Embed Size (px)
Citation preview

Associations of Lys939Gln and Ala499Val polymorphisms ofthe XPC gene with cancer susceptibility: A meta-analysis
Jing He1,2, Ting-Yan Shi1,2, Mei-Ling Zhu1,2, Meng-Yun Wang1,2, Qiao-Xin Li1,2 and Qing-Yi Wei1,3
1 Cancer Institute, Fudan University Shanghai Cancer Center, Shanghai, China2 Department of Oncology, Shanghai Medical College, Fudan University, Shanghai, China3 Department of Epidemiology, The University of Texas, M.D. Anderson Cancer Center, Houston, TX, USA
XPC polymorphisms may alter DNA repair capacity, thus leading to genetic instability and carcinogenesis. Numerous studies
have investigated the associations of XPC Lys939Gln (rs2228001) and Ala499Val (rs2228000) polymorphisms with cancer sus-
ceptibility; however, the findings are inconclusive. We searched literature from MEDLINE and EMBASE for eligible publications
that assessed the associations between these two polymorphisms and cancer risk. We also assessed genotype-mRNA expres-
sion correlation data from HapMap for rs2228001 and rs2228000 in normal cell lines derived from 270 subjects with different
ethnicities. The final analysis included 62 published studies of 25,708 cases and 30,432 controls for the Lys939Gln and 34
studies with 14,877 cases and 17,888 controls for the Ala499Val. Overall, Lys939Gln was significantly associated with an
increased overall cancer risk (Gln/Gln vs. Lys/Lys: OR 5 1.16, 95% CI 5 1.07 2 1.25, p < 0.001; recessive model: OR 5 1.14,
95% CI 5 1.06 2 1.22, p < 0.001; dominant model: OR 5 1.06, 95% CI 5 1.01 2 1.11, p 5 0.015 and Gln vs. Lys: OR 5 1.07,
95% CI 5 1.03 2 1.10, p < 0.001) and further stratifications showed an increased risk for bladder, lung and colorectal cancer,
Asian populations and population-based studies. Likewise, Ala499Val was also significantly associated with an increased over-
all cancer risk (Val/Val vs. Ala/Ala: OR 5 1.21, 95% CI 5 1.07 2 1.36, p 5 0.003 and recessive model: OR 5 1.20, 95%
CI 5 1.08 2 1.34, p 5 0.001) and further stratification showed an increased risk for breast and bladder cancer, particularly in
Asian populations. Interestingly, significantly correlation between XPC genotypes and mRNA expression was found only for
Asian populations as well. Despite some limitations, this meta-analysis established some solid statistical evidence for an
association between XPC polymorphisms and cancer risk, which warrants further validation in single large studies.
Cancer has become a major challenge to public health and�12.7 million cancer cases and 7.6 million cancer deathswere reported according to the GLOBOCAN 2008.1 It islikely that more than 80% of cancer cases may be caused bygene-environment interactions,2 in which environmental fac-tors often cause damage to DNA, but the host repair system
did not perform their functions well in removing such DNAdamage. Therefore, DNA repair capacity plays a critical rolein maintaining the stability and integrity of human genome.
In humans, there are at least five major DNA repair path-ways, consisting of more than 130 genes. The nucleotide exci-sion repair (NER) pathway plays an important role inremoving a wide variety of DNA lesions, including bulkyadducts, cross links, oxidative DNA damage, alkylating damageand thymidine dimers.3–5 At least four steps of reaction (dam-age recognition, damaged DNA incision, gapped DNA repara-tion and DNA ligation) and several key enzymes, including thexeroderma pigmentosum complementation group C (XPC)-RAD23B, are involved in this pathway.3,6 Polymorphisms ofthe NER pathway genes may alter the DNA repair capacity andthus could play an important role in carcinogenesis.7
The XPC gene is located at chromosome 3p25, is one of theeight core genes in the NER pathway and plays an important rolein the early steps of global genome NER, especially in damage rec-ognition, open complex formation and reparation.8 Experimentalstudies have shown that XPC binds to RAD23B to form theXPC-RAD23B complex, which is involved in the DNA damagerecognition and DNA repair initiation in the NER pathway,6,8,9
where the damaged DNA recognition is the rate-limiting step.9
There are at least 102 reported coding-region SNPs(cSNPs) in the XPC gene region (http://www.ncbi.nlm.nih.-gov/projects/SNP). Among all the identified cSNPs of XPC,
Key words: XPC, DNA repair, polymorphism, susceptibility, meta-
analysis
Abbreviations: CI: confidence intervals; cSNPs: coding-region
SNPs; HWE: Hardy-Weinberg equilibrium; NER: nucleotide exci-
sion repair; OR: odds ratio; SNP: single nucleotide polymorphism;
XPC: xeroderma pigmentosum complementation group C
Additional Supporting Information may be found in the online
version of this article.
Grant sponsor: Chinese Thousand Talents Program, Fudan
University
DOI: 10.1002/ijc.28089
History: Received 14 Nov 2012; Accepted 28 Jan 2013; Online 7 Feb
2013
Correspondence to: Qing-Yi Wei, Cancer Institute, Fudan
University Shanghai Cancer Center, 270 Dong An Road, Shanghai
200032, China, Tel.: 186-21 64175590-5315, Fax: 186-21 64172585,
E-mail: [email protected] or Department of Epidemiology, The
University of Texas MD Anderson Cancer Center, 1515 Holcomb
Blvd, Houston, TX 77401, E-mail: [email protected]
MiniReview
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC
International Journal of Cancer
IJC

two common polymorphisms [Lys939Gln (rs2228001) andAla499Val (rs2228000), the former is located in the domaininteracting with TFIIH, while the later with RAD23B] werewidely investigated. Numerous studies have investigated theassociation of Lys939Gln (K939Q)10–65 and Ala499Val(A499V)10,13,14,17,21,22,24,26,29–31,35–40,42,43,45,46,51,53–55,57,58,63–69
polymorphisms of XPC with cancer risk, but the conclusionswere inconclusive. Hence, we performed this meta-analysisfrom all eligible case-control studies to provide an updated,more precise estimation of the associations.
Material and MethodsIdentification and eligibility of relevant studies
We searched literature from MEDLINE and EMBASE for allrelevant studies using the search terms: “XPC”, “variant orpolymorphism” and “cancer or carcinoma or tumor or neo-plasm” (prior to July 28, 2012). All eligible original studies,review articles and other relevant studies were searched man-ually. Only the latest or the largest study would be includedin the current meta-analysis, if studies carried out with thesame subjects or overlapping data from the same institutions.
Studies included in the analysis had to meet the following cri-teria: evaluating the association between XPC K939Q and/orA499V and cancer risk; case-control design; sufficient informa-tion provided to estimate odds ratios (ORs) and their 95% confi-dence intervals (CIs); in addition, observed genotype frequenciesin the controls departure from Hardy-Weinberg equilibrium(HWE) without further evidence from other polymorphisms ofthe XPC gene was excluded from the final analysis.
Data extraction
Two authors (Jing He and Ting-Yan Shi) independentlyextracted data from all the publications for compliance withthe inclusion criteria. Any disagreement was resolved by fullydiscussed until a consensus was reached. The following infor-mation was collected from each study: first author’s surname,year of publication, country of origin, ethnicity, cancer type,control source, total number of cases and controls, genotypemethods and numbers of cases and controls with the Lys/Lys, Lys/Gln and Gln/Gln for K939Q and Ala/Ala, Ala/Valand Val/Val for A499V.
