Embed Size (px)
Citation preview

The 35th Conference on Priorities in Perinatal Care in South Africa was held under the auspices of the Priorities in Perinatal Care Association and sponsored by
Abbvie (Pty) Ltd.
i
Editor’s Note:
The articles included in these Proceedings were, mostly, received electronically and have been included as submitted by the presenter/author.Abstracts were included where articles were not submitted.Articles have not been included for presentations which were withdrawn and not presented at Priorities.In some cases, hyperlinks have been provided to .pdf files as this is how the articles have been submitted for the Proceedings. Click on hyperlink (different colour) in the index to take you to the article as the article is not in the Proceedings.Late submissions received after the Proceedings had been compiled and passwords allocated are included at the end of the Proceedings.References have been excluded due to the numerous different forms of referencing. References are available directly from the presenters.
ii
INDEX
DETECTING FOETUSES AT RISK OF STILLBIRTH: PILOT STUDY RESULTS. Spencer Nkosi
1
THE ROLE OF PLACENTAL HISTOLOGY IN ADVERSE PREGNANCY OUTCOMES AT A REFERRAL HOSPITAL IN THE EASTERN CAPE (Abstract). MS Mabenge
5
THE HIDDEN DANGER OF INTRA-UTERINE GROWTH RESTRICTION. RC Pattinson6
ANTENATAL COMMON MENTAL DISORDERS, SUICIDALITY AND ASSOCIATED RISK FACTORS: A CROSS-SECTIONAL SURVEY FROM A SOCIALLY ADVERSE SETTING, CAPE TOWN. Simone Honikman
9
INTEGRATING MENTAL HEALTH IN TO MATERNAL HEALTH CARE: PROMISING RESULTS TOWARDS CLOSING THE TREATMENT GAP. Simone Honikman
15
SCREENING FOR POSTPARTUM DEPRESSION AT RAHIMA MOOSA MOTHER AND CHILD HOSPITAL. SH Karolia
19
POSTPARTUM DEPRESSION AMONGST WOMEN ADMITTED TO A KANGAROO MOTHER CARE WARD. Elzet Venter
27RISK OF NEONATAL MORTALITY ASSOCIATED WITH FIRST ADMISSION TEMPERATURE AT A SEMI-RURAL HOSPITAL. (LURWMH). N Kapongo
32
INFANTS OF DIABETIC MOTHERS: MATERNAL AND INFANT CHARACTERISTICS AND INCIDENCE OF HYPOGLYCEMIA. Yoliswa Magadla
39
AN ASSESSMENT OF INTENDED INFANT FEEDING PRACTICES OF WOMEN WHO DELIVER AT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL. YP Kennedy
43
INCREASED EXCLUSIVE BREASTFEEDING IN SOUTH AFRICA FROM 2010 TO 2013: IMPACT OF NATIONAL POLICY CHANGE? Debra Jackson
51
CLINICAL FEATURES, LABORATORY FINDINGS AND OUTCOMES OF INFANTS WITH HYPERBILIRUBINAEMIA REQUIRING EXCHANGE BLOOD TRANSFUSION AT CHRIS HANI BARAGWANATH HOSPITAL. Karabo Seake
57
EFFICACY AND SAFETY OF ANTEPARTUM ANTIRETROVIRAL STRATEGIES TO PREVENT PERINATAL HIV TRANSMISSION – THE IMPAACT PROMISE TRIAL (1077). GB Theron 61
i
STUDY TITLE: ‘SELF-INDUCED LATE ABORTION AS A CONTRIBUTOR TO PRETERM BIRTH AND PERINATAL MORBIDITY AND MORTALITY. Dr SD Mandondo
64
OUTCOMES OF BIRTH ASPHYXIA REDUCTION AT PHOLOSONG REGIONAL HOSPITAL.R Magagane 73
THE INCIDENCE, MATERNAL, AND PERINATAL OUTCOMES OF ABRUPTIO PLACENTAE AT NELSON MANDELA ACADEMIC HOSPITAL, MTHATHA. CN Gubu-Ntaba 77
ENDING PREVENTABLE STILLBIRTHS: GLOBAL SITUATION & SOUTH AFRICA’S CONTRIBUTION. Mary Kinney 82
AUDITING STILLBIRTHS AT LOWER UMFOLOZI REGIONAL HOSPITAL: A 12 MONTH REVIEW. Indira Govender 90
RISK FACTORS, REPAIR TECHNIQUES AND SHORT TERM SUBJECTIVE OUTCOME OF OBSTETRICS ANAL SPHINCTER INJURIES AT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL. SM Tshabalala
96
USING FAST AS MONITORING TOOL FOR NEWBORN CARE: EXPERIENCES IN LIMPOPO PROVINCE. PL Mashao
102
KWAZULU-NATAL INITIATIVE FOR NEWBORN CARE (KINC): A MIDPOINT EVALUATION OF A PROGRAM TO IMPROVE NEWBORN CARE IN DISTRICT HOSPITALS IN KWAZULU NATAL (ABSTRACT). SA Phakathi
109
INSIGHTS INTO HEALTH CARE WORKER PERCEPTIONS AND ATTITUDES OF WORKING IN NEONATAL HIGH CARE UNITS. Aurene Wilford
110
USING DISTRICT STRUCTURES FOR STRENGTHENING KANGAROO MOTHER CARE SERVICES: A CASE STUDY FROM TSHWANE DISTRICT. Elise van Rooyen, Anne-Marie Bergh
115
NON-INVASIVE OVERNIGHT MONITORING OF FETAL AND MATERNAL SLEEP PATTERNS (ABSTRACT). Fifer, WP
119
THE WESTERN CAPE PROVINCIAL 1st 1000 DAYS INITIATIVE: A PERINATAL CARE PRIORITY. Malek E
121
INACTIVE CLINICAL GOVERNANCE: IS IT THE PRIMARY CAUSE WHY LIMPOPO IS STILL STRUGGLING TO END PREVENTABLE MATERNAL DEATH? (ABSTRACT). Shisana Baloyi 126
ii
PROVISION, UTILISATION AND FUNCTIONALITY OF MIDWIFE OBSTETRIC UNITS IN FIVE DISTRICTS IN KWAZULU-NATAL (ABSTRACT). AS Voce
128
BARRIERS TO OBSTETRIC CARE AMONGST MATERNAL NEAR MISSES (ABSTRACT). P Soma-Pillay
130
ASSESSMENT OF THE EFFECTIVENESS OF A ONE DAY TRAINING PROGRAMME TO IMPROVE KNOWLEDGE OF OBSTETRIC EMERGENCIES IN EMS PERSONNEL. D Barnard 131
ESMOE-EOST SCALE-UP PROJECT: PRELIMINARY DATA ON IMPACT OF SCALE-UP.RC Pattinson
134
COMMUNITY ENGAGEMENT: A KEY STRATEGY INTERVENTION IN REDUCING OBSTETRIC MORBIDITY AND MORTALITY. Klaas Mongalo
138
TRAINING COURSES AVAILABLE IN THE ESMOE-EOST PROGRAMME (ABSTRACT).CM Bezuidenhout
148
EVERY BABY COUNTS: THE FORTHCOMING WHO PERINATAL MORTALITY AUDIT GUIDE. Kate Kerber
149
THIRTEEN YEARS OF REGIONAL PPIP: TRYING TO HOLD ONTO THE GAINS. Charl Oettle
154
EVALUATION OF THE PERINATAL PROBLEM IDENTIFICATION PROGRAM ACROSS HEALTH FACILITIES IN LIMPOPO PROVINCE, SOUTH AFRICA (2006-2015). Unarine Makungo 159
PERINATAL AND NEONATAL MORTALITY RATES IN BISHOP LAVIS OVER 7 YEARS (ABSTRACT). HJ ODENDAAL
164
ACCREDITATION OF NEONATAL CARE SERVICES IN KWAZULU-NATAL. D. NYASULU 166
ESTABLISHING COMMUNITY BASED MATERNAL DEATH REVIEWS AND THE ASSOCIATED SOCIAL DETERMINANTS IN LIMPOPO: VHEMBE PILOT SITE. Shisana Baloyi 170
AN AUDIT OF CAESAREAN SECTIONS AT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL. YASMIN ADAM
187
iii
ACCEPTABILITY OF MIDWIFE OBSTETRIC UNITS IN FIVE DISTRICTS IN KWAZULU-NATAL (ABSTRACT). AS Voce
192
AUDIT OF MATERNAL NEAR MISS IN THE METRO WEST MATERNITY SERVICES, CAPE TOWN. Ibe Iwuh
194
iv
DETECTING FOETUSES AT RISK OF STILLBIRTH: PILOT STUDY RESULTS
Spencer Nkosi, Bob PattinsonSA MRC Maternal and infant Health Care Strategies Unit
IntroductionStillbirths still remain high, worldwide it is estimated that 2,6 million babies die annually in the third trimester. The ninth report of saving babies in South Africa concluded that between the period of January 2011 up until December 2012, there were 32 6552 stillborn babies in our data.The largest category of Perinatal Deaths (PND) in South Africa is the unexplained stillbirth group. Up to a third in this group are babies with intrauterine growth restriction. If we look at international data, although they have substantially lower perinatal mortality rate than developing countries, their unexplained stillbirth group contains up to 50% of babies clinically growth restricted (Gardosi and Froen).In all these cases, approximately 80% of these mothers during the investigations were regarded as clinically normal. In various meta-analysis and studies published, the use of Doppler in high risk groups has been found to reduce the odds of perinatal death by 38%. The secondary benefits it reduces perinatal admissions, induction of labour and caesarean sections for foetal distress.The use of Doppler in low risk (normal) population was found to be of no value in a meta-analysis done by Alfirevic et al.However, all studies used in the review were performed in developed countries, in the early 90’s and their stillbirth numbers were quite low.Umbiflow is a mobile-connected Doppler device that utilizes a continuous waveform to detect blood within the umbiflow cord.It consists of a hand-held proprietary Doppler probe (transducer) with USB cable that connects to any windows-based notebook on which necessary software is installed. It measures the resistance index (RI) in the umbilical cord and plots it against the gestational age.
1) Umbiflow can accurately measure the RI of the umbilical blood flow as effective as commercial ultrasound machines “gold standard”.
1
2) It was also demonstrated that the technology can be adopted and operated by nurses and midwives at the primary health care centres (PHC) levels.
3) Use of umbiflow for umbilical artery Doppler in patients suspected with reduced symphysis fundal (height) growth in Western Cape lead to a 48% reduction for patients requiring referral to a more specialised level care.
4) Up to 9% of late bookers in a small study in Western Cape had abnormal Doppler and smaller babies which would not have been detected by SF only.
The aim of the study is to ascertain if continuous wave Doppler ultrasound (umbiflow) used to screen an unselected pregnant population in a low/middle income setting and identify foetuses at risk of stillbirth.
Primary outcomes: To compare stillbirth rate in Doppler group versus the no Doppler group.
Secondary outcomes: Caesarean section rate, Small for gestation detection rate, maternal and neonatal morbidity and cost effectiveness.
Methods and materials:Study design The study design chosen was step wedge instead of randomised control trial and the following are the reasons:
1) It would be unethical to withhold an abnormal Doppler result from clinicians managing the pregnant woman as foetuses with abnormal Doppler are at risk of death.
2) Allows introduction of the umbiflow in sites in controlled fashion with adequate training and quality control.
3) Cost effective: - Doesn’t flood system (Human and infrastructure resource). If results on one site show no benefit it is easy to stop on one site than multiple site.
2
3
Location The study is being conducted in Mamelodi, East of Pretoria, part of Tshwane metropolitan. Mamelodi Regional Hospital is situated in the serving 23 antenatal clinics with 3 midwife obstetrics units running 24-hours services. Stanza Bopape was chosen as the first pilot site (MOU). All patients between the gestation of 28 to 32 weeks or SF of 26 to 30cm who agree to participate in the trial were recruited. A consent form is signed. After gestational age was ascertained an umbiflow was done, if it was normal (or low risk) they continued at the clinic and delivered there unless needed upward referral based on criteria. If the umbiflow was intermediate risk/ high risk patients were referred to Mamelodi Hospital to a clinic where the principal investigator performs other investigations namely: Biometric measurements, amniotic fluid index, placenta grading, RI, fetal movements and breathing movements.All the pregnancies were singleton and meeting the criteria for recruitment. Follow ups were done weekly and patients delivered according to set protocol. We delivered patients at more than 38 weeks of gestation or if there was no growth in two successive visits or any obstetrics emergencies.
ResultsThe trial began in July and the results stated below are for six months;763 women recruited by the end of December 2015496 women should have delivered by thenOutcome discussed is of 352 (29% missing)Patients with umbiflow-352 Patients without umbiflow- 34764 stillbirths 66 stillbirths3 MSB 48MSB1FSB 18FSBPNMR: 11.4/1000 PNMR: 19.0/1000
Results of 352 delivered womenHigh risk Medium risk Normal flow Prevalence
Number 19 22 311 5%, 11.6%Stillbirth 1(5.2%) 1(4.5%) 2(0.64%)SGA 5(26.3%) 5(22.7%) 27(8.7%)
4
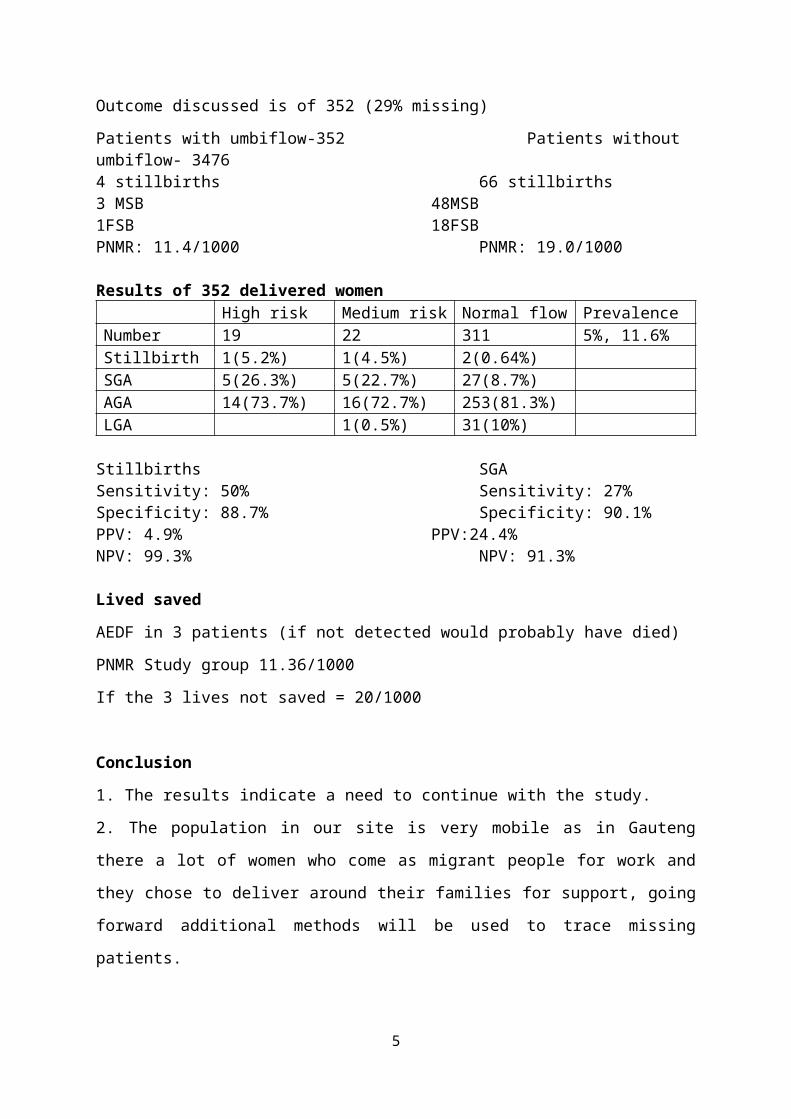
AGA 14(73.7%) 16(72.7%) 253(81.3%)LGA 1(0.5%) 31(10%)
Stillbirths SGASensitivity: 50% Sensitivity: 27%Specificity: 88.7% Specificity: 90.1%PPV: 4.9% PPV:24.4%NPV: 99.3% NPV: 91.3%
Lived savedAEDF in 3 patients (if not detected would probably have died)PNMR Study group 11.36/1000If the 3 lives not saved = 20/1000
Conclusion1. The results indicate a need to continue with the study.2. The population in our site is very mobile as in Gauteng there a lot of women who come as migrant people for work and they chose to deliver around their families for support, going forward additional methods will be used to trace missing patients.
5

THE ROLE OF PLACENTAL HISTOLOGY IN ADVERSE PREGNANCY OUTCOMES AT A REFERRAL HOSPITAL IN THE EASTERN CAPE
Dr MS Mabenge: Head of Department Obstetrics and Gynaecology, Dora Nginza Hospital, Eastern Cape and Walter Sisulu UniversityProf C Wright: Anatomical Pathology, NHLS, Ibhayi, Stellenbosch University and Walter Sisulu University.
IntroductionAdverse pregnancy outcomes continue to pose a challenge and contributes significantly towards litigation in obstetrics globally, but the Eastern Cape Province of South Africa where poverty is rife is noted internationally for its perinatal mortality rate. Dora Nginza Hospital, the only high risk Obstetric referral unit in Port Elizabeth, Eastern Cape serves the western half of the Eastern Cape region. This hospital has a perinatal mortality rate of 60/1000 and a C/S rate of 56%.In order to try to determine the underlying factors leading to these figures, the Obstetrics Department in Dora Nginza Hospital have been submitting placentae for histopathology in cases of unexpected poor birth outcomes (i.e. 5 minute Apgar of below 7 (fresh still birth) since March 2012
MethodPlacentae from mothers whose babies with unexpected poor outcome (5 minute Apgar of below 7, fresh still birth) from March 2012 to 2015
ResultsThe following table illustrate the total number of deliveries in the unit for the past 3 years, the mode of delivery and the HIV status of patients delivered in the unitYear Total deliveries Caesarean section Normal vertex deliveries
HIV Positive2013 6314 3679 2649
1639(26%)2014 6647 3796 2472
1607(24%)2015 6916 3707 2806
1788(26%)Total 19877 11182 7927 5034
1359 placentae of mothers who had adverse pregnancy outcome (as defined above) were received by the pathologist for analysis from March 2012 to July 2013.212 patients (15%) had a diagnosis of intrauterine demise before delivery and 101 patients had fresh still births.242 patients had a c/s delivery of which 115 patients (47%) were sent to theatre for a diagnosis of fetal compromiseA pathological diagnosis of maternal vascular under perfusion was made in 194 placentae while 112 placentae showed fetal thrombotic vasculopathy. Chorioamnionitis with vasculitis indicating fetal response to infection was present in 117 placentae.
Conclusion Adverse pregnancy outcomes often attributed to acts of omission by the physician attending to the pregnant patient during delivery. Placental histology
6
was able to show in a significant number of our patients with adverse outcome primary or contributory factors that would otherwise be difficult to make resulting in unnecessary litigations and costs to the department of health.
7
THE HIDDEN DANGER OF INTRA-UTERINE GROWTH RESTRICTION
RC Pattinson, M MullerSA MRC Maternal and Infant Health Care Strategies Unit, Department of Obstetrics and Gynaecology, University of Pretoria
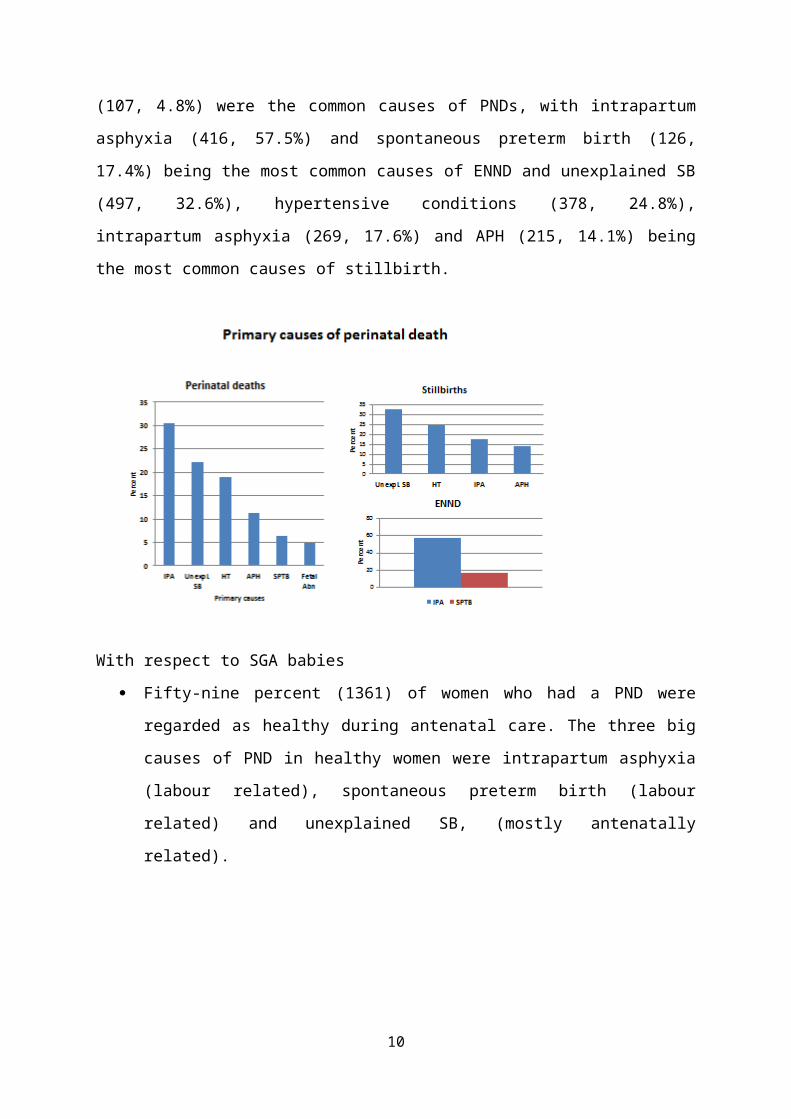
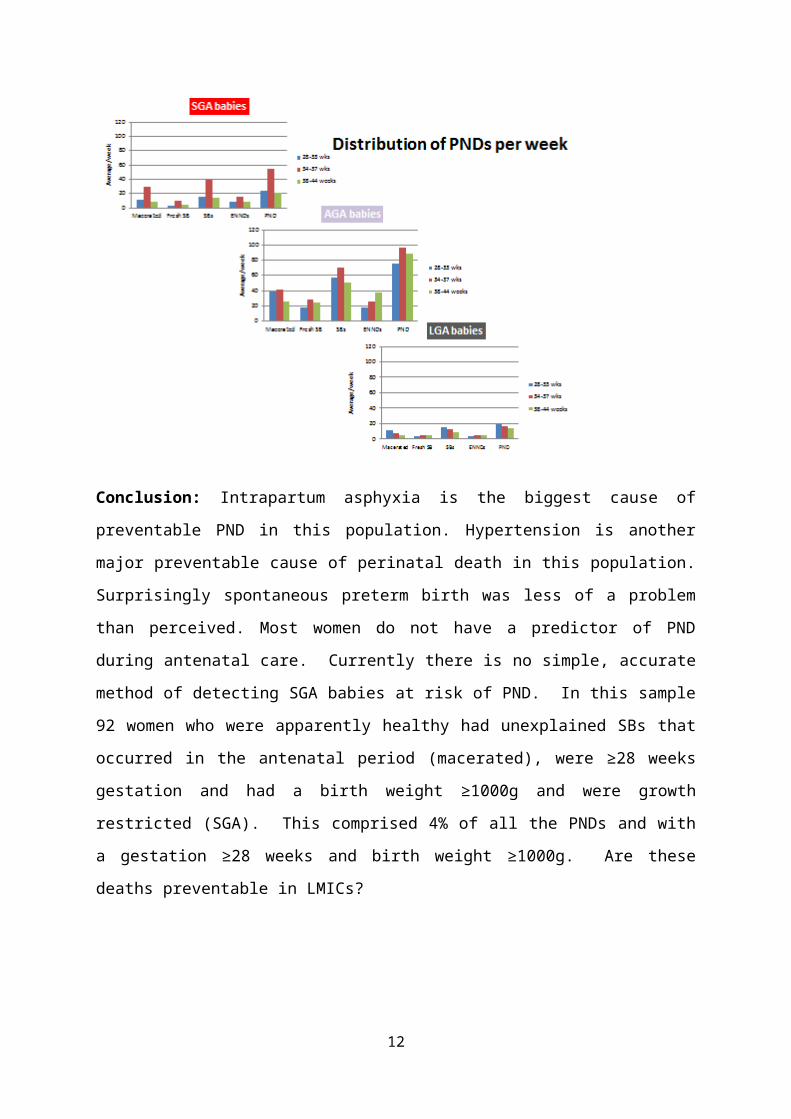
Aim: To uncover the impact of growth restriction on perinatal deathsSetting: Population based data from a mostly rural population in South Africa.Method: An analysis using the Perinatal Problem Identification Programme V3 was performed on a population with respect to gestational age, growth, cause of perinatal death and maternal condition at birth from September 1st 2013 to August 31st 2015. Growth curves of Theron et al. were used to assess fetal weight against gestational age.Results: A total of 150,722 babies were recorded for the two years. A total of 149,308 births 1000g or more were delivered with 3893 perinatal deaths giving a perinatal mortality rate of 24.8/1000 births, a stillbirth rate of 17.0/1000 births and early neonatal death rate of 8.0/1000 live births; of these 2453 (63%) deaths were regarded by the clinicians entering the data as having accurate gestational age by ultrasound and/or dates and/or SF measurement; and 2248 (91.6%) had a gestational age of 28 weeks or more. This population of perinatal deaths forms the core of this analysis. Overall, intrapartum asphyxia (685, 30.5%), unexplained SB (497, 22.1%), hypertensive conditions (426, 19.0%), APH (225, 11.3%) and spontaneous preterm birth (143, 6.4%), fetal abnormality (107, 4.8%) were the common causes of PNDs, with intrapartum asphyxia (416, 57.5%) and spontaneous preterm birth (126, 17.4%) being the most common causes of ENND and unexplained SB (497, 32.6%), hypertensive conditions (378, 24.8%), intrapartum asphyxia (269, 17.6%) and APH (215, 14.1%) being the most common causes of stillbirth.
8
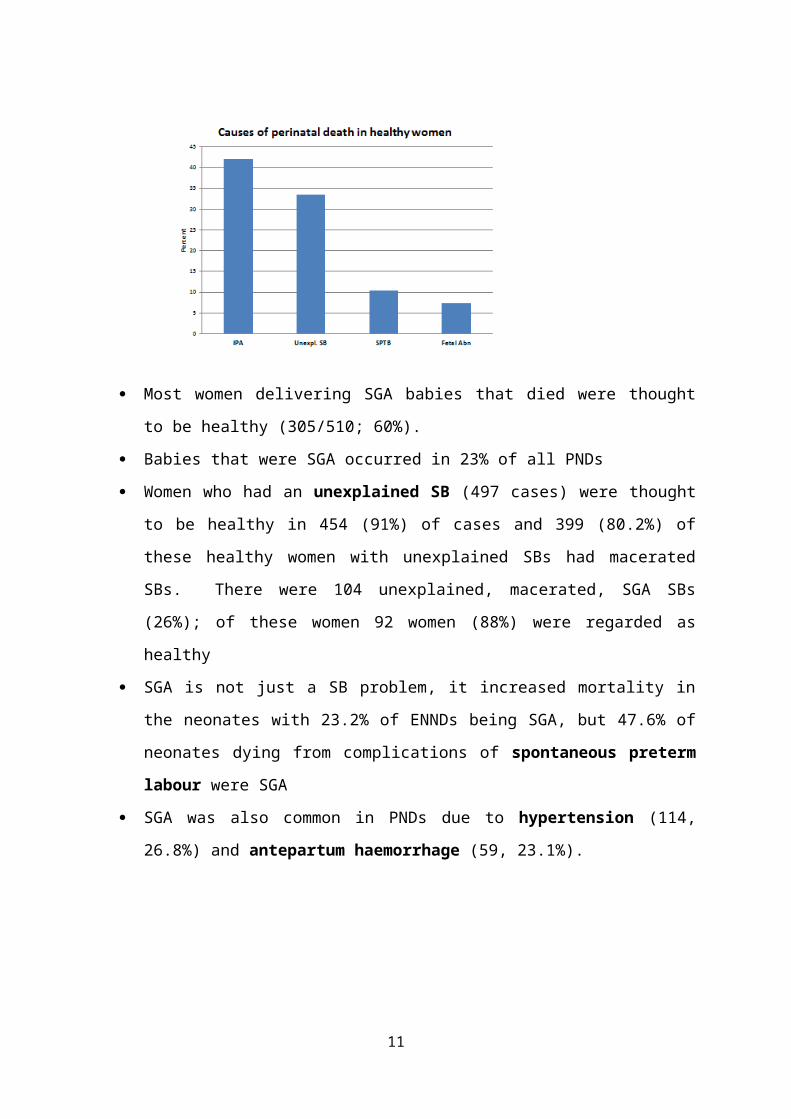
With respect to SGA babies Fifty-nine percent (1361) of women who had a PND were regarded
as healthy during antenatal care. The three big causes of PND in healthy women were intrapartum asphyxia (labour related), spontaneous preterm birth (labour related) and unexplained SB, (mostly antenatally related).
Most women delivering SGA babies that died were thought to be healthy (305/510; 60%).
Babies that were SGA occurred in 23% of all PNDs
9
Women who had an unexplained SB (497 cases) were thought to be healthy in 454 (91%) of cases and 399 (80.2%) of these healthy women with unexplained SBs had macerated SBs. There were 104 unexplained, macerated, SGA SBs (26%); of these women 92 women (88%) were regarded as healthy
SGA is not just a SB problem, it increased mortality in the neonates with 23.2% of ENNDs being SGA, but 47.6% of neonates dying from complications of spontaneous preterm labour were SGA
SGA was also common in PNDs due to hypertension (114, 26.8%) and antepartum haemorrhage (59, 23.1%).
Conclusion: Intrapartum asphyxia is the biggest cause of preventable PND in this population. Hypertension is another major preventable cause of perinatal death in this population. Surprisingly spontaneous preterm birth was less of a problem than perceived. Most women do not have a predictor of PND during antenatal care. Currently there is no simple, accurate method of detecting SGA babies at risk of PND. In this sample 92 women who were apparently healthy had unexplained SBs that occurred in the antenatal period (macerated), were ≥28 weeks gestation and had a birth weight ≥1000g and were growth restricted (SGA). This
10
comprised 4% of all the PNDs and with a gestation ≥28 weeks and birth weight ≥1000g. Are these deaths preventable in LMICs?
11
ANTENATAL COMMON MENTAL DISORDERS, SUICIDALITY AND ASSOCIATED RISK FACTORS: A CROSS-SECTIONAL SURVEY FROM A SOCIALLY ADVERSE SETTING, CAPE TOWN
Simone Honikman 1 , Michael Onah1, Thandi van Heyningen1, Sally Field1, Sue Fawcus2 1 Perinatal Mental Health Project, Alan J. Flisher Centre for Public Mental Health, Department of Psychiatry and Mental Health, University of Cape Town, South Africa.Corresponding email: [email protected] 2Department of Obstetrics and Gynaecology, Faculty of Health Sciences, University of Cape Town, South Africa.
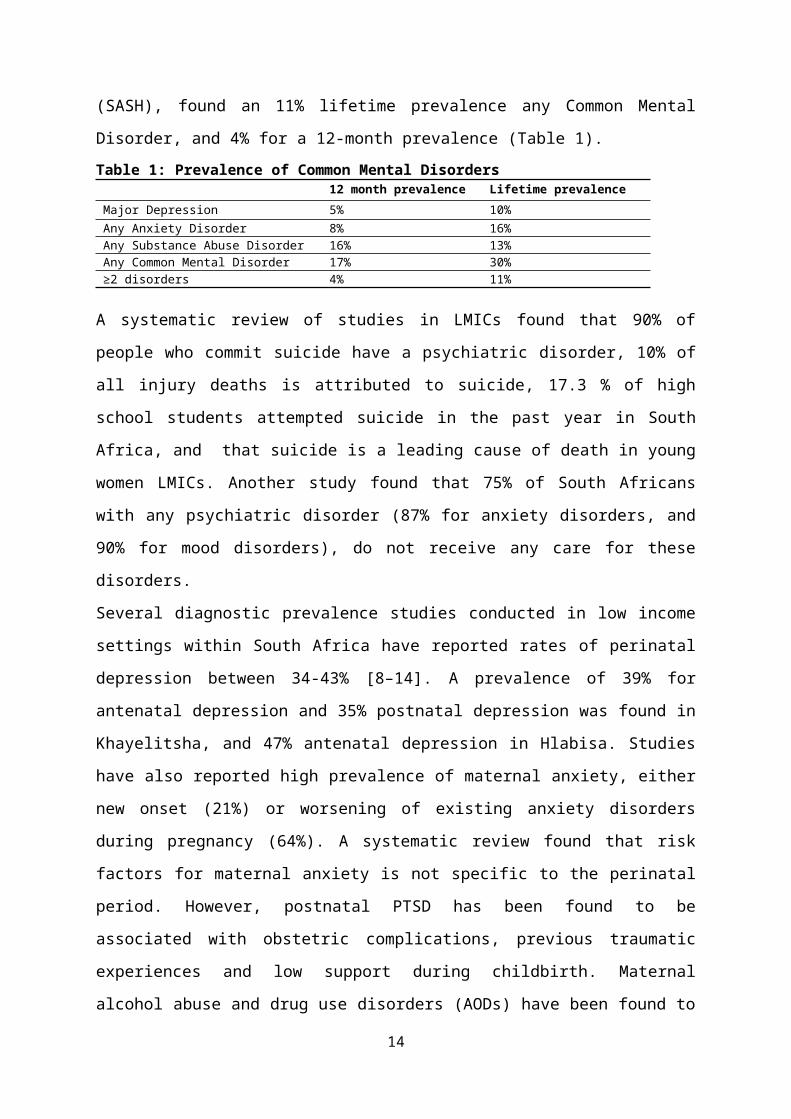
BackgroundThe 2010 Global Burden of Diseases, Injuries, and Risk Factors Study found that mental health disorders accounted for 13% of the global burden of disease, and along with substance use disorders, were the leading cause of disability worldwide. Mental and substance use disorders accounted for 183·9 million (7.4%) disability-adjusted life years (DALYs), 0.5% of all years of life lost to premature mortality (YLLs), and 22.9% of all years lived with disability (YLDs). It is predicted that by 2030, unipolar depression will be the leading contributor to the global burden of disease surpassing cardiovascular disease, road traffic accidents and cancer. Seventy-five percent of people living with mental health conditions are in Low and Medium Income Countries (LMICs). Depression is the 10th highest contributor to burden of disease in South Africa (greater than ischaemic heart disease, protein-energy malnutrition, birth asphyxia and trauma and diabetes mellitus). The South African Stress and Health Study (SASH), found an 11% lifetime prevalence any Common Mental Disorder, and 4% for a 12-month prevalence (Table 1). Table 1: Prevalence of Common Mental Disorders
12 month prevalence Lifetime prevalenceMajor Depression 5% 10%Any Anxiety Disorder 8% 16%Any Substance Abuse Disorder 16% 13%Any Common Mental Disorder 17% 30%≥2 disorders 4% 11%
A systematic review of studies in LMICs found that 90% of people who commit suicide have a psychiatric disorder, 10% of all injury deaths is
12
attributed to suicide, 17.3 % of high school students attempted suicide in the past year in South Africa, and that suicide is a leading cause of death in young women LMICs. Another study found that 75% of South Africans with any psychiatric disorder (87% for anxiety disorders, and 90% for mood disorders), do not receive any care for these disorders.Several diagnostic prevalence studies conducted in low income settings within South Africa have reported rates of perinatal depression between 34-43% [8–14]. A prevalence of 39% for antenatal depression and 35% postnatal depression was found in Khayelitsha, and 47% antenatal depression in Hlabisa. Studies have also reported high prevalence of maternal anxiety, either new onset (21%) or worsening of existing anxiety disorders during pregnancy (64%). A systematic review found that risk factors for maternal anxiety is not specific to the perinatal period. However, postnatal PTSD has been found to be associated with obstetric complications, previous traumatic experiences and low support during childbirth. Maternal alcohol abuse and drug use disorders (AODs) have been found to act as a mechanism for ‘coping with everyday life’ for pregnant women in adverse environments. AODs among pregnant women are also associated with younger age, poverty, unemployment, interpersonal conflict, multiple depressive episodes, anxiety, and suicidality. Low income pregnant women have higher vulnerability to AODs use in both developed and developing country settings. There is also a growing concern about the increase in suicide and suicidal ideation among pregnant women globally. Furthermore, perinatal mental health disorders place women at a much higher risk of maternal mortality due to natural and non-natural causes. However, in many settings, neither maternal mental disorders nor suicidal ideation are screened for and completed suicides are inaccurately audited nor appropriately included in maternal mortality data. Suicide is a leading cause of maternal death in UK (where it has been found to be mostly avoidable) and contributes to 1.7% of pregnancy-related deaths in LMICs. Depression and anxiety are the strongest risk factors for suicide and suicidal ideation among the general population, pregnant women and in the postpartum period. In
13
South Africa, studies found a 27.5% prevalence of any suicidal ideation among pregnant rural women in KZN, and a 7.6% prevalence (2.8% high risk) postnatal women in Khayelitsha. Risk factors identified in these studies included; younger age, lack of employment, being unmarried, being HIV positive, food insecurity, depression and hazardous drinking.
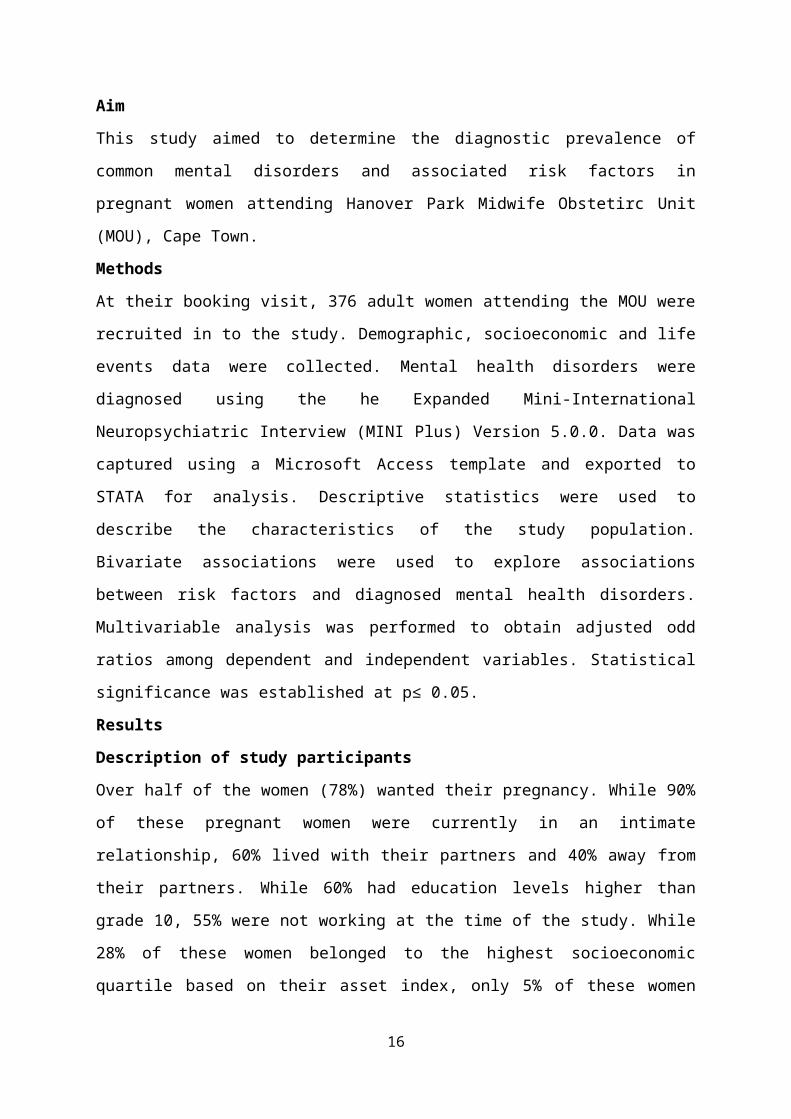
Aim This study aimed to determine the diagnostic prevalence of common mental disorders and associated risk factors in pregnant women attending Hanover Park Midwife Obstetirc Unit (MOU), Cape Town.MethodsAt their booking visit, 376 adult women attending the MOU were recruited in to the study. Demographic, socioeconomic and life events data were collected. Mental health disorders were diagnosed using the he Expanded Mini-International Neuropsychiatric Interview (MINI Plus) Version 5.0.0. Data was captured using a Microsoft Access template and exported to STATA for analysis. Descriptive statistics were used to describe the characteristics of the study population. Bivariate associations were used to explore associations between risk factors and diagnosed mental health disorders. Multivariable analysis was performed to obtain adjusted odd ratios among dependent and independent variables. Statistical significance was established at p≤ 0.05. ResultsDescription of study participantsOver half of the women (78%) wanted their pregnancy. While 90% of these pregnant women were currently in an intimate relationship, 60% lived with their partners and 40% away from their partners. While 60% had education levels higher than grade 10, 55% were not working at the time of the study. While 28% of these women belonged to the highest socioeconomic quartile based on their asset index, only 5% of these women earned a monthly salary above 500 USD. Forty-two percent of the entire sample were food insecure, while 13% indicated food insufficiency. Table 2 provides the descriptive details of the sample.
14
Table 2: Sample descriptive
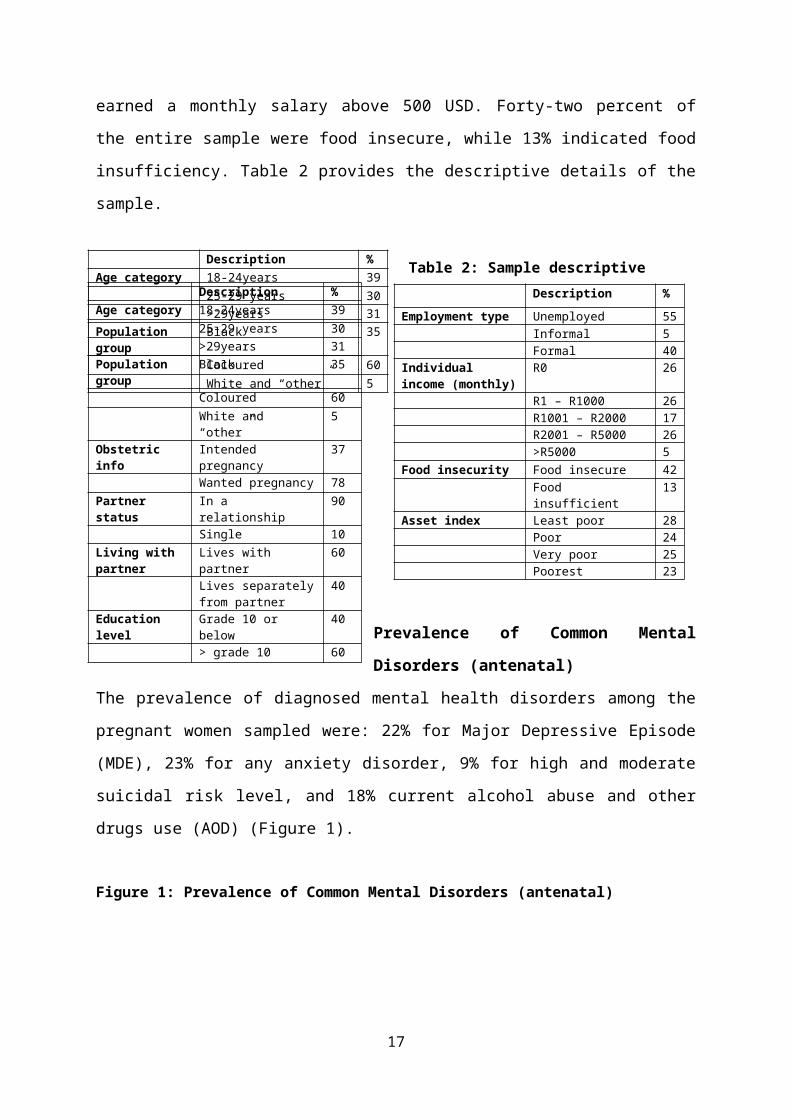
Prevalence of Common Mental Disorders (antenatal)The prevalence of diagnosed mental health disorders among the pregnant women sampled were: 22% for Major Depressive Episode (MDE), 23% for any anxiety disorder, 9% for high and moderate suicidal risk level, and 18% current alcohol abuse and other drugs use (AOD) (Figure 1).
Figure 1: Prevalence of Common Mental Disorders (antenatal)
CMD MDE Any anxiety disorder AOD 0%
10%
20%
30%
40%
50%
60%
70%
23% 22% 23%17%
0.22
0.17
15
Description %Age category 18-24years 3
9 25-29 years 3
0 >29years 3
1Population group
Black 35
Coloured 60
White and “other” 5
Description %Age category
18-24years 39
25-29 years 30 >29years 31Population group
Black 35
Coloured 60 White and “other” 5Obstetric info
Intended pregnancy
37
Wanted pregnancy 78Partner status
In a relationship 90
Single 10Living with partner
Lives with partner 60
Lives separately from partner
40
Education level
Grade 10 or below 40
> grade 10 60
Description %Employment type
Unemployed 55
Informal 5 Formal 4
0Individual income (monthly)
R0 26
R1 – R1000 26
R1001 – R2000 17
R2001 – R5000 26
>R5000 5Food insecurity Food insecure 4
2 Food insufficient 1
3Asset index Least poor 2
8 Poor 2
4 Very poor 2
5 Poorest 2
3
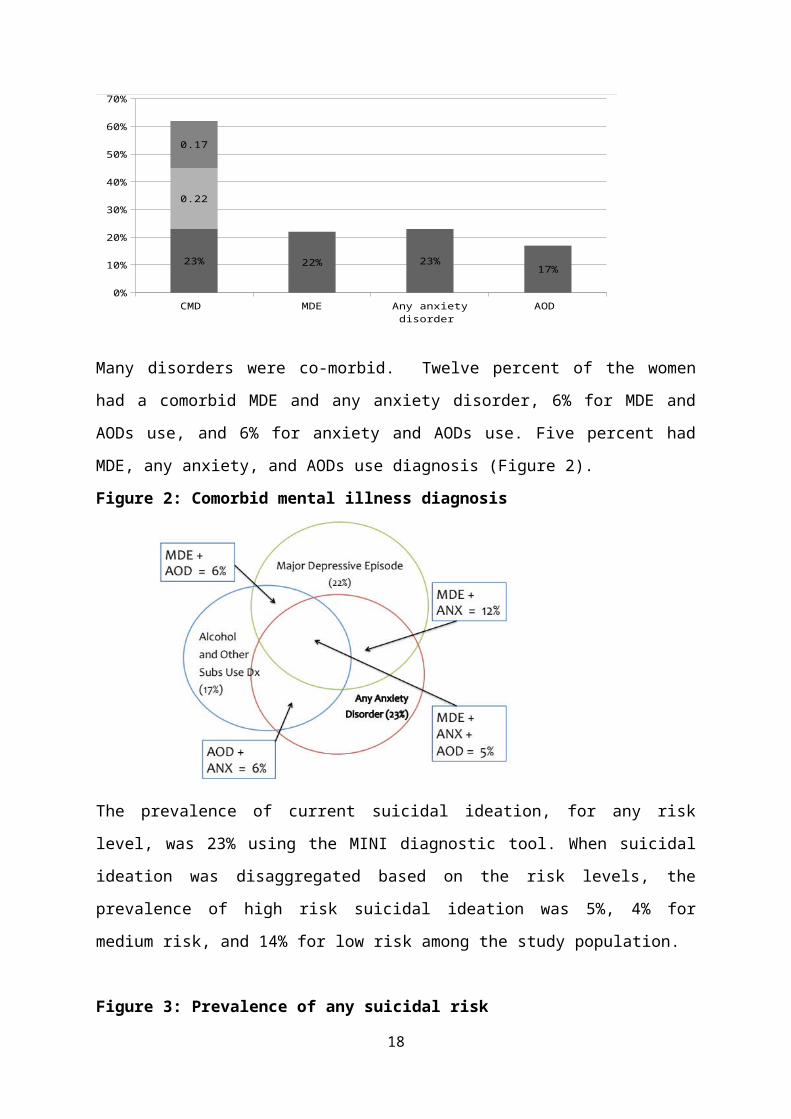
Many disorders were co-morbid. Twelve percent of the women had a comorbid MDE and any anxiety disorder, 6% for MDE and AODs use, and 6% for anxiety and AODs use. Five percent had MDE, any anxiety, and AODs use diagnosis (Figure 2). Figure 2: Comorbid mental illness diagnosis
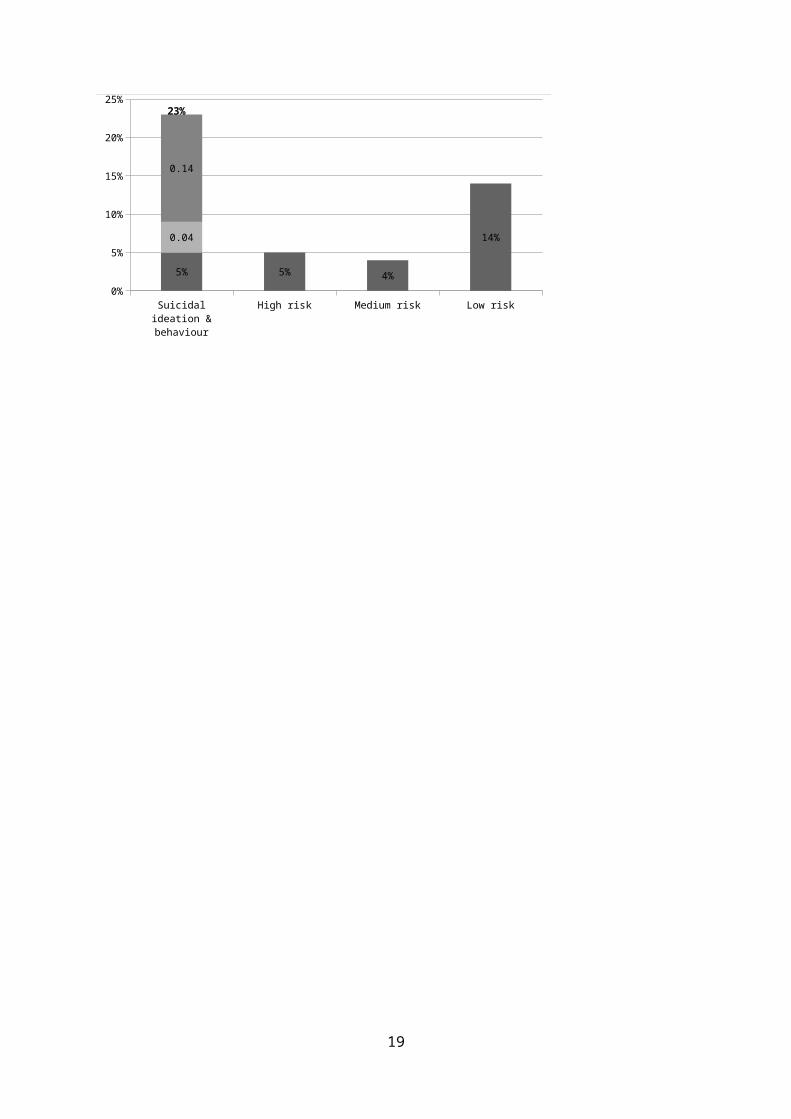
The prevalence of current suicidal ideation, for any risk level, was 23% using the MINI diagnostic tool. When suicidal ideation was disaggregated based on the risk levels, the prevalence of high risk suicidal ideation was 5%, 4% for medium risk, and 14% for low risk among the study population.
Figure 3: Prevalence of any suicidal risk
Suicidal ideation & behaviour
High risk Medium risk Low risk0%
5%
10%
15%
20%
25%
5% 5% 4%
14%0.04
0.14
23%
16
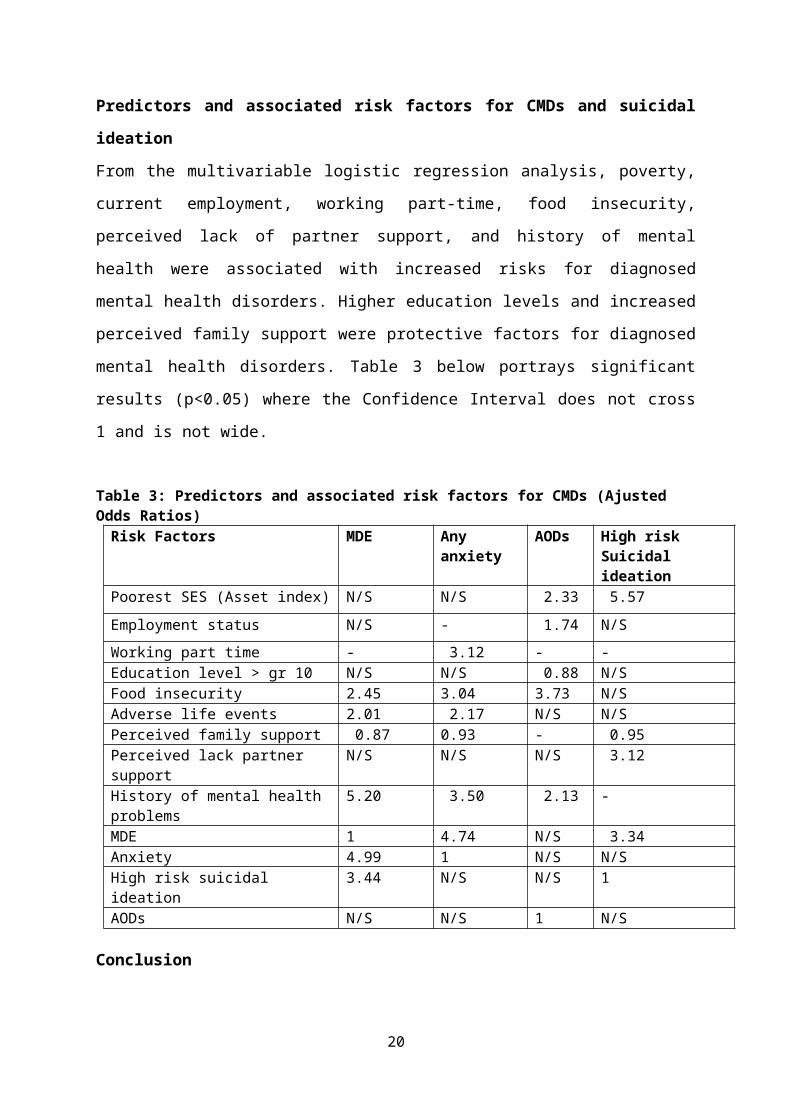
Predictors and associated risk factors for CMDs and suicidal ideationFrom the multivariable logistic regression analysis, poverty, current employment, working part-time, food insecurity, perceived lack of partner support, and history of mental health were associated with increased risks for diagnosed mental health disorders. Higher education levels and increased perceived family support were protective factors for diagnosed mental health disorders. Table 3 below portrays significant results (p<0.05) where the Confidence Interval does not cross 1 and is not wide.
Table 3: Predictors and associated risk factors for CMDs (Ajusted Odds Ratios)
Risk Factors MDE Any anxiety
AODs High risk Suicidal ideation
Poorest SES (Asset index) N/S N/S 2.33 5.57Employment status N/S - 1.74 N/SWorking part time - 3.12 - -Education level > gr 10 N/S N/S 0.88 N/SFood insecurity 2.45 3.04 3.73 N/SAdverse life events 2.01 2.17 N/S N/SPerceived family support 0.87 0.93 - 0.95 Perceived lack partner support
N/S N/S N/S 3.12
History of mental health problems
5.20 3.50 2.13 -
MDE 1 4.74 N/S 3.34 Anxiety 4.99 1 N/S N/SHigh risk suicidal ideation 3.44 N/S N/S 1AODs N/S N/S 1 N/S
ConclusionThere is a high prevalence of common mental health disorders among pregnant women in Hanover Park, many of them co-morbid. These disorders are associated with multiple risk factors. We would advocate that maternal mental health services be integrated into obstetric care to screen and treat this vulnerable group considering that these disorders impact on physical health outcomes, nutrition, foetal development, and obstetric outcomes.
17
INTEGRATING MENTAL HEALTH IN TO MATERNAL HEALTH CARE: PROMISING RESULTS TOWARDS CLOSING THE TREATMENT GAP
Simone Honikman 1 , Michael Onah1, Sally Field11 Perinatal Mental Health Project, Alan J. Flisher Centre for Public Mental Health, Department of Psychiatry and Mental Health, University of Cape Town, South Africa.Corresponding email: [email protected]
BackgroundIn low- and middle-income countries, competing health priorities, and a lack of political will mean that expenditure on mental health is a fraction of that needed to meet the mental health care needs of the population. This treatment gap is most notable for mothers in regions where the maternal health agenda focuses predominantly on reducing maternal mortality. Untreated common perinatal mental disorders (depression and anxiety) can have significant impact on the well-being of mothers. The consequences include increased use of alcohol and substances, suicide, increased risk of experiencing intimate partner violence and loss of economic potential. For the offspring of these mothers, there are increased associated peripartum outcomes related to IUGR, pre-eclampsia and pre-term birth [8] as well as other adverse infant, child and adolescent cognitive, behavioural mental health, physical health and social outcomes. Antenatal and postnatal maternal mental illness have been noted to be associates with separate child outcomes. Furthermore, anxiety disorders and depression are each associated with separate child outcomes. These trans-generational effects have been well established, and are felt particularly in societies facing adversity.
The Perinatal Mental Health Project (PMHP), Alan J Flisher Centre for Public Mental Health, UCTThe vision of the PMHP is for all mothers to have access to mental health support to promote their well-being, and that of their children and communities. To achieve this, the PMHP works towards development and advocacy for accessible maternal mental health care that can be delivered effectively at scale in low resource settings. The PMHP’s
18
demonstration service sites are located at three primary obstetric facilities (Midwife Obstetric Units: MOUs) in low-income settings in Cape Town. As an integrated part of the obstetric care, pregnant women are screened for symptoms of depression and for social risk factors associated with common mental disorders. Scores on these screens determine referral to an onsite mental health counsellor.
The PMHP’s service development components and principlesi. Prepare the service environment: relationship-building with
stakeholders on site; mental health training using self-reflective and participatory style with stakeholders
ii. Support the providers: establish integrated self-care strategies for health workers and counsellors involved in the service
iii. Mental health services should be on site, routine and seamlessly integrated in to maternity care processes
iv. Early detection (through screening)1 of common mental disorders (usually at the booking visit) and on-site referral to counselling.
v. Counselling to draw on evidence-based psychological therapies shown to be effective when delivered by non-mental health professionals, over a restricted number of sessions. Counselling to be adapted to clients’ needs and draw on social support mechanisms and other available services, as required. Tracking and postnatal follow-up is required.
vi. Monitor and evaluate (M&E) service regularly – communicating results with all stakeholders
The PMHP service model M&E methodology Routine monthly monitoring data is captured to assess screening coverage, service uptake, and the number of sessions of counselling provided. All women who have received counselling are followed up six to
1 The PMHP screens with the 10-item, Edinburgh Postnatal Depression Scale (EPDS) [22] as well as an 11-item Risk Factor Assessment (RFA) tool [23] at two of its sites. At the third site, screening is conducted using the 3-item, Whooley questionnaire as advocated by the UK’s NICE Guidelines [24].
19
ten weeks postnatally. They complete a structured assessment and report on their mood symptoms, functioning and on the degree of resolution of the problems that they presented during counselling. Data is collated in an Excel database and mean scores reported.
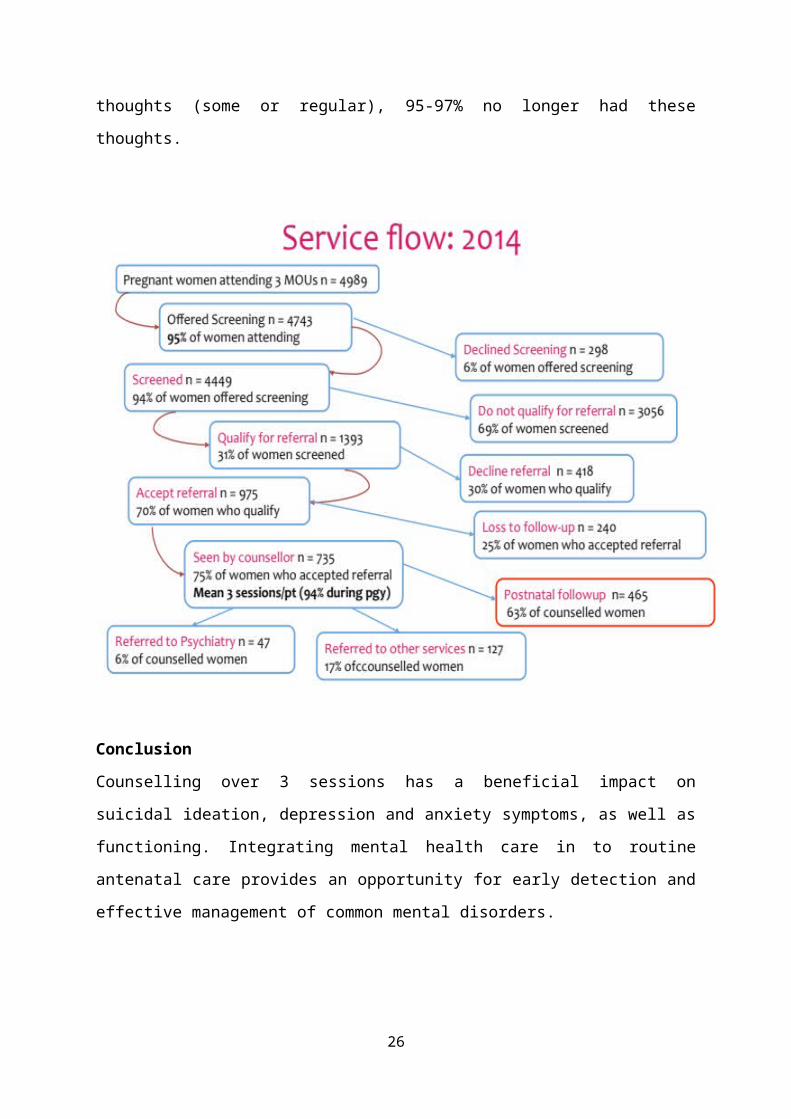
Results for 2014 calendar year (all three service sites)A total of 4 989 women booked for antenatal care at the PMHP service sites. Mental health screening coverage was 95%. Approximately one third (31%) of these women qualified for counselling, with 735 women taking up counselling appointments. The mean number of counselling sessions was 3.1 per client. Referrals were made for further specialist mental health care for 35 women. The figure over page describes the service flow.
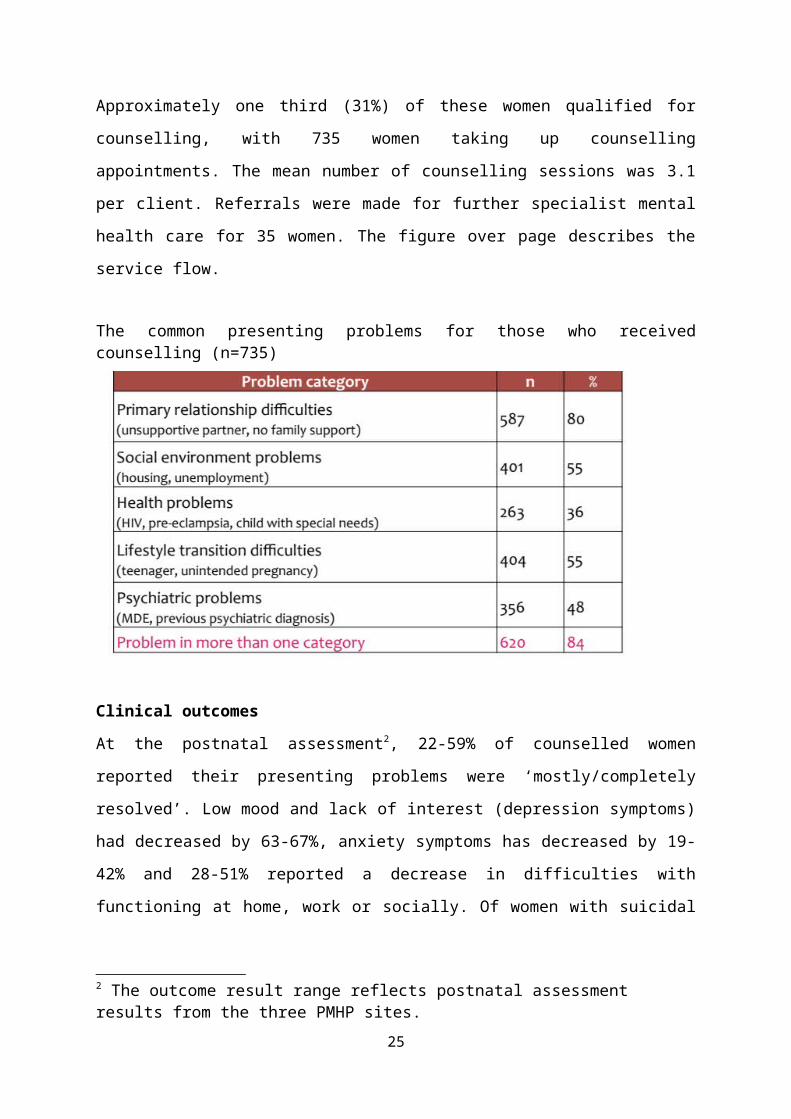
The common presenting problems for those who received counselling (n=735)
Clinical outcomesAt the postnatal assessment2, 22-59% of counselled women reported their presenting problems were ‘mostly/completely resolved’. Low mood and lack of interest (depression symptoms) had decreased by 63-67%, anxiety
2 The outcome result range reflects postnatal assessment results from the three PMHP sites.
20
symptoms has decreased by 19-42% and 28-51% reported a decrease in difficulties with functioning at home, work or socially. Of women with suicidal thoughts (some or regular), 95-97% no longer had these thoughts.
ConclusionCounselling over 3 sessions has a beneficial impact on suicidal ideation, depression and anxiety symptoms, as well as functioning. Integrating mental health care in to routine antenatal care provides an opportunity for early detection and effective management of common mental disorders.
21
SCREENING FOR POSTPARTUM DEPRESSION AT RAHIMA MOOSA MOTHER AND CHILD HOSPITAL
SH Karolia, AJ Wise, KA FrankDepartment of Obstetrics and Gynaecology, University of WitwatersrandSH Karolia, MBChBAJ Wise, MBBCh FCOG (SA), MMED, Dip HIV Man (SA), ACHM (FPD)KA Frank MBBCh, FCOG (SA), MMED
IntroductionMood disorders are the most common and serious maternal psychiatric conditions in the postpartum period and are classified in increasing severity into the postpartum blues, PPD and postpartum psychosis. A large systematic review established the average prevalence rate of PPD at 13%. The prevalence rates in some low resource countries are twice those of developed countries. A study of PPD in a periurban South African population found the point prevalence of PPD to be 34.7% while another study reported a 45.1% prevalence of PPD amongst HIV positive women in rural South Africa. PPD is associated with immediate and long term psychosocial morbidity to the mother, her partner and children. The impact of depressive symptoms in the critical postpartum period impairs mothering behaviour and attenuates maternal sensitivity to the infant. The resultant negative mother-child interaction predispose to adverse outcomes in various domains of infant neurodevelopment. Strong evidence links PPD to future childhood and adolescent psychopathology. Untreated PPD increases the risk for postpartum psychosis, suicide and infanticide. Risk factors that are significantly associated with the development of PPD include: A previous or pre-existing psychiatric illness, marital or partner conflict, recent life stressor and poor social support. PPD is both common and morbid and although effective treatment is available, fewer than half of all cases are recognised. Screening using a validated instrument can improve the rates of detection and treatment of PPD. Clinical outcomes are improved if screening is supported by referral systems aimed at diagnosis, treatment and follow up. South Africa at present has no national screening policy for PPD.
22
In an ongoing effort to improve maternal and perinatal outcomes both antenatal and postnatal care in South Africa is focussed predominantly on physical health. Maternal mental health remains a rather neglected aspect of obstetric care worldwide.
MethodsSettingRMMCH is a regional hospital affiliated to the University of Witwatersrand. Patients accessing care arise mainly from low income households and a growing immigrant population in the catchment area. In addition to referrals, low risk pregnancies are delivered at RMMCH as only one midwife obstetric unit services the area. There are on average eight hundred to one thousand deliveries per month at the hospital. The patient population at RMMCH is therefore representative of the general obstetric population in the area served.
SampleThe study population comprised English speaking women who delivered a live baby after 26 weeks completed weeks of gestation, either by vaginal delivery or caesarean section at RMMCH.Participants were recruited immediately postpartum during the period April to July 2015. Minors, under the age of eighteen were not included in the study and demise of the infant prior to the six-week follow-up was a criterion for exclusion. InstrumentsThe EPNDS is a 10 item self-report scale measuring mainly the emotional symptoms of depression experienced in the past seven days with less emphasis on somatic symptoms as they may be typical of the puerperium. Symptoms are scored based on their severity with a total possible score of 0-30. Screen positive for probable major depression is indicated by a score of 13 or greater or a positive response to the question on self or infant harm. The EPNDS has been validated for use in South Africa at RMMCH in 1998. For major and minor depression combined the sensitivity
23
reported was 80% and specificity 76.6%. A systematic review of studies validating the EPNDS found a larger difference in the sensitivity range when the scale was translated into other languages implying that the tool may be most sensitive when administered in English.
EthicsThe research protocol was approved by the University of Witwatersrand’s Human Research Ethics committee (M141015) and institutional approval was obtained from the CEO of RMMCH.
Data collection procedureParticipants were selected by random sampling from the delivery records in labour ward and caesarean section theatre. Written informed consent was obtained from mothers who were eligible for inclusion to the study. At the enrolment visit a sociodemographic and medical questionnaire was completed by interview and review of the patients’ medical records. Participants were contacted at their convenience six weeks post-delivery to complete the EPNDS. Screen positive patients scoring ≥ 13 or responding positively to the question on self or infant harm were referred to the department of psychiatry at RMMCH.
Data analysisData was captured electronically onto the REDCap data collection programme and analysed using Stata Version 11 (Statacorp, College Station, Texas, USA). Non binary variables were dichotomised and all possible explanatory variables were tabulated against screen outcomes. Chi-squared and Fischer’s exact tests were carried out and variables exhibiting a trend were tested further using multiple backward logistic regression.The sociodemographic variables tested included maternal age, race, nationality, level of education, employment, income and marital status as well as residence and support post-delivery. Obstetric variables tested against outcomes comprised first-time mothers, pregnancy intention,
24
twins, preterm delivery, HIV status, other co-morbidities, mode of delivery, prolonged labour, support and analgesia during labour. Variables relating to neonatal outcomes that were analysed with respect to screen outcomes included the infant’s gender, low birth weight infants, neonatal admission and prolonged separation from the mother after delivery.
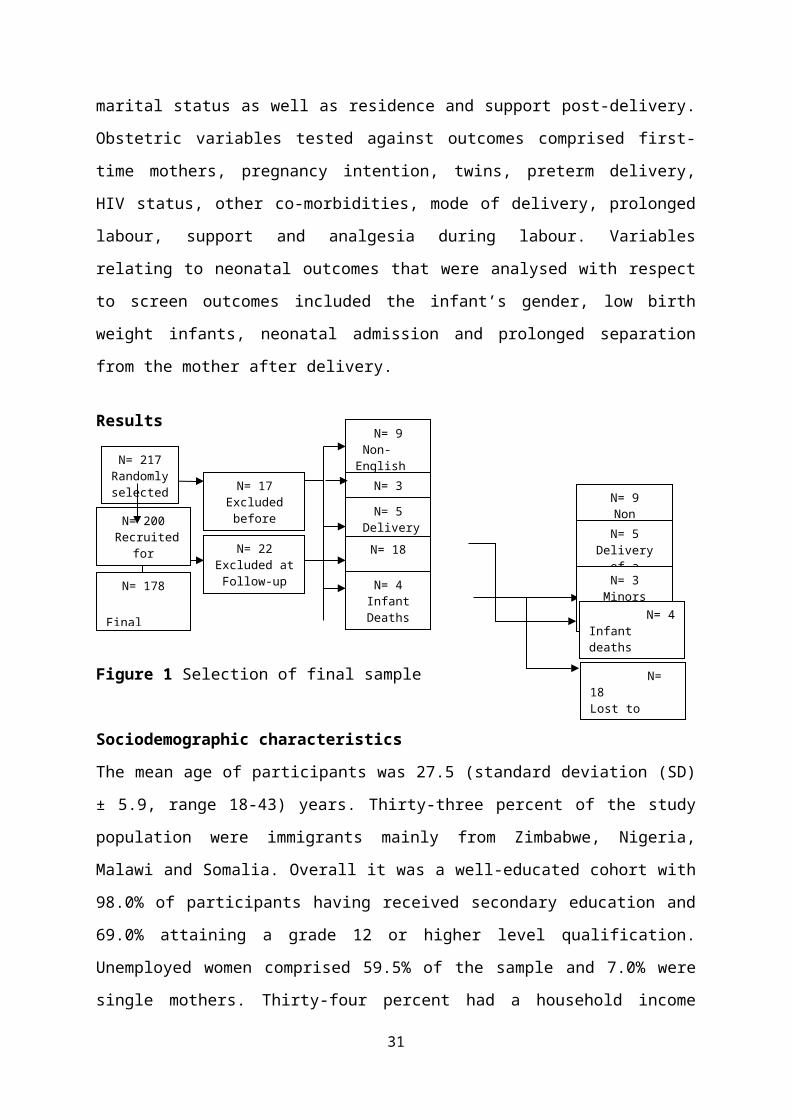
Results
Figure 1 Selection of final sample
Sociodemographic characteristicsThe mean age of participants was 27.5 (standard deviation (SD)± 5.9, range 18-43) years. Thirty-three percent of the study population were immigrants mainly from Zimbabwe, Nigeria, Malawi and Somalia. Overall it was a well-educated cohort with 98.0% of participants having received secondary education and 69.0% attaining a grade 12 or higher level qualification. Unemployed women comprised 59.5% of the sample and 7.0% were single mothers. Thirty-four percent had a household income below R2000 per month and 11.5% reside in informal settlements. Three percent of women report having no support system in the puerperium.
Medical and obstetric characteristicsPrimigravidas comprised 32.5% and grand multiparous females 2.5% of the postnatal sample. The proportions of planned and unplanned were almost equivalent with 52.5% unplanned but 99.5% of mothers wanted their babies following delivery regardless of pregnancy intention. The majority (97.5%) of pregnancies were singleton, the remainder (2.5%) were twin pregnancies. The mean gestational age at delivery was 38.0
25
N= 217 Randoml
y selected N= 9
Non English speakingN= 5
Delivery of a stillbirth
N= 3 Minors
N= 200 Recruited
for participatio
N= 4 Infant deaths
N= 18 Lost to follow up
N= 17 Excluded
before enrolment
N= 9 Non-English SpeakingN= 3
MinorsN= 5 Delivery of a
N= 178 Final
Sample
N= 22 Excluded atFollow-up
N= 18 Lost to follow-up
N= 4 Infant Deaths
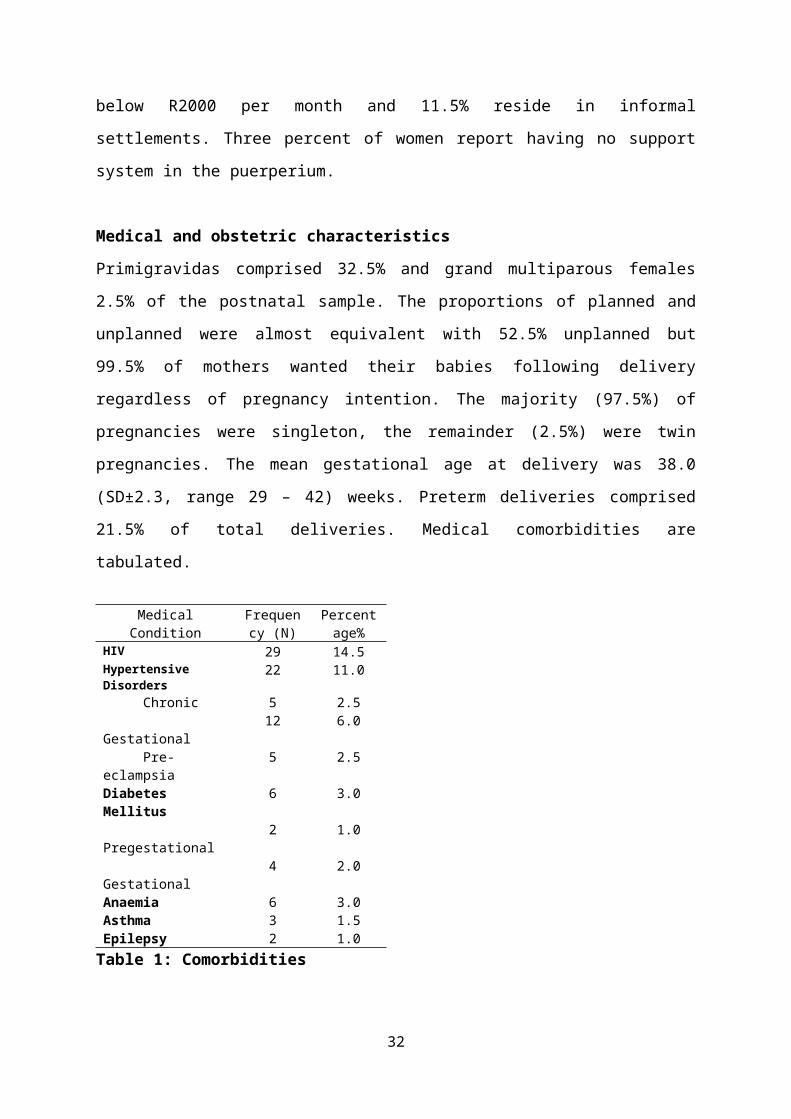
(SD±2.3, range 29 – 42) weeks. Preterm deliveries comprised 21.5% of total deliveries. Medical comorbidities are tabulated.
MedicalCondition
Frequency (N)
Percentage%
HIV 29 14.5Hypertensive Disorders
22 11.0 Chronic 5 2.5 Gestational 12 6.0 Pre-eclampsia 5 2.5Diabetes Mellitus
6 3.0
Pregestational 2 1.0 Gestational 4 2.0Anaemia 6 3.0Asthma 3 1.5Epilepsy 2 1.0
Table 1: Comorbidities
At recruitment 89.2% of HIV infected participants were on antiretroviral therapy. One participant gave a history of PPD in a previous pregnancy, one had overdosed on antenatal supplements in the index pregnancy and was undergoing psychiatric evaluation and three patients reported a family history of depression in a first degree relative.
Perinatal EventsTwo thirds (65.5%) of the study sample delivered vaginally and 34.5% by caesarean section. Included in the vaginaldeliveries are assisted deliveries and vaginal births after previous caesarean section which each comprised 1.5% of total deliveries. Prolonged labour defined as a greater than six-hour duration in active phase occurred in 19.9% of participants. A large proportion (71.8%) of patients were not accompanied by a support person and 67.9% received no analgesia in labour. The mean infant birth weight was 2997.2 (SD ± 563.1, range 1235 – 4610) grams (g). Low birth weight infants under 2500g comprised 17.5% of the neonatal population with 85.7% of these babies born at term. Fourteen percent of neonates required admission after delivery. The majority (93.0%) of mothers opted to breastfeed as the preferred method of feeding.
26
27
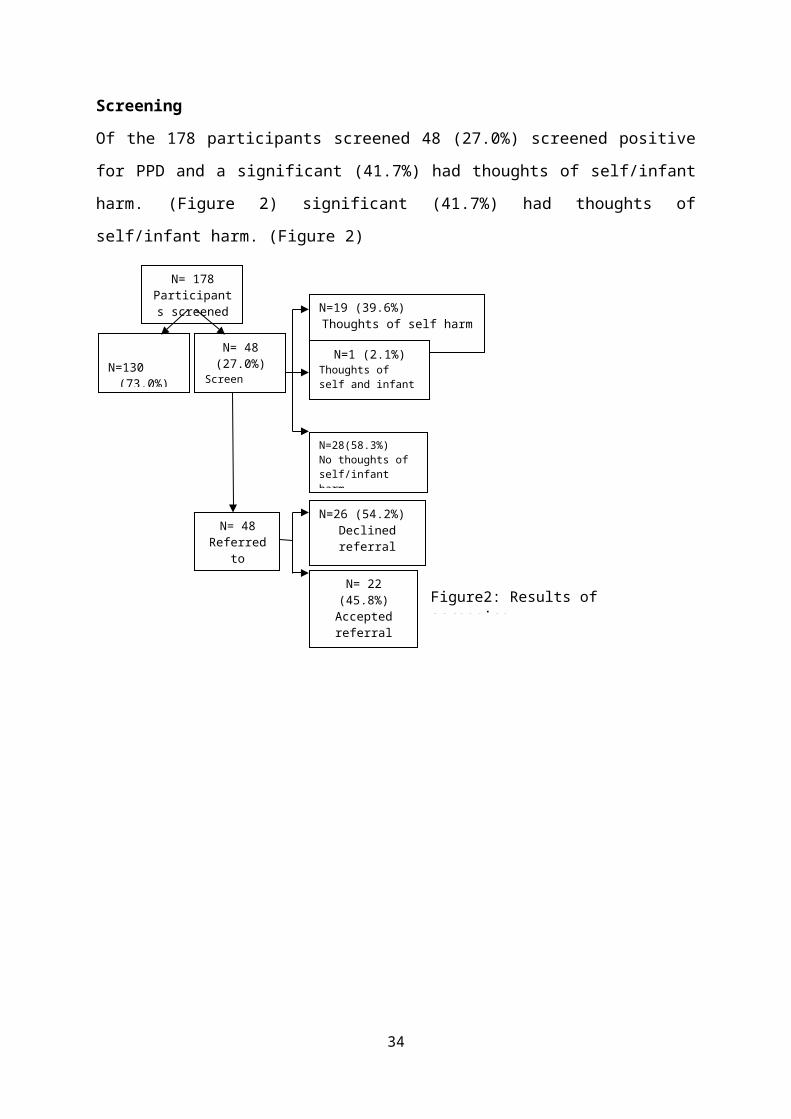
ScreeningOf the 178 participants screened 48 (27.0%) screened positive for PPD and a significant (41.7%) had thoughts of self/infant harm. (Figure 2) significant (41.7%) had thoughts of self/infant harm. (Figure 2)
28
N= 178 Participants
screened
N=130
(73.0%)Screen
N= 48 (27.0%)
Screen positive
N= 48 Referred
to psychiatry
N=19 (39.6%) Thoughts of self harm
N=1 (2.1%) Thoughts of self and infant harm
N=28(58.3%) No thoughts of self/infant harm
N=26 (54.2%)Declinedreferral
N= 22 (45.8%) Accepted referral
enrolment
Figure2: Results of screening
No statistically significant association between any of the sociodemographic, medical and obstetric variables tested against screen positive outcome were demonstrated in this study.
DiscussionAn ethnically diverse puerperal population comprising of both low and high risk obstetric patients were screened for PPD after six postnatal weeks. A significant proportion (43.8%) exhibited symptoms of minor and major depression with 27.0% screening positive for probable major depression. Thoughts of self-harm occurred frequently (41.7%) in participants that screened positive for PPD. Over half (54.2%) of screen positive patients declined referral to psychiatric services following screening. The main reason cited was adequate social support and in some cases time constraints and lack of caregiving to the neonate in the mother’s absence. This reinforces the role of adequate social support in moderating the impact of depressive symptoms. Predisposing factors to an increased
LimitationsThis study is limited by its small numbers and additional 9.0% loss to follow up. Non-English speaking patients were excluded from the study which comprised 4.1% of the initial sample selected. This was to allow the psychometrics of the however unlikely that the results would be altered significantly as a result of this exclusion. Possible explanatory variables that were not assessed in this study included intimate partner violence and use of injectable progestogens.(15)(16)
ConclusionPPD symptomology is common beyond 4 weeks postnatally. It may be difficult to predict patients who at risk of developing PPD antenatally or immediately postpartum. These findings support the rationale of universal screening.
29

