Embed Size (px)
Citation preview
Central Committee of Special Education Dr. Mary Pauly Assistant Superintendent of Special Education
Kim Hoelscher Donna Jackson Kim Janaski Director of Special Education Director of Special Education Director of Special Education Kyle Morrison
Supervisor of Special Education
Central Committee of Special Education Dr. Mary Pauly Assistant Superintendent of Special Education
Nina Blumlein
Kim Hoelscher Donna Jackson Kim Janaski
Director of Revenue and Related Service
Director of Special Education
Director of Special Education
Director of Special Education
Kyle Morrison
Supervisor of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-4746 – Fax (716) 878-9706
REV. 4/23/15
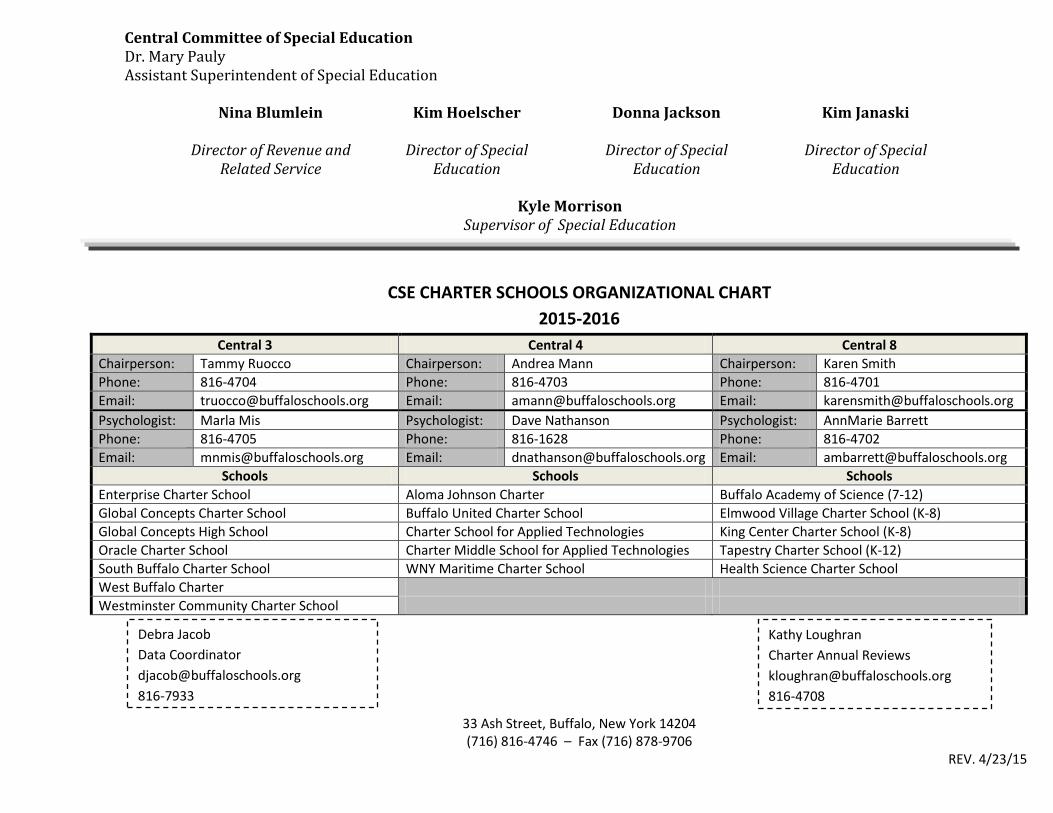
CSE CHARTER SCHOOLS ORGANIZATIONAL CHART
2015-2016
Central 3 Central 4 Central 8
Chairperson: Tammy Ruocco Chairperson: Andrea Mann Chairperson: Karen Smith
Phone: 816-4704 Phone: 816-4703 Phone: 816-4701
Email: [email protected] Email: [email protected] Email: [email protected]
Psychologist: Marla Mis Psychologist: Dave Nathanson Psychologist: AnnMarie Barrett
Phone: 816-4705 Phone: 816-1628 Phone: 816-4702
Email: [email protected] Email: [email protected] Email: [email protected]
Schools Schools Schools
Enterprise Charter School Aloma Johnson Charter Buffalo Academy of Science (7-12)
Global Concepts Charter School Buffalo United Charter School Elmwood Village Charter School (K-8)
Global Concepts High School Charter School for Applied Technologies King Center Charter School (K-8)
Oracle Charter School Charter Middle School for Applied Technologies Tapestry Charter School (K-12)
South Buffalo Charter School WNY Maritime Charter School Health Science Charter School
West Buffalo Charter
Westminster Community Charter School
Debra Jacob
Data Coordinator
816-7933
Kathy Loughran
Charter Annual Reviews
816-4708
Buffalo Public Schools Dr. Pamela C. Brown, Ed.D. Central Committee of Special EducationSuperintendent Dr. Mary Pauly
Assistant Superintendent of Curriculum, Assessment & Leadership Kim Curtin
Director of Special Education
(716) 816‐4746 – Fax (716) 878‐9706 Revised 4/22/15
Students new to Buffalo District enrolling in Charter Schools
The Central Committee on Special Education Placement Office must be made aware of
all students with disabilities entering Charter Schools for the very first time from out of
district or out of state.
Parent Completes ALL Forms:
Transfer Student Information Sheet
Student Racial & Ethnic Identification Form
Request for Student Records
Home Language Questionnaire
Parent Consent Form
Parental Consent for Medicaid Funding
Copy of most current IEP
Forward completed packet to:
Central Committee on Special Education
Designated CSE Chair
33 Ash Street, Room 201
Buffalo, NY 14204

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-4746 • Fax (716) 816-3974 Revised 4/16/13
TRANSFER STUDENT INFORMATION SHEET
Date: Start Date: Student Name: Student’s DOB: Grade: Address: City: Zip Code: Phone #: Emergency #:
Student lives with:
Name: Relationship to student: If student is NOT living with parent, is the parent(s) still the legal guardian? YES NO IF YES:
Parent(s) name(s): Address: Phone #: Emergency #:
Last School attended: District: Phone# Fax: Address: City: Zip Code: School official to contact:
Has the student ever attended the Buffalo Public Schools? YES NO
Was the student a special education student in the Buffalo Public Schools? YES NO

BUFFALO PUBLIC SCHOOLS STUDENT RACIAL AND ETHNIC IDENTIFICATION ESCUELAS PÚBLICAS DE BUFFALO IDENTIFICACIÓN ÉTNICA Y RACIAL DEL ESTUDIANTE
To the Parent/Guardian: The BUFFALO PUBLIC SCHOOL DISTRICT has adopted a policy which requires the collection and recording of the ethnic identity of students in the BUFFALO PUBLIC SCHOOL DISTRICT in accordance with the federal categories and definitions. The information will be used to: - Plan educational programs and make sure that they are readily available to all students. - Analyze differences in academic performance, attendance and completion of school. - Report information to the State and Federal Education Departments. We need your help in order to accomplish this task. Please review the Racial/Ethnic definitions on the back of this page. Put a check (√) in the box for the category or categories which best describe your child. The BUFFALO PUBLIC SCHOOL DISTRICT wishes to assure you that this information will be kept secure and confidential in accordance with all State and Federal student privacy laws and regulations. If the information requested is not provided on this form on behalf of your child, a student records officer from the school or district will be required to identify the group to which the student appears to belong, identifies with, or is regarded in the community as belonging. Thank you for your cooperation. Padre/Encargado: El DISTRITO DE LAS ESCUELAS PÚBLICAS DE BUFFALO requiere de acuerdo con la categoría y definición federal la colección y anotación de la identidad étnica de los estudiantes en el DISTRITO DE LAS ESCUELAS PÚBLICAS DE BUFFALO. La información se usará para: - Diseñar programas educativos y asegurarse que estos estén fácilmente disponibles a todos los estudiantes. - Analizar las diferencias entre el desarrollo académico, asistencia y cumplimiento académico. - Comunicar esta información a los Departamentos de Educación Federal y de Estado. Necesitamos su ayuda para poder llevar a cabo esta tarea. Por favor revise la definición Racial/Étnica en la parte de atrás de esta página. Marque (√) en el encasillado la(s) categoría(s) que mejor describe a su hijo(a). El DISTRITO DE LAS ESCUELAS PÚBLICAS DE BUFFALO desea asegurarle que esta información se mantendrá segura y confidencial de acuerdo con todas las leyes y regulaciones Federales y del Estado para la privacidad de los estudiantes. Si la información que le solicitamos no es completada en esta forma en nombre de su hijo(a), el oficial encargado de la escuela o distrito identificará el grupo en el cual el estudiante parece pertenecer, se identifica, o es considerado que pertenece en la comunidad. Gracias por su cooperación.
CONFIDENTIALITY PROCEDURES AND REGULATIONS PROCEDIMIENTOS Y REGLAS SOBRE LA CONFIDENCIALIDAD
To School Staff: This form will be filed in the student's permanent record as confidential information.
To the Parent/Guardian: The information which you have provided on this form is confidential. It is protected by the Confidentiality Regulations cited below. Al Personal de la Escuela: Esta forma será archivada en el expediente permanente del estudiante como información confidencial.
Al Padre/Encargado: La información que usted ha dado en esta forma es confidencial. Esta protegida por las Reglas de Confidencialidad listada en la parte de abajo.
The Family Educational Rights and Privacy Act (1974) prohibits unauthorized access to student records and unauthorized release of any student record information identifiable by either student name or student identification number.
El Acto de Privacidad y de los Derechos Educacionales de las Familias (1974) prohíbe el acceso sin autorización al expediente del estudiante y la liberación de cualquier información sin autorización que puede identificar al estudiante por medio del nombre o su número de identificación.
Please complete the form on the reverse side of this page Por favor complete la parte de atrás de este formulario
Name of School: Nombre de la Escuela:
Grade Level: Grado:
All students between 5 and 21 years of age have the right to a free public education. Children may not be refused admission because of race, color, creed or national origin, sex, citizenship, handicapping condition, or immigration status.
Todos los estudiantes entre los 5 y 21 años de edad tienen el derecho a una educación pública gratuita. Los estudiantes no pueden dejar de ser matriculados por causa de la raza, color, credo u origen nacional, sexo, ciudadanía, incapacidad, o estatus de inmigrante.
Date of Birth (Month/Day/Year): Fecha de Nacimiento (Mes/Día/Año): / /
Student Name: Last, First, Middle: Nombre del Estudiante: Apellido, Primer y Segundo Nombre:
DIRECTIONS TO PARENT/GUARDIAN/INSTRUCCIONES A LOS PADRES/ENCARGADOS
BLACK: A person having origins in any of the black racial groups of Africa NEGRO: Una persona que tiene cualquier origen con los grupos raciales negros de África
WHITE: A person having origins in any of the original peoples of Europe, North Africa, or the Middle East BLANCO: Una persona que tiene cualquier origen con personas originales de Europa, África del Norte, o el Oriente Medio
NATIVE HAWAIIAN OR OTHER PACIFIC ISLANDER: A person having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands. NATIVO DE HAWAII O OTRAS ISLAS PACIFÍCAS: Una persona que tiene cualquier origen con personas originales de Hawai, Guam, Samoa, o otras Islas Pacíficas
ASIAN: A person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent including for example, Cambodia, China, India, Japan, Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam. ASIÁTICO: Una persona que tiene cualquier origen con personas originales del Sudeste de Asia, o el subcontinente de India, incluyendo por ejemplo, Cambodia, China, India, Japón, Korea, Malasia, Pakistán, las Islas Filipinas, Thailand y Vietnam.
________________________________________________________________ Signature of Parent/Guardián/Other/Firma del Padre/Encargado/Otro
______________________ Date/Fecha
AMERICAN INDIAN OR ALASKA NATIVE: A person having origins in any of the original peoples of North America and who maintains cultural identification through tribal affiliation or community recognition. e.g. Cherokee, Mohawk, Inuit. INDIO AMERICANO O NATIVO DE ALASKA: Una persona que tiene cualquier origen con personas originales de Norte America y quien mantiene identificación cultural por medio de una afiliación indígena o reconocimiento de la comunidad. ej. Cherokee, Mohawk, Inuit.
School District Student Identification Number: Número de Identificación del Estudiante del Distrito
PLEASE ANSWER QUESTIONS (1) and (2). PLEASE READ THEM BEFORE YOU RESPOND. [For question (1) Check (√) the box that best describes your child.] Check (√) only ONE box.
POR FAVOR CONTESTE LAS PREGUNTAS (1) y (2). POR FAVOR LEA ANTES DE CONTESTAR. [Para preguntas (1) Marque (√) el encasillado que mejor describe a su hijo(a)] Marque (√) sólo UN encasillado.
Other (Specify)/Otro (Especifíque): _________________________
Mother/Madre Father/Padre
Guardian/Encargado
BUFFALO PUBLIC SCHOOLS STUDENT RACIAL AND ETHNIC IDENTIFICATION ESCUELAS PÚBLICAS DE BUFFALO IDENTIFICACIÓN ÉTNICA Y RACIAL DEL ESTUDIANTE
1. Is the student Hispanic, Latino, or of Spanish origin? Hispanic, Latino, or of Spanish origin means a person of Cuban, Mexican, Puerto Rican, Central or South American, or other Spanish culture or origin, regardless of race. ¿Es el estudiante Hispano, Latino, o de Origen Español? Hispano, Latino, o origen Español significa una persona que es Cubana, Mexicana, Puertorriqueña, de Centro y Sur América, o de otra cultura o origen Español, sin importar la raza.
YES, Hispanic/SÍ, Hispano
NO, not Hispanic/NO, no Hispano
2. Select one or more races from the following five racial groups [For question (2) Check (√) all groups that apply to your child; check (√) at least ONE box.]:
Seleccione una o más razas de los siguientes cinco grupos raciales [Para preguntas (2) Marque (√) todo grupo que le aplica a su hijo(a), marque (√) por lo menos UN encasillado.]:
Relationship to Student (please check one box below)/Relación con el Estudiante (por favor marque sólo un encasillado):

Buffalo Public Schools Dr. Pamela C. Brown, Ed.D. Central Committee of Special EducationSuperintendent Dr. Mary Pauly
Assistant Superintendent of Curriculum, Assessment & Leadership Kim Curtin
Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816‐4746 – Fax (716) 878‐9706
Revised 4/22/15
REQUEST FOR STUDENT RECORDS
The student, indicated below, has transferred to the Buffalo City Schools District. The Federal
Education Rights and Privacy Act, states, School districts may release student record to another
school or school system without parent consent. 34CFR§99.31(A)(1). Thank you.
Please provide the following information to assist us with appropriate school assignment for
this student and mail or fax to:
33 Ash Street, Buffalo, NY 14201 Rm. 201 or fax: 878‐9706
ATTN: _____________________________________________
Cumulative Record / Transcripts
IEP
Psychological
Social History
Related Services
Education Evaluations
Discharge Recommendations
ESL/Bilingual Services
School Suspensions / Expulsion / Disciplinary Records
504 / ADA
Birth Certificate / Immunization and Health Records
Parent / Guardian, please complete this section:
Students Name: Grade: DOB:
Parent Signature:

The University of the State of New York • The State Education Department • Office of Bilingual EducationAlbany, New York 12234
Home Language Questionnaire (HLQ)TO BE COMPLETED BY SCHOOL PERSONNEL
DISTRICT Please print or type clearly
SCHOOL GRADE
STUDENT NAME
DATE OF BIRTH
STUDENT IDENTIFICATION NUMBER
COUNTRY OF BIRTH / ANCESTRY
NUMBER OF YEARS ENROLLED IN SCHOOL OUTSIDE THE U.S.
NAME/POSITION OF SCHOOL PERSONNEL COMPLETING THIS SECTION
DETERMINATION: ❏ Possible LEP
❏ English Proficient
Dear Parent or Guardian:
In order to provide your child with the
best possible education, we need to
determine how well he or she under-
stands, speaks, reads and writes
English. Your assistance in answering
these questions is greatly appreciated.
Thank You
(✔ boxes that apply)
1. What language(s) is spoken in the student’s ❏ English ❏ Other __________________________________home or residence? specify
2. What language(s) are spoken most of the time ❏ English ❏ Other __________________________________to the student, in the home or residence? specify
3. What language(s) does the student understand? ❏ English ❏ Other __________________________________specify
4. What language(s) does the student speak? ❏ English ❏ Other __________________________________specify
5. What language(s) does the student read? ❏ English ❏ Other _______________ ❏ Does Not Readspecify
6. What language(s) does the student write? ❏ English ❏ Other _______________ ❏ Does Not Writespecify
7. In your opinion, how well does the student understand, speak, read and write English?
_________________________________________________ ____________________________________________________Signature of Parent/Guardian/Other Date HLQ (2/00) 99-337 PM
Month: Day: Year:
Month: Day: Year:
Very well Only a little Not at all
Understands English ❏ ❏ ❏
Speaks English ❏ ❏ ❏
Reads English ❏ ❏ ❏
Writes English ❏ ❏ ❏
(✔ Marque las casillas que aplican)
1. ¿Qué idioma(s) se habla en el hogar ❏ Inglés ❏ Español ❏ Otro ___________________________o residencia del estudiante? (Especifique cuál)
2. ¿En qué idioma(s) se le habla al estudiante ❏ Inglés ❏ Español ❏ Otro ___________________________la mayor parte del tiempo (Especifique cuál)
en el hogar o residencia?3. ¿Qué idioma(s) entiende el estudiante? ❏ Inglés ❏ Español ❏ Otro ___________________________
(Especifique cuál)
4. ¿Qué idioma(s) habla el estudiante? ❏ Inglés ❏ Español ❏ Otro ___________________________(Especifique cuál)
5. ¿En qué idioma(s) lee el estudiante? ❏ Inglés ❏ Español ❏ Otro _____________ ❏ No lee
(Qué idioma)
6. ¿En qué idioma(s) escribe el estudiante? ❏ Inglés ❏ Español ❏ Otro _____________ ❏ No escribe
(Qué idioma)
7. ¿En su opinión, qué tan bien el estudiante entiende, habla, lee y escribe inglés?
The University of the State of New York • The State Education Department • Office of Bilingual EducationAlbany, New York 12234
CUESTIONARIO SOBRE EL IDIOMA QUE SE HABLA EN EL HOGAR(“Home Language Questionnaire, HLQ”) – Spanish
PARA SER COMPLETADO POR EL PERSONAL ESCOLAR(TO BE COMPLETED BY SCHOOL PERSONNEL)
DISTRITO IMPRIMA O ESCRIBA CLARAMENTE (District) (Please print or type Clearly)
ESCUELA GRADO (School) (Grade)
NOMBRE DEL ESTUDIANTE (Student Name)
FECHA DE NACIMIENTO (Date Of Birth)
NUMERO DE IDENTIFICACION DEL ESTUDIANTE (Student Identification Number)
PAIS NATAL O ASCENDENCIA (Country of Birth/Ancestry)
NUMERO DE AÑOS MATRICULADO EN ESCUELA(S) FUERA DE LOS E.U. (Number of years enrolled in school outside the U.S.)
NOMBRE/POSICIÓN DEL PERSONAL ESCOLAR LLENANDO ESTA SECCION (Name/Position School Personnel Completing This Section)
DETERMINACIÓN: ❏ Posiblemente LEP (Possibly LEP)❏ Dominante en Inglés (English Proficient)
Estimado Padre/Madre o Guardián:
Para poder ofrecer a su hijo(a) la mejor
educación posible, necesitamos
determinar cuán efectivamente él o ella
entiende, habla, lee y escribe el idioma
inglés. Su ayuda será apreciada si
contesta estas preguntas.
Gracias.
Muy bien Un poco Nada
Entiende Inglés ❏ ❏ ❏
Habla Inglés ❏ ❏ ❏
Lee Inglés ❏ ❏ ❏
Escribe Inglés ❏ ❏ ❏
_________________________________________________ ____________________________________________________Firma del Padre/Madre/Guardián/Otro Fecha (Signature of Parent/Guardian/Other) (Date)
HLQ (2/00) 99-337 PM
Mes: Día: Año: (Month) (Day) (Year)
Mes: Día: Año: (Month) (Day) (Year)
(Determination)

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-4746 • Fax (716) 816-3974 Revised 4/17/13
PARENT CONSENT FORM
Date: Parent/Legal Guardian of:
DOB:
I give my consent for initial placement of my child in Special Education program/services.
I do not agree to the delivery of Special Education services for my child as recommended on the Individualized Education Program (IEP).
Date: Signature: Relationship to Student: Please Note: Your child will not be placed in a Special Education program without your consent. If you agree with this recommendation, please complete and return to:
If you disagree, no further action will be taken and your child will not be placed into the recommended Special Education program.

33 Ash Street, Buffalo, New York 14204 (716) 816-4746 ♦ Fax (716) 816-3974
“Putting children and families first, to ensure high academic achievement for all.”
Buffalo Public Schools Dr. Pamela C. Brown, Ed.D. . Superintendent
Buffalo Public Schools
Notice Concerning Our receipt of Public Health Insurance Funds
And Your Related Rights.
No Action is Required by You.
We are required to provide you with an annual reminder of your rights related to this District’s receipt of funds through the State Medicaid Program. This money, received through the New York Department of Health helps support services provided to all children. To receive this funding we are required to file claims with the State Medicaid Program for some of the health care service we provide our students. This includes services such as nursing, physical therapy, occupational therapy, psychological counseling, and speech therapy. The information is provided electronically through processes prescribed by the Federal and State governments. It contains information like service code, date of service, and duration. No information is provided without the voluntary consent of the student’s parent or guardian and they can withdraw their consent at any time. Regardless of whether or not the public insurance program pays for these services, or whether or not the parent allows us to bill, these services are provided free of charge to parents for a long as the student needs them. Should you have any questions, wish to consent to our seeking this funding, or wish to withdraw consent you have already granted please contact: Nina Blumlein Director [email protected]

Buffalo Public Schools Dr. Pamela C. Brown, Ed.D. Superintendent
Dear Parent/Guardian of ______________________________: This is to ask your permission (consent) to bill your child’s Medicaid Insurance Program for special education and related services that are on your child’s individualized education program (IEP). This consent allows the school district to bill for covered health-related services and to release information to the school district’s Medicaid Billing Agent for that purpose.
I, _______________________________________________________________ as the parent/guardian of ______________________________________________(Print Child’s Name)_______________(Date of Birth)
have received a written notification from the school district that explains my federal rights regarding the use of public benefits or insurance to pay for certain special education and related services.
I understand and agree that the school district may access Medicaid to pay for special education and related services
provided to my child. I understand that:
• Providing consent will not impact my child’s/my Medicaid coverage; • Upon request, I may review copies of records disclosed pursuant to this authorization; • Services listed in my child’s IEP must be provided at no cost to me whether or not I give consent to bill
Medicaid; • I have the right to withdraw consent at any time; and • The school district must give me annual written notification of my rights regarding this consent.
I also give my consent for the school district to release records/information about my child to the State Medicaid Agency for the purpose of billing for special education and related services that are in my child’s IEP to include nursing, physical therapy, occupational therapy, psychological counseling, and speech therapy. The information is provided electronically through processes prescribed by the Federal and State governments. It contains information like service code, date of service, and duration. No information is provided without my voluntary consent and I can withdraw their consent at any time. I give my consent voluntarily and understand that I may withdraw my consent at any time. I also understand that my child’s right to receive special education and related services is in no way dependent on my granting consent and that, regardless of my decision to provide this consent, all the required services in my child’s IEP will be provided to my child at no cost to me. Parent/Guardian Name and Signature: ____________________________________ Print Name ____________________________________ Date
□Notice given to Parent/Guardian at CSE meeting on _______________. □ Notice mailed/given to Parent/Guardian on __________.
CONSENTIMIENTO DEL PADRE PARA LA DIVULGACIÓN DE INFORMACIÓN EDUCACIONAL PARA LA CUBERTURA POR EL MEDICAID
TERMINOS, DERECHOS Y RESPONSABILIDADES
Por firmar la aplicación presente, yo entiendo y confirmo que:
• He sido informado/a completamente en mi idioma nativo o en algún otro modo de comunicación que al conceder mi consentimiento para la divulgación de información con el propósito de obtener reembolso del Medicaid para los servicios proveídos según el Programa Educativo Individualizado (PEI) de mi hijo/a es voluntario y puede ser revocado en cualquier momento y en caso tal de que yo revoque mi consentimiento, ello no niega (deshace) una acción que ocurrió después que mi consentimiento fue dado y antes que mi consentimiento fue revocado.
• Si yo rehúso mi consentimiento en permitir el uso del seguro Medicaid para el pago de servicios de educación especial, el distrito escolar deberá proveer todos los servicios de educación especial a ningún costo a mi persona.
• El uso del seguro Medicaid para servicios de educación especial no disminuirá la cubertura disponible de por vida, ni aumentaran el costo del seguro, ni resultara en la descontinuación de beneficios, ni resultará en que mi familia tenga que pagar por los servicios requeridos para mi hijo/a fuera de la escuela que sería de lo contrario cubierto por el programa Medicaid o que de lo contrario disminuiría los beneficios de seguro de mi familia bajo el programa Medicaid.
• Yo no incurriré en gastos de mi bolsillo, tales como el pago de un deducible o una cantidad para un co-pago.
Yo, ________________________________________________________,como padre/guardián de (Escriba en letra de molde el nombre del padre o persona en relacion de padre) __________________________________________(Escriba el nombre del niño/a en letra de molde)
Fecha de nacimiento _________________
doy permiso a la agencia pública (distrito escolar, municipio, o proveedor del Medicaid) a que usen el Medicaid para pagar por los servicios del PEI y a tal agencia pública y a cada escuela de educación especial privada aprobada o al proveedor que provea los servicios del PEI a mi hijo/a a divulgar la información concerniente al diagnosis y los códigos de procedimientos para el envío de la factura al Medicaid para los servicios descritos en el PEI de mi hijo/a y para las evaluaciones en relación a estos servicios; y en el evento de una auditoria, el requisito de documentación para el reembolso de los servicios de apoyo por el Medicaid de los archivos educacionales de mi hijo/a a los representantes locales, estatales y federales con el propósito único de reclamar el reembolso del Medicaid para los servicios de apoyo relacionados a la salud cubiertos para cada servicio y para cada año escolar en la cual el servicio fue proveído, según es recomendado en el PEI de mi hijo/a si es que mi hijo/a es elegible o llegase a ser elegible para el Medicaid. Doy mi consentimiento voluntariamente y entiendo que yo podré retirar mi consentimiento en cualquier momento. También entiendo que el derecho de mi hijo/a de recibir una Educación Pública Gratis y Apropiada (Free Appropriate Public Education- FAPE) en ninguna manera depende de que yo conceda mi consentimiento. Firma ____________________________________ Fecha _____________________
□ La notificación entregada al padre / Guardián en la reunión de CSE en ____________________. □ Notificación por Correo / dado al Padre de Familia en ________________.

Graduations – (June, August and January)
Complete the Graduated Students form and submit it to [email protected] (or fax to 716-878-9706 attention Debbie Jacob) by the last week of June. If any of your students graduate in August or January please submit this form within a month of graduating.
Opening Audit – (Summer)
BPS personnel will arrange a meeting prior to your school’s start date to determine if any new entrants to your school to see if they have an IEP or 504 plan. For the Opening Audit – complete the New Students form to list ALL students who are new to your school and the Exited Students form for those students who have left your school. Make sure to bring both forms for your opening audit appointment. Indicate the reason the student has exited (i.e. the student has dropped out, moved out of district, transferred to another charter, non-public or Buffalo Public School) and, where applicable, the specific school they transferred to and the date the student left.
Exits/Enrollment for Students with Disabilities – (Monthly)
Complete the Charter School Enrollment/Exit Report on a monthly basis if you have any new students or exited students so we can identify those that have IEPs or 504 plans, and exit those who have left. If you have no changes, do not submit the form.
Data Verification for State Reporting – (November)
On November 1st, 2015 forward a list of all Special Education students who were enrolled in your school on BEDS day to [email protected] (or fax to 716-878- 9706 attention Debbie Jacob).

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-3717 • Fax (716) 816-3970 Revised 4/16/13
Student and Teacher Assignment for CSE
School Name: CSE Case Manager:
Student Name Grade Level General Education Teacher Special Education Teacher 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20.

“Putting Children and Families First to Ensure High Academic Achievement for All”
Charter School Student Enrollment/Exit Monthly Status Report
Indicator 11: Child Find Data Submission Charter School:_______________________ Date:_____________________
Student Name
I.D.# and/ or DOB
Date of Enrollment
Date of Exit
Exit Reason (i.e., moved out of district, expelled, dropped out, graduated, etc.)
Additional Information/ Comments (i.e., school where student is currently enrolled.)

Exited Students
School Name:Case Manager (Charter Schools Only):Contact Person that can be reached in the summer (include phone number and e-mail):
900 # Last Name First Name DOB GradeDate of Exit
Where the student went? (Dropped out, School the student is attending now/Graduated from High School, etc.)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19

Graduated Students - Please submit by the Last Week of June
School Name:Case Manager (Charter Schools Only):Contact Person that can be reached in the summer (include phone number and e-mail):
900 # Last Name First Name DOBDiploma Date Diploma Type
Post Grad Location Post Grad Plans
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17

Diploma Types:
IEP Diploma (June 2013 only)
Local Diploma
RegentsRegents with HonorsRegents with CTE (Career Education)
Post Grad. Location:
IS: In-StateOS: Out of State
Post Grad. Plans:
Attend a 4 year College in NYSAttend a 2 year College in NYSAttend other postsecondary school in NYSAttend 4 year college outside NYSAttend 2 year college outside NYS Attend other postsecondary outside NYSSeek employmentEnlist in the militaryOtherAdult ServicesUnknown
Local Diploma with Career Education
Certificate of Career Development and Occupational Studies (Beginning the 2013-2014 school year)
Regents with Adv Designation (specify subject area if applicable)

New StudentsMake sure to check all new students - not just the ones that let you know they had an IEP** * If you can not obtain the students 900# make sure to have the Date of Birth (DOB)School Name:Case Manager:900 # Last Name First Name DOB Grade
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25

Suspensions, MDR and Expelled Students
Charter school personnel are responsible for holding suspension hearings for Students with Disabilities. Charter regulations require that you notify the district to conduct a manifestation determination prior to removing a student for more than 10 days.
Contact the Buffalo Public School Manifestation Determination Office in writing via fax (816-3049) to schedule a Manifestation Determination Review (MDR)
Provide to MDR office, via fax (816-3049) the name of the student, the discipline reports, names of the special education and general education teacher, as well as any additional school representatives who will be attending the MDR meeting.
Meetings will be convened at 432 City Hall
For students approaching 10 cumulative days of “suspension”: Contact the MDR Office in writing via fax (816-3049) to request that Pattern
Determination be conducted. Forward to the MDR office, via fax (816-3049) the name of the student, Buffalo I.D. #,
and the discipline records. Following the MDR, the CSE will convene to review IEP recommendations, the need for FBA and/or BIP, and to determine, as applicable, the need for IAES (Interim Alternative Educational Setting) and special education services necessary to enable the student to continue to participate in the general curriculum and progress in meeting the goals set out in the student’s IEP. The Charter school is responsible for providing for providing these services. In cases of expulsion, charter school personnel will email the appropriate CSE chairperson, with the student’s last date of attendance, as well as parent contact information. In addition, the school should inform the parent of the need to register the student at School 12, if the parent is planning on having the child attend a BPS school. The parent should bring immunization records, proof of address, and birth certificate to register the student. School 12 is located at 33 Ash Street, Buffalo, NY 14204. **NOTE: The Charter School is responsible for providing instructional services (FAPE) until the student is enrolled in another school. Should you have any questions, or need to request a reschedule, etc… contact the MDR office at 816-3640.

