Embed Size (px)
Citation preview
Assigning Milestone Evaluations in Internal
MedicineMelvin Blanchard, MD, FACP
Program Director, Internal MedicineChief, Division of Medical Education
Department of Medicine
Internal Medicine program overview ACGME Charges re Competencies Response by IM community ACGME counter response Our program’s approach to evaluation
Outline
Discipline encompassing the study and practice of health promotion, disease prevention, diagnosis, care and treatment of adults 1 of 4 physicians in the US IM residents
Our program: 151 trainees
2/3 inpatient; 1/3 outpatient BJH, VA, community, international ~50 rotations
Internal Medicine Overview
Category Positions
Number of training programs 393
Positions in match 6177
First year fellows 4584
1999 – ACGME launched the Outcomes Project Required PDs to assess trainees in 6 competencies
Patient Care Professionalism Practice-Based Learning and Improvement Interpersonal and Communication skills Medical Knowledge Systems-Based Practice
Competencies required of a physician to deliver competent medical care
ACGME Charge - 1
2009 – ACGME charged specialties with identifying milestones of competency development Observable developmental steps
How do we know that PGY-2 resident will be competent at graduation?
How do we know that graduates from the 393 IM programs can deliver same quality of IM care?
ACGME Charge - 2
2009-12: Published 142 Milestones
Aka Curricular Milestones Point in development that facilitates assessment of
progression from beginner to expected proficiency at end of training
Published 16 Entrustable Professional Activities (EPAs) KSAs critical to practice specialty
Milestones and EPAs categorized by 6 competencies
IM Community Response
Manage patients with diseases across multiple care settings. Provide age-appropriate screening and preventative care. Resuscitate, stabilize, and care for unstable or critically ill patients. Provide perioperative assessment and care. Manage transitions of care. Facilitate family meetings. Enhance patient safety. Improve the quality of health care at individual and systems
levels. Demonstrate personal habits of lifelong learning. Demonstrate professional behavior.
EPAs
142 milestones is too numerous Not optimal format for reporting to the ACGME
ACGME and ABIM combined forces Developed milestones for reporting educational
outcomes Aka Reporting Milestones or Milestones
Grouped into 22 sub-competences Grouped into 6 competencies
With each competency associated with 2 – 5 sub-competencies
ACGME Counter Response
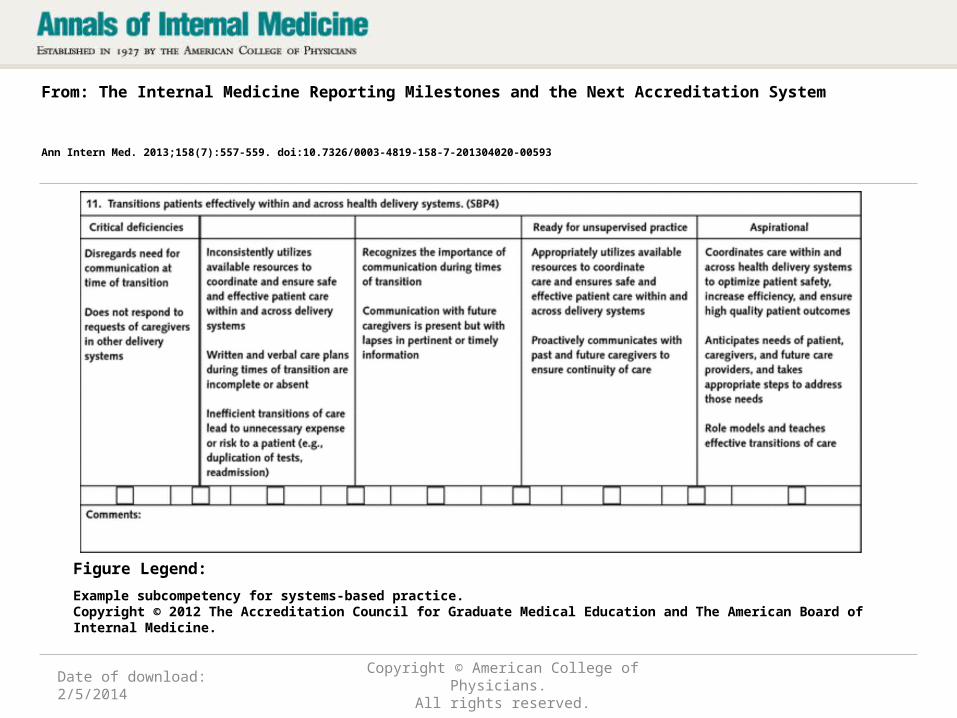
Date of download: 2/5/2014
Copyright © American College of Physicians. All rights reserved.
