Embed Size (px)
Citation preview
ASSOCIATION OFPAEDIATRICCHARTERED
PHYSIOTHERAPISTS
ISSUENO. 115JUNE 2005
CONFERENCE EDITION
In this issue :
Consent – the Welsh Vision
Perceived Efficacy and Goal Setting Systems
Choice – Theory and Practical Application
Collaborative Practices in the Community
The Hopes and Choices of Parents
Questionnaire Survey – Treatment Principles Used in the Management
Of Cerebral Palsy
JUNE 2005A.P.C.P. JOURNAL A.P.C.P. JOURNAL
NATIONAL COMMITTEE OFFICERS AND MEMBERS REGIONAL & SUB-GROUP REPRESENTATIVES
JUNE 2005
EAST ANGLIA LONDON SCOTLAND
Sue Coombe Stephanie Cawker Alison GilmourJenny Lind Physiotherapy Dept. The Wolfson Centre Graysmill SchoolNorfolk & Norwich University Mecklenburgh Square 1 Redhall House DriveHospital LONDON CraiglockhartColney WC1N 2AP EDINBURGHNORWICH NR4 7UZ [email protected] [email protected]@nnuh.nhs.uk
SOUTH WEST SOUTH EAST WALES
Lynda New Ann Martin Jill WilliamsPhysiotherapy Dept Physiotherapy Dept Physiotherapy DeptMilestone School Childrens Therapy Centre The Hollies Special SchoolLonford Lane Goldie Leigh PentwynGLOUCESTER GL2 9EU LODGE HILL SE2 0AY [email protected] [email protected]
NORTH WEST TRENT NORTHERN IRELAND
Elaine Lloyd Claire Hill Felicity DicksonPhysiotherapy Dept Physiotherapy Dept Scrabo Children’s CentreBooth Hall Children’s Hospital Sheffield Children’s Hospital Ards Community HospitalCharlston Rd Blackley Western Bank Church StreetMANCHESTER SHEFFIELD NEWTONARDSM9 7AA S10 2 TH BT23 4AS N. [email protected] [email protected] [email protected]
WEST MIDLANDS NORTH EAST OVERSEAS
Lindsay Rae Mary Harrison Public RelationsPhysiotherapy Dept. 11 Whitsundale Close OfficerThe Children’s Hospital KNARESBOROUGHSteelhouse Lane N YorkshireBIRMINGHAM B4 6NH HG5 [email protected] [email protected]
NEONATAL CARE GROUP CRITICAL CARE GROUP
Barbara Haederle Rachel HuftonSJUH Physiotherapy DeptChild Development Centre Royal Manchester Children’s HospitalBeckett Street Hospital Road, PendleburyLEEDS LS7 MANCHESTER M24 [email protected]
CHAIRMAN Lesley Smith Physiotherapy DeptRoyal Hospital for Sick ChildrenYork Hill NHS Trust Dalnair StGLASGOW G3 8 SJ [email protected]
VICE-CHAIRMAN Peta Smith Physiotherapy DeptMary Sheridan Centre43 New Dover RdCANTERBURY CT1 3AT [email protected]
SECRETARY Laura Wiggins 26 Braidpark DriveGiffnockGLASGOW G46 6NB [email protected]
TREASURER Fiona Down 5 Home Farm CloseHiltonHUNTINGDONCambs PE28 9QW [email protected]
PUBLIC RELATIONS Gill Holmes Child Development CentreOFFICER Alder Hey Children’s Hospital
Eaton Rd LIVERPOOL L12 2AP [email protected]
VICE PUBLIC Lindsay Rae Physiotherapy Dept.RELATIONS OFFICER The Children’s Hospital
Steelhouse LaneBIRMINGHAM B4 6NH [email protected]
EDUCATION Adele Leake Snr Lecturer in Physiotherapy OFFICER School of Health & Social Care
Collegiate Crescent CampusSheffield Hallam UniversitySHEFFIELD S10 2BT [email protected]
PUBLICATIONS Lorna Stybelska Paediatric Physiotherapy DeptOFFICER Cumberland Infirmary
CARLISLECumbria CA2 4HY [email protected]
MEMBERSHIP Susan Cleverely Physiotherapy DeptSECRETARY Orchard House
9 College RoadCHICHESTER PO19 6PQ [email protected]
EDITOR Sally Braithwaite 531 Church RdYardleyBirmingham B33 8PG [email protected]
RESEARCH Jeanne Hartley Physiotherapy DeptOFFICER Great Ormond St Hospital
LONDON WC1N 3JH [email protected]
CIG LIAISON Linda Fisher Special Educational Needs & OFFICER Psychology Service
SE Essex Area Education OfficeThe KnaresBASILDON SS16 5RX [email protected]
DIVERSITY Sue Coombe Jenny Lind Physiotherapy DeptOFFICER Norfolk & Norwich University Hospital
Colney NORWICHNorfolk NR4 7 UZ [email protected]
Committee Members Christine Shaw 42 Cammo GroveEDINBURGHEH4 8EX [email protected]
Sarah Crombie 10a Record RoadEmsworthHants PO10 7NS [email protected]

1 A.P.C.P. JOURNALJUNE 2005
JOURNAL OF THE ASSOCIATION OF PAEDIATRIC CHARTERED PHYSIOTHERAPISTSNUMBER 115 JUNE 2005
Editorial . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Letters to the Editor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
ARTICLESConference Edition
Consent – the Welsh VisionGeraldine Hastings LLM BSc (Hons) MCSP. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Perceived Efficacy and Goal Setting SystemsCarolyn Dunford . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Choice – Theory and Practical ApplicationJenny Carroll MA MCSP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Collaborative Practices in the communityElizabeth Atter MCSP. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
The Hopes and Choices of ParentsCaroline and Jemma Leech . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Poster PresentationQuestionnaire Survey – Treatment Principles Used in the Management Of Cerebral Palsy
A L Bendall MCSP and D M Pickering MCSP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
REGULAR FEATURES
APCP Matters. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26Research and Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Regional Reports & Neonatal Clinical Interest Sub-Group Report . . . . . . . . . . . . . . . . . 31APCP Publications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Book Review. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Here and There . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36Courses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37APCP Research Register . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Regional Representatives. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . inside back cover
The Editorial Board does not necessarily agree with opinions expressed in articles andcorrespondence, and does not necessarily endorse courses and equipment advertised

2A.P.C.P. JOURNAL JUNE 2005
Editorial
EDITORIAL BOARD
Sally Braithwaite – Editor Lesley [email protected] [email protected]
Gill Holmes Alison GilmourGill.Holmes@RLCH-TR>nwest.co.uk [email protected]
Felicity Dickson Jill Williamsfelicity@[email protected] [email protected]
Terry [email protected]
My congratulations go to everybody on the WelshConference Committee who worked so hard to puttogether an excellent, relevant and stimulating pro-gramme. You even seemed to stage manage theweather for us, with many delegates making timefor a run or a walk on the beach. This journal con-tains a taste for all of you of some of the excellentlectures that were presented in Swansea. Those ofyou who were not able to make it missed a treat.International lecturers gave interesting perspectivesof some of the research going on in their parts of theworld. Whilst home grown speakers shared theirgreat depths of knowledge both with the practicalworkshops and with lectures that would have stoodwell on any international stage. It was also goodand a timely reminder for us all to hear from ayoung service user and her mother.
I think very often when we are asked to do a talk ora lecture even at a very local level many therapistsfeel more than a little uncomfortable and dauntedby the prospect. They feel that their expertise is clin-ical and that they are happy treating children andworking with families and fellow professionals butto give a lecture that is a totally different skill - a skillthat exposes us to others. However, it is this expo-sure that we as a profession of paediatric physio-therapists need. We are not good at selling our-selves. We do not go out and tell people what we dobest. We no not share our best practice, so that it canbe developed by our fellow professionals in allfields. If you get the opportunity to talk to groups of
service users, older school children, other profes-sions and members of your team or service – take itwith both hands and use it to promote paediatricphysiotherapy.
It is a also good plan to look for feed back from anytalk or lecture you give. Don’t take the negativethings as a personal criticism but rather tuck themaway to use as a starting point when next you exam-ine how it might be possible for you or your serviceto change practice. They might just provide youwith a grain of an idea for doing something a littledifferently and occasionally point out a very glaringsituation that needs addressing. Criticism is onlydestructive if it is taken or given in a negative way.If some comes in your direction, take it and try anduse it positively.
Finally, on a different note, Congress with the CSPwill be with us in October and APCP will be runninga day of lectures on the Friday. So don’t miss yourchance, come along and take the opportunity tomeet some of your APCP colleagues, network andshare ideas. It can be great fun as well as informa-tive and is often a chance to meet old friends andpeople that you haven’t seen for a long time. Ofcourse this year you will even have the opportunityto meet people that have not followed the same spe-cialist career path as your self. I look forward tomeeting some of you there. It is always really goodto be able to put a face to a name that has only everexisted for me at the end of a telephone, letter oremail.
Sally Braithwaite

3 A.P.C.P. JOURNALJUNE 2005
Letters
Jane Hudson,Marion Sleath,Angela Gregory, Fenella Barnes, Paediatric PhysiotherapyService,St Helen’s House,571 Foxhall Road,Ipswich, Suffolk IP3 8LXTel: 01473 275520Fax: 01473 275575Email: [email protected]
Dear Sally,
We are a small group of Physiotherapists and Physiotherapy Assistantsworking in a school for physically disabled children from nursery to 19 yearsof age.
Due to staff change and increased number of children to treat, the type ofPhysiotherapy treatment given to the children has to change from the more‘hands on’ type of treatment to setting up of individual managementprogrammes to be incorporated into all aspects of daily life.
This has already been implemented to a certain extent in the lower school butat present in the upper school, it is still very much the Physiotherapists doingthe therapy and the Teachers doing the teaching.
In order to provide an efficient integrated Physiotherapy managementprogramme for each child, as a team,we have to be able to work with bothTeachers and Parents. We would therefore be very interested to hear fromany other school based Physiotherapist who has recently had experience ofimplementing a Physiotherapy management programme in senior school forphysically disabled children.
Yours sincerely,Jane Hudson, Senior 1 Paediatric PhysiotherapistMarion Sleath, Senior 2 Paediatric PhysiotherapistAngela Gregory, Physiotherapy AssistantFenella Barnes, Physiotherapy Assistant
Nkem Anagor McspBodyworks PhysiotherapyLimitedCorrespondent25 Eynham Road,PO Box 48348London W12 0WHTel. 07968 614643Email: [email protected]: bodyworksphysiotherapy.co.uk
Dear Sally
I’m writing to make a general call to my colleagues in the field of paediatrics,who are practicing in the London area.
I myself have been working in paediatrics for over 10 years now and itwould be true to say that the path of my career has been “atypical”.However, this has, overtime, proven to be a blessing and I am nowsufficiently confident in the approaches I have developed in the treatment ofmovement dysfunction (first in children with physical disabilities ofneurological origin and in latter times, in the treatment of mainstream(muscular-skeletal) complains in adults), to now seek to work in partnershipwith fellow physiotherapists.
I have specifically chosen to make my initial appeal to my colleagues inpaediatrics, because I believe that knowledge of the origins and developmentof “healthy” or “normal” movement is essential for successful rehabilitationof movement dysfunction - at whatever age or time of life the dysfunctionmay occur. This view has led me to coin the term Movement Rehabilitationto best describe my approach and physiotherapeutic response to dysfunctionand disability.
I am not at the moment making any specific offer, but I am keen to open upa forum of discussion and practical exchange with like-minded colleagues.I’m seeking to hear from any APCP member who has retained interest intreating adult musculo-skeletal complaints, who have some interest incomplementary health techniques and who has a personal interest in thepractice of yoga or a marital art.
Intrigued? Fit the bill? Please do contact me at: [email protected]
SincerelyNkem Anagor Mcsp
4A.P.C.P. JOURNAL JUNE 2005
Letters
Copy for the
SEPTEMBER 2005 JOURNALmust be with the editor by
1st AUGUST 2005
The editorial board reserve the right to edit all material submitted
Stephanie SwainChildren’s CentreCanolfan i BlantSt. David’s HospitalCowbridge Road EastCantonCardiffCF11 9XBPhone 029 2053 6789Fax 029 2053 6779
Dear Sally
I am a Community Paediatric Physiotherapist working with a 3 year oldwith paraplegia. I would like some advice from other members who haveworked with a young child with spinal cord injury and could answer one ormore of my queries:-
1. Can anyone recommend a rehabilitation centre that works with suchyoung children?
2. What orthotics have been used to promote independent mobility andhow successful were they (this child’s recovery has plateaued atL3/4)?
3. Are there any rehabilitation programmes that physiotherapists haveused?
Please reply to me at the address, telephone or fax shown above or via emailat [email protected]
Many thanks
Yours sincerelyStephanie SwainSenior 1 Community Paediatric Physiotherapist

5 A.P.C.P. JOURNALJUNE 2005
SEQ
UI
C
HA
RTER
ED
SO
CIET
Y
OF PH
YSIOTH
ERA
PY
DIG
NA
A.P.C.P.ConferenceWales 2005
held atSwansea University
Thursday 31st March 2005to
Saturday 2nd April 2005
A Taste of Conference for All to Share

6A.P.C.P. JOURNAL JUNE 2005
CCoonnsseenntt -- tthhee WWeellsshh VViissiioonn
Introduction
The CSP Core Standards (CSP, 2005) and Rules ofProfessional Conduct (CSP, 2002) places an obliga-tion on physiotherapists to seek their patient’sinformed consent for all interventions. Therefore,informed consent is pivotal in the physiotherapists’relationship with their patients. For paediatric phys-iotherapists, informed consent raises issues of confi-dentiality and consent to treatment, all of whichmust be dealt with in a format and language under-stood by the child, young person and their family.
The literature has identified various elements to theinformed consent process (see above)1. These ele-ments are more complex when applied to childrenand young people. Information is an important partof the patient journey and a key element in theinformed consent process and overall quality ofpatient experience. Improving consent proceduresand providing better information for patients was acommitment in the NHS Plan (2000) and part of therecommendations of the Kennedy report into theBristol Royal Infirmary (2001). There is also moreevidence of the importance of information forpatients provided in the Welsh AssemblyGovernment’s publication ‘Good practice in consentimplementation guide’ (WAG, 2002). Therefore, infor-mation for decision-making across the NHS hasneeded to be improved. Welsh paediatric physio-therapists are committed to improving communica-tion with and the quality of information for theirpatients and carers alike. Sharing information bringsthe principles of consent and confidentiality togeth-er, by informing, protecting and providing choicefor the patient. Welsh APCP members are currentlypiloting work on consent and information sharing;the history, objectives and progress of which are out-lined below.
Where it began
Since 2003, the author and the CSP Policy Officer forWales have co-facilitated the Consent Subgroup ofthe CSP Wales Paediatric Physiotherapy Network.The purpose of this group has been to develop an
Geraldine Hastings, LL.M. BSc (Hons) MCSPDepartment of Physiotherapy, School ofHealthcare Studies, Cardiff UniversityTy Dewi Sant, Heath Park, Cardiff CF14 4XW
ComprehensionDisclosure Voluntariness Competence
Information Consent
Informed Consent
All Wales paediatric physiotherapy strategy for theclinical implementation of the “Reference Guide toConsent for Examination or Treatment” (WAG, 2002).Prior to the publication of this guidance, Hastings(2001) conducted a survey investigating how paedi-atric physiotherapists in South Wales dealt with con-sent to and refusal of treatment in clinical practice.The findings reported that although there was evi-dence of good practice, particularly in relation torefusal situations, the area of practice whichrequired improvement was the actual ‘how andwhen’ aspects of obtaining consent from childpatients. There were also a number of political driv-ers which gave momentum to the project.
Political Drivers
Firstly, Devolution and the establishment of theWelsh Assembly Government (WAG) in 1999 lead tojob creation - the CSP Policy Officer for Wales. Thisin turn led to the formation of the CSP WalesPaediatric Physiotherapy Network. The purpose ofthis group was to assist with responses to relevantWelsh Assembly policy on behalf of the CSP Wales.
Secondly, the Welsh Assembly Government hadimplemented a programme ‘Children First’, toimprove the quality of health and social services forchildren in particular those in care. These changeswere brought about by the publication of theWaterhouse Report ‘Lost in Care’ (2000), an investi-gation into child abuse in North Wales care homes.As a result, safeguarding the physical health andmental well-being of all children had become a toppriority for governments across the UK. The reportalso paved the way for the appointment of the firstChildren’s Commissioner for Wales.
As mentioned earlier improving information forpatients including children was a commitment inthe NHS Plan (2000) and one of the recommenda-tions of the Kennedy Report (2001). In 2001, theWelsh Assembly Government published the ‘Goodpractice in consent implementation guide’, which wasdeveloped in response to the Kennedy Report, withthe aim of assisting NHS organisations to promotegood practice in the way patients are asked to givetheir consent to treatment, care or research (WAG,2001).
The Carlile Review (March 2002) commissioned inresponse to ‘Lost in Care’ and the Review of Services forChildren with Special Needs gave paediatric physio-therapists in Wales an opportunity to highlight theissues of consent, child protection, and the provisionof information to children/parents/carers.Government ministers heard of the poor facilitiesand access to information for those with visual andlearning disabilities; those in need of translationfacilities including into Welsh medium. In conjunc-tion, there was also the issue of poor access for staffto appropriate IT and printing support to produceacceptable standard information; and also the poor
1 Faden R & Beauchamp T L (1986) A History and Theory of InformedConsent New York: Oxford University Press

