Embed Size (px)
Citation preview

ASSESSMENT OF CHILDREN’S BEHAVIOR BEFORE AND AFTER MASS DRUG
ADMINISTRATION WITH PRAZIQUANTEL IN KENYA USING BASC-2
by
XIANJUE WEI
(Under the Direction of Ye Shen)
ABSTRACT
Schistosomiasis is an underreported infection that can cause anemia, decreased growth,
liver abnormalities, and deficits in cognitive functioning to children. This study used Behavior
Assessment System for Children (BASC-2) to collect the raw data of children’s behaviors with
or without schistosomiasis in Kenya before and after mass drug administration (MDA) with
praziquantel. We performed multiple imputation to deal with the missing data, and applied
several statistical procedures such as paired t-test and linear mixed effect models to investigate
the impact of schistosomiasis infection on children’s behavior and whether the MDA leads to
positive effects on children’s behaviors. The results of this study generally supported our
expectation that children have better behaviors without schistosomiasis, and children’s
behaviors, especially problematic behaviors, will improve significantly after the praziquantel
treatment.
INDEX WORDS: BASC-2, Children Behavior, Schistosomiasis, Mass Drug Administration,
Statistical Analysis

ASSESSMENT OF CHILDREN’S BEHAVIOR BEFORE AND AFTER MASS DRUG
ADMINISTRATION WITH PRAZIQUANTEL IN KENYA USING BASC-2
by
XIANJUE WEI
B.A., Beijing Jiaotong University, China, 2014
A Thesis Submitted to the Graduate Faculty of The University of Georgia in Partial Fulfillment
of the Requirements for the Degree
MASTER OF SCIENCE
ATHENS, GEORGIA
2016

© 2016
XIANJUE WEI
All Rights Reserved

ASSESSMENT OF CHILDREN’S BEHAVIOR BEFORE AND AFTER MASS DRUG
ADMINISTRATION WITH PRAZIQUANTEL IN KENYA USING BASC-2
by
XIANJUE WEI
Major Professor: Ye Shen
Committee: Stephen L. Rathbun
Xiao Song
Electronic Version Approved:
Suzanne Barbour
Dean of the Graduate School
The University of Georgia
May 2016

iv
ACKNOWLEDGEMENTS
I appreciate the advice from Dr. Shen, Dr. Rathbun, Dr. Song, and all the other professors
who taught and helped me. I thank my parents who supported me to have the opportunity to
study in the U.S. and made my American dream come true.

v
TABLE OF CONTENTS
Page
ACKNOWLEDGEMENTS ........................................................................................................... iv
LIST OF TABLES ......................................................................................................................... vi
LIST OF FIGURES ..................................................................................................................... viii
CHAPTER
1 INTRODUCTION .........................................................................................................1
Purpose of Study ......................................................................................................1
Research Question and Hypotheses .........................................................................3
2 MATERIAL AND METHODS .....................................................................................4
Data Collection ........................................................................................................4
BASC-2 ....................................................................................................................5
Multiple Imputation ...............................................................................................10
Statistical Analysis .................................................................................................11
3 RESULTS AND DISCUSSION ..................................................................................16
Results ....................................................................................................................16
Discussion ..............................................................................................................35
4 CONCLUSION ............................................................................................................40
REFERENCES ..............................................................................................................................41
APPENDICES
A MULTIPLE IMPUTATION RESULTS......................................................................44

vi
LIST OF TABLES
Page
Table 1: TRS Scale Definition .........................................................................................................7
Table 2: Example of the Composite T Scores Summary of One Child ...........................................8
Table 3: Factor Correlation from CSA for TRS-C ..........................................................................9
Table 4: Scale and Composite Score Classification ......................................................................12
Table 5: Frequency of the Classification of Children’s Behaviors before Treatment ...................17
Table 6: Mean Composite T Scores before Treatment ..................................................................17
Table 7: Frequency of the Classification of Children’s Behaviors after Treatment ......................19
Table 8: Mean Composite T Scores after Treatment .....................................................................19
Table 9: Mean Scores of Subscales of Externalizing Problems ....................................................20
Table 10: Mean Scores of Subscales of Internalizing Problems....................................................22
Table 11: Mean Scores of Subscales of School Problems .............................................................22
Table 12: Mean Scores of Subscales of Adaptive Skills ...............................................................23
Table 13: Paired T-test: Before-treatment vs After-treatment .......................................................26
Table 14: MANOVA Test and Exact F statistics...........................................................................27
Table 15: Simultaneous and Bonferroni Confidence Interval .......................................................27
Table 16: MANOVA Test and Exact F statistics for Parallel Profiles ..........................................28
Table 17: Paired T-test for Adaptive Scales: Before-treatment vs After-treatment ......................29
Table 18: P-values of Type 3 Tests of Fixed Effect ......................................................................31
Table 19: Solution for Fixed Effects of Externalizing Problems ...................................................32

vii
Table 20: Solution for Fixed Effects of Internalizing Problems ....................................................32
Table 21: Solution for Fixed Effects of School Problems .............................................................33
Table 22: Solution for Fixed Effects of BSI ..................................................................................33
Table 23: Solution for Fixed Effects of Adaptive Skills ................................................................33
Table 24: Mean Changes Following MDA
between Positive and Negative Groups ..........................................................................34
Table 25: McNemar’s Test for F Index .........................................................................................35
Table 26: McNemar’s Test for Consistency Index ........................................................................35

viii
LIST OF FIGURES
Page
Figure 1: Mean Composite T Scores before Treatment .................................................................18
Figure 2: Mean Composite T Scores after Treatment ....................................................................19
Figure 3: Mean Composite T Scores by Status and Time .............................................................20
Figure 4: QQ Plots by Time ...........................................................................................................24
Figure 5: QQ Plots by Status .........................................................................................................25
Figure 6: Profile Plot of Composite Scales: Before-treatment vs After-treatment ........................28
Figure 7: Spaghetti Plots for Externalizing Problems, Internalizing Problems, BSI, School
Problems and Adaptive Skills ........................................................................................30
Figure 8: Mean Changes Following MDA
between Positive and Negative Groups ..........................................................................34

1
CHAPTER 1
INTRODUCTION
Purpose of Study
This study seeks to test the difference in behaviors between school children with and
without schistosomiasis who underwent the mass drug administration (MDA) of praziquantel in
Kenya using the Behavior Assessment System for Children 2nd Edition (BASC-2).
Schistosomiasis is an acute and chronic parasitic disease caused by blood flukes
(trematode worms) of the genus Schistosoma. The World Health Organization (WHO) states that
more than 61.6 million people were reported to have been treated for schistosomiasis in 2014,
and at least 258 million people were estimated to be in need of preventive treatment for
schistosomiasis in 2014 [1]. In comparison to diseases with high mortality such as human
immunodeficiency virus (HIV) and malaria, schistosomiasis exists at the morbidity level and has
been historically underreported [2].
Schistosomiasis is prevalent in tropical and subtropical areas, especially in poor
communities [1], and is concentrated in sub-Saharan Africa [3]. The prevalence of
schistosomiasis is very high in western Kenya, with some areas reporting prevalences as high as
65% [4].
As prevention of exposure to the parasite is challenging in areas where the disease is
endemic, the main approach to preventing morbidity from schistosomiasis is to treat people
annually with praziquantel, usually through Mass Drug Administration (MDA). MDA is the
treatment of the entire population in a geographic area with a curative dose of a drug without

2
first testing for infection and regardless of the presence of symptoms [5]. Since 2003, MDA
using praziquantel was implemented to reach children in primary schools located in areas where
the disease is endemic for schistosomiasis, and all children are treated irrespective of their
infection status [6]. In children, schistosomiasis typically presents with generalized, non-specific
signs and symptoms, making it difficult to identify disease-specific morbidity indicators and
challenging to develop tools for assessing those indicators [3]. In school-aged children, infection
can cause anemia, decreased growth, liver abnormalities, and deficits in cognitive functioning.
Therefore, it is important to prevent schistosomiasis infection in children.
Most previous studies [2-5] about schistosomiasis in children focused on subtle morbidity
including anemia, debilitating, stunted growth, impaired cognitive development, etc., before and
after the treatment. Very few studies investigated children’s behaviors that are vital for their
healthy development of children. In this study, we propose to assess children’s behavior before
and after mass drug administration with praziquantel in Kenya using the BASC-2 tool.
BASC-2 is the second edition of the behavior assessment system for children. It is a
norm-referenced diagnostic tool designed to assess the behavior and self-perceptions of children
and young adults aged 2 through 25 years [7]. It was designed to facilitate the differential
diagnosis and educational classification of a variety of emotional and behavioral disorders of
children and to aid in the design of treatment plans [8]. It typically asks respondents to report
how often a child displays various behaviors, leaving it to them to judge how situational factors
should be taken into account [9]. Teachers rate the presence of behaviors in children on a four-
point frequency scale (i.e., 1=Never, 2=Sometimes, 3=Often, and 4=Almost Always). Raw item
scores are summed and converted by BASC-2 software into T scores for easy comparison. Since
its publication in 1992, the BASC has become one of the most widely used tools for assessing

