Embed Size (px)
Citation preview

Assessment of Lupus (SLE) Mortality in a Patient-Based Community Data Bank Frederick Wolfe1, Kaleb Michaud1,2, Tracy Li3, Robert S. Katz4 1National Data Bank for Rheumatic Diseases, Wichita, KS; 2University of
Nebraska Medical Center, Omaha, NE; 3Bristol-Myers Squibb, Princeton, NJ; 4Rush University Medical Center, Chicago, IL
Abstract
Purpose: SLE studies usually derive from the clinic where the emphasis is on physician and laboratory assessments. Although patient-based assessments may be ideal for assessment of patient reported outcomes and mortality, there have been only rare and small systematic, longitudinal studies of SLE patient outcomes. We have reached into rheumatology practices to develop a community SLE databank to assess SLE outcomes, to determine the risk and predictors of mortality, and to confirm the utility of patient-based databanks in SLE.
Methods: We studied 1,324 patients with SLE, 2,809 with fibromyalgia (FM), 3,825 with non-inflammatory rheumatic disorders (NIRD), and 14,444 with rheumatoid arthritis (RA). Patients were assessed semi-annually by questionnaires that included detailed demographics, all patient-reported outcomes, treatments, and comorbid conditions. The risk of mortality was assessed by age and sex adjusted time-varying Cox regression analyses, expressed as hazard ratio (95% confidence interval). The discriminatory ability of baseline predictors was assessed by Harrell's c (C).
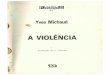
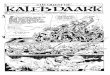
Results: At entry, median age and disease duration of SLE patients was 48.9 and 11.8 years, and 94% were women. Lifetime treatments included corticosteroids (CS) 81.3%, hydroxychloroquine, 82.9%, methotrexate 28.6%, azathioprine 26.0%, and cyclophosphamide 13.0%. During a mean follow-up of 2.5 years, range (0.5 to 10.1 years), 30 of the 1,324 SLE patients died. The resultant estimated 5-year survival was 94.9% (91.5% to 97.0%). Compared with patients with NIRD, FM, and RA, the hazard ratio (HR) for mortality was 2.8 (1.9, 4.1), 3.6 (2.4, 5.4), and 2.1 (1.5, 3.1). In general, the strength of comorbidity predictors was similar across all rheumatic disorders. The HR for stroke was 7.7 (1.7, 31.3), for myocardial infarction 3.3 (0.4, 25.1), and for GI ulcer 3.6 (1.1, 12.2). But confidence intervals overlapped between SLE and the other disorders, and no definite differences among disorders could be identified. Using baseline predictors in patients with SLE, we found that age (HR 1.5 (1.1, 2.1)) per 10 years and being male (HR 3.5 (1.4, 8.8)) increased mortality risk. After adjustment for age and sex, only household income (HR 1.2 per $US 10,000 reduction in income), among demographic predictors, was significantly associated with mortality. In particular, education, ethnicity, and marital status were not significant in this model. Mortality was best predicted by baseline HAQ-II (HR 3.9 (2.1, 7.3), C=0.82), compared with HAQ (HR 1.7 (1.0, 2.7), C=0.67), and SF-36 PCS (HR 0.95 (0.92, 0.99), C=0.75). In multivariable analyses only HAQ-II was significant. Other significant multivariable predictors of mortality included age sex, household income, preexisting renal, cardiovascular and GI ulcer conditions, and azathioprine (HR 1.9 (1.4, 2.6)), prednisone (HR 1.7 (1.0, 2.9)), and hydroxychloroquine (HR 0.5 (0.3, 0.7)). C for the combined model was 0.89.
Conclusion: Patient-based outcomes are highly discriminative for mortality, and functional assessment (HAQ-II) is the best overall predictor of SLE mortality. Patient-based databanks are effective in assessing lupus mortality and other outcomes..
Introduction
SLE outcome studies usually derive from the clinic where the emphasis is on physician and laboratory assessments.
Patient-based assessments are ideal for for self-reported outcomes and mortality.
However, there have been only rare and small systematic, longitudinal studies of such outcomes, probably because of limited lupus prevalence.
We have reached into rheumatology practices to develop a community SLE databank based on semi-annual patients surveys followed by medical confirmation to assess SLE outcomes.
Objectives
Determine the risk and predictors of mortality in a patient-based community data-bank.
Confirm the utility of patient-based data banks in SLE.
Methods
We used the US National Data Bank for Rheumatic Diseases (NDB)Survey RD patients, questionnaires completed every 6 months.
The questionnaires included demographic, treatment, patient-reported outcomes, and comorbid conditions.
Study groups included SLE, RA, Non-inflammatory rheumatic diseases (NIRD), and fibromyalgia.
Assessed by age and sex adjusted time-varying Cox Regression analyses.
The discriminatory ability of baseline predictors was assessed by Harrell’s C concordance statistic.
We used comparison groups, NIRD and fibromyalgia, and compared SLE and other groups to each comparison group.
In multivariable analyses HAQ-II was significant, but not HAQ or SF-36 PCS.
Other multivariable predictors included age sex, income, preexisting renal, cardiovascular and GI ulcer conditions,
Azathioprine - HR 1.9 (1.4, 2.6) Prednisone - HR 1.7 (1.0, 2.9) Hydroxychloroquine - HR 0.5 (0.3, 0.7)
C for the combined model was 0.89.
Mortality is increased in SLE, compared with RA, NIRD, and fibromyalgia.
Patients based outcomes are highly discriminative of mortality.
HAQ-II is the best predictor of SLE mortality.
Patient-based data banks are effective in assessing lupus mortality and other outcomes.
Table 1. Characteristics of SLE Patients at Entry
Figure 1. Comparative Mortality
Table 2. Predictive Ability of Demographic, Treatment, Comorbidity, and PRO Variables in SLE
Multivariable Mortality Predictors
Conclusions