The stratification analysis was conducted by cancer type(publications with no more than two studies would bemerged into the “others” group), ethnicity (for those studiesthat included subjects of different ethnic groups, genotypesdata were extracted separately for each of ethnic groups, cate-gorized as Asians, Caucasians, Africans or Mixed which con-tained more than one ethnic group) and control source(hospital-based and population-based).
Genotype and gene expression correlation analysis
The data of XPC genotypes were available online from theInternational HapMap Project (http://hapmap.ncbi.nlm.nih.-gov/) for the 270 subjects used in the database, whose mRNAexpression data were available online from SNPexp (http://
app3.titan.uio.no/biotools/help.php?app5snpexp) as describedpreviously.70,71 Briefly, the genotyping data were derivedfrom The HapMap phase II release 23 data set consisting of3.96 million SNP genotypes from these 270 individuals ofthree ethnic groups,72 and the mRNA expression data wereobtained from the lymphoblastic cell lines derived also fromthe same 270 individuals.73
Statistical methods
The strength of association between K939Q and A499V poly-morphisms and cancer risk was assessed by calculating ORswith the corresponding 95% CIs. The pooled ORs were alsoestimated for K939Q by homozygous (Gln/Gln vs. Lys/Lys),heterozygous (Lys/Gln vs. Lys/Lys), recessive [Gln/Gln vs.(Lys/Gln1 Lys/Lys)] and dominant models [(Lys/Gln1Gln/Gln) vs. Lys/Lys] as well as allele comparison (Gln vs. Lys)and so was A499V by homozygous (Val/Val vs. Ala/Ala),heterozygous (Ala/Val vs. Ala/Ala), recessive [Val/Val vs.(Ala/Val1Ala/Ala)] and dominant models [(Ala/Val1Val/Val) vs. Ala/Ala] as well as allele comparison (Val vs. Ala).We used Chi square-based Q-test to assess between-studyheterogeneity. When the studies were found to be homogene-ous (with p> 0.10 for the Q test), we chose the fixed-effectsmodel (the Mantel–Haenszel method).74 Otherwise, we chosethe random-effects model (the DerSimonian and Lairdmethod).75 Additionally, the heterogeneity was also quantifiedwith I2 statistics, and I2 lies from 0 to 100% with higher val-ues indicating a greater degree of heterogeneity.76 A standarderror of log (OR) was plotted against its log (OR) for eachpublication to verify the potential publication bias. Weassessed the asymmetry of the funnel plot by Egger’s linearregression test.77 We performed sensitivity analyses to assessthe effect of individual investigations on the overall cancerrisk by excluding each investigation individually and recalcu-lating the ORs and the 95% CIs. Analyses were performedwith the STATA software (version 11.0; Stata Corporation,College Station, TX) and SAS software (version 9.1; SASInstitute, Cary, NC). All the p values were two-sided and pvalues <0.05 were considered significant.
ResultsStudy characteristics
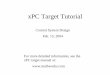
As shown in Figure 1, 165 published records were identified fromMEDLINE and EMBASE by using the search terms described inthe identification and eligibility of relevant studies part. Afterabstracts and texts were assessed, only 72 publications met thecrude inclusion criteria and were subjected for further evaluation.Of these 72 publications, six were excluded for data overlappingwith that of other publications,78–83 four without detailed data forfurther evaluation84–87 and three deviated from HWE.60,88,89 Atotal of 60 publications with a case-control design met the inclu-sion criteria and were included in the final meta-analysis(Supporting Information Table 1). Of these 60 publications, 56publications10–65 with 62 studies for the K939Q, while 33 publica-tions10,13,14,17,21,22,24,26,29–31,35–40,42,43,45,46,51,53–55,57,58,63–69 with 34
MiniReview
2 XPC Lys939Gln and Ala499Val with cancer susceptibility
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

studies for the A499V. Of the 60 publications, four publica-tions23,33,40,44 with two ethnic groups were separated as two inde-pendent studies and two publications25,61 with two cancer typeswere also separated as two independent studies.
The distribution of genotypes for the K939Q and A499Vpolymorphisms in the controls of all studies was consistentwith that expected from the HWE, except for three publica-tions,60,88,89 which assessed the K939Q polymorphism andcancer risk but not A499V and other polymorphisms of theXPC gene; so, we excluded these three in the final analysis.Another three studies17,64,66 were also deviated from HWE;thus the distribution of genotypes for K939Q17,66 or A499V64
in the controls was consistent with that expected from theHWE, which were included in the final analysis. For thosestudies25,36,37,48,49,61 that used the same control group, thecontrol numbers was only calculated once in the total numberof controls. Overall, 62 published studies of 25,708 cases and30,432 controls for the K939Q and 14,877 cases and 17,888controls for the A499V were included in the final meta-analy-sis. Of the 60 publications, sample sizes of case ranged from51 to 1,257 for K939Q and from 52 to 1,061 for A499V. ForK939Q, 11 studies focused on breast cancer, nine on lungcancers, eight on bladder cancer, six on colorectal cancer, fiveon prostate cancer, four on gastric cancer, three on esophagealcancer and melanoma and the others with no more than twostudies; for A499V, eight studies focus on breast cancer, fiveon lung cancers, four on bladder cancer and the others withno more than two studies. There were 30 studies on Cauca-sians, 21 studies on Asians, five studies on Africans andmixed ethnicity and only one on Latinos for K939Q and 14on Caucasians and Asians, five on mixed ethnicity and onlyone on Africans for A499V. Of all the studies, 33 were popu-lation-based, 29 were hospital-based for K939Q, 15 were pop-ulation-based and 19 were hospital-based for A499V. Most of
the cases were confirmed histologically. In most studies, con-trols were mainly matched for sex, age and ethnicity.
Meta-analysis results
K939Q. The overall results for the K939Q polymorphismand cancer risk are shown in Tables 1 and 2 and Figure 2.We found there was a significant association between K939Qand overall cancer risk (homozygous: OR5 1.16, 95%CI5 1.072 1.25, p< 0.001; recessive: OR5 1.14, 95%CI5 1.062 1.22, p< 0.001; dominant: OR5 1.06, 95%CI5 1.012 1.11, p5 0.015 and allele: OR5 1.07, 95%CI5 1.032 1.10, p< 0.001). In the subgroup analysis, a stat-istically significant association was found for lung cancer (re-cessive: OR5 1.18, 95% CI5 1.012 1.40, p5 0.043), bladdercancer (homozygous: OR5 1.44, 95% CI5 1.072 1.93,p5 0.017 and recessive: OR5 1.47, 95% CI5 1.102 1.98,p5 0.010) and colorectal cancer (heterozygous: OR5 1.20,95% CI5 1.022 1.41, p5 0.024 and dominant: OR5 1.17,95% CI5 1.022 1.35, p5 0.023), Asians (homozygous:OR5 1.33, 95% CI5 1.172 1.52, p< 0.001; recessive:OR5 1.27, 95% CI5 1.112 1.45, p< 0.001; dominant:OR5 1.14, 95% CI5 1.062 1.23, p5 0.001 and allele:OR5 1.13, 95% CI5 1.082 1.20, p< 0.001), population-based studies (homozygous: OR5 1.13, 95% CI5 1.042 1.22,p5 0.004; recessive: OR5 1.13, 95% CI5 1.042 1.22,p5 0.005 and allele: OR5 1.05, 95% CI5 1.012 1.09,p5 0.011) and hospital-based studies (homozygous:OR5 1.16, 95% CI5 1.022 1.33, p5 0.030; recessive:OR5 1.13, 95% CI5 1.002 1.27, p5 0.044 and allele:OR5 1.07, 95% CI5 1.012 1.14, p5 0.026).
