Embed Size (px)
Citation preview
Assessment of Treatment System for Substance Use
Disorders
Vladimir Poznyak
Management of Substance AbuseDepartment of Mental Health and Substance Abuse
Delivery Systems for Substance Abuse TreatmentIstanbul, Turkey, 7th September 2005
Assessment of Treatment System
• Boundaries of "Treatment System"
• Resources for treatment and prevention of substance use disorders in the world
• WHO Assessment Instrument for Mental Health Systems
• Assessment Instrument of Treatment System for Substance Use Disorders?
What are the boundaries of "Treatment System" for SUD?
• Shall it include all psychoactive substances?
• Shall it include alcohol and illicit drug policy framework?
• Shall it include health care sectors beyond mental health and substance abuse treatment services?
• Shall it include other sectors beyond health care?
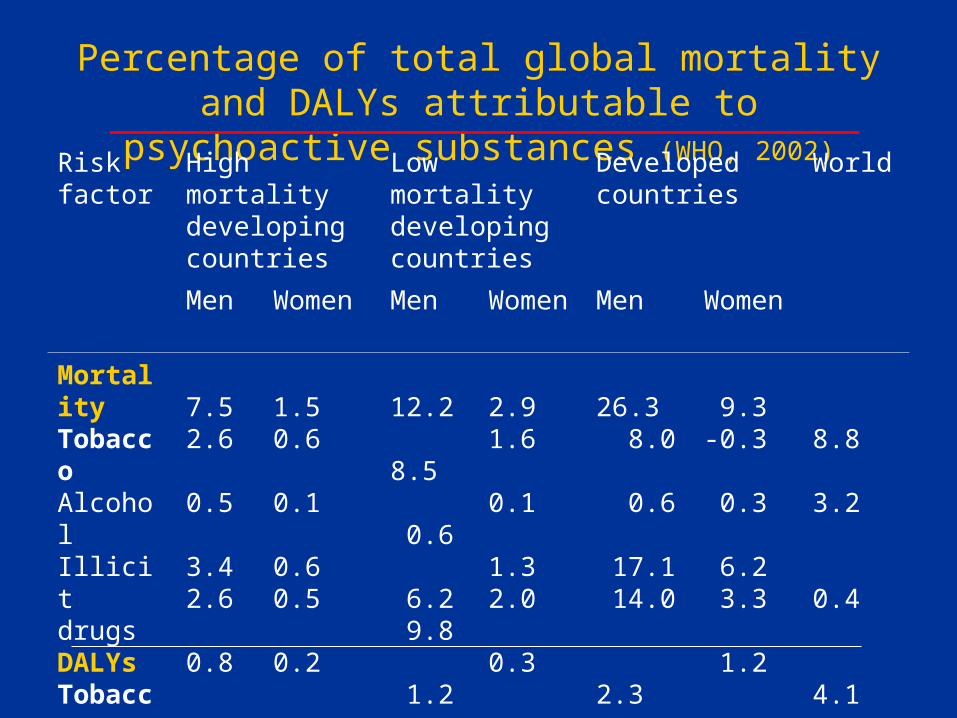
Percentage of total global mortality and DALYs attributable to psychoactive
substances (WHO, 2002)Risk factor
High mortality developing countries
Low mortality developing countries
Developed countries
World
Men Women Men Women Men Women
MortalityTobaccoAlcoholIllicit drugsDALYsTobaccoAlcoholIllicit drugs
7.52.6
0.5
3.42.6
0.8
1.50.6
0.1
0.60.5
0.2
12.2 8.5 0.6 6.2 9.8
1.2
2.91.6
0.1
1.32.0
0.3
26.3 8.0 0.6
17.1 14.0
2.3
9.3-0.3
0.3
6.2 3.3
1.2
8.8 3.2
0.4
4.1 4.0
0.8
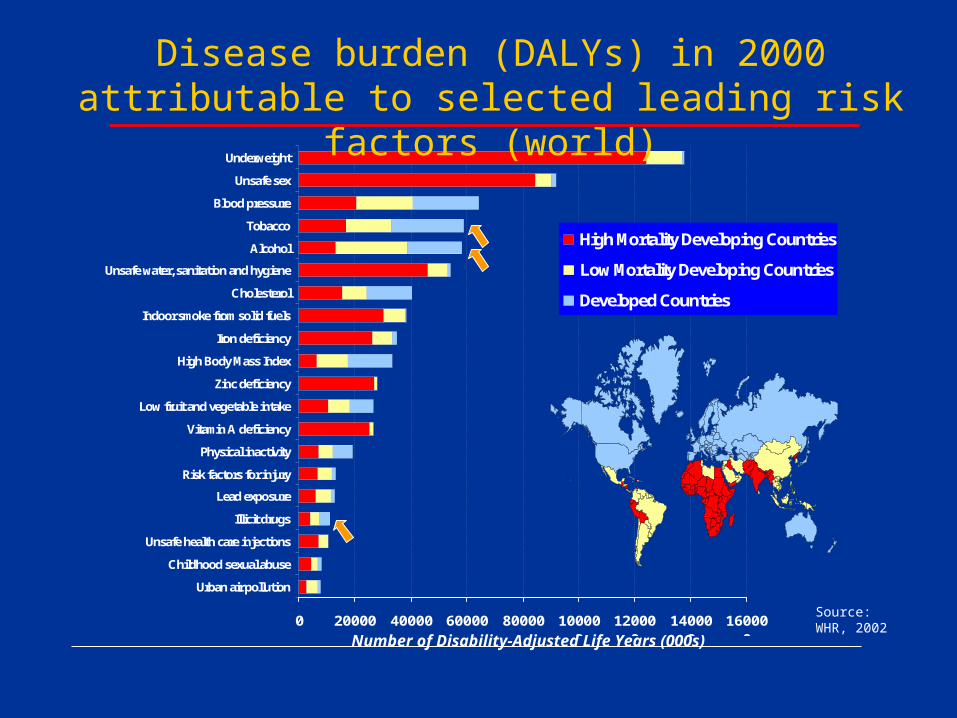
0 20000 40000 60000 80000 100000
120000
140000
160000
Urban air pollution
Childhood sexual abuse
Unsafe health care injections
Illicit drugs
Lead exposure
Risk factors for injury
Physical inactivity
Vitamin A deficiency
Low fruit and vegetable intake
Zinc deficiency
High Body Mass Index
Iron deficiency
Indoor smoke from solid fuels
Cholesterol
Unsafe water, sanitation and hygiene
Alcohol
Tobacco