Initial Referrals
Per 200.4 (a)(iv)(b)(2) of the Regulations of the Commissioner, the parent should be offered “the opportunity to meet to discuss the request for referral, and, as appropriate, the availability of appropriate general education support services for the student.” If the parent wishes to continue the referral process, parental consent for all evaluations will be obtained by the Central Committee on Special Education. Initial Referral According to New York state regulations (200.4): A written request for an initial referral submitted by persons other than the student or a judicial officer shall:
1. State the reason for the referral and include any test results, records or reports upon which the referral is based that may be in possession of the person making the referral.
2. Describe in writing, intervention services, programs or instructional methodologies used to remediate the student’s performance prior to the referral, including supplementary aids or support services provided for the purpose, or state the reason why no such attempts were made.
3. Describe the extent of parental contact or involvement prior to the referral. The Student Intervention Record must be fully completed and include research based documentation for each implemented intervention. The Request for Committee on Special Education Referral (Initial), should be sent to the Supervisor of Special Education, at School #12 with the following documents:
• Student Intervention Record with cover sheet • Copy of current physical exam • Home Language Questionnaire • Related service referral checklists (refer to Related Service section).
Buffalo Public Schools
REQUEST FOR A COMMITTEE ON SPECIAL EDUCATION INITIAL REFERRAL
Date of request: Requested by (name/title): Relationship to Student: Student Name: ____________ Student Number: Date of Birth: Sex: Dominant Language: Address: ZIP: Parent/Guardian: Phone: School: Grade: Teacher/Counselor: Student approved for ESL: Yes No Start Date: Proficient End Date: Parent’s Dominant Language: Interpreter Needed: Yes No REASON FOR REQUEST: (Please describe specific concerns.) FOR NEW REQUESTS/RE-REQUESTS:
• List previous programs, accommodations, and support services:
• Attach the Student Intervention Record and progress monitoring data. This should include specific information about what has been done to meet the student’s educational needs in his/her present setting.
IF ABOVE ARE NOT APPLICABLE, THE BUILDING ADMINISTRATOR IS TO ATTACH A RATIONALE STATEMENT JUSTIFYING THE ABSENCE OF PRE-REFERRAL INTERVENTIONS.

REVISED 4/24/14 2
FOR TRANSFER STUDENTS: Previous District: State: Previous Teacher/Counselor: Phone #: Previous Classification: Previous Services: BUILDING INTERVENTION TEAM: FOR OFFICE USE ONLY:
Date of receipt of request for referral Name and title of Administrator receiving request
Date of copy of request forwarded to Building or SE Administrator
Date Referral forwarded to CSE Chairperson Date received by CSE Chairperson
Name and title of person making Referral to CSE
Date parent notified of Referral
BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
Student Interventions Record
Date completed:
1. Student Information
Student Name: ID Number: DOB:
Native Language: Address:
Translation: Yes No Phone:
Ethnicity: Gender: Male Female
School: Teacher(s):
Grade:
2. Parent/Guardian Information (If other parent, indicate relationship below name)
Parent/Guardian: Parent/Guardian:
Relationship: Relationship:
Address: Address:
City, State & Zip City, State & Zip
Home Tel: Home Tel:
Work Tel: Work Tel:
Native Lang: Native Lang:
Translation: Yes No Translation: Yes No
3. Referral Information
Area of Suspected Disability: Check and describe the specific reason(s) and/or situations that
may indicate the presence of a disability.
Primary Consideration Secondary Consideration
Educational Achievement Educational Achievement
Social/Behavioral Social/Behavioral
Physical Physical
Other: Other:
Attach an RTI packet for each area of concern as applicable: Check what is included
Tier 2 Tier 3
ELA ELA
Math Math
Behavior Behavior

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
4. Background Information
Describe child’s educational, cultural and experiential background and how this may be
affecting progress. This especially pertains to students new to the district and whose native
language is other than English. Regulations require that the determinant factor for eligibility for
a child to have a disability cannot be the lack of appropriate instruction in reading or math or
limited English proficiency.
Is absenteeism or lateness a problem? Yes No
Has student ever been retained? Yes No
5. For Students whose language is other than English
How long has the student been going to school in the USA? _____________________________
Has the student ever received instruction in English as a Second Language?
If yes, indicate test results with the dates and intensity of services provided:
6. Health Information (to be completed by the school nurse)
Are there any medical conditions which may be contributing to the student’s reason for
referral: Yes No If yes, please describe below:
Indicate any medications the student is receiving:
1. 2.
3. 4.
5. 6.
Date of Last Physical Examination: ___________________
Signature of School Nurse: _________________________

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
RtI Individual Student Plan _____ ELA
_____ Math
Tier 2 Intervention _____ Behavior Student Name: School Year:
Classroom Teacher: Tier 2 Intervention Start Date:
Teacher Delivering Intervention: Grade:
A. Identify the Student Problem: (Describe in clear specific terms the student’s academic or behavioral problem.)
B. Select Data Collection Method: (Choose a method of data collection to measure whether the classroom intervention actually
improves the identified student problem (e.g. curriculum‐based measure (CBM), DIBELS, etc.))
How frequently will this data be collected?
C. Collect Data to Calculate Baseline: (What method from the choices below will be used to estimate the student’s baseline
(starting) performance? Generally at least 3‐5 baseline data points are recommended.)
BASELINE DATA
1. Date: Performance: 2. Date: Performance: 3. Date: Performance: 4. Date: Performance: 5. Date: Performance:
D. Determine Intervention Timespan The intervention will last __________ weeks.
E. Set a Performance Goal: (What specific, measureable goal is the student expected to achieve if the intervention is successful?)
Date completing form:
BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
G. Progress Monitoring Data Points and Observations (MAKE ADDITIONAL COPIES AS NEEDED)
1. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
2. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
3. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
4. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
5. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
6. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
7. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
8. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
9. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
*attach additional data if available
H. Intervention Results: (Determine next steps based on
intervention summary.) _____ Success; terminate Tier 2 Intervention
_____ Some progress; continue with Tier 2 Intervention
_____ Minimal to no progress; continue with Tier 2 AND add Tier 3 Intervention
F. Select Researched‐Based Intervention
Intervention Description: Intervention Delivery: Check‐Up Date: Assessment Data: List each intervention that you plan to use to address the student’s concern(s).
List key details about delivery of the intervention, such as: (1) where & when the intervention will be used; (2) the adult‐to‐student ratio; (3) how frequently the intervention will take place; (4) the length of time each session of the intervention will last.
Select a date when the data will be reviewed to evaluate the intervention.
Note what classroom data will be used to establish baseline, set a goal for improvement, and track the student’s progress during this intervention.
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
RtI Individual Student Plan _____ ELA
_____ Math
Tier 3 Intervention _____ Behavior
Student Name: School Year:
Classroom Teacher: Tier 3 Intervention Start Date:
Teacher Delivering Intervention: Grade:
A. Identify the Student Problem: (Describe in clear specific terms the student’s academic or behavioral problem. Use the same description from the student’s Tier 2 intervention form, add results of Tier 2 intervention.)
B. Select Data Collection Method: (Use the same data collection method as the student’s Tier 2 intervention.) How frequently will this data be collected?
C. Collect Data to Calculate Baseline: (Use the Intervention Outcome from the student’s Tier 2 intervention.)
BASELINE DATA
1. Date: Performance: 2. Date: Performance: 3. Date: Performance: 4. Date: Performance: 5. Date: Performance:
D. Determine Intervention Timespan
The intervention will last __________ weeks.
E. Set a Performance Goal: (Use the same goal from the student’s Tier 2 intervention form.)
Date completing form:

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
G. Progress Monitoring Data Points and Observations (MAKE ADDITIONAL COPIES AS NEEDED)
1. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
2. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
3. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
4. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
5. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
6. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
7. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
8. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
9. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
*attach additional data if available
F. Select Researched‐Based Intervention
Intervention Description: Intervention Delivery: Check‐Up Date: Assessment Data:
List each intervention that you plan to use to address the student’s concern(s).
List key details about delivery of the intervention, such as: (1) where & when the intervention will be used; (2) the adult‐to‐student ratio; (3) how frequently the intervention will take place; (4) the length of time each session of the intervention will last.
Select a date when the data will be reviewed to evaluate the intervention.
Note what classroom data will be used to establish baseline, set a goal for improvement, and track the student’s progress during this intervention.
Tier 2 Intervention (To be completed simultaneously with the new, Tier 3 intervention.)
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________
Tier 3 Intervention (To be completed simultaneously with the previous Tier 2 intervention.)
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________
H. Evaluate the Intervention Outcome/Results: (Determine next steps based on intervention summary.)
_____ Success; terminate Tier 3 Intervention _____ Some progress; continue with Tier 2 and Tier 3 Interventions _____ Minimal to no progress; continue with Tier 2 and Tier 3 Intervention; Conference with parent
Conference Date _________________ Result of conference: Attendees _____ Continue with interventions 1. 2. 3. _____ Refer to CSE 4. 5.
BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
7. Other Interventions Attempted to Resolve Referral Concerns Interventions Implementation dates and progress information
Alternative Programs/Differentiated instruction
Start Date: End Date:
Teacher:
Comments on Progress:
Speech Improvement Services Start Date: End Date:
Teacher:
Comments on Progress:
Adjusted Assignments Start Date: End Date:
Teacher:
Comments on Progress:
Schedule Adjustments Start Date: End Date:
Teacher:
Comments on Progress:
Alternative Approaches to Learning Start Date: End Date:
Teacher:
Comments on Progress:
Counseling/Mentoring/Social Skills training
Start Date: End Date:
Teacher:
Comments on Progress:
Other (Behavior Plan) Start Date: End Date:
Teacher:
Comments on Progress:
Consultation with:
Principal/Assistant Principal
Speech Therapist
Psychologist
Guidance Counselor
Other:__________________
Social Worker
Special Ed Teacher
Additional Comments and Details:
8. Work Habits
Always Usually Sometimes Rarely
Completes Class Work
Completes Homework
Motivated to learn
Attentive to task
Can transition between activities
Generalizes learning to new situations
Works independently
Frustrates easily
Distractible
Short attention span
Inconsistent learning

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
9. Speech and Language Information
Indicate any areas that appear problematic for the student:
Articulation
Comprehension of basic
information/vocabulary
Maintaining topic of relevancy
Dysfluencies (stuttering)
Expressing self verbally
Additional Concerns:
*Please include completed speech/language questionnaire if you indicate any
speech/language concerns and screening if available.
10. Indicate the Students Performance Levels
Please describe levels of academic achievement (reading, math, and written language), learning
characteristics, ability to function in classroom, and/or adaptive behavior skills. Include specific
areas of strength and weakness. Attach report cards, standardized test results and
transcripts.
Reading Comprehension
Strengths:
Needs:
Reading Decoding
Strengths:
Needs:
BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
Math Computation
Strengths:
Needs:
Math Concepts/Applications
Strengths:
Needs:
Written Language
Strengths:
Needs:
Learning characteristics, Adaptive Behavior, Strengths and Weaknesses:

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
Please describe levels of social development. Include the quality of the student’s relationship
with peers and adults, adjustment to school and community, and indicate any behaviors that
interfere with the learning environment or may impede the student’s learning process. Attach
Functional Behavioral Assessment (FBA)/Behavior Intervention Plan (BIP), if applicable.
Strengths:
Needs:
Please describe levels of physical development. Include the student’ motor and sensory
development and any physical skills or limitation that may pertain to the leaning process. Are
there any health concerns, diagnoses, etc…? Are there any fine or gross motor concerns, if so
complete the OT/PT checklists as needed.
Please attach the following:
Student’s current report card
Student attendance record
Student schedule
CBM data reports (AIMSweb, STAR, etc…)
Standardized Assessment reports (i.e. TerraNova, State Assessments)
Behavior Plans Data (i.e. BPIS plans, Behavior Modification Plans, other behavior
reports)
Career Plan (high school students only)
Level 1 (age 12 in calendar year and older)
High School Transcript
504 Plan (if applicable)

The University of the State of New York • The State Education Department • Office of Bilingual EducationAlbany, New York 12234
Home Language Questionnaire (HLQ)TO BE COMPLETED BY SCHOOL PERSONNEL
DISTRICT Please print or type clearly
SCHOOL GRADE
STUDENT NAME
DATE OF BIRTH
STUDENT IDENTIFICATION NUMBER
COUNTRY OF BIRTH / ANCESTRY
NUMBER OF YEARS ENROLLED IN SCHOOL OUTSIDE THE U.S.
NAME/POSITION OF SCHOOL PERSONNEL COMPLETING THIS SECTION
DETERMINATION: ❏ Possible LEP
❏ English Proficient
Dear Parent or Guardian:
In order to provide your child with the
best possible education, we need to
determine how well he or she under-
stands, speaks, reads and writes
English. Your assistance in answering
these questions is greatly appreciated.
Thank You
(✔ boxes that apply)
1. What language(s) is spoken in the student’s ❏ English ❏ Other __________________________________home or residence? specify
2. What language(s) are spoken most of the time ❏ English ❏ Other __________________________________to the student, in the home or residence? specify
3. What language(s) does the student understand? ❏ English ❏ Other __________________________________specify
4. What language(s) does the student speak? ❏ English ❏ Other __________________________________specify
5. What language(s) does the student read? ❏ English ❏ Other _______________ ❏ Does Not Readspecify
6. What language(s) does the student write? ❏ English ❏ Other _______________ ❏ Does Not Writespecify
7. In your opinion, how well does the student understand, speak, read and write English?
_________________________________________________ ____________________________________________________Signature of Parent/Guardian/Other Date HLQ (2/00) 99-337 PM
Month: Day: Year:
Month: Day: Year:
Very well Only a little Not at all
Understands English ❏ ❏ ❏
Speaks English ❏ ❏ ❏
Reads English ❏ ❏ ❏
Writes English ❏ ❏ ❏