A499V. The overall results for the A499V polymorphismand cancer risk are shown in Tables 1 and 2 and Figure 3.We found that the A499V polymorphism was also associatedwith an increased overall cancer risk (homozygous:OR5 1.21, 95% CI5 1.072 1.36, p5 0.003 and recessive:OR5 1.20, 95% CI5 1.082 1.34, p5 0.001). In the subgroupanalysis, a statistically significant association was found forbreast cancer (homozygous: OR5 1.21, 95% CI5 1.022 1.45,p5 0.032 and recessive: OR5 1.20, 95% CI5 1.012 1.42,p5 0.039) and bladder cancer (homozygous: OR5 2.04, 95%CI5 1.142 3.65, p5 0.017 and recessive: OR5 1.92, 95%CI5 1.192 3.10, p5 0.008), Asians (homozygous: OR5 1.20,95% CI5 1.002 1.44, p5 0.048 and recessive: OR5 1.18,95% CI5 1.032 1.35, p5 0.018), Caucasians (homozygous:OR5 1.34, 95% CI5 1.092 1.66, p5 0.007 and recessive:OR5 1.34, 95% CI5 1.102 1.65, p5 0.004) and hospital-based studies (homozygous: OR5 1.30, 95% CI5 1.142 1.47,p< 0.001; recessive: OR5 1.29, 95% CI5 1.152 1.44,p< 0.001 and allele: OR5 1.07, 95% CI5 1.012 1.14,p5 0.030).
The XPC mRNA expression by genotypes
The XPC mRNA expression levels by the genotypes of threeethnic groups are shown in Table 3. We found that there
Figure 1. Flow chart of included studies.
MiniReview
He et al. 3
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

existed significant difference in the expression levels for thers2228001A>C (K939Q) polymorphism for the Asian(homozygous: p5 0.003; dominant: p5 0.016; recessive:p5 0.005 and ptrend50.002). We also found significant differ-
ence in the expression levels for the rs2228000C>T (A499V)polymorphism for Asians (homozygous: p5 0.006; recessive:p5 0.002 and ptrend 5 0.010) and for all populations (homo-zygous: p5 0.0004; recessive: p5 0.0002 and ptrend 5 0.028).
Table 1. Meta-analysis of the association between XPC Lys939Gln and Ala499Val polymorphisms and cancer risk
Homozygous Heterozygous Allele
Variables No. of individuals OR (95% CI) Phet I2 (%) OR (95% CI) Phet I2 (%) OR (95% CI) Phet I2 (%)
For Lys939Gln Gln/Gln vs. Lys/Lys Lys/Gln vs. Lys/Lys Gln vs. Lys
All1 25,708/30,432 1.16 (1.07–1.25) 0.000 44.6 1.03 (0.98–1.08) 0.012 31.2 1.07 (1.03–1.10) 0.000 44.0
Cancer type
Breast 5,898/6,696 1.00 (0.88–1.14) 0.271 18.1 0.98 (0.89–1.08) 0.214 24.1 1.00 (0.94–1.06) 0.243 21.0
Lung 3,648/4,957 1.17 (0.99–1.39) 0.226 24.5 0.98 (0.88–1.10) 0.252 21.5 1.05 (0.97–1.14) 0.186 29.1
Bladder 3,244/3,356 1.44 (1.07–1.93) 0.003 67.7 0.98 (0.87–1.12) 0.263 21.0 1.12 (0.99–1.27) 0.013 60.7
Colorectal 2,751/3,607 1.05 (0.89–1.23) 0.637 0.0 1.20 (1.02–1.41) 0.112 44.0 1.07 (0.99–1.16) 0.388 4.5
Prostate 1,966/1,970 1.15 (0.72–1.82) 0.016 67.1 0.99 (0.86–1.13) 0.973 0.0 1.05 (0.90–1.21) 0.154 40.1
Gastric 846/1,816 1.16 (0.89–1.50) 0.490 0.0 1.07 (0.89–1.28) 0.783 0.0 1.06 (0.94–1.20) 0.519 0.0
Esophageal 882/1,537 1.24 (0.96–1.60) 0.998 0.0 1.06 (0.88–1.27) 0.594 0.0 1.10 (0.98–1.25) 0.927 0.0
Melanoma 1,088/1,184 1.51 (0.78–2.92) 0.002 83.6 1.12 (0.71–1.75) 0.004 81.7 1.22 (0.85–1.75) 0.000 87.7
Others 5,385/6,759 1.20 (1.01–1.43) 0.019 50.6 1.06 (0.95–1.18) 0.070 39.6 1.09 (1.00–1.19) 0.010 54.1
Ethnicity
Caucasian 12,545/15,839 1.09 (0.98–1.21) 0.005 44.4 1.01 (0.95–1.07) 0.369 6.2 1.04 (0.99–1.09) 0.005 44.9
Asian 8,309/10,177 1.33 (1.17–1.52) 0.052 36.0 1.09 (1.00–1.19) 0.017 43.7 1.13 (1.08–1.20) 0.122 27.2
African 1,409/1,303 1.06 (0.71–1.58) 0.153 40.3 0.88 (0.75–1.03) 0.605 0.0 0.98 (0.83–1.16) 0.153 40.2
Mixed 3,333/4,265 1.07 (0.93–1.23) 0.392 2.6 0.96 (0.87–1.06) 0.766 0.0 1.02 (0.95–1.09) 0.704 0.0
Latino 112/298 1.39 (0.64–3.03) – – 1.49 (0.94–2.36) – – 1.28 (0.92–1.78) – –
Source of control
HB 11,951/13,044 1.16 (1.02–1.33) 0.000 59.8 1.05 (0.98–1.13) 0.039 34.1 1.07 (1.01–1.14) 0.000 60.9
PB 13,757/18,838 1.13 (1.04–1.22) 0.185 17.8 1.01 (0.96–1.08) 0.062 29.1 1.05 (1.01–1.09) 0.282 11.4
For Ala499Val Val/Val vs. Ala/Ala Ala/Val vs. Ala/Ala Val vs. Ala
All1 14,877/17,888 1.21 (1.07–1.36) 0.002 46.8 0.98 (0.92–1.06) 0.000 51.4 1.05 (0.99–1.11) 0.000 57.4
Cancer type
Breast 3,672/4,692 1.21 (1.02–1.45) 0.628 0.0 0.99 (0.91–1.09) 0.564 0.0 1.04 (0.97–1.12) 0.446 0.0
Lung 2,605/3,329 1.12 (0.91–1.37) 0.558 0.0 1.06 (0.90–1.23) 0.140 42.2 1.05 (0.96–1.16) 0.273 22.3
Bladder 1,513/1,640 2.04 (1.14–3.65) 0.023 68.5 1.10 (0.84–1.44) 0.038 64.5 1.26 (0.95–1.67) 0.001 80.5
Others 7,087/8,839 1.14 (0.95–1.36) 0.007 51.5 0.95 (0.85–1.06) 0.000 61.8 1.02 (0.94–1.10) 0.001 60.6
Ethnicity
Caucasian 6,270/7,574 1.34 (1.09–1.66) 0.022 48.4 1.00 (0.89–1.12) 0.002 59.5 1.08 (0.99–1.18) 0.002 59.4
Asian 5,208/6,559 1.20 (1.00–1.44) 0.029 46.4 1.01 (0.89–1.15) 0.003 58.0 1.07 (0.97–1.17) 0.001 62.8
Mixed 3,347/4,292 0.97 (0.79–1.19) 0.336 12.2 0.94 (0.85–1.03) 0.525 0.0 0.96 (0.80–1.06) 0.272 22.4
African2 52/75 – – – 0.69 (0.26–1.86) – – 0.92 (0.38–2.21) – –
Source of control
HB 8,575/9,331 1.30 (1.14–1.47) 0.324 10.9 1.01 (0.91–1.11) 0.002 54.9 1.07 (1.01–1.14) 0.035 40.5
PB 6,302/9,169 1.10 (0.89–1.36) 0.001 61.2 0.96 (0.87–1.07) 0.014 50.0 1.02 (0.99–1.11) 0.000 69.0
HB, Hospital based; PB, Population based.1The control numbers was only calculated once if the same controls were used.2Smith (2008) was only calculated for heterogeneity model, allele comparing and dominant model, and the number of Val/Val genotype was zero.
