Embed Size (px)
Citation preview
1
AstraZeneca Young Health Programme (India)
Annual Report
November 2011 – October 2012 Project name:
AstraZeneca Young Health Programme – India
Project location:
New Delhi in five resettlement colonies: Madanpur Khadar, Badarpur,
Mangolpuri, Holambi Kalan and Dwarka.
Project duration:
Three years (November 2010-October 2013).
Beneficiaries:
The Young Health Programme (YHP) expects to reach an estimated 31,000 households in five settlement areas of Delhi. The main targets of the project are adolescents and youth and their families and communities. By the end of the three years, the project aims to directly target 30,000 young people (aged 10-24) and influence at least 150,000 people in the wider population indirectly including policy makers, educators, and health professionals in the communities in which these young people live.
Goal and Objectives:
Goal: To make a meaningful difference to health and well-being of marginalised and disadvantaged adolescents by helping them to make informed choices to protect their health, now and in the future. The following are broad objectives for the programme:
Improve health seeking behaviours through raising awareness and knowledge about access to available healthcare systems
Enable adolescents to make better choices about their health and lifestyle through raising awareness and knowledge about healthcare
Establish community based actions to tackle key infections Address the immediate needs of the community related to healthcare,
hygiene and sanitation
Key highlights of YHP to date REACH
By the end of the second year, the YHP India has directly reached 65,250 young people (double the initial target) and also influenced 60,988 wider community members, including health professionals, educators and policy makers.
In Year two, the YHP trained an additional 818 adolescents as Peer Educators. In total there are now 1,403 Peer Educators who are actively delivering health messages to other young people in their schools and communities.
IMPACT
Peer Educators and YHP staff have referred 398 adolescents in need
2
of medical advice or services to health facilities for issues such as TB, dengue, malaria and sexual reproductive health (SRH) issues.
ADVOCACY
Establishment of special clinics with opening times for adolescents in all five project communities, resulting in a steady increase of adolescents accessing health services at Government health facilities, instead of remaining unsupported, or resorting to unqualified doctors known as quacks.
Influenced local government in the resettlement colonies to make small steps towards improving waste disposal and access to clean water.
SUSTAINABILITY
150 young people received training on street theatre which has enabled them to deliver YHP awareness messages through community drama, and also provided them with skills to support and develop their livelihood opportunities.
Training of 295 Government health professionals including Anganwadi workers (family health), ASHA workers (community health) and ANMs (Auxiliary Nurse Midwives) on key YHP thematic areas.
YOUTH VOICE
An editorial committee of children has been formed to support the development of YHP resources such as a programme newsletter, Information Education Communication (IEC) materials such as posters and wall writing (semi-permanent wall painting).
Outcomes:
Summary of main achievements:
The YHP has now completed its second year and has demonstrated impressive
achievements particularly in terms of reach, by already exceeding some of the
original project targets. To date, the programme has successfully reached
65,250 young people directly and 60,988 members of the wider community
indirectly. Note: The numbers of beneficiaries recorded through the above
outreach events is in fact much higher, but in agreement with project partners,
assumptions have been built in to allow for potential overlap of people that may
attend more than one activity. The figures provided are conservative estimates
of those reached.
During the second year, the programme has focussed on a diverse array of
outreach activities including workshops, awareness sessions, community
meetings, street plays, magic shows, video shows, competitions and thematic
camps and fairs. This has been achieved through two key approaches – the
establishment of Nine Health Information Centres (HICs) which serve as a
forum for youth to come together and focus on health-related issues; and the
training and support of 1,403 Peer Educators (677 male, 726 female) who take
a lead in delivering awareness activities among their peers and communities.
3
Additionally Plan and the local partners have continued to strengthen
relationships with government health providers and have successfully
advocated for the creation of special clinics for adolescents.
Objective 1: Capacity building of adolescents by providing relevant information, knowledge on lifestyles and better choices that will help enhance responsive health seeking behaviour As previously reported, the YHP in India has developed a tailored package consisting of a training curriculum and supporting IEC materials on the five YHP themes in India: Life style Education; Health and Wellbeing; Menstrual Hygiene; Sexual and Reproductive Health; and Water and Sanitation. This package is used in the sensitisation of adolescent boys and girls on key health issues through a variety of means including one to one meetings, group meetings, Health Information Centres (HICs) and street plays. The information is supported and reinforced by the cohort of Peer Educators to positively impact upon health-seeking behaviours. HIC staff and existing Peer Educators supported the selection of adolescents to be trained as Peer Educators, identifying young people who were highly motivated, had demonstrated an interest in health issues and were committed to attending the HIC. Selected young people participated in a four day intensive training course covering the five thematic areas, familiarising them with the content and facilitator guide, and building their capacity to communicate and share information effectively with their peers. The training also provided a space to discuss and dispel common myths and misconceptions (for example that masturbation can cause impotence or that wet dreams are a sign of psychological problems). During Year two, an additional 818 Peer Educators were trained, contributing to the total to date of 1,403 Peer Educators (677 males, 726 females) actively sharing with their peers relevant information and knowledge on lifestyles and informed choices to support positive health-seeking behaviours. Each Peer Educator received a training manual which supports them to facilitate meetings and deliver messaging. Once trained and equipped, the Peer Educators started organising individual and group meetings with other young people to raise awareness on taboo issues such as SRH and menstrual hygiene.