RecommendationsLarger studies to examine factors that may be associated with a risk of developing PPD in a South African setting are recommended as well studies to evaluate the feasibility of screening for PPD at the 6-week postnatal clinic visit and barriers to patients accessing psychiatric care.
30
POSTPARTUM DEPRESSION AMONGST WOMEN ADMITTED TO A KANGAROO MOTHER CARE WARD
Elzet Venter 1 , Elise van Rooyen1, Anne-Marie Bergh21 Department of Paediatrics, University of Pretoria; 2 SA MRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria
Introduction:Postpartum depression (PPD) and the risk factors for the development of the disorder have been studied extensively in developed countries. There is a general lack of data on the prevalence of PPD in developing countries. In developed countries, it is estimated to affect 10 to 15% of women after child birth4. In South Africa the prevalence is estimated to be 34.7%.
The effects PPD can have on a baby’s emotional development are numerous. At 6 months babies with mothers suffering from PPD have reduced capabilities to interact verbally and visually. They tend to avert their gaze and turn their body away from the mother. These babies experience more problems with breastfeeding and sleep pattern disturbances. Long term complications include difficulty in forming attachments and diminished skills in emotional, social, cognitive and verbal areas of development8. Preterm and LBW infants are normally at higher risk to incur developmental delays. To prevent this from happening mothers need to be very involved with their infants; they should be able to bond and interact with their infants. In this instance it is even more important to recognise women who may be at risk of developing PPD and to refer them for counselling and therapy.Several risk factors for PPD have been identified. These include a history of depression, either during pregnancy or at other times, stressful events during the past year such as illness, job loss or pregnancy complications, relationship problems, lack of a support system, financial problems, unplanned or unwanted pregnancies, substance abuse or history of abuse and separation of mother and baby. Social stressors and lack of support seems to be more important risk factors while there is not clear evidence that poverty increases the risk.
31
32
Research question:1. How many mothers with low birth weight and or premature infants admitted to a kangaroo mother care ward screened positive for PPD?2. What factors are associated with an increased risk for PPD?
Setting:Kalafong Tertiary Provincial Hospital serves mainly a population with a low income in an urban population. The hospital is a referral hospital for high risk pregnancies. The kangaroo mother care ward is a step down unit for infants discharged from neonatal ICU and high care unit.
Edinburgh Postpartum Depression Scale (EPDS)The EPDS was developed and validated for use in the United Kingdom. It is a 10 point self-reporting instrument. There are 10 questions with a choice of 3 answers. Each of the answers carries a certain value. A score of ≥ 12/30 predicts PPD.In our study we opted to use a modified version of the EPDS. This modified version of the EPDS was validated for use in a South African multilingual urban population. It was administered verbally to participants. A threshold of ≥ 12/30 identified 100% of women with major depression. The positive predictive value was 53% and the negative predictive value was 92%.
Inclusion criteria1. Mothers who voluntarily agree to participate.2. Mothers with babies born less than 37 weeks gestational age.3. Babies with birth weights less than 2500 gram.
Exclusion criteria1. Caregivers other than mothers.2. Mothers unable to communicate sufficiently due to language
constraints.
33
3. Mothers whose babies have died, or have a life threatening genetic or structural abnormality.
4. Teenage mothers younger than 16 years (appropriate age for giving consent).
5. Mothers previously diagnosed with a mood disorder or who are currently on mood stabilising medicine.
Method:Consent was obtained from the Ethics Committee at the University of Pretoria. A short pilot study was conducted during December 2014. An experienced research assistant who was multi-lingual interviewed each mother privately. Informed consent was obtained, the modified EPDS and a demographic questionnaire was completed by the research assistant. The demographic information collected form the mother included the age, citizenship, gravity, parity, pregnancy planned, delivery method, HIV status and social information (education, employment and support). Information about the infant included the birth weight, gestational age and gender. Data was collected from 1 January 2015 until 31 December 2015.
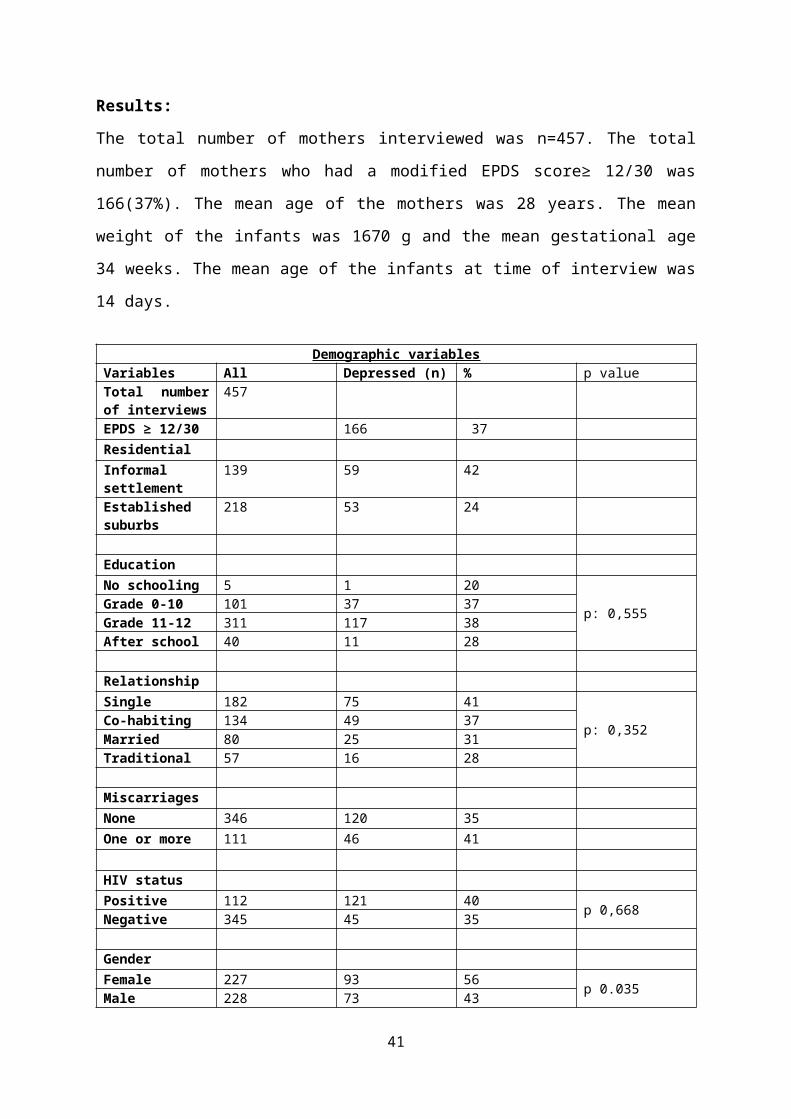
Results:The total number of mothers interviewed was n=457. The total number of mothers who had a modified EPDS score≥ 12/30 was 166(37%). The mean age of the mothers was 28 years. The mean weight of the infants was 1670 g and the mean gestational age 34 weeks. The mean age of the infants at time of interview was 14 days.
Demographic variablesVariables All Depressed
(n)% p value
Total number of interviews
457
EPDS ≥ 12/30 166 37ResidentialInformal settlement
139 59 42
Established suburbs
218 53 24
34
EducationNo schooling 5 1 20
p: 0,555Grade 0-10 101 37 37Grade 11-12 311 117 38After school 40 11 28
RelationshipSingle 182 75 41
p: 0,352Co-habiting 134 49 37Married 80 25 31Traditional 57 16 28
Miscarriages None 346 120 35One or more 111 46 41
HIV statusPositive 112 121 40 p 0,668Negative 345 45 35
GenderFemale 227 93 56 p 0.035Male 228 73 43
The mothers who presented with PPD were 37%. No maternal factors could be identified to show association with PPD. Strangely there were more depressed mothers who delivered a female infant compared to those with male infants. This was also the only statistical significant variable. The reason for this is unclear. A higher percentage of woman (40%) diagnosed HIV positive were screened with having PPD versus HIV negative woman with PPD (35%) but it was not statistically significant.
Limitations:This was an observational descriptive study undertaken amongst mothers admitted in a tertiary referral hospital. High risk pregnancies and deliveries are managed at the institution. Some of the mothers admitted to the unit are non-RSA citizen. Due to language constraints a number of these women could not be interviewed. During the period of the study a part time counsellor was available two days a week to counsel any mother with emotional problems. This counselling service could be a reason why the depression levels of the mothers were not higher.
35
Discussion:Postpartum depression was found to be very prevalent amongst women with low birth weight and or premature infants. A higher PPD prevalence among the premature infants was expected but maybe because of the lodger facilities and counselling services provided at Kalafong hospital. The prevalence was very similar to the findings of the Cape Town study that was done at a well-baby clinic in Cape Town 37% versus 35%. It is important to note that one in three women was found to have symptoms of PPD and that it is important that counselling services and psychologists are available to counsel mothers.Gender was the only associated factor found to be statistically significant amongst the group of women with PPD. The reason for this is unknown. Socioeconomic factors may explain why the women staying in informal settings have an increased percentage of PPD.
Recommendations:We recommend that screening for PPD should be part of routine postnatal care. It is especially important for mothers with low birth weight and or premature infants to have access to counsellors and psychological support. Appropriate treatment and follow-up should be ensured for mothers identified as being diagnosed with PPD in order to prevent complications in the infants.
36
RISK OF NEONATAL MORTALITY ASSOCIATED WITH FIRST ADMISSION TEMPERATURE AT A SEMI-RURAL HOSPITAL. (LURWMH)
N Kapongo , M Malahleha, Z Duze*, (*): Paediatric Department, Neonatal Unit, Lower Umfolozi, Regional War Memorial Hospital (LURWMH).
IntroductionEach year an estimated 3.6 million neonatal deaths occurs globally. The main causes of these deaths are complications due to prematurity, intrapartum- related asphyxia and infections. Neonatal hypothermia as a factor contributing to morbidity and mortality risk of newborns has been recognized by the World Health Organization (WHO). Hypothermia has been defined by WHO as body temperature below the normal range (36.5ºC-37.5ºC) and has been sub-classified into three grades: mild (36.0º C-36.5ºC), moderate (32ºC-35.9ºC) and severe (<32ºC) hypothermia. For each of these classifications, there are guidelines in place for responding to or managing hypothermia. Furthermore, the WHO has published guidelines on thermal care and has included thermal care of newborn as one of the elements of essential newborn care (ENC) that should be provided to all newborns regardless of settings. Despite this recognition within global guidelines and recommendations for neonatal care, there are major gaps in our understanding of the burden, risk factors, and consequences of neonatal hypothermia in our low resource settings where exposure is greatest.It is of little surprise that hypothermia is a common phenomenon in low resources settings, including among babies born in facilities and in the community. Mullany et al described in southern Nepal, 21,459 of 23,240 babies (92.3%) had one or more axillary temperature below 36.5°C, half of babies were moderately to severely hypothermic, and risk peaked in the first 24-72 hours of life. The risk of moderate to severe hypothermia, increased by 41.3% for each 5°C decrease in ambient temperature. Even in the hottest season of the year, almost one-fifth of babies were hypothermic.
37
Hypothermia among newborns is considered an important contributor to neonatal morbidity and mortality in low resource settings. However, in these settings only limited progress has been made towards quantifying the problem and understanding the risk of mortality subsequent to hypothermia. We sought to describe the incidence of neonatal hypothermia and quantify the neonatal mortality and hypothermia association using the first temperature observed in the admission room of a busy Semi-rural unit in the Northern hot setting of Kwazulu- Natal province, South Africa.
Material and Methods
Clinical FacilitiesEmpangeni Neonatal unit is part of a child and Maternal Hospital, Lower Umfolozi District War Memorial Hospital (LUDWMH) in North-East of Kwazulu-Natal, South Africa. This is the only maternity and neonatal regional referral Centre for an area with a population estimated at 2 Million with 16 District hospitals as referring entities. Fifty thousand (50 000) live births occur in the entire area annually including 10 000 at LUDWMH. The neonatal service was introduced at the hospital in 1998 with a 15 unit beds without intensive care facilities. Between 1999 and 2008 the unit was expanded to 92 bed neonatal units: 16 NICU beds, 40 high care, 16 special care beds and a Kangaroo mother care (KMC) unit (20 beds). Because of the burden in neonatal admissions needing mechanical ventilation, our NICU unit is set up to allow only 2.8 meters square around every infant bed which is below the provincial norms of 5 meters squares. Eight full time Paediatric and seven Obstetric consultants run the Paediatric and maternity & Gynecological services, respectively.
Data collectionA prospective, computerized data set of all routine neonatal admissions has been in place at LUDWMH since January 2000. This data base has been up graded to Epi-Info 7 software in January 2016. Additional
38
information was added including admission temperature. On admission, at discharge and during the weekly neonatal morbidity and mortality review, standardized routine clinical and laboratory data on neonates are collected in a monthly edited admission book template compatible with CDC Epi-Info. 7 locally designed data set. Data extracted include Date of admission, patient’s details, maternal details, demographics, presenting signs, admissions diagnosis, final and secondary diagnosis, treatment and procedures & complications, outcomes, date of outcome and basic laboratory tests. Infants admitted to neonatal intensive care unit (NICU) have additional page for standardized NICU details. Formulation of clinical diagnoses follow recognized guidelines for management of common illness with limited resources. A secretary support team helps to update daily the information (final diagnosis, secondary diagnosis, outcome and date of outcome). A monthly data clean-up is done before to run the monthly program which generates result for the monthly report.
Hypothermia definitionHypothermia has been defined by WHO as body temperature below the normal range (36.5º C-37.5 º C) and has been sub-classified into three grades: mild (36.0º C-36.5º C), moderate (32º C-35.9º C) and severe (< 32 º C) hypothermia (3).
Outcomes measured and Analysis model.The main outcomes were hypothermia in the neonatal admission room and neonatal death during the Neonatal stay.A Stepwise unconditional logistic regression was applied to evaluate the variables associated with these two outcomes. For hypothermia, maternal and neonatal characteristics (Maternal age <20 years, antenatal visit attendance, C/S delivery, Male sex, Birthweight <1500g, 5 min- Apgar score 0-6, Neonatal ICU admission, being born in hospital) were considered to be independent variables. Unfortunately, some key variables related to neonatal thermal care (maternal temperature before delivery, Delivery room (DR) temperature, use of cap, positive pressure ventilation with cold
39
air at DR, use of plastic bag/wrap) are not part of the routine capturing system. For Neonatal mortality, maternal and neonatal characteristics at birth, hypothermia at admission, and neonatal morbidity were evaluated as independent variables. Admission to NICU was used as surrogate variable for severity of morbidity. Variables with a value of P < .20 in the univariate analysis were included in the initial logistic model.
40
Statistical AnalysisCapturing and analysis were carried out using CDC Epi-Info-7 programme. This include simple frequency analysis, Stratified analysis to determine stratum specific odds ratio, Chi-square associations to determine odds ratios and confidence intervals, Summary odds ratio and parametric & non parametric one-way analysis of variance test for comparing means, The Logistic Regression command performs conditional or unconditional multivariate logistic regression with automatic dummy variables and support for multiple interactions. A 5% level of significance was used.
ResultsDuring the 8-month study period, 2087 neonates were admitted with 77.1 %( 1606) being in-hospital born. Axillary temperature at admission level was recorded in 2066 (99.1%) neonates, and hypothermia was noted in 75.8% (1568) (mean=35.8º C; Median= 36.0º C; 25th-75th percentile 35.3º C-36.4º C). The different categories of admission temperature are shown in table 2. Only 22.8% (468) of infants had normal skin temperature on admission. The overall hypothermia incidence is 75%. Mild hypothermia and moderate hypothermia are the 2 big categories, 36.8% (95% CI 34.7-38.9%) and 38.6% (95% CI 36.5-40.8%), respectively. Potential determinants of neonatal hypothermia in admission room are reported in table 3. In univariate analysis, birth weight < 1500 g (OR 2.2 (95% CI 1.59-3.12; p < 0.0000) and NICU admission (OR 1.54, 95% CI 1.18-2.01; p < 0.001) were associated with hypothermia. Being born in- hospital was protective of hypothermia on admission (OR 0.67; 95% CI: 0.51-0.82; P < 00032). Table 4 summarize the proportions of some maternal and neonatal variables, according to the neonatal morality outcome. Birth weight < 1500g, which is the surrogate variable for prematurity, showed high proportion (55.6%) in the mortality group compared to 15.2% in the survival group (OR 6.9; 95%CI: 4.7-10.2; P< 0.0000). The surrogate variables of Perinatal asphyxia (5 min Apgar score 0-6) and that of disease severity (NICU admission), were strongly associated with mortality (OR of 2.2 and 4.18,
41
respectively). C/S delivery and in hospital delivery seem to be inversely associated to neonatal mortality (OR 0.57 and 0.65, respectively). The final logistic model showed that being born outside and NICU admission variables are associated with hypothermia on admission (Adjusted OR =2.09; 95% CI: 1.52-2.87) and (Adjusted OR 1.60; 95% CI 1.19-2.16), respectively. An Apgar score 7 or more and birth weight 1500 g or more are protective variables for admission hypothermia (Adjust OR 0.55: 95% CI 0.37-0.081) and (Adjusted OR 0.31: 95% CI 0.21- 0.44), respectively. With regard to neonatal mortality, admission to NICU variable was associated to neonatal mortality outcome (Adjusted OR= 1.92; 95% CI= 1.26-2.94). The following variables were found to be inversely associated with the neonatal mortality outcome: Apgar score 7 or more (Adjusted OR = 0.21; 95% CI 0.12- 0.37), birth weight 1500 g or more (Adjusted OR= 0.12; 95% CI 0.08- 0.20) and born in – hospital (Adjusted OR= 0.54; 95% CI 0.35-0.85). Normo-thermia seems protective of mortality (Adjusted OR 0.83) but this was not statistically significant (95 % CI 0.49- 1, 41).
DiscussionIn this cohort of neonates with 22.9% of out born and 17.69 % of very low birthweight infant’s proportion, the incidence of hypothermia at Nursery admission level, was extremely high. The database shows significant limitations to assess the neonatal thermal care in details because of lack of information related to maternal temperature before delivery, Delivery room temperature, details of incubator temperature during transportation to the neonatal unit, the timing of neonatal admission, lack of detailed information related to hypothermia preventive practices such as use of plastic bag/wrap, use of cap and use gas during resuscitation. Despite these limitations, these results add to the current evidence in the literature arguing for the urgency of initiating practices to maintain normothermia as soon a neonate is born especially Prem neonates and sick neonates. Low-cost interventions for thermal protection, an essential component of newborn care exist and include immediate drying, wrapping, delayed bathing, early breastfeeding initiation, and skin-to-skin
42

contact. The Neonatal Task Force of the International Liaison Committee on Resuscitation recommended in 2010 Consensus on Science that “newborn infants of <28 weeks’ gestation should be completely covered in a polythene wrap or bag up to their necks without drying immediately after birth and then placed under a radiant heater and resuscitated or stabilized in a standard fashion. Infants should be kept wrapped until admission and temperature check. Coverage or adherence to these practices at LURWMH need careful evaluation and quality assurance strategies put in place and systematic implementation plan. In univariate analysis, our data established an association between moderate hypothermia and neonatal mortality (OR 1.95: 95% CI 1.12-3.43; p< 0.01615). The proportion Very low birth infant was a major confounder variable. The studies that provide evidence of the association between hypothermia at NICU admission and neonatal mortality are either retrospective or secondary analyses of data collected to evaluate other primary outcomes. In a Malaysian VLBW study group with 868 patients, the chance of hospital mortality was 1.26 times (95% CI 1.06-1.50 times) greater for infants with body temperature <36.5ºC at NICU admission. More recently, the Brazilian Network on Neonatal Research study, which was prospectively designed to verify an association between early neonatal mortality and hypothermia at NICU admission, showed that the chance of early neonatal death is 1.64-fold (1.03-2.61). It remains unclear whether hypothermia at NICU admission is a cause of neonatal mortality or a marker of high patient acuity. Our review included all neonates, the adjusted OR of normothermia below unity (0, 89) seem seems inversely associated to neonatal mortality but this was not statistically significant (95 % CI: 0.49-1.41).
ConclusionUsing WHO classification, hypothermia is a frequent event on arrival in the admission room. A moderate hypothermia reading on admission was significantly associated with poor outcome in Univariate analysis. Very low birth weight was found to be major confounder mortality’s determinant. It
43
is possible that measures aimed at preventing WHO moderate level hypothermia may dramatically decrease neonatal mortality burden at LURMH.
44
INFANTS OF DIABETIC MOTHERS: MATERNAL AND INFANT CHARACTERISTICS AND INCIDENCE OF HYPOGLYCEMIA
Yoliswa Magadla, Fatima Moosa and Sithembiso VelaphiDepartment of Paediatrics, Chris Hani Baragwanath Academic Hospital and the University of the Witwatersrand
BACKGROUNDDiabetes mellitus (DM) is a multi-
systemic disease with a rapidly increasing incidence and is estimated to double by 2030. This is attributed to increasing trends of urbanization and modernization, which grow in parallel with the epidemics of overweight, obesity and improved diabetes management. It is the most common metabolic disease affecting pregnancy and it may result in adverse fetal
45
and neonatal outcomes. In 2013, 21 million live births were complicated by diabetes during pregnancy according to International Diabetes Federation. Over the past years the outcomes of diabetic pregnancies have improved due to advanced management provided by practitioners for mothers and the newborns. Previous studies have reported higher prevalence of gestational than pre-gestational DM. Hypoglycemia is reported to develop in 20-50% of infants of diabetic mothers (IDM) and 15-25% of hypoglycemic IDM are born to mothers with gestational diabetes. Hypoglycemia is typically noted in neonates who are large for gestational age (LGA) or small for gestational age (SGA) and those infants whose mother had a poor glycemic control during pregnancy. The nadir in IDM blood glucose levels usually occurs between 1-3hrs of life, can persist up to 72hrs and may even last up to a week. No single study is conclusive as to whom and when should neonatal glucose testing be routinely done. A recommendation by Williams et al, is that infants must be screened at 4-6 hours of life with the emphasis that no studies demonstrated harm from few hours of hypoglycemia, but other cohort studies demonstrate that IDM mostly have asymptomatic hypoglycemia in the first hour thus supporting screening earlier in these infants. Holtrop et al also concluded that IDM were likely to develop hypoglycemia by 1hour of age, therefore also supporting the earlier screening recommendation and to stop after 12hours if glucose levels remain above 2.6mmol/l. At Chris Hani Baragwanath Academic Hospital (CHBAH), there is a significant number of IDM who get admitted for monitoring of glucose. The proportion of patients who develop hypoglycaemia is not known and the characteristics of those who develop hypoglycaemia are also not known. The aim of this study was to describe the characteristics of IDM with or without hypoglycaemia and to determine prevalence of hypoglycaemia in IDM.
METHODSThis was a retrospective descriptive study that included only infants with birth weight of 2000g or more, gestational age of 34 weeks or more and admitted to the neonatal unit at CHBAH from January 2012 to December
46
2013 with a diagnosis of being IDM only. Hospital medical records of infants with a diagnosis of IDM were reviewed and maternal and infant demographics, maternal diabetic type and treatment, infant anthropometry, glucose levels and hypoglycemia diagnosis were entered in a data-capturing sheet. Infants were excluded if they had sepsis or medical records were missing.
RESULTSA total of 234 IDM were admitted over this 2-year period and 207 met inclusion criteria. Majority of mothers (94.1%) were of African origin. Median maternal age was 33 years. Only three mothers were of the age <20 years in this study, and all had pre-gestational diabetes. There were no significant statistical differences in maternal age between those with gestational and pre-gestational diabetes. Seven percent of mothers had stillbirths, 14% had miscarriages in previous pregnancies. The common co-morbidity in mothers of these infants was hypertension, present in 24% of mothers. Among the 181 mothers whose type of diabetes was known, 56% had gestational diabetes. Fifty percent of mothers were on insulin, with 56% of those with pregestational diabetes receiving insulin compared to 45% among those with gestational diabetes. The haemoglobin A1c was >7% in 52% of diabetic mothers.
Among the infants, 54% were born preterm, 19% were large for gestational age (LGA) (weight >95th percentile) and 10% were macrosomic (birth weight >4000 grams). There were no statistical significant differences in prevalence of LGA and macrosomia between the two types of maternal diabetes. Pre-gestational diabetic mothers had higher preterm births than gestational diabetic mothers (64% vs 48%, p=0.037).
Among the 207 IDM, 81 (39%) had hypoglycemia (defined as random glucose of <2.6mm0l/l) and it occurred in 42.5% in the pre-gestational DM
47

compared to 36.6% in those with gestational DM (p =0.422). In most (85%) of the infants the hypoglycemia occurred within the first 3 hours of life with no difference between pre-gestational and gestational DM groups with respect to the time of presentation of hypoglycemia. Only one baby developed hypoglycemia after 24hours. In comparing characteristics of IDM with hypoglycaemia to those who normoglycaemia, more babies in the hypoglycaemic group were LGA than in normoglycaemic group (28.2% vs 12.8%, p = 0.009). There were no statistical significant differences in maternal characteristics, type of diabetes or management of diabetes between hypoglycaemic and normoglycaemic IDM.
DISCUSSIONThe main findings in this study were that more than half of IDM are born to mothers with gestational DM that correlates with previous studies8, 9. Most of the mothers with diabetes were of childbearing age and in those who were less than 20 years, all of them had pre-gestational diabetes and specifically all had type 1 DM. Though more than 50% of mothers were managed with insulin, a significant number (37%) were managed with oral hypoglycemic. This is higher than that reported by Van Haltren et al.8 who reported 47.2% on insulin management. Occurrence of previous stillbirths (7%) and miscarriages (13.5%) as well as hypertension (24%) as comorbidity was noted and correlates with previous studies 8, 10. The prevalence of LGA and macrosomia was lower in this study compared to that previously reported by other studies8, 11, which reported prevalence of LGA and macrosomia to be 35% and 12% respectively. The difference between the findings in this study and the above-mentioned studies could be from possible inaccurate dating of gestation in this study, as many mothers did not have antenatal sonars.
About 40% of IDM developed hypoglycemia that is lower than report by Das et al.12 of 56% but higher than 33.5% reported by Van Haltren et al8. Most infants had hypoglycemia within the first 3hours of life which is same as also reported by Nold et al5. The only difference that was found
48
between hypoglycaemic and normoglycaemic infants in this study was the prevalence of LGA, while other studies reported association between development of hypoglycemia with SGA, increased Hba1c and poor maternal control in addition to LGA4, 8. Limitations in this study include retrospective nature of the study thus difficulty finding complete data for example about 12% of mothers the type of diabetes was not recorded. Few mothers had antenatal sonar and this could have contributed to inaccurate dating, therefore made it difficult to give accurate assessment of growth.
CONCLUSION A significant number of IDM developed hypoglycaemia soon after delivery with most patients developing hypoglycaemia within the first 3 hours of life. Large for gestational age was the only infant characteristic found to be significantly associated with hypoglycemia. Based on the findings of this study, we recommend that well IDM weighing 2000 grams or greater at birth or at gestation of 34 weeks or greater have glucose testing at the bedside using a point of care testing system (haemoglucotest) within an hour after delivery then hourly for the first 3-4 hours of life in a high care or triage area while continuing with breast feeding. If the haemoglucotest levels are >2.6 mmols/L with all measurements, then the infant can be transferred to his/ her mother where he/ she can be monitored with haemoglucotests 3 hourly for another 12-24 hours before discharge.
49
AN ASSESSMENT OF INTENDED INFANT FEEDING PRACTICES OF WOMEN WHO DELIVER AT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
YP Kennedy, Y AdamDepartment of Obstetrics and Gynaecology, University of Witwatersrand
IntroductionThe causes of morbidity and mortality in children under the age of 5 are multifactorial, and often relate to poor nutritional status. Early infant feeding practices are important in supporting child health, since nutrition plays a critical role in their growth and development. Breastfeeding (BF) remains an important means to reduce child morbidity and mortality in resource poor countries. The current South African (SA) national infant feeding policy recommends that all children be exclusively breastfed for the first 6 months of life, with introduction of safe and complimentary food at 6 months. Even though breastfeeding initiation in this country is common, with a reported rate of 82% in 2003, EBF seems to be a rare practice. The South African Demographic Health Survey (SADHS) has revealed that in 2003, 20% of babies in this country were never breastfed, and only 8.3% are EBF up to 6 months of life. Many studies have also shown that SA mothers make inappropriate feeding choices, with the introduction of supplementary and/ or complementary foods at an early age. Furthermore, many of the HIV+ mothers who chose to exclusively formula feed did not meet the AFASS criteria.SA struggles with high rates of poverty and unemployment. Encouragement of BF can serve as a beneficial strategy to improve household food and economic security.
MethodsThis was a prospective cohort study of a sample of women who delivered CHBAH in the period from 17 April till 6 May 2015. The study was conducted in the postnatal wards of the hospital - a tertiary care institution in Soweto, SA which is an urban area south of the city of Johannesburg and home to 40% of Johannesburg residents. Its population
50
is predominantly black, with all 11 of the country’s official languages spoken by residents – the main linguistic groups being IsiZulu, Sesotho, Venda and Tsonga.The maternity unit of the CHBAH is the largest maternity unit in SA, with 300 maternity beds and just over 22 000 babies delivered a year.
SampleThis was a convenience sample, with participants recruited from the postnatal wards of CHBAH. Eligibility of interested participants was assessed using the inclusion criteria.Included in the study were mothers who:
Aged 18 years and above were well enough to be with their babies from birth had delivered singletons no less than late preterm (>356 gestation),
with baby’s weight 2500g and above gave birth to normal babies, with Apgar’s no less than 7 at 5
minutes and no neonatal ICU admission
EthicsThis study was done with the approval of the Human Research Ethics Committee at the University of Witwatersrand (ref M140394). Since the study involved patients and patient records that were the property of the CHBAH, approval from the hospital CEO and the Head of Department of Obstetrics and Gynaecology at the hospital was also obtained prior to the study. Participation in the study was completely voluntary, and consent was obtained from the patients before the initial interview.
Data collectionData collection took the form of a researcher administered questionnaire in 2 phases. The initial phase took place in the form of a face to face interview between the participant and researcher, where a questionnaire was filled with the help of some information obtained antenatal records.
51
The second phase took place in the form of a follow up telephonic administered questionnaire 6 weeks later to assess actual infant feeding practices.
Data analysisAnalysis was done using the program STATA version 11.0 from StataCorp®. Categorical variables were described using frequencies and percentages, and presented in frequency tables. Continuous variables were described using medians (with interquartile ranges) or means (with standard deviations). The relationship between continuous responses was determined using the Mann Whitney test. The comparison of categorical variables was investigated, and statistical significance was calculated using the Fisher exact test. A p-value of p< 0.05 represented statistical significance in hypothesis testing, and 95% confidence interval was used to describe the estimation of unknown parameters. The Fisher’s exact test was used because of the small sample size.
Results
Figure 1 Sample overview
A total of 132 participants were recruited for the study and 124 (93.94%) were reached for a follow up interview, with 8 participants (6.06%) lost to follow up (see Figure 1). A majority of these participants were of black ethnicity (99.24%), with an age range of between 18-42 years (mean age 27 years, SD±5.92). The main preferred spoken languages were English 37.88% (n=50), isiZulu 23.48% (n=31), Sotho 21.97% (n=29), Xhosa 6.82% (n=9), Tsonga 3.03% (n=4) and other (Venda and Shona) 3.03%
52
6week follow
up intervie
w124
loss to follow
up8
total132
(n=4). Five participants (3.79%) did not have any particular language preference. This population sample had an unemployment rate of 71.21% (n=94). The majority listed their accommodation type as formal (n=93; 70.45%), with access to piped water and ablution facilities, 34 (25.76%) were living in informal settlements, and 5 (3.79%) were living in a hostel.
Table 1 shows a description of some antenatal factors.
Table 1 A description of antenatal factorsVariable Frequency Percentage (%)
Antenatal care attended n=132Yes 127 96.21%
No 5 3.79%
Type of antenatal care attended n=127
Midwife Obstetric Unit (MOU) 97 76.38%
Secondary/Tertiary Health care Facility
10 7.87%
Private General Practitioner 1 0.79%
Mixed: MOU and Secondary/Tertiary care facility
19 14.96%
Infant feeding education received at antenatal care visits n=132
Yes 115 90.55%
No 12 9.45%
Method of infant feeding education received n=115
Group counseling 80 69.56%
Individual counseling 22 19.93%
Pamphlets 2 1.74%
Mixed group counseling and pamphlets
9 7.83%
Mixed group counseling and individual counseling
2 1.74%
At initial interview, 113 (85.61%) participants had initiated breastfeeding. Table 2 indicates their intended feeding practices.Seventy-seven participants (58.33%) chose the health care provider as their most influential source in decision making. This was followed by a
53
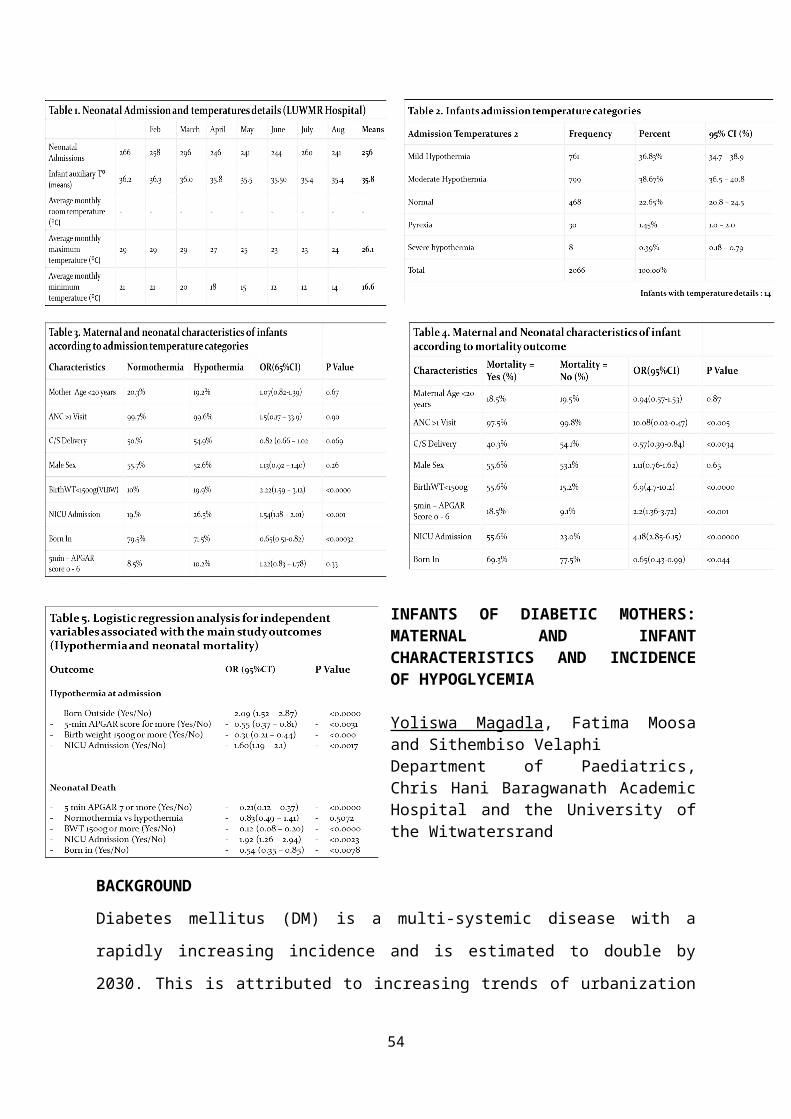
close relative (n=39, 29.54%) and the media (n=12; 9.09%). Two participants (1.52%) listed their peers as their most influential source, and another 2 (1.52%) mentioned that they relied on themselves to make the decision.
Infant feeding Practice n=132 (%)
EBF 91 (68.94%)
Formula feeding 19 (14.39%)
Mixed feeding 21 (15.91%)
Although only 65 (49.24%) of the participants answered the question “what do you understand by the phrase ‘EBF’?” correctly, this population of participants seemed knowledgeable in the benefits of breastfeeding – see Table 3.
Table 2 Intended infant feeding practice
Table 3 Maternal knowledge on the benefits of breastfeeding
54
Statement: n=132 Agree Disagree
Not sure
1. Formula milk is just as good for my baby as breast milk.
20 (15.15%)
93 (70.45%)
19 (14.40%)
2. Breast milk supplies sufficient nutrition for the growth and development of my baby during the first 6 months of life
114 (86.36%)
13 (9.85%)
5 (3.79%)
3. Breast milk can protect my baby against acquiring respiratory infections.
113 (85.61%)
7 (5.30%)
12 (9.09%)
4. Breast milk reduces the chances of my baby acquiring life threatening diarrhea.
112 (84.85%)
7 (5.30%)
13 (9.85%)
5. Breastfeeding provides protection against later development of childhood obesity.
81 (61.36%)
20 (15.15%)
31 (23.48%
6. Breastfeeding allows me to bond with my baby
121 (91.67%)
5 (3.79%)
6 (4.54%)
In addition, amongst the women that were breastfeeding, 103 (78.03%) women had no problems breastfeeding in the presence of close friends and family, but only 73 (55.30%) would be comfortable breastfeeding in public. At 6 week follow up, a large majority of participants (n=86; 69.36%) were still EBF their babies (Table 4). Patient factors that had a positive association with EBF were employment status and parity (p value< 0.05). When infant feeding practices were compared to the intended feeding practices immediately post-delivery, the intention to EBF was directly associated with EBF at six weeks – p value <0.001. Other positive predictors of exclusive breastfeeding in this population group included the knowledge that breast milk provided sufficient nutrition for the baby until 6 months of life (p value = 0.05); as well as maternal comfort to breastfeed in the presence of a family member (p value = 0.015).Table 4 Infant feeding practices at 6 weeks
EBF Formula feeding Mix feeding
Prevalence:n=124 (%)
86/124 (69.36%) 19/124
(15.21%)
19/124 (15.21%)
Parity (p value=0 .001
First time mothers n=45 24/45 (53.33%) 7/45 (15.56%) 14/45 (31.11%)
Multiparous participants n=79
62/79 (78.48%) 12/79 (15.19%) 5/79 (6.43%)
Employment status (p value=0 .009
Student# n=7 3/7 (42.86%) 0/7 (0%) 4/7 (57.14%)
Unemployed n=89 67/89 (75.28%) 14/89 (15.73%) 8/89 (8.99%)
Employed n=28 16/28 (57.14%) 5/28 (17.86%) 7/28 (25.00%)
DiscussionIn this study, the prevalence of breastfeeding was relatively high. The breastfeeding initiation rate of 85.61% was slightly higher than the
55