Blood pressure
Unsafe sex
Underweight
High Mortality Developing Countries
Low Mortality Developing Countries
Developed Countries
Disease burden (DALYs) in 2000 attributable to selected leading risk factors (world)
Number of Disability-Adjusted Life Years (000s)
Source: WHR, 2002
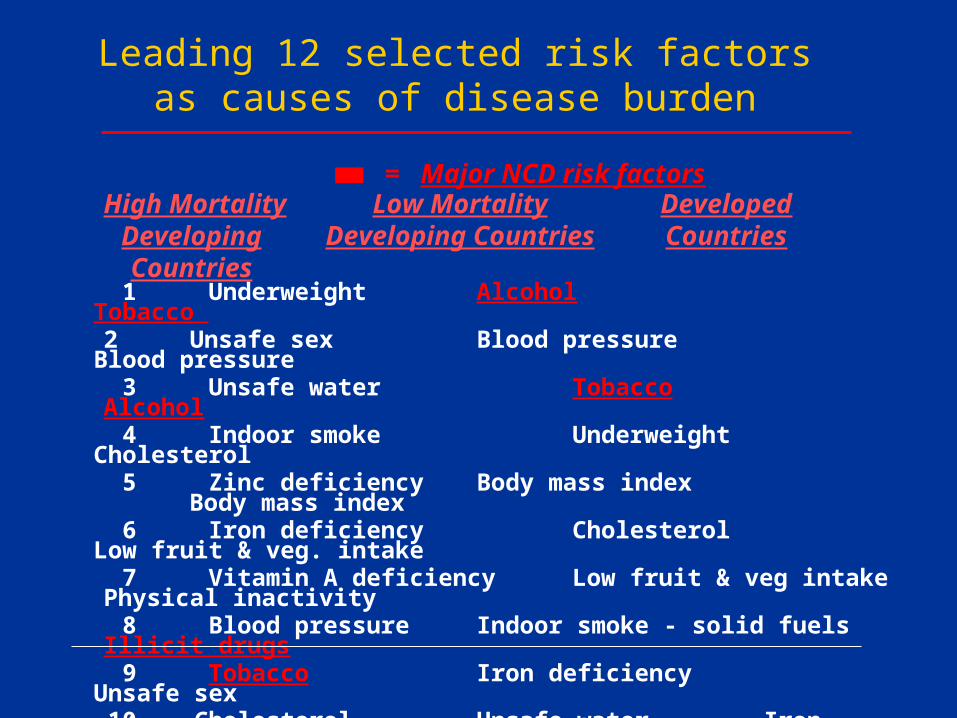
High MortalityDeveloping Countries
Low MortalityDeveloping Countries
= Major NCD risk factors
1 Underweight Alcohol Tobacco 2 Unsafe sex Blood pressure Blood pressure
3 Unsafe water Tobacco Alcohol 4 Indoor smoke Underweight Cholesterol 5 Zinc deficiencyBody mass index Body mass index 6 Iron deficiency Cholesterol Low fruit & veg. intake 7 Vitamin A deficiency Low fruit & veg intake Physical inactivity 8 Blood pressure Indoor smoke - solid fuels Illicit drugs 9 Tobacco Iron deficiency Unsafe sex 10 Cholesterol Unsafe water Iron deficiency 11 Alcohol Unsafe sex Lead exposure 12 Low fruit & veg intake Lead exposure Childhood sexual abuse
DevelopedCountries
Leading 12 selected risk factors as causes of disease burden
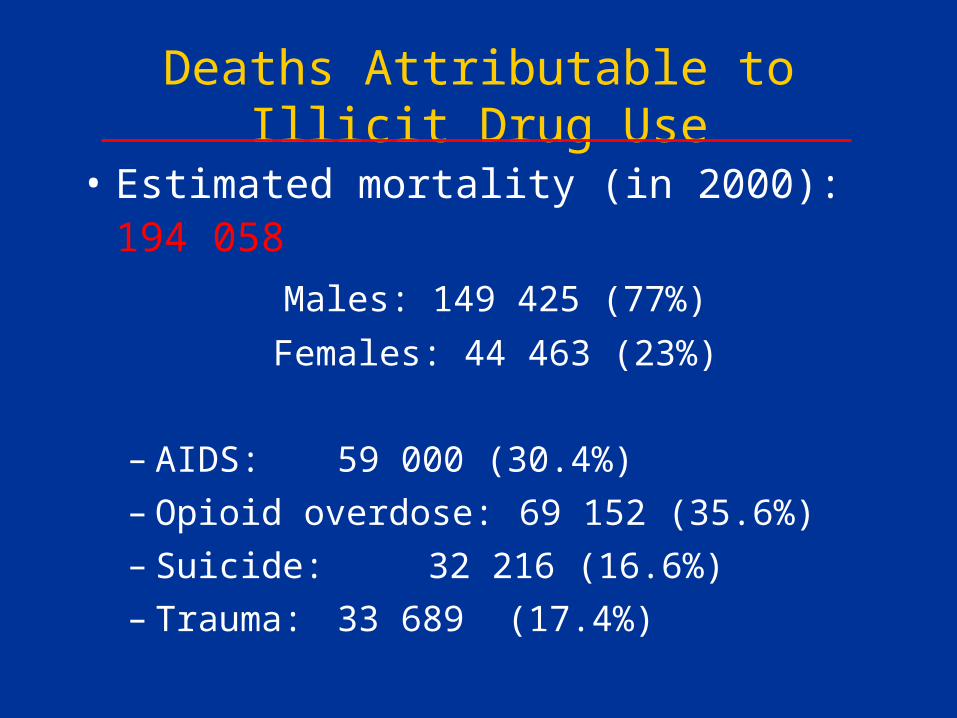
Deaths Attributable to Illicit Drug Use
• Estimated mortality (in 2000): 194 058
Males: 149 425 (77%)
Females: 44 463 (23%)
– AIDS: 59 000 (30.4%)
– Opioid overdose: 69 152 (35.6%)
– Suicide: 32 216 (16.6%)
– Trauma: 33 689 (17.4%)
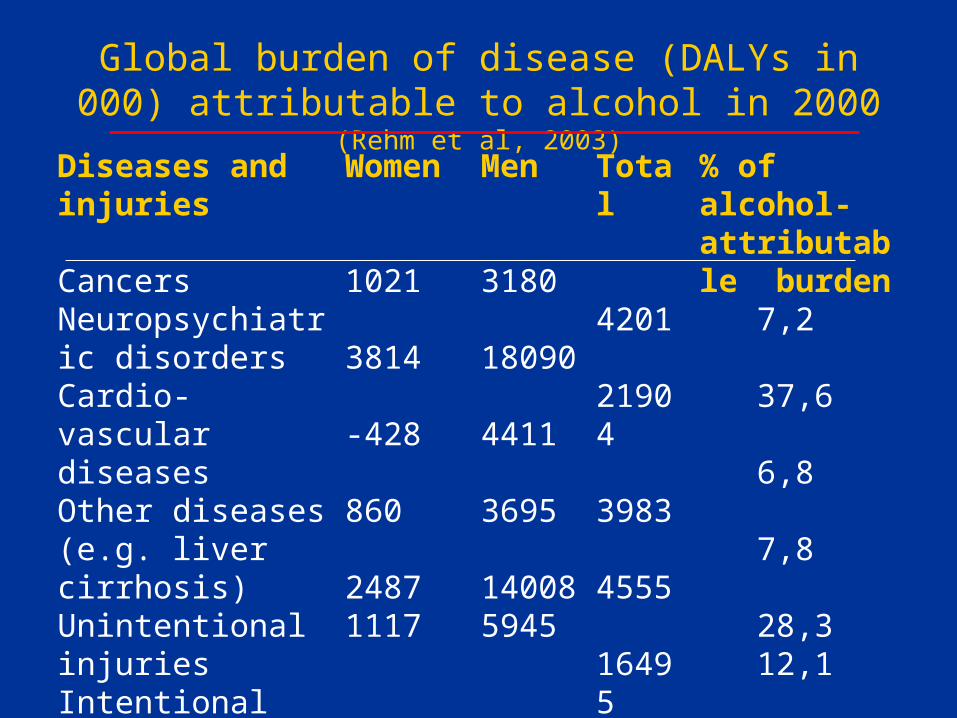
Global burden of disease (DALYs in 000) attributable to alcohol in 2000 (Rehm et al, 2003)
Diseases and injuries
CancersNeuropsychiatric disordersCardio-vascular diseasesOther diseases(e.g. liver cirrhosis)Unintentional injuriesIntentional injuries
Women
1021
3814
-428
860
24871117
Men
3180
18090
4411
3695
140085945
Total
4201
21904
3983
4555
164957062
% of alcohol-attributable burden 7,2
37,6
6,8
7,8
28,3 12,1
Treatment System Addressing Wide Range of Psychoactive Substances
