Embed Size (px)
Citation preview

! !
Association Between Electroretinogram-identified Vigabatrin Toxicity and Subsequent Visual Field Reduction
!!
by
!
!
Ananthavalli Kumarappah
A thesis submitted in conformity with the requirements for the degree of Master of Science
Institute of Medical Science
University of Toronto
© Copyright by Ananthavalli Kumarappah 2014

ii
Association Between Electroretinogram-identified Vigabatrin Toxicity and Subsequent Visual Field Reduction
!
Ananthavalli Kumarappah
Master of Science
Institute of Medical Science University of Toronto
2013
Abstract
Vigabatrin (VGB) is an antiepileptic drug approved for pediatric patients with infantile
spasms. VGB is associated with visual field reductions in 30-50% of adults taking the drug. The
amplitude of the 30-Hz flicker electroretinogram (ERG) is recommended for screening young
children on VGB treatment. To determine if standard ERG tests for VGB toxicity are correlated
with visual field reductions, 22 individuals who were previously on VGB underwent visual
assessment. This study also validated the use of high-resolution OCT for detecting structural
changes associated with VGB toxicity. This study demonstrates that the ERG was associated
with visual field loss, as measured along the temporal meridian. The retinal nerve fibre layer
(RNFL) was attenuated in all children who showed a reduction in the visual fields indicating that
RNFL attenuation may be a sensitive marker for VGB toxicity. We recommend using serial
OCTs to monitor VGB toxicity since it is fast and non-invasive.
! !

iii
Acknowledgements
This thesis would not have been possible without the help, support, and guidance of many
people. I would like to thank my supervisor, Dr. Carol Westall, for her patience, motivation, and
immense knowledge. I could not have imagined a more caring and knowledgeable advisor and
mentor for my project. Thank you for everything!
I would also like to thank the rest of my committee comments, Dr. Carter Snead, Dr.
Karen Gordon, and Dr. Annie Dupuis, for their insightful comments and suggestions.
I would also like to thank Dr. Tom Wright, Melissa Cotesta, as well as other lab members
for providing sound advice and good company.
I am deeply grateful to Dr. Raymond Buncic and Dr. Arun Reginald for their constructive
inputs at different stages of this project. This project would not have been successful without Dr.
Arun Reginald’s involvement and collaboration. Thank you for taking the time to see the
participants during your busy clinic hours.
Many thanks to Aparna Bhan for coordinating all the clinical visits. Thank you to the
Department of Ophthalmology, particularly the Ophthalmic Imaging Unit and the Ophthalmic
Assistants, at Sick Kids for making sure that clinical visits ran smoothly.
I’d also like to thank all of the study participants and their families for giving up their
valuable time, without whom this research would not have been possible. Thank you for making
data collection enjoyable.
Lastly, I would like to thank my family and friends for their emotional support and
encouragement.

iv
Table of Contents
List!of!Tables!.........................................................................................................................................!ix!
List!of!Figures!.........................................................................................................................................!x!
List!of!Abbreviations!.........................................................................................................................!xii!
1!Epilepsy!................................................................................................................................................!1!
1.1!Classification!...............................................................................................................................!1!
1.1.1!Focal!Seizures!........................................................................................................................................!2!
1.1.2!Generalized!Seizures!...........................................................................................................................!2!
1.1.3!Epileptic!Spasms!...................................................................................................................................!3!
2!Infantile!Spasms!................................................................................................................................!4!
2.1!Clinical!Manifestation!..............................................................................................................!4!
2.2!EEG!Findings!...............................................................................................................................!5!
2.3!Classification!...............................................................................................................................!5!
2.4!Treatment!....................................................................................................................................!6!
3!Vision!....................................................................................................................................................!7!
3.1!Image!Formation!.......................................................................................................................!7!
3.2!Retinal!Processing!....................................................................................................................!8!
3.3!Lateral!Connections!..................................................................................................................!8!
3.4!Photoreceptors!..........................................................................................................................!8!
3.5!Bipolar!Cells!..............................................................................................................................!10!
3.6!Ganglion!Cells!...........................................................................................................................!11!
3.7!Convergence!..............................................................................................................................!11!
3.8!Retinal!Glia!................................................................................................................................!11!
4!GABA!...................................................................................................................................................!12!
4.1!GABA!Receptors!.......................................................................................................................!13!
4.1.1!GABAA!Receptors!...............................................................................................................................!13!
4.1.2!GABAB!Receptors!...............................................................................................................................!13!
4.1.3!GABAC!Receptors!...............................................................................................................................!14!
4.2!GABA!in!the!Retina!..................................................................................................................!14!

v
4.3!Excitatory!Effects!of!GABA!....................................................................................................!15!
4.3.1!Excitatory!Effects!During!Development!..................................................................................!15!
4.3.2!Subcellular!and!Regional!Differences!.......................................................................................!16!
4.4!GABA!Response!in!Epilepsy!.................................................................................................!17!
4.4.1!The!Role!of!Excitation!......................................................................................................................!18!
5!Vigabatrin!..........................................................................................................................................!20!
5.1!Regulatory!History!of!Vigabatrin!.......................................................................................!20!
5.2!Pharmacology!of!Vigabatrin!................................................................................................!21!
5.3!Mechanism!of!Action!..............................................................................................................!21!
5.4!Clinical!Efficacy!in!Adults!.....................................................................................................!22!
5.5!Clinical!Efficacy!for!Infantile!Spasms!................................................................................!23!
5.5.1!Randomized!Controlled!Trials!.....................................................................................................!23!
5.6!NonQvision!Adverse!Events!..................................................................................................!25!
5.6.1!Animal!Toxicity!..................................................................................................................................!25!
5.6.2!Clinical!Studies!...................................................................................................................................!25!
6!Vigabatrin!and!Visual!Side!Effects!in!Human!........................................................................!26!
6.1!Vigabatrin!Associated!Visual!Field!Loss!(VGBQVFL)!....................................................!26!
6.1.1!Prevalence!in!Adults!........................................................................................................................!27!
6.1.2!Prevalence!in!Children!....................................................................................................................!28!
6.2!Ophthalmoscopic!Findings!..................................................................................................!30!
6.3!Other!Clinical!Findings!..........................................................................................................!30!
6.4!Retinal!Defects!in!Animal!Studies!......................................................................................!30!
7!Visual!Electrophysiology!..............................................................................................................!32!
7.1!FullQfield!Electroretinogram!(ERG)!...................................................................................!32!
7.1.1!ERG!and!Vigabatrin!..........................................................................................................................!33!
7.2!Multifocal!ERG!..........................................................................................................................!35!
7.2.1!mFERG!and!Vigabatrin!....................................................................................................................!36!
7.3!ElectroQoculogram!..................................................................................................................!36!
7.3.1!EOG!and!Vigabatrin!..........................................................................................................................!36!
7.4!Visual!Evoked!Potentials!......................................................................................................!36!

vi
8!Optical!Coherence!Tomography!(OCT)!...................................................................................!37!
8.1!Basic!Principles!........................................................................................................................!37!
8.2!Clinical!and!SubQclinical!Applications!of!OCT!................................................................!38!
8.3!OCT!and!Vigabatrin!–!Retinal!Nerve!Fibre!Layer!(RNFL)!...........................................!39!
9!Mechanism!of!Vigabatrin!Toxicity!............................................................................................!40!
9.1!GABA!Receptors!and!Excitotoxicity!..................................................................................!40!
9.1.1!Limitations!...........................................................................................................................................!41!
9.2!Role!of!Taurine!.........................................................................................................................!42!
9.2.1!Physiological!Role!of!Taurine!.......................................................................................................!42!
9.2.2!Taurine!and!Vigabatrin!...................................................................................................................!42!
10!Assessment!of!VGBQVFL!in!Young!Children!.........................................................................!44!
10.1!Toxicity!–!Original!Definition!...........................................................................................!44!
10.2!Problems!with!original!definition!..................................................................................!45!
10.2.1!Abnormal!Development!...............................................................................................................!45!
10.2.2!Lack!of!true!baseline!.....................................................................................................................!48!
10.2.3!Poor!recording:!Disagreement!between!eyes!....................................................................!49!
10.2.4!Monocular!Recordings!.................................................................................................................!49!
10.2.5!ArtificiallyUReduced!Baseline!....................................................................................................!50!
10.2.6!Lost!to!FollowUup!............................................................................................................................!51!
10.2.7!Recovery!.............................................................................................................................................!52!
10.3!Toxicity:!Refined!Definition!..............................................................................................!53!
11!Purpose!and!Rationale!...............................................................................................................!54!
12!Hypothesis!......................................................................................................................................!55!
13!Methods!...........................................................................................................................................!56!
13.1!Research!Ethics!Board!Approval!.....................................................................................!56!
13.2!Recruitment!............................................................................................................................!56!
13.3!Inclusion!Criteria!..................................................................................................................!56!
13.3.1!Participants!with!Vigabatrin!Toxicity!....................................................................................!56!
13.3.2!Control!Participants!–!Participants!without!Toxicity!.....................................................!56!
13.4!Exclusion!Criteria!.................................................................................................................!57!

vii
13.5!Patient!Information!.............................................................................................................!57!
13.6!Consent!.....................................................................................................................................!57!
13.7!Study!Protocol!.......................................................................................................................!58!
13.7.1!Clinical!Assessment!.......................................................................................................................!58!
13.7.2!Visual!Fields!......................................................................................................................................!60!
13.7.3!Mydriasis!and!Cycloplegia!..........................................................................................................!61!
13.7.4!Examination!by!the!Ophthalmologist!....................................................................................!62!
13.7.5!Imaging:!Fundus!Photography!..................................................................................................!62!
13.7.6!Imaging:!Optical!Coherence!Tomography!...........................................................................!63!
13.7.7!Photopic!Electroretinogram!......................................................................................................!64!
13.8!Statistical!Analysis!...............................................................................................................!65!
13.8.1!Linear!Mixed!Models!.....................................................................................................................!65!
14!Results!.............................................................................................................................................!66!
14.1!Participant!Demographics!.................................................................................................!66!
14.1.1!Neurological!History!.....................................................................................................................!66!
14.1.2!Identifying!Toxicity:!Demographics!.......................................................................................!67!
14.2!Clinical!Examination!............................................................................................................!70!
14.3!Visual!Fields!...........................................................................................................................!74!
14.4!Examination!by!Ophthalmologist!...................................................................................!78!
14.5!Imaging:!Fundus!Photography!.........................................................................................!79!
14.6!Imaging:!Optical!Coherence!Tomography!....................................................................!80!
14.6.1!200x200!Optic!Disc!Cube!............................................................................................................!80!
14.6.2!Ganglion!Cell!Analysis!...................................................................................................................!84!
14.7!Photopic!Electroretinogram!.............................................................................................!85!
15!Discussion!.......................................................................................................................................!90!
15.1!Demographics!........................................................................................................................!90!
15.1!Visual!Fields!...........................................................................................................................!91!
15.2!Optical!Coherence!Tomography!(OCT)!.........................................................................!95!
15.3!Limitations!..............................................................................................................................!99!
15.3!Conclusions!..........................................................................................................................!101!
16!Future!Directions!......................................................................................................................!102!

viii
References!.........................................................................................................................................!105!
Appendix!A!Q!!SickKids!Research!Ethics!Board!Approval!..................................................!122!
Appendix!B!–!Recruitment!Letter!..............................................................................................!123!
Appendix!C!–!Sample!Consent!and!Assent!Forms!.................................................................!124!
Appendix!D!–!Case!Report!Form!.................................................................................................!139!
Appendix!E!–!Mixed!Model!Code!................................................................................................!142!
Appendix!F!–!Patient!Demographic!Information!..................................................................!143!
Appendix!G!–!Visual!Acuity!and!Contrast!Sensitivity!Results!...........................................!146!
Appendix!H!–!Colour!Vision!Results!..........................................................................................!148!
Appendix!I!–!Goldmann!Visual!Field!Results!.........................................................................!149!
Appendix!J!–!Clinical!Findings!by!an!Ophthalmologist!.......................................................!151!
Appendix!K!–!Fundus!Photography!Results!...........................................................................!153!
KQ1!–!Observer!..............................................................................................................................!153!
KQ2!–!Observer!2!..........................................................................................................................!154!
Appendix!L!–!OCT!Results!.............................................................................................................!155!
LQ1!–!Optic!Disc!Cube!–!Retinal!Nerve!Fibre!Layer!Thickness!by!Quadrants!...........!155!
LQ2!–!Ganglion!Cell!Analysis!.....................................................................................................!156!
Appendix!M!–!FollowQup!ERG!Results!.......................................................................................!158!
Appendix!N!–!Copyright!Acknowledgements!.........................................................................!159!
Figure!7Q1!.......................................................................................................................................!159!
Figure!8Q1!.......................................................................................................................................!163!
Figure!13Q1!....................................................................................................................................!164!
Figure!15Q1!....................................................................................................................................!165!
!
!

ix
List of Tables
Table 3-1 – Comparison of rod and cone photoreceptor properties
Table 5-1 – Clinical studies of vigabatrin in the treatment of infantile spasms
Table 6-1 - Prevalence of vigabatrin-associated visual field loss in adults
Table 6-2 – Prevalence of vigabatrin-associated visual field loss in children
Table 7-1 – Electroretinogram changes associated with vigabatrin therapy
Table 7-2 – Electroretinogram changes associated with vigabatrin-associated visual field loss.
Table 14-1 – Demographic information for study participants
Table 14-2 – Visual acuity and contrast sensitivity results
Table 14-3 – Summary of mixed model results for visual fields by four meridians
Table 14-4 – Evaluation of fundus photography
Table 14-5 – Summary of Optic Disc Cube scan results
Table 14-6 – Summary of mixed model results for RNFL thickness by quadrants
Table 14-7 – Summary of mixed model results for RNFL thickness by clock hours
Table 14-8 – Ganglion cell analysis results
Table 14-9 – Follow-up photopic ERG results

x
List of Figures
Figure 3-1 – Diagram of the retina
Figure 4-1 – The synthesis and breakdown of γ-aminobutyric acid
Figure 5-1 – Structure of GABA and vigabatrin
Figure 7-1 – Standard ISCEV waveforms
Figure 8-1 – Schematic diagram of a time-domain optical coherence tomography system
Figure 10-1 – Boxplot of inter-visit variation of the 30-Hz flicker amplitude
Figure 10-2 – Vigabatrin-free 30-Hz flicker amplitude as a function of age in children with and
without spasms
Figure 10-3 – Plot of 30-Hz flicker amplitudes for participant 1225: Lack of true baseline
Figure 10-4 – Plot of 30-Hz flicker amplitudes for participant 1217: Disagreement between two
eyes
Figure 10-5 – Plot of 30-Hz flicker amplitudes for participant 1222: Monocular recordings
Figure 10-6 – Plot of 30-Hz flicker amplitudes for participant 1300: Artificially reduced
baselines
Figure 10-7 – Plot of 30-Hz flicker amplitudes for participant 1219: Lost to follow-up
Figure 10-8 – Plot of 30-Hz flicker amplitudes for participant 1217: Recovery
Figure 13-1 – Modified 7-Standard Field Protocol for Colour Fundus Photography
Figure 14-1 – Plot of age of vigabatrin initiation
Figure 14-2 – Plot of duration of vigabatrin treatment
Figure 14-3 – Plot of visual acuity scores – ETDRS

xi
Figure 14-4 – Plot of visual acuity scores – Cardiff
Figure 14-5 – Plot of contrast sensitivity scores – M&S
Figure 14-6 – Plot of Goldmann visual fields – I 2e along four meridians
Figure 14-7 – Plot of Goldmann visual fields – I 4e along four meridians
Figure 14-8 – Plot of Goldmann visual fields – IV 4e along four meridians
Figure 14-9 – Goldmann perimetry results of two participants with toxicity
Figure 14-10 – Goldmann perimetry results of a participant without toxicity
Figure 14-11 – Plot of global retinal nerve fibre layer thickness
Figure 14-12 – Plot of retinal nerve fibre layer thickness by quadrants
Figure 14-13 – Spatial mapping of retinal nerve fibre layer thickness differences by clock hour
segments
Figure 14-14 – Spatial mapping of ganglion cell analysis
Figure 14-15 – Plot of raw flicker amplitudes
Figure 14-16 – Plot of change in flicker amplitude from baseline
Figure 14-17 – Plot of flicker amplitude vs duration of vigabatrin
Figure 15-1 – Garway-Heath Map
!

xii
List of Abbreviations
ACTH Adrenocorticotropic hormone
AEDs Anti-epileptic drugs
CNS Central nervous system
CSF Cerebrospinal fluid
EEG Electroencephalogram
ERG Electroretinogram
GABA Gamma-aminobutyric acid
GABA-T GABA-transaminase
GAD Glutamic acid decarboxylase
GFAP Glial fibrillary acidic protein
ILAE International League Against Epilepsy
INL Inner nuclear layer
IPL Inner plexiform layer
IS Infantile spasms
MRM Mollon-Reffin Minimalist
ONL Outer nuclear layer
OPL Outer plexiform layer
RNFL Retinal nerve fibre layer
TSC Tuberous sclerosis complex
VBG Vigabatrin
VGB-VFL Vigabatrin-associated visual field loss
WSKP White sphere kinetic perimetry

1
1 Epilepsy
Epilepsy is one of the most common neurological conditions, with a prevalence of 5-6% in
Canada, and is more likely to develop in infants and the elderly [1, 2]. Epilepsy is not a single
disorder but compromises many conditions which share the commonality of seizures. A seizure
is an episodic behavioral event caused by a sudden, uncontrolled, excessive electrical discharge
of neurons within the cerebral cortex. Epilepsy is a neurological condition characterized by
recurrent (two or more) seizures that are unprovoked by external stimuli such as convulsant
drugs or fever (febrile seizures) [3].
1.1 Classification
Seizures may be characterized electrographically and/or clinically. Electroencephalography
(EEG) performed during the course of a seizure is a valuable tool in the accurate diagnosis of the
seizure [4]. The EEG demonstrates the electrical field potential of aggregates of cortical neurons
as recorded from electrodes placed on the scalp.
The primary system of classifying epileptic seizures was initially developed in 1970 by the
International League Against Epilepsy (ILAE) and has since undergone several revisions [5-8].
The newest revision to the classification system takes into the account scientific advancements
that have occurred in the past few decades and focuses on causes and mechanisms that will aid in
care rather than mere classification. This new system also acknowledges the need for flexibility.
Seizures can be broadly categorized as either generalized seizures or focal (partial) seizures. This
dichotomous classification of seizures is an oversimplification since some conditions (diffuse
hemispheric abnormalities, multifocal abnormalities and bilaterally symmetrical abnormalities)
do not fall into either category [9]. Furthermore, this classification may be arbitrary in cases
where the EEG data are discordant with the clinical manifestation (i.e. clinically generalized
seizures correlated with focal electrographic abnormalities and clinically focal seizures
correlated with generalized electrographic abnormalities) [4, 10, 11]. In the 2010 revised
classification system, the terms generalized and focal are largely abandoned in describing
epilepsies, but are retained to describe seizure initiation and presentation [8].

2
1.1.1 Focal Seizures
In focal seizures, the epileptiform activity starts in a network limited to one hemisphere and
spreads to neighboring regions either unilaterally or bilaterally [6]. Symptoms often depend on
the origin of the electrical discharge [3]. For example, a seizure that begins in the motor cortex
will manifest as motor movements. The abnormal discharge may spread to the other cortical
hemisphere (previously termed secondary generalized seizure).
Generally, focal seizures last 1 -2 minutes (ictal phase) and can be followed by a longer post-
ictal period. Individuals often experience post-ictal weakness (Todd’s paralysis) following a
focal motor seizure [12].
Traditionally, focal seizures were further categorized as simple or complex depending on the
presence or absence of consciousness, respectively. Assessing the level of awareness of
individuals during seizures can be difficult, especially among pre-verbal infants [4].
Furthermore, the distinction between simple and complex seizures is not based on seizure
mechanism nor does it have any implications for treatment and thus this distinction has been
removed in the revised classification system [8]. Instead, the new system advises using accurate
terms to describe the ictal semiology using the Glossary of Ictal Semiology [13, 14].
1.1.2 Generalized Seizures
Generalized seizures arise from bilaterally-distributed networks. Since a greater area of the brain
is affected, the individual experiences a loss of consciousness and more serious symptoms [12].
There are many subcategories of generalized seizures including tonic-clonic (grand mal),
absence (petit mal), myoclonic, tonic, clonic, and atonic seizures.
Tonic-clonic seizures are characterized by a sudden loss of consciousness followed by tonic
contraction of muscles. If the respiratory musculature is involved, the tight glottis forcefully
expels the air causing a loud ictal cry. After 1-2 minutes of the tonic phase, the seizure enters the
clonic (convulsive) phase [15]. Rapid, rhythmic movements of the trunk and limbs, which
gradually slow down as the electrical seizure ends, characterize this phase.

3
Absence seizures are characterized by a short period of behavioral arrest, unresponsiveness or
staring followed by normal activity (no postictal period). Ictal EEG traces for absence seizures
include a 3-Hz spike-wave discharge with sudden onset and termination [15].
1.1.3 Epileptic Spasms
Classifying epileptic spasms present scientists with a challenge since the seizures are usually
bilaterally symmetric (generalized seizures) but arise from a focal pathology. In some instances,
the semiology may be focal. It is unknown whether epileptic spasms are focal, generalized, or
whether their classification is context-specific. Therefore, the revised classification system puts
epileptics spasms in its own category [8].

4
2 Infantile Spasms
In 1841, Dr. William James West originally described infantile spasms (IS) upon witnessing this
phenomenon in his son [16]. IS is an age-specific epileptic syndrome characterized by seizures
involving flexion/extension spasms in clusters and is often accompanied by developmental
regression and a unique pattern on the EEG termed hypsarrhythmia. The term “West syndrome”
is used to describe the disease when all three features of spasms, hypsarrhythmia and
developmental regression are present [17-19].
The incidence of IS ranges from 0.5 to 6 per 10, 000 live births [18, 20, 21] with higher
prevalence in males [22]. It is characterized as a catastrophic epilepsy syndrome of childhood
since it has such a high incidence of developmental regression in infants [23]. Older age of
spasm onset and shorter time to treatment from spasm onset is associated with better
developmental outcome [24]. IS has a mortality rate between 5 and 30% with most deaths being
caused by underlying diseases [25, 26].
Onset of this epileptic disorder usually occurs within the first year of life. Of patients with a
history of IS, 36% are seizure-free by adulthood [27] and 20-50% develop Lennox-Gastaut
syndrome [26, 28, 29]. Lennox-Gastaut syndrome is a childhood epileptic encephalopathy that
usually occurs between two to six of years of age and is characterized by multiple seizure type
and moderate to severe cognitive dysfunction. The similarities between IS and the seizures that
characterize Lennox-Gastaut syndrome suggest that they may be age-dependent manifestations
of the same encephalopathic phenomenon [30].
2.1 Clinical Manifestation
IS is characterized by symmetric muscular contractions of the trunk, head and/or extremities.
Based on the patterns of muscle movements, the spasms can be categorized as flexor, extensor or
extensor-flexor [31]. Flexor spams consist of rapid flexion of the neck, trunk and extremities and
are often referred to as jackknife convulsions. Extensor spasms consist of extension of the neck,
trunk, and extremities. Flexor-extensor spasms are the most common and involve combinations
of neck, trunk, and arm flexion and leg extension, or leg flexion and arm extension. These
individual spasms typically last from less than one second up to five seconds and are followed by

5
a sustained tonic phase (stiffening of the limbs) lasting up to ten seconds. Spasms often occur in
clusters of 3-100 [22, 31].
2.2 EEG Findings
Hypsarrhythmia, first described by Gibbs & Gibbs in 1952, is a unique pattern observed
interictally on the EEG [32] and consists of an asynchronous, disorganized background
consisting of high-voltage slow waves and multifocal spikes. Hypsarrhythmia is most
pronounced during slow-wave sleep and may disappear during REM sleep [33]. Older children
patients may have epileptic spasms without hypsarrhythmia and conversely, hypsarrhythmia may
be seen in other seizure disorders [18].
2.3 Classification
IS has been associated with more than 200 clinical conditions but is generally classified as
symptomatic if the patient exhibits any pre-existing disease signs and as cryptogenic if the child
is neurologically and/or neurodevelopmentally abnormal prior to the onset of spasms, but no
cause can be found. Idiopathic spasms refers to a child who is neurologically normal at the onset
of spasms in whom, no cause of spasms can be found. An estimated 60-70% of the patients have
a known aetiology such as tuberous sclerosis complex (TSC), brain malformations,
mitochondrial encephalopathies, hypoxic-ischemic encephalopathies, metabolic!errors,!
periventricular leukomalacia, or trisomy 21 [23]. With increased availability of better metabolic
and genetic diagnostic tools as well as more sophisticated neuroimaging, the ratio of
symptomatic to idiopathic cases is increasing [34]. In particular, 3T magnetic resonance imaging
(MRI) allows detection of subtle neurodevelopmental abnormalities such as cortical dysplasia
[35].
In light of recent advancements, the ILAE Commission on Classification and Terminology has
suggested abandoning previous used terminology (symptomatic, cryptogenic and idiopathic) for
describing underlying causes [6]. Instead, the commission suggests the use of the following three
categories: genetic, structural/metabolic and unknown. If the seizure arises from a genetic defect,
then it is classified as genetic. Some genetic causes of epilepsy include defect in genes ARX,
CDKL5, FOXG1, GRIN1, GRIN2A, MAGI2, MEF2C, SLC25A22, SPTAN1, and STXBP1 [34]. If

6
the seizure arises from an underlying structural or metabolic condition, such as TSC, then it is
classified as structural/metabolic. The final category “unknown” emphasises that all seizures are
essentially symptomatic but that sometimes, the underlying causes may not be currently known.
Paciorkowski and colleagues [34] also suggest moving away from symptomatic, cryptogenic and
idiopathic classification systems. However, they point out that the distinction between genetic
and structural/metabolic is artificial since TSC and other inherited metabolic disorders have a
genetic cause.
2.4 Treatment
There is much variation in the management of IS with the agents, dose and treatment length
differing from one patient to the next. Adrenocorticotropic hormone (ACTH) was first
discovered to be effective against IS in 1958 [36]. The 2012 evidence-based guidelines
recommend ACTH or VGB as first-line treatment options for IS, with ACTH recommended
preferentially over VGB [37]. Most of the evidence for the effectiveness of other treatment
modalities in IS is class 3 and class 4 evidence [37]. However, prednisone is sometimes used in
lieu of ACTH because of the ease of administration of the former [38]. Side effects associated
with ACTH include increased risk of infections, irritability, development of cushingoid features
and hypertension [22, 39]. Vigabatrin (VGB) (detailed discussion to follow in Section 5) is an
effective anti-epileptic drug and is particularly efficacious in treating seizures associated with
TSC [40]. A literature review [41] of studies investigating the use of VGB on patients with IS
found that 95% of those with an etiology of TSC achieved spasm cessation compared with 54%
of patients with other underlying etiologies. In Canada, VGB is the first line treatment for IS
with ACTH used for those children who fail to respond to VGB. Children who fail to respond to
either of these two drugs may be treated with the ketogenic diet and/or topiramate.
Hancock and colleagues reviewed 18 randomized controlled trials involving patients with IS and
concluded that hormone treatment (prednisolone, tetracosactide depot, and ACTH) resolves
spasms quicker than VGB [42]. However, it is uncertain whether hormone treatment leads to
better outcomes. More studies, particularly long-term studies, are necessary to ascertain the long-
term developmental outcomes associated with various pharmacological agents.

7
3 Vision
Before describing the effects of VGB on vision, it is important to understand the basic principles
of retinal anatomy and physiology. The retina has a laminar organization, in which the cells of
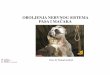
the retina are organized in layers (Figure 3.1).
Figure 3.1 – Diagram of the retina highlighting the different retinal layers and the cells found in
each layer. (Webvision, http://webvision.med.utah.edu/, Simple Anatomy of the Retina, available
under a Attribution, Noncommercial, No Derivative Works Creative Commons License © 2013)!
There are five types of neurons in the retina: photoreceptors, bipolar cells, ganglion cells,
horizontal cells, and amacrine cells. The cell bodies of these neurons are located in the inner
nuclear, outer nuclear, and ganglion cell layers, and the synaptic connections are located in the
inner and outer plexiform layers.
3.1 Image Formation
Light rays emitted by or reflected off a particular object travel through the cornea, aqueous
humour, lens and vitreous humour and are focused on the retina to form an image. The cornea
and lens are involved in refraction (bending) of the light that is necessary for image formation on
the retina. The lens adjusts its shape depending on the distance of the object being viewed in a
process called accommodation; when viewing nearby objects, the lens becomes thicker and

8
rounder, and has a higher refractive power, and when viewing distant objects, the lens becomes
flatter and has a lower refractive power.
3.2 Retinal Processing
At the level of the retina, a ray of incident light passes through all retinal layers before reaching
the photoreceptor layer. The pigmented epithelium, which lies below the photoreceptor layer
and has high melanin content, absorbs light rays preventing scattering.
Photoreceptor cells contain an inner and outer segment; the outer segment is composed of
membranous disks that contain light-sensitive photopigments. The absorption of light by these
photopigments triggers a cascade that allows the electromagnetic radiation to be converted into a
neural signal. The signal is transmitted through the retinal layers, from the photoreceptor cell to
the bipolar cell, and then to the ganglion cell. In response to light stimulation, photoreceptor and
bipolar cells produced graded potentials, whereas ganglion cells produce action potentials. The
neural signal then exits the eye through the optic nerve and reaches the brain.
3.3 Lateral Connections
In addition to the direct pathway of neural signal transmission from photoreceptor cells to
ganglion cells, there are two additional cells, horizontal cells and amacrine cells, that influence
retinal processing. Horizontal cells form synapses with photoreceptor axon terminals and bipolar
cell dendrites within the outer plexiform layer (OPL) [43], whereas amacrine cells form synapses
with bipolar cell axon terminals and ganglion cell dendrites within the inner plexiform layer
(IPL). Both horizontal and amacrine cells release γ-aminobutyric acid (GABA), an inhibitory
neurotransmitter and therefore give rise to lateral inhibition by selectively inhibiting the flow of
information down the direct pathway. Lateral inhibition thus provides the essential building
block for the pattern discrimination required for visual acuity and contrast sensitivity.
3.4 Photoreceptors
There are approximately 125 million photoreceptor cells, which can be classified as rods or
cones depending on the morphology of the outer segment. Table 3-1 summarizes the differences
between the properties of rods and cones.

9
The retina consists of roughly 120 million rods and five million cones. Rods are responsible for
scoptic vision (vision under dim light conditions) and are largely concentrated in the periphery of
the retina. Cones are responsible for photopic vision (vision under bright light conditions), and
are highly concentrated in the fovea, the central region of the retina. Unlike rods, which only
have one kind of photopigment (rhodopsin), cones have one of three different opsin molecules.
These three opsin molecules have varying absorption peaks and provide the basis for human
colour vision.
In the dark, a steady influx of sodium ions (Na+) through cGMP-gated channels found in the
photoreceptor membrane, results in a resting potential of -40 mV. In this depolarized state, the
cell releases the neurotransmitter, glutamate, which binds to receptors and results in the
depolarization of bipolar and horizontal cells. Upon light stimulation, the retinal molecule, which
is a form of Vitamin A, undergoes a change from the 11-cis to an all-trans configuration. This
triggers a biochemical cascade that results in the closure of cGMP-gated Na+ channels of the
photoreceptor membrane. The close of cGMP-gated cation channels halts the inflow of Na+, and
therefore results in the hyperpolarization of the photoreceptor cell membrane. Glutamate release
is a graded response dependent on the level of hyperpolarization.

10
Table 3-1 – Comparison of rod and cone photoreceptor properties. Rods Cones Number 120 million 5 million
Peak wavelength sensitivity 502 nm
420 nm (short wavelength cones) 530 nm (medium wavelength cones) 560 nm (long wavelength cones)
Ability to distinguish colour None Colour-sensitive Sensitivity to dim light Excellent Poor Acuity Poor Excellent Location in retina Primarily in periphery Primarily in fovea
Spatial integration Highly convergent pathways Less convergent pathways
3.5 Bipolar Cells
Individual bipolar cells synapse with rods or cones and with horizontal cells. The bipolar cells
take the signal from photoreceptors and horizontal cells and pass it on to ganglion cells, directly
or indirectly via amacrine cells. Like photoreceptors, the bipolar cells produce graded potentials.
Anatomical studies have suggested that there are 11 types of bipolar cells in the mammalian
retina; ten cone bipolar cells and one rod bipolar cell [44]. Bipolar cells connecting with rods and
some cone photoreceptors depolarize in response to an increase in retinal illumination. These are
ON-center bipolar cells. In the cone pathway, there are also bipolar cells, which hyperpolarize in
response to an increase in retinal illumination: OFF-center bipolar cells. The opposite response
of ON-center and OFF-center bipolar cells is a resultant of different glutamate receptors on their
post-synaptic membranes. OFF-center bipolar cells have ionotropic AMPA/kainate glutamate
receptors that hyperpolarize in response to reduced glutamate. ON-center bipolar cells have
metabotropic glutamate receptors (mGluR6) that depolarizes in reposes to reduced glutamate
[45]. With decreased retinal illumination, cone photoreceptors increase their glutamate release
resulting in hyperpolarization of the ON-center pathway and depolarization of the OFF-center
pathway.
Up until recently, it was believed that bipolar cells did not synapse with both rod and cone
photoreceptors. However, Pang and colleagues showed that a subpopulation of rod bipolar cells

11
receives synaptic input from cones and a subpopulation of cone bipolar cells receives synaptic
input from rods [46].
3.6 Ganglion Cells
Ganglion cells receive information from bipolar cells and amacrine cells. Ganglion cells are the
only cells in the retina that produce action potentials. Specifically, ON-center and OFF-center
ganglion cells receive input from ON-center and OFF-center bipolar cells, respectively. The
action potentials propagate to the brain via the fibres of the optic nerve.
3.7 Convergence
Rod photoreceptors converge their response to ganglion cells to a greater extent than cone
photoreceptors. An average of 120 rods converge their signal to one ganglion cell. An average of
6 cone photoreceptors converge their signal to one ganglion cell with the cones in the fovea
having a 1:1 relation to ganglion cells. This results in rods having higher sensitivity than cones;
the summation of the inputs from many rods increases the likelihood that a ganglion cell will fire
action potentials. Cone photoreceptors, which have lower convergence, are able to discriminate
fine detail (increased visual acuity).
3.8 Retinal Glia
There are three types of glial cells found in the retina: Müller cells, astroglia and microglia.
Müller cells, which are radial glia that span from the outer limiting membrane to the inner
limiting membrane, are the predominant retinal glia. Müller cells are involved in number of
functions including, but not limited to, maintaining homeostasis, glycogen storage, removal of
waste products and stabilizing pH [47]. Müller cells are also involved with the removal of
neurotransmitters, notably glutamate and GABA, following synaptic activation [48].

