Embed Size (px)
Citation preview

Assessment of Chemotherapy Response in ColorectalLiver Metastases in Patients Undergoing HepaticResection and the Correlation to Pathologic ResidualViable Tumor
Michael E Egger, MD, Robert M Cannon, MD, MS, Tiffany L Metzger, BS, Michael Nowacki, MD,Larry Kelly, MD, Cliff Tatum, MD, Charles R Scoggins, MD, MBA, FACS, Glenda G Callender, MD, FACS,Kelly M McMasters, MD, PhD, FACS, Robert CG Martin II, MD, PhD, FACS
BACKGROUND: The Response Evaluation Criteria in Solid Tumors (RECIST), which evaluates maximumtumor diameter only, is commonly used to determine response to chemotherapy in patientswith colorectal liver metastases. Limitations of RECIST include its inability to assess thechanges in tumor enhancement. The aim of this study was to assess the correlation of thesecriteria as well as the modified RECIST (mRECIST) with pathologic tumor response.A novel semi-automated volumetric assessment of tumor size was also investigated.
STUDY DESIGN: A review of a 1,948-patient prospective hepatic database to assess response and pathologiccriteria was performed. Patients undergoing preoperative chemotherapy before hepaticresection for colorectal liver metastases were reviewed. Radiographic responses according toRECIST and mRECIST were determined. The percentage of viable tumor cells comparedwith the total tumor area was determined from the pathologic specimens.
RESULTS: We identified 38 patients with adequate imaging who had undergone anatomic hepatic resec-tion and full pathologic evaluation. The percentages of residual viable tumor in the resectedspecimens were significantly different across RECIST categories (p ¼ 0.045), but not mRE-CIST (p ¼ 0.305). For mRECIST, there were improved and significant linear trends forresidual viable tumor, necrosis, and necrosis þ fibrosis when compared with RECIST (p ¼0.056). Neither RECIST nor mRECIST responses were predictive of residual viable tumorburden in regression analyses. A novel semi-automated volumetric assessment of tumor sizecorrelated well with pathologic tumor size.
CONCLUSIONS: Neither RECIST nor mRECIST were predictive of residual viable burden, although thelinear trend for mRECIST and residual necrosis þ fibrosis compared favorably withRECIST. Continued evaluation for tumor enhancement and standardization of tumor sizeremain a critical unmet need in patients with solid organ disease. (J Am Coll Surg 2013;-:1e12. � 2013 by the American College of Surgeons)
Disclosure Information: Nothing to disclose.
Presented at the Southern Surgical Association 124th Annual Meeting,Palm Beach, FL, December 2012.
Received December 13, 2012; Accepted December 13, 2012.From the Hiram C Polk Jr MD Department of Surgery, Division ofSurgical Oncology, University of Louisville (Egger, Cannon, Metzger,Scoggins, Callender, McMasters, Martin), Department of Pathology,Norton Cancer Institute (Nowacki), and Department of InterventionalRadiology, Norton Healthcare (Kelly, Tatum), Louisville, KY.Correspondence address: Robert CG Martin II, MD, PhD, FACS, HiramC Polk Jr MD Department of Surgery, Division of Surgical Oncology,University of Louisville, 315 East Broadway, Suite 314, Louisville, KY40202. email: [email protected]
1ª 2013 by the American College of Surgeons
Published by Elsevier Inc.
Patients with colorectal liver metastases have a variety oftherapeutic options to treat their disease. Hepatic resec-tion of the colorectal metastases is the cornerstone ofpotentially curative therapy for these patients.1 Neoadju-vant chemotherapy is often given to resectable andborderline-resectable patients. The patient’s response tochemotherapy has been correlated with postsurgicaloutcomes.2-7 Patient selection is critical to identify thosepatients who could benefit from metastasectomy.There is emerging evidence that the pathologic response
to neoadjuvant chemotherapy is closely correlated withclinical outcomes.8-11 The difficulty in the preoperativeassessment of these patients lies in the determination of
ISSN 1072-7515/12/$36.00
http://dx.doi.org/10.1016/j.jamcollsurg.2012.12.037

Abbreviations and Acronyms
DFS ¼ disease-free survivalmRECIST ¼ modified Response Evaluation Criteria in
Solid TumorsOS ¼ overall survivalRECIST ¼ Response Evaluation Criteria in Solid TumorsSVM ¼ semi-automated volume method
2 Egger et al Response Assessment in Liver Metastases J Am Coll Surg
the degree of pathologic response to chemotherapy bynoninvasive means. Standard radiologic criteria forResponse Evaluation Criteria in Solid Tumors (RECIST)might not accurately assess the actual response or outcomesin metastatic colorectal cancer.12-15 Alternative criteriabased on morphologic changes, or modified RECIST(mRECIST), measuring changes in the degree of arterialenhancement might hold promise in the preoperative eval-uation of colorectal liver metastases, with improved corre-lation to pathologic response, particularly in patientstreated with bevacizumab.5-7,16,17 The degree to whichRECIST, mRECIST, and pathologic response criteriaare correlated with outcomes in patients undergoingdiverse neoadjuvant chemotherapy regimens in colorectalliver metastases has not been studied.In addition, limitations still remain because of substan-
tial inter-observer variability when performing tumormeasurements. There is a need for accurate and reproduc-ible lesion measurement assessment, especially within theliver. Recent studies have demonstrated an alarming vari-ation in lesion assessment.18-20 Borradaile and colleagues21
recently reported on a blinded independent central reviewmeta-analysis study of 40 trials and 12,299 subjects inwhich reader pairs did not agree for overall response in23% or date of progression in 31% of all patients. Acomputer-automated segmentation analysis to evaluatetumor volumes can improve human performance.This study was performed to determine how well
RECIST and mRECIST correlated with pathologictumor response and outcomes in patients who underwentliver resection for colorectal liver metastases after neoad-juvant chemotherapy in a single institution. In addition,we evaluated a novel enhanced volumetric modeling oftumor size to see if a standardized computer protocolmight measure pathologic tumor size more accuratelythan the more subjective RECIST and mRECIST.
