Embed Size (px)
Citation preview
April 17th, 2013
Assisted Living/Supportive
Housing/Adult Day Programs
for
Special Populations Final Report
Table of Contents
0. Preliminaries
1. Executive Summary
2. Current State
3. Recommendations
4. Implementation
5. Appendix – Future State
Assisted Living/Supportive
Housing/Adult Day Programs for
Special Populations Final Report
South West
0. Preliminaries
Assisted Living/Supportive
Housing/Adult Day
Programs for
Special Populations
Table of Contents
0. Preliminaries
1. Acknowledgements
2. Context
3. Project Overview
4. Project Timeline
1. Executive Summary
2. Current State
3. Recommendations
4. Implementation
5. Appendix
Assisted Living/Supportive
Housing/Adult Day Programs for
Special Populations
Final Report
South West
© 2013 All rights reserved
Acknowledgments
The assistance of the Executive Sponsors and Steering Committee Members in the creation of this report was appreciated:
Sue McCutcheon, Lead, Access to Care
Executive Sponsors
Andria Appeldoorn, Access to Care Elaine Kerr, Participation Lodge Anita Cole, South West CCAC Michael Robbins, Segue Brian Dunne, Participation House Janine Hamilton, Spruce Lodge Michele Pegg, Co-lead Bruce Rankin, John Gordon Home Julie Girard, South West LHIN Nupee Hardeep Sadra, South West CCAC Carol Weigel, Grey Bruce Home and Community Support Services Kathy Scanlon, One Care Support
Assisted Living/Supportive Housing/Adult Day Programs Steering Committee Members
Sue Hillis, Co-Chair Assisted Living/Supportive Housing/Adult Day Programs Gord Milak, Co-Chair Assisted Living/Supportive Housing/Adult Day Programs
Rebecca McKee, South West LHIN Cate Melito, Woodstock Community Health Centre Kristy McQueen, VON Rose Wilson, Red Cross Christine Vallis, VON Linda Dunn, MHA Craig Hennessy, South West CCAC Lisa Gardner, AH Carolyn Ridley, South West LHIN Margo Collver, Co-Lead Magdalen Carter, Alzheimer Outreach Vicky Heard, West Elgin Community Health Centre Amber Alpaugh-Bishop, Access to Care
Mary Jo Dunlop, Project Co-lead Shirley Koch, Project Co-lead
Arminda Dumpierrez, OPTIMUS | SBR Nas Farzan, OPTIMUS | SBR Greg Harrington, OPTIMUS | SBR
Report Authors
5
© 2013 All rights reserved
Context
This project is part of an ongoing strategic effort to improve Access to Care in the South West LHIN, with a focus on Special Populations – adults with complex needs
Access to Care – Is an approach to care focused on supporting people, specifically seniors and adults with complex needs, to live safely in their homes for as long as possible. Access to Care empowers clients to participate in their own care and ensures that they get the right care at the right time and place. It calls for collaboration and integration across the health system. Note: In the South West LHIN there are three streams of work supporting Access to Care: Home First, Complex Continuing Care and Rehabilitation (CCC/Rehab), and Assisted Living, Supportive Housing, and Adult Day Programs (Assisted Living/Supportive Housing/Adult Day Programs).
Assisted Living/Supportive Housing/Adult Day Programs (AL/SH/ADP) – Is focused on realigning and enhancing community capacity in assisted living, supportive housing and adult day programs so that more LHIN residents are able to live safely and comfortably in the community. Instead of requiring that individuals research and compare available services on their own, a CCAC Care Coordinator will act as the client’s personal navigator of the healthcare system, providing patients with coordinated access to local services. This change supports some of the major goals of the government’s Excellent Care For All strategy – to reduce unnecessary hospital visits and increase the quality of each client’s care experience. Special Populations – Is a part of the Assisted Living/Supportive Housing/Adult Day Programs stream focused on populations living with Physical Disabilities, Acquired Brain Injuries or HIV/AIDS. Youth transitioning to adults who
are Medically Fragile/Technology Dependent (MFTD) were also within scope.
6
© 2013 All rights reserved
Project
Mission
Project
Success
Project Overview
Improve Access to Care through:
Alignment of Assisted Living/Supportive Housing/Adult Day Programs services for Specialized Populations on the basis of current need and projected demand (with a particular focus on populations with the greatest need)
Greater understanding of the current utilization of and demand for Assisted
Living/Supportive Housing/Adult Day Programs services for Special Populations across the South West LHIN
Recommendations that support access to the most appropriate service by Special Population type, including a costing model
Recommendations that support the CCAC’s Expanded Role for coordinated access – including appropriate eligibility criteria for each Special Population group requiring Assisted Living/Supportive Housing/Adult Day Programs services, as applicable
Clearer perspective on the current processes for admitting Specialized Populations to access and receive Assisted Living/Supportive Housing/Adult Day Programs services
Engaged Stakeholders who understand and support the proposed changes
7
© 2013 All rights reserved
Steering Committee
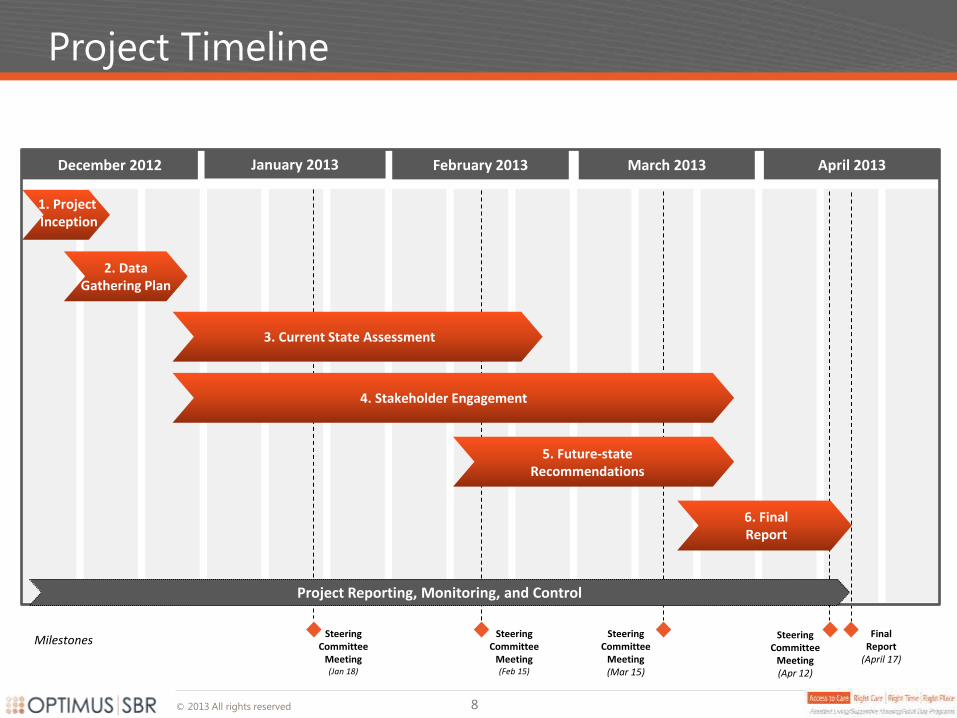
Meeting (Feb 15)
Project Timeline
January 2013 February 2013 March 2013
Milestones Steering
Committee Meeting (Jan 18)
1. Project Inception
2. Data Gathering Plan
December 2012
3. Current State Assessment
4. Stakeholder Engagement
5. Future-state Recommendations
April 2013
Final Report
(April 17)
Steering Committee
Meeting (Mar 15)
Steering Committee
Meeting (Apr 12)
Project Reporting, Monitoring, and Control
6. Final Report
8
Executive Summary
Assisted Living/Supportive
Housing/Adult Day Programs
for
Special Populations
Table of Contents
0. Preliminaries
1. Executive Summary
1. Current State Findings
2. Recommendations
3. Next Steps
2. Current State
3. Recommendations
4. Implementation
5. Appendix
Assisted Living/Supportive
Housing/Adult Day Programs
for
Special Populations
Final Report
South West
© 2013 All rights reserved
Current State
Findings
© 2013 All rights reserved
Definitions
12
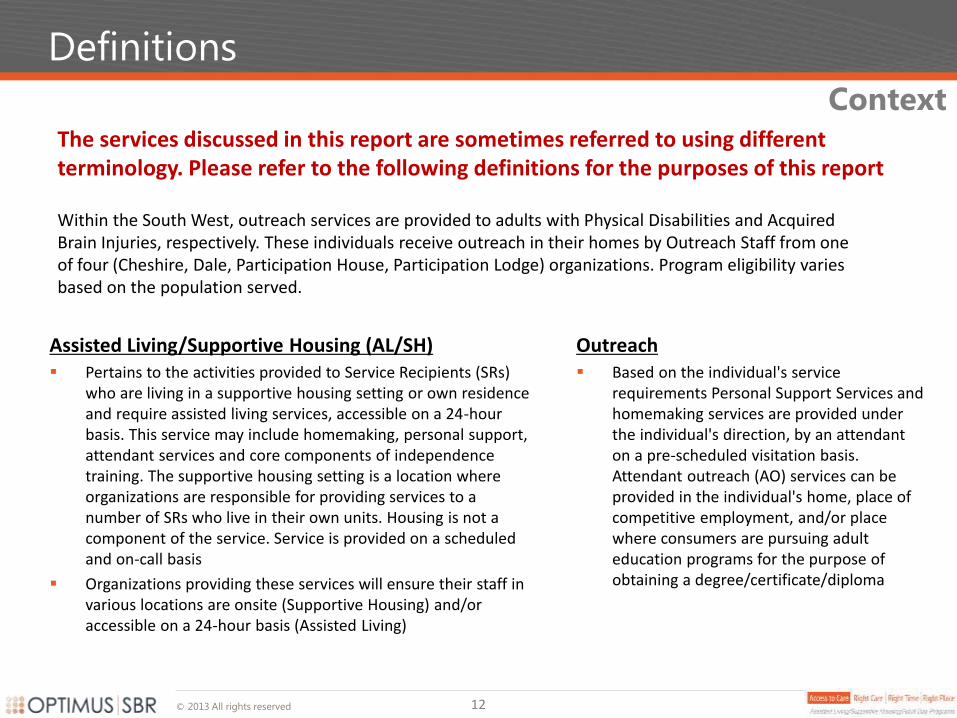
The services discussed in this report are sometimes referred to using different terminology. Please refer to the following definitions for the purposes of this report
Context
Within the South West, outreach services are provided to adults with Physical Disabilities and Acquired Brain Injuries, respectively. These individuals receive outreach in their homes by Outreach Staff from one of four (Cheshire, Dale, Participation House, Participation Lodge) organizations. Program eligibility varies based on the population served.
Assisted Living/Supportive Housing (AL/SH) Pertains to the activities provided to Service Recipients (SRs)
who are living in a supportive housing setting or own residence and require assisted living services, accessible on a 24-hour basis. This service may include homemaking, personal support, attendant services and core components of independence training. The supportive housing setting is a location where organizations are responsible for providing services to a number of SRs who live in their own units. Housing is not a component of the service. Service is provided on a scheduled and on-call basis
Organizations providing these services will ensure their staff in various locations are onsite (Supportive Housing) and/or accessible on a 24-hour basis (Assisted Living)
Outreach Based on the individual's service
requirements Personal Support Services and homemaking services are provided under the individual's direction, by an attendant on a pre-scheduled visitation basis. Attendant outreach (AO) services can be provided in the individual's home, place of competitive employment, and/or place where consumers are pursuing adult education programs for the purpose of obtaining a degree/certificate/diploma
© 2013 All rights reserved 13
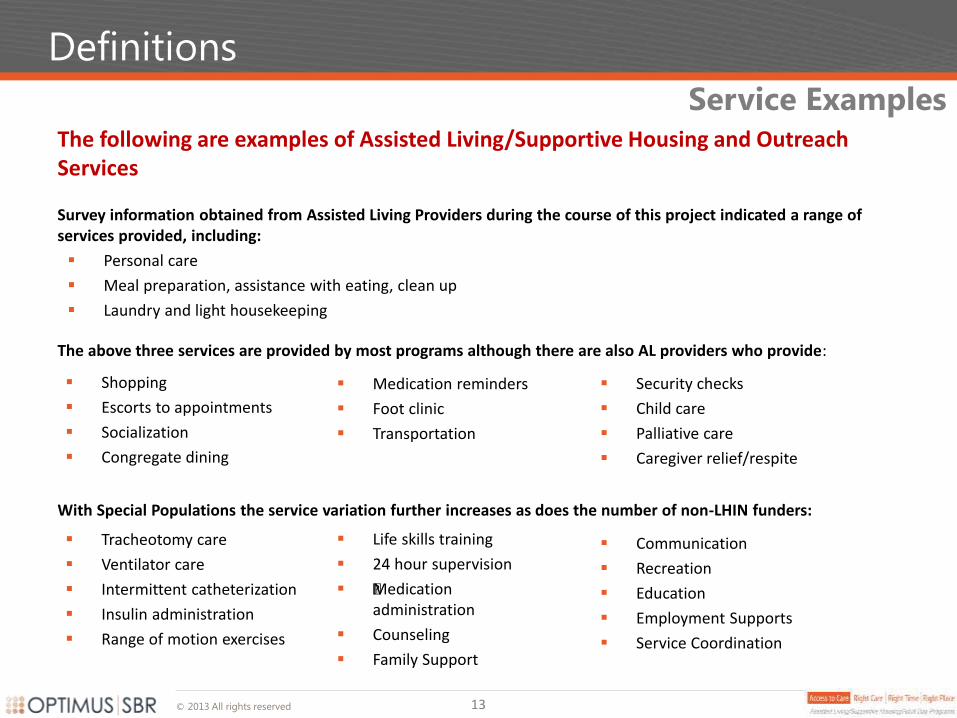
The following are examples of Assisted Living/Supportive Housing and Outreach Services
Survey information obtained from Assisted Living Providers during the course of this project indicated a range of services provided, including:
Personal care
Meal preparation, assistance with eating, clean up
Laundry and light housekeeping
Definitions
Service Examples
The above three services are provided by most programs although there are also AL providers who provide:
With Special Populations the service variation further increases as does the number of non-LHIN funders:
Medication reminders
Foot clinic
Transportation
Security checks
Child care
Palliative care
Caregiver relief/respite
Shopping
Escorts to appointments
Socialization
Congregate dining
Tracheotomy care
Ventilator care
Intermittent catheterization
Insulin administration
Range of motion exercises
Communication
Recreation
Education
Employment Supports
Service Coordination
Life skills training
24 hour supervision
•Medication administration
Counseling
Family Support
© 2013 All rights reserved
Consultations
14
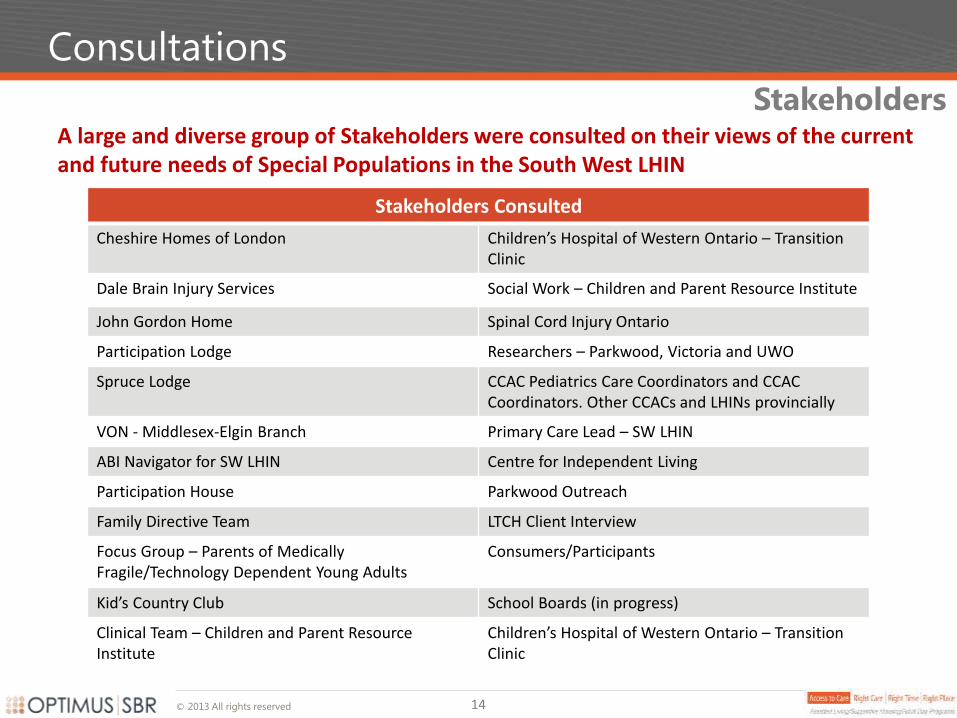
Stakeholders Consulted
Cheshire Homes of London Children’s Hospital of Western Ontario – Transition Clinic
Dale Brain Injury Services Social Work – Children and Parent Resource Institute
John Gordon Home Spinal Cord Injury Ontario
Participation Lodge Researchers – Parkwood, Victoria and UWO
Spruce Lodge CCAC Pediatrics Care Coordinators and CCAC Coordinators. Other CCACs and LHINs provincially
VON - Middlesex-Elgin Branch Primary Care Lead – SW LHIN
ABI Navigator for SW LHIN Centre for Independent Living
Participation House Parkwood Outreach
Family Directive Team LTCH Client Interview
Focus Group – Parents of Medically Fragile/Technology Dependent Young Adults
Consumers/Participants
Kid’s Country Club School Boards (in progress)
Clinical Team – Children and Parent Resource Institute
Children’s Hospital of Western Ontario – Transition Clinic
A large and diverse group of Stakeholders were consulted on their views of the current and future needs of Special Populations in the South West LHIN
Stakeholders
© 2013 All rights reserved
Current Supply and Demand in the South West
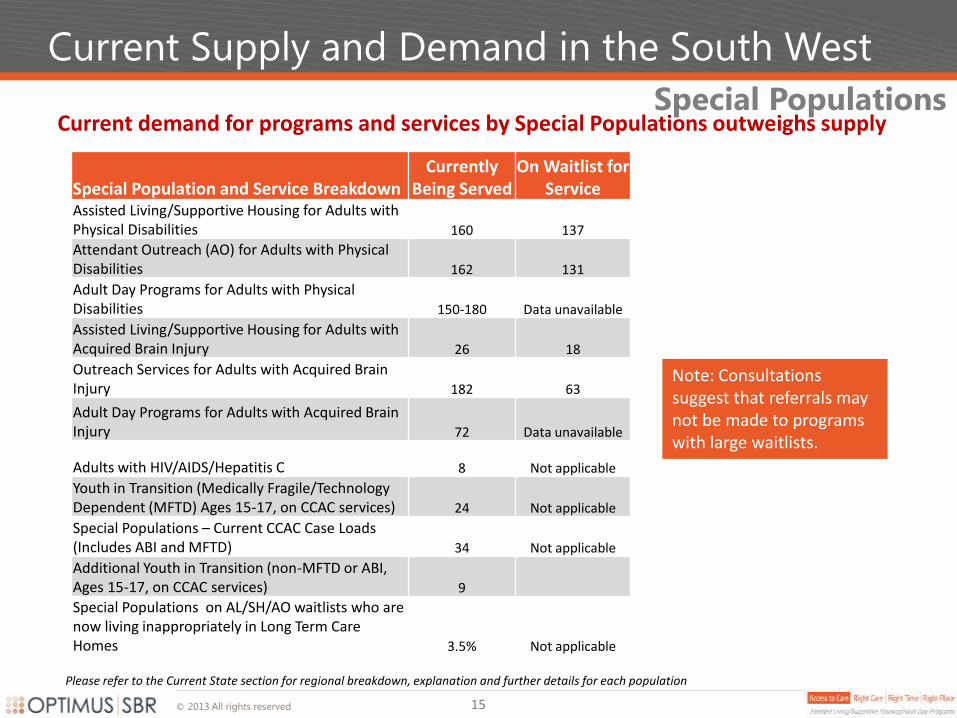
Current demand for programs and services by Special Populations outweighs supply
Note: Consultations suggest that referrals may not be made to programs with large waitlists.
Special Populations
Special Population and Service Breakdown Currently
Being Served On Waitlist for
Service Assisted Living/Supportive Housing for Adults with Physical Disabilities 160 137
Attendant Outreach (AO) for Adults with Physical Disabilities 162 131
Adult Day Programs for Adults with Physical Disabilities 150-180 Data unavailable
Assisted Living/Supportive Housing for Adults with Acquired Brain Injury 26 18
Outreach Services for Adults with Acquired Brain Injury 182 63
Adult Day Programs for Adults with Acquired Brain Injury 72 Data unavailable
Adults with HIV/AIDS/Hepatitis C 8 Not applicable
Youth in Transition (Medically Fragile/Technology Dependent (MFTD) Ages 15-17, on CCAC services) 24 Not applicable
Special Populations – Current CCAC Case Loads (Includes ABI and MFTD) 34 Not applicable
Additional Youth in Transition (non-MFTD or ABI, Ages 15-17, on CCAC services) 9
Special Populations on AL/SH/AO waitlists who are now living inappropriately in Long Term Care Homes 3.5% Not applicable
15
Please refer to the Current State section for regional breakdown, explanation and further details for each population
© 2013 All rights reserved
Current State Funding
Special Population funding has not kept up with demand or inflation, creating significant waitlists for these groups and upcoming deficits particularly in Assisted Living/Supportive Housing
Chronic Underfunding
The result of underfunding has been:
AL/SH units have closed over time, translating into fewer services
AL/SH units for Adults with Physical Disabilities outnumber those whom have ABIs by a 4:1 margin. The ABI population has only 26 Assisted Living/Supportive Housing units in the entire LHIN
Request(s) for permanent reallocation of funds from Outreach programs to Supportive Housing
Decreasing supply - as needs increase as people age in place, fewer people can be served
The Good News:
Last year the LHIN funded LHIN-wide Attendant Outreach ($352,000), ABI Outreach ($175,000) and the Urgent Fund ($225,000). This year funding for Overnight Respite and Day Program space increases for the MF/TD population in London ($525,000) was provided
16
© 2013 All rights reserved
Interview Findings - Summary
17
Key Findings
Demand for services greatly outweighs supply
Need for highly individualized services; there is no one size fits all approach
People wish to participate in system design and in developing their individualized plans
Business processes should not hamper innovation or the ability to respond in a crisis
Transitioning to adulthood is traumatic for families because they lose so much support
People have to relocate to access services
Ministry policies may be outdated when it comes to these populations
Funding shortages have contributed to a lack of access to care for Special Populations, resulting in an underserved population that feels isolated and hopeless
Refer to Client Stories for individual experiences.