Here is an example of a song that the Peer Educators sing to raise awareness to community members: “Listen Listen Listen........ What we want to say…......Education is our
Right…………….Health is our Right......................Playing is our Right”
Seema, Peer Educator, Bardapur
4
Once the Peer Educators had become active for a significant period, the project provides refresher training for them to recap on the content areas and provide a space for reflection and discussion about what was working well or not in the peer to peer outreach. To date, 392 Peer Educators have received refresher training and further training is planned for Year three. In addition to the Peer Educator training, 150 young people from the YHP
communities received specific training to acquire street theatre skills. The
purpose of the training was to build the capacity of the young people to deliver
YHP outreach activities to engage the audiences through drama, public talks
and rallies. The training also provided valuable skills for the young people that
may be of use to them in future livelihood opportunities. Following the training,
the adolescents prepared scripts, songs and poems on the themes of health
and hygiene. They are now using these in their work as ambassadors of the
programme, ensuring healthy lifestyles for themselves and promoting healthier
lifestyles to their peers and communities.
Young people have also been engaged in developing IEC materials for use by
the YHP. Usually this work is outsourced to technical agencies, but it was
recognised that by using the creativity and knowledge of the young people,
there was potential to develop materials that would be far better received and
have greater impact in communities. A poster competition produced a number of
quality images on key themes such as tackling alcoholism, or encouraging
people to visit the clinic when ill.
These posters will be printed and used as IEC materials for the YHP, displayed
in locations such as schools and HICs. The YHP also developed a magazine,
made and edited by young people incorporating health focused poems, songs,
articles, cartoons etc.
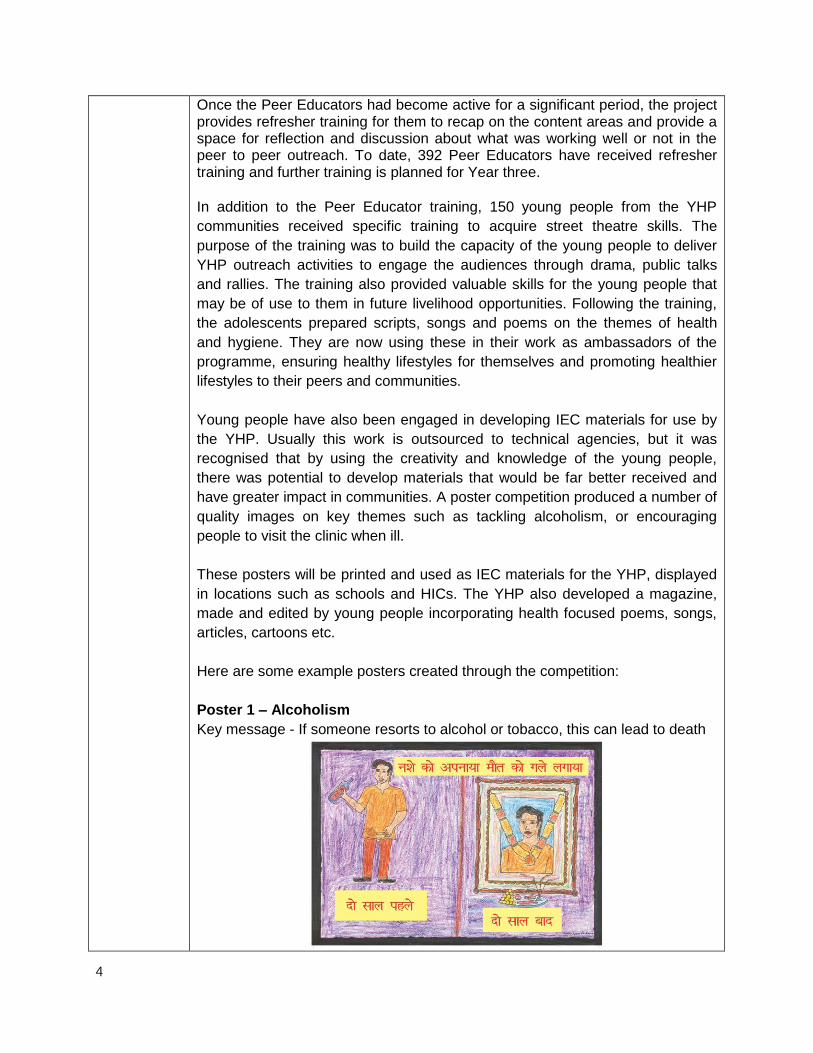
Here are some example posters created through the competition:
Poster 1 – Alcoholism
Key message - If someone resorts to alcohol or tobacco, this can lead to death
5
The left side shows “Two years earlier”, the right side “After ten years” (which is
the picture of their funeral).