MiniReview
4 XPC Lys939Gln and Ala499Val with cancer susceptibility
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

Heterogeneity and sensitivity analyses
Substantial heterogeneities were observed among all studiesfor the XPC K939Q polymorphism and overall cancer risk(homozygous: p< 0.001; heterozygous: p5 0.013; recessive:
p< 0.001; dominant: p5 0.004 and allele: p< 0.001) andA499V (homozygous: p5 0.002; heterozygous: p< 0.001; re-cessive: p5 0.026; dominant: p< 0.001 and allele: p< 0.001).Therefore, we used the random-effects model that generated
Table 2. Meta-analysis of the association between XPC Lys939Gln and Ala499Val polymorphisms and cancer risk by recessive and dominantmodels
Recessive Dominant
Variables No. of studies No. of individuals OR (95% CI) Phet I2 (%) OR (95% CI) Phet I2 (%)
For Lys939Gln Gln/Gln vs. (Lys/Gln 1 Lys/Lys) (Lys/Gln 1 Gln/Gln) vs. Lys/Lys
All1 62 25,708/30,432 1.14 (1.06–1.22) 0.000 45.4 1.06 (1.01–1.11) 0.003 35.8
Cancer type
Breast 11 5,898/6,696 1.01 (0.90–1.14) 0.289 16.2 0.99 (0.90–1.08) 0.213 24.3
Lung 9 3,648/4,957 1.18 (1.01–1.40) 0.183 29.4 1.02 (0.92–1.14) 0.239 23.0
Bladder 8 3,244/3,356 1.47 (1.10–1.98) 0.001 72.5 1.04 (0.92–1.19) 0.189 30.0
Colorectal 6 2,751/3,607 0.95 (0.82–1.10) 0.404 1.9 1.17 (1.02–1.35) 0.187 33.3
Prostate 5 1,966/1,970 1.16 (0.73–1.84) 0.009 70.6 1.02 (0.90–1.16) 0.828 0.0
Gastric 4 846/1,816 1.05 (0.74–1.50) 0.099 52.2 1.09 (0.92–1.29) 0.974 0.0
Esophageal 3 882/1,537 1.20 (0.95–1.52) 0.930 0.0 1.10 (0.93–1.31) 0.704 0.0
Melanoma 3 1,088/1,184 1.39 (0.92–2.11) 0.054 65.8 1.21 (0.73–2.01) 0.000 86.9
Others 13 5,385/6,759 1.19 (1.04–1.37) 0.114 33.5 1.09 (0.97–1.22) 0.022 49.5
Ethnicity
Caucasian 30 12,545/15,839 1.08 (0.98–1.19) 0.005 44.5 1.03 (0.97–1.09) 0.121 23.8
Asian 21 8,309/10,177 1.27 (1.11–1.45) 0.012 45.7 1.14 (1.06–1.23) 0.055 35.5
African 5 1,409/1,303 1.14 (0.75–1.72) 0.105 47.7 0.91 (0.78–1.05) 0.497 0.0
Mixed 5 3,333/4,265 1.09 (0.92–1.30) 0.149 40.9 0.99 (0.90–1.08) 0.937 0.0
Latino 1 112/298 1.14 (0.54–2.39) – – 1.47 (0.95–2.29) – –
Source of control
HB 29 11,951/13,044 1.13 (1.00–1.27) 0.000 57.6 1.08 (1.00–1.17) 0.003 47.4
PB 33 13,757/18,838 1.13 (1.04–1.22) 0.066 28.6 1.04 (0.99–1.10) 0.155 20.1
For Ala499Val Val/Val vs. (Ala/Val 1 Ala/Ala) (Ala/Val 1 Val/Val) vs. Ala/Ala
All1 34 14,877/17,888 1.20 (1.08–1.34) 0.026 35.2 1.02 (0.95–1.10) 0.000 57.1
Cancer type
Breast 8 3,672/4,692 1.20 (1.01–1.42) 0.859 0.0 1.02 (0.93–1.11) 0.430 0.0
Lung 5 2,605/3,329 1.10 (0.91–1.34) 0.718 0.0 1.06 (0.92–1.24) 0.139 42.4
Bladder 4 1,513/1,640 1.92 (1.19–3.10) 0.080 55.7 1.21 (0.88–1.66) 0.005 76.5
Others 17 7,087/8,839 1.16 (0.99–1.37) 0.022 45.3 0.98 (0.88–1.09) 0.000 63.1
Ethnicity
Caucasian 14 6,270/7,574 1.34 (1.10–1.65) 0.029 46.4 1.04 (0.93–1.17) 0.002 60.6
Asian 14 5,208/6,559 1.18 (1.03–1.35) 0.258 17.9 1.05 (0.92–1.20) 0.000 64.5
Mixed 5 3,347/4,292 1.00 (0.83–1.21) 0.452 0.0 0.94 (0.85–1.03) 0.371 6.3
African2 1 52/75 – – – 0.79 (0.31–2.05) – –
Source of control
HB 19 8,575/9,331 1.29 (1.15–1.44) 0.416 3.3 1.05 (0.96–1.15) 0.004 52.9
PB 15 6,302/9,169 1.11 (0.93–1.33) 0.016 49.2 0.98 (0.88–1.11) 0.001 63.2
HB, Hospital based; PB, Population based.1The control numbers was only calculated once if the same controls were used.2Smith (2008) was only calculated for heterogeneity model, allele comparing and dominant model, and the number of Val/Val genotype was zero.
MiniReview
He et al. 5
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

wider CIs for all genetics models. The leave-one-out sensitiv-ity analysis indicated that no single investigation had changedthe pooled ORs qualitatively (data not shown).
Publication bias
The shape of the funnel plot did not reveal any evidence ofobvious asymmetry, and we did not observe significant publi-cation bias in the current meta-analysis by the Egger’s test
for recessive model (p5 0.202 for K939Q and p5 0.092 forA499V). No publication bias was found for other models forK939Q (homozygous: p5 0.261; heterozygous: p5 0.714;dominant: p5 0.873 and allele: p5 0.421) and A499V(homozygous: p5 0.086; heterozygous: p5 0.702; dominant:p5 0.420 and allele: p5 0.336) by the Egger’s test. Theseresults indicated that publication bias might not have a sig-nificant influence on the observed associations of XPC
Figure 2. Forest plot for overall cancer risk associated with the XPC Lys939Gln polymorphism by a recessive model. For each study, the
estimates of OR and its 95% CI are plotted with a box and a horizontal line. �, pooled ORs and its 95% CIs.
MiniReview
6 XPC Lys939Gln and Ala499Val with cancer susceptibility
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

K939Q and A499V polymorphisms with overall cancer riskas assessed in the current meta-analysis.