METHODSA review of an initiation subset was performed froma 1,948 patient prospective hepatic database at a singleacademic institution and then validated with patientswho had been successfully downsized to resection whowere enrolled in the recently completed randomized
controlled trial of FOLFOX with Avastin in combinationwith hepatic arterial therapy or irinotecan (FOLFOXDEBIRI trial).22 Inclusion criteria included age 18 yearsor older, a documented neoadjuvant chemotherapy coursebefore hepatic resection, and a completed hepatic resec-tion with pathologic specimens available for review.Patients were excluded if they did not have a 3-phasethin-cut CT with liver protocol both before and at theconclusion of induction or neoadjuvant chemotherapythat were available for review.Radiographic response to neoadjuvant chemotherapy
was determined according to RECIST and mRECISTby an investigator initially blinded to the patient’s clinicaloutcomes and pathologic response. Response EvaluationCriteria in Solid Tumors were based on the updatedversion 1.1.23 Modified RECIST, which are similar toRECIST with the exception that only contrastingenhancing portions of the tumor are used to assessresponse, were measured as described previously.17 Patho-logic specimens were reviewed by an experienced surgicalpathologist blinded to the patient’s radiographic responsecriteria. The percentage of viable tumor cells in eachresected specimen was determined. Complete pathologicresponse was defined as the complete lack of viable tumorcells in the pathologic specimen under light microscopy.A major pathologic response had 1% to 49% viabletumor cells as an estimated percentage of the entiretumor. Tumors were categorized as a minor pathologicresponse if there were >50% viable tumor cells in thespecimen. The percentages of necrosis and fibrosis werealso measured as estimated percentages of the entiretumor area under microscopic evaluation and categorizedin the same manner as viable tumor cells. All percentageswere estimated based on the cross-sectional area of thetumor specimen available for review. In the case ofmultiple tumors in a single patient, the mean percentageof viable tumor cells was calculated.We evaluated a novel, semi-automated segmentation
volume method (SVM) (INTIO) to determine howwell a volumetric calculation of metastatic liver tumorsbased on 3-phase, liver protocol CT imaging would esti-mate the actual pathologic tumor size in resected colo-rectal liver metastases. The subjects in this pilot studywere actively enrolled in a prospective clinical trial evalu-ating the therapeutic efficacy of drug-eluting transarterialchemoembolization beads (DEBIRI) in downsizing toresection.22 The contrast-enhanced liver protocol CTimages from the preoperative (post-chemotherapy) scanswere evaluated using the semi-automated SVM softwareby investigators blinded to the pathologic findings.Each metastastic lesion was measured in 3 dimensionsprospectively in the resected hepatic specimen during

Table 1. Patient Demographics
Patient demographics
Age, y, median 59
Male, n (%) 29 (76.3)
Disease-free interval from colon resection,mo, median 7.1
Synchronous metastases, n (%) 17 (44.7)
No. of liver lesions, median 2
Size of the largest liver lesion, cm, median 4.0
CEA level at time of hepatic resection, m/dL, median 23.50
Type of hepatic resection, n (%)
Major hepatectomy 28 (73.7)
Right hepatectomy 16 (42.1)
Left hepatectomy 5 (13.2)
Extended right hepatectomy 6 (15.8)
Extended left hepatectomy 1 (2.6)
Sectionectomy or left lateral segmentectomy 8 (21.1)
Subanatomic (wedge) resection 2 (5.3)
Hepatic arterial therapy, n (%) 7 (18.4)
Vol. -, No. -, - 2013 Egger et al Response Assessment in Liver Metastases 3
routine pathologic review. Pathologic tumor volume wasdetermined by multiplying the linear length, width, anddepth measurements from the specimen.Pearson correlation coefficients were calculated for the
estimated tumor sized based on the volumetric softwarecalculations compared with the actual pathologic tumorsize. Univariate and multivariate Cox proportionalhazards models were performed for disease-free survival(DFS) and overall survival (OS) after liver resection.One-way ANOVA and independent sample t-tests wereperformed for the evaluation of differences in continuousvariables as appropriate; likewise, Fisher’s exact testing forcategorical variables was performed. Linear regressionmodels with the viable tumor burden as the dependentvariable were constructed for RECIST, mRECIST, andrelevant patient factors. All tests were 2-sided and a signif-icance level of 0.05 was predetermined. Kaplan-Meiersurvival analyses were performed using the log-rank test.SPSS version 20 (IBM) was used for statistical analysis.Appropriate IRB approval was obtained.
Table 2. Pathologic Residual Viable Tumor Burden Cate-gorized by Type of Radiologic Response Criteria
Radiologic response Mean residualviable tumor (%) p Value*n %
RECIST 0.045
Complete response 1 2.6 15.0
Partial response 17 44.7 29.4
Stable disease 16 42.1 25.1
Progressive disease 4 10.5 64.8
mRECIST 0.305
Complete response 5 19.2 28.8
Partial response 14 53.8 27.9
Stable disease 4 15.4 30.5
Progressive disease 3 11.5 55.0
*1-way ANOVA.mRECIST, modified Response Evaluation Criteria in Solid Tumors;RECIST, Response Evaluation Criteria in Solid Tumors.