3
behavior and emotions in children, adolescents, and young adults [10]. For this study, the BASC-
2 can be very useful for reporting the children’s behaviors and comparing scores across time and
by schistosomiasis status.
To our knowledge, there is no previous study in which the BASC-2 was used to collect
raw data and generate reports about children’s behaviors to detect the differences in children
with and without schistosomiasis, and to evaluate the changes in children’s behaviors before and
after the treatment with praziquantel. Scientific advances in the field calls for the study of the
impact of MDA on behaviors among school-age children using BASC-2 for a better
understanding of the current practices in treating schistosomiasis in Sub-Saharan Africa.
Research Question and Hypotheses
The purpose of the current study is to examine the impact of mass drug administration on
children’s behaviors for those with negative or positive schistosomiasis status by using the
BASC-2 Teacher Rating Scales. Specifically, this research addressed the following questions:
1. Is there a significant change in composite T scores in children after the mass drug
administration of praziquantel?
2. Do school-age children with positive schistosomiasis status have significantly
different scores on the composite scales of the BASC-2 TRS compared to children
with negative status?
3. Is there a greater change in the composite T scores following treatment among
children with positive status compared with those with negative status?

4
CHAPTER 2
MATERIAL AND METHODS
Data Collection
All the data used in this study were collected in Kenya by the U.S. Centers for Disease
Control and the Kenya Medical Research Institute. Six teachers of classes containing children
ages 8-11 years were asked to participate. These teachers were from villages where the 2014
prevalence of schistosomiasis was high and there were at least 15 children with ≥400 eggs/gram
feces using standard diagnostic tests. The class teachers were recruited to help in this study since
they spend more time with the pupils compared to others and were, therefore, in a better position
to offer insights into the pupils’ behaviors.
Prevalence surveys were conducted as usual in January 2015. A total of 36 children from
six different schools were selected for this study. Six children were selected from each school
with a participating teacher: Three children were randomly selected from children with no eggs
in their stools (negative infection status), and three were randomly selected from among those
with at least 400 eggs per gram feces (positive infection status). Parental consent and child assent
were obtained at enrollment. The teacher and investigator were blinded as to which of the
children were infected and which had no eggs in stool.
After training by the research team, teachers used the BASC-2 questionnaires forms to
evaluate the children on days prior to initiation of MDA to collect the before-treatment data.
MDA occurred in February 2015, and following MDA, the teachers evaluated the same children

5
using the BASC-2 to collect the after-treatment data. Changes in scoring between the two time
points were evaluated.
In this study, there are 36 children with a mean age of 9.9 years, with half of them (n=18)
being schistosomiasis positive, and the other half being negative based on the stool results. The
information of each child was collected twice before- and after-treatment, with the expectation
on a full dataset of 72 observations. However, there was one child from whom only before-
treatment data was recorded. Hence, 71 observations were included in the complete-case analysis
and multiple imputation approach was used to serve as a sensitivity check in the following
analysis. Together, there are 29 variables for each observation: name, id, time (before or after),
age, status (negative or positive), school, F Index, Consistency Index, Response Pattern Index,
Externalizing Problems, Internalizing Problems, School Problems, Behavioral System Index
(BSI), Adaptive Skills, Hyperactivity, Aggression, Conduct Problems, Anxiety, Depression,
Somatization, Attention Problems, Learning Problems, Atypicality, Withdrawal, Adaptability,
Social Skills, Leadership, Study Skills, and Functional Communication. The schistosomiasis
status in this study is only from the tests carried out before the treatment.
BASC-2
The Behavior Assessment System for Children (2nd edition; BASC-2) is the most widely
adopted broad-based behavioral rating scale used by school-based practitioners [6].
BASC-2 norms are based on large, representative samples and are differentiated
according to the age, sex, and clinical status of the child. There are two norms which can be
chosen to derive standard scores for the various subscales and composite: sex-based norms and
combined-sex norms [8]. The norm sample we used in this study is the general combined-sex
norm.

6
There are three types of scales in BASC-2: Teacher Rating Scales (TRS), Parent Rating
Scales (PRS), and Self-Report of Personality (SRP) [8]. In this study, we applied the TRS to
evaluate children’s school behaviors.
The TRS is a comprehensive measure of both adaptive and problematic behaviors in the
school setting. It has three forms, with items targeted at three age levels: preschool (2 through 5),
child (6 through 11), and adolescent (12 through 21) [8]. For our study, TRS-C was used, as the
ages of the enrolled students (8-11) fall into the “child” group. The TRS has between 100 and
139 items rated on a 4-point scale of behavioral frequency from “Never” to “Almost Always”.
Our working dataset has information on 129 of these items. Teachers respond to these items with
Never, Sometimes, Often, or Almost Always, respectively corresponding to the score in the
BASC-2 software of 1, 2, 3, and 4.
The BASC-TRS yields 5 composite scales, 10 clinical scales, and 5 adaptive scales. The
broad composite scales are Externalizing Problems, Internalizing Problems, School Problems,
Adaptive Skills and the Behavioral System Index (BSI). The Externalizing Problems contains
Hyperactivity, Aggression, and Conduct problems, which are disruptive in nature. The
Internalizing Problems indicates not acting-out behaviors, including Anxiety, Depression,
Somatization, Atypicality, and Withdrawal. The School Problems reflecting academic difficulties
contains Attention Problems, and Learning Problems. The Adaptive Skills is the core
characteristics of adaptive behaviors, which has five subscales: Adaptability, Functional
Communication, Social Skills, Leadership, and Study Skills. The BSI contains Hyperactivity,
Aggression, Depression, Atypicality, Withdrawal, and Attention problems, and it assesses the
overall level of problem behaviors [8]. Table 1 presents the definition of each individual scale.

7
Table 1 TRS Scale Definition
Category Composite scale Scale Definition
Clinical
scales
Externalizing
Problems
Hyperactivity The tendency to be overly active, rush
through work or activities, and act without
thinking
Aggression The tendency to act in a hostile manner
(either verbal or physical) that is
threatening to others
Conduct Problems The tendency to engage in antisocial and
rule-breaking behavior, including
destroying property
Internalizing
Problems
Anxiety The tendency to be nervous, fearful, or
worried about real and imagined problems
Depression Feelings of unhappiness, sadness, and
stress that may result in an inability to
carry out everyday activities or may bring
on thoughts of suicide
Somatization The tendency to be overly sensitive to and
complain about relatively minor physical
problems and discomforts
Atypicality The tendency to behave in ways that are
considered “odd” or commonly associated
with psychosis
Withdrawal The tendency to evade others to avoid
social contact
School Problems Attention Problems The tendency to be easily distracted and
unable to concentrate more than
momentarily
Learning Problems The presence of academic difficulties,
particularly understanding or completing
homework
Adaptive
scales
Adaptive Skills Adaptability The ability to adapt readily to changes in
the environment
Functional
Communication
The ability to express ideas and
communicate in a way others can easily
understand
Social Skills The skills necessary for interacting
successfully with peers and adults in home,
school, and community settings
Leadership The skills associated with accomplishing
academic, social or community goals,
including the ability to work with others
Study Skills The skills that are conducive to strong
academic performance, including
organizational skills and good study habits

8
The individual scales in Externalizing Problems, Internalizing Problems, School
Problems and the BSI are all clinical scales, which measure maladaptive behaviors, and high
scores for these behaviors indicate problematic levels. The scales in Adaptive Skills are adaptive
scales, which measure positive behaviors, and low scores indicate problematic levels. Table 2 is
an example of the report on the composite T scores BASC-2 created for one child. T scores
indicate the distance of scores from the norm-group mean, with a mean of 50 and a standard
deviation of 10. The BASC-2 T scores are not normalized; they are linear transformations of
raw-scores [8].
Table 2 Example of the Composite T Score Summary of One Child
Raw
score T score
Percentile
rank
95% confidence
interval
Externalizing Problems 139 46 41 43-49
Internalizing Problems 195 69 95 63-75
School Problems 80 39 12 34-44
Behavioral Symptoms
Index 296 49 55 46-52
Adaptive Skills 273 55 60 52-58
To ensure reliability of the scales, BASC-2 employs the factor analysis to generate the
composite T scales. Factor analysis is the statistical technique used in identifying TRS
composites which assess broad dimensions. In BASC-2, each item is placed on one factor
(scale), and all factors are allowed to be correlated [8]. Two types of factor analyses were
performed. The primary technique was covariance structure analysis (CSA). The CSA was used
to evaluate the model and modify it in an appropriate way according to the results of the analysis.
Table 3 is an example of CSA factors that provide information on construct validity of the
composites and scales. From Table 3, the Externalizing Problems factor assesses a behavior
dimension that is common to the content of the Hyperactivity, Aggression and Conduct Problem

