Embed Size (px)
Citation preview

Archives ofDisease in Childhood 1991; 66: 48-51
Association of pneumothorax and hypotension withintraventricular haemorrhage
Dariush Mehrabani, C W Gowen Jr, Arthur E Kopelman
AbstractTo test the hypothesis that acute hypotensionresulting from pneumothorax would beassociated with severe brain injury (grade 3 or4 intraventricular haemorrhage), 67 very lowbirthweight (VLBW) infants of 32 weeks'gestation or less with respiratory distresssyndrome and pneumothorax were studied.Thirty six had pneumothorax associated withsystemic hypotension and 31 had pneumo-thorax with normal blood pressure. Thegroups were similar in gestational age andseverity oftheir respiratory distress syndrome.Thirty two of 36 of infants with pneumothoraxassociated with hypotension (89%) had grade3 or 4 intraventricular haemorrhage. Thispercentage was significantly greater than thepercentage for infants with pneumothorax andnormal blood pressure (three of 31, 10%). Therisk ratio for grade 3 or 4 intraventricularhaemorrhage for infants with pneumothoraxassociated with hypotension was 9-8 comparedwith neonates with pneumothorax and normalblood pressure. These observations areconsistent with the hypothesis that systemichypotension and cerebral hypoperfusion areimportant factors leading to intraventricularhaemorrhage in VLBW infants.
Department ofPediatrics,East Carolina School ofMedicine, Greenville,North Carolina27858-4354, USADariush MehrabaniC W Gowen JrArthur E KopelmanCorrespondence to:Dr Kopelman.Accepted 25 June 1990
Pulmonary air leak is a common complication invery low birthweight (VLBW) infants, occur-ring in up to 35% of those being ventilated forrespiratory distress syndrome.' 2 Severalreports have indicated that pneumothorax isoften associated with, or followed by, intra-ventricular haemorrhage"7 but other studieshave not reported an increased risk of intra-ventricular haemorrhage.8 9 None of thesestudies, however, commented on the severity ofsymptoms caused by the pneumothorax orwhether the pneumothorax was accompanied bysystemic hypotension. A small pneumothoraxmay be asymptomatic or mildly symptomatic,but if the pneumothorax is associated withappreciably raised intrathoracic pressure thencardiac filling, cardiac output, and systemicblood pressure will fall.'0'2 If this happenscerebral infarction is seen as the primary event,with intraventricular haemorrhage not occur-ring until after the systemic blood pressure hasbeen raised to, or above, normal levels." 12
In this study we tested the hypothesis that apneumothorax with systemic hypotensionwould increase the likelihood of severe intra-ventricular haemorrhage in VLBW infantsbeing ventilated for respiratory distresssyndrome. Episodes of pneumothorax after
which the blood pressure remained normalwould be less likely to result in severe intra-ventricular haemorrhage.We studied the incidence of grades 3 and 4
intraventricular haemorrhage among VLBWinfants with pneumothorax that had causedhypotension, and compared it with the incidenceof intraventricular haemorrhage in infants withpneumothorax and normal blood pressure.