national rate (82% in 2003). Furthermore, a large majority of the participants in this study (84.68%) reported that they were still breastfeeding at six weeks, and 69.36% of them were EBF – this is exponentially higher than rates reported nationally. The fact that the participants were very knowledgeable on the benefits of breastfeeding, may have informed their intent to breastfeed, and hence, the high rate of breastfeeding at 6 weeks. The knowledge that breast milk supplied sufficient nutrition for baby in the first 6 months of life was the single most positive predictor of breastfeeding in the knowledge questionnaire. This is because if a mother perceives her breast milk as enough, she will be more motivated to offer her baby only breast milk. The maternal comfort with breastfeeding in the presence of others, another factor that was positively linked with maternal intent to breastfeed in other studies, was also examined in this study. Even though the majority of the participants were comfortable with the way in which they held their babies during feeding, only mothers that were comfortable with breastfeeding in the presence of family members were likely to be breastfeeding at 6 weeks - p value = 0.015. This is evidence that women who receive positive support from family members are more likely to breastfeed, and thus make better infant feeding choices. A disappointing finding was that fewer participants (55%) were comfortable with breastfeeding in public. This may be a reflection of a societal culture that frowns upon women breastfeeding in public spaces; and this has been shown to have a negative impact on continued breastfeeding. Changing such public perceptions and attitudes about breastfeeding could succeed in encouraging appropriate maternal breastfeeding practices. Therefore, it would be important to direct strategies on promotion, protection and support of breastfeeding towards educating family members as well as communities at large on the need to exclusively breastfeed for up to 6 months. A majority of participants received antenatal education on infant feeding practices in the form of group counselling sessions. A concern is that this does not provide an opportunity for individual assessment of appropriate
56
infant feeding choices. A great example is that this would not be an appropriate platform to assess the affordability, feasibility, accessibility, sustainability and safety of chosen continued exclusive replacement feeding - particularly for HIV infected mothers who do not have the option to breastfeed when formula is no longer available. These mothers require continued individualized counselling on and support of the recommended BF practices during the antenatal and as well postnatal periods, and such sessions should involve family members.The fact that a large majority of these women selected the health care professional as their most influential source of information, is an indicator that the role played by maternity care practitioners is an important one, and ongoing health care provider education and training on skills to promote EBF may go a long way in improving breastfeeding rates.
LimitationsDue to the stipulated exclusion criteria, this study did not take into consideration the impact of severe foetal and maternal morbidity on infant feeding practices. Also, because of our age cut off of 18 years, are not able to make any inferences on infant feeding practices of adolescent mothers.
StrengthsAll data was collected and captured by a single researcher, which maintained quality of data. Also, there was a small loss to follow up.
57
INCREASED EXCLUSIVE BREASTFEEDING IN SOUTH AFRICA FROM 2010 TO 2013: IMPACT OF NATIONAL POLICY CHANGE?
Debra Jackson, UNICEF & University of the Western Cape; Sonja Swanevelder, South African Medical Research Council; Carl Lombard, South African Medical Research Counci & University of Cape Town, Tanya Doherty, South African Medical Research Council & University of the Western Cape; and Ameena Goga, South African Medical Research Council & University of Pretoria
Background: South Africa is reported to have one of the lowest Exclusive Breastfeeding (EBF) rates in Africa. National and regional studies between 1998 and 2009 reported EBF rates in infants age 0-3 months from 4% to 25.7% (Table 1). Although questions, settings and methods varied across studies, it is clear that the EBF rate in South Africa has remained consistently low since the late 1990s. Reasons for these low EBF rates have been examined across various settings. The South African HIV epidemic has no doubt been a contributing factor in mothers’ infant feeding decisions, however, low EBF rates pre-date the increased focus on HIV after 2000. Use of commercial infant formula by health services to treat malnutrition and for HIV-positive mothers, has been cited as providing mixed messages to communities about exclusive breastfeeding. Cultural norms for early mixed feeding, urbanization, and mothers returning to work have all been cited. Despite national policies supporting breastfeeding, front line health care personnel, programme managers or policy makers had not consistently supported EBF messaging prior to 2011.
58
Table 1: South African EBF Rates 1998-2009% EBF
StudyTime Period Location
Recall Period
1998 2003
2007
2008
2009
HSRC 0-6 months National Unknown 25.7
DHS0-6 months National 24 hour 7 8.3 0-3 months National 24 hour 10.4 11.2*
Good Start 1 7 weeks KZN, EC, WC 24 hour
HIV+: 18 HIV-: 11
PROMISE-EBF
3 months KZN; WC 24 hour 6 7 day 4
CJ Crooks Hospital 3 months
KZN - Durban Unknown
All: 18 HIV+: 11
Good Start 2 3 months
KZN - Durban 24 hour 14.9
Footnote: HIV+ = HIV positive; HIV- = HIV negative; HSRC=Human Sciences Research Council; DHS = Demographic Health Survey KZN = Kwa Zulu Natal province EC = Eastern Cape province WC = Western Cape province *Data for infants <2 months
In 2011, the National Minister of Health held a consultation on breastfeeding, which lead to a clear shift in national policy to promote ‘exclusive’ breastfeeding in South Africa, through the release of the Tshwane Declaration of Support for Breastfeeding (Tshwane Declaration). By September 2012 free formula milk for HIV-positive mothers was withdrawn from the Prevention of Mother-to-Child Transmission (PMTCT) programme and EBF messaging for front line workers was emphasized as a policy priority. This analysis uses data from the three South Africa National PMTCT Evaluation surveys to examine early EBF rates at six weeks postpartum, in 2010 prior to the Tshwane Declaration, in 2011-12 during the policy transition period, and 2012-13 after complete implementation of the Tshwane Declaration.
Methods: Data from the three national, cross-sectional, facility-based surveys, conducted in 2010, 2011-12 and 2012-13, were analysed. Stratified multi-stage probability sampling proportional to size, followed by random sampling of facilities and consecutive or systematic sampling of participants (caregivers with infants aged 4-8 weeks receiving their 1st
DTP immunization) was conducted.
59
The desired sample size was 12,200 infants to produce national and provincial estimates. Interviews gathered data on maternal socio-demographics, ante- and postnatal care and PMTCT services. Infant feeding was determined using a structured recall of 24 hours and 7 days. Exclusive breastfeeding was defined according to WHO definitions. Data were weighted for sample realisation and population live births.
Text Box 1: WHO Infant Feeding Definitions
Results: 10,182, 10,106 and 9, 120 caregiver-infant pairs were enrolled in 2010, 2011-12, and 2012-13, respectively. National EBF rates at 4-8 weeks of age were 22.9% (95%CI 21.5-24.3) in 2010, 35.7% (95%CI 33.9-37.6) in 2011, and 59.1% (95%CI 57.4-60.7) in 2012, p=<0.001. All nine provinces showed similar statistically significant trends. (Table 2)Logistic regression analysis examined the following factors associated with EBF: maternal - age, education, marital status, parity, employment and HIV status; household - type, water source, fuel for cooking, and toilet; food insecurity; planned pregnancy, antenatal care - initiation (trimester) and attendance (4+); delivery method; child - gender and age in weeks; and receipt of breastfeeding counselling. Many of these variables were predictors for EBF (Table 3). In general mothers with higher socioeconomic status, employed mothers, mothers who are HIV-positive, had a caesarean delivery, reside in Eastern Cape or Limpopo province and who did not receive breastfeeding counselling were significantly less likely to EBF. Older infants (8 weeks of age) were also less likely to be practising EBF.The crude OR comparing 2011 and 2012 to 2010 was 1.88 (95%CI 1.70 – 2.07) and 4.87 (95% CI 4.40 – 5.38), respectively. In univariable analysis with all potential co-factors and in final full logistic model (Table 3) these
60
"Exclusive Breastfeeding" is defined as giving the infant no other food or drink, not even water, except breast milk (including milk expressed or from a wet nurse) for 6 months of life, but allows the infant to receive ORS, drops and syrups (vitamins, minerals and medicines).“Exclusive Formula Feeding” is defined as giving the infant commercial formula without any breastmilk or solids.“Mixed Breastfeeding” is defined as giving the infant breastmilk and other fluids or solids.
estimates did not change by more than 10% suggesting that these increases were seen across all regions and population sub-groups.
61
Discussion & Conclusion: With what seemed to be an intransigently low EBF rate since 1998, South Africa saw a remarkable increase in early EBF (4-8 weeks, mean = six weeks postpartum) from 2010 to 2013 coinciding with major national infant feeding policy change. These increases were seen across all provinces, suggesting a population-wide effect, not just an increase in certain subgroups/locations. Similar increases have been recorded in KZN (ISHMRL 2016) studies, but the SA HANES data do not suggest an increase 2003 (DHS) 11.2% versus SA HANES 2012 12.7% in infants <2 months of age. Possible difference is how questions were asked: 24 hour feeding recall in this study versus no specified time period (mix of ‘from birth’ and ‘current’ questions) for SA HANES.While these increases in EBF were significant and a huge step towards changing the tide of poor infant feeding in South Africa, the 59.1% prevalence is still below desired levels of early EBF and much remains to be done to further improve infant feeding practices. The results of this study suggest several predictors of EBF which could guide future programmatic interventions to further improve EBF rates.
62
Table 2: South African and Provincial EBF Rates at Six (4-8) Weeks Postpartum* 2010 2011 2012 % [95% CI] % [95% CI] % [95% CI]Eastern Cape 15.5 24.8 53.8 [12.0,19.8] [21.0,29.1] [49.0,58.5]Free State 16.1 33.3 53.3 [14.1,18.2] [30.5,36.3] [48.7,57.9]Gauteng 23.2 36.4 65 [20.2,26.5] [31.6,41.6] [61.2,68.6]KwaZulu Natal 33.7 46.6 60.4 [30.2,37.4] [43.0,50.2] [55.9,64.6]Limpopo 19.5 21.3 47.9 [16.1,23.4] [18.0,24.9] [43.0,52.8]Mpumalanga 15.9 47.3 65 [13.1,19.2] [41.2,53.5] [61.7,68.2]Northern Cape 22.1 30.9 61.7 [18.8,25.8] [26.6,35.4] [57.4,65.9]Northwest 24.3 30.4 65.4 [20.7,28.2] [26.8,34.2] [60.6,69.8]Western Cape 17.9 36 54.9 [15.3,20.8] [31.2,41.1] [49.8,59.8]South Africa* 22.9 35.7 59.1 [21.5,24.3] [33.9,37.6] [57.4,60.7]
* Trends for year, adjusting for province significant, p<0.0001
Table 3: Full Adjusted Model for Predictors of EBF at 4-8 Weeks postpartum, 2010-2013.Variable Adjusted Odds
Ratio95% Conf. Interval
Year (Ref: 2010)2011 1.98 1.79 2.182012 5.30 4.78 5.88Province (Ref: EC)FS 1.21 0.98 1.48GP 1.69 1.37 2.08KZN 2.15 1.75 2.63LP 0.96 0.76 1.21MP 1.62 1.30 2.02NC 1.34 1.08 1.67NW 1.49 1.20 1.84WC 1.30 1.03 1.64Mother Age (Ref: <20)20-34y 1.08 0.99 1.1635-50y 1.12 1.01 1.25Mother Education (Ref: No education)Grade 1-7 1.00 0.83 1.21
63

Grade 8-12 0.86 0.72 1.03Tertiary 0.62 0.50 0.77Parity (Ref: Primipara)Multipara 1.16 1.09 1.23Mother Employment (Ref: Employed)Other Income 1.53 1.42 1.65No Income 1.54 1.02 2.31HIV Status (Ref: Negative)Positive 0.66 0.61 0.71Don't Know 0.74 0.56 0.99House Type (Ref: Brick)Informal/Wood 1.09 1.00 1.19Traditional/Mud 1.20 1.01 1.42Water Source (Ref: piped in house/yard)Not piped in house/yard
0.84 0.75 0.93
Toilet (Ref: Indoor Flush)Pit Latrine 1.19 1.07 1.32Portable 0.89 0.59 1.34Other 1.51 0.77 2.96None 1.03 0.82 1.29Fuel for cooking (Ref: Electricity)Wood/Coal 0.84 0.73 0.97Other 0.96 0.57 1.62Food Insecurity (Ref: Yes)No 1.14 1.04 1.24Don't Know 1.65 1.21 2.26Planned Pregnancy (Ref: Yes)No 0.93 0.88 0.99Delivery Method (Ref: Vaginal)Cesarean 0.84 0.78 0.90Infant Age Weeks (Ref: 4 weeks)5 weeks 0.82 0.66 1.026 weeks 0.91 0.75 1.127 weeks 0.86 0.70 1.048 weeks 0.68 0.54 0.86Breastfeeding counseling (Ref: Yes)No 0.57 0.51 0.63
64
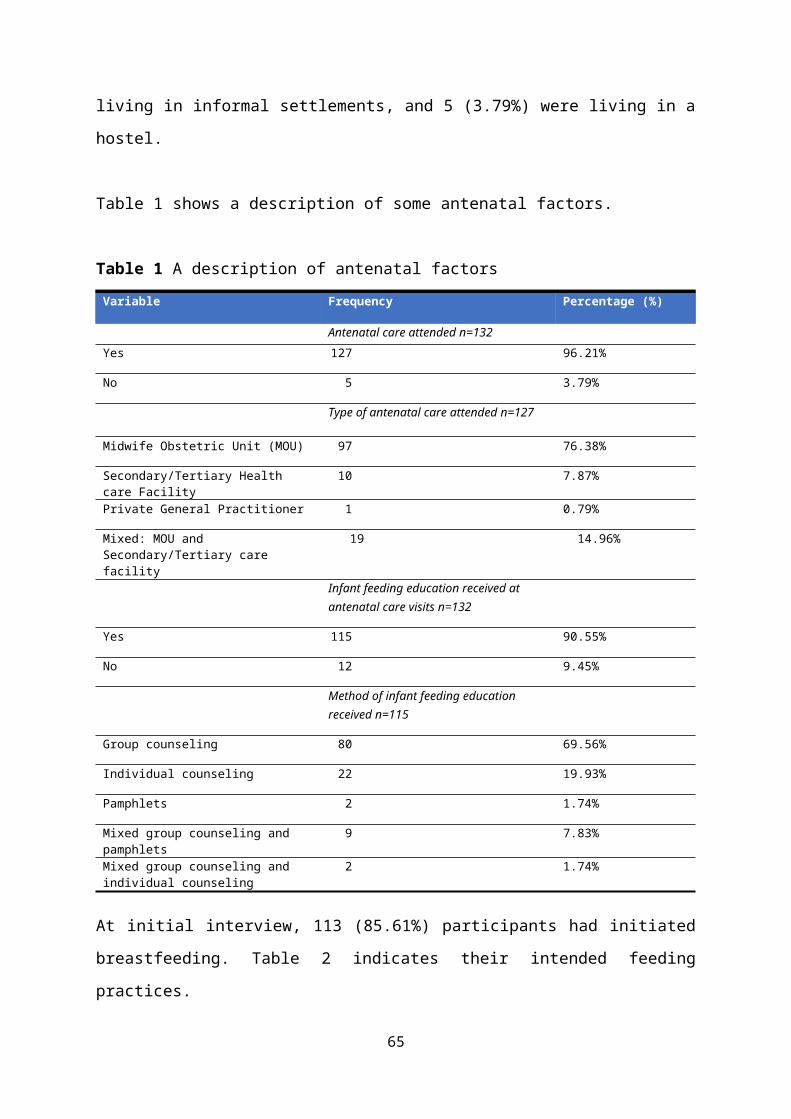
CLINICAL FEATURES, LABORATORY FINDINGS AND OUTCOMES OF INFANTS WITH HYPERBILIRUBINAEMIA REQUIRING EXCHANGE BLOOD TRANSFUSION AT CHRIS HANI BARAGWANATH HOSPITAL
Karabo Seake, Sithembiso VelaphiDepartment of Paediatrics, Chris Hani Baragwanath Academic HospitalFaculty of Health Sciences, University of the Witwatersrand.
BACKGROUNDNeonatal jaundice due to unconjugated hyperbilirubinaemia is the commonest clinical condition that clinician working with neonates encounter on a daily basis. It has become the leading cause of neonatal readmissions. And if severe, reaching levels requiring an exchange blood transfusion, it is associated with serious morbidity and mortality if left untreated or if treatment is delayed. Unconjugated hyperbilirubinaemia is known to be a neurotoxin that can lead to significant neuronal damage. It can present acutely with acute bilirubin encephalopathy (ABE) and on the other side of the spectrum with athetoid cerebral palsy, often called kernicterus and/or sensorineural hearing loss. Factors associated with the development of unconjugated hyperbilirubinaemia, include, early neonatal discharge, blood group incompatibilities, infection and cephalohaematoma. Early discharge has become a common phenomenon globally, with the escalation seen in 1990’s and contributing to up to 50% of readmissions [2]. Haemolytic disease secondary to ABO and Rh incompatibility is another major risk factor. In one study ABO incompatibility contributed to 41.7% of cases with severe jaundice and accounted for 44% of exchange blood transfusions performed.
The need for exchange blood transfusions related to Rh-incompatibility has decreased significantly globally due to development of anti-D immunoglobulins, intensive phototherapy and the use of guidelines for monitoring and managing neonatal jaundice. Exchange blood transfusion is not a benign procedure as it can be associated with apnoeas, necrotizing enterocolitis, hypotension, seizures, cardiac arrest and death. In this study we sought to describe features and short term outcomes of neonates with severe hyperbilirubinaemia requiring exchange blood transfusion (EBT).
65
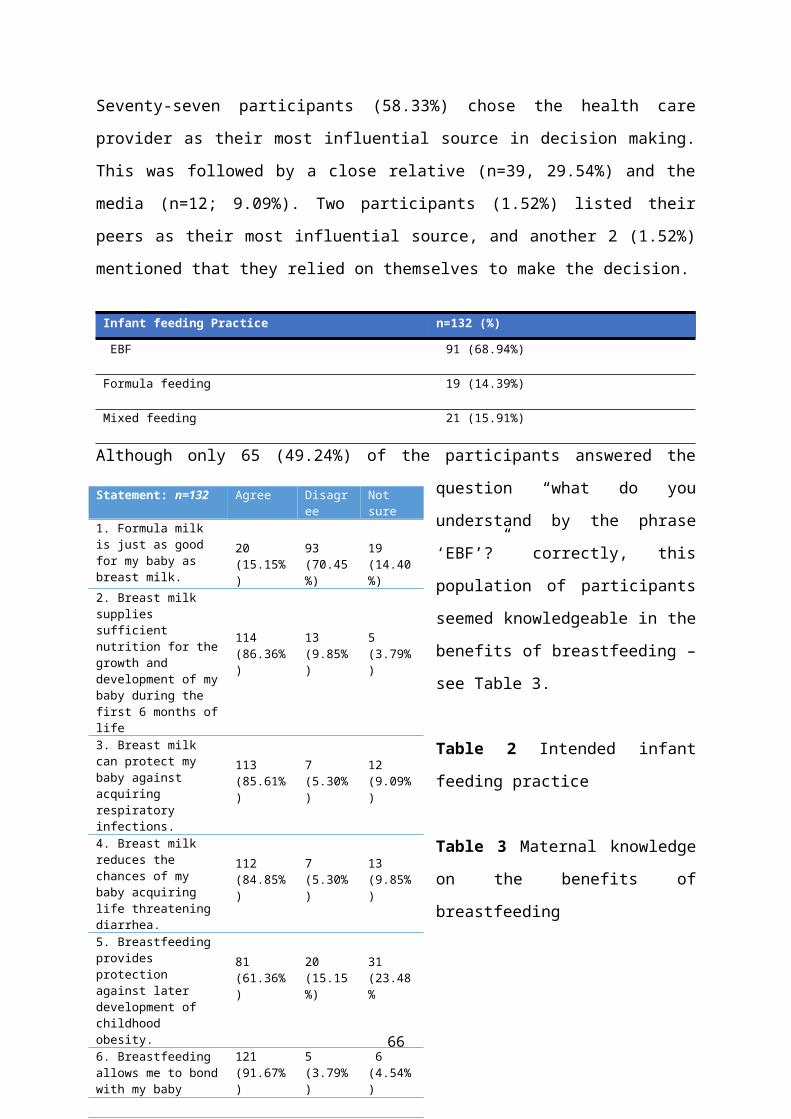
66
STUDY DESIGN AND METHODS This was a retrospective descriptive study conducted at Chris Hani Baragwanath Academic Hospital (CHBAH). It included all neonates with postnatal age <29 days admitted in both the neonatal and paediatrics wards from January 2009 to December 2013 with hyperbilirubinaemia and received exchange blood transfusion. The clinical records were retrieved and relevant data captured. Data was entered into an Excel spreadsheet, and transferred to statistical software, STATISTICA version 12.0 for analysis.
RESULTS A total of 150 patients had EBT performed over the five-year period, from January 2009 to December 2013, an average of 30 EBTs per year. A total of 101 patients’ files were available for review. Majority of these (n=67; 66.3%) were readmissions), with the rest developing jaundice before discharge post-delivery. Maternal and infant characteristics The average maternal age was 26.7 ± 6.8 years, 92.1% delivered at healthcare facilities with 86.1% delivering vaginally and 65.4% weighing >2500g and 49.5% born at gestational age ≥37 weeks. The average birthweight was 2701 ± 614 grams. Neonates who developed severe jaundice while in hospital were more likely to be born in hospital (88.2% vs 25.3%, p<0.001), born by caesarean section (26.5% vs 7.5%, 0.009) and of lower birth weight (2522±850 vs 2792±429, 0.001) than those who were readmitted.
Maternal and infant blood groupAmong 86 mothers with known Rh blood group, 9 (10.5%) were Rh negative and 8 of their infants were Rh positive, thus 9.3% mother - infant pair had Rh incompatibility. Five of the 8 infants with Rh incompatibility were Coombs positive (62.5%) (Table 1). Among the 23 mother – infant pairs who were both Rh positive, 9 (39%) were Coombs positive, and of these 9, 2 were ABO incompatible, suggesting that there are other 7 that were due to incompatibility from minor blood groups or another unknown diagnosis.
67
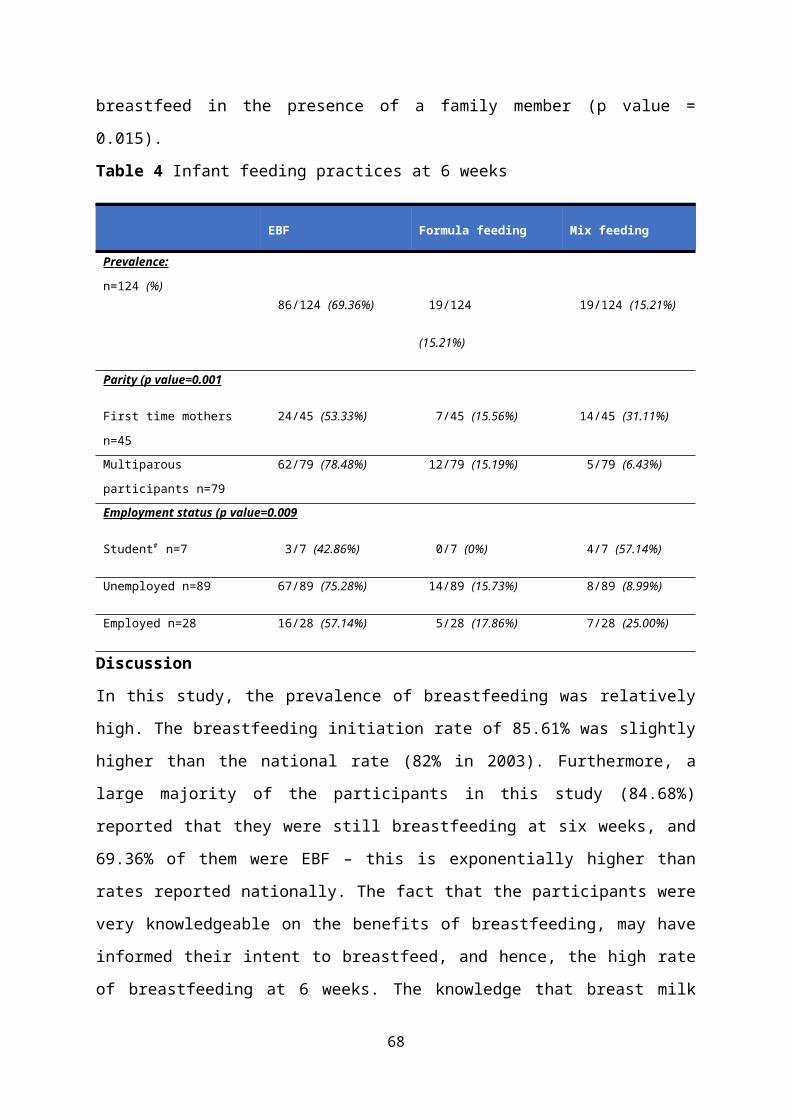
68
The ABO blood groups of mothers and infants requiring EBTMaternal ABO blood groups against infant’s ABO blood groups and possible incompatibilities are shown in Table 2. The common ABO incompatible groups were mother O/infant B (30/57; 53%), mother O/ infant A (17/57; 30%) and mother B/infant A (4/57; 7%). Eighteen of the 57 (32%) infants who had ABO incompatible were Coomb positive, with 37% of the mother O/ infant B and 23% of mother O/ infant A having positive Coombs.
Table 1: Rhesus blood group of mothers and infants receiving exchange blood transfusion
Mothers TotalRh positive Rh
negativeRh unknown
Infa
nt
Rh positive 23(9, 39%)*
8(5,
62.5%)*
5 36
Rh negative 0 1 0 1Rh not recorded
54 0 10 64
Total 77 9 15 101 * = Positive coombs
Table 2. ABO blood groups of mothers and infants who received exchange blood transfusion
Maternal ABO Blood Groups A B O AB Total
Infa
nt’s
ABO
Bl
ood
Gro
up
A 7 4 $ (3, 75%)*
17 $ (4, 23%)*
1 21 $ / 29(7/21, 33%) *
B 1 $ 4(2, 50%)
30 $ (11, 37%)*
0 31 $ /35(11/31, 32%)*
O 3 4(1, 25%)*
5 0 0/12
AB 1 $ 2 $ 2 $ 0 5 $ /5
Total
12 (15%
)
14(17%)
54(67%)
1(1%)
57 $ /81 (70%)(18/57, 32%)*
$ - Number of patients with ABO incompatibility between mother and infant *- the number in parenthesis is a number and percent of patients with positive Coombs
Mortality rate among the patients who received exchange blood transfusion
69
A total of 6 patients died, a mortality rate of 6%. All deaths weighed >2000g and were outpatients (Table 6). Three had acute bilirubin encephalopathy on admission before exchange blood transfusion, two died from sepsis post exchange transfusion and one died from congenital cardiomyopathy. None died during the performance of the procedure. Three had ABO incompatibility.
DISCUSSIONNeonatal jaundice in its severe form can be fatal and among survivors it can be associated with severe morbidity. Screening and monitoring those at risk, implementation of effective treatment modalities has significantly reduced the morbidity and mortality associated with hyperbilirubinaemia[8]. Early discharge makes close monitoring difficult, thus the recommended guidelines, are that if early discharge cannot be avoided, infants should be assessed 48-72 hours post discharge by a professional. The main findings in this study are that two thirds of patients with hyperbilirubinaemia requiring exchange blood transfusions were outpatient, suggesting possible role of early discharge. There was a high number of patients with ABO incompatibility, at 70%, compared to a number of 15.7% previously reported in literature 15.7%. A mortality rate of 6% within the week of the exchange blood transfusion, was also higher than that of 4% and 17.5% reported in other studies[10, 11]. Based on the findings from this study we would like to recommend that pregnant women should have ABO blood group typing at antenatal clinic in addition to Rh. Where possible discharge of well and/ or at low risk neonates should not be allowed earlier than 24 hours of life. All neonates should be screened for hyperbilirubinaemia using transcutaneous bilirubinometer before discharge from any healthcare facility. Neonates with severe hyperbilirubinaemia requiring exchange blood transfusion should be followed up and have neurodevelopmental assessment at regular intervals for at least the first two years of life.
70

EFFICACY AND SAFETY OF ANTEPARTUM ANTIRETROVIRAL STRATEGIES TO PREVENT PERINATAL HIV TRANSMISSION – THE IMPAACT PROMISE TRIAL (1077)
Protocol Chair and Vice Chairs: MG Fowler, J McIntyre, T Chipato, P Flynn, J.Currier
PROMISE Site Principal Investigators:India: BJMC, Pune: R Bhosale, P Sambarey. Malawi: Blantyre: B Makanani, M Mallewa, T Taha UNC-Lilongwe: F Martinson. South Africa: CAPRISA Umlazi, Durban: D Moodley Durban Paeds, Durban: R Bobat, S Pillay. FAM-CRU, Stellenbosch: G Theron. PHRU, Soweto: A Violari. Shandukani, Johannesburg, L Fairlie, A Coovadia. Tanzania: KCMC, Moshi: P Mlay. Uganda: MUJHU, Kampala: M Owor. Zambia: George Clinic, Lusaka: M Mbewe, B.Chi. Zimbabwe: St. Mary’s, Seke North, and Parirenyatwa: T Chipato.
Sponsors:US National Institutes of Health. The study products were provided free of charge by Abbott, Gilead Sciences, Boehringer Ingelheim, and GlaxoSmithKline.
Introduction: There are limited trial data comparing triple antiretroviral drug regimens to antenatal zidovudine and intrapartum nevirapine for preventing perinatal HIV transmission among asymptomatic women with high CD4 cell counts. The study was conducted to maximize prevention of mother-to-child HIV transmission (PMTCT) and optimize maternal/child health and survival. In addition, the relative safety and efficacy of triple ARVs compared to other proven regimens among healthy HIV women with higher CD4 counts was assess. The PROMISE study was done in the context of standard of care for adult HIV treatment and infant feeding. Sites included breastfeeding and formula feeding settings.
Methods: IMPAACT-PROMISE P1077BF/1077FF is an open-label, randomized trial to assess efficacy and safety of different antepartum, intrapartum and postpartum antiretroviral strategies for preventing perinatal HIV transmission. PROMISE is a complex protocol with three randomizations: The antepartum component during pregnancy, the post-partum component during breastfeeding and the Maternal Health component following breastfeeding. The study’s antepartum component compared zidovudine/lamivudine/ lopinavir-ritonavir, tenofovir/emtricitabine/lopinavir-ritonavir and antepartum zidovudine/ single-
71
dose nevirapine plus 6-14 days of postpartum emtricitabine/tenofovir. Outcomes included perinatal HIV transmission through 14 days post-delivery based on two positive infant HIV nucleic acid tests, pregnancy outcomes and maternal/infant safety events. Patients will be follow-up until 96 weeks following recruitment of the last antenatal patient.
Results: The study was conducted at 14 sites in 7 countries. Recruitment commenced midyear in 2010. On 4 November 2014 an interim review by DSMB reported pre-specified efficacy boundary for Antepartum Component was crossed and there were also safety differences between study arms. The recruitment of patients was stopped.
A total of 3,490 primarily African HIV-infected pregnant women were enrolled at >14 weeks gestation, median screening CD4 count was 530 cells/mm3, median enrollment gestational age was 26 weeks, 97% were WHO clinical stage I. The antepartum component of PROMISE was carried out under two versions of maternal randomization. In Version 2, given limited safety date on tenofovir during pregnancy, only hepatitis B positive women could be randomized to the 3rd arm (Arm C: FTC-TDF + LPV-RTV). In Version 2 96% of women who were HBV negative were randomized only to 2 arms: arm A with ZDV alone or arm B with ZDV/3TC + L/R. With more safety information on use of tenofovir during pregnancy available, in Version 3 tenofovir all women were randomized to 3 arms irrespective of their hepatitis B status. Thus most women in Arm C (FTC-TDF + LPV/RTV) were included under Version 3.
Perinatal HIV transmission was significantly lower with triple-antiretroviral drugs: 0.56% for combined triple-antiretroviral drug arms versus 1.8% for zidovudine/nevirapine (difference -1.28%, 95% CI -2.11% to -0.44%). However adverse maternal grade 2-4 events were significantly higher for zidovudine/lamivudine/lopinavir-ritonavir regimens compared to zidovudine/nevirapine: 21.1% versus 17.3%, respectively, p=0.008. There were no maternal deaths. Adverse pregnancy outcomes were significantly higher for zidovudine/lamivudine/lopinavir-ritonavir versus zidovudine/single-dose
72

nevirapine including birth weight<2500 grams (23.0% versus 12.0%, p<0.001); preterm delivery<37 weeks (20.5% versus 13.1%, p<0.001). Under version 3, we there was a significantly increased risk of moderate adverse pregnancy outcomes including low birth weight and preterm delivery for Triple ARVs compared to ZDV alone. Regarding more severe pregnancy outcomes we found that ZDV-3TC + L/R has a significantly lower risk of severe prenancy outcomes compared to TNF FTC + L/R including very preterm delivery at <34 weeks. Risk of early infant death was lower with zidovudine/lamivudine/lopinavir-ritonavir than tenofovir/ emtricitabine/lopinavir-ritonavir (0.6% versus 4.4%, p<0.001).
Conclusions: Antenatal triple-drug regimens resulted in significantly lower perinatal HIV transmission than zidovudine and single-dose nevirapine, supporting WHO 2013 recommendations, but higher risk of adverse maternal and pregnancy outcomes. The difference in risk of early infant deaths in the FTC-TDF triple ARV arm compared to the 3TC-ZDV triple ARV arm was unanticipated and requires further investigation.
73
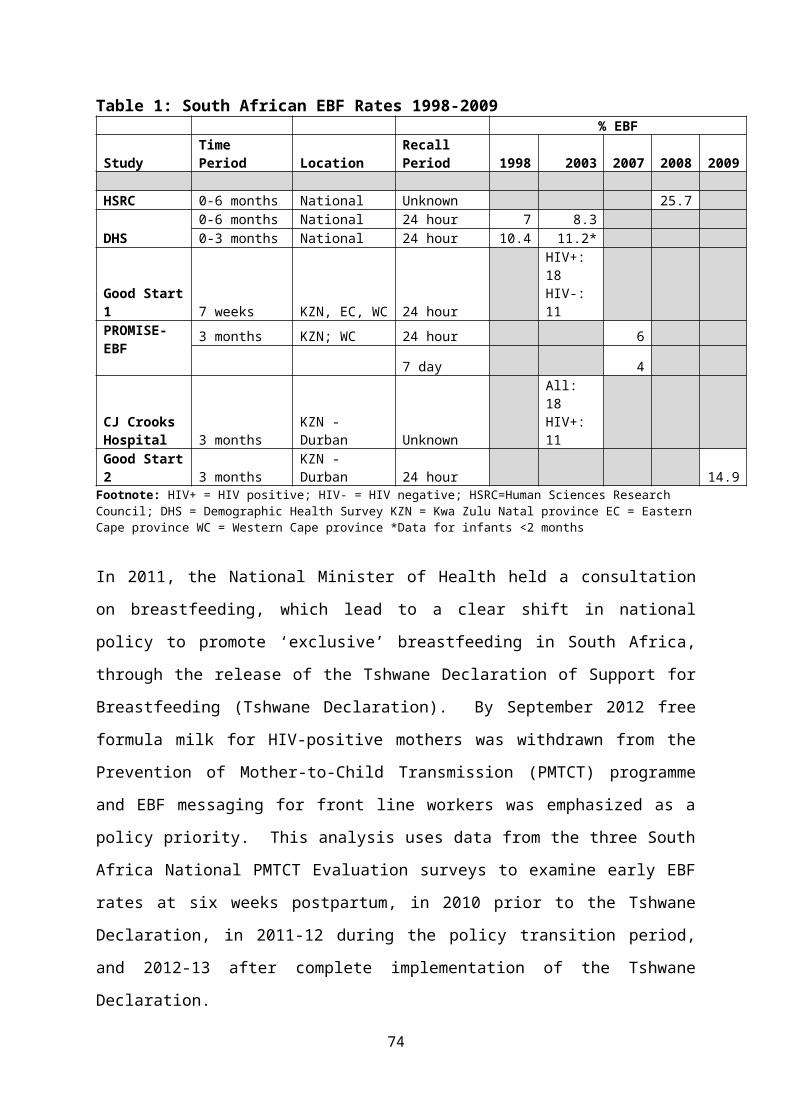
‘SELF-INDUCED LATE ABORTION AS A CONTRIBUTOR TO PRETERM BIRTH AND PERINATAL MORBIDITY AND MORTALITY’
Dr SD Mandondo BSC (Unitra) MBchB ( UCT) FCOG CMSA DCST O&G Amathole ECGJ Hofmeyr
The study of self-induced late abortion as a contributor to pre-term birth and perinatal morbidity and mortality was a retrospective observation study conducted at Frere, a tertiary hospital and Cecilia Makiwane a regional Hospital, both of which are public sector facilities. Between the two there was a total of 11 860 deliveries with 530 (4.46%) deliveries weighing between 500–1 499grams, LBWR 20% and perinatal care index 1,8. The top 5 primary obstetric causes of perinatal deaths in the VLBW babies were hypertension (33%) unexplained IUFD (19.7%), APH (19.7%), SPL (17.5%) and intra-partum asphyxia (9.2%).The study was conducted between 1 July 2011 and 1 January 2012. Eighteen (18) cases of self-medication with misoprostol after 24 weeks’ gestation, as volunteered by mother, were recorded. The dosages ranged from 400 to 1 200 with only 1 neonate surviving.
Research questionThe study sought to demonstrate that self-induced late abortion is a contributor to preterm birth and perinatal morbidity and mortality. Primary Objective: To determine whether self-induced late abortion or pregnancy termination contributes to perinatal morbidity and mortality rates at the East London Hospital complex Secondary Objective: To document clinical features of women who present with self-induced late abortion/pregnancy termination
BACKGROUNDSub-Saharan Africa has the lowest contraceptive use, the most unwanted pregnancies, the fewest safe abortions, and the highest resulting mortality from abortion. For South Africa therefore, reaching the Sustainable Development Goal 3—will be impossible without successfully addressing unsafe abortions. The focus on abortion should be urgent, immediate, and multidimensional. [The Alan Guttmacher Institute report entitled “Abortion worldwide—a decade of uneven progress”, 2009]
SOUTH AFRICAN CONTEXT
74
The legal abortion rate in South Africa is very low (6 per 1 000 women). Many abortions are performed outside the legal sector, despite liberalisation of the abortion law in 1997 [Sedgh et al, Incidents and Trends]. The estimated rate of unsafe (primarily illegal) abortions for the Southern Africa region is nearly three times this legal abortion rate, and South Africa makes up 90% of the region’s population.Most of the studies found in the literature, discuss misoprostol self-medication before 22 weeks and hence the perinatal outcomes are not discussed as these are treated as abortions. A study by Jewkes et al in Gauteng, interviewed a sample of forty-six women attending hospital with incomplete abortion who had abortions induced outside of designated facilities.
Testing to confirm ingestion of MisoptostolIn America according to Fyrie L, et al (2014), efforts to prosecute women for self-induced abortions resulted in patients being acquitted in the USA, as misoprostol could not be found in the bloodstream. This is due to the fact that misoprostol is rapidly metabolized into misoprostol acid (MPA) which can be detected using an assay, however it has a half-life of 20-40 min. There are three validated techniques for detecting misoprostol acid in blood, each with a different lower limit of detection. To analyse blood, a gas-chromatography mass-spectrometry machine or alternatively a liquid-chromatography mass-spectrometry machine is required. Radioimmunoassay has the potential to detect other metabolites, thus it is subject to non-specificity. The effect after taking misoprostol is felt long after ingestion as it stimulates the body to produce its own prostaglandins
History behind the Choice of Termination of Pregnancy Act (CTOP)The findings of a national study of the epidemiology of incomplete abortion which was undertaken in 1994 provided a description of the magnitude of the problem of unsafe abortions. In this study by Rees et al, an estimated 44 686 (95% CI 35 633-53 709) women per year were admitted to South Africa's public hospitals with incomplete abortions. An estimated 425 (95% CI 78-735) women died in public hospitals from complications of abortion. Fifteen per cent (95% CI 13-18) of the patients had severe morbidity while a further 19% (95% CI 16-22) had moderate morbidity.Women under 21 years of age are most vulnerable. This was the study that resulted in Government legalising terminations of pregnancy through the Choice of Termination of Pregnancy Act 92 of 1996. After abortion became legal and available on request in
75
1997, abortion-related infections decreased by 52%, and the abortion mortality ratio from 1998 to 2001 dropped by 91% from its 1994 level. [Jewkes et al, 2002]The mortality index (MI) defined as the total number of patients who died due to abortion divided by the total number of critically ill women remains unchanged showing Mbhele and Pattison et al 2006.
The ActThe Choice of Termination of Pregnancy Act of 1996 (Act 92 of 1996) was designed to determine the circumstances in which and conditions under which the pregnancy of a woman may be terminated; and to provide for matters connected therewith.
Approved Abortion SitesAmended sections of the Choice Act – 2008Section 3 (1) – a) to k) spells out specifically what types of facilities are legalised to perform abortions as well as the required equipment and linkages to hospital facilities for support if needed.The amended Act also imposes a possible imprisonment penalty where the abortion was performed at a non-recognised facility or where prescribed record keeping is not done.
Implications for medical practitioners‘‘(1) Any person who— (a) is not a medical practitioner, or a registered midwife or registered nurse who has completed the prescribed training course, and who performs the termination of a pregnancy referred to in section 2(1)(a); (c) Prevents the lawful termination of a pregnancy or obstructs access to a facility for the termination of a pregnancy; shall be guilty of an offence and liable on conviction to a fine or to imprisonment for a period not exceeding 10 years.’’
Advertising Standards Authority of South Africa (ASA).“Advertising is a service to the public and as such, should be informative, factual, honest, decent and its content should not violate any of the laws of the country” (Preface, Para 11)
76
Appendix A of the ASA, concerning medicinal related products and advertisements containing health claims, states in par 1.2 that, “Advertisements shall not make claims concerning safety of a product or exaggerated claims of safety.” Illegal abortionists violate the Advertising Standards by making claims of affordability, safety and legality. Wording such as, “legal or legalized abortion” on the advertisements is expressly used to deceive a pregnant woman into believing that the advertised abortion conforms to legal requirements. The wording, “affordable or cheap” creates the impression that abortions are otherwise expensive and likely unaffordable. “...These words will appeal to uninformed and financially challenged women...”
77
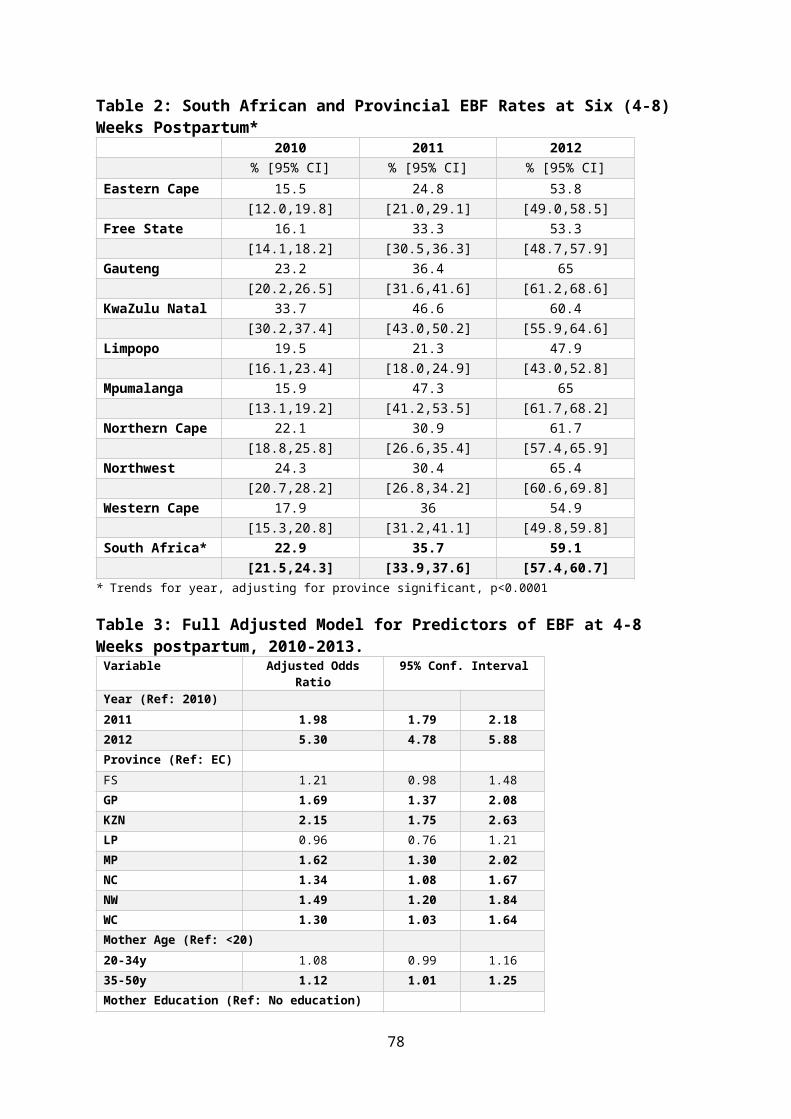
Why Women Still Abort Outside Legal System in SAGirls and women are being lured into illegal, backstreet abortions because of ignorance. Nearly two-thirds of the women (n 38) had self-induced obtaining misoprostol from vendors but a disturbing 23% (n 10) were given misoprostol by a doctor, nurse, or pharmacist. A minority of these women (n 11) indicated that they did this because they experienced barriers to legal service use. Fifteen percent (15%) knew of their legal rights, but did not know of a legal facility. Others did know where to access legal services but feared rude staff (17%) or breaches of confidentiality (6.5%). Others (6.5%) had been unable to get a legal abortion early enough in pregnancy to comply with the law.
Women’s Knowledge of the CTOP ActA study by Morroni et al, showed that 60 percent knew about the Act but this dropped to 40% in rural settings.
Impact of CTOP Act on staff at legalised facilitiesNurses' attitudes included that women should be at least 16 years of age to access these services; women should not be able to access repeated TOPs; nurses would prefer to administer pills rather than to use vacuum aspirations; nurses should work in TOP services by choice only. [Mokgethi N E, Ehlers et al. 2006] TOP personnel are victimised and socially stigmatised. Some professional nurses experienced guilt, depression, anxiety and religious conflicts as a result of participation.De Roubaix et al [2007] concluded that corrective measures including a goal directed educational programme and initiatives like value clarification workshops which have been effective in changing negative attitudes of participants, and may thus address stigmatisation, improve working conditions of TOP personnel, promote societal tolerance and acceptance, and informed consent.
Acceptability of the CTOP ActHarrison, et al note that support for the Act was low (11%) among both community members and nurses. The majority of nurses (56%) and community members (58%) supported abortion in the case of rape or incest, or if the continued pregnancy would endanger a woman's health (61% and 56%, respectively), but few supported abortion, for social or economic reasons.
Misoprostol Dosages and Safety
78
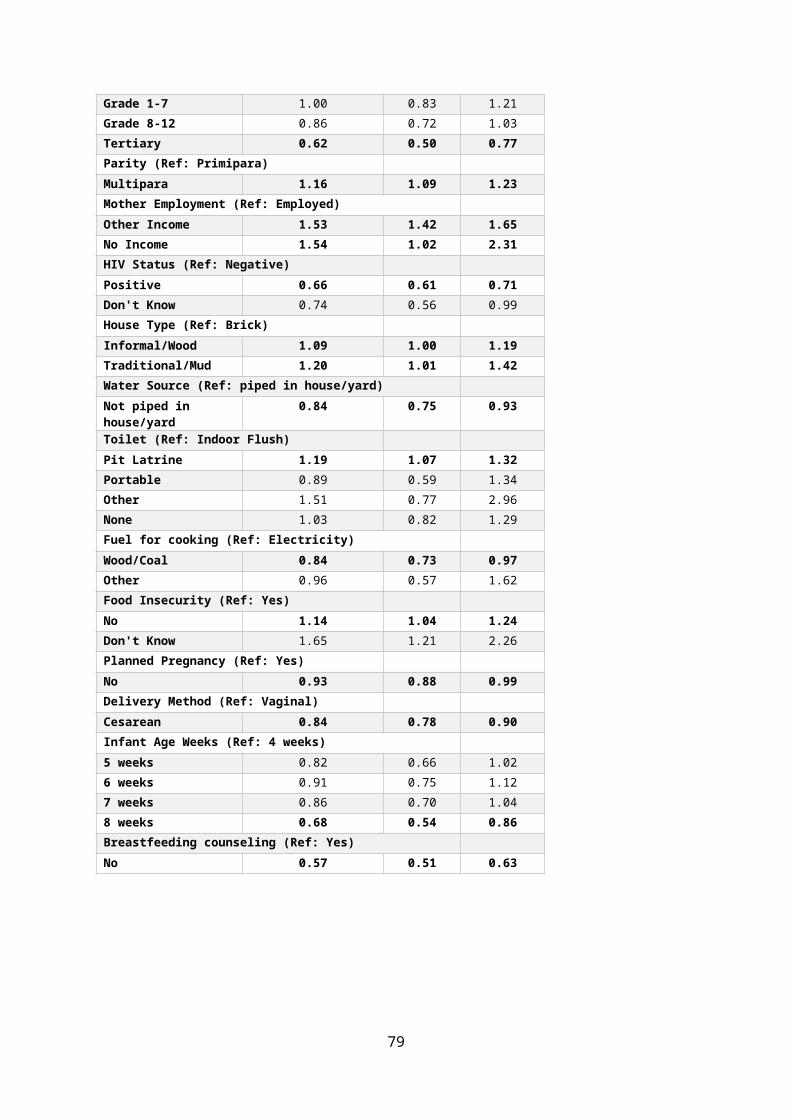
Medical abortion (MA) using Mifepristone and Misoprostol only is a safe, effective, and acceptable option for terminating pregnancies [RCOG 2004, WHO 3003a, Winikoff 2008, von Hertzen 2003, von Hertzen 2007]. At term recommended dose should not exceed 25 μg (1/8 of a tablet) 4-hourly.Caesarean section is associated with an almost 20-fold increase in risk of rupture. OR 20.8, 95% CI 14.1–104.00[). Limb deformities secondary to misoprostol use occur only in first trimester before 10 weeks. [Hofmeyer J]The relative risk of abortion related mortality was 14.7 at 13-15 weeks, 29.5 at 16-20 weeks and 76.6 after 21 weeks, Bartlett et al.Adebeyi et al, 2012 published a case series of thirty-one pregnant adolescents at less than 22 weeks with complications being anaemia, 25% severe sepsis.
METHODSProcedure, Data Management & Analysis Inclusion and Exclusion Criteria Inclusion: patients irrespective of age, who were admitted to Frere and CMH who volunteered misoprostol self-medication at gestational age of 24 weeks in an attempt to self-abort.Exclusion: Patients are not eligible for this study if: They do not meet the inclusion criteria Data collection On receiving a case report, Dr Mandondo personally completed the data collection from the case notes.
79
THE STUDY AND RESULTS
TABLE 1: GA at Self-Abortion, Misoprostol Dose & Reasons DESCRIPTION % N
1. ANC Booking: a) Booked 44.5% 8b) Un-booked (Casualty/GOPD) 50.0% 9c) Booked >300 km 5.5% 1
2. TOP Requested in Current Pregnancy and Declined, Reasons:
a) GA >20 weeks 17.0% 3b) 13-20 weeks, no beds so went over gestation for
TOP 5.5% 13. Gestational Age when Misoprostol taken:
a) 24 weeks 22% 4b) 25-27 weeks 11% 2c) 28-29 weeks 17% 3d) 30-34 weeks 22% 4e) 39 weeks 5.5% 1
4. Misoprostol Dosage ingested:a) 400 PO 11% 2b) 800 PO 55% 10c) 400 PV & 400 PO 11% 2d) 1200 PO 5.5% 1e) Unknown 17.5% 3
5. Source of Misoprostol:a) Phoned advert /Street Vendors 66% 11b) Advert said Dr… (Thought it was health
professional.)Given pamphlet in town
5.5% 1c) Family/friend 5.5% 1d) GP 5.5% 1e) Unknown 27.7% 4
6. Reasons for Self-Abortion:a) Family financial pressure 44% 8b) Schooling/exams 33% 6c) New job prospect 17% 3d) Lost husband 5.6% 1
Results Seventy-six per cent (13) of all births were under 1 500grams – this is very low birth weight, 2 were 1 500-1 999grams low birth weight and 1 was term . Eleven babies were born alive (69%), five stillborn (31%). Neonatal outcomes included 44% (8) early neonatal deaths 11% (2) late neonatal deaths, 22% (4) stillbirths and 5.5% (1) abortion.
80
Steroids had been given to the 2 of the eleven babies born alive and the rest presented in advanced labour or were diagnosed clinically as inevitable miscarriage subsequently delivering >500 gram babies than was clinically estimated. Four (36.3%) of the babies were on CPAP and 5 (45.5%) received surfactant. The major cause of death was immaturity (63.3%), hypoxia asphyxia and septicaemia (9%), HMD (45%), NEC (9%) pulmonary haemorrhage (9%) and intraventricular haemorrhage (9%). The gestational age at the time of taking misoprostol ranged from 24-39 weeks. Gestational age was 24 weeks (22%) in 4 patients, 25-27 weeks (11%) in 2 patients and 2 were unknown. Eight patients were past viability, 3 at 28-29 weeks (16.6%), 4 between 30-34 weeks (22%) and one patient 39 weeks (5.5%). The misoprostol dosages ingested ranged from 400 to 1200 micrograms with 55% taking 800 micrograms PO; 2 patients taking 400mcg PO; (11%) 2 taking 400mcg PO & PV; (11%) and 1 1200 (5.5%). Dosage was unspecified in 3 cases. Information regarding the source of misoprostol was mainly from 11 patients who received it through street adverts of illegal traders with phone numbers provided for contact and misoprostol delivered by unidentified person for payment of R800. The reasons given for self-abortion were mainly financial pressure in 44.4%, new job prospects in 17%, education/exams in 33% and losing husband (5.6%). The clinical presentation varied, 55% (10) presenting in spontaneous preterm labour, 2 BBA. Other presentations included PPROM, abruption with no HPT, APH, septic retained placenta, uterine rupture .one patient was still pregnant and failed to abort now presented for fear that baby may have congenital anomalies. Four patients (22%) had requested TOP in index pregnancy, 3 were declined as they were over the GA >20 weeks, the legal limit for TOP. One opted for adoption but the baby who demised, the other gave birth to a 1 380gram baby (was an ENND due to HMD) and the other had a 1300gram stillborn baby (MSB). One patient was 13-20 weeks’ pregnant when she applied for TOP but due to service overload there were no beds till she reached 20 weeks. She subsequently self-induced abortion and delivered a 1 400gram baby, who after weeks in NICU survived with no morbidities.
81
TABLE 3: Presentation and Management DESCRIPTION %
21. Presenting Complaint: a) Spontaneous preterm b) PPROM c) APH d) Abruption no HPT e) Rupture of uterus f) BBA
56% 5.5% 5.5% 5.5% 5.5% 11%
g) IUFD/Stillborn h) Septic abortion/retained placenta i) Pregnancy (fear baby had congenital anomalies).
5.5% 5.5% 5.5%
23. Steroids given: Yes (2/11 babies born alive).
18%
24. What will they do if baby is alive? a) Adoption b) Keep baby c) Unsure d) Unknown
22% (4) 33% (6) 28% (5) 17% (3)
25. Maternal Complication: a) Anaemia/ blood transfusion b) Repaired uterus c) Manual removal of placenta
5.5% 5.5% 11%
26.Contraception Post-Delivery: a) IUCD b) DEPO c) Refused d) BTL e) Not offered/discussed
17% (3)
17% (3) 17% (3) 5.5% (1) 44% (8)
STUDY CONCLUSION and RECOMENDATIONSSelf-induced late abortion with misoprostol is a contributor to preterm birth and perinatal morbidity and mortality. Babies born to these mothers are of Extremely Low Birth Weight (ELBW) and Low Birth Weight (LBW) increasing perinatal mortality rates and death in the first 30 days after huge costs in NICU. There is under reporting in PPIP of this as an avoidable factor and this need to be escalated in all facilities. Improved epidemiological data are essential, but social visibility is also important once communities and decision makers perceive high neonatal (and maternal) deaths as an issue, public ownership of the problem and progress will be more likely. This is a public health issue with physical, emotional, psychological and financial impacts Illegal trade of misoprostol from street vendors is common and self-medication is under reported and poses a threat to SDG 3.
82
Patients who disclose to misoprostol use often to not want cases reported to police as this will incriminate them as well as the supplier. This possess an ethical dilemma for clinicians. It is disturbing that in Jewkes study misoprostol was sourced from doctors and other health workers and HPCSA need to issue a warning on this practice or specific doctors reported and disciplinary measures taken.Health workers need to be trained to have an index of suspicion and ask about self- medication in a non-threatening way in patients presenting with spontaneous preterm labour. Testing patients for misoprol acid is expensive and often results negative due to timing of presentation.To deal with service demand and eligible patients who wait till more 20 weeks, changing protocol for 2ND trimester TOP to use both mifepristone and misoprostol and so the pregnancy does not advance and patients abort quicker freeing beds to reduce waiting time.To deal with staff attitudes organisation of services and ward for T2 TOP needs attention, dedicated TOP staff need to man the second trimester TOP wards not only OPD so attention is paid to post abortion care as well as de briefing sessions for affected staff.Patients who requested TOP and were unsuitable as well are a significant at-risk group. Community education is required on perinatal risks of abortion at late gestation; risk of illegal self-medication with misoprostol and safe options of adoption: Using a routine screening tool for emotional wellbeing and maternal psychosocial support in pregnancy will identify patients at risk [1] of self-abortion or those who have requested at denied TOP in index pregnancy. Referral to social worker for free counselling, adoption, foster care options can be engaged in timeously. It is evident that maternal and perinatal mortality is both a multi-dimensional health and broader developmental challenge, and that improved sexual and reproductive health is also dependent on a range of other factors including education, decent work, safety, clean water and sanitation, and adequate transport facilities.The involvement of researchers, grassroots organizations, health providers, activists, and media are vital in highlighting the consequences of late abortion.
83
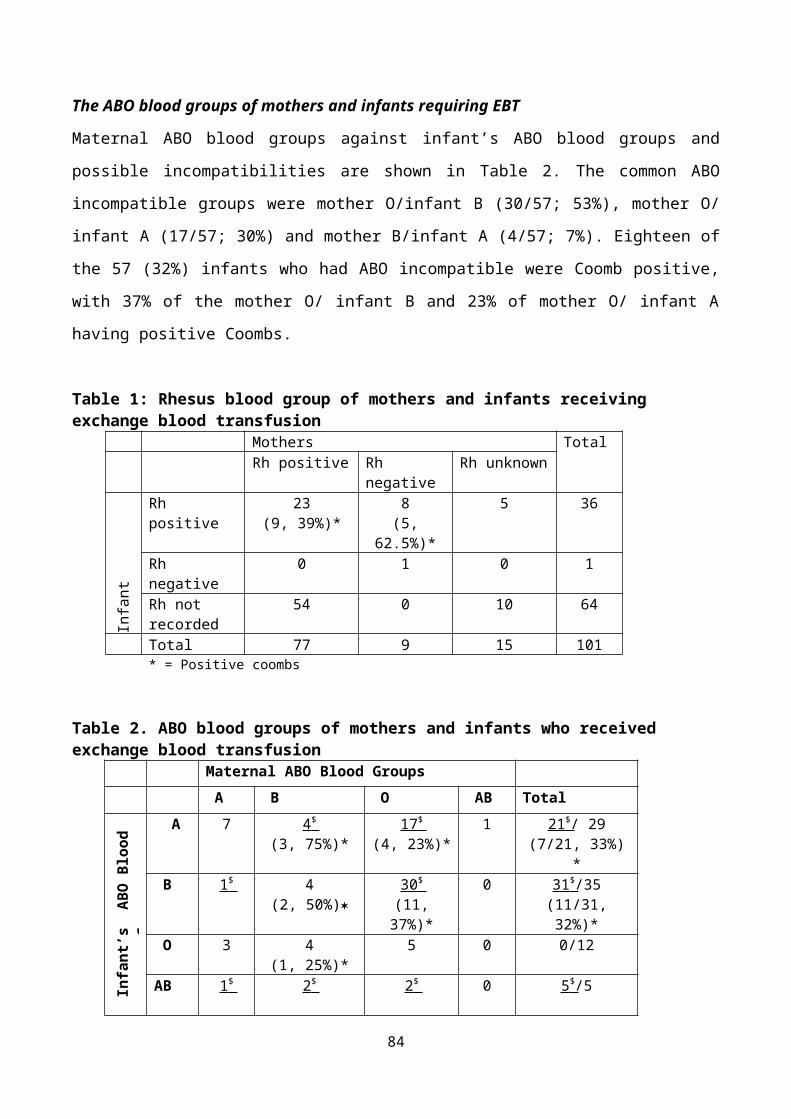
OUTCOMES OF BIRTH ASPHYXIA REDUCTION AT PHOLOSONG REGIONAL HOSPITAL
R Magagane
BackgroundBirth asphyxia is a significant cause of mortality and morbidity. Pholosong Hospital has a population of 1.123 million people. Our catchment area has eighteen local clinics and two MOU’s. The hospital has an Obstetrics and Gynecology department, only operating with 3 medical officers and 36 midwives. The hospital recorded 5036 deliveries between the period of January 2015 and December 2015. The average number of deliveries per month was 419.67 with a 40% caesarian section rate.
Objective 1. To reduce neonatal morbidity and mortality rate 2. To improve maternal health outcomes at Pholosong Hospital.
MethodsThe method of the study was conducted on a prospective and retrospective design. The study was conducted in high risk pregnant women unit at Pholosong. Birth asphyxia is defined as any perinatal insult or injury resulting in suffocation with increased carbon dioxide levels and anoxia. Asphyxia is also defined as hypoxia of such severity as to result in permanent brain damage (according to the Merriam-Webster dictionary). Initially skilled advanced midwives were allocated to do close monitoring, observe, advocate and record all events relating to labour, intra uterine fluid resuscitation and the 24-hour postnatal course from the 1 March 2015. A sample of 1072 high risk pregnant women was obtained along with informed consent from all participants. The period sample was 4 months, beginning on the 1st March 2015 to 30th June 2015. The data was collected by means of direct communication with pregnant women within the sample; maternity case records; morbidity & mortality meetings with feeder clinics and an Obstetric high risk patient handover tool. Proper hand over from shift to shift was emphasized.
84
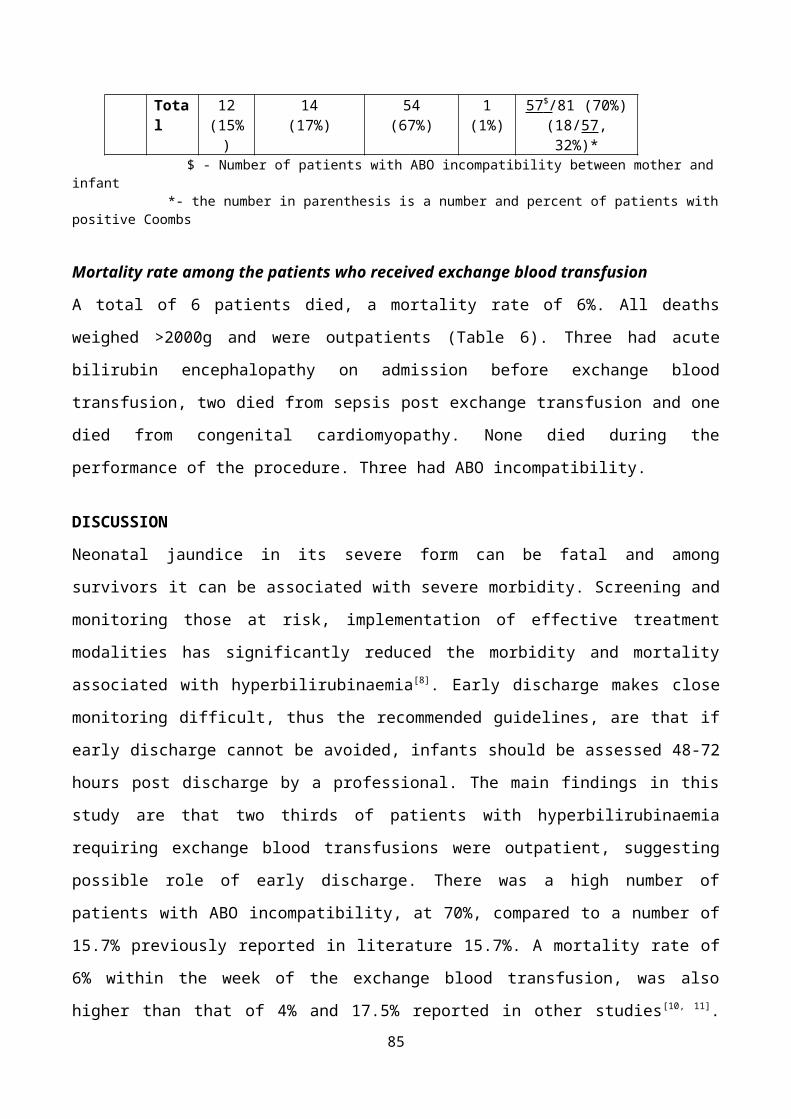
APGAR ScoringScore Grading
8 – 10 Normal birth 6 - 7 Mild birth asphyxia5 – 6 Moderate birth asphyxia0 – 4 severe birth asphyxia
APGAR scores at 10 minutes immediately after delivery provide useful prognostic data before other evaluations of infants. Low APGAR scores at 1 – 5 in 10 minutes have been found to be markers of increased risk of chronic motor disability.
The Thompson ScoringScore Grading1 -10 mild neonatal encephalopathy11 – 14 moderate neonatal
encephalopathy15 – 22 severe neonatal encephalopathy
These scoring systems were used for all infants with Birth Asphyxia so as to enable the Clinician to identify infants that may be at high risk of Neurological development abnormality.
Results• During the study period a total of 1697 deliveries were recorded of which
46.64% were by means of caesarian sections and 53.36% were normal vertex deliveries. During the first four months of the project we had only 1 birth asphyxia – in the study population - 0.09%. There was no maternal death in the sample study. Total maternal deaths out of the project March – June 2015 were four.
85
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec0
5
10
15
20
25
2119
1513
1213 13 13
14
9
56
Birth Asphyxia Incidence at Pholosong Hospital in 2015
Birth Asphyxia Incidence
The graph above shows the steady decline of birth asphyxia incidences during the project period of 1st March 2015 to 30th of June.
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec0
5
10
15
20
25
Birth Asphyxia Monthly Incidence at Pholosong Hospital
Axis Title
When the 2015 birth asphyxia incidences are compared to the figures of 2014, the red trend line shows the exponential increase in Birth Asphyxia’s for 2014
86
compared to the yellow trend line that shows an exponential decrease in birth asphyxia incidences for 2015.
Neonatal StatisticsMeconium Aspiration Without Meconium
March 2015 6 9
April 2015 5 8
May 2015 5 7
June 2015 3 9
The ICU survival rate was: 02 Bag masks ventilation at birth: 52 Persistent pulmonary hypertension: 01Babies with Hypoxic Ischaemic Encephalopathy (HIE): 05Babies discharged at Pholosong had the following, follow up records: 47Deaths: 05
ConclusionThe birth asphyxia incidences have improved since the project initiation in March 2015. From the 1072 sample patients, 500 mothers delivered by means of caesarean section (46.68%) and 572 delivered by means of normal vertex delivery (53.32%). Intra-uterine fluid fetal resuscitation and sound knowledge of CTG interpretation contributed to the reduction of birth asphyxia incidences at Pholosong Hospital in the 2015 sample. APGAR scoring followed by Thompson scoring predicts the severity of neonatal outcome based on morbidity and mortality.
87
THE INCIDENCE, MATERNAL, AND PERINATAL OUTCOMES OF ABRUPTIO PLACENTAE AT NELSON MANDELA ACADEMIC HOSPITAL, MTHATHA
CN Gubu-Ntaba, GAB Buga, JW WandabwaObstetrics and Gynaecology Nelson Mandela Academic Hospital, WSU
IntroductionAbruptio placentae is the premature separation of a normally implanted placenta. It is a life-threatening obstetric complication for both the mother and the foetus. Abruption often happens unexpectedly, and the management depends on the extent of the separation of the placenta, and the maternal and foetal condition.
Background of the studyDepartmental reports in obstetrics and gynaecology in Nelson Mandela Academic Hospital have continued to show that abruptio placentae is a major cause of maternal and perinatal morbidity and mortality, and a common reason for patient to be admitted to our hospital. It was therefore important that there was a study to determine its true impact by investigating the incidence and outcomes related to abruption placenta so as to be able to improve management of these patients.
Statement of the problemNelson Mandela Academic hospital is a tertiary referral hospital with the labour ward receiving high risk patients from district hospitals. Patients with abruptio placentae are commonly referred and contribute to a large number of stillbirths, and prolonged hospitalization of mothers due to associated complications.
METHODSSTUDY DESIGNThis study was a retrospective cross- sectional study which reviewed files of patients diagnosed with placental abruption at Nelson Mandela
88
Academic Hospital over a 2-year period from January 2011 to December 2012. STUDY SITEThe study was conducted at Nelson Mandela Academic Hospital NMAH. NMAH is a 700 bed teaching and referral hospital located in Mthatha in the Eastern Cape Province (ECP). It serves a population of approximately 1.8 million indigent people of ORT.
RESULTS Incidence of placental abruption. During the study period there were 206 women with abruptio placentae out of a total of 8684 deliveries, thus making the hospital-based incidence of abruption placentae 2.3 %.Booking statusThe ANC booking rate was 63 %.The mean number of ANC visits was 1.8 + 1.7 and median 1 (0-3), with minimum number of visits 1 to a maximum of 7 visits. Absence of ANC visit was a significant predictor of maternal deaths (14.9% n=7/47 in un-booked vs. 1.3% n=2/159; RR =11.8 95 % CI 2.6 – 55.1; P<0.0001) and neonatal deaths (38.9 % n= 7/18 un-booked vs. 17.9% n=10/56; RR 2.2 95% CI 1-4.9; P=0.065)
Risk factors for abruptio placentaeTable: Risk factors associated with abruptio placentaeVariables of interest Number (n) percentage (%)Smoking 6 2.9History of previous abruption 10 4.9Hypertension 119 57.8Male sex of fetus 111 53.9PPROM 5 2.4Chorioamnionitis 9 4.4Abdominal Trauma 6 2.9
89
Hypertension refers to all hypertensive disorders of pregnancy. *Some patients had more than one associated risk factor, which explains why the percentages add to more than 100%. Maternal complications of abruptio placentaeTable: Complications associated with abruptio placentaeVariables of interest Number (n) Percentage (%)PPH 36 17.5ICU admission 17 8.25DIC 20 9.7 Renal failure 31 15Pulmonary oedema 11 5.3Emergency hysterectomy 18 8.7Hypovolemic shock 13 6.3No complication 143 69.4
Mode of delivery and maternal mortality
90
Cesarean Section 6/104 Induced Delivery 3/25 Spontaneous Delivery 0/760
2
4
6
8
10
12
5.8
12
0n=
Modes of Delivery
Mar
tern
al M
orta
lity
%
Figure 1 proportions of maternal mortality by modes of delivery.
About 12% of mothers who died were delivered vaginally after induction and 5.8% were delivered by caesarean section.
Male baby and maternal outcomes
Male babies were significantly (P= 0.005) commoner among mothers with PPH (24.3% n=27/111) than female babies (9.5 % n=9/95). Offspring with male sex (15.3 % n=17/111) were significantly (P=0.003) more frequent than offspring with female sex (3.2 % n=3/95) in mothers with DIC. In mothers with pulmonary oedema (n= 11), all the offspring were male with no female offspring (P= 0.002). Offspring with male sex were significantly commoner than offspring with female sex (4.2 % n= 4/95) in mothers who had hysterectomy. Male babies (11 % n=12/109) were significantly (P = 0.033) commoner than female babies (2.1%; n=2/95) among mothers admitted to ICU. Among the mothers who died (n=9), 8 of the babies were male, compared with only one female baby (P=0.031). Low Apgar score was significantly (P< 0.01) commoner among male babies (82% n= 91/111) than among female babies (66.3 % n=63/95) among the women with abruption placentae who delivered live babies. Early neonatal deaths were significantly (P = 0.005) more frequent among male offspring (35.9 % n= 14/39) than female offspring (8.6% n= 3/35). The sex ratio of male
91
offspring: female offspring was significantly (P = 0.05) higher among mothers with low education level (1.3 n=99/89.2 % males and n= 76/80 % females) than that observed among mothers with high education level (0.6 n = 12 males /10.8% and n= 19 females /20%).
Perinatal mortality and birth weights.
Figure 2 Distribution of perinatal mortality by birth weights.
Abruptio placentae is a major cause of perinatal mortality and morbidity. There were only 86 live births in this study; 120 babies were stillborn. Of the live births, there were 17 neonatal deaths. The overall perinatal mortality associated with abruptio placentae in this study was 66.7 %. The high level of perinatal mortality associated with abruptio placentae in this study confirms what others have reported (Konje and Taylor 2001). Birth weight correlated significantly with neonatal outcome. Babies with a birth weight of less than 1500 g had a poorer outcome than babies with a birth- weight of 2500 g or more. These findings confirm that low birth weight is an important factor in neonatal mortality rate among live-born babies in patients with abruption placentae as reported by others (Naidu et al 1996).
92

