Embed Size (px)
Citation preview

Association of STAT4 rs7574865 polymorphism withautoimmune diseases: a meta-analysis
Ya-ling Liang • Hua Wu • Xi Shen •
Pei-qiang Li • Xiao-qing Yang • Li Liang •
Wei-hua Tian • Li-feng Zhang • Xiao-dong Xie
Received: 7 December 2011 / Accepted: 7 June 2012 / Published online: 20 June 2012
� Springer Science+Business Media B.V. 2012
Abstract The association between the signal transducer
and activator of transcription 4 (STAT4) gene rs7574865
single nucleotide polymorphism and different autoimmune
diseases remains controversial and ambiguous. We con-
ducted this study to investigate whether combined evi-
dence shows the association between STAT4 rs7574865
polymorphism and autoimmune diseases. Comprehensive
Medline search and review of the references were used to
get the relevant reports published before September 2011.
Meta-analysis was conducted for genotype T/T (recessive
effect), T/T ? G/T (dominant effect) and T allele in
random effects models. 40 studies with 90 comparisons
including 32 systemic lupus erythematosus (SLE), 19
rheumatoid arthritis (RA), 3 type 1 diabetes (T1D), 11
Systemeric Sclerosis (SSc), 4 inflammatory bowed dis-
eases (IBD), 3 Primary Sjogren’s syndrome (pSS), 4
juvenile idiopathic arthritis (JIA), 2 Primary antiphospho-
lipid syndrome (APS), 1 Autoimmune thyroid diseases, 1
multiple sclerosis, 1 Psoriasis, 1 Wegener’s granuloma-
tosis, 1 Type 2 diabetes, and 1 giant cell arteritis disease
were available for this meta-analysis. The overall odds
ratios for rs7574865 T-allele significantly increased in
SLE, RA, T1D, SSc, JIA, and APS (OR = 1.56, 1.25,
1.13, 1.34, 1.25, and 2.15, respectively, P \ 0.00001) and
in IBD-UC and pSS (OR = 1.11 and 1.33, respectively,
P \ 0.05). This meta-analysis demonstrates that the
STAT4 rs7574865 T allele confers susceptibility to SLE,
RA, T1D, SSc, JIA, APS, IBD-UC, and pSS patients,
supporting the hypothesis of association between STAT4
gene polymorphism and subgroup of autoimmune
diseases.
Keywords STAT4 � Polymorphism � Autoimmune
diseases � Meta-analysis
Introduction
Autoimmune diseases are a various group of complex
diseases caused by loss of immunologic tolerance to self-
antigens, which lead to immune-mediated destruction of
tissues and organs and affect up to 5 % of the world pop-
ulation [1, 2]. The pathogenesis of autoimmune diseases
has been widely considered to be multifactorial, with
genetics, epigenetics, and environments interplaying to
determine disease onset and progression [3–5]. In addition,
Electronic supplementary material The online version of thisarticle (doi:10.1007/s11033-012-1754-1) contains supplementarymaterial, which is available to authorized users.
Y. Liang � H. Wu � X. Shen � P. Li � X. Xie (&)
Key Laboratory of Preclinical Study for New Drugs of Gansu
Province, School of Basic Medical Sciences, Lanzhou
University, Lanzhou City 730000, Gansu Province, China
e-mail: [email protected]
Y. Liang � L. Zhang
Institute of Immunology, School of Basic Medical Sciences,
Lanzhou University, Lanzhou City 730000,
Gansu Province, China
X. Yang
Department of Internal Medicine, The Affiliated Lanzhou
Petrochemical Hospital, Lanzhou City 730060,
Gansu Province, China
L. Liang
Department of Pharmacy, The First Hospital of Lanzhou
University, Lanzhou City 730000, Gansu Province, China
W. Tian
Department of Laboratory Medicine, Traditional Chinese
Medicine Hospital of Gansu Province, Lanzhou City 730050,
Gansu Province, China
123
Mol Biol Rep (2012) 39:8873–8882
DOI 10.1007/s11033-012-1754-1

different autoimmune diseases often coexist within a
family and the increased concordance rates in monozygotic
twins than in dizygotic twins together suggest a hypothesis
that different diseases may share the major susceptibility
factors, which has been strengthened by findings through
meta-analyses of whole-genome scans [6–10]. Until now,
shared susceptibility genetic loci have been documented to
be associated with multiple autoimmune diseases, includ-
ing the genetic major histocompatibility complex (MHC)
and non-MHC polymorphisms [11, 12]. However, except
for MHC alleles associated with nearly all known auto-
immune diseases in diverse populations, it has been proven
difficult to identify non-MHC susceptibility genetic variants.
The single-nucleotide polymorphism (SNP) of signal
transducer and activator of transcription 4 (STAT4) gene
seems to be one of the best examples of a non-MHC
common susceptibility allele for autoimmunity [13].
STAT4 gene maps to chromosome 2q33 and encodes a
transcription factor which play pivotal roles in the differ-
entiation and proliferation of both T helper 1 (Th1) and
Th17 cells [14, 15]. Since Th1 and Th17 lineages are
crucial effectors in chronic inflammatory disorders, STAT4
gene may play an important role in the pathogenesis of
autoimmune diseases. To date, the SNP rs7574865 in
STAT4 gene has been reported to be associated with an
increased risk for diverse complex autoimmune diseases
even in different ethnic populations, such as rheumatoid
arthritis (RA) [16–26], systemic lupus erythematosus
(SLE) [18, 22, 26–32], Sjogren’s syndrome (SS) [33–35],
systemic sclerosis (SSc) [36–39]. However, there are some
autoimmune diseases or other ethnic populations in which
STAT4 rs7574865 does not appear to play a role in sus-
ceptibility [40–44].
We performed this meta-analysis to assess whether
combined evidence shows the association between the
STAT4 rs7574865 SNP and autoimmune diseases, and to
summarize the effect size of the polymorphism associated
with susceptibility of autoimmune diseases between ethnic
groups.
Materials and methods
Identification of eligible studies and data extraction
An exhausted search was conducted for studies on the
association of the STAT4 rs7574865 SNP with autoim-
mune diseases published before September 2011 in
Medline, Embase and Web of science by using combi-
nation of key words such as Medical Subject Heading
(MeSH) terms and/or text words: ‘signal transducer and
activator of transcription 4’, ‘STAT4’, ‘autoimmune
disease’ and ‘autoimmunity’, without restrictions on lan-
guage, race, ethnicity or geographic area. The references
in the studies were also reviewed to identify additional
studies on this topic. Autoimmune diseases were diag-
nosed according to their diagnose criteria. We excluded
those studies which contained overlapping data or fre-
quency of genotypes not in Hardy–Weinberg equilibrium
in controls. The following information was extracted from
each study: author, year of publication, ethnicity of the
study population, demographics, numbers of cases and
controls, and the allele and genotype frequency of the
rs7574865 polymorphism. Extraction from each study was
conducted independently by two authors and consensus
was achieved for all data.