RESULTSFrom October 2007 to January 2012, 38 patients wereidentified with colorectal liver metastases who underwentneoadjuvant or induction chemotherapy before hepaticresection with appropriate imaging for RECIST responsedetermination. In 26 of these patients, mRECIST wereassessable. Patient demographics are summarized inTable 1. Median follow-up was 27 months. All but 2patients (95%) received FOLFOX-based neoadjuvantchemotherapy; the 2 remaining patients received single5-FU therapy. Median number of chemotherapy cyclesgiven was 8; 76% of patients received bevacizumab and18% underwent some form of hepatic arterial therapy.
Response Evaluation Criteria in Solid Tumors vsmodified Response Evaluation Criteria in SolidTumors and residual viable tumor
Table 2 summarizes the residual viable tumor findingswhen categorized into RECIST and mRECIST responsecategories. The average residual viable tumor burdenvaried significantly across RECIST response categories(p ¼ 0.045), but not across mRECIST response cate-gories (p ¼ 0.305). Complete and partial responseswere combined in patients with both RECIST andmRECIST measurements, and RECIST and mRECISTresponses were compared in the 26 patients with bothRECIST and mRECIST data available. Tests for a lineartrend across RECIST and mRECIST radiologic responsecategories for residual viable tumor, necrosis, andnecrosis þ fibrosis were performed (Fig. 1). For RECIST
categories, there was not a statistically significant lineartrend for viable tumor, necrosis, or necrosis þ fibrosis.For mRECIST, there was clearly a more expected signif-icant linear trend for viable tumor, necrosis, andnecrosis þ fibrosis that approached statistical significance(p ¼ 0.056). Residual fibrosis was also analyzed separatelyand responses were similar to residual necrosis. Pathologicresponse was then categorized as complete if there wereno residual viable tumor cells, major if there were 1%to 49% residual viable tumor cells, and minor if therewere �50% residual viable tumor cells. There were nostatistically significant differences in the proportions of
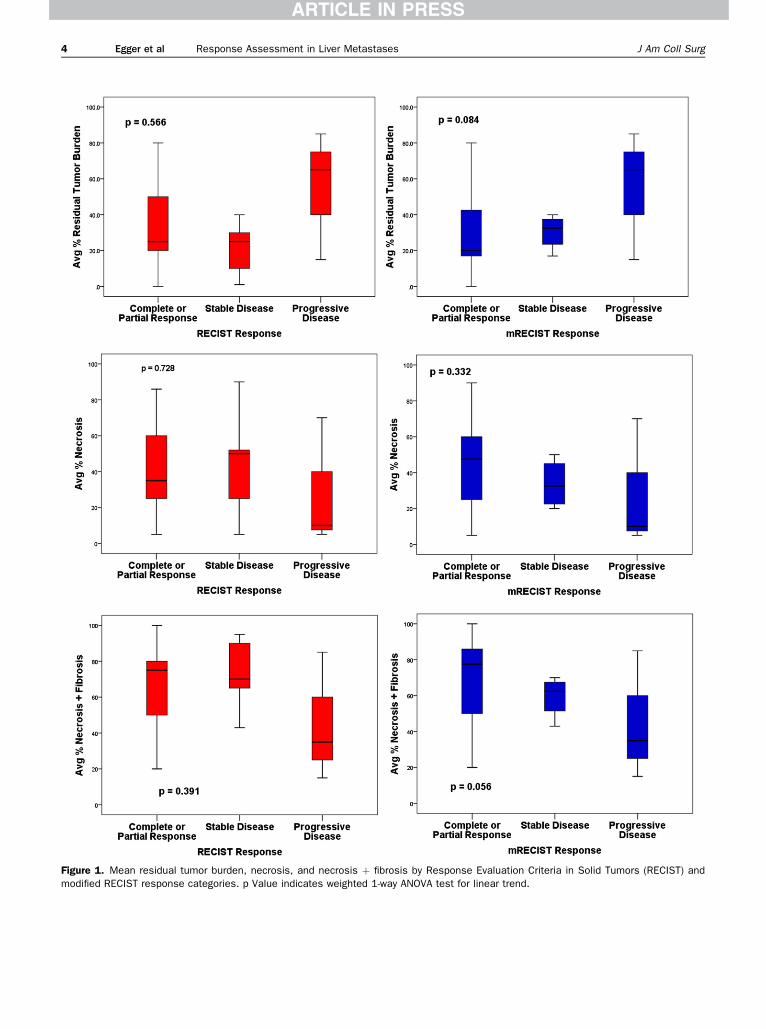
Figure 1. Mean residual tumor burden, necrosis, and necrosis þ fibrosis by Response Evaluation Criteria in Solid Tumors (RECIST) andmodified RECIST response categories. p Value indicates weighted 1-way ANOVA test for linear trend.
4 Egger et al Response Assessment in Liver Metastases J Am Coll Surg

Vol. -, No. -, - 2013 Egger et al Response Assessment in Liver Metastases 5
RECIST or mRECIST responses across the differentpathologic response types (Table 3).Linear regression modeling of the residual viable tumor
burden was performed in patients with both RECISTand mRECIST response criteria. Patients were catego-rized as having a response (complete or partial) or not.We again compared the same patients according toRECIST and mRECIST response criteria. Neithera RECIST nor an mRECIST response was a statisticallysignificant predictor of residual viable tumor burden onunivariate analysis (Table 4). The only statistically signi-ficant variable of residual viable tumor burden was thenumber of chemotherapy cycles, which was positivelycorrelated with residual viable tumor burden. ResponseEvaluation Criteria in Solid Tumors and mRECISTresponses were not significant predictors of residual viabletumor burden when controlling for the number of che-motherapy cycles.