9
[8], since they have a high level of intercorrelation. For Internalizing Problems, Depression,
Atypicality, and Withdrawal contribute more to this factor, while Anxiety and Somatization are
less informed by this factor. The School Problems factor has high correlations with both
Attention Problems and Learning Problems scales [8]. Finally, the Adaptive Skills factor has
very high intercorrelations for all the subscales except Adaptability. The second type of factor
analysis is the principal-axis analysis, which is a purely exploratory method used to see whether
factor-structure models other than those evaluated with CSA could provide a good fit to the scale
intercorrelation data [8]. Since the principal-axis method may reveal a substantially different
factor structure not indicated by CSA, it is considered to be a complement of CSA.
Table 3 Example of Factor Correlation from CSA for TRS-C
TRS-C
Scale Externalizing
Problems
Internalizing
Problems
School
Problems
Adaptive
Skills
Hyperactivity 0.89
Aggression 0.90
Conduct Problems 0.91
Anxiety 0.51
Depression 0.85
Somatization 0.41
Atypicality 0.75
Withdrawal 0.80
Attention Problems 0.91
Learning Problems 0.74
Adaptability 0.39 Functional
Communication 0.86
Social Skills 0.81
Leadership 0.91
Study Skills 0.90
To measure the validity of children’s responses, there are three indexes: F index,
Consistency index, and Response Pattern Index. The F-index score is a tally of the number of
times the respondent provides a very negative behavior rating [8]. The Response Pattern Index is

10
designed to identify forms that may be invalid due to that fact that the respondents are inattentive
to the item content [8]. The Consistency Index identifies cases in which the respondent offer
inconsistent answers to items that usually are answered similarly [8]. If the responses are
consistent, the value of Consistency Index is “acceptable”; otherwise, the Consistency Index is
“caution”. The Response Pattern index is acceptable for all the observations in our study, so we
only conducted further analysis on the F Index and Consistency Index.
In our analysis, the BASC-2 software was used to preprocess the raw data collected from
the BASC-2 TRS-C questionnaires to generate T scores, which were then entered into a working
dataset for further exploration.
Multiple Imputation
Since there are missing data in our study, we attempted to handle it statistically as a
sensitivity check. There are several popular existing practices for handling missing data. Most
procedures in SAS use the Complete-Case Analysis (CCA) by default to deal with missing data.
The approach we adopted, so-called multiple imputation (MI), often assumes that missing values
are missing at random (MAR) in which the probability that a datum is missing may depend on
observed characteristics but not on unobserved characteristics of the subject [11]. Multiple
imputation can provide unbiased statistical results given a correctly specified imputation model
[12].
There are various imputation approaches available for multiple imputation. In our
analysis, considering that we have both continuous and categorical variables to be imputed and
that an arbitrary missing data pattern allows more flexibility over a monotone missing pattern,
we applied the fully conditional specification (FCS) approach, which is based on a flexible

11
selection of univariate imputation distributions without ever formally specifying the joint
multivariate density [13].
There are three steps to dealing with missing data in multiple imputation: the first step is
to introduce random variation into the imputation process and generate several data sets, each
with different imputed values; the second step is perform the desired analysis on each data set;
the last step is to combine the results into a single set of parameter estimates, standard errors, and
test statistics. For our study, in the first step, direct replacement of subjects was done by new
subjects from an identifiable source population based on observed subject characteristics [12],
and the number of imputation datasets we created was 10 (default in SAS 9.4 is 5). In the second
step, each imputed data set again was analyzed using the standard analytical techniques
(calculating means, t test, and longitudinal analysis in this study). And in the third step, “proc
mianalyze” was used to combine the results from the 10 complete data sets. All the results of
multiple-imputation are presented in the Appendices A as a sensitivity check reference to the
primary analysis results from CCA shown in the main text.
Statistical Analysis
In the preprocessing stage for the raw data, the numerical values on a four-point scale (1,
2, 3, and 4) of the question items were entered into the BASC-2 software manually. The BASC-2
software then generated reports for each child and exported them as electronic documents. After
that, the derived T scores for the BASC TRS domains were entered into an Excel spread-sheet
with 71 observations and 29 variables, and it was later converted to a sas7bdat file for further
analysis.
The working dataset was analyzed using SAS version 9.4 (SAS Institute Inc., Cary, NC)
[14]. All tests and confidence intervals used the 5% level of significance.

12
Descriptive statistics were obtained to check the baseline information about children’s
behaviors before mass drug administration. Composite T scores were classified into three ranges
and a frequency table was given. In BASC-2, the scale and composite score classification is
shown in Table 4. We combined average, high and very high (average, low and very low) ranges
together in this analysis, since the three classes represent good behaviors. At-Risk range may
signify potential or developing problems that need to be monitored carefully, while the
clinically-significant range denotes a high level of maladaptive behaviors [8]. The mean scores
of Externalizing Problems, Internalizing Problems, School Problems, Adaptive Skills and the
Behavioral System Index (BSI) were calculated by status (Negative or Positive). A histogram
was presented to describe the mean scores of these five composite scales with negative status and
positive status. Then the analysis was repeated to get information about children’s behaviors
after the MDA.
Table 4 Scale and Composite Score Classification
Classification
T-score Range Adaptive Scales Clinical Scales
Very High Clinically Significant 70 and above
High At-Risk 60-69
Average Average 41-59
At-Risk Low 31-40
Clinically Significant Very Low 30 and below
For calculating the mean T scores of these variables by time and status simultaneously,
time and status were categorized into four groups as follows:
A-: After-treatment and negative status (without schistosomiasis)
A+: After-treatment and positive status (with schistosomiasis)
B- : Before-treatment and negative status
B+: Before-treatment and positive status

13
Further descriptive analysis was conducted for the subscales of each composite scale to
explore which subscale contributed more to the composite T scores of each composite scale, and
should consequently draw more attention.
Normality checking for the dataset was done using the QQ plot by time and status
respectively, to ensure that methods relying on normal distributional assumptions are valid.
To test the first hypothesis on whether there is a significant difference in the composite T
scores between before-treatment and after-treatment, a paired two-sample t-test was conducted.
The paired sample t-test typically consists of a sample of matched pairs of similar units, or one
group of units that has been tested twice, as was the case in our BASC-2 evaluated T scores. In
addition, we also considered the paired two sample Hotelling’s T2 test of multivariate scales as a
supplementary method to test the differences in composite T scales with an adjustment for
multiple comparisons [15]. A profile analysis was conducred as part of the Hotelling’s T2 test,
and confidence intervals were obtained. By using the profile analysis, we can visually compare
the change of mean scores in each composite scale across the before-treatment group and after-
treatment group.
Spaghetti plots were presented by positive and negative group respectively for
Externalizing Problems, Internalizing Problems, School Problems, Adaptive Skills and the
Behavioral System Index (BSI) to explore the difference in trajectories of child’s behaviors
following the MDA.
To test the second hypothesis on whether there is a significant difference between the
schistosomiasis negative and positive groups, multi-level linear mixed effects models were built
for each composite scale. Linear mixed effects models are particularly useful in settings where
repeated measurements are made on the same statistical units (longitudinal study), or where

14
measurements are made on clusters of related statistical units. Longitudinal studies can be very
powerful, both statistically and scientifically, because they enable one to study changes within
individual subjects over time or under varied conditions [16]. To account for correlated outcome
measures, linear mixed effects models estimate a pooled multi-level equation by simultaneously
incorporating fixed and random effects [17].
The following linear mixed-effects model was considered:
Yijk = β0 + β1 Status + β2Time+ β3 Status*Time + εk + εi(k) + eijk ,
where Yijk represents the mean in composite T score of each composite scale for child i at jth
time of the kth school, β0 is the fixed intercept, β1, β2, and β3 are fixed coefficients of status, time
and the interaction term, eijk ~ N(0, σe2) is the measurement error, εk ~ N(0, σb1
2) is the random
effect at school level, εj(k) ~ N(0, σb22) is the random effect at individual level. For all the fits, we
used usual normal maximum likelihood (ML) with an unstructured covariance model. Several
covariance models had been tried, but the AIC of unstructured covariance model was the
smallest one, so we selected unstructured covariance model in the analysis.
Finally, a subgroup analysis and an independent sample t test were run to test the third
hypothesis: whether the change is greater in composite T scores following treatment among
children with positive status than among those with negative status.
Since the F Index and Consistency Index for some children changed after the treatment,
McNemar’s Tests were conducted to test the difference in F Index and Consistency Index
following MDA. In the BASC-2 software, there are 3 levels of F Index and Consistency Index:
acceptable, caution, extreme caution. In our study, we combined the “caution” and “extreme
caution together as flags for extra attention and created a 2x2 McNemar’s Test table. Here we
chose McNemar’s Test over Chi-square Test due to the fact that our variables are paired.