12
4 GABA
γ-Aminobutyric acid (GABA) is an amino acid that was synthesized in 1883 [49]. Initially, it
was known to be a metabolite of plants and microorganisms. In 1950, Eugene Roberts
discovered GABA in mice brains using chromatography techniques [50]. Subsequently, GABA
was discovered in other organs. GABA is the primary inhibitory neurotransmitter in the
mammalian central nervous system (CNS) with approximately 30-40% of the synapses in the
brain involving GABA [51].
GABA is synthesized from glutamate, the brain’s primary excitatory neurotransmitter, in
neurons by glutamic acid decarboxylase (GAD) (Figure 4.1) [52]. Vertebrates have two forms of
GAD: GAD65 and GAD67[53]. GAD65 produces mainly vesicular GABA (released at synapse)
and GAD67 produces cytosolic GABA (pancreatic signal or intracellular metabolite) [54].
Figure 4.1 – The synthesis and breakdown of γ-aminobutyric acid.
After synthesis, GABA is packaged into synaptic vesicles. Upon stimulation of the neuron,
GABA is released into the synaptic cleft via calcium-dependent exocytosis. In the synapse,
GABA binds to specific receptors on both the pre- and postsynaptic neuron and mediates their
effects. The effect of GABA is inactivated by the reuptake of GABA molecules into presynaptic
terminals and surrounding glia. GABA transporters mediate this reuptake. The GABA molecules
taken up by the presynaptic membrane can be recycled into synaptic vesicles while GABA

13
molecules taken up by glia are broken down by GABA-transaminase (GABA-T) to succinic
semi-aldehyde via oxidative deamination. In turn, succinic semi-aldehyde can be either oxidized
by succinic semi-aldehyde dehydrogenase to succinic acid, which can enter the Krebs Cycle, or it
can be converted to gamma-hydroxybutyric acid by succinic semi-aldehyde reductase [55]. The
conversion of glutamate to succinate is known as the “GABA shunt.”
4.1 GABA Receptors
There are currently three known classes of GABA receptors: GABAA, GABAB and GABAC.
4.1.1 GABAA Receptors
GABAA receptors are ligand-gated ion channels that are responsible for fast synaptic inhibition
in the adult CNS [56]. The binding of GABA molecules to these receptors causes the influx of
chloride (Cl-) ions into the cell. As negatively charged ions enter the cell, the neuron becomes
less likely to depolarize. The GABAA receptors are heteropentameric complexes composed of 19
classes of subunits (α 1–6, β 1–3, γ 1–3, δ, ε, θ, π and ρ 1–3) [57]. Different subunit
combinations give rise to different subtypes of GABAA receptors each with unique physiological
and pharmacological properties. The expression of GABAA receptor subunits is
developmentally regulated causing GABA responses to vary between immature and adult
neurons [58]. GABAA receptors complexes contain allosteric binding sites for benzodiazepines,
neurosteroids, and barbiturates [56].
4.1.2 GABAB Receptors
GABAB receptors are G-protein coupled metabotropic receptors that mediate the prolonged
effect of GABA [59, 60]. The binding of GABA to GABAB receptors triggers a G-protein
mediated intracellular signaling cascade. Postsynaptically, this results in the activation of G-
protein mediated inwardly rectifying potassium (K+) (GIRK) channels, causing an efflux of K+
ions. As positively charged ions leave the cell, it becomes more difficult for the neuron to
depolarize. Presynaptically, the GABA triggered G-protein mediated cascade results in alteration
of pre-synaptic voltage-gated calcium channels that mediate neurotransmitter release. Recent
studies show postsynaptic crosstalk between GABAA AND GABAB receptors; activation of

14
GABAB receptor enhances GABAA currents [61, 62]. Currently, baclofen is the only known
agonist of GABAB receptors [63].
4.1.3 GABAC Receptors
Johnston and colleagues identified a third class of GABA receptors that were insensitive to
bicuculline and baclofen (GABAA antagonist and GABAB agonist respectively) [64]. These
GABAC receptors are ligand-gated chloride ion channels that mediate the influx of Cl- ions upon
binding of GABA molecules. As negatively charged ions enter the cell, the neuron becomes less
likely to depolarize.
While both GABAA and GABAC receptors are ionotropic, GABAC receptors are functionally and
spatially distinct from GABAA receptors and are composed mostly of homoligomeric ρ subunits
[65, 66]. Compared to GABAA receptors, GABAC receptors are tenfold more sensitive to GABA,
have slower activation/inactivation kinetics, and have weak desensitization [67, 68]. The
differing kinetic properties of GABAA and GABAC receptors lead to differences in the time
course of the GABA response [69]. Retinal bipolar cells that lack GABAC receptors have briefer
responses to GABA when compared to wild-type mice [70].
GABAA receptors are found throughout the CNS while GABAC receptors have restricted
distribution. GABAC receptors are primarily found in the retina, but are found in others parts of
the CNS including the hippocampus, spinal cord, superior colliculus, and pituitary [65]. Due to
their sustained responses, GABAC receptors are ideally suited for modulation of graded
potentials and play a prominent role in the strong lateral inhibition of the retinal system [67, 71].
4.2 GABA in the Retina
GABAA receptors are found on every type of neuron in the retina (both pre-synaptically and
post-synaptically) except for rod photoreceptors [72]. GABAB receptors are found post-
synaptically on ganglion cells and both pre- and post-synaptically on amacrine cells [73].
GABAC receptors are found predominantly on bipolar cells, coexisting with GABAA receptors
[65, 66]. In the mammalian retina, GABAC receptors are mainly expressed on the axon terminal
regions of bipolar cells but are also found in dendritic regions of bipolar cells. GABAC receptors
are present in rod-driven horizontal cells of white perch [74], cone-driven horizontal cells of

15
catfish [75], ganglion cells of salamander [76] and cone photoreceptors of pigs [77]. They have
not been found in the horizontal cells of mammals [78].
Both GABAA and GABAC receptors are involved in inhibition at the inner plexiform layer with
GABAA receptors being localized at the dendrites of amacrine and ganglion cells and GABAC
receptors being localized at the axon terminals of bipolar cells [79, 80]. The role of GABAC
receptors at the inner plexiform layer was determined using mice that lack GABAC receptors and
by using receptor specific antagonists [71]. Mice lacking GABAC receptors have shortened
GABA currents in rod bipolar cells compared to wild-type mice. The presence of different
GABA receptors contributes to the time course of the GABA response in the retina. In rat bipolar
cells, the initial GABA response is mediated by GABAA receptors and the late GABA response
is dominated by GABAC receptors [71, 81]. The depolarizing effect of GABA at the dendrites of
rod bipolar cells, elicited through GABAA receptors, is thought to contribute to lateral inhibition
and visual discrimination [82].
4.3 Excitatory Effects of GABA
In the adult brain, binding of GABA molecules to GABAA receptors causes influx of chloride,
leading to cell hyperpolarization. However, in certain circumstances, GABAA receptor activation
leads to chloride efflux and subsequently excitation. If the chloride equilibrium potential is
negative respective to the resting membrane potential, then GABA activation causes
hyperpolarization. If the chloride equilibrium potential is positive with respect to the resting
membrane potential, then GABA activation causes depolarization. Chloride concentrations are
influenced by the relative expressions of NKCC1, a Na+/K+/Cl− cotransporter, and KCC2, a
K+/Cl- cotransporter. NKCC1 transports chloride into cells leading to high intracellular chloride
concentrations whereas KCC2, transports chloride ions out of the cell and causes intracellular
chloride concentrations to decrease.
4.3.1 Excitatory Effects During Development
Before the maturation of the glutamate system, GABA is the major excitatory neurotransmitter in
several regions of the mammalian brain including the hippocampus and the neocortex [83, 84].
Rat hippocampal slices exposed to bicuculline, a GABAA receptor blocker, after postnatal day 8

16
(P8) show cell depolarization, an effect that is also observed in adults exposed to bicuculline
[85]. However, between days P0 and P7, bicuculline causes hyperpolarization of the neurons.
This effect is due to the relatively higher concentrations of chloride ions inside the immature
neurons. Activation of the GABAA receptors leads to an efflux of Cl- ions and membrane
depolarization [86]. GABA-mediated chloride ion channels respond based on the
electrochemical gradient across the neuronal membrane.
The expression of NKCC1 during early development allows high intracellular Cl-
concentrations, leading to depolarizing actions of GABA [87, 88]. As development continues,
the expression of NKCC1 decreases and the expression of KCC2 increases [89]. KCC2
transports chloride ions out of the cell and causes the intracellular chloride concentration to
decrease, leading to the hyperpolarizing effect of GABA seen in mature neurons.
The immaturity of the GABA system may lead to the enhanced susceptibility to develop seizures
during early life, especially in children with other underlying pathologies[58].
4.3.2 Subcellular and Regional Differences
In addition to developmental differential expression of NKKC1 and KCC2, there are also
regional and subcellular differences in the expression of these co-transporters.
Recent studies show that in addition to existing on the somatodendritric compartment of the
neuron, GABAA receptors also exist on axons [90]. Unlike somatodendritric GABAA receptors,
axonal GABAA receptors usually depolarize due to the relatively high axonal Cl- concentrations
[91, 92]. Gulyas and colleagues showed higher expression of KCC2 in dendrites of principal
cells and interneurons compared to soma and axons [93]. This explains why the activation of
axonal GABAA receptors increases the excitability of the axon.
Excitatory effects of GABA have been observed in parts of the cerebellar network [94],
substantia nigra [95], hippocampus [96], and cortex [97].
GABA in the Retina
In the retina, GABA seems to have both inhibitory and excitatory effects. KCC2 is preferentially
expressed in ganglion cells, bipolar axons, and OFF bipolar dendrites whereas NKCC1 is

17
preferentially expressed in horizontal cells and ON bipolar dendrites [98]. The differential
distribution of NKCC1 and KCC2 correspond to the opposing effects of GABA seen in different
retinal neurons. The same neuron can express both transporters; NKCC1 and KCC2 are
preferentially expressed on the ON bipolar dendrite and axon, respectively [98]. Horizontal cells
synapse with bipolar cell dendrites and cause depolarization and amacrine cells synapse with
bipolar cell axons and cause hyperpolarization.
4.4 GABA Response in Epilepsy
Perturbations in GABAergic inhibition are associated with various neurological diseases
including epilepsy, anxiety disorders and schizophrenia [99]. Generally speaking, seizures are a
result of an imbalance between excitation and inhibition. However, the mechanisms underlying
seizures are more complex and vary with seizure types.
Both animal studies and clinical research show that epilepsy may stem from GABA dysfunction
and dysregulation and that epilepsy may cause changes in GABA function [58]. Epilepsy-prone
animals have fewer GABA receptors [100] and an increased density of GABAergic neurons in
the inferior colliculus [101] and the hippocampus [102]. Similarly, humans with seizure
disorders were observed to have changes in their GABAergic system. The GABAA receptor
plays an important role in synchronization and desynchronization of thalamocortical circuitry
and changes to these processes lead to absence seizures [99]. Mutations in GABAA receptor
subunits have been associated with several epilepsy types including IS, atypical absences, and
myoclonus [103]. In addition to the physiological consequences of loss of subunit functional
activity, Chiu and colleagues have proposed that alterations of subunits lead to developmental
effects [104]. Vergnes and colleagues found that low-doses of GABAB receptor antagonists
prevent absence seizures but high doses of GABAB receptor antagonists cause convulsive
seizures [105]. This suggests that GABAB receptor-mediated inhibition is involved in preventing
convulsive seizures.
Since GABA opposes the effect of glutamate, an excitatory neurotransmitter involved in kindling
and spread of seizures [106], some anti-epileptic drugs work by increasing CNS concentrations
of GABA [107]. These anti-epileptic drugs (AEDs) include VGB and tiagabine. VGB works by
inhibiting GABA-T and thereby increasing GABA concentrations in the synapse while tiagabine

18
works by inhibiting GABA reuptake transporter GAT1 [108]. In contrast to VGB, tiagabine is
associated with visual fields and electroretinograms that are similar to epilepsy controls [109].
This difference in visual function between the two drugs may be explained by differences in
retinal GABA concentrations. In animal studies, tiagabine does not increase GABA
concentrations in the retina and CSF [110].
4.4.1 The Role of Excitation
The excitatory action of GABA in immature neurons, adult dorsal root ganglion, and adult CA1
hippocampal pyramidal cells have been known for some time [111]. More recently, it has been
understood that the GABA response may also change from hyperpolarizing to depolarizing in
some pathological conditions.
The increased susceptibility of neonates to hypersynchronous activity is thought to reflect the
immaturity of GABAergic inhibitory systems [58]. This also explains the increased prevalence
of seizures among males, since males experience delayed maturation of the GABA system
relative to females. Seizures in neonates do not respond as well to anti-convulsants as they do in
adults [112, 113]. This may be accounted by the excitability of immature neurons caused by
elevated intracellular Cl- levels.
Both animal studies and clinical research show that epilepsy may stem from aberrant changes in
NKCC1 and KCC2 expression. Animal models of neuropathic pain and epilepsy show a down
regulation of KCC2 expression [114, 115]. Mice with reduced KCC2 expression have
hyperexcitable hippocampal CA1 neurons and are more likely to have epilepsy [116, 117].
Patients with temporal lobe epilepsy also have increased NKCC1 expression and reduced KCC2
expression resulting in depolarizing GABAergic neurons [118, 119]. NKCC1 causes
intracellular accumulation of Cl-, thereby facilitating seizures.
This suggests that pharmacological agents that either block NKCC1 activity or act as KCC2
transporters may be effective anticonvulsant therapies. Recent studies show that bumetanide, a
NKCC1 blocker, decreases intracellular chloride levels in neurons, thereby reducing the
hyperpolarizing effect of GABA in the immature mouse brain [120, 121]. Pilot studies in
neonates and adults show suppression of seizure activity with bumetanide therapy [122, 123].

19
However, Wang and Kriegstein caution the use of bumetanide in neonatal seizures since it
disrupts dendritic cortical formation during a critical period and leads to behavioural
abnormalities later in life [124]. Further studies are necessary to assess bumetanide as a
pharmacological therapy for seizures.
!

20
5 Vigabatrin
5.1 Regulatory History of Vigabatrin
Using rational drug design, VGB was synthesized in 1974 in an attempt to create a drug that
would increase CNS levels of GABA and thereby inhibit epileptogenic circuits [125-127]. In the
mid 1980s, the identification of intramyelinic edema in VGB-exposed animals brought clinical
trials to a temporary halt. However, the intramyelinic edema was not demonstrated in primates
and VGB trials resumed [128].
VGB (Sabril®) was first licensed in 1989 by UK and the Republic of Ireland for the effective
management of seizures. VGB soon became available in Canada and in other countries, but not
in USA [129, 130].
In the US, the identification of visual field reductions in 1997 (detailed discussion to follow in
Section 6) slowed down the regulatory process. In 2009, VGB was approved by the U.S Food
and Drug Administration (FDA) as a monotherapy for treating IS in children 1 month to 2 years
of age and as an adjunctive therapy for refractory complex partial seizures in adults. This
approval came following placebo-controlled trials [131, 132], open trials [133, 134] and dose-
response trials [135] that found VGB to be effective in seizure management.
Due to concerns of visual field reductions, specific guidelines have been developed for patients
undergoing VGB therapy 136]. Lundbeck implemented a comprehensive Risk Evaluation and
Mitigation Strategy (REMS) through the Support, Help and Resources for Epilepsy (SHARE)
program [137]. This program requires that all VGB users undergo periodic visual assessment.
The dosage of VGB should start at 50 mg/kg/day, and if necessary, increase up to 150
mg/kg/day. Visual field testing must be done no later than four weeks after initiation of treatment
(baseline) and should be continued every 3 months while on treatment to determine if retinal
toxicity has developed. After discontinuation of the drug, assessment should be done every 3 – 6
months. VGB should be issued to patients on a trial basis and efficacy should be assessed two to
four weeks after initial dose. If VGB therapy is deemed successful, then it can be continued for
6-9 months [136].

21
5.2 Pharmacology of Vigabatrin
VGB is orally administered and is produced as a racemic mixture with equal proportions of the
S(+) and R(-) enantiomers. The pharmacologically active compound is the S(+) enantiomer,
which binds to GABA-T [138]. VGB has a favourable pharmacokinetic profile with >90%
bioavailability, negligible plasma protein binding and <5% liver metabolism [139]. VGB is
absorbed rapidly in the gastrointestinal tract and plasma concentrations reach peak levels 1 to 2
hours following administration. VGB has a half-life between five to eight hours in adults [140].
VGB can be detected in the cerebrospinal fluid (CSF) six hours following a single dose
administration with CSF concentrations being 10% of plasma concentrations [141]. Oral
administration of VGB produces dose-related increases in GABA concentrations in human CNS
[142]. VGB is primarily eliminated through renal excretion and due to low hepatic metabolism, it
is excreted mainly unchanged. Within 24 hours of oral administration, 50% of the S(+)
enantiomer and 60% of the R(-) enantiomer is recovered from urine [140].
5.3 Mechanism of Action
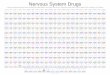
VGB (4-amino-6-hexenoic acid) is a structural analogue of the inhibitory transmitter, GABA,
and differs from GABA by the addition of a vinyl group (Figure 5.1). It was specifically
designed to stop seizures by irreversibly inhibiting GABA-T, the enzyme responsible for the
breakdown of GABA in the central nervous system [125]. GABA-T is present in neurons and
glia and is responsible for breaking down GABA into succinic semialdehyde via oxidative
deamination. The inhibition of GABA-T leads to a dose-dependent increase in free GABA in all
areas of the mouse brain [143]. Since VGB binds to GABA-T irreversibly, re-synthesis of the
enzyme is the only way to restore GABA-T activity. Animal studies show that administration of
a single dose of VGB causes GABA levels to be elevated for 24 hours [125]. Using non-invasive
1H magnetic resonance spectroscopy, patients receiving standard doses of VGB were found to
have 2-3 times the concentration of GABA in the brain compared to controls [144].

22
!
Figure 5.1 – A) Structure of γ –aminobutryic acid (GABA). B) Structure of γ –vinyl GABA
(vigabatrin).
In addition to inhibiting GABA-T, VGB has also been found to decrease uptake of GABA by rat
astrocytes [145] and to stimulate GABA release [146]. These mechanisms of action lead to a
build-up of GABA in the brain, retina and cerebrospinal fluids [144, 147]. VGB-induced
increases in GABA concentrations above 1.8 mmol/kg have been associated with a twofold
decrease in seizure frequency [148].
This increase in GABA levels is most marked in the retina, where GABA increases to 260% of
control levels in Sprague Dawley rats [110]. Furthermore, following VGB administration,
concentrations in the retina are up to 18.5 times higher than in the brain in animal studies [149].
This is likely due to differences in the permeability of VGB in the blood-retina barrier and the
blood-brain barrier.
Recently VGB has been shown to alter mTOR pathway activation in a mouse model of TSC
[150]. Mutations associated with TSC lead to loss of inhibitory control of the mTOR pathway
and subsequently glial proliferation. VGB’s ability to inhibit the mTOR pathway may explain its
increased efficacy in IS patients with an etiology of TSC.
5.4 Clinical Efficacy in Adults
Various randomized control trials have been carried out in adult patients with different seizure
types to determine the efficacy of VGB. Gidal and colleagues reviewed ten randomized trials
looking at adults on VGB as an add-on therapy for uncontrolled seizures [151]. Most patients
had partial seizures (without or without secondary generalization) and some patients had

23
generalized seizures. With VGB treatment, 24–67% of patients achieved a ≤50% reduction in
seizure activity with VGB being particularly effective for patients with partial seizures. VGB is
also effective in treating cocaine and methamphetamine dependency [152, 153].
5.5 Clinical Efficacy for Infantile Spasms
Early studies examined the efficacy of VGB in childhood refractory epilepsies. Children with
partial seizures responded well to VGB while children with myoclonic epilepsies and Lennox-
Gastaut syndrome did not respond as well [132, 134]. In a cohort of children with refractory IS,
VGB was associated with complete suppression of spasms in 43% of patients and 68% of the
patients achieved 50% or greater reduction in seizure frequency [133].
5.5.1 Randomized Controlled Trials
Since these early studies, several randomized controlled trials have examined the efficacy and
tolerability of VGB in children with infantile spams (Table 5-1).
Table 5-1 – Randomized controls trials of vigabatrin in the treatment of IS. VGB: Vigabatrin!
Author, Year Number of patients treated with VGB
Comparison Treatment (n)
Cessation of spasms – VGB
Cessation of spasms – Comparison
Adverse Events with VGB
Chiron et al, 1997 [40]
Initial:11 Crossover: 7
Hydrocotisone (Initial: 11)
Initial: 100% Crossover: 100%
Initial: 45% 44%
Vigevano et al, 1997 [154]
Initial:23 Crossover: 5
ACTH (Initial: 9; Crossover: 12)
Initial: 48% Crossover: 40%
Initial: 74% Crossover: 92% 13%
Appleton et al, 1999 [131] Initial: 20 Placebo VGB
initial:35% Initial: 10% 60%
Elterman et al, 2001 [135]
Low dose: 75 High dose : 67 NA Low dose: 11%
High dose : 36% NA 90%
Lux et al, 2004 [38, 155]
Initial: 52 Crossover: 12
Tetracosactide (Initial: 55; Crossover: 19)
Initial: 54% Crossover: 75%
Initial: 73% Crossover: 74% 10%
Corticotropin and other corticosteroids were long considered the standard of care for treating IS.
One of the first randomized controlled trials for VGB compared VGB with hydrocortisone [40].

24
This response-mediated crossover study only included individuals with an aetiolgy of TSC.
After one month of treatment, all 11 patients on VGB achieved spasm cessation compared to five
of the 11 patients on hydrocortisone. The seven patients who did not respond to hydrocortisone
were crossed to VGB and all achieved spasm cessation.
In another response-mediated crossover study, this time comparing VGB and ACTH, VGB had
better tolerability and similar efficacy for cryptogenic cases of IS [154]. VGB is more effective
in patients with TSC and cerebral malformations whereas corticotropin is more effective in
patients with perianal hypoxic/ischemic injuries [154]. Other studies have also shown VGB to be
highly efficacious for etiologies of TSC [40, 133].
Elterman and colleagues designed a large, Class III, double-blind randomized controlled trial that
examined the differences in efficacy between low-dose (18-36 mg/kg/day) and high-dose VGB
treatment(100-148 mg/kg/day) [135]. High-dose VGB therapy was associated with shorter
response times and higher efficacy rates. Following three months of VGB treatment, 65% of
patients with IS achieved spasm-cessation. Longer-term follow-up of patients treated with VGB
monotherapy show relapse rates of 12% and 25% in primary responders with high-dose and low-
dose VGB treatment, respectively [156].
The United Kingdom IS Study (UKISS) was a large randomized controlled study that looked at
both the short-term and long-term differences between individuals from 150 UK hospitals treated
with VGB and hormonal therapy (ACTH or prednisolone) [38, 155, 157]. Within 14 days of
treatment initiation, hormonal therapy was better at controlling spasms; 54% of patients on VGB
and 73% of patients on hormonal therapy achieved spasm cessation. Longer-term follow up at
14 months and at 4 years, did not show any significant differences between the two groups in
terms of development, adverse events or rate of seizure cessation.
Another randomized controlled trial (The International Collaborative Infantile Spasms Study) is
currently underway in Europe and Australia to investigate efficacy of VGB and hormonal
therapy (tetracosactide depot and/or prednisolone) versus hormonal therapy alone [158]. This
multi-centre study is anticipated to be completed by 2014.

25
5.6 Non-vision Adverse Events
5.6.1 Animal Toxicity
Administration of high doses of VGB (1,000 mg/kg/day) resulted in decreased food intake
resulting in weight loss and death in rats and dogs [128]. Rodents and dogs exposed to high
doses of VGB developed intramyelinic edema (microvacuolation) in the brain, most notably in
white-matter tracts (cerebellum, reticular formation and optic tract in rats and columns of fornix
and optic tract in dogs).
5.6.2 Clinical Studies
VGB is well tolerated with treatment-related adverse events usually being mild [156]. In a
retrospective study of 250 infants on VGB for IS, only 13% showed adverse events[159]. A later
study[135] examining the tolerability of VGB in 167 patients found that the most common
adverse events were sedation(25%), insomnia(9%) and irritability(9%). These effects are mild
and only 6.3% of the patients discontinued treatment due to adverse events[135]. The UKISS
study found that compared to hormone therapy, VGB caused increased drowsiness, decreased
irritability and increased appetite [38, 155].
Intramyelinic edema has not been observed in adult patients [160, 161]. However, some infants
treated with VGB also show intramyelinic edema in subcortical structures[162, 163]. Recent
reports also show MRI changes and restricted diffusion-weighted images in the thalamus, basal
ganglia, and brainstem of patients receiving VGB treatment [164]. However, these effects are
reversible upon discontinuation of the drug.
!

26
6 Vigabatrin and Visual Side Effects in Human
6.1 Vigabatrin Associated Visual Field Loss (VGB-VFL)
In 1997, Eke, Talbot and Lawden [165] reported symptomatic constriction of the visual field in
three adults following VGB treatment. In one case, the nasal fields were affected to a greater
extent than the temporal fields. The other two cases did not show this pattern of nasal
predominance.
Soon after, other studies reported similar findings of constricted visual fields in adults on VGB
for refractory partial onset seizures [166], focal epilepsy [167] and complex partial seizures
[168].
The visual field constriction associated with VGB (Vigabatrin Associated Visual Field Loss;
VGB-VFL) is a bilateral, concentric constriction with temporal and macular sparing [169].
Compared to controls with epilepsy and tiagabine-treated patients, VGB-treated adult patients
had an average of 20-40 degree field loss as measured by Goldmann kinetic perimetry [109].
Kalviainen and colleagues designed the first and only RCT investigating visual field reductions
for VGB-exposed patients. 135 patients with new-onset partial epilepsy were assigned either
VGB or carbamazepine between 1988 and 1995 [170]. A subset of those patients (n=50; ages: 19
– 73 years) continued with study treatment and were followed up for ophthalmological
examination. Visual fields were assessed using Goldmann Kinetic perimetry. 41% (13/32) of
VGB-treated patients developed visual field reductions and none of the 18 carbamazepine-
treated patients developed visual field reductions. Of the 13 patients with visual field reductions,
3 had severe reductions and 10 had mild reductions. None of the individuals noticed any
abnormalities prior to the study.
Vanhatalo and Pääkkönen reported the first incidences of visual field constrictions in children;
two girls, ages 10 and 15, with complex partial epilepsy showed VGB-associated field loss
similar to those reported in adults [171]. Subsequent studies have also identified field loss in
children receiving VGB treatment [172-174].

27
Most measurements of visual fields are obtained in a light-adapted state (cone system). To
determine whether the rod system is also affected with VGB therapy, Banin and colleagues
assessed dark-adapted visual fields [175]. Patients with constriction of the visual fields in the
light-adapted state also show constrictions of the dark-adapted visual fields, suggesting
involvement of both the cone and rod systems in VGB toxicity.
Risk factors for VGB-VFL include male gender, use of additional AEDs, and longer duration of
VGB treatment [176].
6.1.1 Prevalence in Adults
Initially, the incidence of visual field constriction was estimated to be less than 0.1% but
subsequent studies suggested that this was an underestimate since many cases are asymptomatic
[177-179]. In adults treated with VGB for refractory partial epilepsy, 53% had mild visual field
defects (60–80° monocular temporal field retained), 17% had moderate defects (30–60° temporal
field retained) and 2% had severe defects (<30° temporal field retained) [180]. Many patients do
not recognize the constriction since VGB does not impair central visual acuity. Only a small
fraction of the patients experience symptomatic visual field reductions and these reductions may
be noticed 3 months to 3 years after initiation of VGB treatment.
Table 6-1 – Prevalence of Vigabatrin-Associated Visual Field Loss in adults. VFL = Visual field loss
Author Method of Perimetry Prevalence (n) Daneshvar et al, 1999 [178] Static 29% (41)
Kälviäinen et al, 1999 [170] Kinetic 41% (32); 31% mild VFL, 9% severe VFL
Miller et al, 1999 [179] Static and Kinetic “nearly 50%” (39) Wild et al, 1999 [181] Static and Kinetic 29% (99) Lawden et al, 1999 [169] Static 52% (31) Ardnt et al, 1999 [182] Static 60% (12/20) Newman et al, 2002 [183] Kinetic 20% (100) Van der Torren et al, 2002 [184] Static 69%(29)
Jensen et al, 2002 [185] Kinetic 30% (3/10)
Midelfart et al, 2000 [186] Static 83% (15/18 right eyes); 33% mild, 50% severe

28
Table 6-1 highlights some studies that examined the prevalence of VGB-VFL. The range of
prevalence estimates is large due to different methods of field assessment and different criteria.
A recent systematic review of thirty-two studies published between 1999 and 2009 estimated the
prevalence of vigabatrin-associated visual field defects to be 52% (95% CI 46-59) in adults
[187].
6.1.2 Prevalence in Children
Perimetric testing is much more difficult in young and developmentally delayed children and
thus estimates of the prevalence of VGB-VFL in infants are scarce. In a group of 153 children
who had been on VGB, only 12 children were able to perform visual field testing (Goldmann).
Five of the 12 children (42%) showed VGB-VFL whereas only one of the 12 (8%) children on
other AEDs showed visual field reductions [172]. Table 6-2 gives a summary of estimated
prevalence of VGB-VFL in pediatric cohorts.
Maguire and colleagues conducted a systematic review of ten pediatric studies and estimated the
prevalence of visual field constrictions to be 34% (95% CI 25-42) in children exposed to VGB
and 7% in unexposed controls [187]. The age range of the participants in the studies was 2.5
years – 21 years and none of the participants had been exposed to VGB in infancy.
To date, there are only two studies that examine VFL using conventional methods in
children with VGB-exposure during infancy [172, 188]. Gaily and colleagues reported visual
field results in 16 school-age children, all of whom were exposed to VGB during infancy. One
VGB-exposed child showed mild VFL. Similar results were observed by Wohlrab and
colleagues [189]; one of 15 children exposed to VGB during infancy showed VFL. These studies
seem to indicate that the prevalence of the VGB-VFL is lower in younger children.
Since conventional perimetric testing methods such as Humphreys Visual Field Analyzer
and Goldmann Perimetry may not be feasible in young children and in children with
developmental delay, non-conventional methods of measuring visual fields are used often. Werth

29
& Schädler [190] assessed visual fields using a non-commercial arc perimeter and preferential
looking methods. Agrawal and colleagues [191] employed white sphere kinetic perimetry
(WSKP) to measure the extent of visual fields in children. WSKP has better compliance rates
than Goldmann perimetry (28/31 versus 9/31) and both tests yield similar results. The proportion
of children who develop constriction of the visual field as measured by WSKP (8/28; 29%) is
similar to the proportion reported by Werth & Schädler using arc perimetry (8/30; 27%).
Table 6-2 – Prevalence of Vigabatrin-Associated Visual Field Loss in children.
Author Method of Perimetry Prevalence (n) Unable to perform Visual Fields
Wohlrab et al, 1999 [172] Kinetic 42% (12) 92%
Iannetti et al, 2000 [174] Kinetic and Static 19% (21) 30%
Gross-Tsur et al, 2000 [192] Kinetic and Static 65%(17) 29%
Pelosse et al, 2001 [193] Kinetic 55%(11) 21%
Vanhatalo et al, 2002 [173] Kinetic 19% (91) NA
Spencer & Harding, 2003 [194] Kinetic and Static 36%(11) 72%
Pojda-Wilczek et al, 2005 [195] Static 53%(20) NA
Ascaso et al, 2003 [196] Static 20%(15) NA
Werth & Schädler, 2006 [190] Static 27% (30) 46%
Agrawal et al, 2009 [191] Kinetic 29% (28) 10%
Russell-Eggit et al, 2000 [197] Kinetic 71% (10/14) NA

30
6.2 Ophthalmoscopic Findings
Ophthalmoscopic abnormalities have been described in association with VGB-VFL. In the
original cases described by Eke and colleagues [165], two individuals had “slightly pale” optic
discs and the other individual had a “slightly atrophic” peripheral retina. In a cohort of twelve
patients with VGB-VFL, four had optic disc pallor, five had slightly pale discs and the remaining
three individuals had normal optic discs [169]. Miller and colleagues found that retinal
abnormalities were present in 72% (23/32) of VGB-treated individuals and absent in all ten
controls with epilepsy [179].
Clinical fundoscopy examinations of children on VGB have shown peripheral retinal atrophy and
secondary optic nerve atrophy [198]. In mild cases of visual field loss, the nasal quadrant of the
optic disc is affected and in more severe cases, all quadrants except the temporal quadrant are
affected [199]. Since this pattern of nasal nerve fibre loss is characteristic of VGB toxicity and
differs from the nerve atrophy patterns seen in other optic neuropathies where temporal fibres are
affected, it is often referred to as “inverse atrophy.” This is consistent with a post-mortem
examination of the eyes of a VGB-exposed adult; the optic nerves were severely atrophic and the
macular fibres were relatively persevered [200]. This pattern is in agreement with the loss of
peripheral ganglion cells.
6.3 Other Clinical Findings
In a study examining visual function in adults on VGB for complex partial epilepsy, some
patients showed reduced visual acuity and abnormal colour vision [179]. However, 28% of
patients treated with carbamazepine also show abnormal colour vision and hence colour vision
abnormalities may not be specific to VGB [201]. There is a slight correlation between the extent
of the visual field and contrast sensitivity in VGB-treated patients [202].
6.4 Retinal Defects in Animal Studies
The first report of retinal toxicity described the disorganization of the outer nuclear layer (ONL)
near the peripheral retina of VGB-exposed albino, but not pigmented, rats [203]. Since the
identification of VGB-VFL in humans in 1997, various studies have examined the cellular origin
of retinal defects using animal models. Duboc and colleagues confirmed the disorganization of

31
the ONL and also found photoreceptor damage with VGB administration [204]. Photoreceptor
damage is present in central areas and photoreceptor nuclei moved into the inner/outer segment
and toward the RPE [204, 205]. These changes precede changes in the electroretinogram (ERG),
(irreversible reduction in amplitudes of the photopic and flicker responses) [204].
Prior to the onset of ONL disorganization, VGB-treated mice demonstrated neuronal plasticity in
the retina [205]. This suggests that VGB treatment can have various step-wise outcomes starting
with changes in plasticity and ONL disorganization and leading to changes in various ERG
measures.
Immunohistochemical examination reveals the accumulation of GABA in Müller glial cells of
VGB-treated rats, but not controls [206]. VGB administration also led to gliosis as demonstrated
by increased glial fibrillary acidic protein (GFAP) expression [204, 207]. However, it is
uncertain whether the glial reaction precedes or follows the photoreceptor damage.
!

32
7 Visual Electrophysiology
7.1 Full-field Electroretinogram (ERG)
The full-field electroretinogram (ERG) is a visual electrophysiological test used in clinic to
quantify the mass electrical response of the retina to light stimulation.
In darkness the photoreceptor is in a depolarized state, with a membrane potential of roughly -40
mV. Progressive increases in the intensity of a flash causes the potential across the receptor
membrane to become more negative, and the response saturates when the membrane potential
reaches about -65 mV. This is the first stage of the ERG response.
Depending on the state of retinal light adaptation and the testing conditions, the ERG response
can vary greatly. To reduce this variability and to make results from various testing centres
comparable, the International Society of Clinical Electrophysiology of Vision (ISCEV) have
described 5 standard full-field ERG responses (Figure 7-1) [208].
(1) Dark-adapted 0.01 ERG (rod response) – maximal response of dark-adapted retina to dim
light
(2) Dark-adapted 3.0 ERG (combined rod–cone response) – maximal response of dark-adapted
retina to bright light
(3) Dark-adapted 3.0 oscillatory potentials – scotopic and photopic wavelets on characteristic
waveforms
(4) Light-adapted 3.0 ERG (cone response) – response of light-adapted retina to bright light
(5) Light-adapted3.0 flicker (30 Hz flicker) – response of light-adapted retina to light flickering
at 30 Hz
The first three tests are performed after adaptation to a dark background. The last two tests are
performed after adaptation to a light background, allowing the cone-system to be isolated.

33
By changing the stimulus and testing parameters, the ERG can be used to noninvasively measure
responses from various retinal cells. The leading edge of the a-wave reflects activity of the
photoreceptors and the b-wave reflects activity of inner retinal cells (bipolar, horizontal and
amacrine cells). ERG oscillatory potentials are observed in the rising phase of the b-wave and are
thought to arise mainly from photoreceptor activity. These studies, which were performed on
rabbit retina, also reveal that ON bipolar cells and horizontal cells in the OFF pathway do not
contribute much to the oscillatory potential response [209].
!
Figure 7-1 – Sample waveform of the standard electroretinogram tests as defined by The
International Society for Clinical Electrophysiology of Vision (ISCEV). Large arrowheads
(pointing down) indicate the onset of a visual stimulus (light) and dotted arrows (pointing right)
indicate the implicit time, the time required from the onset of visual stimuli until the peak of
wave. The a-wave amplitude is measured from the baseline to the trough, while the b-wave
amplitude is measured from the a-wave trough to the b-wave peak. Source: Marmor et al., 2009
[208]; Copyright permission has been obtained, please see Copyright Acknowledgements.
7.1.1 ERG and Vigabatrin
Various electrophysiological measures of visual function have been used to detect putative VGB-
induced retinal toxicity.

34
Several ERG responses, including cone b-wave amplitude, 30-Hz flicker amplitude and photopic
oscillatory potentials, correlate with VGB therapy (Table 7-1) and VGB-VFL (Table 7-2). Cone
system dysfunction, as measured by ERG, is associated with symptoms of visual blurring and
visual field reductions [177].
Table 7-1 – Electroretinogram changes associated with vigabatrin therapy. Reference n Findings Arndt et al, 1999 [182] 20 Unrecordable OPs (10/20) Van der Torren et al, 2002 [184] 29 adults Reduced scotopic b-wave amplitude (11/29)
Reduced photopic b-wave amplitude (11/29)
Comaish et al, 2002 [217] 14 adults Reduced cone and rod b-wave amplitudes Reduced and delayed of OPs
Jensen et al, 2002 [185] 10; 9 adults and 1 child
Abnormal OP (8/10) Abnormal cone/rod response (9/10)
Morong et al, 2003 [216] 26 infants Reduced OP amplitudes Parisi et al, 2003 [215] 1 child Reduced cotopic threshold
Kjellstrom et al, 2011 [218] 14 children Reduced amplitudes for rod b-wave, combined rod-cone response, and 30-Hz flicker response
Moskowitz et al, 2012 [219] 114 children Abnormal photopic d-wave (113/114); Abnormal scotopic log σ and photopic b-wave implicit time (>50%)
!
Harding and colleagues attempted to separate the electrophysiological responses associated with
VGB use from those associated with VGB-VFL [210]. 18 of 26 VGB-exposed patients had
visual field loss and this loss was associated with reduced amplitude and increased latency of the
cone response. The amplitude of the flicker response was the best predictor of VGB-VFL with a
sensitivity of 100% and a specificity of 75%. Miller and colleagues also found that the flicker
response correlated strongly with the degree of visual field loss in adults on VGB for complex
partial seizures [179]. However, in another study of individuals with VGB-VFL, only one of ten
cases was associated with reduction in the 30-Hz flicker response [178].
Photopic amplitude, scotopic a-wave latency, and latency of OP2 were associated with VGB
therapy but not with field loss [210]. Some of the changes in the ERG may result from the
elevated GABA levels caused by VGB (i.e. non-toxic change) while other changes in the ERG
may result from retinal toxicity. To separate the effects of the drugs from toxicity effects, several
studies have performed electrophysiological testing following VGB discontinuation.

35
Some electrophysiological responses may be reversible in patients with mild reductions in visual
fields following discontinuation of VGB [211, 212]. Following at least six VGB-free months,
there is recovery of the ERG rod b-wave amplitude [211] and oscillatory potentials [213]. The
recovery of the photopic and scotopic oscillatory potentials suggests that amacrine cells of the
inner retina are affected with VGB therapy. VGB increases retinal GABA levels. Amacrine cells,
which have a high density of GABA receptors, may cause abnormal ERG responses in patients
on VGB. Changes in the retinal GABA concentrations produce dose-dependant changes in the
ERG responses. The rabbit retina is affected by GABA levels; high concentrations of
extracellular GABA reduce the a-wave amplitude and low concentrations of extracellular GABA
enhances the amplitudes of a- and b-waves [214].
Table 7-2 – Electroretinogram changes associated with visual field loss.
Reference N (Visual Field Abnormality) Findings
Eke et al, 1997 [165] 3 adults Reduced OP amplitude (2/3)
Krauss et al, 1998 [177] 4 adults Reduced cone b-wave (4/4); Reduced OP amplitude (4/4)
Daneshvar et al, 1999 [178] 12 Reduced b-wave amplitude (4/10)
Reduced flicker amplitude (1/10)
Harding et al, 2000 [210] 18 adults
Reduced 30-Hz flicker amplitude Latency of photopic a-wave Latency of OP1
Ponjavic & Andreasson, 2001 [221] 7 adults Reduced 30 Hz flicker amplitudes (7/7)
Besch et al, 2002 [220] 18 adults Altered OP waveform
!
7.2 Multifocal ERG
While the full-field ERG provides a summed response of all the cells of the retina, the multifocal
ERG (mFERG) records local responses of the retina [222-224]. Multiple focal areas of the retina
are simultaneously stimulated providing a topographical measure of cone-driven retinal activity.