7 A.P.C.P. JOURNALJUNE 2005
Consent - the Welsh Version
quality assurance monitoring and audit of informa-tion produced. In 2004, response to the SafeguardingVulnerable Children Report gave paediatric physio-therapists another opportunity to stress the impor-tance of communication and information sharingbetween professionals in the public and private sec-tors.
Reasons for Sharing Information
The overall aim of the project is to improve theinformed consent process and share informationabout treatment modalities and activities through-out Wales, a view supported by the Welsh AssemblyGovernment in their ‘Informing Healthcare’ frame-work (WAG, 2003). The framework discusses thesignificant opportunities and benefits for healthcareprofessionals in general if they are able to communi-cate and share documents, messages and imageseasily regardless of location along with the ability toaccess information from a wide range of sources.The group also considered that sharing informationwould establish ‘best practice’ and in turn improvethe provision and quality of paediatric physiothera-py services, as generally, resources are limited interms of both time and finance. In addition, manypaediatric physiotherapists are isolated working inrural communities. Consequently, sharing informa-tion would help the difficulties these physiothera-pists have in keeping up to date with clinical devel-opments. The sub group is also conscious of com-munication difficulties between paediatric physio-therapists in North and South Wales thus are keen toimprove these relationships. There is also a need forinformation to be available in Welsh medium withinthe NHS (Welsh Language Act, 1993). Although theCSP is not a statutory organisation and thus is notobliged to provide bilingual information, its’ mem-bers work in the NHS. It is good practice as a resultfor members to endeavour to do so. Another impor-tant indeed crucial reason for sharing information isto improve the overall quality of the child or youngperson’s health care experience, to provide thepatient with a choice and empower them to have a‘voice’.
The emerging objectives of the sub group were to:
1. Develop written guidance and training pack-age around issues of informed consent in Wales.
2. Develop standardised therapy information leaflets to assist the informed consent process.
3. Standardise consent forms where possible in accordance with Welsh Assembly Government policy.
Consent Guidance Implementation Issues
The new consent to treatment forms were intro-duced in April 2002, with each NHS Trust adoptingthe model consent to treatment policy into their pro-cedures by October 2002. The feedback from paedi-atric physiotherapists was that they considered thenew forms unfriendly particularly for children andyoung people. Some trusts in Wales allowed alterna-tives to be developed so long as they adhered to thenew guidance, whereas, others insisted on adoptingthe WAG forms. Obviously, there is a contractualobligation for all paediatric physiotherapists asemployees to follow Trust policy; however, it is stillnecessary to be fully conversant with what is expect-ed during the process especially with such compli-cated forms. The subgroup identified education andtraining needs on such matters as how to use con-sent forms appropriately, clarification of issues suchas legal requirements, parental responsibility andrefusal of treatment. It was felt that training could becascaded down from within the group over time inaddition to any courses staff attended. Therefore, theworking party considered that on completion theconsent and sharing information project wouldenhance any Trust/LHB guidance and policy.
Standardisation of consent forms and information
The sub group agreed that where possible consentforms should be standardised. It considered that theexisting work in Gwent Healthcare Trust should bethe model for a standardised approach to consentfor examination and/or treatment by paediatricphysiotherapists across Wales. The sub group alsoagreed that in most instances verbal consent wasadequate. However, some treatment modalities andactivities were identified to require further riskassessment. Those areas identified were ReboundTherapy, Riding for the Disabled, Electrotherapy,Postural Support, Botulinum toxin,Orthotics/Casting, Respiratory Care, Orthopaedics,Exercise therapy, Water-based activity/hydrothera-py, Mobility – including use of equipment andVideo/Photography. It was felt that these treatmentmodalities and activities would require moredetailed information for children, young people andtheir families in order to gain consent. It was agreedthat the development of standardised information,for example, leaflets, videos and CD ROMs on an AllWales basis would be valuable, so the subgroupembarked on the mission of information gatheringand sharing. A survey was undertaken across Walesto establish common ground on risk assessmentareas and gather information leaflets, videos etc.There was an excellent response from 80% of thosesurveyed. A gap analysis revealed a variety of infor-mation being used for different therapeutic inter-ventions, with not much duplication in terms ofinformation resources available; however, it becameevident that many departments had little or noresources. Although the survey was highly success-

8A.P.C.P. JOURNAL JUNE 2005
ful there were also restrictions to the groups’ effortsas they had simultaneously written to Local HealthAuthorities and Local Health Boards to enquireabout their policies on sharing information. Onceagain, there was a good response rate but it becameapparent that these agencies differed in structure,culture and management. Consequently, some werewilling to allow sharing of information resourcesand some were not.
Work in Progress
Currently the subgroup has decided to adopt theGwent Healthcare Trust consent model as the stan-dardised format for the informed consent process. Itis also attempting to reduce the numbers of differentconsent forms being used across Wales by highlight-ing the specific therapeutic requirements of paedi-atric physiotherapists. The subgroup will establishlocal clinical interest groups to evaluate the informa-tion leaflets gathered in the survey and standardisewhere possible. Then templates will be uploaded tothe APCP Wales website and the iCSP Wales webpage to increase access for all paediatric physiother-apists. It is hoped that this work will feed into APCPNational Executive Committees plans for informedconsent guidance for all APCP members.
References1. The Chartered Society of Physiotherapy (2005)
Core Standards London: CSP
2. The Chartered Society of Physiotherapy (2002)Rules of Professional Conduct London: CSP
3. Faden R & Beauchamp T L (1986)A History and Theory of Informed ConsentNew York: Oxford University Press
4. Welsh Assembly Government (2001)The NHS Plan: Improving Health in Wales - A Plan for the NHS with its PartnersCardiff, National Assembly for WalesAvailable online atwww.wales.nhs.uk/Publications/NHSStrategydoc.pdf
5. Kennedy I. Howard R. Jarman B. MacLean M.(2001)Learning from Bristol: The Report of the PublicInquiry into children’s heart surgery at theBristol Royal Infirmary 1984-1995 London: Stationery OfficeAvailable online at www.bristol-inquiry.org.uk
Consent - the Welsh Version 6. Welsh Assembly Government (2001)Reference Guide to Consent for Examination orTreatment Available online at www.wales.nhs.uk
7. ‘Lost in Care’: Tribunal of Inquiry into Child Abusein North Wales Great Britain Welsh Office (2000)London: Stationery Office
8. Hastings G (2001)Bending your arm: refusal of physiotherapy interven-tion in adolescence (LL.M Dissertation, University of Bristol:Faculty of Law)
9. Carlile A. et al (2001) The Review of Safeguards forChildren and Young People treated and cared for bythe NHS in Wales – “Too Serious a Thing”Cardiff, National Assembly for Wales Available online at www.wales.gov.uk/subi-health/content/keypubs/pdf/safeguards_text-e.pdf
10. Welsh Assembly Government (2002)Health & Social Services Committee Review ofServices for Children with Special Health NeedsAvailable online at www.wales.gov.uk/subi-health
11. Department of Health (2004)National Service Framework for Children,Young People and Maternity Services (The NHS Wales Consultation is availableonline at www.wales.nhs.uk/nsf)
12. Welsh Assembly Government (2004)Safeguarding Vulnerable Children Reviewwww.wales.gov.uk/subichildren
13. Welsh Assembly Government (2003)Informing Healthcare – TransformingHealthcare Using Information and ITwww.wales.nhs.uk/ihc

9 A.P.C.P. JOURNALJUNE 2005
Perceived Efficacy and GoalSetting System
Carolyn DunfordEveswell Children’s CentreSt John’s RoadNewportGwent NP9 8GR
Children’s rights to express their views areenshrined in the United Nations Convention on theRights of the Child and most therapists are willingto listen. The reality is, however, that obtaining theperspective of young children can be very challeng-ing. Parents are a valuable and reliable source ofinformation and, thus, parents are often used asproxies for their children’s views (Glascoe 2000).Research indicates that children and adults oftenhave different priorities for intervention (McGavin1998, Pollock and Stewart 1998). Furthermore, chil-dren and young people have clearly stated a desireto be actively involved in decisions regarding theirhealth and its management (Turner 2003).
Enabling children to voice their views requires care-ful attention to the language used -provision of con-crete stimuli such as pictures and clarity of responseoptions. Young children have been shown to accessphysical competence most accurately.
In order to give valid consent to treatment parentsand children should understand what the treatmentis and why it is being proposed. When children settheir own goals for treatment this is made easier.
Newer methods are required to assist young chil-dren in sharing their perspectives of the impact oftheir disability on daily activities. Careful attentionto the language that is used in the questions, theaddition of concrete stimuli such as pictures, theclarity of the response options and the context forthe assessment can improve the validity of theresults. One instrument that uses these techniquesand enables young children with disabilities to sharetheir perspectives is the Perceived Efficacy and GoalSetting System (PEGS).
The PEGS enables children aged 6-9 years to selfreport their perceived competence in everydayactivities and set goals for intervention. The PEGS isbased on All About Me (Missiuna 1998). It comprisesof 24 cards depicting children performing everydayactivities. It includes self-care, school and leisuretasks. It has a forced choice format and takes about20-30 minutes to administer.
The rationale behind the PEGS is based on theknowledge that family centred services result inpositive outcomes for children and parents/carers.Identifying priorities and desired outcomes for
treatment is a central tenet of family-centred thera-py. Explicit and challenging goals can enhance andsustain motivation. Understanding the child’s per-ceived self-efficacy is a necessary part of the process.
A study of 35 children with developmental coordi-nation disorder (DCD) examined children’s percep-tions of the impact of DCD on activities of daily liv-ing using the PEGS (Dunford, Missiuna, Street andSibert, in press). The children were aged 5-10 years,29 boys and six girls and came from a range of socio-economic backgrounds. All 35 of the children wereclearly able to identify whether they thought theywere “good” or “not good” at performing the 24daily tasks depicted on the PEGS cards and to indi-cate whether the child shown was “a lot” or “a little”like them. The children’s top goals for therapy werebeing better at gross motor sports (riding a bike,playing football), independence in self-care activi-ties (dressing, using cutlery) and schoolwork andhandwriting. Parent and teacher concerns were col-lected via a questionnaire with the question “Whatare your main concerns for this child?” Parents topconcerns were about motor skills, schoolwork,handwriting and attention/concentration skills.Teacher’s top concerns were about handwriting,motor skills and schoolwork.
Presentation of a couple of case histories follows todemonstrate the use of the PEGS. Mark is an eight-year boy who was referred to physiotherapy andoccupational therapy by the educational psycholo-gist because of concerns about his coordination.Assessment with the Movement Assessment Batteryfor Children (Henderson and Sugden) found that histotal impairment score placed him below the firstpercentile. His goals selected using the PEGS were:
Tying shoelaces “cos I can’t do them”Writing neatly “it goes all over the place”Skipping “everyone else can do it”Riding a bike “so I can go on bike not scooter”
Rachel is a 10? year-old girl referred to physiothera-py and occupational therapy by the school healthnurse because of concerns about her coordination.She scored below the first percentile on theMovement Assessment Battery for Children. Usingthe PEGS she identified her goals for therapy as:
Being frustrated by her stammerScissors “I like cutting & making things”Skipping “I would like to join in with myfriends”Running “don’t want to come last”
Using the PEGS has had an impact on service provi-sion in order to be able to treat the goals the childrenwere identifying. Therapy now places a greateremphasis of self-care and leisure activities as well asschool based skills such as writing. Links have beendeveloped with the Sports Development Officer andfootball, rebound and bike skills groups are runjointly with occupational therapists, physiothera-