15
McNemar’s Test does not test for independence, but consistency in response across two variables
[18].

16
CHAPTER 3
RESULTS AND DISCUSSION
Results
Baseline information about children’s behaviors before the mass drug administration,
such as the frequency of the overall range of children’s behaviors (Table 5) and the means of the
composite T scores of the Externalizing Problems, Internalizing Problems, School Problems,
Adaptive Skills and BSI (Table 6) were obtained. From Table 5, more schistosomiasis positive
children are in the at-risk range and the clinically-significant range than schistosomiasis negative
children in all of the five composite scales. In both schistosomiasis status groups, children
behaved the worst on internalizing problems, in which most of them are categorized into the
below-average range, and the best on adaptive skill with none in the clinically-significant range.
From Table 6 and Figure 1, the mean scores of the Externalizing Problems, Internalizing
Problems, School Problems and BSI are larger in the positive group than in the negative group,
suggesting that children with schistosomiasis have more severe problematic behaviors. Among
these composite scales, the difference between negative group (54.61) and positive group (61.72)
is the greatest for the mean score of the Externalizing Problems. The mean scores of
Externalizing Problems, School Problems and BSI from the schistosomiasis positive status group
are in the at-risk range, as compared with those categorized as average from the schistosomiasis
negative status group. Regarding Internalizing Problems, both mean scores exceed the average
range, reaching the at-risk range in the negative group, and the clinically-significant range in the
positive group. For Adaptive Skills, the mean score in the positive group is smaller than that of

17
the negative group, indicating that children in the positive group performed worse on adaptive
scales. However, the difference in the two groups (46.83 vs. 44.83) is relatively small, and both
are in the average range. The standard deviations from all the composite scales except
Internalizing Problems are larger in the positive group, suggesting lower within-group
heterogeneities from the children in the negative group.
Since missing data only occur in the after-treatment measurement, no imputation was
conducted in the baseline analyses.
Table 5 Frequency of the Classification of Children’s Behaviors before Treatment
Status Range Externalizing
Problems
Internalizing
Problems
School
Problems
Behavioral
Symptoms
Index
Adaptive
Skills
Negative Average 13 (72.22%) 3 (16.67%) 11(61.11%) 13 (72.22%) 14 (77.78%)
At-risk 4 (22.22%) 8 (44.44%) 7 (38.89%) 3 (16.67%) 4 (22.22%)
Clinically
significant 1 (5.56%) 7 (38.89%) 0 (0.00%) 2 (11.11%) 0 (0.00%)
Positive Average 9 (50.00%) 3 (16.67%) 9 (50.00%) 8 (44.44%) 10 (55.56%)
At-risk 3 (16.67%) 4 (22.22%) 6 (33.33%) 5 (27.78%) 8 (44.44%)
Clinically
significant 6 (33.33%) 11 (61.11%) 3 (16.67%) 5 (27.78%) 0 (0.00%)
Table 6 Mean Composite T Scores before Treatment
Status
Mean (Std Dev)
Externalizing
Problems
Internalizing
Problems
School
Problems
Behavioral
Symptoms Index
Adaptive
Skills
Negative 54.61 (8.17) 68.44 (13.32) 54.72 (8.65) 55.39 (8.57) 46.83 (6.91)
Positive 61.72 (11.74) 70.83 (11.25) 57.06 (12.26) 61.39 (11.42) 44.83 (8.90)

18
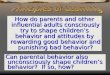
Figure 1 Mean Composite T Scores before Treatment
Similar analyses as conducted at baselined were repeated for the after-treatment
measures. After the mass drug administration, in the negative group, we observed no children in
the clinically-significant range in the Externalizing Problems, School Problems, BSI and
Adaptive Skills, and very few in the at-risk range (Table 7). For Internalizing Problems, yet more
children are in the non-average range, with minimal difference between the two groups with
different infection status. Compared to before-treatment (Table 5), overall children’s behaviors
improved in all the composite scales in both groups, with more children in the average range and
less children in the at-rick and clinically-significant range.
Table 8 and Figure 2 report the results from the after-treatment measures. The mean
scores of all the composite scales are larger in the positive group for clinical scales, while
smaller for adaptive scales. In both groups, except for Internalizing Problems, mean scores are
all in the average range for all composite scales, but mean score of Internalizing Problems spread
out in all three ranges. All of the mean scores are smaller from the after-treatment measures for
clinical scales, and larger for adaptive scales than measures from the before-treatment. The
0
10
20
30
40
50
60
70
80
Externalizing
Problem
Internalizing
Problem
School Problem Behavioral
Symptoms Index
Adaptive Skills
Negative Positive

19
results suggest that children’s problematic and adaptive behaviors were both improved after the
MDA with praziquantel.
A sensitivity check considering missing data with multiple imputation was implemented
and minimal differences were detected (Appendices A. Table 1).
Table 7 Frequency of the Classification of Children’s Behaviors after Treatment
Status Range Externalizing
Problems
Internalizing
Problems
School
Problems
Behavioral
Symptoms
Index
Adaptive
Skills
Negative
Average 16 (88.89%) 7 (38.89%) 18 (100.00%) 14 (77.78%) 15 (83.33%)
At-risk 2 (11.11%0 6 (33.33%) 0 (0.00%) 4 (22.22%) 3 (16.67%)
Clinically
Significant 0 (0.00%) 5 (27.78%) 0 (0.00%) 0 (0.00%) 0 (0.00%)
Positive
Average 11 (64.71%) 5 (29.41%) 13 (76.47%) 10 (58.82%) 12 (70.59%)
At-risk 5 (29.41%) 6 (35.29%) 4 (23.53%) 5 (29.41%) 4 (23.53%0
Clinically
Significant 1 (5.88%) 6 (35.29%) 0 (0.00%) 2 (11.76%) 1 (5.88%)
Table 8 Mean Composite T Scores after Treatment
Status
Mean (Std Dev)
Externalizing
Problems
Internalizing
Problems
School
Problems
Behavioral
Symptoms Index
Adaptive
Skills
Negative 52.22 (4.83) 62.22 (10.69) 49.94 (6.90) 53.94 (6.92) 49.61 (9.06)
Positive 56.71 (7.93) 66.59 (13.25) 51.71 (9.82) 57.47 (9.68) 46.71 (10.04)
Figure 2 Mean Composite T Scores after Treatment
0
10
20
30
40
50
60
70
Externalizing
Problem
Internalizing
Problem
School Problem Behavioral
Symptoms Index
Adaptive Skills
Negative Positive

20
Figure 3 Mean Composite T Scores by Status and Time
Further analyses on all the subscales under each composite scale were conducted. From
Table 9, for Externalizing Problems, the mean score of Aggression is the highest. The other two,
Hyperactivity and Conduct Problem, have similar mean scores that are below the composite T
scores of the Externalizing Problems.
The results of multiple imputation (Appendices A. Table 2) suggest that overall
difference in mean scores is negligible, while the change of standard deviation in Conduct
Problem is worth noticing.
Table 9 Mean Scores of Subscales of Externalizing Problems
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
Externalizing
problem 61.72 (11.74) 54.61 (8.17) 56.71 (7.93) 52.22 (4.83)
Hyperactivity 59.17 (10.07) 52.78 (6.20) 55.24 (7.51) 51.61 (4.77)
Aggression 64.89 (13.53) 56.44 (12.25) 58.59 (8.02) 54.56 (7.25)
Conduct Problem 58.78 (12.98) 53.50 (7.33) 54.59 (10.33) 50.06 (4.39)
0
10
20
30
40
50
60
70
80
Externalizing
Problem
Internalizing
Problem
School Problem Behavioral
Symptoms Index
Adaptive Skills
B- B+ A- A+

21
From Table 10, for Internalizing Problems, Somatization has the highest mean score with
a considerable margin over the other subscales. Almost all the mean scores of these subscales are
at average range in both groups at each time.
After multiple imputation (Appendices A. Table 3), the mean scores of all the subscales
except Atypicality had a negligible increase. All the standard deviations increased, and the
changes in Anxiety, Atypicality, and Withdrawal are large while the others can be neglected.
From Table 11, for School Problems, the mean T score of Learning Problem is larger
than that of Attention Problem, suggesting that children may behave better on Attention
Problem, while both of the mean scores are still in the average range.
Sensitivity checks with multiple imputation (Appendices A. Table 4) showed minimal
differences that are considered to be negligible.
Results on Adaptive Skills are presented in Table 12. Functional Communication has the
smallest mean T score which represents the worst behavior, while Social Scales has the largest
mean T score. All the mean T scores of subscales are in the average range. Consistent with the
previous analysis for the Adaptive Skills, results from subscales further confirmed that most
children’s adaptive behaviors are good.
When the missing data were handled (Appendices A. Table 5), the mean scores of
Adaptability, Functional Communication, and Study Skills had slight increases; the mean score
of Social Skills increased over 1.0, but the mean score of Leadership decreased slightly. The
standard deviations of all of the subscales increased, with a dramatic change observed in Study
Skills. All the differences in mean scores are negligible, but the changes in the standard
deviations of Adaptability, Leadership, and Study Skills are of note.