DiscussionIn this meta-analysis including 25,708 cases and 30,432 con-trols for the K939Q and 14,877 cases and 17,888 controls forthe A499V, we found that XPC K939Q and A499V polymor-phisms were significantly associated with overall cancer riskin the homozygous and recessive models. Further, stratifica-tion analysis showed that the association was more evidentfor cancer risk of the lung, bladder and colorectum, Asiansand population-based controls for K939Q and the breast andbladder, Asians and Caucasians and hospital-based controls
for A499V. To our knowledge, there is no reported meta-analysis that has comprehensively have evaluated the associa-tion between the XPC K939Q and A499V polymorphismsand overall cancer risk as we did here.
There were three meta-analyses focused on XPCLys939Gln and Ala499Val polymorphisms and overall cancerrisk. In a meta-analysis by Qiu et al.90 including 16 studies of6,797 cases and 9,018 controls for K939Q and 11 studies of5,581 cases and 6,351 controls for A499V, an increased over-all cancer risk was observed for both Lys939Gln andAla499Val in the homozygous model. The 939Gln/Gln geno-type was associated with an increased risk for lung cancer,whereas the 499Val/Val genotype was associated with risk for
Figure 3. Forest plot for overall cancer risk associated with the XPC Ala499Val polymorphism by a recessive model. For each study, the
estimates of OR and its 95% CI are plotted with a box and a horizontal line. �, pooled ORs and its 95% CIs.
MiniReview
He et al. 7
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

bladder cancer, compared with their corresponding wild-typehomozygous genotypes. In another meta-analysis including9,091 patients and 11,553 controls for K939Q and 5,227patients and 5,959 controls for A499V, there was no signifi-cant association between the K939Q polymorphism and over-all cancer risk, except for an elevated lung cancer risk underthe recessive genetic model, nor a significant associationbetween A499V and overall cancer risk but an increased can-cer risk in Caucasians under the recessive genetic model andhomozygous comparison.91 In the third meta-analysis thatincluded 33 published case-control studies with 14,080 casesand 14,011 controls for K939Q and 7,603 cases and 7,772controls for A499V, statistically significant associations wereobserved for lung cancer under a recessive genetic model forthe K939Q polymorphism, but for A499V, a significantlyincreased overall cancer risk, particularly for bladder cancer,in both homozygous and the recessive models.92 However,some of these significant findings were not found in thismeta-analysis. For example, Qiu et al.90 found that theK939Q polymorphism was associated with an increased risk
for lung cancer in homozygous model by five studies but thisincreased risk was not present in this analysis including addi-tional four more studies. Likewise, we found that the K939Qpolymorphism was associated with risk of bladder cancer andcolorectal cancer, which was not found by the previous threemeta-analyses; although we also found this polymorphismwas associated with an increased risk for Asians, this risk wasnot found by others, likely because our analysis included amuch larger sample size, leading to an increased statisticalpower.
The XPC gene is located at 3p25, containing 16 exons and15 introns and encoding a protein of 940 amino acids that canform a XPC-RAD23B complex with RAD23B.8,93 This complexis specifically involved in global genome repair and works asthe earliest damage detector to initiate the NER pathway.8 Pre-vious studies have shown that polymorphisms in DNA repairgenes may lead to altered DNA repair capacity and may thuscontribute to cancer susceptibility.94,95 Sanyal et al.79 was thefirst to find that the K939Q polymorphism in exon 15 of theXPC gene was significantly associated with bladder cancer risk.
Table 3. XPC mRNA expression by the genotypes of SNPs, using data from the HapMap1
rs2228001 (Lys939Gln) rs2228000 (Ala499Val)
Genotypes No. Mean 6 SD P2 Ptrend3 genotypes No. Mean 6 SD P2 Ptrend
3
CEU4 AA 29 10.77 6 0.28 0.611 CC 38 10.77 6 0.35 0.764
AC 40 10.80 6 0.35 0.720 CT 37 10.80 6 0.31 0.641
CC 12 10.68 6 0.38 0.422 TT 6 10.64 6 0.29 0.403
Dominant 52 10.77 6 0.35 0.984 Dominant 43 10.78 6 0.31 0.862
Recessive 69 10.79 6 0.32 0.316 Recessive 75 10.78 6 0.33 0.294
YRI4 AA 51 10.62 6 0.26 0.809 CC 73 10.59 6 0.25 0.386
AC 23 10.51 6 0.20 0.087 CT 11 10.66 6 0.24 0.386
CC 10 10.67 6 0.25 0.548 TT 0 – –
Dominant 33 10.56 6 0.22 0.300 Dominant 11 10.66 6 0.24 0.386
Recessive 74 10.58 6 0.25 0.299 Recessive – –
Asian4 AA 35 10.32 6 0.29 0.002 CC 34 10.47 6 0.28 0.010
AC 40 10.43 6 0.25 0.093 CT 37 10.44 6 0.25 0.702
CC 10 10.64 6 0.24 0.003 TT 14 10.21 6 0.28 0.006
Dominant 50 10.48 6 0.26 0.016 Dominant 51 10.38 6 0.28 0.155
Recessive 75 10.38 6 0.27 0.005 Recessive 71 10.46 6 0.26 0.002
All4 AA 115 10.57 6 0.32 0.146 CC 145 10.61 6 0.30 0.028
AC 103 10.59 6 0.33 0.565 CT 85 10.63 6 0.32 0.610
CC 32 10.67 6 0.29 0.118 TT 20 10.34 6 0.34 0.0004
Dominant 135 10.61 6 0.32 0.293 Dominant 105 10.57 6 0.34 0.415
Recessive 218 10.58 6 0.32 0.150 Recessive 230 10.61 6 0.31 0.0002
CEU: 90 Utah residents with ancestry from northern and western Europe; Asian: 45 unrelated Han Chinese in Beijing and 45 unrelated Japanese inTokyo; YRI: 90 Yoruba in Ibadan, Nigeria.1Genotyping data and mRNA expression levels for XPC by genotypes were obtained from the HapMap phase II release 23 data from EBV-transformedlymphoblastoid cell lines from 270 individuals.2Two-side Student’s t test within the stratum.3P values for the trend test of XPC mRNA expression among three genotypes for each SNP from a general linear model.4There were missing data because genotyping data were not available.
MiniReview
8 XPC Lys939Gln and Ala499Val with cancer susceptibility
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

After that discovery, many studies were conducted to furtheraccess the association between K939Q polymorphism and riskof various cancers in different populations.
For the K939Q polymorphism, the frequency of the XPC939Gln/Gln genotype was found to be significantly higher inpatients than in controls in some studies,32,34,45,46,52,56,59,61
but not in others,27 For the A499V polymorphism, Val/Valwas more frequent in patients than in controls as reported insome studies,26,35,46,54,58,68 but not inothers.10,13,14,17,21,22,24,29–31,36–40,42,43,45,51,53,55,57,63–67,69 Overall,we found that individuals carrying the 939Gln/Gln genotypehad significantly increased cancer risk, compared with thosewho had the wild Lys/Lys genotype. In the subgroup analysis,the XPC 939Gln/Gln carriers had a significantly increasedcancer risk for the lung, bladder and colorectum, particularlyin Asians, and the 499Val/Val carriers also showed anincreased risk in homozygous and recessive models, and thiscancer risk was also found for the breast and bladder, partic-ularly in Asians as well. It is likely that the observed discrep-ancies in cancer risk by subgroups may be attributed totumor specificity, ethnic difference and sample sizes. We alsofound that Asians had a relatively higher risk than Cauca-sians, especially for carriers of the K939Q polymorphism,which was also evidenced by ethnic differences in mRNAexpression by genotypes.