10A.P.C.P. JOURNAL JUNE 2005
pists and a sports coach. These groups are run inlocal leisure centres. The self-care issues are usuallymost appropriately addressed at home. Therapy hasmoved out of the children’s centre into more appro-priate environments. The PEGS has also led to a dif-ferent therapeutic relationship with the children asthe starting point is to ask them what they wantfrom therapy and then to work on their goals. Thislets the children know that the therapist is listeningto them. Once children’s goals have been met thendischarge is easy, even if the impairment has notchanged, the impact of the impairment has beenreduced.
In conclusion, collaborative goal setting needs toinvolve all participants including the child. Childrenwith DCD share concerns about physical/motorskills, academic activities and pencil skills with theirparents and teachers. However, the children haveadditional concerns about self-care and leisure activ-ities. The PEGS is a suitable tool to enable childrento express their views and set goals for therapy.
Perceived Efficacy and Goal Setting System
11 A.P.C.P. JOURNALJUNE 2005
Choice -Theory and PracticalApplication
Jenny Carroll MA MCSPBobath Children’s Therapy Centre Wales
Choice is the ability to “make a selection” or “tohave or demonstrate a preference”, or “to be able todecide between possibilities” and it is about “havinga right”, “the right to choose” (Concise OxfordDictionary).
In everyday life people make hundreds of choices,whether and when to get up, what to wear, what tohave for breakfast, when, where, with whom to eatit, which bowl to put their cereal in, how much milkto have in their tea, the list goes on and on.
For some children with cerebral palsy however,even such basic choices may not be possible. Somechildren are not able to decide not to have breakfastin the morning perhaps, for example, if they werefeeling unwell or not hungry or they may not be ableto choose to stop eating because they are full up.
Choice is of fundamental importance to us ashumans and how choice is managed is one ofhumanities defining characteristics. Much ofmodern legislation (Children Act 1989 and 2004,Human Rights Act 1998,) encourages therapists toenable children to have choice both in their therapyand their lives. The legislation gives children theright to make choices however, how many childrenwith disabilities are equipped to take advantage ofthese rights? Do physiotherapists have aresponsibility to enable children to make choices(within their personal limits)? Should enablingchoice, in fact, be one of paediatric physiotherapists’major responsibilities?
This paper reviews the role of choice in therapy andconversely the role of therapy in choice.
Why are choices so important?
Choices are a vital part of development. Typicallychildren begin to make choices very early in life andtheir ability to begin making their own choices isfundamental to becoming an independent being andpart of the separation process from their mother.Children can choose to run away, or to throw a toyfrom their high chair, thus facilitating learning aboutspace and their environment. They can choose to eattheir lunch, or not, which bits to eat first, what toleave. This ability develops with an understandingof possibilities and alternatives and of short andlonger term consequence of choices.
For many children with cerebral palsy making thoseearly choices and the initial separation presentsnumerous difficulties and impairment of theirchoice making capacity can begin very early in life.It is perhaps useful to look at all the elementsinvolved in choice making in order to consider thecomplexity and challenges faced.
The factors and processes involved in choice makingare highly complex and interlinked. Choices arebased on knowledge and experience, which isaccessed via our memory. The ability to reframe aconcept is important (Bandler and Grindler 1979and 1982 Sandidge and Ward 1999) and therefore tobe able to consider other possibilities; this requiresadvanced perceptual skills and abstract thought.Cognitive skills are used to help us process choicesand speech to convey them or to explore options.An advanced understanding of concepts of time isalso important in understanding how choices mademay impact on the future. These are high level skillswhich are, in turn, supported by other skills.
These skills, including to be able to attend, thelanguage to understand options and choices and asensory system processing information competentlyare important if the higher level skills are to beattained.
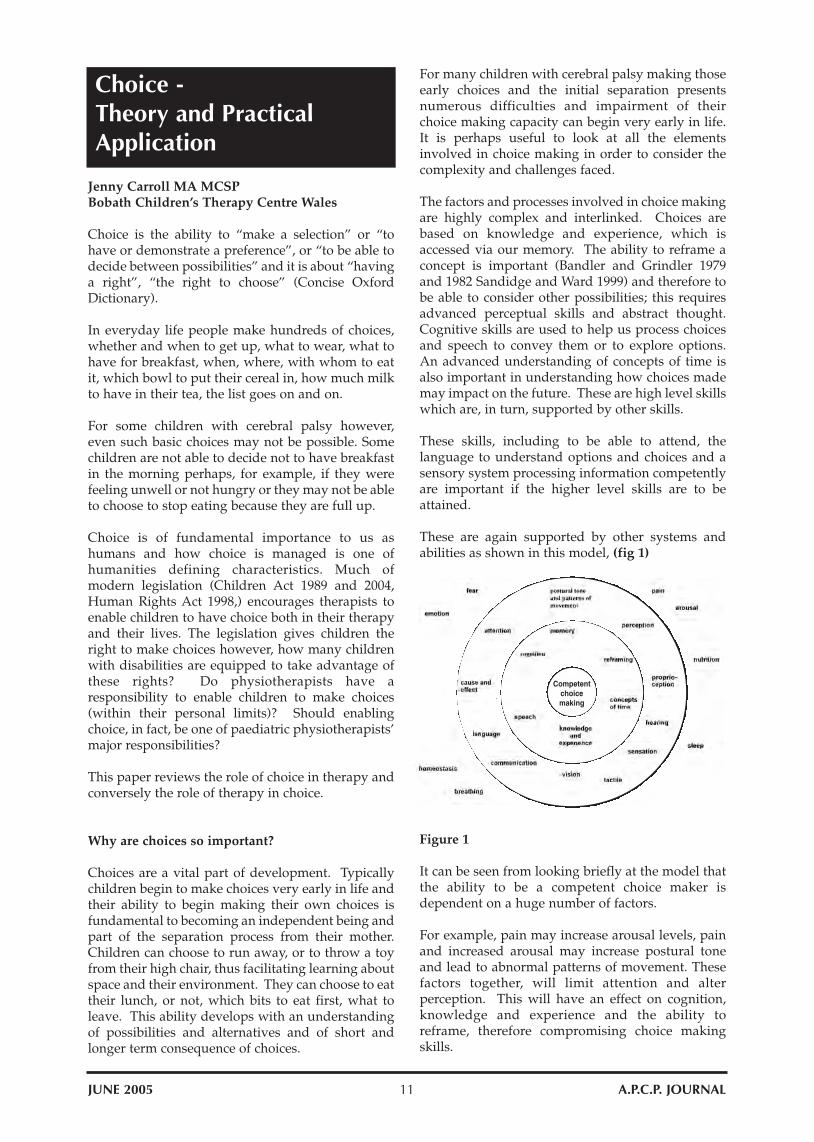
These are again supported by other systems andabilities as shown in this model, (fig 1)
Figure 1
It can be seen from looking briefly at the model thatthe ability to be a competent choice maker isdependent on a huge number of factors.
For example, pain may increase arousal levels, painand increased arousal may increase postural toneand lead to abnormal patterns of movement. Thesefactors together, will limit attention and alterperception. This will have an effect on cognition,knowledge and experience and the ability toreframe, therefore compromising choice makingskills.
Competentchoicemaking
12A.P.C.P. JOURNAL JUNE 2005
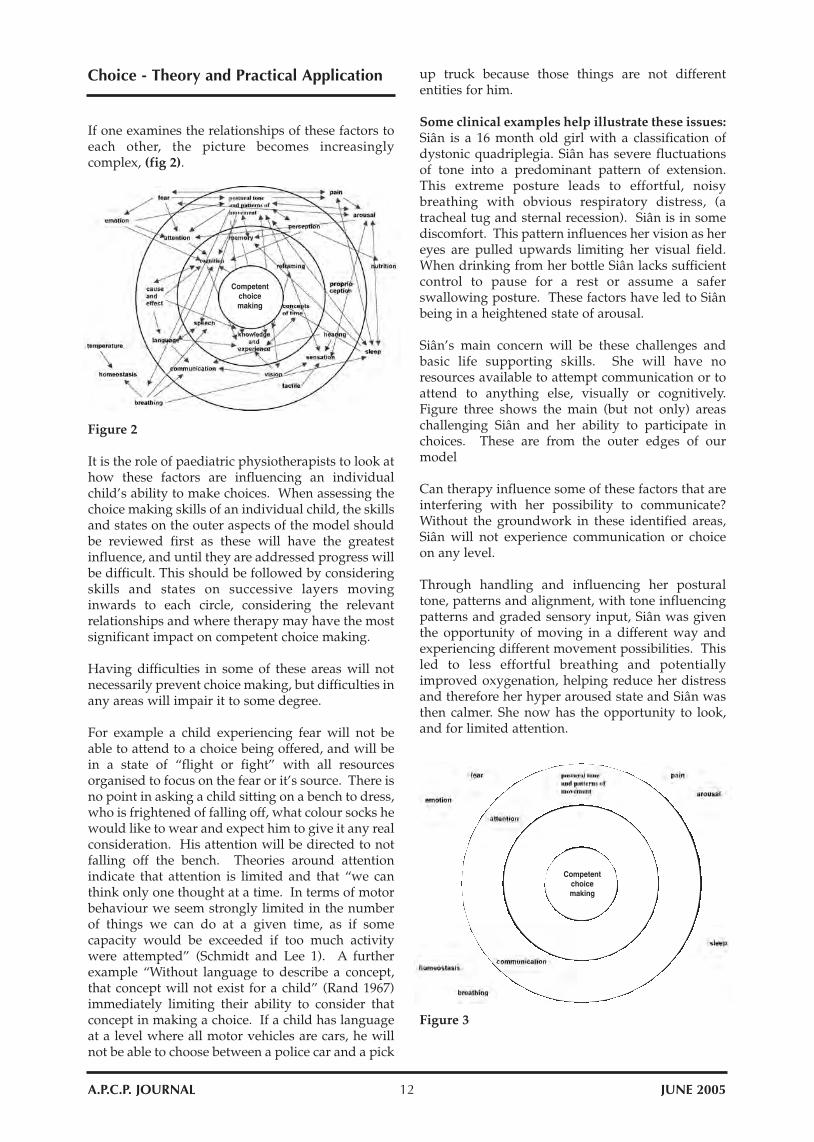
If one examines the relationships of these factors toeach other, the picture becomes increasinglycomplex, (fig 2).
Choice - Theory and Practical Application
Figure 2
It is the role of paediatric physiotherapists to look athow these factors are influencing an individualchild’s ability to make choices. When assessing thechoice making skills of an individual child, the skillsand states on the outer aspects of the model shouldbe reviewed first as these will have the greatestinfluence, and until they are addressed progress willbe difficult. This should be followed by consideringskills and states on successive layers movinginwards to each circle, considering the relevantrelationships and where therapy may have the mostsignificant impact on competent choice making.
Having difficulties in some of these areas will notnecessarily prevent choice making, but difficulties inany areas will impair it to some degree.
For example a child experiencing fear will not beable to attend to a choice being offered, and will bein a state of “flight or fight” with all resourcesorganised to focus on the fear or it’s source. There isno point in asking a child sitting on a bench to dress,who is frightened of falling off, what colour socks hewould like to wear and expect him to give it any realconsideration. His attention will be directed to notfalling off the bench. Theories around attentionindicate that attention is limited and that “we canthink only one thought at a time. In terms of motorbehaviour we seem strongly limited in the numberof things we can do at a given time, as if somecapacity would be exceeded if too much activitywere attempted” (Schmidt and Lee 1). A furtherexample “Without language to describe a concept,that concept will not exist for a child” (Rand 1967)immediately limiting their ability to consider thatconcept in making a choice. If a child has languageat a level where all motor vehicles are cars, he willnot be able to choose between a police car and a pick
up truck because those things are not differententities for him.
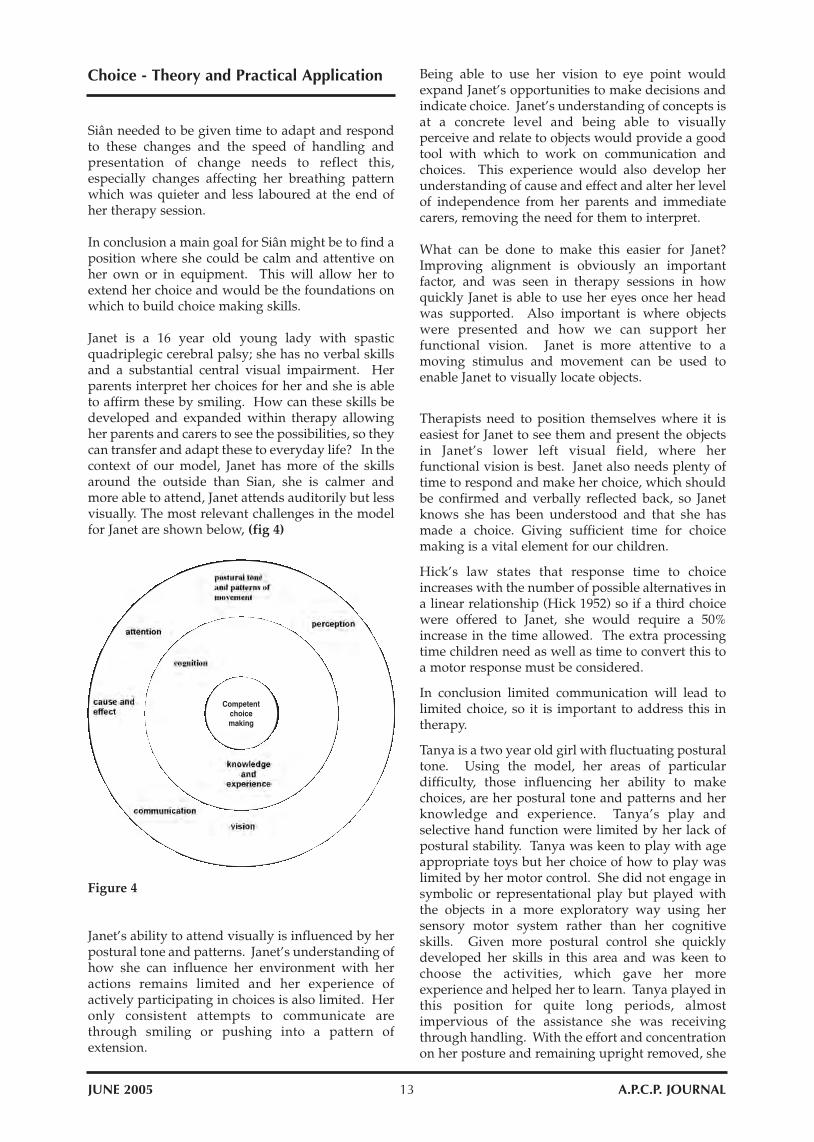
Some clinical examples help illustrate these issues: Siân is a 16 month old girl with a classification ofdystonic quadriplegia. Siân has severe fluctuationsof tone into a predominant pattern of extension.This extreme posture leads to effortful, noisybreathing with obvious respiratory distress, (atracheal tug and sternal recession). Siân is in somediscomfort. This pattern influences her vision as hereyes are pulled upwards limiting her visual field.When drinking from her bottle Siân lacks sufficientcontrol to pause for a rest or assume a saferswallowing posture. These factors have led to Siânbeing in a heightened state of arousal.
Siân’s main concern will be these challenges andbasic life supporting skills. She will have noresources available to attempt communication or toattend to anything else, visually or cognitively.Figure three shows the main (but not only) areaschallenging Siân and her ability to participate inchoices. These are from the outer edges of ourmodel
Can therapy influence some of these factors that areinterfering with her possibility to communicate?Without the groundwork in these identified areas,Siân will not experience communication or choiceon any level.
Through handling and influencing her posturaltone, patterns and alignment, with tone influencingpatterns and graded sensory input, Siân was giventhe opportunity of moving in a different way andexperiencing different movement possibilities. Thisled to less effortful breathing and potentiallyimproved oxygenation, helping reduce her distressand therefore her hyper aroused state and Siân wasthen calmer. She now has the opportunity to look,and for limited attention.
Figure 3
Competentchoicemaking
Competentchoicemaking
13 A.P.C.P. JOURNALJUNE 2005
Choice - Theory and Practical Application
Siân needed to be given time to adapt and respondto these changes and the speed of handling andpresentation of change needs to reflect this,especially changes affecting her breathing patternwhich was quieter and less laboured at the end ofher therapy session.
In conclusion a main goal for Siân might be to find aposition where she could be calm and attentive onher own or in equipment. This will allow her toextend her choice and would be the foundations onwhich to build choice making skills.
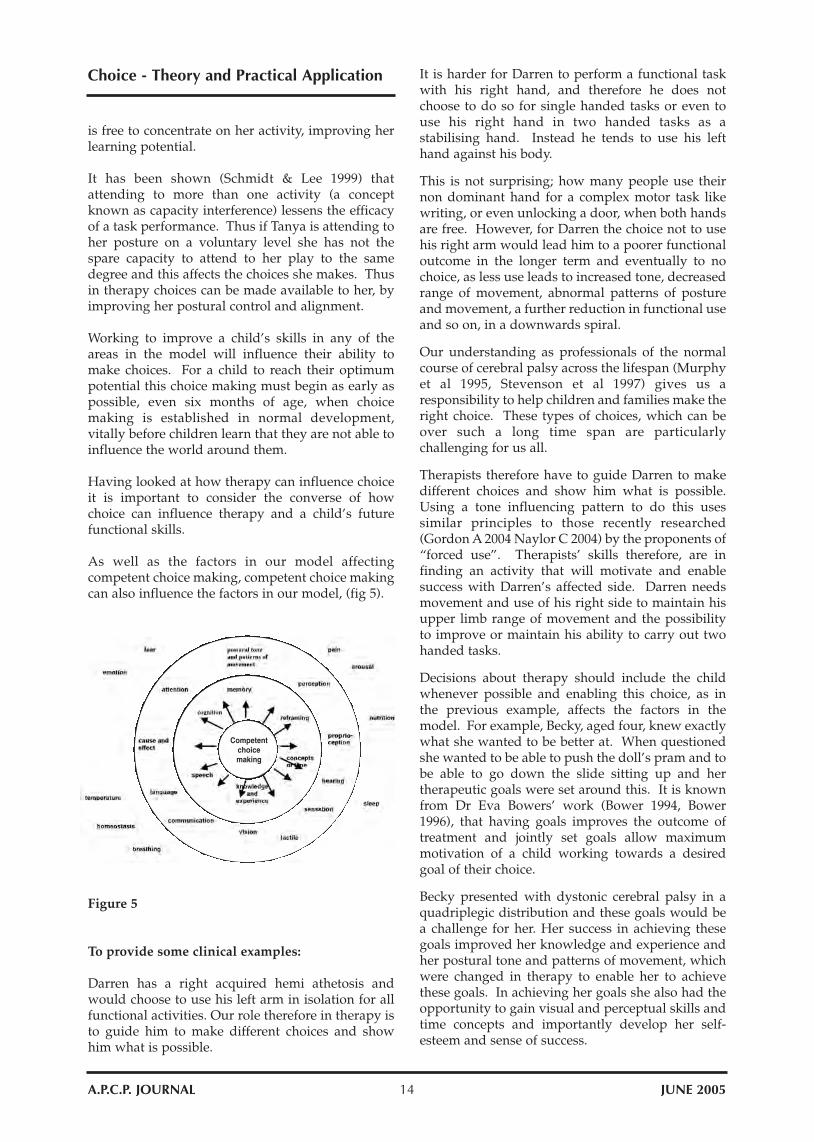
Janet is a 16 year old young lady with spasticquadriplegic cerebral palsy; she has no verbal skillsand a substantial central visual impairment. Herparents interpret her choices for her and she is ableto affirm these by smiling. How can these skills bedeveloped and expanded within therapy allowingher parents and carers to see the possibilities, so theycan transfer and adapt these to everyday life? In thecontext of our model, Janet has more of the skillsaround the outside than Sian, she is calmer andmore able to attend, Janet attends auditorily but lessvisually. The most relevant challenges in the modelfor Janet are shown below, (fig 4)
Figure 4
Janet’s ability to attend visually is influenced by herpostural tone and patterns. Janet’s understanding ofhow she can influence her environment with heractions remains limited and her experience ofactively participating in choices is also limited. Heronly consistent attempts to communicate arethrough smiling or pushing into a pattern ofextension.
Being able to use her vision to eye point wouldexpand Janet’s opportunities to make decisions andindicate choice. Janet’s understanding of concepts isat a concrete level and being able to visuallyperceive and relate to objects would provide a goodtool with which to work on communication andchoices. This experience would also develop herunderstanding of cause and effect and alter her levelof independence from her parents and immediatecarers, removing the need for them to interpret.
What can be done to make this easier for Janet?Improving alignment is obviously an importantfactor, and was seen in therapy sessions in howquickly Janet is able to use her eyes once her headwas supported. Also important is where objectswere presented and how we can support herfunctional vision. Janet is more attentive to amoving stimulus and movement can be used toenable Janet to visually locate objects.
Therapists need to position themselves where it iseasiest for Janet to see them and present the objectsin Janet’s lower left visual field, where herfunctional vision is best. Janet also needs plenty oftime to respond and make her choice, which shouldbe confirmed and verbally reflected back, so Janetknows she has been understood and that she hasmade a choice. Giving sufficient time for choicemaking is a vital element for our children.
Hick’s law states that response time to choiceincreases with the number of possible alternatives ina linear relationship (Hick 1952) so if a third choicewere offered to Janet, she would require a 50%increase in the time allowed. The extra processingtime children need as well as time to convert this toa motor response must be considered.
In conclusion limited communication will lead tolimited choice, so it is important to address this intherapy.
Tanya is a two year old girl with fluctuating posturaltone. Using the model, her areas of particulardifficulty, those influencing her ability to makechoices, are her postural tone and patterns and herknowledge and experience. Tanya’s play andselective hand function were limited by her lack ofpostural stability. Tanya was keen to play with ageappropriate toys but her choice of how to play waslimited by her motor control. She did not engage insymbolic or representational play but played withthe objects in a more exploratory way using hersensory motor system rather than her cognitiveskills. Given more postural control she quicklydeveloped her skills in this area and was keen tochoose the activities, which gave her moreexperience and helped her to learn. Tanya played inthis position for quite long periods, almostimpervious of the assistance she was receivingthrough handling. With the effort and concentrationon her posture and remaining upright removed, she
Competentchoicemaking
14A.P.C.P. JOURNAL JUNE 2005
Choice - Theory and Practical Application
is free to concentrate on her activity, improving herlearning potential.
It has been shown (Schmidt & Lee 1999) thatattending to more than one activity (a conceptknown as capacity interference) lessens the efficacyof a task performance. Thus if Tanya is attending toher posture on a voluntary level she has not thespare capacity to attend to her play to the samedegree and this affects the choices she makes. Thusin therapy choices can be made available to her, byimproving her postural control and alignment.
Working to improve a child’s skills in any of theareas in the model will influence their ability tomake choices. For a child to reach their optimumpotential this choice making must begin as early aspossible, even six months of age, when choicemaking is established in normal development,vitally before children learn that they are not able toinfluence the world around them.
Having looked at how therapy can influence choiceit is important to consider the converse of howchoice can influence therapy and a child’s futurefunctional skills.
As well as the factors in our model affectingcompetent choice making, competent choice makingcan also influence the factors in our model, (fig 5).
Figure 5
To provide some clinical examples:
Darren has a right acquired hemi athetosis andwould choose to use his left arm in isolation for allfunctional activities. Our role therefore in therapy isto guide him to make different choices and showhim what is possible.
It is harder for Darren to perform a functional taskwith his right hand, and therefore he does notchoose to do so for single handed tasks or even touse his right hand in two handed tasks as astabilising hand. Instead he tends to use his lefthand against his body.
This is not surprising; how many people use theirnon dominant hand for a complex motor task likewriting, or even unlocking a door, when both handsare free. However, for Darren the choice not to usehis right arm would lead him to a poorer functionaloutcome in the longer term and eventually to nochoice, as less use leads to increased tone, decreasedrange of movement, abnormal patterns of postureand movement, a further reduction in functional useand so on, in a downwards spiral.
Our understanding as professionals of the normalcourse of cerebral palsy across the lifespan (Murphyet al 1995, Stevenson et al 1997) gives us aresponsibility to help children and families make theright choice. These types of choices, which can beover such a long time span are particularlychallenging for us all.
Therapists therefore have to guide Darren to makedifferent choices and show him what is possible.Using a tone influencing pattern to do this usessimilar principles to those recently researched(Gordon A 2004 Naylor C 2004) by the proponents of“forced use”. Therapists’ skills therefore, are infinding an activity that will motivate and enablesuccess with Darren’s affected side. Darren needsmovement and use of his right side to maintain hisupper limb range of movement and the possibilityto improve or maintain his ability to carry out twohanded tasks.
Decisions about therapy should include the childwhenever possible and enabling this choice, as inthe previous example, affects the factors in themodel. For example, Becky, aged four, knew exactlywhat she wanted to be better at. When questionedshe wanted to be able to push the doll’s pram and tobe able to go down the slide sitting up and hertherapeutic goals were set around this. It is knownfrom Dr Eva Bowers’ work (Bower 1994, Bower1996), that having goals improves the outcome oftreatment and jointly set goals allow maximummotivation of a child working towards a desiredgoal of their choice.
Becky presented with dystonic cerebral palsy in aquadriplegic distribution and these goals would bea challenge for her. Her success in achieving thesegoals improved her knowledge and experience andher postural tone and patterns of movement, whichwere changed in therapy to enable her to achievethese goals. In achieving her goals she also had theopportunity to gain visual and perceptual skills andtime concepts and importantly develop her self-esteem and sense of success.
Competentchoicemaking

