integrative, adolescence-specific, treatment, including
psychotherapy, system therapy and pharmacotherapy– Relapse prevention and follow-up

Empirical research on PD in adolescence
• Is it allowed to give a diagnosis of PD to an adolescent?
• Is it wise to give a diagnosis of PD to an adolescent?
• How often do PD occur in adolescence?
• How do PD develop throughout adolescence?

Is it allowed to give a diagnosis of PD to an adolescent?
• DSM‑IV‑TR (APA, 2000, p. 687): – PD can be diagnosed in adolescents
• Clinicians should be careful• Symptoms have to be present during 1 year• Exception: antisocial PD should not be
diagnosed before the age of 18 yrs
• How well is this known in the field???

Is it wise to give a diagnosis of PD to an adolescent?
• This is also an empirical issue– Can PD be diagnosed in a reliable way in
adolescence?– Is it a valid diagnosis?
• Diagnosis refers to the same characteristics• Diagnosis correlates with similar associated
problems • Diagnosis predicts similar problems in the
future• Diagnosis has some stability over time

Is it wise to give a diagnosis of PD to an adolescent? 1. Reliability
• There are as many PD adolescents as PD adults in a clinical sample (Westen, Shedler
et al., 2003; Grilo, McGlashan et al., 1998) and in a community sample (Johnson, Cohen et al., 2000).
• Almost all specific PD occur in the same frequency
• Exception: antisocial and avoidant PD
• These PD adolescents show a similar pattern of co-morbidity
• 2/3 between 2 and 9 PD diagnoses in a clinical sample• 50% 2 or more in a community sample

Is it wise to give a diagnosis of PD to an adolescent? 2. Construct validity
• EFA on all PD symptoms gives evidence for 10 empirically derived factors, similar to DSM IV PD categories (Durrett & Westen, 2005)
• Q analysis based on clinical descriptions gives evidence for similar categories of PD in adults and adolescents (Westen, Shedler et al., 2003)
• EFA on personality symptoms (DIPSI, SIPP) has a similar structure in adolescents as in adults (De Clercq et al., 2006; Feenstra et al., 2007)
Personality pathology in adolescence has a similar structure as personality pathology in adults

Is it wise to give a diagnosis of PD to an adolescent? 3. Concurrent validity
• PD diagnosis in adolescence is associated with: – More suicidal ideation and acts (Westen et al., 2003; Braun-
Scharm, 1996)– More problems at school and less friends (Westen en al., 2003)– More behavioral problems and problems at school (Johnson et al.,
2005)– Alcohol abuse, smoking and illegal drug abuse (Serman et al.,
2002)– More sexual partners and high risk sexual contacts (Lavan &
Johnson, 2002)– More violent acts (assault, burglary, initiating fights, threatening)– More MH service use, more medication use (Kasen et al., 2007)

Is it wise to give a diagnosis of PD to an adolescent? 4. Predictive validity
• PD diagnosis in adolescence predicts: – Subsequent failure in school (Johnson et al., 2005)– More negative affects, distress, problems in social support, living,
mobility, finances and health in adulthood (Chen et al., 2006)– More health problems, more problematic social contacts, less
psychological wellbeing and more adversities in early adulthood (Chen et al., 2006)
– More conflicts with family members in early adulthood (Johnson et al., 2004)
– More depression in early adulthood (Daley et al., 1999)– More interpersonal stress in early adulthood (Daley et al., 2006)– More relational dysfunctioning in romantic relations (Daley et al.,
2000)– More anxiety, mood and substance abuse disorders in early
adulthood (Johnson et al., 1999)– More illegal dugs abuse and crisis intervention (Levy et al., 1999)

Is it wise to give a diagnosis of PD to an adolescent? Differences
– Internal consistency of PD criteria of a given PD is generally lower in adolescence than in adulthood (except for BPD and dependent PD) (Becker et al., 2001)
– The overlap of criteria from different PDs is larger, suggesting a more diffuse range of psychopathology (Becker et al., 1999)
– There is evidence for more co-morbidity between different (A, B, C) clusters (Becker et al., 2000)