(✔ Marque las casillas que aplican)
1. ¿Qué idioma(s) se habla en el hogar ❏ Inglés ❏ Español ❏ Otro ___________________________o residencia del estudiante? (Especifique cuál)
2. ¿En qué idioma(s) se le habla al estudiante ❏ Inglés ❏ Español ❏ Otro ___________________________la mayor parte del tiempo (Especifique cuál)
en el hogar o residencia?3. ¿Qué idioma(s) entiende el estudiante? ❏ Inglés ❏ Español ❏ Otro ___________________________
(Especifique cuál)
4. ¿Qué idioma(s) habla el estudiante? ❏ Inglés ❏ Español ❏ Otro ___________________________(Especifique cuál)
5. ¿En qué idioma(s) lee el estudiante? ❏ Inglés ❏ Español ❏ Otro _____________ ❏ No lee
(Qué idioma)
6. ¿En qué idioma(s) escribe el estudiante? ❏ Inglés ❏ Español ❏ Otro _____________ ❏ No escribe
(Qué idioma)
7. ¿En su opinión, qué tan bien el estudiante entiende, habla, lee y escribe inglés?
The University of the State of New York • The State Education Department • Office of Bilingual EducationAlbany, New York 12234
CUESTIONARIO SOBRE EL IDIOMA QUE SE HABLA EN EL HOGAR(“Home Language Questionnaire, HLQ”) – Spanish
PARA SER COMPLETADO POR EL PERSONAL ESCOLAR(TO BE COMPLETED BY SCHOOL PERSONNEL)
DISTRITO IMPRIMA O ESCRIBA CLARAMENTE (District) (Please print or type Clearly)
ESCUELA GRADO (School) (Grade)
NOMBRE DEL ESTUDIANTE (Student Name)
FECHA DE NACIMIENTO (Date Of Birth)
NUMERO DE IDENTIFICACION DEL ESTUDIANTE (Student Identification Number)
PAIS NATAL O ASCENDENCIA (Country of Birth/Ancestry)
NUMERO DE AÑOS MATRICULADO EN ESCUELA(S) FUERA DE LOS E.U. (Number of years enrolled in school outside the U.S.)
NOMBRE/POSICIÓN DEL PERSONAL ESCOLAR LLENANDO ESTA SECCION (Name/Position School Personnel Completing This Section)
DETERMINACIÓN: ❏ Posiblemente LEP (Possibly LEP)❏ Dominante en Inglés (English Proficient)
Estimado Padre/Madre o Guardián:
Para poder ofrecer a su hijo(a) la mejor
educación posible, necesitamos
determinar cuán efectivamente él o ella
entiende, habla, lee y escribe el idioma
inglés. Su ayuda será apreciada si
contesta estas preguntas.
Gracias.
Muy bien Un poco Nada
Entiende Inglés ❏ ❏ ❏
Habla Inglés ❏ ❏ ❏
Lee Inglés ❏ ❏ ❏
Escribe Inglés ❏ ❏ ❏
_________________________________________________ ____________________________________________________Firma del Padre/Madre/Guardián/Otro Fecha (Signature of Parent/Guardian/Other) (Date)
HLQ (2/00) 99-337 PM
Mes: Día: Año: (Month) (Day) (Year)
Mes: Día: Año: (Month) (Day) (Year)
(Determination)
Reevaluation
Parent and/or School Requested Reevaluation
The Student Intervention Record must be completed fully and include documentation for each implemented research based intervention. Send a completed Student Intervention Record with cover sheet, Request for Committee on Special Education Meeting, (Reevaluation) and any Related Service referral checklists to the Supervisor of Special Education, at School #12.
State Mandated Three Year Reevaluation According to New York State Regulations of the Commissioner of Education, 200.4 (b)(4), a student with a disability have a reevaluation at least once every three years, “except where the school district and the parent agree in writing that such reevaluation is unnecessary.” The following information should be sent to the CSE chairperson:
IEP Information Planning Worksheet for Charter/Non-Public Schools Report Card Attendance Record Reading Test Results/Running Records Standardized Test Results High School Credits/Transcripts Level I Assessment Related Service Progress Summaries Cumulative Record Card BIP Progress Monitoring Reports Discipline Records Career Plan
The Student Intervention Record is required if the student is being considered for a change of classification or a more restrictive placement. For all Reevaluation or Reevaluation/AR meetings the following fields of the IEP draft should be updated: • Academic, Social, and Physical Present Levels of Performance (PLEP) • Goals (please leave current goals in for matter of discussion) • For students age 15 or turning 15 within the year, complete Measurable Post- Secondary goals and Coordinated Set of Transition Activities reflecting the information in the Academic PLEP • Do NOT enter any information under the Effects of Student Needs. Only Psychologist/Speech Therapist complete this section.

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-4746 • Fax (716) 816-3974 Revised 4/29/13
REQUEST FOR A COMMITTEE ON SPECIAL EDUCATION MEETING REEVALUATION
Student: School: Student ID#: Date of Birth: Grade:
Parent/Guardian: Teacher/Counselor: Relationship to Student: Emergency Contact#:
Address: Mother’s Work #: Father’s Work #:
Home Phone#: Language: REASON FOR CSE MEETING: (Please describe specific concerns.)
Attach Student Intervention Record IF ABOVE ARE NOT APPLICABLE, THE BUILDING ADMINISTRATOR OR CENTRAL OFFICE SPECIAL EDUCATION ADMINISTRATOR IS TO ATTACH A RATIONALE STATEMENT JUSTIFYING THE ABSENCE OF EITHER THE EDUCATIONAL BENEFIT OR STUDENT INTERVENTION RECORD FORMS. Signature: Title: Date: Forward to District Representatives/CSE Chair Date
Return to Referring Teacher for More Data
Date
Building Administrator Date Received
Central Office Special Education Administrator
Date Received
Forward to Related Service Supervisor
Date
Date request for referral received by CSE/District Representative
Date

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-4746 • Fax (716) 816-3974 Revised 4/29/13
ATTACHMENT TO THE REQUEST FOR A CSE MEETING REEVALUATION
Student Name: I.D. #: School: Date Request: The School is requesting that the CSE conduct a reevaluation. Why is the School requesting this reevaluation?
What records, reports, or other relevant information was used in the decision to request this revaluation?
Were there any other options considered prior to requesting this reevaluation?
Is there any other relevant information that the CSE should be aware of?

IEP INFORMATION PLANNING WORKSHEET FOR CHARTER & NON‐PUBLIC SCHOOLS
Student Name: DOB:
Address: Phone #: Cell #:
Email:
School: Grade: Teacher:
Please return this form (Fax: 878‐9706 to appropriate chair) along with the following
information/documents at least 2 weeks prior to scheduled meeting date:
Report Card Level 1 Vocational Assessment
Attendance Record IEP Progress Reports
Schedule Diagnostic Related Service Summaries
Reading Test Results/Running Records Cumulative Record Card
Standardized Test Results Discipline Reports
High School Credits/Transcripts Behavior Intervention Plan Progress Monitoring
Summer School Information Additional RTI data
Career Plan
Please include statement reflecting CAN DO skill levels & abilities, progress, strengths,
weaknesses, NEEDS, learning styles & modalities, and work habits.
Reading
o Strengths:
o Needs:
Written Language
o Strengths:
o Needs:

Math
o Strengths:
o Needs:
Social/Emotional/Behavior (interests, strengths, difficulties, needs)
Other Pertinent Information (i.e. work habits, task completion rate, learning modalities,
attendance, additional diagnosis/health or medical information, etc...)
Academic/Behavioral Interventions (including Start/End dates, Frequency, duration,
setting, & Student Response: Progress Monitoring Data):
Physical Development (Health history, diagnoses, etc…):

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
Student Interventions Record
Date completed:
1. Student Information
Student Name: ID Number: DOB:
Native Language: Address:
Translation: Yes No Phone:
Ethnicity: Gender: Male Female
School: Teacher(s):
Grade:
2. Parent/Guardian Information (If other parent, indicate relationship below name)
Parent/Guardian: Parent/Guardian:
Relationship: Relationship:
Address: Address:
City, State & Zip City, State & Zip
Home Tel: Home Tel:
Work Tel: Work Tel:
Native Lang: Native Lang:
Translation: Yes No Translation: Yes No
3. Referral Information
Area of Suspected Disability: Check and describe the specific reason(s) and/or situations that
may indicate the presence of a disability.
Primary Consideration Secondary Consideration
Educational Achievement Educational Achievement
Social/Behavioral Social/Behavioral
Physical Physical
Other: Other:
Attach an RTI packet for each area of concern as applicable: Check what is included
Tier 2 Tier 3
ELA ELA
Math Math
Behavior Behavior

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
4. Background Information
Describe child’s educational, cultural and experiential background and how this may be
affecting progress. This especially pertains to students new to the district and whose native
language is other than English. Regulations require that the determinant factor for eligibility for
a child to have a disability cannot be the lack of appropriate instruction in reading or math or
limited English proficiency.
Is absenteeism or lateness a problem? Yes No
Has student ever been retained? Yes No
5. For Students whose language is other than English
How long has the student been going to school in the USA? _____________________________
Has the student ever received instruction in English as a Second Language?
If yes, indicate test results with the dates and intensity of services provided:
6. Health Information (to be completed by the school nurse)
Are there any medical conditions which may be contributing to the student’s reason for
referral: Yes No If yes, please describe below:
Indicate any medications the student is receiving:
1. 2.
3. 4.
5. 6.
Date of Last Physical Examination: ___________________
Signature of School Nurse: _________________________

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
RtI Individual Student Plan _____ ELA
_____ Math
Tier 2 Intervention _____ Behavior Student Name: School Year:
Classroom Teacher: Tier 2 Intervention Start Date:
Teacher Delivering Intervention: Grade:
A. Identify the Student Problem: (Describe in clear specific terms the student’s academic or behavioral problem.)
B. Select Data Collection Method: (Choose a method of data collection to measure whether the classroom intervention actually
improves the identified student problem (e.g. curriculum‐based measure (CBM), DIBELS, etc.))
How frequently will this data be collected?
C. Collect Data to Calculate Baseline: (What method from the choices below will be used to estimate the student’s baseline
(starting) performance? Generally at least 3‐5 baseline data points are recommended.)
BASELINE DATA
1. Date: Performance: 2. Date: Performance: 3. Date: Performance: 4. Date: Performance: 5. Date: Performance:
D. Determine Intervention Timespan The intervention will last __________ weeks.
E. Set a Performance Goal: (What specific, measureable goal is the student expected to achieve if the intervention is successful?)
Date completing form:

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
G. Progress Monitoring Data Points and Observations (MAKE ADDITIONAL COPIES AS NEEDED)
1. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
2. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
3. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
4. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
5. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
6. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
7. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
8. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
9. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
*attach additional data if available
H. Intervention Results: (Determine next steps based on
intervention summary.) _____ Success; terminate Tier 2 Intervention
_____ Some progress; continue with Tier 2 Intervention
_____ Minimal to no progress; continue with Tier 2 AND add Tier 3 Intervention
F. Select Researched‐Based Intervention
Intervention Description: Intervention Delivery: Check‐Up Date: Assessment Data: List each intervention that you plan to use to address the student’s concern(s).
List key details about delivery of the intervention, such as: (1) where & when the intervention will be used; (2) the adult‐to‐student ratio; (3) how frequently the intervention will take place; (4) the length of time each session of the intervention will last.
Select a date when the data will be reviewed to evaluate the intervention.
Note what classroom data will be used to establish baseline, set a goal for improvement, and track the student’s progress during this intervention.
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
RtI Individual Student Plan _____ ELA
_____ Math
Tier 3 Intervention _____ Behavior
Student Name: School Year:
Classroom Teacher: Tier 3 Intervention Start Date:
Teacher Delivering Intervention: Grade:
A. Identify the Student Problem: (Describe in clear specific terms the student’s academic or behavioral problem. Use the same description from the student’s Tier 2 intervention form, add results of Tier 2 intervention.)
B. Select Data Collection Method: (Use the same data collection method as the student’s Tier 2 intervention.) How frequently will this data be collected?
C. Collect Data to Calculate Baseline: (Use the Intervention Outcome from the student’s Tier 2 intervention.)
BASELINE DATA
1. Date: Performance: 2. Date: Performance: 3. Date: Performance: 4. Date: Performance: 5. Date: Performance:
D. Determine Intervention Timespan
The intervention will last __________ weeks.
E. Set a Performance Goal: (Use the same goal from the student’s Tier 2 intervention form.)
Date completing form:

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
G. Progress Monitoring Data Points and Observations (MAKE ADDITIONAL COPIES AS NEEDED)
1. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
2. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
3. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
4. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
5. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
6. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
7. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
8. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
9. Date ____/____/____ Results:___________
Was progress made? YES NO Continue intervention OR Modify intervention
*attach additional data if available
F. Select Researched‐Based Intervention
Intervention Description: Intervention Delivery: Check‐Up Date: Assessment Data:
List each intervention that you plan to use to address the student’s concern(s).
List key details about delivery of the intervention, such as: (1) where & when the intervention will be used; (2) the adult‐to‐student ratio; (3) how frequently the intervention will take place; (4) the length of time each session of the intervention will last.
Select a date when the data will be reviewed to evaluate the intervention.
Note what classroom data will be used to establish baseline, set a goal for improvement, and track the student’s progress during this intervention.
Tier 2 Intervention (To be completed simultaneously with the new, Tier 3 intervention.)
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________
Tier 3 Intervention (To be completed simultaneously with the previous Tier 2 intervention.)
Push in Pull out Ratio: __________________ Frequency: _____________ Duration of session: __________ Instructor: ____________________
H. Evaluate the Intervention Outcome/Results: (Determine next steps based on intervention summary.)
_____ Success; terminate Tier 3 Intervention _____ Some progress; continue with Tier 2 and Tier 3 Interventions _____ Minimal to no progress; continue with Tier 2 and Tier 3 Intervention; Conference with parent
Conference Date _________________ Result of conference: Attendees _____ Continue with interventions 1. 2. 3. _____ Refer to CSE 4. 5.
BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
7. Other Interventions Attempted to Resolve Referral Concerns Interventions Implementation dates and progress information
Alternative Programs/Differentiated instruction
Start Date: End Date:
Teacher:
Comments on Progress:
Speech Improvement Services Start Date: End Date:
Teacher:
Comments on Progress:
Adjusted Assignments Start Date: End Date:
Teacher:
Comments on Progress:
Schedule Adjustments Start Date: End Date:
Teacher:
Comments on Progress:
Alternative Approaches to Learning Start Date: End Date:
Teacher:
Comments on Progress:
Counseling/Mentoring/Social Skills training
Start Date: End Date:
Teacher:
Comments on Progress:
Other (Behavior Plan) Start Date: End Date:
Teacher:
Comments on Progress:
Consultation with:
Principal/Assistant Principal
Speech Therapist
Psychologist
Guidance Counselor
Other:__________________
Social Worker
Special Ed Teacher
Additional Comments and Details:
8. Work Habits
Always Usually Sometimes Rarely
Completes Class Work
Completes Homework
Motivated to learn
Attentive to task
Can transition between activities
Generalizes learning to new situations
Works independently
Frustrates easily
Distractible
Short attention span
Inconsistent learning

BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
9. Speech and Language Information
Indicate any areas that appear problematic for the student:
Articulation
Comprehension of basic
information/vocabulary
Maintaining topic of relevancy
Dysfluencies (stuttering)
Expressing self verbally
Additional Concerns:
*Please include completed speech/language questionnaire if you indicate any
speech/language concerns and screening if available.
10. Indicate the Students Performance Levels
Please describe levels of academic achievement (reading, math, and written language), learning
characteristics, ability to function in classroom, and/or adaptive behavior skills. Include specific
areas of strength and weakness. Attach report cards, standardized test results and
transcripts.
Reading Comprehension
Strengths:
Needs:
Reading Decoding
Strengths:
Needs:
BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
Math Computation
Strengths:
Needs:
Math Concepts/Applications
Strengths:
Needs:
Written Language
Strengths:
Needs:
Learning characteristics, Adaptive Behavior, Strengths and Weaknesses:
BPS COMMITTEE ON SPECIAL EDUCATION CHARTER/NON‐PUBLIC SCHOOLS
Please describe levels of social development. Include the quality of the student’s relationship
with peers and adults, adjustment to school and community, and indicate any behaviors that
interfere with the learning environment or may impede the student’s learning process. Attach
Functional Behavioral Assessment (FBA)/Behavior Intervention Plan (BIP), if applicable.
Strengths:
Needs:
Please describe levels of physical development. Include the student’ motor and sensory
development and any physical skills or limitation that may pertain to the leaning process. Are
there any health concerns, diagnoses, etc…? Are there any fine or gross motor concerns, if so
complete the OT/PT checklists as needed.
Please attach the following:
Student’s current report card
Student attendance record
Student schedule
CBM data reports (AIMSweb, STAR, etc…)
Standardized Assessment reports (i.e. TerraNova, State Assessments)
Behavior Plans Data (i.e. BPIS plans, Behavior Modification Plans, other behavior
reports)
Career Plan (high school students only)
Level 1 (age 12 in calendar year and older)
High School Transcript
504 Plan (if applicable)
Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-4746 • Fax (716) 816-3974 Revised 4/29/13
Process for Vocational Assessments
• is the initial phase of a student’s transition plan that includes input from student, parent and teacher.
Level 1 Vocational Assessment:
• is a data gathering process that must be completed by age 12 and updated annually prior to the annual CSE meeting.
• is completed by the lead Special Education teacher who is responsible for bringing the completed document to the CSE meeting.
• findings are reflected in the PLEP statement and used to develop post secondary transition outcomes.
It is one of the responsibilities of the Committee on Special Education (CSE) to review the data collected from the updated vocational assessments during each CSE meeting. Evidence
from this information should be reflected in both the PLEP and transition plan in the IEP document.
Level 1 Vocational Assessment Checklist
Select Level 1 Assessment from A or B
Complete the form with parent/guardian, teacher and student input.
There must be evidence that the Level I document has been updated yearly prior to the CSE meeting.
Use Level I to begin to examine educational programs and career options based on the students’ needs, preferences and abilities.
Hold the CSE meeting.
Use findings from Level I Assessment to complete PLEP statement and post secondary outcomes on IEP document.
Put completed Level I Assessment in student’s IEP folder held by the CSE Chair.