15 A.P.C.P. JOURNALJUNE 2005
Choice - Theory and Practical Application
Acknowledgements:
1. Bandler, R and Grindler, J 1979 “Finding newWays” (137-193) in Frogs into Princes NeuroLinguistic Programming Real People Press UtahUSA.
2. Bandler, R and Grindler, J 1982 “Reframing”Real People Press Utah USA.
3. Bower, E 1994 Measuring motor goals inchildren with cerebral palsy. ClinicalRehabilitation 8: 198-206.
4. Bower, E 1996 A randomised controlled trial ofdifferent intensities of physiotherapy anddifferent goal-setting procedures in 44 childrenwith cerebral palsy, Developmental Medicineand Child Neurology 38, 226-237.
5. Gordon, A From notes during presentation atInternational Workshop, Reorganisation ofhand function in children with brain lesionsPisa 2004.
6. Mc Nevin, N and Wulf, G Attentional focus onsupra-postural tasks affects on postural control.
7. Murphy, KP Molnar, GE and Lankasky, K 1995Medical and functional status of adults withcerebral palsy. Developmental Medicine andChild Neurology, 37 1075-108 Naylor, C Fromnotes during presentation at InternationalWorkshop Reorganisation of hand function inchildren with brain lesions Pisa 2004.
8. Rand, Ayn 1967 Abstractions from Abstractionsin Introduction to objectivist epistemology.
9. Sandidge, RL, Ward, AC, “Reframing” chapter11 in Quality Performance in Human Services.
10. Schmidt, R & Lee, T “Attention andPerformance” page 63 in Motor Control andLearning A Behavioural Emphasis 1999 3rdedition USA.
11. Schmidt, R & Lee, T “Attention andPerformance” page 62 in Motor Control andLearning A Behavioural Emphasis 1999 3rdedition USA.
12. Stevenson, CJ Pharoah, POD and Stevenson, R1997 Cerebral palsy the transition from youth toadulthood. Developmental Medicine and ChildNeurology 39 336-342.
13. Woollacott, M and Shumway-Cook 2002Attention and the control of posture and gait,: areview of an emerging area of research.
A further clinical example where the choices madecould affect future function is Ben. Ben was a youngman of 10 who had no ideas about functional goalsand because he had no insight into his own abilities,he felt he could do everything OK already, or at leastas well as he would ever be able. His initial choicetherefore was not to participate in therapy. Thischoice was partly as he did not know what might bepossible to achieve, and partly that he was afraid oftrying and was unsure what might be expected ofhim. This choice would limit Ben’s potential and hisfuture choices.
Ben’s reluctance to try new things, limited hispossible movement patterns, limited his knowledgeand experience and his independence, not just in thepresent, but in the future. Not trying them alsoincreased his concern and stress when thesechallenges were encountered. Ben initially becamequite upset when trying a new activity wassuggested.
With support and explanation he was able to make adifferent choice resulting in success of which he wasobviously very proud, having removed his ownshoes, socks and splints for the first time ever.
Therapists’ skills must be used to help childrenreframe possibilities and ensure they are notlimiting their own future choices. For example, Benwas limiting his future ability to get himself readyfor bed independently, which limited his choicearound bedtimes, to sleep over at a mates, to beindependent on a school trip and so on.
The ability to make choices and the choices made areclearly strongly linked to a child’s independence.This independence is important at all levels, fromthe child’s ability to be positioned on their own or inequipment and gain some sense of self, to being ableto communicate needs to carers, to being able to getyourself food and drink when you are hungry orthirsty and not having to wait for a carer, toultimately, complete physical and emotionalindependence.
Choice must be introduced in therapy as early aspossible. The model suggested provides a possibleframework for thinking about choice and its inter-relationships and preceding skills and facilitatesthought about choice.
As stated, choice is a fundamental aspect of ourhumanity and legislation provides us all, includingchildren, with the right to make choices, but thisalone is insufficient. It is therapists’ role to facilitateand enable that choice to be as much a reality aspossible for children with special needs and we as
physiotherapists have the knowledge and skills tohelp them maximise their choice making potential.

16A.P.C.P. JOURNAL JUNE 2005
Collaborative Practice inthe Community
Elizabeth A. Atter. M.C.S.P., S.R.P. Senior Paediatric Physiotherapist
Managing a heavy caseload in a busy communitydepartment requires good organisational andplanning skills and some creative thinking.
Over recent years, increased awareness of the needsof children with Developmental Co-ordinationDisorder (DCD) has given rise to large numbers ofchildren being referred for physiotherapy assess-ment and treatment. (The children who present withpredominantly gross motor co-ordination difficul-ties do particularly well with physiotherapy inter-vention. However, improvements in other areashave also been reported. For example, improve-ments with handwriting, self-help skills, attentionand concentration, speech and language and selfesteem.)
A creative solution was needed in order to meettheir needs making the best use of availableresources.
In an effort to manage the large numbers of childrenrequiring treatment, a return to group therapy wasemployed. This meant that groups of 8 to 10 childrencould be treated for an hour per week for 6 weeks byone or two physiotherapists and a physiotherapyassistant. (Blocks of treatment coincided with schoolterms and were felt to be as effective as the 8 or 10week blocks referred to by Michelle Lee and JudithPeters in their research.)
It was felt that treating children with motor co-ordination difficulties in a “Medical” setting couldhave the effect of placing the child in the “sick childrole” and make them more aware of theirdifficulties.
Children’s perceptions and feelings aboutthemselves, their identities and self esteem arelargely influenced by how well their bodies move.(Marsh and Shavelson 1985 as cited in Winnick J.P.2000 Adapted Physical Education and Sport.) It canalso make the parents/carers less confident abouthelping their children themselves as they perceivethat what we are doing is something mystical.
Working with groups of children being physicallyactive also required a move from the physiotherapydepartment into local Leisure Centres. This led tochildren experiencing success in a place where theymight not normally attend and would be more likelyto visit in the future.
The benefits of group physiotherapy are:
1. The children work in a group of peers withsimilar abilities which helps their success ratiosand therefore, their self esteem.
2. Motivation and competition can be experiencedwithin a “safe” environment.
3. Development of social skills with turn takingand learning to be an “intelligent spectator”.
4. There are more opportunities to“Catch the childbeing good”. Working with smaller groups ofchildren with similar abilities enables thephysiotherapist to recognise desirablebehaviour and good skill performance whichcan then be rewarded with praise. This helps thechild learn good practice and internalisepositive messages about him/herself. This canhelp improve self esteem and ultimately, selfefficacy.
5. Parents are encouraged to stay during thesessions and in the case of Dance therapy, to joinin. This helps them to recognise their ownchild’s abilities and gives an opportunitytoencourage use of other Community basedleisure facilities away from“Physiotherapy”
The Children’s Centre in Cardiff was able to offer 3different types of group physiotherapy; Recreationaltherapy, Rebound therapy and Creative dancetherapy.
Recreational Therapy uses activities which arelinked to the key stages in the National curriculumfor PE. e.g. co-ordination, throwing, catching,kicking, striking and dance. The children also learnto work independently and in co-operation with apartner or in a team. The activities are adapted intogames for primary school-aged children and gamesskills and circuit training for young people. Theaims of the session are to work towards the childbecoming a physically educated person who hascompetence at a variety of motor skills, is physicallyfit, values physical activity, can be creative and canappreciate the performance of others and self. (E.g.how to be an intelligent spectator.)
Gaining knowledge of how to analyse and adaptactivities and understand the requirements of thecurriculum for PE means that physiotherapists cancollaborate with school teachers to help integrate oradapt the class activities to allow for successfulparticipation for the patient.
Rebound Therapy is the therapeutic use of thetrampoline to challenge balance, Righting reactions,improve postural tone, co-ordination,proprioception, cardio-pulmonary function and tohave FUN! The children practice their social skills byturn taking, being responsible for each other’s safetyon the trampoline and by being “Intelligentspectators” in order to motivate each other.Rebound therapy has also been reported to help