BPD in adolescence
• Frequency of BPD and BPD traits is similar in adolescent and adult clinical sample (Becker et al., 2002)
• Symptoms and phenomenology of BPD is similar for adolescent girls and adults (Bradley et al., 2005)
• Internal consistency of BPD criteria in adolescence is high (.76) (Becker et al., 1999)
• Q analysis gives evidence for similar subgroups of BPD girls as in adults (Bradley et al., 2005)

BPD in adolescents: Types and associated axis 1 disorders• Different types of BPD (Bradley et al., 2005)
– High functioning and internalizing– Histrionic– Depressive internalizing– Angry and externalizing case study
• Associated axis 1 disorders (Becker, 2006)
– Suicidal gestures and emptiness (depressive disorders and alcohol abuse disorders)
– Affective instability, uncontrolled anger and identity disturbance (anxiety disorder and conduct disorder)
– Unstable relationships and fear of abandonment (anxiety disorder)
– Impulsivity and identity disturbance (conduct disorder and substance abuse disorder)

BPD in adolescence: some differences
• Individual BPD criteria have a higher general positive predictive power than in adults (1 symptom generally predicts better the overall disorder)
• Fear of abandonment is the best inclusion criterion in adolescence (if present, high predictive power for BPD)
• Uncontrolled anger is for adolescents the best exclusion criterion, for adults impulsivity (if absent, no BPD)
• Taken together is affective instability for adolescents and impulsivity for adults the most useful criterion.

Prevalence of PD in adolescence
• PD 14,4% (CIC study)• Cluster A 5,9%
– Paranoid 3,3%– Schizoid 1,1%– Schizotypal 1,7%
• Cluster B 7,1%– Borderline 2,4%– Histrionic 2,5%– Narcissistic 3,1%
• Cluster C 4,9%– Avoidant 2,0%– Dependent 2,2%– Obsessive-compulsive 1,1%

Course of PD in adolescence
• CIC-study– PD traits decrease with 28% between adolescence and
early adulthood (Johnson et al., 2000)– Stability is lowest between 14 and 16 yrs (Johnson et al.,
2000)• Clinical samples
– Modest stability for dimensional measures of personality pathology (Daley et al., 1999; Grilo et al., 2001)
– After two yrs: 74% diagnosis PD (83% girls, 56% boys); stability of specific PD is low (Chanen et al., 2004)
– Stability is high for schizoid and antisocial PD; modest for borderline, histrionic and schizotypal PD and low for other Pds (Chanen et al., 2004)

Is it wise to give a diagnosis of PD to an adolescent? General conclusions
• The diagnosis of PD can be made in a reliable way in adolescence• About 10-15% of adolescents have a PD• The diagnosis of PD in adolescence has excellent concurrent
validity: it is associated with many parameters of distress and dysfunctioning.
• The diagnosis of PD has modest predictive validity. It reliably predicts dysfunctioning in the future, but the diagnostic stability of specific PD categories is rather small. Diagnostic stability of the general PD diagnosis on the other hand is good.
• As in adults, co-morbidity is high, but probably broader (encompassing aspects of other PD clusters).
• BPD in adolescents has got excellent internal consistency, construct validity and concurrent validity.
• There is evidence that the weaker stability of BPD can be ascribed mainly to the instability of the affective and impulsive symptoms.

How to conceive personality disorders?
• PD is a chronic condition of structural vulnerability, that develops from early childhood through adolescence into adulthood and that expresses itself in interaction with a changing environment in a fluctuating pattern of maladaption. – Chronic condition, but fluctuating expression– Expression depends on context– Expression might depend on developmental
factors– Different developmental pathways, starting from
childhood

Structure of the workshop
• Assessment of PD in adolescence– Empirical research on PD in adolescence– Assessment of PD in adolescence and indication for
treatment setting
• Designing a flexible treatment trajectory– Preparation phase– Integrative, adolescence-specific, treatment, including
psychotherapy, system therapy and pharmacotherapy– Relapse prevention and follow-up

AssessmentGeneral remarks
• Use of multiple informants (parents, teachers, children)
• Attitude of the clinician
• Assessment should be evidence based
• Aim not only diagnostic assessment, but also to increase the motivation of the patient

AssessmentDevelopmental history
• Indicators of high risk for the development of personality disorders