Evaluation of the statistical association
Allele frequency of the STAT4 rs7574865 SNP were
determined by the allele counting method. Point estimates
of risks, ORs and their 95 % confidence intervals were
determined for each study. Hardy–Weinberg equilibrium
of the observed frequencies of genotypes in controls was
examined by using a Chi-square test. In this meta anal-
ysis, the contrasts of the allelic effect of T (variant allele)
versus G (common allele), and also T/T versus G/T ? G/
G genotypes as well as T/T ? G/T versus G/G genotypes
were examined. And these contrasts correspond to the
recessive and dominant effects of the T-allele, respec-
tively. The genotype-specific risk of T/T versus G/G and
G/T versus G/G were also analysed. Cochrane’s Q-sta-
tistics were used to assess the within- and between-study
variations or heterogeneity [45]. The heterogeneity test
was used to assess the null hypothesis that all studies
were evaluating the same effect. When a significant
Q-statistic (P \ 0.10) indicated heterogeneity across stud-
ies, the random effects model was used for meta-analysis,
and if heterogeneity across studies was not indicated, the
fixed effects model was used. Fixed effects assume that
genetic factors have similar effects on autoimmune dis-
eases susceptibility across all studies, and that observed
variations between studies are caused by chance alone [46].
Random effects model assumes that different studies may
have substantial diversity and assesses both within- and
between-study variation [47]. A recently developed mea-
sure I2 = 100 % 9 (Q - df)/Q was used to quantify the
effect of heterogeneity [45]. I2 ranges between 0 and
100 % and represents the proportion of between-study
variability that can be attributed to heterogeneity rather
than chance. Adjectives low, moderate and high were used
to define I2 values of 25, 50 and 75 %, respectively [45].
Potential publication bias was assessed by examining fun-
nel plots and using Egger’s test [48, 49]. When there was
8874 Mol Biol Rep (2012) 39:8873–8882
123

an indication of publication bias, we used trim and fill
method to estimate the number of missing studies and to
estimate an adjusted OR and its CI for the corresponding
studies [50]. Statistical manipulations were undertaken by
using program RevMan 5.0 (Oxford, UK) and STATA
10.0 (Statacorp., College Station, TX). The power of each
study was computed as the probability of detecting an
association between the STAT4 rs7574865 SNP and
autoimmune diseases at the 0.05 level of significance,
assuming an OR of 1.5 (small effect size). The power
analysis was performed by using the PS (power and sample
size calculation) software (version 3.0.43; 2009) [51],
which obtained from the website http://www.mc.vanderbilt.
edu/prevmed/ps/index.htm.
Results
Studies included in the meta-analysis
Fifty-two relevant studies with the STAT4 rs7574865 SNP
and autoimmune diseases were identified through Medline
and PubMed searches and a review of references. Seven
studies were excluded because they are not case–control
Table 1 Meta-analysis of the STAT4 rs7574865G [ T polymorphism in autoimmune diseases
Diseases Comparison Sample size No. of
studies
Test of association Test of heterogeneity Publication bias
Case Control OR 95 %CI P value Q P value I2 P value
SLE T versus G 22,798 39,620 32 1.56 1.51–1.62 <0.00001 34.53 0.30 10 0.062
GT ? TT versus GG 11,399 19,810 32 1.70 1.62–1.79 <0.00001 32.91 0.37 6
TT versus GT ?GG 11,399 19,810 32 1.97 1.83–2.12 <0.00001 21.74 0.89 0
RA T versus G 38,332 40,018 19 1.25 1.19–1.30 <0.00001 28.47 0.06 37 0.002
GT ? TT versus GG 19,166 20,009 19 1.26 1.21–1.31 <0.00001 22.80 0.20 21
TT versus GT ?GG 19,166 20,009 19 1.41 1.30–1.53 <0.00001 18.11 0.45 1
T1D T versus G 17,420 21,202 3 1.13 1.08–1.18 <0.00001 2.62 0.27 24
GT ? TT versus GG 8,710 10,601 3 1.15 1.08–1.22 <0.00001 2.57 0.28 22
TT versus GT ?GG 8,710 10,601 3 1.21 1.07–1.37 0.003 0.58 0.75 0
IBD T versus G 6,646 7,248 4 1.04 0.89–1.21 0.64 9.67 0.02 69
GT ? TT versus GG 3,323 3,624 4 1.06 0.89–1.25 0.53 8.18 0.04 63
TT versus GT ?GG 3,323 3,624 4 0.98 0.78–1.22 0.83 5.10 0.16 41
IBD-CD T versus G 3,718 7,248 4 0.97 0.81–1.17 0.75 9.48 0.02 68
GT ? TT versus GG 1,859 3,624 4 0.97 0.80–1.18 0.79 7.28 0.06 59
TT versus GT ?GG 1,859 3,624 4 0.88 0.56–1.39 0.59 7.29 0.06 59
IBD-UC T versus G 2,928 7,248 4 1.11 1.00–124 0.04 3.17 0.37 5
GT ? TT versus GG 1,464 3,624 4 1.17 1.03–1.33 0.04 3.14 0.37 5
TT versus GT ?GG 1,464 3,624 4 1.14 0.87–1.50 0.35 4.52 0.21 34
SSc T versus G 7,604 11,464 11 1.34 1.25–1.44 <0.00001 6.25 0.79 0 0.223
GT ? TT versus GG 3,802 5,732 11 1.34 1.23–1.47 <0.00001 4.84 0.90 0
TT versus GT ?GG 3,802 5,732 11 1.83 1.55–2.17 <0.00001 10.28 0.42 3
pSS T versus G 594 3,216 3 1.33 1.09–1.63 0.005 1.33 0.46 0
GT ? TT versus GG 297 1,608 3 1.45 1.12–1.88 0.005 0.31 0.86 0
TT versus GT ?GG 297 1,608 3 1.38 0.86–2.21 0.18 2.78 0.25 28
JIA T versus G 6,224 17,638 4 1.25 1.16–1.33 <0.00001 1.58 0.66 0
GT ? TT versus GG 3,112 8,819 4 1.30 1.19–1.41 <0.00001 1.39 0.71 0
TT versus GT ?GG 3,112 8,819 4 1.36 1.14–1.63 0.0007 1.29 0.73 0
APS T versus G 316 1,656 2 2.15 1.66–2.79 <0.00001 0.06 0.81 0
GT ? TT versus GG 158 828 2 2.76 1.91–3.98 <0.00001 0.20 0.65 0
TT versus GT ?GG 158 828 2 2.43 1.41–4.17 0.001 0.31 0.58 0
The bold-italics values in test of association are positive results with statistically significant differences (P \ 0.05)