• Tobacco
• Alcohol
• Illicit drugs
• Prescribed psychotropic medicines
• Inhalants
• …
Treatment System Addressing Wide Range of Substance-Related Disorders
• Intoxication
• Harmful use/abuse
• Dependence
• Substance-induced disorders
• Co-occurring conditions
Treatment System as Part of the Prevention Continuum
• Primary prevention – Ensuring that a disorder, process or problem will not occur (control of
dependence-producing substances, structural and environmental changes, risk and protective factor detection and control…)
• Secondary prevention – Early identification and management (terminating or modifying for the
better) of substance use disorders (harmful use/abuse and substance dependence)
• Tertiary prevention– Stopping or retarding the progress of a disorder, process or problem
and its sequelae even though the basic condition persists (chronic care and rehabilitation, strategies for harm reduction and improvement of quality of life)
WHO Expert Committee on Drug Dependence, 28th and 30th Reports (WHO, 1993, 1998).
What are the boundaries of "Treatment System" for SUD?
• Shall it include all psychoactive substances?Yes
• Shall it include alcohol and illicit drug policy framework?
Yes• Shall it include health care sectors beyond mental
health and substance abuse treatment services? Yes
• Shall it include other sectors beyond health care? Yes
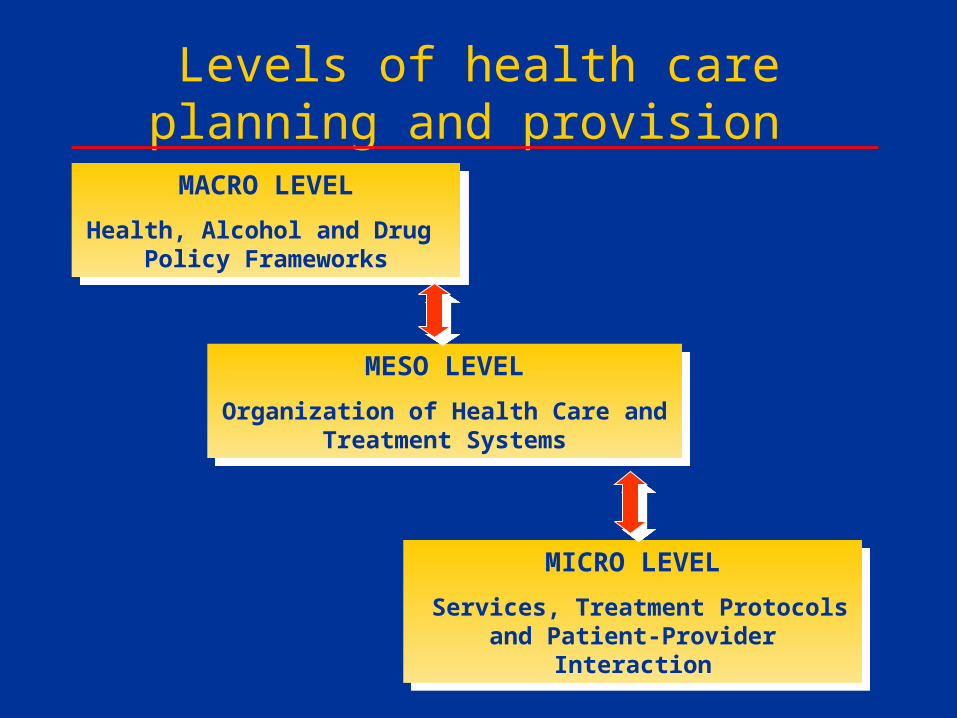
Levels of health care planning and provision
MACRO LEVEL
Health, Alcohol and Drug Policy Frameworks
MACRO LEVEL
Health, Alcohol and Drug Policy Frameworks
MESO LEVEL
Organization of Health Care and Treatment Systems
MESO LEVEL
Organization of Health Care and Treatment Systems
MICRO LEVEL
Services, Treatment Protocols and Patient-Provider Interaction
MICRO LEVEL