© 2013 All rights reserved
Current State Assessment
18
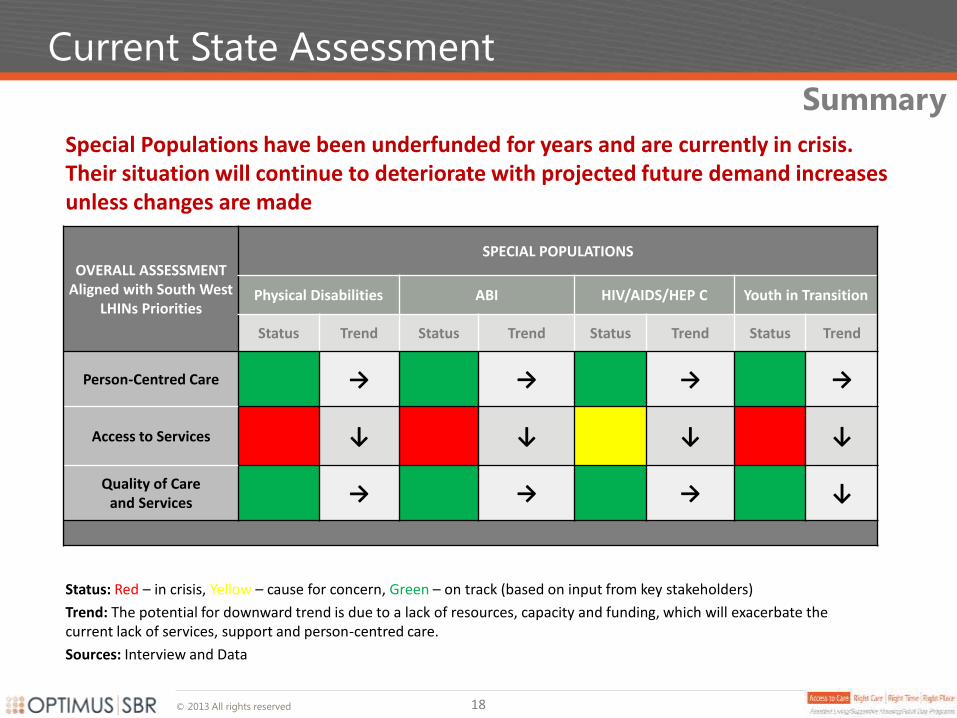
Special Populations have been underfunded for years and are currently in crisis. Their situation will continue to deteriorate with projected future demand increases unless changes are made
OVERALL ASSESSMENT Aligned with South West
LHINs Priorities
SPECIAL POPULATIONS
Physical Disabilities ABI HIV/AIDS/HEP C Youth in Transition
Status Trend Status Trend Status Trend Status Trend
Person-Centred Care → → → →
Access to Services ↓ ↓ ↓ ↓
Quality of Care and Services → → → ↓
Summary
Status: Red – in crisis, Yellow – cause for concern, Green – on track (based on input from key stakeholders)
Trend: The potential for downward trend is due to a lack of resources, capacity and funding, which will exacerbate the current lack of services, support and person-centred care.
Sources: Interview and Data
© 2013 All rights reserved
Recommendations
© 2013 All rights reserved
Recommendations
20
Person-centered – the primary focus is on the population’s needs and of their caregivers and families
High-impact – focus on prioritiy issues such as limited access to services versus secondary issues
Innovative and Flexibile – care models reflect the wide range of needs of individuals/caregivers
Evidence-based – recommendations are based on evidence, data and research where possible
Realistic – limited funding and potential for new investments are taken into account
CCAC Expanded Role – the expanded role of the CCAC is reflected in process related recommendations
South West LHIN Alignment – recommendation categories align with the SW LHINs performance areas
of focus
Recommendations were driven by the following:
Guiding Principles
© 2013 All rights reserved
Recommendations Overview
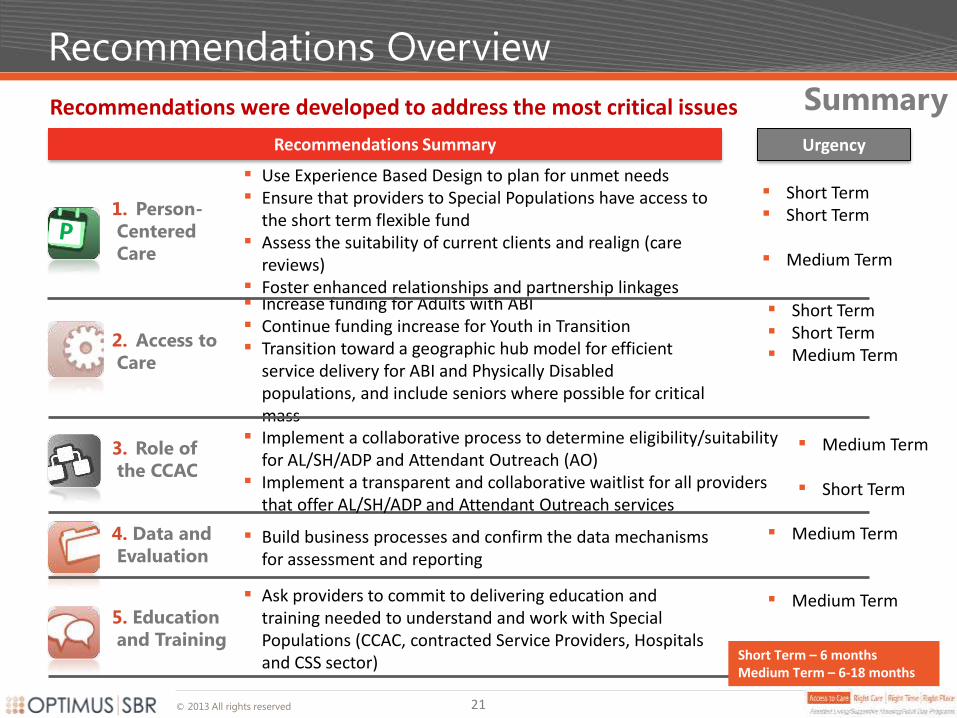
Recommendations were developed to address the most critical issues
21
Increase funding for Adults with ABI Continue funding increase for Youth in Transition Transition toward a geographic hub model for efficient
service delivery for ABI and Physically Disabled populations, and include seniors where possible for critical mass
Recommendations Summary
Summary
1. Person-
Centered
Care
2. Access to
Care
4. Data and
Evaluation
3. Role of
the CCAC
Implement a collaborative process to determine eligibility/suitability
for AL/SH/ADP and Attendant Outreach (AO) Implement a transparent and collaborative waitlist for all providers
that offer AL/SH/ADP and Attendant Outreach services
Use Experience Based Design to plan for unmet needs Ensure that providers to Special Populations have access to
the short term flexible fund Assess the suitability of current clients and realign (care
reviews) Foster enhanced relationships and partnership linkages
Build business processes and confirm the data mechanisms for assessment and reporting
Ask providers to commit to delivering education and training needed to understand and work with Special Populations (CCAC, contracted Service Providers, Hospitals and CSS sector)
5. Education
and Training Short Term – 6 months Medium Term – 6-18 months
Urgency
Short Term Short Term
Medium Term
Short Term Short Term Medium Term
Medium Term
Short Term
Medium Term
Medium Term
© 2013 All rights reserved
Recommendations – Person-Centred Care
22
Realigning Special Populations with the use of a flex fund and deploying Experience Based Design should improve outcomes
All Special Populations
Use Experience Based Design as a framework to develop an approach to address unmet
needs. This will address the needs of those with highly individualized care, providing much
needed support for families and caregivers
Ensure that providers to Special Populations have access to the short term flexible fund in
order to:
avoid their inappropriate admission to ER or LTCHs
mitigate against family breakdown (this could include individualized funding models)
Conduct Care Reviews (Individual Assessments)
Assess the suitability of current clients and programs, and realign as required
Identify who could manage with just attendant outreach or in a cluster model vs. building based services
Examine where a lower cost Adult Day Program (ADP) solution can be used instead of Attendant Outreach
Where possible transition the individual to the most appropriate provider. The overall model of care should be more focused on providing supports to enable independent living where possible, and include some combination of all three types of services (AL/SH, Attendant Outreach and ADP), as required
© 2013 All rights reserved
Recommendations – Access to Care
ABI and Youth in Transition
Lack of funding necessitates the prioritization of those with the highest needs. Individuals with ABIs are at particular risk due to chronic underfunding
Increase funding and resources for Adults with Acquired Brain Injuries. The ABI and MFTD populations are falling through the cracks and they have a general lack of alternatives. The exact amount of funding will need to be informed by the Care Reviews. The range of additional funding needed is provided in the financial projection scenarios
Prioritize Youth in Transition funding. Families whose children are MFTD, as well as the Care Coordinators and other clinical staff involved in their current care, expressed extreme concern about the lack of resources available to these children, particularly as they transition to adulthood and the organizations from whom they receive those services change. In light of recent funding in the City of London, further work is needed to define the urgent needs of families for funding priorities. Consider implementing a working group with parents
Move toward a geographic hub for efficient service delivery. Transition toward a geographic hub model for efficient service delivery for ABI and Physically Disabled populations, and include seniors where possible for critical mass
23
© 2013 All rights reserved
Recommendations – Role of the CCAC
24
Due to the complexity and wide variance in needs of Special Populations, Subject Matter Experts must work together with the CCAC to define eligibility criteria
Implement a collaborative process to determine eligibility/suitability for Assisted
Living/Supportive Housing/Adult Day Programs and Attendant Outreach services. A
collaborative team of CCAC and CSS colleagues should form a working group to fully
outline eligibility and prioritization for specific programs, and determine business
processes for comprehensive and multidisciplinary/multi-partner (in some cases)
assessments. This would include services related to the medically fragile/technology
dependent youth in transition and adult population
Implement a transparent and collaborative waitlist with providers of Assisted
Living/Supportive Housing/Adult Day Programs and Attendant Outreach. The provision of
service for those waitlisted needs to be determined as part of a collaborative process
with the partners involved; in many instances, CCAC would require the assistance of other
partners to care for those on waitlist as they alone may not be able to meet the client’s
needs Include Attendant Outreach Services and individuals with Hepatitis C in the Expanded
Role of the CCAC for AL/SH and Adult Day Program. Providers noted separate business
processes for these individuals as inefficient CCAC should include Attendant Outreach in its mix of coordinated services
All Special Populations
© 2013 All rights reserved
Recommendations – Data and Evaluation
25
Build business processes and confirm the data mechanisms for assessment and reporting (e.g. Adult Day Program data, etc.)
Identify the best data sources between the providers and the CCAC as business processes are built and confirmed
Propose a mandatory requirement for regular reporting to the LHIN using a ubiquitous reporting tool:
Current and Waitlisted Clients Numbers
Region of Residence
Client Age
Date of Application for Service
Date of Start of Service (if applicable)
Discharge Date (if applicable)
Program/Service Applied for
Primary Diagnosis/Client Classification (i.e. ABI, Physically Disabled, HIV/HEP
C)
Recommended Frequency of Reporting: Quarterly
All Special Populations
There is a need to implement new robust data collection and evaluation processes to leverage in making informed decisions about Special Populations going forward
© 2013 All rights reserved
Recommendations – Education and Training
26
Leverage Human Resources and existing infrastructure in light of funding pressures
Ask providers to commit to delivering education and training needed to understand and work with Special Populations (CCAC, contracted Service Providers, Hospitals and CSS sector)
In depth education planning is required to assist Care Coodinators in their understanding of options for these populations, including available housing, programming, day programs, respite, etc. This should also include education to help partners understand the CCAC role
Providers should explore communal training to reduce costs and build awareness of one another's capabilities using the Train the Trainer model
Providers should explore collaborative staff sharing models where possible to leverage economies of scale and account for potential staffing shortages
Where possible providers should explore the ability of their sector partners to train, assess, and provide ongoing support for their clients
Further explore respite and convalescent care options in all settings to leverage available resources and accommodate the needs of these special populations despite the reluctance of some parents of MF/TD young adults
All Special Populations
© 2013 All rights reserved
Implementation
© 2013 All rights reserved
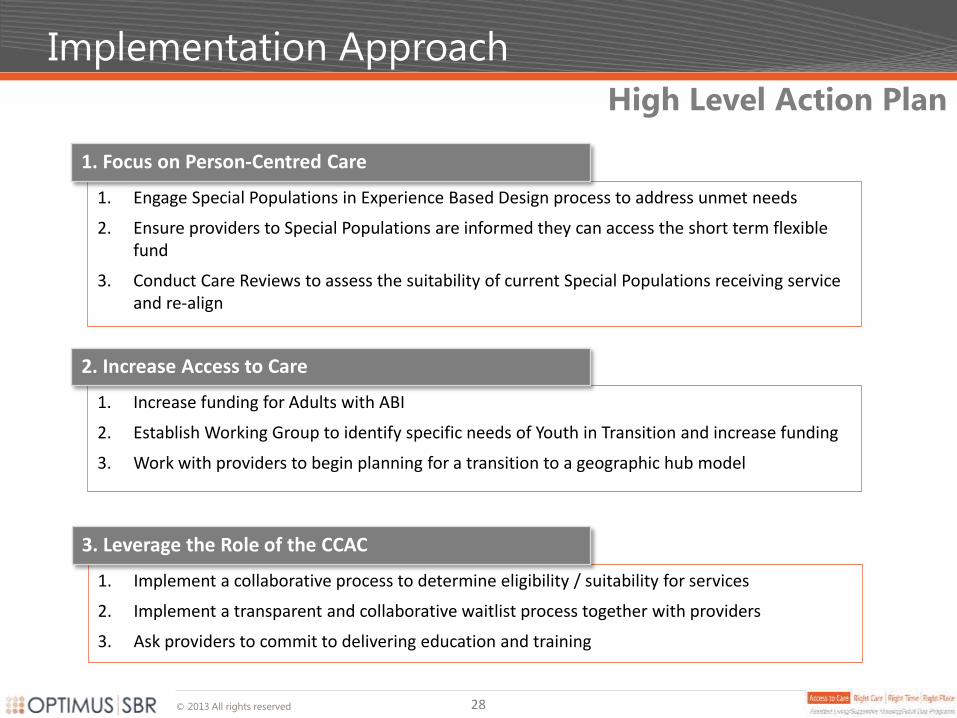
Implementation Approach
28
1. Engage Special Populations in Experience Based Design process to address unmet needs
2. Ensure providers to Special Populations are informed they can access the short term flexible fund
3. Conduct Care Reviews to assess the suitability of current Special Populations receiving service and re-align
1. Focus on Person-Centred Care
1. Increase funding for Adults with ABI
2. Establish Working Group to identify specific needs of Youth in Transition and increase funding
3. Work with providers to begin planning for a transition to a geographic hub model