Several limitations in the current up-to-date meta-analysisshould be addressed, although we included the latest studiesfor K939Q and A499V polymorphisms of XPC and cancerrisk. First, a number of studies had insufficient numbers foreach cancer type and relatively small sample size (<1,000 forcases), except for seven studies,20,23,39,44,45,50,55 which may
have attenuated the statistical power, particularly for sub-group analysis. Second, because of the lack of original data,our results were based on unadjusted estimates of ORs with-out adjustment for individual’s age and sex, environment fac-tors (such as smoking, pack-years and drinking), especiallywhen we found significant associations between XPC poly-morphisms and cancer risk of the lung, bladder and colorec-tum. Third, due to missing information about disease status,incomplete histological details may also have influenced theinterpretation. Fourthly, there existed some heterogeneitythat may be ascribed to cancer type, ethnic difference andvariation in sample sizes, study designs and genotypingmethods; hence, we used the random-effects model that gen-erated wider CIs for all genetics models. Finally, we justchose the literatures from MEDLINE and EMBASE, whichmay have missed publications for other languages.
In conclusion, we performed this updated meta-analysiscombining the latest published studies, and we drew amore precise and robust estimation for associations ofK939Q and A499V polymorphisms of XPC with cancerrisk. Specifically, the 939Gln/Gln carriers may have anincreased cancer risk, especially for the bladder cancer,lung cancer, colorectal cancer and Asians. The 499Val/Valcarriers may also have an increased cancer risk underhomozygous and recessive models, especially for breast can-cer, bladder cancer and Asians. Therefore, well-designedprospective studies including more SNPs of XPC and othergenes of the NER pathway with larger sample sizes, wellmatched cancer-free controls, more information aboutenvironmental factors, such as smoking and drinking, areneeded to validate our findings.
References
1. Jemal A, Bray F, Center MM, et al. Global cancerstatistics. CA Cancer J Clin 2011;61:69–90.
2. Lichtenstein P, Holm NV, Verkasalo PK, et al.Environmental and heritable factors in thecausation of cancer–analyses of cohorts of twinsfrom Sweden, Denmark, and Finland. N Engl JMed 2000;343:78–85.
3. Friedberg EC. How nucleotide excision repairprotects against cancer. Nat Rev Cancer2001;1:22–33.
4. Wood RD, Mitchell M, Sgouros J, et al.Human DNA repair genes. Science2001;291:1284–9.
5. De Silva IU, McHugh PJ, Clingen PH, et al.Defining the roles of nucleotide excision repairand recombination in the repair of DNAinterstrand cross-links in mammalian cells. MolCell Biol 2000;20:7980–90.
6. Wood RD. DNA damage recognition duringnucleotide excision repair in mammalian cells.Biochimie 1999;81:39–44.
7. Goode EL, Ulrich CM, Potter JD. Polymorphismsin DNA repair genes and associations withcancer risk. Cancer Epidemiol Biomarkers Prev2002;11:1513–30.
8. Sugasawa K, Ng JM, Masutani C, et al.Xeroderma pigmentosum group C proteincomplex is the initiator of global genome
nucleotide excision repair. Mol Cell 1998;2:223–32.
9. Thoma BS, Vasquez KM. Critical DNA damagerecognition functions of XPC-hHR23B and XPA-RPA in nucleotide excision repair. Mol Carcinog2003;38:1–13.
10. Weiss JM, Weiss NS, Ulrich CM, et al.Interindividual variation in nucleotide excisionrepair genes and risk of endometrial cancer.Cancer Epidemiol Biomarkers Prev 2005;14:2524–30.
11. Blankenburg S, Konig IR, Moessner R, et al.Assessment of 3 xeroderma pigmentosum groupC gene polymorphisms and risk of cutaneousmelanoma: a case-control study. Carcinogenesis2005;26:1085–90.
12. Sak SC, Barrett JH, Paul AB, et al. The polyAT,intronic IVS11-6 and Lys939Gln XPCpolymorphisms are not associated withtransitional cell carcinoma of the bladder. Br JCancer 2005;92:2262–5.
13. Hu Z, Wang Y, Wang X, et al. DNA repair geneXPC genotypes/haplotypes and risk of lungcancer in a Chinese population. Int J Cancer2005;115:478–83.
14. Lee GY, Jang JS, Lee SY, et al. XPCpolymorphisms and lung cancer risk. Int J Cancer2005;115:807–13.
15. Vogel U, Overvad K, Wallin H, et al.Combinations of polymorphisms in XPD, XPCand XPA in relation to risk of lung cancer.Cancer Lett 2005;222:67–74.
16. Festa F, Kumar R, Sanyal S, et al. Basal cellcarcinoma and variants in genes coding forimmune response, DNA repair, folate and ironmetabolism. Mutat Res 2005;574:105–11.
17. Wu X, Gu J, Grossman HB, et al. Bladder cancerpredisposition: a multigenic approach to DNA-repair and cell-cycle-control genes. Am J HumGenet 2006;78:464–79.
18. Kietthubthew S, Sriplung H, Au WW, et al.Polymorphism in DNA repair genes and oralsquamous cell carcinoma in Thailand. Int J HygEnviron Health 2006;209:21–9.
19. Hirata H, Hinoda Y, Matsuyama H, et al.Polymorphisms of DNA repair genes areassociated with renal cell carcinoma. BiochemBiophys Res Commun 2006;342:1058–62.
20. Garcia-Closas M, Malats N, Real FX, et al.Genetic variation in the nucleotide excision repairpathway and bladder cancer risk. CancerEpidemiol Biomarkers Prev 2006;15:536–42.
21. Huang WY, Berndt SI, Kang D, et al. Nucleotideexcision repair gene polymorphisms and risk ofadvanced colorectal adenoma: XPCpolymorphisms modify smoking-related risk.
MiniReview
He et al. 9
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

Cancer Epidemiol Biomarkers Prev 2006;15:306–11.
22. Li C, Hu Z, Liu Z, et al. Polymorphisms in theDNA repair genes XPC, XPD, and XPG and riskof cutaneous melanoma: a case-control analysis.Cancer Epidemiol Biomarkers Prev 2006;15:2526–32.
23. Mechanic LE, Millikan RC, Player J, et al.Polymorphisms in nucleotide excision repairgenes, smoking and breast cancer in AfricanAmericans and whites: a population-based case-control study. Carcinogenesis 2006;27:1377–85.
24. Shen J, Desai M, Agrawal M, et al.Polymorphisms in nucleotide excision repairgenes and DNA repair capacity phenotype insisters discordant for breast cancer. CancerEpidemiol Biomarkers Prev 2006;15:1614–9.
25. Ye W, Kumar R, Bacova G, et al. The XPD751Gln allele is associated with an increased riskfor esophageal adenocarcinoma: a population-based case-control study in Sweden.Carcinogenesis 2006;27:1835–41.
26. An J, Liu Z, Hu Z, et al. Potentially functionalsingle nucleotide polymorphisms in the corenucleotide excision repair genes and risk ofsquamous cell carcinoma of the head and neck.Cancer Epidemiol Biomarkers Prev 2007;16:1633–8.
27. Hirata H, Hinoda Y, Tanaka Y, et al.Polymorphisms of DNA repair genes are riskfactors for prostate cancer. Eur J Cancer2007;43:231–7.
28. Hansen RD, Sorensen M, Tjonneland A, et al.XPA A23G, XPC Lys939Gln, XPD Lys751Glnand XPD Asp312Asn polymorphisms,interactions with smoking, alcohol and dietaryfactors, and risk of colorectal cancer. Mutat Res2007;619:68–80.