Services, Treatment Protocols and Patient-Provider Interaction
WHO Assessment of Resources and Systems in Mental Health and
Substance Abuse• WHO ATLAS Project– Mental Health Resources in the World 2001
– Country Profiles on Mental Health Resources 2001
– Country Resources for Neurological Disorders 2004
– Child and Adolescent Mental Health (in preparation)
– Epilepsy Care in the World 2005
– Intellectual Disabilities (in preparation)
– Psychiatric Training (in preparation)
– Role of Nurses in Mental Health Care (in preparation)
– Substance Abuse (ATLAS-SU)
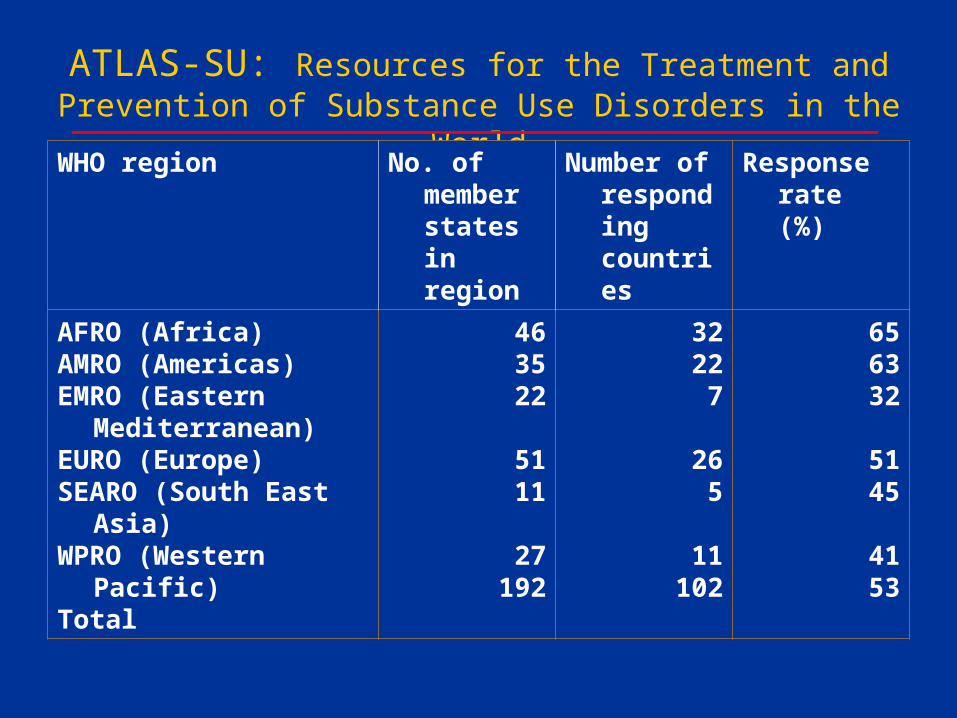
ATLAS-SU: Resources for the Treatment and Prevention of Substance Use Disorders in the World
WHO region No. of member states in region
Number of responding countries
Response rate (%)
AFRO (Africa)AMRO (Americas)EMRO (Eastern
Mediterranean)EURO (Europe)SEARO (South East
Asia)WPRO (Western
Pacific)Total
463522
5111
27192
32227
265
11102
656332
5145
4153
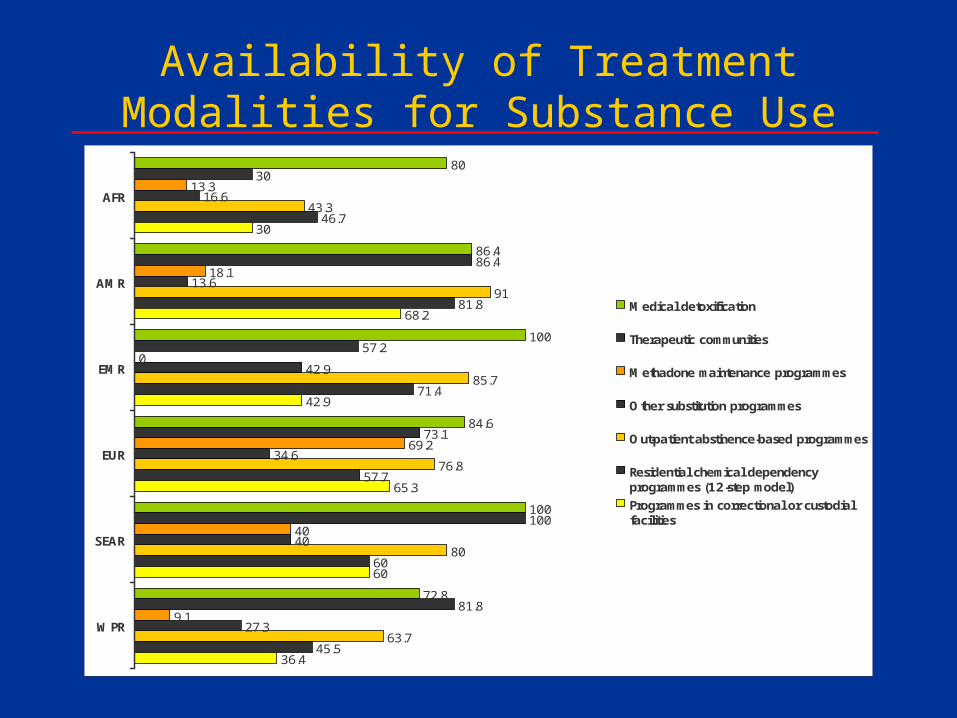
Availability of Treatment Modalities for Substance Use Disorders in WHO
Regions80
86.4
100
84.6
100
72.8
30
86.4
57.2
73.1
100
81.8
13.3
18.1
0
69.2
40
9.1
16.6
13.6
42.9
34.6
40
27.3
43.3
91
85.7
76.8
80
63.7
46.7
81.8
71.4
57.7
60
45.5
30
68.2
42.9
65.3
60
36.4
AFR
AMR
EMR
EUR
SEAR
WPR
Medical detoxification
Therapeutic communities
Methadone maintenance programmes
Other substitution programmes
Out-patient abstinence-based programmes
Residential chemical dependencyprogrammes (12-step model)
Programmes in correctional or custodialfacilities
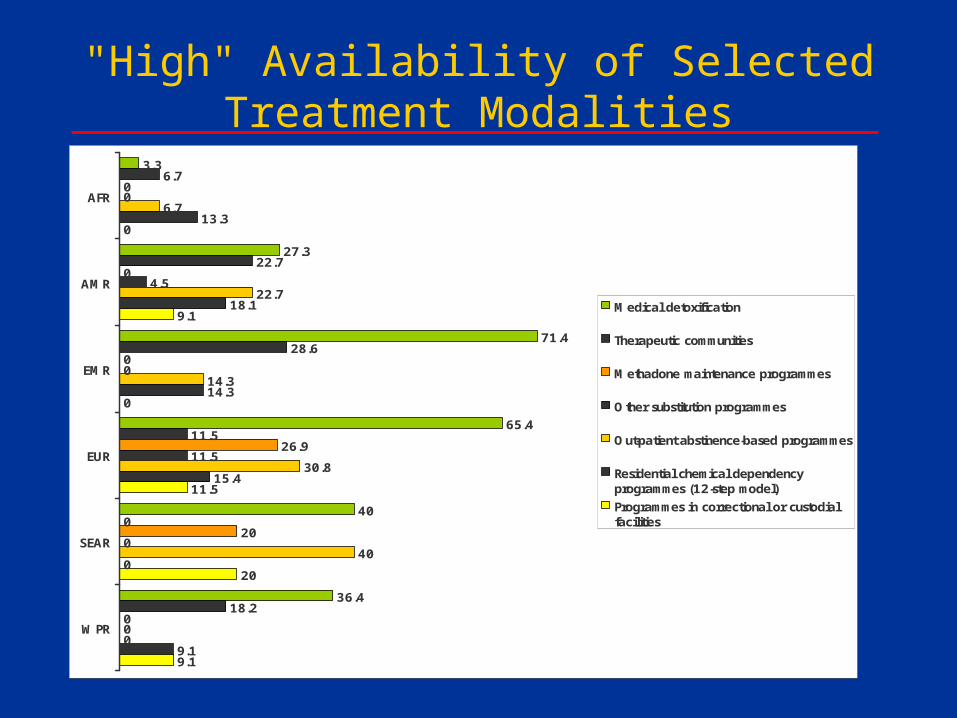
"High" Availability of Selected Treatment Modalities
3.3
27.3
71.4
65.4
40
36.4
6.7
22.7
28.6
11.5
0
18.2
0
0
0
26.9
20
0
0
4.5
0
11.5
0
0
6.7
22.7
14.3
30.8
40
0
13.3
18.1
14.3
15.4
0
9.1
0
9.1
0
11.5
20
9.1
AFR
AMR
EMR
EUR
SEAR
WPR
Medical detoxification