Patients and methodsWe retrospectively identified 82 infants fromthe records of our neonatal intensive care unitwho were admitted between 1 January 1983 and31 December 1986, were of 32 weeks' gestationor less, required mechanical ventilation forrespiratory distress syndrome, and developed apneumothorax. Fifteen were excluded from thestudy: five with hypoplastic lungs, one in whomthe pneumothorax occurred as a terminal event,one in whom the pneumothorax was secondaryto a thoracotomy for ligation of a patent ductusarteriosus, and two with congenital defects ofthe central nervous system. In addition, sixothers were excluded because they did not havea cranial ultrasound scan carried out after theirpneumothorax, or because they had not under-gone necropsy to see if there was an intra-ventricular haemorrhage.The remaining 67 infants were studied. Two
of the authors (DM, CWG) reviewed eachneonate's chart to find out if the pneumothoraxwas associated with systemic hypotension.Blood pressure was monitored continuously bya transducer attached to an indwelling umbilicalarterial catheter. Systemic hypotension, definedas a sudden fall in the mean blood pressure toless than two standard deviations below themean for age (30 mm Hg or less,'3) resultedfrom a pneumothorax in 36 infants. An addi-tional 31 infants had a pneumothorax but didnot develop hypotension. Cranial ultrasoundscans were independently scored according tothe Papile system by a radiologist and a neo-natologist (AEK) who did not know the medicalhistory.3 The most severe grade of intra-ventricular haemorrhage on any ultrasound scanwas used for the infant's score. For infants whodied (n=4) before ultrasound examination, theseverity of intraventricular haemorrhage wasdetermined at necropsy.For each infant we recorded birth weight,
sex, race, gestational age, Apgar score at oneand five minutes, obstetric complications, timeof first pneumothorax, and ventilator settingsboth at 12 hours of age and immediately beforethe first pneumothorax. The total number of
48

Association ofpneumothorax and hypotension with intraventricular haemorrhage
days on the ventilator and being treated withoxygen, and the mortality, were also noted.The incidence ofintraventricular haemorrhage
was determined for each group. Data werecompared by the x2 test and the unpairedStudent's t test. The relative risks for intra-ventricular haemorrhage for each group werecalculated to answer the following question: ispneumothorax with systemic hypotension asso-ciated with an increased incidence of grades 3and 4 intraventricular haemorrhage comparedwith pneumothorax during and after which theblood pressure remains normal?
ResultsAlthough the infants in the two groups were ofsimilar gestational age (28-6 (1-8) weekscompared with 29- 1 (2 2) weeks) the mean birthweight of the hypotensive infants (1026 (293)was lower than that of the group with normalblood pressure (1250 (356) g, p<001) (table 1).In addition there were more boys in the hypo-tensive group (25 of 36, 69%) than in thegroup with normal blood pressure (15 of 31,42%) (p<0 03).The average age of occurrence of the first
pneumothorax was 29 hours (range 4-127) and32 hours (range 2-100) in the hypotensive andnormotensive groups, respectively. Thepneumothorax was bilateral in about half theinfants in each group; pneumothorax was rightsided in about 66% of the unilateral pneu-mothoraces in each group.Mean baseline measurements of blood
pressure before the pneumothoraces weresimilar in the two groups (table 2). In all theinfants who became hypotensive the meanarterial pressure fell when the pneumothoraxoccurred from 40 (7-1) mm Hg to 19-2 (10-1)mm Hg (p<0-001). Mean blood pressures didnot change significantly during the pneumo-thorax in the normotensive group.
After the pneumothorax the arterial oxygentension fell significantly (from 9-73 kPa to7 07 kPa, p<0 05) and the arterial carbondioxide tension rose (from 4 80 kPa to 6 67 kPa,
p<0 05) in the hypotensive infants, but didnot change significantly in the normotensiveinfants (from 8 66 kPa to 8 13 kPa and from5-33 kPa to 6-00 kPa, respectively).There were no significant differences between
the groups in ventilator mean airway pressure at24 hours of age, but a significantly higherfractional inspiratory oxygen (F,o2) was requiredin the hypotensive infants (0-75 compared with0-62, p<005). There was no significantdifference between the groups in mean airwaypressure just before pneumothorax.
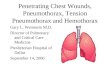
RELATIONSHIP BETWEEN INTRAVENTRICULARHAEMORRHAGE AND PNEUMOTHORAXThe incidence of intraventricular haemorrhagefor each study group is shown in the figure.Only one infant (3%) in the hypotensive grouphad a normal cranial ultrasound scan comparedwith 24 infants (77%) in the group with normalblood pressure. Thirty two infants, 89% ofthose in the hypotensive group, had grade 3 or 4haemorrhages. The increased incidence of grade3 or 4 intraventricular haemorrhage in thisgroup of infants with pneumothorax and hypo-tension is highly significant compared with thegroup whose blood pressure remained normal (3of 31, 10%, p<0-01). The relative risk of grade3 or 4 intraventricular haemorrhage was 9-8 for
U Pneumothorax with hypotension
100 | Pneumothorax with normal blood pressure
80
u601~404
0L20
0None 1/2 3 4
Grade of intraventricular haemorrhage
Infants with pneumothorax and hypoension had a higherincidence ofgrade 3 and 4 intraventricular haemorrhage.(*p<O0O1).
