ASTHMA PATHOPHYSIOLOGY ASTHMA OVERVIEW Presented by: Michelle
Harkins, MD University of New Mexico
Slide 2
This session will cover Review asthma statistics Define asthma
Outline key pathophysiologic features Review signs and symptoms of
asthma Reference to NAEPP EPR-3: asthma severity classification
system-including impairment and risk domains Diagnosing asthma
Slide 3
Slide 4
Prevalence vs Incidence Prevalence - the proportion or
percentage of a population that has disease at a specific point or
period of time Incidence the number of new cases of disease that
develop in a population of individuals at risk during a specific
point or period of time
Slide 5
1980-1996 prevalence of asthma in US increased Since 1999,
mortality and hospitalization due to asthma have decreased
Slide 6
Trends in Asthma Morbidity and Mortality. American Lung
Association, Epidemiology and Statistics Unit, Research and Program
Services Division. September, 2012.
Slide 7
Slide 8
Slide 9
New Mexico BRFSS Results for 2010: Current Prevalence: Percent
of New Mexico Children who Currently Have Asthma by Various
Demographic Characteristics Race/Ethnicity: White, Non-Hispanic
8.1% Hispanic 7.4% Native American 13.1% SOURCE: Centers for
Disease Control and Prevention (CDC). Behavioral Risk Factor
Surveillance System Survey Data. Atlanta, Georgia: U.S. Department
of Health and Human Services, Centers for Disease Control and
Prevention, 2009
Slide 10
Trends in Asthma Morbidity and Mortality. American Lung
Association, Epidemiology and Statistics Unit, Research and Program
Services Division. September, 2012.
Slide 11
Slide 12
Asthma age-adjusted hospitalization rates per 10,000 standard
population by county, New Mexico, 2007-2011 average
Slide 13
Asthma hospitalization rates per 10,000 standard population
among youth (0-14 years) by county, New Mexico, 2007-2011
average
Slide 14
Trends in Asthma Morbidity and Mortality. American Lung
Association, Epidemiology and Statistics Unit, Research and Program
Services Division. September, 2012.
Slide 15
Slide 16
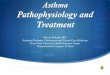
Asthma Age-Adjusted Death Rates Based on the 1940 and 2000
Standard populations, 1979-2005
197919801981198219831984198519861987198819891990199119921993199419951996199719981999200020012002200320042005
19400.91.0 1.21.11.2 1.31.4 1.51.4 1.5 1.4 1.21.11.0 0.9
20001.31.41.5 1.71.61.8 1.92.02.1 2.22.02.12.2 2.12.01.71.61.5
1.41.3
Slide 17
Asthma Patient Demographics US Population = 305.8 Million (US
Census, 2/18/09); Asthma Patients = 7.7% Prevalence (NHIS 2007) Age
Asthma Physician Market Dynamics Study 3/9910/99 NHIS 2007 Age 18+
y 16.2 million 71% Age 2 canisters per month of inhaled short-
acting beta2 agonist Risk Factors for Death from Asthma
Slide 50
Chronic use of systemic corticosteroids Poor perception of
airflow obstruction or its severity Co-morbid conditions (other
diseases) Serious psychiatric disease or psychosocial problems Low
socioeconomic status and urban residence Illicit drug use
Sensitivity to alternaria-mold Lack of written asthma action plan
Risk Factors for Death from Asthma
Slide 51
Recurrent episodes of coughing or wheeze Asthma may be present
without a wheeze - cough may be the sole symptom Shortness of
breath or difficulty breathing Chest Tightness Wheezing does not
always mean asthma Absence of symptoms and physical findings at the
time of the examination does not exclude asthma Diagnosing
Asthma
Slide 52
Asthma Diagnosis by history of wheeze, shortness of breath,
cough, chest tightness Spirometry can help define the severity of
the disease, however may be normal if asthma is under control Lack
of bronchodilator response does not rule out asthma Following Peak
Flows may be useful
Slide 53
Spirometry should be performed: at initial assessment after
treatment is initiated and symptoms and PEFs have stabilized at
least every 1-2 years to assess maintenance of airway function if
well controlled More often if poor asthma control Measures of
Assessment & Monitoring
Slide 54
Peak Flows may be performed: In all moderate and severe
persistent asthmatics establish a personal best useful in
exacerbations and maintenance/ changes of therapy, Can be helpful
with poor perceivers Measures of Assessment & Monitoring
Slide 55
< 2 Years Old: When Is It Asthma? Family history of asthma
Atopy, eczema Perinatal exposure to aeroallergens and irritants
(e.g., passive smoke) Wheezing triggered by factors other than
upper respiratory infections Risk Factors for Developing
Asthma
Slide 56
< 2 Years Old: When Is It Asthma? TWO GROUPS OF INFANTS
WHEEZE ASTHMANOT ASTHMA
Slide 57
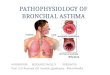
Asthma Predictive Index MAJOR CRITERIA Atopic dermatitis
Parental Asthma MINOR CRITERIA Wheezing apart from colds Allergic
rhinitis Blood eosinophilia 1 of 2 major criteria or 2 minor
criteria > of children with a positive index had some active
asthma symptoms between 6 and 13 years of age In an infant or young
child with > 3 episodes of wheezing in the past year
Slide 58
Asthma: Children vs. Adults Children Present with symptoms of
cough noisy or rapid breathing, usually before 5 years of age
Adults Present with symptoms of cough, shortness of breath, chest
pain, wheezing, often intermittent or nocturnal
Slide 59
Asthma Misdiagnosis Commonly Misdiagnosed in Children as:
CHRONIC/WHEEZY BRONCHITIS RECURRENT CROUP RECURRENT UPPER
RESPIRATORY INFECTION RECURRENT PNEUMONIA Commonly Misdiagnosed in
Adults as: RECURRENT BRONCHITIS
Slide 60
Asthma Severity Assessments < 6 year old often cannot
perform reliable Pulmonary Function Tests (PFTs) or peak flow
measurements Older children with even severe symptoms often have
fairly normal PFTs between episodes Severity assessment often
focuses on symptoms more than lung function measurements CHILDREN
PFTs play more important role in assessment PFTs performed at
diagnosis and routinely at least every 1-2 years ADULTS
Slide 61
Long-Term Management of Asthma in Children: Initiation of
Control Therapy Symptoms > 2 x week Severe exacerbations < 6
weeks apart 2 or more burst of prednisone in 6 months for ages 0-4
2 or more burst of prednisone in 1 year for ages 5-11 Positive
Asthma Predictive Index