AssessmentIntelligence
• Importance of intelligence testing
Case: Kaufman Adolescent and Adult Intelligence Test (KAIT)
Total
-
Crystallized Definitions Aud. Compreh. Double mean.
110 (75) 12 11 12
Fluid Rebus learning Logical steps Mystery codes
92 (30) 8 10 8

AssessmentNeuropsychological testing
• Gives additional information to validate the diagnosis of a PD
• Indicates the impact of a PD

AssessmentSymptoms
Case: Brief Symptom Inventory (BSI)Scale Description Score Norm patients Norm population
SOM Somatization 0.429 Below average Above average
O-C Obsessive-Compulsive 1.667 Above average High
I-S Interpersonal Sensivity 1.25 Average High
DEP Depression 2.0 Above average Very high
ANX Anxiety 2.333 High Very high
HOS Hostility 2.8 Very high Very high
PHOB Phobic Anxiety 0.8 Average High
PAR Paranoid Ideation 2.4 High Very high
PSY Psychoticism 1.8 High Very high
GSI Global Severity Index 1.717 Above average Very high
PST Positive Symptom Total 34.0 Average High
PSDI Positive Symptom Distress Index 2.676 High Very high

AssessmentSymptoms
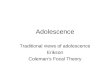
Case: Child Behaviour Checklist (CBCL)
50
60
70
80
90
100
Intern. Extern. Total
BiologicalfatherStepmother

AssessmentAxis I
Case: Anxiety Disorders Interview Schedule for DSM-IV, Child Version (Adis-C), Complemented with modules from the Structured Clinical Interview for DSM-IV axis I disorders (SCID-I)
Diagnosis axis I:- Posttraumatic stress disorder- Substance dependence- Conduct disorder

AssessmentAxis II
Case: Structured Clinical Interview for DSM-IV axis II Personality Disorders (SCID-II)
Diagnosis axis II: Borderline Personality Disorder- Frantic efforts to avoid real or imagined abandonment- A pattern of unstable and intense interpersonal relationships characterized by
alternating between extremes of idealization and devaluation- Identity disturbance- Impulsivity- Recurrent suicidal behavior, gestures or threats, or self-mutilating behavior- Affective instability- Chronic feelings of emptiness- Inappropriate, intense anger or difficulty controlling anger- Transient, stress-related paranoid ideation or severe dissociative symptoms

AssessmentSpecific borderline characteristics
• Suicide Risk Assessment
• Assessment of dissociation
Case: Diagnostic Interview for Borderlines (DIB-R), included in Clinical Interview

AssessmentStructural characteristics
Case: Questionnaires
• NEO-PI-R
0123456789Neuro
Extra
OpenAltrui
Conscient

AssessmentStructural characteristics
Case: Projective tests (Rorschach)

AssessmentCompetence
Case: Competentie Belevingsschaal voor Adolescenten (CBSA), derived from the Self-Perception Profile for Adolescents (SPPA)
Sv Sa Sp Fv Gh Hv Ge
Scale scores 17 18 6 19 8 15 15
Percentile 95 82 4 97 3 16 48

AssessmentFamily
Case: Family Assessment Device (FAD)
Scale Stepmother Patient Father
Problem solving 2,667 3,000 3,167
Communication 3,000 2,556 2,667
Role fulfillment 2,636 2,273 2,272
Affective respons 3,000 2,833 3,000
Affective involvement 2,714 2,429 3,429
Family culture 2,667 2,667 2,667
Global functioning 3,083 2,917 3,167

AssessmentConclusions case
• Patient is diagnosed with a BPD on axis 2 and an associated PTSD, conduct disorder and substance dependence on axis 1.
• Underlying we see a low-level borderline organization: identity is fragmented, object representation are split, reality testing is fragile, defenses are immature.
• Nevertheless, we also see some adaptive coping mechanisms and a good self-reflexive capacity during the assessment.
• Because of her traumatically developed attachment, patient is unable to experience any form of ‘ safe’ intimacy or nearness.
• When stress increases (e.g. in case of approaching separation) patient loses the capacity to reflect and her adaptive coping mechanisms. She then turns to maladaptive coping mechanisms, like splitting, and aggressive and anti-social behavior to restore the lost balance. This antisocial behavior has to be understood as a way to protect her autonomy and her ‘self’ against unbearable feelings provoked by intimacy and related fear for abandonment.