22
Table 10 Mean Scores of Subscales of Internalizing Problems
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
Internalizing
Problem 70.83 (11.25) 68.44 (13.32) 66.59 (13.25) 62.22 (10.69)
Anxiety 62.17 (13.25) 59.17 (13.00) 60.06 (12.39) 55.28 (9.00)
Depression 60.56 (11.00) 54.78 (9.32) 58.76 (12.90) 55.17 (7.16)
Somatization 77.72 (10.87) 80.44 (16.27) 70.88 (15.32) 68.94 (15.75)
Atypicality 52.83 (9.67) 52.78 (6.79) 57.65 (10.25) 53.50 (7.74)
Withdrawal 55.61 (9.11) 52.11 (11.88) 55.76 (12.14) 55.06 (12.12)
Table 11 Mean Scores of Subscales of School Problems
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
School
Problem 57.06 (12.26) 54.72 (8.66) 51.71 (9.82) 49.94 (6.90)
Attention Problem 52.83 (9.67) 52.78 (6.79) 49.82 (8.37) 48.61 (6.71)
Learning Problem 60.00(13.91) 55.89 (9.69) 53.53 (10.57) 51.44 (7.02)
Results on Adaptive Skills are presented in Table 12. Functional Communication has the
smallest mean T score which represents the worst behavior, while Social Scales has the largest
mean T score. All the mean T scores of subscales are in the average range. In consistent with the
previous analysis for the Adaptive Skills, results from subscales further confirmed that most
children’s adaptive behaviors are good.
When the missing data were handled (Appendices A. Table 5), the mean scores of
Adaptability, Functional Communication, and Study Skills had slight increases; the mean score
of Social Skills increased over 1.0, but the mean score of Leadership decreased slightly. The
standard deviations of all of the subscales increased, with a dramatic change observed in Study

23
Skills. All the differences in mean scores are negligible, but the changes in the standard
deviations of Adaptability, Leadership, and Study Skills are of note.
Table 12 Mean Scores of Subscales of Adaptive Skills
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
Adaptive
Skills 44.83 (8.90) 46.83 (6.91) 46.71 (10.04) 49.61 (9.06)
Adaptability 45.22 (6.44) 45.39 (5.92) 44.41 (6.47) 46.00 (8.49)
Functional
Communication 41.50 (12.32) 45.83 (9.69) 42.59 (13.69) 46.17 (9.90)
Social Skills 47.28 (9.27) 47.61 (7.96) 50.41 (10.91) 53.00 (10.66)
Leadership 47.22 (8.58) 48.33 (8.42) 49.71 (8.21) 51.00 (7.82)
Study Skills 46.39 (10.89) 48.67 (7.75) 48.12 (9.96) 52.00 (6.74)
As a helpful diagnostic procedure, the Quantile-Quantile (QQ) Plots of the Externalizing
Problems, Internalizing Problems, School Problems, BSI and Adaptive Skills by time and by
status are shown in Figure 4 and Figure 5. No obvious violations on the normal distribution
assumptions were detected.

24
Figure 4 QQ Plots by Time

25
Figure 5 QQ Plots by Status

26
To test whether there is a significant difference in composite T scores between before-
after-treatment measures, a paired-sample t test was performed. Table 13 shows the results from
the paired t-test. All the p-values of the composite scales except Adaptive Skills are less than
0.05, suggesting significant differences in children’s behaviors following treatment for
Externalizing Problems, Internalizing Problems, School Problems, and BSI. All the significant
variables are clinical scales, which measure problematic levels. These evidences indicate that the
problematic behaviors of children significantly improve after the treatment.
From the results of multiple imputation (Appendices A. Table 6), the mean differences in
all clinical scales decreased with an increasing p-value, yet still remain all-significant. For
Adaptive Skill, the mean difference increased with a lower p-value that is over 0.05. In
summary, conclusions from the testing of the difference in composite T scores following MDA
did not change after dealing with the missing data.
Table 13 Paired T-test: Before-treatment (𝑋1) vs After-treatment (𝑋2)
Variable 𝑿𝟏 − 𝑿𝟐
SE(𝑿𝟏 − 𝑿𝟐
) t d.f. p-value
Externalizing
Problem 4.00 1.34 2.97 34 0.0054
Internalizing
Problem 5.37 2.07 2.59 34 0.0139
School Problem 5.26 1.35 3.91 34 0.0004
BSI 2.89 1.37 2.11 34 0.0425
Adaptive Skill -2.43 1.34 -1.81 34 0.0784
Hotelling’s T2 test was conducted for multivariate analysis with multiple comparison
adjustments. From Table 14, we reject the hull hypothesis (F = 6.06; d.f. = 5, 30; p = 0.0005).
Results of the paired Hotelling’s T2 test indicate that the mean composite T score of at least one
of the five composite scales changed following the MDA with praziquantel.

27
Table 14 MANOVA Test and Exact F statistics
Statistic Value F Value Num DF Den DF Pr > F
Wilks’ Lambda 0.49769 6.06 5 30 0.0005
Pillai’s Trace 0.50231 6.06 5 30 0.0005
Hotelling-Lawley Trace 1.00926 6.06 5 30 0.0005
Roy’s Greatest Root 1.00926 6.06 5 30 0.0005
Simultaneous and Bonferroni 95% confidence intervals were computed for the
Hotelling’s T2 test. The mean score of the School Problems decreased by 5.26 (95% confidence
interval, 0.15858, 10.3557) following the MDA with praziquantel. Since all the remaining
intervals include zero, the mean scores of the Externalizing Problems, Internalizing Problems,
BSI and the Adaptive Skills did not change significantly following the treatment.
Table 15 Simultaneous and Bonferroni Confidence Interval:
Before-treatment (𝑋1) vs After-treatment (𝑋2)
Variable 𝑿𝟏 − 𝑿𝟐
95% confidence interval
Simultaneous Bonferroni
Externalizing Problem 4.00 (-1.09538, 9.0954) (0.33094, 7.6691)
Internalizing Problem 5.37 (-2.47891, 13.2218) (-0.28141, 11.0243)
School Problem 5.26 (0.15858, 10.3557) (1.58579, 8.9285)
BSI 2.89 (-2.30298, 8.0744) (-0.85054, 6.6220)
Adaptive Skill -2.43 (-7.49852, 2.6414) (-6.07932, 1.2222)
A profile plot was drawn to see the difference of mean composite T scores between
before- and after-treatment measures. From Figure 6, the largest difference is seen from the
Internalizing Problems, with a comparable difference observed from the School Problems as
well. The results of Hotelling’s T2 test for parallel profiles are shown in Table 15. We found
strong evidence against the null hypothesis of parallel profiles (F = 6.14; d.f. = 4, 31; p =
0.0009). The change in mean composite T scores following MDA depends on the composite
scales.

28
Figure 6 Profile Plot of Composite Scales: Before-treatment vs After-treatment
Table 16 MANOVA Test and Exact F statistics for Parallel Profiles
Statistic Value F Value Num DF Den DF Pr > F
Wilks’ Lambda 0.55813 6.14 4 31 0.0009
Pillai’s Trace 0.44187 6.14 4 31 0.0009
Hotelling-Lawley Trace 0.79170 6.14 4 31 0.0009
Roy’s Greatest Root 0.79170 6.14 4 31 0.0009
The p-value of the Adaptive Skills is not significant, yet it reaches marginal significance.
Hence, we extended analyses to the subscales of the Adaptive Skills. From Table 17, the p-value
of both Social Skills and Study Skills are significant, while the other three are not,, suggesting
different impacts on the subscales from MDA.