2. Increase Access to Care
1. Implement a collaborative process to determine eligibility / suitability for services
2. Implement a transparent and collaborative waitlist process together with providers
3. Ask providers to commit to delivering education and training
3. Leverage the Role of the CCAC
High Level Action Plan
© 2013 All rights reserved
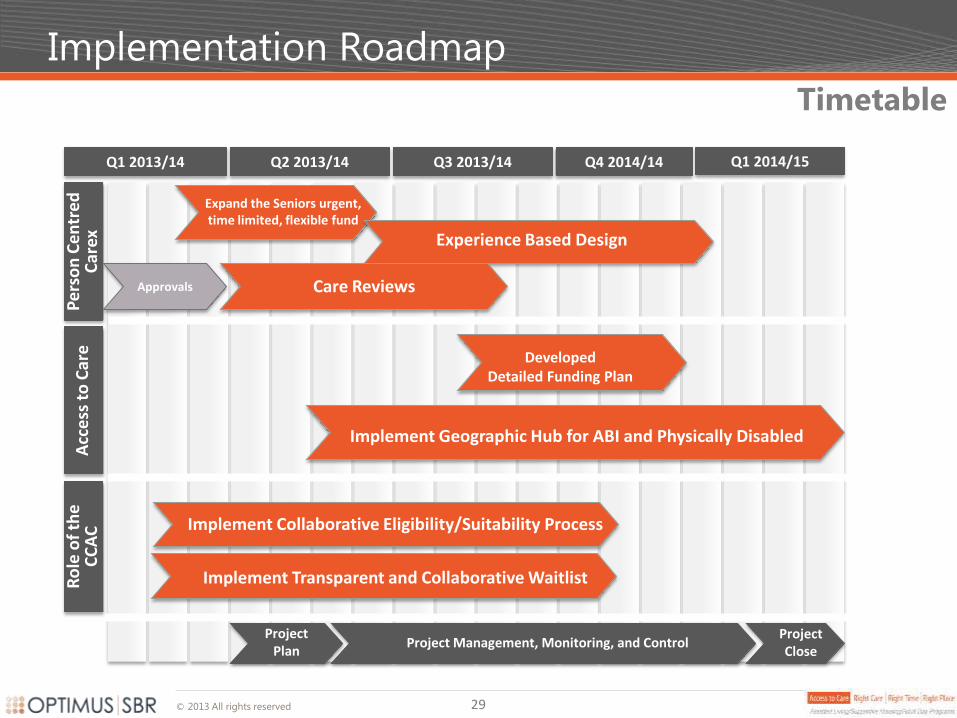
Implementation Roadmap
29
Q1 2013/14 Q2 2013/14 Q3 2013/14 Q4 2014/14 Q1 2014/15
Pe
rso
n C
en
tre
d
Car
ex
Project Close
Project Management, Monitoring, and Control Project
Plan
Expand the Seniors urgent, time limited, flexible fund
Acc
ess
to
Car
e
Implement Collaborative Eligibility/Suitability Process
Approvals
Experience Based Design
Care Reviews
Implement Geographic Hub for ABI and Physically Disabled
Developed Detailed Funding Plan
Timetable R
ole
of
the
C
CA
C
Implement Transparent and Collaborative Waitlist
Main Report • Assisted Living/Supportive
Housing/Adult Day Programs for Special Populations
Current State
Assisted Living/Supportive
Housing/Adult Day Programs
for
Special Populations
Table of Contents
0. Preliminaries
1. Executive Summary
2. Current State
1. Consultations
2. Current Demand
3. Funding
4. Interview Findings
5. Client Stories
6. Summary
3. Recommendations
4. Implementation
5. Appendix – Future State
Assisted Living/Supportive
Housing/Adult Day Programs
for
Special Populations Draft Final Report
South West

© 2013 All rights reserved
Consultations
33
Stakeholders Consulted
Cheshire Homes of London Children’s Hospital of Western Ontario – Transition Clinic
Dale Brain Injury Services Social Work – Children and Parent Resource Institute
John Gordon Home Spinal Cord Injury Ontario
Participation Lodge Researchers – Parkwood, Victoria and UWO
Spruce Lodge CCAC Pediatrics Care Coordinators and CCAC Coordinators. Other CCACs and LHINs provincially
VON - Middlesex-Elgin Branch Primary Care Lead – SW LHIN
ABI Navigator for SW LHIN Centre for Independent Living
Participation House Parkwood Outreach
Family Directive Team LTCH Client Interview
Focus Group – Parents of Medically Fragile/Technology Dependent Young Adults
Consumers/Participants
Kid’s Country Club School Boards (in progress)
Clinical Team – Children and Parent Resource Institute
Children’s Hospital of Western Ontario – Transition Clinic
A large and diverse group of Stakeholders were consulted on their views of the current and future needs of Special Populations in the South West LHIN
Stakeholders
© 2013 All rights reserved
Current Demand
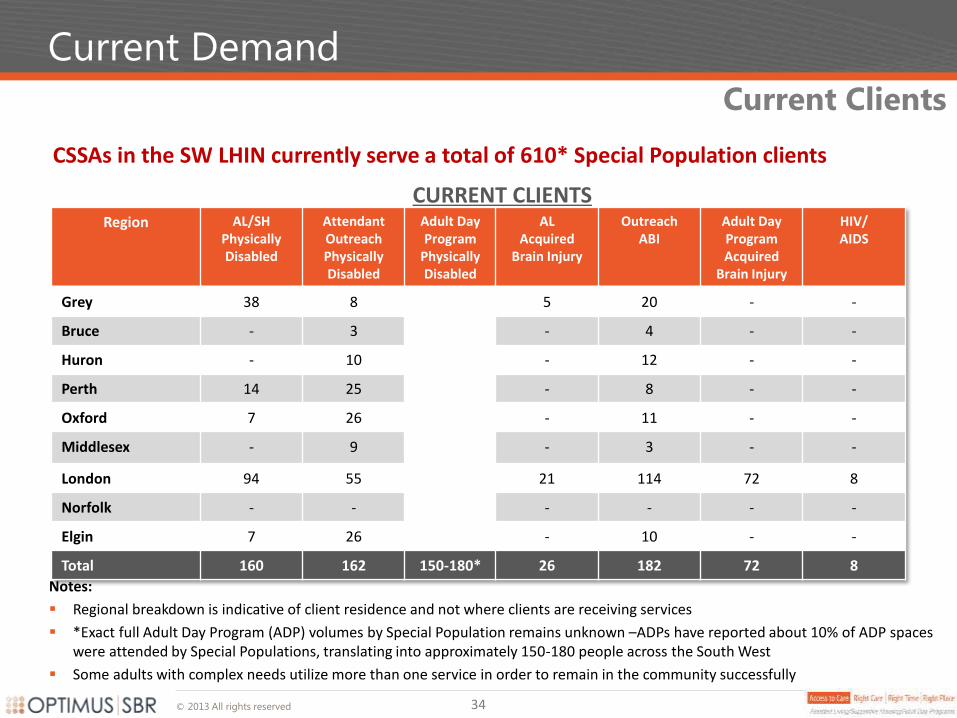
CSSAs in the SW LHIN currently serve a total of 610* Special Population clients
Notes:
Regional breakdown is indicative of client residence and not where clients are receiving services
*Exact full Adult Day Program (ADP) volumes by Special Population remains unknown –ADPs have reported about 10% of ADP spaces were attended by Special Populations, translating into approximately 150-180 people across the South West
Some adults with complex needs utilize more than one service in order to remain in the community successfully
Current Clients
Region AL/SH Physically Disabled
Attendant Outreach Physically Disabled
Adult Day Program
Physically Disabled
AL Acquired
Brain Injury
Outreach ABI
Adult Day Program Acquired
Brain Injury
HIV/ AIDS
Grey 38 8 5 20 - -
Bruce - 3 - 4 - -
Huron - 10 - 12 - -
Perth 14 25 - 8 - -
Oxford 7 26 - 11 - -
Middlesex - 9 - 3 - -
London 94 55 21 114 72 8
Norfolk - - - - - -
Elgin 7 26 - 10 - -
Total 160 162 150-180* 26 182 72 8
CURRENT CLIENTS
34
© 2013 All rights reserved
Current Demand
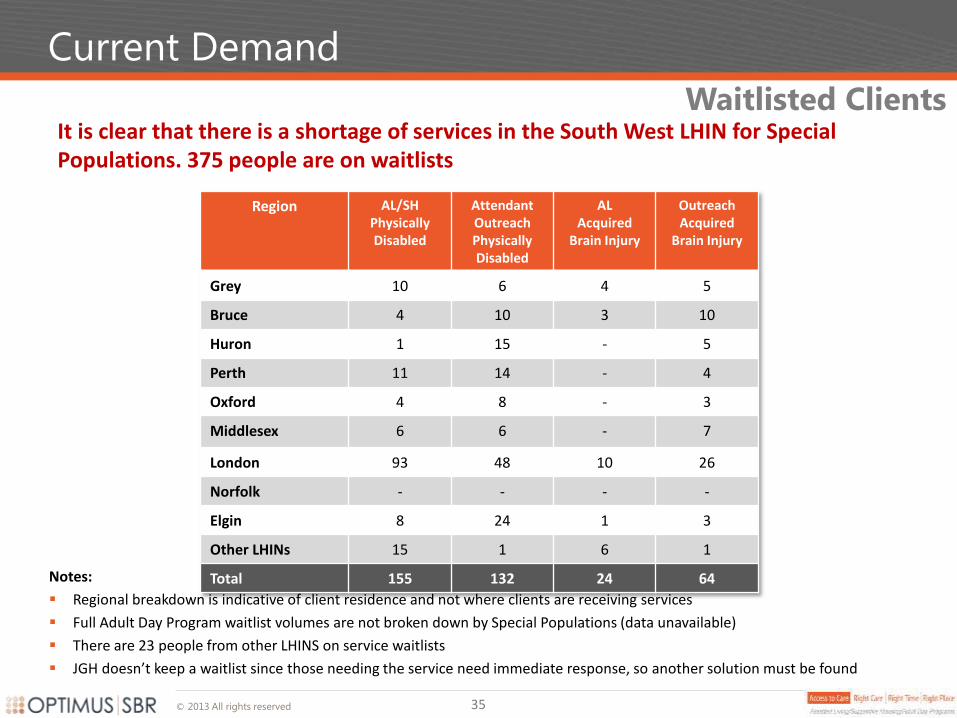
It is clear that there is a shortage of services in the South West LHIN for Special Populations. 375 people are on waitlists
Notes:
Regional breakdown is indicative of client residence and not where clients are receiving services
Full Adult Day Program waitlist volumes are not broken down by Special Populations (data unavailable)
There are 23 people from other LHINS on service waitlists
JGH doesn’t keep a waitlist since those needing the service need immediate response, so another solution must be found
Waitlisted Clients
Region AL/SH Physically Disabled
Attendant Outreach Physically Disabled
AL Acquired
Brain Injury
Outreach Acquired
Brain Injury
Grey 10 6 4 5
Bruce 4 10 3 10
Huron 1 15 - 5
Perth 11 14 - 4
Oxford 4 8 - 3
Middlesex 6 6 - 7
London 93 48 10 26
Norfolk - - - -
Elgin 8 24 1 3
Other LHINs 15 1 6 1
Total 155 132 24 64
35
© 2013 All rights reserved
Current Demand
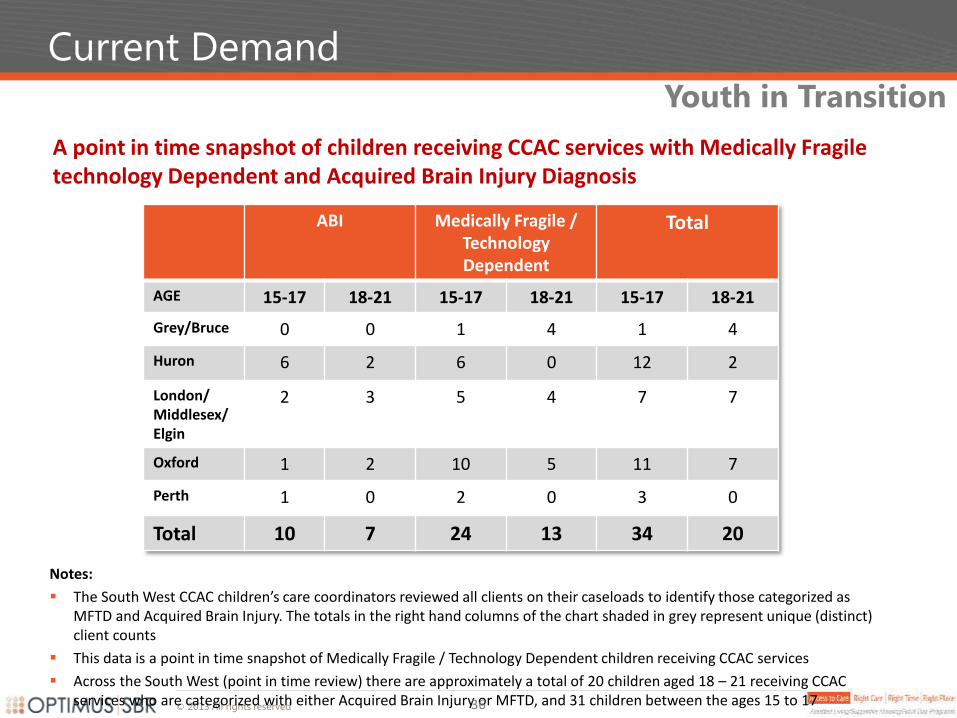
A point in time snapshot of children receiving CCAC services with Medically Fragile technology Dependent and Acquired Brain Injury Diagnosis
Youth in Transition
ABI Medically Fragile / Technology Dependent
Total
AGE 15-17 18-21 15-17 18-21 15-17 18-21
Grey/Bruce 0 0 1 4 1 4
Huron 6 2 6 0 12 2
London/ Middlesex/ Elgin
2 3 5 4 7 7
Oxford 1 2 10 5 11 7
Perth 1 0 2 0 3 0
Total 10 7 24 13 34 20
Notes:
The South West CCAC children’s care coordinators reviewed all clients on their caseloads to identify those categorized as MFTD and Acquired Brain Injury. The totals in the right hand columns of the chart shaded in grey represent unique (distinct) client counts
This data is a point in time snapshot of Medically Fragile / Technology Dependent children receiving CCAC services
Across the South West (point in time review) there are approximately a total of 20 children aged 18 – 21 receiving CCAC services who are categorized with either Acquired Brain Injury or MFTD, and 31 children between the ages 15 to 17 36
© 2013 All rights reserved
Current Demand
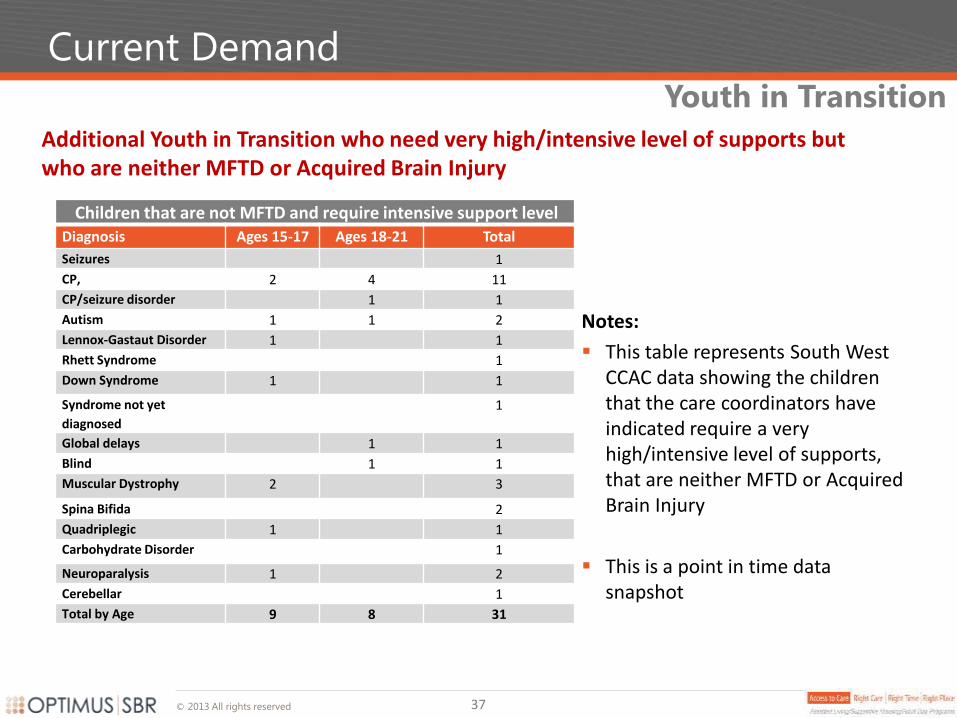
Additional Youth in Transition who need very high/intensive level of supports but who are neither MFTD or Acquired Brain Injury
Youth in Transition
Notes:
This table represents South West CCAC data showing the children that the care coordinators have indicated require a very high/intensive level of supports, that are neither MFTD or Acquired Brain Injury
This is a point in time data snapshot
Children that are not MFTD and require intensive support level Diagnosis Ages 15-17 Ages 18-21 Total
Seizures 1
CP, 2 4 11
CP/seizure disorder 1 1
Autism 1 1 2
Lennox-Gastaut Disorder 1 1
Rhett Syndrome 1
Down Syndrome 1 1
Syndrome not yet
diagnosed
1
Global delays 1 1
Blind 1 1
Muscular Dystrophy 2 3
Spina Bifida 2
Quadriplegic 1 1
Carbohydrate Disorder 1
Neuroparalysis 1 2
Cerebellar 1
Total by Age 9 8 31
37
© 2013 All rights reserved
Current Demand – Transitional Support Services
Housing instability is a key marker of extreme poverty, and is both a cause and effect of the ongoing AIDS crisis in North America. Rates of HIV infection among homeless persons are as much as 16 times higher than in the general population (Denning and Dinenno, 2010; Kerker, 2005; Robertson, 2005; Culhane, 2001)
There was a 10% increase in new HIV diagnoses in Southwestern Ontario between 2009 and 2010 and an average of 15 newly-diagnosed HIV cases and 6 newly-diagnosed AIDS cases were reported in Middlesex-London per year between 2000 and 2010
JGH captures a large number of people who would be homeless otherwise
JGH enjoys strong partnerships with the London Intercommunity Health Centre, the Family Health Team at Centre for Hope, shelters – working collaboratively to develop a proposal for a medical respite facility to provide medical care for all homeless who are discharged (not just addictions)
JGH is really seeing the impact of the intervention – 3 people admitted to JGH and deemed palliative have had their diagnosis now deemed stable – the miracle – getting the drugs and nutrition and a home
The John Gordon Home (JGH) is the only AL provider serving the HIV/AIDS/HEP C population
HIV/AIDS/HEP C
38
© 2013 All rights reserved
Current Demand
Geographic View
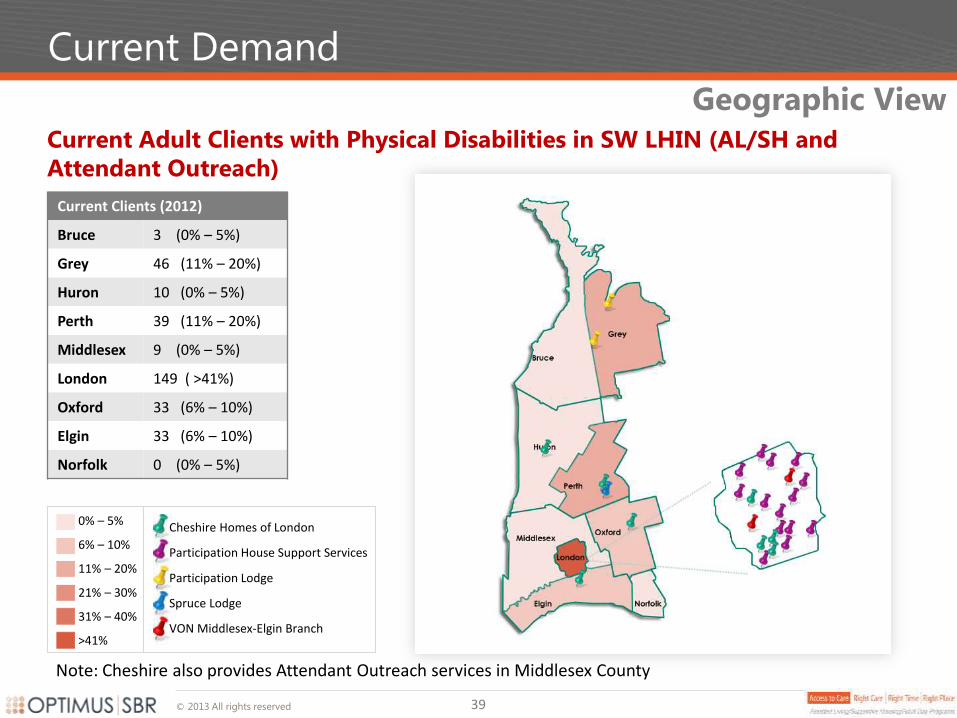
Current Adult Clients with Physical Disabilities in SW LHIN (AL/SH and
Attendant Outreach)
Current Clients (2012)
Bruce 3 (0% – 5%)
Grey 46 (11% – 20%)
Huron 10 (0% – 5%)
Perth 39 (11% – 20%)
Middlesex 9 (0% – 5%)
London 149 ( >41%)
Oxford 33 (6% – 10%)
Elgin 33 (6% – 10%)
Norfolk 0 (0% – 5%)
0% – 5%
6% – 10%
11% – 20%
21% – 30%
31% – 40%
>41%
Cheshire Homes of London
Participation House Support Services
Participation Lodge
Spruce Lodge
VON Middlesex-Elgin Branch
39
Note: Cheshire also provides Attendant Outreach services in Middlesex County
© 2013 All rights reserved
Current Demand
Geographic View
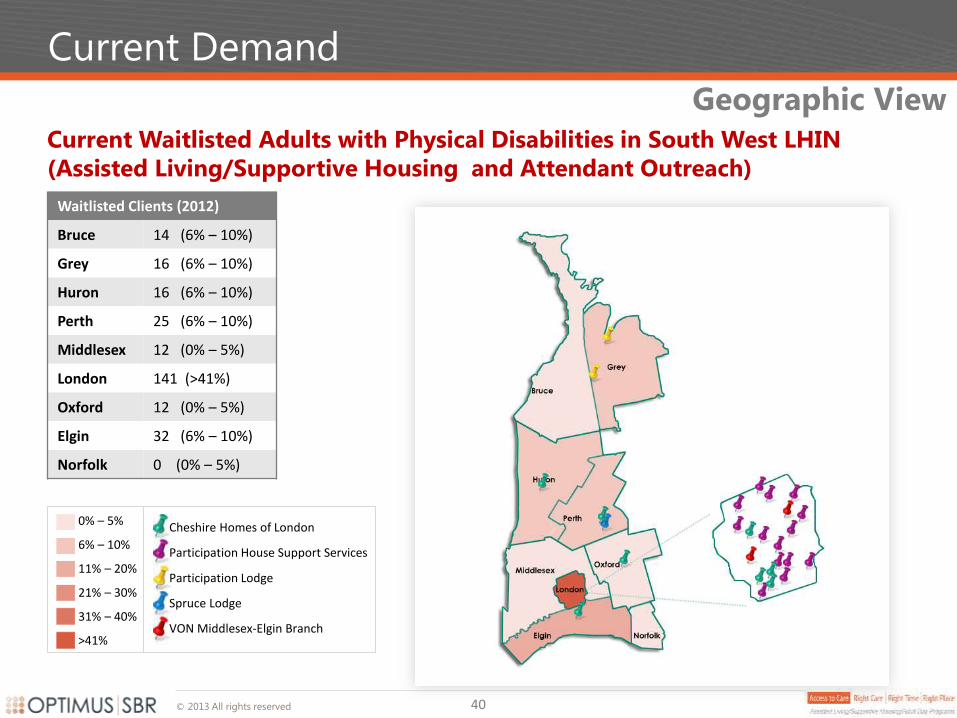
Current Waitlisted Adults with Physical Disabilities in South West LHIN
(Assisted Living/Supportive Housing and Attendant Outreach)
Waitlisted Clients (2012)
Bruce 14 (6% – 10%)
Grey 16 (6% – 10%)
Huron 16 (6% – 10%)
Perth 25 (6% – 10%)
Middlesex 12 (0% – 5%)
London 141 (>41%)
Oxford 12 (0% – 5%)
Elgin 32 (6% – 10%)
Norfolk 0 (0% – 5%)
0% – 5%
6% – 10%
11% – 20%
21% – 30%
31% – 40%
>41%
Cheshire Homes of London
Participation House Support Services
Participation Lodge
Spruce Lodge
VON Middlesex-Elgin Branch
40
© 2013 All rights reserved
Current Demand
Geographic View
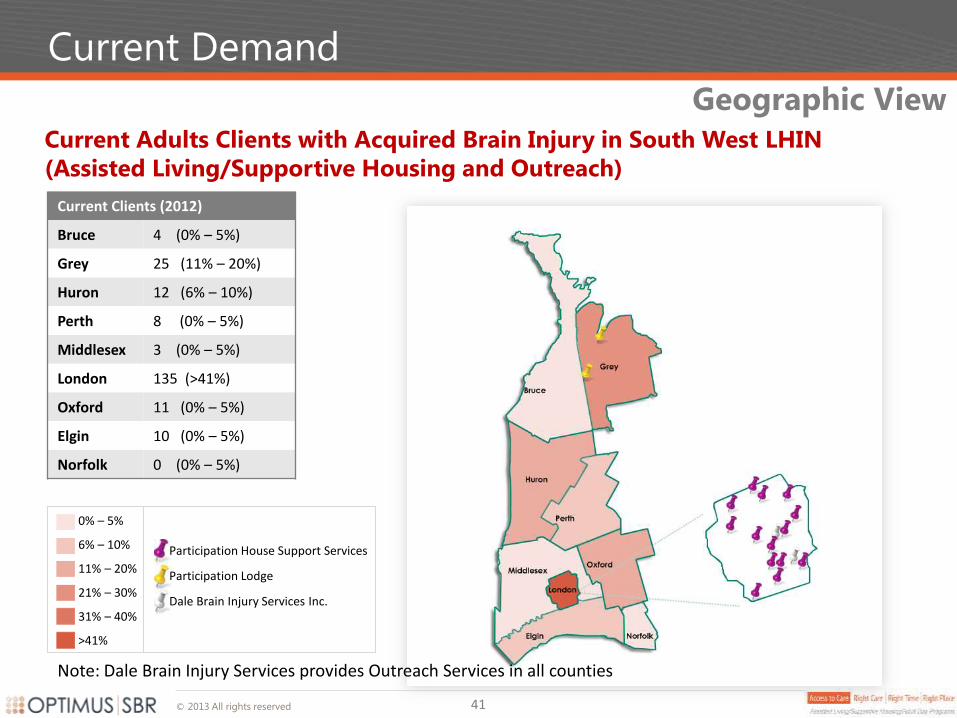
Current Adults Clients with Acquired Brain Injury in South West LHIN
(Assisted Living/Supportive Housing and Outreach)
Current Clients (2012)
Bruce 4 (0% – 5%)
Grey 25 (11% – 20%)
Huron 12 (6% – 10%)
Perth 8 (0% – 5%)
Middlesex 3 (0% – 5%)
London 135 (>41%)
Oxford 11 (0% – 5%)
Elgin 10 (0% – 5%)
Norfolk 0 (0% – 5%)
0% – 5%
6% – 10%
11% – 20%
21% – 30%
31% – 40%
>41%
Participation House Support Services
Participation Lodge
Dale Brain Injury Services Inc.
41
Note: Dale Brain Injury Services provides Outreach Services in all counties
© 2013 All rights reserved
Current Demand
Geographic View
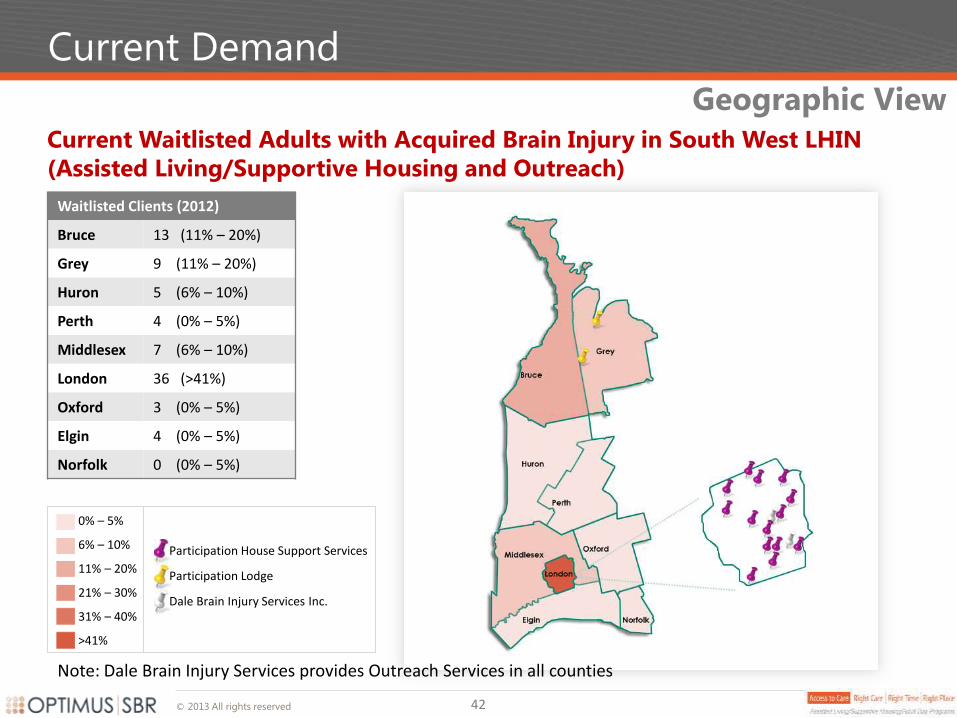
Current Waitlisted Adults with Acquired Brain Injury in South West LHIN
(Assisted Living/Supportive Housing and Outreach)
Waitlisted Clients (2012)
Bruce 13 (11% – 20%)
Grey 9 (11% – 20%)
Huron 5 (6% – 10%)
Perth 4 (0% – 5%)
Middlesex 7 (6% – 10%)
London 36 (>41%)
Oxford 3 (0% – 5%)
Elgin 4 (0% – 5%)
Norfolk 0 (0% – 5%)
0% – 5%
6% – 10%
11% – 20%
21% – 30%
31% – 40%
>41%
Participation House Support Services
Participation Lodge
Dale Brain Injury Services Inc.