The bold values in test of heterogeneity are positive results with statistically significant differences (P \ 0.10)
OR odds ratio, 95 % CI 95 % confidence interval, No. number, SLE systemic lupus erythematosus, RA rheumatoid arthritis, T1D Type 1 diabetes,
IBD inflammatory bowel disease, CD Crohn’s disease, UC ulcerative colitis, SSc systemeric sclerosis, pSS primary Sjogren’s syndrome, JIAjuvenile idiopathic arthritis, APS primary antiphospholipid syndrome
Mol Biol Rep (2012) 39:8873–8882 8875
123

Study or SubgroupBarton 2008-validationBarton 2008-WTCCCBen Hamad 2011Daha 2009Kelly 2010Kobayashi 2008-IORRAKobayashi 2008-RIKENKobayashi 2008-TukushimaLee 2007Liang 2011Martinez 2008Orozco 2009-DutchOrozco 2009-SpanishOrozco 2009-SwedishPalomina-Morales 2008Remmers 2007-EIRARemmers 2007-NARACRemmers 2007-ReplicationSuarez-Gestal 2009
Total (95% CI)Total eventsHeterogeneity: Tau² = 0.00; Chi² = 4.97, df = 4 (P = 0.29); I² = 20%Test for overall effec t: Z = 6.68 (P < 0.00001)
Events1658
88170
432215
1092822704795178303433457158198765340526665
3591
Total67983716
280170814462962221818822064
416111817521846
546514
3058121420262768
9542
Events13041288
67384176464581338601195272387538132258388575583784
2179
Total60485868
400173213201490187610001816
624143217862592
570820
1762261926523612
6806
Weight0.0%0.0%0.0%0.0%0.0%
24.4%25.1%18.0%24.6%
7.9%0.0%0.0%0.0%0.0%0.0%0.0%0.0%0.0%0.0%
100.0%
M-H, Random, 95% CI1.17 [1.08, 1.27]1.11 [1.00, 1.22]1.66 [1.14, 2.42]1.19 [1.02, 1.39]1.14 [0.92, 1.41]1.29 [1.13, 1.47]1.31 [1.15, 1.50]1.17 [1.00, 1.37]1.27 [1.11, 1.45]1.65 [1.27, 2.13]1.59 [1.32, 1.91]1.19 [1.01, 1.39]1.26 [1.09, 1.45]1.35 [1.03, 1.77]1.36 [1.08, 1.72]1.18 [1.03, 1.36]1.38 [1.18, 1.62]1.24 [1.09, 1.42]1.14 [1.01, 1.28]
1.29 [1.20, 1.39]
R A Control O dds Ratio Odds RatioM-H, Random, 95% CI
0.2 0.5 1 2 5C on trol R A
Study or SubgroupSuarez-Gestal 2009Remmers 2007-ReplicationRemmers 2007-NARACRemmers 2007-EIRAOrozco 2009-SwedishOrozco 2009-SpanishOrozco 2009-DutchMartinez 2008Daha 2009Barton 2008-WTCCCBarton 2008-validation
Total (95% CI)Total eventsHeterogeneity: Tau² = 0.00; Chi² = 16.95, df = 10 (P = 0.08); I² = 41%Test for overall effect: Z = 7.26 (P < 0.00001)
Events665526340765158457433303432881
1658
6618
Total2768202612143058
546184617521118170837166798
26550
Events784583575388132538387272384
12881304
6635
Total3612265226191762
570259217861432173258686048
30673
Weight11.0%
9.4%7.9%9.1%3.4%8.9%7.9%6.1%7.8%
13.2%15.1%
100.0%
M-H, Random, 95% CI1.14 [1.01, 1.28]1.24 [1.09, 1.42]1.38 [1.18, 1.62]1.18 [1.03, 1.36]1.35 [1.03, 1.77]1.26 [1.09, 1.45]1.19 [1.01, 1.39]1.59 [1.32, 1.91]1.19 [1.02, 1.39]1.11 [1.00, 1.22]1.17 [1.08, 1.27]
1.22 [1.16, 1.29]
RA Control Odds Ratio Odds RatioM-H, Random, 95% CI
0.2 0.5 1 2 5Control RA
AStudy or SubgroupBarton 2008-validationBarton 2008-WTCCCBen Hamad 2011Daha 2009Kelly 2010Kobayashi 2008-IORRAKobayashi 2008-RIKENKobayashi 2008-TukushimaLee 2007Liang 2011Martinez 2008Orozco 2009-DutchOrozco 2009-SpanishOrozco 2009-SwedishPalomina-Morales 2008Remmers 2007-EIRARemmers 2007-NARACRemmers 2007-ReplicationSuarez-Gestal 2009
Total (95% CI)Total eventsHeterogeneity: Tau² = 0.00; Chi² = 28.65, df = 18 (P = 0.05); I² = 37%Test for overall effect : Z = 9.83 (P < 0.00001)
Events1658
88170
432215
1092822704795178303433457158198765340526665
10692
Total67983716
280170814462962221818822064
416111817521846
546514
3058121420262768
38332
Events13041288
67384176464581338601195272387538132258388575583784
9315
Total60485868
400173213201490187610001816
624143217862592
570820
1762261926523612
40019
Weight9.9%8.7%1.2%5.1%3.3%6.4%6.5%5.0%6.4%2.4%4.1%5.2%5.9%2.3%2.9%6.0%5.2%6.2%7.3%
100.0%
M-H, Random, 95% CI1.17 [1.08, 1.27]1.11 [1.00, 1.22]1.66 [1.14, 2.42]1.19 [1.02, 1.39]1.14 [0.92, 1.41]1.29 [1.13, 1.47]1.31 [1.15, 1.50]1.17 [1.00, 1.37]1.27 [1.11, 1.45]1.65 [1.27, 2.13]1.59 [1.32, 1.91]1.19 [1.01, 1.39]1.26 [1.09, 1.45]1.35 [1.03, 1.77]1.36 [1.08, 1.72]1.18 [1.03, 1.36]1.38 [1.18, 1.62]1.24 [1.09, 1.42]1.14 [1.01, 1.28]
1.25 [1.19, 1.30]
RA Control Odds Ratio Odds RatioM-H, Random, 95% CI
0.2 0.5 1 2 5Control RA
B
C
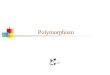
Fig. 1 ORs and 95 % CI of individual studies and pooled data for stratification study of the association of the STAT4 rs7574865 T allele and
RA. Heterogeneity disappeared in subgroups. a Results in total patients. b Results in Asians. c Results in European
8876 Mol Biol Rep (2012) 39:8873–8882
123

study or contain duplicated results. And 45 studies met the
inclusion criteria, of these, four studies were finally
excluded because of no sufficient genotype data [52, 53] or
strongly deviation from Hardy–Weinberg equilibrium [23,
54], and one study was excluded because of using osteo-
arthritis patients as controls [16]. Since different studies or
subgroups in each study were treated independently, a total
of 90 comparisons including 32 SLE, 19 RA, 3 type 1
diabetes (T1D), 11 Systemeric Sclerosis (SSc), 4 inflam-
matory bowel diseases (IBD), 3 Primary Sjogren’s syn-
drome (pSS), 4 JIA, 2 Primary antiphospholipid syndrome
(APS), 1 Autoimmune thyroid diseases (AITD), 1 multiple
sclerosis (MS), 1 Psoriasis (Ps), 1 Wegener’s granuloma-
tosis (WG), 1 Type 2 diabetes (T2D), and 1 giant cell
arteritis (GCA) disease were available for this meta-anal-
ysis (Table S1).