17 A.P.C.P. JOURNALJUNE 2005
with the articulation of speech and to assist thedevelopment of receptive and expressive language.The easily achievable goals offer “The just rightchallenge” so stretch the children’s abilities withoutallowing them to fail.
Following the 6 week course, the parents oftenasked to continue with the treatment as theirchildren had made such good improvements.However, this was not possible unless it was foundat review appointment that the child would benefitfrom further physiotherapy intervention. It becamenecessary to find somewhere for the children toprogress to so links were made with a trampolinecoach who was qualified to teach children withspecial needs. She now runs several sessions a weekand grades the activities to enable the children towork towards trampoline awards. This means thatthe activities fit into “normal family life”, meet therequirements of the physiotherapy aims oftreatment, consolidate gross motor skills and lead tosuccesses away from the health setting.
Creative dance therapy uses a qualified danceteacher working together with the physiotherapistin a local community dance studio. Discussions areheld prior to the start of the sessions about thephysical and emotional needs of the group ofchildren and the “Physiotherapy aims of treatment”.The teacher then uses her expertise to usemovements that provide the children withopportunities to practice perceptuo-motor skills,improve spatial awareness and give possibilities toexplore their own movement abilities andlimitations of the physical self. Dance is a wonderfulmedium to encourage expressive movementbecause there is no wrong or right way to do it. Theparents were encouraged to take part whereverpossible to give them the opportunity to have apositive, nurturing experience with their childinstead of the often negative relationship that canprevail from having a child with special needs.
After the block of treatment sessions, parents wereencouraged to enrol their child at the dance centre inorder to access the mainstream classes. One boyjoined a Break Dancing group (much to his mother’samazement) and the girls joined in with the Discodancing classes. The children with morepronounced movement difficulties were able to joina special needs class with their siblings invited toaccompany them.
The use of normal sports and recreational activitiesallows the children to consolidate the skills theylearn in the physiotherapy groups. It allows them topursue physical activities away from the “Health”setting and try activities that fit into normal family
Collaborative Practice in the Community life rather than making time for “Therapy”. Oftenthe children will do activities and games at a Leisurecentre when they would refuse to do exercises orcomply with treatments in the department and onceintroduced, it encourages the families to use localamenities after discharge from Physiotherapy.
Collaboration has already been discussedpreviously in this article, taking place betweenphysiotherapists and schools, trampoline coachesand community dance centres. It can be useful tosource activity provision that meets the needs of thechildren before they are discharged. This may meanvisiting local authority and private facilities. Someeducation for the leisure centre and coaching staffmay be necessary in order for them to gain a greaterunderstanding of the specific needs of the clientgroup or child, any precautionary advice to helpimprove the success rate of the participation andprevent injury (e.g. from hypermobile joints) andhow to adapt physical activity to help facilitateinclusion. Linking in with the local Disability SportsAdvisor will also be extremely helpful when lookingfor suitable mainstream and exclusive disabledactivities in the locality.
When using local leisure facilities for group therapysessions, it is advisable to carry out a riskassessment specific to the activity and the venuebefore you organise the block of treatments. Thismeans that any potential risks are considered andsafety factors can be put in place to limit anypotential hazards. It is also important to check outthe Insurance cover for the venue and for youractivity.
In summary, the use of therapy groups can helpmanage busy case lists and thinking creatively canlead to the experience being more than aboutphysiotherapy. The benefits are financial, practicaland for the child, psychological. Working incollaboration with outside agencies can enhanceknowledge of an activity and client group and givea wider understanding of special populations topeople responsible in the community for offeringphysical activity for leisure and recreation. It alsoraises our professional profile.
Children with a disability may have experiencedfailure in physical activity situations previously andwill therefore require careful programme planningto help foster “Affective goals” (self esteem and selfefficacy) which will in turn improve theirmotivation and pursuit of physical activity as a lifelong pastime. This is something that we may notassess formally during our intervention (althoughwe may be aware of it) however, it can haveenormous implications for the child and theirtreatment outcomes.
There should be no barriers to physical activity forany disability groups. Although this article refers to

18A.P.C.P. JOURNAL JUNE 2005
Collaborative Practice in the Community
children with DCD, the same steps can be taken forchildren with other movement and learningdifficulties. It just takes time, planning andunderstanding to work towards sensitive inclusionin the community.
Everyone needs to be physically active for liferegardless of age, sex and abilities and asphysiotherapists, we can help start children on thepath to a healthier, physically active lifestyle whenwe collaborate with our colleagues in the field ofleisure and recreation.
Address for correspondence: The PhysiotherapyDepartment, The Children’s Centre, St. David’sHospital, Cowbridge Road East, Canton, Cardiff.CF11 9XB

19 A.P.C.P. JOURNALJUNE 2005
The Hopes and Choices of Parents
Caroline and Jemma addressed conference to givedelegates food for thought from a mother andchild’s perspective of the services which are onoffer to them
• I am Caroline and this is Jemma
• We have been invited to talk to you about theChoices and Hopes of Parents, and the Hopes ofChildren.
• I am mum not only to Jemma but also to four-year old twins, Kirsty and Rory. I am also Headof Press and Public Affairs for Welsh NationalOpera.
• Jemma is seven. She is an author, a poet, acomposer, a librettist and will be the writer of theNovel of the Year 2009 – so she tells me regularly.
• Jemma has a wonderful dad, Perryn, who is sointricately involved in the story I am about to tellyou, that I hope he will forgive my first personsingular presentation. Jemma and I wouldn’thave got this far without his steadfast support,his love and his unfailingly positive attitudeabout the future.
Jemma and I were both so delighted to be invited totake part in this conference, but I suspect for verydifferent reasons. For me it is a chance to offer you,the vocational professionals, a chance to have aglimpse into the life on the other side of your caselist, so that you might feel a little more aware of thepressures on this side of the care equation.
For Jemma, as she put it ‘it is my chance to tell theworld my story’ and this invitation has given her thefeeling that at least a small part of that worldbelieves in her.
You see, Jemma has spent almost her entire life notbeing believed in – even within our family, we hadfor a very long time no real understanding of whatshe understood, what she was thinking or what shewas capable of achieving.
It has only been since her fifth birthday that theenormity of her intellect, her potential, and herambition to fulfil that potential, has started to comethrough. So what agonies of frustration and despairmust she have gone through for those first fiveyears? I shudder when I think about it.
Let me give you a potted history:
Jemma was born in London in July 1997 – shesuffered birth asphyxia and has athetoid cerebralpalsy as a result. By the time she was six months oldit was apparent that all was not right with herdevelopment, and we were allocated all theappropriate therapists, doctors, play specialists etcto see us through the nightmare ride ofunderstanding and accepting the reality of having adisabled child.
But one thing was clear to us from the very start –Jemma was bright. There was a gleaming shining‘something’ in her eyes, a sense of fun and mischiefand keen desire to learn. She couldn’t talk, but shewas clearly desperate to take an active part in herown life, despite the frustrations of the difficulties ofcommunication and the seemingly insurmountablephysical hand she had been dealt. That brightnesswas clear to us, but we spent five years or moretrying to get everyone else to believe us.
So, clutching the diagnosis of cerebral palsy, andJemma at the age of six months, we began ourtravels into the rather alien world of ‘The TherapyZone’ – a rather frightening and confusing maze.But there was one bright light guiding us as wewent.
Right at the beginning, Jemma was assigned to aLambeth Health physiotherapist called JanJosefsson - a lovely, warm and very knowledgeablephysio. As legions of speech therapists andoccupational therapists came and went on a regularbasis, Jan stayed with us straight and true. In reality(and I think probably to the chagrin of hersuperiors!) she took on the role of our keyworkerand we looked to her for advice far beyond thephysio boundaries. She and I went on a voyage ofdiscovery to research communication devices andfull body splints, and examining any number ofalternative therapies, some of which we tried, andmany we didn’t!
Our relationship with that physio, Jan, was pivotalin my understanding and development of my life asa parent of a disabled child, quite apart fromJemma’s own physical development. Jemma and Iboth trusted Jan as a very close friend andcounsellor.
From the age of one, Jemma was put through anhour of exercises by me and one of a team ofwonderful volunteers who each came to help usonce a week. The therapy programme wasprescribed by the Brainwave team in Bridgewater,Somerset.
Over the next few years, the programme wasupdated according to her developing abilities, and‘within her own standards’ she did develop – herhead control became better and she could roll over.But the most important result of the Brainwave

20A.P.C.P. JOURNAL JUNE 2005
The Hopes and Choices of Parents
programme came from the continual developmentof the flashcard exercise, which eventually proved tobe the gateway which allowed us into Jemma’sremarkable intellect.
Every programme started with flashcards, andbuilding on her understanding of letters and thensmall words, I was able to create a system ofcolumns and rows of letters. Jemma was able topunch on a vertical column and then one letter onthe appropriate horizontal row offered to her.
Using this two stage process, Jemma was able tobuild up very slowly words and sentences – and Imean very slowly – but at last she was able tocommunicate proactively. So one month before her5th birthday, Jemma’s communication dam burst.This new discovery, Spell-talking as we call it,changed her life overnight.
After the first month or so of rather tentative, almostpidgin English, her intellect really started to showthrough. At five years, one month, she describedherself: I am enigmatic’ and nine months later shewrote a 250-word short story called The RunawayTwins.
When we moved to Wales at the end of 2002 whenJem was five and a half, our new speech therapist,Paul Deare, took one look at our cobbled-togethersystem and suggested that we could speed it up byadding colour to it, and it worked.
As Jemma got faster, her outlook on life becamemore ambitious. At six years old she told me ‘Iwould like to outperform the world’s expectationsof a poor disabled soul by writing a history of theworld’s peoples’, - as you can see, irony is a majortool in her writing!
By six and a half, she was planning herautobiography. It will be, she told me:
My Story by Jemma LeechEveryone we know is in it, and the mainprotagonists are my family. The book will chartthe progress of the life of a young girl who ismaimed for life in a birth accident, but whotriumphs over all her problems to outperform theworld’s expectations of her by writing a best-seller.
PS It is for everyone who likes The RailwayChildren.
And that was just before she told me that althoughshe loved me very much, ‘sometimes you are themost demanding old cow on the planet’! So you canimagine that I was getting a bit nervous about thisautobiography!
Late last year, she told me that there was no point in
her learning Welsh, because ‘my bestseller will onlybe written in English’. I am glad to report howeverto those Welsh speakers here, that she did write apoem in Welsh for this year’s Eisteddfod at school!
Jemma’s communication took another huge leap lastsummer when she made it very plain to me througheye-pointing that she wanted to try to use analphabet toy which was lying around. And to myamazement she discovered, that with a bit of asteadying hand (or what they now call ‘facilitation’in technical parlance) she was able to hit lettersdirect.
This of course has opened up a whole new area ofcommunication for her. Having battled with herpoor motor skills over the last few years to try tomaster switches for computerised communication,Jemma has since the New Year been using aspecialised keyboard, called Intellikeys, which withthe help of a facilitator, allows her to access theinternet, email, a number keypad, as well as thewhole alphabet for typing. Plans are also afoot forher to use it for music composition too – she has anopera in her head apparently, and is just desperate toget it out!
And using a basic communication software packageto speak what she types, Jemma has even had a livephone conversation with her grandparents inScotland – alright, it takes several minutes betweeneach line of dialogue, but it is live and it is proactive.
The next step is to try to organise her a properportable communication device, and an electricwheelchair. At that stage the world can only be heroyster.
Since we moved to Wales in late 2002, Jemma hasgone to the most wonderful school – PalmerstonPrimary in Barry – a centre of excellence in the Valeof Glamorgan for the inclusion of children withphysical disabilities. The staff, have been brilliant atgetting her settled and trying to develop her abilitiesfurther, without making huge issues out of herdisabilities.
The therapy team attached to the school have alsobeen wonderful. In particular, we must just mentionJemma’s physio Anne Mahingtheralingham and herOT Jenny Jones, who have given Jem (and me!) suchcare and attention. We value them more than theywill ever realise.
Once we moved to Wales, Jemma was put throughthe standard Educational Psychology tests, and evenour understanding of her abilities was blown out thewater. At six years old, her intellectual range laybetween 13 and 17 years of age, with her numeracylikely to be even further beyond that. Thankfully,the school is taking Jemma’s intellect very seriously,currently teaching her literacy at Year 6 level whileshe remains in Year 3 for everything else. But myhusband and I, along with the schoolteachers, and of

21 A.P.C.P. JOURNALJUNE 2005
course Jemma herself, are now faced with somemajor decisions to make.
How do you educate a child like Jemma whoseabilities are at such extremes? One suggestion wasthat she should move into secondary school thisSeptember – aged just eight. Or that we remove herfrom school entirely and employ (at our own cost ofcourse) a tutor for her.
So what do we do? An article in The Times inOctober gave us a few ideas, but we are open to anyothers. So answers on a postcard please to CarolineLeech, address: the Rock next to the Hardplace!
So that is Jemma’s story – perhaps an unusual one,but the one I can best use as a reference as I moveonto the subject in hand in more general terms.
The Choices and Hopes of Parents
There is one major thing to say about Choice as aparent - I have no choice. I didn’t sit down to planmy first pregnancy and think, gosh wouldn’t it addcolour to my life to have a disabled child. None ofus did.
Most of us began our lives as mothers and fathersexpecting to have to wrestle with no more traumasthan Pampers vs Huggies or mashed carrot vsmashed banana. But suddenly that all changes andyou find yourself the mother of a severely disabledchild.
Suddenly, along with the trauma of coming to termswith that fact, you are also suddenly having to shareyour baby and your life with the dozens ofprofessionals each wanting to offer a small bit of thehelp from their own corner. And while every parentknows that they are all trying to help, it can oftenfeel that these professionals each want to take a littlebit from you too.
If you can imagine my life – it was already rather full– small baby, full time job and career, house, family,and friends – the usual stuff. But on top of that I hadto find time to share my life with Jemma’s • paediatrician, • neonatologist, • GP, • special needs dentist, • health visitor, • special needs health visitor, • physiotherapist, • speech therapist, • occupational therapist, • dietician, • orthotist, • ophthalmist,
• orthopaedic surgeon, • lycra-splint team, • physical therapy team, • early years development specialist, • wheelchair specialist
– I’m sure I have forgotten someone!
That’s a lot of people to cram into an already busylife – and those are only the health professionals!
By the time you add in the education people –
• educational psychologist• head teacher• class teacher• learning support assistant• education officers• communication assessors• IT teacher• mobility officer
And we haven’t started on the social workers,housing grants officers and motability people yet!
Do you wonder why my head (and my diary) ispermanently spinning!
What makes life so much easier is when theprofessionals understand your difficulties. Forworking parents it makes all the difference to be ableto arrange to have appointments at the beginning orend of a day, or if they must be during the day iehospital clinics, to have those appointments well inadvance, not to be called in at a few days notice. Oreven better to be able to run appointments together,ie Jemma’s physio and OT often join together to saveme one appointment.
Another invaluable person was the one who, whilebeing a specialist in their own field, was also awareof what was going on in related areas. I got somegreat ideas and advice from a speech therapist aboutthe education process, and suggestions aboutschools from our physio.
The pressures upon any parent bringing up anychild these days are huge. But the pressures onthose of us bringing up a disabled or special needschild is a hundred times more. And the people thatmake enormous differences to our lives are you – thevocational professionals.
We may not have a choice, but you do. Your Choicehas been to work to help and bring out the potentialin disabled children – for that you have my respect,and you deserve a hearty vote of thanks – not justfrom me, but from every child and every parentwhose life you make a difference to.
OK, I was being deliberately provocative when Isaid I have no choices in all this. Of course I do.Every day I am faced with making small choicesabout Jemma’s life, and every so often I am facedwith some frighteningly huge choices to make about
The Hopes and Choices of Parents