Computer-aided evaluation of semi-automatedvolume method, tumor volumetrics, and tumor sizeprediction
Patients with distinct lesions who underwent liver resec-tion after neoadjuvant chemotherapy for colorectal livermetastases formed our initial test set to evaluate thesemi-automated volumetric measurements calculated bySVM (INTIO). An example of the volumetric measure-ments and calculations are presented in Figure 2. Mediansize of the tumors by SVM estimation was 8.1 cm3; themedian actual pathologic tumor volume was 8.4 cm3.The difference between the estimate SVM tumor volumeand actual pathologic tumor volume were not statisticallysignificantly different by a paired sample t-test (mean dif-ference �60.6 cm3; p ¼ 0.106) (Table 5). There wasa high degree of correlation between the estimated tumor
Table 3. Pathologic Response Type Categorized by Radiologic
Radiologic response
n % Complete respons
RECIST 2 (5.3)y
Complete response 1 2.6 0
Partial response 17 44.7 100
Stable disease 16 42.1 0
Progressive disease 4 10.5 0
mRECIST 1 (3.9)y
Complete response 5 19.2 100
Partial response 14 53.8 0
Stable disease 4 15.4 0
Progressive disease 3 11.5 0
*Fisher’s exact test.yn (%).mRECIST, modified Response Evaluation Criteria in Solid Tumors; RECIST,
volume based on preoperative volumetric measurementsand the actual pathologic tumor volume, with a Pearsoncorrelation coefficient ¼ 0.908; p < 0.001 (Fig. 3).For survival analysis, Cox proportional hazards
modeling was used for both OS and DFS from thetime of hepatic resection. All covariates having a univariaterisk ratio with p > 0.20 were included in the multivariatemodel. Initially, the RECIST and mRECIST categorieswere excluded to determine the relevant covariates thatwould need to be controlled in the models evaluatingthe importance of the RECIST and mRECIST response.The model for OS is summarized in Table 6. Age andresidual viable tumor burden were independent riskfactors for worse OS. Response Evaluation Criteria inSolid Tumors and mRECIST response categories weredichotomized into responders (complete or partial) ornonresponders (stable or progressive disease). Each ofthese covariates was added to our baseline multivariatemodel to determine their contribution to the risk of deathafter liver resection. Neither having a RECIST responsenor an mRECIST response was significantly associatedwith differences in OS in the models (p ¼ 0.935 and0.772, respectively). The DFS Cox proportional hazardsmodel was constructed in the same manner (Table 7).The presence of synchronous liver metastases was theonly statistically significant independent risk factor forworse DFS. When the RECIST response and mRECISTresponse covariates were tested in the full model againneither were significantly associated with differences inDFS (p ¼ 0.763 and 0.259, respectively). In the DFSmodel with a RECIST response covariate, residual viabletumor burden was an independent risk factor for worseDFS (hazard ratio ¼ 1.018; p ¼ 0.047).Kaplan-Meier survival analysis revealed significant
differences in OS for both RECIST and mRECIST
Response Criteria
Pathologic response, %
p Value*e Major response Minor response
25 (65.8)y 11 (28.9)y 0.067
4.0 0
36.0 54.5
56.0 18.2
4.0 27.3
18 (69.2)y 7 (26.9)y 0.123
11.1 28.6
61.1 42.9
22.2 0
5.6 28.6
Response Evaluation Criteria in Solid Tumors.

Table 4. Univariate and Multivariate Linear Regression Models to Predict the Residual Viable Tumor Burden for ResponseEvaluation Criteria in Solid Tumors and Modified Response Evaluation Criteria in Solid Tumors
ParameterUnivariate estimate
(95% CI)Univariatep value
Multivariate estimate(95% CI)
Multivariatep value
RECIST model
RECIST response 4.31 (�14.15 to 22.77) 0.634 12.28 (�14.51 to 39.07) 0.342
No. of chemotherapy cycles 3.71 (0.41 to 7.00) 0.030 2.68 (�1.33 to 6.68) 0.174
mRECIST model
mRECIST response �12.84 (�33.04 to 7.35) 0.202 9.54 (�34.60 to 53.69) 0.6501
No. of chemotherapy cycles 3.71 (0.41 to 7.00) 0.030 3.67 (0.26 to 7.08) 0.037
mRECIST, modified Response Evaluation Criteria in Solid Tumors; RECIST, Response Evaluation Criteria in Solid Tumors.
6 Egger et al Response Assessment in Liver Metastases J Am Coll Surg
responses (complete or partial response vs stable orprogressive disease) (Fig. 4). There were no significantdifferences in DFS across RECIST and mRECIST(Fig. 5). When the pathologic responses were categorizedinto complete, major, and minor responses, there weretrends toward differences in DFS and OS, but thesedifferences were not statistically significant (Fig. 6).
DISCUSSIONThe most important finding in this study is that bothstandard RECIST for estimating response to chemo-therapy and mRECIST, which takes into account theloss of arterial enhancement, were only weakly correlatedwith the residual viable tumor burden. There appearedto be an improved linear trend of mRECIST responseand residual necrosis þ fibrosis compared with theRECIST response. Neither criterion could adequatelypredict pathologic response to neoadjuvant chemo-therapy. Response Evaluation Criteria in Solid Tumors
Figure 2. Sample image of automated volumetric me
and mRECIST responses were not risk factors for worseDFS or OS. A new semi-automated evaluation of cross-sectional liver imaging might hold promise in the preop-erative assessment of hepatic tumor volume. The mostplausible reason for this still remains a substantialhuman variation in establishing accurate tumor diameterfor multiple hepatic tumors. There is a lack of standard-ization with regard to patient orientation (ie, axial,sagittal, coronal planes, which all tumors should bemeasured in), measuring of edema and/or enhancementof the tumor, and reproducibility across multiple bodyimagers who read this scans, because one radiologistwill not always read the same patients’ scans during theirtreatment.Hepatic resection techniques have improved to the
point that elective liver resection for colorectal livermetastases can be performed with low morbidity andmortality.24 The challenge to treating patients with colo-rectal liver metastases lies not in the technical aspects ofthe resection, but in the selection of those patients who
asurements by semi-automated volume method.