Association of the STAT4 rs7574865 SNP
and susceptibility of autoimmune diseases
The overall ORs for T allele, T/T and T/T ? G/T geno-
types in SLE, RA, T1D, SSc, pSS, JIA, and APS patients
were significantly increased than those in controls
(Table 1; Fig. S1, Fig. 1). The meta-analysis of the STAT4
rs7574865 SNP showed TT genotype (recessive effect),
GT ? TT genotype (dominant effect) and the risk T-allele
associated with susceptibility of SLE, RA, T1D, SSc, JIA,
and APS (Table 1). The overall ORs for T-allele were 1.56,
1.25, 1.13, 1.34, 1.25, and 2.15 in SLE, RA, T1D, SSc, JIA,
and APS, respectively (P \ 0.00001). The meta-analysis
also showed the association of TT ? GT genotype
(OR = 1.45, 95 % CI = 1.12–1.88, P = 0.005) and
T-allele (OR = 1.33, 95 % CI = 1.09–1.63, P = 0.005)
with pSS, but not TT genotype. There was no association
of the STAT4 rs7574865T allele and susceptibility of IBD.
However, when stratified IBD in IBD-CD and IBD-UC
subgroups, T-allele and G/T ? T/T genotype significantly
associated with IBD-UC (OR = 1.11, 95 % CI =
1.00–1.24, P = 0.04; OR = 1.17, 95 % CI = 1.03–1.33,
P = 0.04, respectively; Table 2 and Fig. 2), no association
were observed between STAT4 rs7574865T allele and
IBD-CD. The genotype-specific analysis also showed a
dose–response relation between the T-allele and the risk of
the autoimmune diseases (Table 2).
Table 2 Meta-analysis of genotype-based risk of STAT4 rs7574865G [ T polymorphism in autoimmune diseases
Diseases Comparison Sample size No. of
studies
Test of association Test of heterogeneity
Case Control OR 95 %CI P value Q P value I2
SLE GT versus GG 9,565 18,015 32 1.54 1.46–1.63 <0.00001 25.66 0.74 0
TT versus GG 6,046 11,597 32 2.48 2.29–2.69 <0.00001 27.90 0.63 0
RA GT versus GG 17,591 18,886 19 1.22 1.17–1.27 <0.00001 0.00 0.64 0
TT versus GG 11,624 12,941 19 1.54 1.42–1.68 <0.00001 22.39 0.22 20
T1D GT versus GG 8,189 10,089 3 1.14 1.05–1.24 0.003 0.00 0.34 8
TT versus GG 5,498 7,221 3 1.50 0.98–2.29 0.06 0.09 0.08 61
IBD GT versus GG 3,162 3,456 4 1.03 0.93–1.14 0.57 6.07 0.11 51
TT versus GG 2,157 2,409 4 1.00 0.79–1.25 0.97 6.16 0.10 51
IBD-CD GT versus GG 1,781 3,456 4 0.96 0.85–1.09 0.55 5.00 0.17 40
TT versus GG 1,240 2,409 4 0.87 0.53–1.44 0.60 8.50 0.04 65
IBD-UC GT versus GG 1,381 3,456 4 1.13 0.99–1.29 0.07 3.32 0.34 10
TT versus GG 916 2,409 4 1.22 0.92–1.61 0.17 3.61 0.31 17
SSc GT versus GG 3,468 5,422 11 1.25 1.14–1.37 <0.00001 5.90 0.82 0
TT versus GG 2,312 3,698 11 1.99 1.67–2.37 <0.00001 8.92 0.54 0
pSS GT versus GG 272 579 3 1.48 1.13–1.94 0.004 0.23 0.89 0
TT versus GG 168 1,056 3 1.73 1.06–2.82 0.03 1.50 0.47 0
JIA GT versus GG 2,905 8,397 4 1.27 1.16–1.39 <0.00001 1.16 0.76 0
TT versus GG 1,887 5,785 4 1.50 1.25–1.79 <0.0001 1.45 0.69 0
APS GT versus GG 136 765 2 2.57 1.75–3.78 <0.00001 0.62 0.43 0
TT versus GG 78 522 2 3.71 2.05–6.70 <0.00001 0.13 0.72 0
The bold-italics values are positive results with statistically significant differences (P \ 0.05)
The bold values are marginal significance values (P near 0.05)
OR odds ratio, 95 % CI 95 % confidence interval, No. number, SLE systemic lupus erythematosus, RA rheumatoid arthritis, T1D type 1 diabetes,
IBD inflammatory bowel disease, CD Crohn’s disease, UC ulcerative colitis, SSc systemeric sclerosis, pSS primary Sjogren’s syndrome, JIAjuvenile idiopathic arthritis, APS primary antiphospholipid syndrome
Mol Biol Rep (2012) 39:8873–8882 8877
123

Evaluation of study quality and heterogeneity
The distribution of the genotype in the control group of
each study in this meta-analysis was consistent with
Hardy–Weinberg equilibrium. The statistical power of each
study ranged from 22.4 to 100 % (Table S1). Forty-six of
the 90 comparisons used in this meta-analysis had more
than 80 % statistical power to an effect, and excluding the
low power study did not materially affect the overall
results. Heterogeneity was found in meta-analysis for
T-allele and RA and for T-allele and G/T ? T/T genotype
and IBD. For RA, heterogeneity disappeared when
restricted the study just in Asians or in Europeans and
yielded largely similar result to those from the total dataset
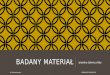
(Fig. 1). For IBD patients, heterogeneity disappeared in
IBD-UC and also IBD-CD subgroups after excluding the
highest OR, and an interesting phenomenon on the protect
effect of T-allele against IBD-CD appeared (Fig. 2).
Evaluation of sensitivity and publication bias
Sensitivity analyses of different diseases yielded very
similar results compared to those got from the total dataset.
