-
DefinitionIt is a syndrome characterized by AIRFLOW OBSTRUCTION
that varies markedly, both spontaneously and with
treatment.Narrowing of the airways is usually reversible, but in
some patients with chronic asthma there may be an element of
irreversible airflow obstruction
-
pathologically by bronchial inflammation with prominent
eosinophil infiltration physiologically by bronchial
hype-reactivity, and clinically by variable cough, chest tightness
and wheeze
-
EpidemiologyIt affects approximately 10-15% of children and
5-10% of adultsPrevalence is greater in industrialized
countriesPrevalence is increasing world-wide
-
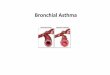
Pathology of asthmaInfiltration with inflammatory cells (esp.
eosinophils and T-lymphocytes)Patchy epithelial sheddingAirway
smooth muscle thickeningSubepithelial fibrosisMucus gland and
goblet cell hyperplasiawidespread mucus plugging in fatal
asthma
-
Mechanisms of asthmaInflammation underlies airway
hyperresponsivenessThe inflammation is of characteristic pattern
and it involves interaction between many inflammatory cellsThis
results in the release of multiple inflammatory
mediatorsInflammatory mediators result in bronchoconstriction,
mucus secrition, exudation of plasma and airway
hyperresponsiveness
-
Neural mechanism may amplify the asthmatic
inflammationStructural changes may occur with subepithelial
fibrosis, airway smooth muscle hyperplasia and new vessel
formation. These changes may underlie irreversible airflow
obstruction
- Types of asthmaAllergic (extrinsic) asthmaNon-allergic
(intrinsic) asthmaOccupational asthmaAspirin induced asthma Asthma
of infancy(
-
Allergic asthmaOnset usually in childhoodMay persist into
adulthoodRemission in adolescence is commonAssociated with allergic
rhinitis and atopic dermatitis in variable combination
-
Intrinsic asthmaOnset in adultsNo external inciter is
recognizedOften associated with perennial non-allergic
rhinitisAccounts for approx. 10% of adult asthma
-
Occupational asthmaDue to exposure to chemical sensitizers at
workUnrelated to atopic statusSome occur in atopics due to allergen
exposure at work
-
Aspirin induced asthmaSpecial type of intrinsic asthmaIt is a
metabolic, pharmacological disorderacute asthma attacks on first
and subsequent exposure to aspirin and NSAID
-
Asthma of infancyRecurrent bouts of significant airflow
limitation in small airways from viral infectionsOften remits as
child gets oldernot associated with atopySometimes called wheezy
bronchitis
-
Clinical features
Symptoms TriggersPhysical signs
-
SymptomsWheeze-- intermittent, worse on expiration,
chracteristically relieved by an inhaled 2- agonistCough-- usually
unproductiveChest tightnessSOB Prodromal symptoms may precede an
attack
-
TriggersAllergens (house dust mite, pollen, animal dander,
moulds)Irritants (tobacco smoke, air pollutants, strong odours,
fumes)Physical factors (exercise, cold air, hyperventillation,
laughter, crying)Upper respiratory tract viral
infectionsEmotionsOccupational agents (chemical sensitizers,
allergens)Drugs (beta blockers,NSAID)Food additives
(metabisulphite,tartrazine)Change in weatherEndocrine factors
(menstrual cycle, pregnancy,thyroid disease)
-
Physical signsExpiratory ronchi- widespreadHyperinflation of
chestUse of accessory musclesAssociated signs: nasal polyps,
flexure eczema
-
DD in adultsMechanical obstruction of airwaysCOPDHeart
failurePEVasculitidesCarcinoid syndrome with hepatic
secondaries
-
Principles of treatmentEducate patients to develop a partnership
in asthma managementAssess and monitor severity with objective
measurement of lung functionAvoid or control asthma
triggersEstablish medication plans for chronic managementEstablish
plans for managing exacerbationsProvide regular follow-up care
-
Clinical evaluation of severityNumber of daytime attacks lasting
more than 24 hrs and needing extra medicationThe presence of
completely symptom-free intervals lasting more than 4 weeks without
medicationThe frequency of waking at night due to asthma
symptomsThe amount of absence from work or school because of
asthmaThe ability of the patients to keep up with peers in normal