29. Bai Y, Xu L, Yang X, et al. Sequence variations inDNA repair gene XPC is associated with lungcancer risk in a Chinese population: a case-control study. BMC Cancer 2007;7:81.
30. Jorgensen TJ, Visvanathan K, Ruczinski I, et al.Breast cancer risk is not associated withpolymorphic forms of xeroderma pigmentosumgenes in a cohort of women from WashingtonCounty, Maryland. Breast Cancer Res Treat2007;101:65–71.
31. Zhou RM, Wang N, Guo W. [Correlation ofpolymorphisms in xeroderma pigmentosum groupC to the risk of ovarian carcinoma]. Zhonghua LiuXing Bing Xue Za Zhi 2008;29:91–2.
32. Fontana L, Bosviel R, Delort L, et al. DNA repairgene ERCC2, XPC, XRCC1, XRCC3polymorphisms and associations with bladdercancer risk in a French cohort. Anticancer Res2008;28:1853–6.
33. Chang JS, Wrensch MR, Hansen HM, et al.Nucleotide excision repair genes and risk of lungcancer among San Francisco Bay Area Latinosand African Americans. Int J Cancer2008;123:2095–104.
34. Raaschou-Nielsen O, Sorensen M, Overvad K,et al. Polymorphisms in nucleotide excisionrepair genes, smoking and intake of fruit andvegetables in relation to lung cancer. Lung Cancer2008;59:171–9.
35. Yang ZH, Liang WB, Jia J, et al. The xerodermapigmentosum group C gene polymorphisms andgenetic susceptibility of nasopharyngealcarcinoma. Acta Oncol 2008;47:379–84.
36. Guo W, Zhou RM, Wan LL, et al.Polymorphisms of the DNA repair gene
xeroderma pigmentosum groups A and C andrisk of esophageal squamous cell carcinoma in apopulation of high incidence region of NorthChina. J Cancer Res Clin Oncol 2008;134:263–70.
37. Dong Z, Guo W, Zhou R, et al. Polymorphismsof the DNA repair gene XPA and XPC and itscorrelation with gastric cardiac adenocarcinomain a high incidence population in North China. JClin Gastroenterol 2008;42:910–5.
38. McWilliams RR, Bamlet WR, Cunningham JM,et al. Polymorphisms in DNA repair genes,smoking, and pancreatic adenocarcinoma risk.Cancer Res 2008;68:4928–35.
39. Shen J, Gammon MD, Terry MB, et al.Xeroderma pigmentosum complementation groupC genotypes/diplotypes play no independent orinteraction role with polycyclic aromatichydrocarbons-DNA adducts for breast cancerrisk. Eur J Cancer 2008;44:710–7.
40. Smith TR, Levine EA, Freimanis RI, et al.Polygenic model of DNA repair geneticpolymorphisms in human breast cancer risk.Carcinogenesis 2008;29:2132–8.
41. Abbasi R, Ramroth H, Becher H, et al. Laryngealcancer risk associated with smoking and alcoholconsumption is modified by geneticpolymorphisms in ERCC5, ERCC6 and RAD23Bbut not by polymorphisms in five othernucleotide excision repair genes. Int J Cancer2009;125:1431–9.
42. Pan J, Lin J, Izzo JG, et al. Genetic susceptibilityto esophageal cancer: the role of the nucleotideexcision repair pathway. Carcinogenesis2009;30:785–92.
43. Li LM, Zeng XY, Ji L, et al. [Association of XPCand XPG polymorphisms with the risk ofhepatocellular carcinoma]. Zhonghua Gan ZangBing Za Zhi 2010;18:271–5.
44. Agalliu I, Kwon EM, Salinas CA, et al. Geneticvariation in DNA repair genes and prostatecancer risk: results from a population-basedstudy. Cancer Causes Control 2010;21:289–300.
45. Long XD, Ma Y, Zhou YF, et al. Polymorphismin xeroderma pigmentosum complementationgroup C codon 939 and aflatoxin B1-relatedhepatocellular carcinoma in the Guangxipopulation. Hepatology 2010;52:1301–9.
46. de Verdier PJ, Sanyal S, Bermejo JL, et al.Genotypes, haplotypes and diplotypes of threeXPC polymorphisms in urinary-bladder cancerpatients. Mutat Res 2010;694:39–44.
47. Gangwar R, Mandhani A, Mittal RD. XPC genevariants: a risk factor for recurrence of urothelialbladder carcinoma in patients on BCGimmunotherapy. J Cancer Res Clin Oncol2010;136:779–86.
48. Engin AB, Karahalil B, Engin A, et al. Oxidativestress, Helicobacter pylori, and OGG1 Ser326Cys,XPC Lys939Gln, and XPD Lys751Glnpolymorphisms in a Turkish population withcolorectal carcinoma. Genet Test Mol Biomarkers2010;14:559–64.
49. Engin AB, Karahalil B, Engin A, et al. DNArepair enzyme polymorphisms and oxidativestress in a Turkish population with gastriccarcinoma. Mol Biol Rep 2011;38:5379–86.
50. Liu D, Wu HZ, Zhang YN, et al. DNA repair genesXPC, XPG polymorphisms: Relation to the risk ofcolorectal carcinoma and therapeutic outcome withoxaliplatin-based adjuvant chemotherapy.MolCarcinog 2011;51Suppl 1:E83–93.
51. Doherty JA, Weiss NS, Fish S, et al.Polymorphisms in nucleotide excision repair
genes and endometrial cancer risk.Cancer Epidemiol Biomarkers Prev2011;20:1873–82.
52. Goncalves FT, Francisco G, de Souza SP, et al.European ancestry and polymorphisms in DNArepair genes modify the risk of melanoma: acase-control study in a high UV index region inBrazil. J Dermatol Sci 2011;64:59–66.
53. Wu Y, Jin M, Liu B, et al. The association ofXPC polymorphisms and tea drinking withcolorectal cancer risk in a Chinese population.Mol Carcinog 2011;50:189–98.
54. Jiao X, Ren J, Chen H, et al. Ala499Val (C>T)and Lys939Gln (A>C) polymorphisms of theXPC gene: their correlation with the risk ofprimary gallbladder adenocarcinoma-a case-control study in China. Carcinogenesis2011;32:496–501.
55. Roberts MR, Shields PG, Ambrosone CB, et al.Single-nucleotide polymorphisms in DNA repairgenes and association with breast cancer risk inthe web study. Carcinogenesis 2011;32:1223–30.
56. Rouissi K, Bahria IB, Bougatef K, et al. The effectof tobacco, XPC, ERCC2 and ERCC5 geneticvariants in bladder cancer development. BMCCancer 2011;11:101.
57. Wu YY, Ma XY, Yao KY, et al. [Association ofXPC gene polymorphisms with breast cancerrisk]. Zhejiang Da Xue Xue Bao Yi Xue Ban2011;40:252–8.
58. Yang X, Liu D, Wu H, et al. Association of XPCpolymorphisms with susceptibility and clinicaloutcome to chemotherapy in breast cancerpatients. Cancer Sci, in press; doi: 10.1111/j.1349–7006.2012.02312.x.
59. Liu Y, Chen Z, Wei Q, et al. Poly (AT)polymorphism in the XPC gene and smokingenhance the risk of prostate cancer in a low-riskChinese population. Cancer Genet 2012;205:205–11.