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 (716) 816-4746 • Fax (716) 816-3974 Revised 4/29/13
• is an optional career assessment to be used when the Level I is NOT sufficient to create a realistic transition plan.
Level II Vocational Assessment:
• is available on the subsequent pages
• is completed by the lead Special Education teacher which includes input from student, parent and teacher.
Level II Checklist
There must be evidence that the Level I document has been updated yearly prior to the CSE meeting.
Complete Level II Assessment and Transition Questionnaire Summary Form.
Complete the form with parent/guardian, student, and teacher input.
Use Level II along with Level I to begin to examine educational programs and career options based on the students’ needs, preferences and abilities.
Hold the CSE meeting.
Use findings from Level I and Level II Assessments to complete PLEP statement and post secondary outcomes on IEP document.
Put completed Level II Assessment in student’s IEP folder held by the CSE Chair.

LEVEL I ASSESSMENT School Year 20 -20 Student: Date of Birth: Diploma Expectations: Regents IEP School: Anticipated Date of Graduation: Program: Cumulative Records Reviewed by: Date: Teacher: Interests/Preferences/Strengths:
POST HIGH SCHOOL VOCATIONAL PLANS Student
Interview Date: _______________________
Parent/Guardian Interview Date: _______________________
School Representative Teacher: ____________________________ Counselor: ___________________________ Other: _______________________________
Recommendations/Needs:
Referrals/Activities:
LEVEL I ASSESSMENT School Year 20 - 20
Student: Date of Birth:
School Attending: Program:
District: Counselor:
Teacher: Diploma Expectations: Regents IEP
Anticipated Date of Graduation:
Post-Secondary Goal
Student: What do you plan to be doing after finishing high school?
Parent: What would you like to see your child doing after completing his/her educational program?
Interests/Strengths/Preferences (hobbies/courses/work):
Things that you have tried but you don’t like:
Recommendations/Needs (if appropriate):
Referrals/Activities:
Signatures:
Student: Teacher:
Parent: Counselor:
Other:
Original: Permanent File Date of Interview: CSE Office Parent Teacher

Commencement.doc / page 1
NEW YORK STATE EDUCATION DEPARTMENT
Career Plan Commencement Level
1. Personal Data Name: _____________________________________________________________________________ Student Identification Number: _________________________________________________________ School: _____________________________________________________________________________ 2. Review of Student Career Plan Possible Participants (Initials)
Grade Level:
Date of Review:
Student:
Parent/ Guardian:
Teacher:
Counselor:
Other:
3. Knowledge
A. Self-knowledge: Who am I? Interests: List your top three choices for each of the following areas of interest: Grade Level:
1a. Personal: Out-of-school activities that you enjoy
1b. Academic: Classes or subjects you enjoy the most
1c. Work Preferences: Working with people, ideas, and things
Attachment 1

Commencement.doc / page 2
2. Abilities: List personal skills and talents that will be helpful in a career choice:
Grade Level:
My Personal Abilities . . .
Career areas where my abilities will be useful . . .
Personal and academic areas I need to strengthen:
Grade Level:
I need to strengthen . . .
Steps I will take to strengthen these areas . . .
B. Career Exploration: Where am I going? 1. School and/or Community Experiences: I have participated in the following school and/or community
experiences:
Grade Level:
School and/or Community Experiences: Skills Acquired Through Experience:
2. Work Experiences: I have participated in the following work experiences:
Grade Level:
Work Experiences: Skills Acquired Through Work Experience:

Commencement.doc / page 3
3. Careers of Interest and Characteristics: I am interested in the following careers and have discovered the following information about these careers:
Grade Level:
Careers of Interest:
Education Requirements:
Skills I Need to Acquire:
Work Environment:
Job Outlook:
C. Future Goals and Decision-Making: How do I get there? 1. Career Goals and Action Steps: Grade Level:
Goals: (resulting from career exploration
activities)
Education Plan: (courses that relate to my
career interests)
Action Steps: (what I need to do to accomplish my goals)
Check Off Completed
Steps 4. Skills/Application: What do I need to know? What skills are important to me?
What am I learning? Why am I learning it? How can I use it? Directions: The following skills are needed to succeed in life, work, and education beyond high school. Using the
scale provided, identify for each skill the level of achievement you believe you possess at the beginning of the commencement level and the level you believe you achieved by the end of your senior year. Briefly describe a classroom experience or an activity that helped you develop each skill and identify how each skill can be used in your life and future work experiences.
Skills:
Beginning
(Check Off)
Skill Level I Possess
Experiences/Activities/Application:
Final
Achieved
Skill Level I Have
(Check Off) Basic Skills: Uses a combination of techniques to read, listen to, and analyze complex information; conveys information in oral and written form; uses multiple computational skills to analyze and solve mathematical problems.
Highly Least Developed Developed
Highly Least Developed Developed
Thinking Skills: Demonstrates the ability to organize and process information and apply skills in new ways.
Highly Least Developed Developed
Highly Least Developed Developed

Commencement.doc / page 4
Skills:
Beginning
(Check Off)
Skill Level I Possess
Experiences/Activities/Application:
Final
Achieved
Skill Level I Have
(Check Off) Personal Qualities: Demonstrates skills in setting goals, monitoring progress, and improving performance.
Highly Least Developed Developed
Highly Least Developed Developed
Interpersonal Skills: Communicates effectively and helps others to learn a new skill.
Highly Least Developed Developed
Highly Least Developed Developed
Technology: Applies knowledge of technology to identify and solve problems.
Highly Least Developed Developed
Highly Least Developed Developed
Managing Information: Uses technology to acquire, analyze and organize data, and communicates information.
Highly Least Developed Developed
Highly Least Developed Developed
Managing Resources: Allocates time and financial and human resources to complete a task.
Highly Least Developed Developed
Highly Least Developed Developed
Systems: Demonstrates an understanding of the relationship between the performance of a system and the goals, resources, and functions of an organization.
Highly Least Developed Developed
Highly Least Developed Developed
5. Culminating Activity Directions: Briefly describe the activity that you completed. Indicate the most important thing you learned
about yourself through this activity. Describe how this self knowledge will influence your plans for the future.
Activity:
Self Knowledge/Future Plans:
BUFFALO PUBLIC SCHOOLS Department of Special Education
LEVEL 2 Vocational Assessment Form
Student: ____________________________________________________ Date of Birth _______________ Date __________________________ School ___________________ Teacher__________________________
Use this information to complete the IEP (Present levels and needs statements, transition page, goals/objectives) Source: VESID Transition Toolbox 12/2005
Student Version Dreams/ Goals: What are your hopes and dreams during high school or after graduation?____________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________Employment/Career: What job would you like to have after high school or college graduation? (for example, sales person, electrician, lawyer, etc.)________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ What other careers do you think might be interesting? _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Post Secondary Education/Training: After you graduate from high school, what type of further education/training would you like to pursue? (For example, 2 or 4 year college, trade school, apprenticeship programs, supported employment, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ If you are interested in college, do you know what you will need to apply for the school of your choice? (for example, grade point average, community service, etc.) __ Yes __ No Abilities: What are your talents and skills that will help you in school? ______________________________________________________________________________________________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ ______________________________________________________________________________________________________________________________________________________________

LEVEL 2 Vocational Assessment Form
Student: ____________________________________________________ Date of Birth _______________ Needs: Think about school and your career choices. What skills do you need to develop at this time to be a successful student/ worker? (for example, homework, study skills, organizational skills, chores, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Fears/Behaviors: What might stand in the way of reaching your dreams? (for example, attitude, behavior, etc.) __________________________________________________________ _______________________________________________________________________________ ______________________________________________________________________________________________________________________________________________________________ _______________________________________________________________________________ What will I do to work on my needs this year? At home-_______________________________________________________________________ _______________________________________________________________________________ In school- ______________________________________________________________________ _______________________________________________________________________________ What do you like to do when you have free time?_____________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Favorite Subject:________________________________________________________________ What do you dislike?_____________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Community Living: After graduation, where do you plan on living? (For example, independently, supported apartments, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________Comments: _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________

BUFFALO PUBLIC SCHOOLS Department of Special Education
LEVEL 2 Vocational Assessment Form
Student: ____________________________________________________ Date of Birth _______________ Date __________________________ School ___________________ Teacher__________________________
Use this information to complete the IEP (Present levels and needs statements, transition page, goals/objectives) Source: VESID Transition Toolbox 12/2005
Parent/ Guardian Version Parent/ Guardian’s Name _______________________________________________ Dreams/ Goals: What are your future hopes and dreams for the student during high school or after graduation?______________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Employment/Career: What jobs do you see the student having after high school graduation? (for example, sales person, electrician, lawyer, etc.)________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ What other careers do you think he/she should pursue? _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Post Secondary Education/Training: After he/she graduates from high school, what type of further education/training do you see him/her pursuing? (For example, 2 or 4 year college, trade school, apprenticeship programs, supported employment, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ If he/she is interested in college, do you know what is needed to apply for the school of his/her choice? (for example, grade point average, community service, etc.) __ Yes __ No Abilities: What are the student’s talents and skills that will help him/her in school? ______________________________________________________________________________________________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________
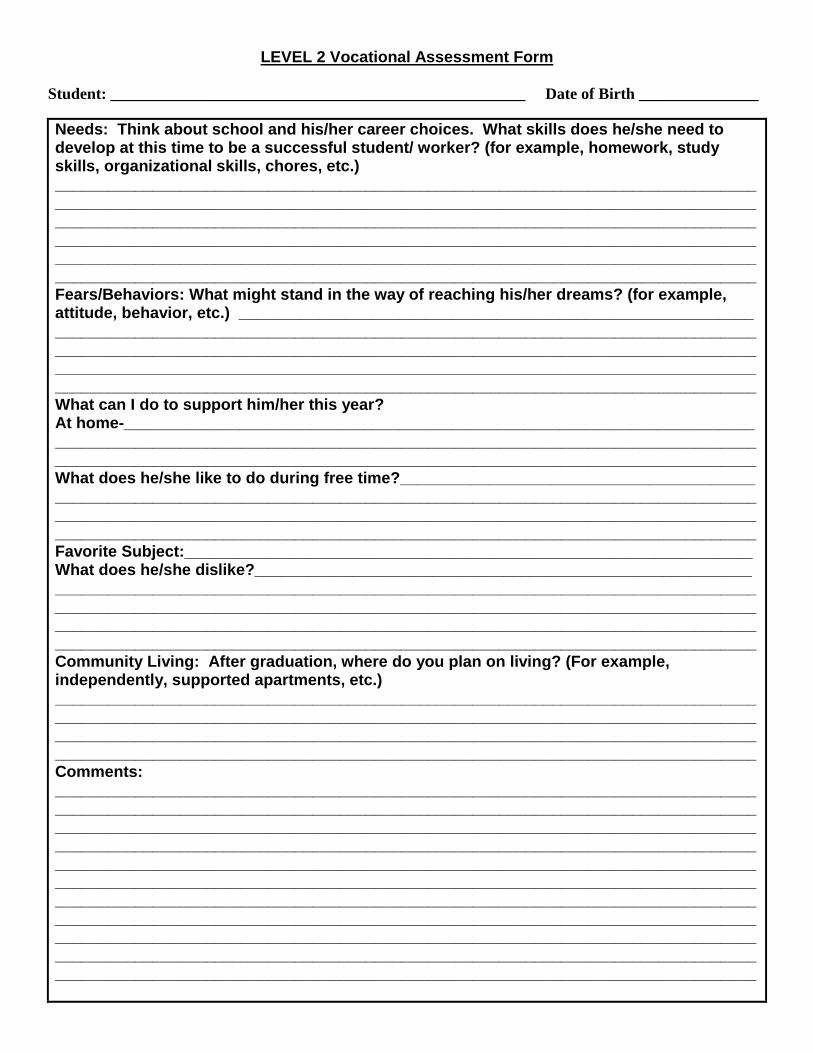
LEVEL 2 Vocational Assessment Form
Student: ____________________________________________________ Date of Birth _______________ Needs: Think about school and his/her career choices. What skills does he/she need to develop at this time to be a successful student/ worker? (for example, homework, study skills, organizational skills, chores, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Fears/Behaviors: What might stand in the way of reaching his/her dreams? (for example, attitude, behavior, etc.) __________________________________________________________ _______________________________________________________________________________ ______________________________________________________________________________________________________________________________________________________________ _______________________________________________________________________________ What can I do to support him/her this year? At home-_______________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ What does he/she like to do during free time?________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Favorite Subject:________________________________________________________________ What does he/she dislike?________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Community Living: After graduation, where do you plan on living? (For example, independently, supported apartments, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________Comments: _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________

BUFFALO PUBLIC SCHOOLS Department of Special Education
LEVEL 2 Vocational Assessment Form
Student: ____________________________________________________ Date of Birth _______________ Date __________________________ School ___________________ Teacher__________________________
Use this information to complete the IEP (Present levels and needs statements, transition page, goals/objectives) Source: VESID Transition Toolbox 12/2005
Teacher Version Post Secondary Education/Training: After he/she graduates from high school, what type of further education/training do you see him/her pursuing? (e.g., 2 or 4 year college, trade school, apprenticeship programs, supported employment, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ If he/she is interested in college, do you know what is needed to apply for the school of his/her choice? (for example, grade point average, community service, etc.) __ Yes __ No Abilities: What are the student’s talents and skills that will help him/her in school? ______________________________________________________________________________________________________________________________________________________________ _______________________________________________________________________________ Needs: Think about school and his/her career choices. What skills does he/she need to develop at this time to be a successful student? (for example, homework, study skills, organizational skills, chores, etc.) _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Fears/Behaviors: What might stand in the way of reaching his/her dreams? (for example, attitude, behavior, etc.) __________________________________________________________ _______________________________________________________________________________ ______________________________________________________________________________________________________________________________________________________________ What can the school provide to support the student’s needs this year? (e.g., career zone website, classroom interventions, presentations, site visits, etc.) _______________________________________________________________________________ _______________________________________________________________________________ What does he/she like to do during free time?________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________ Favorite Subject:________________________________________________________________ What does he/she dislike?________________________________________________________ _______________________________________________________________________________ Comments: _______________________________________________________________________________ _______________________________________________________________________________ _______________________________________________________________________________