From assessment to indication: levels of treatment setting
• Outpatient treatment
• Partial hospitalization
• Brief inpatient hospitalization
• Extended inpatient hospitalization

Indication for treatment setting: Considerations about case study• Based on APA guidelines: extended inpatient treatment
– Persistent risk behavior– Severe symptoms interfering with family and school life– Risk of assaultive behavior towards others– Co-morbid substance abuse
• Based on extra adolescent considerations (Bleiberg, 2001): extended inpatient treatment– Insufficient resources to provide a safe environment at home– Need for more structure and support
• Based on clinical experience– There is a serious pitfall that she cannot deal with the pressure
for attachment in an inpatient setting (psychological testing)

Structure of the workshop
• Assessment of PD in adolescence– Empirical research on PD in adolescence– Assessment of PD in adolescence and indication for
treatment setting
• Designing a flexible treatment trajectory– Preparation phase– Integrative, adolescence-specific, treatment, including
psychotherapy, system therapy and pharmacotherapy– Relapse prevention and follow-up

Designing a flexible treatment trajectory
• Treatment should be seen as a continuous trajectory– During different years (2-5 years)– With changing intensity
• Stepped up and down: – Preparation phase focused at psycho-education and
motivation, crisis management and context regulation– A residential phase to decrease stress at home and start a
therapeutic process– A day treatment phase to strengthen the achievements and
anchoring them in real life– A follow-up of booster sessions to support the internalized
therapeutic process
• Involving psychotherapy, system therapy and pharmacotherapy

Designing a flexible treatment trajectory
Assessment
Psychotherapy
Psycho-education
Commitment
Preparation phase
Treatment phase
System therapy
Post treatmentphase
Context regulationCrisis management
Pharmacotherapy

Structure of the workshop
• Assessment of PD in adolescence– Empirical research on PD in adolescence– Assessment of PD in adolescence and indication for
treatment setting
• Designing a flexible treatment trajectory– Preparation phase– Integrative, adolescence-specific, treatment, including
psychotherapy, system therapy and pharmacotherapy– Relapse prevention and follow-up

Preparation phase: goals
• Psycho education
• Context regulation
• Crisis management plan

Preparation phase: methods for psycho-education
• Psycho-education is a necessary part of the treatment of PD (APA guidelines)
• Explanation about the symptoms, the origin and the course of the disorder, and the possibilities of treatment.
• Giving hope. It is not about ‘learning to live with the disorder’, but about ‘curing’.
• For patients and their family there’s often relief that the problems have a name, so they can start to understand them.
• Psycho-education helps to bring order in the chaos

Preparation phase: methods for psycho-education
• Practical tips:– Try to use the language adolescents are
familiar with. Words like ‘psychiatric illness’ can be frightening.
– Mind the intelligence and cognitive skills of the adolescent and the parents and adapt your explanation to their limitations
– It might be necessary to dose the information and plan different sessions

Preparation phase: methods for psycho-education
• Examples of standardized sentences for explaining the diagnosis:– You came here because you have problems for quite
a while and treatment didn’t help you enough so far.– We’ve had several sessions with you and your
parents and asked you to participate in some psychological testing.
– We think it’s important to find out what is really going on, in order to suggest a treatment designed for the problems you have

Preparation phase: methods for psycho-education
– Your problems can be understood as making part of a (borderline) personality disorder.
– Easily speaking, it means that you have difficulties in dealing with your self, with your feelings, thoughts and behavior, and difficulties in contacts with other people.
– A borderline PD consists of 9 characteristics, 5 is enough for the diagnosis. This means that every patient with a borderline PD is different from every other patient.
– We now want to give you some information about the characteristics. Do you agree with that?

Preparation phase: methods for psycho-education
• Fear of abandonment:– You are afraid that people will drop you.– You are convinced that people don’t care for you and
that you’re worth nothing.– You will do everything to avoid people leaving you, for
example sending text messages all the time, insisting on your contacts on MSN
– People get irritated, feeling of being suffocated en they will try to avoid your claim
– So what happens is just that scenario where you are so afraight of

Preparation phase: methods for psycho-education
• Affect instability:– You feel like your affect is never stable, you can never
be happy for some longer time– Sometimes you feel so depressed en sad that suicide
is all you can think of, and 1 minute later you are euphoric en busy
– You are easily irritated and your parents have the feeling they have to tread on eggs when you’re at home

Preparation phase: methods for psycho-education
• From the psychological testing we learned that you have a splitted inner world, with anger and emptiness as the only possible ways of expressing your feelings.
• This means that your emotions are not easily accessible, and it is very difficult for you to differentiate what you really feel and experience. You don’t have tools to make your inner feelings more comprehensible for yourself.