36
7.2.1 mFERG and Vigabatrin
The mFERG shows reductions in the amplitude of the peripheral retinal response in some of the
patients on VGB therapy [169]. In a study of adults with epilepsy on VGB, all 19 patients with
VGB-VFL showed abnormalities in the (wide-field) mFERG (100% sensitivity) while only 2 of
the 13 patients without VGB-VFL showed abnormalities (86% specificity) [225].
7.3 Electro-oculogram
The electro-oculogram (EOG) is a measure of the potential that exists between the cornea and
the retina (Bruch’s membrane). During a saccade, electrodes placed on the medial and lateral
canthi can detect a large potential difference (5 mV). During dark adaptation, the standard
potential changes according to the level of illumination. The Arden ratio is the ratio of the
maximum potential during the light exposure (light peak) and the minimum potential during dark
adaptation (dark trough). This index is reflective of the functionality of the retinal pigmented
epithelium as well as photoreceptors.
7.3.1 EOG and Vigabatrin
A reduction of the Arden Index has been associated with VGB treatment [169, 178, 182, 226]
and VGB-VFL [178, 227].
Lawden and colleagues found the Arden Index to increase with discontinuation of VGB therapy,
but not reaching the levels found in participants without VGB exposure [169]. The RPE is
affected by increased retinal GABA levels [228] and changes in the Arden ratio may be
indicative of drug effects rather than toxicity effects.
7.4 Visual Evoked Potentials
Visual evoked potentials, which reflect post-retinal neural function, were delayed in three of ten
patients with VGB-VFL [178]. Other studies found the evoked potentials to be slightly abnormal
or normal with VGB therapy [177-179, 181].

37
8 Optical Coherence Tomography (OCT)
8.1 Basic Principles
Optical Coherence Tomography (OCT) is a non-contact, non-invasive imaging technique based
on low-coherence interferometry that was developed in the early 1990s by Massachusetts
Institute of Technology [229]. Since its introduction, it has developed significantly to provide in-
vivo, high-resolution (1-15 µm), cross-sectional images of the retina in real-time and proves to
be an invaluable tool in medical diagnostics.
The principle behind OCT is similar to ultrasound imaging; however, OCT uses light instead of
sound to construct images [230]. Cross-sectional images are obtained by projecting a near-
infrared light on the retina and measuring the intensity and time delay of the backscattered light.
A broadband source emits light near-infrared light. The light is split into two separate paths: the
sample arm and the reference arm. The reference arm contains a reflecting mirror that can be
positioned to vary the time delay of the light. The light reflected by the tissue in the sample arm
will interfere coherently with the light in the reference arm when the optical path distances differ
by less than the coherence length of the light source.
Due to a variation in tissue properties, different tissues backscatter light differently. This
variation allows the differentiation of various layers of the retina. Light that travels for a greater
distance takes a greater amount of time to return to the detector. The data is processed and a
false-colour image representing the tissue structures is generated. This is the basis of time
domain OCT (Figure 8-1).
Spectral domain OCT (SD-OCT) uses a Fourier transformation to convert the signals to images.
In SD-OCT, the reference arm is fixed [230]. SD-OCT machines have increased axial resolution
and faster scanning speeds compared with time domain OCT machines.
!
!

38
Figure 8-1 – Schematic diagram of a Time-Domain Optical Coherence Tomography system.
Source: http://obel.ee.uwa.edu.au/; Copyright permission has been obtained, please see
Copyright Acknowledgements.
8.2 Clinical and Sub-clinical Applications of OCT
Ophthalmic applications of OCT are well developed since the transparency of the ocular media
allows minimal scattering of the projected light. Even though the first commercial OCT
machines were available in 1996, its use was limited by the slow scanning speed [230]. The
development of the SD-OCT greatly improved scanning speed and definition allowing its
widespread use in clinic.
Medical applications of OCT are most common. In ophthalmology clinic, OCT can be used for
in-situ qualitative and quantitative analysis of tissues and can be used to evaluate both the
anterior and posterior segments of the eye. OCT has been used for aiding diagnosis of diabetic
retinopathy, age-related macular degernation, and venous occlusions [231]. In neuro-
ophthalmology, OCT is particularly useful for examining the peripapillay retinal nerve fibre
layer (RNFL) and optic nerve head morphology. Spectral domain OCT has several advantages
over the older, time-domain OCT and other instruments such as the confocal scanning laser

39
ophthalmoscope and the scanning laser polarimetry in measuring RNFL thickness. RNFL
assessment may be more sensitive and more specific than disc imaging for detecting early
glaucoma [232] and OCT may be better than scanning laser polarimetry for quantifying RNFL
thickness in preperimetric glaucomatous damage [233].
Structural assessment done using OCT is highly repeatable in healthy controls, glaucoma
patients [234] and VGB-exposed adults with epilepsy [235].
8.3 OCT and Vigabatrin – Retinal Nerve Fibre Layer (RNFL)
Clinical fundoscopy examination of children on VGB has shown peripheral retinal atrophy and
secondary optic nerve atrophy (see Section 6.2).
RNFL attenuation can be quantified by OCT. Choi & Kim describe a case of an 18-year old male
on VGB for refractory epilepsy with bilateral visual field constrictions and discernable RNFL
loss as measured by OCT [236].
Other studies found similar associations between RNFL attenuation and VGB-VFL in adults
[236-239]. This thinning is most prominent in the nasal quadrant, with the temporal regions
spared. The temporal regions are preserved even in patients with large cumulative exposure to
VGB and moderate or severe visual field reductions [240].
Some VGB-exposed individuals without field loss also show RNFL attenuation suggesting that
OCT may be more sensitive than visual fields in detecting retinal defects [239]. Clayton and
colleagues found a strong linear correlation between visual field size, as measured in mean
radial degrees, and RNFL thickness in adults on VGB treatment using both spectral-domain OCT
(r = 0.768, p < 0.001) and time-domain OCT (r = 0.814, p < 0.001) [235]. Clayton and
colleagues also found the temporal quadrant to be the least affected which is in agreement with
other studies [237, 238], but found RNFL thinning to be most prominent in the superior and
inferior quadrants which contrasts with other studies.
!

40
9 Mechanism of Vigabatrin Toxicity
Based on the studies described above, VGB clearly causes several changes at the level of the
retina. ERG studies show damage to the retina with VGB treatment. Specifically, the cone
photoreceptor pathways seem to be affected as shown by consistent changes in the photopic b-
wave and flicker response [177-179, 210, 213, 241]. The reversible changes seen on the EOG
indicate an effect to the photoreceptor-retinal pigment epithelium interface [169, 178, 182, 226].
And several studies note atrophy of the retinal nerve fibre layer [198, 239].
Changes in the ERG associated with VGB therapy indicate retinal dysfunction as the
pathophysiology causing visual field reductions. However, the mechanism of VGB toxicity in
the retina is not well understood. VGB and/or the elevated levels of GABA may cause the retinal
damage.
9.1 GABA Receptors and Excitotoxicity
The ERG response of the eye is dependent on inner retinal GABAergic cells. As previously
discussed in Section 4, GABA acts as a neurotransmitter in a functional retina. In the OPL,
GABAergic transmission is present between horizontal cells and photoreceptors, horizontal cells
and other horizontal cells, and horizontal cells and bipolar cells [242]. In the IPL, GABAergic
transmission is present between amacrine cells and bipolar cells, amacrine cells and other
amacrine cells, and amacrine cells and ganglion cells. The presence of GABA agonists alters the
normal cellular response in the cat retina. The photopic response is reduced and delayed in the
cat retina following administration of GABAA agonists delta-amino valeric acid, muscimol, and
THIP [243]. Administration of picrotoxin, a chloride channel blocker, causes reductions in the b-
wave of the ERG through its action on GABAC receptors [244].
In the retina, an additional class of GABA receptors, GABAC receptors, is present. GABAC
receptors (see Section 4.1) are more sensitive and have slower activation/inactivation kinetics
than GABAA receptors. Furthermore, as discussed in Sections 4.3 and 4.4, GABA can be
excitatory in the physiological adult retina, and in pathological states [82, 98].
In a recent review article, Heim and Gidal postulate that retinal damage may be the result of
GABA-induced excitotoxicity [245]. VGB, which works by inhibiting GABA-T in the brain,

41
may have a greater effect in the retina [246] since concentrations of VGB in the retina are up to
18.5 times higher than in the rodent brain following VGB administration [149]. This is likely due
to the increased permeability of VGB in the blood-retina barrier compared to the blood-brain
barrier. This level of accumulation in the retina is not seen following topiramate or gabapentin
administration [149].
The increase in retinal GABA levels has a marked effect on retinal GABA-T activity and retinal
GABA levels. In the retina of rats with intraperitoneal injection of VGB, GABA-T activity is
undetectable and GABA concentrations increase five-fold compared to controls [206]. GABA
increases to 260% of control levels in the retina of Sprague Dawley rats following a single dose
administration of VGB [110]. With excess GABA in the retina, the receptors may be over-
activated and become excitatory [247]. This leads to an osmotic imbalance and subsequently cell
lysis and cell death. Alternatively, the very high levels of VGB itself in the retina may have a
direct toxic effect, unrelated to GABA or GABA-T.
9.1.1 Limitations
Based on this theory of GABA excitatoxicity, all GABAergic drugs should produce similar
effects. To determine if the field defects seen in VGB is a class effect or if it is specific to the
drug, it is important to examine other antiepileptic drugs that work by building up GABA
concentrations. Tiagabine is an antiepileptic drug that works by prolonging GABA reuptake at
synapses. There has been a single report of minor reductions in visual fields in an adult treated
with tiagabine for bipolar disorder [248]. The field loss was reversible upon drug
discontinuation. This seems to be an incidental finding and other studies do not show field losses
with tiagabine treatment [109]. Rodent studies show that with tiagabine administration, GABA
does not accumulate in the retina [110]. The GABA transporters (GAT-1, GAT-2, GAT-3 and
BGT-1) are differentially distributed throughout the CNS. Tiagabine mediates its affect by
inhibiting GAT-1 and it predominately affects the hippocampus and cerebral cortex [249]. VGB
leads to GABA increases throughout the brain while tiagabine causes GABA increases in certain
synapses in certain areas of the brain [149]. This suggests that the visual field loss is not a class
effect and that it is specific to VGB or to the increased levels of VGB in the retina.

42
9.2 Role of Taurine
9.2.1 Physiological Role of Taurine
Taurine (2-aminoethane- sulfonic acid) is an amino acid that can be obtained from diet (human
breast milk, meat and seafood) and can also be synthesized minimally de novo. Taurine is found
in the brain, retina, muscle tissue and other organs with particularly high concentrations in the
retina. All ocular tissues contain taurine and taurine is the most abundant amino acid in the
retina, vitreous, lens, iris-ciliary body and cornea [250].
In the mammalian body, taurine is necessary for production of bile salts, osmoregulation and
inhibition of oxidative stress. In the retina, it also plays a prominent role in retinal development
[251] and protects against free radical damage and RPE cell death [252, 253]. Taurine depletion
leads to retinal degeneration (loss of retinal photoreceptors) [254] and visual dysfunction [255].
Deprivation of taurine causes disorganization of the photoreceptor layer with the photoreceptor
nuclei moving toward the RPE [255].
Depletion of taurine, by inhibiting the taurine transporter or by exposure to environmental
lighting, causes reductions in ERG amplitudes [256, 257]. Children with low-taurine diets also
show reduction in ERG responses [258]. With taurine supplementation, there is recovery of the
ERG responses.
9.2.2 Taurine and Vigabatrin
Decreased plasma taurine concentrations are associated with VGB treatment and taurine
deficiency may be a risk factor for developing VGB-VFL. Five of six infants treated with VGB
for at least six months had taurine levels below age-similar controls [259]. For one of these six
patients, pre-drug taurine levels were measured and were within normal limits. This suggests that
VGB treatment causes taurine deficiency. This deficiency may result from the increase in GABA
concentrations caused by VGB; GABA competitively inhibits the taurine transporter inhibiting
taurine uptake in the RPE [260].
To determine if taurine deficiency plays a role in the development of VGB-VFL, Jammoul and
colleagues co-treated adult rats with VGB and taurine [259]. Rats treated with VGB and taurine

43
showed higher ERG amplitudes and higher cone densities compared to rats treated with VGB
alone. Taurine supplementation of VGB-treated rats does not stain as extensively for glial
fibrillary acid protein (GFAP), a marker of retinal lesions. Furthermore, disorganization of the
photoreceptor layer caused by VGB treatment was reduced with supplementation [261]. More
recently, it was shown that taurine increases survival of retinal ganglion cells in various animal
models of ganglion cell degeneration (glaucoma, retinitis pigmentosa) [262]. These studies
suggest the taurine deficiency may cause retinal damage and that taurine supplementation may
prevent VGB-VFL.
!

44
10 Assessment of VGB-VFL in Young Children
In adults, visual fields can be easily mapped using instrumentation such as the Humphrey Visual
Field Analyzer or the Goldmann perimeter. However, assessing visual fields through
conventional perimetric testing methods proves to be challenging and inaccurate in young (< 4
years) or developmentally delayed children and thus there has been much interest in developing
surrogate measures of retinal toxicity. Several ERG responses have been found to correlate with
VGB-associated visual field defects (see Section 7.1.1). The light-adapted 30-Hz flicker
amplitude, which is a measure of the cone pathway activity, is the best predictor of VGB-VFL
with a sensitivity of 100% and a specificity of 75% [210]. This measure does not show
improvement after discontinuation of VGB treatment [213] indicating that it is a result of retinal
toxicity and not due to the treatment itself. The 30-Hz flicker is currently used as the standard
biomarker of VGB-VFL at the Hospital for Sick Children (SickKids), Toronto.
10.1 Toxicity – Original Definition
Retinal toxicity is defined as a repeatable decrease in age-expected 30-Hz flicker amplitude from
the individual’s pre-drug ERG. Ideally, the child will undergo an ERG before the initiation of
VGB treatment and will have follow-up ERGs every three to six months.
To analyze the ERG responses, the raw amplitude values are first log-transformed. Then, using
previously published data from our group, the ERG values are normalized according to age
[263]. This is done by subtracting the log of the age-expected ERG amplitude (log µV) from the
log of the study subject data. The resulting values from the right and left eye are averaged and
this measure is the outcome used to identify toxicity.
Age-corrected pre-drug ERG values of the child are compared with age-corrected values on each
subsequent visit. If the child exhibits a significant reduction (> 0.2 log microvolts) from pre-drug
amplitude on two consecutive visits, the child is deemed to have retinal toxicity. The value of 0.2
log units was obtained by examining ERG responses of individuals (n=6) who had multiple pre-
drug recordings. The maximum inter-visit variation in these individuals was 0.2 log units
(Figure 10-1). The recurrent ERG reduction of two consecutive visits reduces the possibility of a
false positive. This is important because ERG amplitudes can be artificially reduced due to poor

45
positioning under the Ganzfeld, electrode placement, Bell’s phenomenon where the eye drifts up,
and intermittent restlessness under sedation.
Figure 10-1 –Test re-test 30-Hz flicker ERG amplitude from 6 children with IS and no VGB
treatment. All data are corrected for age at test. Data are plotted as ∆ERG, which is the
difference (test 2 – test 1) (log µV) in log age adjusted light adapted 30-Hz flicker ERG
amplitude. The test-retest difference data are plotted against age at first ERG. Based on these
data, it is unlikely that ERG amplitudes will reduce by more than 0.2 log units on subsequent
visits. Therefore, a reduction of the flicker amplitude by more than 0.2 log units is considered
significant.
10.2 Problems with original definition
10.2.1 Abnormal Development
Prior to VGB therapy, children with IS have been found to have reductions in contrast sensitivity
as measured by visual evoked potentials [264]. This suggests that abnormalities in contrast
sensitivity are a result of retinal or cortical dysfunction associated with IS. Before initiation of
VGB treatment, some patients with IS have abnormal flicker responses compared to normally
developing children [241], complicating the assessment of retinal function during treatment. The
variability in the ERG responses is due to the underlying retinal dysfunction. Work done by our

46
lab suggests that certain etiological factors are associated with a greater likelihood of having
abnormal baseline measures (McFarlane, in progress). Reduction in visual functions may result
from reduced GABA transmission during critical developmental periods [264, 265].
The retinal electrophysiology of children with IS does not follow the same developmental trend
as that of typically developing children (Figure 10-2). The group without spasms shows an
increase in amplitude with age, while individuals with spasms do not show the same level of
increase. Children without spasms have a flicker response that increases in amplitude from 60
µV to 68 µV from three months of age to six months of age. In children without spasms, the
increase in amplitude is a mere 2 µV: from 76 µV at three months of age to 78 µV at six months
of age. Interestingly, the group with IS seems to have higher flicker amplitudes early in
development.
The development of the flicker ERG amplitudes of children with spasms may be affected by the
IS, other co-morbidities, and/or by their medications. Due to this difference in development, age-
correction may not be appropriate.

47
A
B
Figure 10-2 – Plot of pre-vigabatrin flicker ERG amplitudes as a function of age (months) of
testing in children with spams(A) and children without spasms (B).

48
10.2.2 Lack of true baseline
In an ideal situation, a patient will have a baseline prior to VGB initiation. However, this is not
always possible. For our purposes and as defined by FDA guidelines, we take flicker amplitudes
recorded within four weeks of initiating VGB treatment as true baseline. However, some
individuals are seen in Visual Electrophysiology clinic long after initiating treatment (Figure 10-
3). If such a circumstance arises, the individual’s first ERG is taken as the baseline for ERG
assessment. The problem with this approach is that it may fail to capture the pre-drug function of
the retina. If the flicker ERG amplitudes are abnormal before the true baseline ERG examination
which precedes VGB treatment, the tests may fail to identify toxicity since toxicity is dependent
on having a true baseline.
Figure 10-3 – Plot of flicker amplitude (log µV) of the right (blue line) and left (red) eye as a
function of duration of VGB treatment for patient 1225. The participant does not have a true
baseline (ERG recorded within 4 weeks of VGB initiation. The participant had her first ERG at
88 months, which was used as baseline. Green circles indicate flicker amplitudes that are
significantly reduced (>0.2 log units) from baseline.

49
10.2.3 Poor recording: Disagreement between eyes
VGB-VFL is characterized by bilateral constriction of the peripheral fields. Therefore, we expect
both eyes to show similar ERG amplitudes. However, in some recordings, there are large
differences between the eyes (Figure 10-4). This is most likely an artifact (Bell’s phenomenon)
caused by one eye rolling up to a greater extent than the other eye. In this situation, it may be
more accurate to discard the lower value.
Figure 10-4 – Plot of flicker amplitude (log µV) of the right (blue line) and left (red) eye as a
function of duration of VGB treatment for participant 1217. Green circles indicate flicker
amplitudes that are significantly reduced (>0.2 log units) from baseline. The ERG taken at 58
months shows a large difference (0.3 log units) between the right and left eye.
10.2.4 Monocular Recordings
In an ideal situation, both eyes are recorded simultaneously. However, not all individuals are
cooperative with Burian-Allen electrodes (sedated ERGs) or DTL electrodes in both eyes. If a
sedated child wakes up during electrode placement or testing, s/he may not cooperate with
binocular testing. In older subjects with unsedated ERGs, after placing electrode on one eye, they
may feel uncomfortable with having it on the second eye. In such situations, ERGs are recorded
monocularly (Figure 10-5).

50
Figure 10-5 – Plot of flicker amplitude (log µV) of the right (blue line) and left (red) eye as a
function of duration of VGB treatment for participant 1222. Green circles indicate flicker
amplitudes that are significantly reduced (>0.2 log units) from baseline. The ERG is done
monocularly on all visits. The first two recordings are from the left eye and the last three
recordings are from the right eye.
10.2.5 Artificially-Reduced Baseline
The classification of toxicity is dependent on a reliable baseline. The baseline needs to capture
the true function of the retina so that subsequent ERGs can be used to measure any decline in
retinal function. Section 10.2.2 discusses the implications of having the first ERG performed
months after VGB initiation. In certain situations, the baseline is recorded within four weeks of
VGB initiation but the baseline may be artificially low. This is likely due to poor electrode
placement and may result in an under diagnosis of toxicity.
In situations where the ERG amplitude increases by greater than 0.15 log units from the baseline,
the baseline can be considered to be artificially low (Figure 10-6). The greatest increase we
expect from inter-visit variation is 0.15 log units (Figure 10-1).

51
Figure 10-6 – Plot of flicker amplitude (log µV) of left eye as a function of duration of VGB
treatment for participant 1300. The participant’s flicker amplitude increases by more than what is
expected from inter-visit variation (0.15 log units). This suggests that the baseline is not a good
measure of the retinal function of the individual.
10.2.6 Lost to Follow-up
To reduce the likelihood of the flicker amplitude being artificially reduced, classifying an
individual as having toxicity requires two consecutive ERGs showing reduced amplitudes.
However, some individuals show a reduction in the flicker amplitude but are not seen again in
the clinic (Figure 10-7). This may cause an under diagnosis of toxicity since some of these
individuals may have shown a reduction in the flicker amplitude, had a follow-up ERG been
performed.

52
Figure 10-7 – Plot of flicker amplitude (log µV) of the right (blue line) and left (red) eye as a
function of duration of VGB treatment for participant 1219. Green circles indicate flicker
amplitudes that are significantly reduced (>0.2 log units) from baseline. The last ERG recorded
shows a significant reduction from baseline. This individual is categorized as not having toxicity
since the classification of toxicity requires two consecutive reductions from baseline.
10.2.7 Recovery
Toxicity is defined as a sustained reduction in the flicker response. In some patients, there is a
recovery in the amplitude of the ERG response following two degraded responses (Figure 10-8).
If toxicity is understood as an irreversible effect, the ERG should not show a recovery. Does a
recovery suggest that toxicity did not occur and that the previous degraded responses were an
artifact (false positive due to Bell’s phenomenon, poor electrode placement, etc)? Or does it
indicate that the toxic changes at the level of the retina, as measured by the ERG, are reversible?
What role does drug discontinuation play in ERG recordings?

53
Figure 10-8 – Plot of flicker amplitude (log µV) of the right (blue line) and left (red) eye as a
function of duration of VGB treatment for participant 1217. Green circles indicate flicker
amplitudes that are significantly reduced (>0.2 log units) from baseline. The ERGs recorded at
97 and 113 months of VGB treatment show a significant reduction from baseline and thus the
individual is categorized as having toxicity. However, the ERG recorded 127 months after
initiating VGB therapy shows recovery of the flicker amplitude.
10.3 Toxicity: Refined Definition
These problems have caused us to redefine our original definition of toxicity. VGB toxicity is
now defined as a significant reduction of the 30-Hz flicker amplitude from baseline on two
consecutive visits. If the child is over 6 months of age at time of baseline test, then a significant
reduction is taken as a reduction of 0.2 log units. If the child is less than 6 months of age,
significant reduction is a reduction from baseline by 0.15 log units (rather than 0.2 log units).
This accounts for development that occurs in the first six months of life.
Recordings from one eye only were analyzed per visit. When binocular recordings were
available, the amplitude of the flicker response was compared between right and left eyes, and
the recording with the greater amplitude was selected for analysis.
!

54
11 Purpose and Rationale
The primary purpose of this study was to assess whether current electrophysiological markers for
retinal toxicity due to VGB correlate with visual function loss. The study also aimed to validate
the use of high-resolution OCT for detecting structural changes due to VGB. The population
tested was individuals over 7 years of age who were previously on VGB and monitored by the
Visual Electrophysiology Unit (SickKids) for toxicity.
In 2009, the U.S Food and Drug Administration (FDA) approved VGB for the treatment of IS. It
is a particularly efficacious monotherapy for IS associated with TSC [133]. VGB works by
irreversibly inhibiting the GABA-T, the enzyme responsible for the breakdown of GABA,
leading to the build-up of GABA in the brain and retina [266].
In 1997, it was recognized that VGB is associated with visual field defects, specifically bilateral
constriction, in adults [165-168]. The prevalence of VGB-VFL is estimated to be 30-50% in
adults [187]. In infants and children unable to undergo perimetric testing, the current standard
biomarker of VGB-VFL is the light-adapted 30 Hz flicker response amplitude, which is a
measure of cone pathway function. This measure has been shown to be the best predictor of
VGB-VFL with a sensitivity of 100% and a specificity of 75% [210]. The Hospital for Sick
Children has been monitoring young children unable to do perimetry for VGB toxicity since
1999. Now that these individuals are older, some of them are able to do perimetric testing. One
of the aims of this study was to determine if the standard ERG tests for VGB toxicity done in
childhood are correlated with reductions in the visual field (Goldmann kinetic perimetry) later in
life.
This study also aimed to validate the use of high-resolution OCT (SD-OCT, Cirrus; Carl Zeiss
Meditec) for detecting the structural changes (RNFL attenuation) associated with VGB toxicity.
Previously, studies in adults have associated RNFL attenuation with VGB-VFL (see section 8.3).
The current study aimed to validate structural markers for retinal toxicity identified in the adult
population for use in the pediatric population. OCT may be an ideal tool for monitoring toxicity
since it is fast and non-invasive.
!

55
12 Hypothesis
We hypothesized that there will be functional and structural changes in individuals with VGB
toxicity as identified by the ERG.
Diagnosis of vigabatrin toxicity, as defined by the 30-Hz flicker amplitude, in childhood will be
associated with visual field reductions as determined by Goldmann perimetry later in life.
Vigabatrin toxicity will be associated with attenuation of the retinal nerve fibre layer as
determined by optical coherence tomography.
!

56
13 Methods
13.1 Research Ethics Board Approval
The SickKids Research Ethics Board approved the current study (see Appendix A for letter of
approval).
13.2 Recruitment
Individuals who were monitored in the Visual Electrophysiology Unit (VEU), SickKids for VGB
toxicity were recruited in collaboration with Dr. Raymond Buncic, a staff neuro-ophthalmologist.
The parents/guardians were familiar with Dr. Buncic since he has seen these children previously
in the eye clinic. Individuals who developed VGB toxicity (as defined above) as well as
individuals who did not show toxicity were identified by review of hospital charts. Letters signed
by Dr. Buncic, detailing the nature of the study, its relevance, and the tests involved were mailed
out (Appendix B). The letters invited parents/guardians to fill in and mail the reply card or to
phone the VEU if they were interested in participating in the study. Individuals that had not
responded within 2 weeks were contacted via phone regarding the study. Parents/guardians
interested in enrolling their children in the study were contacted by telephone to be booked for an
appointment in Dr. Buncic’s or Dr. Arun Reginald’s neuro-opthalmology clinic.
13.3 Inclusion Criteria
13.3.1 Participants with Vigabatrin Toxicity
a) Previously on VGB
b) Monitored by the VEU for development of toxicity and shows toxicity (requires a
baseline and at least TWO follow-up ERGs)
c) Seven years of age or older
13.3.2 Control Participants – Participants without Toxicity
a) Previously on VGB

57
b) Monitored by the VEU for toxicity and does not show toxicity (requires a baseline and at
least TWO follow-up ERGs)
c) Seven years of age or older
13.4 Exclusion Criteria
None.
Due to the limitations in sample size, there were no exclusion criteria. Some patients presented
with various co-morbidities, some of which may have an impact on the results. There was
consideration of each participant’s medical history when analyzing and interpreting results.
When necessary, the results of particular tests were removed from the analysis. For example, the
presence of occipital cortex lesions rendered the visual results unreliable. Therefore, such results
were excluded from analysis.
13.5 Patient Information
The SickKids Electronic Patient Chart (EPC) was used to obtain contact information, dates of
diagnosis, medical history, medications and dosages that the patient may be taking. REB
approval was obtained for accessing this information.
13.6 Consent
This research was conducted in compliance with the tenets of the Declaration of Helsinki. The
parents/guardians of each participant provided informed consent on behalf of their child
following a verbal explanation of the study. An appropriate amount of time was allotted to read
the form and have any questions or concerns addressed before obtaining signatures. Whenever
possible, the protocols of the study were explained to the child and the child provided verbal
assent to participate in the study. The consent and assent forms (see Appendix C) for all study
participants contained the following information:
• Names, positions and contact information of all investigators involved in the
study

58
• Purpose of the research
• A clear description of each test
• Information about potential harms and potential benefits
• Participant’s right to confidentiality
• Participant’s right to refuse or withdraw from the study at any time
13.7 Study Protocol
Consenting patients underwent clinical evaluation consisting of visual acuity, contrast sensitivity
and colour vision in the VEU intake room by the graduate student or an orthoptist. This was
followed by a visual field examination (Goldmann kinetic perimetry) by an ophthalmic assistant.
A neuro-ophthalmologist (Dr. Raymond Buncic or Dr. Arun Reginald) examined the patients to
determine the overall health of the eye and to look for clinical signs of VGB toxicity. An
ophthalmic photographer imaged the retina using fundus photography and spectral domain
optical coherence tomography (SD-OCT, Cirrus; Carl Zeiss Meditec). These tests took
approximately two to three hours. Not all children were able to complete all the tests due to
developmental and cognitive delays.
As an optional component of the study, consented children underwent a shortened ERG protocol
(light-adapted only) on a separate day. Only participants who were able to successfully complete
OCT assessment underwent the ERG procedure.
All participants were tested in the Ophthalmology and Vision Sciences Department, SickKids.
All clinical and electrophysiological testing was monocular and both eyes were tested when
possible. A case report was used to document participant information (see Appendix D).
13.7.1 Clinical Assessment
Information about drug dosage, concurrent drug usage, co-morbidities, age at diagnoses, etiology
of seizures etc. was collected from electronic patient charts. Parents/guardians were also
questioned about the general health, current medications and allergies of the child. Parents were
also questioned about any ocular symptoms that they may have noticed in the child (ex. Does

59
your child bump into things often?). Any required refractive correction was worn during clinical
assessment.
Visual Acuity
Visual acuity refers to the ability to resolve fine detail and is the most commonly used measure
of functional vision [267]. Visual acuity is specified by the visual angle subtended by the
smallest detail identified by the observer. The visual angle is determined by the absolute size of
the object and its distance from the observer. The smallest angle that allows an object (i.e. letter)
to be resolved from a uniform background is termed the minimal angle of resolution (MAR) and
can be measured in a logarithmic scale (logMAR).
To test visual acuity, Early Treatment Diabetic Retinopathy Study (ETDRS) Visual Acuity Chart
(Precision Vision; Villa Park, IL) was used since it is less subjective than Snellen or Sloan tests
[268, 269]. The chart is advantageous since it consists of multiple rows with five equally legible
letters in each row and because the spacing between each letter is proportional to the letter size.
The acuity changes from one row to the next in a logarithmic faction (0.1 log unit per row).
Participants were asked to read the letters monocularly at a distance of 4 meters. The right eye
was tested first (with the left eye being occluded) unless the right eye was a weak eye. The
measurements were taken with full correction for refraction whenever possible (Best Corrected
Visual Acuity – BCVA).
In children with mild developmental delay HOTV methods were used. The child needed to
match the letter (H, O, T or V) on the wall chart with those on the response card by pointing to
the corresponding letter.
Preferential looking methods using Cardiff cards were used to estimate visual acuity for children
with higher levels of developmental delay, who are unable to communicate the letter/picture that
they see [270]. To standardize the methods, preferential looking assessments were done on all
research subjects. For each visual acuity level, there are two Cardiff cards: one consisting of a
picture located on the top half and the other card contains the identical picture on the bottom
half. The examiner does not know in advance the position of the object and must track the child’s
eye movements. If the child looks toward the object, the examiner assumes that the child can see

60
the target and if the child does not look toward the object, the examiner assumes that the child
cannot see the object. For this test, participants were seated 55 cm away from the examiner.
Contrast Sensitivity
While visual acuity measures an individual’s ability to resolve high spatial frequencies, it does
not give any information about the individual’s ability to detect low spatial frequencies. Contrast
sensitivity gives information about an individual’s ability to detect a wide range of frequencies.
Contrast sensitivity was measured using the M&S smart system II (MSSSII; M&S Technologies
Inc, Illinois). This system provides easy assessment and produces results that are comparable to
the results produced by the Pelli-Robson chart [271]. The contrast levels change in a logarithmic
fashion. Participants were seated 4m away from the screen and were asked to read the letters as
the examiner systematically decreased the contrast levels using a keypad.
Colour Vision
The current study used the Mollon-Reffin Minimalist Test (MRM) to assess colour deficiencies
[272]. The individual is required to pick a coloured chip among a set of five gray chips under
standardized lighting (C.I.E. source C). The test consists of three series that lie along the
dichromatic confusion line (green– protan; red – deutan; blue-yellow – triton). Each series
contains six chips of varying saturation, allowing the deficiency to be scaled. The MRM test is
effective at testing acquired colour vision defects in children as young as three years of age and
yields better results than the American Optical Hardy Rand Rittler (HRR) test [273].
13.7.2 Visual Fields
A visual field test is clinically used to assess an individual’s entire scope of vision. It tests the
central and peripheral vision. A visually normal adult can see 60o nasally, 110o temporally, 75o
inferiorly and 60o superiorly.
Goldmann Perimetry
The Goldmann test was used to assess the extent of participants’ visual fields. Each eye was
tested individually with the alternate eye patched. The Goldmann is a kinetic test where the
stimulus moves from the periphery (non-seeing area) and towards the centre along a set meridian

61
[274, 275]. The participant must maintain fixation in the centre and press the buzzer as soon as
s/he sees the stimulus. The same stimulus is used along various meridians and by joining these
points together an isopter can be drawn. This procedure is repeated with stimuli of differing
sizes and intensities. The stimulus size can vary between 0 to V, with V being the largest size.
The stimulus intensity can vary between 1 and 4 (4 is the brightest) with each 5 decibels (dB)
change and between a-e for each additional 1 dB change (e is the brightest). For example, the I
2e and the I 4e stimulus have same size but the I 4e stimulus is brighter by 10 dB. The IV 4e and
I 4e stimuli have the same intensity but the IV 4e stimulus is larger. For the current study, the
following stimuli were used: I 2e, I 4e and IV 4e.
The accuracy of the test depends on the individual’s ability to follow the examiner’s commands,
maintain fixation and respond appropriately. The examiner provided a subjective measure of the
participant’s fixation and reliability (poor, fair and good).
Confrontational Method
Confrontational method is a rudimentary and simple way of measuring the visual field. This is a
qualitative assessment that is done by presenting an appropriate stimulus in each quadrant of the
field while the examiner ensures central fixation. Participants with developmental delay who
were not able to perform the Goldmann perimetry underwent modified confrontational screening
when possible.
13.7.3 Mydriasis and Cycloplegia
Mydriatics are agents that dilate the pupil and increase retinal illumination, allowing the entire
posterior segment to be visualized. Cycloplegics are agents that paralyze the ciliary muscles and
reduce accommodation. Mydriasis and cycloplegia are required in the examination of the eye and
are necessary for refraction, fundus photography and electroretinography. Although pupillary
dilation is not necessary for OCT, it increases quality and reproducibility of images. In a study of
38 patients with glaucoma, 29 patients provided good images without dilation [276]. The
remaining nine patients whose pupils were not dilated were unable to provide good images but
were able to provide good images following dilation. Poor image quality without dilation is
associated with small pupil size and cataracts. Even though most participants taking VGB do not

62
have cataracts, dilation improves access to the retina in patients with limited attention and
increased mobility.
First, the cornea was anesthetized using a drop of 0.5% proparacaine hydrochloride (Alcaine®;
Alcon Laboratories Inc, Texas, USA), a topical corneal anesthetic. The mydriatic agent that was
employed was 2.5% phenylephrine (Mydfrin®; Alcon Laboratories Inc, Texas, USA). A drop of
1% tropicamide (Mydriacyl®; Alcon Laboratories Inc, Texas, USA), a cycloplegic agent, was
also administered.
13.7.4 Examination by the Ophthalmologist
Ophthalmologic examination included slit lamp inspection and dilated fundus examination. The
optic nerve, macula, and the retinal periphery were examined in detail. All findings were
recorded in the case notes. The ophthalmologist checked for typical signs of toxicity (inverse
atrophy).
13.7.5 Imaging: Fundus Photography
All participants had fundus photographs taken with a Zeiss Digital FF 450 Fundus Camera or a
Zeiss Visucam 200 Fundus Camera (Carl Zeiss Canada Ltd; Toronto, Canada). Protocol for this
involved taking the modified 7-standard stereoscopic fields for color photography as described
by Airlie House (see Figure 13-1) with Fields 1 and 3 modified to include the macula. However,
due to cognitive and developmental delays, this protocol was not feasible in all study
participants.