Conclusion
Abruptio placentae is a very serious obstetric condition with significant maternal and perinatal morbidity and mortality. The maternal and perinatal morbidity and mortality rates are far higher in a poorly resourced setting such as ours than in the bigger cities. Improvement in the care of antenatal mothers at all levels is clearly essential for a quick diagnosis and management of abruptio to reduce this morbidity and mortality. Improvement in health-seeking behaviour of antenatal mothers is also important. More research is needed for prediction and prevention of abruptio placentae.
93
ENDING PREVENTABLE STILLBIRTHS: GLOBAL SITUATION & SOUTH AFRICA’S CONTRIBUTION
By Mary Kinney on behalf of The Lancet Ending preventable stillbirths Series Advisory Group and Study Group
BackgroundIn the first year of the new development era, defined by the Sustainable Development Goals (SDGs), there were 2.7 million newborn deaths, 2.6 million babies stillborn and 303,000 maternal deaths. Many of these deaths were preventable, with known solutions. The Lancet’s Ending preventable stillbirth Series, published in January 2016, exposes the neglected issue of 2.6 million stillbirths each year (Froen et al., 2016, Lawn et al., 2016, Heazell et al., 2016, Flenady et al., 2016, de Bernis et al., 2016).
The Series provides updated global and national stillbirth rate estimates, assesses the impact of stillbirths on women and societies, and presents evidence for action to end preventable stillbirths by 2030. As a collaboration of 216 authors, investigators, and advisers representing 43 countries and more than 100 organisations, the Series present a renewed call to action for the post-2015 era, framed within the context of health, survival, and overall quality of care for women and their babies. This Series follows The Lancet’s Stillbirth Series in 2011, Every Newborn Series in 2014 and Midwifery Series in 2014 and shows that more must be done to integrate stillbirth prevention within global and national agendas for high quality health care for women, adolescents, and babies.
This short paper for the South African Perinatal Priorities Conference summarizes the main findings of the Series, makes the case for strengthening action to end preventable stillbirths and calls for improved bereavement care within the maternal and child health continuum, founded upon ensuring a woman’s right to quality healthcare for herself and her baby during pregnancy and childbirth.
Methods and analyses used
94

The Series contains five academic papers, two articles and four comments. Multiple methods were used in the different to assess data. A policy analysis examined global and national reports and policies, financial commitments and research advancements. Data from 157 countries was collected and analyses to model country level stillbirth rate and intrapartum stillbirth rate estimates. A novel risk factor analysis was undertaken as well as a series of systematic reviews and meta-syntheses with respect to direct, indirect, and intangible costs of stillbirth on parents, families, and health-care providers. The Lives Saved Tool was used to determine the magnitude of quality and equity gaps in terms of lives saved and cost. An organisational network analysis examined relationships among 33 organisations working to prevent stillbirths.
Main findings
1. Global burden of stillbirths: Where? When? Why? Worldwide in 2015, there were 18.4 stillbirths per 1000 total births. The average annual rate of reduction for stillbirths (2.0%) has been far slower than that for either maternal (3.0%) or post-neonatal mortality of children younger than 5 years (4.5%) (Lawn et al., 2016). At present rates, more than 160 years will pass before a pregnant woman in Africa has the same chance of giving birth to a live baby as does a woman in a high-income country today. In every region, there are countries making more rapid progress, showing that further improvement in stillbirth rate reduction is possible.
Most of the world's 2.6 million stillbirths each year occur in low- and middle-income countries (98%), with three-quarters in sub-Saharan Africa and south Asia. About 60% occur in rural areas and more than half in conflict and emergency zones, affecting the families most underserved by healthcare systems. Half of all stillbirths occur during labour—1.3 million each year (Lawn et al., 2016). In all countries, the risk of stillbirth is highest for the most marginalised populations. Social disadvantage is
95
associated with a doubling of the risk of stillbirth in high-income countries, an effect which is likely to be even greater in low- and middle-income countries (Flenady et al., 2016). This disparity reflects structural inequalities, including racism and inequity of opportunity.
2. Stillbirths: A heavy burden for societyStillbirth remains hidden from society, and has wide-reaching consequences for parents, care providers, communities, and society that are frequently overlooked and underappreciated. The estimated direct financial cost of a stillbirth is 10-70% greater than the cost of a live birth (Heazell et al., 2016). Costs of healthcare provision associated with stillbirth are often an out-of-pocket expense for families, as are costs of funeral and burial or cremation of the baby. Parents may lose income due to time off work, reduced working hours, or reduced productivity. Survey data show parents may only be working at 26% of normal work productivity 30 days after the stillbirth of their baby, increasing to just 63% of normal productivity after 6 months.
Disenfranchised grief is common, whereby parents' grief after stillbirth is not legitimised or accepted by health professionals, family members, or society. A survey found that bereaved parents felt their community believed that "parents should try to forget their stillborn baby and have another child" (Flenady et al., 2016). Many parents suppress their grief in public. Women whose babies have been stillborn often feel stigmatised, socially isolated, and less valued by society and, in some cases, are subject to abuse and violence. Stigma and taboo exacerbate trauma for families, and fatalism impedes progress in stillbirth prevention. Negative psychological symptoms often persist for years after stillbirth.
An estimated 4.2 million women are living with depression associated with stillbirth (Heazell et al., 2016). Care providers are also deeply affected both personally and professionally, experiencing guilt, anger, blame, anxiety, and sadness, as well as fear of litigation and disciplinary action.
96
3. Preventing deaths with health system improvements and an integrated approach
Most stillbirths, as well as maternal and newborn deaths, are preventable through high quality antenatal and intrapartum care within the continuum of care for women and children. The belief that many stillbirths are unavoidable due to congenital abnormalities is widespread, yet these account for a median of only 7.4% of stillbirths (Lawn et al., 2016). Major stillbirth risk factors are well known and often overlap, including maternal age >35 years, maternal infections (notably syphilis and malaria), non-communicable diseases, obstetric complications, and nutrition and lifestyle factors (see Figure). In high-income countries, 90% of stillbirths occur in the antepartum period, often associated with preventable lifestyle factors (Lawn et al., 2016, Flenady et al., 2016).
Stillbirth prevention and response requires an integrated approach within the framework of quality care across the continuum (de Bernis et al., 2016). Neglect of stillbirths reduces and hides the full potential of programmes for women's and children's health. The stillbirth rate is the most sensitive marker of quality and equity of health care and health systems.
97
Figure: Regional variation in population attributable risk of stillbirth for factors with adequate risk data and appropriate prevalence data, from Lawn et al, Stillbirths: rates, risk factors, and acceleration towards 2030. Lancet. 2016.
4. No one left behind: The case for investing in stillbirth prevention
Investing in stillbirth prevention is a smart investment for economies and societies. The cost of averting stillbirth in low- and middle-income countries would be returned almost 25-fold through the economic and social value these live children would provide their families, communities and nations (ten Hoope-Bender et al.). Action to prevent stillbirths – especially to increase access to quality healthcare in pregnancy and childbirth – will yield multiple returns on investment by reducing maternal and neonatal deaths and morbidities as well as improving child development outcomes (de Bernis et al., 2016). Scaling up proven antenatal and intrapartum interventions in the 75 highest burden countries could prevent 823,000 stillbirths, 1,145,000 neonatal deaths and 166,000 maternal deaths annually with universal coverage by 2030 at an additional annual cost of US $2,150 for each life saved (Heazell et al., 2016). Deliberate integration of action to prevent stillbirths within the continuum of maternal and child healthcare is a necessary step to achieving the SDGs by 2030 and supporting the UN’s commitment to “leaving no one behind”.
98
Box: Targets for ending preventable stillbirths and improving bereavement support by 2030
MORTALITY TARGETS BY 2030: Country burden: 12 stillbirths or
fewer per 1000 total births in every country
Equity: All countries set and meet targets to close equity gaps and use data to track stillbirths
UNIVERSAL HEALTH CARE COVERAGE TARGETS: Family planning (by 2020): 120
million more women and girls with access to contraceptives
Sexual and reproductive healthcare: Universal access to services and integration into national strategies and programmes
Antenatal care: Universal comprehensive quality antenatal care
Care during labour and birth: Universal effective and respectful intrapartum care
MILESTONES: Every Newborn global and national
milestones Respectful care, including
bereavement support after a death: Global consensus on a package of care after a death in pregnancy or childbirth for the affected family, community, and caregivers in all settings
Stigma: All countries to identify
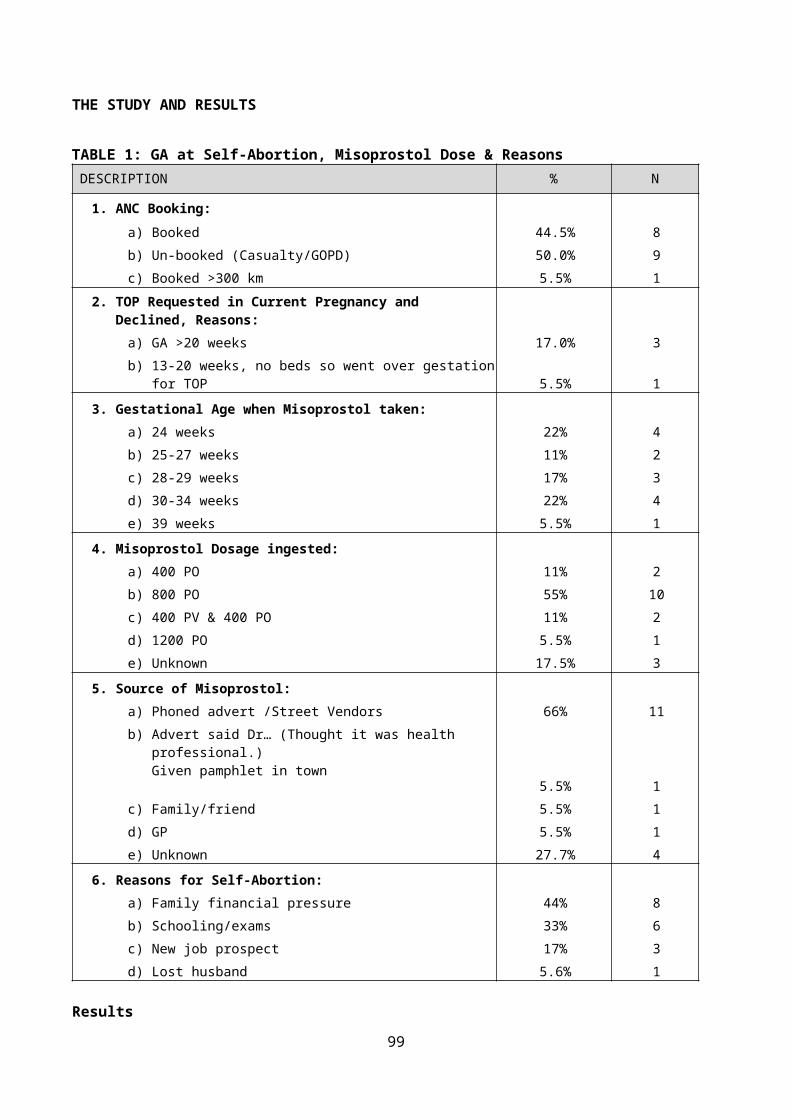
5. Greater progress is neededThe high global burden of stillbirths along with slow progress in reduction, limited attention and persistent stigma led the independent Expert Review Group for the accountability of the Global Strategy for Women’s and Children’s Health (2010-2015) to call for the integration of stillbirths within the post-2015 agenda, stating that “A further issue that has been even more neglected than adolescent health is stillbirths”(World Health Organization, 2015). In the past five years, progress in systematic integration of stillbirth prevention within global and national initiatives has been uneven. A target to end preventable stillbirths was included in the Every Newborn action plan and endorsed by 194 countries at the World Health Assembly in 2014. Data for tracking stillbirth has increased and WHO's "100 Core Health Indicators" now include the stillbirth rate. Yet mentions of stillbirth remain limited in most relevant policies, research, and funding. Only 15 of 67 national health plans assessed mentioned stillbirths and fewer incorporated a stillbirth rate target (Froen et al., 2016).
Limited progress reflects stillbirths’ exclusion from the Millennium Development Goals. The sheer burden of 2.6 million deaths, together with the interlinkages between stillbirth prevention and the prevention of maternal and newborn deaths, point to the urgency of ensuring this situation is not repeated in the post-2015 agenda, despite the fact that stillbirths are also missing from SDG targets and indicators.
ConclusionThe Lancet’s Ending preventable stillbirths Series set out a renewed call to action to end preventable deaths—stillbirths, newborn and maternal deaths—and improve bereavement support by 2030, including targets and milestones from the United Nations-endorsed Every Newborn Action Plan (World Health Organization & UNICEF, 2014) (see Box). The stillbirth rate is an important indicator of quality of care in pregnancy and childbirth, as
99

well as a sensitive marker of health systems’ strength, measuring not only progress in achieving SDG targets for reduction of neonatal, maternal, and under 5 mortality, but also progress on other targets aimed at reducing poverty and increasing equity and access to healthcare. Effective implementation of the SDGs and the Global Strategy will be maximised by acknowledging, incorporating, and counting stillbirths.
Meeting these targets will require that the global health community, country leaders, and individual women and men collaborate more effectively in support of the following actions: (1) deliberate leadership at global and country levels, especially from policy makers; (2) increased voice, especially of women, to break the silence and reduce stigma and taboo surrounding stillbirths; (3) implementation of integrated interventions across the maternal and child health continuum, with investment that is commensurate with the scale of the global burden of stillbirth; (4) definition and use of indicators to measure progress and quality of care; and (5) investigation of gaps in knowledge on stillbirth prevention and bereavement support (de Bernis et al., 2016). If attention to stillbirth is not increased, 2.6 million families each year will continue to be left behind, and global initiatives including the SDGs will fail to be fully realized.
South Africa provides an example to other countries on integration of stillbirth prevention efforts into existing and new strategies. For example, it is one of the few countries in Africa to consistently record and report stillbirths and the Department of Health set a target stillbirth rate within the current national strategic and has incorporated stillbirth rate as a priority indicator. Michalow and colleagues published a paper in 2015 with the first analysis in South Africa to assess the impact of scaling up interventions to avert stillbirths and demonstrated that South Africa can achieve the global stillbirth rate target of 12 per 1000 births by effective scale up of 13 priority interventions, which will also prevent maternal and newborn deaths (Hofman et. al., 2015).
100
Lancet Ending preventable stillbirths Series Advisory GroupJose M Belizán, Institute for Clinical Effectiveness and Health Policy, Buenos Aires, Argentina; Zulfi Bhutta, The Hospital for Sick Children, Toronto, Canada; Amy Boldosser-Boesch, Family Care International, New York, NY, USA; Romano Byaruhanga; St Raphael of St Francis Hospital, Nsambya, Kampala, Uganda; Mariam Claeson, Bill & Melinda Gates Foundation, Seattle, WA, USA; Gary L Darmstadt, Department of Pediatrics, Stanford University, Stanford, CA; USA; Frances Day-Stirk, International Confederation of Midwives, The Hague, Netherlands; Kim E Dickson (UNICEF Headquarters, New York, NY, USA; Soo Downe, University of Central Lancashire, Preston, UK; Jacqueline Dunkley-Bent, Well Being Foundation Africa, London, UK; David Ellwood, Griffith University, Gold Coast, Australia; Jan Jaap Erwich, University of Groningen, Groningen, Netherlands; Lynn Farrales, University of British Columbia, Vancouver, Canada; Rachel Firth, Wellbeing Foundation, Lagos, Nigeria; Robert Goldenberg (Columbia University, New York, USA; Robin Gorna, Partnership for Maternal, Newborn & Child Health, Geneva, Switzerland; Nana Kuo, Every Woman Every Child, New York, NY, USA; Ana Langer, Maternal Health Task Force, Harvard University, Boston, MA, USA; James A Litch, Global Alliance to Prevent Prematurity and Stillbirth, Seattle, WA, USA; Gillian Mann, Department for International Development, London, UK; Betsy McCallon, White Ribbon Alliance, Washington, DC, USA; Janna Patterson, Bill & Melinda Gates Foundation, Seattle, WA, USA; Bob Pattinson, University of Pretoria, Pretoria, South Africa; Craig Rubens, Global Alliance to Prevent Prematurity and Stillbirth, Seattle, WA, USA; Jessica Ruidiaz, Era en Abril, Buenos Aires, Argentina; Toyin Saraki, Wellbeing Foundation, Lagos, Nigeria; Bob Silver, University of Utah Health Sciences Center, Salt Lake City, UT, USA; Peter Singer, Grand Challenges Canada, Toronto, Canada; William Stones, University of St Andrews, St Andrews, UK; Katherine Taylor, US Agency for International Development, Washington, DC, USA; Marleen Temmerman, Department of Reproductive Health and Research, WHO, Geneva, Switzerland; Lara Vaz, Save the Children and Saving Newborn Lives, Washington, DC, USA; Donna Vivio, US Agency for International Development, Washington, DC, USA; Linda Weisert, Children's Investment Fund Foundation, London, UK; Jennifer Zeitlin, Paris Descartes University, Paris, France
Lancet Ending preventable stillbirths Series Study Group Hannah Blencowe, London School of Hygiene and Tropical Medicine, UK; Luc de Bernis, UNFPA, Switzerland; Vicki Flenady, International Stillbirth Alliance and Mater Medical Research Institute, Australia; Frederik Froen, Norwegian Institute of Public Health, Norway; Alexander Heazell, International Stillbirth Alliance and University of Manchester, UK; Mary Kinney, Saving Newborn Lives, Save the Children, South Africa; Joy E Lawn, London School of Hygiene and Tropical Medicine, UK; Susannah Hopkins Leisher, International Stillbirth Alliance and Mater Medical Research Institute, Australia
101
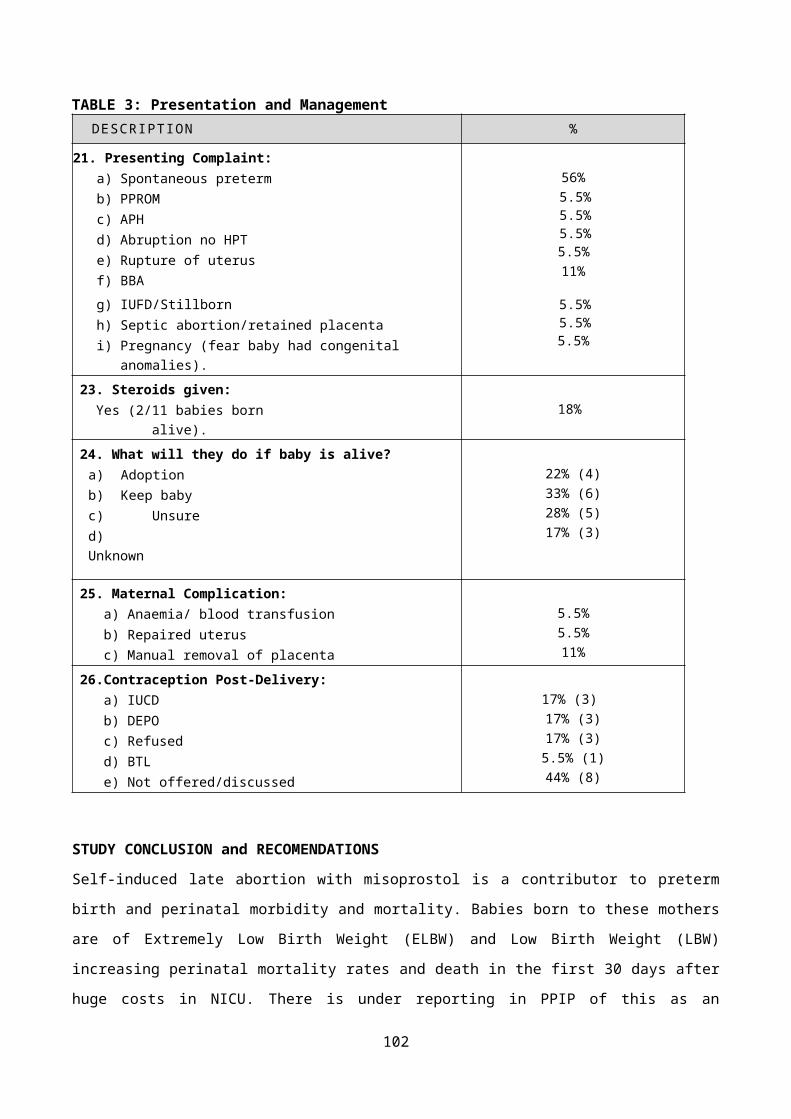
AUDITING STILLBIRTHS AT LOWER UMFOLOZI REGIONAL HOSPITAL: A 12 MONTH REVIEW
Dr Indira Govender
Introduction
The World Health Organisation (WHO) defines a stillbirth as a baby born with no signs of life at or after 28 week’s gestation, or with a birth weight of at least 1000g. Although the total number of stillbirths worldwide was estimated to be 2.6 million in 2009, the literature on stillbirths from developed countries remains small and even less so for developing countries. Most (98%) stillbirths occur in low and middle-income countries, with two-thirds of all stillbirths occurring in rural families. But global policy appears to reflect social stigma and beliefs as these figures go unmentioned in the UN Millennium Development Goals, the Global Burden of Disease study or routine reports from the WHO. The 9th Saving Babies report for the period 2012 to 2013, based on data collected on the Perinatal Problem Identification Programme (PPIP), reported South Africa's total stillbirth rate (SBR) and rate for stillbirths weighing 1000g or more (SBR 1000g+) to be 23.1 and 17.6 respectively per 1000 total births. The SBR and SBR 1000g+ for KwaZulu-Natal province (KZN) is 26.2 and 19.7 respectively per 1000 total deliveries, and the SBR and SBR 1000g+ for regional hospitals in the latest Saving Babies report is 30.2 and 22.6 respectively per 1000 total deliveries.
Lower Umfolozi War Memorial Regional Hospital (LURWMH), located in the semi-rural part of northern KZN, specialises in maternal and child health services and covers a population of 2.5 million over three health districts: uThungulu, Umkhanyakude and Zululand. Whilst gazetted a Regional hospital, LUWMRH provides a unique combination service receiving direct referrals from 21 local clinics, functions as the local district hospital and provides a tertiary service for 17 district hospitals in the three districts that make up Region 4 of KZN. Using the average rates for the three
102
districts, the SBR and SBR 1000g+ for Region 4 is 23.4 and 18.0 respectively per 1000 total deliveries.
Perinatal audit meetings are conducted on a daily basis during the week at the hospital and all stillbirths, amongst other adverse perinatal outcomes, are reviewed in detail. Individual maternity case records are summarised using a paper-based form known as the "Hands Up" Mortality and Morbidity Extraction Tool (HUMMET) and then entered into the electronic PPIP database. The HUMMET form was developed by the hospital's Head of Department (HOD) for Obstetrics and Gynaecology (O&G) in 2010 and is implemented in all referring facilities of Region 4. Records on the hospital's PPIP database between 1 April 2014 and 31 March 2015 show that there were 8,795 deliveries including 346 stillbirths, of which 249 weighed more than 1000g. There were 310 corresponding HUMMET forms for 305 patients during the study period, representing 90% of the total number of stillbirths reported on the PIPP tool.
The purpose of the audit was to obtain a more detailed understanding of factors affecting perinatal outcomes at a local level and inform future interventions to improve outcomes in this context. Ethics approval to conduct a retrospective audit of the forms was granted by the hospital's ethics committee. Data collected from the HUMMET forms was further summarised and entered into a Microsoft Excel spreadsheet.
Results:Table 1 compares the SBR and SBR 1000+ during the study period at LUWMRH to data in the latest Saving Babies report. Due the proportion of referrals from outside the facility, the SBR and SBR 1000+ is an over-estimate. However, when using the average rates for the 3 districts in Region 4, the SBR and SBR 1000+ are similar to national and provincial rates.
SBR SBR
103
1000+South Africa 23.1 17.6KwaZulu-Natal
26.2 19.7
Regional Hospitals
30.2 22.6
LUWMRH 39.3 28.3Region 4 23.4 18.0
Table 1: Comparing SBR
Table 2 lists the stillbirth outcomes and mode of delivery. Although the majority of stillbirths were macerated, indicating poor antenatal care, this figure includes intra-uterine deaths that are referred to the facility for induction of labour.
Total stillbirths = 310Outcome Number
(%)Mode of delivery Number
(%)Macerated stillbirth (MSB) 225 (73) Normal vaginal
delivery 232 (75)Fresh stillbirth (FSB) 85 (27) Caesarean section 78 (25)
Table 2: Stillbirth outcomes and mode of deliveryTable 3 lists the weight categories at delivery which include stillbirths with a gestational age of less than 28 weeks but weighing more than 500g.
Total stillbirths = 309Weight at delivery Number
(%)500g - 999g 78 (25)1000g - 1499g 78 (25)1500g - 2499g 106 (34)> 2499g 47 (15)
Table 3: Weight categories
Table 2 describes basic antenatal care demographics of the patients. Total number of patients = 305
Maternal Age Maternal Parity Antenatal careNumber of
visits to antenatal clinic
Category
Number (%)
Category
Number (%)
Category
Number (%)
Category
Number (%)
</= 18 yrs 30 (10) 0 114
(37)Unbook
ed 19 (6) None 17 (6)19 - 34
yrs241 (79) 1 - 4 185
(61) Booked 286 (94) 1 - 3 93 (31)
>/= 35 yrs 33 (11) > 4 6 (2)
1st visit < 20
weeks157 (51) > 4 191
(63)Unknow
n 0 Unknown 0 Unknow
n 2 (1) Unknown 0
Table 2: Basic antenatal care demographics
104
Table 3 below describes basic antenatal care booking blood results.Total number of patients = 305
Rapid test result Number (%) HIV result Number (%)Syphilis positive 13 (4) Negative 171 (56)Syphilis unknown 22 (7) Positive 127 (42)Rhesus negative 9 (3) CD4 < 350 34 (27)*Rhesus unknown 11 (4) CD4 unknown 45 (35)*
Table 3: Basic booking blood results *Percentage of HIV positive patients
Graph 4 illustrates the number of patients with adverse outcomes in previous pregnancies.
0 5 10 15 20 25 30 35 40 45
41
10
13
Past obstetric history (n = 305)
Previous Abruptio/Pre-eclampsia/Eclampsia
Previous SB
Previous miscarriage
Graph 4: Past obstetric history
Graphs 5 illustrates the most common obstetric causes of stillbirths; some conditions occur simultaneously in the same patient. Abruptio placentae was the biggest cause, followed by hypertensive disorders in pregnancy. The number of stillbirths with congenital abnormalities is also an overestimate due the referral cases that deliver at LUWMRH.
0
20
40
60
80
100
120
36
109
18
79
65
18
Most common obstetric causes of stillbirths (n)
Unexplained IUD Abruptio placentae Congenital abnormalityGestational Hypertension Pre-eclampsia Eclampsia
Graph 5: Obstetric causes of stillbirths
Regarding the most common avoidable factors, 15% of patients reported a late response to reduced foetal movements and 9% of patients
105
experienced a delay in transfer to the referring facility, either from clinic to the local district hospital or to LUWMRH.
Graph 6 illustrates the most common areas of substandard care at clinic level.
0 5 10 15 20 25 30 35 40
37
31
24
15
15
10
9
Areas of substandard care at clinic level (n)
Not screened for DM
Foetal kick count chart not used
Delayed referral
Inappropriate management of in-fections
Inappropriate foetal monitoring/ In-complete ANC assessment or records
Inappropriate management of pre-eclampsia/elevated BP
Inappropriate use of growth chart
Graph 6: Areas of substandard care at clinic level
Graph 7 illustrates the most common areas of substandard care at hospital level.
0 5 10 15 20 25 30 35 40
38
15
12
8
Areas of substandard care at hospital level (n)
Missed abruptio placentae
Delay in C/S
Inappropriate foetal monitoring/ missed foetal distress
Inappropriate management of obstetric condition/emergency
Graph 7: Areas of substandard care at hospital level
Discussion:Most women who delivered stillbirths during the study period were multiparous and between the ages of 19 and 34 years but early booking (before 20 week’s gestation) at antenatal clinic is still a challenge. Twenty-one percent of women (64 cases) noted to have had a previous adverse outcome need special attention and early antenatal care for close follow-up in future pregnancies. Hypertensive disorders are a major risk factor for stillbirth; in November 2015 a workshop aimed at improving the
106
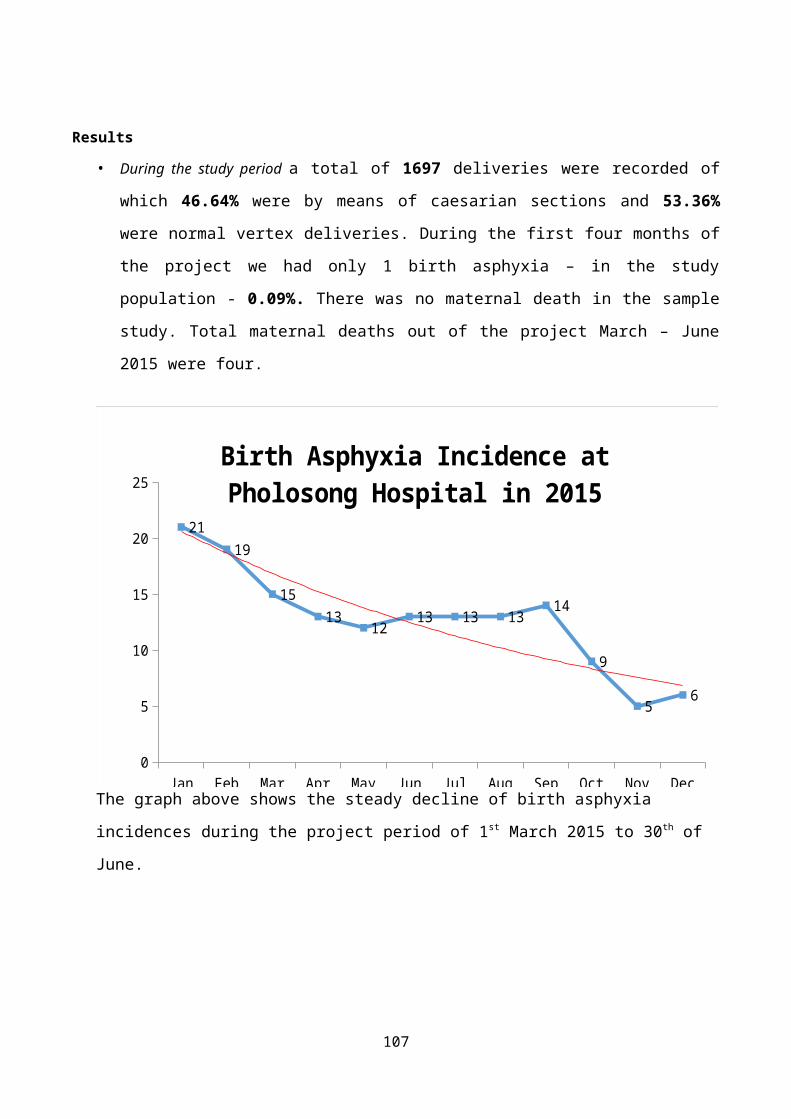
skills of health-care workers was held and the management of these patients will be closely monitored. Together with stillbirths identified as having congenital abnormalities, a significant number are unexplained. This baseline study will be used to motivate for further investigations in these cases.
The late response from some pregnant women to reduced foetal movements is a complex issue that needs further investigation, as well as evaluating the effectiveness of the foetal kick count chart.
The reasons for delays in caesarean sections at hospital level in these cases range from administrative, such as a delay in transfer between facilities or staff shortages, to health care worker-related. The nature of the delay also varies from a matter of hours to days, depending on whether the case was an emergency or elective.
A major limitation to this study is missing and incomplete HUMMET forms, most likely resulting in an underestimate of the findings. Outstanding blood results are often collected after delivery but not in time to be entered onto the HUMMET form when presented in the audit meeting.
Conclusion:This audit provides useful information on the severity and volume of complicated obstetric cases being referred to LUWMRH, and the population it serves. However, further quantitative and qualitative research is needed to better understand the obstacles that women encounter to early booking and their health-seeking behaviour.
Although in-service training for doctors and nurses at clinics and hospitals, in the form of ESMOE is ongoing, these programs also need to be evaluated and updated based on local data. RISK FACTORS, REPAIR TECHNIQUES AND SHORT TERM SUBJECTIVE OUTCOME OF OBSTETRICS ANAL SPHINCTER INJURIES AT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
Tshabalala SM, Oyebajo AB, Adam Y.
107
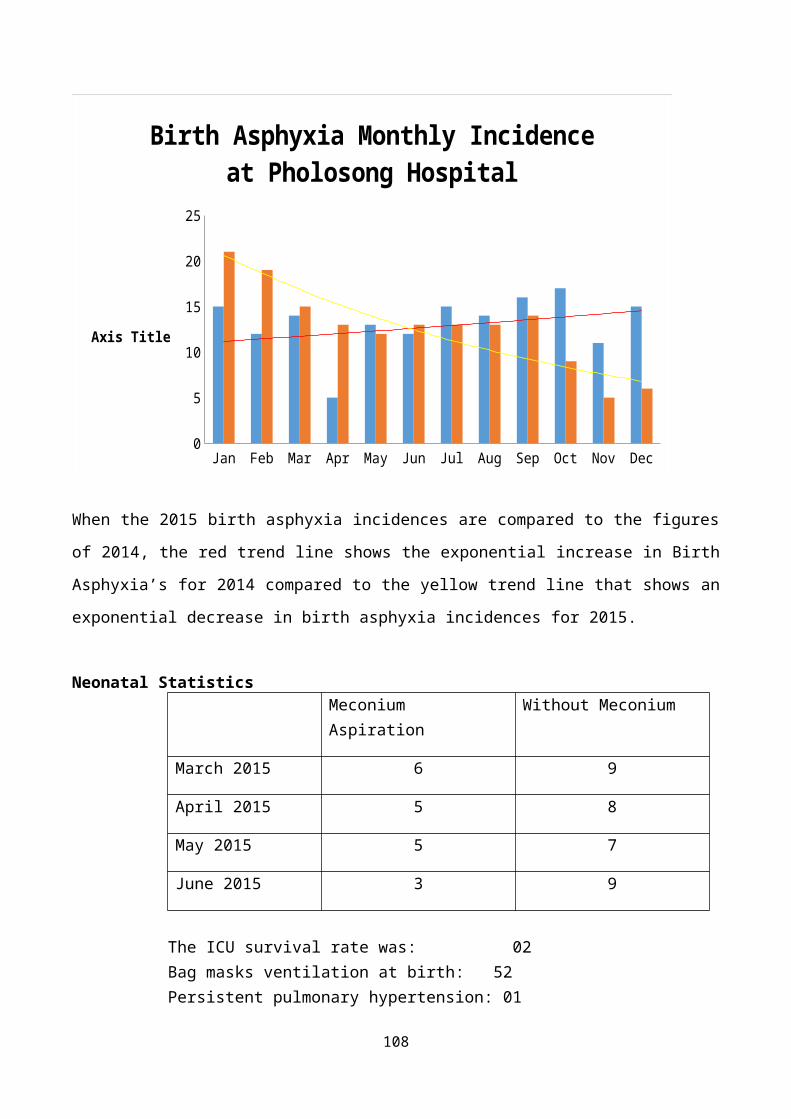
Department of Obstetrics and Gynaecology, University of the Witwatersrand, South Africa.
IntroductionObstetric anal sphincter injuries (OASIS) involve injuries to the anal sphincter, its innervation or both following child birth.It can be a cause of considerable morbidity i.e. faecal and flatus incontinence, faecal urgency (described as inability to defer defaecation for more than 15 minutes) and superficial dyspareunia.It is estimated that 1-4 % of vaginal deliveries are complicated by obstetric anal sphincter injuries internationally. The figures may be higher, considering that a large number of OASIS are under reported partly due to occult injuries only identified by endo-anal ultrasonography and poor understanding of the perineal anatomy by health care workers attending to labouring women. This results in OASIS being missed. Incontinence is embarrassing for the sufferers, many times people who suffer from incontinence do not seek help. The risk factors for OASIS include:Maternal: Primigravida, certain racial groups i.e. Black and Indian race are at a higher risk compared to their Caucasian counterparts.Fetal: Birth weight above 4000g, large neonatal head circumference, occipito- posterior position and shoulder dystocia.Labour causes: Prolonged second stage, precipitous labour.Iatrogenic: assisted delivery (Forceps and vacuum), epidural anaesthesia, extended episiotomy or a median episiotomy.Classification of OASIS1st degree: Perineal skin2nd degree: Skin and perineal muscles3A <50 % of the external anal sphincter is involved.3B >50 % of the external anal sphincter is involved.3C Internal and external sphincter involvement4th degree: anal sphincter complex plus anal mucosa5th degree: also called the button -hole tear, the anal sphincters are intact but the anal mucosa is torn.
108
Most of the reported literature is from Europe and America, with little data about the condition in our population, this study hopes to provide local data with possibly some new insights. This study aims to highlight the need for follow up (in the form of a post-natal clinic) At post- natal clinic symptoms will be sought for by a health care worker instead of relying on the patient to report the symptoms.
Objectives1. To evaluate the risk factors for OASIS at CHBAH2. To describe the methods used to repair 3rd and 4th degree tears at
CHBAH3. To asses’ outcome post repair based on the patient’s symptoms.
Methods Setting:
The study was performed at Chris Hani Baragwanath Academic Hospital. CHBAH is a tertiary, academic hospital located in Soweto. The maternity department is regarded as one of the largest in South Africa, with annual deliveries of more than 22000 babies.
Study populationThe population was made up of women who gave birth vaginally at CHBAH, its surrounding hospitals and clinics that refer to CHBAH. The women included were those whose deliveries were complicated by 3rd and 4th degree perineal tears. Inclusion criteria: 18 years and older. Exclusion criteria: 1, 2nd degree tears.
Sample sizeSixty patients
Data management Data was collected prospectively
109
The bed letter was used to complete a data sheet. A telephonic interview was held at six and twelve weeks’ post-partum to establish the presence of sequelae.
Study design A descriptive studyStatistics Simple statistics with standard descriptive tests was used and results
were presented as percentages, frequencies, means +- standard deviation (SD), medians and ranges.
Ethics The study was approved unconditionally by the University of the
Witwatersrand, Human Research Ethics Committee. A clearance certificate M120970 was granted.
ResultsThere were 123 patients with 3rd and 4th degree tears during the study period. Sixty met the inclusion criteria. The incidence of OASIS during the study period was 0.5%.The mean age of our study population was 23, SD of 5.5 and a median of 22.Seventy-three percent (73%) of the study population were primigravids.Twenty-five (25 %) of our study population were HIV positive.Of the positive 40% were on treatment, the remaining 60% were on what was known as PMTCT (prevention of mother to child) regimen, where pregnant women received AZT® antenatally and Neviripine and Tenofivir ® in labour.Ninety per cent of the study population gave birth at CHBAH, 3 % gave birth at home.An episiotomy (Medio-lateral) was performed in 63% of casesVacuum assisted delivery was performed in 18% of cases and 3% had forceps assisted delivery.Two percent (2%) of babies were above 4000g at birth.
110