Preparation phase: methods for psycho-education
• You are very frightened, and you can only control that feeling by showing aggression.
• It is very difficult for you to make a difference between experiences in reality, and what you feel inside. F.e. when your therapist sets limits, when you are thinking of the humiliations of your stepfather, you will not always be able to make a distinction between these 2 situations. You will confuse your inner and outer world.

Preparation phase: methods for psycho-education
• Because you are impulsive, as well in changing schools, living with your parents, using drugs and alcohol, as having sex with boys, there is a chance that you will be impulsive in terminating the treatment also.
• It will be important to focus on that when it’s difficult for you to fully cooperate.

Preparation phase: methods for psycho-education
• You find it very difficult when people want to make close contact with you. You do not trust intimate relationships. You prefer to break contact yourself, to avoid that people will leave you.
• Therefore it will be extremely important to keep that pattern in mind in the relationship with your therapists.

Preparation phase: goals
• Psycho-education
• Context regulation
• Crisis management plan

Preparation phase: methods for context regulation
• What should be arranged for the treatment to be able to start? – Financially– Juridical– Mobility (transport to treatment setting)– Structured daily activity (in case of outpatient) – Safe weekend destination (in case of
inpatient)

Preparation phase: methods for context regulation
• How can continuity before, during and after treatment be improved? – Contact with referring psychiatrist/psychologist– Contact with school– Home visit by social worker– Social network, neighborhood etc
• Use a clear therapeutic frame– What rules about drugs and alcohol? – Give an information sheet with basis rules,
expectancies, treatment methods

Preparation phase: goals
• Psycho-education
• Context regulation
• Crisis management plan

Preparation phase: methods for crisis management
• Severe PD lead almost by definition to crises during treatment.• Crises give agitation and can interfere with countertransference,
leading to splitting in a team.• Designing a plan for crisis management gives control and
predictability• The goal is to stabilize the crisis so the treatment process is not
jeopardized• Make clear agreements with patient and parents in advance,
specifically about the availability of therapists• Give clear roles to staff members in dealing with the crisis: medical
care, psychological care, decision about transfer to other setting• Agree with patient and parents on a plan for crisis management
during the weekend or evening. Put it on paper.

Structure of the workshop
• Assessment of PD in adolescence– Empirical research on PD in adolescence– Assessment of PD in adolescence and indication for
treatment setting
• Designing a flexible treatment trajectory– Preparation phase– Integrative, adolescence-specific, treatment, including
psychotherapy, system therapy and pharmacotherapy– Relapse prevention and follow-up

Designing a flexible treatment trajectory
Assessment
Psychotherapy
Psycho-education
Commitment
Preparation phase
Treatment phase
System therapy
Post treatmentphase
Context regulationCrisis management
Pharmacotherapy

Designing an integrative, adolescence-specific treatment
• Psychotherapy is treatment of first choice– Dialectical Behavior Therapy– Mentalization Based Treatment– (Schema Focused Therapy)
• Pharmacotherapy should be considered as an ‘enabler’ of psychotherapy
• System therapy is a necessary complement of psychotherapy in adolescence

Some general remarks about psychotherapy for severe PD
• Two evidence based models for treating BPD in adults (Cochrane review, 2006)– Dialectical Behavior Therapy (Linehan, 1991)– Mentalization Based Treatment (Bateman &
Fonagy, 1999, 2004, 2006)

Dialectical Behavior Therapy
• Based on cognitive-behavioural therapy• Hierarchy of interventions:
– Interventions aimed at reducing self-mutilating behaviour– Interventions aimed at behaviour that interferes with the
therapeutic process– Interventions aimed at improving quality of life
• Out-patient individual therapy, once a week, in combination with group therapy
• Empirical evidence for effectiveness of DBT (Koons, 2001; Linehan 1991, 1999, 2002; Turner, 2000; van den Bosch, 2002)
• Adaptations made for adolescents!