63
Figure 13-1 – Modified 7-Standard Field Protocol for Colour Fundus Photography. Source:
Fundus Photography Reading Centre, University of Wisconsin School of Medicine and Public
Health; Copyright permission has been obtained, please see Copyright Acknowledgements.
13.7.6 Imaging: Optical Coherence Tomography
A spectral domain OCT (Cirrus; Carl Zeiss Meditec Inc, Dublic, CA) with a theoretical axial
resolution in retinal tissue of 5µm and a scan velocity of 27,000 axial scans/second was used to
obtain cross-sectional images of the retina. The Optic Disc Cube 200x200 scan and the Macular
Cube 512x128 scan were performed on study participants, when possible. Raster scans provided
additional qualitative information. Reflectivity profiles and automated segmentation algorithms
were used to measure the thickness of the retinal layers.
The optic disc cube scan consists of 200 B-scans, with each B-scan composed of 200 A-scans,
and covers an area of 6 mm x 6 mm around the disc, acquiring data from the optic disc and the
peripapillary region. Using the Cirrus machine’s built in algorithms, the center of the optic disc
is identified and retinal nerve fibre layer (RNFL) thickness along a 3.4 mm diameter circle
centered on the optic disc is calculated. This is used to calculate the global average RNFL
thickness. The machine also provides RNFL thickness of each quadrant (superior, inferior, nasal,
and temporal), and of all 12 clock hour sectors.
Fundus Photograph Reading Center University of Wisconsin School of Medicine and Public Health Department of Ophthalmology and Visual Sciences
ACCORD Forms, Labeling, Study Conventions, and Imaging Procedures Page 11 of 36 Effective Date: Supersedes Date: New
(Photos courtesy Richard Hackel)
Visit our website http://eyephoto.ophth.wisc.edu/Photographers.html, and click on the Modified 7-Standard Field Photography Tutorial to view a color fundus photography tutorial on acquiring the 7 modified fields in a quick and easy manner.
The following descriptions of the standard fields assume that there are two cross hairs in the camera ocular, one vertical and the other horizontal intersecting (note: although not in Zeiss FF450, Canon, and Kowa) in the center of the ocular.
Field 1M - Disc: Center the temporal edge of the optic disc in the center of the cross hairs in the ocular. Field 2 - Macula: Center the macula near the intersection of the cross hairs in the ocular (note: although not in Zeiss FF450, Canon, and Kowa). If your fundus camera has a central “gray” artifact near the intersection of the cross hairs this should be placed about 1/8 – 1/4 DD above the center of the macula to keep from obscuring the center of the macula. A suitable position can often be obtained by rotating the camera temporally from the Field 1M position, without vertical adjustment.
Field 3M - Temporal to Macula: Position the intersection of the cross hairs in the ocular 1.0-1.5DD temporal to the center of the macula (note: although not in Zeiss FF450, Canon, and Kowa). If Field 2 was centered above the center of the macula, as suggested above, Field 3M may be centered 1.0-1.5 DD temporal to Field 2, a position easily achieved by rotating the camera without making any vertical adjustment or movement of the fixation device.
Field 4 - Superior Temporal: The lower edge of the field is tangent to a horizontal line passing through the upper edge of the optic disc and the nasal edge of the field is tangent to a vertical line passing through the center of the disc.
It is convenient to take Field 6 immediately after Field 4 by pivoting the camera nasally.
1M 2 3M
Right Eye
1M 2 3M
Left Eye
4 6
7 5
4
5
6
7

64
The macular volume scans consist of 128 horizontal B-scans of 512 A-scans each and cover a 6
mm x 6 mm area. Based on the macular scan, a ganglion cell analysis report providing
information about the ganglion cell layer (GCL) and the inner plexiform layer (IPL) was
generated. The elliptical annulus centered about the fovea is divided into six sectors.
Signal Strength
In newer OCT machines, signal strength is used as an alternative to signal-to-noise ratio (SNR)
to discriminate quality of images. The signal strength measurement is an advanced parameter
that incorporates SNR with the uniformity of the signal within a scan. Signal strength is
measured on a scale of 1 to 10, with 1 indicating low image quality and 10 indicating excellent
image quality. For meaningful analysis, all poor-quality scans, defined as those with signal
strength <6, were excluded. Signal strength is influenced by media opacity, pupil size and
refractive error.
13.7.7 Photopic Electroretinogram
All ERGs were performed by the Visual Electrophysiology Unit according to the standards set
by The International Society for Clinical Electrophysiology of Vision (ISCEV) [208].
System and Recording Parameters
ERG measurements was recorded using the Espion Color Dome (Diagnosys LLC, Lowell, MA).
A camera attached to the Color Dome allowed the participant’s fixation during recordings to be
monitored during testing.
Electrodes
Dawson – Trick – Litzkow (DTL) microfiber disposable electrodes (LKC Technologies) [277]
were used in the current study. DTL electrodes are preferred over Burian-Allen lenses for their
ease of use and comfort. DTL electrodes are mono-polar electrodes. The low-mass nylon fibres
are impregnated with metallic silver and span the eye, resting along the lower edge of the cornea.
Adhesive sponge pads secure the electrodes to the temporal and nasal canthi. Surface Ag/AgCl
electrodes attached to the forehead and earlobes with electrode paste served as ground and

65
reference electrodes, respectively. Measurements from the right and left eye were taken
simultaneously.
Stimuli
The ERG responses that were evaluated included the single flash photopic response (2.29
cd.s.m−2), the 30 Hz flicker response (2.29 cd.s.m−2) and the long flash response. Artifacts from
disruptions such as blinking were removed from the data before averaging the results.
Amplitudes were log transformed. For implicit times, the age expected value was subtracted
from the observed value with positive values representing delayed responses relative to the
expected values.
13.8 Statistical Analysis
All statistical analyses were performed using R version 2.15 and SAS version 9.3.
13.8.1 Linear Mixed Models
Mixed models offer several advantages over traditional analyses. In traditional analysis, it is
assumed that observations from a population are independent and identically distributed. But,
this assumption is not always correct. Mixed models allow clustered data and longitudinal data to
be properly analyzed. Repeated-measures studies, where observations on subjects are repeated
across time or under different conditions, can be analyzed with mixed models.
In the current study, multiple measurements were observed in each participant; the visual field
and OCT data had multiple repeated levels. The visual field was analyzed along four meridians.
The RNFL around the optic disc was measured along four quadrants and twelve clock-hour
sectors. Therefore mixed models were used to account for the correlation within subjects while
allowing for fixed and random effects of the covariates. Please see Appendix E for the code.
!

66
14 Results
14.1 Participant Demographics
14.1.1 Neurological History
Detailed demographics of all study participants are presented in Appendix F. Twenty-two
participants who had been treated with VGB and were monitored for toxicity at VEU, SickKids
were tested. While all of these study participants were monitored for toxicity at SickKids, not all
of these participants were seen in SickKids’s Neurology department (outside referrals). We do
not have detailed neurological history for participants who were not seen in SickKids’s
Neurology department.
Through review of the hospital’s patient charts, we were able to identify the reason for
prescribing VGB for most of the participants. Sixteen of the 22 participants were on VGB for IS,
three for other seizure disorders and we were unable to positively identify the reason for VGB
use in the remaining three participants. Neurologists from outside of SickKids treated these three
children and we do not know for sure whether they had IS or not. Based on their age at VGB
treatment, two of these three individuals may have been treated for IS.
The other seizure disorders for which VGB was prescribed (n=3) included intractable epilepsy,
partial complex seizures secondary to TSC, and complex seizure disorder secondary to
congenital cytomegalovirus infection. The participant treated with VGB for intractable epilepsy
had IS as an infant for which he was treated with ACTH. After his IS had settled, he developed
another intractable seizure disorder, for which he was treated with VGB from 11 to 13 years of
age. The other two individuals did not have IS; they had EEG recordings that did not show
hypsarrhythmia.
Review of electronic patient charts showed hypsarrhythmia in ten of twelve participants with
available EEG recordings. The other participants may not have had an EEG done or may have
had an EEG done at another institution. Furthermore, some of the files from SickKids were
harder to access since Electronic Patient Charts are only available for visits occurring after 2000.
However, hard copies of these patient files do exist in SickKids records.

67
Some of the patients were taking other AEDs concurrently with VGB treatment and some were
still taking other AEDs at time of testing. Two of the participants were part of a study while on
VGB treatment and were assigned either Flunarizine or a placebo. None of the participants were
still on VGB at the time of the testing.
14.1.2 Identifying Toxicity: Demographics
Seven participants did not have a true baseline (baseline within four weeks of initiating VGB
therapy). For these participants, their first ERG recording was used as the baseline. In the seven
individuals without a true baseline, their first ERG was recorded months to years after VGB
initiation.
Based on the ERG recordings taken while on VGB therapy, the participants were divided into
two groups: those having toxicity (subjects) and those not having toxicity (controls). Eight of the
22 participants were identified as having toxicity.
This is a diverse group of participants with wide-ranging cognitive abilities. Some participants
still have epileptic disorders and for others, the epileptic disorders have resolved. In addition to
analyzing the data based on toxicity status, we have also distinguished those who are able to
perform OCT and/or Goldmann visual field testing from those who are unable to perform such
tests as an indicator of disease severity and cognitive outcome. Goldmann visual field testing
requires high cognitive ability; participants need to follow instructions for an extended period of
time (approximately 20-40 min). OCT testing requires less cognitive ability; participants need to
place chin on chin rest and maintain fixation for 30 seconds at a time. If participants are able to
cooperate and maintain good visual fixation, the total time for OCT imaging session is
approximately 5 min. Based on this, participants who are able to perform both Goldman visual
field testing have the highest cognitive ability, participants who are able to perform OCT testing
only have lower cognitive abilities, and participants who are unable to perform either test have
the lowest cognitive abilities. It is important to note that this is a very rudimentary scale and does
not capture true cognitive ability or differences based on age. We are only using this as marker
for cognitive ability and disease severity since we were unable to perform formal
neuropsychological assessments.

68
Nine of 14 participants without toxicity were able to perform Goldmann visual field testing and
OCT imaging. Three of eight participants with toxicity were able to undergo both assessments;
and one participant with toxicity was able to undergo OCT imaging only. Using the Fisher exact
test, there is no difference in terms of cognitive ability between these groups.
Table 4-1 provides a comparison of the demographic information between the subjects and
controls. Three of the eight participants with toxicity and eight of the 14 participants without
toxicity were male.
Table 14-1 – Demographic information for study participants.
No Toxicity (n=14) Toxicity (n=8) p-value Sex (Male/Female) 8/6 3/5 0.7#
Age at Testing (years) 11.5 ± 2.1 (8.8 to 14.5) 15.4 ± 5.6 (10.5 to 23.4) 0.3
Age at VGB initiation (months) 9.5 ± 8.0 (2.7 to 40) 33.3 ± 50.5 (2.6 to 137) 0.3
Duration of VGB treatment (months)
16.0 ± 10.8 (2.5 to 36.5) 45.3 ± 49.1 (8.8 to 120) 0.07
Time since VGB discontinuation (years) 9.7 ± 2.0 (6.3 to 12.6) 8.8 ± 2.9 (3.1 to 12.6) 0.4
Not having a true baseline 29%b (4/14) 38% (3/8) 1.0#
Able to perform Goldmann Visual Field testing
64% (9/14) 38% (3/8) 0.4#
Able to perform OCT imaging 64% (9/14) 50% (4/8) 0.7#
Data are presented as mean ± SD (range); p-values are for Wilcoxon Two-Sample Test; # -
Analyzed using Fisher’s exact test.
Age of VGB initiation ranged from 3 months of age to 11 years of age in participants with
toxicity and from 3 to 40 months in control participants. Figure 14-1 is a scatterplot showing the
age at which participants started VGB treatment. The age at VGB initiation for the two groups
was not statistically significant (Wilcoxon Two Sample Test, p=0.3). Most of the participants
started VGB treatment under two years of age; only three of the 22 participants starting VGB

69
after two years of age. The two individuals who started VGB much later (i.e after five years of
age) both show toxicity.
The length of VGB treatment ranged from 3 months to ten years. Figure 14-2 is a scatterplot
showing the duration of VGB treatment for participants with and without toxicity. All
participants, except one, were on VGB continuously. This participant stopped VGB treatment
and then restarted VGB six months later. There is no significant difference in the duration of
VGB treatment between the two groups (Wicox Rank Sum, p=0.07).
Figure 14-1 – A plot illustrating the age range at which participants started VGB treatment. Blue
diamonds represent the values for participants without toxicity and red diamonds represent the
values for participants with toxicity. Filled diamonds represent participants who are able to
perform Goldmannn visual field testing and OCT imaging, asterisk represents participants who
are able to perform OCT imaging only and unfilled diamonds represent participants who are
unable to perform either Goldmann visual fields or OCT imaging.
020
4060
80100120140
Age
at V
GB
Initi
atio
n (m
onth
s)
No Toxicity Toxicity

70
Figure 14-2 – Plot illustrating the duration of VGB treatment for all participants. Blue diamonds
represent the values of participants without toxicity and red diamonds represent the values of
participants with toxicity. Filled diamonds represent participants who are able to perform
Goldmannn visual field testing and OCT imaging, asterisk represents participants who are able to
perform OCT imaging only and unfilled diamonds represent participants who are unable to
perform either Goldmann visual fields or OCT imaging.
14.2 Clinical Examination
Visual acuity, contrast sensitivity and colour vision were attempted in all patients. However, due
to developmental and cognitive delays, we were unable to obtain some of these measures in
some participants.
Visual acuity was measured in all eight participants with VGB toxicity. Five participants were
assessed using ETDRS charts (+/- Cardiff cards). Of the three study participants who were
unable to be tested using ETDRS charts, two were assessed using Cardiff cards and one
participant was assessed using Teller cards.
Of the fourteen participants without VGB toxicity, visual acuity was measured in thirteen
individuals. Of the participants without toxicity, nine participants were assessed using ETDRS
charts (+/- Cardiff cards) and five participants were assessed using Cardiff cards only. The other
participant had severe global developmental delay and could not be assessed using ETDRS or
020
4060
80100120
VG
B D
urat
ion
(mon
ths)
No Toxicity Toxicity

71
Cardiff cards. In this participant, it could only be concluded that she was able to fix and follow
light.
Of the eight participants with toxicity, contrast sensitivity and colour vision were assessed in six.
Of the 14 participants without toxicity, contrast sensitivity was assessed in nine participants and
colour vision was measured in 11 participants. Refractive error was measured in most
participants.
Two of the nine participants without toxicity have visual acuity scores above 0.2 logMAR (upper
limit of visual acuity for a typically developing 8-year old child) as assessed by ERDRS charts.
Three of the five participants without toxicity have visual acuity scores above 0.2 logMAR as
assessed by ERDRS charts.
Figure 14-3 – Distribution of the visual acuity scores as measured by the ETDRS charts (testing
distance: 4 metres). All values plotted are averaged between the right and left eyes. Blue
diamonds represent the scores of participants without toxicity and red diamonds represent the
scores of participants with toxicity. Filled diamonds represent participants who are able to
perform Goldmannn visual field testing and OCT imaging, asterisk represents participants who
are able to perform OCT imaging only and unfilled diamonds represent participants who are
unable to perform either Goldmann visual fields or OCT imaging. Dashed line represents the
upper limit of visual acuity for a typically developing 8-year old child.
0.0
0.2
0.4
0.6
Vis
ual A
cuity
- E
TDR
S(lo
gMA
R)
No Toxicity Toxicity

72
Of the 17 individuals who were able to perform colour vision testing, 13 participants had a
perfect score along all three colour confusion lines. One participant with toxicity showed a mild
reduction along all three axes. The other three participants, two of whom did not have VGB
toxicity, had slight reductions along the tritan line.
Results for visual acuity, contrast sensitivity and colour vision assessments are presented in
detail in Appendix G and Appendix H. The distribution of results for visual acuity measured with
ETDRS charts, visual acuity measured with Cardiff cards, and contrast sensitivity are displayed
in boxplots (Figure 14.3, Figure 14-4, and Figure 14-5, respectively). Table 14-2 provides a
summary of the results.
Figure 14-4 – Distribution of the visual acuity scores as measured by Cardiff cards (testing
distance: 55 cm). All values plotted are averaged between the right and left eyes. Blue diamonds
represent the scores of participants without toxicity and red diamonds represent the scores of
participants with toxicity. Filled diamonds represent participants who are able to perform
Goldmannn visual field testing and OCT imaging, asterisk represents participants who are able to
perform OCT imaging only and unfilled diamonds represent participants who are unable to
perform either Goldmann visual fields or OCT imaging. Dashed line represents the upper limit of
visual acuity for a typically developing 8-year old child.
0.00
0.05
0.10
0.15
0.20
0.25
0.30
Vis
ual A
cuity
- C
ardi
ff(lo
gMA
R)
No Toxicity Toxicity

73
Figure 14-5 – Distribution of the contrast sensitivity scores as measured by M&S Smart System
II (testing distance: 4 metres). All values plotted are averaged between the right and left eyes.
Blue diamonds represent the scores of participants without toxicity and red diamonds represent
the scores of participants with toxicity. Filled diamonds represent participants who are able to
perform Goldmannn visual field testing and OCT imaging, asterisk represents participants who
are able to perform OCT imaging only and unfilled diamonds represent participants who are
unable to perform either Goldmann visual fields or OCT imaging. Dashed line represents the
upper limit of contrast sensitivity for a typically developing 8-year old child.
Table 14-2 – Visual acuity and contrast sensitivity results for participants
No Toxicity Toxicity p-value Visual Acuity – ETDRS (logMAR) 2/9 (22%) 3/5 (60%) 0.3
Visual Acuity – Cardiff (logMAR) 0/11 1/5 (20%) 0.3
Contrast Sensitivity – M&S 3/9 (33%) 4/6 (67%) 0.3
Data are presented as proportion (percentages) of participants scores above the upper limits of a
typically developing 8-year old; p-values are for 2-tailed Fisher’s exact test.
02
46
810
Con
trast
Sen
sitiv
ity
No Toxicity Toxicity

74
14.3 Visual Fields
In most participants, the visual field was analyzed with three different targets: I 2e, I 4e and IV
4e. Three of the eight participants with toxicity were able to perform Goldmann perimetry.
However, one of these subjects had occipital lobe damage and thus his visual field results were
not used for analysis. He showed severe constriction of the visual fields. In another participant
with toxicity, only the large target size was used for analysis due to lack of cooperation.
Nine of the 14 control participants were able to perform Goldmann perimetry. In one control
participant, the large target (I IV 4e) was not used to test the visual field of the left eye due to
time constraints.
The extent of the visual field from the fovea (measured in degrees) along the temporal, superior,
nasal and inferior meridians were recorded for each target size from the hand-drawn output
reports. Appendix I provides detailed information on the visual field measurements using the
different target sizes in all participants. Figure 14-6, Figure 14-7, and Figure 14-8 illustrates the
extent of the visual field as measured using the I 2e, I 4e and IV 4e target sizes, respectively.
Figure 14-6 – Distribution of the extent of the visual field along the four meridians as measured
by Goldmann perimetry (target size I 2e). All values plotted are averaged between the right and
left eyes. Blue diamonds represent the scores of participants without toxicity and red diamonds
represent the scores of participants with toxicity.
1015
2025
3035
4045
Ext
ent o
f vis
ual f
ield
(deg
rees
from
fove
a)
Temporal Superior Nasal Inferior

75
Figure 14-7 – Distribution of the extent of the visual field along the four meridians as measured
by Goldmann perimetry (target size I 4e). All values plotted are averaged between the right and
left eyes. Blue diamonds represent the scores of participants without toxicity and red diamonds
represent the scores of participants with toxicity.
Figure 14-8 – Distribution of the extent of the visual field along the four meridians as measured
by Goldmann perimetry (target size IV 4e). All values plotted are averaged between the right and
left eyes. Blue diamonds represent the scores of participants without toxicity and red diamonds
represent the scores of participants with toxicity.
5060
7080
90
Ext
ent o
f vis
ual f
ield
(deg
rees
from
fove
a)
Temporal Superior Nasal Inferior
3040
5060
70
Ext
ent o
f vis
ual f
ield
(deg
rees
from
fove
a)
Temporal Superior Nasal Inferior

76
The primary measures that we were interested in were measures obtained from using the large
target size (IV 4e). The large target provides an estimate of the extent of the peripheral visual
field whereas the small target size is a measure of more central fields. Table 14-3 provides a
summary of the mixed model results for visual fields along four meridians as measured by the IV
4e target size. The interaction term shows significance indicating that toxicity is meridian
specific. The model shows significant differences along the temporal and nasal meridians
between participants with toxicity and participants without toxicity.
Table 14-3 – Summary of mixed model results for visual fields by meridians.
Meridian No Toxicity – LS Means
Toxicity – LS Means Difference p-value
Temporal (Degrees) 79.7 (75.5-83.9) 64.0 (55.1-72.9) 15.7 (5.8-
25.6) 0.006
Superior (Degrees) 47.7 (45.4-50.0) 46.0 (41.1-50.9) 1.7 (-3.7-7.0) 0.5
Nasal (Degrees) 57.3 (54.0-60.7) 45.8 (38.7-52.8) 11.6 (3.8-
19.4) 0.008
Inferior (Degrees) 58.5 (49.7-67.3) 1.5 (-8.2-
11.2) 0.7
Data are presented as estimate (95% confidence interval) and are measured as degrees from the
central fixation.
The extent of the peripheral visual field (target size: IV 4e) as measured along the temporal and
nasal meridians were significantly smaller in participants with toxicity when compared to
participants without toxicity. If we use Wild’s classification of visual fields [181], both
participants with toxicity show a mild constriction of the visual field (fields extending 50o – 70o
along the temporal meridian). The first individual showed a nasal inflection (Figure 14-9 A).
The other individual with toxicity did not show the typical pattern of bilateral concentric
constriction with nasal predominance(Figure 14-9 B).

77
Figure 14-9 – A) Goldmann visual field of a 12-year female who was on VGB for 73 months for
complex partial seizures and had toxicity as defined by the ERG (ID:1209). Participant had been
off VGB for 4.5 years at time of Goldmann perimetry. Testing was done using target sizes I 2e, I
4e, and IV 4e. Reliability and fixation: okay. B) Goldmann visual field of a 23-year male who
was on VGB for 29 months for intractable epilepsy and had toxicity as defined by the ERG (ID:
1226). Participant had been off VGB for 9.8 years at time of Goldmann perimetry. Testing was
done using target size IV 4e. Reliability: very poor; fixation: good.
A
B

78
Eight of the nine participants without toxicity had normal visual fields according to Wild’s
classification (visual field extending >70o along the temporal meridian). The only participant
without toxicity showing a visual field reduction had a visual field measure that was at the cut-
off of normality with the temporal meridian extending to approximately 70o in the right eye and
68 o in the left eye. Figure 14-10 is the Goldmann visual field of an individual who does not
develop toxicity.
Figure 14-10 – Goldmann visual field of a 9-year male who was on VGB for 9 months IS and
did not have toxicity as defined by the ERG(ID:1239). Participant had been off VGB for 7.8
years at time of Goldmann perimetry. Testing was done using target sizes I 2e, I 4e, and IV 4e.
Reliability and fixation: good.
14.4 Examination by Ophthalmologist
The eyelids, conjunctiva, cornea, anterior chambers, pupil, lens and vitreous of all participants
were examined by a neuro-ophthalmologist using a slit lamp. Following dilation, the fundi were
examined by indirect ophthalmoscopy. All abnormal findings were recorded (see Appendix J for
details).
The fundi were found to be normal by indirect ophthalmoscopy in one of eight participants with
toxicity and in 12 of 14 participants without toxicity. One participant with toxicity had retinal
hamaratomas in the context of TSC. The fundi changes observed included inverse atrophy,

79
diffuse atrophy or both. Inverse atrophy is the characteristic retinal atrophy associated with VGB
damage and involves atrophy of the nasal neuroretinal rim with relative sparing of the temporal
neuroretinal rim [198]. Four participants who were identified as having VGB toxicity using the
ERG showed clinical signs of VGB retinal damage and none of the participants without toxicity
showed patterns of inverse atrophy. Two participants with toxicity and two participants without
toxicity showed funduscopic patterns of RFNL reductions that were not specific to VGB defects
(generalized/diffuse RNFL reductions).
14.5 Imaging: Fundus Photography
Fundus photographs was taken in four of the eight participants with toxicity and in eight of the
14 participants without toxicity. Two different neuro-ophthalmolgoists, Dr. Raymond Buncic
(Reviewer #1) and Dr. Arun Reginald (Reviewer #2), independently reviewed the available
fundus photos of the participants. They were masked to the grouping of toxicity vs. control.
Appendix K provides detailed results of each reviewer’s evaluations. Table 14-4 provides a
summary of their findings.
Table 14-4 – Evaluation of fundus photography
Normal Inverse Atrophy
Diffuse Atrophy
Inverse and Diffuse Atrophy
No Toxicity Reviewer # 1 8 0 0 0 Reviewer #2 4 1 3 0
Toxicity Reviewer # 1 2 1 1 0 Reviewer #2 0 1 3 0
Values represent the total number of individuals in each category. Numbers in brackets indicate
the ratio of participants with toxicity to participants without toxicity.
In the present study, the fundus photographs of the participants were categorized into four
groups: normal, inverse atrophy, diffuse atrophy, and inverse and diffuse atrophy. There were
marked differences between the evaluations by the two reviewers as well as differences between
indirect ophthalmoscopy and fundus photography. There was agreement between the reviewers
in 50% (6/12) of the cases. Compared to reviewer #2, reviewer #1 classified the photographs as
being normal more frequently. Reviewer #1 did not find any patterns of inverse or diffuse
atrophy in all eight participants without toxicity. Of the same eight participants, reviewer #2

80
classified one participant as having inverse atrophy, three as having diffuse atrophy and only
four as having physiological fundus. Reviewer #2 found all participants with toxicity to have
either inverse or diffuse atrophy (1 inverse atrophy and 3 diffuse atrophy). However, reviewer #1
found two of these participants to have physiological fundi.
There are differences between classification of the participants based on fundus photography and
based on fundus exam by indirect ophthalmoscopy. Reviewer #1 is more in agreement with
results from indirect ophthalmoscopy (agreement in 75% of cases) than reviewer#2 (agreement
in 50% of cases). Interestingly enough, reviewer #2 performed the majority of the indirect
ophthalmoscopy examinations. This discrepancy likely results from poor-quality, under-exposed
fundus photography images. In his review, reviewer#2 commented on the difficultly and the
ensuing uncertainty in assessing the photos.
14.6 Imaging: Optical Coherence Tomography
Imaging using OCT was performed in 13 participants; in the remaining nine participants
developmental delay and level of cooperation did not allow imaging.
14.6.1 200x200 Optic Disc Cube
13 of the 22 subjects were able to perform OCT imaging: four with VGB toxicity and nine
without VGB toxicity. The summary measures (group mean and standard deviation) of the
RNFL thickness at the optic disc, as a function of quadrant, for the groups with and without
toxicity are given in Table 14-5.
Table 14-5 – Results of Optic Disc Scan
Data are presented as mean ± SD (range); p-value for student t-test.
No Toxicity N=9 Toxicity N=4 p-value Signal Strength 9.1 ± 0.6 (8 to 10) 9.0 ± 1.1 (7.5 to 10) Global Average (µm) 95.9 ± 6.0 (88.5 to 103.5) 68.5 ± 4.2(63 to 72) <0.0001**

81
Individuals with VGB toxicity exhibited attenuated global RNFL at the optic disc compared to
individuals without VGB toxicity (p<0.0001, Student t-test) (Figure 14-11). Three of the four
individuals with VGB toxicity manifested thinning of the nasal, superior and inferior quadrants
in the presence of a normal temporal nerve fiber layer(Figure 14-12). The other participant with
toxicity exhibited attenuated superior and inferior quadrants in the presence of normal nasal and
temporal quadrants. Table 14-6 presents the mixed model results of the RNFL parameters by
quadrants. The model shows that toxicity is quadrant specific and that significant differences
exist along the nasal, superior and inferior quadrants between participants with toxicity and
participants without toxicity.
Figure 14-11– Distribution of the global retinal nerve fibre layer!thickness!(μm)!as!measured by
the 200x200 Optic Disc Protocol (Cirrus; Carl Zeiss Meditec Inc, Dublic, CA). All values plotted
are averaged between the right and left eyes. Blue diamonds represent the values of participants
without toxicity and red diamonds represent the values of participants with toxicity.
7080
90100
Mea
n R
etin
al N
erve
Fib
re L
ayer
Thi
ckne
ss (µ
m)
No Toxicity Toxicity

82
Figure 14-12– Distribution of the retinal nerve fibre layer!thickness!(μm)!by!quadrants!as!
measured by the 200x200 Optic Disc Protocol (Cirrus; Carl Zeiss Meditec Inc, Dublic, CA). All
values plotted are averaged between the right and left eyes. Blue diamonds represent the values
of participants without toxicity and red diamonds represent the values of participants with
toxicity.
Table 14-6 – Summary of mixed model results for retinal nerve fibre layer thickness by
quadrants
Quadrant No Toxicity – LS Means of RNFL Thickness (µm)
Toxicity - LS Means of RNFL Thickness (µm)
Difference in RNFL Thickness (µm)
p-value
Temporal 65.7 (58.3-73.1) 62.1 (51.0-73.2) 3.5 (-9.8-16.9) 0.6 Nasal 66.6 (59.9-73.3) 48.9 (38.8-58.9) 17.7 (5.7-29.8) 0.008 Superior 127.4 (122.7-132.1) 79.4(72.3-86.4) 48.0 (39.5-56.5) <0.0001 Inferior 123.7 (113.9-133.5) 83.5 (68.8-98.2) 40.2 (22.5-57.9) 0.0004 Data are presented as estimate (95% confidence interval).
The Cirrus OCT system also calculated individual RNFL thickness of all 12 clock-hour sectors
for each eye. RNFL thickness parameters in participants with and without toxicity as determined
by the mixed model are presented in Table 14-7 (details in Appendix L).
4060
80100
120
140
Ret
inal
Ner
ve F
ibre
Lay
er T
hick
ness
(µm
)
Superior Nasal Inferior Temporal

83
Table 14-7 – Summary of mixed model results for retinal nerve fibre layer thickness by clock
hours.
Clock Hour
Controls – LS Means of RNFL Thickness (µm)
Subjects - LS Means of RNFL Thickness (µm)
Difference in RNFL Thickness (µm)
p-value
12:00 133.4 (123.1-143.8) 76.5 (61.0-92.0) 56.9 (38.4-75.5) <0.0001 1:00 121.1 (105.5-136.7) 76.4 (53.0-99.8) 44.7 (16.6-72.8) 0.005 2:00 83.4 (70.9-95.8) 58.8 (40.1-77.4) 24.6 (2.2-47.1) 0.03 3:00 49.7 (44.7-54.6) 44.6 (37.2-52.0) 5.0 (-3.9-13.9) 0.2 4:00 64.6 (54.7-74.4) 43.6 (28.9-58.4) 20.9 (3.2-38.6) 0.02 5:00 101.1 (88.7-113.5) 54.1 (35.6-72.7) 47.0 (24.7-69.3) 0.0007 6:00 129.8 (110.0-149.5) 81.5 (51.9-111.1) 48.3 (12.7-83.9) 0.01 7:00 139.8 (129.4-150.3) 114.9 (99.2-130.6) 25.0 (6.1-43.8) 0.01 8:00 70.1 (60.3-79.8) 72.8 (58.2-87.3) -2.7 (-20.2-14.8) 0.7 9:00 51.3 (42.6-59.9) 55.9 (42.9-68.8) -4.6 (-20.2-11.0) 0.5 10:00 76.3 (65.1-87.4) 56.8 (40.0-73.5) 19.5 (-0.5-39.6) 0.06 11:00 125.4 (110.5-140.4) 82.0 (59.6-104.4) 43.4 (16.5-70.4) 0.005 Data are presented as estimate (95% confidence interval).
Figure 14-13 uses a colour scale to represent the distribution of p-values, with smaller p-values
(greater differences) being represented on the red end of the spectrum and larger p-values
(smaller differences) being represented on the green end of the spectrum.
There were statistically significant differences (α=0.05; p < 0.004 with Bonferroni correction for
multiple comparisons) between the two groups in clock hour segments 12:00 and 5:00. Less
significant differences exist in clock hour segments 2:00, 4:00 and 6:00. Spatial mapping shows
that all superior segments are significantly attenuated and that the temporal segments are the
least attenuated. The interaction terms in the mixed models show significance indicating that
toxicity is clock-hour segment specific.

84
Figure 14-13 – Plot of p-values of based on mixed model results of the retinal nerve fibre layer
thickness by clock-hour segments. The average of the right and left eyes were analyzed. Left
eyes were treated as mirror images; 2:00 to 4:00 represents the nasal clock hours, 5:00 to 7:00
represents the inferior clock hours, 8:00 to 10:00 represents the temporal clock hours and 11:00
to 1:00 represents the superior clock hours. Sectors 11:00, 12:00, 1:00 and 5:00 show significant
differences between the two groups with Bonferroni correction.
14.6.2 Ganglion Cell Analysis
Ganglion cell analysis provides the thickness of the ganglion cell layer plus the inner plexiform
layer using the macular cube protocol. Table 14-8 provides a summary of the ganglion cell
analysis for participants with and without toxicity. The average thickness of the combined
ganglion cell layer and inner plexiform layer did not show significant differences between the
two groups. However, upon spatial analysis, we note a slight reduction in the thickness of the
6:00 segment (Figure 14-14).
Legend
! p<0.004 *
! p<0.01
! p<0.05
! p>0.05
Note: Bonferroni correction,

85
Table 14-8 – Ganglion cell analysis for study participants
No Toxicity N=9 Toxicity N=4 p-value Signal Strength 9.4 ± 0.5 (8.5 to 10) 9.8 ± 0.3 (9.5 to 10) Average GCL/IPL (µm) 80.1 ± 5.7 (72.5 to 89) 75.7 ± 6.0(70 to 82) 0.9
Minimum GCL/IPL (µm) 77.3 ± 5.0 (68 to 86.5) 72.1 ± 7.8 (64 to
79.5) 0.9
Data are presented at mean ± SD (range) and are measured as degrees from the fovea; p-values
are for Wilcoxon Two-Sample Test.
Figure 14-14 – Plot of p-values of pair-wise comparisons (one-tailed) of the combined ganglion
cell layer and inner plexiform layer thickness by clock-hour segments. The average of the right
and left eyes were analyzed. Left eyes were treated as mirror images. Sector 6:00 shows slight
attenuation in the group with VGB toxicity.
14.7 Photopic Electroretinogram
A shorted ERG protocol using DTL electrodes was done on 4 subjects with toxicity and 4
subjects without toxicity. The ERG was performed binocularly in all participants, with the
exception of three participants (two participants with toxicity and one participant without
toxicity) who were tested monocularly due to reduced cooperating (see Appendix M for details).
Recordings from one eye only were analyzed per testing session. When binocular recordings
Legend
! p<0.008 *
! p<0.01
! p<0.05
! p>0.05
Note: Bonferroni correction,

86
were available, the amplitude of the flicker response was compared between right and left eyes,
and the recording with the greater amplitude was selected for analysis.
Table 14-9 provides a summary of the findings between the two groups. None of the participants
had 3.0 flicker amplitudes that were below the 5th percentile based on age-corrected normal
values (Figure 14-15). Three of the four participants with toxicity have flicker amplitudes below
the mean age-expected value of 97 µV while only one of the four participants without toxicity
falls below this value. The participants with VGB toxicity have lower flicker amplitude
compared to participants without toxicity (mean: 87 µV vs 114 µV). However, this difference is
not significant.
Table 14-9 – ERG results for study participants
No Toxicity N=4 Toxicity N=4 p-value
Age (years) 11.4 ± 3.2 (9.0 to 15.8) 14.8 ± 5.7 (10.5 to 23.2) 0.3
Time since VGB discontinuation (years) 9.3 ± 2.2 (7.6 to 12.6) 6.4 ± 3.2(3.1 to 9.8) 0.5
Follow-up Flicker Amplitude!(μV) 114 ± 32 (80 to 156) 87 ± 40 (60 to 146) 0.2
Change in Flicker Amplitude from Baseline (μV)
33 ± 24 (10 to 63) -30± 38 (-66 to 24) 0.1
Data are presented at mean ± SD (range); p-values are for Wilcoxon Two-Sample test.
There seems to be a difference in the change of the flicker amplitude from baseline between
participants with and without toxicity, however this is not significant (Figure 14-16). All
participants without toxicity show an increase in flicker amplitude compared to baseline as
indicated by positive delta values. Only one participant with toxicity showed an increase in the
amplitude from baseline. The other three participants with toxicity have reduced amplitudes.

87
Figure 14-14 – Distribution of the raw 3.0 flicker amplitude (µV) as measured using DTL
electrodes on the follow-up visit. When a subject has recordings from both the right and left eye,
the higher amplitude is plotted. Blue diamonds represent the amplitudes of participants without
toxicity and red diamonds represent the amplitudes of participants with toxicity. The solid line
represents the mean value of the flicker amplitude in typically developed eyes (97 µV). The
dotted lines represent the 5th and 95th percentiles of the distribution of flicker amplitudes in
typically developed eyes.
A moderate negative correlation (r = -0.59) was present between the amplitude of the flicker
response on the follow-up visit and the duration of VGB treatment (Figure 14-17). However,
this was not significant (p=0.12). Interestingly, all four participants who were on VGB for less
than 24 months, have flicker amplitudes greater than 100 µV.
6080
100
120
140
160
Flic
ker A
mpl
itude
(µV
)
No Toxicity Toxicity

88
Figure 14-16 – Distribution of the change in flicker amplitude from baseline (µV) as measured
using DTL electrodes. All values plotted are calculated by subtracting the current flicker
amplitude from the flicker amplitude obtained from the subject’s initial visit (baseline). Positive
values indicate an increase in the flicker amplitude and negative values indicate a reduction in
the flicker amplitude from baseline measurement. When binocular recordings were available, the
amplitude of the flicker response was compared between right and left eyes, and the recording
with the greater amplitude was selected for calculating the differences. Blue diamonds represent
the differences of participants without toxicity and red diamonds represent the difference of
participants with toxicity.
-0.3
-0.2
-0.1
0.0
0.1
0.2
0.3
Cha
nge
in F
licke
r Am
plitu
de fr
om B
asel
ine
(µV
)
No Toxicity Toxicity

89
!
Figure 14-17 – Flicker amplitude (log µV) as a function of duration of vigabatrin treatment
(months) (r = -0.61, p=0.11). Open circles represent participants exposed to vigabatrin but with
no VGB toxicity and filled circles represent participants with VGB toxicity.
0 20 40 60 80 100 120
1.8
1.9
2.0
2.1
2.2
Duration of Vigabatrin (months)
Flic
ker A
mpl
itude
(log
µV
)

90
15 Discussion
The present study investigated the functional and structural changes in individuals with VGB
toxicity as identified by the electroretinogram. To our knowledge, a long-term follow-up study
consisting of visual field examination and OCT imaging of children assessed using the ERG for
VGB toxicity has never been done before. The current study examined the standard
electrophysiological marker for detection of VGB toxicity, the 30-Hz flicker amplitude.
Structural and functional changes associated with diagnosis of VGB toxicity were examined
using OCT, Goldmann perimetry and fundus photography. ERGs were recorded to examine
long-term retinal changes associated with VGB discontinuation. The major findings were that
both visual field reductions and attenuation of the RNFL as determined by optical coherence
tomography are associated with VGB toxicity. The pattern of RNFL loss (attenuation of the
nasal RNFL and the sparing of the temporal RNFL) is in accordance with the visual field pattern
observed with VGB toxicity.
15.1 Demographics
In the current study, the participants with toxicity have been on VGB for a significantly longer
duration than the participant group without toxicity (p=0.02). This suggests that there may be
differences between the two groups. The group with toxicity may have greater disease severity or
may have other co-morbidities that increase their susceptibility to developing toxicity. Other
studies have found correlations between visual field loss and duration of VGB therapy and
dosage [176, 278]. Similarly, our study suggests duration of treatment may affect development
toxicity. However, it is important to note that diagnosis of toxicity is also dependent on the
number of ERG tests since classification of toxicity requires two consecutive ERG tests that
show reduced flicker amplitudes. Therefore, individuals who are on VGB longer will have more
ERG tests and are more likely to be categorized as having toxicity. And individuals who are on
VGB for a very short time may not have undergone the three tests (baseline and two follow-ups)
necessary for diagnosing toxicity, particularly since ERG tests are usually scheduled three to six
months apart.
IS is a catastrophic epilepsy syndrome of childhood since it has such a high incidence of
developmental regression in infants [23]. It is important to note that there is a wide range of

91
outcomes for individuals with seizures in infancy. Some patients achieve spasm cessation
immediately while others have chronic epilepsy. In the current study, participants had no
developmental delay, mild developmental delay, and severe developmental delay. The study was
not designed to identify a relationship between VGB duration and disease severity. Given the
small number of participants in this study it is difficult to establish concrete relationships but this
study does seem to suggest that some relationship between VGB duration and cognitive outcome
exists. Of the five individuals who have been on VGB for over 30 months, only one participant
was able to perform Goldmann visual field testing. It is well known that chronic or intractable
epilepsy is associated with neuropsychological impairment. AEDs also contribute to cognitive
deficits (impaired attention, vigilance, and psychomotor speed) [279]. Older age of spasm onset
and shorter time to treatment from spasm onset is associated with better developmental outcome
[24, 280].
Cognitive outcome is dependent on underlying pathology, and individuals with previously
defined cryptogenic IS have better outcomes than individuals with symptomatic IS [280]. A
study in Iceland found all children with cryptogenic IS to achieve spasm cessation and to have
normal intellectual development [281]. The current study consists of participants with both
symptomatic and cryptogenic disease. Some underlying etiologies present in this cohort were
TSC, Down syndrome, Rett syndrome, neurofibromatosis 1, and G6PD deficiency. Due to small
sample sizes, we were unable to ascertain a relationship between etiology and disease severity.
15.1 Visual Fields
This study supported our hypothesis and we were able to confirm the association of VGB
toxicity, as defined by the 30-Hz flicker amplitude, and visual field reductions as determined by
Goldmann perimetry later in life. The 30-Hz flicker amplitude has a sensitivity of 100% and a
specificity of 89% for detecting mild visual loss along the temporal visual field.
Similar to other studies, this study shows that visual field loss is evident in VGB-treated patients.
Of the 11 individuals with Goldmann perimetry results, three (25%) showed asymptomatic
visual field loss. This is consistent with the values reported in a recent literature review [187].