42
Note: Dale Brain Injury Services provides Outreach Services in all counties
© 2013 All rights reserved
Current Demand
Geographic View
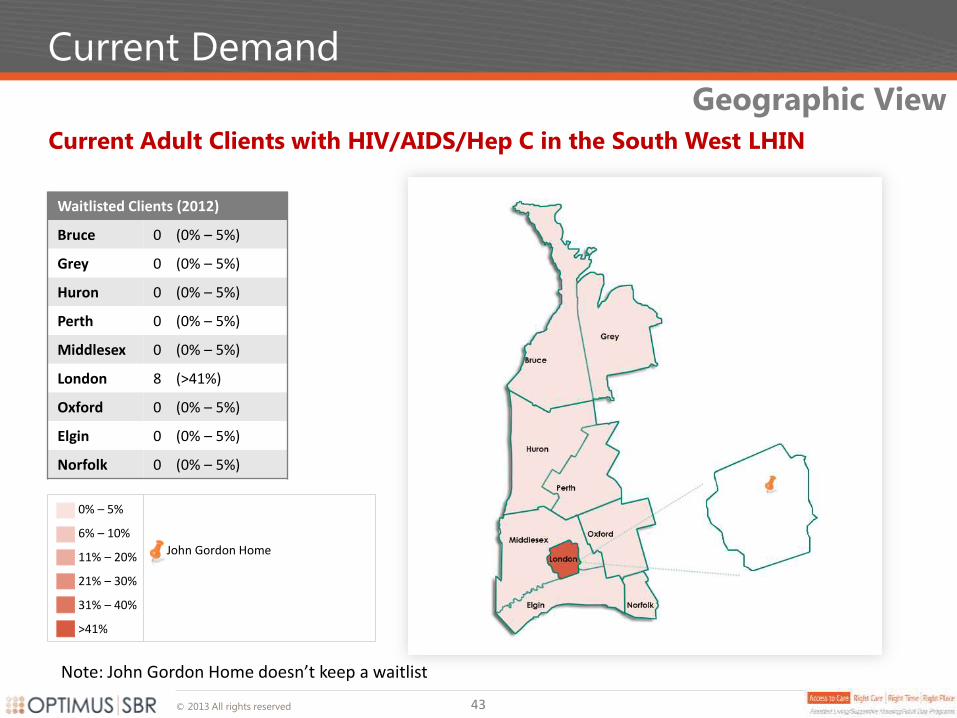
Waitlisted Clients (2012)
Bruce 0 (0% – 5%)
Grey 0 (0% – 5%)
Huron 0 (0% – 5%)
Perth 0 (0% – 5%)
Middlesex 0 (0% – 5%)
London 8 (>41%)
Oxford 0 (0% – 5%)
Elgin 0 (0% – 5%)
Norfolk 0 (0% – 5%)
Current Adult Clients with HIV/AIDS/Hep C in the South West LHIN
0% – 5%
6% – 10%
11% – 20%
21% – 30%
31% – 40%
>41%
John Gordon Home
Note: John Gordon Home doesn’t keep a waitlist
43
© 2013 All rights reserved
Current Demand – Long Term Care (LTC)
Based on the Cheshire experience, approximately 3.5% of Special Populations awaiting service (AL/SH or Attendant Outreach) are inappropriately living in Long Term Care Homes as of April 2013
Consultations suggest that when shortages in service occur that those in need may be inappropriately placed in other types of housing such as Long Term Care Homes, particularly in non-urban regions were options are more limited. It is known that some of these individuals could be living in their own units with the appropriate outreach services in place.
While long term care is a very appropriate level of care for the right individual, it is important that clients in long term care as part of their transition are not lost and that their housing needs are addressed in order that they can be served in the right place.
Cheshire Experience:
There were approximately 200 Special Populations adults awaiting service at Cheshire Homes of London as of April 2013
Of these individuals, 7 (3.5%) were currently living in Long Term Care Homes and awaiting AL/SH and Outreach services
LTC Estimate
44
© 2013 All rights reserved
Current State Funding
Special Population funding has not kept up with demand or inflation, creating significant waitlists for these groups and upcoming deficits particularly in Assisted Living/Supportive Housing
Chronic Underfunding
The result of underfunding has been:
AL/SH units have closed over time, translating into fewer services
AL/SH units for Adults with Physical Disabilities outnumber those whom have Acquired Brain Injuries by a 4:1 margin. The Acquired Brain Injury population has only 26 Assisted Living/Supportive Housing units in the entire LHIN
Request(s) for permanent reallocation of funds from Outreach programs to Supportive Housing
Decreasing supply - as needs increase as people age in place, fewer people can be served
The Good News:
Last year the LHIN funded LHIN-wide Attendant Outreach ($352,000), Acquired Brain Injury Outreach ($175,000) and the Urgent Fund ($225,000). This year funding for Overnight Respite and Day Program space increases for the MF/TD population in London ($525,000) was provided
45
© 2013 All rights reserved
Interview Findings - Summary
46
Key Findings
Demand for services greatly outweighs supply
Need for highly individualized services; there is no one size fits all approach
People wish to participate in system design and in developing their individualized plans
Business processes should not hamper innovation or the ability to respond in a crisis
Transitioning to adulthood is traumatic for families because they lose so much support
People have to relocate to access services
Ministry policies may be outdated when it comes to these populations
Funding shortages have contributed to a lack of access to care for Special Populations, resulting in an underserved population that feels isolated and hopeless
Refer to Client Stories for individual experiences.
© 2013 All rights reserved
Interview Findings
Current Challenges
It’s clear that demand far outweighs supply for services
We’ve also discovered that while the care needs of Special Populations, whom are more likely to suffer from multiple chronic conditions, generally increase in magnitude as they age in comparison to non-Special Populations, funding has not kept up, meaning that over time they are having to compromise either quality or quantity of care
We’ve learned that the lack of bridge funding means that some clients and families have to use ERs and LTCHs in times of crises. This may contribute to the use of ERs for non-emergencies, potentially contributing to ALC use of acute and post-acute care beds
We heard from the client families we met with that there isn’t enough respite support available to them, and that this is leaving them susceptible to burn-out and additional stress
We also heard that clients and their families sometimes feel alone as a result of what they perceive to be insufficient continuity in service planning
Funding for AL/SH projects has not increased for several years necessitating fewer spaces and fewer people served
System Challenges Funding shortages have contributed to a lack of access to care for Special Populations
47
© 2013 All rights reserved
Interview Findings
Special Populations require an increased focus on person-centered care that provides individuals and families input and choice into the type of care they receive
What Clients do not want in a Future Model
It’s been echoed in the Living Longer, Living Well report and elsewhere – clients and their families want choice, and they’re concerned that their ability to make the choices they believe are best may be compromised if they lose control of the process
Moreover, we heard concerns that the centralization of care management may hamper coordination between health service providers and between those providers and patient families
Concern was also expressed that waitlisted clients would be left to their own devices, not receiving the guidance the support they require. Accountability about managing the needs of waitlisted clients was noted as a particularly important requirement to mitigate against this
Finally, the highly specialized features of Special Populations were highlighted – these individuals are different than typical patients in that the focus of a future model ought to be about providing them with the individualized solutions designed to support them rather than fix them
Client Needs
48
© 2013 All rights reserved
Interview Findings
Special Populations require a flexible approach to coordinating needed services. Care Coordinators can play a central role if they work closely with Stakeholders
Key Success Factors to Implementation
Stakeholders whom we engaged by-and-large believe that clients and their families are most knowledgeable about their care needs and that individual-tailored funding would best position them to make choices about the services they need, which, as is often the case, may involve receiving services from more than one service provider
We heard repeatedly that the future role of the CCAC as Care Coordinator must have sufficient flexibility to allow service providers to work collaboratively to manage crises as they occur, and this is particularly important given that one of the outcomes may be reduced use of hospital ERs
Care Coordinators play a central role working closely with stakeholders in coordinating the necessary supports for clients that are awaiting services, especially considering the long waiting lists
The implementation of the Care Coordinator as system navigator must occur seamlessly so as to not impact clients
Implementation
49
© 2013 All rights reserved
Interview Findings – Summary
Special Populations and their families feel isolated, alone, frustrated and hopeless
Client Experience
Investigation of other models in terms of accessing service
No one wants a model in which there can be a barrier between a client/family and a potential provider. Those involved feel it will impact the ability of the individual and provider(s) to deploy innovative solutions
Models in which funding does not recognize the changing needs of the individual do not support the individual/family/caregiver for successful living in the community
Transition to adult services is traumatic for families and their children
There is fear of losing more control and independence
There is the fear that the medical model will be reinstated for Adults with Physical Disabilities who live in an Independent Living environment; they don’t want to be “cared for”. They are not sick. “Why doesn’t anyone value the ability to be maintained in the community as a productive member of society?” (Client)
Other Special Populations too want to be as independent as possible
Many older adults with physical disabilities had to fight for Independent Living and Direct Funding for Attendant Services– they don’t want to lose that
Money for Special Populations and their families is an ongoing issue
Most people with disabilities (all these Special Populations) are poor
Individuals/Families in crisis don’t receive the support they need
The current system has limited ability to respond to people and families in crisis or to be proactive in preventing crisis
50
© 2013 All rights reserved
Interview Findings – Summary Continued
Individuals are both grateful for and frustrated with their services
Client Experience
Relocation to access services
“There was no similar service in Guelph. When you think about all the years (14) I have tried different
things.” (Client)
There are people on waitlists for services that are provided in the South West LHIN from outside the
South West LHIN
There are people waitlisted for supportive housing willing to relocate from one city to another
Numerous individuals told us they moved to London for the services
The impact they have
“I had honestly forgotten that there are nice people.” (Client)
They shared their detailed programming and schedules and told us how it helped them cope in the
community
Q -“If you didn’t come here and you were still at home. How would life be different?” (Co-Lead)
A – “I would be probably be dead by now. “ (Client)
“Just being able to get groceries every week. That was a huge step up.” (Client)
And when they are not available
Sometimes families qualify for service but no workers are available in their geography
Parents say “Give me the money then; I can’t work because I have to look after my child.” (Parent)
Parents pay privately for a worker to attend Fanshawe with their medically fragile daughter
51
© 2013 All rights reserved
Current Clients – Medically Fragile Children
Client Stories
Parents of Medically Fragile Children suffer from lack of support and respite
What if your job required you to work 24 hours a day 7 days a week? What if when you did get a break, you had to be ‘on call’ and available to respond to an emergency? What if you never had a night of uninterrupted sleep? What if you were so exhausted that you could barely go on, but someone you love depended on you for their every want and need, year after year after year? What if you became too old, or too ill to care for them any longer? What if you were the parent of a medically fragile child? Who are these children? Client Example: Cerebral Palsy, spastic, quadriplegic, scoliosis, developmentally delayed, requires 24/7 total care, chest physio, uses a wheelchair and is non verbal. Mom has not worked outside of the home resulting is loss of income and lack of retirement funding. Lack of sleep takes its toll on parents who have not had a vacation in years. This is a Special Population whose caregivers have limited respite resources and will have even fewer respite and support options once their ‘child’ turns 18. The father of a 29 year old medically fragile daughter stated: “We love her but need a break to help us rejuvenate and perhaps have a holiday. The government seems to think there is a miraculous cure after our kids turn 18.” While there is often dollars available for families to contract out care providers, frequently there are no workers, or a very limited pool of workers available, especially in rural areas where staff have to travel long distance for what is often limited hours of work. The time spent searching for candidates puts enormous stress and pressure on families/caregivers. ..Continued on the next slide…
52
© 2013 All rights reserved
Current Clients – Medically Fragile Children Cont’d
Client Stories Resources who support families with medically fragile children must be specially trained; regular staff turnover puts additional strain families
These same staff require extensive, specialized training and this training must be repeated with every new person when staff turnover occurs, which is often frequent, and yet consistency of care is one of the things that has been reported as being extremely important to the families of medically fragile children. These children/young adults are sometimes unable to verbalize or express their needs, so having someone there that knows how to read the signs and communicate with them is critical. The mother of a medically fragile 10 year old describes it as a wild “quest to find others to care for our fragile and vulnerable child”. If a client is lucky enough to have a trained worker from a home care agency, there are often limits in place that affect the type of care that can be provided. For example, many agencies have a 40-50 lb lift restriction, so in order to lift or transfer this 10 year old client – who happens to be 55 lbs. – there would need to be 2 workers present. As parents/caregivers age, their worries only increase. What will happen to their children when they are no longer able to care for them themselves? Even Long-term care is not an option as they often don’t have the equipment, staff or resources necessary to provide adequate care to support the complex, extensive care required for this population. The other respite resources that exist do not have nurses or doctors on site and so parents must remain close to home and available to come and get their child in the event of an emergency. A mother writing advocating for additional supports for her daughter expressed that their family was continually “trying to find creative ways to not let our circumstances rob us of a fulfilling, happy family life.” Sounds like a fair request.
53
© 2013 All rights reserved
Current Clients – Acquired Brain Injury
Client Stories
The ability of Adults with Acquired Brain Injuries to access services is sometimes the difference between being homeless rather than being able to improve their lives
G is a young man who came from an abusive household. Unable to continue living at home he found himself living in rooming houses. He had been successful with a job but had had a devastating bike injury coming home from work one day and that was a major setback. Over the last couple of years he found himself often living on the streets. About six months ago he was severely beaten and in addition to a broken jaw, broken arm, broken leg, he also suffered a brain injury. While in hospital at Parkwood he was referred to Dale Brain Injury Services but G described it as Dale finding him. G had no resources. Dale took him into an assisted living environment, and subsidized his treatment until such time as he could complete his application for the Ontario Disability Support Program. The Dale staff helped him through all his paperwork, they help him with his instrumental activities of daily living and they are the difference between G being homeless and being on his way to a better life.
54
© 2013 All rights reserved
Current State Assessment
55
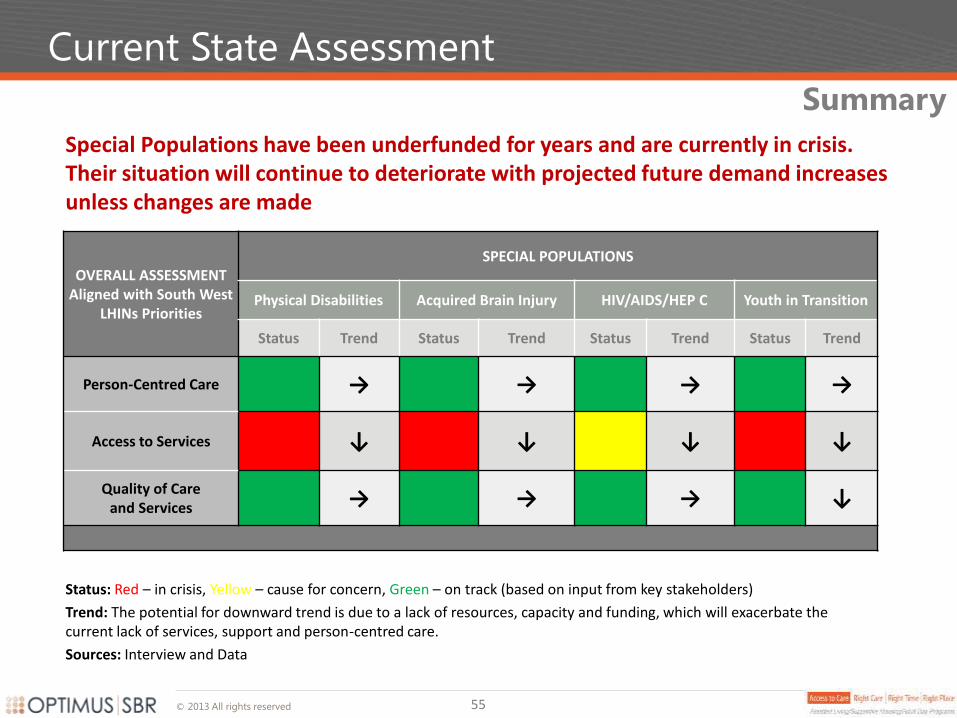
Special Populations have been underfunded for years and are currently in crisis. Their situation will continue to deteriorate with projected future demand increases unless changes are made
OVERALL ASSESSMENT Aligned with South West
LHINs Priorities
SPECIAL POPULATIONS
Physical Disabilities Acquired Brain Injury HIV/AIDS/HEP C Youth in Transition
Status Trend Status Trend Status Trend Status Trend
Person-Centred Care → → → →
Access to Services ↓ ↓ ↓ ↓
Quality of Care and Services → → → ↓
Summary
Status: Red – in crisis, Yellow – cause for concern, Green – on track (based on input from key stakeholders)
Trend: The potential for downward trend is due to a lack of resources, capacity and funding, which will exacerbate the current lack of services, support and person-centred care.
Sources: Interview and Data
Recommendations
Assisted Living/Supportive
Housing/Adult Day
Programs for
Special Populations
Table of Contents
1. Recommendation Guiding Principles
2. Recommendation Summary
3. Key Recommendations by Area
1. Person-Centred Care
2. Access to Care
3. Role of the CCAC
4. Data and Evaluation
5. Education and Training
4. Key Recommendations by Population
1. Physical Disability
2. Acquired Brain Injury
3. HIV/AIDS/HEP C
4. Youth in Transition
5. Additional Recommendations
6. Implementation Considerations
Assisted Living/Supportive
Housing/Adult Day Programs
for
Special Populations
Recommendations
South West
© 2013 All rights reserved
Recommendations
58
Person-centered – the primary focus is on the population’s needs and their caregivers and
families
High-impact – focus on prioritiy issues such as limited access to services versus secondary
issues
Innovative and Flexibile – care models reflect the wide range of needs of
individuals/caregivers
Evidence-based – recommendations are based on evidence, data and research where
possible
Realistic – limited funding and potential for new investments are taken into account
CCAC Expanded Role – the expanded role of the CCAC is reflected in process related
recommendations
South West LHIN Alignment – recommendation categories align with the SW LHINs
performance areas of focus
Recommendations were driven by the following:
Guiding Principles
© 2013 All rights reserved
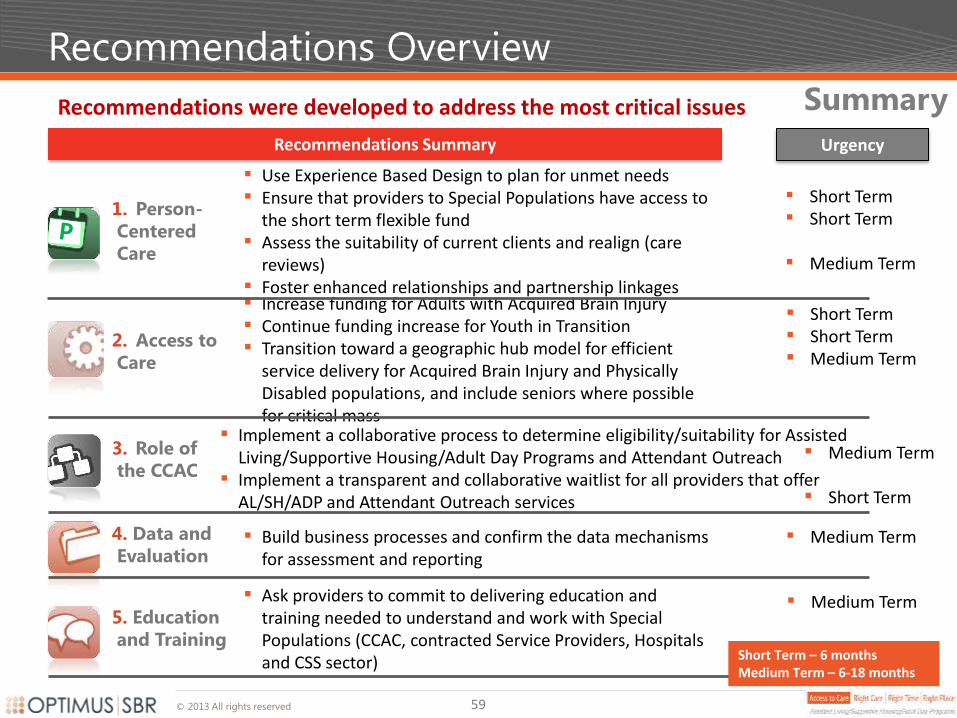
Recommendations Overview
Recommendations were developed to address the most critical issues
59
Increase funding for Adults with Acquired Brain Injury Continue funding increase for Youth in Transition Transition toward a geographic hub model for efficient
service delivery for Acquired Brain Injury and Physically Disabled populations, and include seniors where possible for critical mass
Recommendations Summary
Summary
1. Person-
Centered
Care
2. Access to
Care
4. Data and
Evaluation
3. Role of
the CCAC
Implement a collaborative process to determine eligibility/suitability for Assisted
Living/Supportive Housing/Adult Day Programs and Attendant Outreach Implement a transparent and collaborative waitlist for all providers that offer
AL/SH/ADP and Attendant Outreach services
Use Experience Based Design to plan for unmet needs Ensure that providers to Special Populations have access to
the short term flexible fund Assess the suitability of current clients and realign (care
reviews) Foster enhanced relationships and partnership linkages
Build business processes and confirm the data mechanisms for assessment and reporting
Ask providers to commit to delivering education and training needed to understand and work with Special Populations (CCAC, contracted Service Providers, Hospitals and CSS sector)
5. Education
and Training Short Term – 6 months Medium Term – 6-18 months
Urgency
Short Term Short Term
Medium Term
Short Term Short Term Medium Term
Medium Term
Short Term
Medium Term
Medium Term
© 2013 All rights reserved
Recommendations – Person-Centred Care
60
Realigning Special Populations with the use of a flex fund and deploying Experience Based Design should improve outcomes
All Special Populations
Use Experience Based Design as a framework to develop an approach to address unmet
needs. This will address the needs of those with highly individualized care, providing much
needed support for families and caregivers
Ensure that providers to Special Populations have access to the short term flexible fund in
order to:
avoid their inappropriate admission to ER or LTCHs; and
mitigate against family breakdown (this could include individualized funding models)
Conduct Care Reviews (Individual Assessments)
Assess the suitability of current clients and programs, and realign as required
Identify who could manage with just attendant outreach or in a cluster model vs. building based services
Examine where a lower cost Adult Day Program (ADP) solution can be used instead of Attendant Outreach
Where possible transition the individual to the most appropriate provider. The overall model of care should be more focused on providing supports to enable independent living where possible, and include some combination of all three types of services (AL/SH, Attendant Outreach and ADP), as required
© 2013 All rights reserved 61
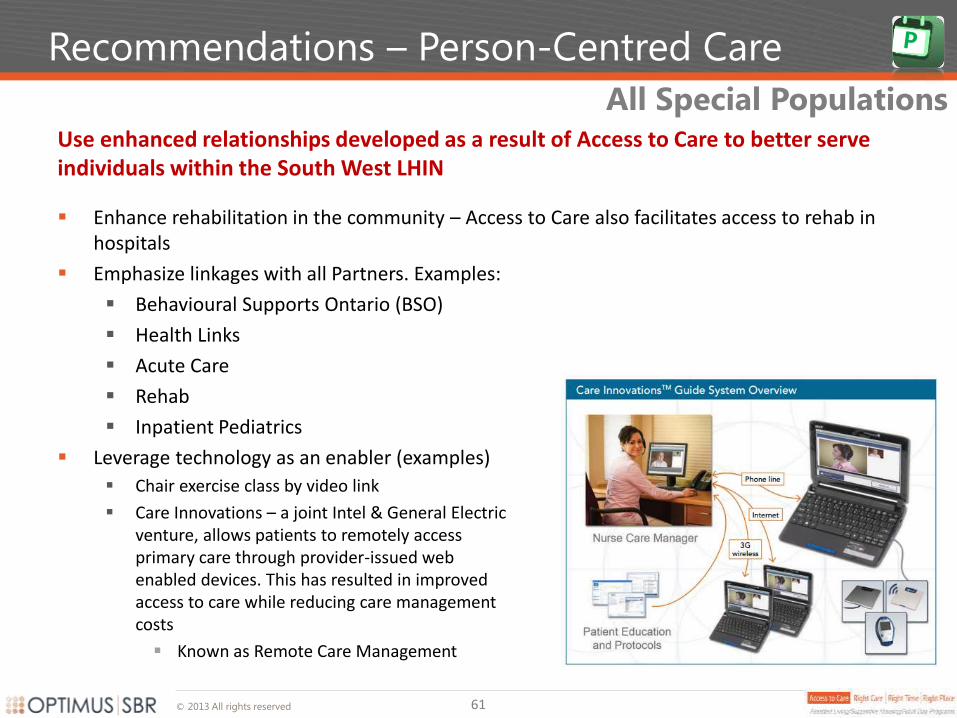
Use enhanced relationships developed as a result of Access to Care to better serve individuals within the South West LHIN
Enhance rehabilitation in the community – Access to Care also facilitates access to rehab in hospitals
Emphasize linkages with all Partners. Examples:
Behavioural Supports Ontario (BSO)
Health Links
Acute Care
Rehab
Inpatient Pediatrics
Leverage technology as an enabler (examples)
Chair exercise class by video link
Care Innovations – a joint Intel & General Electric venture, allows patients to remotely access primary care through provider-issued web enabled devices. This has resulted in improved access to care while reducing care management costs
Known as Remote Care Management
Recommendations – Person-Centred Care
All Special Populations
© 2013 All rights reserved
Recommendations – Access to Care
Acquired Brain Injury and Youth in Transition
Lack of funding necessitates the prioritization of those with the highest needs. Individuals with ABIs are at particular risk due to chronic underfunding
Increase funding and resources for Adults with Acquired Brain Injuries (ABI). The ABI and Medically Fragile/Technology Dependent (MFTD) populations are falling through the cracks and they have a general lack of alternatives. The exact amount of funding will be determined by the Care Reviews. The range of additional funding needed is provided in the financial projection scenarios
Prioritize Youth in Transition funding. Families whose children are MFTD, as well as the Care Coordinators and other clinical staff involved in their current care, expressed extreme concern about the lack of resources available to these children, particularly as they transition to adulthood and the organizations from whom they receive those services change. In light of recent funding, further work is needed to define the urgent needs of families for funding priorities. Consider implementing a working group with parents
Move toward a geographic hub for efficient service delivery. Transition toward a geographic hub model for efficient service delivery for ABI and Physical Disabilities populations, and include seniors where possible for critical mass
62
© 2013 All rights reserved
Recommendations – Access to Care
All Special Populations
Many providers use existing Assisted Living/Supportive Housing buildings as their base of operations for their outreach programs. This model is efficient and should not be changed
Gradually shift to geographic hubs from building based models, where possible. This will require substantial time and effort on the part of some providers to fully implement. Sufficient behaviour management training may be required
Continue to support existing Supportive Housing units for those needing 24/7 support
Expand the capacity for more intense rehabilitation to be provided in the community through CCAC and other appropriate providers. For example use IT to deliver rehab / maintenance programs
Connect Parkwood researchers/clinicians and CCAC Self Management Program Managers to explore innovative technology-based models of care for those with spinal cord injuries
Where possible transition the individual to the most appropriate provider – the CCAC and CSS providers to Adults with Disabilities share many long successful service plans to these individuals
There was investment in Attendant Outreach for Adults with Physical Disabilities in 2012/13. This is helping reduce but not eliminate service waitlists
63
© 2013 All rights reserved
Recommendations – Role of the CCAC
64
Due to the complexity and wide variance in needs of Special Populations, Subject Matter Experts must work together with the CCAC to define eligibility criteria
Implement a collaborative process to determine eligibility/suitability for AL/SH /ADP
and Attendant Outreach services. A collaborative team of CCAC and CSS colleagues
should form a working group to fully outline eligibility and prioritization for specific
programs, and determine business processes for comprehensive and
multidisciplinary/multi-partner (in some cases) assessments
Implement a transparent and collaborative waitlist with providers of Assisted
Living/Supportive Housing/Adult Day Programs and Attendant Outreach. The provision of
service for those waitlisted needs to be determined as part of a collaborative process
with the partners involved; in many instances, CCAC would require the assistance of other
partners to care for those on waitlist as they alone may not be able to meet the client’s
needs
Include Attendant Outreach Services and individuals with Hepatitis C in the Expanded
Role of the CCAC for AL/SH and ADP. Providers noted separate business processes for
these individuals as inefficient CCAC should include Attendant Outreach in its mix of coordinated services
All Special Populations
© 2013 All rights reserved
Recommendations – Role of the CCAC
Care Coordinators should work closely with Subject Matter Experts to provide the best care coordination options for Special Populations
While Assisted Living/Supportive Housing/Adult Day Programs providers have adapted the
use of the interRAI-CHA assessment tool (and are often familiar with the RAI-HC, CA and
PC), these instruments don’t, in isolation, help to develop the comprehensive service
plans some of these populations require. A collaborative eligibility, assessment and
planning process should be initiated to develop business processes that include subject
matter experts for assessment based on the individual’s needs and degree of specialization
(complexity)
John Gordon Home (JGH) is participating in the Common Measures Project. With the
support of the Ontario HIV/AIDS Treatment Network (OHTN), JGH and 5 other HIV/AIDS
Housing Programs in Ontario are implementing a common intake/assessment tool. The
tool has been approved and JGH begun implementation in March, 2013. A key benefit of
this tool is that it will allow JGH to follow residents after they leave and monitor their
situations
Assessment and Eligibility
65
© 2013 All rights reserved
Recommendations – Role of the CCAC
CCACs should use collaboration and ensure transparency to manage waitlists
CCACs should monitor and maintain a collaborative and transparent waitlist for Special Populations
In most cases, if CCAC services are appropriate to the client need, the CCAC should provide service to these individuals until such time as they can be transitioned to the most appropriate longer term provider. Where this is not possible the CCAC Care Coordinator should work with the most appropriate provider toward a short term solution for the individual
The provision of service for those waitlisted needs to be determined as part of a collaborative process with the partners involved; in many instances, CCAC would require the assistance of other partners to care for those on waitlist as they alone may not be able to meet the individual’s needs
The CCAC to facilitate collaborative “care conferencing,” including pre-discharge, with specific providers as necessary to ensure individuals waiting for service are connecting to supports while waiting
Waitlist Management
66
© 2013 All rights reserved
Recommendations – Data and Evaluation
67
Build business processes and confirm the data mechanisms for assessment and reporting (e.g. Adult Day Program data, etc.)