Publication bias was found for the meta-analysis of SLE and
RA diseases (Table 1); therefore, we used the ‘‘trim and
fill’’ method to correct the publication bias and its impact on
pooled estimated of OR (Fig. 3), the estimated number of
missing studies is 5 for SLE and 6 for RA, and the adjusted
pooled OR estimated is 1.544 (95 % CI 1.466–1.627) for
SLE and 1.12 (95 % CI 1.142–1.262) for RA, which still
significantly increased the risk for SLE and RA, respec-
tively. No publication bias was found in the meta-analysis
Study or SubgroupDiaz-Gallo 2010Glas 2010Martinez 2008Moon 2010
Total (95% CI)Total eventsHeterogeneity: Tau² = 0.02; Chi² = 9.67, df = 3 (P = 0.02); I² = 69%Test for overall effect: Z = 0.47 (P = 0.64)
Events374524313277
1488
Total180026421348856
6646
Events538595272146
1551
Total259227661432458
7248
Weight27.5%29.1%24.2%19.1%
100.0%
M-H, Random, 95% CI1.00 [0.86, 1.16]0.90 [0.79, 1.03]1.29 [1.07, 1.55]1.02 [0.80, 1.30]
1.04 [0.89, 1.21]
IBD Control Odds Ratio Odds RatioM-H, Random, 95% CI
0.2 0.5 1 2 5Control IBD
Study or SubgroupDiaz-Gallo 2010Glas 2010Martinez 2008Moon 2010
Total (95% CI)Total eventsHeterogeneity: Chi² = 3.17, df = 3 (P = 0.37); I² = 5%Test for overall effect: Z = 2.03 (P = 0.04)
Events185199163167
714
Total804928704492
2928
Events538595272146
1551
Total259227661432458
7248
Weight29.3%35.1%20.6%14.9%
100.0%
M-H, Fixed, 95% CI1.14 [0.94, 1.38]1.00 [0.83, 1.19]1.28 [1.03, 1.60]1.10 [0.84, 1.44]
1.11 [1.00, 1.24]
IBD Control Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.2 0.5 1 2 5Control IBD-UC
Study or SubgroupDiaz-Gallo 2010Glas 2010Martinez 2008Moon 2010
Total (95% CI)Total eventsHeterogeneity: Tau² = 0.02; Chi² = 9.48, df = 3 (P = 0.02); I² = 68%Test for overall effect: Z = 0.31 (P = 0.75)
Events189326150110
775
Total996
1714644364
3718
Events538595272146
1551
Total259227661432
458
7248
Weight27.2%30.0%24.0%18.9%
100.0%
M-H, Random, 95% CI0.89 [0.74, 1.08]0.86 [0.74, 1.00]1.29 [1.03, 1.62]0.93 [0.69, 1.25]
0.97 [0.81, 1.17]
IBD Control Odds Ratio Odds RatioM-H, Random, 95% CI
0.2 0.5 1 2 5Control IBD-CD
Study or SubgroupDiaz-Gallo 2010Glas 2010Martinez 2008Moon 2010
Total (95% CI)Total eventsHeterogeneity: Chi² = 0.26, df = 2 (P = 0.88); I² = 0%Test for overall effect: Z = 2.33 (P = 0.02)
Events189326150110
625
Total996
1714644364
3074
Events538595272146
1279
Total259227661432458
5816
Weight34.5%52.6%
0.0%12.9%
100.0%
M-H, Fixed, 95% CI0.89 [0.74, 1.08]0.86 [0.74, 1.00]1.29 [1.03, 1.62]0.93 [0.69, 1.25]
0.88 [0.79, 0.98]
IBD Control Odds Ratio Odds RatioM-H, Fixed, 95% CI
0.2 0.5 1 2 5Control IBD-CD
A
B
C
D
Fig. 2 ORs and 95 % CI of
individual studies and pooled
data for stratification study of
the association of the STAT4
rs7574865 T allele and IBD.
The aggregate OR and 95 %CI
of the risk allele are also given.
Heterogeneity disappeared in
the subgroups of IBD-UC and
IBD-CD after excluding the
highest OR study. a Results for
total patients. b Results for IBD-
UC. c Results for IBD-CD. D:
Results for IBD-CD after
excluded Martinez’s study
8878 Mol Biol Rep (2012) 39:8873–8882
123

of SSc. And we didn’t perform the publication bias analysis
on those of which the study number was less than five.
Discussion
As is known, the size of case–control studies often is a
limiting factor to produce enough power to detect any but
the most strongly associated loci. Meta-analysis of existing
data provides an obvious potential solution for resolving
contradictory results and increasing the statistical power
[55, 56]. In the present study, we combined the evidence on
the association of the STAT4 rs7574865 SNP and sus-
ceptibility of autoimmune diseases. The results of this
meta-analysis provide strong evidence on an association of
the STAT4 rs7574865 SNP with autoimmune diseases
including SLE, RA, T1D, SSc, pSS, JIA, and APS. In
addition, there was also a trend to increase the OR for TT
genotype compared with that for GT ? TT genotype in
autoimmune diseases, indicating that individuals with
homozygous for the T-allele may have the greatest risk of
multiple autoimmune diseases.
Autoimmune diseases usually share several clinical
signs and symptoms, have common pathogenesis and
genetic factors, and this phenomenon has been described as
‘‘autoimmune tautology’’ [57]. Non-random clustering of
disease susceptibility loci has been observed in both rodent
models of autoimmune disease and linkage studies of
human autoimmune diseases [57–59]. The accumulating
common genetic background evidence for autoimmune
diseases inferred that the phenotypes of autoimmune dis-
eases may have a clinical behaviour independent from their
genetic causes, and perhaps underlie similar immunoge-
netic mechanism, which will be helpful to us understand
the common mechanisms of these disorders and to discover
new therapeutic interventions [60]. This finding that the
STAT4 rs7574865T allele is associated with subgroup of
autoimmune diseases provides further support for the idea
that susceptibility to multiple autoimmune diseases may
have some common alleles or pathways, which is similar to
Lee’s results [61].
No association was found between the STAT4 rs7574
865T allele and IBD, however, the STAT4 rs7574865T
allele did show a risk effect to IBD-UC subgroup but a
protective effect against IBD-CD after excluded the
greatest OR which caused the heterogeneity, and this result
was consistent with previous report by Diaz-Gallo [42],
which adding a further example of the differences in
genetic background between these two intestinal inflam-
matory disorders [42], and suggested that they are more
likely to share some genetic susceptibility loci but differ at
others [62].
STAT4 is a key signaling molecule for IL-12, IL-17,
IL-23 and type IIFNs in T cells and NK cells. IL-12, IL-17
and IL-23 are important cytokines to activate STAT4 and
then to direct Th cells toward the differentiation of Th1 and
Th17 cells, respectively [15, 63]. Upon cytokine signalling,
STAT4 is phosphorylated and forms homodimers which
translocate to the nucleus and initiate transcription of
STAT4 target genes [14]. Genetic variants of STAT4 may
be involved in regulating the balance of IL-12 versus IL-23
effect, and then affect the prevalence of inflammatory
diseases via dysregulation of the Th1 and Th17 differen-
tiation. Studies on mouse models of infectious and
inflammatory diseases have revealed that STAT4 is an
important factor to mediate inflammatory immunity [64].
STAT4-deficient mice display less severe disease and
decreased parameters of inflammation compared with wild
type mice [65–70]. Inhibitory oligodeoxy-nucleotides or
antisense oligonucleotides targeting at STAT4 could sup-
press the disease in arthritis models [71]. All these studies
and the association of STAT4 with different autoimmune
diseases suggest that STAT4 is very important in the
development of inflammatory process and may be a suit-
able therapeutic target for autoimmune diseases.
Filled funnel plot with pseudo 95% confidence limits
Filled funnel plot with pseudo 95% confidence limitsth
eta
, fil
led
s.e. of: theta, filled
0 .1 .2
-.2
0
.2
.4
.6
theta
, fil
led
s.e. of: theta, filled
0 .1 .2 .3
0
1
2
3
A
B
Fig. 3 Funnel plot with 95 % CI of studies on STAT4 re7574865T
alelle and SLE (a) and RA (b) by trim and fill method
Mol Biol Rep (2012) 39:8873–8882 8879
123

The susceptibility SNP rs7574865 is located within
intron 3 of STAT4, a noncoding region, it is suspected that
it may influence the gene expression of STAT4 on the level
of transcription and spice variation [13], or it may be linked
to causative mutations. Until now, the main alternatively
spliced isoforms of STAT4 have been described as
STAT4a and STAT4b. STAT4b is the shorter form of the
full-length STAT4a by lacking 44 amino acids at the C
terminus and is not as efficient as STAT4a in directly
inducing IFN-c gene expression activated by IL-12 in Th1
cells [72]. A recent study reported that a different level of
expression of STAT4 in osteoblasts was correlated with the
STAT4 risk haplotype [73]. And the expression level of
STAT4 in Peripheral Blood Mononuclear Cell (PBMC)
was also reported to be correlated with the risk allele of
STAT4 rs7574865 [27]. The precisely mechanisms of the
intronic risk SNP influencing cell type-specific gene
expression remain to be defined [74].