92
In the current study, only one of four participants defined as having ERG toxicity showed
recovery of the 30-Hz flicker amplitude on the follow-up ERG after over eight years since VGB
discontinuation. The recovery observed in the individual may be a result of poor ERG recordings
during initial VGB toxicity monitoring. Clinical notes indicate that the he was awake and
distressed in two of the ERG testing sessions, and therefore, he may have been incorrectly
classified as having toxicity. The other three participants (75%) with toxicity did not show
recovery. Overall, this study shows that visual field loss and reductions in flicker amplitude exist
3-13 years after VGB discontinuation, which suggests that visual field loss and reduced flicker
responses are permanent, irreversible drug-induced toxicity effects. This finding is consistent
with other studies [169, 181].
Kjellström and colleagues evaluated the long-term prognosis of adults on VGB and found visual
field reductions and ERG abnormalities (reduced 30-Hz flicker response, rod response, and
mixed cone-rod response) 4-6 years following VGB discontinuation [282]. However, a long-term
follow-up of children treated with VGB in infancy, shows a lower frequency of visual field loss
than what has been previously reported in the literature [188]. This may be because the children
included in the study had good seizure outcome.
It is unclear whether seizure type, developmental delay, or the presence of other co-morbidities
have an effect on the risk of developing visual field loss. This is complicated by the difficulty in
performing reliable perimetric testing on developmentally-delayed and cognitively-impaired
individuals. Werth & Schadler found comparable visual field reductions in young children and
developmentally-delayed adolescents (age range: 1- 15 years) using a noncommercial arc
perimeter and a forced-choice, preferential-looking method [190]. Agrawal and colleagues found
similar trends using white sphere kinetic perimetry [283] in children with mild to severe
developmental delay [191]. However, most modified perimetric methods cannot be used in
individuals with profound developmental delay. Thus, it is uncertain whether individuals with
profound developmental delay are more susceptible to retinal damage with VGB treatment.
Our study shows that the ERG is associated with visual field loss, as measured along the
temporal meridian. Using Wild’s classification of normal fields (temporal visual fields extending

93
>70o from central fixation) with the large Goldmann target (IV4E) [181], ERG classification of
toxicity has a sensitivity of 100% and a specificity of 89%.
Previous studies have examined the relationship between the light adapted fast 30-Hz flicker
cone ERG and VGB-VFL [179, 210, 221]. Understanding this relationship is of particular
importance since it is recommended that patients less than two years of age be monitored for
VGB-associated retinal defects using the ERG. Harding and colleagues found the 30-Hz flicker
amplitude to be the best predictor of visual field loss with a sensitivity of 100% and a specificity
of 75% [210]. Other studies have also found strong correlations between the 30-Hz flicker
response and visual field loss [179, 221]. However, the majority of these studies were not based
on a pediatric population, primarily due to difficulties assessing visual fields in young children.
This is of concern because most individuals are prescribed VGB for IS, an epileptic disorder
observed in children less than two years of age. Spencer and Harding [194] explored the
relationship between field-specific VEP, ERG and visual field loss in a pediatric population (age
range: 3 – 15 years). Of the various ERG parameters, only the 30-Hz flicker with a cut-off
amplitude below 70µV served as a good predictor of visual field loss with a sensitivity of 75%
and a specificity of 71%. The Field-specific VEP was also found to be a good predictor of visual
field loss with a sensitivity of 75% and a specificity of 85.7%. The aforementioned study, like
ours, was limited by the number of children able to perform perimetry (11/39; 28.2%). The study
supports our findings that a degradation of the 30-Hz flicker response is associated with visual
field loss.
Previous studies that have examined the relationship between ERG and visual field loss in VGB
have not controlled for other existing co-morbidities. In some children, the 30-Hz flicker
response is abnormally reduced before the initiation of VGB treatment [284]. Our study
overcomes this shortfall by defining toxicity based on each child’s own baseline (pre-drug) ERG
response.
In the current study, the visual field showed differences along the temporal and nasal meridians
between the groups with and without VGB toxicity, with the most prominent differences
occurring along the temporal meridian. In contrast to the typical patterns of VGB-VFL, none of

94
the patients showed a nasal predominance of the field loss. This may be because nasal field loss
is not as easily captured by kinetic perimetry [238].
Furthermore, the origin of the defects is not clear in individuals who are able to perform
perimetric testing and show abnormal results. The visual field defect may arise from the retina or
from higher-level visual processing. One subject was classified as having VGB toxicity based on
previous ERG results. His visual field testing showed severe constriction (less than 50o along the
temporal meridian from central fixation), particularly in the left eye. However, on the follow-up
ERG, the participant showed total recovery, indicating that the visual field loss was not retinal in
origin. Examination of the patient history revealed occipital lobe damage acquired through
seizure order and this likely contributed to the severe visual field loss observed in the child.
Russell-Eggitt and colleagues [197] found a high prevalence of visual field loss in VGB-treated
children (71%) and further examination revealed that four out of 14 children had pre-existing
visual pathway damage [197]. This highlights the broader scope of visual field defect acquisition
beyond VGB therapy alone.
It is important to note that some of the tested individuals have taken other anti-seizure
medications for an extended period of time and have other existing co-morbidities that may
possibly contribute to the observed visual field defect. Visual field abnormalities have been
observed with phenytoin, diazepam and carbamazepine [285, 286]. Furthermore, synergistic
interactions of AEDs need to be taken into account.
Some studies found a correlation between visual field loss and duration of VGB therapy and
dosage [176, 278]. VGB-VFL can occur as early as 6 weeks and as late as 10 years after
initiating VGB therapy [288, 289]. However, the majority of the patients with VGB-VFL have
been on VGB for longer than six to 12 months [290]. In our study, the participant group with
toxicity have been on VGB for a significantly longer duration than the participant group without
toxicity (p=0.02), with suggests a relationship between VGB retinal defects and drug
dosage/duration. Or it may be the result of our lab’s definition of toxicity. Since our definition of
VGB toxicity relies on serial assessments, individuals with more ERG assessments are more
likely to be categorized as having toxicity. Thus, a limitation of our study is the lack of control
for number of ERG assessments.

95
15.2 Optical Coherence Tomography (OCT)
Previous studies have examined the relationship between VGB-VFL (functional changes) and
peripapillary RNFL attenuation (structural changes) as measured by OCT [235, 237-240].
Similar studies have been performed using scanning laser ophthalmoscopy [239] and scanning
laser polarimetry [291] and have yield the same conclusions.
In recent years, there has been much interest in developing OCT as a tool to detect VGB-VFL,
which has been done primarily in adults. In a 2006 study by Wild and colleagues, all adult
patients with VGB-VFL exhibited RNFL thickness values that were below the lower 95%
confidence interval for normality (100% sensitivity) [239]. Further studies have also shown
similar trends in children and in adults with learning disabilities [292]. Our study further
supports the notion that thinning of the RNFL is a marker for VGB-VFL. Moseng and colleagues
observed that RNFL attenuation occurs with advanced visual loss (loss within 30o of central
fixation) and with peripheral loss only. Also, individuals with VGB exposure but no visual field
loss may exhibit an attenuated RNFL [238, 239], which suggests that structural changes at the
neuroretina may occur before functional vision loss. In patients with glaucoma, changes in the
RNFL are often detected well in advance of visual field defects [293].
Our study also explored the relationship between structural and functional changes to the retina.
Our study is unique because the functional change that it measured was the 30-Hz flicker
amplitude, and it measured it in a pediatric population. Our findings confirmed that there is a
thinning of the RNFL in patients with VGB retinal damage, which is important for various
reasons. First, it suggests that OCT may be used as an alternative to ERG to monitor VGB
toxicity in children. Secondly, it helps elucidate the mechanism of VGB-induced retinal damage.
A previous study of 12 adult patients taking VGB also showed a relationship between
RNFL thickness and ERG abnormalities [294]. The 30-Hz flicker response was found to share a
linear relationship with superior RNFL thickness (r=+0.73, p=0.007), inferior RNFL thickness
(r=+0.75, p=0.005), and total RNFL thickness(r=+0.64, p=0.026). Our study shows a similar
trend between ERG diagnosis of toxicity and attenuation of the RNFL in a pediatric cohort.

96
Lawthom and colleagues showed that the nasal quadrant is the most sensitive marker for VGB-
VFL; 11/11 patients with VGB-VFL had attenuated nasal RNFL and none of the 13 patients on
other non-GABAergic anti-epileptic drugs had nasal RNFL attenuation [238]. The finding of a
normal temporal quadrant in the presence of abnormal nasal, superior and inferior quadrants is in
agreement with the results of our study and others [237, 238, 291, 294, 295]. In contrast to the
study by Lawthom and colleagues, our study shows the most prominent difference between
individuals with without toxicity occur at the inferior and superior quadrants of the RNFL. Other
studies have also show superior/inferior RNFL thinning as the most common change [235, 291,
294].
Attenuation of the nasal RNFL and the sparing of the temporal RNFL are in accordance with the
visual field pattern observed with VGB toxicity. VGB causes a bilateral, peripheral visual field
loss with relative sparing of the central visual field. Visual fields are performed while
maintaining central fixation (macula) while an optic disc scan is centered at the optic disc.
Therefore, there is no direct retinotopic correspondence between visual field results and imaging
of the optic disc (i.e. temporal disc does not correspond to temporal visual field). The Garway-
Heath map is important in understanding the anatomical relationship between visual fields and
changes at the optic nerve head [296] (Figure 15-1).
The Garway-Heath map divides the optic disc into six sections. The areas of the nasal disc,
which consist of the three sectors that range from 81o to 270o, correspond to areas that fall on the
boundaries of the visual field. The areas of the temporal disc, which consist of sectors that range
from 271o to 80o, correspond to more central visual fields. In particular, the central macular
region (dark gray) of the visual field is associated with the temporal sector of the disc from 311o
to 40 o.
This map reveals that the central macular region is associated with the temporal sector of the
disc, the superior arcuate region of the visual field with the inferior temporal disc and the inferior
arcuate region of the visual field with the superior temporal disc. Our results show that VGB
toxicity spares the temporal sector of the optic disc; the unaffected temporal nerve fibres
originate from the fovea and the papillomacular bundles and are responsible for central vision.

97
Figure 15-1 – The Garway-Heath map relates visual field test points (A) to regions of the optic
nerve heard (B).Source: Garyway-Heath et al., 2000 [296]. Copyright permission has been
obtained, please see Copyright Acknowledgements.
The current study also highlights that RNFL attenuation can exist even in the presence of a
normal clinical examination. While evidence of disc cupping, pallor or atrophy have been
reported in patients on VGB therapy [198, 239], there are many reports of normal fundus exams
in patients with VAFVL [181, 221, 291]. Perhaps, optic atrophy only occurs with further
progression of toxicity. However, Durnian & Clearkin found no evidence of optic atrophy, disc
cupping, or pallor upon clinical examination in eight adult patients (duration of VGB treatment
range: 18 months – 13 years) with known VGB-VFL [291]. This suggests that some individuals
may be less susceptible to optic atrophy even with long term VGB treatment.
Most of the studies that have examined the relationship between VGB-VFL and RNFL thickness
are in adult patients and were on VGB for a longer period. Evaluation by scanning laser
polarimetry in eight adult patients (mean duration of VGB: 81 months; range: 18 – 154 months)
with VGB-VFL revealed reduced RNFL parameters. The study by Wild and colleagues found
reduced RNFL thickness in the group consisting of adult participants who had been exposed to
VGB and manifested VGB-VFL. Individuals in this group were exposed to VGB for over 5 years
(mean: 10.1 ± 1.9 years). Most participants in the current study were exposed to VGB in infancy
made about the size of sectors. The mean variability inassigned ONH positions to visual field test points can be aguide to appropriate sector size. The mean standard devia-tion of assigned values was 7.2°. This means that 95% of thetime a visual field test point will be associated with aposition at the ONH within approximately 14° either side ofa mean. In other words, the range of possible positions at theONH covers almost 30° for each visual field test point.When clusters of field test points are considered (sectors ofthe visual field), ONH sector size should probably be greaterthan 30° to take account of this variability. The map illus-trated in this article (Figure 7) consists of four 40° sectors,one 90° sector, and one 110° sector. The different sectorsizes represent a compromise between minimal practicalsector size and the number of visual field test points for eachONH sector.A significant feature of the visual field test is the vari-
ability across the field in the density of test points in relationto ONH sectors. The poles of the ONH are much moredensely sampled (arcuate areas of the field) than the tem-poral and nasal parts of the ONH (central and temporalareas of the field). This is likely to have a marked effect onthe ease with which glaucomatous damage at the ONH isidentified by the visual field. Criteria for glaucomatousvisual field loss typically require a cluster of points withabnormal sensitivity.20–22 If neuroretinal rim loss is focal,or uneven, the chances of obtaining a cluster of abnormalpoints will be greatest where the sampling is densest, that is,at the poles of the disc. It is, therefore, hardly surprisingthat, in early glaucoma, thinning at the poles is frequentlythe earliest identified sign.23,24 Focal loss elsewhere is lesslikely to result in a cluster of depressed field points, and theeyes remain categorized as “ocular hypertensive” or “glau-coma suspect.”
Anatomy of the RNFL
In this study, the course of RNFL defects is used to identifythe region of origin of nerve fibers. An assumption is thatthe ganglion cell axons travel in bundles toward the ONH
without any tendency to move to adjacent bundles or dis-perse, thereby preserving a retinotopic organization.The organization of the ganglion cell axons in the RNFL
and ONH is controversial.25 There are two aspects that needconsideration:1. The organization of nerve fibers within the RNFL andONH with respect to the circumferential origin of theaxon;
2. The organization of nerve fibers within the RNFL andONH with respect to the eccentricity of the origin ofthe axon.
Studies of the nerve fiber layer organization have been madein different species of the macaque monkey by injection ofhorseradish peroxidase or radioactive amino acid into theoptic nerve head or retina or by making photocoagulationburns to the retina.26–29 These have determined that a levelof organization exists within the RNFL with respect to theeccentricity of the origin of the axons, although the studiesdo not agree on the detail. Some studies have concluded thatthe longer axons, from more peripheral ganglion cells, tendto lie deeper (scleral) to shorter axons,28,29 with some in-termixing.28 Others have concluded that the axons fromperipheral ganglion cells are scattered throughout the thick-ness of the RNFL26 or lie in the superficial (vitreal) part ofthe RNFL.27 The latter study found a degree of organizationwithin the RNFL, with respect to eccentricity of origin, andextensive intermingling of fibers as they crossed the ONHmargin. The contrasting findings in some of these studiesmay relate in part to species variation in RNFL organiza-tion. Stratification in the rhesus monkey has been found tobe less prominent than in the owl monkey,28 and differencesbetween the owl monkey and macaques have been not-ed,27,30 as well as differences between different species ofmacaque.27,31These experimental studies agree that there is a clear
organization with respect to the circumferential origin ofaxons.27,28 Injections of horseradish peroxidase at the ONHmargin result in labeling of ganglion cells in a wedge-shaped sector of retina extending into the periphery, with a
Figure 7. A division of the visual field (A) and optic nerve head (B) into sectors according to the results of this study.
Garway-Heath et al ! Mapping the Visual Field to the Optic Disc
1813

98
and were on it for a much shorter time (mean of 45 months for the group with toxicity and mean
of 16 months for the group without toxicity). The current study confirms that attenuation of the
RNFL can occur with 16 months of VGB treatment. Unfortunately, the participants who showed
toxicity on the ERG with nine and 13 months of VGB treatment were unable to undergo OCT
imaging. Therefore, we were unable to discern whether RNFL attenuation occurs prior to 16
months of VGB treatment.
Some studies have not found correlations between RNFL thickness and cumulative dose of VGB
or duration of VGB treatment [291]. However, Lawthom and colleagues found a moderate
correlation between nasal RNFL thickness and cumulative dose of VGB (p<0.01) [238]. The
current study reveals a trend between RNFL thickness and duration of VGB therapy. However,
the linear correlation was not significant, potentially due to the small sample size.
VGB toxicity is characterized by damage to ganglion cells and therefore loss of ganglion cells
have been measured by damage to the optic nerve head and by visual field loss. OCT allows
assessment of the peripapillary RNFL as well as the whole retina, including the macula. Various
studies have reported on the excellent inter-visit reproducibility of FD-OCT macular imaging
and its potential for tracking glaucoma progression [297, 298]. Therefore, OCT analysis of the
macular regions in addition to analysis at the optic nerve head may provide insight into VGB-
VFL. The ganglion cell analysis report provides information about the ganglion cell layer (GCL),
which is composed of cell bodies, and the inner plexiform layer (IPL), which is composed of
RGC dendrites. The current study analyzed macular imaging in VGB-exposed patients and found
that there were no differences observed in the ganglion cell analysis between participants with
and without VGB toxicity. Macular thickness is correlated with RNFL thickness and visual fields
in patients with glaucoma; Tan and colleagues found that changes in the macula occur prior to
detectable change in visual fields [299]. Wild and colleagues reported that all patients with VGB
exposure (with and without visual field loss) exhibited macular thickness values that were within
the 95% confidence limits of normality [239]. This finding is in agreement with typical patterns
of retinal toxicity. VGB does not cause macular damage.
It is known that VGB causes increased GABA levels in the retina but the mechanism leading to
visual field loss is not well understood. Patients on sodium valproate monotherapy, an anti-

99
epileptic drug that works by inhibiting GABA-T and succinic semialdehyde dehydrogenase and
by stimulating the GABA-synthesizing enzyme, benzymeglutamic acid dehydrogenase, did not
result in attenuation of the RNFL. Ozkul and colleagues examined visual function in patients on
sodium valproate and found that visual acuity, colour vision, visual field, and ERGs were all
normal [300].
ERG results highlight a dysfunction of the cone pathway [177-179, 210, 213, 241] in conjunction
with visual field loss. This finding is supported by histological evidence revealing
disorganization of the photoreceptor layer with VGB administration. However, OCT imaging
studies reveal that VGB toxicity is not limited to the level of the photoreceptors [198, 239]; VGB
has an overall toxic effect on the neuro-retina. Atrophy of the peripapillary RNFL may represent
primary damage or may be the result of secondary retrograde atrophy. VGB therapy is associated
with the simultaneous loss of retinal ganglion cells and photoreceptor change in neonatal rats
[259] and in a human post-mortem examination [200], suggesting that photoreceptor damage and
ganglion cell damage may occur simultaneously.
15.3 Limitations
OCT imaging, Goldmann visual fields and follow-up ERGs were not possible for all study
participants, and thus information is unavailable for some participants.
The number of participants able to perform visual field testing and OCT imaging is limited by
compliance. Visual field testing is particularly challenging for young children and
developmentally-delayed individuals since long periods of cooperation and concentration are
required. Nearly 20% of adults with epilepsy are unable to undergo perimetric testing [210].
OCT imaging is less demanding than Goldmann perimetry; one subject was able to comply with
OCT imaging but was unable to undergo Goldmann perimetry.
While kinetic perimetry usually provides better results than static perimetry due to increased
interaction between tester and participant [173], the test remains very challenging for young
children and individuals with developmental delay. Even when perimetric testing is possible, the
results may be inconclusive due to poor fixation or reliability. Visual fields require a high level
of attention from the subject, as limited attention may show an artificially-reduced visual field.

100
Although it has been recommended that abnormal visual field results be verified through
multiple testing [188], we did not repeat abnormal tests in our study. In this study, we only have
reliable visual field results from two individuals with toxicity and despite both of these
individuals showing mild visual field reductions, we need to be cautious about the
generalizability of these results.
Previous studies showed that RNFL and macular thickness measurements obtained using
Fourier-domain OCT are repeatable in healthy children [301]and that OCT imaging is more
sensitive than clinical examinations in detecting various macular pathologies [302]. From our
study, 59% of the participants were able to produce quality OCT images with dilation. However,
41% of our participants have developmental delay and were unable to meet the cognitive
demands of testing.
Even though our study shows a strong relationship between ERG diagnosis of toxicity and visual
field loss, there are many shortcomings associated with ERG monitoring for toxicity, some of
which are discussed in Section 10. One problem is that ERG responses may be artificially
reduced due to poor electrode placement, Bell’s phenomenon or a child waking up during the
procedure. However, by defining VGB toxicity as the observation of two consequent reductions
in the flicker ERG, we minimize the probability of falsely categorizing a study participant as
having toxicity (false positive). Another problem with our definition of toxicity is that we define
a significant reduction based on inter-visit variations in ERG recordings from six individuals.
Given the variability of the ERG response, we may be underestimating the inter-visit variability
and thus over classifying toxicity.
Defining toxicity depends on having a reliable baseline and not having such a true pre-drug
baseline may affect the results. However, in this study we were not able find any differences in
the visual field and OCT outcomes of individuals with a true baseline and individuals with a
baseline recorded months after VGB initiation. Only one individual without a true baseline was
able to complete Goldmann perimetry.

101
15.3 Conclusions
The current study investigated functional and structural changes in individuals who were
monitored for VGB toxicity using ERG. The study confirmed the hypothesis and demonstrated
that VGB toxicity, as defined by ERG, is associated with visual field reductions and attenuation
of the RNFL. The pattern of RNFL loss (attenuation of the nasal RNFL and the sparing of the
temporal RNFL) is in accordance with the visual field pattern observed with VGB toxicity.
Adults taking VGB are often monitored for visual field loss using either Goldmann perimetry or
the Humphrey Field Analyzer. As suggested by other studies [235, 237-240], OCT would be a
suitable adjunct tool to objectively monitor VGB-induced retinal defects in adults who are
unable to perform perimetry, and in young children. The correlations between ERG diagnosis of
toxicity and visual field reductions, and the correlations between ERG diagnosis of toxicity and
RNFL attenuation support this view.
!

102
16 Future Directions!
Our study was limited by a small sample size. Therefore, further studies are required to confirm
if diagnosis of drug toxicity is indeed associated with visual field loss and attenuation of the
RNFL in a larger population.
Our study also provides preliminary data to support the use of OCT as a biomarker of retinotoxic
changes due to VGB.
ERG recording in young children (< 45 kg) requires sedation; however, general anesthesia is
required for those who are unable to be sedated. There has been rising concern regarding the
neurological and cognitive impact of anesthesia on the developing brain. Anesthesia exposure in
the developing rodent and macaque brains has been shown to induce neuroapoptosis [303].
Researchers followed a cohort of 2868 children in Australia from pre-birth up to ten years of age
and found that those exposed to anesthesia before three years of age experienced deficits in
abstract reasoning, and in receptive and expressive language compared to their counterparts
[304]. This effect was observed even with a single exposure to anesthesia, in contrast to previous
studies revealing cognitive deficits with two or more exposures to anesthesia [305].
Given the risks associated with anesthesia, the variability of the flicker response, artificially-
reduced amplitudes and the length of ERG testing, it is clear that an alternative to ERG
recordings for monitoring VGB toxicity is needed. OCT seems to be an ideal alternative; it is a
rapid, non-invasive procedure that allows for health care practitioners to quantitatively monitor
structural changes associated with VGB toxicity without sedation or anesthesia. RNFL thickness
measurements obtained from SD-OCT are highly repeatable in healthy individuals [306]. OCT
has been used to image children with glaucoma [307], unilateral amblyopia [308],
oculocutaneous albinism [309], and uveitis [310]. OCT may be of particular use since visual
field defects may exist in the presence of a normal fundus exam.
In our study, all participants were over seven years of age. However, most children that are
prescribed VGB for IS are under two years of age. The OCT protocol used in our study, which
requires the participant to sit upright and maintain fixation on a visual target, would not be
feasible for infants. In infants, access to the retina is limited by lack of cooperation and fixation,

103
and increased movement. Thus, to obtain good images in infants, scan quality must be improved
while retaining a short capture time. The hand-held OCT, which has been designed for pediatric
clinical use, may be a sound alternative to ERG for monitoring VGB toxicity. The development
of SD-OCT has vastly reduced motion artifacts and decreased scan time compared to TD-OCT,
making hand-held imaging possible. The hand-held SD-OCT has been successfully used in
imaging the optic nerve, fovea and posterior pole in a pediatric population (age range: 31 weeks
postmenstrual age to 1.5 years) [311]. To gain access to the eye, the examiner may hold the eye
open using two fingers, or by using a lid speculum. Hand-held OCT has also been used to detect
preretinal and intraretinal hemorrhages in Shaken Baby Syndrome [312, 313]. This device has
been used in a pediatric population for monitoring or managing intraocular retinoblastoma [314],
retinopathy of prematurity [315], and ocular albinism [316]. The hand-held OCT can be used on
infants under anesthesia, with the infant in the supine position, or under sedation. OCT can also
be used on a young infant without sedation, which may be more challenging. A sucrose pacifier
can be used to reduce stress during imaging [317]. The ability to image infants and neonates
without anesthesia is a big step forward for pediatric retinal imaging.
The Hospital for Sick Children has a hand-held SD-OCT (Bioptogen Inc., Research Triangle
Park, NC). A study at our centre that includes OCT testing on infants undergoing sedated ERGs
for the monitoring of VGB toxicity will determine if OCT imaging is feasible. Infants with a co-
morbidity of TSC will have to be excluded from the proposed study since the presence of retinal
hamaratomas will affect RNFL thickness. Such a study may also indicate when changes at the
RNFL occur and whether these changes occur before or after changes at the photoreceptor level.
Our current study shows a correlation between VGB toxicity and RNFL thickness, but it is not
known when these changes occur. If attenuation of the RNFL is a long-term change that occurs
months to years after functional damage to the retina, then it would not be a good early
biomarker of toxicity. However, if RNFL changes occur prior to the detection of visual field
reductions, then it could be an excellent predictor of toxicity.
If OCT can detect early clinical biomarkers of visual field loss in VGB therapy, a normative
database for young children needs to be developed. Previous pediatric studies have established
confidence intervals based on small sample sizes. However, a large, normative database of

104
RNFL thickness for children, such as those provided by OCT manufacturers for adults could
greatly improve OCT application in in the pediatric population.
A study similar to the one proposed was attempted at the Children’s National Medical Center in
Washington, DC [318]. The objective of the study was to explore the relationship between
clinical examination under anesthesia, RNFL thickness, and ERG responses. However, on initial
exam, many children presented with abnormal values of RNFL thickness; 18 of 34(53%) eyes
had RNFL thickness values that were either above the 95th percentile or below the 5th percentile
of age-expected norms. This study highlights the importance of controlling for co-morbidities if
OCT is to be used as a tool for monitoring toxicity. As with ERG assessment of toxicity, an
individual would need to have a baseline (pre-drug) RNFL measurement and changes from this
baseline should be monitored on a regular basis. Such serial monitoring would provide better
sensitivity and specificity than measuring absolute differences from a normative database.
Previous trend-based analysis of patients with glaucoma show that progressive thinning of the
RNFL can be monitored effectively [319, 320].
Another area for further investigation includes analyzing the ganglion cell layer at the optic disc,
which can be done using existing segmentation software. Our study found differences in the
nerve fibre layer, which is composed of ganglion cell axons, at the optic disc. Since the ganglion
cell layer consists of ganglion soma, we will be better able to determine if VGB toxicity is
neuronal or axonal. In addition, animal studies show that taurine, an amino acid that is protective
against VGB retinal toxicity, accumulates in the GCL [262]. Also, human post-mortem
examination shows atrophy of ganglion cells in the periphery and loss of nerve fibres in a VGB-
treated adult [200]. By examining the effect of VGB on both the GCL and the RNFL, we will be
able to better understand the mechanism of VGB retinal toxicity.
!

105
References 1. Tellez-Zenteno, J.F., et al., National and regional prevalence of self-reported epilepsy in
Canada. Epilepsia, 2004. 45(12): p. 1623-9. 2. Forsgren, L., et al., The epidemiology of epilepsy in Europe - a systematic review. Eur J
Neurol, 2005. 12(4): p. 245-53. 3. Hopkins, A. and R. Appleton, Epilepsy, the facts. 2nd ed. Oxford medical
publications1996, Oxford ; New York: Oxford University Press. 161 p. 4. Nordli, D.R., Jr., et al., Recognition and classification of seizures in infants. Epilepsia,
1997. 38(5): p. 553-60. 5. Gastaut, H., Clinical and electroencephalographical classification of epileptic seizures.
Epilepsia, 1970. 11(1): p. 102-13. 6. Berg, A.T., et al., Revised terminology and concepts for organization of seizures and
epilepsies: report of the ILAE Commission on Classification and Terminology, 2005-2009. Epilepsia, 2010. 51(4): p. 676-85.
7. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. From the Commission on Classification and Terminology of the International League Against Epilepsy. Epilepsia, 1981. 22(4): p. 489-501.
8. Berg, A.T. and J.J. Millichap, The 2010 revised classification of seizures and epilepsy. Continuum (Minneap Minn), 2013. 19(3 Epilepsy): p. 571-97.
9. Engel, J., Jr., A proposed diagnostic scheme for people with epileptic seizures and with epilepsy: report of the ILAE Task Force on Classification and Terminology. Epilepsia, 2001. 42(6): p. 796-803.
10. Hamer, H.M., et al., Symptomatology of epileptic seizures in the first three years of life. Epilepsia, 1999. 40(7): p. 837-44.
11. Luna, D., O. Dulac, and P. Plouin, Ictal characteristics of cryptogenic partial epilepsies in infancy. Epilepsia, 1989. 30(6): p. 827-32.
12. Chabolla, D.R., Characteristics of the epilepsies. Mayo Clin Proc, 2002. 77(9): p. 981-90.
13. Askalan, R., et al., Prospective preliminary analysis of the development of autism and epilepsy in children with infantile spasms. J Child Neurol, 2003. 18(3): p. 165-70.
14. Blume, W.T., et al., Glossary of descriptive terminology for ictal semiology: report of the ILAE task force on classification and terminology. Epilepsia, 2001. 42(9): p. 1212-8.
15. Alarcon, G., Electroclinical classification of seizures. Introduction to Epilepsy, 2012. 107.
16. West, W.J., On a peculiar form of infantile convulsions. Lancet, 1841. 1: p. 724–725. 17. Kossoff, E.H., Infantile spasms. Neurologist, 2010. 16(2): p. 69-75. 18. Wong, M. and E. Trevathan, Infantile spasms. Pediatr Neurol, 2001. 24(2): p. 89-98. 19. Lux, A.L. and J.P. Osborne, A proposal for case definitions and outcome measures in
studies of infantile spasms and West syndrome: consensus statement of the West Delphi group. Epilepsia, 2004. 45(11): p. 1416-28.
20. Hrachovy, R.A. and J.D. Frost, Jr., Infantile epileptic encephalopathy with hypsarrhythmia (infantile spasms/West syndrome). J Clin Neurophysiol, 2003. 20(6): p. 408-25.
21. Hrachovy, R.A. and J.D. Frost, Jr., Infantile spasms. Handb Clin Neurol, 2013. 111: p. 611-8.

106
22. Cowan, L.D. and L.S. Hudson, The epidemiology and natural history of infantile spasms. J Child Neurol, 1991. 6(4): p. 355-64.
23. Partikian, A. and W.G. Mitchell, Neurodevelopmental and epilepsy outcomes in a North American cohort of patients with infantile spasms. J Child Neurol, 2010. 25(4): p. 423-8.
24. O'Callaghan, F.J., et al., The effect of lead time to treatment and of age of onset on developmental outcome at 4 years in infantile spasms: evidence from the United Kingdom Infantile Spasms Study. Epilepsia, 2011. 52(7): p. 1359-64.
25. Snead, O.C., 3rd, J.W. Benton, and G.J. Myers, ACTH and prednisone in childhood seizure disorders. Neurology, 1983. 33(8): p. 966-70.
26. Trevathan, E., C.C. Murphy, and M. Yeargin-Allsopp, The descriptive epidemiology of infantile spasms among Atlanta children. Epilepsia, 1999. 40(6): p. 748-51.
27. Riikonen, R., Long-term outcome of patients with West syndrome. Brain Dev, 2001. 23(7): p. 683-7.
28. Lombroso, C.T., A prospective study of infantile spasms: clinical and therapeutic correlations. Epilepsia, 1983. 24(2): p. 135-58.
29. Ohtahara, S., Y. Yamatogi, and Y. Ohtsuka, Prognosis of the Lennox syndrome-long-term clinical and electroencephalographic follow-up study, especially with special reference to relationship with the West syndrome. Folia Psychiatr Neurol Jpn, 1976. 30(3): p. 275-87.
30. Donat, J.F. and F.S. Wright, Seizures in series: similarities between seizures of the west and Lennox-Gastaut syndromes. Epilepsia, 1991. 32(4): p. 504-9.
31. Kellaway, P., et al., Precise characterization and quantification of infantile spasms. Ann Neurol, 1979. 6(3): p. 214-8.
32. Gibbs, F.A. and E.L. Gibbs, Atlas of electroencephalography: Volume 2, Epilepsy1952, Cambridge (MA): Addison-Wesley.
33. Hrachovy, R.A., J.D. Frost, Jr., and P. Kellaway, Hypsarrhythmia: variations on the theme. Epilepsia, 1984. 25(3): p. 317-25.
34. Paciorkowski, A.R., L.L. Thio, and W.B. Dobyns, Genetic and biologic classification of infantile spasms. Pediatr Neurol, 2011. 45(6): p. 355-67.
35. Shields, W.D., Infantile spasms: little seizures, BIG consequences. Epilepsy Curr, 2006. 6(3): p. 63-9.
36. Sorel, L. and A. Dusaucy-Bauloye, [Findings in 21 cases of Gibbs' hypsarrhythmia; spectacular effectiveness of ACTH]. Acta Neurol Psychiatr Belg, 1958. 58(2): p. 130-41.
37. Go, C.Y., et al., Evidence-based guideline update: medical treatment of infantile spasms. Report of the Guideline Development Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology, 2012. 78(24): p. 1974-80.
38. Lux, A.L., et al., The United Kingdom Infantile Spasms Study (UKISS) comparing hormone treatment with vigabatrin on developmental and epilepsy outcomes to age 14 months: a multicentre randomised trial. Lancet Neurol, 2005. 4(11): p. 712-7.
39. Riikonen, R. and M. Donner, ACTH therapy in infantile spasms: side effects. Arch Dis Child, 1980. 55(9): p. 664-72.
40. Chiron, C., et al., Randomized trial comparing vigabatrin and hydrocortisone in infantile spasms due to tuberous sclerosis. Epilepsy Res, 1997. 26(2): p. 389-95.
41. Hancock, E. and J.P. Osborne, Vigabatrin in the treatment of infantile spasms in tuberous sclerosis: literature review. J Child Neurol, 1999. 14(2): p. 71-4.