DBT in adolescenceAdaptations (Miller et al., 2007)
• Parents participate in the skill groups (multifamily skill training group)
• Shorter treatment• Simpler hand-outs• Simpler diary• Including family therapy (as-needed base)• Including extra skills that are relevant for parents or
siblings• Telephone consultations for parents• A new module: walking the middle path, introducing
three new dialectical dilemma’s

Mentalization Based Treatment
• Psychodynamic oriented treatment program
• Attachment theory
• Primary aim: to enhance mentalization
• Outpatient treatment program (18 months)
• Empirical evidence for effectiveness of MBT (Bateman, 1999)

Some general remarks about pharmacotherapy for severe PD
• Psychotherapy is treatment of first choice
• Pharmacotherapy as “enabler”, to make psychotherapy “more possible”
• No evidence based treatment methods
• Guidelines for adults, warnings for children and adolescents
• Controversies, for instance about SSRi’s

Some general remarks about pharmacotherapy for severe PD
• Be aware of the differences in pharmacokinetics in children and adolescents:– Percentage of body fat– Lipophile binding– Speed of metabolism– Plasma proteins– Demolition

Some general remarks about pharmacotherapy for severe PD
• Symptom-targeted pharmacotherapy in patients with PD is confusing.
• Is the symptom (f.e. negative affect) part of the personality disorder, or is it part of an axis-1 disorder (f.e. major depressive disorder)
• Cochrane review: no exclusion of axis 1 disorders, except for psychotic disorders

Some general remarks about pharmacotherapy for severe PD
• APA-guidelines (2001):– 3 algorithms:
• Affective dysregulation• Impulsive behavior• Cognitive-perceptual symptoms
• No clinical trials • More practice based than evidence based

Pharmacotherapy: some case study interventions
• Because of the seriousness of the symptoms of our patient we choose a combinations of different products:– Escitalopram 10 mg for heavy mood changes– Quetiapine 300 mg for cognitive-perceptual
symptoms, psychotic-like fears and impulsivity– Topiramate 50 mg for dissociation, the images of
sexual abuse and humiliations of step father– Diazepam 5 mg for the side effects after alcohol stop.

Some general remarks about system therapy for severe PD
• Is a necessary part of the treatment of a PD adolescent, on practice based arguments
• Youngsters can only change and grow within the context of their family. When there is no continuity between the therapy and the milieu at home, changes will not last long.
• Several different models have proven their solidity, but there is no evidence based background.
• New research can support the guideline of always working with the family of the adolescent.

Some general remarks about system therapy for severe PD
• I-BAFT: integrative borderline adolescent family therapy
• Multidimensional family therapy, based on attachment theory
• Integrative family therapy with genograms and core qualities

How to design a flexible and effective
treatment integrating those components?
• Therapeutic relationship including limit setting
• How does developmental phase affect therapy for severe PD’s?
• What are goals and methods in different phases of the therapeutic process?

Therapeutic relation
• Install a therapeutic alliance based on cooperation
• Be transparent (about interventions, treatment goals etc)
• Avoid an expert or moralizing position.
• Balance between acceptance/validation and change/empathic confrontation

Therapeutic relation: limit setting
• It is probably impossible to avoid setting limits (and it is probably damaging)
• There are three principles to keep in mind: – Adolescents should be given a proper (and growing)
responsibility– Limits should not be administered in an automatic,
procedural way, but with the mind of the adolescent in mind
– Therapists should be transparent about the ‘why’ of limit setting
• Be aware of extremes: authoritarian control versus excessive leniency (Miller et al., 2007)

How does developmental phase affect therapy for severe PD’s?
• Methods and interventions– Cognitive, emotional, social and identity
development determine how to do therapy• Attune to cognitive level, …
• Content/issues– Developmental tasks determine what therapy
is about (treatment goals)• Sexual identity, separation from parents, …

Developmental guidelines for choosing methods and
interventions• Based on cognitive development
– Be concrete (especially with adolescents under 15 yrs)
– Visualize– Be careful with metaphors– Don’t lean too much on hypothetical thinking– Support critical thinking– Practice meta-thinking