Table 5. Comparison of Semi-Automated Volume MethodEstimatesof TumorVolumetoActualPathologicTumorVolume
Estimatedtumor volumeby SVM, cm3
Actualpathologic tumorvolume, cm3
Difference betweenestimated and pathologic
tumor volume, cm3
111.5 253.5 �142
42.6 274.6 �232.03
20 0.1 19.88
0.9 0.5 0.41
14.3 28.5 �14.2
9.2 11 �1.8
8.5 13.3 �4.83
7.7 12.1 �4.4
1.8 5.7 �3.93
1.3 2 �0.73
1.9 0.5 1.41
1.4 0.2 1.18
1.6 0.5 1.11
123.2 650 �526.8
18.5 82.8 �64.3
5.2 4 1.2
SVM, semi-automated volume method.
Vol. -, No. -, - 2013 Egger et al Response Assessment in Liver Metastases 7
will benefit and experience prolonged survival after meta-stasectomy. Patient and tumor factors can be used topredict post-resection survival reasonably well.25-27 Neo-adjuvant, or preoperative, chemotherapy is commonlyused to treat occult metastases and assess the intrinsicbiology of disease to determine if the patient will undergohepatic resection. Initially used for unresectable colorectalliver metastases, neoadjuvant chemotherapy increasingly
Figure 3. Correlation of preoperative estimated tumor volumesbased on semi-automated volume method with actual pathologictumor volume.
is being used upfront in patients with resectabledisease.28,29 Progression of disease when a patient is onchemotherapy is generally considered a poor prognosticsign, although some evidence exists that some of thesepatients might still have good outcomes after resec-tion.2,30,31 Patient and tumor factors considered togetherwith the patient’s response to chemotherapy are impor-tant predictors of outcomes after hepatic resection forcolorectal liver metastases.Defining response to neoadjuvant therapy objectively
can be difficult. Well-defined radiologic criteria havebeen defined to assess and semi-quantify the patient’sresponse to chemotherapy. One such set of criteria arethe RECIST guidelines based on changes in the cross-sectional diameters of the tumors.23 These guidelineshave their limitations in assessing the response of hepaticlesions to chemotherapy. No consideration is given to thechanges in the arterial enhancement of the tumors. Modi-fied RECIST have been used for hepatocellular carcinomathat consider the changes in the contrast-enhancedportion of the liver tumors with good success.17,32,33 ThemRECIST can outperform standard RECIST for colo-rectal liver metastases, but this question requires addi-tional study.6 Recently, a set of morphologic responsecriteria used to evaluate the response to neoadjuvantchemotherapy in colorectal liver metastases has beenreported to correlate with outcomes.5,7 Which radiologiccriteria correlate best with clinical outcomes is an impor-tant question to study.There is evidence that the degree of pathologic
response is an important end point for the evaluation ofresponse to neoadjuvant chemotherapy in colorectal livermetastases. Blazer and colleagues9 reported that the typeof pathologic response (complete, major, or minor) wasan independent predictor of survival in 305 patientswith colorectal liver metastases treated with prehepatec-tomy chemotherapy. These are the pathologic responsecategories used in the current study. Subsequent studieshave supported the importance of the pathologic responseto chemotherapy in determining survival outcomes.34-36
Although most studies assess pathologic response bymeasuring viable residual tumor, an alternative methodis to measure fibrosis or necrosis.11 Although it certainlyis logical that the pathologic response of the metastatictumors to chemotherapy is an important indicator offuture outcomes, one is faced with the difficult task ofassessing pathologic response by noninvasive means todetermine whether the patient should undergo resectionafter chemotherapy.Radiologic response criteria can serve as a reasonable
proxy by which one can estimate the pathologic response.This supposition was the underlying hypothesis of this

Table 6. Multivariate Model for Overall Survival in Patients Undergoing Liver Resection for Colorectal Liver Metastases
Risk factorUnivariate hazardratio (95% CI)
Univariatep value
Multivariatehazard
ratio (95% CI)Multivariate
p value
Age 1.05 (0.99�1.12) 0.086 1.07 (1.00�1.15) 0.045
Synchronous liver metastasis 2.76 (0.76�10.05) 0.125 3.82 (0.63�23.03) 0.144
>1 metastasis 2.66 (0.69�10.29) 0.158 2.27 (0.41�12.49) 0.346
Residual viable tumor burden 1.02 (0.99�1.05) 0.141 1.03 (1.00�1.06) 0.036
Response Evaluation Criteria in Solid Tumors and modified Response Evaluation Criteria in Solid Tumors criteria were nonsignificant in the multivariatemodel.