107
42. Hancock, E.C., J.P. Osborne, and S.W. Edwards, Treatment of infantile spasms. Cochrane Database Syst Rev, 2013. 6: p. CD001770.
43. Baylor, D.A., M.G. Fuortes, and P.M. O'Bryan, Receptive fields of cones in the retina of the turtle. J Physiol, 1971. 214(2): p. 265-94.
44. Kolb, H., K.A. Linberg, and S.K. Fisher, Neurons of the human retina: a Golgi study. J Comp Neurol, 1992. 318(2): p. 147-87.
45. Snellman, J. and S. Nawy, Regulation of the retinal bipolar cell mGluR6 pathway by calcineurin. J Neurophysiol, 2002. 88(3): p. 1088-96.
46. Pang, J.J., et al., Direct rod input to cone BCs and direct cone input to rod BCs challenge the traditional view of mammalian BC circuitry. Proc Natl Acad Sci U S A, 2010. 107(1): p. 395-400.
47. Garcia, M. and E. Vecino, Role of Muller glia in neuroprotection and regeneration in the retina. Histol Histopathol, 2003. 18(4): p. 1205-18.
48. Bringmann, A., et al., GABA and Glutamate Uptake and Metabolism in Retinal Glial (Muller) Cells. Front Endocrinol (Lausanne), 2013. 4: p. 48.
49. C, S., Ueber die oxydation des piperidins. Ber Dtsch Chem Ges 1883. 16: p. 643–9. 50. Roberts, E. and S. Frankel, gamma-Aminobutyric acid in brain: its formation from
glutamic acid. J Biol Chem, 1950. 187(1): p. 55-63. 51. Roberts, E., et al., GABA in nervous system function. Kroc Foundation series v 51976,
New York: Raven Press. xv, 554 p. 52. Huang, Z., Drug discovery research : new frontiers in the post-genomic era2007,
Hoboken, N.J.: Wiley-Interscience. xix, 521 p., 16 p. of plates. 53. Erlander, M.G., et al., Two genes encode distinct glutamate decarboxylases. Neuron,
1991. 7(1): p. 91-100. 54. Pinal, C.S. and A.J. Tobin, Uniqueness and redundancy in GABA production. Perspect
Dev Neurobiol, 1998. 5(2-3): p. 109-18. 55. Enna, S.J., GABA. Advances in pharmacology,2006, San Diego: Academic
Press/Elsevier. xv, 344 p., 8 p. of plates. 56. Michels, G. and S.J. Moss, GABAA receptors: properties and trafficking. Crit Rev
Biochem Mol Biol, 2007. 42(1): p. 3-14. 57. Rudolph, U. and H. Mohler, GABA-based therapeutic approaches: GABAA receptor
subtype functions. Curr Opin Pharmacol, 2006. 6(1): p. 18-23. 58. Briggs, S.W. and A.S. Galanopoulou, Altered GABA signaling in early life epilepsies.
Neural Plast, 2011. 2011: p. 527605. 59. Benarroch, E.E., GABAB receptors: structure, functions, and clinical implications.
Neurology, 2012. 78(8): p. 578-84. 60. Pinard, A., R. Seddik, and B. Bettler, GABAB receptors: physiological functions and
mechanisms of diversity. Adv Pharmacol, 2010. 58: p. 231-55. 61. Connelly, W.M., et al., GABAB Receptors Regulate Extrasynaptic GABAA Receptors. J
Neurosci, 2013. 33(9): p. 3780-5. 62. Tao, W., et al., Postsynaptic GABAB receptors enhance extrasynaptic GABAA receptor
function in dentate gyrus granule cells. J Neurosci, 2013. 33(9): p. 3738-43. 63. Bowery, N.G., GABAB receptor: a site of therapeutic benefit. Curr Opin Pharmacol,
2006. 6(1): p. 37-43. 64. Johnston, G.A., GABAc receptors: relatively simple transmitter -gated ion channels?
Trends Pharmacol Sci, 1996. 17(9): p. 319-23.

108
65. Qian, H. and H. Ripps, Focus on molecules: the GABAC receptor. Exp Eye Res, 2009. 88(6): p. 1002-3.
66. Encyclopedia of the eye. 1st ed2010, Boston, MA: Elsevier. 67. Feigenspan, A. and J. Bormann, GABA-gated Cl- channels in the rat retina. Prog Retin
Eye Res, 1998. 17(1): p. 99-126. 68. Qian, H., GABAC Receptors in the Vertebrate Retina, in Webvision: The Organization of
the Retina and Visual System, H. Kolb, E. Fernandez, and R. Nelson, Editors. 1995: Salt Lake City (UT).
69. Eggers, E.D. and P.D. Lukasiewicz, GABA(A), GABA(C) and glycine receptor-mediated inhibition differentially affects light-evoked signalling from mouse retinal rod bipolar cells. J Physiol, 2006. 572(Pt 1): p. 215-25.
70. McCall, M.A., et al., Elimination of the rho1 subunit abolishes GABA(C) receptor expression and alters visual processing in the mouse retina. J Neurosci, 2002. 22(10): p. 4163-74.
71. Lukasiewicz, P.D., et al., GABAC receptor-mediated inhibition in the retina. Vision Res, 2004. 44(28): p. 3289-96.
72. Lam, D.M., Neurotransmitters in the vertebrate retina. Invest Ophthalmol Vis Sci, 1997. 38(3): p. 553-6.
73. Slaughter, M.M. and Z.H. Pan, The physiology of GABAB receptors in the vertebrate retina. Prog Brain Res, 1992. 90: p. 47-60.
74. Qian, H. and J.E. Dowling, Novel GABA responses from rod-driven retinal horizontal cells. Nature, 1993. 361(6408): p. 162-4.
75. Dong, C.J. and F.S. Werblin, Zinc downmodulates thf GABAc receptor current in cone horizontal cells acutely isolated from the catfish retina. J Neurophysiol, 1995. 73(2): p. 916-9.
76. Zhang, J. and M.M. Slaughter, Preferential suppression of the ON pathway by GABAC receptors in the amphibian retina. J Neurophysiol, 1995. 74(4): p. 1583-92.
77. Picaud, S., et al., GABAA and GABAC receptors in adult porcine cones: evidence from a photoreceptor-glia co-culture model. J Physiol, 1998. 513 ( Pt 1): p. 33-42.
78. Blanco, R., C.F. Vaquero, and P. de la Villa, The effects of GABA and glycine on horizontal cells of the rabbit retina. Vision Res, 1996. 36(24): p. 3987-95.
79. Grunert, U., Distribution of GABAA and glycine receptors in the mammalian retina. Clin Exp Pharmacol Physiol, 1999. 26(11): p. 941-4.
80. Wassle, H., et al., Glycine and GABA receptors in the mammalian retina. Vision Res, 1998. 38(10): p. 1411-30.
81. Lukasiewicz, P.D. and C.R. Shields, A diversity of GABA receptors in the retina. Semin Cell Dev Biol, 1998. 9(3): p. 293-9.
82. Varela, C., et al., Depolarizing effect of GABA in horizontal cells of the rabbit retina. Neurosci Res, 2005. 53(3): p. 257-64.
83. Maric, D., et al., GABA expression dominates neuronal lineage progression in the embryonic rat neocortex and facilitates neurite outgrowth via GABA(A) autoreceptor/Cl- channels. J Neurosci, 2001. 21(7): p. 2343-60.
84. Barker, J.L., et al., GABAergic cells and signals in CNS development. Perspect Dev Neurobiol, 1998. 5(2-3): p. 305-22.
85. Ben-Ari, Y., et al., Giant synaptic potentials in immature rat CA3 hippocampal neurones. J Physiol, 1989. 416: p. 303-25.

109
86. Chen, G., P.Q. Trombley, and A.N. van den Pol, Excitatory actions of GABA in developing rat hypothalamic neurones. J Physiol, 1996. 494 ( Pt 2): p. 451-64.
87. Plotkin, M.D., et al., Expression of the Na-K-2Cl cotransporter is developmentally regulated in postnatal rat brains: a possible mechanism underlying GABA's excitatory role in immature brain. J Neurobiol, 1997. 33(6): p. 781-95.
88. Delpy, A., et al., NKCC1 cotransporter inactivation underlies embryonic development of chloride-mediated inhibition in mouse spinal motoneuron. J Physiol, 2008. 586(4): p. 1059-75.
89. Rivera, C., et al., The K+/Cl- co-transporter KCC2 renders GABA hyperpolarizing during neuronal maturation. Nature, 1999. 397(6716): p. 251-5.
90. Trigo, F.F., A. Marty, and B.M. Stell, Axonal GABAA receptors. Eur J Neurosci, 2008. 28(5): p. 841-8.
91. Price, G.D. and L.O. Trussell, Estimate of the chloride concentration in a central glutamatergic terminal: a gramicidin perforated-patch study on the calyx of Held. J Neurosci, 2006. 26(44): p. 11432-6.
92. Pugh, J.R. and C.E. Jahr, Axonal GABAA receptors increase cerebellar granule cell excitability and synaptic activity. J Neurosci, 2011. 31(2): p. 565-74.
93. Gulyas, A.I., et al., The KCl cotransporter, KCC2, is highly expressed in the vicinity of excitatory synapses in the rat hippocampus. Eur J Neurosci, 2001. 13(12): p. 2205-17.
94. Chavas, J. and A. Marty, Coexistence of excitatory and inhibitory GABA synapses in the cerebellar interneuron network. J Neurosci, 2003. 23(6): p. 2019-31.
95. Gulacsi, A., et al., Cell type-specific differences in chloride-regulatory mechanisms and GABA(A) receptor-mediated inhibition in rat substantia nigra. J Neurosci, 2003. 23(23): p. 8237-46.
96. Woodin, M.A., K. Ganguly, and M.M. Poo, Coincident pre- and postsynaptic activity modifies GABAergic synapses by postsynaptic changes in Cl- transporter activity. Neuron, 2003. 39(5): p. 807-20.
97. Gulledge, A.T. and G.J. Stuart, Excitatory actions of GABA in the cortex. Neuron, 2003. 37(2): p. 299-309.
98. Vardi, N., et al., Evidence that different cation chloride cotransporters in retinal neurons allow opposite responses to GABA. J Neurosci, 2000. 20(20): p. 7657-63.
99. Wong, C.G., T. Bottiglieri, and O.C. Snead, 3rd, GABA, gamma-hydroxybutyric acid, and neurological disease. Ann Neurol, 2003. 54 Suppl 6: p. S3-12.
100. Horton, R.W., S.A. Prestwich, and B.S. Meldrum, gamma-Aminobutyric acid and benzodiazepine binding sites in audiogenic seizure-susceptible mice. J Neurochem, 1982. 39(3): p. 864-70.
101. Roberts, R.C., C.E. Ribak, and W.H. Oertel, Increased numbers of GABAergic neurons occur in the inferior colliculus of an audiogenic model of genetic epilepsy. Brain Res, 1985. 361(1-2): p. 324-38.
102. Peterson, G.M., C.E. Ribak, and W.H. Oertel, A regional increase in the number of hippocampal GABAergic neurons and terminals in the seizure-sensitive gerbil. Brain Res, 1985. 340(2): p. 384-9.
103. Kang, J.Q., et al., Slow degradation and aggregation in vitro of mutant GABAA receptor gamma2(Q351X) subunits associated with epilepsy. J Neurosci, 2010. 30(41): p. 13895-905.

110
104. Chiu, C., et al., Developmental impact of a familial GABAA receptor epilepsy mutation. Ann Neurol, 2008. 64(3): p. 284-93.
105. Vergnes, M., et al., Opposite effects of GABAB receptor antagonists on absences and convulsive seizures. Eur J Pharmacol, 1997. 332(3): p. 245-55.
106. Meldrum, B.S., The role of glutamate in epilepsy and other CNS disorders. Neurology, 1994. 44(11 Suppl 8): p. S14-23.
107. Czapinski, P., B. Blaszczyk, and S.J. Czuczwar, Mechanisms of action of antiepileptic drugs. Curr Top Med Chem, 2005. 5(1): p. 3-14.
108. Angehagen, M., et al., Novel mechanisms of action of three antiepileptic drugs, vigabatrin, tiagabine, and topiramate. Neurochem Res, 2003. 28(2): p. 333-40.
109. Krauss, G.L., et al., A controlled study comparing visual function in patients treated with vigabatrin and tiagabine. J Neurol Neurosurg Psychiatry, 2003. 74(3): p. 339-43.
110. Sills, G.J., et al., Visual field constriction: accumulation of vigabatrin but not tiagabine in the retina. Neurology, 2001. 57(2): p. 196-200.
111. Stein, V. and R.A. Nicoll, GABA generates excitement. Neuron, 2003. 37(3): p. 375-8. 112. Painter, M.J., et al., Phenobarbital compared with phenytoin for the treatment of neonatal
seizures. N Engl J Med, 1999. 341(7): p. 485-9. 113. Kahle, K.T. and K.J. Staley, The bumetanide-sensitive Na-K-2Cl cotransporter NKCC1
as a potential target of a novel mechanism-based treatment strategy for neonatal seizures. Neurosurg Focus, 2008. 25(3): p. E22.
114. Cohen, I., et al., On the origin of interictal activity in human temporal lobe epilepsy in vitro. Science, 2002. 298(5597): p. 1418-21.
115. Coull, J.A., et al., Trans-synaptic shift in anion gradient in spinal lamina I neurons as a mechanism of neuropathic pain. Nature, 2003. 424(6951): p. 938-42.
116. Woo, N.S., et al., Hyperexcitability and epilepsy associated with disruption of the mouse neuronal-specific K-Cl cotransporter gene. Hippocampus, 2002. 12(2): p. 258-68.
117. Tornberg, J., et al., Behavioural phenotypes of hypomorphic KCC2-deficient mice. Eur J Neurosci, 2005. 21(5): p. 1327-37.
118. Huberfeld, G., et al., Perturbed chloride homeostasis and GABAergic signaling in human temporal lobe epilepsy. J Neurosci, 2007. 27(37): p. 9866-73.
119. Munoz, A., et al., Cation-chloride cotransporters and GABA-ergic innervation in the human epileptic hippocampus. Epilepsia, 2007. 48(4): p. 663-73.
120. Dzhala, V.I., et al., NKCC1 transporter facilitates seizures in the developing brain. Nat Med, 2005. 11(11): p. 1205-13.
121. Stafstrom, C.E., Neonatal seizures: is a novel, mechanism-based treatment finally on the horizon? Epilepsy Curr, 2006. 6(4): p. 130-2.
122. Eftekhari, S., et al., Bumetanide reduces seizure frequency in patients with temporal lobe epilepsy. Epilepsia, 2013. 54(1): p. e9-12.
123. Kahle, K.T., et al., Decreased seizure activity in a human neonate treated with bumetanide, an inhibitor of the Na(+)-K(+)-2Cl(-) cotransporter NKCC1. J Child Neurol, 2009. 24(5): p. 572-6.
124. Wang, D.D. and A.R. Kriegstein, Blocking early GABA depolarization with bumetanide results in permanent alterations in cortical circuits and sensorimotor gating deficits. Cereb Cortex, 2011. 21(3): p. 574-87.

111
125. Jung, M.J., et al., gamma-Vinyl GABA (4-amino-hex-5-enoic acid), a new selective irreversible inhibitor of GABA-T: effects on brain GABA metabolism in mice. J Neurochem, 1977. 29(5): p. 797-802.
126. Schechter, P.J. and Y. Tranier, Effect of elevated brain GABA concentrations on the actions of bicuculline and picrotoxin in mice. Psychopharmacology (Berl), 1977. 54(2): p. 145-8.
127. Lippert, B., et al., 4-amino-hex-5-enoic acid, a selective catalytic inhibitor of 4-aminobutyric-acid aminotransferase in mammalian brain. Eur J Biochem, 1977. 74(3): p. 441-5.
128. Gibson, J.P., et al., Chronic toxicity studies with vigabatrin, a GABA-transaminase inhibitor. Toxicol Pathol, 1990. 18(2): p. 225-38.
129. Lerner, J.T., N. Salamon, and R. Sankar, Clinical profile of vigabatrin as monotherapy for treatment of infantile spasms. Neuropsychiatr Dis Treat, 2010. 6: p. 731-40.
130. Shields, W.D. and J.M. Pellock, Vigabatrin 35 years later - from mechanism of action to benefit-risk considerations. Acta Neurol Scand Suppl, 2011(192): p. 1-4.
131. Appleton, R.E., et al., Randomised, placebo-controlled study of vigabatrin as first-line treatment of infantile spasms. Epilepsia, 1999. 40(11): p. 1627-33.
132. Luna, D., et al., Vigabatrin in the treatment of childhood epilepsies: a single-blind placebo-controlled study. Epilepsia, 1989. 30(4): p. 430-7.
133. Chiron, C., et al., Therapeutic trial of vigabatrin in refractory infantile spasms. J Child Neurol, 1991. Suppl 2: p. S52-9.
134. Livingston, J.H., et al., Vigabatrin in the treatment of epilepsy in children. Br J Clin Pharmacol, 1989. 27 Suppl 1: p. 109S-112S.
135. Elterman, R.D., et al., Randomized trial of vigabatrin in patients with infantile spasms. Neurology, 2001. 57(8): p. 1416-21.
136. Mackay, M.T., et al., Practice parameter: medical treatment of infantile spasms: report of the American Academy of Neurology and the Child Neurology Society. Neurology, 2004. 62(10): p. 1668-81.
137. Guideline for prescribing vigabatrin in children has been revised. Vigabatrin Paediatric Advisory Group. BMJ, 2000. 320(7246): p. 1404-5.
138. Rey, E., et al., Pharmacokinetics of the individual enantiomers of vigabatrin (gamma-vinyl GABA) in epileptic children. Br J Clin Pharmacol, 1990. 30(2): p. 253-7.
139. Rey, E., G. Pons, and G. Olive, Vigabatrin. Clinical pharmacokinetics. Clin Pharmacokinet, 1992. 23(4): p. 267-78.
140. Haegele, K.D. and P.J. Schechter, Kinetics of the enantiomers of vigabatrin after an oral dose of the racemate or the active S-enantiomer. Clin Pharmacol Ther, 1986. 40(5): p. 581-6.
141. Menachem, E.B., et al., Effects of single doses of vigabatrin on CSF concentrations of GABA, homocarnosine, homovanillic acid and 5-hydroxyindoleacetic acid in patients with complex partial epilepsy. Epilepsy Res, 1988. 2(2): p. 96-101.
142. Grove, J., et al., Increased gamma-aminobutyric acid (GABA), homocarnosine and beta-alanine in cerebrospinal fluid of patients treated with gamma-vinyl GABA (4-amino-hex-5-enoic acid). Life Sci, 1981. 28(21): p. 2431-9.
143. Bohlen, P., S. Huot, and M.G. Palfreyman, The relationship between GABA concentrations in brain and cerebrospinal fluid. Brain Res, 1979. 167(2): p. 297-305.

112
144. Mattson, R.H., et al., Vigabatrin: effects on human brain GABA levels by nuclear magnetic resonance spectroscopy. Epilepsia, 1994. 35 Suppl 5: p. S29-32.
145. Leach, J.P., et al., Effects of tiagabine and vigabatrin on GABA uptake into primary cultures of rat cortical astrocytes. Seizure, 1996. 5(3): p. 229-34.
146. Ben-Menachem, E., Mechanism of action of vigabatrin: correcting misperceptions. Acta Neurol Scand Suppl, 2011(192): p. 5-15.
147. Petroff, O.A. and D.L. Rothman, Measuring human brain GABA in vivo: effects of GABA-transaminase inhibition with vigabatrin. Mol Neurobiol, 1998. 16(1): p. 97-121.
148. Petroff, O.A., et al., Human brain gamma-aminobutyric acid levels and seizure control following initiation of vigabatrin therapy. J Neurochem, 1996. 67(6): p. 2399-404.
149. Sills, G.J., et al., Vigabatrin, but not gabapentin or topiramate, produces concentration-related effects on enzymes and intermediates of the GABA shunt in rat brain and retina. Epilepsia, 2003. 44(7): p. 886-92.
150. Zhang, B., et al., Vigabatrin inhibits seizures and mTOR pathway activation in a mouse model of tuberous sclerosis complex. PLoS One, 2013. 8(2): p. e57445.
151. Gidal, B.E., et al., Vigabatrin: a novel therapy for seizure disorders. Ann Pharmacother, 1999. 33(12): p. 1277-86.
152. Brodie, J.D., et al., Randomized, double-blind, placebo-controlled trial of vigabatrin for the treatment of cocaine dependence in Mexican parolees. Am J Psychiatry, 2009. 166(11): p. 1269-77.
153. Fechtner, R.D., et al., Short-term treatment of cocaine and/or methamphetamine abuse with vigabatrin: ocular safety pilot results. Arch Ophthalmol, 2006. 124(9): p. 1257-62.
154. Vigevano, F. and M.R. Cilio, Vigabatrin versus ACTH as first-line treatment for infantile spasms: a randomized, prospective study. Epilepsia, 1997. 38(12): p. 1270-4.
155. Lux, A.L., et al., The United Kingdom Infantile Spasms Study comparing vigabatrin with prednisolone or tetracosactide at 14 days: a multicentre, randomised controlled trial. Lancet, 2004. 364(9447): p. 1773-8.
156. Elterman, R.D., et al., Vigabatrin for the treatment of infantile spasms: final report of a randomized trial. J Child Neurol, 2010. 25(11): p. 1340-7.
157. Darke, K., et al., Developmental and epilepsy outcomes at age 4 years in the UKISS trial comparing hormonal treatments to vigabatrin for infantile spasms: a multi-centre randomised trial. Arch Dis Child, 2010. 95(5): p. 382-6.
158. Lux, A.L., Latest American and European updates on infantile spasms. Curr Neurol Neurosci Rep, 2013. 13(3): p. 334.
159. Aicardi, J., et al., Vigabatrin as initial therapy for infantile spasms: a European retrospective survey. Sabril IS Investigator and Peer Review Groups. Epilepsia, 1996. 37(7): p. 638-42.
160. Mauguiere, F., et al., No effect of long-term vigabatrin treatment on central nervous system conduction in patients with refractory epilepsy: results of a multicenter study of somatosensory and visual evoked potentials. PMS Study Multicenter Group. Epilepsia, 1997. 38(3): p. 301-8.
161. Sivenius, J., et al., Vigabatrin (gamma-vinyl-GABA): neuropathologic evaluation in five patients. Epilepsia, 1993. 34(1): p. 193-6.
162. Milh, M., et al., Transient brain magnetic resonance imaging hyperintensity in basal ganglia and brain stem of epileptic infants treated with vigabatrin. J Child Neurol, 2009. 24(3): p. 305-15.

113
163. Pearl, P.L., et al., Cerebral MRI abnormalities associated with vigabatrin therapy. Epilepsia, 2009. 50(2): p. 184-94.
164. Fong, C.Y., et al., An investigation into the relationship between vigabatrin, movement disorders, and brain magnetic resonance imaging abnormalities in children with infantile spasms. Dev Med Child Neurol, 2013. 55(9): p. 862-7.
165. Eke, T., J.F. Talbot, and M.C. Lawden, Severe persistent visual field constriction associated with vigabatrin. BMJ, 1997. 314(7075): p. 180-1.
166. Wilson, E.A. and M.J. Brodie, Severe persistent visual field constriction associated with vigabatrin. Chronic refractory epilepsy may have role in causing these unusual lesions. BMJ, 1997. 314(7095): p. 1693.
167. Wong, I.C., G.E. Mawer, and J.W. Sander, Severe persistent visual field constriction associated with vigabatrin. Reaction might be dose dependent. BMJ, 1997. 314(7095): p. 1693-4.
168. Blackwell, N., J. Hayllar, and G. Kelly, Severe persistent visual field constriction associated with vigabatrin. Patients taking vigabatrin should have regular visual field testing. BMJ, 1997. 314(7095): p. 1694.
169. Lawden, M.C., et al., Visual field defects associated with vigabatrin therapy. J Neurol Neurosurg Psychiatry, 1999. 67(6): p. 716-22.
170. Kalviainen, R., et al., Vigabatrin, a gabaergic antiepileptic drug, causes concentric visual field defects. Neurology, 1999. 53(5): p. 922-6.
171. Vanhatalo, S., L. Paakkonen, and I. Nousiainen, Visual field constriction in children treated with vigabatrin. Neurology, 1999. 52(8): p. 1713-4.
172. Wohlrab, G., et al., Visual field constriction is not limited to children treated with vigabatrin. Neuropediatrics, 1999. 30(3): p. 130-2.
173. Vanhatalo, S., et al., Visual field constriction in 91 Finnish children treated with vigabatrin. Epilepsia, 2002. 43(7): p. 748-56.
174. Iannetti, P., et al., Visual field constriction in children with epilepsy on vigabatrin treatment. Pediatrics, 2000. 106(4): p. 838-42.
175. Banin, E., et al., Retinal function abnormalities in patients treated with vigabatrin. Arch Ophthalmol, 2003. 121(6): p. 811-6.
176. Wild, J.M., et al., Vigabatrin and epilepsy: lessons learned. Epilepsia, 2007. 48(7): p. 1318-27.
177. Krauss, G.L., M.A. Johnson, and N.R. Miller, Vigabatrin-associated retinal cone system dysfunction: electroretinogram and ophthalmologic findings. Neurology, 1998. 50(3): p. 614-8.
178. Daneshvar, H., et al., Symptomatic and asymptomatic visual loss in patients taking vigabatrin. Ophthalmology, 1999. 106(9): p. 1792-8.
179. Miller, N.R., et al., Visual dysfunction in patients receiving vigabatrin: clinical and electrophysiologic findings. Neurology, 1999. 53(9): p. 2082-7.
180. Sergott, R.C., et al., Vigabatrin-induced peripheral visual field defects in patients with refractory partial epilepsy. Epilepsy Res, 2010. 92(2-3): p. 170-6.
181. Wild, J.M., et al., Characteristics of a unique visual field defect attributed to vigabatrin. Epilepsia, 1999. 40(12): p. 1784-94.
182. Arndt, C.F., et al., Outer retinal dysfunction in patients treated with vigabatrin. Neurology, 1999. 52(6): p. 1201-5.

114
183. Newman, W.D., K. Tocher, and J.F. Acheson, Vigabatrin associated visual field loss: a clinical audit to study prevalence, drug history and effects of drug withdrawal. Eye (Lond), 2002. 16(5): p. 567-71.
184. van der Torren, K., H.S. Graniewski-Wijnands, and B.C. Polak, Visual field and electrophysiological abnormalities due to vigabatrin. Doc Ophthalmol, 2002. 104(2): p. 181-8.
185. Jensen, H., et al., Vigabatrin and retinal changes. Doc Ophthalmol, 2002. 104(2): p. 171-80.
186. Midelfart, A., E. Midelfart, and E. Brodtkorb, Visual field defects in patients taking vigabatrin. Acta Ophthalmol Scand, 2000. 78(5): p. 580-4.
187. Maguire, M.J., et al., Prevalence of visual field loss following exposure to vigabatrin therapy: a systematic review. Epilepsia, 2010. 51(12): p. 2423-31.
188. Gaily, E., H. Jonsson, and M. Lappi, Visual fields at school-age in children treated with vigabatrin in infancy. Epilepsia, 2009. 50(2): p. 206-16.
189. Wohlrab, G., et al., Vigabatrin therapy in infantile spasms: solving one problem and inducing another? Epilepsia, 2009. 50(8): p. 2006-8.
190. Werth, R. and G. Schadler, Visual field loss in young children and mentally handicapped adolescents receiving vigabatrin. Invest Ophthalmol Vis Sci, 2006. 47(7): p. 3028-35.
191. Agrawal, S., et al., Visual fields in young children treated with vigabatrin. Optom Vis Sci, 2009. 86(6): p. 767-73.
192. Gross-Tsur, V., et al., Visual impairment in children with epilepsy treated with vigabatrin. Ann Neurol, 2000. 48(1): p. 60-4.
193. Pelosse, B., et al., [Study of visual field and vigabatrin treatment in children]. J Fr Ophtalmol, 2001. 24(10): p. 1075-80.
194. Spencer, E.L. and G.F. Harding, Examining visual field defects in the paediatric population exposed to vigabatrin. Doc Ophthalmol, 2003. 107(3): p. 281-7.
195. Pojda-Wilczek, D., et al., [The function of eye and vision system in children and youth treated with vigabatrin--our own experiences]. Klin Oczna, 2005. 107(10-12): p. 654-7.
196. Ascaso, F.J., et al., Visual field defects in pediatric patients on vigabatrin monotherapy. Doc Ophthalmol, 2003. 107(2): p. 127-30.
197. Russell-Eggitt, I.M., et al., Vigabatrin-associated visual field defects in children. Eye (Lond), 2000. 14 ( Pt 3A): p. 334-9.
198. Buncic, J.R., et al., Characteristic retinal atrophy with secondary "inverse" optic atrophy identifies vigabatrin toxicity in children. Ophthalmology, 2004. 111(10): p. 1935-42.
199. Frisen, L. and K. Malmgren, Characterization of vigabatrin-associated optic atrophy. Acta Ophthalmol Scand, 2003. 81(5): p. 466-73.
200. Ravindran, J., et al., Visual field loss associated with vigabatrin: pathological correlations. J Neurol Neurosurg Psychiatry, 2001. 70(6): p. 787-9.
201. Nousiaine n, I., R. Kalviainen, and M. Mantyjarvi, Color vision in epilepsy patients treated with vigabatrin or carbamazepine monotherapy. Ophthalmology, 2000. 107(5): p. 884-8.
202. Nousiainen, I., R. Kalviainen, and M. Mantyjarvi, Contrast and glare sensitivity in epilepsy patients treated with vigabatrin or carbamazepine monotherapy compared with healthy volunteers. Br J Ophthalmol, 2000. 84(6): p. 622-5.

115
203. Butler, W.H., G.P. Ford, and J.W. Newberne, A study of the effects of vigabatrin on the central nervous system and retina of Sprague Dawley and Lister-Hooded rats. Toxicol Pathol, 1987. 15(2): p. 143-8.
204. Duboc, A., et al., Vigabatrin, the GABA-transaminase inhibitor, damages cone photoreceptors in rats. Ann Neurol, 2004. 55(5): p. 695-705.
205. Wang, Q.P., et al., Treatment of epilepsy: the GABA-transaminase inhibitor, vigabatrin, induces neuronal plasticity in the mouse retina. Eur J Neurosci, 2008. 27(8): p. 2177-87.
206. Neal, M.J., et al., Immunocytochemical evidence that vigabatrin in rats causes GABA accumulation in glial cells of the retina. Neurosci Lett, 1989. 98(1): p. 29-32.
207. Ponjavic, V., et al., Alterations in electroretinograms and retinal morphology in rabbits treated with vigabatrin. Doc Ophthalmol, 2004. 108(2): p. 125-33.
208. Marmor, M.F., et al., ISCEV Standard for full-field clinical electroretinography (2008 update). Doc Ophthalmol, 2009. 118(1): p. 69-77.
209. Dong, C.J., P. Agey, and W.A. Hare, Origins of the electroretinogram oscillatory potentials in the rabbit retina. Vis Neurosci, 2004. 21(4): p. 533-43.
210. Harding, G.F., et al., Separating the retinal electrophysiologic effects of vigabatrin: treatment versus field loss. Neurology, 2000. 55(3): p. 347-52.
211. Graniewski-Wijnands, H.S. and K. van der Torren, Electro-ophthalmological recovery after withdrawal from vigabatrin. Doc Ophthalmol, 2002. 104(2): p. 189-94.
212. Johnson, M.A., et al., Visual function loss from vigabatrin: effect of stopping the drug. Neurology, 2000. 55(1): p. 40-5.
213. Westall, C.A., et al., Changes in the electroretinogram resulting from discontinuation of vigabatrin in children. Doc Ophthalmol, 2003. 107(3): p. 299-309.
214. Gottlob, I., L. Wundsch, and F.K. Tuppy, The rabbit electroretinogram: effect of GABA and its antagonists. Vision Res, 1988. 28(2): p. 203-10.
215. Parisi, P., et al., Scotopic threshold response changes after vigabatrin therapy in a child without visual field defects: a new electroretinographic marker of early damage? Neurobiol Dis, 2004. 15(3): p. 573-9.
216. Morong, S., et al., Longitudinal changes in photopic OPs occurring with vigabatrin treatment. Doc Ophthalmol, 2003. 107(3): p. 289-97.
217. Comaish, I.F., et al., The effects of vigabatrin on electrophysiology and visual fields in epileptics: a controlled study with a discussion of possible mechanisms. Doc Ophthalmol, 2002. 104(2): p. 195-212.
218. Kjellstrom, U., S. Andreasson, and V. Ponjavic, Electrophysiological evaluation of retinal function in children receiving vigabatrin medication. J Pediatr Ophthalmol Strabismus, 2011. 48(6): p. 357-65.
219. Moskowitz, A., et al., Electroretinographic (ERG) responses in pediatric patients using vigabatrin. Doc Ophthalmol, 2012. 124(3): p. 197-209.
220. Besch, D., et al., Visual field constriction and electrophysiological changes associated with vigabatrin. Doc Ophthalmol, 2002. 104(2): p. 151-70.
221. Ponjavic, V. and S. Andreasson, Multifocal ERG and full-field ERG in patients on long-term vigabatrin medication. Doc Ophthalmol, 2001. 102(1): p. 63-72.
222. Bearse, M.A., Jr. and E.E. Sutter, Imaging localized retinal dysfunction with the multifocal electroretinogram. J Opt Soc Am A Opt Image Sci Vis, 1996. 13(3): p. 634-40.

116
223. Hood, D.C., Assessing retinal function with the multifocal technique. Prog Retin Eye Res, 2000. 19(5): p. 607-46.
224. Sutter, E.E. and D. Tran, The field topography of ERG components in man--I. The photopic luminance response. Vision Res, 1992. 32(3): p. 433-46.
225. McDonagh, J., et al., Peripheral retinal dysfunction in patients taking vigabatrin. Neurology, 2003. 61(12): p. 1690-4.
226. Harding, G.F., et al., Visual electrophysiological effect of a GABA transaminase blocker. Doc Ophthalmol, 1998. 97(2): p. 179-88.
227. Hardus, P., et al., The value of electrophysiology results in patients with epilepsy and vigabatrin associated visual field loss. Acta Ophthalmol Scand, 2001. 79(2): p. 169-74.
228. Peterson, W.M. and S.S. Miller, Identification and functional characterization of a dual GABA/taurine transporter in the bullfrog retinal pigment epithelium. J Gen Physiol, 1995. 106(6): p. 1089-122.
229. Huang, D., et al., Optical coherence tomography. Science, 1991. 254(5035): p. 1178-81. 230. Fercher, A.F., Optical coherence tomography - development, principles, applications. Z
Med Phys, 2010. 20(4): p. 251-76. 231. Buabbud, J.C., M.M. Al-latayfeh, and J.K. Sun, Optical coherence tomography imaging
for diabetic retinopathy and macular edema. Curr Diab Rep, 2010. 10(4): p. 264-9. 232. Medeiros, F.A., et al., Comparison of retinal nerve fiber layer and optic disc imaging for
diagnosing glaucoma in patients suspected of having the disease. Ophthalmology, 2008. 115(8): p. 1340-6.
233. Schrems, W.A., et al., Comparison of scanning laser polarimetry and optical coherence tomography in quantitative retinal nerve fiber assessment. J Glaucoma, 2010. 19(2): p. 83-94.
234. Vizzeri, G., et al., Agreement between spectral-domain and time-domain OCT for measuring RNFL thickness. Br J Ophthalmol, 2009. 93(6): p. 775-81.
235. Clayton, L.M., et al., Retinal nerve fiber layer thickness in vigabatrin-exposed patients. Ann Neurol, 2011. 69(5): p. 845-54.
236. Choi, H.J. and D.M. Kim, Visual field constriction associated with vigabatrin: retinal nerve fiber layer photographic correlation. J Neurol Neurosurg Psychiatry, 2004. 75(10): p. 1395.
237. Moseng, L., et al., Retinal nerve fibre layer attenuation: clinical indicator for vigabatrin toxicity. Acta Ophthalmol, 2011. 89(5): p. 452-8.
238. Lawthom, C., P.E. Smith, and J.M. Wild, Nasal retinal nerve fiber layer attenuation: a biomarker for vigabatrin toxicity. Ophthalmology, 2009. 116(3): p. 565-71.
239. Wild, J.M., et al., Detecting vigabatrin toxicity by imaging of the retinal nerve fiber layer. Invest Ophthalmol Vis Sci, 2006. 47(3): p. 917-24.
240. Clayton, L.M., et al., Patterns of peripapillary retinal nerve fiber layer thinning in vigabatrin-exposed individuals. Ophthalmology, 2012. 119(10): p. 2152-60.
241. Westall, C.A., et al., The Hospital for Sick Children, Toronto, Longitudinal ERG study of children on vigabatrin. Doc Ophthalmol, 2002. 104(2): p. 133-49.
242. Marc, R.E., Structural organization of GABAergic circuitry in ectotherm retinas. Prog Brain Res, 1992. 90: p. 61-92.
243. Frumkes, T.E. and R. Nelson, Functional role of GABA in cat retina: I. Effects of GABAA agonists. Vis Neurosci, 1995. 12(4): p. 641-50.

117
244. Chappell, R.L., et al., GABA(C) receptors modulate the rod-driven ERG b-wave of the skate retina. Doc Ophthalmol, 2002. 105(2): p. 179-88.
245. Heim, M.K. and B.E. Gidal, Vigabatrin-associated retinal damage - potential biochemical mechanisms. Acta Neurol Scand, 2012. 126(4): p. 219-28.
246. Cubells, J.F., et al., In vivo action of enzyme-activated irreversible inhibitors of glutamic acid decarboxylase and gamma-aminobutyric acid transaminase in retina vs. brain. J Pharmacol Exp Ther, 1986. 238(2): p. 508-14.
247. Staley, K.J., B.L. Soldo, and W.R. Proctor, Ionic mechanisms of neuronal excitation by inhibitory GABAA receptors. Science, 1995. 269(5226): p. 977-81.
248. Kaufman, K.R., F.E. Lepore, and B.J. Keyser, Visual fields and tiagabine: a quandary. Seizure, 2001. 10(7): p. 525-9.
249. Borden, L.A., et al., Tiagabine, SK&F 89976-A, CI-966, and NNC-711 are selective for the cloned GABA transporter GAT-1. Eur J Pharmacol, 1994. 269(2): p. 219-24.
250. Heinamaki, A.A., A.S. Muhonen, and R.S. Piha, Taurine and other free amino acids in the retina, vitreous, lens, iris-ciliary body, and cornea of the rat eye. Neurochem Res, 1986. 11(4): p. 535-42.
251. Neuringer, M., et al., Dietary taurine is necessary for normal retinal development in monkeys. Prog Clin Biol Res, 1985. 179: p. 53-62.
252. Hanna, J., et al., Protective effect of taurine against free radicals damage in the rat myocardium. Exp Toxicol Pathol, 2004. 56(3): p. 189-94.
253. Saransaari, P. and S.S. Oja, Characteristics of taurine release induced by free radicals in mouse hippocampal slices. Amino Acids, 2004. 26(1): p. 91-8.
254. Schmidt, S.Y., E.L. Berson, and K.C. Hayes, Retinal degeneration in cats fed casein. I. Taurine deficiency. Invest Ophthalmol, 1976. 15(1): p. 47-52.
255. Leon, A., W.R. Levick, and M.G. Sarossy, Lesion topography and new histological features in feline taurine deficiency retinopathy. Exp Eye Res, 1995. 61(6): p. 731-41.
256. Lake, N., Electroretinographic deficits in rats treated with guanidinoethyl sulfonate, a depletor of taurine. Exp Eye Res, 1986. 42(1): p. 87-91.
257. Rapp, L.M., L.A. Thum, and R.E. Anderson, Synergism between environmental lighting and taurine depletion in causing photoreceptor cell degeneration. Exp Eye Res, 1988. 46(2): p. 229-38.
258. Geggel, H.S., et al., Nutritional requirement for taurine in patients receiving long-term parenteral nutrition. N Engl J Med, 1985. 312(3): p. 142-6.
259. Jammoul, F., et al., Taurine deficiency is a cause of vigabatrin-induced retinal phototoxicity. Ann Neurol, 2009. 65(1): p. 98-107.
260. Sivakami, S., et al., The gamma-aminobutyric acid transporter and its interaction with taurine in the apical membrane of the bovine retinal pigment epithelium. Biochem J, 1992. 283 ( Pt 2): p. 391-7.
261. Jammoul, F., et al., Taurine deficiency damages photoreceptors and retinal ganglion cells in vigabatrin-treated neonatal rats. Mol Cell Neurosci, 2010. 43(4): p. 414-21.
262. Froger, N., et al., Taurine provides neuroprotection against retinal ganglion cell degeneration. PLoS One, 2012. 7(10): p. e42017.
263. Westall, C.A., C.M. Panton, and A.V. Levin, Time courses for maturation of electroretinogram responses from infancy to adulthood. Doc Ophthalmol, 1998. 96(4): p. 355-79.