physical activityThe number and type of medications required on
regular basisThe frequency of using extra relief medications on an
as needed basisThe frequency of hospital admissionThe of
life-threatening episodes
-
MEDICATIONS
SteroidsBeta-agonistsCromolynMethylxanthinesLeukotriene
modifiersAnticholinergics
-
CORTICOSTEROIDSProven most effective benefit for chronic
controlInhaled form preferredInhibit inflammatory cell migration
and activationDecrease airway responsivenessReverse beta-receptor
down regulationImprove spirometry
-
CORTICOSTEROIDSSide effects include thrush, cough,
dysphoniaDexamethasone not includedRisks for children and growth
suppression not an issueUsed for any classificationSystemic
steroids reserved for severe
-
CROMYLYN/NEDOCROMILAnti-inflammatory effect from blockage of
chloride channels for mast cellsHelp inhibit allergy response and
exercise responseProven to improve improve peak flow and reduce
beta-agonist useDosage usually 4 times per daySafety well knownLess
predictable response than corticosteroids
-
LONG ACTING BETA AGONISTSNot to be used for acute
exacerbationsDirectly stimulates beta receptors to relax bronchial
smooth muscleEspecially useful for nocturnal symptomsStudies show
that tolerance does not developCan cause tachycardia, hypokalemia,
prolonged QT interval
-
METHYLXANTHINES? Mechanism but does provide mild
bronchodilationNot the preferred chronic therapy Numerous adverse
effects, risk of toxicity, drug interactions, and lab
monitoring
-
LEUKOTRIENE MODIFIERS
Use in children not widely approvedFew side effects-reported
liver effectsDrug interactions with theophylline, warfarin,
terfenadineOral formulations once dailyWork to decrease
leukotrienes and decrease inflammationStudies mostly on mild
asthma-improves sx and increase peak flow
-
QUICK RELIEF DRUGSShort acting beta-agonist work within 30
minutesAll asthma patients should have this
availableAnticholinergics can give relaxation of bronchial smooth
muscle-no role in long term management
-
STEPWISE APPROACH
Severe PersistentHigh dose corticosteroidLong acting
bronchodil.Oral steroidsModerate PersistentAnti-inflammatoryLong
acting bronchodil.Mild PersistentAnti-inflammatory orLeukotriene
modMid IntermittentNo daily medications
-
Asthma is a chronic inflammatory disorder of the airway which
manifest by symptoms such as episodic breathlessness, wheezing,
chest tightness and cough particularly at night and the early
morning.
Inflammation makes the airways sensitive to stimuli such as
allergens, chemical irritation, tobacco smoke cold air or
exercise.
Bronchial asthma is one of the most common chronic disease, is
of all asthmatic patients suffer from chro nic symptoms recuiri
continuous administration of anti asthmatic drugs.
-
Chronic asthma is the asthma for which we should give continuous
and cautions treatments in drily clinical practice.
Chronic asthma is characterized by : Clinically : recurrent
episodes of dyspnea and wheezing caused by reversible airway
narrowing. 2. Physiologically : increased airway responsiveness. 3.
Pathologically : by inflammation of the airway Eo infiltration and
damage to the airway epithelioma.4. Immunologically : increased Ig
eproduction.
-
Ask patients : Dose the patients have ;Reccurent attacks of
wheezing Cough or wheeze at night?Cough or wheeze after exercise
Cough, wheeze of chest tightness of exposure to allergens or
pollutants
Classive severity of asthma : Step I: INTERMITTEN Step II: MILD
PERSISTENT Step III : MODERATE PERSISTENT Step IV : SEVERE
PERSISTENT
-
1. QUICK RELIEF SABA ANTI CHOLENERCKSSHORTACTING THEOPHYLLIN
ADRENALIN INJECTION 2. LONGTERM PREVENTIVE Corticosteroid Soding
cromoglycate Nedocromil LABA Sustained released theophylline
Ketotifen
-
Monitoring the course of asthma :
Review of symptoms Measurement of lung function as much as
possible Long-term peak flow monitoring for patients with
persistent asthma is important for providing objective measurement
of the course of the disease.
-
THE BEST way to stop asthma attacks is presentation. Identify
and avoid triggers eg : Domestic dust mites Animal allergens
Tobacco smoke Cackroach Rold Smoke Cold Physical activity
-
*