8 Egger et al Response Assessment in Liver Metastases J Am Coll Surg
studydthat radiologic response criteria would correlatewith pathologic response in patients undergoing neoadju-vant chemotherapy before liver resection for colorectalliver metastases. In this study, we were unable to demon-strate that either standard RECIST or mRECIST couldaccurately predict the underlying pathologic response tochemotherapy. Although we did show that there wasa statistically significant variation in the percentage ofresidual viable tumor across different RECIST (Table 1),an actual RECIST response was not able to accuratepredict the residual viable tumor burden in our linearregression model. For both mRECIST and RECIST,progressive disease was characterized by a distinctly worsepathologic response compared with responsive and stabledisease. Based on previous reports, we had suspected thatmRECIST would outperform RECIST, however, thevariation in residual tumor burden was similar betweenthe 2 criteria.Modified RECIST measures loss of arterial enhance-
ment and might be capturing the development of necrosisand fibrosis rather than the loss of viable tumor cells thatis seen with tumor shrinkage as assessed by RECIST.Figure 1 demonstrates how there appears to be a progres-sive increase in the degree of necrosis and fibrosis as oneprogresses from mRECIST disease progression to stabledisease, and finally a complete or partial response. Wesuggest that there is no such similar orderly progressionin residual tumor burden according to RECIST. Instead,the residual tumor burden only increases substantiallyin patients with progressive disease; these patients areclearly not responding to chemotherapy and likely will
Table 7. Multivariate Model for Disease-Free Survival in Patient
Risk factorUnivariate HazardRatio (95% CI)
Synchronous liver metastasis 3.98 (1.74�9.06)
>1 metastasis 2.23 (0.98�5.05)
Residual viable tumor burden 1.01 (1.00�1.03)
Response Evaluation Criteria in Solid Tumors and modified Response Evaluatimodel.
not benefit from resection. The linear trend of increasingnecrosis þ fibrosis and decreasing residual viable tumorburden as the radiologic response improved was more pro-nounced, but not statistically significant, in mRECISTcompared with RECIST. Modified RECIST can offerthe clinician slightly more subtle discrimination amongthe stable or partial responders in whom prognosis isquite variable.Previous work has correlated radiologic changes to
pathologic response in colorectal liver metastases.Morphologic criteria were significantly correlated withresidual viable tumor burden in a single institution studyof 50 patients.5 More recently, Shindoh and colleagues7
have shown that morphologic response criteria were supe-rior to RECIST in predicting major pathologic response.There are several potential explanations for our finding ofthe generalized inability of mRECIST to predict patho-logic response. This is a relatively small study and mightbe underpowered to find clinically significant differences.The patients in this study were not enrolled in a formalneoadjuvant protocol and, as such, received a variety of5-FU�based chemotherapy regimens, sometimes withoutbevacizumab. Treatment duration was not specified andimaging intervals were not standardized. The intervalbetween the completion of chemotherapy and resectionwas not standardized, although our institutional practiceis to perform hepatic resection approximately 6 weeksafter the conclusion of chemotherapy. Although thisstudy setting is quite generalizable to the practice ofsurgical oncology in centers nationwide, there might besome confounding factors in our models. Radiologic
s Undergoing Liver Resection for Colorectal Liver Metastases
Univariatep value
MultivariateHazard
Ratio (95% CI)Multivariate
p value
0.001 3.63 (1.35�9.81) 0.011
0.055 1.80 (0.68�4.73) 0.236
0.123 1.02 (1.00�1.04) 0.051
on Criteria in Solid Tumors criteria were nonsignificant in the multivariate

Figure 4. Kaplan-Meier survival analysis of overall survival for patients with either a complete or partial(A) Response Evaluation Criteria in Solid Tumors (RECIST) or (B) modified RECIST radiologic response to neoadjuvantchemotherapy before undergoing liver resection for colorectal liver metastases.
Vol. -, No. -, - 2013 Egger et al Response Assessment in Liver Metastases 9
and pathologic responses are still very important toconsider, as we found that there were significant survivaldifferences in Kaplan-Meier analysis based on RECISTand mRECIST (Fig. 4). These survival differences werenot confirmed in our multivariate Cox proportionalhazard modeling, likely due to an underpowered study.We did find that the number of chemotherapy cycles
was positively correlated with the residual viable tumorburden, that is, patients who received chemotherapylonger had more residual viable tumor (worse pathologicresponse). The likely explanation for this is that patients
Figure 5. Kaplan-Meier survival analysis of disease-free(A) Response Evaluation Criteria in Solid Tumors (RECIST) orchemotherapy before undergoing liver resection for colorec
who had a good radiographic response did not undergoprolonged chemotherapy regimens; they were resected.Longer chemotherapy cycles were likely performed inpatients with more equivocal responses or progressivedisease after changes to their regimen, which explainsour findings. Additional study is needed to help charac-terize the relationship between RECIST, mRECIST,and pathologic response criteria and to identify thosepatients in whom radiographic response rates are themost suitable estimate of true pathologic response bywhich clinical decisions can be made.
survival for patients with either a complete or partial(B) modified RECIST radiologic response to neoadjuvanttal liver metastases.

Figure 6. Kaplan Meier analysis of (A) overall survival and (B) disease-free survival when stratified by pathologicresponse in patient undergoing liver resection after neoadjuvant chemotherapy for metastatic colorectal cancer.