118
264. Mirabella, G., et al., Contrast sensitivity is reduced in children with infantile spasms. Invest Ophthalmol Vis Sci, 2007. 48(8): p. 3610-5.
265. Ito, M., H. Mikawa, and T. Taniguchi, Cerebrospinal fluid GABA levels in children with infantile spasms. Neurology, 1984. 34(2): p. 235-8.
266. Petroff, O.A., et al., Human brain GABA levels rise rapidly after initiation of vigabatrin therapy. Neurology, 1996. 47(6): p. 1567-71.
267. Roberts, J. and K.R. Duyan, Visual acuity of children, United States. National Center for Health Statistics Vital and health statistics Series 11: Data from the National Health Survey Data from the health examination survey,1970, Washington,: U.S. Health Services and Mental Health Administration. iv, 35 p.
268. Bailey, I.L. and J.E. Lovie, New design principles for visual acuity letter charts. Am J Optom Physiol Opt, 1976. 53(11): p. 740-5.
269. Ferris, F.L., 3rd, et al., New visual acuity charts for clinical research. Am J Ophthalmol, 1982. 94(1): p. 91-6.
270. Adoh, T.O., J.M. Woodhouse, and K.A. Oduwaiye, The Cardiff Test: a new visual acuity test for toddlers and children with intellectual impairment. A preliminary report. Optom Vis Sci, 1992. 69(6): p. 427-32.
271. Chandrakumar, M., et al., A new method for testing letter contrast sensitivity in a clinical setting: Comparing M&S
smart system II letter contrast test with Pelli-Robson chart in Association for Research in Vision and Ophthalmology2012: Fort Lauderdale, Florida.
272. International Research Group on Colour Vision Deficiencies. Symposium (10th : 1989 : Cagliari Italy), et al., Colour vision deficiencies X : proceedings of the tenth Symposium of the International Research Group on Colour Vision Deficiencies, held in Cagliari, Italy, 25-28 June 1989. Documenta ophthalmologica Proceedings series1991, Dordrecht ; Boston: Kluwer Academic Publishers. xxvi, 638 p.
273. Shute, R.H. and C.A. Westall, Use of the Mollon-Reffin minimalist color vision test with young children. J AAPOS, 2000. 4(6): p. 366-72.
274. Dersu, I., et al., Understanding Visual Fields, Part I; Goldmann Perimetry. Journal of Ophthalmic Medical Technology, 2006. 2(2).
275. Katz, J., et al., Automated perimetry detects visual field loss before manual Goldmann perimetry. Ophthalmology, 1995. 102(1): p. 21-6.
276. Smith, M., et al., Effect of pupillary dilatation on glaucoma assessments using optical coherence tomography. Br J Ophthalmol, 2007. 91(12): p. 1686-90.
277. Dawson, W.W., G.L. Trick, and C.A. Litzkow, Improved electrode for electroretinography. Invest Ophthalmol Vis Sci, 1979. 18(9): p. 988-91.
278. Wild, J.M., et al., Visual field loss in patients with refractory partial epilepsy treated with vigabatrin: final results from an open-label, observational, multicentre study. CNS Drugs, 2009. 23(11): p. 965-82.
279. Meador, K.J., Cognitive outcomes and predictive factors in epilepsy. Neurology, 2002. 58(8 Suppl 5): p. S21-6.
280. Kivity, S., et al., Long-term cognitive outcomes of a cohort of children with cryptogenic infantile spasms treated with high-dose adrenocorticotropic hormone. Epilepsia, 2004. 45(3): p. 255-62.
281. Luthvigsson, P., et al., Epidemiologic features of infantile spasms in Iceland. Epilepsia, 1994. 35(4): p. 802-5.

119
282. Kjellstrom, U., et al., Full-field ERG and visual fields in patients 5 years after discontinuing vigabatrin therapy. Doc Ophthalmol, 2008. 117(2): p. 93-101.
283. Quinn, G.E., et al., Visual fields measured with double-arc perimetry in eyes with threshold retinopathy of prematurity from the cryotherapy for retinopathy of prematurity trial. The CRYO-Retinopathy of Prematurity Cooperative Group. Ophthalmology, 1996. 103(9): p. 1432-7.
284. Westall, C.A., et al., The Hospital for Sick Children, Toronto, Longitudinal ERG study of children on vigabatrin. Documenta Ophthalmologica, 2002. 104(2): p. 133-49.
285. Takahashi, S., M. Sumiotomo, and H. Furuya, Change in peripheral visual fields under IV sedation with diazepam. Anesth Prog, 1989. 36(4-5): p. 159-60.
286. Harding, G.F., Severe persistent visual field constriction associated with vigabatrin. Four possible explanations exist. BMJ, 1997. 314(7095): p. 1694.
287. Arndt, C.F., et al., The effect on vision of associated treatments in patients taking vigabatrin: carbamazepine versus valproate. Epilepsia, 2002. 43(8): p. 812-7.
288. Clayton, L.M., et al., Delayed, rapid visual field loss in a patient after ten years of vigabatrin therapy. Eye (Lond), 2010. 24(1): p. 185-6.
289. Schmitz, B., et al., Visual field constriction in epilepsy patients treated with vigabatrin and other antiepileptic drugs: a prospective study. J Neurol, 2002. 249(4): p. 469-75.
290. Krauss, G.L., Evaluating risks for vigabatrin treatment. Epilepsy Curr, 2009. 9(5): p. 125-9.
291. Durnian, J.M. and L.G. Clearkin, Retinal nerve fibre layer characteristics with vigabatrin-associated visual field loss--could scanning laser polarimetry aid diagnosis? Eye (Lond), 2008. 22(4): p. 559-63.
292. Lawthom, C., P.E. Smith, and J. Wild, Optical coherence tomography identifies vigabatrin-attributed visual field loss in children and learning-disabled adults. Invest Ophthalmol, 2007. 48(E-Abstract 955).
293. Sommer, A., et al., Clinically detectable nerve fiber atrophy precedes the onset of glaucomatous field loss. Arch Ophthalmol, 1991. 109(1): p. 77-83.
294. Kjellstrom, U., S. Andreasson, and V. Ponjavic, Attenuation of the retinal nerve fibre layer and reduced retinal function assessed by optical coherence tomography and full-field electroretinography in patients exposed to vigabatrin medication. Acta Ophthalmol, 2013.
295. Akcakaya, A.A., et al., Detecting retinal vigabatrin toxicity in patients with partial symptomatic or cryptogenic epilepsy. Eur J Ophthalmol, 2010. 20(4): p. 763-9.
296. Garway-Heath, D.F., et al., Mapping the visual field to the optic disc in normal tension glaucoma eyes. Ophthalmology, 2000. 107(10): p. 1809-15.
297. Tan, O., et al., Detection of macular ganglion cell loss in glaucoma by Fourier-domain optical coherence tomography. Ophthalmology, 2009. 116(12): p. 2305-14 e1-2.
298. Mwanza, J.C., et al., Macular ganglion cell-inner plexiform layer: automated detection and thickness reproducibility with spectral domain-optical coherence tomography in glaucoma. Invest Ophthalmol Vis Sci, 2011. 52(11): p. 8323-9.
299. Tan, O., et al., Mapping of macular substructures with optical coherence tomography for glaucoma diagnosis. Ophthalmology, 2008. 115(6): p. 949-56.
300. Ozkul, Y., et al., Visual functions in epilepsy patients on valproate monotherapy. J Clin Neurosci, 2002. 9(3): p. 247-50.

120
301. Altemir, I., et al., Reproducibility of optical coherence tomography measurements in children. Am J Ophthalmol, 2013. 155(1): p. 171-176 e1.
302. Shields, C.L., et al., Optical coherence tomography in children: analysis of 44 eyes with intraocular tumors and simulating conditions. J Pediatr Ophthalmol Strabismus, 2004. 41(6): p. 338-44.
303. Brambrink, A.M., et al., Isoflurane-induced neuroapoptosis in the neonatal rhesus macaque brain. Anesthesiology, 2010. 112(4): p. 834-41.
304. Ing, C., et al., Long-term differences in language and cognitive function after childhood exposure to anesthesia. Pediatrics, 2012. 130(3): p. e476-85.
305. Wilder, R.T., et al., Early exposure to anesthesia and learning disabilities in a population-based birth cohort. Anesthesiology, 2009. 110(4): p. 796-804.
306. Tan, B.B., et al., Comparison of retinal nerve fiber layer measurement between 2 spectral domain OCT instruments. J Glaucoma, 2012. 21(4): p. 266-73.
307. El-Dairi, M.A., et al., Correlation between optical coherence tomography and glaucomatous optic nerve head damage in children. Br J Ophthalmol, 2009. 93(10): p. 1325-30.
308. Dickmann, A., et al., Unilateral amblyopia: An optical coherence tomography study. J AAPOS, 2009. 13(2): p. 148-50.
309. Meyer, C.H., D.J. Lapolice, and S.F. Freedman, Foveal hypoplasia in oculocutaneous albinism demonstrated by optical coherence tomography. Am J Ophthalmol, 2002. 133(3): p. 409-10.
310. Skarmoutsos, F., et al., The use of optical coherence tomography in the management of cystoid macular edema in pediatric uveitis. J AAPOS, 2006. 10(2): p. 173-4.
311. Maldonado, R.S., et al., Optimizing hand-held spectral domain optical coherence tomography imaging for neonates, infants, and children. Invest Ophthalmol Vis Sci, 2010. 51(5): p. 2678-85.
312. Muni, R.H., et al., Hand-held spectral domain optical coherence tomography finding in shaken-baby syndrome. Retina, 2010. 30(4 Suppl): p. S45-50.
313. Scott, A.W., et al., Imaging the infant retina with a hand-held spectral-domain optical coherence tomography device. Am J Ophthalmol, 2009. 147(2): p. 364-373 e2.
314. Rootman, D.B., et al., Hand-held high-resolution spectral domain optical coherence tomography in retinoblastoma: clinical and morphologic considerations. Br J Ophthalmol, 2013. 97(1): p. 59-65.
315. Chavala, S.H., et al., Insights into advanced retinopathy of prematurity using handheld spectral domain optical coherence tomography imaging. Ophthalmology, 2009. 116(12): p. 2448-56.
316. Chong, G.T., et al., Abnormal foveal morphology in ocular albinism imaged with spectral-domain optical coherence tomography. Arch Ophthalmol, 2009. 127(1): p. 37-44.
317. Gal, P., et al., Efficacy of sucrose to reduce pain in premature infants during eye examinations for retinopathy of prematurity. Ann Pharmacother, 2005. 39(6): p. 1029-33.
318. Mets, R.B., et al., Utility of Optical Coherence Tomography in Monitoring Vigabatrin Retinal Toxicity, in The Association for Research in Vision and Ophthalmology 20112011: Fort Lauderdale, Florida.

121
319. Lee, E.J., et al., Trend-based analysis of retinal nerve fiber layer thickness measured by optical coherence tomography in eyes with localized nerve fiber layer defects. Invest Ophthalmol Vis Sci, 2011. 52(2): p. 1138-44.
320. Medeiros, F.A., et al., Detection of glaucoma progression with stratus OCT retinal nerve fiber layer, optic nerve head, and macular thickness measurements. Invest Ophthalmol Vis Sci, 2009. 50(12): p. 5741-8.
! !

122
Appendix A - SickKids Research Ethics Board Approval
RESEARCH ETHICS BOARD
Dr. Carol Westall
Ophthalmology
The Hospital for Sick Children
Dear Dr. Westall:
Yours truly,
Richard SugarmanChair, Research Ethics Board
Your study "Vigabatrin and Infantile Epilepsy"
REB File No.: 1000015923
On behalf of the REB, I am writing to confirm that the above noted study was re-approved by the REB for one year ending in May 2014. The REB approved continuing review at level 2B. As necessary, the Clinical Research Office will be contacting you to arrange follow-up.
Please note that, in accordance with the Personal Health Information Protection Act of Ontario, you are responsible for adhering to all conditions and restrictions imposed by the REB governing the use, security, disclosure, return and disposal of the research subjects’ personal health information. You are also responsible for reporting immediately any privacy breaches to the REB Chair and to Janice Campbell, the Sick Kids privacy officer.
May 10, 2013
THE HOSPITAL FORSICK CHILDREN
555 University AveToronto, OntarioCanada M5G 1X8
www.sickkids.ca
Co-Investigator(s): Thomas Wright, Raymond Buncic, Carole Panton, Melissa Cotesta, Michelle Mcfarlane, Arun Reginald

123
Appendix B – Recruitment Letter
April 29, 2013 Dear Family,
As you know, your child has attended the Visual Electrophysiology Unit at Sick Kids for a vision test and diagnostic test called the electroretinogram (ERG). The test was part of the protocol to determine whether the anti-epileptic drug, vigabatrin, was affecting your child’s vision. Your child’s doctor(s) used vigabatrin to control infant seizures. It has been found that some patients taking vigabatrin develop vision problems. It has been some time since your child stopped using vigabatrin. Now that your child has matured, we would like to perform some follow-up tests of your child’s current vision status. This includes a clinical eye exam as well as some testing to see how well your child’s side vision is working. Some of these tests will require standard eye drops that will make your child’s pupils larger. We will give you an update on our findings once we have completed the tests on the group of children all of whom had been taking vigabatrin. Participation in the study will involve visiting the Hospital for approximately 2-3 hours. This visit will allow your child to have a comprehensive eye exam at the Hospital with a physician who will discuss any significant clinical findings with you. Participation in research is voluntary and you will be reimbursed $20 for out of pocket expenses and $10 for lunch. If you have any additional expenses, we are more than willing to discuss compensation with you. Please be assured that whether or not your child participates in this project will not affect any future care your child receives at the Hospital for Sick Children in any way. Please return the enclosed postcard indicating whether or not you wish to participate in the study. Alternatively you may contact Aparna Bhan (Research Coordinator) via email at [email protected] or via phone at (416) 813-1500 ext. 228589 in The Department of Ophthalmology and Vision Sciences, The Hospital for Sick Children. If we do not hear from you within two weeks, Aparna will contact you shortly after to give you more information regarding the study. Thank you for considering this request. Yours sincerely,
Ray Buncic MD FRCSC Ophthalmologist Department of Ophthalmology and Vision Sciences
Carol Westall PhD Director of Visual Electrophysiology Unit Department of Ophthalmology and Vision Sciences

124
Appendix C – Sample Consent and Assent Forms
THE HOSPITAL FOR SICK CHILDREN Department of Ophthalmology Visual Electrophysiology Unit Phone (416) 813-6516 Hospital for Sick Children (SickKids)
RESEARCH CONSENT FORM (For Parents of Patients)
Title of Research Project: Vigabatrin and Infantile Epilepsy Investigators Director of Electrophysiology: Dr.Carol Westall Responsible Individual: Dr. Carol Westall Senior Orthorptist: Carole Panton O.C. (C) Orthoptist: Melissa Cotesta OA Research Manager: Thomas Wright Ophthalmologist: Dr. J. Raymond Buncic Ophthalmologist: Dr. Arun Reginald Research Coordinator Aparna Bhan Graduate Student: Ananthavalli Kumarappah Purpose of the research: The drug vigabatrin is used to help control seizures. In some people the drug might cause problems with vision. This might be related to some small changes of the retina. The retina is the inner lining of the eye that makes a picture of what we see (like film in a camera). While your child was on vigabatrin, the electroretinogram (ERG) was used to assess retinal function. We want to better understand what is happening to the eyes in children on vigabatrin and assess if the ERG is associated with changes in the retina. It has been some time since your child stopped using vigabatrin. Now that your child is older, we would like to perform some follow-up tests of your child’s current vision status. Your child will have complete clinical assessment including visual acuity (test to see smallest detail visible), contrast sensitivity (ability to see low contrast on white background), colour vision, ophthalmoscopy (examination of the back of the eye), visual fields (test of side vision),
The Hospital for Sick Children The Hospital for Sick Children
Name: D.O.B.:
Hosp#:

125
fundus photography (pictures of the back of the eye) and OCT imaging. If the routine clinical examinations show any abnormalities we will discuss these findings with you and refer your child for further testing if required. Description of the research: The following tests will be performed once your child’s ophthalmologist has referred them to the Eye Clinic and an appointment has been made. Visual Fields Your child will be asked to fixate in the centre while a light is moved from the peripheral (side) to the centre. As soon as your child detects the light, s/he is required to press the button on the buzzer. Optical Coherence Tomography (OCT) We will take some photographs of the inside of your child’s eyes. Photographs of your child’s eyes will be done with an imaging technique known as high resolution OCT. This technique requires your child to look at a target and is painless. It will take approximately 20 minutes to complete. These photographs will not include your child’s face. Mollon-Reffin Minnimalist Colour Testing The test will require your child to pick up the coloured chip among a set of five gray chips under standardized lighting. This will test us how well your child can see colours. Fundus Photography We will take some photographs of the inside of your child’s eye. We will ask you to complete a separate consent form for these photographs. Patient’s health records will be reviewed for purposes of this study for information about drug history, co-morbidities etc. Standard clinic intake tests may be performed including vision, colour vision, refractive error, and / or ophthalmoscopy. The entire examination will take approximately two and a half hours. Potential Harms (Injury, Discomforts or Inconvenience): There are minimal harms associated with participation in this study. The eye drops cause slight stinging, but this resolves within 10 seconds. The drops which we use to dilate your child’s pupils may cause his/her vision be blurred up close for 4-8 hours. The risks involved in this study are no greater than those for normal clinic protocol. Potential Benefits: To the individual: Your child may not benefit directly from participating in this study. Ophthalmological and neurological care will continue whether your child continues in this study or not. Our research team will send you a letter detailing our findings when the study is completed.

126
To Society: Knowledge gained from this study will hopefully allow physicians to optimize Vigabatrin therapy to ensure patients receive the maximum benefit whilst minimizing visual toxicity. Better control of the risks associated with this powerful therapy will make its use in a wider patient population more feasible.�� Confidentiality: We will respect you and your child’s privacy. No information about who you are will be given to anyone or be published without your permission, unless the law makes us do this.
For example, the law could make us give information about you • If a child had been abused • If you have an illness that could spread to others • If you or someone else talks about suicide (killing themselves), or • If the court orders us to give them the study papers
Sick Kids Clinical Research Monitors or the regulator of the study may see your health record to check on the study. By signing this consent form, you agree to let these people look at your records. We will put a copy of this research consent form in your patient health record and give you a copy as well. The data produced from this study will be stored in a secure, locked location. Only members of the research team (and maybe those individuals described above) will have access to the data. Following completion of the research study the data will be kept as long as required by the Sick Kids “Records Retention and Destruction” policy. The data will then be destroyed according to this same policy. Reimbursement Compensation will be provided at a rate of $30.00 for each testing session in recognition of your time and effort. If you stop taking part in the study, you will be compensated for those tests your child has undergone up until that point. Participation: Participation in research is voluntary. You can withdraw your child from the study at any time. The care you get at Sick Kids will not be affected in any way by whether you take part in this study. New information that we get while we are doing this study may affect your decision to take part in this study. If this happens, we will tell you about this new information ask you again if you still want to be in the study.

127
During this study we may create new tests, new medicines, or other things that may be worth some money. Although we may make money from these findings, we cannot give you any of this money now or in the future because you took part in this study. We will give you a copy of this consent form for your records. In some situations, the study doctor or the company paying for the study may decide to stop the study. This could happen even if the medicine given in the study is helping you. If this happens, the study doctor will talk to you about what will happen next. If your child becomes ill or harmed because your child took part in this study, we will treat your child for free. Your signing this consent form does not interfere with your child’s legal rights in any way. The staff of the study, any people who gave money for the study, or the hospital are still responsible, legally and professionally, for what they do. Sponsor / Funder of the study The sponsor of this research is Sick Kids Hospital. The funder of this research is Lundbeck Pharmaceuticals. Conflict of Interest Some of the people doing this study may have a conflict of interest. That means that they may benefit personally, financially, or in some other way from this study . Dr. Westall (Principal Investigator) has received or may receive for research related to the present study money, or one or more of the following other benefits: speaker's fees, travel assistance, industry-initiated research grants, investigator- initiated research grants, consultant fees, honoraria, gifts, intellectual property rights such as patents, etc. from sponsor(s) that have activities related to the present study.

128
Title of Research Project: Vigabatrin and Infantile Epilepsy Parental Consent By signing this form, I agree that:
1) You have explained this study to me. You have answered all my questions. 2) You have explained the possible harms and benefits (if any) of this study. 3) I know what I could do instead of having my child take part in this study. I understand
that I have the right to refuse to let my child take part in the study. I also have the right to take my child out of the study at any time. My decision about my child taking part in the study will not affect my child’s health care at SickKids.
4) I am free now, and in the future, to ask any questions about the study. 5) I have been told that my child’s medical records will be kept private. You will give no
one information about my child, unless the law requires you to. 6) I understand that no information about my child will be given to anyone or be published
without first asking my permission. 7) I have read and understood pages 1 to 5 of this consent form. I agree, or consent, that my
child ________________________ may take part in this study. _____________________________________ ____________________________________ Printed Name of Parent/Legal Guardian Parent/Legal Guardian’s signature & date _____________________________ ________________________________ Printed Name of person who explained consent Signature & date ________________________________ _________________________________ Printed Witness’name (if the parent/legal Witness’ signature & date Guardian does not read English) If you have any questions about this study, please call Aparna Bhan at (416) 813 1500 ext. 228589. If you have questions about your rights as a subject in a study or injuries during a study, please call the Research Ethics Manager at (416 )813-5718.

129
Research Assent Form (For study subjects lacking ability to give consent)
Study Title: Vigabatrin and Infantile Epilepsy
Investigators:
Dr Carol Westall Principal Investigator
Thomas Wright Research Manager
Aparna Bhan Research Coordinator
Dr Ray Buncic Ophthalmologist
Arun Reginald Ophthalmologist
Carole Panton Senior Orthoptist
Melissa Cotesta Orthoptist
Ananthavalli Kumarappah Graduate Student
Why are we doing this study?
Often people who take the drug vigabatrin develop eye problems. When you were
taking vigabatrin, we looked at your eyes to see if there were any problems using
ERG. Now, we want to look at your visual function and compare it with the ERG
tests that you did when you were younger.
Name: ______________________
DoB:
________________________
MRN:
_______________________

130
What will happen during this study?
We will use drops that will make your pupils (the black part of your eye) larger.
You will be doing some tests that test how well you can see. We will also test your
side vision. We will ask you to look at a light in a machine while we take pictures
of the back of your eye.
Are there good and bad things about the study?
The eye drops may sting when we put them in your eye. This will only last for a
few seconds then it will go away.
Your eyes may be blurred after the test; this might stop you from things like
reading. You may also not like being in bright lights. This will go away after one
day at the most.
Who will know about what I did in the study?
If we feel your health may be in danger, we may have to report your results to your
doctor.
Can I decide if I want to be in the study?
Nobody will be angry or upset if you do not want to be in the study. We are talking
to your parent/legal guardians about the study and you should talk to them about it
too. You can decide to stop the study at any time
Assent:

131
I was present when ____________________________ read this form and said that he or she agreed, or
assented, to take part in this study.
_____________________________________ _____________________________
Printed Name of person who obtained assent Signature & Date
!

132
THE HOSPITAL FOR SICK CHILDREN Department of Ophthalmology Visual Electrophysiology Unit Phone (416) 813-6516 Hospital for Sick Children (SickKids)
RESEARCH CONSENT FORM (For Parents of Subjects Prescribed Vigabatrin)
Title of Research Project: Vigabatrin and Infantile Epilepsy . Investigators Director of Electrophysiology: Dr.Carol Westall Responsible Individual: Dr. Carol Westall Senior Orthorptist: Carole Panton O.C. (C) Orthoptist: Melissa Cotesta OA Research Manager: Thomas Wright Ophthalmologist: Dr. J. Raymond Buncic Ophthalmologist: Dr. Arun Reginald Research Coordinator Aparna Bhan 416 813 1500 ext 228589 Graduate Student: Ananthavalli Kumarappah Purpose of the research: The drug vigabatrin is used to help control seizures. In some people the drug might cause problems with vision. This might be related to some small changes of the retina. The retina is the inner lining of the eye that makes a picture of what we see (like film in a camera). We want to better understand what is happening to the eyes in children on vigabatrin. It has been some time since your child stopped using vigabatrin. Recently, we saw your child as part of our research study examining vision status of children who had been monitored using the electroretinogram (ERG) for vigabatrin toxicity. We would like to supplement the vision results with a follow-up ERG. This ERG will be very different from the ERGs that your child underwent while on vigabatrin. The ERG protocol will be much shorter (there will be no dark-adaptation) and we will be using a thin fibre placed in the lower eyelid to record the responses. These electrodes are more comfortable than the contact-lens electrodes.
Name: D.O.B.:
Hosp#:

133
The electroretinogram (ERG) is an electrophysiological test to measure the electrical response of the retina. ERGs are a routine clinical test used to assess retinal function when a retinal disease is suspected or known. We want to better understand what is happening to the eyes in people undergoing vigabatrin treatments. Description of the research: The following test will be performed once an appointment has been made. Electroretinogram (ERG): While your child’s pupils are still large, we will test how well the retina is working. To do this we will place a small piece of fibre across the front of each of your child’s eyes. The fibre will be placed with sticky tape to the bridge of the nose. It will be placed under the coloured part of the eyes, and we will place it on your child’s face with tape, at the other side of your child’s eyes. We will put drops in your child’s eyes which will make the pupils bigger and the vision blurred. We will then flash some lights at your child’s eyes. The fibre will pick up electrical signals from the retina. The test will take approximately 35 minutes. Potential Harms (Injury, Discomforts or Inconvenience): There are minimal harms associated with participation in this study. The eye drops cause slight stinging, but this resolves within 10 seconds. The drops which we use to dilate your child’s pupils may cause his/her vision be blurred up close for 4-8 hours. The risks involved in this study are no greater than those for normal clinic protocol. Potential Benefits: To the individual: Your child may not benefit directly from participating in this study. Ophthalmological and neurological care will continue whether your child continues in this study or not. Our research team will send you a letter detailing our findings when the study is completed. To Society: Knowledge gained from this study will hopefully allow physicians to optimize vigabatrin therapy to ensure patients receive the maximum benefit whilst minimizing visual toxicity. Better control of the risks associated with this powerful therapy will make its use in a wider patient population more feasible.�� Confidentiality: We will respect you and your child’s privacy. No information about who you are will be given to anyone or be published without your permission, unless the law makes us do this.
For example, the law could make us give information about you • If a child had been abused • If you have an illness that could spread to others • If you or someone else talks about suicide (killing themselves), or • If the court orders us to give them the study papers

134
Sick Kids Clinical Research Monitors or the regulator of the study may see your health record to check on the study. By signing this consent form, you agree to let these people look at your records. We will put a copy of this research consent form in your patient health record and give you a copy as well. The data produced from this study will be stored in a secure, locked location. Only members of the research team (and maybe those individuals described above) will have access to the data. Following completion of the research study the data will be kept as long as required by the Sick Kids “Records Retention and Destruction” policy. The data will then be destroyed according to this same policy. Reimbursement Compensation will be provided at a rate of $10.00 for the testing session in recognition of your time and effort. If you stop taking part in the study, you will be compensated for those tests your child has undergone up until that point. Participation: Participation in research is voluntary. You can withdraw your child from the study at any time. The care you get at Sick Kids will not be affected in any way by whether you take part in this study. New information that we get while we are doing this study may affect your decision to take part in this study. If this happens, we will tell you about this new information ask you again if you still want to be in the study. During this study we may create new tests, new medicines, or other things that may be worth some money. Although we may make money from these findings, we cannot give you any of this money now or in the future because you took part in this study. We will give you a copy of this consent form for your records. In some situations, the study doctor or the company paying for the study may decide to stop the study. This could happen even if the medicine given in the study is helping you. If this happens, the study doctor will talk to you about what will happen next. If your child becomes ill or harmed because your child took part in this study, we will treat your child for free. Your signing this consent form does not interfere with your child’s legal rights in any way. The staff of the study, any people who gave money for the study, or the hospital are still responsible, legally and professionally, for what they do. Sponsor / Funder of the study The sponsor of this research is Sick Kids Hospital. The funder of this research is Lundbeck Pharmaceuticals.

135
Conflict of Interest Some of the people doing this study may have a conflict of interest. That means that they may benefit personally, financially, or in some other way from this study . Dr. Westall (Principal Investigator) has received or may receive for research related to the present study money, or one or more of the following other benefits: speaker's fees, travel assistance, industry-initiated research grants, investigator- initiated research grants, consultant fees, honoraria, gifts, intellectual property rights such as patents, etc. from sponsor(s) that have activities related to the present study. Consent By signing this form, I agree that:
1) You have explained this study to me. You have answered all my questions. 2) You have explained the possible harms and benefits (if any) of this study. 3) I know what I could do instead of having my child take part in this study. I understand
that I have the right to refuse to let my child take part in the study. I also have the right to take my child out of the study at any time. My decision about my child taking part in the study will not affect my child’s health care at SickKids.
4) I am free now, and in the future, to ask any questions about the study. 5) I have been told that my child’s medical records will be kept private. You will give no
one information about my child, unless the law requires you to. 6) I understand that no information about my child will be given to anyone or be published
without first asking my permission. 7) I have read and understood pages 1 to 5 of this consent form. I agree, or consent, that my
child ________________________ may take part in this study. ______________________________________________________________________________ Printed Name of Parent/Legal Guardian Parent/Legal Guardian’s signature & date _____________________________ ______________ _ ________ Printed Name of person who explained consent Signature & date ________________________________ ______________________ Printed Witness’name (if the parent/legal Witness’ signature & date Guardian does not read English) If you have any questions about this study, please call Aparna Bhan at (416)-813-1500 ext. 328589. If you have questions about your rights as a subject in a study or injuries during a study, please call the Research Ethics Manager at (416)813-5718. !

136
Research Assent Form (For control subjects lacking ability to give consent)
Study Title: Vigabatrin and Infantile Epilepsy
Investigators:
Dr Carol Westall Principal Investigator
Thomas Wright Research Manager
Aparna Bhan Research Coordinator
Dr Ray Buncic Ophthalmologist
Dr. Arun Reginald Ophthalmologist
Carole Panton Senior Orthoptist
Melissa Cotesta Orthoptist
Ananthavalli Kumarappah Graduate Student
Why are we doing this study?
Often people who take the drug vigabatrin develop eye problems. When you were
taking vigabatrin, we looked at your eyes to see if there were any problems using
ERG. Your ERGs did not show any problems. Now, we want to do another ERG
and compare it with the ERG tests that you did when you were younger. This ERG
will be very different from the ERGs that you underwent while on vigabatrin. The
Name: ______________________
DoB:
________________________
MRN:
_______________________

137
ERG protocol will be much shorter (there will be no dark-adaptation) and we will
be using a thin fibre placed in the lower eyelid to record the responses. These
electrodes are more comfortable than the contact-lens electrodes.
What will happen during this study?
We will use drops that will make your pupils (the black part of your eye) larger.
You will be doing a special test called an Electroretinogram (ERG).
For the ERG, we will put drops into both your eyes to enlarge the pupils (the black
part in the middle of your eye). Then we ask you to sit in-front of our equipment.
We will put something that looks like a thin piece of thread across your eyes. The
thread will be placed beside your eyes with a sticky tape. We will then ask you to
look at some bright flashing lights.
Are there good and bad things about the study?
The eye drops may sting when we put them in your eye. This will only last for a
few seconds then it will go away.
Your eyes may be blurred after the test; this might stop you from things like
reading. You may also not like being in bright lights. This will go away few hours.
Who will know about what I did in the study?
If we feel your health may be in danger, we may have to report your results to your
doctor.
Can I decide if I want to be in the study?