18%
42%
37%
3%
Repair of OASIS
Overlap End to end
Not clearly stated Never repaired
Figure 1: Repair of OASISThe majority of the surgeons at CHBAH preferred the end to end technique (42%) over the Over-lap technique (18%). In 37% of the cases the tear was not further classified into 3a or 3b or 3c, it was just labelled a third degree tear.Three percent of the study population were not repaired primarily, 24 hours lapsed whilst waiting to be operated on. The hospitals’ protocol entails that 3rd and 4th degree tears ought to be repaired within 6 hours of delivery and not more 24 hours post-delivery. The tear is deemed contaminated and susceptible to wound break down after 24hours.Lack of theater time was the reason why they were not repaired. Theater was inundated with emergency caesarean sections.
Specialist Medical Officer Snr Reg Jnr Reg
15%
9%
31%
45%
Level of expertise
Surgeon
% Po
pulati
on
Figure 2: Level of expertiseA junior registrar was defined as registrars in their 1st and second year of training, a senior registrar was a registrar who was in their 3rd or fourth year of training in the field of Obstetrics and Gynaecology. The medical officer group entailed doctors working in the department post community
111
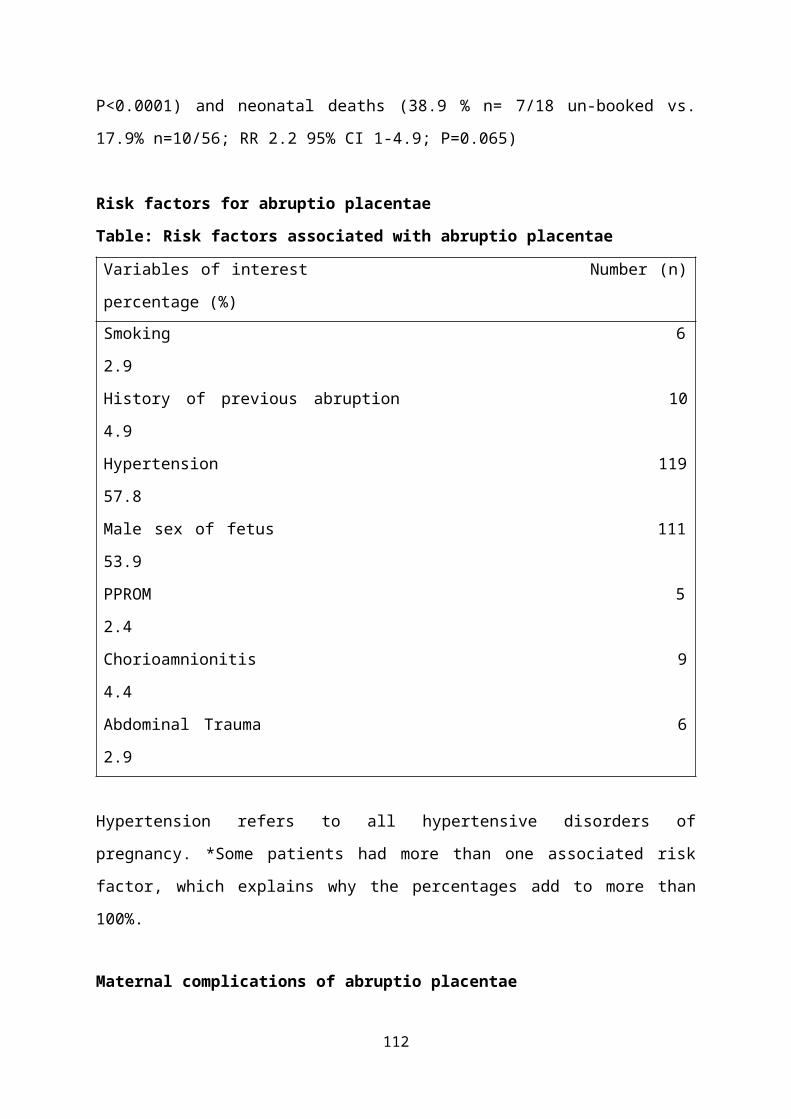
service training and those that have completed their registrar -ship, however have not attained the College of Medicine specialist exams.
Vicryl Not clearly stated PDS
53%
38%
9%
Suture material
Material type
% Po
pulati
on
Figure 3 Suture materialEighty- three (83%) of the patients received antibiotics post repair.Sixty -two (62%) of patients were prescribed for: laxative or stool softener post repair.At 6 weeks only
At 12 weeks only
Both 6 and 12 weeks
Not reached at 6 & 12 weeks
6 (10%)
2(3%) 37 (62%)
15 (25%)
Table 1: Telephonic interview. Patients who answered the questionnaire.The majority of the patients remained asymptomatic at follow up.The small number that were symptomatic, leakage of gas was the most common complaint 82%. Symptoms did improve with time.
DiscussionThe incidence of OASIS at CHBAH is lower than most reported incidences in the literature at 0.5%.The majority of the patients were primigravids’ (73%), making a link between primigravidity and the risk of sustaining an OASIS, a case control study would be needed to illustrate this relation better.Surgeons at CHBAH need to familiarize themselves with the current classification of perineal tears and to document them as such.
112
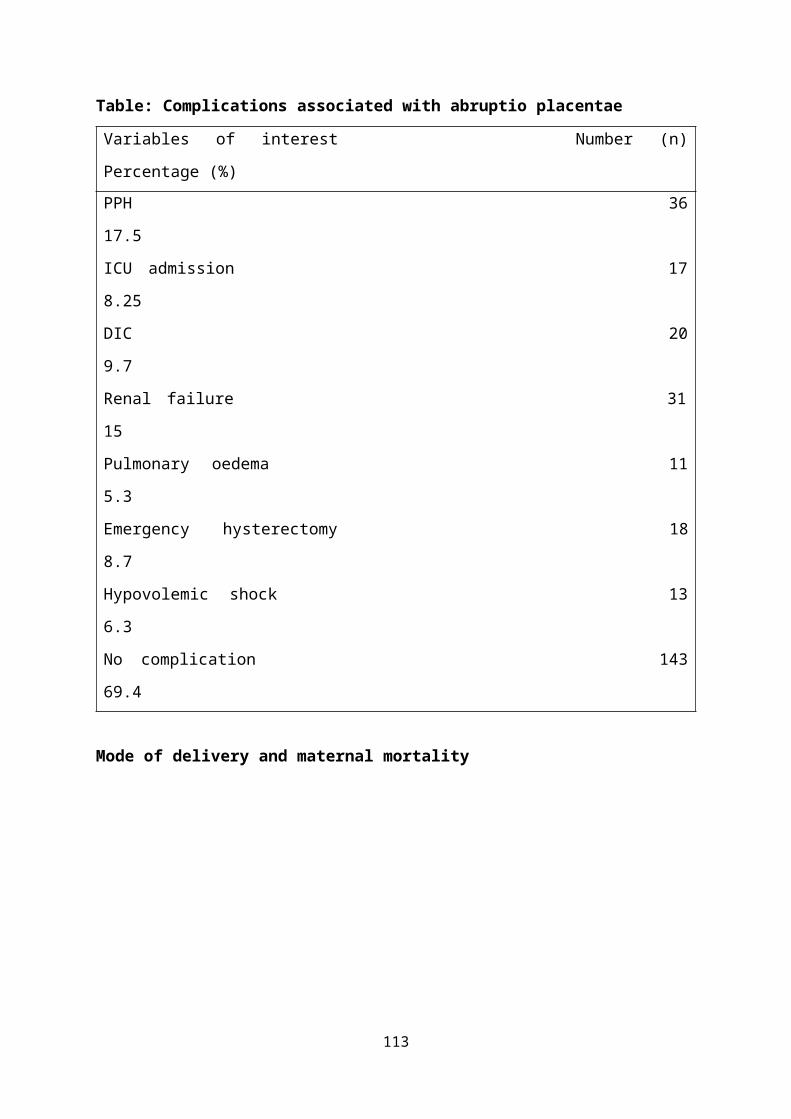
Post-operative care is good at CHBAH, the majority of patients received antibiotics as well as stool softeners. There was a 33% loss of follow up, which is significant considering a small study population (n= 60) to begin with.The 3% of patients that were not repaired primarily, at 12 weeks the patients hadn’t been repaired due to lack of theater time. At 6 and 12 weeks they experienced a full spectrum of sequelae (leakage of gas, liquid and solid stool). This further highlights the importance of primary repair, a golden opportunity to get the patients repaired and healed.
Strengths It was a prospective study Follow up at 6 and 12 weeks post repair.
Limitations Follow up at 6 and 12 weeks was done by means of a telephonic
interview. Some participants changed contact details without informing the researcher.
Hawthorne effect: Behaviour patterns changed as soon as doctors learnt of an ongoing study.
Pre-delivery symptoms of AI were not sought for prior enrolling patients into the study
We excluded women under the age of 18, for ethical reasons. It would have also been fruitful to be able to track down the
symptomatic patients post repair to the surgeon as per level of expertise.
113
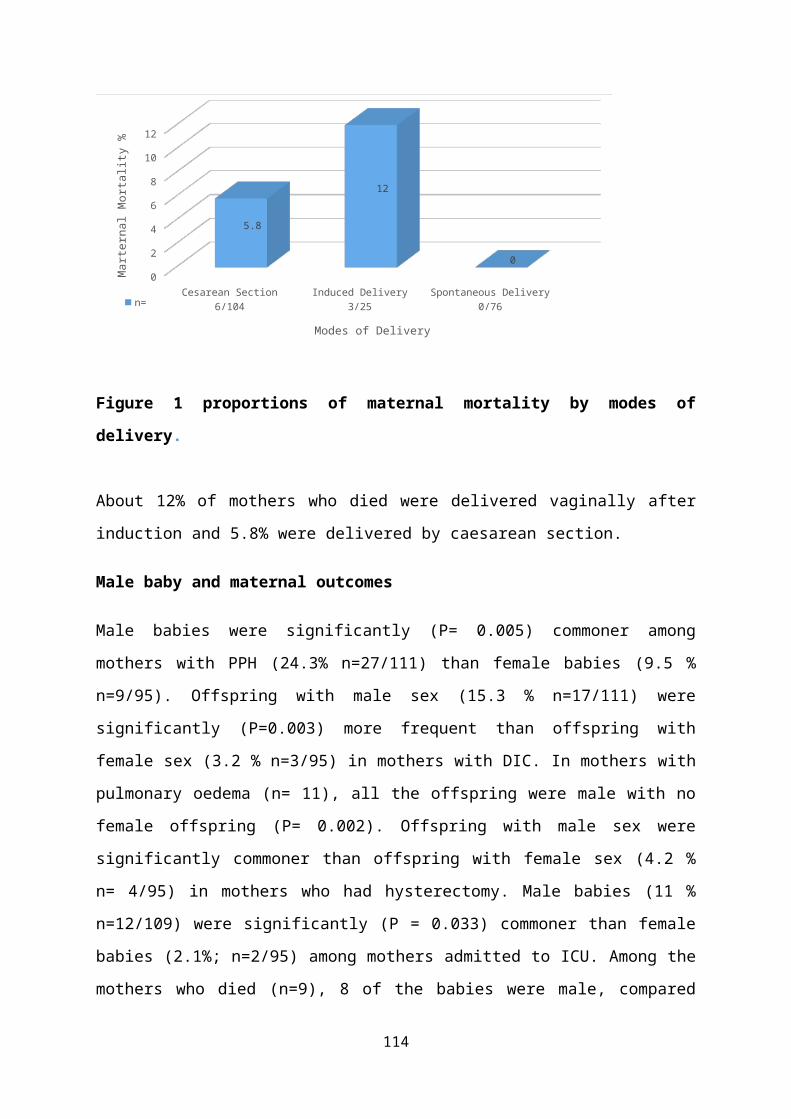
USING FAST AS MONITORING TOOL FOR NEWBORN CARE: EXPERIENCES IN LIMPOPO PROVINCE
PL Mashao, Dr Anne Robertson and Dr Joy Summerton
BackgroundThe Essential Newborn Care (ENC) Toolkit contains Norms and Standards and a Comprehensive Assessment Tool for Newborn Care. UNICEF and NDOH requested that a simpler tool be developed that would allow the DCST to assess, support and monitor newborn care, and assist provinces, districts and facilities in planning.The Health Systems Approach needed to be incorporated as well as the HHAPI-NesS recommendations of NaPeMMCo.FAST Includes :
• H-Health systems• H- Human resources• A-Asphyxia• P-Prematurity Quality of care• I-Infection• Nes – Neonatal survival strategy (monitoring)• S-Social mobilisation,
IntroductionLINC has focussed on the DCSTs as the vehicle for improving newborn care. LINC has developed, piloted and adapted the Facility Assessment and Support Tool (FAST). The comprehensive tool follows the HHAPINesS approach and it is based on the norms and standards of the newborn toolkit. The FAST includes tools to identify bottlenecks for each of the HHAPINesS pillars, and templates to help facility management and DCSTs develop interventions to address identified bottlenecks as well as track improvement in newborn care at a facility and district level on a quarterly basis. The FAST applies the Appreciative Inquiry Approach (AIP), which focuses on capitalising on what works well, rather than only identifying what does not work well.
114
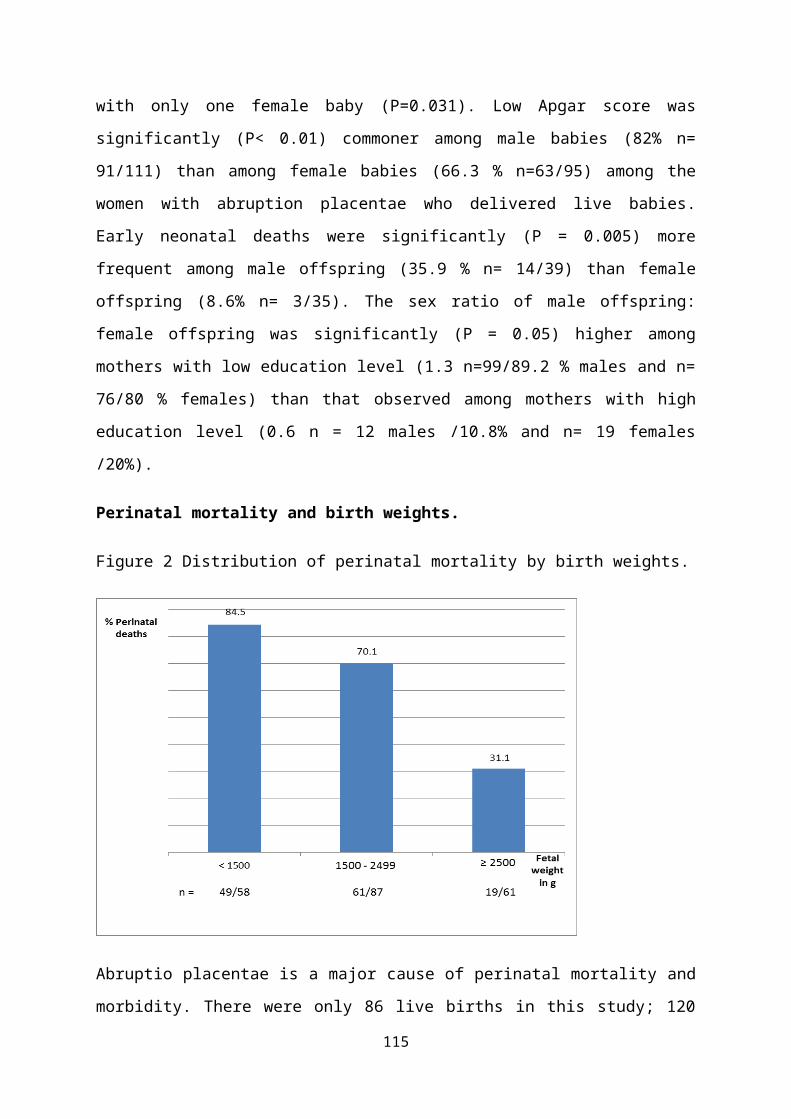
A bottleneck analysis dashboard has also been developed to interpret the scores of the FAST and it is tracked quarterly as part of M&E. DCSTs and facility management find the dashboard most useful to give them a quick and easily interpreted visual summary of how they fair in newborn care.The Limpopo provincial plan was completed in 2014 in consultation with the MCWH directorate. Limpopo’s strategy to support the development of district plans through district-specific planning workshops facilitated by the provincial paediatrician and provincial neonatal coordinator, worked well. DCSTs and facility management were capacitated to develop plans that are realistic, focused and measurable. All 5 districts of Limpopo have submitted newborn implementation plans that have been aligned to the provincial newborn implementation plan.
Elements of the FAST toolHealth SystemsLeadership of the facility and unitFunding and planning
• Infrastructure• Equipment• Drugs and Supplies
Human resources• Numbers according to N&S• Rotation
115
DISCOVER
DREAM
DESIGN
DELIVER
• Coverage of ESMOE, HBB, MSSN
Asphyxia• Readiness for Resuscitation• Quality of intrapartum care TBD
Premature care• Clinical Audit• CPAP availability and use• Antenatal steroids
Infection • Handwashing and other measures• Breastfeeding and routine care in Postnatal• MBFHI status and progress
MethodA health system tool, based on the pillars of the health system was developed for the DCST to assess, support and monitor newborn care and to help them identify and score bottlenecks as very major (red) significant (orange) minor (yellow and none (green). All 5 districts are using Fast tool to assess newborn care in Limpopo.
Progress, achievements and challengesThe FAST includes an M&E framework to track progress in newborn care at a facility level. It includes tracking scores on the HHAPINesS pillars on a quarterly basis (includes key national PPIP/DHIS indicators). An M&E framework has also been developed for tracking progress at district and provincial levels. DCSTs are being supported and mentored to complete the M&E framework, interpret data and support facilities to develop improvement plans based on data.
116
H- Health System N=7 N=7 N=7 N=6*(of 8) n=8 District (M) District (L)
Leadership
86% 64% 75% 60% 28% 100% 80%
100% 28% 100% 60% 71% 100% 100%
43% 43% 50% 60% 57% 100% 100%
2 1 1 0 44 1
1 0 1 0 22 1
Infrastructure > 80%51% 68% 45% 62% 63%
80% 86%
Equipment>80% 47% 66% 61% 56% 61%
85% 80%
>80% 91% 92% 78% 62% 88%86% 80%
>80%66% 66% 65% 73% 70%
88% 76%
Facility Plan and VisionSnr Doctor in NNUNeonatal Unit manager
Paediatricians in Reg Hosp / DCST
3 in regional 1 in DST
Obstetricians in Reg Hosp/DCST
3 in regional 1 in DST
Infrastructure assesnment FAST 2
Equipment assessment FAST 3
Supplies and drugs
Drugs and supplies FAST 4
Infection control
Infection Assessment FAST 5
H- Health System
N=7 N=7 N=7 N=6*(of 8) n=8 District (M) District (L)
Leadership
86% 64% 75% 60% 28% 100% 80%
100% 28% 100% 60% 71% 100% 100%
43% 43% 50% 60% 57% 100% 100%
2 1 1 0 44 1
1 0 1 0 22 1
Infrastructure > 80%51% 68% 45% 62% 63%
80% 86%
Facility Plan and VisionSnr Doctor in NNUNeonatal Unit manager
Paediatricians in Reg Hosp / DCST
3 in regional 1 in DST
Obstetricians in Reg Hosp/DCST
3 in regional 1 in DST
Infrastructure assesnment FAST 2
H- Health System N=7 N=7 N=7 N=6*(of 8) n=8 District (M) District (L)
Leadership
86% 64% 75% 60% 28% 100% 80%
100% 28% 100% 60% 71% 100% 100%
43% 43% 50% 60% 57% 100% 100%
2 1 1 0 44 1
1 0 1 0 22 1
Infrastructure > 80%51% 68% 45% 62% 63%
80% 86%
Equipment>80% 47% 66% 61% 56% 61%
85% 80%
>80% 91% 92% 78% 62% 88%86% 80%
Facility Plan and VisionSnr Doctor in NNUNeonatal Unit manager
Paediatricians in Reg Hosp / DCST
3 in regional 1 in DST
Obstetricians in Reg Hosp/DCST
3 in regional 1 in DST
Infrastructure assesnment FAST 2
Equipment assessment FAST 3
Supplies and drugs
Drugs and supplies FAST 4
The two (2) hospitals used as examples of good improvement are an example of successful implementation of suggested changes at facility level.
117
A- Asphyxia TargetDistrict A District B District C District D District E Hospital A Hospital B
N=7 N=7 N=7 N=6*(of 8) n=8 District (M) District (L)
A-asphyxia
> 80% 74% 72% NA NA NA 100% 80%
TBD NA NA NA NA NA NA NA
> 80% 100% 63% 81% 51% 33% High 90%
> 80% 100% 47% 89% 26% 67% High 90%
< 15 26.3 21.7 18.5 28.2 20.7 14,7 16,2
2 5.7 4.7 5.1 6.3 5.7 3,3 5.2
815.7
13 11.816.3
15,76 10,8
Resucitation equipment
FAST 10
Intrapartum care
HBB coverage
ESMOE coverage
Still Birth Rate
NNMR > 2,5kg
NNMR> 500g
Most DCSTs and facilities supported by LINC are still not fully competent in using PPIP. LINC needs to intensify this support so that data is accurate and used for decision making. This support will be included in the extension proposal.DCSTS’s in all 5 districts demonstrated confidence and interest in using Fast tool. In addition, the M&E framework needs to be aligned to facility, district and provincial newborn implementation plans. DCSTs need to be supported to ensure alignment of these two processes and thus to report against these. The M&E framework with completed 2014, and 2015 data for LINC supported facilities in Limpopo is attached. According to the DHIS Neonatal Mortality data for Limpopo (2013-2014) shows a decline in mortality rates.
Lessons from evaluationPaediatric DCST’s are using the FAST tool and the HHAPI-NeSS dashboard FAST has helped with facility Assessment, planning and monitoringAll facilities in 5 districts of Limpopo have submitted newborn implementation plansBottlenecks have been identified – and include
• Leadership• Allocation and Rotation of staff• Training does not lead to implementation – need to address all
bottlenecks and provide mentoring
118
• Intrapartum care is a problem, and bottlenecks causing that need to be unpacked
Using quarterly indicators is not useful –• Too much variation – do annual or biannual• Monthly and quarterly raw data, mortality reviews and audits
DCSTs are showing better leadership due to the Appreciative Inquiry Approach(AID) and having tools to guide them with facility support visitsDCST are using data from the HHAPI-NesS dashboard to advocate for resources such as equipment, drugs and supplies and human resourcesFacility management are more receptive to change when they have an objective assessment of their level of compliance to norms and standards, and when the AIA is applied Lower mortality rates in districts where DCST and management are effectively applying the non-rotation policy for LINC-MSSN trained staff
Suggested improvementsIntegrated Maternal and Neonatal ToolUse existing maternal health components e.g. staffing, training, Antenatal steroids, routine careDeveloped comprehensive maternal health componentUsed by all role players – Managers and DCST – and supported by administrative sectionInfrastructure, equipment and supply section is done in detail annually using the ENC toolkit
Human resource sectionManagement (CEO, Clinical and Nursing Managers) responsible for a staff establishment and non-rotation and then support training and development and monitoring coverageInclude a formal mentoring plan and mentoring tools post training – DCST responsibleCommunity engagement needs to be strengthened in the service and in monitoring.
119
Look at developing an APP so data uploaded at facility level and by different role players can be analysed at district and provincial level
120
ConclusionThe Facility Assessment and Support Tool (FAST) is a valuable tool to support newborn care improvement. Bottlenecks are identified. Maternal care can be integrated. DCST’s to focus on clinical support components. Management to be responsible for Health Systems components. Information to support Data elements. Further work on the tool will make it a valuable tool to support Maternal and Newborn care at Facility.
121
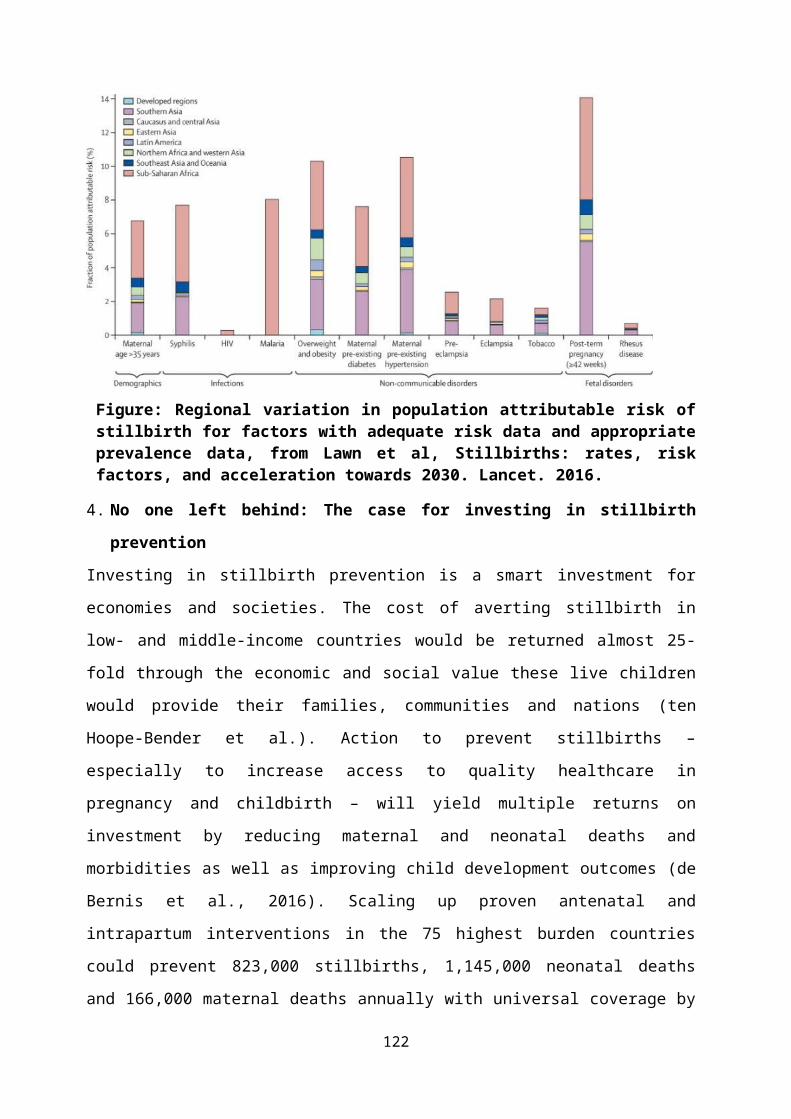
KWAZULU-NATAL INITIATIVE FOR NEWBORN CARE (KINC): A MIDPOINT EVALUATION OF A PROGRAM TO IMPROVE NEWBORN CARE IN DISTRICT HOSPITALS IN KWAZULU NATAL (ABSTRACT)
Phakathi SA, Haskins JL, Horwood C, Nyasulu D.
Introduction Infant mortality in South Africa (SA) is unacceptably high with a substantial number of deaths occurring during the neonatal period. The KwaZulu-Natal (KZN) Department of Health (DoH) has adopted KINC to improve newborn care, using a three-pronged approach of training, mentoring and accreditation.
MethodologyA comprehensive survey tool was completed in all 38 district hospitals in KZN at baseline and after 18 months of KINC implementation. In order to compare performance among participating hospitals and between baseline and follow-up, we generated performance scores for hospitals. A score for resources was based on data about staffing; equipment; infrastructure, and consumables. A care practises score was generated from data on admission policies; monitoring and evaluation activities; record keeping; appropriately deployed equipment; kangaroo mother care and postnatal care. Hospitals were also scored for availability of resuscitation equipment. Scores were combined to calculate an overall score for each hospital. Results The average score increased from baseline to follow-up in each of the 3 domains. There was a positive change of 28.0% for resources, 11.9% for care practices and 24.5% for resuscitation equipment. There was an increase in the resources score in 34/38 hospitals, in the care practices score in 30/38 hospitals and in the resuscitation score in 34/38 hospitals. The hospitals were scored out of a total of 90 points: at baseline the average score was 42.5 which increased to 53.5 at follow up, an increase of 20.6%.
Conclusions Hospital performance on provision of newborn care improved over an 18 months period of KINC implementation.
122
INSIGHTS INTO HEALTH CARE WORKER PERCEPTIONS AND ATTITUDES OF WORKING IN NEONATAL HIGH CARE UNITS
Aurene WilfordCentre for Rural Health
South Africa has one of the highest neonatal death rates in the world (Lozano et al., 2011). Some research refers to this issue as a silent epidemic (Mayosi et al., 2012). A recent study cited 14 576 neonatal deaths recorded on the SA National Perinatal Problem Identification Programme (PIPP) data base, between January 2012 – December 2013 from 588 PPIP sites (2012-2013 Saving Babies Report, 2014). Many of these deaths occur in community health centres and district hospitals (Saving Babies 9th report, 2012-2013). Strides have been taken by the Government to improve quality of care (QoC) for newborns and to decrease their mortality and morbidity rates. In KwaZulu-Natal (KZN) programmes like the KwaZulu-Natal initiative for Newborn Care (KINC) programme spanning three years (2013-2016) is one such way of trying to assess and improve service provision and care. This was a large quantitative facility review. However, there are aspects of care not considered in a quantitative analysis. It is the softer observational aspects of care that also need to be considered in trying to understand the QoC. Our study forms part of the larger quantitative KINC facility review and uses a qualitative embedded case study design. This study used structured and unstructured observations, photographs and in-depth interviews, so as to more comprehensively understand the complex issues surrounding QoC amongst neonates in SA. This presentation is an analysis of in-depth interviews that were carried out on registered nurses in the district hospitals. We found that overall nurses felt under-resourced, cramped and unsupported in their role and work in a high pressure environment, where many cope by making contingency plans to get through their days. Regardless of such difficulties, all nurses interviewed had an altruistic attitude to their jobs. When asked what they like about working in the nursery one nurse said:
123
Nurse: I like babies… I like to see them getting better…I have got a strong bond with the babies that’s what I can say.
Working with babies is difficult and stressful by its nature. One nurse said:Nurse: a baby has to be observed…because when we are admitting the baby in the nursery there is no doctor there, there is no case sheet that’s coming to tell you….this is respiratory distress, this is convulsion, this is hypoglycaemia, it all your observation. So with that I think um yah the staff is scared
In observations it was found that these nurses worked very hard, and in the interviews they all felt exhausted, unsupported and overworked.
Nurse: It’s very hard to work here in SA as a nurse… we are everything… I put up drips, take blood, I’m a nurse, I’m a Dr, I’m a nurse I’m a porter… I take bloods to lab… I’m also a data capturer, if I need to do something on the computer...
Another nurse spoke specifically of workload saying:Nurse: Since 2005 our workload has tripled… too many babies…
Nurses felt that some Drs do not have the skills to manage premature or sick babies. This results in nurses feeling unsupported and often had to make crucial decisions alone.
Nurse: most of the doctors …they don’t always understand the babies’ specific complication …you find that they don’t know what treatment to be given to this baby, what actions supposed to be taken for these babies you know…babies are like mismanaged and end up dying because they do not know what to do.
Nurses shoulder a lot of responsibility in counselling, they feel unsupported. In one interview the nurse described what she does:
Nurse:…I take the mother to a private room…Mama you know your baby is sick hey? The Drs and nurses are doing their best for baby to be better…
Another nurse on asking how dealing with mother distress affected her responded saying:
Interviewer: the mother distress must be difficult for you?Nurse: ehe…mmm… I need a clinical psychologist… hey… stress….
124
Nurses felt unsupported by doctors in terms of their workload also:Nurse: And with the …she just leaves everything for me. I think you saw that I’m taking bloods, it not my work to take bloods, it not my work to do the IVs the putting up of the drip but for the sake of the patients I just do it
All nurses in every hospital we visited expressed that they were short staffed.
Nurse: This work affects me physically… it affects my family…I have to just say ok they are short staffed they are calling
Such responses show nurses feel unsupported by the health system. Many high care nurseries are structurally small and nurses are acutely aware of overcrowding issues and infection. Countless times we heard similar concerns as the one below:
Nurse: In the nursery it’s very small … it’s very small…there is no space
Another said:Nurse: Ah sometimes we run short of the beds because its overcrowded
When asked how they deal with this shortage of space, it was verbalised that they prioritise:
Interviewer: So what do you do…? Do you give some (babies) to the mothers to keep because there are no enough beds?Nurse: Yes … you prioritise, you see those that are not that sick.
Another nurse said:Nurse: Yes because you can’t chase admissions away and say no we full we not taking babies. We can’t! We have to take the baby even if we are full and see what we can do.
Additionally, referral hospitals are unsupportive and often overcrowded, leaving district hospitals to care for tiny babies without adequate equipment.
Nurse:… Sometimes we have babies that needs to go to level 2 at [referral hospital] and when they are full we have to stay with that baby and there is nothing more that we can do because that baby
125

needs to be ventilated, we do have a CPAP machine but some other babies are very sick and need to be ventilated so we don’t have one. If they are full at [referral hospital] we have to stay with that baby and to see that baby dying is sad.
Despite the daily stresses that nurses faced, they made contingency plans and tried to cope with the situation at hand. Other than space issues, nurses dealt with other infrastructural challenges such as access to plug points; phones and computers. There were also logistical issues and stores issues that were hospital specific that added to stress on a daily basis for nurses. One nurse said the following:
So we have no BCG not water for irrigation, so I told pharmacy to please write a letter saying that in this hospital we don’t have that…so I pinned it here in nursery.
Many hospitals were affected by water shortages too. Additionally, there was insufficient equipment in many high care units. Nurses do the best they can with what they have but are acutely aware of the care they are giving. Generally, nurses all worked as a team and felt supported by their matrons. However at a higher management level, the nurses felt unsupported.
Nurse: The leadership and management is very poor
They knew their concerns were taken up by management and that management were aware of the concerns, yet nothing ever happens.
Nurse: They do listen but there are no actions taken, so I don’t know if they listen or pretend to be listening to you but there are no actions taken.
Somewhere in the hospital system, the messages get lost and the status quo does not change.One nurse spoke of going to training, feeling empowered yet coming back and not being able to change the situation:
Nurse: They tried and send us for training but when we come back we were willing to change things but we can’t!
126
Nurses felt added pressure and workload when mothers were non-compliant to hospital hygiene standards or when mothers did not listen regarding care of the baby.
Interviewer: Do you often get mothers who are no compliant with your (sanitation) protocolNurse: Yes we often get, that’s why I go and ask did you watch your hands, did you spray your hands etc.
This requires nurses to constantly check up on mothers and make sure they are complying. Nurses also verbalised that the teenage mothers required extra care and instruction in the care and feeding of their baby. Overall, nurses felt overworked and unsupported in their roles due to many factors. Nurses make contingency plans to deal with challenges. The high care units were all too small to accommodate the demands. Further, management need to develop skills in coping with specific issues. Peer support at higher levels, like action learning, could improve management of the units. Additionally, the non-rotation of staff is crucial to the sustainability of newborn care and consideration needs to be given to the issue of staff retention in such a stressful environment.
127
USING DISTRICT STRUCTURES FOR STRENGTHENING KANGAROO MOTHER CARE SERVICES: A CASE STUDY FROM TSHWANE DISTRICT
Elise van Rooyen1,2, Anne-Marie Bergh 2, Ute Feucht1,3, Rinah Skhosana31Department of Paediatrics, University of Pretoria; 2SA MRC Unit for Maternal and Infant Health Care Strategies, University of Pretoria; 3Tshwane District Clinical Specialist Team
IntroductionComplications of prematurity are a major contributor to neonatal death rates (41%) and under-five deaths (14%) in South Africa. One high-impact, low-tech, cost-effective intervention to reduce neonatal mortality and morbidity is kangaroo mother care (KMC). There is currently a global drive towards accelerated implementation of facility-based KMC services, with a target of >75% of babies with birthweights of <2000g to receive KMC across the world by 2025.
In the Tshwane District (Gauteng Province, South Africa), changes in district boundaries and health system re-organisation resulted in not all hospitals having been part of previous KMC training initiatives (4 of 8 hospitals by 2013). With the expanding population in the district and subsequent rise in number of deliveries, obstetric and neonatal services at tertiary and regional hospitals became increasingly congested. Additionally, the four district hospitals frequently up-referred babies to higher levels of care, but very few down-referrals occurred, which negatively impacted on the already existing neonatal bed shortages.
AimThe aim of the presentation was to describe a quality improvement (QI) initiative undertaken in 2013-2015, using KMC as an entry point for improving neonatal care in the Tshwane District. The presentation illustrated how the Tshwane District Clinical Specialist Team (DCST) was instrumental in accelerating KMC implementation and leveraging partner-ships with other district structures, including the nutrition and maternal-
128
and-child health sub-directorates. The project was done in conjunction with experienced local KMC implementers, without any additional funding.
The projectFigure 1 gives an overview of the sequence of events included in the initiative over a period of 18 months. There were three one-day workshops that were attended by a multidisciplinary team from each hospital (doctors, nurses, dieticians and other allied health workers), as well as a multidisciplinary team from the district, including nutrition and mother-and-child health officials. Each workshop had the following components:• report from each hospital on the achievements and challenges in terms
of KMC implementation; • skills building sessions; and • development of an action plan for each hospital.
Figure 1. Sequence of activities
In the periods between the workshops hospitals in the early stages of KMC implementation undertook benchmark visits to hospitals with comprehensive and established services. Eight months after the first workshop, each hospital received a walk-through support visit that served as an in-service capacity building opportunity for hospital staff and the district supervisors. Additionally the progress in terms of KMC implementation was measured with a standardised tool. All activities reflected a non-hierarchical approach in the spirit of on-going mentoring.
Did we make a difference?
129
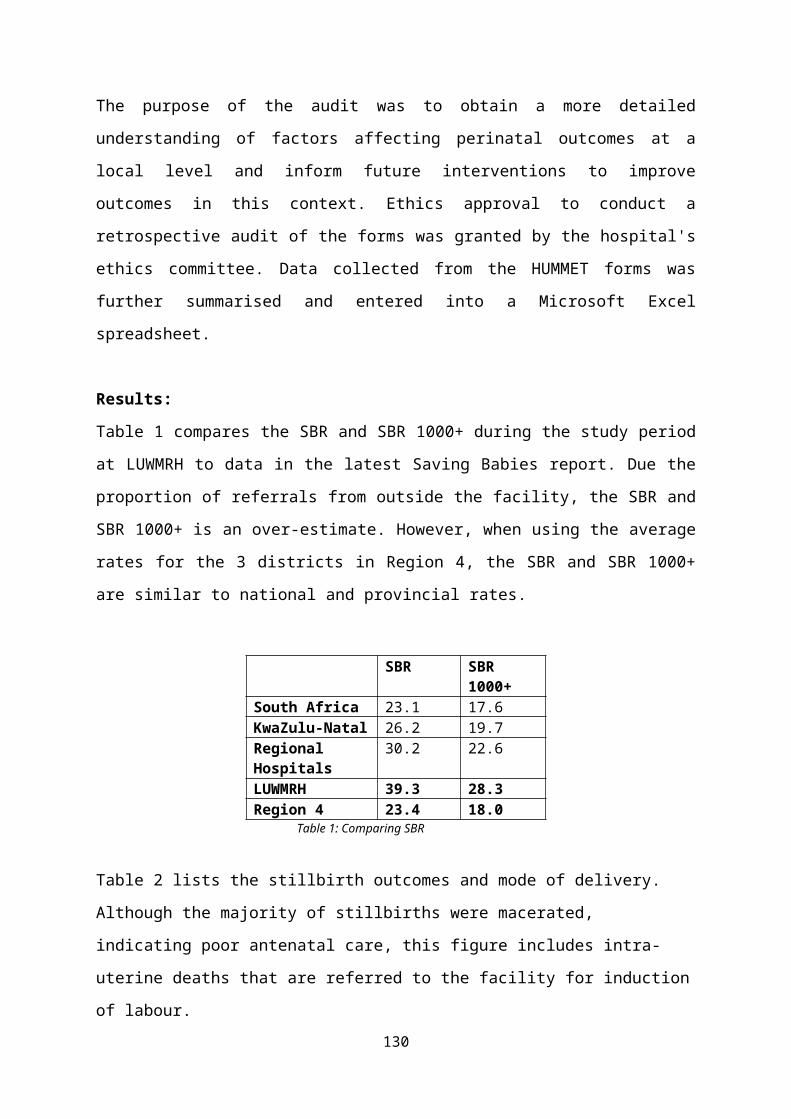
Although the full impact of QI initiatives are difficult to measure objectively, a number of observations were made. For example, district hospitals nearly doubled their KMC bed capacity, as depicted in Table 1.
KMC implementation status in the Tshwane District was plotted on the stages-of-change model (Figure 2). This indicated that two hospitals had reached the level of sustainable practice, while three hospitals performed on the level of integration into routine. One hospital demonstrated evidence of practice, while the other two hospitals scored just below this level.
Other observations included the following: • a high degree of interdisciplinary transfer of learning;• staff empowerment;• visible improvement in staff morale and enthusiasm during the project
period;• in-facility KMC ownership through the promotion of home-grown
solutions;• strengthened in-facility KMC collaboration (including allied health
workers like dieticians, occupational-, speech- and physiotherapists); and
130
Table 1. Increased bed capacity in district hospitals
Figure 2. Overview of performance of hospitals on the stages-of-change model
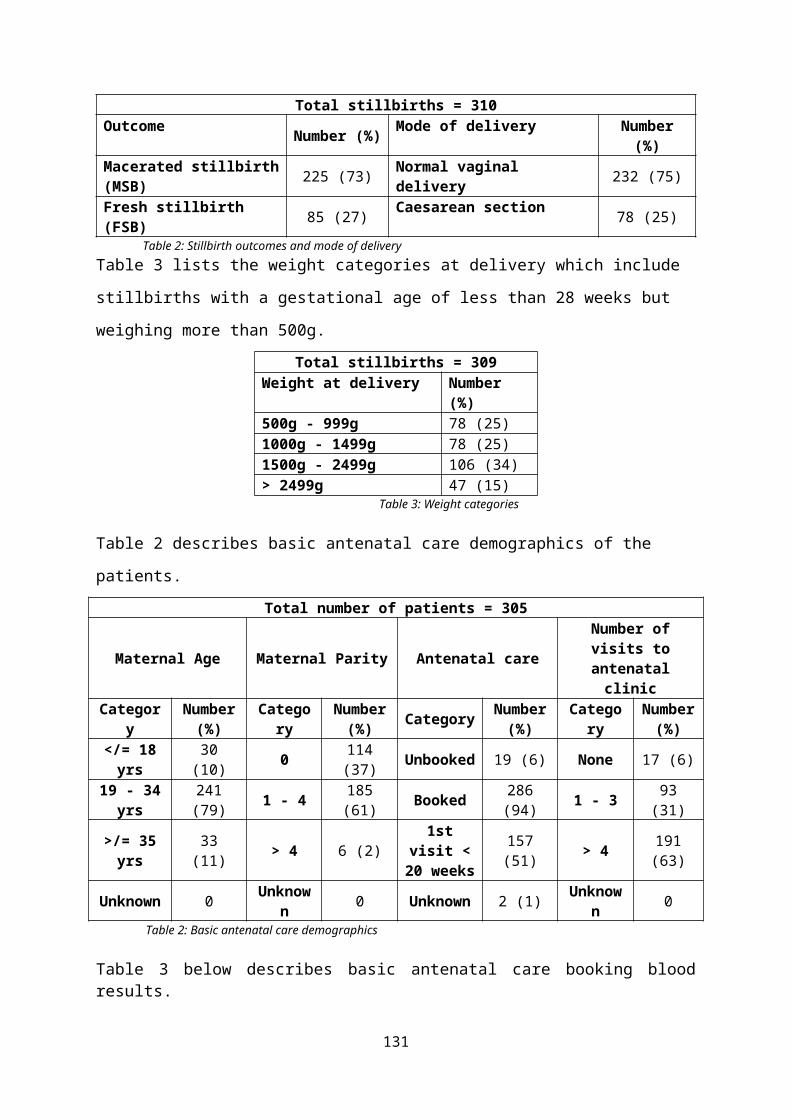
• improved collaboration between tertiary and district hospitals, including:‒ more down-referrals to district hospitals, and‒ cross-referrals between hospitals for specialised neonatal follow-up
services (e.g. ophthalmological examinations and cardiac sonography).
ConclusionThe KMC quality improvement initiative provided the potential for combining clinical expertise, mentoring and health systems improvement. The team approach had the potential to effect change, with interdisciplinary knowledge transfer enabling health systems improvements on a larger scale. The permanent presence of the DCST in the district allowed for continuous supportive supervision with a view to promoting accountability, mentoring and follow-up beyond a once-off project. The KMC environment also provided the time and space for integration of other maternal and child health services for high-risk populations (e.g. family planning, HIV prevention and immunisation services).
131

NON-INVASIVE OVERNIGHT MONITORING OF FETAL AND MATERNAL SLEEP PATTERNS (ABSTRACT)
Fifer, WP 3 , Odendaal HJ1, Lucchini M2,3, Myers MM3
1. Department of Obstetrics and Gynaecology, Stellenbosch University2. Politecnico di Milano 3. Departments of Psychiatry and Pediatrics, Columbia University, New York City
IntroductionRecently, epidemiological studies of singleton antepartum stillbirth have been directed at the risk factors associated with maternal physiology. A study in New Zealand reported a 2.54-increased risk for of late stillbirth (>28 weeks gestation) in mothers sleeping on the back, and 1.74-increased risk in those sleeping on the right side, compared in both instance to the left side the night before. A study in Australia of stillbirth at 32 or greater weeks gestation observed a 6.24 increased risk of stillbirth for supine sleep compared to the left side. Growth restriction was more prevalent in the stillbirths to women reporting sleeping on the back. The working hypothesis resulting from these findings is that the inferior vena cava and aorta may be less likely to be occluded in pregnant women who are in the left lateral position. Monitoring both fetal and maternal heart rate during sleep as a function of sleep position could shed light on the mechanisms underlying this putative risk.
MethodsMaternal heart rate (MHR) and fetal heart rate (FHR) were recorded overnight at home using the Monica AN24TM device, which was also used for physiological assessments in the Safe Passage Study (www.safepassagestudy.org). Maternal sleep position and movement was recorded using the Zephyr Biopatch device. This provided the opportunity to look at MHR and variability and FHR patterns as a function of maternal sleep position. A cohort of 100 maternal fetal dyads at 34-38 weeks gestation provided data during overnight sleep in the home which ranged from 6-9 hours. Measures of long and short term HR variability were summarized for both fetus and mother. Fetal sleep state was assessed via visual inspection of fetal HR acceleration patterns.
ResultsMaternal heart rate changed as a function of sleep position with the highest heart rates observed while in the supine position. The lowest MHR was seen in the left lateral position. Maternal heart rate while in the right lateral position was intermediate and significantly higher than that observed while in the left sided position. No significant differences were seen in fetal heart by position, though robust changes in both FHR and FHR variability were observed as a function of fetal sleep state codes. Circadian changes in both FHR and MHR were seen with heart rates decreasing over night for both mother and fetus. Fetal heart was lower in state 1F (quiet sleep) then in either 3F (active sleep) or 4F (active awake). Changes in FHR patterns following maternal position change are currently being examined.
ConclusionsWe report the first evidence, to our knowledge, of variation in maternal and fetal heart rate patterns as a function of maternal sleep position in the natural (home) environment. Robust circadian patterns were observed for both mother and fetus. Further analysis incorporating fetal sleep state codes, maternal and fetal movement patterns and the effect of alcohol and maternal smoking and other
132
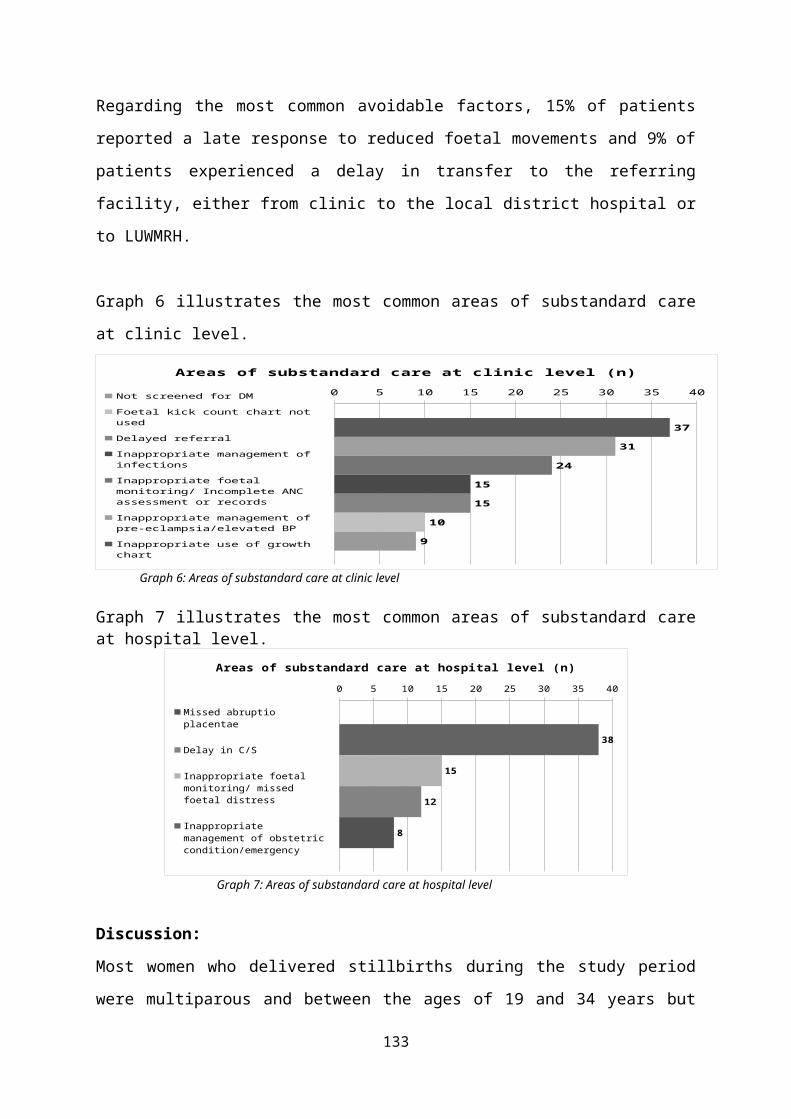
adverse conditions will be forth coming. Further studies are also needed to explore possible mechanisms such as positional effects on maternal cardiac output and blood pressure that may elicit alterations in fetal heart rate and autonomic activity and possibly confer risk for stillbirth. This research was funded by the grants from the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the Sackler Institute of Developmental Psychobiology.
133
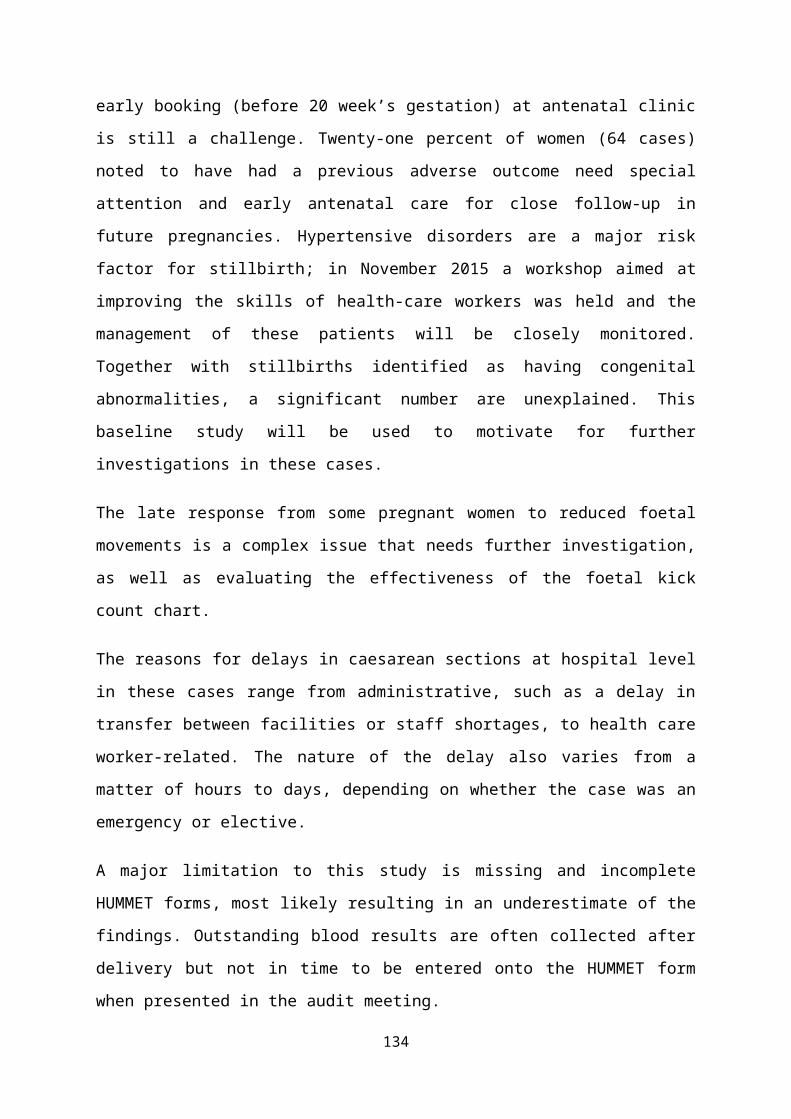
THE WESTERN CAPE PROVINCIAL 1st 1000 DAYS INITIATIVE: A PERINATAL CARE PRIORITY
Malek E*#, Goeiman H#, Marais F#, Champion M#, Naledi T**, Arends E#@ (*Department of Paediatrics, Tygerberg Hospital & Faculty of Health Sciences University of Stellenbosch; #Western Cape Health Department 1st 1000days Initiative EXCO, ** Western Cape Health Department Chief Director Health Programs, @ Western Cape Health Department Director Women’s Health Program)
IntroductionThe unique window of opportunity during the first 1000 days of life (from conception to the end of the second year of life) is recognised globally. Neuroscientific advances have defined three core areas of influence critical to this period, namely nutrients (nutrition and health), relationships (interaction with caregivers who in turn are supported by healthy communities), and environmental aspects (both intra-uterine and beyond).
The effects of toxic stress (defined as unrelentless overwhelming adversity experienced by the caregiver resulting in continuous stress response of the infant) during and following pregnancy, on the developing infant brain, results in that infant developing permanently distorted stress responses, poor social skills and diminished achievement of scholastic and economic potential. In essence, the community surrounding the pregnant mother is to her what the uterine environment is to the infant.
Infant attachment is affected by the response of the mother to her infant’s cues, and these are signifiantly distorted in mothers who are experiencing toxic stress due to mental health problems, intimate partner violence and/or who are addicted to substances. The effects of toxic stress on the infant can be buffered by the presence of stable, responsive caregiver relationships. Supporting families for responsive, positive parenting is key to development and violence prevention.
Many studies have highlighted concerns around the high rates of intimate partner violence, maternal depression and anxiety as well as related addictive behaviours such as smoking, alcohol and substance abuse by pregnant women in the Western Cape. Clear statements of intent by the Western Cape Provincial Government to address these were made during the Western Cape Provincial
134
Summit on Improving Wellness held in November 2011 and have subsequently incorporated in the Western Cape Health Care 2030 Plan which aims to broaden the focus of its activities from only that of illness towards promoting wellness. The Western Cape Provincial Government has adopted five Transversal Strategic Goals for the 2014-2019 Provincial Strategic Plan (PSP), (Figure 1). Provincial Strategic Goal 3 (PSG3) aims to increase wellness and safety and reduce social ills towards ensuring inclusive, safe, resilient and healthy communities, youth, families and children. One of the strategic priorities for PSG Goal 3 is to have safe and healthy children and one of the key interventions to realise this strategic priority is to optimise opportunities in the first 1000days of life, toward optimising this critical period of infant brain development.
Figure 1 Figure 2
Method An intersectoral Provincial Strategic Parent, Infant and Child Health and Wellness (PICH) working group (WG) was established (with terms of reference) as a platform for the provision of technical and operational support to promote
135
caregiver (maternal/parental), infant and child wellness, whilst adopting an inclusive “all of government” and “all of society” approach. This strategic approach allows for a public health approach to optimise opportunities to focus on upstream factors.
The role of the Parent, Infant and Child Health and Wellness working group has emerged as a transversal forum of various government services departments, academia, researchers and NGO partners to guide the agenda around the First 1000 Days.
Results (outputs to date) First 1000 Days advocacy has led to it being prioritised in the Provincial Government of the Western Cape as one of 7 key projects within Strategic Goal 3 for the term 2014 to 2019. This is clearly being showcased as such to the broader public in provincial information hubs and on the official provincial webpage. The Western Cape First 1000 Days Initiative Communication campaign was officially launched by the Western Cape Provincial MEC for Health on 17 February 2016.
A transversal communications strategy for the First 1000 Days Initiative has included the Western Cape Departments of Health, Social Development and Education and includes (i) an external public awareness campaign aimed at caregivers and for which a unique identifier was developed (see Figure 2) with branding of vehicles and magazine inserts, and (ii) an internal awareness campaign aimed at health and other sector staff through a series of Roadshow workshops and materials. A set of 1st 1000day Initiative key messages to inform the transversal communications campaign were developed by the Working Group for both external and internal stakeholders
The Western Cape Health Department has been mandated as the lead department in the intersectoral PSG3 cluster with the First 1000 Days Initative has become a lead project adopted by the Health Department. A mandated, non-vertical project governance structure for the 1st 1000 day Initiative is in place in context of bigger transversal structural arrangements, and coordinates the activiites relating to the three main domains (Communications, Health and Intersectoral).
136
A framework for the 1st 1000 days Initiative has been developed spanning across the life cycle to map gaps in existing services impacting on the 1st 1000days time period and to address gaps (incl policy, practice and outcomes) in the three core areas related to the First 1000 Days Initiative (Figure 3)
An implementation package including a staff orientation & training participatory workshop package and toolkit is being developed for health (and other sector) employees working with adolescents, pregnant women and their partners/families, as well as parents and caregivers of young children.
Extending the current service package during Antenatal care is the main focus for 2016 and includes the development and testing of maternal psycho-social risk screening tools and referral pathways at primary health care Basic Antenatal Care clinics and Midwife Obstetric units, and at community household worker level, as well as building additional topics into the existing infant feeding counselling checklist used during antenatal care (to include aspects the RTHB, parenting preparedness, and maternal mental wellbeing and supportive partner/family relationships).
A new provincial postnatal health care policy and checklist has been developed and has included infant mental health screening questions and other components relevant to the 1st 1000days Initiative.
A monitoring and evaluation strategy is being developed, using the MCHN&N Dashboard indicators as a basis and exploring additional measures including audits and social development indicators. A number of partnerships non-governmental organisations and intersectoral collaborative projects are being explored, toward strengthening parenting and support for mothers within the first 1000 days of life (ranging from strengthening community worker programmes to offering parenting support to extending health departmental policy on providing support to breastfeeding women in the workplace to all other government departments), and includes collaboration with site-specific integrated service delivery models to strengthen referral pathways for service support for pregnant women with alcohol, substance abuse and
137
smoking addictions, intimate partner violence/domestic abuse, and maternal psychosocal stressors and mental health problems.
Figure 3
ConclusionsHigh level recognition of, interest in and support for the 1st 1000days Initiative as an example of a transversal government initiative has been obtained. This has been a key enabler for improving the quality and scope of service delivery during pregnancy and the first two years of life at all levels. Senior provincial managers are now being held accountable to their respective institutional contributions to the First 1000 Days Initiative and related services via the performance management system.
Although many related service components are being delivered, the opportunity now provides for the significance of these to be acknowledged and the quality improved. Many gaps have been identified and these are now being systematically addressed. Clinicians providing care for women before and during pregnancy and to infants and children during the first 2 years of life have a key leadership and advocacy role in advancing societal awareness and promoting shared responsibility for optimising the critical opportunity for optimal brain development during the 1st
1000 days of life toward addressing complex social issues.
138
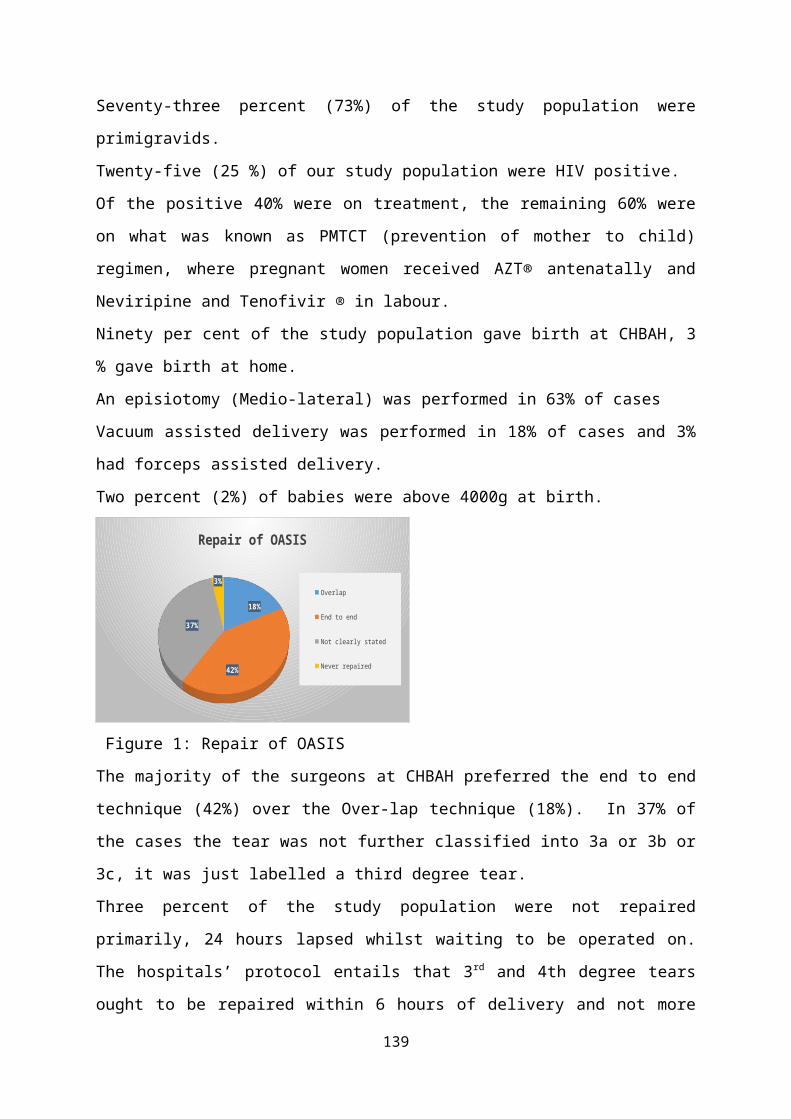
INACTIVE CLINICAL GOVERNANCE: IS IT THE PRIMARY CAUSE WHY LIMPOPO IS STILL STRUGGLING TO END PREVENTABLE MATERNAL DEATH? (ABSTRACT)
Shisana BaloyiChief Specialist and Head of Clinical O&G Limpopo Department of Health, NCCEMD Member.
Background:South Africa did not meet the MDG 4&5 targets though the recent sixth saving mother report 2011-2013 showed some decline in maternal mortality. This decline is accounted to the reduction in NPRI deaths. Also worrying is the escalating C/S haemorrhage related mortality. Evidenced based key intervention strategies to end preventable maternal deaths were generated for application to improve the quality, coverage and implementation of care. This includes PHC re-engineering including the DCSTs, the WBOTs, ESMOE-EOST and the numerous protocols guidelines, monographs and programmes produced by the NCCEMD to guide and improve practice.Despite all this interventions Limpopo Province is struggling to reduce maternal mortality significantly. Some districts performances have been a mixture of good, bad and worse. More worrying is that some of the worst performers were districts that are well resourced and covered in terms of the above intervention packages.
Objective:To identify best practices from the districts which demonstrated progress in reducing preventable maternal mortality.
Methods:A retrospective comparative descriptive audit of the maternal deaths from 2011-2015 in four rural districts, 24 district and 5 regional hospitals of Limpopo was conducted. This investigation was conducted in two parts; the first part is an observational study to determine the trend in maternal mortality for the 2011-2013 triennium and 2014. The second part is an audit of all maternal death files for January – December 2015.Each district was paired with a district with similar intervention packages for comparison on their maternal mortality and each maternal death file was assessed against the Dashboard for Implementation of Key Interventions Ending Preventable Maternal Death (DIKIE PMD). DIKIE PMD assess the quality, coverage and implementation of maternal care. DIKIE PMD is a checklist constructed from Saving mother’s recommendations of 2011-2013; CARMMA Assessment Dashboard and locally produced recommendations. Interviews were held with managers of institutions where maternal death occurred during 2015 for information not available in the file.
Findings and Conclusions: All the basic requirements that are needed are generally in place to
improve maternal care in Limpopo. The quality of maternity care in the province is poor, marked with
prolonged and irregular abnormal monitoring, managing patients at an inappropriate level and a considerable delay in seeking senior assistance.
Patients are transferred or referral is considered very late when the patient has reached irreversible state so that the patient can die outside of the facility where the treatment was initiated. An attempt to make the maternal death for another referral facility.
Serious skills and knowledge gap among the Community service doctors. Non-compliance to CD standards have contributed to maternity mortality.
139
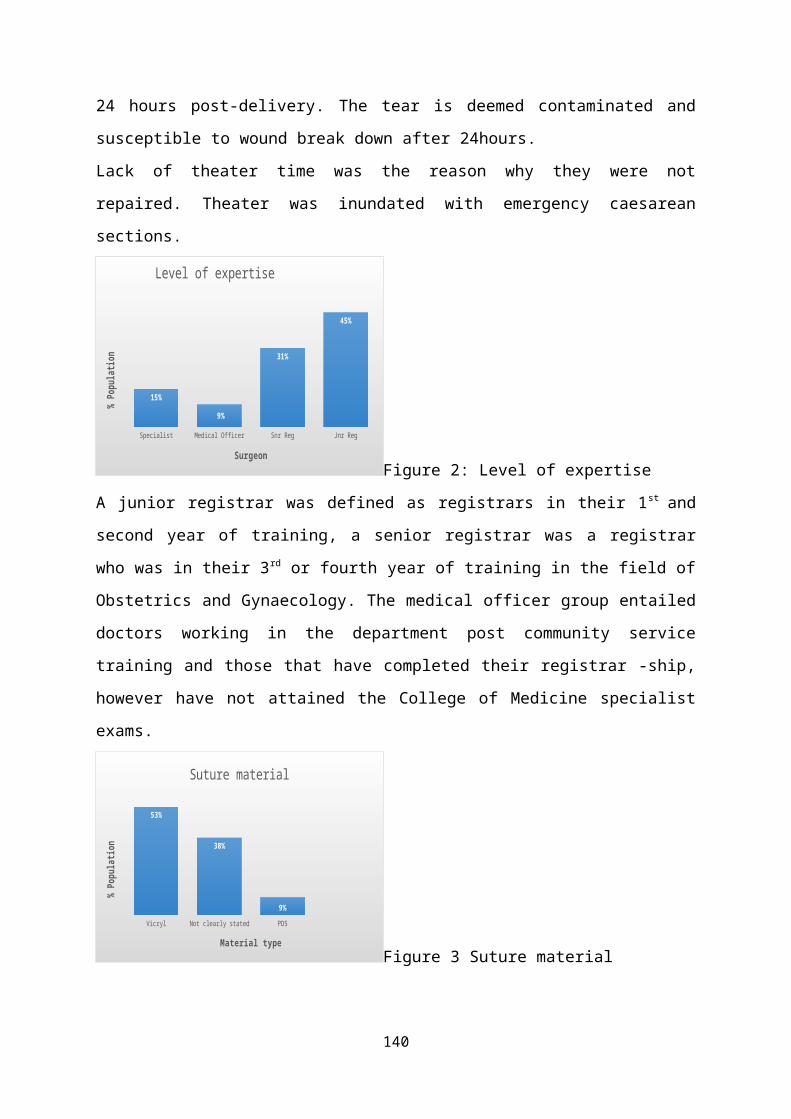
Action audit cycle is not completed. Inactive Clinical Governance can be one factors affecting interventions’
sustainability. Clinical Governance and Supervision deserves a serious attention in Limpopo. Protocols dissemination should be supplemented by workshop and mentoring of healthcare workers.
DCST role is not yet fully excercised, the team is still confused especially the Family Physicians Primary Health Care component. Workshop and mentoring of this group is necessary.
Recommendations.Training of O&G interns in Limpopo has to be stopped until the training and supervision has been restructured. The process of implementing the Saving Mother recommendations in the health care institutions should be monitored regularly and be part of supervision and outreach activities. The DCST is well placed to ensure compliance by ensuring attendance at all review meetings and providing clinical governance by responding to issues arising from review meetings.Better strategies for monitoring progress of implementation of the recommendations should be devised. Reporting and investigation of adverse outcomes Near miss) may assist health authorities to implement relevant quality assurance programs in maternal and neonatal services.Sessional doctors with no skills in managing pregnant women and are unwilling to be trained should have their contracts.Quality improvement of medical notes is the responsibility of clinical managers and supervisors in facilities and should be ongoing.
140
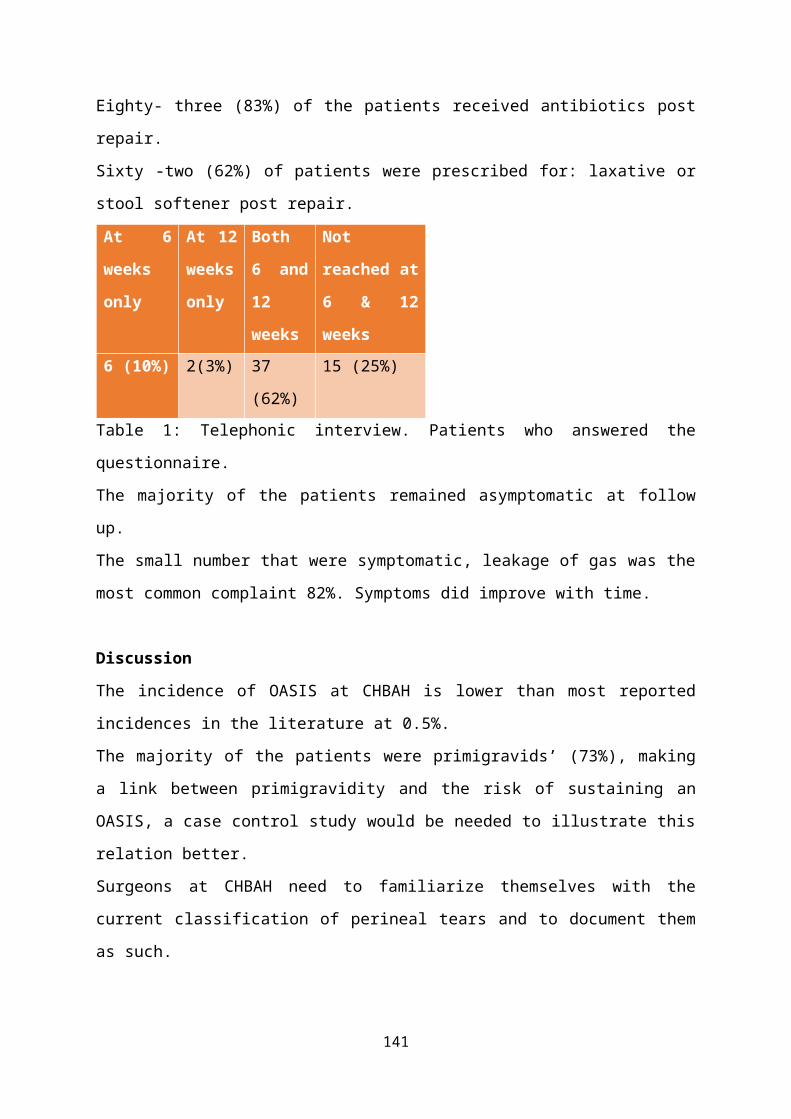
PROVISION, UTILISATION AND FUNCTIONALITY OF MIDWIFE OBSTETRIC UNITS IN FIVE DISTRICTS IN KWAZULU-NATAL (ABSTRACT)
Voce, AS, Public Health Medicine, University of KwaZulu-Natal
IntroductionIncreasing the proportion of deliveries with skilled birth care in an enabling environment contributes to lowering maternal mortality ratios. Increasing the proportion of midwife-led deliveries contributes to increasing the proportion of deliveries with skilled birth care. The promotion of midwife-led deliveries is in line with evidence that supports midwife-led care as a safe, cost-efficient option of choice for the management of low-risk pregnancies and deliveries. In order to increase the proportion of midwife-led deliveries, and to improve access to skilled birth care and to life saving interventions closer to where women live, the KwaZulu-Natal Department of Health implemented a policy in 2012, of promoting Midwife Obstetric Units (MOUs). Three-years post-inception of the policy, an assessment of the utilisation of the MOUs in five districts was commissioned by the KwaZulu-Natal Department of Health, with a view to informing further policy implementation. The assessment had the objectives of: (1) Establishing the availability and geographic distribution of MOUs; (2) Ascertaining the utilisation of MOUs; and (3) Determining the functionality of MOUs.
MethodsAn observational, descriptive, cross-sectional survey, utilising both primary and secondary data, was implemented. Primary data was collected on-site in five districts, at each of 25 MOUs, utilising a facility-review checklist, between mid-July and end-August 2015. Secondary data was garnered from data routinely captured in the District Health Information System. The dimensions measured included: the availability and distribution of MOUs; the utilisation of MOUS; and the functionality of MOUS, in terms of: type of MOU, infrastructure, staffing, Basic Essential Obstetric Care signal functions, availability of functional equipment and drugs and supplies, and emergency referral support and the utilisation of obstetric ambulances.
ResultsOverall, there appears to be an oversupply of delivery sites per population in each district. More specifically, there appears to be an undersupply of MOUs and an oversupply of Level 1 delivery sites. MOUs are generally underutilised, with only 4 of the 25 MOUs (16%) conducting an average of > 50 deliveries per month. With regard to functionality: the 25 MOUs in the five districts under investigation are stand-alone delivery facilities, providing a full range of maternal health services, from antenatal to postnatal care. None of the MOUs had back up for interruptions in water and electricity supply. Generally there were unsafe staffing allocations, when assessing ADM coverage, midwife allocation to labour wards, rotation practices, and day/night staffing distributions. None of the MOUs could perform six of the assessed Basic Essential Obstetric Care signal functions; 52% MOUs had an equipment functionality index of <0.80; 24% MOUs had a drug availability index of <0.80; and 28% had experienced stock-outs in the last three months. Furthermore, there was inadequate emergency referral support, a function of both a weak referral system and inadequate inter-facility emergency transport.
DiscussionThe number and distribution of delivery sites requires a district-by-district analysis, taking into consideration population distribution, population density, and terrain and transport routes. In the determination of the required number
141
and distribution of MOUs per district, a hybrid approach to the establishment of MOUs may need to be implemented (both stand-alone and alongside). The number and distribution of delivery sites per district has implications for staffing and equipping of, and the provision of emergency referral support, to MOUs. Furthermore, the number of delivery sites affects the utilisation of MOUs. Currently, MOUs in the Five Districts are underutilised, and fall short of the estimated proportion of deliveries that could be midwife-led in South Africa, contributing to birth care that is both unsafe and not cost-effective. However, the MOUs are not fully functional, and therefore promoting public utilisation of the MOUs is ethically questionable. Interventions for ensuring appropriate availability and distribution, and ensuring functional MOUs are required at various levels of the health system in order to strengthen the policy directive, the operationalization of policy and the management of MOUs in the Province.
142
BARRIERS TO OBSTETRIC CARE AMONGST MATERNAL NEAR MISSES (ABSTRACT)
P Soma-Pillay, RC Pattinson
BackgroundAccess and timely referral to appropriate obstetric care is an important component of the health-care system. A significant proportion of serious obstetric complications occur in women without any recognisable risk factors. These patients are sometimes unaware of their disease pathology and may encounter further delays in the health system before finally accessing appropriate treatment.
Aims and objectivesThe objective of the study was to determine the delays/barriers in providing obstetric care to women who are classified as a maternal near miss.
MethodsThis was a descriptive study at Steve Biko Academic Hospital, a tertiary referral hospital in Pretoria, South Africa. One hundred cases of maternal near misses were prospectively identified using the WHO criteria. The “three delays model” was used to identify the phases of delay in the health system and recorded by the medical physician caring for the patient.
ResultsOne or more factors causing a delay in accessing care were identified in 83% of near miss cases. First and third phase delays were the most important causes of barriers. Lack of knowledge of the problem (40%) and inadequate ante-natal care (37%) were important first phase delays. Delay in patient admission, referral and treatment (37%) and sub-standard care (36%) were problems encountered within the health system. The above causes were also the most important factors causing delays for the leading causes of maternal near misses - obstetric haemorrhage, hypertension/preeclampsia and medical and surgical conditions.
ConclusionMaternal morbidity and mortality rates may be reduced by educating the community about symptoms and complications related to pregnancy and training healthcare workers to identify and manage obstetric emergencies.
143
ASSESSMENT OF THE EFFECTIVENESS OF A ONE DAY TRAINING PROGRAMME TO IMPROVE KNOWLEDGE OF OBSTETRIC EMERGENCIES IN EMS PERSONNEL
D Barnard*, AM Bergh*, JD Makin*, RC Pattinson**MRC Maternal and Infant Health Care Strategies Unit, Obstetrics and Gynaecology Department, University of Pretoria.
IntroductionThree ministerial committees work under the Department of Health to record and reduce maternal and child mortality namely National Committee on Confidential Enquiry into Maternal Death (NCCEMD), Perinatal Problem Identification Program (PPIP) and Committee for Morbidity and mortality in Children (CoMMiC). These committees have identified three pillars for improving preventable maternal, perinatal and child mortality. The pillars are knowledgeable and skilled health care providers, appropriately resourced health facilities and rapid inter-facility transport. The quality and speed of inter-facility transport play an important role in continuity of care and directly impacts on maternal and perinatal care. The effect of efficient transport has been well studied in the developed world, developing countries, and in systematic reviews, showing improved outcomes in maternal and perinatal care when obstetric transport improves.
AimA pilot study to test a one day workshop aimed at Basic Life Support (BLS) and Intermediate Life Support (ILS) personnel to assess if knowledge improves after the workshop.
SettingBLS and ILS personnel in Polokwane, Mpumalanga, South Africa
MethodsAfter obtaining the scope of practice of Emergency Medical Services (EMS) personnel the ESMOE (Essential steps in management of Obstetric emergencies) course was adapted into a one day training programme. This was trialled on Advanced Life Support (ALS) recruits. The programme was adjusted and then tested on BLS and ILS recruits. Prior to the training, all participants completed an anonymous pre-test multiple choice assessment of knowledge. The same test
144
was repeated at the end of the training day and the results for pre-test and post-test compared to assess improvement in knowledgeResults20 EMS personnel attended the interfacility 1 day workshop and all completed the pre- and post-test.
Pre-test mean score
Post-test mean score
BLS
4.27 6.63
ILS 5.22 7.44Mean difference in total score 2.29 points. P value = 0.00220 EMS personnel attended the interfacility 1 day workshop and all completed the pre- and post-test.
Pre-test mean score Post-test mean scoreBLS 4.27 6.50ILS 4.50 7.11
Mean difference in total score 2.42 points. P value < 0.001
DiscussionThe distribution of EMS personnel in South Africa is BLS 66.68%, ILS 29.04 %, and ALS 3.25%. The remainder is composed of Emergency Care Technicians (ECT) 1.03 %. The latter is an intermediate qualification, between ILS and ALS, only offered in some provinces. This distribution shows a bottom-heavy spread; with only 3 provinces having > 35 ALS qualified EMS personnel. All obstetric patients are classified as priority 1 (P1) and therefore qualifies for having an ALS trained paramedic as part of the ambulance crew. Due to the shortage of ALS personnel, obstetric patients are mostly transported by one BLS and one ILS crew member. If one looks at the scope of practice of the BLS and ILS personnel, one can see why this poses a problem to continuity of care. Medication administration allowed by EMS personnel scope of practice:
BLS ILS1 Activated Charcoal 1 Acetyl Salicylic Acid 2 Oral Glucose Powder/ Gel
2 Activated Charcoal
3 Medical Oxygen 3 β2 Stimulants 4 Nitrous Oxide : Oxygen 4 Dextrose 50%
5 Oral Glucose Powder/ Gel 6 Ipratropium Bromide 7 Medical Oxygen
145
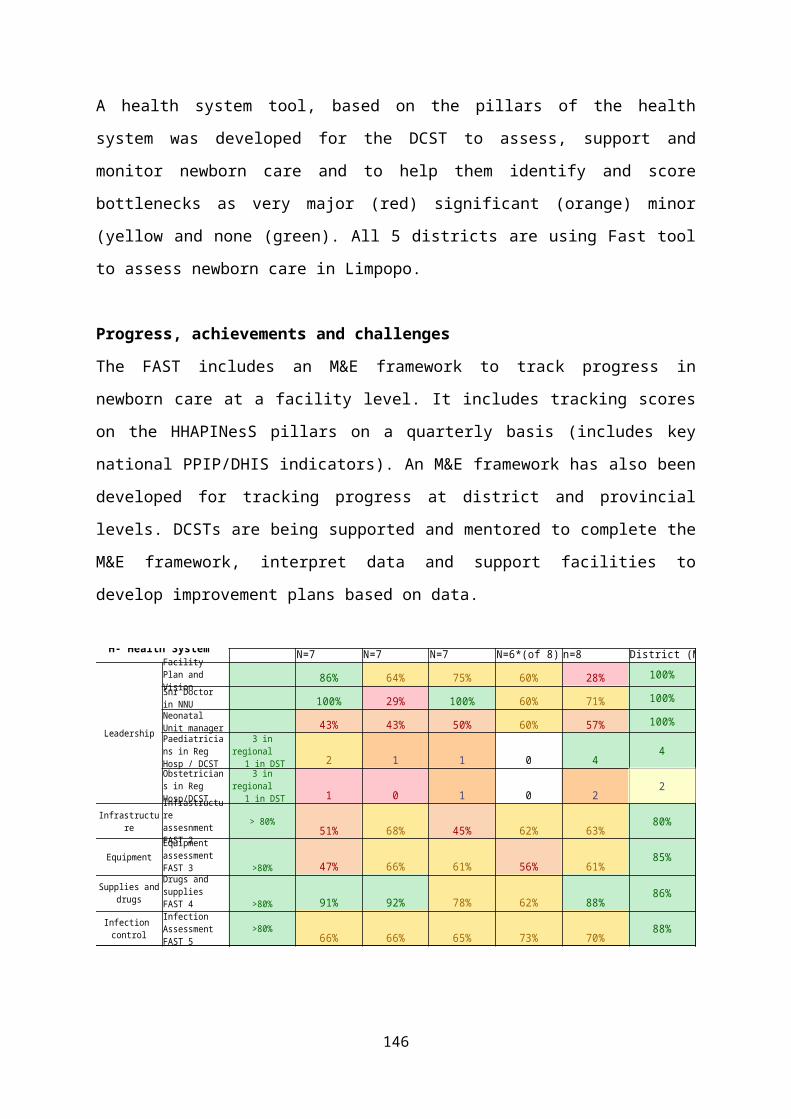
8 Nitrous Oxide : Oxygen
Neither BLS nor ILS can do bimanual compression, listen to the foetal heart, interpret foetal heart abnormalities, administer tocolysis, control blood pressure, or manage malpresentation, obstructed labour or cord prolapse. Neither can administer MgSO4, misoprostol, oxytocin or antihypertensives. BLS personnel cannot establish IV access or change the flow rate of existing IV fluid. Two broad groups of obstetric patients are transported by the EMS service namely pre-facility transport (where a patient is collected from home) and interfacility transport (between primary, secondary and tertiary levels of care). In both cases, patients are high risk. In the former, the patients have not been seen, diagnosed and stabilised by a midwife or medical doctor. In the latter, patients are often transferred to a higher level of care because they have already been identified as high risk. These patients are dependent on continuity of care and often require interventions to influence the outcome of both mother and neonate. Our data shows that the base-line knowledge of obstetric emergencies of BLS and ILS personal is low. If one analyses the marks achieved in the pre-test, the mean score was 4.56. This does not equate to 45.6%. The test is a True/False multiple choice-based questionnaire (MCQ). Any MCQ has a component of guesswork and therefore has an element of uncertainty. The uncertainty is displayed in two features. One is the reliability of test scores and the other is the reliability of interpretation of test scores. In a two-choice question, one can achieve a 50% mark by merely guessing. For this reason, a ‘pass mark’ should only be given if a test mark above 80% is achieved. Using this formula, a mark of 74%, which is the highest mark achieved in the post-test scores, equates to 38% knowledge. This low base-line knowledge in obstetric and perinatal emergencies, together with the limited scope of practice of the majority of EMS personal, makes continuity of care a pressing challenge.
ConclusionThe base-line knowledge of obstetric emergencies in EMS personnel is low. A one-day workshop is effective to improve this knowledge, however the scope of practice of EMS personnel does not allow for continuum of care of obstetric patients. This poses a substantial challenge in the quest to improved maternal and perinatal care.
146
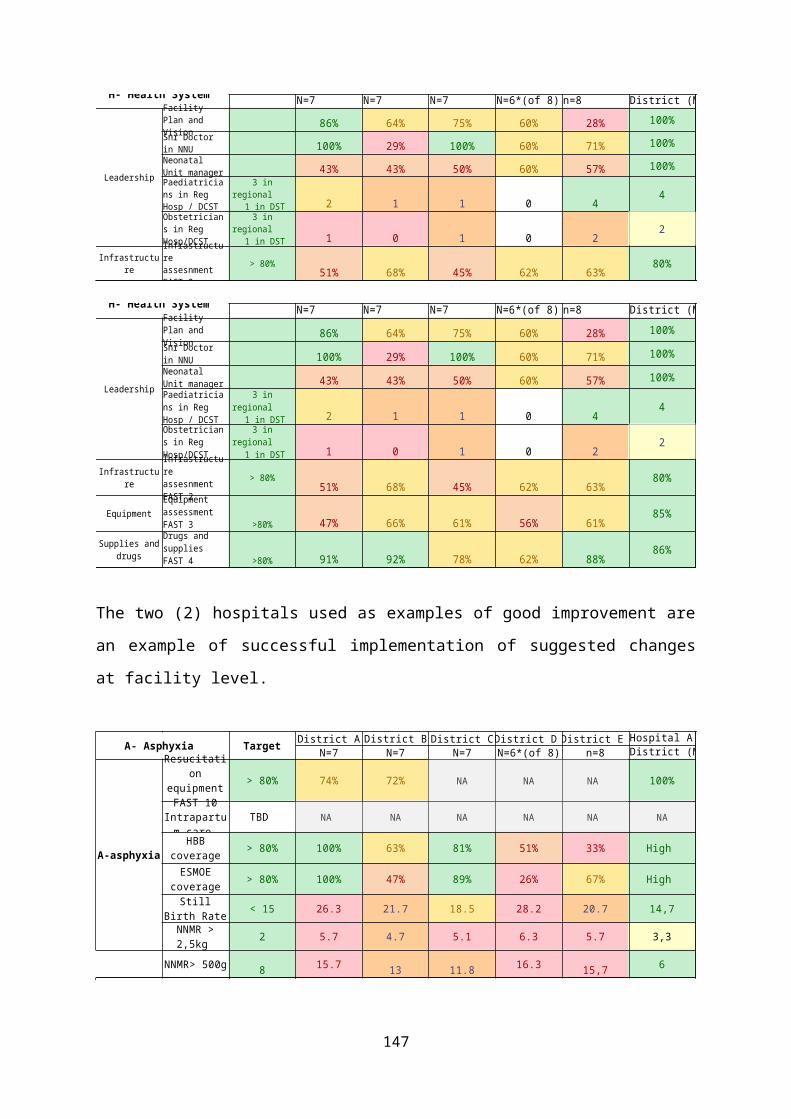
147
ESMOE-EOST SCALE-UP PROJECT: PRELIMINARY DATA ON IMPACT OF SCALE-UP
RC Pattinson for ESMOE-EOST teamSAMRC Maternal and Infant Health Care Strategies Unit, University of Pretoria; Centre for Maternal and Newborn care, Liverpool School of Tropical Medicine
Objective: To reduce stillbirths, neonatal and maternal deaths by improving emergency obstetric and neonatal care.
Method: The Essential Steps in Managing Obstetric Emergencies (ESMOE) – Emergency Obstetric Simulation Training (EOST) scale-up programme took place in the 12 “most in need” districts in South Africa from September 2012-December 2014. A baseline survey was conducted in the 12 districts from July to September 2012 and the survey was repeated one year after the training. Training took place by conducting a three-day and a two-day workshop per week for 6-9 weeks per district. A total of 3237 health care professionals (645 doctors, 303 advanced midwives, 2130 professional nurses and 159 other) were trained in 144 workshops (72 three-day and 72 two-day workshops). In each district more than eighty percent of the health care professionals involved in maternity care were trained.
Results: The knowledge and skills significantly improved in doctors by 17% and 33%,
respectively; in advanced midwives by 13% and 29%; and in professional nurses with midwifery by 16% and 31%.
148
There was a significant improvement in functionality of community health centres (CHCs) and district hospitals
o 92.3% of CHCs could perform at least 5 basic emergency obstetric care (EmOC) signal functions one year after saturation training compared with 34.6% before.
o 56% of district hospital could perform all 9 comprehensive EmOC signal functions one year after saturation training compared with 41% before.
149
More than half of the facilities had successfully introduced emergency drills (EOST exercises).
Significantly fewer maternal deaths occurred after saturation training to end 2014 compared with maternal deaths from beginning 2011 to before saturation training.
o The total institutional maternal mortality ratio (iMMR) decreased 22% from 217 before to 169/100 000 live births after saturation training (p<0.001; RR 0.78, 95% CI 0.67-0.90).
o The direct iMMR decreased 20% from 107.5 before to 86.0/100 000 live births after saturation training (p=0.042; RR 0.80, 95% CI 0.65-0.992).
Significantly fewer stillbirths and early neonatal deaths occurred after training to end 2014 compared with baseline to saturation training.
o The perinatal mortality rate (PNMR) for babies ≥1000g was 23.6/1000 births after versus 27.8/1000 births before (p<0.00001; RR 0.929, CI - 0.91 - 0.951).
o The PNMR ≥ 2500g 10.6/1000 births was after versus 11.6/1000 births before (p=0.027; RR 0.91, 95% CI 0.84-0.99).
150
Conclusion: The ESMOE-EOST scale-up programme has fulfilled all the Kirkpatrick criteria required for the successful introduction of a programme. ESMOE-EOST should be scaled up to the remaining districts and hard-to-access populations like sessional doctors, nursing tutors, emergency services personnel and private hospitals.
151