LEVEL 2 Vocational Assessment Form
Student: ____________________________________________________ Date of Birth _______________
6
TRANSITION QUESTIONNAIRES SUMMARY FORM
Directions: Using the student, parent and teacher’s questionnaires, list the number identified for each item in the corresponding column. This information should be used as a reference to complete the IEP (Present Levels and Needs Statements, Transition Page and the Goals/Objectives).
Area Student Results Parent Results Teacher Results Action
Needed? Employment/Training 1 Knows job requirements 2 Can choose job based on interest/abilities
3 Understands how to get a job
4 Good attitude and habits Education/Training 5 Likes to work with hands 6 Likes jobs requiring reading and writing
7 Prefers working with other people
Daily Living 8 Able to live independently 9 Can take care of money Community Participation 10 Can participate in leisure activities
11 Knows how to use community resources
Self-Awareness/Advocacy 12 Knows and can explain strengths and needs
13 Expresses feelings and ideas appropriately
14 Can explain medical needs 15 Can set goals 16 Can accept/follow directions Getting Along with Others
17 Gets along with friends
18 Gets along with teachers/ other adults in school




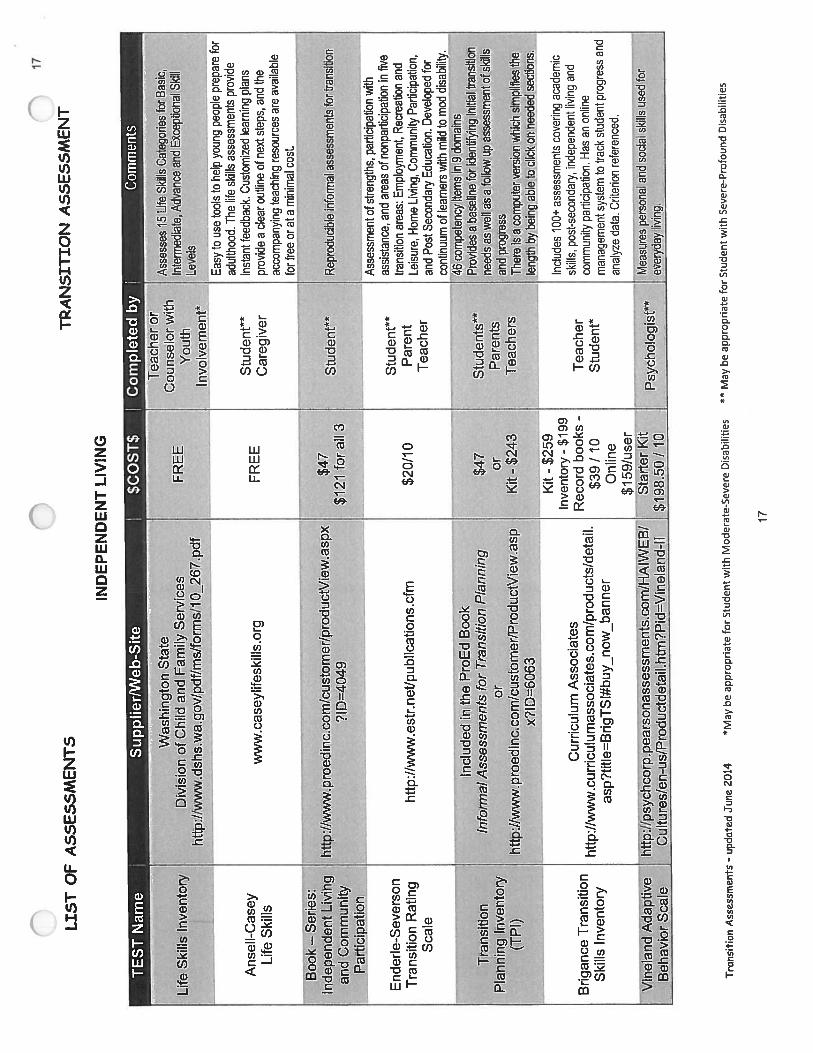

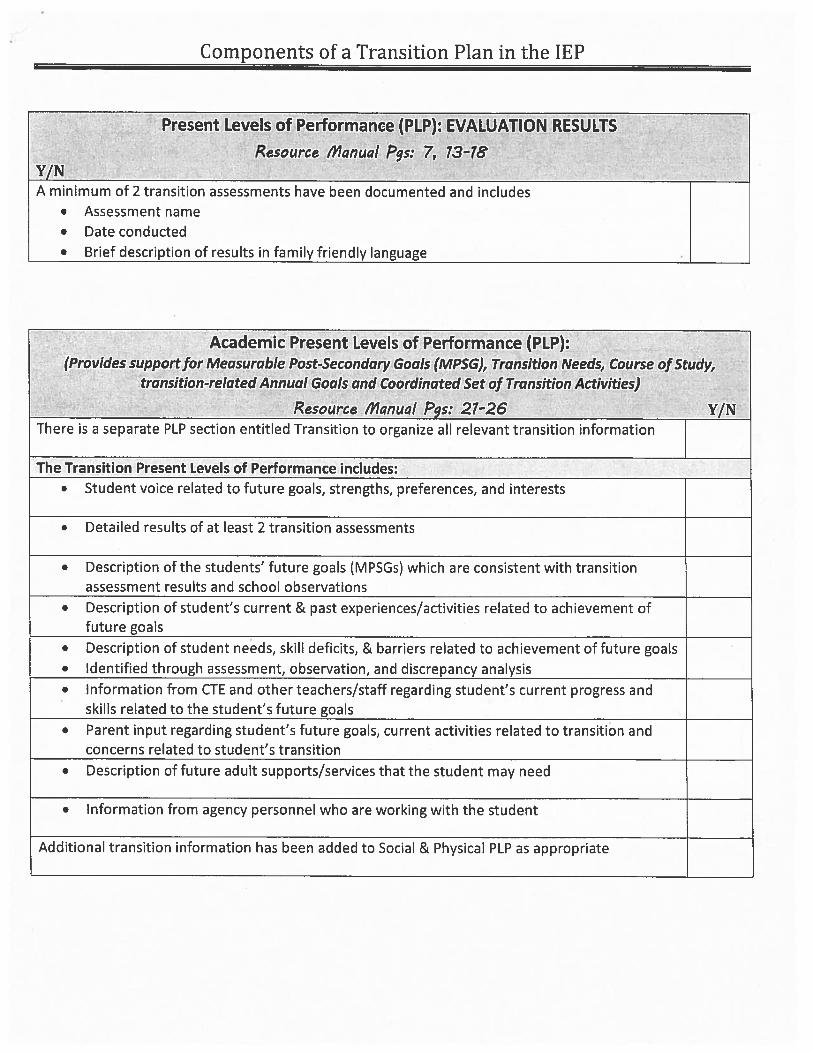
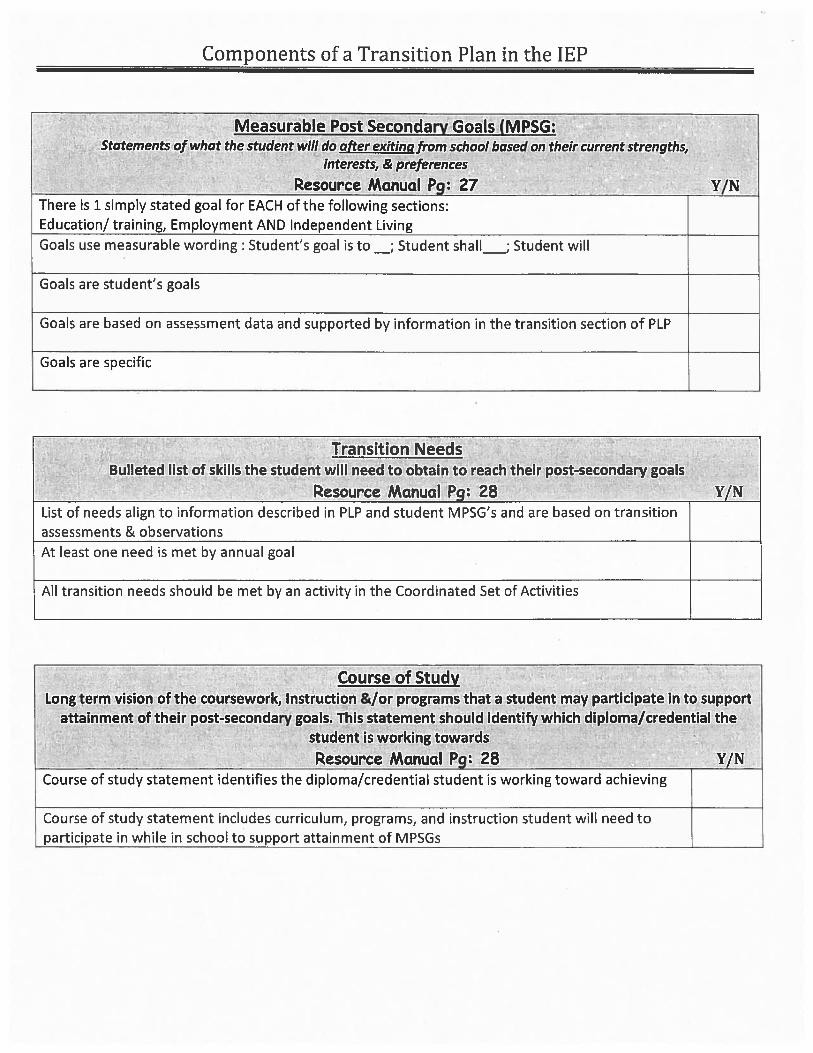

Edited 4/17/13
Transition Planning Completion of a Level I Assessment is required beginning at age 12. The results of this assessment are to be included in the Academic Present Levels area of the IEP. Transition planning is required for students with disabilities, beginning at age 15 (or turning 15 during the implementation period of the IEP). Information needs to include coordinated set of transition activities and post secondary measurable goals which will reasonably enable students to meet their post-secondary goals for living, further education, and employment. Transition planning and services must also be integrated into the PLEP (Career/Vocation/Transition). See below. Measurable Post-Secondary Goals and Transition Needs - to be in effect when the student is age 15 (and at a younger age, if appropriate), document the long term goals for living, working and learning as an adult. In addition, the IEP for these students must include a statement of the transition service needs of the student that focuses on the student's courses of study, taking into account the student's strengths, preferences and interests as they relate from school to post-school activities.
Education/Training Employment Independent Living Skills (when appropriate) Transition Needs Courses Of Study
Coordinated Set of Transition Activities (School To Post School) - Beginning not later than the first IEP to be in effect when the student is age 15 (and at a younger age, if determined appropriate).
Instruction Service/Activity Date School District/Agency Responsible Related Services Service/Activity Date School District/Agency Responsible Community Experiences Service/Activity Date School District/Agency Responsible Development of Employment and Other Post-school Adult Living Objectives Service/Activity Date School District/Agency Responsible Acquisition of Daily Living Skills (if applicable) Service/Activity Date School District/Agency Responsible Functional Vocational Assessment (if applicable) Service/Activity Date
School District/Agency Responsible

Related Services Contact should be made with the Central Committee on Special Education Director, Nina Blumlein, via email at [email protected] for concerns or information regarding: Occupational Therapy, Physical Therapy, Psychological Counseling, Vision Services, Assistive Technology, Speech and Language or Hearing Services and Student Equipment. Whether BPS personnel deliver related services to your school or your charter school has independent related services providers, all related service evaluations must be processed through the Central CSE staff, even if Buffalo staff does not provide the service. All related service reports and/or summary updates need to be sent to the Central CSE prior to the scheduled meeting. Provide this information two weeks prior to the CSE meeting. When requesting Occupational Therapy, Physical Therapy, Psychological Counseling services or Assistive Technology services for the first time, it is necessary to complete the Occupational Therapy Screening Referral Form and Documentation of Interventions Implemented, or Physical Therapy Referral Form and Documentation of Interventions Implemented, or, Assistive Technology Evaluation Referral Form or referral for Counseling Evaluation. This form must be submitted with a Request for a Committee on Special Education Meeting (Reevaluation) or Request for a Committee on Special Education Referral (Initial).
BUFFALO PHYSICAL THERAPY DEPARTMENT DATA SUMMARY
School Year_____________________ AR Reevaluation Student ID# Name DOB CA School Grade Present Level of Service per cycle Minutes/Session Ind. Group Progress Towards Goals:
Present Levels: Rationale/Need for Service Recommendation: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
M,C,T Related Service
TORC # of sessions
Minutes/ Session
I or G Start Date
Reason for non-participation in general education setting
Recommendation for Health Related Support Services Indicated on Student Individual Education Program. I recommend that Occupational Therapy Services indicated for this student are in accordance with the frequency, duration and cycle as indicated on the Individualized Education Program (IEP). Signature Date Signature Date

BUFFALO COUNSELING DEPARTMENT DATA SUMMARY
School Year____________________ AR Reevaluation Student ID# Name DOB CA School Grade Present Level of Service per cycle Minutes/Session Ind. Group Progress Towards Goals: Present Levels: Rationale/Need for Service Recommendation: M=Modify C = Continue T = Terminate M,C,T Related
Service Location Spec or Gen Ed
# of sessions
Minutes/ Session
I or G Start Date
Reason for non-participation in general education setting
Recommendation for Health Related Support Services Indicated on Student Individual Education Program. I recommend that Counseling indicated for this student are in accordance with the frequency, duration and cycle as indicated on the Individualized Education Program (IEP). NYS Certified Counselor Date

BUFFALO VISION DEPARTMENT DATA SUMMARY
School Year____________________ AR Reevaluation Student ID# Name DOB CA School Grade Present Level of Service per cycle Minutes/Session Ind. Group Progress Towards Goals: Present Levels: Rationale/Need for Service Recommendation: M=Modify C = Continue T = Terminate M,C,T Related
Service Location Spec or Gen Ed
# of sessions
Minutes/ Session
I or G Start Date
Reason for non-participation in general education setting
Recommendation for Health Related Support Services Indicated on Student Individual Education Program. I recommend that Counseling indicated for this student are in accordance with the frequency, duration and cycle as indicated on the Individualized Education Program (IEP). NYS Certified Counselor Date

01/2012
Buffalo Public Schools Department of Hearing Impaired/Deaf
Summary Report
AR Reevaluation Meeting Date: Student ID # Name: DOB CA School Grade
Classification HI Primary RS Hearing Acuity: Unaided Aided Description of Loss Mode of Communication: Sign Language Only Total Communication Oral Communication Progress Towards Goals: Present Levels: Rationale/Need for Service Recommendation:
Goals:
M,C,T, Status TORC Ratio Frequency Period Duration Start Date Reason for non-participation in a general education setting
Teacher of the Deaf/ Hearing Handicapped Date
BPS Speech-Language DepartmentSpeech-Language Summary Report
5/9/20132:51 PM
AR Reevaluation Ammend Student Id #:
Name: DOB CA School GR SI RS
Present Level of Service: per cycle Minutes/Session Ind Group
Ratio Duration
Date:TSHH
Date:
6 day cycle
I recommend this student receive Speech-Language Therapy in accordance with the frequency, duration and cycle as indicated below.
NYS Licensed Speech-Language Pathologist
Speech/Language Therapy
School
Location ICD-9
Prescription/Recommendation for Health Related Support Services:
PeriodRelated Service
Signature License #
Signature
End Date
Functional Performance and Learning Characteristics- Present Levels (PLEP):
Developmental and functional needs of the student for speech service:
Frequency Start Date
Progress in Therapy for 2012-2013:
Rev: 1/31/13
Phone #Address:

OCCUPATIONAL THERAPY SCREENING REFERRAL FORM AND
DOCUMENTATION OF INTERVENTIONS IMPLEMENTED
Check areas which apply to the student who you are referring: Performance Components
Gross Motor Skills Seems weaker than others his/her age, tires easily Difficulty with hopping, jumping, skipping, or running compared to classmates Appears stiff or awkward in his/her movements Clumsy, bumps into things, falls out of his/her chair Reluctant to participate in sports and group physical activities Poor desk posture (slumps, leans on arms, holds face too close to work)
Fine Motor Skills Difficulty with drawing, coloring, copying, cutting or avoidance of these activities Poor pencil grasp, drops pencil frequently or holds pencil too tightly Lines drawn are tight, wobbly, too faint, too dark, or breaks pencil often Lacks well established dominance after six years of age/laterality
Regulation of Sensory Systems Reacts negatively to touch or seeks out excessive contact (laying on others) Tends to wear coat when not needed; will not allow long sleeves to be pulled up Has trouble keeping hands to self, will poke or push other children Apt to touch everything he/she sees, seems to learn through touching Dislikes being cuddled or hugged Student scratches and rubs skin often Vestibular Sensation Fearful of activities involving moving through space ex. Swinging or gym games Observed poor balance or avoids activities that challenge balance Excessive craving for swinging, bouncing, sliding, merry-go-rounds or rocking School aide/teacher reports child to be easily carsick/bus sick History of frequent inner ear infections Apt to be impulsive, heedless, accident prone Distracted by background noise or internal thoughts/impulses
Visual Motor Integration/Visual Perception Difficulty discriminating colors, shapes, completing puzzles Letter reversals after first grade Difficulty in visual-tracking (difficulty following objects with eyes) Difficulty in copying designs, numbers or letters Difficulty imitating gestures/movements Poor organization of written work
Social/Emotional Does not accept changes in routine easily Becomes easily frustrated; gives up easily Acts out behaviorally, difficulty getting along with others Easier to handle in small groups or individually Marked mood variations, outbursts, or tantrums Frequently out of seat
Name: DOB: School: Teacher: Grade: Pupil Service Center: ID#: Health concerns: Medication: Special Alerts:

OCCUPATIONAL THERAPY SCREENING REFERRAL FORM AND
DOCUMENTATION OF INTERVENTIONS IMPLEMENTED
Please complete and return to Related Services Office – School 12 - 33 Ash Street – Buffalo, NY 14204 Page 2 of 2
Student’s Name: Date of Birth:
Specifically document strategies/interventions tried to alleviate problems/concerns listed above. Specify date, length and type of intervention: List specific educational objectives to be met by Occupational Therapist:

PHYSICAL THERAPY REFERRAL FORM AND
DOCUMENTATION OF INTERVENTIONS IMPLEMENTED
Please complete and return to Related Services Office – School 12 - 33 Ash Street – Buffalo, NY 14204 Page 1 of 2
Name: DOB:
School: Teacher: Grade:
Pupil Service Center: ID#:
Health concerns:
Special alerts and environmental restrictions:
Medication:
Indications for use:
Below are areas of concern in the domain of physical therapy:
FUNCTIONAL MOBILITY
Difficulty getting on and off school bus safely Difficulty walking on uneven surfaces and negotiating curbs Difficulty negotiating stairs Difficulty keeping up with class in the hallways, trips?, falls? Difficulty keeping up with peers on field trips Difficulty efficiently exiting during fire drill
GROSS MOTOR SKILLS
Seems weaker than others his/her age, tires easily Appears short of breath after minimal exertion Appears stiff or awkward in his/her movements Clumsy, bumps into things, falls out of his/her chair Difficulty with hopping, jumping, skipping, running, using playground equipment
MOVEMENT OBSERVATIONS
Difficulty following directions for gross motor activities Movements in impulsive, careless Lacks safety awareness Reluctant to participate in sports and group physical activities

PHYSICAL THERAPY REFERRAL FORM AND
DOCUMENTATION OF INTERVENTIONS IMPLEMENTED
Please complete and return to Related Services Office – School 12 - 33 Ash Street – Buffalo, NY 14204 Page 2 of 2
Student’s Name: Date of Birth:
Specifically document strategies/interventions tried to alleviate problems/concerns listed above. Specify date, length and type of intervention: List specific educational objectives to be met by Physical Therapist:

Buffalo Public Schools Referral for Counseling Evaluation
Please complete all sections:
Student’s Name: Date of request: Student ID #: Date of Birth: Teacher: School:
1) List specific behaviors or concerns that indicate a need for counseling:
2) Specifically document strategies/interventions tried to alleviate problems/concerns listed above. Specify date, length and type of intervention:
3) List specific educational objectives to be met by counseling:

Buffalo Board of Education Assistive Technology Service
462 Grider Street Buffalo, New York 14215
(716) 816-4080 ext. 1137, FAX (716) 897-8081
5/7/2013 1 | P a g e
Assistive Technology Evaluation Referral Form
Student Name: DOB: Age: School: Grade:
School Contact Person: Telephone: Person Completing Form Date Completed
Parent(s)/Guardian’s Names: Parent/Guardian Telephone#: Student’s Primary Language: Family Primary Language:
Disability (Check all that apply) Speech/Language PDD – ASD Cognitive Disability Other Health Impairment Emotional/Behavioral Disability Specify Orthopedic Impairment Specific Learning Disability
Type Health Impairment Vision Impairment Specify
Specify Traumatic Brain Injury Classroom Setting
Regular Educational Classroom Self - Contained Consultant Teacher Services Specify
Specify Other Home Instruction Specify
Current Service Providers Speech Language Hearing Services Physical Therapy Mobility Services Vision Services Other Occupational Therapy Specify
Medical Considerations (Check all that apply) History of Seizures Fatigues easily Has degenerative medical condition Has frequent pain
Specify Has frequent upper respiratory infections Has frequent ear infections Has allergies to: Has multiple health problems Specify
Specify Has digestive problems Currently taking medication for Other
Specify Specify Other Concerns:
Assistive Technology Currently In Place (Check all that apply) None Low Tech Writing Aid(s)

5/7/2013 2 | P a g e
Communication Boards(s) Dedicate Communication Device Low Tech/Visual Aids Specify Environmental Control Unit Amplification system Power Wheelchair Manual Wheelchair Switches Portable Word Processor
Specify Computer Other: Type (Platform)
Specify Word Prediction What do you feel are the student’s major assets?
Fine Motor Skills Uses both hands Uses one hand Uses fingers right left
Specify Hand dominance right left
Assistive Technology Justification: What OUTCOMES do you expect from the assistive technology evaluation to improve performance in these targeted areas? Who would be in charge of implementing and maintaining assistive technology recommendations? Teacher(s):

Response To Intervention This must be completed PRIOR to requesting an Assistive Technology Evaluation THIS WILL BE RETURNED TO YOU IF YOU DO NOT COLLECT DATA FOR 12 WEEKS
What’s expected of a student at this age/grade level? What are his peers
doing? (I.e. write two sentences, write a three paragraph report? Add,
subtract single digits, carry on a conversation, etc.)
How is the student achieving grade level
expectation for the area of concern? SPECIFY
Baseline Measurement (i.e., Teacher observation, Tally,
etc.) BE SPECIFIC
Intervention/Accommodation - modification tried. (Be Specific) (See Tools and
Strategies to use BEFORE requesting an AT
Evaluation)
Dates of interventions. Weeks 1 thru 6 (must be 6
weeks) Reading
Writing
Math
Communication
Other
Response To Intervention This must be completed PRIOR to requesting an Assistive Technology Evaluation THIS WILL BE RETURNED TO YOU IF YOU DO NOT COLLECT DATA FOR 12 WEEKS
Progress/Data for Weeks 1 thru 6 (Did it work? If not
why didn’t it work?)
If no progress during first 6 weeks, describe the modification-
accommodation tried during Weeks 7 thru 12. (use additional paper if
necessary)
Dates of interventions. Weeks 7 thru
12 (must be 12 weeks total)
Progress/Data for weeks 7 through 12 (Did it work? If not, why didn’t it work) BE SPECIFIC Additional Comments

Tools and Strategies to use BEFORE requesting an Assistive Technology Evaluation
Begin with No Tech and move through to High Tech. DON’T begin with High Tech.
Classroom Management and Environment
• Student planner- personal calendar and notebook for student to keep records of events, assignments, important dates, etc.
Low Tech
• Visual schedule- order of student turn-taking, daily schedule, order of tasks
• Check lists- “Did I…?” or “TO DO… “ lists which students check as they go
• Prompt cards- to illustrate the steps required to complete a task, including materials needed
• Environmental labels- using pictures, words, photos, or symbols to designate where items belong in the class
• Basket/bins- use bin or baskets for work “to do” and work “done” clearly defined
Comprehending, Composing, and Organizing
Learning: No Tech
• finger tapping- syllabification • Provide extensive preview of material • Multi modal presentation-use as many inputs as possible
(visual, auditory, tactile) • Visualization-teach imagery • Connect information- overtly note the link to previously
mastered knowledge
Materials: Low Tech
• Notebook- a specific location to record key points • Exemplars/models- post examples of completed
assignments, noting scores awarded • Materials list- personal or class list of items needed to
complete task Organizing time or space:
• Color coded template: assign specific colors to parts of speech for sentences or other grammatical sequences
• Highlight- main ideas or other key information (character, setting, problem).
• tab/flag: designate main ideas or other key information • Index cards: segment component of a paragraph or story so
they may be physically manipulated. Learning:
• Word dice • Personal materials: student is given a personal version of
class materials, to increase focus, customize it to their needs. • Pictures: photos, pictures with words to convey ideas and
promote recall of information.
• Word wall • Story Grammar Marker: to preview/review story narrative and
support reading of text • Word rings: laminated vocabulary cards or sentence strips
hooked on to large metal book rings • Word Windows: bind together sequences of letter cards and
word windows- student flip cards • Story starters • Word games
• Personal recorder: small hand held for students to record their homework assignments
Mid Tech
• Hand held talking dictionary/speller
• Power point slide show” create slides of words for word identification
High Tech
• Inspiration/Kidspiration- provides a variety of formats for visually representing, organizing, recording, and relating ideas and concepts
Mechanics of Writing/Drawing
• Allow more time to complete assignments No Tech
• Reduce quantity of final product • Explore different forms of writing (print versus cursive) • Model writing first: teacher/peer/aide writes the word to show
the student how to form letters • Use “fill in the blank” answer format • Modify worksheets- simplify; make templates for student to
complete • Use multiple choice format • Support spelling skills through use of word searchers and
crossword puzzles • Warm up exercises: for hands/arms prior to writing
• Word walls: reinforce frequently used words and topic/story vocabulary
Low Tech
• Word rings • Spelling journals • Vertical/slant surfaces can support access, especially for
young children • Slant board or notebook turned sideways sloping toward
student • Easel • Little blackboard, chalkboard or write on/wipe off board • Felt board • Handwriting instructional booklets: Beginning Connected
cursive writing… • Tactile letters: “writing” letters in sand, finger paints, puff
paints, glitter • Magnetic alphabet board • Scrabble letters or tiles
• Dot to dot letters • Pencil grips: stabilizes grip on pen or pencil (See OT) • Adapted pencils • Nitewriter lighted pen: supports visual tracking while writing • Shift position of paper • Enhanced lined paper(see OT) • Plastic writing guides • Finger grip ruler: keeps fingers out of way while drawing a line
• Voice recorder: record homework assignments, Mid Tech
• All-turn-it-spinner: story parts can be written on a wheel and randomly selected by student
• Hand held talking dictionary/speller • Language Master
Mathematics
• Minimize number of items on page No Tech
• Eliminate need to copy problems- have student record answers only when possible
• Avoid mixing signs – to avoid confusion • Provide additional time • Peer/adult support • Cross age tutoring • Mental arithmetic- if writing presents barrier have student
narrate math process • Finger math • Mnemonic devices • Multimodal instruction
• Modified paper: bold line, raised, assorted graph, enlarged graph (see OT)
Low Tech
• Rubber stamps • Finger pinch ruler • Math matrix: charts/tables; number fact sheets 100’s… • Mathline: tangible number rod with gliding markers • Number lines: raised, large, tactile, life size, used to show
size… • Computational aides: abacus, counters, manipulatives,
beads, base ten blocks… • Enlarge worksheets/print • Highlighter tape • Tangrams: Chinese, manipulative piece puzzles
• Calculators Mid Tech
• Tape recorder: • Automatic number stamp • Coin-u-lator
• Any Mac or Windows based Math Software program High Tech

Edited 4/17/13
Post-Secondary Exit Summary For students who are graduating, aging out, or leaving school, a Post-Secondary Exit Summary will need to be completed and reviewed with the student and parent prior to the end of the school year. Directions for completing this task using IEP Direct:
• In IEP Direct click on the student name. Under State Forms, click on Post Secondary Exit Summary.
• Click on Import and the Academic, Social and Physical PLEP statements will populate the exit summary. These statements can be edited, as needed.
• Complete the School contact name, title, phone number, graduation date, and diploma type fields and Save.
• Send Invite letters to student and parent (Student Invite for Summary Exit) and (Parent Invite for Summary Exit) for your scheduled exit planning meeting.
• Conduct exit summary meeting. • When the Post-Secondary Exit Summary is accurate, it can be printed by going to
Letters/Reports and putting a check mark in front of the CSE Report-Post-Secondary Student Exit Summary, Process and Print.
• Send exit summary report to the student’s family, and to the Central CSE (along with any supporting documents; i.e.: copy of invitation letters, attendance sheet) for the student’s file.