The potential limitations of these studies may be heter-
ogeneity and publication bias. In order to avoid the hetero-
geneity and publication bias existed in RA and IBD studies
compromising the interpretation of the meta-analysis, we
conducted stratified analysis to identify the sources of heter-
ogeneity. For RA, Asian studies showed similar OR with those
of population of European origin and statistical analysis found
no evidence of heterogeneity. For IBD, stratified studies in UC
and CD showed reversed results and the heterogeneity dis-
appeared when excluded one study. We also used trim and fill
method to correct the publication bias existed in SLE and RA
studies and found it did not materially alter the results.
Therefore, the results of this meta-analysis are not much likely
affected by these limitations. Since the subgroup of analysis
for T1D, IBD, pSS, JIA, and APS included no more than five
studies for the meta-analysis, we could not draw funnel plots
for each of them. This may not have enough power to explore
the association between the STAT4 rs7574865T SNP and
these diseases.
Conclusion
This meta-analysis demonstrates that STAT4 rs7574865
SNP confers susceptibility to autoimmune diseases
including SLE, RA, T1D, SSc, pSS, JIA, and APS, which
provides further evidence on the involvement of STAT4
gene in the aetiology of subgroup of autoimmune diseases
and also supports the hypothesis that common genes
underlie diverse autoimmune phenotypes.
Acknowledgments This work was funded by platform of Genetic
Resource of Chinese Population Project, Ministry of Science and
Technology of P. R. China (Grant No.2006DKA21301) and the
National Natural Science Foundation of China (Grant No. 81071701
and No. 30972708).
References
1. Marrack P, Kappler J, Kotzin BL (2001) Autoimmune disease:
why and where it occurs. Nat Med 7:899–905
2. Davies AJ (2008) Immunological tolerance and the autoimmune
response. Autoimmun Rev 7:538–543
3. Lleo A, Battezzati PM, Selmi C, Gershwin ME, Podda M (2008)
Is autoimmunity a matter of sex? Autoimmun Rev 7:626–630
4. Boscolo P, Youinou P, Theoharides TC, Cerulli G, Conti P
(2008) Environmental and occupational stress and autoimmunity.
Autoimmun Rev 7:340–343
5. Invernizzi P, Gershwin ME (2009) The genetics of human
autoimmune disease. J Autoimmun 33:290–299
6. Simpson CR, Anderson WJ, Helms PJ, Taylor MW, Watson L,
Prescott GJ, Godden DJ, Barker RN (2002) Coincidence of
immune-mediated diseases driven by Th1 and Th2 subsets sug-
gests a common aetiology. A population-based study using
computerized general practice data. Clin Exp Allergy 32:37–42
7. Heward J, Gough SC (1997) Genetic susceptibility to the
development of autoimmune disease. Clin Sci (Lond) 93:479–
491
8. Corporaal S, Bijl M, Kallenberg CG (2002) Familial occurrence
of autoimmune diseases and autoantibodies in a Caucasian pop-
ulation of patients with systemic lupus erythematosus. Clin
Rheumatol 21:108–113
9. Becker KG (2001) The common genetic hypothesis of autoim-
mune/inflammatory disease. Curr Opin Allergy Clin Immunol
1:399–405
10. Morahan G, Peeva V, Mehta M, Williams R (2008) Systems
genetics can provide new insights into immune regulation and
autoimmunity. J Autoimmun 31:233–236
11. McCluskey J, Peh CA (1999) The human leucocyte antigens and
clinical medicine: an overview. Rev Immunogenet 1:3–20
12. Brand O, Gough SC, Heward J (2005) HLA, CTLA-4 and
PTPN22:the shared genetic master-key to autoimmunity? Expert
Rev Mol Med 7:1–15
13. Korman BD, Kastner DL, Gregersen PK, Remmers EF (2008)
STAT4: genetics, mechanisms, and implications for autoimmu-
nity. Curr Allergy Asthma Rep 8:398–403
14. Watford WT, Hissong BD, Bream JH, Kamnno Y, Muul L,
O’Shea JJ (2004) Signaling by IL-12 and IL-23 and the immu-
noregulatory roles of STAT4. Immunol Rev 202:139–156
15. Mathur AN, Chang HC, Zisoulis DG, Stritesky GL, Yu Q,
O’Malley JT, Kapur R, Levy DE, Kansas GS, Kaplan MH (2007)
Stat3 and Stat4 direct development of IL-17-secreting Th cells.
J Immunol 178:4901–4907
16. Stark K, Rovensky J, Blazickova S, Grosse-Wilde H, Ferencik S,
Hengstenberg C, Straub RH (2009) Association of common
polymorphisms in known susceptibility genes with rheumatoid
arthritis in a Slovak population using osteoarthritis patients as
controls. Arthritis Res Ther 11:R70
17. Daha NA, Kurreeman FA, Marques RB, Stoeken-Rijsbergen G,
Verduijn W, Huizinga TW, Toes RE (2009) Confirmation of
STAT4, IL2/IL21, and CTLA4 polymorphisms in rheumatoid
arthritis. Arthritis Rheum 60:1255–1260
18. Kobayashi S, Ikari K, Kaneko H, Kochi Y, Yamamoto K, Shi-
mane K, Nakamura Y, Toyama Y, Mochizuki T, Tsukahara S
et al (2008) Association of STAT4 with susceptibility to rheu-
matoid arthritis and systemic lupus erythematosus in the Japanese
population. Arthritis Rheum 58:1940–1946
19. Martinez A, Varade J, Marquez A, Cenit MC, Espino L, Perdi-
gones N, Santiago JL, Fernandez-Arquero M, de la Calle H,
Arroyo R et al (2008) Association of the STAT4 gene with
increased susceptibility for some immune-mediated diseases.