COMMUNITY ENGAGEMENT: A KEY STRATEGY INTERVENTION IN REDUCING OBSTETRIC MORBIDITY AND MORTALITY
Klaas Mongalo 1 , Phophi Ramathuba2, Shisana Baloyi3, Makgabo4, Herkie Sandenbergh5, J Maphalu6, Robert Sirwali7, Ntsie Kgaphole8, Aldina Ntsewa9, Ntodeni Ndwamato10, Linah Maepa11, Raymond Omoighe12, MachikeTthobejane13, Owo14, Mulimisi Ramavhuya15, Eddy Mhlanga16, Elizabet Matidze17, Muleya181Senior MO and Head of Maternity Voortrekker Hospital Limpopo,2 MEC for Health Limpopo Province,3 Chief Specialist and Head of Clinical O&G Limpopo DoH, 4Provincial Co-ordinator for Traditional Health Care Practitioner Limpopo DoH, 5DCST Obstetrician Mopani Limpopo DoH , 6DCST Obstetrician Waterberg Limpopo DoH, 7District Executive Health Manager Vhembe, 8SGM DHS Limpopo DoH, 9District Executive Health Manager Waterberg, 10Chief Specialist and Head of Clinical Family Medicine Limpopo DoH, 11District Executive Health Manager Sekhukhune, 12DCST Family Physician Sekhukhune Limpopo DoH,13 District Executive Health Manager Capricon, 14DCST Family Physician Waterberg Limpopo DoH, 15DCST Family Physician Waterberg Limpopo DoH, 16Chief Specialist and Head of Clinical O&G Mpumalanga DoH, 17ASGM DHS Limpopo DoH,18
Principal MO and Head of Maternity at Elisras Hospital.
BackgroundLimpopo has been experiencing an increase in obstetric morbidity and mortality with community level avoidable factors. Some were arising from the traditional health care practitioners (THP) activities e.g patients presenting in labour with potent uterotonics herbal medication which causes precipitate labour, morbidities related to unsafe termination of pregnancy, advise and treatment of HIV AIDS complications, THP remedies related perinatal morbidity and mortality such as liver toxicity and renal failure. Parturant patients could present to labour ward having taken herbal medication containing potent uterotonics, the patients complicates with post-partum haemorrhage due to uterine rupture or secondary uterine atony and poor fetal outcome from intrauterine fetal hypoxia. Slow progress in achieving the MDGs in some other countries was attributed to the failure to incorporate community participation into health programmes. Rosato et al recommended that community participation was important in supporting the provision of local health services and in delivering interventions at the community level. In over 40% of maternal deaths have community level avoidable factor. Findings by Lasi et al in a Cochrane review of 18 Cluster randomized trial showed that community based packages significantly reduce maternal morbidity by 25%, neonatal mortality by 24% and stillbirth by 16%, and also increased healthy behaviours such as referrals for pregnancy-related complications and early breast feeding.Eighty per cent of the maternal deaths were related to direct obstetric causes such as severe bleeding (haemorrhage), infection, complications of unsafe
152
abortion, eclampsia, and obstructed labour, with other social determinants like lack of access to healthcare, illiteracy and poverty. Maternal experience’s during her pregnancy journey, antenatal and intrapartum, has a direct bearing on the foetal outcome. With early recognition and intervention, the majority of maternal and neonatal deaths could be prevented. Community engagement trials conducted in Makwanpur, Nepal found some reduction in maternal and neonatal mortality of up to 88% and 72% respectively. But the same strategy in other trials has shown variable and non-significant impacts on maternal and neonatal outcomes.
AimThe aim this paper is to assess both the effectiveness of community-based intervention packages in reducing maternal, and perinatal morbidities and mortality and improving neonatal outcomes, as well as the impact of different strategies (home visitation, home-based care, community support groups/women groups, and so on) on reported outcomes by in increasing public health services utilisation.
Objective:The objective of the project was firstly to observe the effect of community mobilization on the public health facility services utilization by the community namely ANC visit before 20 wks, Couple year protection and contraception uptake, Cervical cancer screening coverage , Delivery in facility rate with Skill Birth Attendance(SBA), Mother Post Natal Care at 6 days, Choice of Termination Of Pregnancy(CTOP) uptake. Secondly to observe the impact on maternal and child health outcome association with community mobilization.: Still birth rate, Inpatient neonatal death rate, Institutional Maternal Mortality.A ‘community-based intervention’ can be defined as one that is delivered by any person within the community, including healthcare personnel or lay individuals, and implemented locally at the woman’s home, village or defined community, but not in a public health facility.
Method:Retrospective and prospective observational study in the 5 districts of Limpopo where community mobilization and Maternal and Perinatal Health Imbizos has been conducted between 2014-2015. Community engagement intervention
153
packages included additional training for outreach workers (community midwives, community/village health workers called ward based outreach teams (CHW/WBOTS)) , Traditional Health Care Practitioners (THP), Faith Based Healers, Traditional Birth Attendants (TBAs) in maternal care during pregnancy, delivery and in the postpartum period and in routine new born care. Additional training was defined as training other than the usual training that health workers receive from their governmental or non-governmental organisation and could include a combination of training in providing basic antenatal, natal and postnatal care; preventive essential new born care; breastfeeding counselling; management and referral of sick newborns. Interventions at Community level was establishments of WBOTs/CHWs who were engaged in education of patients/community and THP about the current status of maternal and child health in Limpopo, issues about primary health care, importance of early ANC, post natal visits care, HIV/TB information and encourage each member to know their HIV status, contraceptives choices, CTOP info, promoting skilled birth attendance, exclusive breastfeeding, early referral, motivating social worker intervention. Linking THP/FBH with Public Health Care Facilities. Establishing village health care watch groups within WBOTS who create a data of all pregnant women at the community, all HIV/TB patients and enforce compliance by Directly Observed Therapy (DOT).During community Imbizos participants were divided into various commissions to discuss improvement plan on the identified gaps contributing to poor maternal and child health outcome. All discussions from the various commissions were collated and summarised.Primary health outcomes assessed were indicators associated with public health services utilization by the community namely ANC visit before 20 wks, Couple year protection and contraception uptake, Cervical cancer screening coverage , Delivery in facility rate with Skilled Birth Attendance(SBA), Mother Post Natal Care at 6 days, Choice on Termination Of Pregnancy(CTOP) uptake. Secondary outcomes were reduction in maternal and perinatal morbidity and mortality. Maternal mortality is defined as number of maternal deaths per 100 000 live births. Maternal death is defined as the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management10
154
Neonatal mortality is defined as the number of neonatal deaths from any cause among total live births (early neonatal mortality includes deaths in the first week of life; late neonatal mortality includes deaths from seven to 28 days of life). Perinatal mortality is defined as stillbirths and early neonatal deaths. Stillbirth is defined as foetal death after 28 weeks of gestation but before delivery of the baby’s head per 1000 total births.
Results: Community members consulted were 2750 and comprised of WBOTS/CHW(1002), traditional health care practitioners (1200), faith healers (350), traditional birth attendants (150), councillors (40) and traditional leadership (8) of the local districts.
Table 1: Summary of the co-operation document synthesized with the Community and Public Health officials. Areas of Improvement by the Community discussed at the different commisions
Improvement plan agreed by the commissions during the Community Imbizos
1.How can the Community/WBOTs assist the PHC to improve health care services?2.How can community assist in the early booking of women to Antenatal Care services?3.How can the communities and THP & Faith Based Organisation participate and be involved in the reduction of child and maternal mortality in the district?4.What should the community do in order to improve Emergency Management Services (EMS) response times?5. Community participation in ensuring optimum use of public health facilities for family planning and CTOP.
1.Early referral to Public Health Facilities.2.Men to be actively involved in reproductive health issues and encourage those pregnant for early ANC booking, 3. Enhance THP, TBA & Faith Healers collaboration with Public health, Facilities, Traditional health practices to be regulated, CTOP only at Public Health facilities, local media & radio broadcast of agreed co-operation, promote contraceptives , early referral to Hospital, establish a THP regulatory body for accountability ,report unregistered & unscrupulous THP, discourage use of herbal remedies causing severe uterine contractions, be involved in health awareness campaigns, clinic committees and to be trained in health promotion4. Create space for Maternity waiting home for high risk pregnant mothers.5. Work on Public health personnel attitude, educate community about the dangers of unsafe TOP
155
ANC visit before 20 weeks increased by >10% more especially in districts with functional WBOTS. Facility delivery increased by 5%. CTOP at public health facilities increased by 15%. See Figure I-III.Institutional Maternal Death reduced by 14.9 %. From January to December 2015 there were 8(3.9%) cases of maternal deaths associated with THP remedies, 3 in Postpartum Haemorrhage secondary to uterine ruptures, 3 septic miscarriages complication from unsafe TOP by THP, one ectopic pregnancy who died at casualty brought by the THP for the ‘’drip’’ and one presented with liver failure probably due to herbal hepatotoxicity as there were no other underlying medical conditions and acute fatty liver disease of pregnancy(AFLP) excluded. Figure IVa- IVb.The biggest effect of Community Mobilization has been the increase in couple year protection and Implanon Insertion. Figure V-VI Postnatal visit, Cervical Cancer screening and still births are still areas requiring attention for improvement in Limpopo. Figure VII-X
CAPRICON MOPANI SEKHUKHUNE VHEMBE WATERBERG PROVINCIAL0
10
20
30
40
50
60
41.7
50.1
42.947.4 46.8
49.946.2
54.9
47.853.7
49.9 50.4
Comparison of Before and after COMMUNITY MOBI-LIZATION
2014 2015
AN
C V
ISIT
BEF
ORE
20
WKS
%
WBOTS WBOTS
Figure I: ANC Visit before 20 weeks .
156
CAPRICON MOPANI SEKHUKHUNE VHEMBE WATERBERG PROVINCIAL0
20
40
60
80
100
120
81.390.9 89.4 89.9
80.686.884.9
100.693.4 93
80.991
Comparison of Before and after COMMUNITY MOBI-LIZATION
2014 2015FACI
LITY
DEL
IVER
Y W
ITH
SBA
%
WBOTS WBOTS
Figure II: Facility Delivery with Skilled Birth Attendant
<18YS >18YRS <12 WEEKS
>12 WEEKS
TOTAL CTOP
02000400060008000
10000
739
7357 7822
274
8096
955
83568906
405
9311
Comparison of before and after COMMUNITY MOBILIZATION
2014 2015
CTO
P AT
PU
BLIC
FAC
IL-IT
IES
Figure III: CTOP at Public Health Facilities
157
CAPRICON
MOPANE
SEKHUKHUNE
VHEMBE
WATERBERG
PROVINCE
0
150300
347.8
160.78 164.97 132.06176.79 196.83
322.7
131.3 149.293.4
133.4167.4
Comparison of before and after COMMUNITY MOBILISATION
2013/14 2014/15iMM
R/10
0000
live
bi
rths
THP/FBHTHP/FBH
THP/FBH
Figure IVa: Institutional Maternal Mortality Rate
Figure IVa: Institutional Maternal Mortality Rate
Figure IV b: Institutional Maternal Mortality and the underlying causes.
158

CAPRICON
MOPANI
SEKHUKHUNE
VHEMBE
WATERBERG
PROVINCIAL
0204060
39.6 36.529.4
38.4 37.3 36.742.9 42.7 40.2
51.5 52.7 49.2
Comparison of before and after COMMUNITY MOBILIZATIOM
2014 2015COU
PLE
YEAR
PRO
-TE
CTIO
N % WBOTSWBOTS
Figure V: Couple Year Protection
CAPRICON MOPANI SEKHUKHUNE VHEMBE WATERBERG PROVINCIAL0
10000
20000
30000
40000
50000
60000
70000
80000
90000
1197 2145 1289 1196 11556982
16318 1569812081 15479
9990
76548
Comparison of Before and after COMMUNITY MOBI-LIZATION
2014 2015
IMPL
ANO
N IN
-SE
RTIO
N
Figure VI: Number of Implanon Inserted
159
CAPRICON MOPANI SEKHUKHUNE VHEMBE WATERBERG PROVINCIAL0
10
20
30
40
50
60
70
80
90
67.1
80.7
61.9
78.771.2 72.372
80.6
61.3
77.1
67.572.4
Comparison of Before and after COMMUNITY MOBI-LIZATION
2014 2015
MO
THER
PO
ST N
ATAL
CA
RE A
T 6
DAYS
%
Figure VII: Mother Post Natal Care at 6 days.
CAPRICON MOPANI SEKHUKHUNE VHEMBE WATERBERG PROVINCIAL0
10
20
30
40
50
60
7062.1 61.8
5147.3
57.1 55.654.658.8
41.738.8
41.747.9
Comparison of Before and after COMMUNITY MOBI-LIZATION
2014 2015
CERV
ICAL
CAN
CER
SCRE
ENIN
G C
OVE
RAG
E %
Figure VIII: Cervical Cancer Screening Coverage
160
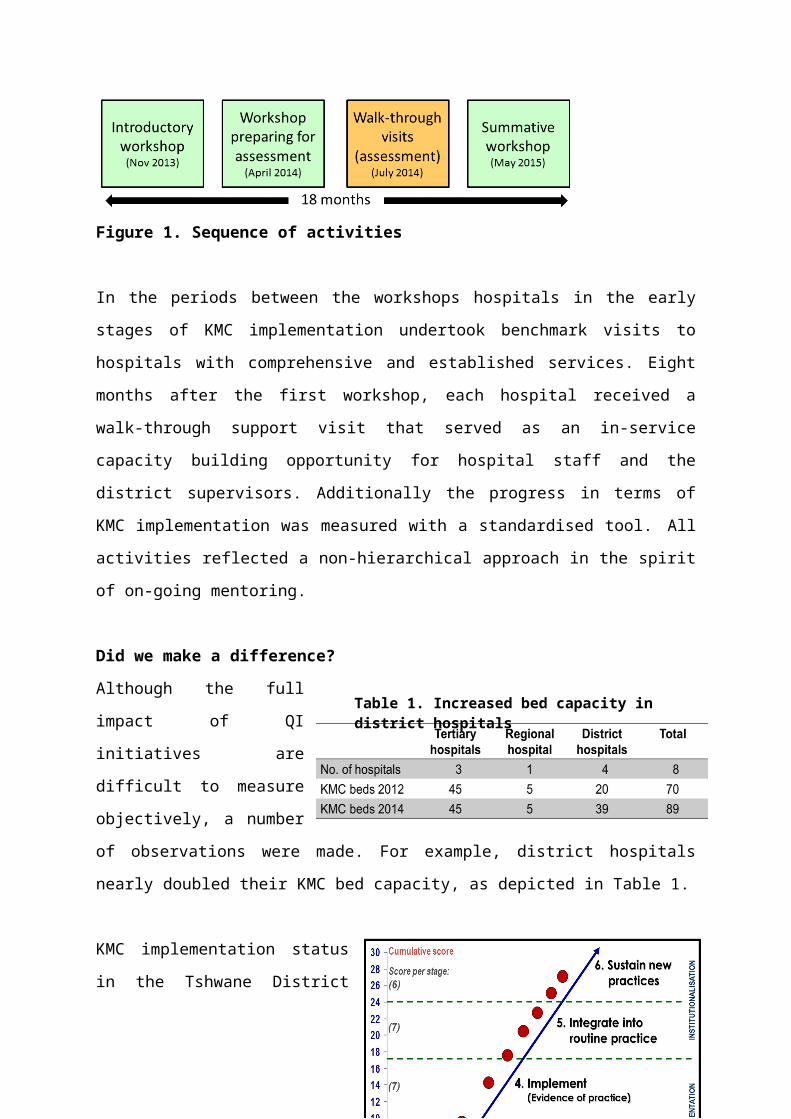
CAPRICONMOPANI
SEKHUKHUNEVHEMBE
WATERBERG
PROVINCIAL0
102030 29.9
20.1 22.917.3
20.9 21.127.5
20.2 22.316.2
22 21.4
Comparison of before and after COMMUNITY MOBILIZATION
2014 2015
STILL
BIRT
H RAT
E PER
10
00
Figure VIIII : Still Birth Rate
Pro Cap Mo Sek VhWat
0.0
5.0
10.0
15.0
20.0
25.0
13.6
21.2
13.3 12.1 9.1
12.2 13.0
19.2
11.6 12.1
8.3
15.7
2013/2014 2014/2015
NNMR: 2013/14 and 2014/15 DHIS
Figure X : Neonatal Mortality Rate
161
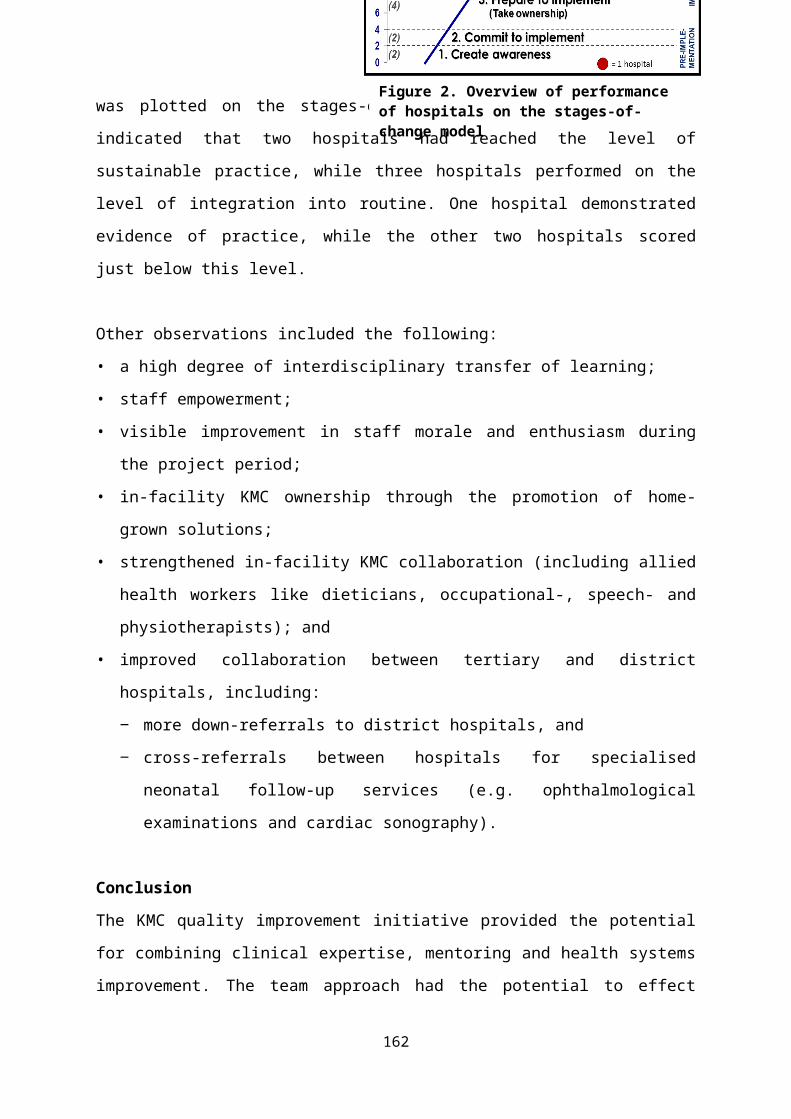
Conclusion:Community participation is able to augment some of the key strategists towards Ending Preventable Maternal Mortality by emphasizes increasing community referral system, demand for public health care, women’s access to maternal health products and antenatal risk screening by health workers . Community mobilisation strategies improve care seeking patterns and reduces obstetric morbidity. Collaboration between the public health care and Traditional health care systems for maternity care deserves urgent attention. Health education and training could play a major role in combating many of the adverse outcome associated with THP remedies and practices.The results of the study provides encouraging evidence that the benefits of community-based strategies may extend across the continuum of maternal, newborn and woman’s health care. Investing in community engagement has positive rewards in the long term.
162
TRAINING COURSES AVAILABLE IN THE ESMOE-EOST PROGRAMME (ABSTRACT)
CM Bezuidenhout, JD Makin, RC Pattinson, A-M BerghMRC Maternal and Infant Health Care Strategies Research Unit and Obstetrics and Gynaecology Department, University of Pretoria
BACKGROUND AND AIM: Since the inception of the Essential Steps on Managing Obstetric Emergencies(ESMOE-EOST) programme, the need was identified to diversify the original basic 3-day course to cater for different cadres of health workers. This poster will give an overview of the current available ESMOE-EOST courses.
METHOD:A mapping analysis was done of the different available courses and the total number of participants for each of the different courses.
RESULTS:There are 4 different types of master training courses available or in the pipeline, namely for hospitals, community health centres (CHCs), nursing tutors and (EMS) workers (pipeline). The core courses for hospitals and CHCs are 3 and 2 days long, respectively and are available as competency-based or drill-based courses. The main groups of participants are medical interns, doctors and midwives. Other participants include basic and advanced EMS workers and nursing tutors who will be responsible for rolling out ESMOE-EOST to nursing students. For all these courses annual refreshers are or will be available in future.
Some of the results that will be included on the poster are the following:MASTER TRAINING Nr ESMOE COURSES Nr Partifipants CategoriesHospitals* 636 3 day Basic 5545 Drs 2883CHCs 543 3 day Drill base 530 Nursing 6342
1 day Refresher (2015) 2015 Total 9225
*Include nrs trained in KZN
CONCLUSIONThere is no one-size-fits-all model for training health workers in emergency obstetric and neonatal care. The diversification of the ESMOE-EOST courses is an attempt to fulfil this need.
163
EVERY BABY COUNTS: THE FORTHCOMING WHO PERINATAL MORTALITY AUDIT GUIDE
Kate Kerber, consultant to WHO
Access to reliable data about the numbers and causes of death and timely dissemination of information to those who need it for taking action is essential for planning and implementing health services. The process of routine identification and notification of deaths is a continuous action cycle linking quality improvement from local to national level. The World Health Organization (WHO) and the African Union have promoted the use of maternal death surveillance and response as a key approach for ending preventable maternal deaths. The tools for maternal death surveillance and response were developed through as a collaborative activity amongst partners and have been taken up widely. Although women and their babies share the same period of highest risk, often with the same health workers present, there has been less movement towards capturing similar information for stillbirths and neonatal deaths, including basic information for every birth and death, along with a critical review of selected deaths.
In support of the Every Newborn Action Plan measurement improvement agenda, WHO is finalizing a perinatal death review guide and related tools in collaboration with several individual experts, institutions and partner agencies, drawing heavily on South Africa’s experience with the Perinatal Problem Identification Programme (PPIP).
Why is a perinatal mortality audit guide important?
Understanding the number and causes of death is key to tackling the burden of 2.6 million neonatal deaths and 2.6 million stillbirths each year. Yet many resource-poor settings lack effective Civil Registration and Vital Statistics (CRVS) systems for births, deaths and causes of death. Each year, half of the world’s babies do not receive a birth certificate; most neonatal deaths and almost all stillbirths have no death certificate, let alone information on causes and contextual factors contributing to these
164

deaths. Many countries have limited capacity for capturing neonatal deaths beyond the health facility level, especially those whose births are not registered, and very few countries have a system for tracking stillbirths at all despite increasing demand for data. Applying the audit cycle to the circumstances surrounding deaths is an established quality improvement strategy that can highlight breakdowns in clinical care at the local level as well as in higher-level processes at district or national level, and improve the CRVS system overall.
Mortality audit for stillbirths and neonatal deaths also contributes to global targets and achievements. Audit as a strategy is covered under two of the five objectives in the Every Newborn Action Plan (ENAP): to address quality of care at birth and to generate data for decision-making and action. The ENAP Metrics Roadmap and the Measurement and Accountability for Health Roadmap both aim to increase investment and capacity of national health management information systems, of which mortality audit is a part. Mortality audit is also a key strategy to ensure accountability for women’s and children’s health acknowledged by the global Commission on Information and Accountability and the new Global Strategy 2.0 for Women’s, Children’s, and Adolescents’ Health. Audit also fits into the Sustainable Development Goals (SDG) framework as a mechanism to track progress for SDG target 3.2 which aims to reduce neonatal mortality to at least as low as 12 per 1,000 live births in all countries by 2030.
What is the guide about?
This guide describes the process of setting up a system for capturing basic information on each birth and death and reviewing instances of stillbirth and neonatal death in a no-blame, inter-disciplinary setting to learn underlying lessons about why each death occurred and to improve quality of care and to prevent future deaths (Box 1). A number of tools, forms and additional resources accompany the guide as annexes.
165
166
Box 1. Contents of the guide
The guide addresses issues around definitions and cause of death classification including the new ICD-Perinatal Mortality classification, as well as different systems for assigning modifiable factors. The third chapter describes the steps required to establish and complete the mortality audit cycle (Figure 1). Given the importance of a supportive environment for successful audit, Chapter 4 describes how to create an enabling environment that supports reflective practice. Chapter 5 provides information on expanding a mortality audit system from individual facilities to a network of linked facilities at regional and national level, including linkages to CRVS and community surveillance systems.
167
Figure 1. The audit cycle
Who is the guide for?
The guide introduces concepts and provides tools for adaptation that will be relevant for stakeholders across the health system including health professionals, planners and managers, epidemiologists, demographers and others who measure mortality trends and policy makers working in maternal and perinatal health. It is important that those with the power to implement the recommended changes actively participate in the process of reviewing deaths, assigning causes and modifiable factors, and identifying the solutions; this guide is for them. The use of audit findings to improve health outcomes is central to the implementation of mortality audit. Stakeholders at all levels who can drive change, such as community leaders, civil society, and parent groups, should be involved in the processes of setting up a mortality audit system to ensure that the recommended changes take place.
168

The guide may also be useful for those looking to promote linkages with CRVS in order to ensure that every birth and death are counted. However, this guide does not cover the full scope of including community births, deaths and stakeholders and is not aimed at community implementation as a starting point for mortality audit.
What does this guide aim to achieve?
This guide aims to establish a framework to assess the burden of stillbirths and neonatal deaths, including trends in numbers and causes of death; to generate information about modifiable factors contributing to stillbirths and neonatal deaths and to use the information to guide action in order to prevent similar deaths in the future; and to provide accountability for results and compel decision-makers to give the problem of stillbirths and neonatal deaths due attention and response.
We know that large scale, long term implementation of mortality audit on its own doesn’t necessarily lead to reduced mortality and improved care. It is not sufficient to count deaths and calculate mortality rates, or even to identify systemic problems contributing to these deaths. Mortality audit is only useful if the reviews lead to action based on the findings. While the guide provides examples and recommendations for initiating and expanding mortality audit, it is important to note that there is not a long list of requirements for completing audit. One of the more important tenets from existing systems is to decide to learn with the experience and adapt the approach as needed.
The tools are being field tested in select low- and middle-income countries prior to finalization and dissemination later in 2016. I would like to acknowledge WHO, the work of the expert review group who contributed materials and who have reviewed the guide, and many thanks to the participants at Priorities in Perinatal Care 2016 who provided insightful feedback for the guide based on their experience with PPIP.
169
THIRTEEN YEARS OF REGIONAL PPIP: TRYING TO HOLD ONTO THE GAINS
Charl OettleWorcester Hospital.
IntroductionThe perinatal mortality and morbidity meeting is a standard and recognised part of good obstetric practice, where each death and near miss is examined with the aim of preventing such a death/near miss from happening again. The Perinatal Problem Identification Program (PPIP) was developed to make the paperwork and analysis easier, and has been used as an audit tool for perinatal mortality throughout the Worcester Hospital Geographic Service Area (GSA) since 2003. The data from 2003-2011 was presented in 2012 at the conference for Priorities in Perinatal Care. This paper looks at what has happened in the region in the following four years, i.e. 2012-2015, and summarises thus thirteen years of focussed perinatal audit.
MethodsMeetings were held monthly or bimonthly by the same obstetrician each time. They were attended by all the hospital doctors, some of the sessional general practitioners (GPs), the labour ward nursing staff and as many of the clinic sisters responsible for antenatal care that could be persuaded to come. Cases were prepared before the meeting, and presented by the medical officer in charge of the labour ward. Basic data was collected for each death, and a primary obstetric and final neonatal cause of death was decided on. In addition, any avoidable factors that possibly or probably led to the death of the child were noted and coded. At the meeting, any issues raised by the death/near-miss that related to antenatal, intrapartum and/or postpartum care were used as springboards for teaching, presentation of protocols and discussion. Feedback to relevant non-attending staff, and appropriate follow-up of individual patients was also arranged. The data was checked against the maternity registers and the basic data set and then entered into PPIP at the hospital; once it had been validated, it was forwarded to the obstetrician, the regional office and the provincial office, who in turn have added it to the national data base. The data for the MOU at Grabouw have been excluded from the analysis, as it refers to a different service area.
Results117 581 births were recorded in the thirteen years covered by this paper. The number of births has increased gradually, at a rate of around 1%/year; the region currently
170
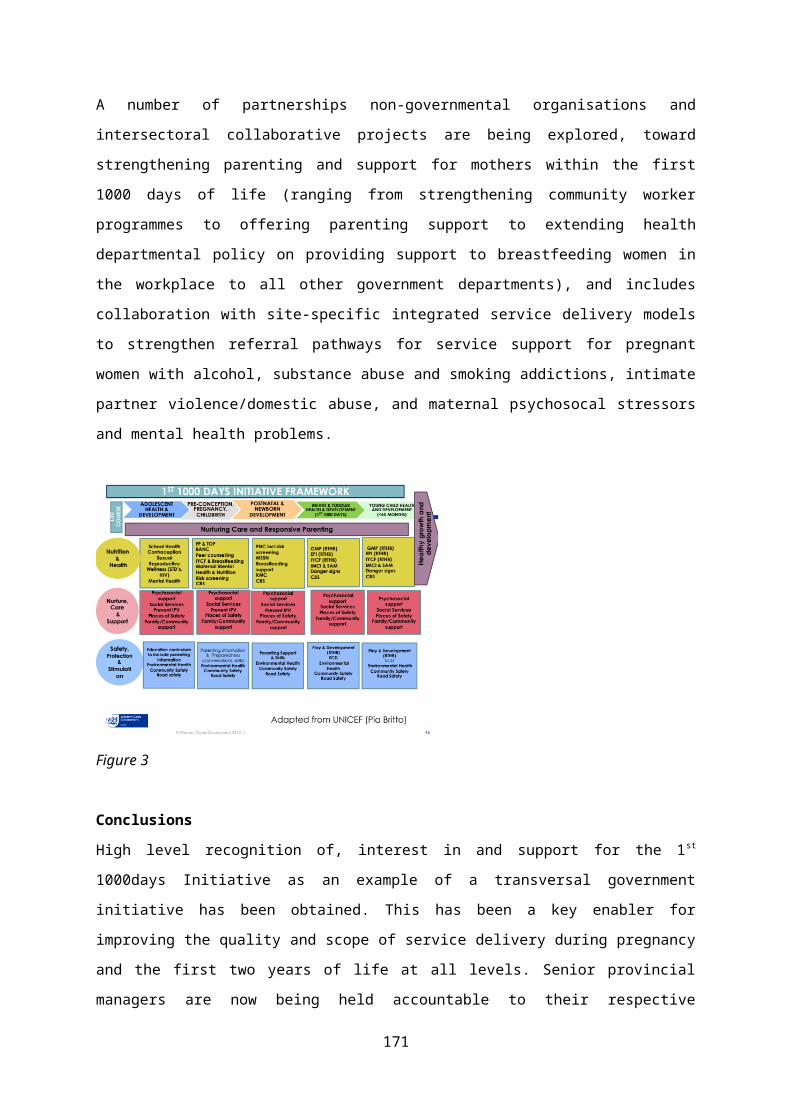
does around 9500/year. The perinatal mortality rate of babies ≥1kg had decreased from 22.6/1000 to 15.1/1000 by 2011. In the last four years, it dropped to 14.1, and has since risen to 17.2/1000 (Fig 1).
Fig. 1. Perinatal mortality ≥1kg in Worcester GSA 2003-2015
The neonatal mortality rate (NNMR) of babies ≥1kg had decreased from 8.0/1000 to 5.3/1000 live births by 2011; in the last four years it has stayed within the range 6.1 to 7.2/1000 (Fig 2).
Fig. 2. Neonatal mortality rate ≥1kg in Worcester GSA 2003-2015
The decrease from 24.3% to 20.9% noted in the low birth weight rate (LBWR) to 2011 has continued steadily, and stands now at 18.7%. The perinatal care index (PCI) (a measure of the impact of LBW on the PNMR) has remained under 1.0, ranging between 0.7 and 0.9. The stillbirth:neonatal death ratio (SB:NNDR) has been 1.3:1 over the past four years.
171
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
0123456789
Individual audits were done on 99.3% of the deaths that occurred (3810 deaths). The main causes of death of babies ≥1kg were: antepartum haemorrhage (22.5%); intrapartum asphyxia and trauma (18%); unexplained intrauterine death (14%); preterm labour (13.6%) and intrauterine growth impairment (8.7%); these five causes represent 76.8% of the deaths. The unavoidable PNMR of babies ≥1kg was 8.5/1000; in the last four years this has been 7.1/1000. The final causes of neonatal deaths ≥1kg were hypoxia (33%); prematurity (26%); congenital abnormalities (13%) and infections (14%); these represent 86% of the neonatal deaths.
The caesarean section (C/S) rate which had increased steadily, from 12.7% in 2003 to 21.5% in 2011, has continued to rise, albeit more slowly, and stands now at 22.1% (Fig 3). A total of 22 053 C/S (18.7%) were done in the period.
Fig. 3. Caesarean section rate (%) in Worcester GSA 2003-2015
3709 women were unbooked (3.2%); 608 of their babies died, with a PNMR of 163/1000. 8500 babies (8.0%) were born before arrival (BBA). Of these, 978 died, with a PNMR of 115/1000. The unbooked and the BBA rates have come down steadily over the years, from 4.6 to 2.1% and 10.0 to 5.9% respectively (Figs 4&5). Teenage deliveries (<18 years) increased from 5.1% to 9.0% in 2011, but have since come down to 7.3%. Fig.4. Unbooked rate (%) in Worcester GSA 2003-2015
172
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
0
5
10
15
20
25
173
Fig.5. Born before arrival rate (%) in Worcester GSA 2003-2015
DiscussionThe previous paper documented substantial achievements in the various parameters of perinatal care. The last four years have not had the same degree of improvement, though there have been some gains. The factors that impact on perinatal mortality are manifold, and complexly interwoven, and are deeply influenced by socioeconomic circumstances, which are less open to influence by the health services. (The decreasing LBWR may point to an improvement in socioeconomic status, better nutrition, and less alcohol and tobacco use). There has been a concerted effort by the maternal and child health division in the region to address problems related to pregnancy and childbirth. Booking rates are high, at 97.9%, despite large areas with widely scattered population. Point-of-care screening of HIV, Rh and Syphilis is offered throughout. BANC (Basic Antenatal Care) training of nursing staff has been extensively rolled out, and has over 80% coverage; ESMOE (Essential Skills in Managing Obstetric Emergencies) training has been offered to all the district hospitals, and is mandatory for intern training; the SMS service MomConnect has been started in the region, and carries reminders and health education messages to patients; attention too has been given to the emergency and district transport systems. Although the regular audit meetings are unlikely to be the explanation for the improvement, there have been certain details in the structure of the outreach that make it plausible that they have played a role. The focus of these meetings has been uniformly that of changing practice, and to a very large extent, there has been commitment to the idea by the medical and nursing staff. Teaching is centred on cases with which the staff are all familiar, and is likely to be better remembered. The meetings have been driven throughout by a committed single obstetrician with the authority to insist on change in practice. This has allowed a consistency of message. There have been side benefits for the service – health workers in the district have had
174
a fixed contact person at the regional hospital, who has a clear understanding of the constraints under which they work. PPIP puts analysed data directly into the hands of local managers – the obstetrician’s familiarity with the PPIP software has allowed him to give on-site support to those using the program. The cross checking of the data has resulted in a quality that makes it useful for decision making, both locally, and at Provincial level.
Some shortcomings and concerns should be noted. There has been a seemingly inexorable rise in the number of caesarean sections, although this appears to be stabilising somewhat. Some of the hospitals in the region do insufficient deliveries per year to maintain skills, and the heavy reliance on junior community service staff without stable senior backup is of concern. It means too that each year one starts from scratch to train up staff to an acceptable level of competence. The rate of teenage deliveries has tended to stabilise at around 7-8%. The BBA rate has been essentially unchanged for the past four years. There are still far too many children dying from asphyxia. They represent the second highest primary cause of death, and the highest final cause of neonatal death of babies ≥1kg. (The numbers say nothing of those asphyxiated babies that did not die, who continue long after to burden the lives of their caregivers and the health services, and who represent an enormous medicolegal risk). Despite the comparatively encouraging data presented, there are still too many avoidable deaths. If these had not been, the mortality rates would be well under 10/1000, which is comparable with those of first world countries. Continuity of the process of audit and feedback is not a given, there has to be a committed driver of the system.
There are no grounds for complacency in the provision of antenatal and obstetric services – as the rates come down, it becomes more and more difficult to hold onto the gains, let alone to continue with the improvement. This is the more so as budgetary and staffing constraints begin to take effect on service provision.
175