BUFFALO PUBLIC SCHOOLS Student Invitation for Exit Summary
Date: __________________
__________________ __________________ __________________ DOB: _______________ Dear _____________________: A meeting is scheduled to review your transition plan and to develop a summary document of academic and functional performance. If you require an interpreter, translator, reader, a location that is physically accessible, or any other special accommodations, please contact me prior to the scheduled meeting in order to make the appropriate arrangements. The meeting is scheduled for: Date: __________________ Place: ____________________
Time: __________________ Purpose: Exit Summary Meeting The people attending the meeting will be: .______________________________________ We hope that you will make every effort to attend. If you are unable to attend the meeting, at your request, we will arrange to participate by individual or conference calls. We will also discuss and help plan your transition from high school to adult life. If you have any questions or concerns, please do not hesitate to call. Sincerely, __________________
“Putting children and families first to ensure high academic achievement for all”

BUFFALO PUBLIC SCHOOLS Parent Invitation for Student Exit Summary
Date: ____________________
______________________ ______________________ ______________________ Re: ___________________ DOB: ________________ Dear ________________________ A meeting is scheduled to review your child’s transition plan and to develop a summary document of academic and functional performance. If you require an interpreter, translator, reader, a location that is physically accessible, or any other special accommodations, please contact me prior to the scheduled meeting in order to make the appropriate arrangements. The meeting is scheduled for: Date: ___________________ Place: ___________________________
Time: _______________________
Purpose: Exit Summary Meeting
The people attending the meeting will be: ______________________________________ We hope that you will make every effort to attend. If you are unable to attend the meeting, at your request, we will arrange to participate by individual or conference calls. We will also discuss and help plan your child’s transition from high school to adult life. If you have any questions or concerns, please do not hesitate to call. Sincerely, _____________________ _____________________
“Putting children and families first to ensure high academic achievement for all”
Edited 4/17/13
Additional Responsibilities Ensure a meeting location is available in your school, on the date of the CSE meeting. Ensure the expected attendees have been informed about the date, time, and location of the CSE meeting. Ensure all meeting attendees should be prepared to discuss and contribute to the development of the IEP. AT MINIMUM, THE GENERAL EDUCATION TEACHER AND THE SPECIAL EDUCATION TEACHER OF THE STUDENT ARE REQUIRED TO BE IN ATTENDANCE. ONLY THE PARTIES INDICATED ON THE INVITATION LETTER MAY BE INCLUDED IN THE MEETING, UNLESS INVITED AT THE REQUEST OF THE PARENT. If a change in the recommended level of service to a less restrictive setting/service is warranted, complete the request for a Committee on Special Education Meeting form (Amendment and rationale page) and return to your assigned chairperson. Ensure 408 Implementation procedures/requirements are followed. Ensure Progress Reports are completed and provided to parents at the intervals designated on the IEP. This includes progress reporting of a Behavioral Intervention Plan (BIP), as applicable (BIP progress reports are to be submitted to Central CSE, in addition to the parents, as they are not available for the CSE to collect through IEPDirect).

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 1 (716) 816-4746 • Fax (716) 816-3974 Revised 5/01/13
ANNUAL REVIEW
Notification of Annual Review Meetings
Annual Review meetings will be scheduled to be held on or before the annual review by date, as indicated under the “Committee Recommendations” section of the IEP. Case Managers will be notified via e-mail of scheduled annual review meetings. Please ensure that this information is disseminated to appropriate staff expeditiously. This includes the general education teacher(s), special education teacher(s), and related service providers, as applicable.
• Provide a list of service provider(s) for each student with disabilities in your building to the chairperson so that parents receive notification of anticipated attendance on the meeting invitation letter
Preparing for Annual Review
To ensure compliance with regulations, and that the annual review meeting runs smoothly and efficiently, please:
• Notify appropriate staff of the meeting, and the availability of the draft for editing/updating in a timely fashion
• Ensure the availability of meeting space, and coverage for staff members to be in attendance*
• Ensure that students who will be 14 years during the implementation period of the document (or younger, as appropriate) are released from class and encouraged to attend the meeting
• Ensure that all necessary documents are available for discussion the day of the meeting, i.e., as applicable; all related service progress summary reports, behavior intervention plan, Level 1 Transition Assessment, etc., (please have these documents at the table on the day of the meeting; it is not necessary to fax this documentation to the annual review chairperson before the annual review meeting).
*Note: At minimum, the general education teacher and special education teacher of the student are required to be in attendance. Only the parties indicated on the invitation letter may be included in the meeting, unless invited at the request of the parent.
• It is recommended that teachers be encouraged to review the NYS “Guide to Quality Individualized Education Program (IEP) Development and Implementation” for information on developing/writing a quality IEP that is reasonably calculated to allow educational benefit for students. If you do not have this document, please contact the Annual Review Chairperson, and it will be forwarded to you
Completing the Annual Review Draft

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 2 (716) 816-4746 • Fax (716) 816-3974 Revised 5/01/13
via e-mail. Another resource is the “Overview” section of the “Guide to Completing the IEP Planning Sheet”. Teachers are not required to submit the “Student Intervention Record” or “IEP Planning Sheets” for Annual Review.
• Teachers should complete the majority o0f the items in the draft in preparation for the meeting, including: Special Alerts, the Academic Achievement, Social Development, and Physical Development present levels, strengths, and needs areas; Management Needs; Students Needs Related to Special Factors; Measurable Post Secondary Goals (if student is or will be 15 years or older during implementation period of the IEP ); Measurable Annual Goals; Programs; Related Services; Supplementary Aids and Services; Assistive Technology (deleting technology no longer required or updating dates of technology is continuing); Supports for School Personnel on behalf of the Student (consultation services); Test Accommodations; and Coordinating Sets of Transition Activities (if student is or will be 15 years or older during implementation period of the IEP). Ensuring that these areas of the IEP have been drafted prior to the meeting helps to support the ability to finalize the documents promptly, allowing timely 408 Implementation.
• Teachers should not edit the following sections: “Committee Meeting or Agreement Information”, “Committee Recommendations”, “Effect of Student Needs”, “Participation in Assessments”, “Participation with Students without Disabilities”, and “Special Transportation” areas of the IEP.
• An additional area that is recommended to be edited by teachers is the “Statewide and District Wide Assessments” section. Student scores on State ELA & Math assessments, Terra Nova, NYSESLAT, and Regents and/or RCT exams can be entered in this area.
• Start and End Dates on the IEP should reflect the date of the meeting, and one year from the meeting date (i.e., if the meeting is scheduled September 10th, the start date will be 9/10/13 and the end date will be 9/10/14).
• Beginning at age 12, a Level 1 Transition Assessment is required to be completed. The information obtained through this assessment is to be included in the Academic Present Levels Statements. Each subsequent year, this information is to be reviewed & updated. If the student will be 15 years during the implementation period of the document, 2 additional fields must be opened and completed, “Measurable Postsecondary Goals and Transition Needs” and “Coordinated Set of Transition Activities (School to Post-School)”.
• There should be alignment throughout the IEP. The present levels and needs statements are the foundation from which the IEP is built. There should be detailed information regarding the effect of the disability on the student’s access, participation, and progress in the general curriculum. This includes the strategies, modifications, and accommodations the student requires in order to access, participate, and progress in the general curriculum.

Buffalo Public Schools Central Committee on Special Education Dr. Pamela C. Brown Will Keresztes Superintendent Associate Superintendent for Educational Services Kim Curtin Director of Special Education
33 Ash Street, Buffalo, New York 14204 3 (716) 816-4746 • Fax (716) 816-3974 Revised 5/01/13
• At the annual review it is expected that the progress the student has made toward the goals of the previous IEP will be reviewed/discussed. It is recommended that teachers be prepared to review and discuss data that has been collected during the implementation period of the IEP, as it pertains to targeted goals. Information regarding student progress toward pervious goals should be included in the present levels statement. If recommending a continuation of a goal, the present levels statements should include information regarding the barriers to achieving the goal/ goals, and what instructional strategies/practices/interventions will be employed to ensure the student will be able to meet the targeted goal.
Measurable Annual Goals and the Annual Review Meeting
• Annual Goals must be “skilled-based”, and must align with the needs statements. They are not curriculum goals.
• Annual Goals must be measurable.
• The “Schedule” of the measurable annual goals section indicates how often data will be collected to track student progress, not how often progress will be reported. “Quarterly” is not an appropriate recommendation for tracking progress toward goals. At minimum it would be expected that there would be a monthly tracking schedule in order to have 2 pieces of data to review at the end of a quarter and evaluate progress.
• Change of Classification
Changes that are Not Allowable at an Annual Review
The following are examples of changes to an existing IEP that are not allowable at an annual review meeting:
• Change to a More Restrictive Setting
• Completion of a Functional Behavioral Assessment
• Adding a Related Service (an evaluation is required)
• Adding Assistive Technology, such as computer access (an evaluation is required)
• Recommending a Second Language Exemption
• Changing to Alternate Assessment
• Adding Special Transportation
• Changing Diploma Status

Guide to Completing the IEP Planning Sheets
Overview
Academic Achievement, Functional Performance and Learning Characteristics
*Note: Select & add each skill area text box to enter information regarding present levels of performance. At minimum, Reading, Mathematics, and Written Language sections should be included. For students 12 years and older, the Career/Vocational/Transition section is also required. Present Levels of Performance Statements and Needs Statements should:
-Include information related to the student’s levels of knowledge and development in subject and skill areas, including activities of daily living, level of intellectual functioning, adaptive behavior, expected rate of progress in acquiring skills and information and learning style. -Student Strengths, Preferences, Interests - Academic, developmental and functional needs of the student, including consideration of student needs that are of concern to the parent.
Describe: • What the student can do (student’s current functioning) • How the student learns best (acquires skills and information). • What strategies work best to teach the student (i.e., what instructional supports
have been effective or not effective in addressing the need area in the past year) • What progress the student has made toward previous goals • What the student’s strengths and weaknesses are • (For students 12 years and older), student’s abilities and needs in relation to
desired school/post-school outcome. • Concerns of the parent Include: • evaluation/assessment data that is instructionally relevant, easily understood
(free of jargon), and provides baseline data from which to measure progress. • Input from multiple sources • statements of priority needs that can lead to measurable goals and objectives *note: - present level statements must contain a baseline statement to justify all program mods, test accommodations, assistive tech, and supports for school personnel on behalf of the student
Reading
: What is the student expected to be able to do according to the core curriculum standards? Include information which describes the student’s functioning/abilities/needs with regard to the pillars of reading (i.e., phonemic awareness/decoding skills, vocabulary, fluency, context clues, and comprehension (independent reading/ listening; literal/inferential).
Math: What is the student expected to be able to do according to the core curriculum standards? Include information which describes the student’s functioning/abilities/needs with regard to conceptual understanding (involves the understanding of mathematical ideas and procedures and includes the knowledge of basic arithmetic facts)., procedural fluency (the skill in carrying out procedures flexibly, accurately, efficiently, and appropriately), and problem solving (the ability to formulate, represent, and solve mathematical problems)..
Written Language
: What is the student expected to be able to do according to the core curriculum standards? Include information which describes the student’s functioning/abilities/needs with regard to, for example, word study, spelling, grammar and mechanics, speaking, written expression, (including expressing ideas, i.e., brainstorming/drafting), sentence structure, organization, paragraph development, editing, etc.
Study Skills
: (as applicable) Include information which describes the student’s functioning/abilities/needs with regard to, for example, attention to task (independent and teacher directed activities), organizational skills, assignment completion, learning behaviors/strategies, test preparation & performance, etc.
Career/Vocational/Transition
: (must be included in the academic present levels area for students 12 years and older) Include information obtained from the student and parent through completion of a Level 1 Transition Assessment.
_______________________________________________________________________
Social Development
Present Levels of Performance Statements should:
include information regarding the degree and quality of the student's: • relationships with peers and adults • feelings about self • and social adjustment to school and community environments.
Describe (in relation to the student’s relationships with peers and adults, feelings about self, and social adjustment): • What the student can do. • What the student’s strengths and weaknesses are. • The impact of student behavior on learning • How the student interacts with peers and adults • What strategies work best to teach the student (i.e., what behavioral supports
have been effective or not effective in addressing the need area in the past year). • What progress the student has made toward previous goals. • Concerns of the parent Include: • evaluation/assessment data that is instructionally relevant, easily understood
(free of jargon), and provides baseline data from which to measure progress (i.e., Counseling Evaluation or Summary Report; Functional Behavioral Assessment, Social History, etc).
• Input from multiple sources (i.e, Observations, Teacher Reports, Positive Behavioral support data, etc.).
• statements of priority needs that can lead to measurable goals and objectives

Physical Development
Present Levels of Performance Statements should: Include information regarding the degree (extent) and quality of the student's:
• motor and sensory development • health, • vitality, • and physical skills or limitations which pertain to the learning process
Describe (in relation to the degree and quality of the student’s motor & sensory development, health, vitality, physical skills and limitations): • What the student can do. • What the student’s strengths and weaknesses are. • What strategies work best to teach the student. • What progress the student has made toward previous goals. • Concerns of the parent Include: • evaluation/assessment data that is instructionally relevant, easily understood
(free of jargon), and provides baseline data from which to measure progress (i.e., Medical Records; Physical or Occupational Therapy Evaluations or Summary Reports, Social History, etc).
• Input from multiple sources (Observations, Teacher Reports, etc.). • statements of priority needs that can lead to measurable goals and objectives
Management Needs
List the nature (type) and degree (extent) to which:
• environmental modifications (i.e., consistency of routine; limited visual/auditory distractions; adaptive behavior)
• and human resources (i.e., assistance in locating classes and following schedules; assistance in note taking)
• or material resources are required to enable the student to benefit from instruction (i.e., instructional material in alternative formats).
**The Management Needs PLEP does not contain a recommendation of programs or services.
December 2011

IEP Planning Worksheets Student Name_______________ Grade__________ I.D.#______________________ Teacher_____________ Reading: Evaluation data and implications: _____________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student expected to be able to do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What can the student do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student having difficulty with? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ How does the Student learn best (what strategies/supports are effective) ? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ Strengths, preferences, concerns of parent:____________________________________________________ ______________________________________________________________________________________ What does the student need to be able to do to participate and progress in the general curriculum?________ ______________________________________________________________________________________ ______________________________________________________________________________________

Math
Evaluation data and implications: _____________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student expected to be able to do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What can the student do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student having difficulty with? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ How does the Student learn best (what strategies/supports are effective)? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ Strengths, preferences, concerns of parent:____________________________________________________ ______________________________________________________________________________________ What does the student need to be able to do to participate and progress in the general curriculum?________ ______________________________________________________________________________________ ______________________________________________________________________________________

Written Language
Evaluation data and implications: _____________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student expected to be able to do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What can the student do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student having difficulty with? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ How does the Student learn best (what strategies/supports are effective) ? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ Strengths, preferences, concerns of parent:____________________________________________________ ______________________________________________________________________________________ What does the student need to be able to do to participate and progress in the general curriculum?________ ______________________________________________________________________________________ ______________________________________________________________________________________

Study Skills
Evaluation data and implications: _____________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student expected to be able to do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What can the student do? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What is the student having difficulty with? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ How does the Student learn best (what strategies/supports are effective) ? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ Strengths, preferences, concerns of parent:____________________________________________________ ______________________________________________________________________________________ What does the student need to be able to do to participate and progress in the general curriculum?________ ______________________________________________________________________________________ ______________________________________________________________________________________

Career/Vocation/Transition
Evaluation data and implications (Results of Level 1 Transition Assessment): _____________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What are the student’s goals? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What are the parents’ goals for the student? What are their concerns (if any)? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What skills are required for the student to meet his/her transition goals? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What are the student’s strengths?___________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ What are the student’s transition needs? ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________

CHAPTER 408
IEP IMPLEMENTATION RESPONSIBILITY CHECKLIST
Student: ID#: 900 Date Developed: ___/___/___ DOB: ___/___/___ Designated Lead Special Education Teacher or Service Provider:
(If incorrect, please indicate the correct name and return to the Placement Office at School #12, 33 Ash Street, Buffalo NY 14204)
Please be advised that a copy of a student’s IEP must remain confidential in accordance with applicable federal and state regulations, including the confidentiality provisions of IDEA and FERPA (Family Education Rights and Privacy Act). These laws prohibit the further disclosing of this IEP or the information contained within it to any other person without the written consent of the student’s parent/guardian, except as otherwise authorized under IDEA and FERPA.
*Inform/Receive IEP Signature Date Informed/Received 1.
2.
3.
4.
5.
6.
7.
8.
*Inform Only Signature Date Informed 9.
10.
11.
12.
13.
14.
15.
*Inform means that as a teacher or service provider for this student, you are aware of your responsibilities with the implementation of this student’s IEP
___/___/___ Signature of CSE member completing form Date Revised 2008-CC