138
Nobody will be angry or upset if you do not want to be in the study. We are talking
to your parent/legal guardians about the study and you should talk to them about it
too. You can decide to stop the study at any time
Assent:
I was present when _____________________________________ read this form and said that he or she
agreed, or assented, to take part in this study.
_____________________________________ __________________________________
Printed Name of person who obtained assent Signature & Date

139
Appendix D – Case Report Form
CASE REPORT FORM, REB# 1000015923 Version Date: 2012.12.17
Hospital for Sick Children Department of Ophthalmology 555 University Avenue, Toronto, Ontario, M5G 1X8 416-813-7654 ext. 3606
Project Title: Vigabatrin and Infantile Epilepsy
PI: Dr. Carol Westall
Subject ID:
Testing session #:
Date
DD/MM/YY
1.0 Patient Information
Gender: M F Age: __________
Time/date booked:________________
Diagnosis:
Co-morbidities:
Consent obtained:
Yes No
2.0 Drug History Vigabatrin Other AEDs Non AEDs Ever on? (Y/N)
Date Initiated? (YY/MM/DD)
Currently on? (Y/N)
Duration? (Months)
Current Dose? (g/kg)
Cumulative Dose? (g/kg)
Date off? (YY/MM/DD)
___________________
___________________
___________________
___________________
___________________
___________________
___________________
____________________
____________________
____________________
____________________
____________________
____________________
____________________
____________________________
____________________________
____________________________
____________________________
____________________________
____________________________
____________________________
3.0 Intake (Scoring)
Tester:_______________
Visual Acuity ETDRS, Chart 2
Z R K D C
D N C H V C D H N R
R V Z O S
O S D V Z N O Z C D
R D N S K
O K S V Z
K S N H O H O V S N
V C S Z H
C Z D R V S H R Z C
D N O K R
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
-0.1
-0.2
-0.3
ETDRS, Chart 3 R N O V S
Z C R D H N V S O K
D R Z K O
S N H C V C R V S Z
V K C N H
S V K D N
K D H Z C H Z C O R
O K D H N
Z O N K C R H S V D
D S O R Z
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
-0.1
-0.2
-0.3
Colour Vision Mollon-Reffin Minimalist OD OS
First Tested P____ D____ T____ P____ D____ T____
Binocular: P____ D____ T____ Notes:_______________________________________________________________________________________
Contrast Sensitivity M&S Smart System II OD OS
First Tested _______________ _______________
Binocular: _____________ Notes:_____________________________________________________________________________________
Visual Acuity Cardiff Teller OD OS
First Tested _________ _________
Binocular: _________ Notes:______________________________________________________________________________________
OD OS First Tested
_________ _________
Binocular: _________
Page 1
TIME STARTED TIME FINISHED

140
!
CASE REPORT FORM, REB# 1000015923 Version Date: 2012.12.17
Hospital for Sick Children Department of Ophthalmology 555 University Avenue, Toronto, Ontario, M5G 1X8 416-813-7654 ext. 3606
Project Title: Vigabatrin and Infantile Epilepsy
PI: Dr. Carol Westall
Subject ID:
Testing session #:
Date
DD/MM/YY
4.0 Visual Fields - Goldmann
Tester: _______________________
OD OS First Tested IVE IIE IE
Notes
5.0 Ophthalmic Examination
Tester: _______________________ OD Normal OS Normal _________ Lids _________ _________ Conjunctiva _________ _________ Cornea _________ _________ Anterior Chamber _________ _________ Pupil _________ _________ Lens _________ _________ Vitreous _________ _________ Disc _________ _________ Macula _________ _________ Periphery _________
OD OS Yes / No Toxicity Yes / No ____, ____ x ____ Refractive Error ____, ____ x ____ EOM: Normal Other Notes ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
6.0 Dilation Orders
Administer: OU Name: ________________ Proparacaine 0.5% Signed: _______________ Cyclopentolate 1% Date: _________________ Phenylephrine 2.5% Time: _________
Administered by: ________________________ Date: _________ Signed: ________________________________ Time: _________
7.0 Imaging – Fundus Photography and OCT Fundus Photography Tester: _______________ OD OS
Disc Macula
OCT Tester: _______________ OD OS
Disc Cube, 200x200, 6x6x2 Macula Cube, 512X128
Page 2
TIME STARTED TIME FINISHED
TIME STARTED TIME FINISHED
TIME STARTED TIME FINISHED TIME STARTED TIME FINISHED
Notes

141
!
CASE REPORT FORM, REB# 1000015923 Version Date: 2012.12.17
Hospital for Sick Children Department of Ophthalmology 555 University Avenue, Toronto, Ontario, M5G 1X8 416-813-7654 ext. 3606
Project Title: Vigabatrin and Infantile Epilepsy PI: Dr. Carol Westall
Subject ID:
Testing session #:
Date
DD/MM/YY
1.0 Patient Information
Gender: M F Age: __________
Time/date booked:________________
Diagnosis:
Co-morbidities:
Consent obtained:
Yes No
2.0 ERG Assessment: Time Started Time Finished Pupil Dilated? □ Yes □ No
Notes

142
Appendix E – Mixed Model Code libname valli "c:\work\carol westall\ananthavalli kumarappah"; options ls=140 ps=90 nodate nocenter nonumber; title; PROC IMPORT OUT= valli.vigabatrin DATAFILE= "C:\ work\carol westall\ananthavalli kumarappah\data for model.xlsx" DBMS=EXCEL REPLACE; RUN; Proc sort data=valli.vigabatrin; by toxicity; run; Proc means data=valli.vigabatrin n min q1 mean median q3 std maxdec=2; By toxicity; Class quadrant; Var rnfl; Run; Proc sort data=valli.vigabatrin; by id quadrant; run; Data first; set valli.vigabatrin; by id; if first.id; run; Proc mixed data=valli.vigabatrin; Class toxicity quadrant id; Model rnfl=toxicity quadrant toxicity*quadrant/residual ddfm=kr; Repeated quadrant/subject=id type=csh; slice toxicity*quadrant/sliceby=quadrant pdiff cl; RUN;

143
Appendix F – Patient Demographic Information
ID Sex ERG Baseline Toxicity Age at Research Visit (Years)
Years since VBG
discontinuation 1209 F Yes Yes 12.1 4.5 1212 M Yes Yes 10.5 8.4 1213 F Yes Yes 11.0 9.7 1217 F No Yes 13.2 3.1 1219 F Yes No 8.7 7.2 1222 F Yes Yes 14.2 12.6 1225 F No Yes 23.4 8.9 1226 M Yes Yes 23.2 9.8 1228 M No No 9.2 8.0 1233 M No No 14.4 11.6 1235 F Yes No 13.4 10.3 1236 M No Yes 11.1 9.1 1239 M Yes No 9.0 7.8 1251 M Yes No 11.7 9.0 1254 M No No 12.6 10.6 1256 F Yes No 12.3 11.7 1268 F Yes No 14.4 11.3 1269 M Yes No 14.0 11.9 1284 M Yes No 11.1 9.8 1287 M Yes No 9.7 6.3 1300 F No No 15.8 12.6 1312 F Yes No 8.8 7.6

144
ID
Age at VGB
initiation (months)
VGB Duratio
n (months
)
Reason for VGB Other AEDs with Other co-morbiditeis
1209 19.8 73 Partial complex seizures secondary to TSC
Carbamazepine, Valproic acid
TSC with multiple renal angiomyolipomata, Cognitive delay,
Eczema
1212 9.4 16 IS Developmental delay (mild), Strabimus (surgery for right
esotropia) 1213 7.7 9 IS 1217 2.6 120 IS
1219 15.4 3 IS Phenobarbital, ACTH
Autism spectrum disorder, Developmental Delay, Ketotic hypoglycemia, Rett syndrome (caused by CDKL5 mutation)
1222 6.5 13 IS Developmetnal delay, Corneal clouding
1225 63.6 113 NA Cerebral palsy, Global
developmental delay, Lennox-Gastaut syndrome, Scoliosis
1226 137.0 29 Intractable Epilepsy Topiramate, Lamotrigine, Zonisamide
1228 4.3 11 NA ACTH, Phenobarbital 1233 8.6 25 NA Lamotrigine, Domperidone Down syndrome, Osteopenia
1235 3.7 33 Complex seizure disorder secondary to congenital
CMV infection
Clobazam, Phenobarbital, Topiramate
Intractable seizures, global developmental delay
1236 6.6 17 IS Phenobarbital Visual impairment, Global
developmental delay; Spastic diplegia

145
1239 5.7 9 IS Flunarizine or placebo 1251 11.5 21 IS Phenobarbital
1254 10.7 13 IS Phenobarbital, Lamotrigine Hypoxic ischemic encepholpathy, Hyperglycemia
1256 4.8 3 IS
1268 13.3 25 IS Neurofibromatosis type 1,
Moyamoya disease, Autism spectrum disorder
1269 7.4 17 IS 1284 5.8 10 IS Amblyopia 1287 33.9 7 IS Tuberous sclerosis, G6PD deficiency 1300 2.7 37 IS ACTH Global developmental delay 1312 4.6 10 IS Flunarizine or placebo

146
Appendix G – Visual Acuity and Contrast Sensitivity Results
ID Visual Acuity – ETDRS (logMAR) Visual Acuity – Cardiff (logMAR) Contrast Sensitivity – M&S (unit)
1209 Right: 0 Left: 0
Right: 0 Left: 0
Right: 2 Left: 2
1212 Right: 0.66 Left: 0.62 NA Right: 3.2
Left: 1.6
1213 NA Right: 0 Left: 0 Binocular: 4
1217 Right: 0.36 Left: 0.36 NA Right: 5
Left: 5
1219 NA Right: 0.1 Left: 0.1 NA
1222 Right: 0.34 Left: 0.36
Right: 0.3 Left: 0.3
Right: 4 Left: 4
1225 NA NA NA
1226 Right: 0.04 Left: 0
Right: 0 Left: 0
Right: 3.2 Left: 3.2
1228 Right: 0.1 Left: 0.1
Right: 0 Left: 0
Right: 2 Left: 1.6
1233 NA Right: 0 Left: 0 NA
1235 NA NA NA
1236 NA Right: 0.2 Left: 0.2 NA
1239 Right: 0 Left: 0.1
Right: 0 Left: 0
Right: 2 Left: 1.6
1251 Right: 0.02 Left: 0
Right: 0 Left: 0
Right: 2.5 Left: 2.5
1254 NA Right: 0 Left: 0 NA

147
1256 Right: -0.1 Left: 0
Right: 0 Left: 0
Right: 1.25 Left: 1.6
1268 Right: 0.2 Left: 0.2
Right: 0 Left: 0
Right: 1.25 Left: 1.6
1269 Right: 0.4 Left: 0.36 NA Right: 8
Left: 10
1284 Right: 0.7 Left: -0.1 NA Right: 1.6
Left: 1.6
1287 Right: 0.1 Left: -0.04
Right: 0 Left: 0
Right: 2.5 Left: 4
1300 NA Right: 0 Left: 0 NA
1312 Right: 0.2 Left: 0.1
Right: 0 Left: 0
Right: 10 Left: 4
!

148
Appendix H – Colour Vision Results ID Protan Deutan Tritan
1209 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1212 Right: 3 Left: 1
Right: 2 Left: 1
Right: 1 Left: 0.5
1213 Binocular: 1 Binocular: 1 Binocular 0.5
1217 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1219 NA NA NA
1222 Right: 1 Left: 1
Right: 1 Left: 1
Right: 1 Left: 1
1225 NA NA NA
1226 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1228 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1233 NA NA NA 1235 NA NA NA 1236 NA NA NA
1239 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 1
1251 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1254 Right: 1 Left: 1
Right: 1 Left: 1
Right: 2 Left: 2
1256 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1268 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1269 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1284 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1287 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5
1300 Binocular: 1 Binocular: 1 Binocular: 0.5
1312 Right: 1 Left: 1
Right: 1 Left: 1
Right: 0.5 Left: 0.5

149
Appendix I – Goldmann Visual Field Results Target size: I 2e (all values are recorded as degrees from fovea)
ID Temporal Superior Nasal Inferior Right Left Right Left Right Left Right Left
1209 4 29 20 12 18 11 13 13 1212 NA NA NA NA NA NA NA NA 1213 NA NA NA NA NA NA NA NA 1217 NA NA NA NA NA NA NA NA 1219 NA NA NA NA NA NA NA NA 1222 NA NA NA NA NA NA NA NA 1225 NA NA NA NA NA NA NA NA 1226 NA NA NA NA NA NA NA NA 1228 33 8 10 9 23 14 22 11 1233 NA NA NA NA NA NA NA NA 1235 NA NA NA NA NA NA NA NA 1236 NA NA NA NA NA NA NA NA 1239 33 29 18 15 26 24 28 25 1251 25 26 10 12 13 16 21 13 1254 NA NA NA NA NA NA NA NA 1256 42 36 22 18 15 26 22 22 1268 26 31 18 12 26 20 17 21 1269 41 48 15 22 28 24 28 28 1284 31 33 25 25 23 28 28 22 1287 28 32 17 19 22 28 22 25 1300 NA NA NA NA NA NA NA NA 1312 29 29 12 12 15 19 12 21
Target size: I 4e (all values are recorded as degrees from fovea)
ID Temporal Superior Nasal Inferior Right Left Right Left Right Left Right Left
1209 34 53 34 28 40 25 37 36 1212 29 3 16 6 8 4 9 3 1213 NA NA NA NA NA NA NA NA 1217 NA NA NA NA NA NA NA NA 1219 NA NA NA NA NA NA NA NA 1222 NA NA NA NA NA NA NA NA 1225 NA NA NA NA NA NA NA NA 1226 NA NA NA NA NA NA NA NA

150
1228 63 69 48 46 52 58 52 53 1233 NA NA NA NA NA NA NA NA 1235 NA NA NA NA NA NA NA NA 1236 NA NA NA NA NA NA NA NA 1239 78 78 38 42 57 60 55 55 1251 71 72 43 39 49 52 54 52 1254 NA NA NA NA NA NA NA NA 1256 69 60 35 41 45 49 42 50 1268 60 58 45 34 42 43 47 52 1269 72 81 38 48 33 58 51 62 1284 75 78 48 43 52 54 57 53 1287 72 76 40 49 55 59 49 52 1300 NA NA NA NA NA NA NA NA 1312 51 47 34 38 44 48 51 37
Target size: IV 4e (all values are recorded as degrees from fovea)
ID Temporal Superior Nasal Inferior Right Left Right Left Right Left Right Left
1209 63 69 42 43 52 38 55 48 1212 45 7 34 8 22 11 29 7 1213 NA NA NA NA NA NA NA NA 1217 NA NA NA NA NA NA NA NA 1219 NA NA NA NA NA NA NA NA 1222 NA NA NA NA NA NA NA NA 1225 NA NA NA NA NA NA NA NA 1226 55 69 47 52 52 41 67 64 1228 78 79 52 51 58 62 59 57 1233 NA NA NA NA NA NA NA NA 1235 NA NA NA NA NA NA NA NA 1236 NA NA NA NA NA NA NA NA 1239 84 83 42 48 60 64 58 60 1251 81 82 53 44 56 60 65 65 1254 NA NA NA NA NA NA NA NA 1256 80 80 44 48 58 60 66 62 1268 74 72 50 41 47 50 54 57 1269 90 NA 47 NA 62 NA 68 NA 1284 81 83 48 51 53 59 57 61 1287 82 78 48 53 57 64 55 54 1300 NA NA NA NA NA NA NA NA 1312 70 68 43 48 51 49 60 54

151
Appendix J – Clinical Findings by an Ophthalmologist
ID Slit Lamp Examination Fundus Examination Refraction EOM Toxicity
1209 Normal Astrocytic hamaratoma
(OU) in context of Tuberous Sclerosis
R: +2.50 L: +1.50 +0.75 x90 Normal No
1212 Normal
Mild atrophy of disc, macula and periphery (OU); Reduced RNFL
(OU)
R: -0.50 L: -1.50 +0.75 x90
Mild extropia Yes
1213 Normal Normal R: 0.00 (plano) L: -0.50 Normal No
1217 Normal Mild atrophy of RNFL and disc secondary to
CNS disease
R: +2.50 +1.00 x120 L: +1.00 +1.50 x90 Normal No
1219 Normal Normal R: 0.00 (plano) L: 0.00 (plano) Normal No
1222 Normal Mild reduction of
RNFL; No demarcation typical of toxicity
R: 0.00 (plano) L: 0.00 (plano)
Inferior oblique
overaction (OU)
No
1225 Normal Toxicity; NFL
reduction globally and superimposed toxicity
R: +2.00 L: +2.00 Normal Yes
1226 Normal Toxicity R: +0.50 L: +0.50 Normal Yes
1228 Normal Normal R: 0.00 (plano) L: 0.00 (plano) Normal No
1233 Normal Generalized pallor
(OU); General RNFL reduction (OU)
Normal No
1235 Normal Mild reduction of peripheral RNFL
R: 0.00 (plano) L: 0.00 (plano) Normal Yes
1236 Normal Normal R: +0.50 L: +0.50 Normal No
1239 Normal Normal R: +1.00 L: +2.00
Small extropia No
1251 Normal Normal R: 0.00 (plano) L: 0.00 (plano) Normal No
1254 Normal Normal R: 0.00 (plano) L: 0.00 (plano) Normal No
1256 Normal Normal R: -3.00 L: -3.00 Normal No
1268 Lisch Normal R: -6.00 Normal No

152
Nodules (OU)
L: -6.00
1269 Normal Normal NA Normal No
1284 Normal Normal R: +1.50 L: 0.00 (plano) Normal No
1287 Normal Mild reduction in reflex and RNFL (OU) - not
specific to toxicity
R: +1.50 L: 0.00 (plano) Normal No
1300 Intermittent ptosis (OS) Normal R: +0.25 +2.50 x90
L: +0.25 +2.50 x90 Normal No
1312 Normal Normal R: -1.00 L: -1.00 Normal No
!

153
Appendix K – Fundus Photography Results
K-1 – Observer
!

154
K-2 – Observer 2

155
Appendix L – OCT Results
L-1 – Optic Disc Cube – Retinal Nerve Fibre Layer Thickness by Quadrants
ID Signal Strength Global Superior
Quadrant Nasal
Quadrant Inferior
Quadrant Temporal Quadrant
Right Left Right Left Right Left Right Left Right Left Right Left 1209 10 10 69 66 72 74 44 40 99 90 62 60 1212 9 9 64 62 73 80 47 39 78 82 59 47 1213 NA NA NA NA NA NA NA NA NA NA NA NA 1217 8 7 82 62 113 55 73 57 89 62 52 72 1219 NA NA NA NA NA NA NA NA NA NA NA NA 1222 NA NA NA NA NA NA NA NA NA NA NA NA 1225 NA NA NA NA NA NA NA NA NA NA NA NA 1226 9 10 77 66 76 92 44 47 88 80 99 46 1228 10 8 93 93 130 127 56 62 129 131 56 53 1233 NA NA NA NA NA NA NA NA NA NA NA NA 1235 NA NA NA NA NA NA NA NA NA NA NA NA 1236 NA NA NA NA NA NA NA NA NA NA NA NA 1239 8 10 99 108 120 131 70 74 140 161 66 67 1251 10 9 93 90 130 125 75 69 100 109 65 57 1254 NA NA NA NA NA NA NA NA NA NA NA NA 1256 10 9 95 82 123 106 59 55 125 105 73 60 1268 8 9 91 93 119 136 42 72 115 112 88 50 1269 10 10 103 104 130 139 73 69 116 119 89 89 1284 9 9 108 99 143 135 91 70 149 126 51 66 1287 9 10 93 92 129 127 75 69 114 115 54 58 1300 NA NA NA NA NA NA NA NA NA NA NA NA 1312 8 8 95 95 118 125 59 59 130 130 74 66
!

156
L-2 – Ganglion Cell Analysis
ID Signal Strength Average GCL/IPL
Minimum GCL/IPL
Right Left Right Left Right Left 1209 10 10 80 84 76 83 1212 10 10 71 69 68 60 1213 NA NA NA NA NA NA 1217 NA NA NA NA NA NA 1219 NA NA NA NA NA NA 1222 NA NA NA NA NA NA 1225 NA NA NA NA NA NA 1226 9 10 76 74 73 73 1228 8 10 71 74 64 72 1233 NA NA NA NA NA NA 1235 NA NA NA NA NA NA 1236 NA NA NA NA NA NA 1239 9 10 88 87 87 78 1251 10 9 77 80 67 78 1254 NA NA NA NA NA NA 1256 10 10 76 75 75 75 1268 7 10 78 76 77 72 1269 9 10 88 90 87 86 1284 10 9 82 79 79 76 1287 10 10 81 81 82 81 1300 NA NA NA NA NA NA 1312 NA NA NA NA NA NA

157
ID 12:00 2:00 4:00 6:00 8:00 10:00 Right Left Right Left Right Left Right Left Right Left Right Left
1209 84 84 82 85 79 84 74 81 82 86 82 84 1212 78 81 69 72 70 70 69 67 69 58 71 66 1213 NA NA NA NA NA NA NA NA NA NA NA NA 1217 NA NA NA NA NA NA NA NA NA NA NA NA 1219 NA NA NA NA NA NA NA NA NA NA NA NA 1222 NA NA NA NA NA NA NA NA NA NA NA NA 1225 NA NA NA NA NA NA NA NA NA NA NA NA 1226 76 70 74 84 72 78 69 70 80 73 84 71 1228 65 74 74 71 71 72 71 72 74 76 71 76 1233 NA NA NA NA NA NA NA NA NA NA NA NA 1235 NA NA NA NA NA NA NA NA NA NA NA NA 1236 NA NA NA NA NA NA NA NA NA NA NA NA 1239 89 86 90 88 89 88 84 78 87 90 91 90 1251 82 80 88 77 77 78 65 81 74 82 77 83 1254 NA NA NA NA NA NA NA NA NA NA NA NA 1256 77 77 79 73 78 73 74 75 74 75 75 78 1268 79 78 75 77 75 76 81 80 80 72 77 70 1269 87 91 92 92 91 88 85 83 85 90 88 94 1284 84 81 81 79 78 76 82 79 84 81 84 80 1287 82 80 82 80 82 81 80 80 81 81 80 83 1300 NA NA NA NA NA NA NA NA NA NA NA NA 1312 NA NA NA NA NA NA NA NA NA NA NA NA
!

158
Appendix M – Follow-up ERG Results
ID Flicker!Amplitude!!(μV) Right&Eye& Left Eye
1209 75 NA 1212 146 131 1213 NA NA 1217 66 NA 1219 NA NA 1222 NA NA 1225 NA NA 1226 60 49 1228 116 NA 1233 NA NA 1235 NA NA 1236 NA NA 1239 101 86 1251 143 156 1254 NA NA 1256 NA NA 1268 NA NA 1269 NA NA 1284 NA NA 1287 NA NA 1300 80 47 1312 NA NA
!

159
Appendix N – Copyright Acknowledgements
Figure 7-1
11/27/13 Rightslink Printable License
https://s100.copyright.com/CustomerAdmin/PLF.jsp?ref=d3aab3ee-28e3-4acc-a8c8-4b5d4528e407 1/4
SPRINGER LICENSETERMS AND CONDITIONS
Nov 27, 2013
This is a License Agreement between Ananthavalli Kumarappah ("You") and Springer
("Springer") provided by Copyright Clearance Center ("CCC"). The license consists of your
order details, the terms and conditions provided by Springer, and the payment terms and
conditions.
All payments must be made in full to CCC. For payment instructions, please seeinformation listed at the bottom of this form.
License Number 3253700819521
License date Oct 21, 2013
Licensed content publisher Springer
Licensed content publication Documenta Ophthalmologica
Licensed content title Standard for clinical electroretinography
Licensed content author Michael F. Marmor
Licensed content date Jan 1, 1990
Volume number 73
Issue number 4
Type of Use Thesis/Dissertation
Portion Figures
Author of this Springer article No
Order reference number
Title of your thesis /
dissertation
Association between vigabatrin toxicity identified by ERG and
subsequent visual field reduction
Expected completion date Jan 2014
Estimated size(pages) 100
Total 0.00 CAD
Terms and Conditions
Introduction
The publisher for this copyrighted material is Springer Science + Business Media. By clicking
"accept" in connection with completing this licensing transaction, you agree that the following
terms and conditions apply to this transaction (along with the Billing and Payment terms and
conditions established by Copyright Clearance Center, Inc. ("CCC"), at the time that you
opened your Rightslink account and that are available at any time at
http://myaccount.copyright.com).
Limited License

160
!
1/22/2014 Rightslink Printable License
https://s100.copyright.com//CustomerAdmin/PLF.jsp?ref=bbee525b-002c-4c7a-8ce9-cefeee98de57 2/4
Limited LicenseWith reference to your request to reprint in your thesis material on which Springer Science andBusiness Media control the copyright, permission is granted, free of charge, for the useindicated in your enquiry.
Licenses are for one-time use only with a maximum distribution equal to the number that youidentified in the licensing process.
This License includes use in an electronic form, provided its password protected or on theuniversity’s intranet or repository, including UMI (according to the definition at the Sherpawebsite: http://www.sherpa.ac.uk/romeo/). For any other electronic use, please contactSpringer at ([email protected] or [email protected]).
The material can only be used for the purpose of defending your thesis, and with a maximumof 100 extra copies in paper.
Although Springer holds copyright to the material and is entitled to negotiate on rights, thislicense is only valid, subject to a courtesy information to the author (address is given with thearticle/chapter) and provided it concerns original material which does not carry references toother sources (if material in question appears with credit to another source, authorization fromthat source is required as well).
Permission free of charge on this occasion does not prejudice any rights we might have tocharge for reproduction of our copyrighted material in the future.
Altering/Modifying Material: Not PermittedYou may not alter or modify the material in any manner. Abbreviations, additions, deletionsand/or any other alterations shall be made only with prior written authorization of the author(s)and/or Springer Science + Business Media. (Please contact Springer at([email protected] or [email protected])
Reservation of RightsSpringer Science + Business Media reserves all rights not specifically granted in thecombination of (i) the license details provided by you and accepted in the course of thislicensing transaction, (ii) these terms and conditions and (iii) CCC's Billing and Payment termsand conditions.
Copyright Notice:DisclaimerYou must include the following copyright and permission notice in connection with anyreproduction of the licensed material: "Springer and the original publisher /journal title,volume, year of publication, page, chapter/article title, name(s) of author(s), figure number(s),original copyright notice) is given to the publication in which the material was originallypublished, by adding; with kind permission from Springer Science and Business Media"
Warranties: None
Example 1: Springer Science + Business Media makes no representations or warranties withrespect to the licensed material.
Example 2: Springer Science + Business Media makes no representations or warranties withrespect to the licensed material and adopts on its own behalf the limitations and disclaimersestablished by CCC on its behalf in its Billing and Payment terms and conditions for this

161
!
1/22/2014 Rightslink Printable License
https://s100.copyright.com//CustomerAdmin/PLF.jsp?ref=bbee525b-002c-4c7a-8ce9-cefeee98de57 3/4
licensing transaction.
Indemnity
You hereby indemnify and agree to hold harmless Springer Science + Business Media and
CCC, and their respective officers, directors, employees and agents, from and against any and
all claims arising out of your use of the licensed material other than as specifically authorized
pursuant to this license.
No Transfer of License
This license is personal to you and may not be sublicensed, assigned, or transferred by you to
any other person without Springer Science + Business Media's written permission.
No Amendment Except in Writing
This license may not be amended except in a writing signed by both parties (or, in the case of
Springer Science + Business Media, by CCC on Springer Science + Business Media's behalf).
Objection to Contrary Terms
Springer Science + Business Media hereby objects to any terms contained in any purchase
order, acknowledgment, check endorsement or other writing prepared by you, which terms are
inconsistent with these terms and conditions or CCC's Billing and Payment terms and
conditions. These terms and conditions, together with CCC's Billing and Payment terms and
conditions (which are incorporated herein), comprise the entire agreement between you and
Springer Science + Business Media (and CCC) concerning this licensing transaction. In the
event of any conflict between your obligations established by these terms and conditions and
those established by CCC's Billing and Payment terms and conditions, these terms and
conditions shall control.
Jurisdiction
All disputes that may arise in connection with this present License, or the breach thereof, shall
be settled exclusively by arbitration, to be held in The Netherlands, in accordance with Dutch
law, and to be conducted under the Rules of the 'Netherlands Arbitrage Instituut' (Netherlands
Institute of Arbitration).OR:
All disputes that may arise in connection with this present License, or the breach
thereof, shall be settled exclusively by arbitration, to be held in the Federal Republic of
Germany, in accordance with German law.
Other terms and conditions:
v1.3
If you would like to pay for this license now, please remit this license along with yourpayment made payable to "COPYRIGHT CLEARANCE CENTER" otherwise you will beinvoiced within 48 hours of the license date. Payment should be in the form of a checkor money order referencing your account number and this invoice numberRLNK501140144.Once you receive your invoice for this order, you may pay your invoice by credit card.Please follow instructions provided at that time.
Make Payment To:Copyright Clearance CenterDept 001P.O. Box 843006Boston, MA 02284-3006

162
!
1/22/2014 Rightslink Printable License
https://s100.copyright.com//CustomerAdmin/PLF.jsp?ref=bbee525b-002c-4c7a-8ce9-cefeee98de57 4/4
For suggestions or comments regarding this order, contact RightsLink CustomerSupport: [email protected] or +1-877-622-5543 (toll free in the US) or +1-978-646-2777.
Gratis licenses (referencing $0 in the Total field) are free. Please retain this printablelicense for your reference. No payment is required.

163
Figure 8-1
Re: Permission to use Copyright Material in Masters ThesisDavid Sampson [[email protected]]Sent:May 6, 2013 8:11 PMTo: Ananthavalli Kumarappah
Dear Ananthavalli,I would be happy for you to use this figure attributed as you suggest.Kind regards,David Sampson
________________________
David D. Sampson, PhD
Head, Optical+Biomedical Engineering LaboratoryWinthrop Professor, School of Electrical, Electronic & Computer EngineeringDirector, Centre for Microscopy, Characterisation & Analysis
Director, Nanoscale Characterisation Centre WA
Director WA nodes:
Australian Microscopy & Microanalysis Research Facility
National Imaging Facility
The University of Western Australia
M018, 35 Stirling Highway, Crawley, WA 6009, Australia
T +61-8-6488 2770 Assistant/ 7112 Direct
M +61-(0)414 239 586
F +61-8-6488 1319
ISI Researcher ID B-2931-2011
From: Ananthavalli Kumarappah <[email protected]>Date: Monday, 6 May 2013 11:45 PMTo: David Sampson <[email protected]>Subject: Permission to use Copyright Material in Masters Thesis
Hello,
I am a University of Toronto graduate student completing my Master’s thesis entitled "Association Between Vigabatrin
Toxicity Identified by ERG and Subsequent Visual Field Reduction”.
My thesis will be available in full-text on the internet for reference, study and / or copy. Except in situations where a
thesis is under embargo or restriction, the electronic version will be accessible through the U of T Libraries web
pages, the Library’s web catalogue, and also through web search engines.I will also be granting Library and Archives

164
Figure 13-1
RE: Permission to use Copyright Material in Masters ThesisMichael Neider [[email protected]]Sent:June 7, 2013 2:23 PMTo: Ananthavalli Kumarappah
Hello Ananthavalli Kumarappah, Thank you for contacting us about the use of this procedure as part of your Master’s thesis. On behalf of the Fundus Photograph Reading Center, we grant you permission to reference the ACCORD Forms, Labeling, Study Conventions,and Imaging Procedure in your thesis. Please include the “ACCORD Eye Study Research Group” in the credit line for use of the procedure. Thank you for your inquiry. We are happy that you might find the procedure to be useful. Michael
Michael Neider, FOPS, BA
Director, Imaging Services | Fundus Photograph Reading CenterDistinguished Researcher - Emeritus
Dept. of Ophthalmology and Visual Sciences | University of Wisconsin -‐ Madison
8010 Excelsior Drive, Suite 100 | Madison, WI 53717 -‐ 1951
phone: (608) 410-‐0628 | email: [email protected] | web: http://eyephoto.ophth.wisc.edu
From: Ananthavalli Kumarappah [mailto:[email protected]] Sent: Monday, June 03, 2013 12:57 PMTo: Michael NeiderSubject: Permission to use Copyright Material in Masters Thesis
Hello,
I am a University of Toronto graduate student completing my Master’s thesis entitled "Association Between Vigabatrin Toxicity Identified by ERG and Subsequent Visual FieldReduction”.
My thesis will be available in full-text on the internet for reference, study and / or copy. Except in situations where a thesis is under embargo or restriction, the electronic version willbe accessible through the U of T Libraries web pages, the Library’s web catalogue, and also through web search engines.I will also be granting Library and Archives Canada andProQuest/UMI a non-exclusive license to reproduce, loan, distribute, or sell single copies of my thesis by any means and in any form or format. These rights will in no way restrictrepublication of the material in any other form by you or by others authorized by you.
I would like permission to allow inclusion of the following material in my thesis: Figure 1 foundon https://www.accordanc.org/secureEYE/docs/general/ACCORD%20Forms,%20Labeling%20Study%20Conventions%20and%20Imaging%20Procedures.pdf%20(Appendices).pdf aswe are using fundus photos for this project. The material will be attributed through a citation.
Please confirm in writing or by email that these arrangements meet with your approval.
SincerelyAnanthavalli Kumarappah

165
Figure 15-1
1/21/2014 Rightslink Printable License
https://s100.copyright.com/AppDispatchServlet 1/5
ELSEVIER LICENSE
TERMS AND CONDITIONS
Jan 21, 2014
This is a License Agreement between Ananthavalli Kumarappah ("You") and Elsevier("Elsevier") provided by Copyright Clearance Center ("CCC"). The license consists of yourorder details, the terms and conditions provided by Elsevier, and the payment terms andconditions.
All payments must be made in full to CCC. For payment instructions, please see
information listed at the bottom of this form.
Supplier Elsevier LimitedThe Boulevard,Langford LaneKidlington,Oxford,OX5 1GB,UK
Registered Company Number 1982084
Customer name Ananthavalli Kumarappah
Customer address 525 University Ave
TORONTO, ON M5G1X8
License number 3313720689005
License date Jan 21, 2014
Licensed content publisher Elsevier
Licensed content publication Ophthalmology
Licensed content title Mapping the visual field to the optic disc in normal tension glaucomaeyes
Licensed content author David F Garway-Heath,Darmalingum Poinoosawmy,Frederick WFitzke,Roger A Hitchings
Licensed content date October 2000
Licensed content volumenumber
107
Licensed content issuenumber
10
Number of pages 7
Start Page 1809
End Page 1815
Type of Use reuse in a thesis/dissertation
Portion figures/tables/illustrations
Number offigures/tables/illustrations
1
Format both print and electronic
Are you the author of this No

166
1/21/2014 Rightslink Printable License
https://s100.copyright.com/AppDispatchServlet 2/5
Elsevier article?
Will you be translating? No
Title of yourthesis/dissertation
Association between vigabatrin toxicity identified by ERG andsubsequent visual field reduction
Expected completion date Jan 2014
Estimated size (number ofpages)
100
Elsevier VAT number GB 494 6272 12
Permissions price 0.00 USD
VAT/Local Sales Tax 0.00 USD / 0.00 GBP
Total 0.00 USD
Terms and Conditions
INTRODUCTION
1. The publisher for this copyrighted material is Elsevier. By clicking "accept" in connectionwith completing this licensing transaction, you agree that the following terms and conditionsapply to this transaction (along with the Billing and Payment terms and conditions establishedby Copyright Clearance Center, Inc. ("CCC"), at the time that you opened your Rightslinkaccount and that are available at any time at http://myaccount.copyright.com).
GENERAL TERMS
2. Elsevier hereby grants you permission to reproduce the aforementioned material subject tothe terms and conditions indicated.
3. Acknowledgement: If any part of the material to be used (for example, figures) hasappeared in our publication with credit or acknowledgement to another source, permissionmust also be sought from that source. If such permission is not obtained then that material maynot be included in your publication/copies. Suitable acknowledgement to the source must bemade, either as a footnote or in a reference list at the end of your publication, as follows:
“Reprinted from Publication title, Vol /edition number, Author(s), Title of article / title ofchapter, Pages No., Copyright (Year), with permission from Elsevier [OR APPLICABLESOCIETY COPYRIGHT OWNER].” Also Lancet special credit - “Reprinted from TheLancet, Vol. number, Author(s), Title of article, Pages No., Copyright (Year), with permissionfrom Elsevier.”
4. Reproduction of this material is confined to the purpose and/or media for which permissionis hereby given.
5. Altering/Modifying Material: Not Permitted. However figures and illustrations may bealtered/adapted minimally to serve your work. Any other abbreviations, additions, deletionsand/or any other alterations shall be made only with prior written authorization of Elsevier Ltd.(Please contact Elsevier at [email protected])
6. If the permission fee for the requested use of our material is waived in this instance, pleasebe advised that your future requests for Elsevier materials may attract a fee.

167
1/21/2014 Rightslink Printable License
https://s100.copyright.com/AppDispatchServlet 3/5
7. Reservation of Rights: Publisher reserves all rights not specifically granted in the
combination of (i) the license details provided by you and accepted in the course of this
licensing transaction, (ii) these terms and conditions and (iii) CCC's Billing and Payment terms
and conditions.
8. License Contingent Upon Payment: While you may exercise the rights licensed immediately
upon issuance of the license at the end of the licensing process for the transaction, provided
that you have disclosed complete and accurate details of your proposed use, no license is
finally effective unless and until full payment is received from you (either by publisher or by
CCC) as provided in CCC's Billing and Payment terms and conditions. If full payment is not
received on a timely basis, then any license preliminarily granted shall be deemed
automatically revoked and shall be void as if never granted. Further, in the event that you
breach any of these terms and conditions or any of CCC's Billing and Payment terms and
conditions, the license is automatically revoked and shall be void as if never granted. Use of
materials as described in a revoked license, as well as any use of the materials beyond the
scope of an unrevoked license, may constitute copyright infringement and publisher reserves
the right to take any and all action to protect its copyright in the materials.
9. Warranties: Publisher makes no representations or warranties with respect to the licensed
material.
10. Indemnity: You hereby indemnify and agree to hold harmless publisher and CCC, and
their respective officers, directors, employees and agents, from and against any and all claims
arising out of your use of the licensed material other than as specifically authorized pursuant to
this license.
11. No Transfer of License: This license is personal to you and may not be sublicensed,
assigned, or transferred by you to any other person without publisher's written permission.
12. No Amendment Except in Writing: This license may not be amended except in a writing
signed by both parties (or, in the case of publisher, by CCC on publisher's behalf).
13. Objection to Contrary Terms: Publisher hereby objects to any terms contained in any
purchase order, acknowledgment, check endorsement or other writing prepared by you, which
terms are inconsistent with these terms and conditions or CCC's Billing and Payment terms
and conditions. These terms and conditions, together with CCC's Billing and Payment terms
and conditions (which are incorporated herein), comprise the entire agreement between you
and publisher (and CCC) concerning this licensing transaction. In the event of any conflict
between your obligations established by these terms and conditions and those established by
CCC's Billing and Payment terms and conditions, these terms and conditions shall control.
14. Revocation: Elsevier or Copyright Clearance Center may deny the permissions described
in this License at their sole discretion, for any reason or no reason, with a full refund payable
to you. Notice of such denial will be made using the contact information provided by you.
Failure to receive such notice will not alter or invalidate the denial. In no event will Elsevier
or Copyright Clearance Center be responsible or liable for any costs, expenses or damage
incurred by you as a result of a denial of your permission request, other than a refund of the
amount(s) paid by you to Elsevier and/or Copyright Clearance Center for denied permissions.
LIMITED LICENSE
The following terms and conditions apply only to specific license types:

168
1/21/2014 Rightslink Printable License
https://s100.copyright.com/AppDispatchServlet 4/5
15. Translation: This permission is granted for non-exclusive world English rights onlyunless your license was granted for translation rights. If you licensed translation rights youmay only translate this content into the languages you requested. A professional translatormust perform all translations and reproduce the content word for word preserving the integrityof the article. If this license is to re-use 1 or 2 figures then permission is granted for non-exclusive world rights in all languages.
16. Website: The following terms and conditions apply to electronic reserve and authorwebsites:Electronic reserve: If licensed material is to be posted to website, the web site is to bepassword-protected and made available only to bona fide students registered on a relevantcourse if:This license was made in connection with a course,This permission is granted for 1 year only. You may obtain a license for future websiteposting, All content posted to the web site must maintain the copyright information line on the bottomof each image, A hyper-text must be included to the Homepage of the journal from which you are licensing athttp://www.sciencedirect.com/science/journal/xxxxx or the Elsevier homepage for books athttp://www.elsevier.com , andCentral Storage: This license does not include permission for a scanned version of the materialto be stored in a central repository such as that provided by Heron/XanEdu.
17. Author website for journals with the following additional clauses:
All content posted to the web site must maintain the copyright information line on the bottomof each image, and the permission granted is limited to the personal version of your paper.You are not allowed to download and post the published electronic version of your article(whether PDF or HTML, proof or final version), nor may you scan the printed edition tocreate an electronic version. A hyper-text must be included to the Homepage of the journalfrom which you are licensing at http://www.sciencedirect.com/science/journal/xxxxx . As partof our normal production process, you will receive an e-mail notice when your article appearson Elsevier’s online service ScienceDirect (www.sciencedirect.com). That e-mail will includethe article’s Digital Object Identifier (DOI). This number provides the electronic link to thepublished article and should be included in the posting of your personal version. We ask thatyou wait until you receive this e-mail and have the DOI to do any posting.
Central Storage: This license does not include permission for a scanned version of the materialto be stored in a central repository such as that provided by Heron/XanEdu.
18. Author website for books with the following additional clauses: Authors are permitted to place a brief summary of their work online only.A hyper-text must be included to the Elsevier homepage at http://www.elsevier.com . Allcontent posted to the web site must maintain the copyright information line on the bottom ofeach image. You are not allowed to download and post the published electronic version ofyour chapter, nor may you scan the printed edition to create an electronic version.
Central Storage: This license does not include permission for a scanned version of the materialto be stored in a central repository such as that provided by Heron/XanEdu.
19. Website (regular and for author): A hyper-text must be included to the Homepage of the

169
!
1/21/2014 Rightslink Printable License
https://s100.copyright.com/AppDispatchServlet 5/5
journal from which you are licensing at http://www.sciencedirect.com/science/journal/xxxxx. or for books to the Elsevier homepage at http://www.elsevier.com
20. Thesis/Dissertation: If your license is for use in a thesis/dissertation your thesis may besubmitted to your institution in either print or electronic form. Should your thesis be publishedcommercially, please reapply for permission. These requirements include permission for theLibrary and Archives of Canada to supply single copies, on demand, of the complete thesisand include permission for UMI to supply single copies, on demand, of the complete thesis.Should your thesis be published commercially, please reapply for permission.
21. Other Conditions:
v1.6
If you would like to pay for this license now, please remit this license along with yourpayment made payable to "COPYRIGHT CLEARANCE CENTER" otherwise you will beinvoiced within 48 hours of the license date. Payment should be in the form of a checkor money order referencing your account number and this invoice numberRLNK501207122.Once you receive your invoice for this order, you may pay your invoice by credit card.Please follow instructions provided at that time.
Make Payment To:Copyright Clearance CenterDept 001P.O. Box 843006Boston, MA 02284-3006
For suggestions or comments regarding this order, contact RightsLink CustomerSupport: [email protected] or +1-877-622-5543 (toll free in the US) or +1-978-646-2777.
Gratis licenses (referencing $0 in the Total field) are free. Please retain this printablelicense for your reference. No payment is required.