Identify the best data sources between the providers and the CCAC as business processes are built and confirmed
Propose a mandatory requirement for regular reporting to the LHIN using a ubiquitous reporting tool:
Current and Waitlisted Clients Numbers
Region of Residence
Client Age
Date of Application for Service
Date of Start of Service (if applicable)
Discharge Date (if applicable)
Program/Service Applied for
Primary Diagnosis/Client Classification (i.e. Acquired Brain Injury, Physically
Disabled, HIV/HEP C)
Recommended Frequency of Reporting: Quarterly
There is a need to implement new robust data collection and evaluation processes to leverage in making informed decisions about Special Populations going forward
All Special Populations
© 2013 All rights reserved
Recommendations – Education and Training
68
Leverage Human Resources and existing infrastructure in light of funding pressures
Ask providers to commit to delivering education and training needed to understand and work with Special Populations (CCAC, contracted Service Providers, Hospitals and CSS sector)
In depth education planning is required to assist Care Coodinators in their understanding of options for these populations, including available housing, programming, day programs, respite, etc. Education should be provided to providers also to understand CCAC role
Providers should explore communal training to reduce costs and build awareness of one another's capabilities using the Train the Trainer model
Providers should explore collaborative staff sharing models where possible to leverage economies of scale and account for potential staffing shortages
Where possible providers should explore the ability of their sector partners to train, assess, and provide ongoing support for their clients
Further explore respite and convalescent care options in all settings to leverage available resources and accommodate the needs of these special populations despite the reluctance of some parents of MF/TD young adults
All Special Populations
© 2013 All rights reserved
Recommendations – Education and Training
Since access to affordable, accessible housing is a barrier to receiving care in the community, explore the creation of a position within the South West LHIN for an expert on housing issues that can work across ministries to assist providers to come up with innovative solutions for those requiring housing. This would prevent premature admission to long term care
The South West LHIN has already initiated a dialogue with municipal housing providers. Assisted Living providers should be included in future discussions where appropriate in order to help develop housing solutions
Encourage any municipalities who have not opted to continue with Ontario Renovates to reconsider their decision in order to improve access for residents
Further explore respite and convalescent care options in all settings to leverage available resources and accommodate the needs of these special populations despite the reluctance of some parents of MF/TD young adults
Specific expertise on housing for Adults with Physical Disabilities is needed to address a growing issue driven primarily by a lack of Assisted Living/Supportive Housing
People with Physical Disabilities
69
© 2013 All rights reserved
Population Specific Recommendations
Those Adults with Physical Disabilities who are accustomed to independent living do not wish to be “medicalized”
That those Adults with Physical Disabilities who are currently on Direct Funding not be included in the Expanded Role of the CCAC unless they have a need to access professional services
Ensure access to Adult Day Programs for Adults with Physical Disabilities who wish to participate
Maintaining as much independence as possible is key to maximizing the quality of life for Adults with Physical Disabilities
People with Physical Disabilities
70
© 2013 All rights reserved
Population Specific Recommendations
Acquired Brain Injury should become a priority group within specialized populations. Acquired Brain Injury is such a specialty that lack of appropriate supports often results in the Acquired Brain Injury client being inappropriately placed in long term care, ending up homeless or incarcerated
Parkwood is hard-pressed to provide sufficient outreach until community providers have an opening and the Acquired Brain Injury Navigator for the South West LHIN spends two days per week at the jail looking out for brain injured clients
The South West LHIN should provide additional funding for Outreach in order to address the most severe injuries on the waitlist and prevent inappropriate placement
Currently providers often cobble together resources to serve people in crisis or on a waitlist. It will be essential to maintain this flexibility and not create business processes that get in the way of innovation
Continue to support the Adult Day Program for Acquired Brain Injury; deemed essential by its members to successful living in the community
Acquired Brain Injury population is so highly specialized that a lack of appropriate care impacts other parts of the healthcare system
Acquired Brain Injury
71
© 2013 All rights reserved
Population Specific Recommendations
It is recommended that the South West LHIN support JGH as they pursue current research projects
Transition Housing/Care is a relatively new service model. JGH is participating in two research projects to quantify and assess its benefits
The Transitional Housing Study is a multi-site community-based pilot study that aims to understand the individual and structural factors relevant to ‘housing readiness’ among persons living with HIV/AIDS (PHA), the range of support services and practices that best enhance ‘housing readiness’, and the changing needs of PHAs throughout residency. Preliminary findings indicate that three key services provided by transitional housing programs that encouraged housing readiness among participants include: management of HIV drug therapies; personal assistance with appointments; and service referrals
The second research project is the Common Measures Project mentioned previously
JGH to report to South West LHIN quarterly on the demand for housing that they have been unable to meet for future transitional housing planning
Recognize the importance of the values of GIPA and MIPA: greater involvement and meaningful involvement of PHAs and the role PHAs play in the governance, leadership and activities in the sector, also known as ‘Nothing About Us Without Us’
The John Gordon Home is currently looking at how to address the housing issues for the HIV/AID/HEP C populations
HIV/AIDS/HEP C
72
© 2013 All rights reserved
Population Specific Recommendations
More comprehensive discharge planning - don’t just refer to one provider but wrap the person in the centre with the support they require
This population may include those that are developmentally delayed as well as medically complex
Human resources are a concern with this population. Families experience continual retraining of support workers for their children with complex conditions. In some instances even though they are eligible for service they cannot find staff in their geographic location
In some circumstances parents have been so desperate for support they have requested that the money allowed to purchase services be redirected to them to help with overall household expenses and the cost of caregiving by the parent. Explore individualized funding models for these life long conditions with the flexibility for parents to purchase what they need
The need for respite for these families is significant. Kids Country Club provides respite for those until they are 18 and parents whose children are treated at CPRI benefit from their admission with time free from caregiving. After that no respite is available for these families unless it is delivered in complex and continuing care or long-term care. The parents and children are reluctant to use these options
Individualized Funding models should be explored to mitigate the lack of resources and funding for the Special Populations, whom typically fall through the cracks
Youth in Transition
73
© 2013 All rights reserved
Population Specific Recommendations
To assist with future service planning for the MF/TD population at all ages, additional data and information needs to be collected by CCAC and CSS providers
College\university students don't have the same support as younger kids at school. The education assistance that are in the classroom also go away at 18 or after 7 years of high school (or 21). Further consider ways to support college and university students
Increase the number of day program spaces and other respite services where possible
Assess innovative Housing models – specific suggestions for innovative housing models were presented during these consultations. It would be of benefit to communities to further investigate the feasibility of these models and how the CCAC and CSS providers can better support these families such as:
Additional group homes Parents offered to buy a home for their children with CCAC or other staff supports Use wing of an existing facility with specialized staff Individualized funding
Families/Caregivers need additional supports for Medically Fragile/technology Dependent Youth who age into adults at home
Youth in Transition
74
© 2013 All rights reserved
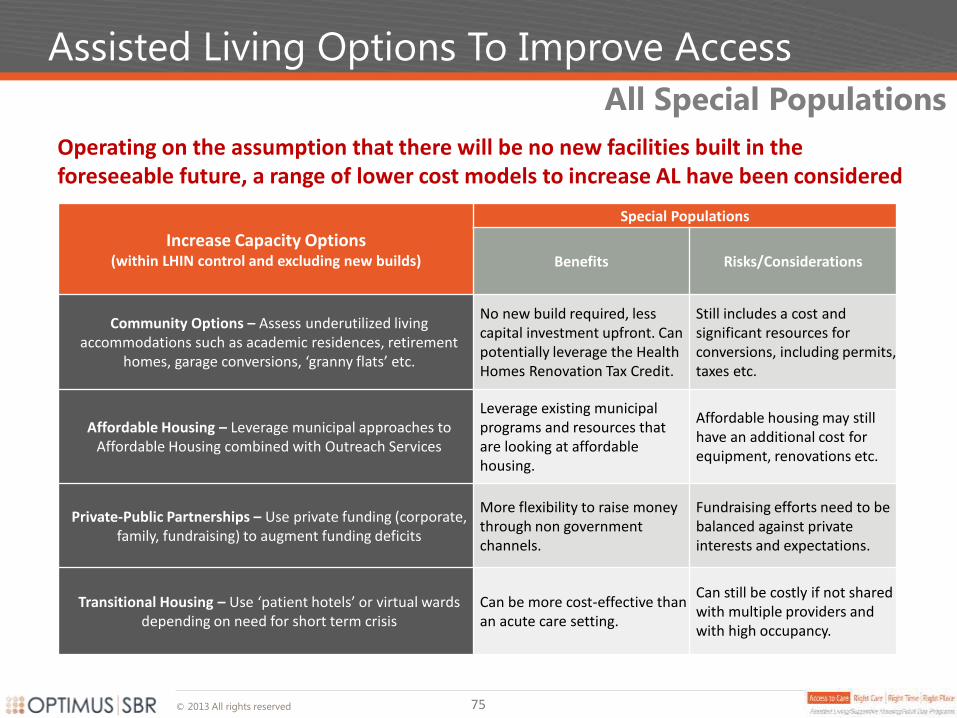
Assisted Living Options To Improve Access
Operating on the assumption that there will be no new facilities built in the foreseeable future, a range of lower cost models to increase AL have been considered
Increase Capacity Options
(within LHIN control and excluding new builds)
Special Populations
Benefits Risks/Considerations
Community Options – Assess underutilized living accommodations such as academic residences, retirement
homes, garage conversions, ‘granny flats’ etc.
No new build required, less capital investment upfront. Can potentially leverage the Health Homes Renovation Tax Credit.
Still includes a cost and significant resources for conversions, including permits, taxes etc.
Affordable Housing – Leverage municipal approaches to Affordable Housing combined with Outreach Services
Leverage existing municipal programs and resources that are looking at affordable housing.
Affordable housing may still have an additional cost for equipment, renovations etc.
Private-Public Partnerships – Use private funding (corporate, family, fundraising) to augment funding deficits
More flexibility to raise money through non government channels.
Fundraising efforts need to be balanced against private interests and expectations.
Transitional Housing – Use ‘patient hotels’ or virtual wards depending on need for short term crisis
Can be more cost-effective than an acute care setting.
Can still be costly if not shared with multiple providers and with high occupancy.
All Special Populations
75
© 2013 All rights reserved
Additional Recommendations
Other opportunities to improve the provision of services to Special Populations exist despite the reality that increasing access and system capacity remain the primary issues
All Special Populations
Use various models of community-based Restorative and Rehabilitative Care
and deploy technology innovatively to maintain individuals in their own
homes for as long as possible
Use Day Programming models with appropriately skilled staff and activities to
create appropriate wrap around supports for successful community living
Define Crisis Prevention roles amongst partners so that there is increased
collaboration to problem-solve in times of crises. Include transitional housing
solutions
More effective navigation support and tools for Special Populations and their
families/caregivers, especially during transition to adulthood
Improve Transportation options to access community services, including rural
settings
Additional Recommendations Common to ALL Special Populations
76
© 2013 All rights reserved
Recommendations – Implementation
Collaboration – Include provider partners and consumers at the table for a transparent and
collaborative approach that is person-centred and links the transitions across the continuum of
care
Specialized Resources – Explore where specialistis among the South West LHIN providers,
CCAC and representatives from other Ministries would be beneficial
Leverage Existing Resources – Train other providers on Special Populations and continue using
respite supports in Long Term Care
Align with other Inititiatives – Identify dependencies and linkages with other
iniatitives/programs
Deploy IT – Identify further e-enablers and proceed with ER Notification for CSS clients and
two way communication strategy as planned
Metrics – Move forward with considerable thought on agreed upon metrics that meaure the
success of the implementation of these recommendations, considering ALC is not currently
used
The following should be considered during implementation:
Successful implementation of creative solutions to care for these highly specialized populations requires that partners, individuals and families be at the planning table
Considerations
77
Implementation
Assisted Living/Supportive
Housing/Adult Day Programs for
Special Populations Final Report
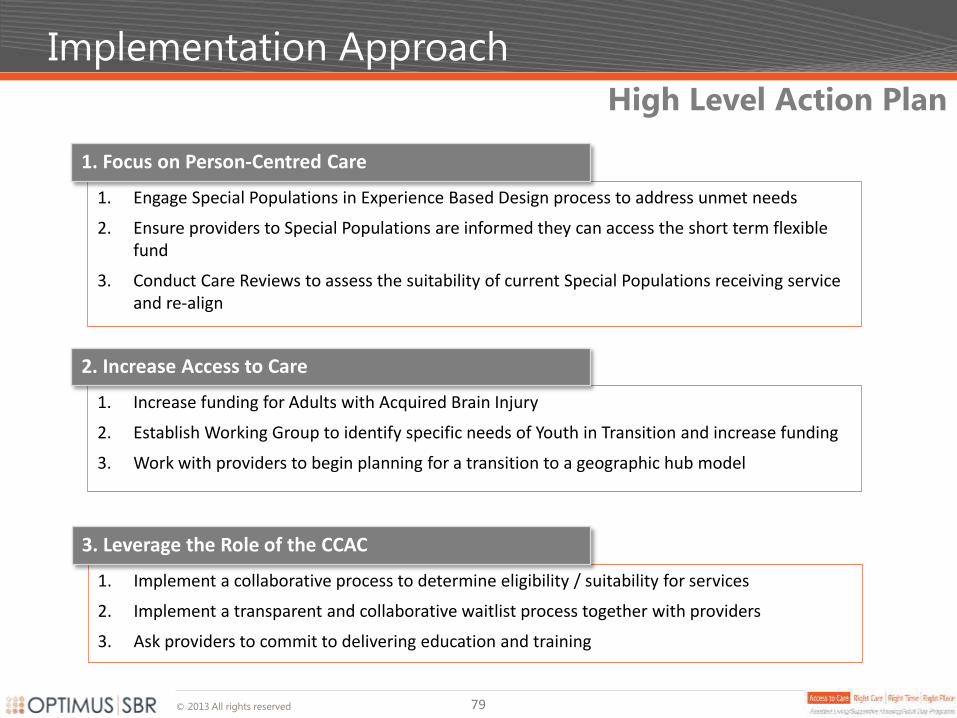
© 2013 All rights reserved
Implementation Approach
79
1. Engage Special Populations in Experience Based Design process to address unmet needs
2. Ensure providers to Special Populations are informed they can access the short term flexible fund
3. Conduct Care Reviews to assess the suitability of current Special Populations receiving service and re-align
1. Focus on Person-Centred Care
1. Increase funding for Adults with Acquired Brain Injury
2. Establish Working Group to identify specific needs of Youth in Transition and increase funding
3. Work with providers to begin planning for a transition to a geographic hub model
2. Increase Access to Care
1. Implement a collaborative process to determine eligibility / suitability for services
2. Implement a transparent and collaborative waitlist process together with providers
3. Ask providers to commit to delivering education and training
3. Leverage the Role of the CCAC
High Level Action Plan
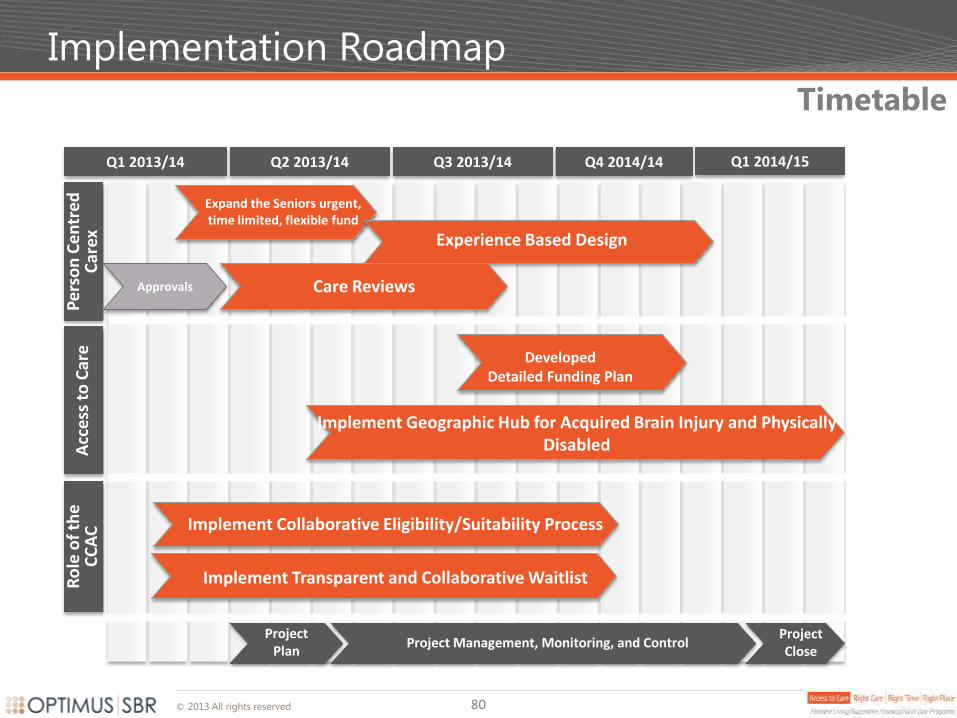
© 2013 All rights reserved
Implementation Roadmap
80
Q1 2013/14 Q2 2013/14 Q3 2013/14 Q4 2014/14 Q1 2014/15
Pe
rso
n C
en
tre
d
Car
ex
Project Close
Project Management, Monitoring, and Control Project
Plan
Expand the Seniors urgent, time limited, flexible fund
Acc
ess
to
Car
e
Implement Collaborative Eligibility/Suitability Process
Approvals
Experience Based Design
Care Reviews
Implement Geographic Hub for Acquired Brain Injury and Physically Disabled
Developed Detailed Funding Plan
Timetable R
ole
of
the
C
CA
C
Implement Transparent and Collaborative Waitlist
Appendix – Future State
Assisted Living/Supportive
Housing/Adult Day Programs for
Special Populations Final Report
Table of Contents
0. Preliminaries
1. Executive Summary
2. Current State
3. Recommendations
4. Implementation
5. Appendix Future State
1. Methodology
2. Projections for Physical Disabilities
3. Projections for Acquired Brain Injury
4. Projections for HIV/AIDS
5. Costing Summary
Assisted Living/Supportive
Housing/Adult Day Programs
for
Special Populations Final Report
South West
© 2013 All rights reserved
Future State Disclaimer
Important Disclaimer for Forecasting Future Demand
Due to the lack of a comprehensive reporting mechanism, projecting the future demand for services by Special Populations is challenging.