Therapeutic communities
Methadone maintenance programmes
Other substitution programmes
Out-patient abstinence-based programmes
Residential chemical dependencyprogrammes (12-step model)
Programmes in correctional or custodialfacilities
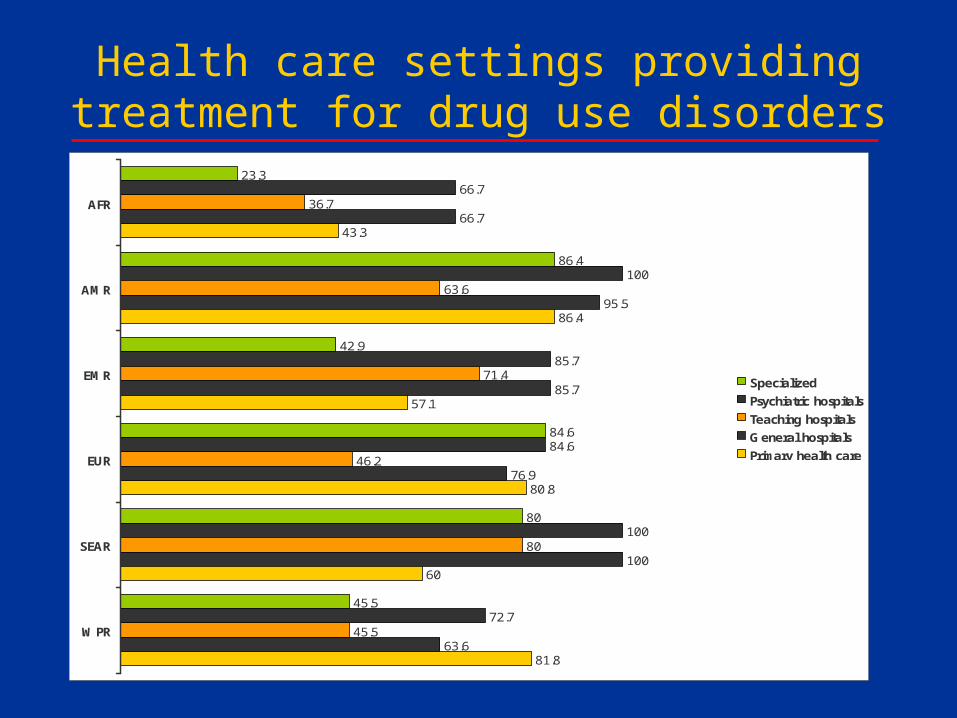
Health care settings providing treatment for drug use disorders
23.3
86.4
42.9
84.6
80
45.5
66.7
100
85.7
84.6
100
72.7
36.7
63.6
71.4
46.2
80
45.5
66.7
95.5
85.7
76.9
100
63.6
43.3
86.4
57.1
80.8
60
81.8
AFR
AMR
EMR
EUR
SEAR
WPR
Specialized
Psychiatric hospitals
Teaching hospitals
General hospitals
Primary health care
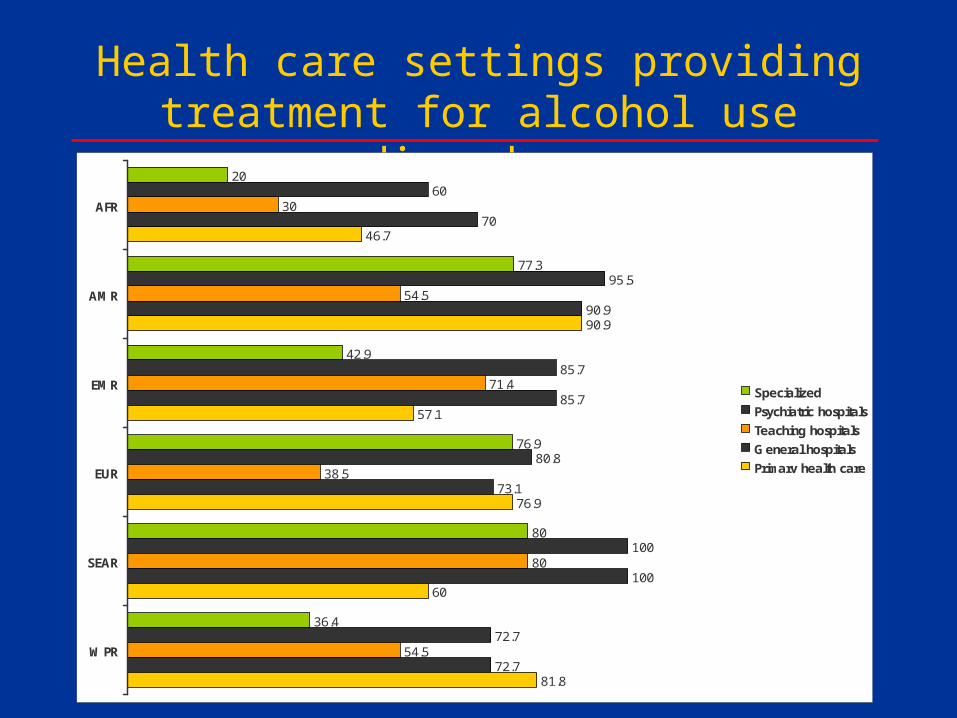
Health care settings providing treatment for alcohol use disorders
20
77.3
42.9
76.9
80
36.4
60
95.5
85.7
80.8
100
72.7
30
54.5
71.4
38.5
80
54.5
70
90.9
85.7
73.1
100
72.7
46.7
90.9
57.1
76.9
60
81.8
AFR
AMR
EMR
EUR
SEAR
WPR
Specialized
Psychiatric hospitals
Teaching hospitals
General hospitals
Primary health care
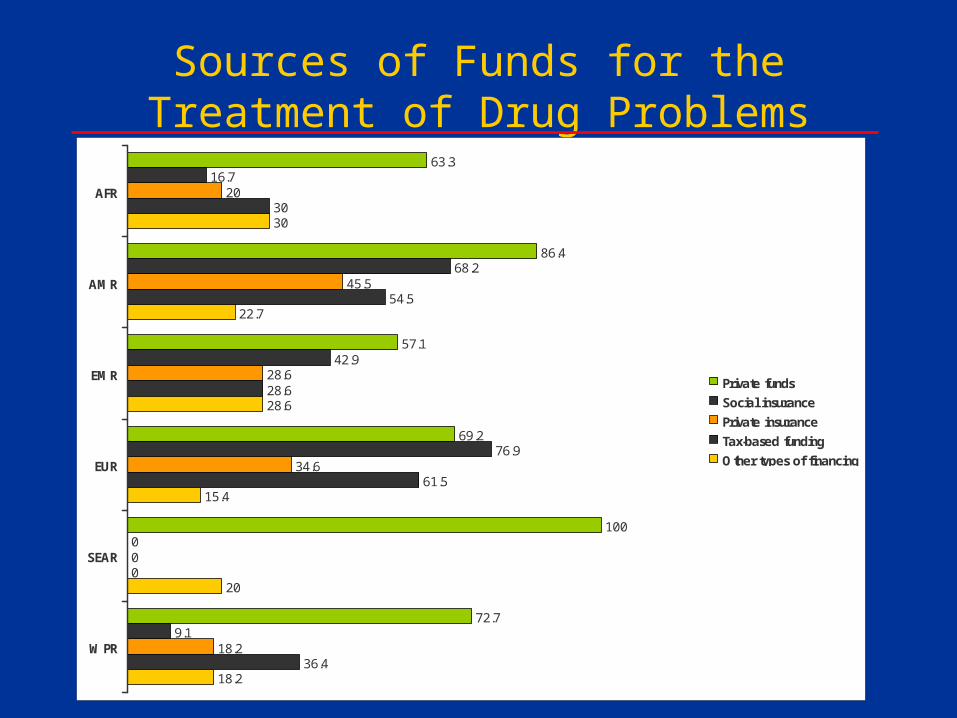
Sources of Funds for the Treatment of Drug Problems
63.3
86.4
57.1
69.2
100
72.7
16.7
68.2
42.9
76.9
0
9.1
20
45.5
28.6
34.6
0
18.2
30
54.5
28.6
61.5
0
36.4
30
22.7
28.6
15.4
20
18.2
AFR
AMR
EMR
EUR
SEAR
WPR
Private funds
Social insurance
Private insurance
Tax-based funding
Other types of financing
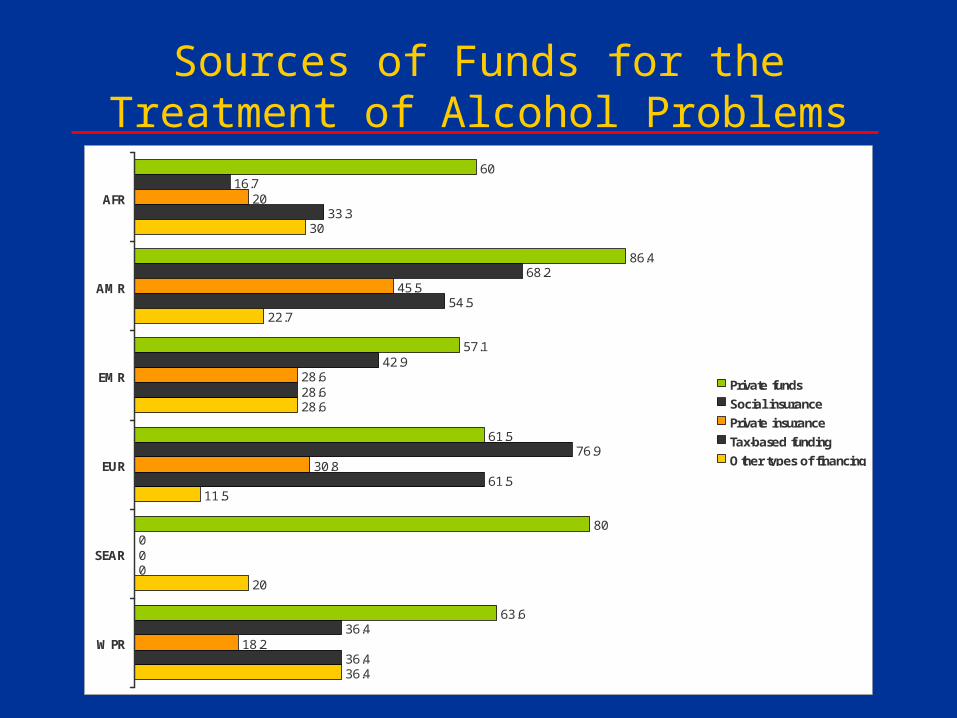
Sources of Funds for the Treatment of Alcohol Problems
60
86.4
57.1
61.5
80
63.6
16.7
68.2
42.9
76.9
0
36.4
20
45.5
28.6
30.8
0
18.2
33.3
54.5
28.6
61.5
0
36.4
30
22.7
28.6
11.5
20
36.4
AFR
AMR
EMR
EUR
SEAR
WPR
Private funds
Social insurance
Private insurance
Tax-based funding
Other types of financing
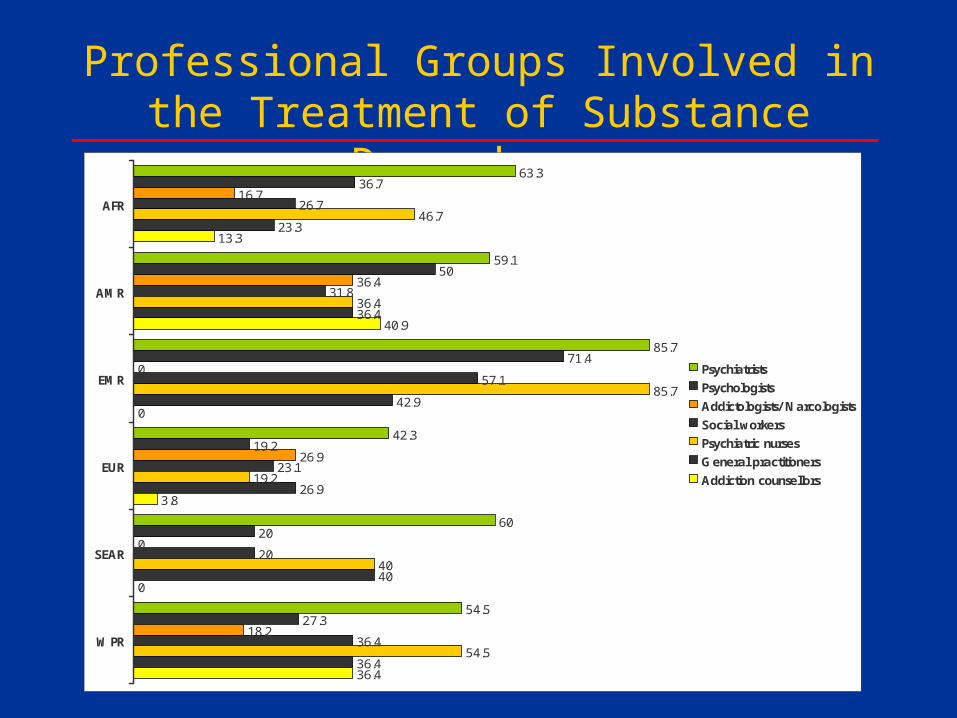
Professional Groups Involved in the Treatment of Substance Dependence
63.3
59.1
85.7
42.3
60
54.5
36.7
50
71.4
19.2
20
27.3