Developmental guidelines for choosing methods and
interventions• Based on emotional development
– Be aware that affective instability is the core of BPD in adolescents
– Start by identifying ‘simple’ emotions before proceeding to complex mental states
– Give words to identify emotions– Learn to discriminate between intensities and
sorts of emotions– Reinforce proper expression of emotions

Developmental guidelines for choosing methods and
interventions• Based on social development
– Let the adolescent ‘save face’ – Be aware of the enhanced vulnerability in
groups– Be aware that the attachment to peers might
be as important (or even more) than the attachment to therapists
– Invest in installing a positive, accepting group norm

Developmental guidelines for choosing methods and
interventions• Based on identity development
– Support autonomy• What do you want to change? • How do you want to use this session?
– Offer opportunities to separate• Support critical thinking• Give privacy• Tolerate experimenting behavior

Developmental guidelines for determining treatment goals
• Based on developmental tasks (12-15 yrs)– Dealing with physical changes– Constructing own frame of reference (norms, values)– Connect with peers
• Based on developmental tasks (15-20 yrs)– Becoming more independent from feedback of peers
and adults– Developing a stronger self-esteem– Developing social and professional skills– Re-constructing a relationship with parents

Goals and methods in different phases of the therapeutic process
• Start phase
• Middle phase
• End phase

Start phase:Goals
• Install a secure, predictable environment
• Enhance motivation / commitment
• Agree upon prior treatment goals
• Start by improving a sense of competence in the adolescent and his/her family
• Medication

Start phase: some methodological issues
• About motivation– ‘Roll with resistance’– Do not convince from an expert position– Let the adolescent motivate himself by
eliciting self-motivating expressions– Use authentic and focused reinforcements to
highlight advances• How was it for you to experience you succeeded in
managing stress in this way?

Start phase:some methodological issues
• About improving competence– Start by thinking about or even teaching skills
to cope with stress– Assist caregivers in achieving skills to remain
in control even when facing internal and interpersonal turmoil
• Psycho-education• Skill group

Start phase: some case study interventions
• We predicted upcoming relational patterns– If you tell me you always tend to break up friendships
after some months, this might be happening here too.
• We looked for agreement on prior symptoms– She was frightened by her cutting and burning, being
afraid she would lose control– About trauma: I understand this is something
extremely important for you, which we will have to work on further in treatment, but at this moment I notice that talking about it gives you a lot of tension and often leads to cutting yourself.

Start phase: some case study interventions
• We looked for alternatives to cope with stress
• We made a concrete ‘minute-to-minute’ crisis plan
• There was a joined consult with the therapist and psychiatrist about medication
• The family was taught some basic skills to prevent discussions from escalating

Middle phase:Goals
• Help the adolescent to relate symptoms to mental states that occur in the context of relations
• Help the adolescent to face developmental tasks, including developing a new relationship with parents

Middle phase:some methodological issues
• About developing a reflective stance– Identify and validate actual or recent mental
states– Differentiate and contextualize– Internalize and help to take responsibility– Digest and help to tolerate ambivalence– Integrate in alternative behavior and mental
states

Middle phase: some case study interventions
• Tania often started therapy announcing how ‘crap’ she felt– What do you mean by ‘crap’? How sad, angry,
anxious? – Can you remember when you noticed some change in
how you felt? Attitude: it might be worth to explore in detail how you came to feel this way
– Can you understand why this (trigger) made you feel this way?
– How is it to understand yourself in this way?

Middle phase: some case study interventions
• After three months, acting out dramatically increased (drinking, crossing limits)
• She wanted to stop treatment because it got ‘boring’– Can you help me to understand how it got this far? Where did
you notice a change in motivation? – This enhanced reflective stance made her aware of her fear for
intimacy of group members• I cannot tolerate it anymore. I don’t want to experience a
goodbye of group members anymore• She experienced extremely aggressive thoughts including
group members, which made her angry– With this broadening perspective, she was invited to rethink her
decision to stop. – We accepted her decision.

End phase:Goals
• Anticipate on reintegration
• Prepare for loss associated with leaving
• Relapse prevention

End phase:some methodological issues
• About relapse prevention– Identify ‘traps’– Identify future life stressors– Identify successful coping and new
competencies– Make a written therapy summary with your
patient

Follow-up
• Stepped down care: gradually less intensive treatment and more intensive reintegration in school, work etc
• Booster sessions