From: The Internal Medicine Reporting Milestones and the Next Accreditation System
Ann Intern Med. 2013;158(7):557-559. doi:10.7326/0003-4819-158-7-201304020-00593
Example subcompetency for systems-based practice.Copyright © 2012 The Accreditation Council for Graduate Medical Education and The American Board of Internal Medicine.
Figure Legend:
• Competencies• Curricular milestones• Reporting milestones• Milestones• Entrustable Professional Activities• Narratives • Sub-competencies
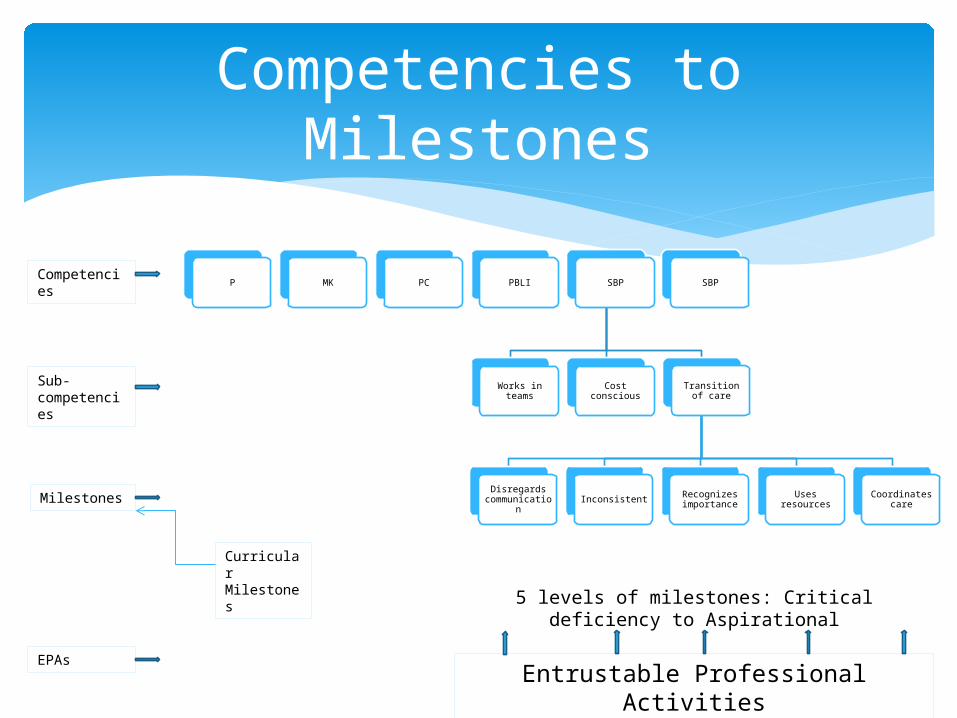
P MK PC PBLI SBP
Works in teams Cost conscious Transition of
care
Disregards communicatio
nInconsistent Recognizes
importance Uses resources Coordinates care
SBP
5 levels of milestones: Critical deficiency to Aspirational
Entrustable Professional Activities
Competencies
Competencies to Milestones