In the absence of more accurate data, the utilized methodology provides the best means in forecasting future service requirements.
Regardless of the potential margin of error of the forecasted numbers, the fact remains that there is significantly more demand than supply in programs and services for Special Populations.
A PDSA approach for the highest needs populations appears to be the most practical way to begin to address the issue of access to care.
*The Institute of Healthcare Improvement defines PDSA (Plan-Do-Study-Act) as way to implement change by developing a plan to test the change (Plan), carrying out the test (Do), observing and learning from the consequences (Study), and determining what modifications should be made to the test (Act).
83
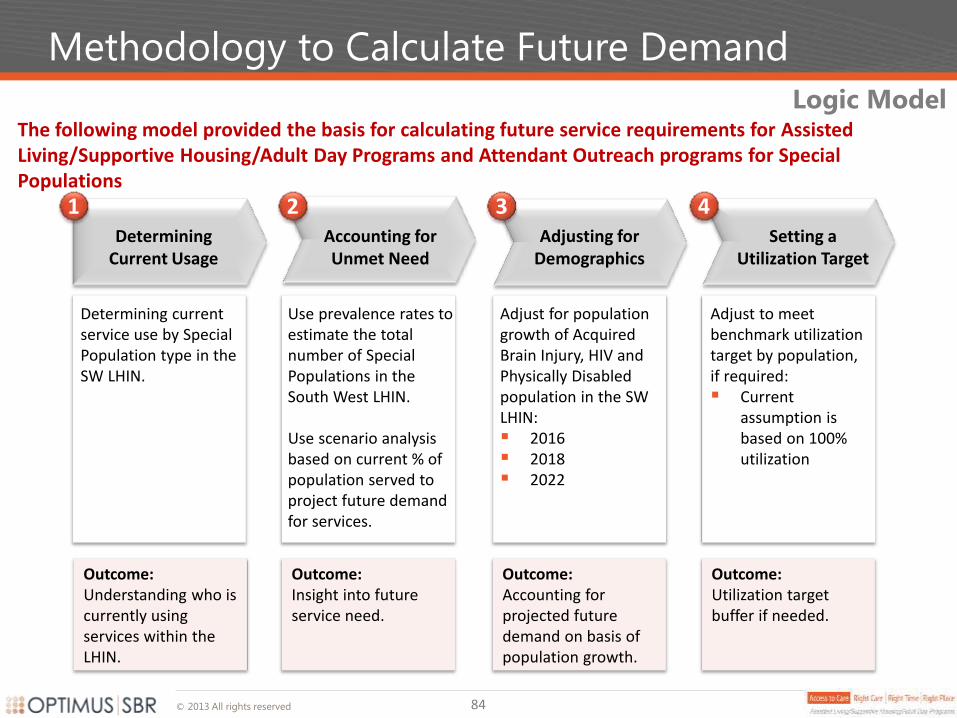
© 2013 All rights reserved
Outcome: Understanding who is currently using services within the LHIN.
Methodology to Calculate Future Demand
The following model provided the basis for calculating future service requirements for Assisted Living/Supportive Housing/Adult Day Programs and Attendant Outreach programs for Special Populations
1 2 4 Setting a
Utilization Target
Adjust to meet benchmark utilization target by population, if required: Current
assumption is based on 100% utilization
Adjusting for Demographics
Adjust for population growth of Acquired Brain Injury, HIV and Physically Disabled population in the SW LHIN: 2016 2018 2022
3
Use prevalence rates to estimate the total number of Special Populations in the South West LHIN. Use scenario analysis based on current % of population served to project future demand for services.
Accounting for Unmet Need
Determining current service use by Special Population type in the SW LHIN.
Determining Current Usage
Outcome: Insight into future service need.
Outcome: Accounting for projected future demand on basis of population growth.
Outcome: Utilization target buffer if needed.
Logic Model
84
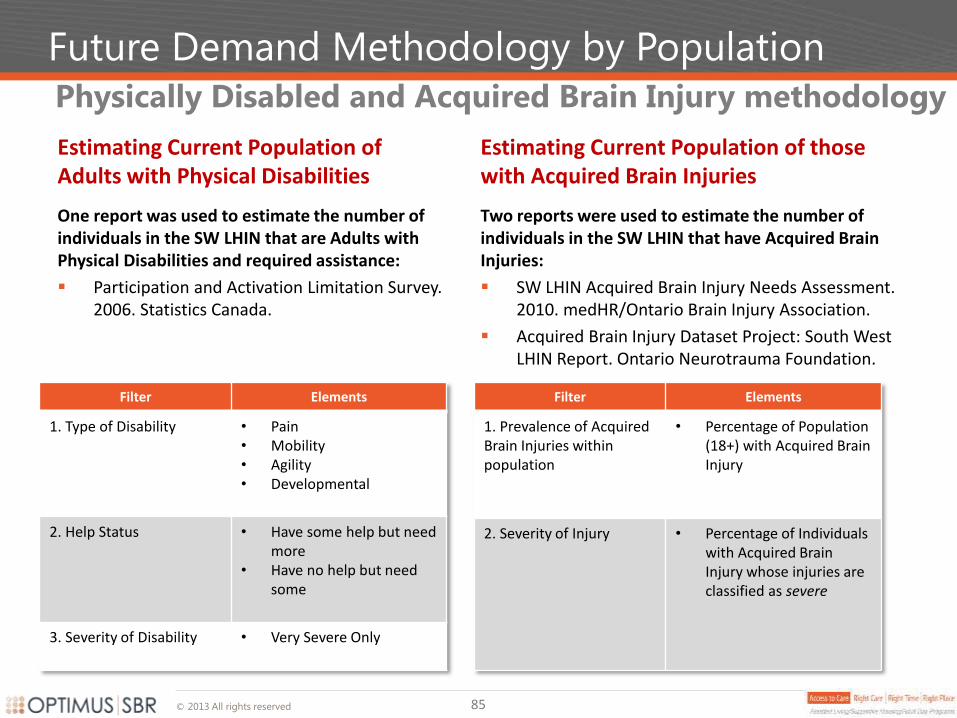
© 2013 All rights reserved
Future Demand Methodology by Population
Estimating Current Population of Adults with Physical Disabilities
One report was used to estimate the number of individuals in the SW LHIN that are Adults with Physical Disabilities and required assistance:
Participation and Activation Limitation Survey. 2006. Statistics Canada.
Physically Disabled and Acquired Brain Injury methodology
Filter Elements
1. Type of Disability • Pain • Mobility • Agility • Developmental
2. Help Status • Have some help but need more
• Have no help but need some
3. Severity of Disability • Very Severe Only
Estimating Current Population of those with Acquired Brain Injuries
Two reports were used to estimate the number of individuals in the SW LHIN that have Acquired Brain Injuries:
SW LHIN Acquired Brain Injury Needs Assessment. 2010. medHR/Ontario Brain Injury Association.
Acquired Brain Injury Dataset Project: South West LHIN Report. Ontario Neurotrauma Foundation.
Filter Elements
1. Prevalence of Acquired Brain Injuries within population
• Percentage of Population (18+) with Acquired Brain Injury
2. Severity of Injury • Percentage of Individuals with Acquired Brain Injury whose injuries are classified as severe
85
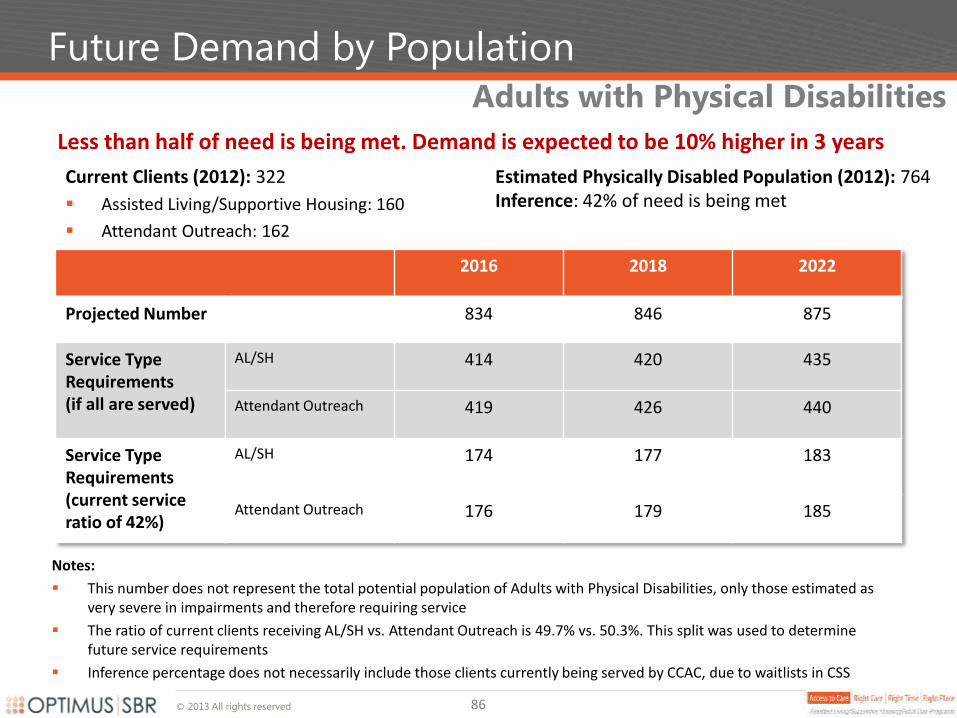
© 2013 All rights reserved
Future Demand by Population
Notes:
This number does not represent the total potential population of Adults with Physical Disabilities, only those estimated as very severe in impairments and therefore requiring service
The ratio of current clients receiving AL/SH vs. Attendant Outreach is 49.7% vs. 50.3%. This split was used to determine future service requirements
Inference percentage does not necessarily include those clients currently being served by CCAC, due to waitlists in CSS
Less than half of need is being met. Demand is expected to be 10% higher in 3 years
Adults with Physical Disabilities
2016 2018 2022
Projected Number 834 846 875
Service Type Requirements (if all are served)
AL/SH 414 420 435
Attendant Outreach 419 426 440
Service Type Requirements (current service ratio of 42%)
AL/SH 174 177 183
Attendant Outreach 176 179 185
Current Clients (2012): 322
Assisted Living/Supportive Housing: 160
Attendant Outreach: 162
Estimated Physically Disabled Population (2012): 764 Inference: 42% of need is being met
86
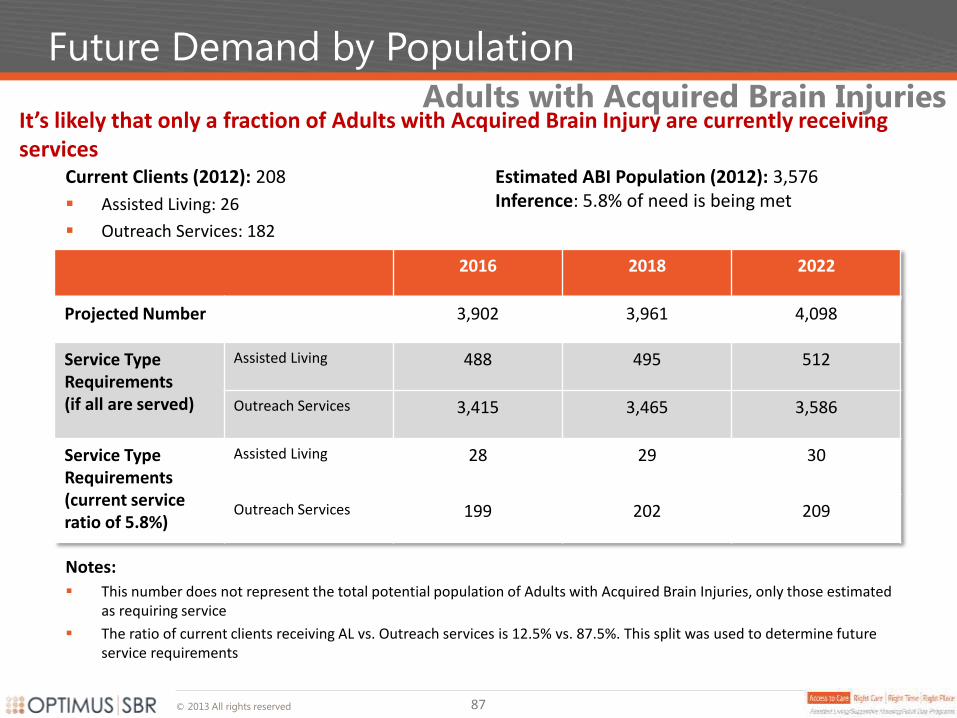
© 2013 All rights reserved
Future Demand by Population
It’s likely that only a fraction of Adults with Acquired Brain Injury are currently receiving services
Adults with Acquired Brain Injuries
2016 2018 2022
Projected Number 3,902 3,961 4,098
Service Type Requirements (if all are served)
Assisted Living 488 495 512
Outreach Services 3,415 3,465 3,586
Service Type Requirements (current service ratio of 5.8%)
Assisted Living 28 29 30
Outreach Services 199 202 209
Current Clients (2012): 208
Assisted Living: 26
Outreach Services: 182
Estimated ABI Population (2012): 3,576 Inference: 5.8% of need is being met
Notes:
This number does not represent the total potential population of Adults with Acquired Brain Injuries, only those estimated as requiring service
The ratio of current clients receiving AL vs. Outreach services is 12.5% vs. 87.5%. This split was used to determine future service requirements
87
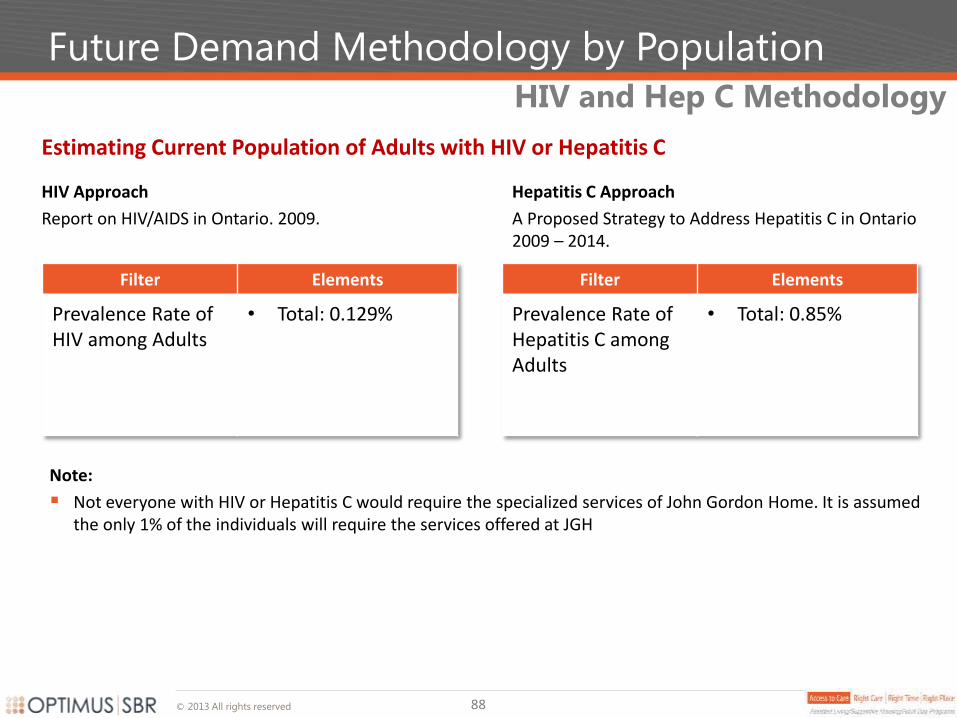
© 2013 All rights reserved
Future Demand Methodology by Population
Estimating Current Population of Adults with HIV or Hepatitis C
HIV Approach
Report on HIV/AIDS in Ontario. 2009.
HIV and Hep C Methodology
Filter Elements
Prevalence Rate of HIV among Adults
• Total: 0.129%
Hepatitis C Approach
A Proposed Strategy to Address Hepatitis C in Ontario 2009 – 2014.