10 Egger et al Response Assessment in Liver Metastases J Am Coll Surg
Our institutional practice is to use contrast-enhanced,3-phase liver protocol CT imaging to evaluate patientswith colorectal liver metastases, determine resectability,and monitor for chemotherapy response. Alternativeimaging modalities, such as MRI and PET, are alsoused to evaluate these patients. Our preference for CTimaging is based on issues of practicality and reproduc-ibility. Positron emission tomography imaging is notvery sensitive for the evaluation of hepatic metastasesand their response to chemotherapy.37 Manipulation ofthe detection levels can alter the conclusions drawnfrom the studies and limit reproducibility. Magnetic reso-nance imaging comes with real-world logistic challengesthat complicate its use. Often the MRI-compatibility ofthe patient’s Medi-Port is unknown. Images are also oftennondiagnostic in obese patients or in patients who havelimited breath-holding capacity. For these reasons, ourpreferred imaging modality is contrast-enhanced CT.The preliminary report of the semi-automated volu-
metric estimations of pathologic tumor size might bea promising new application of preoperative imagingand assessment in patients with colorectal liver metastases.Any measurements of tumor response, even if made byseemingly objective measures, such as cross-sectionaltumor diameter, are subject to error and variability.Morphologic criteria and mRECIST add an additionallevel of subjectivity by assessing the degree of enhance-ment in the tumor or subjective measures of morphologicchanges. Semi-automated, volumetric analyses that canestimate tumor size with a high degree of accuracy andreproducibility will form the foundation of the next
generation of image-based tumor assessment criteria.The next step for the application of this technology isto assess how well computer-aided measurements cantrack tumor volume changes and enhancement changesover time.The conclusions drawn from this study must consider
the inherent limitations of the study design and review.There is a potential for selection bias, as the 38 patientsin this study represent a small portion of the patientstreated at our institution during the 4-year study period.The most common reason for exclusion from the studywas the lack of adequate pre- and post-treatment imagingby which radiologic responses could be determined. Thecritical importance of high-quality, dedicated hepaticprotocol imaging is more necessary than ever before tomake well-informed, evidence-based decisions aboutpatient care. The study might be underpowered to detectclinically significant variations in the residual viabletumor burden across the different response criteria.
CONCLUSIONSWe report that the pathologic response to neoadjuvantchemotherapy is an important end point in patientswith metastatic colorectal cancer that correlates with post-operative outcomes. Response Evaluation Criteria inSolid Tumors and mRECIST are unsatisfactory surro-gates to assess or estimate the pathologic response, asthere is a great deal of variability in residual viable tumorburden within response categories. The mRECIST,however, might have improved capabilities to assess

Vol. -, No. -, - 2013 Egger et al Response Assessment in Liver Metastases 11
residual necrosis and fibrosis compared with RECIST.Thoughtful clinical judgment by experienced multidisci-plinary teams consisting of surgeons, radiologists, andoncologists remain our best tool for evaluating patientsfor liver resection of colorectal liver metastases. Emergingtechnologies that can help estimate tumor volumes fromcross-sectional imaging can help clinicians better evaluateresponse to chemotherapy in these patients.
Author Contributions
Study conception and design: Egger, Cannon, Scoggins,Callender, McMasters, Martin
Acquisition of data: Egger, Cannon, Metzger, Nowacki,Kelly, Tatum, Martin
Analysis and interpretation of data: Egger, Cannon,Nowacki, Kelly, Tatum, Scoggins, Callender, Martin
Drafting of manuscript: Egger, Cannon, Metzger,Nowacki, Kelly, Tatum, Scoggins, Callender,McMasters, Martin
Critical revision: Egger, Cannon, Metzger, Nowacki,Kelly, Tatum, Scoggins, Callender, McMasters, Martin
REFERENCES
1. Brown RE, Bower MR, Martin RC. Hepatic resection forcolorectal liver metastases. Surg Clin North Am 2010;90:839e852.
2. Allen PJ, Kemeny N, Jarnagin W, et al. Importance ofresponse to neoadjuvant chemotherapy in patients undergoingresection of synchronous colorectal liver metastases.J Gastrointest Surg 2003;7:109e115.
3. GruenbergerB, ScheithauerW,PunzengruberR, et al. Importanceof response to neoadjuvant chemotherapy in potentially curablecolorectal cancer liver metastases. BMC Cancer 2008;8:120.
4. Small RM, Lubezky N, Shmueli E, et al. Response to chemo-therapy predicts survival following resection of hepatic colo-rectal metastases in patients treated with neoadjuvant therapy.J Surg Oncol 2009;99:93e98.
5. Chun YS, Vauthey JN, Boonsirikamchai P, et al. Associationof computed tomography morphologic criteria with pathologicresponse and survival in patients treated with bevacizumab forcolorectal liver metastases. JAMA 2009;302:2338e2344.
6. Chung WS, Park MS, Shin SJ, et al. Response evaluation inpatients with colorectal liver metastases: RECIST version 1.1versus modified CT criteria. AJR Am J Roentgenol 2012;199:809e815.
7. Shindoh J, Loyer EM, Kopetz S, et al. Optimal morphologicresponse to preoperative chemotherapy: an alternate outcomeend point before resection of hepatic colorectal metastases.J Clin Oncol 2012;30:4566e4572.
8. Rubbia-Brandt L, Giostra E, Brezault C, et al. Importance ofhistological tumor response assessment in predicting theoutcome in patients with colorectal liver metastases treatedwith neo-adjuvant chemotherapy followed by liver surgery.Ann Oncol 2007;18:299e304.
9. Blazer DG 3rd, Kishi Y, Maru DM, et al. Pathologic responseto preoperative chemotherapy: a new outcome end point after
resection of hepatic colorectal metastases. J Clin Oncol 2008;26:5344e5351.
10. Klinger M, Tamandl D, Eipeldauer S, et al. Bevacizumabimproves pathological response of colorectal cancer livermetastases treated with XELOX/FOLFOX. Ann Surg Oncol2010;17:2059e2065.
11. Poultsides GA, Bao F, Servais EL, et al. Pathologic response topreoperative chemotherapy in colorectal liver metastases:fibrosis, not necrosis, predicts outcome. Ann Surg Oncol2012;19:2797e2804.
12. Grothey A, Hedrick EE, Mass RD, et al. Response-indepen-dent survival benefit in metastatic colorectal cancer: a compar-ative analysis of N9741 and AVF2107. J Clin Oncol 2008;26:183e189.
13. Saltz LB, Clarke S, Diaz-Rubio E, et al. Bevacizumab incombination with oxaliplatin-based chemotherapy as first-line therapy in metastatic colorectal cancer: a randomizedphase III study. J Clin Oncol 2008;26:2013e2019.