EVALUATION OF THE PERINATAL PROBLEM IDENTIFICATION PROGRAM ACROSS HEALTH FACILITIES IN LIMPOPO PROVINCE, SOUTH AFRICA (2006-2015)
Unarine Makungo 1,2 , Lolly Mashao 3,1 South African Field Epidemiology Training Programme (SAFETP), National Institute for Communicable Disease (NICD), 2 School Of Health Systems and Public Health, University of Pretoria, Pretoria, South Africa; South Africa Field Epidemiology Training Program3 Limpopo Initiative for New-born care
Introduction
The need for evaluations and accurate data is vital for countries and governments to monitor the gaps in the current obstetric and neonatal care that impact on maternal and perinatal outcomes. The perinatal and maternal mortality rate is a vital indicator of the quality of ante-natal, obstetric and neonatal care in health facilities. In 1990 there was an estimated 12.7 million deaths decreasing to 6.3 million in 2015 among children under five, with neonatal deaths. In the 2012-2013 saving babies report there were a total of 47 238 total perinatal deaths in South Africa, 16 827 neonatal deaths and 32 662 still births.A functional PPIP facility needs to analyze results and generate mortality rates and trends over time. Hence we conducted this study to estimate trends of perinatal mortality in Limpopo Province from year 2006 -2015 and to determine challenges of program among users.
Material and methods
The study was conducted using PPIP data comprising of all public hospital facilities from 2006 -2015.The study was a retrospective descriptive study. The following perinatal indicators were included in the analysis: Perinatal mortality rate, neonatal mortality rate, early neonatal mortality rate in grams and still births rate.
Sample size All 35 Limpopo hospital facilities PPIP data from 2006 to 2015 was included in the study. Data from the clinic was excluded from the analysis.
Data collectionData was extracted from PPIP software into Microsoft Excel.
176
Results and Discussion
Limpopo PPIP is only reporting data from the hospital facilities and clinic are not yet fully capturing PPIP data. Rates displayed are slightly different from DHIS rates as it captures an additional 30% of deliveries from clinics. Limpopo Newborn Care received no funding from 2011 and only resumed in 2014 resulting in poor support for neonatal wards that may have affected perinatal indicators outcomes.
2006 2007 2008 2009 2010 2011 2012 2013 2014 20150
10
20
30
40
50
60
Perinatal mortality rate per district in Limpopo province (2006-2015)
VhembeCapriconSekhukhuneWaterbergMopani
Perin
atal
deat
h ra
te/1
000
birt
hs
Figure 1: Total perinatal neonatal mortality rates in Limpopo province from 2006-2015
Trends above show a high perinatal mortality rate among the five districts. These trends are above the provincial target of 30/1000 births. Capricorn district with the average highest rate of above 40/1000 death receives high risk obstetric and neonatal patients from the four other district. Over the 10 year period there has not been a significant positive decline among the districts. However Mopani districts perinatal mortality rate indicate a positive decline from 2013 to 2015 from 41.6 to 34.6/1000 births, however it has not reached the provincial target.
177
2006 2007 2008 2009 2010 2011 2012 2013 2014 20150
5
10
15
20
25
Neonatal mortality rate per district,Limpopo province (2006-2015)
VhembeCapriconSekhukhuneWaterbergMopani
Neo
nata
l mor
talit
y ra
te/1
000
live
birt
h
Figure 2: Neonatal mortality rate per district in Limpopo province from 2006 to 2015
Neonatal mortality rate has remained high above the provincial target of 12/1000 live births. Vhembe district neonatal mortality declined from 14.3 to 11.7/1000 live births in 2012 to 2015 respectively. In the same year Capricorn district has been on a steady increase from 2012 to 2015 from14.3 to 21.9/1000 live births .Mopani district shows a positive steady decline from 2013 to 2015 at 18.5 to 15.6/1000 live births, however it still remains above the provincial target.
2006 2007 2008 2009 2010 2011 2012 2013 2014 20150
50
100
150
200
250
300
350
400
450
500
Neonatal mortality rate >1000-1499g
Vhembe 1000-1499gCapricon 1000-1499gSekhukhune 1000-1499gWaterberg 1000-1499gMopani 1000-1499g
NM
R/10
0 liv
e b
irth
s
Figure 3: Neonatal mortality rate (>1000-1499g), per district in Limpopo province from 2006 to 2015
In this neonatal mortality target of babies born weighing > 1000g to 1500g ,the rate are significantly higher than the provincial target of 150/1000 live births. Mopani district had a highest pick of 475.4/1000 live births in 2012, and a consistent decline has been observed from 2012 to 325.6/1000 live births in 2015, which is still above provincial target. In 2014 to 2015 Sekhukhune, Waterberg and Vhembe district seem to be experiencing a gradual decline in mortality rate from 407.4 to 325.6; 257.1 to
178
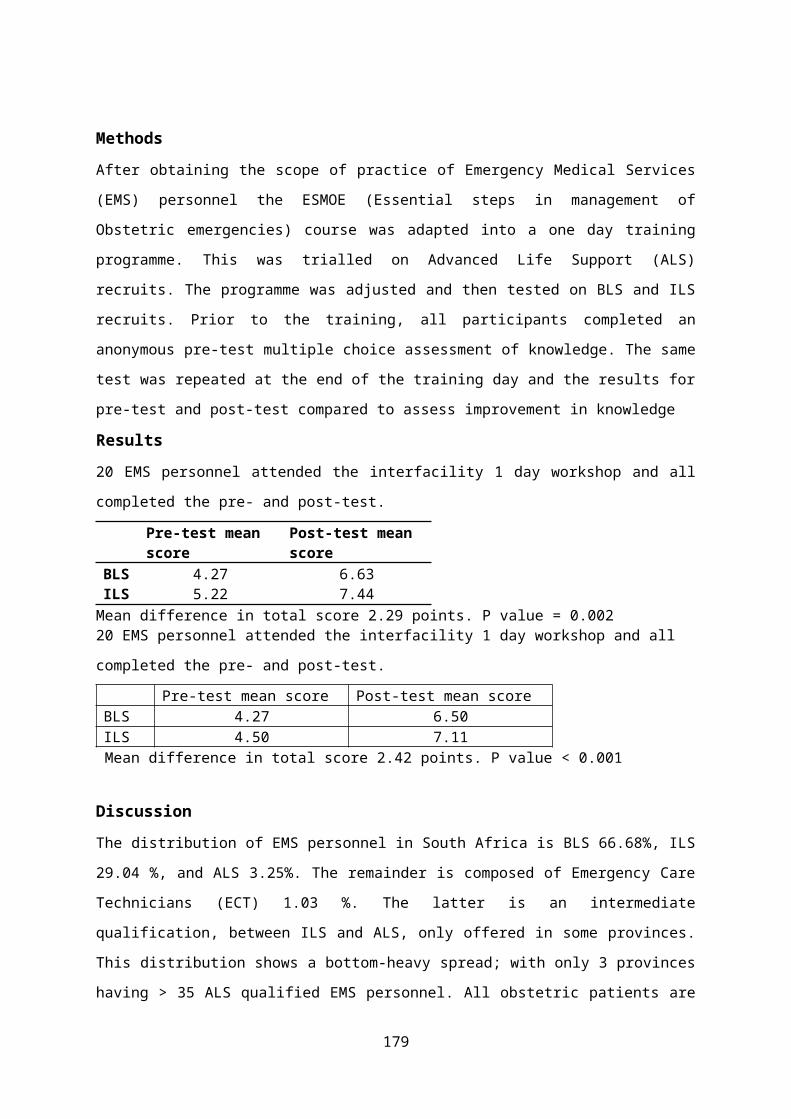
239.7 and 320.4 to 300/1000 live births respectively. Capricorn district which consist of two tertiary referral hospitals has had the lowest mortality rate when compared to the other four districts although still above the provincial target over the 10 year period. However from 2013 to 2015 a consistent mortality rate increase is observed.
2006 2007 2008 2009 2010 2011 2012 2013 2014 20150
20
40
60
80
100
120
140
Neonatal mortality rate > 1500 -1999g
Vhembe 1500-1999gCapricon 1500-1999gSekhukhune 1500-1999gWaterberg 1500-1999gMopani 1500-1999g
NM
R/10
00 l
ive
birt
hs
Figure 4: Neonatal mortality rate (>1500-1999g), per district in Limpopo province from 2006 to 2015
Neonatal mortality had remained higher than the provincial target of 60/1000 live births across all district. Progress has not been consistent ,however from 2008 to 2011 the was a positive decline from Sekhukhune and Capricorn district, with Capricorn district staying along the target from 2009 to 2013 at 61.8, 57.6,63.2 to 63.3/1000 live births during the respective years. In 2013 to 2015 there was a sudden increase from 63.3 to 92.1/1000 live births .Mopani district has had a gradual increase in neonatal mortality from 82.1/1000 live births in 2006 to 113/1000 live births in 2012,which was followed by a consistent decline from 2012 to 2015 at 101.6/1000 live births. Among the other districts Vhembe had a consistent significant decline in neonatal mortality from 2008 which was at 98.8/1000 live births to 66.5/1000 live births in 2015.
179
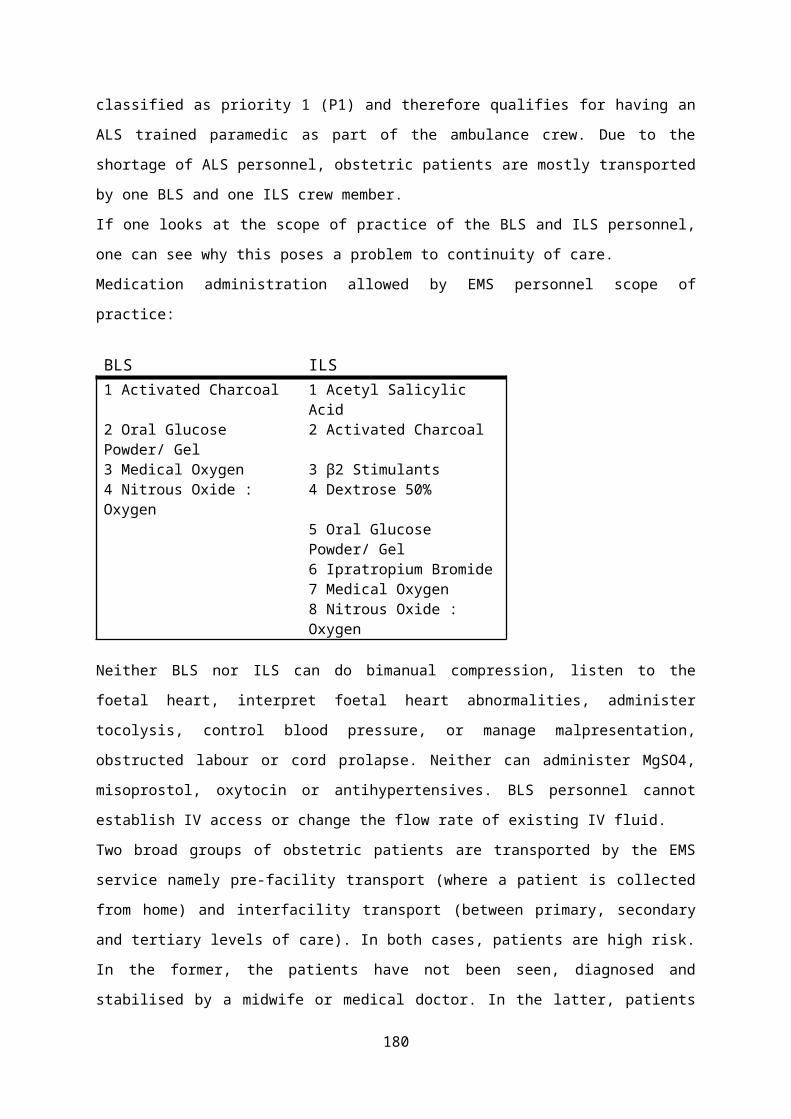
2006 2007 2008 2009 2010 2011 2012 2013 2014 20150
5
10
15
20
25
30
35
Still birth rate per district ,Limpopo Province
VhembeCapriconSekhukhuneWaterbergMopani
Still
birt
h rt
ae/1
000
live
birt
h
Figure 5: Still birth rate per district in Limpopo province from 2006 to 2015
Vhembe district still birth rate has remained below the provincial target of 20/1000 live births. The referral district has had the highest still births rate throughout the 10 year period. Waterberg and Mopani district remained above the provincial target throughout the years, however is evident from 2014 to 2015 from 24.3 to 20.6 and 24.3 to 20.6/1000 births respectively.
Conclusions
PPIP data is only representative of perinatal deaths occurring in public health facilities. Deaths occurring in private hospitals, homes and clinics are not represented. Perinatal mortality trends in this study do not indicate a significant improvement in mortality over time. Findings from this study suggest that PPIP is not being used in facilities to inform change in practice or other factors might be playing a role on poor progress. Studies need to be conducted to investigate if poor resource, infrastructure, poor clinical and nursing practice are contributing factor. Hospital facilities have poor understanding and interpretation of PPIP data as evidenced by poor change in practice. Skilled PPIP users are not passing on the skills to ensure sustainability which is precipitated by lack of interest among other professionals to learn PPIP, staff resigning, changing jobs and constant rotation of staff.There is a need to evaluate the perinatal review meetings to identify the use of PPIP and to inform action required. A robust strategy is required to reduce perinatal mortality in health facilities.
180
PERINATAL AND NEONATAL MORTALITY RATES IN BISHOP LAVIS OVER 7 YEARS (ABSTRACT)
HJ Odendaal 1 , CA Wright2, P T Schubert2, CA Groenewald1, LT Brink1, E Geldenhuys1,D Mason1
1 Department of Obstetrics and Gynaecology, Stellenbosch University2 Department of Anatomical Pathology, Stellenbosch University
IntroductionThe Safe Passage Study (SPS)(www.safepassagestudy.org) is a prospective study to determine the effects of alcohol consumption and smoking during pregnancy on stillbirths and infant deaths during the first year of life. During seven years 7060 participants were recruited from the antenatal clinics in Bishop Lavis and Belhar. All infants were followed up for one year.
ObjectiveTo determine stillbirth, early and late neonatal, perinatal and infant mortality rates in a well-defined community where the outcomes of all pregnancies were recorded.
MethodsAll participants in the study were meticulously followed up antenatally until delivery. After delivery, examination of the new born was done within four days. Further follow-up was at the ages of one month and one year. Participants were requested to notify the study personnel of all deliveries. Stillbirths or infant deaths were followed up as soon as possible after it had occurred. The antenatal records of all participants were clearly marked with the study logo to enable health care workers to notify the study personnel of all new admissions. In addition, one of the study personnel checked the registers of the admissions room and labour and neonatal wards, several times a day and at least once over weekends, for participants who may have delivered. In case of a stillbirth, the participant was visited by one of the study personnel and also the dedicated social worker of the study as soon as possible to start with bereavement counselling and to obtain informed consent for autopsy. If consent was obtained at recruitment, the placenta was collected for histological examination. Antenatal, labour, delivery and neonatal records were photocopied to have the data readily available for medical chart abstractions. If delivery had occurred outside Bishop Lavis MOU, Karl Bremer or Tygerberg Hospitals, the medical superintendent of the particular hospital was requested in writing to send a copy of the labour records. Abovementioned information was then used to prepare presentations for one of the Perinatal Mortality Meetings of the Department of Obstetrics and Gynaecology. If available, information on the histological information of the placenta or autopsy findings was also presented. At the end of the presentation a probable cause of death was assigned. Gestational age was determined by ultrasound, done at the recruitment or second antenatal visit. Care was taken to only select stillbirths at or after a gestation of 22 weeks. Cases where demise most likely occurred before 22 weeks but where the delivery was at or after 22 weeks were excluded from the study.
ResultsDelivery was not recorded in 160 participants, for the following reasons: 94 withdrawals, 56 miscarriages and 10 lost to follow up. After delivery there were another 40 withdrawals. The study therefore consists of 6783 live births and 129 stillbirths. There were almost the same number of deliveries in each year over seven years. Over the seven years (2008-2015), the spontaneous miscarriage rates increased from 4.1 during the first year to 11.0/1000 births during the last 3 years. The stillbirth rate was 16.7/1000, the early neonatal death rate 3.7/1000, the late neonatal death rate 1.2/1000 and perinatal mortality rate 21.3/1000. The prevalence rate of preterm deliveries was 13.5%. The rates of stillbirths, perinatal deaths or
181
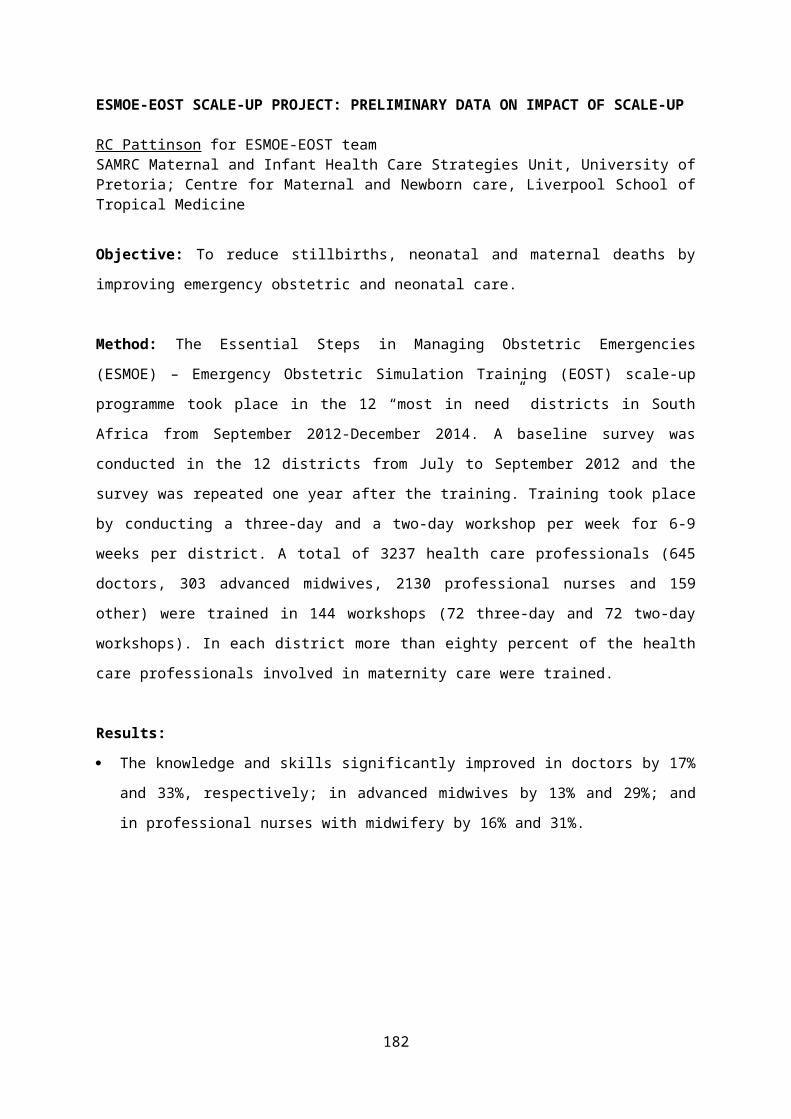
preterm deliveries did not improve over seven years. Only the infant demise rate after 28 days showed a downward trend.
ConclusionsThe underlying causes of stillbirths and preterm deliveries should be addressed to improve perinatal mortality. Good care during pregnancy and labour, as such, is not sufficient.
182
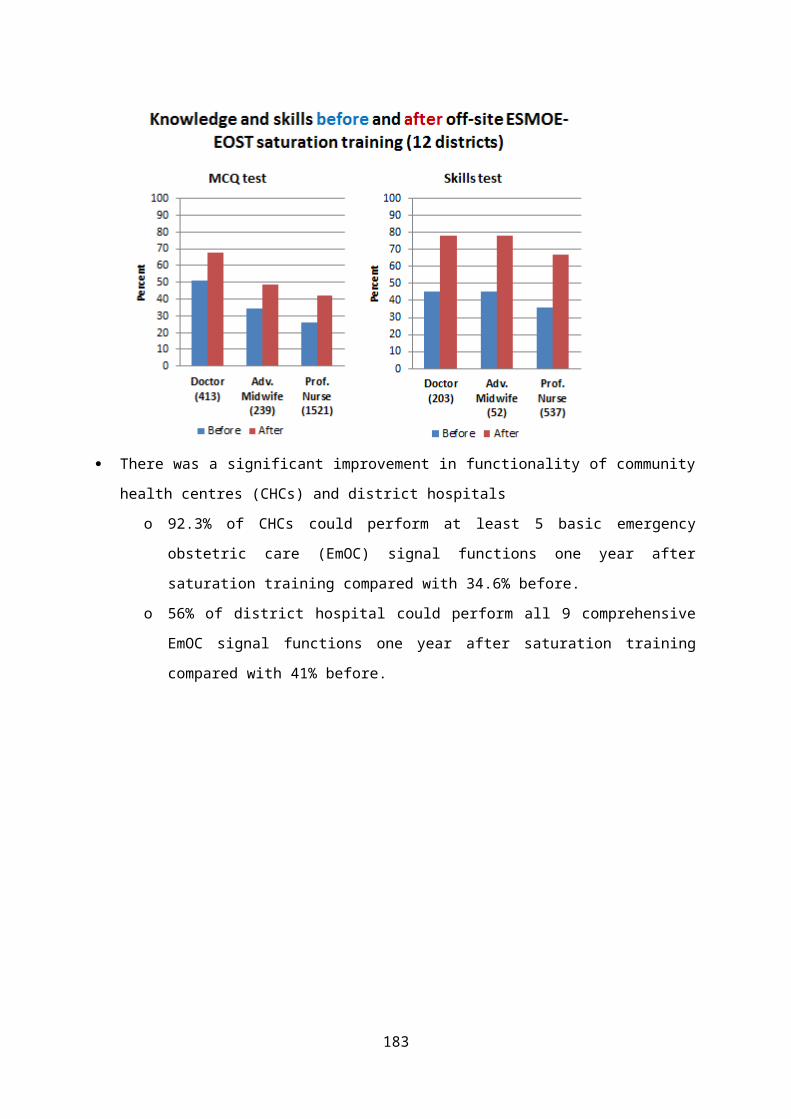
ACCREDITATION OF NEONATAL CARE SERVICES IN KWAZULU-NATAL
D. NYASULU 1 , L.HASKINS, R. DAVIDGE2, C. HORWOOD1
1. Centre for Rural Health, University of KwaZulu-Natal, Durban 2. KwaZulu-Natal Department of Health
BackgroundDespite interventions implemented over the past decade, neonatal mortality has not changed substantially and the neonatal mortality rate has remained in the range of 11-14 per 1,000 live births. The Saving Babies Report, 2012/2013, reflects the early neonatal death rate as 21/1000 live births with the majority of these deaths occurring in 1000-1499 weight category. In KwaZulu Natal province, deaths in the first 28 days account for up to 42.2% of infants and 30.6% of fewer than five deaths.
In recent years KwaZulu-Natal Department of health introduced various initiatives and interventions aimed at improving the quality of neonatal care across the province. These interventions include the following:
The creation of a 4-tier neonatal service The introduction of norms for infrastructure and equipment The provision of equipment including all that is required to establish
2 high care beds Policies around staff deployment The roll out of KINC and NELS for the development of staff in
neonatal services The introduction of clinical tools to ensure the efficient and effective
management of small and sick newborns. These include the KINC chart booklet, standard operating procedures (SOPs), and policies on admission and discharge as well as ventilator support.
Outreach programmes for ongoing support of neonatal services
One essential aspect of any intervention aimed at improving health care is evaluation especially evaluation of neonatal health care. It is also true to state that evaluation of neonatal care is more difficult than any other area of health care. Although mortality rates have been used as an indication of success,
183

neonatal mortality rates are influenced greatly by many factors such as access to obstetric care, period of gestation, facilities, and staffing. The KINC accreditation programme for neonatal services has been developed in order to strengthen the implementation of the programmes, ensure the ongoing improvement of neonatal services and provide an objective tool for measuring the success thereof.
AimThe main aim of this accreditation is to benchmark facilities against DOH norms and standards for ongoing monitoring of neonatal services by assessing each facility using a standardised tool adapted for both district and regional hospitals.
Methodology All facilities providing neonatal services in KZN were assessed for accreditation. One day is spent in each facility, starting with meeting with senior management for briefing and feedback on completion of assessment. An accreditation team was put together and trained on the use of the tools. The team comprised of the following:
CRH coordinators DOH Outreach support consultants DCST teams i.e. DCST paediatrician, DCST ADM and DCST Paeds
nurses Facility Assistant Nursing Manager; Operational Manager and Med
Officer in charge of Nursery
Components of Accreditation The assessment has three components namely Pre assessment facility review which is conducted by the facility
Nursing Service Manager prior to the start of assessment. On the day of accreditation, data captured in the pre-assessment facility review tool is assessed regarding compliance with stipulated norms.
Facility assessment involves assessment of input and processes as well as output indicators. It is conducted on the day of assessment by accreditation team together with the hospital ANM / Nursery/Mat OM.
184
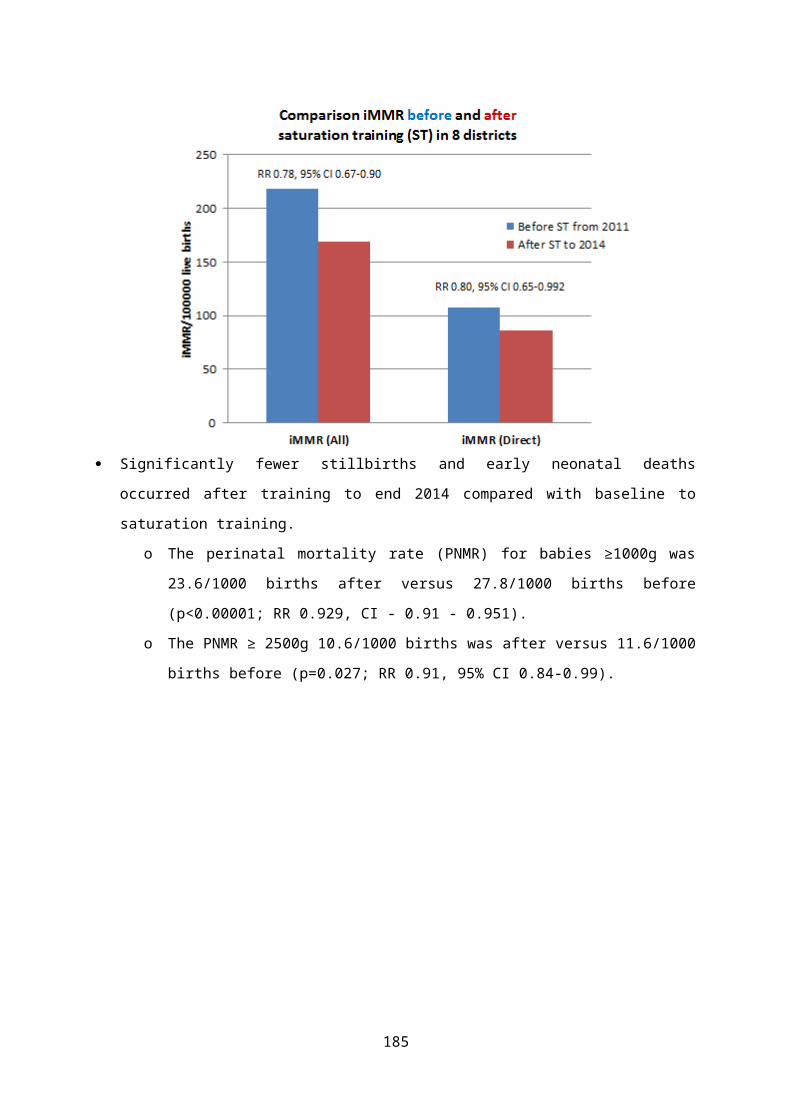
Clinical audits are conducted by Outreach Support Consultants, DCSTs and Facility Medical Officer in-charge of nursery. Four records selected discharged babies who were born and nursed in the facility must be selected and audited by the auditing team.
Provider Skills Assessments and Maternal interviews are conducted by members of assessing Team.
INDICATORS ASSESSED Fifteen indicators were selected for this assessment.
Input & Process Indicators
Output Indicators
Clinical audits HCP Skills assessments
Maternal Interviews
Infrastructure: Neonatal UnitMaternity UnitResus EquipmentSupport ServicesStaffing
Process Indicators: Statistics Systems
Care assessment:Labour WardNeonatal
UnitPN UnitKMCMonitoring &
Evaluation
4 clinical records: 2 Prem babies
weighing 1500g & below
1x Sick Term1xWell Well Term
First examination of the newborn
Neonatal resuscitation in the labour ward
Neonatal resuscitation in the neonatal Nursery
Kangaroo mother careBreastfeedingCPAP initiation Intubation (Regional
Hospitals)
Post natal ward X3 mothers
Neonatal nursery X 2 mothers
Critical Items to achieve a Silver Accreditation
Critical Items to achieve a Gold Accreditation
Critical Items to achieve a Platinum Accreditation
Total score of 50% One indicator per
category above 60% Dedicated MO that does
not rotate for 6 months 50% non rotation of
nursing staff Hand washing facilities
are appropriate There is a functional
resuscitaire and resuscitation trolley available in
Labour ward Caesar theatre Neonatal
nursery 100% of pre-term deliveries receive antenatal steroids
Total score of 65% Eight indicators must be
above 60% The Operational
Nurse/Sister in charge has an appropriate qualification
Hand spray at every bed
50% of maternity staff have received HBB training
Functional nasal CPAP is available and used
Record and infection audits are conducted monthly
Total score of 80% Twelve indicators must
score above 60% Numbers of nurses /
shift meets the norms for beds
beds correctly spaced with no overcrowding
There are records of weekly HBB fire drills
In and out surfactant therapy is available and used
Clinical audits are conducted annually
10% institutional reduction targets in NMR, PCI and IHMR have been met
Results: Results will be available by end of April 2016.
185
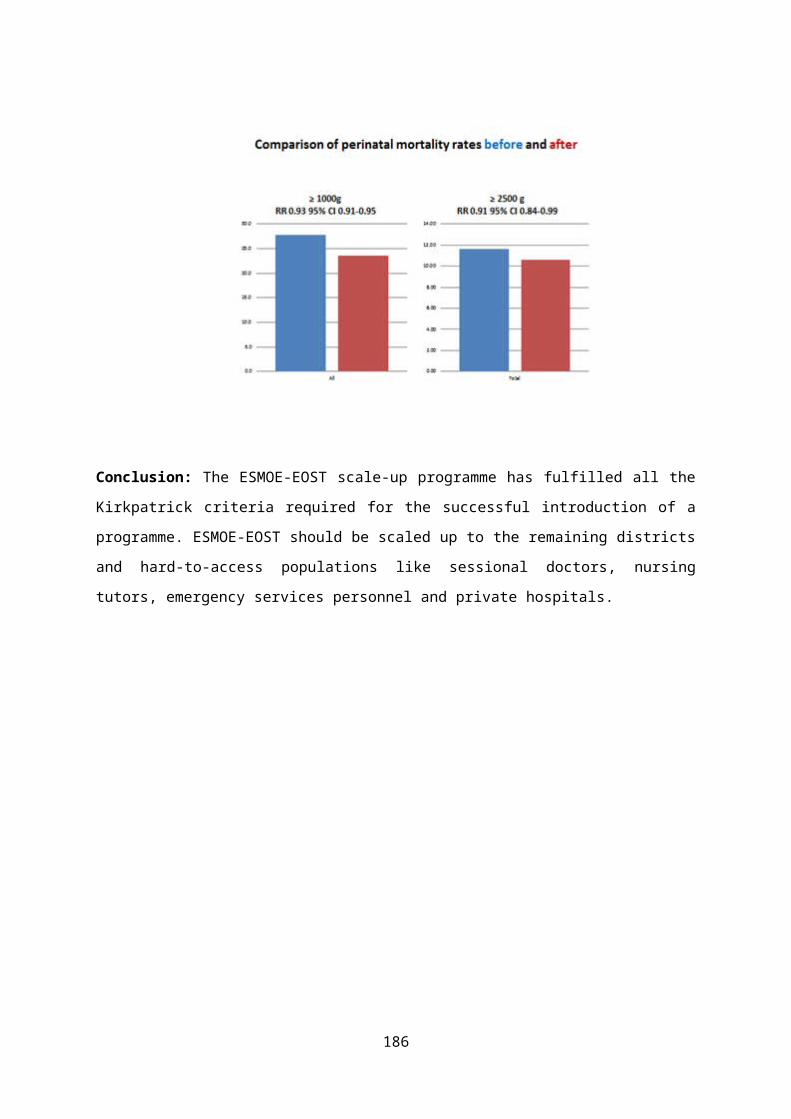
Lessons learnt: Communication with the facility prior to the assessment makes the
process run smoothly Training of a team of accreditors to undertake the assessment is essential The use of a multidisciplinary team during the assessment, including
outreach paediatricians, DCST members, MCWH co-ordinators, nursing service managers and operational managers allowed for improved working relationships
KINC training and mentoring has contributed to high scored in terms of compliance with infrastructure and equipment but there is still a need to address the actual quality of care as seen in the clinical audit of records
ConclusionAccreditation of newborn care using standardised tools may be a useful way of providing a baseline against which to monitor newborn care and identify improvementsThe awarding of silver, gold and platinum award for newborn care will act as a motivation for health workers towards achievement of standards
ACKNOWLEDGEMENTSFunding was provided by ELMA PhilanthropiesWe would like to thank the following organisations and people for their support:
KZN DoH especially Dr Neil McKerrow District Clinical Specialist Team member who participated in this
accreditation District Outreach Paediatricians Hospital staff especially Maternity Nursing Service Managers, Operational
Managers and Medical Officers from all District and Regional hospitals in KwaZulu-Natal
186

ESTABLISHING COMMUNITY BASED MATERNAL DEATH REVIEWS AND THE ASSOCIATED SOCIAL DETERMINANTS IN LIMPOPO: VHEMBE PILOT SITE
Shisana Baloyi 1 , Tinyiko Nkondo2, Robert Sirwali3, Elizabeth Matidze4,Phanuel Phamphe5,Thatheni Motshoare6, Mulimisi Ramavhuya7, Hellen Mhinga8,Monica Machavana9,Ester Moshabela101Chief Specialist and Head of Clinical O&G Limpopo DoH, 2District specialist forensic pathologist, 3District Executive Health Manager Vhembe, 4ASGM Special Project and Provincial MCW&Nutrition DoH Limpopo, 5MCWH Manager Department of Health Vhembe District Limpopo, 6Chairperson Religious and Faith Healers/ Faith Based Organization (NICSA- National Interface Council of South Africa), 7DCST Family Physician Vhembe Limpopo DoH, 8 DCST midwife,Vhembe DoH;9DCST PHC, Vhembe DoH, MCHW Co-ordinator .
BackgroundMaternal mortality remains a major challenge to health systems globally, with the low- and middle-income countries (LMICs) worst affected. Maternal mortality in Limpopo has increased in the last triennium of 2011-2013, 759 recorded Maternal Deaths(MD) with 30 Community Maternal Deaths (CMD), 225 MD and 13 CMD for 2014. Maternal Death Reviews (MDRs) are qualitative and in‐depth studies of the causes of maternal death. MDRs provides detailed information on various factors that contributed to the death at community, facility, district, regional and national level that are needed to be addressed to reduce maternal deaths. MDRs can assist to identify preventable factors or any actions that could have been taken to prevent that death. Available literature demonstrates that where MDRs have been implemented, they have contributed to reducing maternal deaths and improving the quality of maternal care, especially when the process is supported by political and legislative instruments. The Confidential Enquiries system of recording and analysing maternal deaths has been in operation since 1 October 1997 in South Africa. This current enquiry is based on system of investigating maternal deaths that occur in private facilities and the public health system. The community MDs and community factors are not identified or addressed by the current Confidential Enquiry. Social, cultural & environmental factors across a woman’s life course affect risk for direct & indirect causes of death, these
187
factors are not addressed during the MDR. Over 40% deaths have community level avoidable factors. No systematic approach for identifying and notifying maternal deaths that occur outside of health facilities and at home.Community factors not identified or addressed by the current Confidential Enquiry are such as activities associated with the Traditional Health Care Practitioners and the effect of their remedies. These activities are rarely assigned to be the primary cause of death or the underlying cause or contributory factors.Two types of MDRs are described: Facility Based Maternal Death Review (FBMDR) and Community Based Maternal Death Review (CBMDR). FBMDR is a process to investigate and identify causes, mainly clinical and systemic, which lead to maternal deaths in the health facilities; and to take appropriate corrective measures to prevent such deaths. CBMDR is a process in which deceased’s family members, relatives, neighbours or other informants and care providers are interviewed, through a technique called “Verbal Autopsy” (VA), to elicit information for the purpose of identification of various factors – whether medical, socio-economic or systemic, which lead to maternal deaths; and thereby enabling the health system to take appropriate corrective measures at various levels to prevent such deaths. National Committee for Confidential Enquiry into Maternal Deaths (NCCEMD) in South Africa proposes establishment of community death reporting and investigation of maternal deaths using the VA approach. NCCEMD identified Vhembe as a pilot site based on the previous Provincial maternal death reports accounting for some community maternal deaths. “Verbal autopsy” has been widely used as a method of ascertaining causes of death in children in places where the majority of deaths occur without medical supervision”.
Aim:To improve the identification and notification of maternal deaths through a community monitoring process and develop an enquiry process for deaths occurring outside the formal health setting.
188
Purpose and Objectives:To determine the extent of deaths occurring outside of facilities, explore the social determinants, assess factors contributing to these deaths and compare with those reported through the facility maternal death review process. This investigation should assist to develop a community based monitoring process and intervention to reducing maternal death.
189
SettingRural Vhembe District, Limpopo with dominant traditional authority, found to be the ideal side for piloting as traditional authority is very organize making it easy to trace any deaths as the burial of the deceased cannot take place without the permission of the local chief or traditional leader. Once the death has occurred the family has to contact the local traditional authority to request the burial site.
Research design and methods:Narrative description of a focused group discussion comprising of provincial senior health managers, members of the NCCEMD, Vhembe District senior health care managers, district clinical specialist team, traditional leaders, members of Limpopo Provincial Maternal Death Assessors, Vhembe district specialist forensic pathologist, Members of the Religious and Faith Based Organizations, traditional health care practitioners, members from the Vhembe Funeral Parlor Association. Literature reports on verbal autopsies from other places like CARE Sierra Leone LIFT‐UP study, were analyzed. A focus group is a group of individuals selected and assembled by researchers to discuss and comment on, from personal experience, the topic that is the subject of the research. A qualitative descriptive exploratory design was followed within the context of the Vhembe district in Limpopo. A qualitative approach is described as a systemic, interactive, subjective approach, used to describe life experiences and give meaning to them. A qualitative approach was chosen for this study, which enabled participants to share their experiences and knowledge pertaining to the community maternal deaths. On the first day of the consultations delegates present were from National Interfaith Council of South Africa (NICSA), Traditional Health Practitioners, District Health Officials, District Clinical Specialist Team, Vhembe Forensic Pathology Specialist and Provincial Head of Clinical Specialist (O&G) for Limpopo Province. Funeral Parlour’s Associations meeting was held a month earlier on. The first was to exchange
190
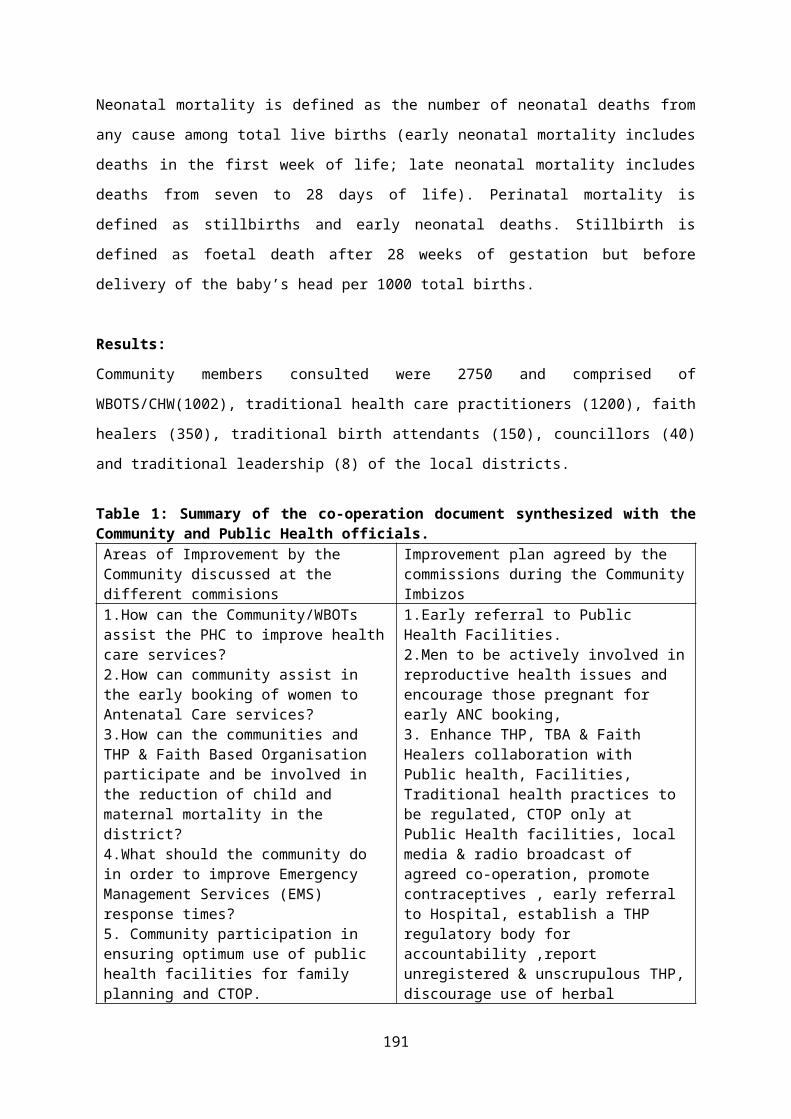
knowledge with the community and the various social formations about the definition of maternal death, causes of maternal deaths and the factors contributing to maternal deaths outside the health care facilities.We defined maternal death as death of a female from any cause related to or aggravated by pregnancy or its management (excluding accidental or incidental causes) during pregnancy and childbirth or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy15. A late maternal death is “The death of a woman from direct or indirect obstetric causes, more than 42 days, but less than 1 year after termination of pregnancy.” Despite being caused by pregnancy-related events, these deaths do not count as maternal deaths in routine civil registration systems.Statistics from the Limpopo Chapter of the Saving Mother Report (2011-2013) were shared with delegates. Various causes were highlighted to the delegates with some of the causes well known to both the traditional healers and the western trained health care officials. Examples of such are retained placenta related morbidities and mortalities. It was noted that Limpopo’s institutional Maternal Mortality rate has been escalating at an alarming rate with an increase on community maternal deaths. All the delegates agreed that the majority of the causes of the maternal deaths are preventable and that working together can make a huge impact in reducing the current escalating maternal deaths. From the perspective of NICSA and Traditional Health Practitioners, abortion is leading as the cause of Maternal Deaths outside health care facilities. This is due to very easy access to the many unscrupulous illegal Abortionist in the villages: This illegal Abortionists creates tension between the registered traditional healers and healthcare officials. Traditional healers are blamed for the maternal morbidities and deaths arising from illegal activities by the unscrupulous Abortionists. The majority of patients and the family members of women who have undergone illegal or unsafe backyard Abortion keep these as a secret. One has to be meticulous with history and diligent with clinical examination not to miss the diagnosis of unsafe TOP.
191

The Forensic Pathologist Specialist for Vhembe, attested to this practice of keeping the act undercover and indicates that the only time it will surface is when there is maternal death. There is a cultural belief prohibiting the burial of a mother with a fetus, and the district pathologist will be engaged for the post-mortem and delivery of the dead fetus. The maternal death will be an accidental discovery. These deaths are missed from the NCCEMD data and the DHIS as the forensic pathologist do not have the maternal death notification forms. The other factors compounding the missing of many community maternal deaths, is when the deceased woman even when pregnant is certified by general practitioners at home, traditional healer’s place and at our health facilities (casualty and clinics) as dead on arrival and death is ascribed as due to natural causes like pneumonia and other sicknesses as it will be narrated by the family of the deceased. The corpse is then handed to the funeral parlour whose interest is in the burial business of the corpse. The maternal death notification and surveillance needs to be improved to involve all the relevant stake holders concerned, i.e the community, the public and private (general practitioners) health care facilities, funeral parlours and the forensic pathology department. With the current status it is very likely that many community maternal deaths have been missed in the past as “natural deaths”. NICSA is very concerned about the mushrooming of this unregistered traditional healers and illegal Abortionists in the community. One of the major stumbling block dealing with this unscrupulous Abortionist is the legal framework of arresting these perpetrators as there should be a complainant to open the criminal case. The complainant unfortunately is the victim who has undergone the illegal unsafe TOP and does not want to divulge who, how, when and where the procedure was performed. Delay in referring the patients by some of the traditional and faith healers to medical facilities for joint management of the female patient for ANC and other treatment which are beyond the scope of the traditional healers was one of the areas of concern acknowledged by both parties which
192
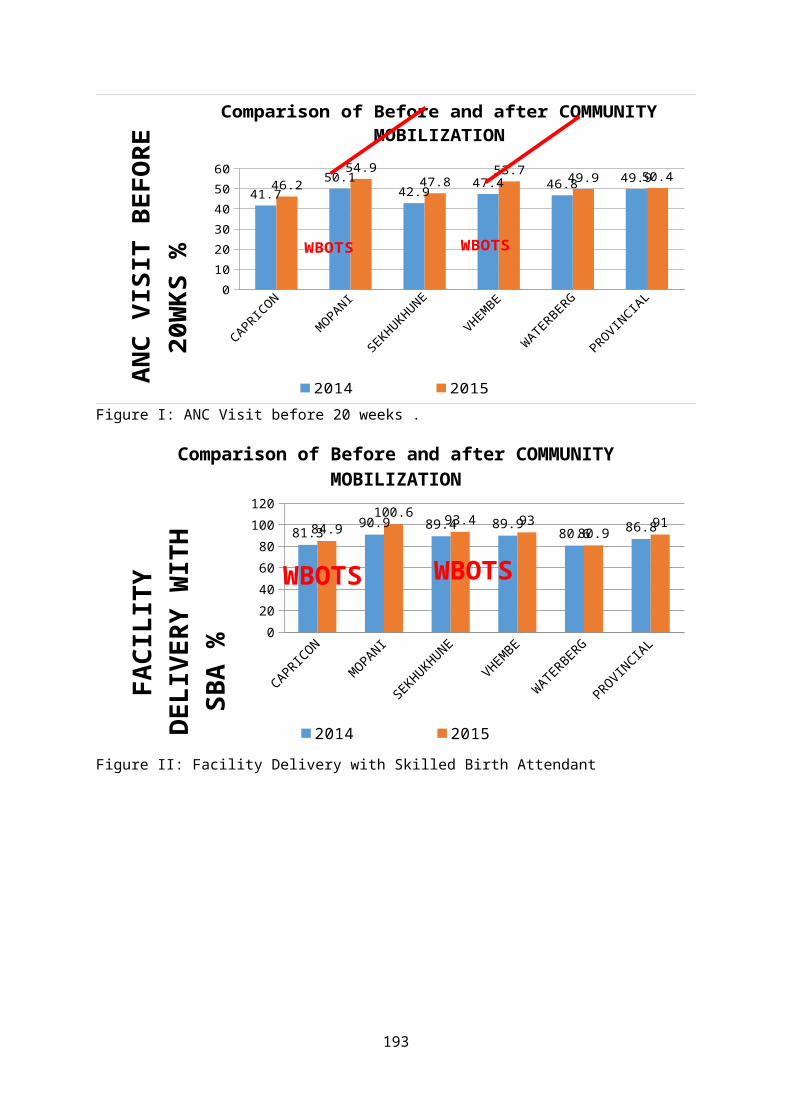
deserve attention. The traditional and faith healers could only accept that this situation happens in some cases where they were not aware that the woman was pregnant and requested to be assisted with pregnancy testing. The latest focus is on a healthy working relationship with the members of the police service and forensic pathology to report maternal deaths found at home or anywhere outside health facility. A continuous awareness is created amongst the health professionals to identify maternal deaths happening elsewhere in the facility other than the gynaecological wards and maternity units.
Results:Deaths reported included mothers who suddenly collapsed and were certified dead either at a health facility or by EMS- excluding inter-facility transfers, found dead by partners or relatives, victims of violence-stabbed or shot and bled to death, victims of motor vehicle accidents. Some deaths were reported by colleagues-doctors and midwives and other co-workers- while attending funerals of relatives. A follow-up would be made with members of the family and the maternal death would then be confirmed.Many community maternal deaths continue to be missed as these deaths are certify outside health facility as deaths arising from natural causes by the General Practitioners. Maternal deaths encountered by the Forensic Pathologist are also not notified as they do not have the MDNF forms.MD in Limpopo has increased in the last triennium of 2011-2013, 759 deaths with 30 CMD reported. For the period January to December 2014, 225 deaths with 13 CMD reported and 204 deaths with 10 CMD for the year 2015. See figure I.Maternal deaths outside of facility in Limpopo had the following: Found dead by partners or relatives, victims of violence who got stabbed or shot and then bled to death, victims of motor vehicle accidents, and those reported by colleagues-doctors and midwives and other co-workers while
193
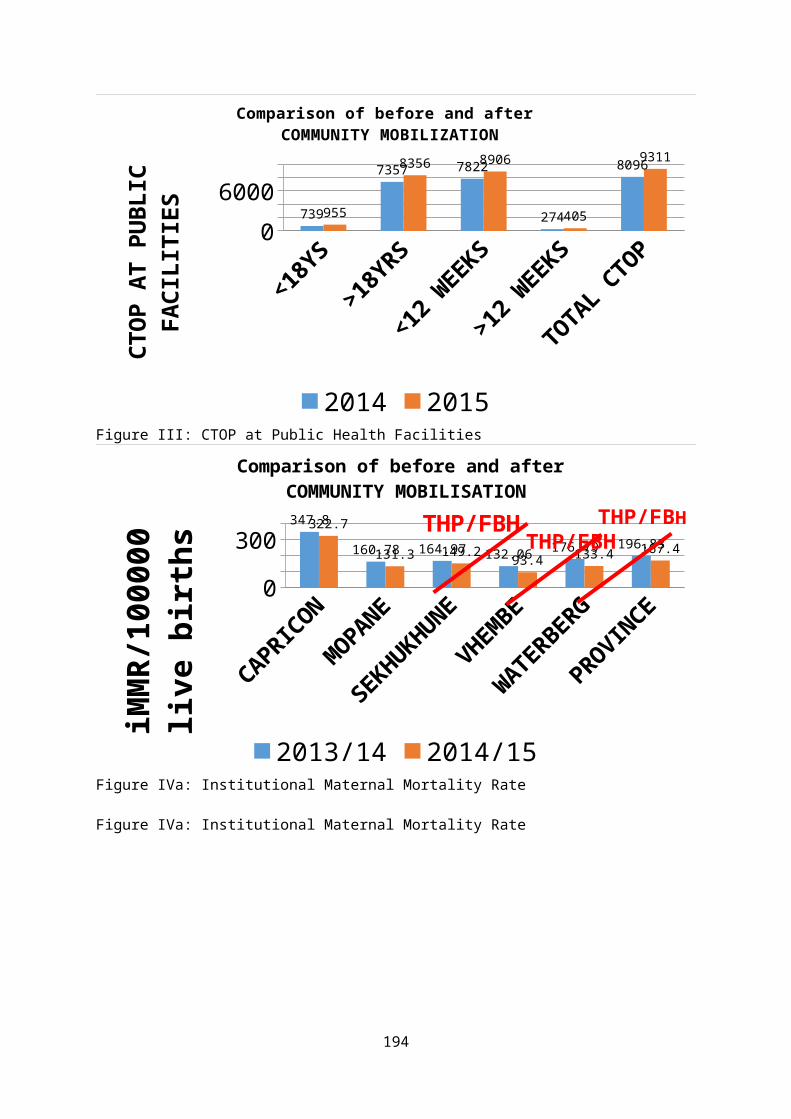
attending funerals of relatives. A follow-up would be made with members of the family and the maternal death would then be confirmed.Avoidable factors were identified in 13 CMD for 2014 & 2015.Delay in seeking treatment contributed to more than 21 %(5 patients). Lack of transportation delayed or prevented access to the health facilities in 10% of the rural deaths. Barrier to access to safe termination of pregnancy contributed to 3 CMD. Fifty-seven percent (5 patients) were related to the THP activities either remedies or delayed referral to public health facilities or lack of knowledge. Figure II-IIIMany maternal deaths continue to be missed as some General Practitioners (GP) often certify the cause of death as from natural causes. There is a need for education to the public and GP’s about Maternal Death(MD).
Findings and recommendations:Maternal deaths encountered by the Forensic Pathologist are often not notified as they do not have the Maternal Death Notification Forms. There is a need for maternal deaths forms to be placed at the department of Forensic pathology. There is a need for the district municipality to formulate by-laws to be able to deal with this scourge of Illegal Abortionist and the increasing number of unregistered traditional and faith healers in our communities.Community maternal deaths are related to:
Complications of abortions performed by illegal abortionist, mainly to the teenagers and elderly women due to unplanned and unwanted pregnancies, indicating a problem with access to TOP services from our public institutions.
Delay in referring the patients to the state health care center from the Traditional Health Care Practitioners.
Logistics (location of the traditional healers) and with the traditional healer unaware that their client was pregnant.
194
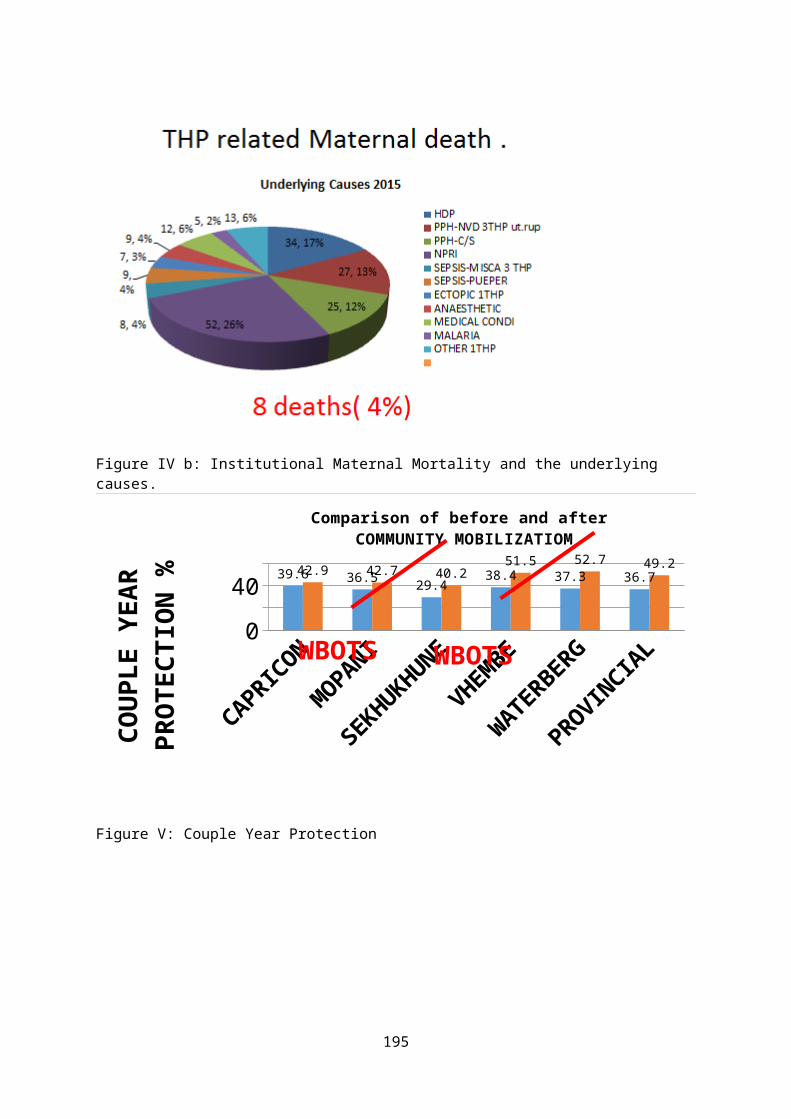
Late maternal death is currently not accounted and mostly misclassified.Appropriate community and health-service interventions to reduce maternal mortality need to be explored such as health education and improving co-operation with the traditional health care practitioners and public health care system.To create a working relationship with the members of the police service and forensic pathology to report maternal deaths found at home or anywhere outside health facility.A continuous awareness program has to be created amongst the health professionals to identify maternal deaths happening elsewhere in the facility other than the gynaecological wards and maternity units.Any community death of a woman from 9 years should be investigated to exclude community MD.Multi-center site investigations on Community Maternal Death is recommended.A check list form for conducting verbal autopsy adapted from CARE Sierra Leone LIFT‐UP study created with the focus group is recommended. Annexure 1.
Figure I : Reported institutional (iMD) and community (CMD)
AGE
Probable CAUSE
Social Factors
?PREVENTABL
195
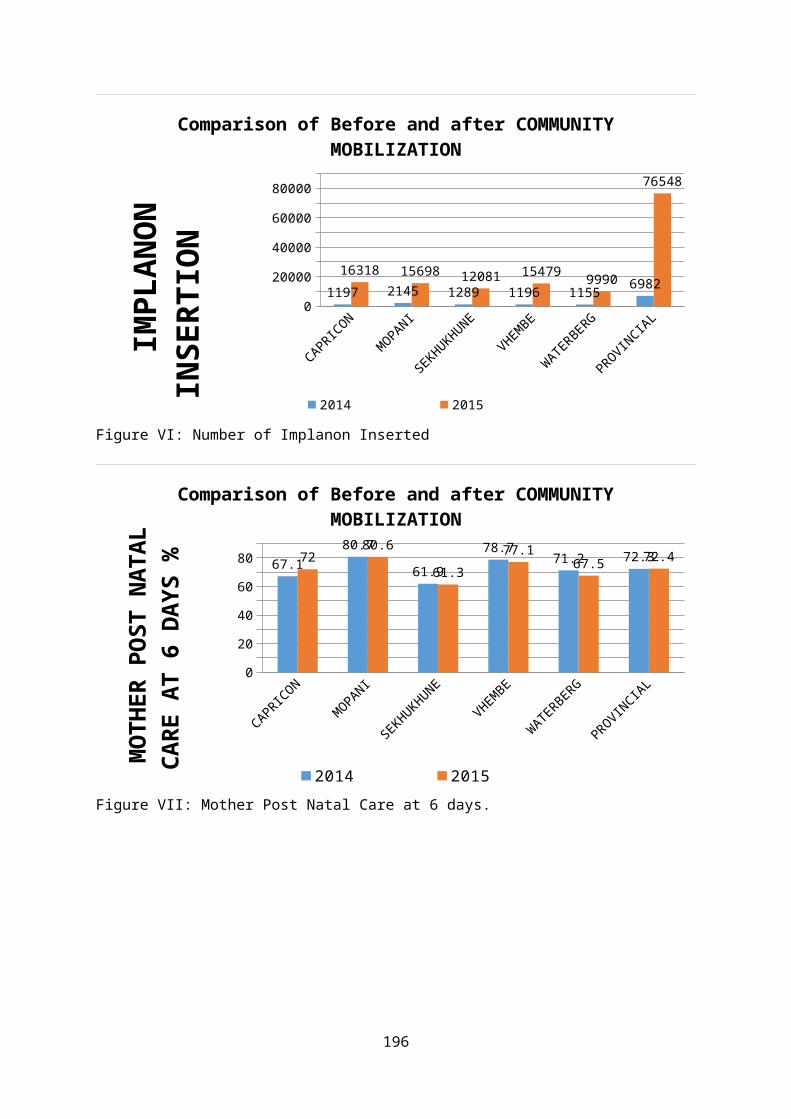
E28yrs MVA none35 yrs
CARDIAC Distance/access
yes
32 yrs
PPH THP yes
21 yrs
ECCLAMPSIA THP yes
35 yrs
Pulmonary Embolism
Financial/access
yes
33yrs
Mutilation by Panga
Family Violance
yes
23- 38yrs
7 Unkown
Figure II: 2014 Community maternal deaths.n=13
AGE
Probable CAUSE
Social Factors
?PREVENTABLE
9yrs Septic abortion(SA) Access for CTOP Yes . 16ys Suicide Access for CTOP Yes35ys MVA NO44yrs
SA from Unsafe TOP Access for safe CTOP
Yes
25yrs
Collapsed ?
27yrs
HIV+ at THP THP Yes
24yrs
Ecclampsia +Herbal Med
THP yes
22yrs
Ectopic THP yes
38yrs
Chronic H/T Delayed seeking yes
28yrs
Unknown
196
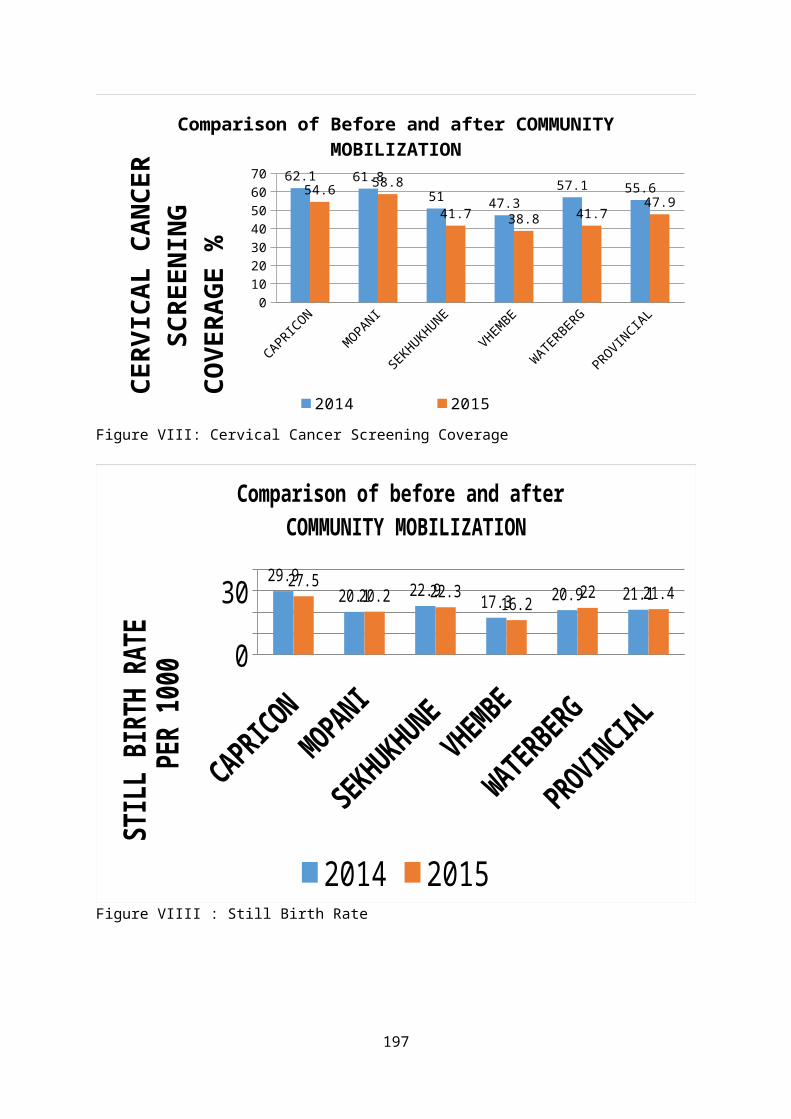
Figure III: 2015 Community maternal deaths.n=10
Department of Health
COMMUNITYBASED MATERNAL DEATH REVIEW FORMCOMMUNITY BASED INVESTIGATION (Verbal Autopsy) QUESTIONNAIRE FOR INVESTIGATION OF
MATERNAL DEATHS(To be filled by investigation team, ref: para 4.12 & 4.13 of MDR guidelines)
Name of District: ………………………………………………… Block: ………………………………………………….
NAME OF THE SUB CENTRE
NAME OF THE VILLAGE
NAME & AGE OF THE PREGNANT WOMAN/MOTHER (DECEASED)
ADDRESS
NAME OF HUSBAND/OTHER(FATHER/MOTHER)
PLACE OF DEATH (Home/institution/In transit/Village/Town etc.) Specify
DATE & TIME OF DEATH
NAME & DESIGNATION OF THE INVESTIGATOR(S) ALONG WITH MOBILE PHONE NUMBERS
DATE OF INVESTIGATION
PROBABLE CAUSE OF DEATH
197
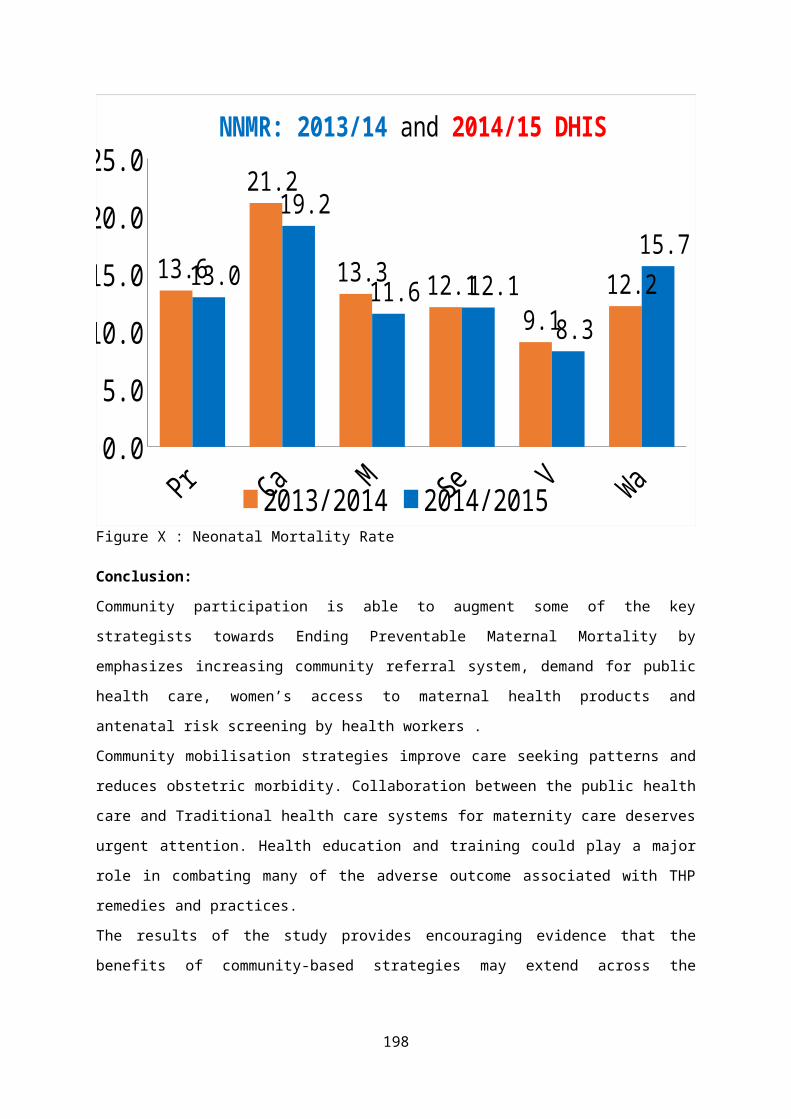
MODULES
MODULE - I Page No. 1 - 2
Should be used for collection of general information for all maternal deaths irrespective of whether deaths occurred during antenatal or intranatal or postnatal period or due to abortion.
MODULE - II Page No. 3 - 4
Should be used for the deaths occurring during the antenatal period including abortion MODULE - III Page No. 5 - 8
Should be used for the deaths occurring during delivery or postnatal period
GENERAL INSTRUCTIONS1. The Community Based Investigation (Verbal Autopsy) is a technique whereby family
members, relatives, neighbours or other informants and care providers are interviewed to elicit information on the events leading to the death of the mother during pregnancy/ abortion/ delivery / after delivery in their own words to identify the medical and non medical (including socio-economic) factors for the cause of death of the mother.
2. It is preferable to give advance information about the purpose of visit to the relatives of the deceased who were with the mother from the onset of complications till the death, and obtain their consent.
3. CONFIDENTIALITY: After the formal introduction to the respondents, the investigating official should give assurance that the information will be kept confidential.
4. Throughout the interview, the interviewer should be very polite and sensitive questions should be avoided.
5. Make all the respondents seated comfortably and explain to them that the information that they are going to provide will prevent death of mothers in
198