Sub-competencies
Milestones
EPAs
Curricular Milestones
What did we do?• Broke 22 sub-competencies into sub-sub competencies
– Each sub-sub competency can be used as a question on a rotation evaluation
• Rotations divided among 5 faculty– Each faculty work with core faculty/rotation directors to select
evaluation questions appropriate to rotation
• Tracked assignment to assure each sub-competency measured multiple times
• Data from conference attendance, ITE, journal club participation, etc. also feed into evaluation system
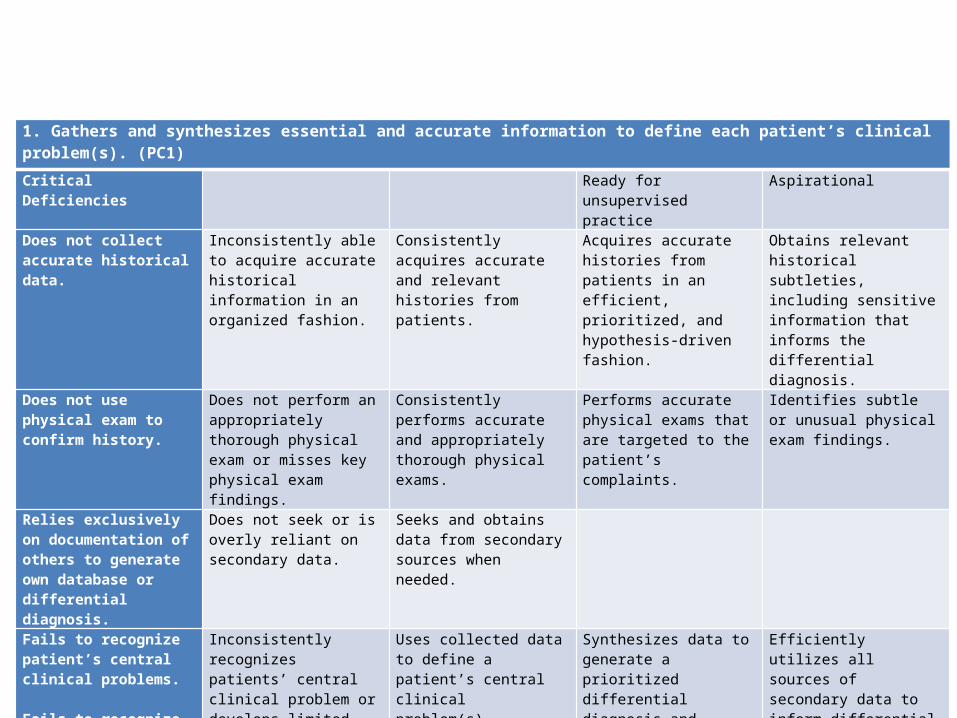
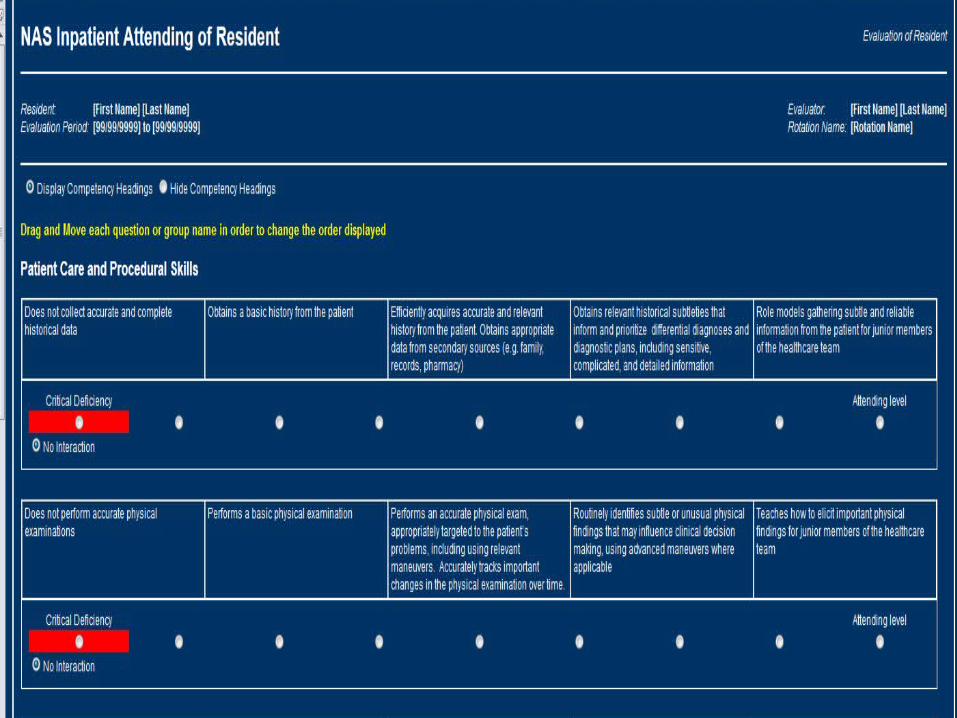
1. Gathers and synthesizes essential and accurate information to define each patient’s clinical problem(s). (PC1)
Critical Deficiencies Ready for unsupervised practice
Aspirational
Does not collect accurate historical data.