Table I Clinical characteristics of the study groupsPneumothorax with Pneumothorax with p Valuehypotension (n=36) normal blood
pressure (n=31)Mean (SD) birth weight (g) 1026 (293) 1250 (356) <0-01Mean (SD) gestational age (weeks) 28-6 (1-8) 29-1 (2-2) 0 3Mean Apgar scores at 1 min/5 min 3/5 3/5No (%) boys 25 (69) 15 (48) 0-07No (%) black infants 15 (42) 18 (58) 0-6No (%) born in hospital 22 (61) 21 (68) 0-6No (%) vaginal births 24 (67) 12 (39) 0-02No (%) with breech presentation 6 (17) 6 (19) 0-8No (%) with rupture of membranes for >24 hours 6 (17) 5 (16) 0 9No (%) with respiratory distress syndrome grade 3 or 4 21 (58) 13 (42) 0-2
Table 2 Mean (SD) arterial blood pressure (mm Hg)Before pneumothorax During pneumothorax After recovery
of pneumothorax
Pneumothorax with hypotension 40-0 (7-1)* 19-2 (10-1)* 37 9 (7 8)Pneumothorax withnormal blood pressure 36-8 (4-8) 36-3 (4-7) 37-3 (4 3)
*p<0 001.
49

Mehrabani, Gowen3Jr, Kopelman
infants who became hypotensive compared withthose whose blood pressure remained normal.
Because the study was retrospective we werenot able to control for the timing of the cranialultrasound scans. We therefore cannot saywhether the pneumothorax preceded the intra-ventricular haemorrhage in all cases. Never-theless, 17 infants in the hypotensive group hadcranial ultrasound scans carried out both before,and within 24 hours after, their pneumothorax.Before the pneumothorax 10 of these 17 infantshad normal cranial ultrasound scans and sevenhad either a grade 1 or grade 2 intraventricularhaemorrhage. On repeat cranial ultrasoundexamination of the same infants after thepneumothorax, none had a normal cranialultrasound, one had a grade 1-2 intraventricularhaemorrhage, and 16 had grade 3 or 4 intra-ventricular haemorrhages. Though we cannotbe certain that pneumothorax with a fall inblood pressure preceded the intraventricularhaemorrhage in all cases, we believe that theobservation in these 17 infants make it likelythat severe intraventricular haemorrhagefollowed the development of pneumothorax.
MORTALITY AND MORBIDITYMortality was significantly higher in the hypo-tensive group (15 of 36, 42% compared with 3 of31, 10%; p<0005). Among the survivinginfants, there was no difference between groupsin the length of time the infants receivedassisted ventilation or supplemental oxygen.Residual brain damage was more commonamong the surviving hypotensive infantscompared with the infants whose blood pressureremained normal; nine of 36 (25%) comparedwith none of three of survivors developedunilateral periventricular leucomalacia withporenchephaly (p<0005), and 19 of 36 (53%)compared with one of 31 (3%) developedventriculomegaly (p<0-01).