Filter Elements
Prevalence Rate of Hepatitis C among Adults
• Total: 0.85%
Note:
Not everyone with HIV or Hepatitis C would require the specialized services of John Gordon Home. It is assumed the only 1% of the individuals will require the services offered at JGH
88
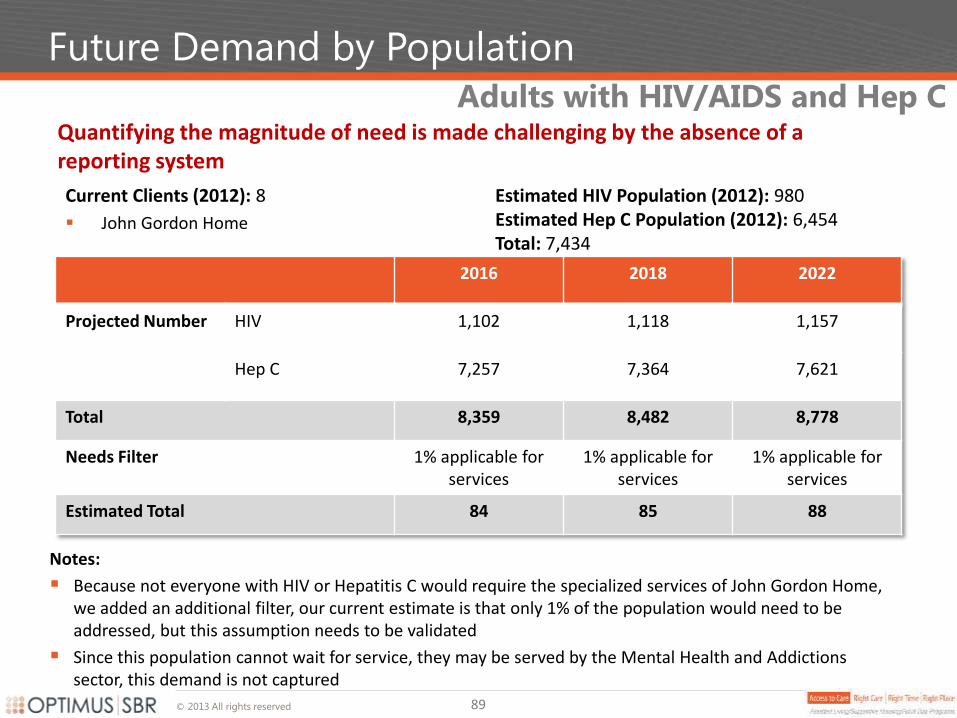
© 2013 All rights reserved
Future Demand by Population
Quantifying the magnitude of need is made challenging by the absence of a reporting system
Adults with HIV/AIDS and Hep C
2016 2018 2022
Projected Number HIV 1,102 1,118 1,157
Hep C 7,257 7,364 7,621
Total 8,359 8,482 8,778
Needs Filter 1% applicable for services
1% applicable for services
1% applicable for services
Estimated Total 84 85 88
Current Clients (2012): 8
John Gordon Home
Estimated HIV Population (2012): 980 Estimated Hep C Population (2012): 6,454 Total: 7,434
Notes:
Because not everyone with HIV or Hepatitis C would require the specialized services of John Gordon Home, we added an additional filter, our current estimate is that only 1% of the population would need to be addressed, but this assumption needs to be validated
Since this population cannot wait for service, they may be served by the Mental Health and Addictions sector, this demand is not captured
89
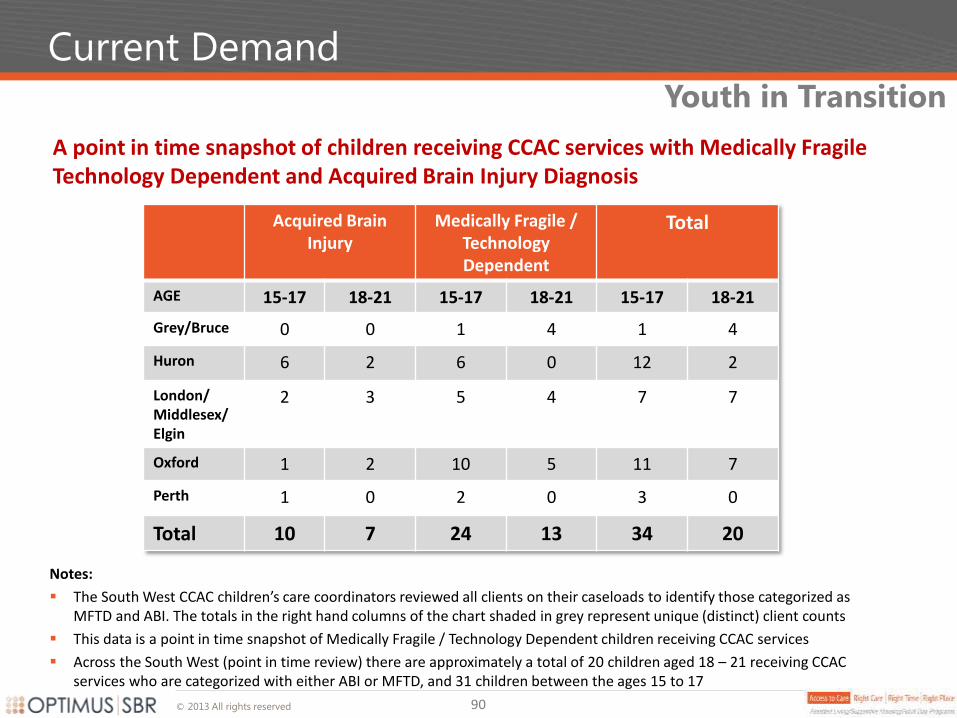
© 2013 All rights reserved
Current Demand
A point in time snapshot of children receiving CCAC services with Medically Fragile Technology Dependent and Acquired Brain Injury Diagnosis
Youth in Transition
Acquired Brain Injury
Medically Fragile / Technology Dependent
Total
AGE 15-17 18-21 15-17 18-21 15-17 18-21
Grey/Bruce 0 0 1 4 1 4
Huron 6 2 6 0 12 2
London/ Middlesex/ Elgin
2 3 5 4 7 7
Oxford 1 2 10 5 11 7
Perth 1 0 2 0 3 0
Total 10 7 24 13 34 20
Notes:
The South West CCAC children’s care coordinators reviewed all clients on their caseloads to identify those categorized as MFTD and ABI. The totals in the right hand columns of the chart shaded in grey represent unique (distinct) client counts
This data is a point in time snapshot of Medically Fragile / Technology Dependent children receiving CCAC services
Across the South West (point in time review) there are approximately a total of 20 children aged 18 – 21 receiving CCAC services who are categorized with either ABI or MFTD, and 31 children between the ages 15 to 17
90
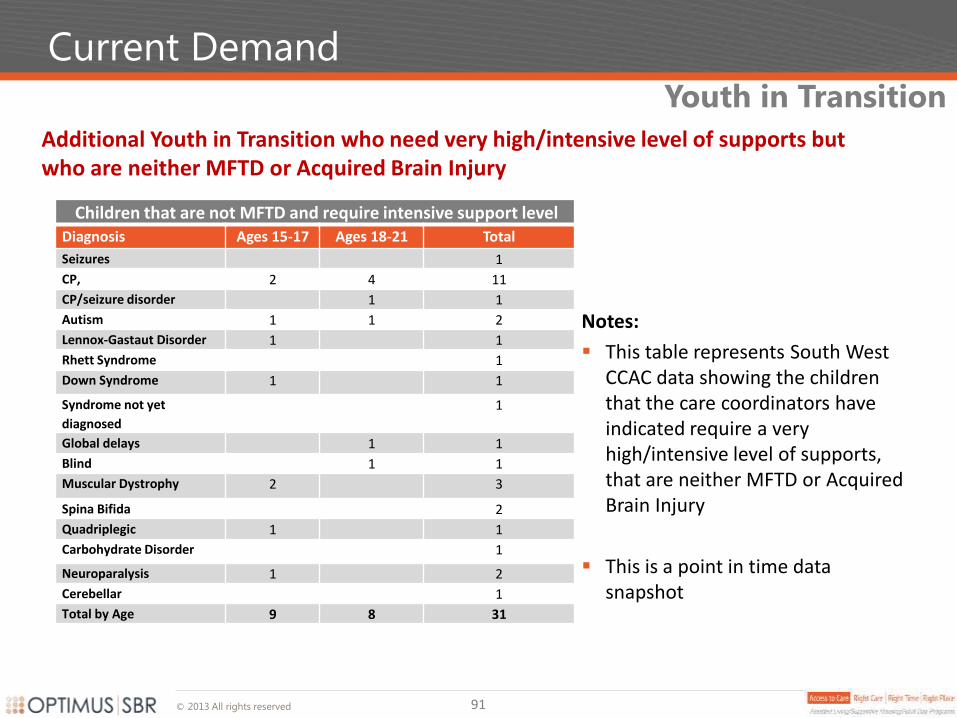
© 2013 All rights reserved
Current Demand
Additional Youth in Transition who need very high/intensive level of supports but who are neither MFTD or Acquired Brain Injury
Youth in Transition
Notes:
This table represents South West CCAC data showing the children that the care coordinators have indicated require a very high/intensive level of supports, that are neither MFTD or Acquired Brain Injury
This is a point in time data snapshot
Children that are not MFTD and require intensive support level Diagnosis Ages 15-17 Ages 18-21 Total
Seizures 1
CP, 2 4 11
CP/seizure disorder 1 1
Autism 1 1 2
Lennox-Gastaut Disorder 1 1
Rhett Syndrome 1
Down Syndrome 1 1
Syndrome not yet
diagnosed
1
Global delays 1 1
Blind 1 1
Muscular Dystrophy 2 3
Spina Bifida 2
Quadriplegic 1 1
Carbohydrate Disorder 1
Neuroparalysis 1 2
Cerebellar 1
Total by Age 9 8 31
91
© 2013 All rights reserved
Financial Projections
Financials projections for 2016, 2018 and 2022 have been made on the basis of 3 scenarios: 1. Maintaining the Status Quo; 2. Reducing the Service Waitlist; and 3. Servicing Total Projected Need. Some scenarios have multiple options
1. Maintaining the Status Quo
1. No Increase: Assumes that 2013 service levels are maintained
2. Population Increase: Assumes that service levels increase with the population growth of individuals 18 year of age and older
2. Population Increase + Waitlist Reduction
1. 25%: Assumes that service levels increase with the population growth of individuals 18 years of age and older, and additional resources are added to provide service to 25% of waitlisted individuals
2. 50%: Assumes that service levels increase with the population growth of individuals 18 years of age and older, and additional resources are added to provide service to 50% of waitlisted individuals
3. 100%: Assumes that service levels increase with the population growth of individuals 18 years of age and older, and additional resources are added to provide service to 100% of waitlisted individuals
3. Servicing Total Projected Need
1. All Need: Assumes that service levels are increased to meet all projected need
Scenario Overviews
92
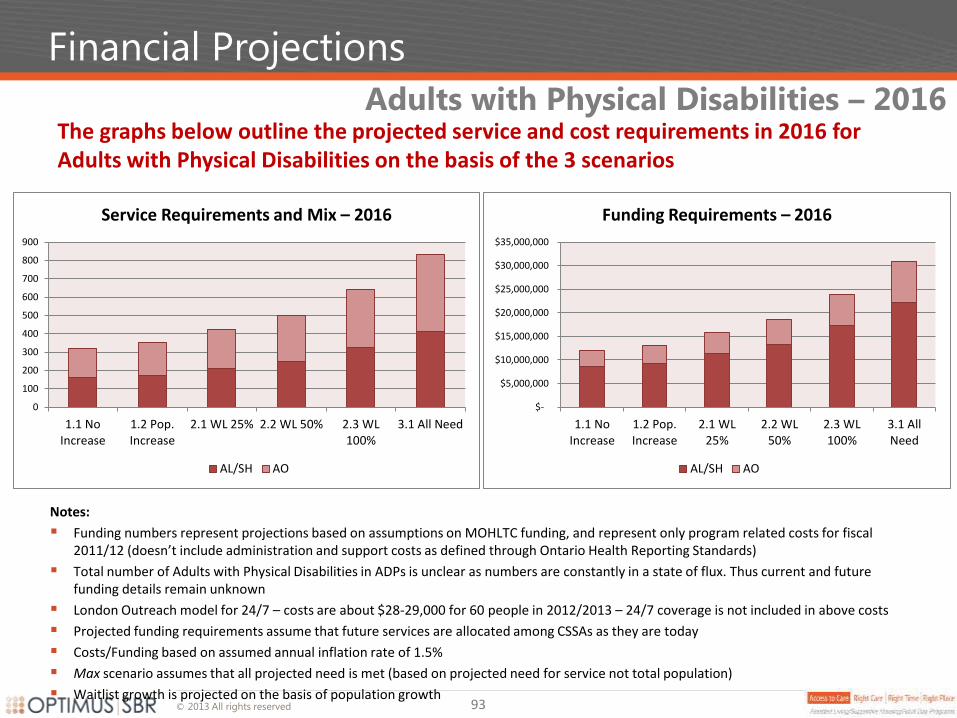
© 2013 All rights reserved
Financial Projections
The graphs below outline the projected service and cost requirements in 2016 for Adults with Physical Disabilities on the basis of the 3 scenarios
Adults with Physical Disabilities – 2016
0
100
200
300
400
500
600
700
800
900
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL 25% 2.2 WL 50% 2.3 WL100%
3.1 All Need
Service Requirements and Mix – 2016
AL/SH AO
$-
$5,000,000
$10,000,000
$15,000,000
$20,000,000
$25,000,000
$30,000,000
$35,000,000
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL25%
2.2 WL50%
2.3 WL100%
3.1 AllNeed
Funding Requirements – 2016
AL/SH AO
93
Notes:
Funding numbers represent projections based on assumptions on MOHLTC funding, and represent only program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Total number of Adults with Physical Disabilities in ADPs is unclear as numbers are constantly in a state of flux. Thus current and future funding details remain unknown
London Outreach model for 24/7 – costs are about $28-29,000 for 60 people in 2012/2013 – 24/7 coverage is not included in above costs
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Costs/Funding based on assumed annual inflation rate of 1.5%
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
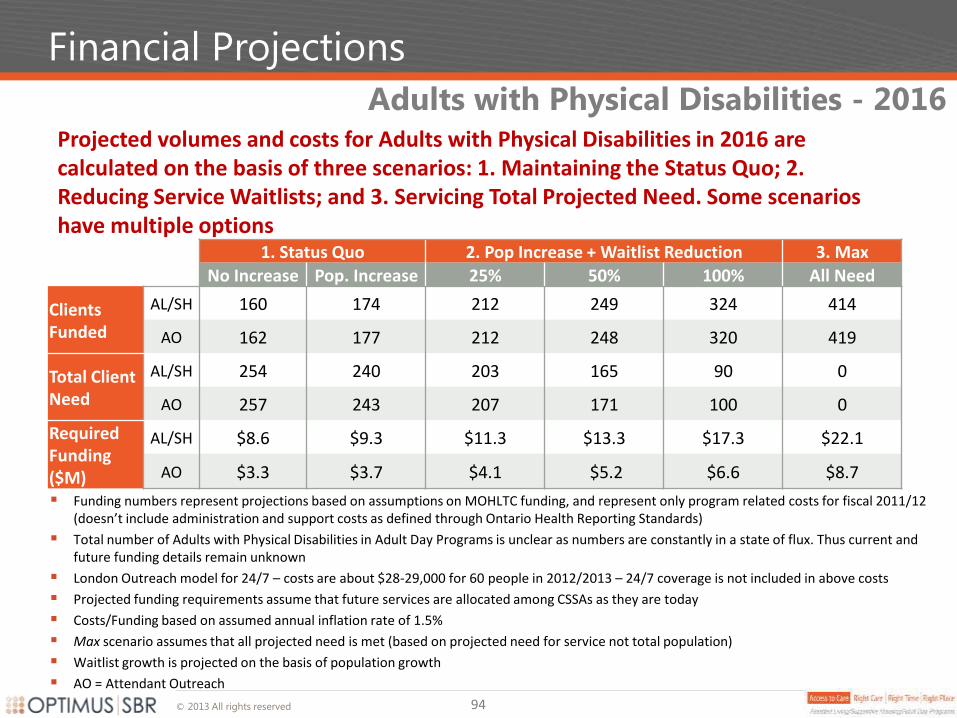
© 2013 All rights reserved
Financial Projections
94
Projected volumes and costs for Adults with Physical Disabilities in 2016 are calculated on the basis of three scenarios: 1. Maintaining the Status Quo; 2. Reducing Service Waitlists; and 3. Servicing Total Projected Need. Some scenarios have multiple options
Notes:
Funding numbers represent projections based on assumptions on MOHLTC funding, and represent only program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Total number of Adults with Physical Disabilities in Adult Day Programs is unclear as numbers are constantly in a state of flux. Thus current and future funding details remain unknown
London Outreach model for 24/7 – costs are about $28-29,000 for 60 people in 2012/2013 – 24/7 coverage is not included in above costs
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Costs/Funding based on assumed annual inflation rate of 1.5%
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
AO = Attendant Outreach
Adults with Physical Disabilities - 2016
1. Status Quo 2. Pop Increase + Waitlist Reduction 3. Max
No Increase Pop. Increase 25% 50% 100% All Need
Clients Funded
AL/SH 160 174 212 249 324 414
AO 162 177 212 248 320 419
Total Client Need
AL/SH 254 240 203 165 90 0
AO 257 243 207 171 100 0
Required Funding ($M)
AL/SH $8.6 $9.3 $11.3 $13.3 $17.3 $22.1
AO $3.3 $3.7 $4.1 $5.2 $6.6 $8.7
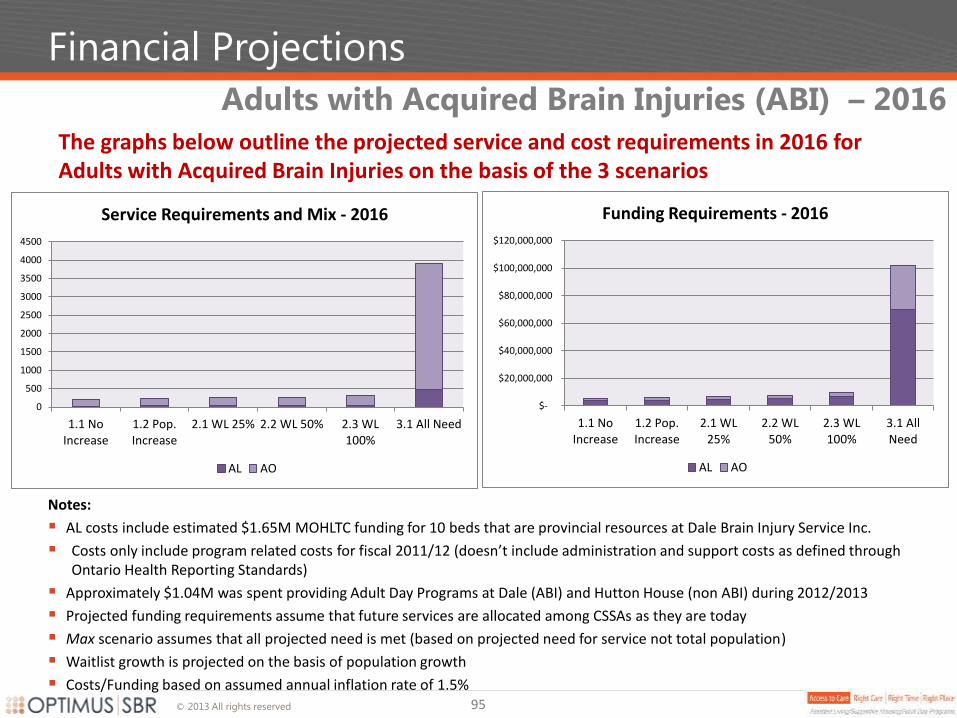
© 2013 All rights reserved
Financial Projections
The graphs below outline the projected service and cost requirements in 2016 for Adults with Acquired Brain Injuries on the basis of the 3 scenarios
Adults with Acquired Brain Injuries (ABI) – 2016
95
0
500
1000
1500
2000
2500
3000
3500
4000
4500
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL 25% 2.2 WL 50% 2.3 WL100%
3.1 All Need
Service Requirements and Mix - 2016
AL AO
$-
$20,000,000
$40,000,000
$60,000,000
$80,000,000
$100,000,000
$120,000,000
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL25%
2.2 WL50%
2.3 WL100%
3.1 AllNeed
Funding Requirements - 2016
AL AO
Notes:
AL costs include estimated $1.65M MOHLTC funding for 10 beds that are provincial resources at Dale Brain Injury Service Inc.
Costs only include program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Approximately $1.04M was spent providing Adult Day Programs at Dale (ABI) and Hutton House (non ABI) during 2012/2013
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
Costs/Funding based on assumed annual inflation rate of 1.5%
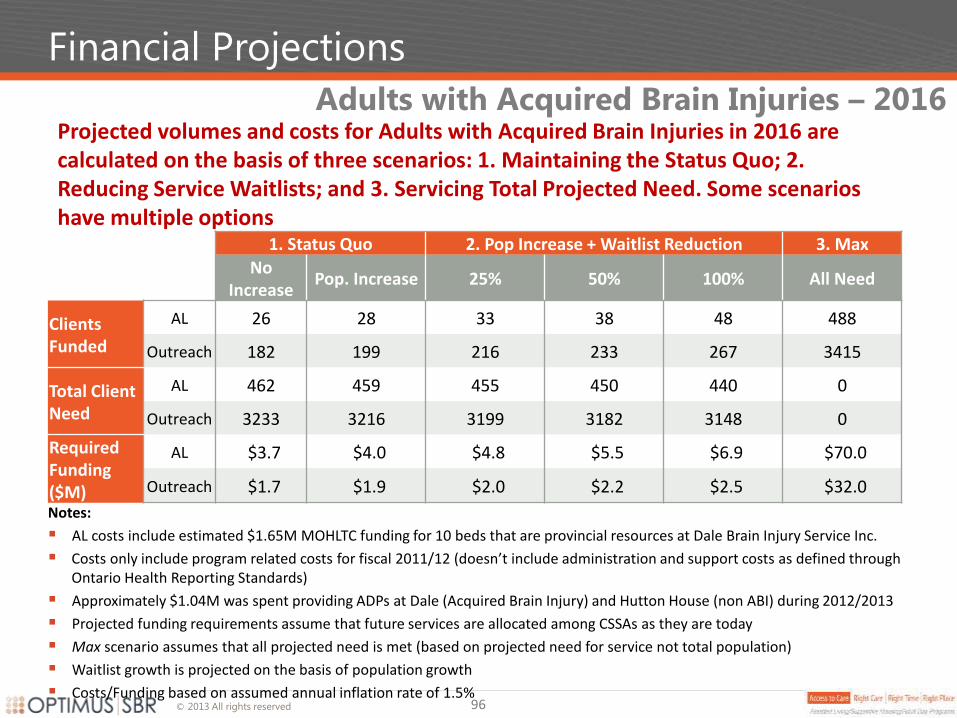
© 2013 All rights reserved
Financial Projections
96
Notes:
AL costs include estimated $1.65M MOHLTC funding for 10 beds that are provincial resources at Dale Brain Injury Service Inc.