22A.P.C.P. JOURNAL JUNE 2005
Jemma’s future. That is where you can make adifference to me, and others like me.
Supporting us in our decisions, and sharing with usyour knowledge and experience, gives us Choice,and therefore Hope. Showing us you understandour pressures, rejoicing in small triumphs, believingin our knowledge of our own child and helping uswork our way through the maze that confronts us, isall it takes to keep us hoping that it is all going towork out fine.
I am sure that it is not always easy for you to stick toyour Choice. It must be hard to be the person whois standing between the Health AuthorityManagement, with its constant eye on the bottomline and on keeping to budget, and the anguishedparent who is just desperate to see their child haveany opportunity to reach its potential, howevercostly that might be.
I am sure that you have all had experience of parentsat the end of their tether. In my case, Jemma’stherapists and teachers are now used to myemotional outburst being in the form of floods oftears on a fairly regular basis. But I know there areparents whose outbursts come in the form of angerand even violence. I cannot excuse that of course,but perhaps can offer you a rationale for it. Lovely,warm and friendly people that you are, you are alsosometimes the front face of a big institution whichsays ‘No’.
I am a professional, educated, literate and (how shallI put it?) rather assertive person, and yet I have attimes felt utterly demoralised and downhearted bymy attempts get the best, or at least an adequate,provision in education and healthcare for my child.It feels that there has yet to be a moment when I amnot in the middle of a battle for something.
I cannot bear to think of those who have not had:
• a solid education, • who do not have access to a computer to write
the endless letters to the Education or HealthAuthorities,
• who do not feel they have the confidence or theright to take on people in power or
• who perhaps do not have English as their firstlanguage
How on earth do they cope? And how much dotheir children miss out on as a result?
How many children do you know who are goingwithout something – a piece of equipment or somespecialist help – because their parents can’t fighthard enough for it?
The lucky ones
I know I am one of the lucky ones – my child mayhave disabilities, but she also has huge abilities too.And they will lead her undoubtedly to great things,and as she puts it, will let her outperform theworld’s expectations of this poor disabled soul, I amsure. And as she keeps telling me, Jemma believesthat she is one of the lucky ones too. She has onehope for herself and for other disabled children, thehope that they will be believed in. But of course shecan tell you about it herself.
We had hoped that her communication devicewould have been here today so she could addressyou personally, but time has got away from us. Butbelieve me, the words that follow are all Jemma’s:
The Hopes and Choices of Parents
23 A.P.C.P. JOURNALJUNE 2005
“For competent and caring people like yourselves, a tale such as mine ultimately will move and amaze you,but it will not change the way you deal with your child patient list, will it?
“A child is not like a toy, now and then to be taken out of the cupboard for a fun half an hour until somethingmore interesting catches your eye. He ought to have the full attention of his team of expert doctors, therapistsand teachers, or opportunities for development will just fly by, leaving pain and frustration in its wake.
“Decades ago, a child like mewould have been stuck in a homefor cripples, and left there to rot,till death gave them a chance toescape the misery. Even copingnowadays with disabilities likemine is no bed of roses.
“Going heavenwards eventuallyforms a fairly final closure on agonyand ‘poor soul’-dom, but for thoseof us for whom the bell does not yettoll, few hopes are more ferventlyfought for than that of a child whowants to be believed in.
“Being believed in hasn’t yet meantthat I can expect a certain futurewhere all my abilities are acceptedwithout lots of lobbying from mymum. But it does mean that myparents have had their own hopefulfilled. Belief in their deep understanding of me, and my needs and ambitions, has given them a sense ofbeing empowered to change the world; my world at first, but get her wound up enough and my mum willlet nothing get in the way of every disabled child having the same chances as me to reach their true potential.
“But she can’t do it alone, you are the ones who fight on the front line every day, and the hopes of childrenlike me lie firmly in your hands. Please look after them - Hope is a very fragile thing.”
Need I say more?
Caroline and Jemma Leech
April 2005
The Hopes and Choices of Parents

24A.P.C.P. JOURNAL JUNE 2005
Questionnaire Survey on TreatmentPrinciples used in the Management ofCerebral Palsy
Bendall AL1 and Pickering DM2Junior Physiotherapist, University Hospital of Wales,Heath Park, Cardiff 1; Lecturer in Physiotherapy,Cardiff University, Ty Dewi Sant, Cardiff, CF14 4XN.Email: [email protected] Tel 029 2074 4604 2Introduction
IntroductionChildren with Cerebral Palsy (CP) present common-ly with spasticity which provides physiotherapistswith the management challenge of maintainingalignment during growth and minimising the longterm effects of this sensory/motor disorder(Edwards, 2002). The involvement of the paediatricphysiotherapist in linking specialist knowledge totheir treatments is paramount and a wide range oftreatment principles have evolved to manage CPand the associated spasticity in the UK (Scrutton,1984).
In the literature there is common agreement thatearly intervention is the most beneficial and themotivation of the child and family involvement is ofparamount importance in determining the outcome(Levitt, 2004; Bower and McLellan, 1994).
There have been periodic calls for the scrutiny of theeffect of physiotherapy on children with CP (Baxand MacKeith, 1970; Mead, 1968). There are limitedsources of rigorous physiotherapy research thathave evaluated treatment effectiveness on childrenwith CP (Bower and McLellan, 1994; Knox andEvans, 2002). The recent Clinical GovernanceAgenda is driving the need for Evidence BasedPractice and so physiotherapists must be able to jus-tify their clinical reasoning on a sound basis (Jones etal, 2000).
The stronger the knowledge base upon which phys-iotherapists underpin their clinical practice mustsurely give better value for money and qualityassurance (Higgs and Titchen, 2001). There is there-fore a real demand to focus on the ways that physio-therapists are acquiring knowledge of treatmentprinciples. Additionally, physiotherapists need theskills to interpret this evidence
Aims
• To identify the treatment principles that are usedcurrently by community paediatric physiothera-pists.
Poster PresentationAPCP Conference - Swansea 2005
• To identify where the knowledge and expertisewas learnt for the range of treatment principlesused.
MethodA literature search was conducted for evidence oftreatment principles used in the management of CP.Those treatments available are Bobath/Neuro-Developmental Treatment (NDT), ConductiveEducation (CE), Doman Delacato, MovementOpportunities Via Education (MOVE), Rood,Sensory Integration (SI) and Vojta (Hare et al ,1988;Levitt, 2004). In addition an eclectic approach isdescribed which uses a combination of several dif-ferent principles (Levitt, 2004).
The School of Healthcare Studies Ethics committeeat the University of Wales College of Medicineapproved the study.
A questionnaire was designed based on the evi-dence found of treatment approaches. The question-naire survey was carried out : 120 questionnaireswere sent to eighteen randomly selected children’scentres from the Child Development Directory.
Figure 1: Bar chart of where treatment principleslearnt.
Other
Vojta
SensoryIntegration
Rood
M.O.V.E.
DomanDelacato
ConductiveEducation
Bobath/NDT
0 10 20 30 40 50 60
Trea
tmen
t P
rin
cip
le
Number of Respondents
Undergraduate
Formal in-service training
Informal from colleagues
Self taught

25 A.P.C.P. JOURNALJUNE 2005
Poster Presentation
ResultsA response rate of 63% was achieved with 76 ques-tionnaires being returned. All respondents werefemale which is a fair representation of this speciali-ty. The mean time spent working in Paediatrics was13.3 years with a mean of 18 children on their case-load with the spastic type of CP.
Table 1 shows the 4 most commonly used treatmentprinciples: Bobath/NDT: (96%), SI: (36%), MOVE:(18%)and CE: (18%). In addition 4 treatment princi-ples were reported which were not found in the lit-erature review, namely: Brazelton, Halliwick, NancyHilton and Targeted Training. All of the respondentsused a combination of principles and demonstratedan ‘eclectic approach’ to patient management.
The results were analysed by descriptive statisticslooking for trends.
Figure 1 shows a bar chart of where the respondentshad learnt their treatment principles which demon-strates a predominance for in-service and informalfrom colleagues. Of the respondents only 28% hadattended post-graduate courses. There was a trendfor physiotherapists to have read more about a treat-ment they were not currently using and less aboutone they used frequently.
Treatment principle 1st 2nd 3rdchoice choice choice
Bobath/NDT 72 1 0CE 0 9 5Doman Delacato 0 0 0MOVE 1 8 5Rood 0 4 0SI 0 23 4Vojta 3 0 0Eclectic 0 2 2Halliwick 0 1 0Nancy Hilton 0 0 1Targeted Training 0 2 1
Table 1 reports the frequencies of treatment princi-ples chosen in order of preference.
DiscussionThe results showed that 28% of respondents had notattended any postgraduate courses and many hadlearnt most of their skills from in-service training orinformal from colleagues. Gosling (1997) suggeststhat postgraduate courses and qualifications havelittle relevance to patients needs and so the motiva-tion to follow such postgraduate training is mini-mal.
The study demonstrated that in current practicephysiotherapists are using treatment principleswhich have a limited evidence base, and there wasevidence that less had actually sought literary infor-mation and read about these treatment principles.Furthermore, those respondents who had notattended postgraduate courses would not have thebenefit of the present undergraduate courses wherestudents are taught how to retrieve and appraise lit-erature. This could suggest perhaps a training needfor those who have not been able to learn the skillsof information retrieval and critical appraisal(Bardin, 1998).
It was clear that Bobath/NDT and SI were the twomost frequently selected treatment principles andthe knowledge base for these came primarily fromformal/informal training from colleagues. If this is arepresentative trend, it would suggest that quality ofin-service/informal training should be of the high-est standard. This on going professional develop-ment requires the resources and skill mix to ensurestaff competency in the effective management of CP.
ConclusionsThere is a need to demonstrate evidence based prac-tice in the management of CP in children. Thisinvolves physiotherapists updating their knowledgealthough currently from a limited evidence base.
To give these patients the best, most cost effectivetreatment more rigorous evidence is needed, butthen physiotherapists require the necessary skills
AcknowledgementsThe authors would like to gratefully acknowledgethe time the respondents gave to participate to pro-vide this data and wish to assure anonymity andconfidentiality of the data.

26A.P.C.P. JOURNAL JUNE 2005
APCP MATTERS
News from National Committee
National Committee met prior to the opening ofconference in Swansea with a packed agenda andslightly more pressure on time than usual.
Sally Braithwaite was able to report that theproposed DCD meeting had taken place with GillBrown attending as a representative from NAPOT.The objectives of the group include producing aworking document for DCD which would berelevant throughout the UK and include otherdisciplines. A mapping exercise will identify currentpractice with the proposed date for a furthermeeting being September 05.
There will be a further meeting of the Botulinumtoxin group in July with a larger meeting scheduledfor the autumn where it is hoped to also gatherinformation about current practice and present thework to date. These meetings will take place inLondon, dates to be confirmed.
The Neuromuscular interest group inauguralmeeting will be held at CSP, London on 27th Mayand Gill Holmes will represent APCP at thismeeting. It is hoped that the Neuromuscular Interestgroup will become the third A.P.C.P. affiliatedgroup.
Peta Smith and Jeanne Hartley are collaboratingwith Prabh Sulaman, PRO at CSP to produce andpromote a “Tummy Time” leaflet with particularrelevance for Plagiocephaly.
The booklet, “Handle me with care, Supportingyour premature baby’s development “and otherleaflets have now been produced and are availabledirect from Bliss www.bliss.org.uk.
The Outcome Measures Pack, produced incollaboration with PPIMS was available atconference and can be purchased from LornaStybelska, A.P.C.P. Publications officer. Thecommittee thanked Adele Leake for herconsiderable input to this project.
Committee members have been invited tocontribute to or comment on a wide range of topicsincluding public health and ethical issues andclinical topics such as the new Paediatric on-callpackage.Progress with the re-designed website has beenslower than anticipated, however we hope to seesome progress before the July committee with a re-launch in October at CSP congress.
Education and Research committee continues to
develop and promote courses Adele Leake hasproduced an information pack for teachers and atutor support pack for physiotherapists who agreeto teach on APCP courses. She is reviewingprocedures for quality assurance of courses runusing the APCP name and for validation of courses.Jeanne Hartley is working to support paediatricphysiotherapists with an interest in research.
Planning continues for CSP congress in October2005 and future conferences in Glasgow 2006 andSouth East Region 2007.
The next National Committee meeting will be on 8thJuly and your regional representative will be happyto raise any issues on your behalf.
Many Thanks to Wales for their generous hospitality
Laura WigginsSecretary
Clinical Interest Group Liaison Committee report
This is a brief report on what is happening in theClinical Interest Group Liaison Committee (CIGLC).The group now meets three times a year, the lastmeeting was Wednesday 19th January and the nextis 25th May 2005.
‘Time off’ issues to support CI/OG activity wasdiscussed again and it was highlighted howimportant it is for CI/OG members to promote theirinvolvement to their managers, especially as thework is beneficial to CPD and the Knowledge andSkills Framework Profile. Different ways to supportthis included: ensuring the time off required forCI/OG representation was agreed by managers;emphasising the benefits of being a CI/OG memberusing the CI/OG Information Pack; encouragingsupportive managers to write short articles aboutthe benefits of staff being members of CI/OGs forManagers News or similar as well as seekingsupport from members of the Association ofChartered Physiotherapists in Management.
Involvement of the CSP in response to the ‘PublicHealth in England’ agenda was highlighted. A draftpolicy briefing had been circulated for discussion,consultation and involvement. The final draft of thepaper will be circulated to the CSP committees inMay 2005 and should include examples ofphysiotherapy services.
The CIGLC continue to work with the CSP officersto develop: the Society’s future Education Role;Interactivecsp; Electronic CPD, Congress 2005 and2006; ARC; involvement with the DoH and DfESnational consultations and the Information Papersto support our practice and professional

27 A.P.C.P. JOURNALJUNE 2005
development. Much of this is done throughconsultation with members of the committee (andthen to their own committees), short life workingparties or electronic and teleconferencingcommunications. The minutes of the CIGLCmeetings and all draft Information Papers arecirculated to your national committee and regionalrepresentatives so please feel free to contact them fordetailed information or if you wish to take part inany of the consultations.
On a more general note, the CSP continue to supportthe CI/OGs in many ways, not least through thecapitation awards, the training for the CI/OGsOfficers and the work involved in maintainingcommunication to ensure active involvement andconsultation.
For any further information or any queries please donot hesitate to contact me on 01268 886237 or [email protected] [email protected].
Linda FisherClinical Interest Group Liaison Officer
APCP Matters