29
Table 17 Paired T-test for Adaptive Scales: Before-treatment (𝑋1) vs After-treatment (𝑋2)
Variable 𝑿𝟐 − 𝑿𝟏
SE(𝑿𝟐 − 𝑿𝟏
) t d.f. p-value
Adaptability -0.09 1.26 -0.07 34 0.9462
Social Skills 4.29 1.76 2.44 34 0.0200
Leadership 2.69 1.56 1.73 34 0.0940
Study Skills 2.74 1.31 2.09 34 0.0444
Functional
Communication 0.77 1.79 0.43 34 0.6689
Spaghetti plots were drawn to see the trends of child’s behaviors following the MDA.
From Figure 7, for Externalizing Problems and School Problems, the changes in the positive
group are more substantial than those observed from the negative group following treatment,
with subject-level trajectories being highly heterogeneous. For Internalizing Problem, BSI, and
Adaptive Skills, the difference of the changes between the groups with positive and negative
status is not obvious and the subject-level heterogeneity is further confirmed.

30
Figure 7 Spaghetti Plots for Externalizing Problems, Internalizing Problems, BSI, School
Problems and Adaptive Skills

31
Linear mixed effects models were built for each composite scale. From Table 17, for
status, the p-values of Externalizing Problems and BSI are significant, indicating that the average
of the mean scores for children’s behaviors in Externalizing Problems and Behavioral Symptoms
Index are significantly different for the negative and positive groups. For before- and after-
treatment comparison, the p-value of BSI is not significant from this model, while it was
significant from the previous paired t-test, indicating that an adjusted model reduces the evidence
in favor of a significant change. For the interaction Status*Time, since none of the p-values for
each composite scale is significant, changes over time doesn’t appear to differ between infected
and non-infected subjects.
Results after the multiple imputation (Appendices A. Table 7) show that, for the
comparisons between infection status, the p-values of Internalizing Problems and Adaptive Skills
had a dramatic increase while the p-values for other composite scales did not increase much. The
p-value of Externalizing Problems and School Problems are still significant, and the others are
not significant. For the before- and after- treatment comparison, similar as the results from the
status comparison, the p-values of Internalizing Problems increased a significant amount that
leads to a fundamental change in the conclusion. On the contrary, the p-value of BSI reached the
0.05 significance level after missing values were handled by multiple imputation. These results
are worthy of notice. For the interaction term, the p-values did not change significantly and no
previous conclusions from CCA were violated.
Table 18 P-values of Type 3 Tests of Fixed Effect
Effect
P Values
Externalizing
Problems
Internalizing
Problems
School
Problems
Behavioral
Symptoms Index
Adaptive
Skills
Time 0.0074 0.0142 0.0006 0.0522 0.0897
Status 0.0041 0.2632 0.3053 0.0192 0.1918
Time*Status 0.3064 0.6307 0.8296 0.3574 0.7152

32
Tables 19 to Table 23 present the solutions for fixed effects from the linear mixed effects
models fitted for the five composite scales. The P-values for the interaction terms in all five
models are not significant at the 0.05 level, reflecting a lack of evidence in support of a deviation
in the change of composite scales between the infection positive and negative subjects.
From the results after multiple imputation (Appendices A. Table 8-12), the single
estimates of Time and Time*Status changed slightly, but the overall influence of Time and
Status on each Composite T scale stayed relatively unchanged.
The fitted model can be written as:
E(Externalizing Problems) = 61.72 -5.13Time-7.11Status+2.74Time*Status
E(Internalizing Problems) = 70.83 -4.26Time-2.39Status-1.96Time*Status
E(School Problems) = 57.06 -5.35Time-2.33Status+0.58Time*Status
E(BSI) = 61.39 -3.94Time-6.00Status+2.49Time*Status
E(Adaptive Skills) = 44.83 +1.81Time+2.00Status+0.97Time*Status
Table 19 Solution for Fixed Effects of Externalizing Problems
Effect Status Estimate S.E. DF t p-value
Intercept 61.72 2.50 5 24.66 <.0001
Time After -5.13 1.88 33 -2.72 0.0102
Status Negative -7.11 2.27 33 -3.14 0.0036
Time*Status After*Negative 2.74 2.63 33 1.04 0.3064
Table 20 Solution for Fixed Effects of Internalizing Problems
Effect Status Estimate S.E. DF t p-value
Intercept 70.83 3.24 5 21.86 <.0001
Time After -4.26 2.89 33 -1.47 0.1501
Status Negative -2.39 3.56 33 -0.67 0.5072
Time*Status After*Negative -1.96 4.05 33 -0.49 0.6307

33
Table 21 Solution for Fixed Effects of School Problems
Effect Status Estimate S.E. DF t p-value
Intercept 57.06 2.98 5 19.17 <.0001
Time After -5.35 1.90 33 -2.82 0.0081
Status Negative -2.33 2.36 33 -0.99 0.3292
Time*Status After*Negative 0.58 2.66 33 0.22 0.8296
Table 22 Solution for Fixed Effects of BSI
Effect Status Estimate S.E. DF t p-value
Intercept 61.39 2.84 5 21.64 <.0001
Time After -3.94 1.91 33 -2.06 0.0470
Status Negative -6.00 2.33 33 -2.57 0.0148
Time*Status After*Negative 2.49 2.67 33 0.93 0.3574
Table 23 Solution for Fixed Effects of Adaptive Skills
Effect Status Estimate S.E. DF t p-value
Intercept 44.83 2.63 5 17.03 <.0001
Time After 1.81 1.87 33 0.97 0.3409
Status Negative 2.00 2.26 33 0.88 0.3834
Time*Status After*Negative 0.97 2.62 33 0.37 0.7152
Further, separate analyses with independent sample t test were carried out to test the
difference of the before-treatment and after-treatment measures between the positive and
negative groups. From Figure 8, there is no obvious trend that the mean difference of before-
treatment and after-treatment in positive group is larger than in negative group. And the results
of t test (Table 24) show that all the p-value are not significant at the 0.05 level. Thus, the change
of composite T scores following MDA is not relative to schistosomiasis status, i.e., greater in
positive group than in negative group.
After multiple imputation (Appendices A. Table 13), the mean differences in positive
group for Externalizing Problems, Internalizing Problems, and School Problems had a very tiny
decreasing while the mean differences for BSI and Adaptive Skills increased a little. In

34
comparison to other obvious increase of standard deviation after multiple imputation in other
analyses, the standard deviation in positive group almost did not change. For each confidence
interval, 0 is included, which means that there is no significant difference following MDA
between negative and positive group.
Table 24 Mean Changes following MDA
between Positive and Negative Groups
Variable
Mean Standard Error
P-value Positive Negative Positive Negative
Externalizing Problems 5.71 2.39 2.09 1.68 0.4475
Internalizing Problems 4.47 6.22 3.04 2.89 0.9275
School Problems 5.76 4.78 1.71 2.10 0.3455
Behavioral Symptoms
Index 4.41 1.44 2.00 1.87 0.8795
Adaptive Skills -2.06 -2.78 1.92 1.92 0.9203
Figure 8 Mean Changes following MDA
between Positive and Negative Groups
Additionally, two important indexes from BASC-2 are worthy of attention. One is the F
Index, aiming to test whether the distribution is highly skewed. The other is the Consistency
-4
-3
-2
-1
0
1
2
3
4
5
6
7
Externalizing
Problems
Internalizing
Problems
School Problems Behavioral
Symptoms Index
Adaptive Skills
Positive Negative

35
Index, which tests the respondent disregarded the item content. From Table 25, we notice that
some children with acceptable F index may have caution F index after the treatment, while the
caution F index could also become acceptable after the treatment for others. McNemar’s Test
statistic for F Index is 0.0769 with d.f. = 1, represented by a p-value close enough to 1. The result
suggests that there is a no significant difference from before-treatment to after-treatment with
regard to the F Index distributions.
Table 25 McNemar’s Test for F Index
Before-treatment After-treatment
Acceptable Caution
Acceptable 19 6
Caution 7 3
A parallel analysis was also performed for the Consistency index. Table 26 shows that
more children switched from Acceptable to Caution after-treatment than the other direction.
McNemar’s Test statistic for Consistency Index is 8.0667 with d.f. = 1 and p-value=0.0074. The
result suggests that there is a statistically significant difference from before-treatment to after-
treatment reflected by the Consistency Index. Overall, children tend to achieve better consistency
with their responses after-treatment than before-treatment.
Table 26 McNemar’s Test for Consistency Index
Before-treatment After-treatment
Acceptable Caution
Acceptable 8 2
Caution 13 12
Discussion
The purpose of the present study is to determine the impact of MDA with praziquantel on
children’s behaviors by using the BASC-2 Teacher Rating scales. As schistosomiasis is still