16.7
36.4
0
26.9
0
18.2
26.7
31.8
57.1
23.1
20
36.4
46.7
36.4
85.7
19.2
40
54.5
23.3
36.4
42.9
26.9
40
36.4
13.3
40.9
0
3.8
0
36.4
AFR
AMR
EMR
EUR
SEAR
WPR
Psychiatrists
Psychologists
Addictologists/ Narcologists
Social workers
Psychiatric nurses
General practitioners
Addiction counsellors
WHO-AIMS
World Health Organization Assessment Instrument for Mental Health Systems
Developed by the Evidence and Research Team of the Department of Mental Health
and Substance Abuse
(S. Saxena, A. Lora, M. van Ommeren, T. Barrett,
J. Morris)
in collaboration with experts within and outside WHO
WHO-AIMS Version 2.1
Aim: assessment of mental health systems in less-resourced countries/states/provinces for
• Generating awareness and facilitating improvements• Developing information-based plans with base-line
information and targets• Monitor progress
Structured in:• 6 domains • 28 facets • 156 items
Domains of WHO-AIMS
• Policy and Legislative Framework
• Mental Health Services
• Mental Health in Primary Health Care
• Human Resources
• Public Education and Links with Other Sectors
• Monitoring and Research
Domain "Policy and Legislative Framework": Facets
• Mental health policy
• Mental health plan
• Mental health legislation
• Monitoring and training on human rights
• Financing of mental health services
Domain "Mental Health Services": Facets
• Organizational integration of services• Mental health outpatient facilities• Day treatment facilities• Community-based psychiatric inpatient units• Community residential facilities• Mental hospitals• Forensic inpatient units• Other residential facilities• Availability of psychosocial treatment in mental health
facilities• Availability of essential psychotropic medicines• Equity of access to mental health services
Domain "Mental Health Services": Facet "Organizational Integration of Services":