Arthritis Rheum 58:2598–2602
8880 Mol Biol Rep (2012) 39:8873–8882
123

20. Orozco G, Alizadeh BZ, Delgado-Vega AM, Gonzalez-Gay MA,
Balsa A, Pascual-Salcedo D, Fernandez-Gutierrez B, Gonzalez-
Escribano MF, Petersson IF, van Riel PL et al (2008) Association
of STAT4 with rheumatoid arthritis: a replication study in three
European populations. Arthritis Rheum 58:1974–1980
21. Suarez-Gestal M, Calaza M, Dieguez-Gonzalez R, Perez-Pampin
E, Pablos JL, Navarro F, Narvaez J, Marenco JL, Herrero-Beau-
mont G, Fernandez-Gutierrez B et al (2009) Rheumatoid arthritis
does not share most of the newly identified systemic lupus ery-
thematosus genetic factors. Arthritis Rheum 60:2558–2564
22. Palomino-Morales RJ, Rojas-Villarraga A, Gonzalez CI, Ramirez
G, Anaya JM, Martin J (2008) STAT4 but not TRAF1/C5 vari-
ants influence the risk of developing rheumatoid arthritis and
systemic lupus erythematosus in Colombians. Genes Immun
9:379–382
23. Zervou MI, Sidiropoulos P, Petraki E, Vazgiourakis V, Krasou-
daki E, Raptopoulou A, Kritikos H, Choustoulaki E, Boumpas
DT, Goulielmos GN (2008) Association of a TRAF1 and a
STAT4 gene polymorphism with increased risk for rheumatoid
arthritis in a genetically homogeneous population. Hum Immunol
69:567–571
24. Barton A, Thomson W, Ke X, Eyre S, Hinks A, Bowes J, Gib-
bons L, Plant D, Wilson AG, Marinou I et al (2008) Re-evalua-
tion of putative rheumatoid arthritis susceptibility genes in the
post-genome wide association study era and hypothesis of a key
pathway underlying susceptibility. Hum Mol Genet 17:2274–
2279
25. Lee HS, Remmers EF, Le JM, Kastner DL, Bae SC, Gregersen
PK (2007) Association of STAT4 with rheumatoid arthritis in the
Korean population. Mol Med 13:455–460
26. Remmers EF, Plenge RM, Lee AT, Graham RR, Hom G, Behrens
TW, de Bakker PI, Le JM, Lee HS, Batliwalla F et al (2007)
STAT4 and the risk of rheumatoid arthritis and systemic lupus
erythematosus. N Engl J Med 357:977–986
27. Abelson AK, Delgado-Vega AM, Kozyrev SV, Sanchez E, Ve-
lazquez-Cruz R, Eriksson N, Wojcik J, Linga Reddy MV, Lima
G, D’Alfonso S et al (2009) STAT4 associates with systemic
lupus erythematosus through two independent effects that cor-
relate with gene expression and act additively with IRF5 to
increase risk. Ann Rheum Dis 68:1746–1753
28. Kawasaki A, Ito I, Hikami K, Ohashi J, Hayashi T, Goto D,
Matsumoto I, Ito S, Tsutsumi A, Koga M et al (2008) Role of
STAT4 polymorphisms in systemic lupus erythematosus in a
Japanese population: a case-control association study of the
STAT1-STAT4 region. Arthritis Res Ther 10:R113
29. Suarez-Gestal M, Calaza M, Endreffy E, Pullmann R, Ordi-Ros J,
Domenico Sebastiani G, Ruzickova S, Jose Santos M, Papaste-
riades C, Marchini M et al (2009) Replication of recently iden-
tified systemic lupus erythematosus genetic associations: a case-
control study. Arthritis Res Ther 11:R69
30. Yang W, Ng P, Zhao M, Hirankarn N, Lau CS, Mok CC, Chan
TM, Wong RW, Lee KW, Mok MY et al (2009) Population
differences in SLE susceptibility genes: STAT4 and BLK, but not
PXK, are associated with systemic lupus erythematosus in Hong
Kong Chinese. Genes Immun 10:219–226
31. Kiyohara C, Washio M, Horiuchi T, Tada Y, Asami T, Ide S,
Atsumi T, Kobashi G, Takahashi H (2009) Cigarette smoking,
STAT4 and TNFRSF1B polymorphisms, and systemic lupus ery-
thematosus in a Japanese population. J Rheumatol 36:2195–2203
32. Harley JB, Alarcon-Riquelme ME, Criswell LA, Jacob CO,
Kimberly RP, Moser KL, Tsao BP, Vyse TJ, Langefeld CD, Nath
SK et al (2008) Genome-wide association scan in women with
systemic lupus erythematosus identifies susceptibility variants in
ITGAM, PXK, KIAA1542 and other loci. Nat Genet 40:204–210
33. Korman BD, Alba MI, Le JM, Alevizos I, Smith JA, Nikolov NP,
Kastner DL, Remmers EF, Illei GG (2008) Variant form of
STAT4 is associated with primary Sjogren’s syndrome. Genes
Immun 9:267–270
34. Nordmark G, Kristjansdottir G, Theander E, Eriksson P, Brun JG,
Wang C, Padyukov L, Truedsson L, Alm G, Eloranta ML et al
(2009) Additive effects of the major risk alleles of IRF5 and
STAT4 in primary Sjogren’s syndrome. Genes Immun 10:68–76
35. Palomino-Morales RJ, Diaz-Gallo LM, Witte T, Anaya JM,
Martin J (2010) Influence of STAT4 polymorphism in primary
Sjogren’s syndrome. J Rheumatol 37:1016–1019
36. Tsuchiya N, Kawasaki A, Hasegawa M, Fujimoto M, Takehara
K, Kawaguchi Y, Kawamoto M, Hara M, Sato S (2009) Asso-
ciation of STAT4 polymorphism with systemic sclerosis in a
Japanese population. Ann Rheum Dis 68:1375–1376
37. Dieude P, Guedj M, Wipff J, Ruiz B, Hachulla E, Diot E, Granel
B, Sibilia J, Tiev K, Mouthon L et al (2009) STAT4 is a genetic
risk factor for systemic sclerosis having additive effects with
IRF5 on disease susceptibility and related pulmonary fibrosis.
Arthritis Rheum 60:2472–2479
38. Gourh P, Agarwal SK, Divecha D, Assassi S, Paz G, Arora-Singh
RK, Reveille JD, Shete S, Mayes MD, Arnett FC, Tan FK (2009)
Polymorphisms in TBX21 and STAT4 increase the risk of sys-
temic sclerosis: evidence of possible gene–gene interaction and
alterations in Th1/Th2 cytokines. Arthritis Rheum 60:3794–3806
39. Rueda B, Broen J, Simeon C, Hesselstrand R, Diaz B, Suarez H,
Ortego-Centeno N, Riemekasten G, Fonollosa V, Vonk MC et al
(2009) The STAT4 gene influences the genetic predisposition to
systemic sclerosis phenotype. Hum Mol Genet 18:2071–2077
40. Lee HS, Park H, Yang S, Kim D, Park Y (2008) STAT4 poly-
morphism is associated with early-onset type 1 diabetes, but not
with late-onset type 1 diabetes. Ann N Y Acad Sci 1150:93–98
41. Kelley JM, Hughes LB, Malik A, Danila MI, Edberg Y, Alarcon
GS, Conn DL, Jonas BL, Callahan LF, Smith EA et al (2010)