36
prevalent in many areas, especially in the sub-Saharan Africa, there is a need for early
prevention. Previously researchers [3] concluded that the schistosomiasis burden has been
underreported, and the signs and symptoms of schistosomiasis on children are non-specific.
Given these existing challenges, more efforts are demanded to protect children from
schistosomiasis. Despite much research devoted to the better understanding of the prevalence,
transmission, and subtle morbidity [2-5], few have investigated the impacts of schistosomiasis
infection and its treatment on school-age children’s behaviors. Our study seeks to fill in this gap.
The BASC-2 is an instrument commonly used in educational and psychological areas for the
assessment of children’s behaviors [6]. In this study, we applied BASC-2 to examine differences
in composite T scores on clinical and adaptive scales between children with positive and
negative status of schistosomiasis, as well as between before- and after-treatment with
praziquantel.
From the results, the change in mean scores for School Problems is most substantial, and
it is also the only composite scale reaching significance when before- and after- treatment score
are compared in both paired t-test and Hotelling’s T2 test. The findings are in consistent with
literatures reporting that schistosomiasis can directly cause a reduced ability to learn [19]. It
appears that schistosomiasis can also cause children to be aggressive and/or overly active, since
the mean differences in Externalizing Problems are highly significant not only following the
treatment, but also between the two infection status groups. Often, behaviors included in
Externalizing Problems are obvious act-out behaviors that are relatively easy for teachers to
notice, and that would partly explain the directly detected differences even with a limited sample
size. Although the change in the overall Adaptive Skills is only marginally different, the
differences in Social Skills and Study Skills following MDA are both significant. This suggests

37
that the MDA might have the largest impacts on these two adaptive behaviors. Alternatively, the
Study Skills is also considered to be highly correlated with the ability of learning, and can be
directly influence by schistosomiasis infection.
The significant results we received from paired two sample t test differ from the results
from the Hotelling’s T2 test. From the paired t test, the differences of mean scores between
before-treatment and after-treatment are significant for Externalizing Problems, Internalizing
Problems, School Problems and the BSI, all of which are clinical scales. The Hotelling’s T2 test
only detects the difference in School Problem as statistically significant, as it controls the
experiment-wise error rate and thus is relatively conservative with Bonfferoni or similar
corrections for the multiple comparison issue. Compared to the significance level (α = 0.05) used
in paired t test, Bonferroni procedure is more conservative with a significance level of 𝛼
𝑛 (n is the
total number of hypothesis tested). As a consequence, we achieved relatively conservative results
from the Hotelling’s T2 test. However, given the limited sample size in this study, we only
consider the Hotelling’s T2 test as a supplementary analysis to confirm some of the conclusions
from the previous analysis, i.e. the School Problem scale changed significantly from before- to
after- treatment. While the nice feature of controlling overall type-I error in multiple comparison
settings from the approach is well acknowledged and appreciated, it could potentially reduce the
power in small sample scenarios. Therefore, it is more appropriate to view the insignificant
results on the Externalizing Problems, Internalizing Problems, and the BSI from the Hotelling’s
T2 test as indications for follow-up confirmatory studies with larger sample size.
A higher level of heterogeneity in composite scales’ changing trajectories were observed
in the children belonging to the negative status group, with the composite T scores did not
change much for some but increase or decrease dramatically for others. The discrepancy is more

38
substantial in the Externalizing Problems and School Problems. One possible explanation is that
some children in the schistosomiasis negative group were in fact false negative, with eggs being
present but not detected from the stool.
Multiple imputation approaches were implemented as a sensitivity check for several main
statistical analyses to deal with the missing data. In general, results did not differ significantly
and most of the changes were negligible. Therefore, we conclude that the primary complete-case
analyses as presented in the main manuscript are valid and robust.
Several limitations of this study are worth noting. The sample size for this study was
relatively small, with a total of 36 students form six different schools, which may potentially
make some of the analyses underpowered. Future studies with a significantly increased sample
size are warranted to confirm our findings. With a larger sample size, conclusions on the
interaction effects between treatment and infection status could be more deterministic. In
addition, only TRS was used in this study. We believe that future studies using PRS and SRP
will certainly add more in-depth discussions on the topic. The age group of children from 8 to 11
is narrow; hence, most of the findings from the current study are only representative of the
“child” category from TRS. However, we hope that this work could pave the ways for studies
looking into the application of BASC-2 to other age groups such as “preschool” or “adolescent”
in future schistosomiasis research. The adjusted covariates in this study are very few, so findings
are subject to potential biases due to confounding. For instance, the socioeconomic status (SES)
including some quantification of family income, parental education, etc., if available, can be
included as covariates, as those have been previously reported to impact children’s behaviors
[20]. In addition, schools in closest proximity to lakes or rivers tend to have high schistosomiasis
prevalence rates [4], thus, if spatial information such as the distance from the schools to water

39
bodies can be collected and adjusted in future studies, it will enhance our knowledge in better
understanding the geographic impacts. Further, the original BASC-2 was designed for children
samples taken in the United States and Latin America [8], and this study applied the same tool to
children in Kenya Future research is demanded to verify to the validity of using BASC-2 to
assess children’s behaviors in African countries, where the culture and social economic
situations are certainly quite different.

40
CHAPTER 4
CONCLUSION
In general, children with negative schistosomiasis status have better behaviors than those
with positive status at both before- and after-treatment. All behaviors as assessed by mean T
scores from composite scales showed improvements after the mass drug administration with
praziquantel. For Externalizing Problems, Internalizing Problems, School Problems, and BSI, all
of which belonging to the clinical scales, there are significant decrease in mean composite T
scores following treatment. For Externalizing Problems and BSI, the school-age children
schistosomiasis positive obtain significantly different scores compared to children
schistosomiasis negative. The changes in composite T scores following treatment for children
with negative schistosomiasis status are not larger than those with positive status. There is also a
significant difference on Consistency Index between before-treatment and after-treatment.

41
REFERENCE
1. Schistosomiasis. (2016). Retrieved April 11, 2016, from
http://www.who.int/mediacentre/factsheets/fs115/en/
2. Samuels, A. M., Matey, E., Mwinzi, P. N., Wiegand, R. E., Muchiri, G., Ireri, E., . . .
Secor, W. (2012). Schistosoma mansoni Morbidity among School-Aged Children: A
SCORE Project in Kenya. The American Society of Tropical Medicine and Hygiene,
87(5), 874-882.
3. Davis, S. M., Wiegand, R. E., Mulama, F., Kareko, E. I., Harris, R., Ochola, E., . . . Won,
K. Y. (2015). Morbidity Associated with Schistosomiasis Before and After Treatment in
Young Children in Rusinga Island, Western Kenya. The American Society of Tropical
Medicine and Hygiene, 92(5), 952-958.
4. Odiere, M. R., Opisa, S., Odhiambo, G., Jura, W. G., Ayisi, J. M., Karanja, D. M., &
Mwinzi, P. N. (2011). Geographical distribution of schistosomiasis and soil-transmitted
helminths among school children in informal settlements in Kisumu City, Western
Kenya. Parasitology, 138(12), 1569-1577.
5. Use of Antimalarials to Reduce Malaria Transmission. (2015). Retrieved April 11, 2016,
from http://www.cdc.gov/malaria/malaria_worldwide/reduction/mda_mft.html
6. Hass, M. R., Brown, R. S., Brady, J., & Johnson, D. B. (2012). Validating the BASC-
TRS for Use with Children and Adolescents with an Educational Diagnosis of Autism.
Remedial And Special Education, 33(3), 173-183.