DiscussionIntraventricular haemorrhage occurs in about35% of premature neonates weighing less than1500 at birth, and is a serious cause of mortalityand morbidity.3 In addition, one recent reportshowed a significant association between hypo-tension and cerebral lesions or death.'2 Intra-ventricular haemorrhage originates in thecapillary network of the germinal layer, which ishighly vascular and poorly supported. Thepathogenesis of intraventricular haemorrhage iscomplex, but its occurrence is greatest inVLBW infants with respiratory distresssyndrome.'4A close association between pneumothorax
and the occurrence and extension of intra-ventricular haemorrhage has been reportedpreviously by Dykes et al who found that if apremature infant had an alveolar rupture, therisk of intraventricular haemorrhage wasincreased 2-5-fold compared with similarinfants without alveolar rupture.5 Of all the riskfactors studied, they found that the presence ofpneumothorax had the strongest association
with the later development of intraventricularhaemorrhage. Lipscomb et al,4 Hill et al,6 andThorburn et al'5 also reported a close associationbetween the development of a pneumothoraxand a later intraventricular haemorrhage.Cooke,8 and Van De Bor et al,9 however, didnot find an increased incidence ofintraventricularhaemorrhage in premature infants withpneumothorax. The apparent discrepancyamong these previous studies might be causedby differences in the severity of the pneumo-thoraces in the populations studied.Pneumothorax in an infant can be virtually
asymptomatic or may be associated with severecirculatory disturbances including hypotensionand hypoperfusion. When severe pneumo-thorax leads to inadequate cardiac filling andsystemic hypotension (air block syndrome)cerebral ischaemia may be induced, with thearterial watershed zones in the periventricularregions of the brain being particularly prone. "
Published data about the effect of pneumo-thorax on arterial blood pressure are somewhatconflicting. Hypotension secondary to pneumo-thorax has been clearly shown in both animaland human studies.2 12 16-lg Other studies,however, have reported either no change in thearterial blood pressure or an increase in thearterial blood pressure with pneumothorax.6 20It is likely that the effect of pneumothorax onarterial blood pressure in both animals andhumans can be explained by the difference inthe severity of the pneumothoraces studied.When there is sufficient intrathoracic pressureto compress the intrathoracic vessels severely,systemic hypotension will result (air blocksyndrome).Our study has shown that 89% of our 36
infants with pneumothorax resulting in systemichypotension developed grade 3 or 4 intra-ventricular haemorrhage. This percentage wassignificantly greater than for infants withpneumothorax that was not associated withhypotension (9%). There was also a highermortality among the infants with pneumothoraxand hypotension than among infants withpneumothorax but no fall in blood pressure(42% compared with 10%, p<0 005). Inaddition, infants with pneumothorax resultingin hypotension had a higher incidence of peri-ventricular leucomalacia with porencephaly(25% compared with 0%, p<0.01) and ventri-cular dilation (53% compared with 3%, p<0-01).The development ofperiventricular leucomalaciaand ventricular dilatation in these infants isconsistent with them having experienced anepisode ofsevere cerebral ischaemia or infarction,or both.One possible problem with this comparison is
that the infants with pneumothorax associatedwith hypotension had a lower mean birth weightand there was a preponderance of boys. Thegroups were of similar gestational age, however,and the severity of their respiratory distresssyndrome was similar (as shown by similarmean airway pressures on assisted ventilationand similar findings on chest radiographs. Weare unable to say definitively that their higherincidence of grade 3 and 4 intraventricularhaemorrhage is solely the result of their
50

Association ofpneumothorax and hypotension with intraventricular haemorrhage 51
pneumothorax with associated hypotension.Nevertheless, those infants who developed apneumothorax with hypotension had anextremely high incidence of intraventricularhaemorrhage (89%), identifying them as agroup at extreme risk. No other single factor orcombination of risk factors has been as stronglypredictive of severe intraventricular haemor-rhage. We therefore believe that these resultsstrongly suggest (but cannot prove directly) thatthe pneumothorax associated with hypotensionwas the cause of the haemorrhage.
These observations support the theory thatcerebral hypoperfusion or ischaemia precedesdevelopment of severe intraventricular haemor-rhage. 1" Recent reports indicate that prematureinfants who develop hypotension in the firstdays of life are likely to have cerebral paren-chymal injury or severe intraventricularhaemorrhage, while infants of similar gestationalage who are not hypotensive do not developthese injuries." 12 These infants lack cerebralautoregulation so that hypotension resultsdirectly in cerebral hypoperfusion. " We believeit is possible that the cerebral hypoperfusionthat accompanies the systemic hypotensioncauses infarction of both the periventricularwhite matter and the germinal matrix. Later,when the blood pressure and cerebral bloodflow are raised to normal values, the germinalmatrix capillaries rupture and germinal matrixor intraventricular haemorrhages develop.