Items• Existence and functions of a national or
regional "mental health authority"
• Organization of MH services by catchments areas/service areas
• Mental hospitals organizationally integrated with mental health outpatient facilities – Proportion of mental hospitals organizationally
integrated with outpatient facilities (numerator)– Total number
Domain "Public Education and Links with Other Sectors": Facets
• Public education and awareness campaigns on mental health
• Links with other sectors: formal collaboration
• Links with other sectors: activities
Links with other sectors: activities
ITEMS• Provision of employment for people with severe
mental disorders• Primary and secondary schools with mental health
professionals• Promotion and prevention activities in primary and
secondary schools• Educational activities with police officers• Educational activities with judges and lawyers• Mental health care of prisoners• Social welfare benefits
Framework for Analysis of Treatment Systems and Services for SUD
• Needs assessment• Policy framework• Availability of services• Adequacy• Accessibility• Affordability • Equity • Effectiveness (improving health and well-being)• Efficiency (maximising health gains)• Utilization
Common Problems in Organization of Health and Social Services
• Inadequate Services/Systems
• Inaccessible Services
• Unaffordable Services
• Underutilized Services
• Fragmented services
• Discontinuous services
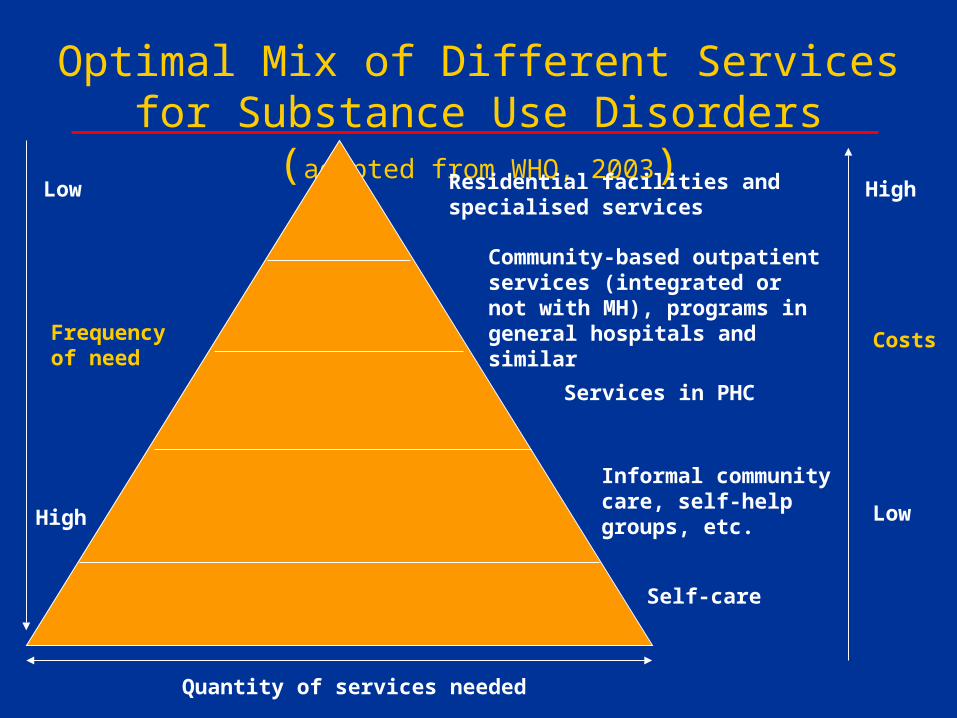
Optimal Mix of Different Services for Substance Use Disorders (adapted from WHO,
2003)Residential facilities and specialised services
Community-based outpatient services (integrated or not with MH), programs in general hospitals and similar
Services in PHC
Informal community care, self-help groups, etc.