60. Forsti A, Angelini S, Festa F, et al. Singlenucleotide polymorphisms in breast cancer. OncolRep 2004;11:917–22.
61. Mittal RD, Mandal RK. Genetic variation innucleotide excision repair pathway genesinfluence prostate and bladder cancersusceptibility in North Indian population. IndianJ Hum Genet 2012;18:47–55.
62. Gil J, Ramsey D, Stembalska A, et al. The C/Apolymorphism in intron 11 of the XPC geneplays a crucial role in the modulation of anindividual’s susceptibility to sporadic colorectalcancer. Mol Biol Rep 2012;39:527–34.
63. Sakoda LC, Loomis MM, Doherty JA, et al. Germline variation in nucleotide excision repair genesand lung cancer risk in smokers. Int J MolEpidemiol Genet 2012;3:1–17.
64. Shen M, Berndt SI, Rothman N, et al.Polymorphisms in the DNA nucleotide excisionrepair genes and lung cancer risk in Xuan Wei,China. Int J Cancer 2005;116:768–73.
65. Long XD, Ma Y, Huang YZ, et al. Geneticpolymorphisms in DNA repair genes XPC, XPD,and XRCC4, and susceptibility to Helicobacterpylori infection-related gastric antrumadenocarcinoma in Guangxi population, China.Mol Carcinog 2010;49:611–8.
66. Blankenburg S, Konig IR, Moessner R, et al. Noassociation between three xerodermapigmentosum group C and one group G genepolymorphisms and risk of cutaneous melanoma.Eur J Hum Genet 2005;13:253–5.
67. Broberg K, Bjork J, Paulsson K, et al.Constitutional short telomeres are strong genetic
MiniReview
10 XPC Lys939Gln and Ala499Val with cancer susceptibility
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC

susceptibility markers for bladder cancer.Carcinogenesis 2005;26:1263–71.
68. Sak SC, Barrett JH, Paul AB, et al.Comprehensive analysis of 22 XPCpolymorphisms and bladder cancer risk. CancerEpidemiol Biomarkers Prev 2006;15:2537–41.
69. Monroy CM, Cortes AC, Lopez M, et al.Hodgkin lymphoma risk: role of geneticpolymorphisms and gene-gene interactions inDNA repair pathways. Mol Carcinog2011;50:825–34.
70. Holm K, Melum E, Franke A, et al. SNPexp-aweb tool for calculating and visualizingcorrelation between HapMap genotypes and geneexpression levels. BMC Bioinformatics2010;11:600.
71. He J, Qiu LX, Wang MY, et al. Polymorphisms inthe XPG gene and risk of gastric cancer in Chinesepopulations. Hum Genet 2012;131:1235–44.
72. International HapMap Consortium. TheInternational HapMap Project. Nature2003;426:789–96.
73. Stranger BE, Forrest MS, Dunning M, et al.Relative impact of nucleotide and copy numbervariation on gene expression phenotypes. Science2007;315:848–53.
74. Mantel N, Haenszel W. Statistical aspects of theanalysis of data from retrospective studies ofdisease. J Natl Cancer Inst 1959;22:719–48.
75. DerSimonian R, Laird N. Meta-analysis in clinicaltrials. Control Clin Trials 1986;7:177–88.
76. Higgins JP, Thompson SG. Quantifyingheterogeneity in a meta-analysis. Stat Med2002;21:1539–58.
77. Egger M, Davey Smith G, Schneider M, et al.Bias in meta-analysis detected by a simple,graphical test. BMJ 1997;315:629–34.
78. Rouissi K, Ouerhani S, Hamrita B, et al. Smokingand polymorphisms in xenobiotic metabolismand DNA repair genes are additive risk factors
affecting bladder cancer in Northern Tunisia.Pathol Oncol Res 2011;17:879–86.
79. Sanyal S, Festa F, Sakano S, et al. Polymorphismsin DNA repair and metabolic genes in bladdercancer. Carcinogenesis 2004;25:729–34.
80. Zhou RM, Li Y, Wang N, et al. [Correlation ofXPC Ala499Val and Lys939Gln polymorphismsto risks of esophageal squamous cell carcinomaand gastric cardiac adenocarcinoma]. Ai Zheng2006;25:1113–9.
81. Zhu Y, Lai M, Yang H, et al. Genotypes,haplotypes and diplotypes of XPC and risk ofbladder cancer. Carcinogenesis 2007;28:698–703.
82. Mandal RK, Gangwar R, Kapoor R, et al.Polymorphisms in base-excision & nucleotide-excision repair genes & prostate cancer risk innorth Indian population. Indian J Med Res2012;135:64–71.
83. Hu ZB, Wang YG, Ma HX, et al. [Association oftwo exonic genetic polymorphisms in the DNArepair gene XPC with risk of lung cancer inChinese population]. Zhonghua Yi Xue Yi ChuanXue Za Zhi 2005;22:415–8.
84. Wen H, Ding Q, Fang ZJ, et al. Population studyof genetic polymorphisms and superficial bladdercancer risk in Han-Chinese smokers in Shanghai.Int Urol Nephrol 2009;41:855–64.
85. Cai XL, Gao YH, Yu ZW, et al. [A 1:1 matchedcase-control study on the interaction betweenHBV, HCV infection and DNA repair gene XPCAla499Val, Lys939Gln for primary hepatocellularcarcinoma]. Zhonghua Liu Xing Bing Xue Za Zhi2009;30:942–5.
86. Hung RJ, Baragatti M, Thomas D, et al. Inheritedpredisposition of lung cancer: a hierarchicalmodeling approach to DNA repair and cell cyclecontrol pathways. Cancer Epidemiol BiomarkersPrev 2007;16:2736–44.
87. Berndt SI, Platz EA, Fallin MD, et al. Geneticvariation in the nucleotide excision repair
pathway and colorectal cancer risk.Cancer Epidemiol Biomarkers Prev 2006;15:2263–9.
88. Zhang L, Zhang Z, Yan W. Single nucleotidepolymorphisms for DNA repair genes inbreast cancer patients. Clin Chim Acta2005;359:150–5.
89. Millikan RC, Hummer A, Begg C, et al.Polymorphisms in nucleotide excision repairgenes and risk of multiple primary melanoma:the Genes Environment and Melanoma Study.Carcinogenesis 2006;27:610–8.
90. Qiu L, Wang Z, Shi X. Associations between XPCpolymorphisms and risk of cancers: a meta-analysis. Eur J Cancer 2008;44:2241–53.
91. Zhang D, Chen C, Fu X, et al. A meta-analysis of DNA repair gene XPCpolymorphisms and cancer risk. J Hum Genet2008;53:18–33.
92. Francisco G, Menezes PR, Eluf-Neto J, et al. XPCpolymorphisms play a role in tissue-specificcarcinogenesis: a meta-analysis. Eur J Hum Genet2008;16:724–34.
93. Khan SG, Muniz-Medina V, Shahlavi T, et al.The human XPC DNA repair gene:arrangement, splice site information contentand influence of a single nucleotidepolymorphism in a splice acceptor site onalternative splicing and function. NucleicAcids Res 2002;30:3624–31.
94. Shen MR, Jones IM, Mohrenweiser H.Nonconservative amino acid substitution variantsexist at polymorphic frequency in DNA repairgenes in healthy humans. Cancer Res1998;58:604–8.
95. Shen H, Sturgis EM, Khan SG, et al. An intronicpoly (AT) polymorphism of the DNA repair geneXPC and risk of squamous cell carcinoma of thehead and neck: a case-control study. Cancer Res2001;61:3321–5.
MiniReview
He et al. 11
Int. J. Cancer: 00, 000–000 (2013) VC 2013 UICC