In summary, we found that 89% of 36 VLBWinfants with respiratory distress syndrome whodeveloped a pneumothorax with hypotensionalso developed a grade 3 or 4 intraventricularhaemorrhage. These severe degrees of intra-ventricular haemorrhage have been associatedwith early mortality or neurological handicap insurvivors. Based on our results, additionalprospective studies should be carried out todetermine the incidence and severity of braininjury in VLBW infants after episodes ofmoderate and severe hypotension.
1 Hill RT, Rhodes PG. Pneumothorax and pneumomediastinumin infants with idiopathic respiratory distress syndromereceiving continuous positive airway pressure. Pediatrics1975;55:493-6.
2 Ogata EB, Gregory GA, Kitterman JA, et al. Pneumothoraxin the respiratory distress syndrome: incidence and effect ofvital signs, blood gases, and pH. Pediatrics 1976;58:177-83.
3 Papile LA, Burstein J, Bumstein R, et al. Incidence andevolutionofsubependymalandintraventricularhemorrhage:a study of infants with birth weights less than 1500 grams.J Pediatr 1978;92:529-34.
4 Lipscomb AP, Thornburn RJ, Reynolds EOR, et al.Pneumothorax and cerebral haemorrhage in preterminfants. Lancet 1981;i:414-6.
5 Dykes FD, Lazzara A, Ahmann P, et al. Intraventricularhemorrhage: a prospective evaluation of etiopathogeneses.Pediatrics 1980;66:42-9.
6 Hill A, Perlman MB, Volpe JJ. Relationship ofpneumothoraxto occurrence of intraventricular hemorrhage in the pre-mature newborn. Pediatrics 1982;69:144-9.
7 Kopelman A, Wimmer J, Engelke S, et al. Severe intra-cerebral hemorrhage in preterm infants impact on mortalityand neurologic status. In: Jones CT, Nathanielsz PW, eds.The physiological development of the fetus and newborn. Part7: Perinatal physiology and clinical care. Orlando: AcademicPress, 1985:777-82.
8 Cooke RWI. Factors associated with periventricular haemor-rhage in very low birth weight infants. Arch Dis Child1981;56:425-31.
9 Van De Bor M, Van Bel F, Lineman R, Ruys JH. Perinatalfactors and periventricular-intraventricular hemorrhage inpreterm infants. Am j Dis Child 1986;140:1125-30.
10 Macklin MT, Macklin CC. Malignant interstitial emphysemaof the lungs and mediastinum as an important occultcomplication in many respiratory diseases and otherconditions: an interpretation of the clinical literature inlight of laboratory experiment. Medicine 1984;23:281.
11 Lou HC. The 'lost autoregulation hypothesis' and brainlesions in the newborn. Brain Dev 1988;10:143-6.
12 Miall-Allen VM, de Vries LS, Dubowitz LMS, WhitelawAGL. Blood pressure fluctuation and intraventricularhemorrhage in the preterm infant of less than 31 weeks'gestation. Pediatrics 1989;83:657-61.
13 Shortland DB, Evans DH, Levene MI. Blood pressuremeasurements in very low birth weight infants over the firstweek of life. J Perinat Med 1988;16:93-7.
14 Volpe JJ. Neurology of the newborn. 2nd Ed. Philadelphia:WB Saunders, 1987.
15 Thornburn RJ, Lipscomb AP, Stewart AL, et al. Timing andantecedents of periventricular hemorrhage and cerebralatrophy in very preterm infants. Early Hum Dev 1982;7:221-38.
16 Easley CS, Wartman FS, Cruze M, et al. Effect of tensionpneumothorax on regional brain blood flow in the neonatalpiglet. Medical Science Research 1989;17:711-3.
17 Batton DG, Heilman J, Nardis EE. Effect of pneumothorax-induced systemic blood pressure alteration on the cerebralcirculation in newborn dogs. Pediatrics 1984;74:350-3.
18 Monin P, Vert P. Pneumothorax. Clin Perinatol 1978;5:335-50.
19 Brazy JE, Blackmon LR. Hypotension and bradycardiaassociated with air block in the neonate. J Pediatr1977;90:796.
20 Simmons DH, Hemingway A, Ricchiuti N. Acute circulatoryeffects of pneumothorax in dogs. J Appl Physiol 1958;12:257-60.