Costs only include program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Approximately $1.04M was spent providing ADPs at Dale (Acquired Brain Injury) and Hutton House (non ABI) during 2012/2013
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
Costs/Funding based on assumed annual inflation rate of 1.5%
Projected volumes and costs for Adults with Acquired Brain Injuries in 2016 are calculated on the basis of three scenarios: 1. Maintaining the Status Quo; 2. Reducing Service Waitlists; and 3. Servicing Total Projected Need. Some scenarios have multiple options
1. Status Quo 2. Pop Increase + Waitlist Reduction 3. Max
No
Increase Pop. Increase 25% 50% 100% All Need
Clients Funded
AL 26 28 33 38 48 488
Outreach 182 199 216 233 267 3415
Total Client Need
AL 462 459 455 450 440 0
Outreach 3233 3216 3199 3182 3148 0
Required Funding ($M)
AL $3.7 $4.0 $4.8 $5.5 $6.9 $70.0
Outreach $1.7 $1.9 $2.0 $2.2 $2.5 $32.0
Adults with Acquired Brain Injuries – 2016
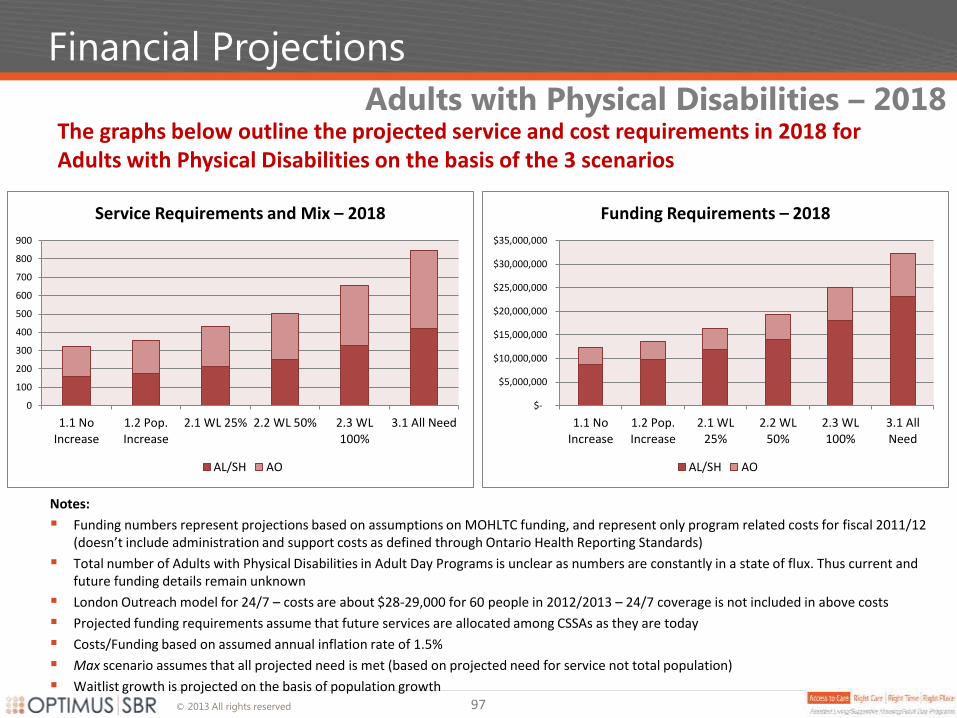
© 2013 All rights reserved
Financial Projections
The graphs below outline the projected service and cost requirements in 2018 for Adults with Physical Disabilities on the basis of the 3 scenarios
Adults with Physical Disabilities – 2018
0
100
200
300
400
500
600
700
800
900
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL 25% 2.2 WL 50% 2.3 WL100%
3.1 All Need
Service Requirements and Mix – 2018
AL/SH AO
$-
$5,000,000
$10,000,000
$15,000,000
$20,000,000
$25,000,000
$30,000,000
$35,000,000
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL25%
2.2 WL50%
2.3 WL100%
3.1 AllNeed
Funding Requirements – 2018
AL/SH AO
97
Notes:
Funding numbers represent projections based on assumptions on MOHLTC funding, and represent only program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Total number of Adults with Physical Disabilities in Adult Day Programs is unclear as numbers are constantly in a state of flux. Thus current and future funding details remain unknown
London Outreach model for 24/7 – costs are about $28-29,000 for 60 people in 2012/2013 – 24/7 coverage is not included in above costs
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Costs/Funding based on assumed annual inflation rate of 1.5%
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
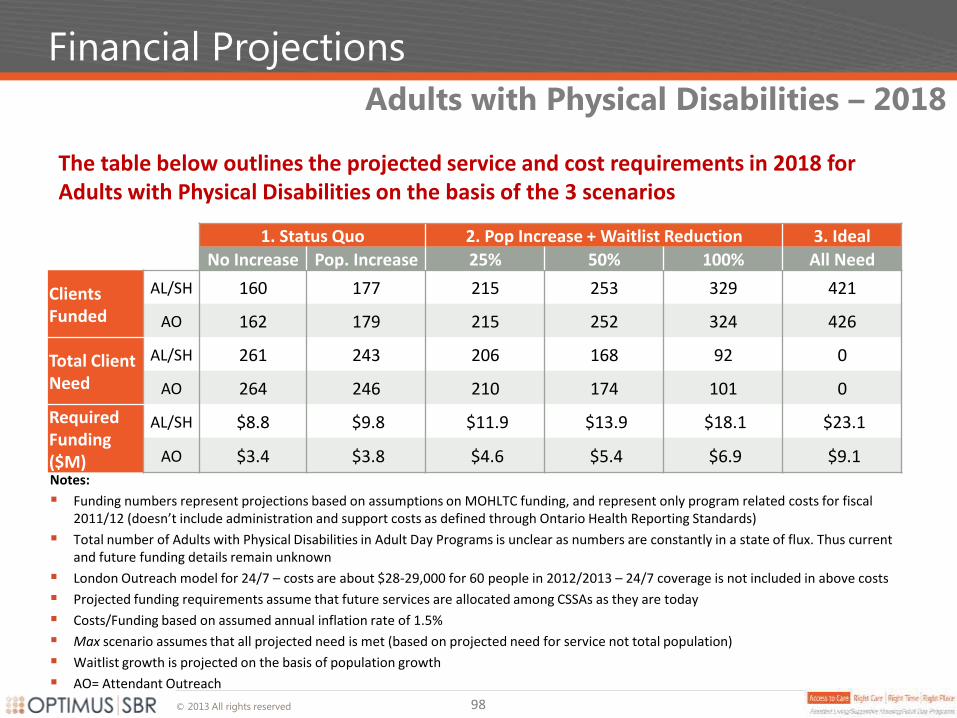
© 2013 All rights reserved
Financial Projections
The table below outlines the projected service and cost requirements in 2018 for Adults with Physical Disabilities on the basis of the 3 scenarios
Adults with Physical Disabilities – 2018
98
1. Status Quo 2. Pop Increase + Waitlist Reduction 3. Ideal
No Increase Pop. Increase 25% 50% 100% All Need
Clients Funded
AL/SH 160 177 215 253 329 421
AO 162 179 215 252 324 426
Total Client Need
AL/SH 261 243 206 168 92 0
AO 264 246 210 174 101 0
Required Funding ($M)
AL/SH $8.8 $9.8 $11.9 $13.9 $18.1 $23.1
AO $3.4 $3.8 $4.6 $5.4 $6.9 $9.1 Notes:
Funding numbers represent projections based on assumptions on MOHLTC funding, and represent only program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Total number of Adults with Physical Disabilities in Adult Day Programs is unclear as numbers are constantly in a state of flux. Thus current and future funding details remain unknown
London Outreach model for 24/7 – costs are about $28-29,000 for 60 people in 2012/2013 – 24/7 coverage is not included in above costs
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Costs/Funding based on assumed annual inflation rate of 1.5%
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
AO= Attendant Outreach
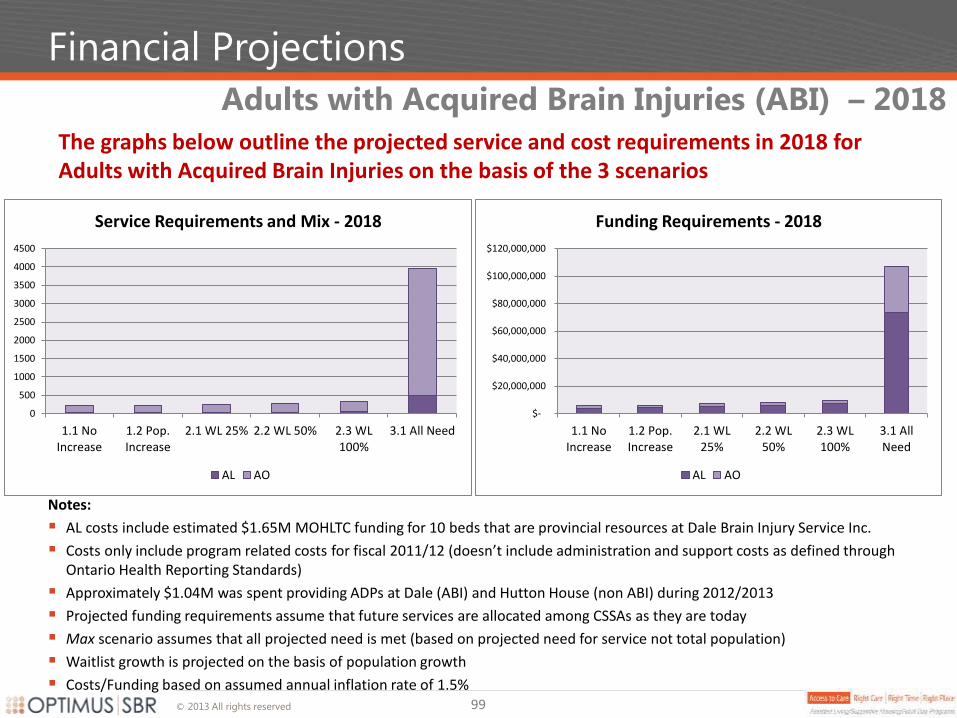
© 2013 All rights reserved
Financial Projections
The graphs below outline the projected service and cost requirements in 2018 for Adults with Acquired Brain Injuries on the basis of the 3 scenarios
Adults with Acquired Brain Injuries (ABI) – 2018
99
Notes:
AL costs include estimated $1.65M MOHLTC funding for 10 beds that are provincial resources at Dale Brain Injury Service Inc.
Costs only include program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Approximately $1.04M was spent providing ADPs at Dale (ABI) and Hutton House (non ABI) during 2012/2013
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
Costs/Funding based on assumed annual inflation rate of 1.5%
0
500
1000
1500
2000
2500
3000
3500
4000
4500
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL 25% 2.2 WL 50% 2.3 WL100%
3.1 All Need
Service Requirements and Mix - 2018
AL AO
$-
$20,000,000
$40,000,000
$60,000,000
$80,000,000
$100,000,000
$120,000,000
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL25%
2.2 WL50%
2.3 WL100%
3.1 AllNeed
Funding Requirements - 2018
AL AO
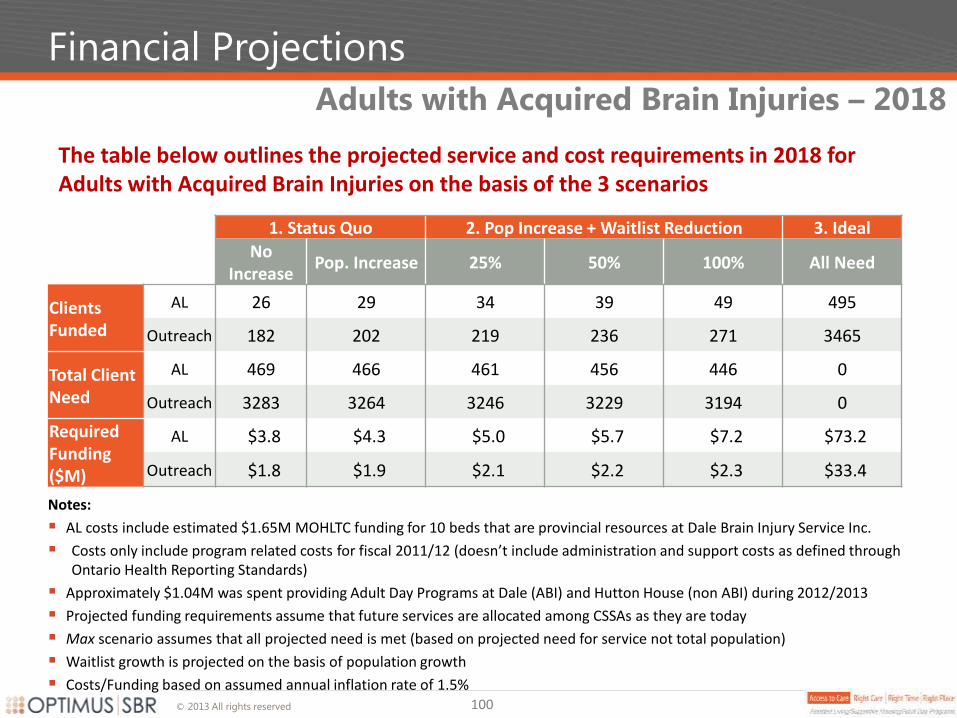
© 2013 All rights reserved
Financial Projections
The table below outlines the projected service and cost requirements in 2018 for Adults with Acquired Brain Injuries on the basis of the 3 scenarios
Adults with Acquired Brain Injuries – 2018
100
1. Status Quo 2. Pop Increase + Waitlist Reduction 3. Ideal
No
Increase Pop. Increase 25% 50% 100% All Need
Clients Funded
AL 26 29 34 39 49 495
Outreach 182 202 219 236 271 3465
Total Client Need
AL 469 466 461 456 446 0
Outreach 3283 3264 3246 3229 3194 0
Required Funding ($M)
AL $3.8 $4.3 $5.0 $5.7 $7.2 $73.2
Outreach $1.8 $1.9 $2.1 $2.2 $2.3 $33.4
Notes:
AL costs include estimated $1.65M MOHLTC funding for 10 beds that are provincial resources at Dale Brain Injury Service Inc.
Costs only include program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Approximately $1.04M was spent providing Adult Day Programs at Dale (ABI) and Hutton House (non ABI) during 2012/2013
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
Costs/Funding based on assumed annual inflation rate of 1.5%
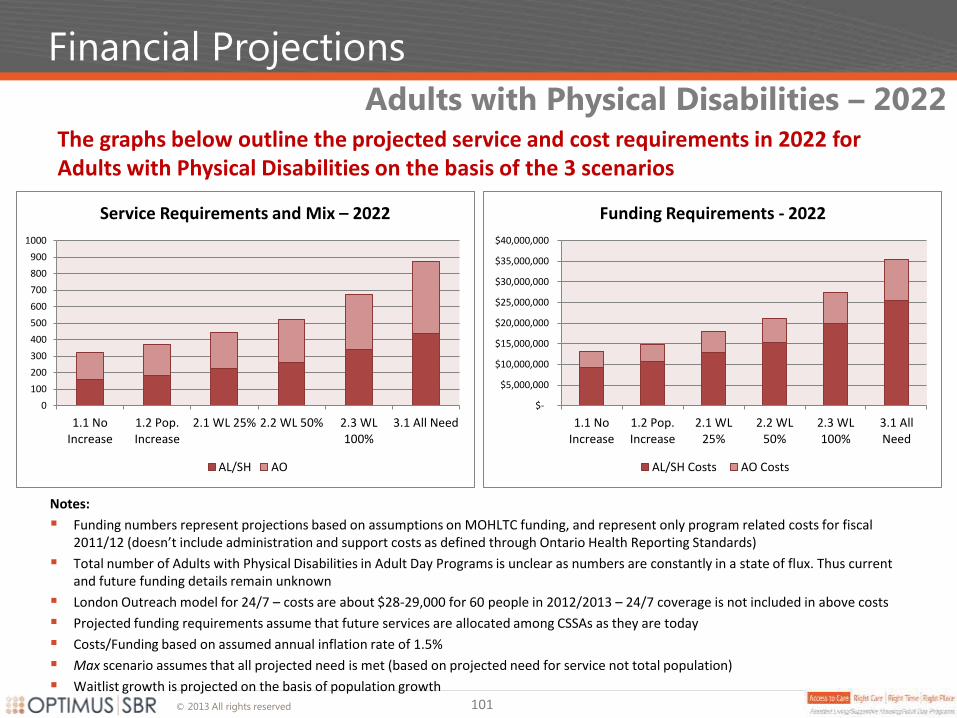
© 2013 All rights reserved
Financial Projections
The graphs below outline the projected service and cost requirements in 2022 for Adults with Physical Disabilities on the basis of the 3 scenarios
Adults with Physical Disabilities – 2022
0
100
200
300
400
500
600
700
800
900
1000
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL 25% 2.2 WL 50% 2.3 WL100%
3.1 All Need
Service Requirements and Mix – 2022
AL/SH AO
$-
$5,000,000
$10,000,000
$15,000,000
$20,000,000
$25,000,000
$30,000,000
$35,000,000
$40,000,000
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL25%
2.2 WL50%
2.3 WL100%
3.1 AllNeed
Funding Requirements - 2022
AL/SH Costs AO Costs
101
Notes:
Funding numbers represent projections based on assumptions on MOHLTC funding, and represent only program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Total number of Adults with Physical Disabilities in Adult Day Programs is unclear as numbers are constantly in a state of flux. Thus current and future funding details remain unknown
London Outreach model for 24/7 – costs are about $28-29,000 for 60 people in 2012/2013 – 24/7 coverage is not included in above costs
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Costs/Funding based on assumed annual inflation rate of 1.5%
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
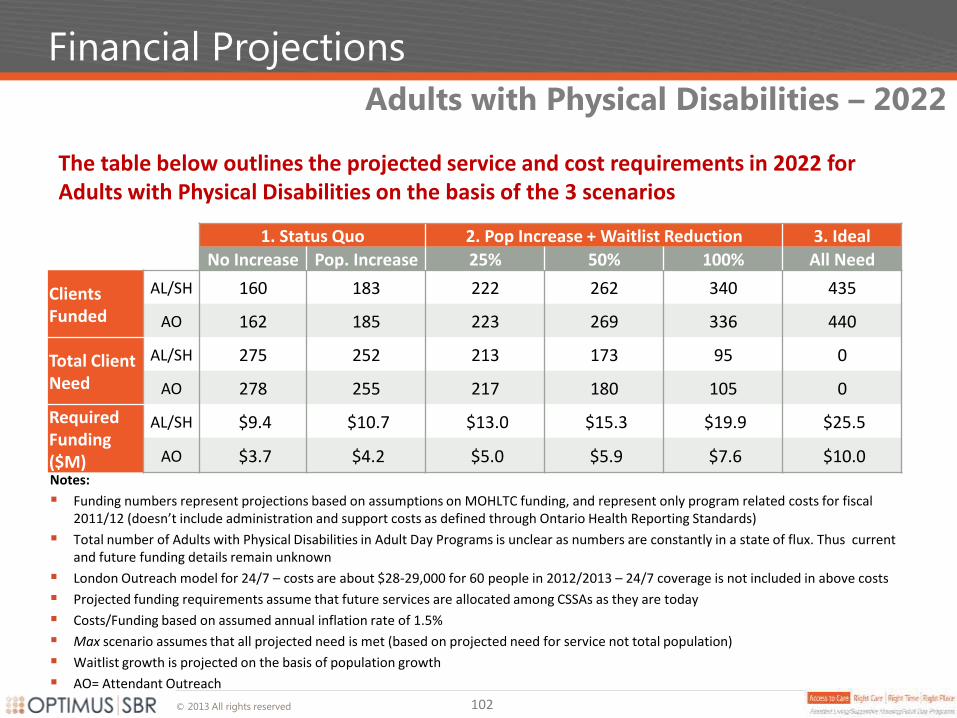
© 2013 All rights reserved
Financial Projections
The table below outlines the projected service and cost requirements in 2022 for Adults with Physical Disabilities on the basis of the 3 scenarios
Adults with Physical Disabilities – 2022
102
1. Status Quo 2. Pop Increase + Waitlist Reduction 3. Ideal
No Increase Pop. Increase 25% 50% 100% All Need
Clients Funded
AL/SH 160 183 222 262 340 435
AO 162 185 223 269 336 440
Total Client Need
AL/SH 275 252 213 173 95 0
AO 278 255 217 180 105 0
Required Funding ($M)
AL/SH $9.4 $10.7 $13.0 $15.3 $19.9 $25.5
AO $3.7 $4.2 $5.0 $5.9 $7.6 $10.0 Notes:
Funding numbers represent projections based on assumptions on MOHLTC funding, and represent only program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Total number of Adults with Physical Disabilities in Adult Day Programs is unclear as numbers are constantly in a state of flux. Thus current and future funding details remain unknown
London Outreach model for 24/7 – costs are about $28-29,000 for 60 people in 2012/2013 – 24/7 coverage is not included in above costs
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Costs/Funding based on assumed annual inflation rate of 1.5%
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
AO= Attendant Outreach
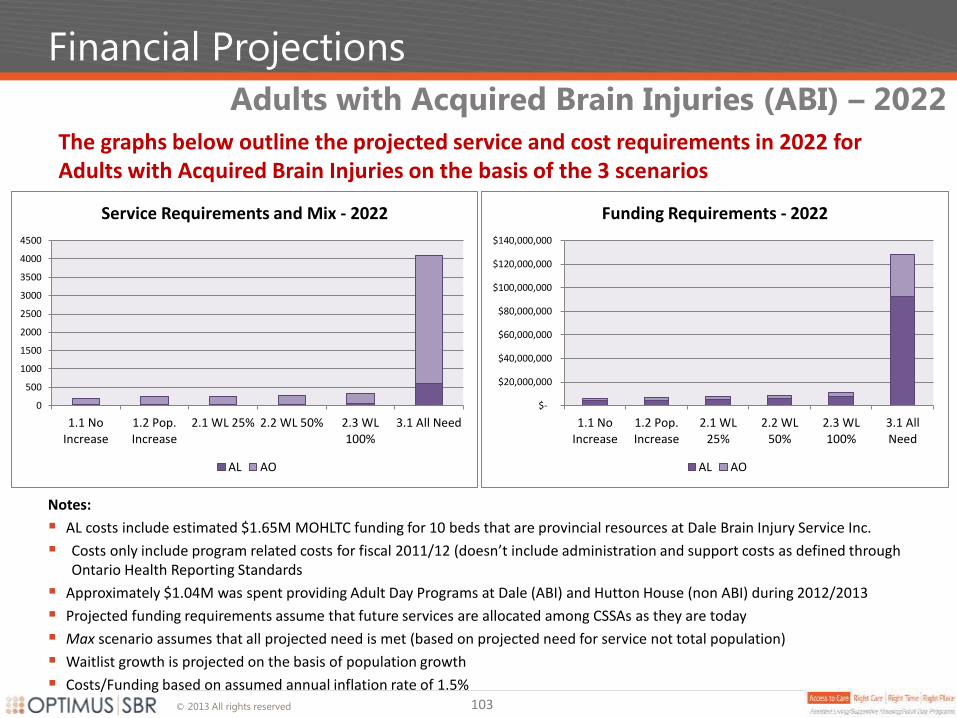
© 2013 All rights reserved
Financial Projections
The graphs below outline the projected service and cost requirements in 2022 for Adults with Acquired Brain Injuries on the basis of the 3 scenarios
Adults with Acquired Brain Injuries (ABI) – 2022
103
Notes:
AL costs include estimated $1.65M MOHLTC funding for 10 beds that are provincial resources at Dale Brain Injury Service Inc.
Costs only include program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards
Approximately $1.04M was spent providing Adult Day Programs at Dale (ABI) and Hutton House (non ABI) during 2012/2013
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
Costs/Funding based on assumed annual inflation rate of 1.5%
0
500
1000
1500
2000
2500
3000
3500
4000
4500
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL 25% 2.2 WL 50% 2.3 WL100%
3.1 All Need
Service Requirements and Mix - 2022
AL AO
$-
$20,000,000
$40,000,000
$60,000,000
$80,000,000
$100,000,000
$120,000,000
$140,000,000
1.1 NoIncrease
1.2 Pop.Increase
2.1 WL25%
2.2 WL50%
2.3 WL100%
3.1 AllNeed
Funding Requirements - 2022
AL AO
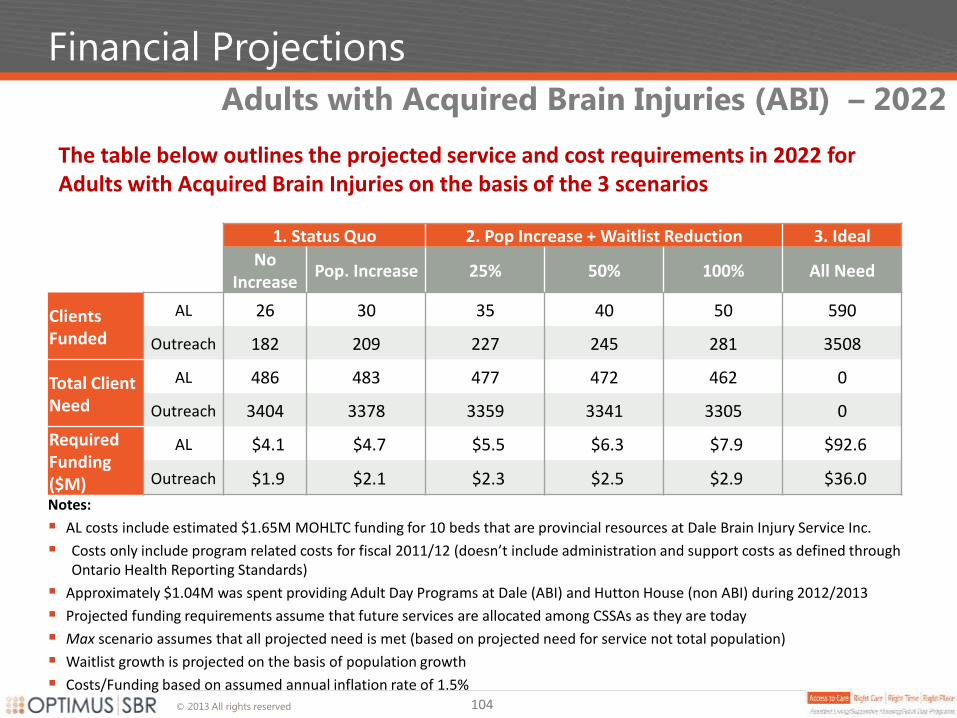
© 2013 All rights reserved
Financial Projections
The table below outlines the projected service and cost requirements in 2022 for Adults with Acquired Brain Injuries on the basis of the 3 scenarios
Adults with Acquired Brain Injuries (ABI) – 2022
104
1. Status Quo 2. Pop Increase + Waitlist Reduction 3. Ideal
No
Increase Pop. Increase 25% 50% 100% All Need
Clients Funded
AL 26 30 35 40 50 590
Outreach 182 209 227 245 281 3508
Total Client Need
AL 486 483 477 472 462 0
Outreach 3404 3378 3359 3341 3305 0
Required Funding ($M)
AL $4.1 $4.7 $5.5 $6.3 $7.9 $92.6
Outreach $1.9 $2.1 $2.3 $2.5 $2.9 $36.0
Notes:
AL costs include estimated $1.65M MOHLTC funding for 10 beds that are provincial resources at Dale Brain Injury Service Inc.
Costs only include program related costs for fiscal 2011/12 (doesn’t include administration and support costs as defined through Ontario Health Reporting Standards)
Approximately $1.04M was spent providing Adult Day Programs at Dale (ABI) and Hutton House (non ABI) during 2012/2013
Projected funding requirements assume that future services are allocated among CSSAs as they are today
Max scenario assumes that all projected need is met (based on projected need for service not total population)
Waitlist growth is projected on the basis of population growth
Costs/Funding based on assumed annual inflation rate of 1.5%