28A.P.C.P. JOURNAL JUNE 2005
RESEARCH AND EDUCATION
RESEARCH
Early spring has been extremely busy for me but oneof the highlights had to be the APCP Conference inWales. What a stimulating event- so good that Ichanged much of a talk on CP I was giving at aconference in Majorca four days later to includesome of the fascinating insights into listening tochildren and their families about what is importantfor them. Never one to have things ready until theabsolute last minute changing what I wanted to saywas not a problem and the talk was all the better forme having been to Wales! It was very nice to meetsome of the people who have been in touch since Ibecame research officer too – at last I can put faces toyour names.
Research Group Meeting: April 18th 2005.
Our little group is slowly expanding and hopefullywill continue to, as an increase of 25 % in attendeesat the last meeting was very welcome! This numbermay not be highly significant statistically due to thesmall population but a fourth person to join theusual three was highly significant for us! Otherpeople have been in contact about the group but theday was not convenient so we have changed the dayof the next meeting in the hope that more of you willconsider joining us.
The next meeting will be on Thursday June 30th atGreat Ormond Street Hospital from 2-4pm. Thetopic will be critical appraisal of a Journal article andwill be led by Lucy Alderson who is studying for aPhD. If you would like to come please could you letme know – mainly so that I can send you the articlewe are going to look at – but also so I can let youknow where in Great Ormond Street we will be!
Just in case you can’t make it the next meeting willbe on Thursday 22nd September at Queen Mary’sHospital in Roehampton when we hope to discuss:How can you do research as a full time clinicianwith no spare time? Should make for an interestingdiscussion!
These meetings do not have to be London based –they are only in London because that is where thegroup is – so far. If you would like to join us butcan’t travel a long distance how about finding out ifthere are like-minded people in your own area
One of the things we did talk about at the lastmeeting was how useful some of the parent groupsare for accessing information about conditions, datagathering, long term prognosis, outcomes etc. Frommy own perspective I am a big fan of TAG (TheArthrogryposis Group) and attended theirconference last year as a speaker. However the bigthing for me was meeting young people and adults
with arthogryposis and listening to their opinionsabout health provision, (particularlyphysiotherapy!), as well as finding out about theirachievements and problems. Many of thesecondition specific groups hold conferences everyyear. We thought it might be useful to let you knowwhen some of these meetings are just in case any ofyou are thinking of carrying out studies of thequalitative nature or looking at outcomes you mightfind some rich information available to you shouldyou attend. If you know of any conferences comingup please let me know.
So to get you started:
The Jennifer Trust Conference September 10th 2005at Whipsnade Zoo, Bedfordshire.
There will be a full programme of presentations onthe latest drug trials, genetic studies etc regardingSpinal Muscular Atrophy. www.jtsma.org.uk
TAG annual Conference (The ArthrogryposisGroup) 23rd –25th September 2005 in Manchester.www.tagonline.org.uk
FUNDING OPPORTUNITIES:
As you may guess, a lot of the information I getabout research funding gives very short notice forapplications or arrives just as the copy date for thenext Journal has passed - by the time you get thenext Journal there are a couple of weeks left to getapplications in. If any of you are looking for fundingfor projects do give me a call – you may strike lucky!If any of you should have information aboutfunding please do consider sharing the informationvia these pages.
Health Foundation: Leading Practice ThroughResearch
The final round of this award scheme has justopened.
This award enables mid-career professionals, from awide range of backgrounds in the health sector, toundertake research as a means of enhancing abilityto make a direct difference to the quality of patientcare or the health of the population in the UK.
A broad range of quantitative and qualitativeresearch activities will be considered eligible forsupport. The Health Foundation is particularlyinterested in receiving requests from applicantswishing to upon a professional career through thedevelopment of leadership skills, which mayinclude aspects of management training (i.e.influencing and negotiating skills), team building orspecific leadership training.
The award may be held for a minimum of 6 monthsand a maximum of 2 years (full or part-time).Healthcare practitioners,, health improvementpractitioners (including public health professionals)and health service managers and policy-makers areeligible to apply.

29 A.P.C.P. JOURNALJUNE 2005
Deadline for the receipt of applications is 4th August2005
This needs to be accessed viahttp://www.grantfinder.co.uk/profile.php?p=downloads&newsflash=UN3910_UE6890_Health_Foundation.doc
Commonwealth Fund 2006-07 HarknessFellowships.
Anyone interested in spending 12 months in theUSA conducting a health policy oriented researchstudy should look at Alex Warne’s posting on theICSP website. Information about the programme,eligibility and selection criteria, a list of suggestedprojects and the application process can be found atthe Commonwealth Fund website. The deadline forreceipt of applications is September 1st 2005.
Sorry for the short notice of this one (again fromiCSP) – but this may be the one for youoooo!
The Nancie Finnie Charitable Trust research fund
Applications are invited from suitably qualifiedtherapists wishing to undertake research in the areaof rehabilitation of the child with CP.Multidisciplinary projects are encourages. The Trustis small providing for an annual distribution offunds in the range of £25,000 - £30.000.
Application form and guidelines fro the Trust’sprincipal office: 18 Nassau Road, Barnes, LondonSW13 9QE, enclosing a large S.A.E.
Applications no later than 30th June 2005.
Well that’s all for now. Please do contact me if youwould like to have a chat about your researchprojects or ideas or even think of joining our groupfor peer support!
Jeanne HartleyResearch Officer
EDUCATION
Recent courses.
There have been two recent APCP courses held“Introduction to Paediatrics” in Belfast and“Advanced course on Cerebral Palsy” in Derby, bothcourses were very well evaluated and the courseparticipants found the courses informative andvaluable.
Research and Education Quality Assurance Pilot Scheme.
The education committee is undertaking a pilotscheme to evaluate a quality assurance mechanismfor APCP courses. The aim of the QA scheme is toensure that all APCP courses are of the same highquality. This will enable our members and theirfunding bodies to have confidence in the standard ofcourses approved by the APCP. We aim to have thepilot scheme up and running in the next few monthsand will ask some course organisers to participate inthe scheme. The results of the pilot will be availablefor congress in October to help to inform the nextyears planning for the education committee.
Congress 2005 – 7th October
Don’t forget to look out for the congress programmeon the CSP web site, we have tried to ensure that theprogramme is applicable to many members.
• Chronic fatigue syndrome can be a verychallenging part of our case load, both in theacute and community setting, often leavingphysiotherapists feeling frustrated and lackingappropriate skills. Robyn Hudson will presentinformation based upon an internationalperspective of working with children withChronic Fatigue syndrome.
• Pilates has been gaining great impetus in boththe recreational and therapeutic exercise fields.Despite this, very few Physiotherapists havebeen successfully using Pilates with Children asthe transition from an adult to a child friendlyapproach takes creativity and innovation.Maryanne Horton has been using Pilates withchildren for many years and will share herinsight and experience, to help explain howPilates might be appropriately applied withinpaediatric practice.
It should be a very interesting day. Put the date inyour diaries!
Call for new teachers
Thanks to the few people who volunteered theirservices to teach on APCP courses in the future, wenow have an expanding database of people to callon. We still need more of you to help. I’m sure manymore of you regularly teach undergraduate studentsand induct new members of staff into yourworkplace and you would be ideal teachers for our“Introduction to paediatrics” courses which run allover the UK. If you are interested we will offer yousupport and payment for your teaching, you will beoffered dates, times and places which you can acceptor decline as suits you. You are not bound to teachfor us if you just express an interest. If you areinterested, please write to me or drop me an email.
Adele LeakeEducation Liaison Officer
30A.P.C.P. JOURNAL JUNE 2005
Award to be presented at the APCP Day at Congress in October.

31 A.P.C.P. JOURNALJUNE 2005
REGIONAL ANDSUB-GROUP REPORTS
SOUTH WEST
Firstly many thanks to Ruth Davies who has servedas chairperson for the last 4 years and to Clare Olsenwho has been our regions treasurer, both of who willstand down at the next regional AGM. They haveboth performed sterling jobs during their time aspart of the south west regional committee and wewish them both well. This will leave vacancies onthe regional committee and we will shortly be look-ing for willing recruits to fill these posts and com-mittee member vacancies.
A hydrotherapy course, an introduction to theHalliwick concept is due to be held in Southamptonin May (still to take place at the time of going topress, but under Clare’s supervision, no doubt ahuge success). A PE course is still planned for theDorchester area, due to difficulties finding a suitablevenue in the area a firm date is yet to be announced.A sensory integration course is being planned inSalisbury in the summer. Watch out for future flyers.
Here’s hoping for a warm dry summer this year.
LYNDA NEW
SCOTLAND
We are delighted that Dr Terry Poutney has agreedto lead our Study Day on Friday 17th June 2005under the title of postural management. Terry’s pre-sentations will give a comprehensive view of pos-tural management from assessment using theChailey levels of functional ability, through the bio-mechanical approach to the prescription of posturalequipment and the evidence base for changingmanagement of the hip.
Our Regional Annual General Meeting will be heldjust before lunch. Over lunch there will also be timeto network and also look over the equipment exhibi-tion.
Our Study Day is being held for the first time in theCraighalbert Centre in Cumbernauld. We hope thiscentral location will enable as many members aspossible from across the country, to attend.
Plans for APCP Conference 2006 are well underway.The conference accommodation at The Moat houseHotel in Glasgow is booked and we are structuringour programme around the title, Living andLearning—Challenging Expectations. TheNeonatal and Critical Care SIG Groups will also beinvolved in the programme planning. Althoughplanning is at an early stage, we hope to provide aprogramme, which will be of interest to as wide aspectrum of paediatric physiotherapists as possible.
ALISON GILMOUR
NORTH EAST
The study day in April on ‘Postural Management‘with Terry Pountney was a resounding success. Theday was oversubscribed and it was great to see somany members at the AGM. Terry’s presentationwill have given delegates renewed ammunition toseek essential funding for postural managementequipment.
Our next study day, ‘Multi-disciplinary Approach tothe Management of DCD’, will be held in thePostgraduate Centre of Goole District Hospital onWednesday 9th November 2005. There will be threespeakers:- Heather Angilley PT, Sarah Stanley OTand Bron Canwell, Specialist Teacher. Further detailsfor the day will be sent out on a flyer at a later dateto NE members and will also be in ‘events’ on ICSPPaeds Network.
On behalf of our local committee, I would like tothank two of our retiring members for their hardwork and commitment. They have both held veryresponsible posts, giving of their free time withoutquestion for the benefit of the NE region and aregoing to be greatly missed. Jayne Hallford has com-pleted her eight years on the committee and hasbeen the Treasurer for the latter years. Jan Kelly hasresigned from her post as Course Co-ordinator.However, we look forward to meeting new mem-bers at our next committee meeting towards the endof June. Should anyone consider joining the commit-tee at this stage it is not too late - you can be co-opted on.
Finally, congratulations to Wales for hosting anexcellent annual conference in Swansea.
MARY HARRISON
LONDON
It is the most beautiful sunny day and as I write thisit reminds me of the last day of conference inSwansea which was equally gorgeous. I and manyothers couldn’t resist a walk down the beach beforeheading home. What a fantastic setting for an excel-lent few days. London regional committee all wishto say a big thank you to the organisers for a stimu-lating and highly relevant programme and greatentertainment. We were rather disappointed no onefrom the region responded to the offer of a freeplace. Next time go for it you never know - it couldbe you!
Continuing with conference we were delighted tosee the team from St Mary’s Paddington with 2superb poster presentations. We extend our congrat-ulations to Rebecca Biggs who won the competitionwith an exceptional piece of work which was highlyacclaimed by the judges. It is great to know there issuch a lot of talent out there.
Talents continue with some excellent collaborativework coordinated by Charlton Park School,Greenwich, looking into all aspects of equipmentuse in paediatrics which was reported on in the last

32A.P.C.P. JOURNAL JUNE 2005
journal. The ‘Standing network’ sound an excitingproject which will pool current research and experi-ence to offer real benefit to us clinicians using equip-ment.
I am very pleased to report all committee places arenow filled with 3 new additions. Thank you forcoming forward we now have a great mix of grades,and also representation from the private sector. Weare currently working on the new programme of lec-tures which will be advertised as usual by flyer andemail. The committee send congratulations toVathana who is getting married in May, we excuseyou from the AGM! We also send very best wishesfor a speedy recovery to our treasurer Sarah Priorwho has been unwell.
If you don’t get information at your London work-place (you may belong to another region because ofyour home address) let Christina have your workaddress. If you have any news to share, researchprojects, team developments etc drop Christina orme a line so we can add them to the information wecirculate. Have a great summer.
STEPHANIE CAWKER
SOUTH EAST
Once again – greetings from the South East.
Since my last report I have attended the APCPConference in Wales. This was the last Spring con-ference as, from now on, Conference will be in theAutumn. APCP joins CSP Congress in Birminghamon 7th October this year - you might want to thinkabout joining us for the day?
There were some excellent speakers at Conference inWales (you should have been there!) and we wereblessed with spring sunshine. The energetic amongus went for long walks/runs along the beach ofSwansea Bay and the less energetic explored thedelights of the Mumbles. As always the opportunityto network with paediatric physiotherapists fromother parts of the country was a real bonus and theexchange of ideas very stimulating - I took part in avery lively workshop on Consent!
Closer to home we have just about completedarrangements for the Study Evening and AGM on15th September 2005 at Bluewater near Dartford. Asyou may remember from this column, and theQuestionnaire which we organised last year, we arevery keen to encourage attendance at this year’smeeting - so look out for the flyers, applicationforms and the “Special Offer”.
Finally, although 2007 seems a long way off, the timefor us to organise APCP Conference in the SouthEast is rushing towards us. Finding a venue is thefirst challenge, so - if any of you have used/know ofa venue with excellent conference facilities, superb
Regional and Sub-Group Reports accommodation and easy road, rail and flight linksplease get in touch with me asap. My contactsdetails are at the back of the Journal.
Have a good summer.
ANN MARTIN
WALES
My most important news is of course – Conference,held in Swansea at the end of March. Having occu-pied most of our lives for about eighteen months,the moment came and, I think for most people onthe organising committee, passed in a haze of worry,apprehension, fear and then giggling relief when werealised that all was well and the Conference was asuccess. All of those who were delegates wereimpressed by the standard of speaker and the vari-ety of subjects on which they spoke whilst stilladhering to the main theme of “children’s voices,parent’s choices”. The evaluation forms certainlyconfirmed this impression, as did your many cardsand phone calls in the week following.
Roy Noble was a star turn at the Conference dinner,as were the Morriston Orpheous Choir and YMabon. Delegates were impressed, if not stunnedinto an appreciative silence for the choir and muchpraise for Mr Noble came from everywhere.
All in all, an excellent three days of information,communication and education; and, on the last day,the sun came out!
Copies of speakers’ presentations are available inthis edition and in subsequent Journals, plus photo-graphs of the events.
JILL WILLIAMS
NORTHERN IRELAND
Since the last journal we have had our A.G.M. It wasgood to see those of you who where able to make itthat evening. However it is disappointing that somay of our members do not make these eveningmeetings.
Following our AGM we had a most interesting andinformative talk by Deirdre Martin on BabyMassage. Deirdre raised our awareness to atreatment modality, which few of us know muchabout. The discussion continued over wine andcheese!
Felicity attended the national conference inSwansea. We look forward to her feedback on theevent some time later this year
Gemma Lipscomb has taken on the role as APCP repon the N.I. C.S.P board. We are grateful to her andfeel it is important to have a paediatric voice on thiscommittee
Hopefully you have all been making use ofinteractive CSP. The new interactive APCP siteshould be going live soon. Sheila McNeill has agreed