MODULE – IContains general information, information about previous pregnancies wherever applicable. It should be used for all the maternal deaths irrespective whether occurred during antenatal, delivery or postnatal period including abortion)
I. BACKGROUND INFORMATION Tick (√) the correct answer for each question:
1.1 Resident/Visitor death1.2 Type of death Abortion Antenatal Delivery
deathPost natal
1.3Place of death
Home Sub health Centre
CHC PHCMedical college Hosp.
Dist. Hosp.
Sub Dist. Hosp. Pvt. Hosp.Transit/on the way
Others (specify)
1.4 Specify the name and place of the institution or village where death occurred
1.5 Onset of fatal illness Date / / Time _ _: _ _ _ _1.6 Admission in final institution (if
applicable)Date / / Time _ _: _ _ _ _
1.7 Death Date / / Time _ _: _ _ _ _1.8 Gravida 1 2 3 4 5&more1.9 Para (number of previous live
births)0 1 2 3 4&more
1.10 Abortions(induced or spontaneous)
0 1 2 3 4&more
1.11 Previous stillbirths 0 1 2 3 4&more1.12 Living children 0 1 2 3 4&more1.13 Weeks of pregnancy if
applicable<16 weeks
16-28 weeks
>28 weeks
1.14 Age at death2. FAMILY HISTORY
No Details Deceased Mother
2.1 Age at marriage
<18yrs18-25 yrs26-30yrs31-35 yrs36yrs or moreNot Married
2.2 Religion SikhHindu
MuslimChristianOthers
199
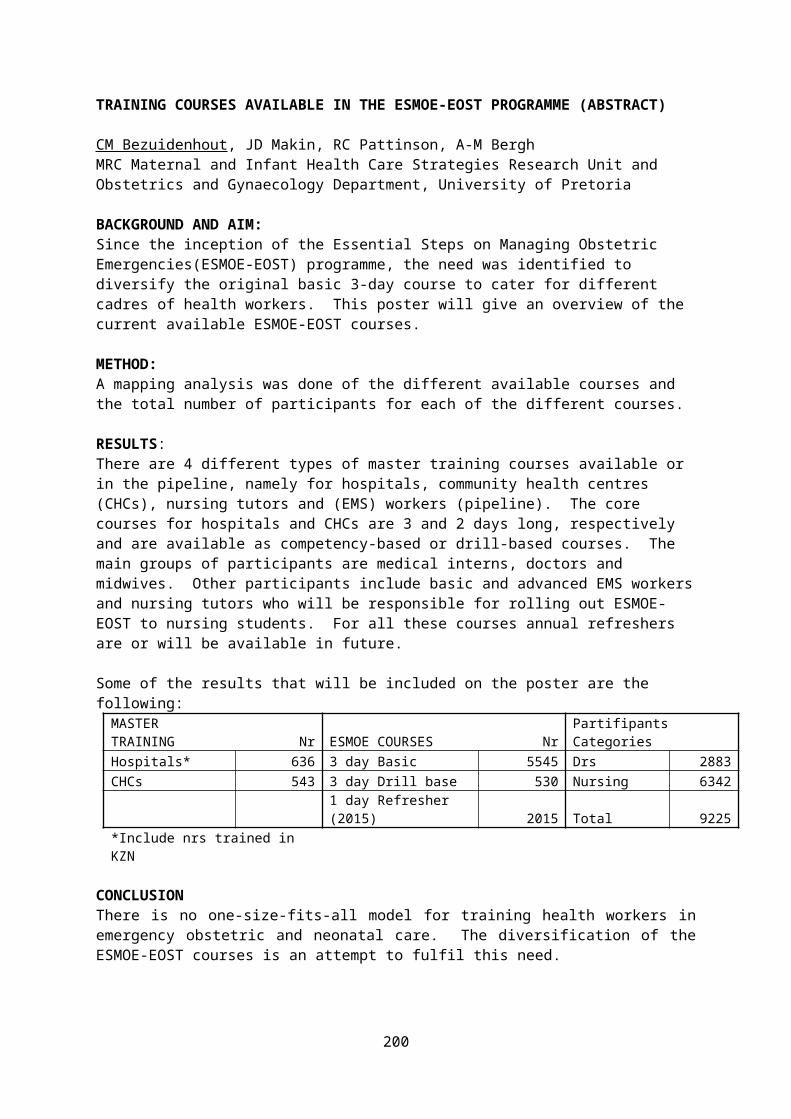
2.3 Community
SCSTBCOBCOthers
2.5 Occupation
House WifeAgri. LabourerCultivatorNon-Agri. daily wagesGovt .EmployeePrivate employeeSelf employedBusinessOther (Specify)
2.6 Education
IlliterateUpto 8th standardUpto 12th standardGraduate
3. INFANT SURVIVAL3.1 Infant status: Still
birthlive Birth
Died immediately after birth
Alive at 7 days Alive at 28 days
4. AVAILABILITY OF HEALTH FACILITIES, SERVICES AND TRANSPORT(4.1 & 4.2 to be filled by the investigator before the interview)
4.1 Name and location of the nearest government/private facility providing Emergency Obstetric Care Services
4.2 Distance of this facility from the residence
4.3 Number of institutions visited before death (in the order of visits)
4.4 Reasons given by providers for the referral
No explanation given
Lack of blood
Lack of staff Others (specify)
4.5 Used 108:Y/N5. CURRENT PREGNANCY (to be filled from the information given by the respondents)
5.1 Pregnancy Registration YES NOAntenatal Care YES NO
5.2 If yes, place of Antenatal checkup
Sub Centre PHC/CHCGov. Hosp. Pvt. HospitalVHND Govt. & Pvt. Hospital
5.3 Number of antenatal check ups
Nil 4 and above 1-3 Not Known
5.4 Hb Level 5.5 High Risk category: Y/N
5.6 Told About Risk Factors: Y/N
5.7 Name & phone no. Of concerned ANM
200
MODULE - 116. DEATHS DURING THE ANTENATAL PRIOD(This module to be filled for the maternal deaths that occurred during the antenatal period including deaths due to abortion. In addition to module –II, module – I should also be filled for all maternal deaths)
6.1 Did the mother had any problem during antenatal period?
Not knownNOYes
6.2 If yes, was she referred anytime during her antenatal period?
YES
Don’t know
6.3 What was the symptom for which she sought care?
Headache
Edema
Anemia
High Blood Pressure
Bleeding p/v
No foetal movements
Fits
Sudden excruciating pain
High fever with rigor
Other (specify)
6.4 If YES, did she attend any hospital?
YES NODon’t know
6.5 In case of not seeking care from the hospital is it due to
Severity of the complications not known
Institution far away
No attendant available No money
Beliefs and customs Lack of transport
Others ( specify)
7. FOR ABORTION DEATHS FILL THE FOLLOWING QUESTIONS7.1 Did she die while having
an abortion or within 6 weeks after having an abortion?
While having an abortion
Within 6 weeks after having an abortion
Don’t know
7.2 If abortion, was the abortion spontaneous or induced, including MTP?
Spontaneous Induced MTP Don’t know
7.3 If the abortion was Oral medicine Traditional Instrumentati Don’t know
201
induced, how was it induced?
vaginal herbal application
on
7.4 If the abortion was induced, where did she have the abortion?
Home Government hospital (specify level)
Private clinic/center
Don’t know
7.5 If the abortion was induced, who performed the abortion?
Doctor Nurse Others (specify)
Don’t know
7.6 If induced, what made family seek care?
Bleeding started spontaneously Wanted to terminate the pregnancy
7.7 If the abortion was spontaneous, where was the abortion completed
Home Govt. Hospital (specify level)
Private clinic/centre
Don’t know
7.8 How many weeks of pregnancy completed at the time of abortion
7.9 Whether she had any of these symptoms after abortion?
High fever Foul smelling discharge
Bleeding Shock
7.10 After developing complications following abortion, did she seek care?
7.11 If yes, whom/where did she seek care?
Government hospital (specify level)
Private clinic/center
Quack Don’t know
7.12 In case of not seeking appropriate care, is it due to
Severity of complications not known
Beliefs and customs
No money
No attender available Institution far away Lack of transport
Not applicable Others, please specify
7.13 Date of spontaneous abortion/date of termination of pregnancy
7.14 Date & time of death
MODULE - III(To be used for the deaths occurring during delivery, for these deaths, Module I should also be filled)8. INTRANATAL SERVICES (Tick “√” wherever applicable)
8.1 Place of delivery Home Sub centreCHC PHCMedical College District HospitalSub district Hospital Private HospitalTransit Any other place
(specify)8.2 Admission (not
applicable for home Date / / Time _ _: _ _ _ _
202
delivery and transit)8.3 Delivery Date / / Time _ _: _ _ _ _8.4 Time interval
between onset of pain and delivery (in hours)
Hours: _ __ _ _ _
8.5 Who conducted the delivery – if at home or in private institution (Not applicable for transit delivery)
ANM Staff Nurse/M . Asst
Doctor Dai
Quack Others
8.7 Type of delivery NormalAssisted Caesarean
8.8 Outcome of the delivery
Live birth Still birthMultiple births
8.9 During the process of labour/delivery, did the mother have any problems?
Prolonged labour primi>12 hrs subsequent deliveries >8 hrs
Severe bleeding/ bleeding with clots – (one salwar/saree/skirt soaked =500ml)
Labour pain which disappeared suddenly
Inversion of the uterus
Retained placenta Convulsions
Severe breathlessness/cyanosis/oedema UnconsciousnessHigh fever Others (specify):
8.10 Did she seek treatment, if yes by whom and what was the treatment given by the ANM/Nurse/LHV/MO/others? (give details)
8.11 Was she referred? YES NO
Not Known
8.12 Did she attend the referral centre?
YES NO
Not KnownIf yes, time interval between admission & delivery (if delivered)
8.13 In case of noncompliance of referrals, state the reasons
Intensity of complications not known
Institution far away
No attendant available No money
Beliefs & Customs Lack of Transport
Others
8.14 Was there delay in Decision making Mobilizing fundsArranging transport others
8.15 Any information given to the relatives about the Yes No
203
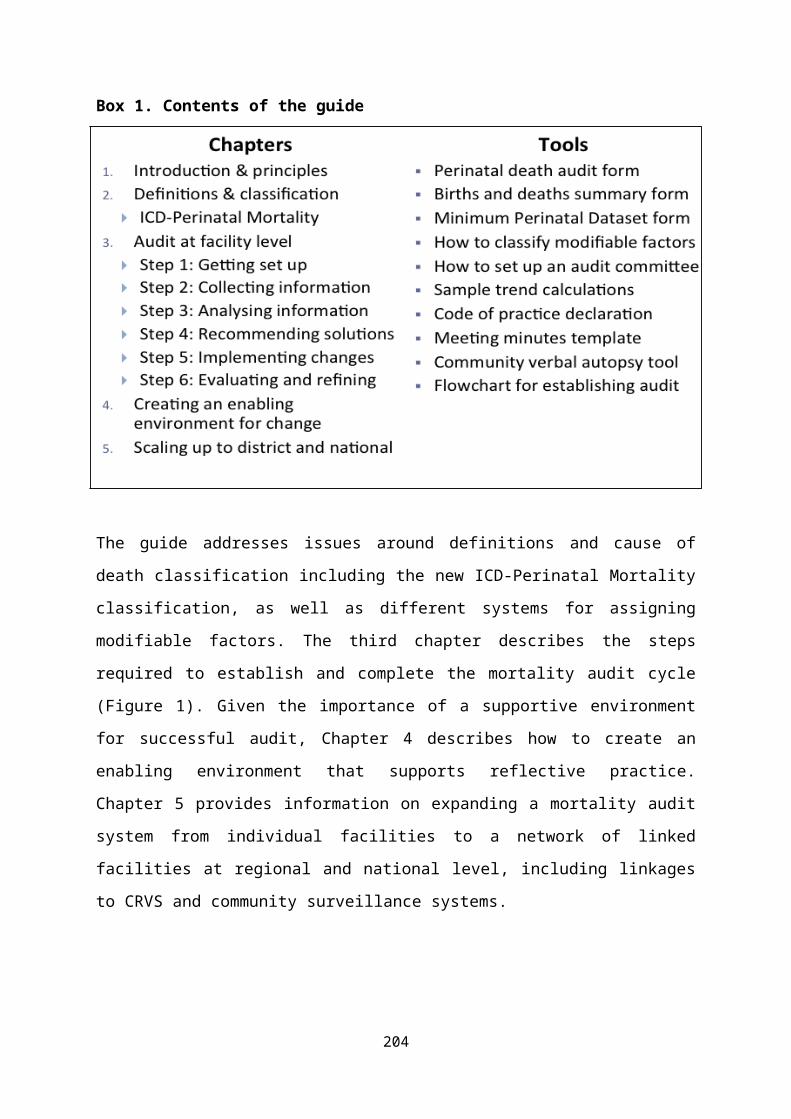
nature of complication from the hospital
8.16 If yes describe
8.17 Was there any delay in initiating treatment
Yes No
8.18 If yes, describe
9. POST NATAL PERIOD (Tick ‘√’ wherever applicable)9.1 No. Of Postnatal checkups Nil < 3 checkups
>/=3 checkups Don’t know9.2 Did the mother had any
problem following delivery
YES NoNot known
9.3 Time interval between detection of complication & death( in hours/minutes)9.4 Specific problem during
post natal periodSevere bleeding Severe fever and foul
smelling discharge
Sudden chest pain & collapse
Unconsciousness/visual disturbance
Bleeding from multiple sites
Severe leg pain swelling
Abnormal behaviour
Severe anemia
Others (specify)
9.5 Did she seek treatment Yes No
9.6 If yes, by whom ANM Nurse
LHV MO Others (specify)
9.7 What was the treatment given (give details)
9.8 Was she referred? Yes NoNot Known Not applicable
9.9 Did she attend the referral centre?
Yes NoNot Known Not applicable
9.10 In case of non compliance of referrals, state the reasons
Intensity of complications not known
Institution far away
No attendant available
No money
Beliefs & customs Lack of transport
Others (specify):
204
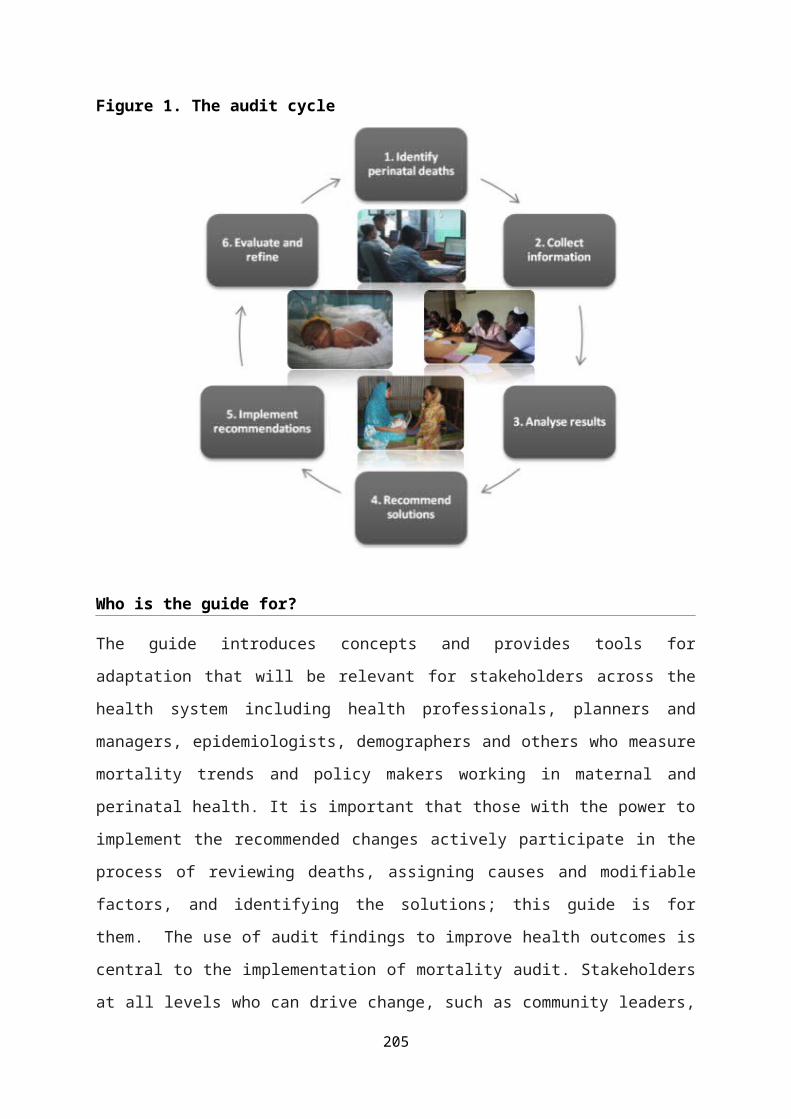
10. REPORTED CAUSE DEATH
10.1 Name and address of the facilities she went – decisions and time taken for action
Yes No
Don’t known
10.2 If yes, what was the cause of death?
11. OPEN HISTORY (In narrative form): (explore)11.1 Name and address of the facilities she went – decisions and
time taken for action11.2 How long did it take to make the arrangements to go from first
centre to higher centers and why those referrals were made and how much time was spent at each facility and time spent at each facility before referrals were made and difficulties faced through the process
11.3 Transportation method used11.4 Transportation cost? (at each stage of referral)11.5 Travel time – at each stage11.6 Care received at each facility?11.7 Total money spent by family11.8 How did the family arrange the money?11.9 Any other
Investigator – 1 Investigation – 2 Investigation - 3Signature Signature SignatureName: Name: Name:Designation: Designation: Designation:Place of posting: Place of posting: Place of Posting:Mobile Phone Number: mobile Phone Number: Mobile Number:Date: Date: Date:
205

AN AUDIT OF CAESAREAN SECTIONS AT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
Yasmin Adam, John Mwinyoglee, Bandile Masuku, Ermos NicolaouDepartment of Obstetrics & Gynaecology, Chris Hani Baragwanath Academic Hospital & the University of the Witwatersrand
Introduction:In 1985 the WHO convened a meeting with a panel of experts and it was decided that the ideal caesarean section rate should be between 10 and 15%. They have subsequently made a statement that “every effort should be made to provide a caesarean section to women in need rather than to achieve a specific rate”.
Caesarean sections are associated with short term and long term complications and are more expensive. Caesarean sections have an overall complication rate of between 11-14 %.Healthcare facilities may have caesarean section rates which are different from the country rate because of differences in the case mix of the populations served. Chris Hani Baragwanath Academic Hospital(CHBAH) is a Tertiary hospital which also provides district hospital services to four Medical Obstetric units. Therefore, a population based caesarean section rate does not apply to this hospital. Robson’s classification is a method of comparing caesarean section rates in a standardized manner. It is useful for looking at what factors (spontaneous labour, gestational age, previous caesarean section) contribute to the caesarean section rate, but does not say what the reason for the increase is.
The caesarean section rate at CHBAH was 34.45% in 2010 and increased to 39.78% in 2015. The hospital is a teaching hospital with doctors of different seniority. This study was undertaken to describe the indications of caesarean sections, the correctness of the indications and to categorize the caesarean sections using Robson’s classification. The short term neonatal and maternal outcomes were also described.
206
Methods:Study Setting:CHBAH is a tertiary referral hospital. Patients needing Tertiary care are referred to the hospital from three regional/secondary hospitals and one district hospital. There are four Midwife Obstetric Units that also refer patients to this hospital. The unit delivered 20 324 women in 2015.Study Design: A retrospective study using medical files of women who had a caesarean section performed between the 23rd of June to the 29th June 2015. Demographic factors, labour findings (for those women who had been in active labour), findings at caesarean section, immediate neonatal outcomes, and immediate maternal outcomes was recorded. At least two researchers evaluated the correctness of the indication. The data was entered into a redCAP database and analyzed using STATA version 14.Ethics Approval:Ethics approval was obtained from the University of the Witwatersrand Human Research Ethics Committee. Permission was also obtained from the CEO of the hospital.
Results:The rate of caesarean sections in this week was 49%. There were 148 women who had had a caesarean section and this was an analysis of 107 patients. The mean age of the women was 26.2 (SD±6.85), with a range of 15-42. The median parity was 1 (IQR=0-2, range-0-3). The median weight was 71.3 (IQR=60.0-82.7) with a range of 45.6 to 122.9.
The median haemoglobin was 11.3 (10.1-12.6; and a range of 5.1- 15.5). The table (1.1) below shows the co-morbidities and associated factors. All the women were using antiretroviral therapy. The median CD4 count was 316.5 (IQR=172-422, range- 80-731).
207
Table 1: Co-MorbiditiesCo-Morbidities Percentag
eRPR positive 1.1HIV positive 22.3Diabetes 1.9Hypertension, pre-eclampsia, eclampsia
27.1
Previous ectopic pregnancy 3.7Post dates 10.3Anemia 15.9Previous caesarean section 20.6Abdominal surgery 0.9No co-morbidities 13.1
The type of anaesthetic given was a spinal in 78.5% of cases, spinal/epidural in 0.9%, an epidural in 4.7%, a general anaesthetic in 15.0% and a spinal/general anaesthetic in 4.7%.
There was agreement with performing a caesarean section 85.5% of cases, there was no agreement in 2% of the case. Partial agreement was found in 10.5% of cases which meant an agreement with one of the indications and not all that was recorded in the file. In 2% of cases a decision could not be reached because of insufficient notes or no CTG in the file.
Fetal distress
Dystocia
Breech
Multiple pregnancy
Second Stage
Previous Caesar
IUGR
Pre-eclamsia/ecalmpsis
Abruption
Placenta previa
0 10 20 30 40 50 60
Percentage
Ind
icati
on
Figure 3: A description of the frequency of indications
The median birthweight was 2995g (IQR = 2435-3440, range-905-3930) and the median APGAR score was 10 (IQR=9-10, range of 5-10) at 5 minutes.
208
Figure 2:Seniority of doctor making the decision
4.2% 1.0%
67.7%
25.0%
2.1%
InternJunior MORegistrarConsultantUnknown
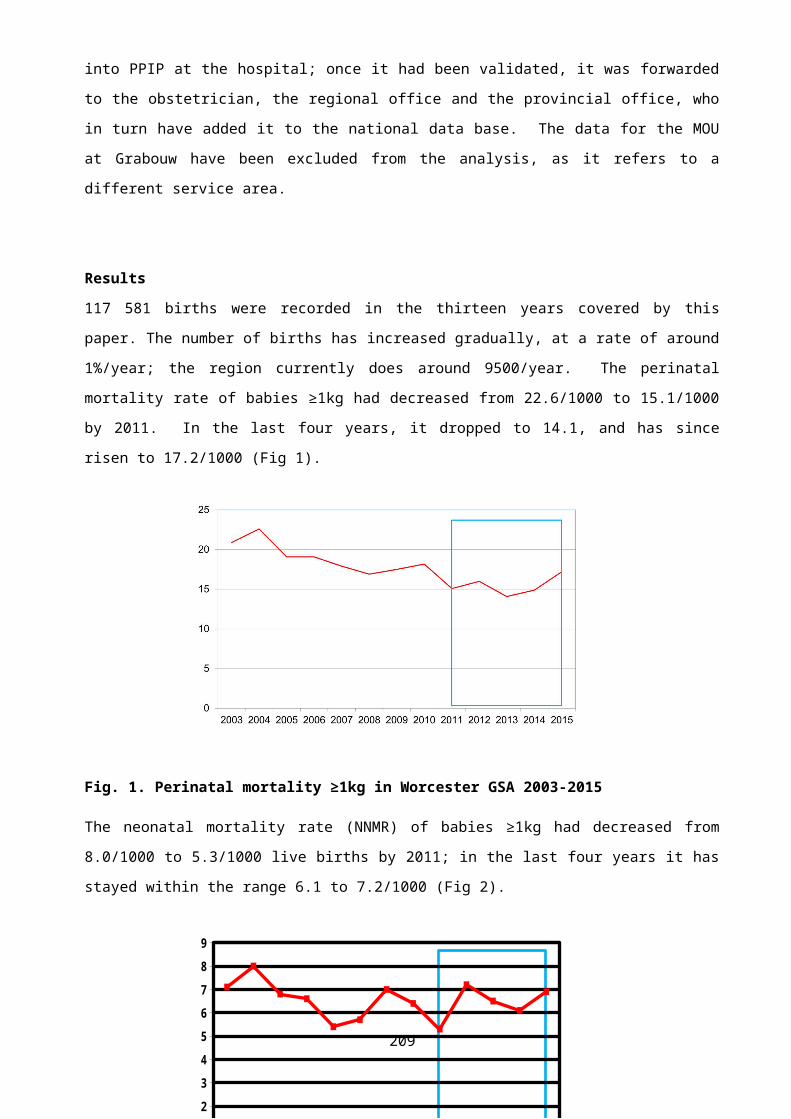
The complications are shown in table below. The anaesthetic related complication was a headache thought to be due to a spinal anaesthesia
Table 2: Complications
Complication PercentageMassive Blood transfusion 8.4Post-Partum Haemorrhage 14.0B-Lynch 2.8Ventilation (not for anaesthetic purposes)
8.4
Anaesthetic related 0.9Neonatal (mark from forceps at caesar)
0.9
Using Robson’s Ten group classification to categorise patients –we found the following
1. Nulliparous, single, cephalic, ≥ 37 weeks, in spontaneous labour (23.5%)
2. Nulliparous, single, cephalic, ≥ 37 weeks, induced or caesarean section before labour (9.2%)
3. Multiparous, cephalic, ≥ 37 weeks, in spontaneous labour (11.22%)
4. Multiparous, cephalic, ≥ 37 weeks, induced or caesarean section before labour (7.14%)
5. Previous Caesarean section, single, cephalic, ≥ 37 weeks (10.37%)
6. All nulliparous, single, breech presentation (1.0%)7. All multiparous, single, breech presentation, including
previous caesarean section (3.1%)8. All multiple pregnancies, including previous caesarean section
(3.1%)9. All abnormal lies, including previous caesarean section (1.02)10. All single, cephalic, ≤36 weeks, including previous
caesarean section
209
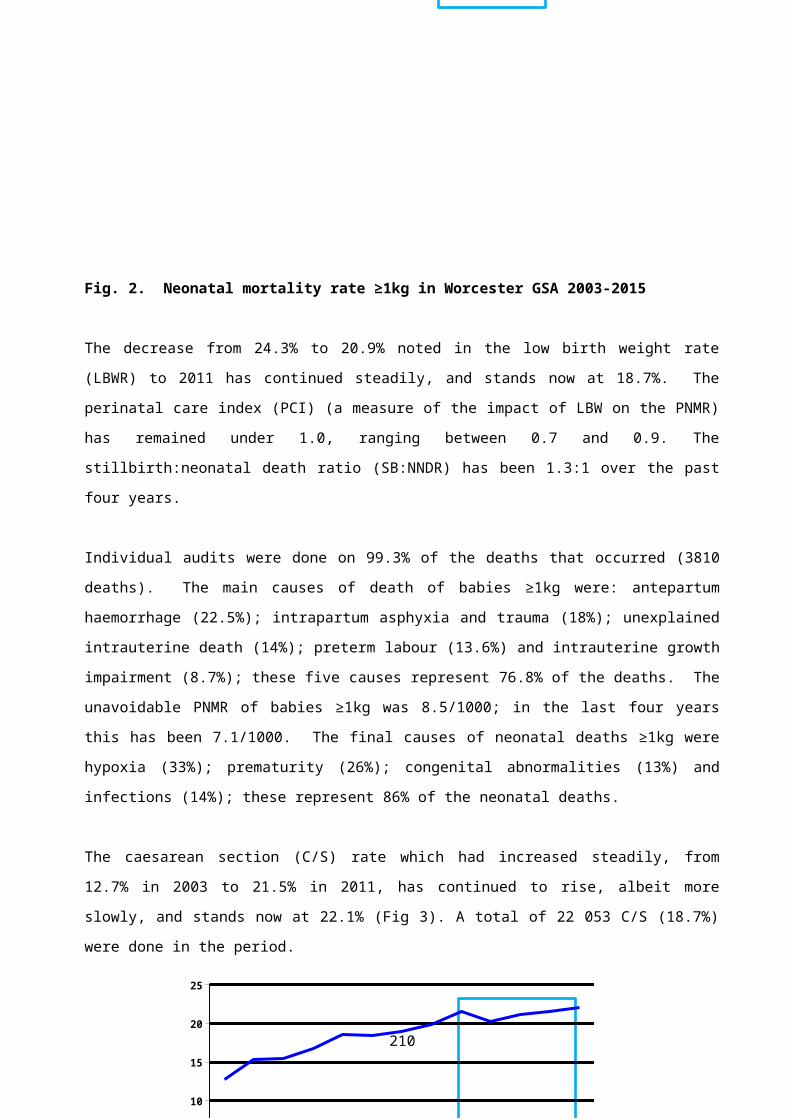
Discussion:Caesarean sections are on the rise all over the world. We can justify the rate of 49% for this week. The agreement of 85.5% was an absolute agreement. In more than 10%, there was agreement that a caesarean section needed to be performed, but that there was a difference in the indication noted or that one of the indications was not noted. We found that the most common indications for caesarean section was foetal distress, dystocia and previous caesarean section which is similar to that noted in other studies(6, 7). The use of electronic foetal heart rate tracing has been shown to have a high false positive rate, however we agreed with the diagnosis with foetal distress in most of the patients(8). We do not do any foetal blood tests to confirm a low pH in the foetus. We had a high Caesar rate in multiparous women in spontaneous labour of 11%. This may be because we are a district hospital to the four MOU’s and that the true denominator should be to include births in these MOU’s.The maternal complications were high and are a reminder that caesarean section is not benign and should be a justified procedure(9).
Conclusion:We believe that the caesarean section rate during this week of the 23 rd to the 29th June 2015 was justified. There may be room to doing Foetal Blood sampling to assess Foetal blood pH.
210
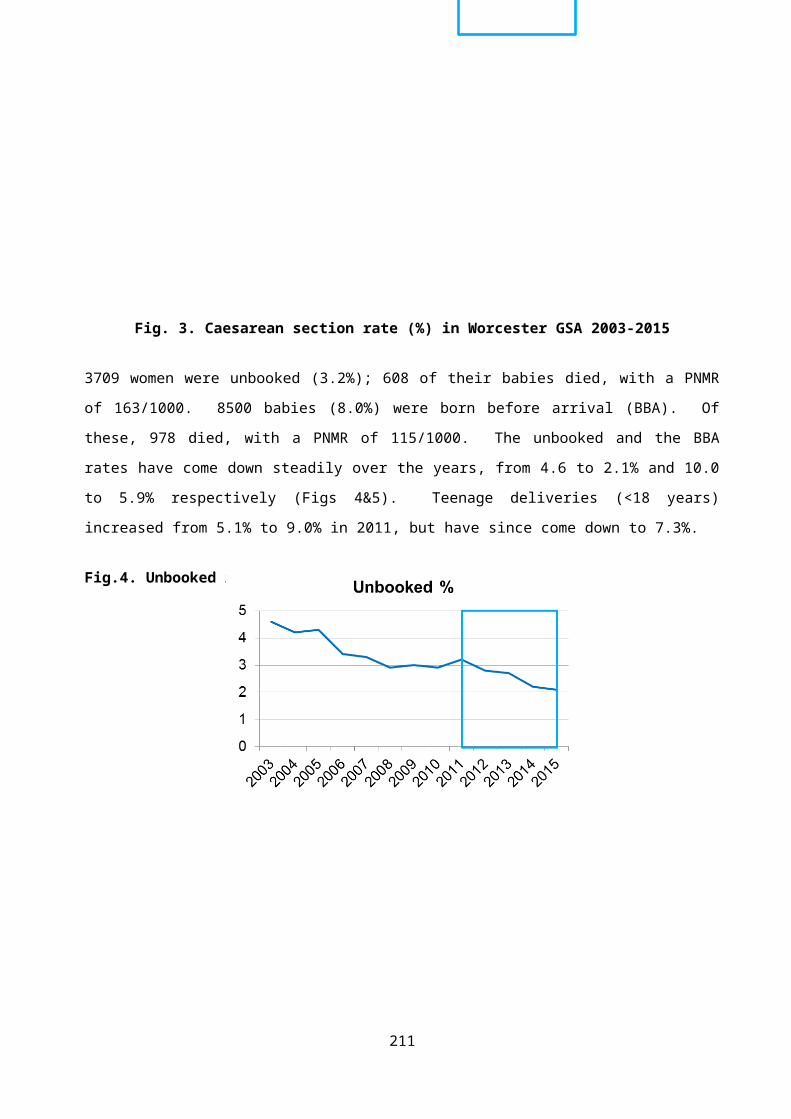
ACCEPTABILITY OF MIDWIFE OBSTETRIC UNITS IN FIVE DISTRICTS IN KWAZULU-NATAL
Voce, ASPublic Health Medicine, University of KwaZulu-Natal
IntroductionIncreasing the proportion of deliveries with skilled birth care in an enabling environment contributes to lowering maternal mortality ratios. Increasing the proportion of midwife-led deliveries contributes to increasing the proportion of deliveries with skilled birth care. The promotion of midwife-led deliveries is in line with evidence that supports midwife-led care as a safe, cost-efficient option of choice for the management of low-risk pregnancies and deliveries. In order to increase the proportion of midwife-led deliveries, and to improve access to skilled birth care and to life saving interventions closer to where women live, the KwaZulu-Natal Department of Health implemented a policy in 2012, of promoting Midwife Obstetric Units (MOUs). Three year’s post-inception of the policy, an assessment of the utilisation of the MOUs in five districts was commissioned by the KwaZulu-Natal Department of Health, with a view to informing further policy implementation. The assessment included examining the acceptability of MOUs to women and community opinion leaders.
MethodsA mixed method study, comprising both quantitative and qualitative data collection was implemented to explore: community perceptions of pregnant women; health seeking preferences of pregnant women for birth care; decision making process in selecting a delivery site; perceptions of midwife-led compared to doctor-led birth care; and experiences of having delivered in an MOU.Quantitative data was generated through interviews conducted with 258 pregnant women, recruited from antenatal clinics attached to the 25 MOUs in the Five Districts under investigation. Qualitative data was generated from open-ended questions incorporated into the questionnaire utilised with pregnant women, and from Focus Group Discussions conducted with women who had previously delivered in an MOU, and community opinion leaders. Quantitative data was analysed descriptively, reporting frequency distributions. Qualitative data was analysed using an inductive thematic approach.
ResultsThe respect and care granted to pregnant women reportedly differed according to the perceived status of the woman, whether by the community generally, the family or health workers. While 75% pregnant women reported knowing they could deliver in an MOU, 38% reported an intention to deliver in an MOU, and 42% reported a preference for midwife-led care. A majority of pregnant women (76%) reported they themselves, alone or with their partner, were the final decision makers with regard to where they would deliver. With regard to the relationship with the father of the current unborn child, 9% pregnant women reported no relationship, 73% reported a stable relationship but living apart, and 19% reported a stable relationship and living together. Challenges reportedly deterring the decision to deliver in MOUs included: previous experience when delivering in an MOU; 24-hour staff coverage not always available in the MOU; midwife attitudes; delayed emergency response-time; lack of provision of food; location of relatives. Reasons provided by pregnant women for preferring midwife-led compared to doctor-led birth care were similar and related to: the perceived competence of the health professional, the attitude and perceived
211
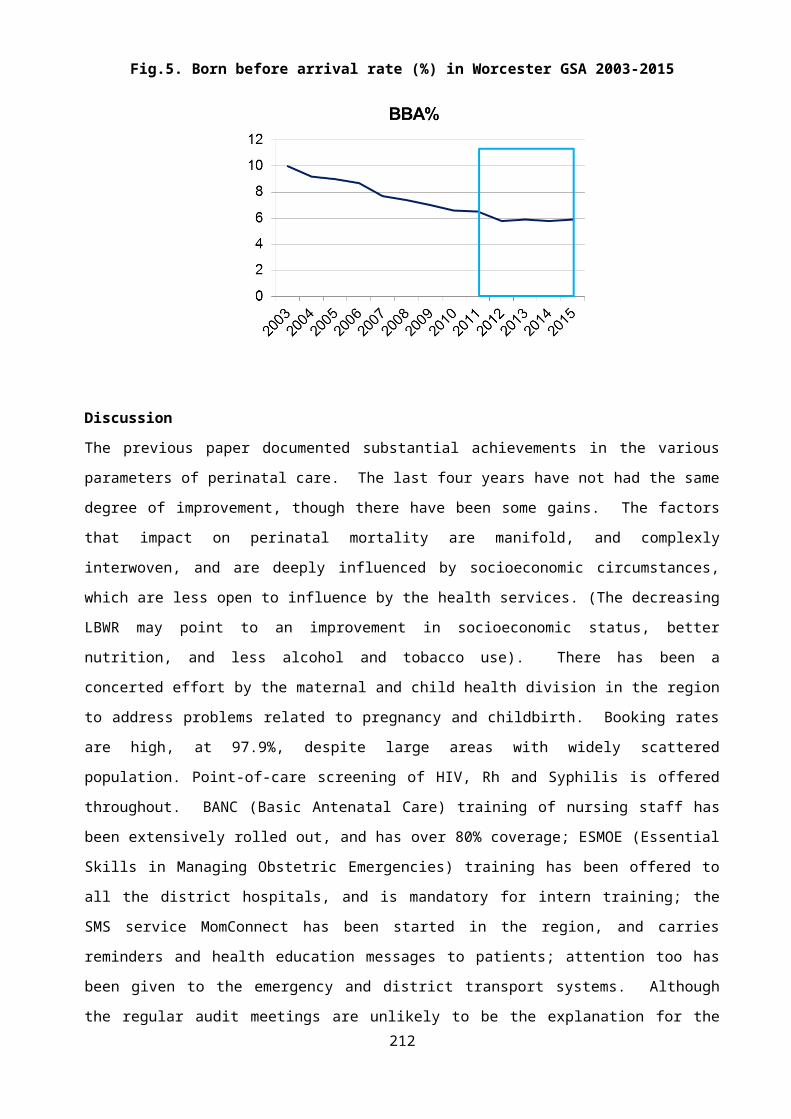
trustworthiness of the practitioner, previous experiences with a particular type of practitioner, and practicalities with regard to proximity of, and transport to the delivery site.
DiscussionThere is a distinction between preferred site of delivery and preferred attendant. The principal reasons provided for preferring the hospital as a delivery site relate to considerations about staffing, equipment, being able to get the care that is required and the promptness of emergency care in the event of complications, pointing to the need for ensuring fully functional and safe MOUs that provide quality care.Reasons provided for preferring midwife-led care to doctor-led care were similar and point to the need for a whole-system reorientation to client-centred care, engendering trust between pregnant women and health care providers through relationships that are caring and compassionate, respectful and responsive to individual questions and needs.
212
AUDIT OF MATERNAL NEAR MISSES IN THE METRO WEST MATERNITY SERVICES, CAPE TOWN
Ibe Iwuh, MBBS(MW), FCOG(SA), MMED(UCT)*, Sue Fawcus*, Leanne SchoemanDepartment of Obstetrics and Gynaecology, University of Cape Town
Introduction Maternal near miss describes a life threatening event or complication, occurring during pregnancy or within 42 days after the end of the pregnancy, which may lead to acute severe morbidity but not to death (R). Maternal mortality has been systematically monitored globally for many years, however near miss audits have recently gained some recognition by WHO and in both developed and developing countries. The Confidential Enquiry into Maternal Deaths in South Africa was introduced in 1998 and estimates the MMR to be much higher in South Africa than in developed countries but slightly lower than the average for sub-Saharan Africa. Recent statistics for 2012 by the Health Data and Monitoring group estimate the overall MMR to be 410 MDs per 100,000 live births. However, the institutional MMR as measured by the NCCEMD and presented in Saving Mothers reports has dropped from 176.2 per 100,000 in 2008- 2011 to 146.7 per 100,000 in 2011-2012. One of the first Near miss audits was conducted in Pretoria in …… ®.The benefits of auditing maternal near miss cases are: it allows health systems to review the quality of health care service; provides an opportunity to motivate for resources to facilitate training for health care workers and allows patient related factors to be examined in more detail because the patient survives and can describe them.In Metro West maternal mortality has been audited since 1953 but there has never been a near miss audit
Objectives 1) To measure the near miss rate, the maternal mortality ratio and the
mortality index in Metro West maternity services, Cape Town.2) To perform an in-depth investigation of the associated demographic,
213
clinical and health system factors of the near miss cases, 3) To provide input into the development of an on-going system of
auditing near misses cases in Metro West
Methods A retrospective observational study was conducted over 6 months between mid- March 2014 to mid -September 2014 in Metro West. This service includes 9 level one maternity facilities which refer all complicated maternal cases to two secondary hospitals, New Somerset (NSH) and Mowbray Maternity (MMH); or to the tertiary hospital, Groote Schuur Maternity Centre (GSH).All cases of near miss managed at the three hospitals were identified weekly by the author with the assistance of onsite health providers. These cases included near misses that occurred at level one facilities and were referred on to one or more of the three hospitals. Strict criteria were used to ascertain a case as a near miss according to the WHO near miss definitions. The folders of all the near misses were reviewed and relevant data entered into a data collection form which was adapted from the WHO near miss data form. In addition, these identified folders were reviewed by two senior obstetric specialists to confirm adherence to the WHO inclusion criteria for near miss classification, and also to determine avoidable factors in the management of the near miss cases. Maternal deaths occurring during the same time period of the Near Miss audit were identified from monthly mortality meetings and the ongoing maternal mortality audit system in Metro West.Live births occurring during the study period in all the 12 facilities of Metro West were obtained from CLINICOM and routinely measured perinatal statistics, for the denominator in measuring rates.
Results There were a total of 112 maternal near miss cases and 13 maternal deaths identified between the 15th of March 2014 and the 15th of September 2014 in the Metro West Maternity service. Therefore, the total
214
number of women with life threatening conditions (severe maternal outcomes) was 125 (total maternal deaths plus total near miss cases). There were 19,524 deliveries and 19,222 Live births in Metro West maternity facilities between March and September 2014. Table 1 shows the maternal near miss indicators.
Table 1 Near miss and maternal death rates and ratios Near miss Indicator Numbers, Rates, RatiosNumber Near Miss cases ( NM) 112Number Maternal Deaths (MD) 13Number Total Deliveries 19524Number live births 19222Near miss rate (NMR)* 5.83Maternal mortality rate (MMR) ** 67.6Severe maternal outcome rate(SMOR)*** 6.5Near miss : Maternal death Ratio 8.6 : 1Mortality index**** 10.4%
*NMR = MNM/ live births X 1000 **MMR = MD/live births X 100,000 ***SMOR = MDs + MNMs / live births X 1000 ****Mortality index = MDs/ MNMs+MDs x 100%
The maternal near miss rate was 5.83 near miss cases per 1000 live births and the maternal mortality rate was 67.6 maternal deaths per 100,000 live births The maternal near miss to maternal death ratio was 8.6:1; for every 9 near misses there was one maternal death. The mortality index was 10.4%; this means that of the 125 cases with life threatening conditions (severe maternal outcomes), 10.4% of them died.Table 2 shows the demographics characteristics of the women with near misses.
215
Table 2 Demographic characteristics of near miss cases. PARAMETER NUMBER PERCENTAGES AGE < 18 18-34 >35
49513
3.684.811.6
PARITY P0 P1-4 P5
46651
41.1580.9
RESIDENCE Mitchells Plain Gugulethu Mowbary Retreat Vanguard Han over Park Atlantis Vredenburg
274312116634
0.890.381.079.820.050.050.03
Booking Status Booked Unbooked
9913
88.411.6
HIV Status HIV positive HIV negative Unknown
25852
22.375.91.8
There were 25 (22.3%) of the near miss cases who were HIV positive. The majority of near misses 99(88.4%) had antenatal care. The largest number of near misses 72% were from poor suburbs; 43(38.4%) from the Gugulethu Area and 27 (24.1%) from the Mitchells Plain Area.Hypertension, obstetric haemorrhage and pregnancy related sepsis were the major obstetric complications causing the near miss cases accounting for 50 (44.6%), 38(33.9%), and 13 (11.6%) respectively (see Table 3). These three conditions all had low mortality indices; 1.9%, 1.9% and 0 for hypertension, pregnancy related sepsis and haemorrhage respectively.
216
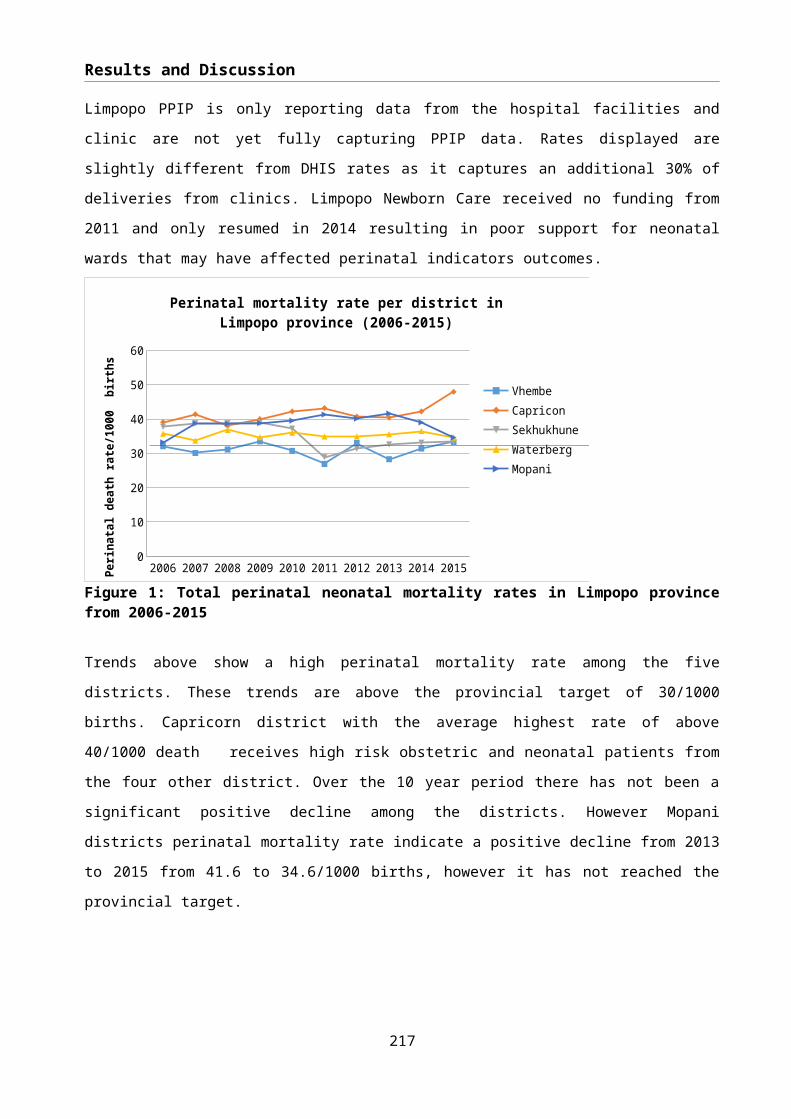
Table 3. Obstetric complications causing near misses; and their mortality indices Causes Number
s(%)
Mortality Index (%)
Hypertension 50 (44.6) 1.9Obstetric Haemorrhage 38 (33.9) 0.00Pregnancy Related Sepsis 13 (11.6) 1.9Non Pregnancy related infection
2 (1.8) 66.7
Acute collapse 2 (1.8) 33.3Medical/Surgical 7 (6.3) 33.3
Less common conditions causing near misses were medical /surgical conditions, non-pregnancy related infections and acute collapse; accounting for 7 (6.3%), 2 (1.8%), and 2 (1.8%) of near misses respectively. Although these numbers were small, these three conditions accounted for more maternal deaths with mortality indices of 66.7 %, 33.3% and 33.3% for non- pregnancy related infections, medical /surgical conditions, and acute collapse respectively.For the 112 near misses, there were 52 (46.4%) with one or more organ dysfunction, the most common being circulatory and respiratory dysfunction.In terms of clinical management, there were 141 critical interventions for the 112 near misses (some women had more than one). These included 39 (27.6%) of the near missess who had massive blood transfusion; 34 (24.1%) who had a hysterectomy; 45 (31.9%) who required intubation and ventilation; and 23 (16.3%) who were admitted to the tertiary hospital main Intensive Care Unit.Table 5 Critical Interventions for near miss casesCRITICAL INTERVENTION NUMBER (%) Blood transfusion 39 (27.6)Hysterectomy 34 (24.1%)Ventilation 45 (31.9%)ICU admission 23 (16.3%)
In terms of health system factors, 63 (56.3%) of the near misses occurred initially at a level one facility and were all referred to level 3 (GSH); 38 (33.9%) of near misses initially occurred at the secondary hospitals and 11(9.8%) at level 3 (GSH).
217
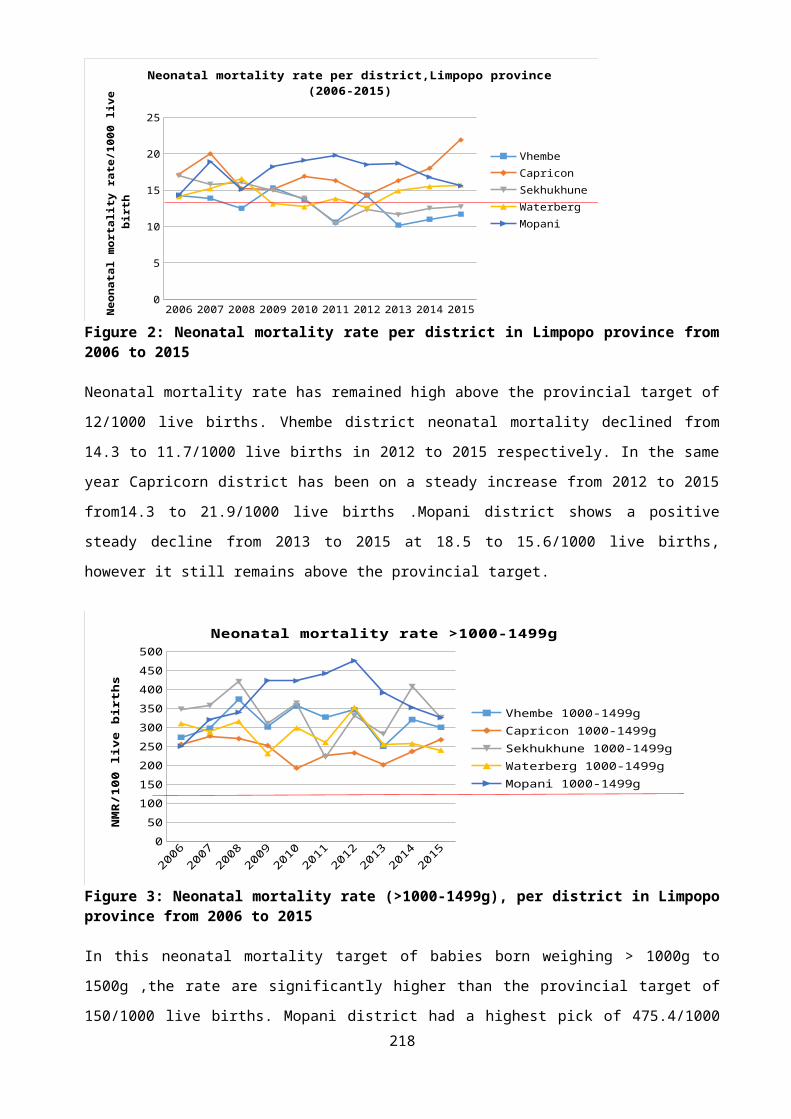
Table 6 shows the referral patterns: all near misses occurring at level one were referred to level 3; and 26 of the 38 occurring at level 2 were referred to level 3.
218
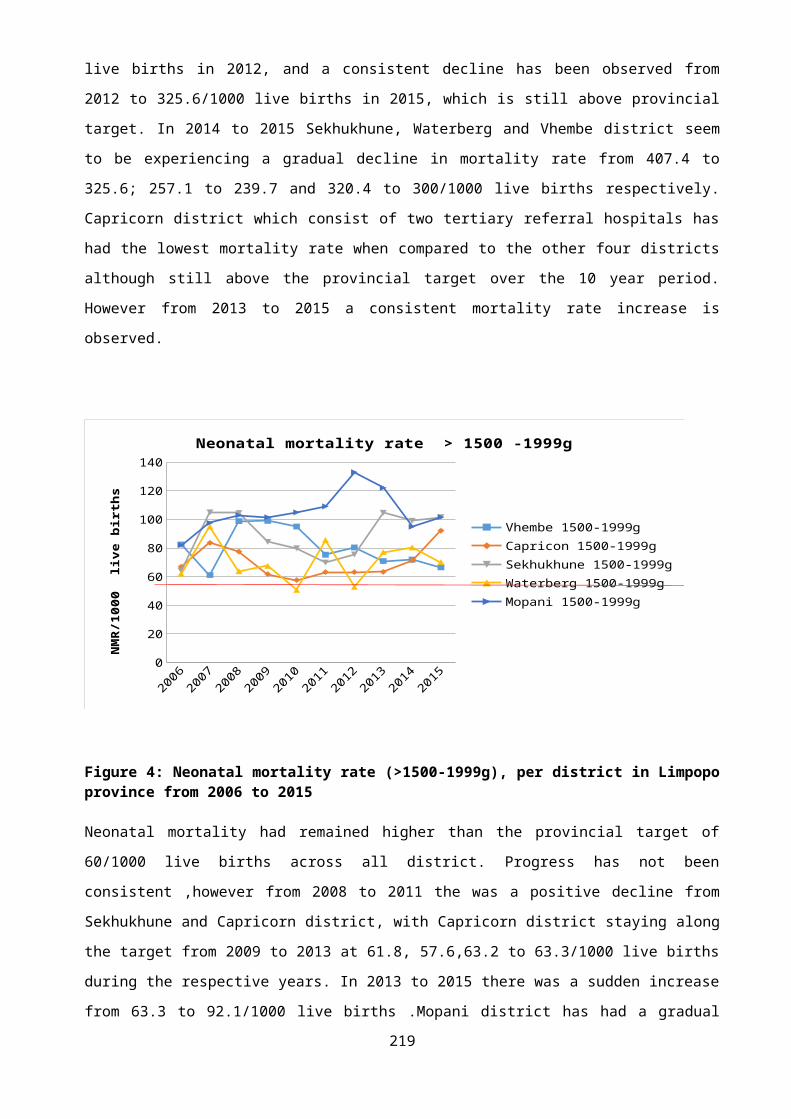
Table 6 Referral system Route Number of patients Percentages Level 1 to level 3 63 56.3Level 2 to level 3 26 23.2Occurred in level 3 11 9.8
Analysis of avoidable factors showed that, the most common problems were lack of antenatal clinic attendance (11.6%) and inter-facility transport problems (6.3%).For health provider related avoidable factors, the highest number of avoidable factors were identified at level 2 (38.2%), followed by level one (25.9%) and level 3 (7.1%). The most common factors were problem recognition, monitoring and substandard care.
Discussion The study used the WHO Near miss audit tool for defining and investigating near misses, as well as calculating rates and ratios. This tool was found to be useful but some adjustments were made to it to make it more relevant to our context. This study found the maternal near miss rate (MNMR) to be 5.83 per 1000 and maternal mortality ratio of 67.6 per 100, 000. This is similar in studies done in other developing countries such as Pakistan with maternal near miss rate of 8.6, India at 3-4.4 per 1000 and Bagdad 5.06 per 1000. In developed countries, such as Canada, UK and Scotland the MNMR is 0.7, 1.2 and 1.34 per 1000 respectively, which is very low compared to the rest of the African continent as well as some parts of Asia, but this is an indication of standard of care and service provision in these individual countries. Mortality and morbidity studies in the US found a MMR of 6.5 deaths per 100,000 LBs which is 10 times less than what we found in our study. However, the maternal near miss rate (MNM) rate in the US of 8.1 per 1000 is higher than the NMR of 5.83 in our study. The above findings support the suggestion that where there is low maternal mortality it might translate to high maternal near miss because those who survived but almost died will join the pool of women who are near misses.
219
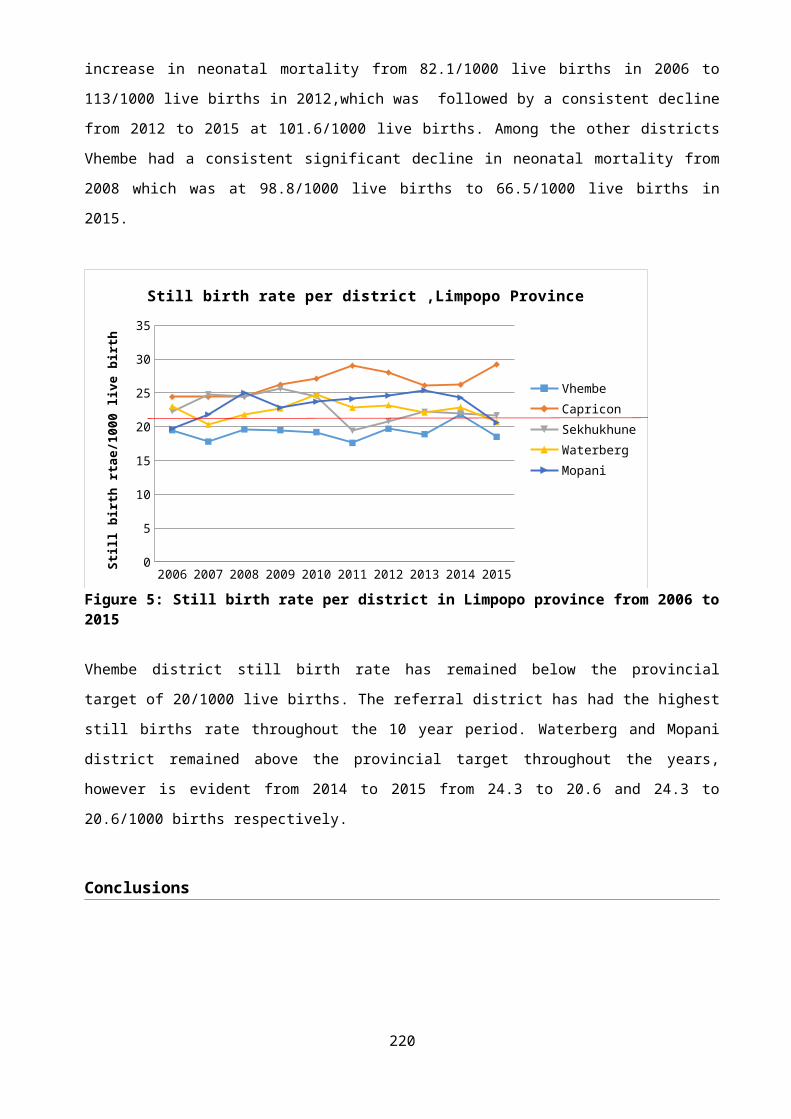
In our study, the maternal death to near miss ratio is 1:8.6 this means that for every 9 women who survived severe complications from pregnancy, 1 died.This finding of MD: MNM is similar to what they found in a prospective study in Brazil and Bagdad 1:8.6 and 1:9 respectively. However, in the Brazilian study they identified patients as ICU admissions, while in the study done in Bagdad, they followed the WHO strict near miss criteria; making the two studies not strictly comparable.The mortality index is used as an important parameter that expresses the quality or standard of care offered to patients in a particular system, the higher the figure, the poorer the quality of care provided, and vice versa.Our study found an overall mortality index of 10.4%, this is relatively higher that some Western countries, however comparable if not better than some other countries. A study in Karachi, had a MI of 12%, and in Bagdad, where they also used similar methodology involving the WHO criteria, the MI was 11%.Our MI was very low for Hypertensive disorders, PRS and OH at 1.9 %, 1.9% and 0% respectively. While for NPRI, AC and Med/Surgical disorders were 66.7%, 33.3 % and 33.3% respectively. In the Metro West Maternity Service, most of the practices and interventions for major obstetric emergencies such as APH, PPH, hypertensive disorders in pregnancy follow international standards set by WHO, NICE, RCOG and ACOG The MMR of 67.6 in our study is lower than for most other countries in sub Saharan Africa. For example, In Malawi the MMR I is 450 per 100, 000, in Nigeria it is 630, while in Sierra Leone it is 1003 per 100,000 live births. However, the figure for the Metro West is higher when compared with some countries in Europe or the American continent, for the UK it is 12, for the Netherlands it is 3-4 per 100 000 and for the US it is 8-12 per 100 000.The major cause of maternal deaths in our study was NPRI, which included HIV associated infections such as TB, PCP pneumonia and meningitis.In our study obstetric haemorrhage did not feature as a cause of maternal death but was the second most frequent maternal complication
220
associated with near miss. This is an important finding, reflecting that despite high numbers of patients with severe obstetric haemorrhage, the prompt and timely interventions according to protocols, prevented them from dying. Whereas our study had an OH MI of zero; other studies have shown higher OH MI, for example in Karachi they found the OH mortality index to be 17.2 %.However, while commending appropriate and timely management of obstetric haemorrhage in preventing death, it is also important to investigate whether any of the OH near misses could have been avoided by better preventative maternity care. Obstetric haemorrhage remains the second most frequent cause of maternal death in South Africa except for the Western Cape which is the only province where MMR from this cause has reduced. Thus, more in depth analysis of the OH near miss cases in the Metro West district of Cape Town could enable better identification of the factors that ensure survival from OH and this information could assist other provinces tackling their higher OH MMRs.In our study 50 (45%) of the 112 near misses were associated with hypertensive disorders of pregnancy. However, the MI for hypertensive disorders in our study was found to be at 1.9%, this is relatively low compared to the Karachi study were the mortality index was 8.5% for hypertensive disorders The study showed lower MI for hypertensive disorders, and the reason could be related to the strict and streamlined referral protocols in Metro West, effective emergency transport services between levels of care, timely intervention and extensive use of drugs such as magnesium sulphate and rapid acting antihypertensive agents. For example, in our results, out of the 50 patients with hypertensive disorders, 48 were given magnesium sulphate and all patients with Eclampsia received magnesium sulphate promptly within 12 hours. The above is according to standard WHO and international recommendations. It is unfortunate that the data collection tool did not include use of rapid acting hypertensive agents and it is recommended that this should be included in future adaptations of the WHO near miss audit tool.
221
The high mortality indices associated with NPRIs (66 %) and Acute collapse (33%) is consistent with other studies, such as the Karachi study, but our MI for NPRI was twice what they found. In our study medical/surgical disorders in pregnancy had the third highest mortality index. It is possible that the MIs for these conditions were high in our study because care algorithm for managing these three conditions (NPRI, acute collapse, medical and surgical disorders) may not be as streamlined as that for haemorrhage or that patients presented for care late in the disease process. However, the numbers of these three conditions in our study were too small to draw conclusions.
Conclusion.The near miss rates and maternal mortality ratio in Metro West were lower than for some other developing countries, but higher than rates in high income countries. The mortality index was low for direct obstetric conditions such as hypertensive disorders, obstetric haemorrhage and pregnancy related sepsis, reflecting good quality of care and referral mechanisms for these conditions. The mortality indices for non-pregnancy related infections, medical/surgical conditions and acute collapse were much higher and, suggest that medical problems may need more focused attention.The study showed that the WHO near miss audit tool was an effective tool for measuring severe maternal morbidity and quality of care in the Metro West Maternity facilities.Near miss auditing was found to be feasible and ongoing routine audits would be valuable for the Metro West Maternity Services. This would require institutionalization of the Near Miss identification and monitoring systems.
222