42
7. Community-University Partnership for the Study of Children, youth, and Families
(2011). Review of the Behavior Assessment System for Children –Second Edition
(BASC-2). Edmonton, Alberta, Canada.
8. Reynolds, C. R., & Kamphaus, R. W. (2004). BASC 2, Behavior assessment system for
children. Circle Pines, MN: American Guidance Service.
9. Hartley, A., Wright, J., Zakriski, A., & McCarthy, C. (n.d). The Influence of Clinical
Experience and Assessment Method on the Evaluation of Child Behavior Change.
Journal of Psychopathology and Behavioral Assessment, 36(3), 358-370.
10. Kabatereine, N., Tukahebwa, E., Kazibwe, F., Namwangye, H., Zaramba, S., Brooker, S.,
& ... Fenwick, A. (n.d). (2006). Progress towards countrywide control of schistosomiasis
and soil-transmitted helminthiasis in Uganda. Transactions Of The Royal Society Of
Tropical Medicine And Hygiene, 100(3), 208-215.
11. Donders, A., van der Heijden, G., Stijnen, T., & Moons, K. (n.d). Review: A gentle
introduction to imputation of missing values. Journal of Clinical Epidemiology, 59(10),
1087-1091.
12. Mitra, R., & Reiter, J. P. (2016). A comparison of two methods of estimating propensity
scores after multiple imputation. Statistical Methods In Medical Research, 25(1), 188-
204. doi:10.1177/0962280212445945
13. Van Buuren, S. (2007). Multiple imputation of discrete and continuous data by fully
conditional specification. Statistical Methods in Medical Research, 16(3), 219.
14. SAS Institute Inc. (n.d.). SAS (Version 9.4) [Computer software], Cary, NC

43
15. Freeman, J., & Modarres, R. (2006). Efficiency of t -Test and Hotelling's T2 -Test After
Box-Cox Transformation. Communications In Statistics: Theory & Methods, 35(6),
1109-1122. doi:10.1080/03610920600672203.
16. Burton, P., Gurrin, L., & Sly, P. (1998). Extending the simple linear regression model to
account for correlated responses: an introduction to generalized estimating equations and
multi-level mixed modelling. Statistics in Medicine, 17(11), 1261-1291.
17. Muth, C., Bales, K. L., Hinde, K., Maninger, N., Mendoza, S. P., & Ferrer, E. (2016).
Alternative Models for Small Samples in Psychological Research: Applying Linear
Mixed Effects Models and Generalized Estimating Equations to Repeated Measures
Data. Educational And Psychological Measurement, 76(1), 64-87.
18. The Difference Between a Chi-Square Test and a McNemar Test. (n.d.). Retrieved April
27, 2016, from http://www.theanalysisfactor.com/difference-between-chi-square-test-
and-mcnemar-test/
19. Epidemiological situation. (n.d.). Retrieved April 27, 2016, from
http://www.who.int/schistosomiasis/epidemiology/en/
20. Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic Status and Child Development.
Annual Review of Psychology, 53, 371-399.

44
APPENDICES A
MULTIPLE IMPUTATION RESULTS
Table 1 Mean Composite T Scores after Treatment (by Imputation)
Status
Mean (Std Dev)
Externalizing
Problems
Internalizing
Problems
School
Problems
Behavioral
Symptoms Index
Adaptive
Skills
Negative 52.22 (4.83) 62.22 (10.69) 49.94 (6.90) 53.94 (6.92) 49.61 (9.06)
Positive 56.44 (8.87) 66.83 (13.67) 51.75 (10.17) 57.01 (10.01) 47.10 (11.04)
Table 2 Mean Scores of Subscales of Externalizing Problems (by Imputation)
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
Externalizing
problem 61.72 (11.74) 54.61 (8.17) 56.44 (8.87) 52.22 (4.83)
Hyperactivity 59.17 (10.07) 52.78 (6.20) 54.43 (8.78) 51.61 (4.77)
Aggression 64.89 (13.53) 56.44 (12.25) 57.98 (8.43) 54.56 (7.25)
Conduct Problem 58.78 (12.98) 53.50 (7.33) 55.39 (13.41) 50.06 (4.39)
Table 3 Mean Scores of Subscales of Internalizing Problems (by Imputation)
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
Internalizing
Problem 70.83 (11.25) 68.44 (13.32) 66.83 (13.67) 62.22 (10.69)
Anxiety 62.17 (13.25) 59.17 (13.00) 60.70 (15.31) 55.28 (9.00)
Depression 60.56 (11.00) 54.78 (9.32) 58.52 (13.00) 55.17 (7.16)
Somatization 77.72 (10.87) 80.44 (16.27) 71.30 (16.17) 68.94 (15.75)
Atypicality 52.83 (9.67) 52.78 (6.79) 56.13 (13.64) 53.50 (7.74)
Withdrawal 55.61 (9.11) 52.11 (11.88) 56.28 (15.61) 55.06 (12.12)

45
Table 4 Mean Scores of Subscales of School Problems (by Imputation)
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
School
Problem 57.06 (12.26) 54.72 (8.66) 51.75 (10.17) 49.94 (6.90)
Attention Problem 52.83 (9.67) 52.78 (6.79) 49.75 (9.09) 48.61 (6.71)
Learning Problem 60.00(13.91) 55.89 (9.69) 53.60 (11.09) 51.44 (7.02)
Table 5 Mean Scores of Subscales of Adaptive Skills (by Imputation)
Composite
Scales Subscales
Mean (Std Dev)
Before MDA After MDA
Positive
Group
Negative
Group
Positive
Group
Negative
Group
Adaptive
Skills 44.83 (8.90) 46.83 (6.91) 47.10 (11.04) 49.61 (9.06)
Adaptability 45.22 (6.44) 45.39 (5.92) 44.87 (9.43) 46.00 (8.49)
Functional
Communication 41.50 (12.32) 45.83 (9.69) 42.81 (15.45) 46.17 (9.90)
Social Skills 47.28 (9.27) 47.61 (7.96) 51.65 (13.07) 53.00 (10.66)
Leadership 47.22 (8.58) 48.33 (8.42) 48.99 (11.51) 51.00 (7.82)
Study Skills 46.39 (10.89) 48.67 (7.75) 48.79 (15.45) 52.00 (6.74)
Table 6 Paired T-test: Before-treatment (𝑋1) vs After-treatment (𝑋2) (by Imputation)
Variable 𝑿𝟏 − 𝑿𝟐
SE(𝑿𝟏 − 𝑿𝟐
) t d.f. p-value
Externalizing
Problem 3.84 1.33 2.90 35 0.0064
Internalizing
Problem 5.25 2.06 2.58 35 0.0142
School Problem 5.14 1.33 3.89 35 0.0004
BSI 2.77 1.36 2.06 35 0.0468
Adaptive Skill -2.47 1.34 -1.87 35 0.0698

46
Table 7 P-values of Type 3 Tests of Fixed Effect (by Imputation)
Effect
P Values
Externalizing
Problems
Internalizing
Problems
School
Problems
Behavioral
Symptoms Index
Adaptive
Skills
Time 0.0176 0.2006 0.0132 0.0365 0.3338
Status 0.0027 0.5080 0.3317 0.0137 0.4088
Time*Status 0.3223 0.6030 0.8549 0.2984 0.8677
Table 8 Solution for Fixed Effects of Externalizing Problems (by Imputation)
Effect Status Estimate S.E. DF t p-value
Intercept 61.72 2.53 5 24.38 <.0001
Time After -5.28 2.20 34 -2.40 0.0176
Status Negative -7.11 2.37 34 -3.00 0.0027
Time*Status After*Negative 2.90 2.93 34 0.99 0.3223
Table 9 Solution for Fixed Effects of Internalizing Problems (by Imputation)
Effect Status Estimate S.E. DF t p-value
Intercept 70.83 3.28 5 21.62 <.0001
Time After -4.00 3.12 34 -1.28 0.2006
Status Negative -2.39 3.61 34 -0.66 0.5080
Time*Status After*Negative -2.22 4.27 34 -0.52 0.6030
Table 10 Solution for Fixed Effects of School Problems (by Imputation)
Effect Status Estimate S.E. DF t p-value
Intercept 57.06 3.00 5 19.03 <.0001
Time After -5.30 2.13 34 -2.49 0.0132
Status Negative -2.33 2.40 34 -0.97 0.3317
Time*Status After*Negative 0.53 2.87 34 0.18 0.8549
Table 11 Solution for Fixed Effects of BSI (by Imputation)
Effect Status Estimate S.E. DF t p-value
Intercept 61.39 2.84 5 21.65 <.0001
Time After -4.38 2.08 34 -2.10 0.0365
Status Negative -6.00 2.43 33 -2.47 0.0137
Time*Status After*Negative 2.93 2.82 33 1.04 0.2984

47
Table 12 Solution for Fixed Effects of Adaptive Skills (by Imputation)
Effect Status Estimate S.E. DF t p-value
Intercept 44.83 2.67 5 16.82 <.0001
Time After 2.27 2.34 34 0.97 0.3338
Status Negative 2.00 2.42 34 0.83 0.4088
Time*Status After*Negative 0.51 3.06 34 0.17 0.8677
Table 13 Mean Difference of Before-treatment and After-treatment
between Positive and Negative Groups (by Imputation)
Variable
Mean Standard Deviation 95% Confidence
Limits Positive Negative Positive Negative
Externalizing
Problems 8.04 5.5 6.32 5.00 (-4.36, 20.43)
Internalizing
Problems 10.62 11.78 7.54 6.70 (-4.16, 25.40)
School Problems 7.37 8.11 5.33 5.85 (-3.08, 17.82)
Behavioral Symptoms
Index 7.62 6.56 5.28 4.44 (-2.72, 17.97)
Adaptive Skills 6.40 6.56 5.04 5.36 (-3.48, 16.29)