Self-care
Quantity of services needed
Low
High
Frequency of need
Costs
High
Low
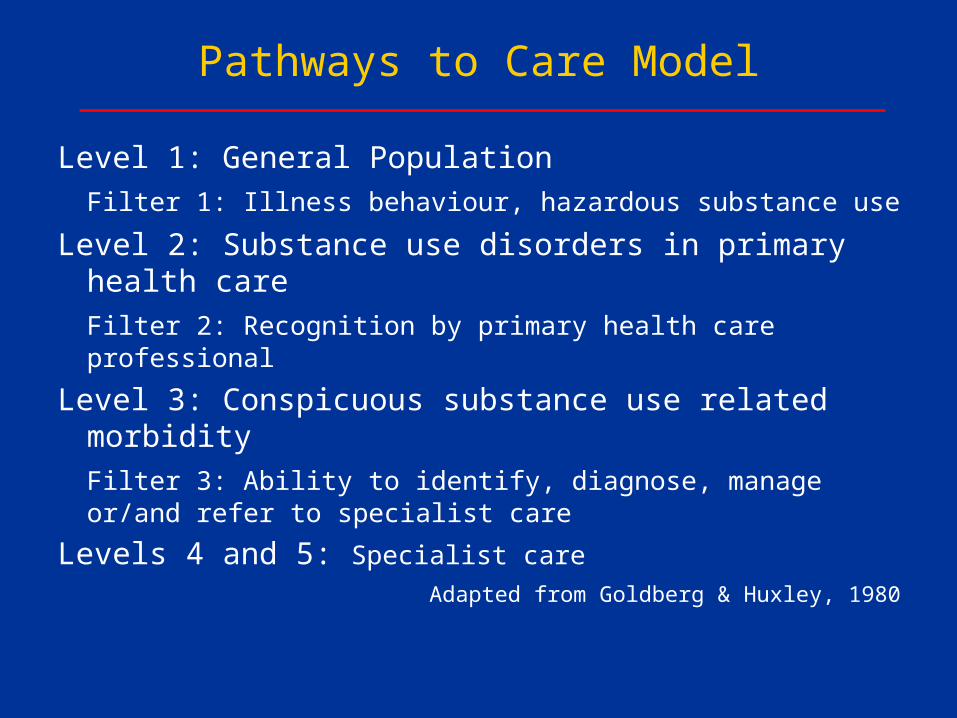
Pathways to Care Model
Level 1: General Population
Filter 1: Illness behaviour, hazardous substance use
Level 2: Substance use disorders in primary health care
Filter 2: Recognition by primary health care professional
Level 3: Conspicuous substance use related morbidity
Filter 3: Ability to identify, diagnose, manage or/and refer to specialist care
Levels 4 and 5: Specialist care
Adapted from Goldberg & Huxley, 1980
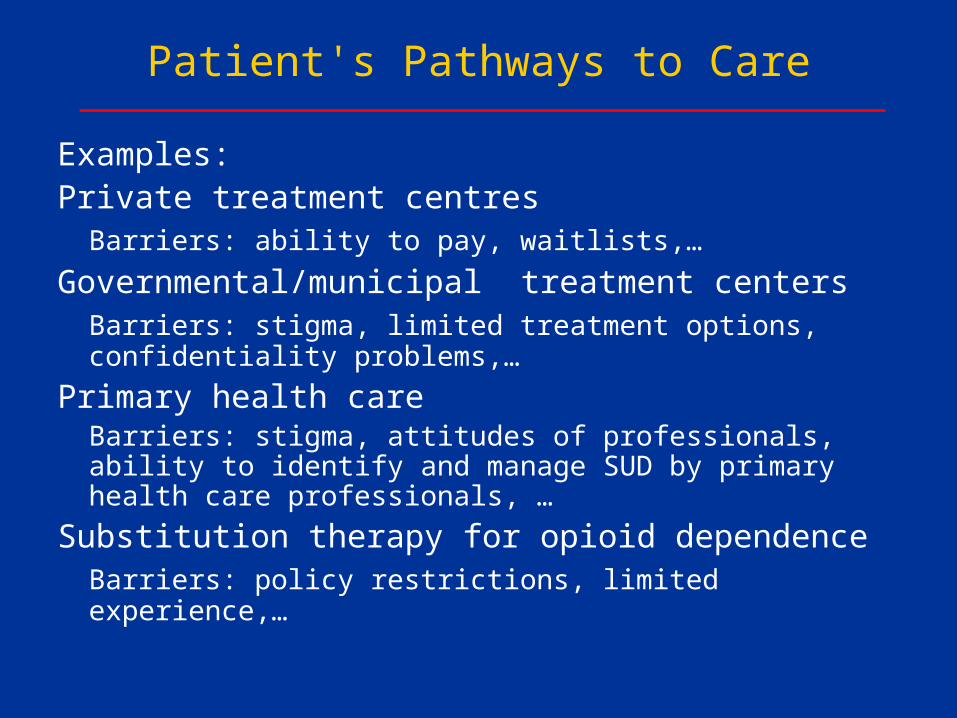
Patient's Pathways to Care
Examples:Private treatment centres
Barriers: ability to pay, waitlists,…
Governmental/municipal treatment centersBarriers: stigma, limited treatment options, confidentiality problems,…
Primary health care Barriers: stigma, attitudes of professionals, ability to identify and manage SUD by primary health care professionals, …
Substitution therapy for opioid dependenceBarriers: policy restrictions, limited experience,…
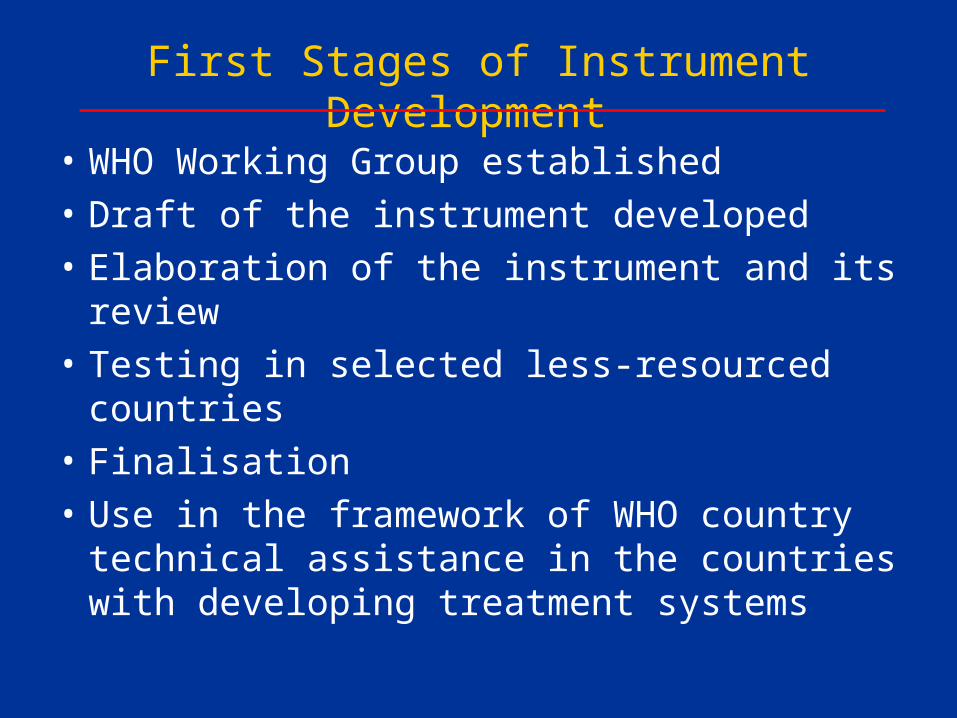
First Stages of Instrument Development
• WHO Working Group established
• Draft of the instrument developed
• Elaboration of the instrument and its review
• Testing in selected less-resourced countries
• Finalisation
• Use in the framework of WHO country technical assistance in the countries with developing treatment systems
Neuroscience of Substance Use and Dependence (WHO, 2004)
" Treatment must be accessible to all in need. Effective interventions exist and can be integrated into health systems, including primary health care. The health care sector needs to provide the most cost-effective interventions. "
Contact details:
www.who.int/substance_abuse/Management of Substance Abuse
WHO Department of Mental Health and Substance Abuse