Genetic variants of STAT4 associated with rheumatoid arthritis in
persons of Asian and European ancestry do not replicate in
African Americans. Ann Rheum Dis 69:625–626
42. Diaz-Gallo LM, Palomino-Morales RJ, Gomez-Garcia M, Car-
dena C, Rodrigo L, Nieto A, Alcain G, Cueto I, Lopez-Nevot
MA, Martin J (2010) STAT4 gene influences genetic predispo-
sition to ulcerative colitis but not Crohn’s disease in the Spanish
population: a replication study. Hum Immunol 71:515–519
43. Palomino-Morales R, Vazquez-Rodriguez TR, Morado IC, Cas-
taneda S, Ortego-Centeno N, Miranda-Filloy JA, Lamas JR,
Martin J, Gonzalez-Gay MA (2009) Lack of association between
STAT4 gene polymorphism and biopsy-proven giant cell arteri-
tis. J Rheumatol 36:1021–1025
44. Wieczorek S, Holle JU, Muller S, Fricke H, Gross WL, Epplen JT
(2009) A functionally relevant IRF5 haplotype is associated with
reduced risk to Wegener’s granulomatosis. J Mol Med 88:413–421
45. Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a
meta-analysis. Stat Med 21:1539–1558
46. Egger M, Smith GD, Phillips A (1997) Meta-analysis: principles
and procedures. NBMJ 315:1533–1537
47. DerSimonian R, Laird N (1986) Meta-analysis in clinical trials.
Control Clin Trials 7:177–188
48. Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in
meta-analysis detected by a simple, graphical test. BMJ 315:
629–634
49. Begg CB, Mazumdar M (1994) Operating characteristics of a
rank correlation test for publication bias. Biometrics 50:
1088–1101
50. Duval S, Tweedie R (2000) Trim and fill: a simple funnel-plot-
based method of testing and adjusting for publication bias in
meta-analysis. Biometrics 56:455–463
51. Dupont WD, Plummer WD Jr (1990) Power and sample size
calculations. A review and computer program. Control Clin Trials
11:116–128
Mol Biol Rep (2012) 39:8873–8882 8881
123

52. Fredi M, Tincani A, Yin H, Delgado-Vega AM, Borghi MO,
Meroni PL, Alarcon-Riquelme ME (2010) IRF5 is associated
with primary antiphospholipid syndrome, but is not a major risk
factor. Arthritis Rheum 62:1201–1202
53. Sanchez E, Nadig A, Richardson BC, Freedman BI, Kaufman
KM, Kelly JA, Niewold TB, Kamen DL, Gilkeson GS, Ziegler JT
et al (2011) Phenotypic associations of genetic susceptibility loci
in systemic lupus erythematosus. Ann Rheum Dis 70:1752–1757
54. Zervou MI, Mamoulakis D, Panierakis C, Boumpas DT, Goul-
ielmos GN (2008) STAT4: a risk factor for type 1 diabetes? Hum
Immunol 69:647–650
55. Attia J, Ioannidis JP, Thakkinstian A, McEvoy M, Scott RJ,
Minelli C, Thompson J, Infante-Rivard C, Guyatt G (2009) How
to use an article about genetic association: B: are the results of the
study valid? JAMA 301:191–197
56. Zintzaras E, Lau J (2008) Synthesis of genetic association studies
for pertinent gene-disease associations requires appropriate
methodological and statistical approaches. J Clin Epidemiol
61:634–645
57. Anaya JM (2010) The autoimmune tautology. Arthritis Res Ther
12:147
58. Becker KG (2004) The common variants/multiple disease
hypothesis of common complex genetic disorders. Med Hypothe-
ses 62:309–317
59. Tait KF, Marshall T, Berman J, Carr-Smith J, Rowe B, Todd JA,
Bain SC, Barnett AH, Gough SC (2004) Clustering of autoim-
mune disease in parents of siblings from the Type 1 diabetes
Warren repository. Diabet Med 21:358–362
60. Anaya JM, Gomez L, Castiblanco J (2006) Is there a common
genetic basis for autoimmune diseases? Clin Dev Immunol 13:
185–195
61. Lee YH, Rho YH, Choi SJ, Ji JD, Song GG, Nath SK, Harley JB
(2007) The PTPN22 C1858T functional polymorphism and
autoimmune diseases—a meta-analysis. Rheumatology (Oxford)
46:49–56
62. Silverberg MS, Cho JH, Rioux JD, McGovern DP, Wu J, Annese
V, Achkar JP, Goyette P, Scott R, Xu W et al (2009) Ulcerative
colitis-risk loci on chromosomes 1p36 and 12q15 found by
genome-wide association study. Nat Genet 41:216–220
63. Jacobson NG, Szabo SJ, Weber-Nordt RM, Zhong Z, Schreiber
RD, Darnell JE Jr, Murphy KM (1995) Interleukin 12 signaling in
T helper type 1 (Th1) cells involves tyrosine phosphorylation of
signal transducer and activator of transcription (Stat)3 and Stat4.
J Exp Med 181:1755–1762
64. Kaplan MH (2005) STAT4: a critical regulator of inflammation in
vivo. Immunol Res 31:231–242
65. Chitnis T, Najafian N, Benou C, Salama AD, Grusby MJ, Sayegh
MH, Khoury SJ (2001) Effect of targeted disruption of STAT4
and STAT6 on the induction of experimental autoimmune
encephalomyelitis. J Clin Invest 108:739–747
66. Finnegan A, Grusby MJ, Kaplan CD, O’Neill SK, Eibel H,
Koreny T, Czipri M, Mikecz K, Zhang J (2002) IL-4 and IL-12
regulate proteoglycan-induced arthritis through Stat-dependent
mechanisms. J Immunol 169:3345–3352
67. Simpson SJ, Shah S, Comiskey M, de Jong YP, Wang B, Miz-
oguchi E, Bhan AK, Terhorst C (1998) T cell-mediated pathology
in two models of experimental colitis depends predominantly on
the interleukin 12/Signal transducer and activator of transcription
(Stat)-4 pathway, but is not conditional on interferon gamma
expression by T cells. J Exp Med 187:1225–1234
68. Afanasyeva M, Wang Y, Kaya Z, Stafford EA, Dohmen KM,
Sadighi Akha AA, Rose NR (2001) Interleukin-12 receptor/
STAT4 signaling is required for the development of autoimmune
myocarditis in mice by an interferon-gamma-independent path-
way. Circulation 104:3145–3151
69. Yang Z, Chen M, Ellett JD, Fialkow LB, Carter JD, McDuffie M,
Nadler JL (2004) Autoimmune diabetes is blocked in Stat4-
deficient mice. J Autoimmun 22:191–200
70. Holz A, Bot A, Coon B, Wolfe T, Grusby MJ, von Herrath MG
(1999) Disruption of the STAT4 signaling pathway protects from
autoimmune diabetes while retaining antiviral immune compe-
tence. J Immunol 163:5374–5382
71. Hildner KM, Schirmacher P, Atreya I, Dittmayer M, Bartsch B,
Galle PR, Wirtz S, Neurath MF (2007) Targeting of the tran-
scription factor STAT4 by antisense phosphorothioate oligonu-
cleotides suppresses collagen-induced arthritis. J Immunol 178:
3427–3436
72. Hoey T, Zhang S, Schmidt N, Yu Q, Ramchandani S, Xu X,
Naeger LK, Sun YL, Kaplan MH (2003) Distinct requirements
for the naturally occurring splice forms Stat4alpha and Stat4beta
in IL-12 responses. EMBO J 22:4237–4248
73. Sigurdsson S, Nordmark G, Garnier S, Grundberg E, Kwan T,
Nilsson O, Eloranta ML, Gunnarsson I, Svenungsson E, Sturfelt
G et al (2008) A risk haplotype of STAT4 for systemic lupus
erythematosus is over-expressed, correlates with anti-dsDNA and
shows additive effects with two risk alleles of IRF5. Hum Mol
Genet 17:2868–2876
74. Gregersen PK, Olsson LM (2009) Recent advances in the
genetics of autoimmune disease. Annu Rev Immunol 27:363–391
8882 Mol Biol Rep (2012) 39:8873–8882
123