33 A.P.C.P. JOURNALJUNE 2005
Regional and Sub-Group Reports
to take on a local moderator role for the site in theinitial period (so if you’ve any queries please seeher!)
As a committee we hope to meet in the next fewweeks to plan next year’s events. There is still a lotof discussion as to when it would be best to hold ourmeetings to facilitate best attendances. Some of ourcommittee want to retire from office, however weare having trouble recruiting replacements. If youfeel this is something you could do please do nothesitate to contact us
Looking at our membership we could do withrecruiting some new members. Can we encourageyou to promote APCP particularly with new and/oryounger colleagues? We would especially lookforward to any ideas they may have for us oncommittee!
Hopefully we will be in touch with you towards theend of the summer with details of next year’sevents.
ALISON MOUNSTEPHEN
NEONATAL SPECIAL INTEREST GROUP
(Affiliated to the APCP)
BLISS BOOKLET
At last, the long awaited BLISS booklet is finishedand available for ordering. To get your copies of “Handle me with care – supporting your prematurebaby’s development” go on line at www.bliss.org.ukor phone 08712448506, as professionals you willneed to pay P&P. Parents can order on line as well orby phone on 02078209471 and they receive theircopies free of charge.
This booklet is one of a series of publicationssupporting the preterm baby. It is recommended tobe read together with another booklet called “Lookat me – I’m talking to you”, which is a directtranslation from a French booklet called “Je vousparle, regardez moi” and is produced bySPARADRA and sponsored by the PampersInstitute. This booklet deals with the emotionalneeds of the preterm and enables parents tounderstand what the baby is saying to them. Thecontent is based on research by Dr Heidelise Als.
We hope you find them helpful and ask that youencourage lots of feedback, and direct it to BLISSand Peta Smith so that all comments can be taken onboard.
COMPETENCIES
A selection of the committee met in December atNottingham to review those competencies mostrelevant to Physiotherapists working in the field ofNeonates. A tabletop discussion proved very usefuland we were able to send feedback on these for“Skills for Health” to consider. There will be morework on this in the future.
AGM & STUDY DAY
This is scheduled to be in Bristol on Wednesday the19th October. Details will be posted on the icsp website.
ADVANCE NOTICE FOR 2006 APCPCONFERENCE
We plan to hold a Satellite Neonatal Conference atthe APCP Conference in 2006 in Glasgow, 10 – 12November. The theme will be “Nature and Nurture”and this will offer delegates the opportunity toattend lectures from the Neonatal Conference aswell. This is a really exciting opportunity and wehope to have as fantastic an experience as we did inEdinburgh.
MEMBERSHIP
Can I please remind everyone that you should haverenewed your membership at the beginning of theyear. You are required to do so on an annual basisand if you do not, then you will not be on thedatabase and will also not receive a copy of this. Fordetails contact Nicky McNarry on [email protected]
Congratulations to our secretary Nicky McNarryand her husband on the arrival of Max, we wish youall the best and hope you enjoy your time off to‘play, and practise’.
BARBARA HAEDERLE
34A.P.C.P. JOURNAL JUNE 2005
APPLICATION FORM FOR A.P.C.P. PUBLICATIONSDated June 2004
2005 Paediatric Outcome Measurement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £20.00
2003Special Educational NeedsCode of Practice 2001Guidance for Paediatric Physiotherapists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £10.00
2002Paediatric Physiotherapy Guidance for Good Practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £5.00
Obstetric Brachial Plexus PalsyA guide to physiotherapy management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £10.00
Hip Dislocation in Children with Cerebral PalsyA guide to physiotherapy management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £7.50
Evidence Based Practice• Management of Obstetric Brachial Plexus Palsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £3.00• Hip Subluxation and Dislocation in Children with Cerebral Palsy . . . . . . . . . . . . . . . . . . . . . . . . . . . . £3.00
OR . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £5.00 for the pair
Paediatric Manual Handling – Guidelines for Paediatric Physiotherapists . . . . . . . . . . . . . . . . . . . . . . . . £10.00
Human Postural Reactions – Lessons from Purdon Martin by Dr J Foley . . . . . . . . . . . . . . . . . . . . . . . . . . £5.00
Baby Massage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £1.50
The Children Act 1989 “A synopsis for Physiotherapists” . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . £1.00
POSTAGE AND PACKING INCLUDED IN THE PRICE WITH ALL THE ABOVE.
FOR MORE THAN 10 COPIES OR FOR POSTING TO OUTSIDE UK – POSTAGE UPON REQUEST.
TERMS: CASH WITH ORDERS ** CHEQUES & POSTAL ORDERS MADE PAYABLE TO:A.P.C.P PUBLICATIONS AND INCLUDED WITH ORDER PLEASE.
SEND ORDER WITH PAYMENT TO :
LORNA STYBELSKA, PAEDIATRIC PHYSIOTHERAPY DEPARTMENT,CUMBERLAND INFIRMARY, CARLISLE, CUMBRIA CA2 7HY.
WORK TEL: 01228 814739e-mail: [email protected]
Name and Address for Delivery: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .

35 A.P.C.P. JOURNALJUNE 2005
BOOK REVIEW
Handle me with care – Supporting your premature baby’sdevelopment.Look at me – I’m talking to you! Watching andunderstanding your premature baby
Even though I had never reviewed a book in my life…and I apologise inadvance if I haven’t done it properly!...I was delighted to be asked if I couldreview these newly published booklets by BLISS which were produced incollaboration with the APCP Neonatal Group. Mainly because as aphysiotherapist working on a Neonatal Unit, they are just what I wanted!
On first impressions, these booklets look very professional but friendly andpersonal at the same time, with eye-catching titles. From the outset, bothare very clear about their contents and their aims in meeting the needs of a premature baby.
The Handle me with care booklet provides information on the preterm baby’s physical needs anddevelopment through supportive positioning and handling whilst on the neonatal unit and at home. It statesquite clearly that every baby is different and the importance of parents and staff working together. It alsoincludes the appropriate safety notes. The text is quite detailed hence the 37 page booklet but it is very wellpresented and easy to read. It is supported by fabulous real life pictures (my favourite bits!). I also like thesection which helps parents to recognise their baby’s signals and body language which is reinforced in theLook at me booklet. The “at home” section is very useful with advice on sleeping and playtime positions aswell as information on supported sitting. The text is well supported by references.
The Look at me booklet covers a preterm baby’s emotional needs and helps parents to understand theirbaby’s body language and behaviours. It encourages parents to provide the appropriate physical and socialenvironment in which their baby can grow and develop, giving them a positive role whilst their baby is onthe neonatal unit. Again, this booklet is well presented with some nice illustrations.
These two booklets complement each other beautifully!
I thought it would be a good idea to ask a few other people what they thought and this is what they had to say:
“Wonderful booklets, nice and clear, just simply helped me to understand my little girl’s behaviours and how I couldhelp to provide a better environment for her to develop” (Parent)
“Lovely to have professional looking written reinforcement to complement the information given to parents on the unitand at home. Demonstrates the importance of parents being involved with their baby’s development so giving them adefinite role. Very useful teaching tools also!”
(Sarah Davies, Senior II Physiotherapist and Bethan Sheen, Junior Physiotherapist, Llandough Children’s Centre)
“Very useful for parents. Excellent!” (Nurses on the Neonatal Outreach Team)
Thank you to all who were involved in the publication of these booklets – I will be recommending them toeveryone!
Sian Howells Senior PhysiotherapistChildren’s Centre Llandough HospitalCardiff

36A.P.C.P. JOURNAL JUNE 2005
FORWARD -Bath Pain Management Unit LaunchesAdolescent Newsletter
The Bath Pain management unit has been runningthree-week residential programmes for adolescentssince 1999. We have seen over 200 adolescents in thistime.
The programmes were set up for adolescents whoseexperience of chronic pain was making a significantand detrimental impact on their developing lives.Adolescents reported reduction in schoolattendance, sporting activities, socialising, andchanges in sleep and eating patterns, all of whichinfluenced their mood and physical health.
The programme is run by an interdisciplinary teamcomprising of Physiotherapists, ClinicalPsychologists, Occupational Therapists, SpecialistNurse and Paediatric Rheumatologist and Specialistin pain medicine. The programme focuses onreturning adolescents to school/college or to startwork, return to age appropriate activities, soadolescents can live a full and satisfying life with theongoing presence of pain.
HERE AND THERE
The programme content comprises bodyconditioning, activity engagement, moodmanagement, healthy living information and painand medication education. Six adolescents areinvited onto each programme with theiraccompanying adult. Our data shows their physicalfunctioning, anxiety and depression and schoolingare all significantly improved at three-month follow-up.
The unit is launching its first ever edition ofFORWARD, the adolescent service newsletter. It hastwo purposes to inform our colleagues of what wedo on our programmes and to provide a forum forour adolescents and parents to share their tips forsuccess and stories of their progress. If you wouldlike to be added to our mailing list please send yourname and address to [email protected] (details protected by data protectionact). For more information about the unit visit ourwebsite www.bath.ac.uk/pain-management.
THE BATH TEAM
37 A.P.C.P. JOURNALJUNE 2005
COURSES
APCP at CSP
CONGRESS
2005
Come and join us on FRIDAY 7th OCTOBER
at the International Conference Centre in Birmingham
APCP’s day at Congress will include talks on Chronic Fatigue Syndrome and Pilates for Children.
As well as networking and catching up with old friends there will also be the opportunity to attend APCP’s AGM.
Please look in Frontline for further information.
Tickets for day attendance are available.
SEQ
UI
C
HA
RTER
ED
SO
CIET
Y O
F PHYSIO
THER
APY
DIG
NA

38A.P.C.P. JOURNAL JUNE 2005
Courses
Paediatric Physiotherapy andOccupational Therapy:
A critical approach to advancing specialist knowledgeand practice
Run as part of the MSc Physiotherapy programme
This block attendance module will run from September 2005 – May 2006 for part time students only
The module critically analyses the issues relevant to clinical effectiveness and explores and evaluates:
• the principles of good communication in various settings with children, families and other professionals
• how psycho-social issues influence interventions with children • the legal & ethical issues in relation to working with children.
This module has been developed in association with theAssociation of Paediatric Chartered Physiotherapists
For further details contact: Gill Baer ([email protected]) or Fiona Coutts [email protected]
Details of the full MSc programme can be obtained athttp://healthsciences.qmuc.ac.uk/
LEARNING-RESOURCES/postmsc/home.htm
SEQ
UI
C
HA
RTER
ED
SO
CIET
Y
OF PH
YSIOTH
ERA
PY
DIG
NA
39 A.P.C.P. JOURNALJUNE 2005
THE APCP RESEARCH GROUP REGISTER
If you would like to be a member of the APCP research group, please fill in the formbelow and return it to Jeanne Hartley, Research Officer, Physiotherapy Department,Great Ormond Street, London, WC1N 3 JH. This information will be used to inform youof reseach study days and help us to learn more about our members’ research interest.
Name
ContactAddress
Post Code
Tel. No.
Fax No.
E-Mail:
What are your research interests?
Are you undertaking any type of research project small or large? YES?NOIf so please give a brief summary . . .
Would you be happy for other physiotherapists with similar research interests to be put intouch with you? YES/NO
Thank you for completing this form.
40A.P.C.P. JOURNAL JUNE 2005
SEQ
UI
C
HA
RTER
ED
SO
CIET
Y
OF PH
YSIOTH
ERA
PY
DIG
NA
SEQ
UI
C
HA
RTER
ED
SO
CIET
Y
OF PH
YSIOTH
ERA
PY
DIG
NA
DON’T FORGET TO BOOK YOUR PLACE
AT CONGRESS FOR7TH OCTOBER
– REMEMBER THIS ISPAEDIATRIC DAY
JUNE 2005A.P.C.P. JOURNAL A.P.C.P. JOURNAL
NATIONAL COMMITTEE OFFICERS AND MEMBERS REGIONAL & SUB-GROUP REPRESENTATIVES
JUNE 2005
EAST ANGLIA LONDON SCOTLAND
Sue Coombe Stephanie Cawker Alison GilmourJenny Lind Physiotherapy Dept. The Wolfson Centre Graysmill SchoolNorfolk & Norwich University Mecklenburgh Square 1 Redhall House DriveHospital LONDON CraiglockhartColney WC1N 2AP EDINBURGHNORWICH NR4 7UZ [email protected] [email protected]@nnuh.nhs.uk
SOUTH WEST SOUTH EAST WALES
Lynda New Ann Martin Jill WilliamsPhysiotherapy Dept Physiotherapy Dept Physiotherapy DeptMilestone School Childrens Therapy Centre The Hollies Special SchoolLonford Lane Goldie Leigh PentwynGLOUCESTER GL2 9EU LODGE HILL SE2 0AY [email protected] [email protected]
NORTH WEST TRENT NORTHERN IRELAND
Elaine Lloyd Claire Hill Felicity DicksonPhysiotherapy Dept Physiotherapy Dept Scrabo Children’s CentreBooth Hall Children’s Hospital Sheffield Children’s Hospital Ards Community HospitalCharlston Rd Blackley Western Bank Church StreetMANCHESTER SHEFFIELD NEWTONARDSM9 7AA S10 2 TH BT23 4AS N. [email protected] [email protected] [email protected]
WEST MIDLANDS NORTH EAST OVERSEAS
Lindsay Rae Mary Harrison Public RelationsPhysiotherapy Dept. 11 Whitsundale Close OfficerThe Children’s Hospital KNARESBOROUGHSteelhouse Lane N YorkshireBIRMINGHAM B4 6NH HG5 [email protected] [email protected]
NEONATAL CARE GROUP CRITICAL CARE GROUP
Barbara Haederle Rachel HuftonSJUH Physiotherapy DeptChild Development Centre Royal Manchester Children’s HospitalBeckett Street Hospital Road, PendleburyLEEDS LS7 MANCHESTER M24 [email protected]
CHAIRMAN Lesley Smith Physiotherapy DeptRoyal Hospital for Sick ChildrenYork Hill NHS Trust Dalnair StGLASGOW G3 8 SJ [email protected]
VICE-CHAIRMAN Peta Smith Physiotherapy DeptMary Sheridan Centre43 New Dover RdCANTERBURY CT1 3AT [email protected]
SECRETARY Laura Wiggins 26 Braidpark DriveGiffnockGLASGOW G46 6NB [email protected]
TREASURER Fiona Down 5 Home Farm CloseHiltonHUNTINGDONCambs PE28 9QW [email protected]
PUBLIC RELATIONS Gill Holmes Child Development CentreOFFICER Alder Hey Children’s Hospital
Eaton Rd LIVERPOOL L12 2AP [email protected]
VICE PUBLIC Lindsay Rae Physiotherapy Dept.RELATIONS OFFICER The Children’s Hospital
Steelhouse LaneBIRMINGHAM B4 6NH [email protected]
EDUCATION Adele Leake Snr Lecturer in Physiotherapy OFFICER School of Health & Social Care
Collegiate Crescent CampusSheffield Hallam UniversitySHEFFIELD S10 2BT [email protected]
PUBLICATIONS Lorna Stybelska Paediatric Physiotherapy DeptOFFICER Cumberland Infirmary
CARLISLECumbria CA2 4HY [email protected]
MEMBERSHIP Susan Cleverely Physiotherapy DeptSECRETARY Orchard House
9 College RoadCHICHESTER PO19 6PQ [email protected]
EDITOR Sally Braithwaite 531 Church RdYardleyBirmingham B33 8PG [email protected]
RESEARCH Jeanne Hartley Physiotherapy DeptOFFICER Great Ormond St Hospital
LONDON WC1N 3JH [email protected]
CIG LIAISON Linda Fisher Special Educational Needs & OFFICER Psychology Service
SE Essex Area Education OfficeThe KnaresBASILDON SS16 5RX [email protected]
DIVERSITY Sue Coombe Jenny Lind Physiotherapy DeptOFFICER Norfolk & Norwich University Hospital
Colney NORWICHNorfolk NR4 7 UZ [email protected]
Committee Members Christine Shaw 42 Cammo GroveEDINBURGHEH4 8EX [email protected]
Sarah Crombie 10a Record RoadEmsworthHants PO10 7NS [email protected]
ASSOCIATION OFPAEDIATRICCHARTERED
PHYSIOTHERAPISTS
ISSUENO. 115JUNE 2005
CONFERENCE EDITION
In this issue :
Consent – the Welsh Vision
Perceived Efficacy and Goal Setting Systems
Choice – Theory and Practical Application
Collaborative Practices in the Community
The Hopes and Choices of Parents
Questionnaire Survey – Treatment Principles Used in the Management
Of Cerebral Palsy





