14. Neumann UP, Thelen A, Rocken C, et al. Nonresponse topre-operative chemotherapy does not preclude long-termsurvival after liver resection in patients with colorectal livermetastases. Surgery 2009;146:52e59.
15. Gallagher DJ, Zheng J, Capanu M, et al. Response to neoad-juvant chemotherapy does not predict overall survival forpatients with synchronous colorectal hepatic metastases. AnnSurg Oncol 2009;16:1844e1851.
16. Choi H, Charnsangavej C, Faria SC, et al. Correlation ofcomputed tomography and positron emission tomography inpatients with metastatic gastrointestinal stromal tumor treatedat a single institution with imatinib mesylate: proposal of newcomputed tomography response criteria. J Clin Oncol 2007;25:1753e1759.
17. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assess-ment for hepatocellular carcinoma. Semin Liver Dis 2010;30:52e60.
18. Marten K, Auer F, Schmidt S, et al. Inadequacy of manualmeasurements compared to automated CT volumetry inassessment of treatment response of pulmonary metastasesusing RECIST criteria. Eur Radiol 2006;16:781e790.
19. Gierada DS, Pilgram TK, Ford M, et al. Lung cancer: interob-server agreement on interpretation of pulmonary findings atlow-dose CT screening. Radiology 2008;246:265e272.
20. Singh S, Pinsky P, Fineberg NS, et al. Evaluation of readervariability in the interpretation of follow-up CT scans atlung cancer screening. Radiology 2011;259:263e270.
21. Borradaile K, FordR,O’NealM,ByrneK.Discordance betweenBICR readers. Applied Clinical Trials Online. Available at:http://www.appliedclinicaltrialsonline.com/appliedclinicaltrials/article/articleDetail.jsp?id=693554. Accessed November 1,2010.
22. Martin RC 2nd, Scoggins CR, Tomalty D, et al. Irinotecandrug-eluting beads in the treatment of chemo-naive unresect-able colorectal liver metastasis with concomitant systemic fluo-rouracil and oxaliplatin: results of pharmacokinetics and phaseI trial. J Gastrointest Surg 2012;16:1531e1538.
23. Eisenhauer EA, Therasse P, Bogaerts J, et al. New responseevaluation criteria in solid tumours: revised RECIST guideline(version 1.1). Eur J Cancer 2009;45:228e247.
24. Choti MA, Sitzmann JV, Tiburi MF, et al. Trends in long-term survival following liver resection for hepatic colorectalmetastases. Ann Surg 2002;235:759e766.

12 Egger et al Response Assessment in Liver Metastases J Am Coll Surg
25. Nordlinger B, Guiguet M, Vaillant JC, et al. Surgical resectionof colorectal carcinoma metastases to the liver. A prognosticscoring system to improve case selection, based on 1568patients. Cancer 1996;77:1254e1262.
26. Mala T, Bohler G, Mathisen O, et al. Hepatic resection forcolorectal metastases: can preoperative scoring predict patientoutcome? World J Surg 2002;26:1348e1353.
27. Kattan MW, Gonen M, Jarnagin WR, et al. A nomogram forpredicting disease-specific survival after hepatic resection formetastatic colorectal cancer. Ann Surg 2008;247:282e287.
28. Adam R, Avisar E, Ariche A, et al. Five-year survival followinghepatic resection after neoadjuvant therapy for nonresectablecolorectal. Ann Surg Oncol 2001;8:347e353.
29. ChuaTC, Saxena A, LiauwW, et al. Systematic review of random-ized and nonrandomized trials of the clinical response andoutcomes of neoadjuvant systemic chemotherapy for resectablecolorectal liver metastases. Ann Surg Oncol 2010;17:492e501.
30. Chiappa A, Bertani E, Makuuchi M, et al. Neoadjuvantchemotherapy followed by hepatectomy for primarily resect-able colorectal cancer liver metastases. Hepatogastroenterology2009;56:829e834.
31. Vigano L, Capussotti L, Barroso E, et al. Progression whilereceiving preoperative chemotherapy should not be an absolutecontraindication to liver resection for colorectal metastases.Ann Surg Oncol 2012;19:2786e2796.
32. Edeline J, Boucher E, Rolland Y, et al. Comparison of tumorresponse by Response Evaluation Criteria in Solid Tumors(RECIST) and modified RECIST in patients treated with sor-afenib for hepatocellular carcinoma. Cancer 2012;118:147e156.
33. Shim JH, Lee HC, Kim SO, et al. Which response criteria besthelp predict survival of patients with hepatocellular carcinomafollowing chemoembolization? A validation study of old andnew models. Radiology 2012;262:708e718.
34. Tanaka K, Takakura H, Takeda K, et al. Importance ofcomplete pathologic response to prehepatectomy chemo-therapy in treating colorectal cancer metastases. Ann Surg2009;250:935e942.
35. Chan G, Hassanain M, Chaudhury P, et al. Pathologicalresponse grade of colorectal liver metastases treated withneoadjuvant chemotherapy. HPB (Oxford) 2010;12:277e284.
36. Gruenberger T, Arnold D, Rubbia-Brandt L. Pathologicresponse to bevacizumab-containing chemotherapy in patientswith colorectal liver metastases and its correlation withsurvival. Surg Oncol 2012;21:309e315.
37. Ramos E, Valls C, Martinez L, et al. Preoperative staging ofpatients with liver metastases of colorectal carcinoma. DoesPET/CT really add something to multidetector CT? AnnSurg Oncol 2011;18:2654e2661.





