Inconsistently able to acquire accurate historical information in an organized fashion.
Consistently acquires accurate and relevant histories from patients.
Acquires accurate histories from patients in an efficient, prioritized, and hypothesis-driven fashion.
Obtains relevant historical subtleties, including sensitive information that informs the differential diagnosis.
Does not use physical exam to confirm history.
Does not perform an appropriately thorough physical exam or misses key physical exam findings.
Consistently performs accurate and appropriately thorough physical exams.
Performs accurate physical exams that are targeted to the patient’s complaints.
Identifies subtle or unusual physical exam findings.
Relies exclusively on documentation of others to generate own database or differential diagnosis.
Does not seek or is overly reliant on secondary data.
Seeks and obtains data from secondary sources when needed.
Fails to recognize patient’s central clinical problems. Fails to recognize potentially life threatening problems.
Inconsistently recognizes patients’ central clinical problem or develops limited differential diagnoses.
Uses collected data to define a patient’s central clinical problem(s).
Synthesizes data to generate a prioritized differential diagnosis and problem list.
Efficiently utilizes all sources of secondary data to inform differential diagnosis.
Effectively uses history and physical examination skills to minimize the need for further diagnostic testing.
Role models and teaches the effective use of history and physical examination skills to minimize the need for further diagnostic testing.
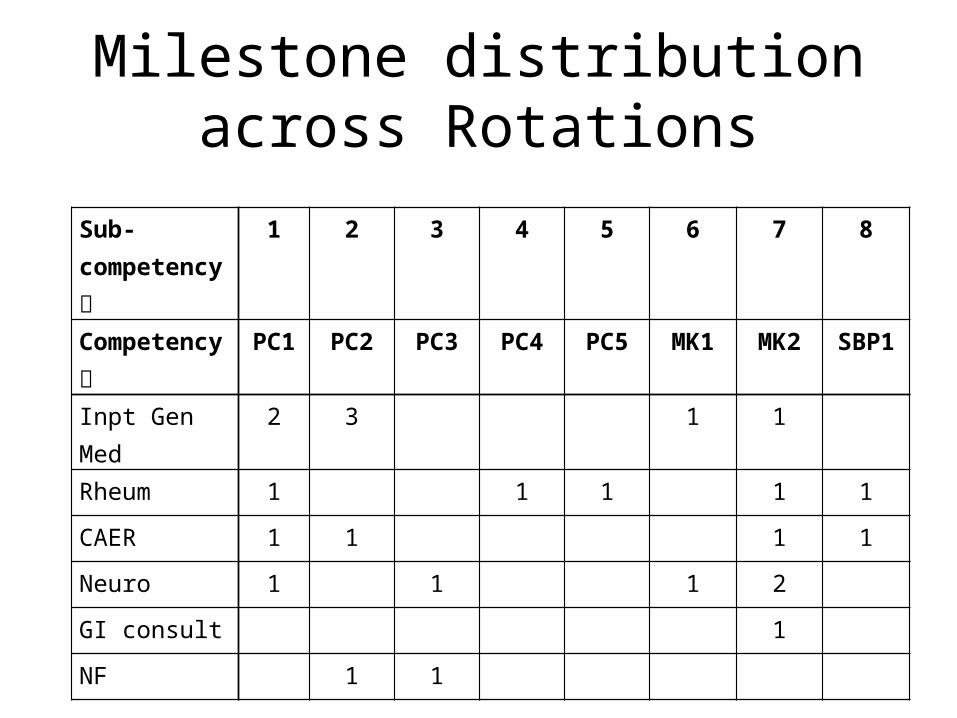
Milestone distribution across Rotations
Sub-competency
1 2 3 4 5 6 7 8
Competency PC1 PC2 PC3 PC4 PC5 MK1 MK2 SBP1
Inpt Gen Med 2 3 1 1
Rheum 1 1 1 1 1
CAER 1 1 1 1
Neuro 1 1 1 2
GI consult 1
NF 1 1