Poster 2 – Peer pressure
Key message – friends who motivate you to drink, smoke or take drugs – you
should say “Bye Bye” to.
Other messages on the poster include disagreeing with the statement
‘everything is excused at a party’.
In addition to the activities of the Peer Educators, the HICs have continued to
play a critical role in imparting relevant information to young people in the
targeted communities. During the second year of the project, in response to the
overwhelming demand and popularity, the YHP has established additional HICs
in four of the project areas so there are now nine operating in total (a tenth was
planned for year two but lack of staff capacity to run it have restricted it from
becoming active). Open six days per week from 10.00 am to 5.00 pm, the HICs
provide a resource library and a safe space for local youth (aged 10-24). The
centres open in two shifts; morning time allotted to boys and the afternoon time
for girls. Initially the centres aimed to receive about 40 youths each day but that
number quickly grew – and each centre now regularly receives attendance
between 70-90 youths each day. Now the HICs are well known in the area the
YHP has received multiple requests from young people and their parents to
open the HICs on Sunday and holidays also! (although this is not in the current
plan). The HICs aim to provide an informative centre so that young people can
better understand the risks that they are confronted with, including substance
abuse, unsafe sex, teenage pregnancy, parenting, school dropout, crime, and
violence.
Each week at the HIC, the young people and staff mutually decide the theme of
the topics to be covered which are then advertised on the HIC noticeboards.
Learning sessions are led by either HIC staff or the Peer Educators in the form
of talks, debates or workshops. The topics covered will vary but include issues
such as changes during adolescence, dengue, malaria and tuberculosis (TB).
6
The HICs are therefore building the capacity of young people at two levels,
firstly so the trained Peer Educators develop themselves, and secondly
providing health, education and career related information to new members who
are accessing HIC services. Additionally, installed question boxes at the HIC are
also enabling young people to ask reproductive & sexual health related queries,
which they may be more comfortable asking anonymously. The work of the
HICs is recognised and respected by parents and communities as supporting
young people to channel their energies constructively rather than wasting time
and money on non-productive or anti-social activities.
Objective 2: To establish community based actions on key infections
The project has established 59 community stakeholder groups with the aim of
bringing people together to debate on issues relating to the health and safety of
young people, and to develop and follow action plans on key issues identified.
The groups consist of men, women, community leaders and young people who
live and work in the community. These groups were familiarized with the project,
and the role they could play in contributing towards the YHP. Over the last year,
the groups have identified public spaces for wall writing (semi-permanent
painted posters), and message dissemination, which will have a positive impact
on the community and young people particularly. The community wall writing
depicted focused messaging on the five thematic areas being promoted by the
Peer Educators.
Here are some example slogans used in wall writing
The project team has also carried out 237 community meetings, which reached
up to 4,591 community members across the five communities. The objective of
the meetings is to sensitize the community on thematic issues, which are a pre
cursor for improving young people’s health. During these meetings, the
emphasis was on the role that community members could play in improving
young people’s health. The issues focussed on during meetings are tailored to
Young Health Programme says…..No AIDS!
By adopting small-small good habits- using toilet for defecation and ensuring cleanliness in the physical environment we can protect ourselves and our community from many diseases.
7
the needs and knowledge gaps of each community. For example, in one
community the meeting might focus on looking at the various natural changes
that happen to young people during adolescence. In a different community they
were very concerned about safety of girls and the YHP supported them to link
up with an organisation who could provide them with self-defence training. The
community members were also given quality IEC materials for their further
reading and absorption. The YHP has received very positive feedback from
these meetings about the project objectives and also the approach of
strategically disseminating thematic information in an accessible manner.
The YHP has continued to deliver a series of mass awareness activities focused
on issues such as health prevention and promotion, encouraging treatment-
seeking behaviours, low-cost nutrition interventions etc. The activities have used
a diverse array of mediums including health-themed street plays, puppet shows,
video shows, rallies, public talks and health melas (fairs).
Changing the mind-set In the project area, many topics relating to sexual and reproductive health (SRH) are not openly discussed and this can lead to deeply entrenched misconceptions or ignorance on basic health topics that are particularly relevant for young people experiencing the changes associated with adolescence. The YHP is trying to tackle this mind-set through promoting accurate information on SRH and encouraging young people to talk to each other and their families on tabooed topics. One example that the YHP came across was that of a girl who had started her period at the young age of nine years old. For her mother who had started her periods much later at 16 years of age, this seemed highly unnatural. Afraid her daughter would be considered abnormal or be at risk of rape, the mother pressed a hot iron on her daughter’s chest to try and halt the development of her breasts. The girl was seriously injured by this action. After hearing this story, YHP staff visited the girl’s home to check on her welfare, and also to talk to her mother. They talked to the mother and daughter about the normal biological changes during adolescence, explaining that the process was different for each person and there was nothing unnatural about the girl starting her periods at such a young age. Following the meeting the mother said that she better understood some of the issues now and has committed not to harm her daughter again in the future.
8
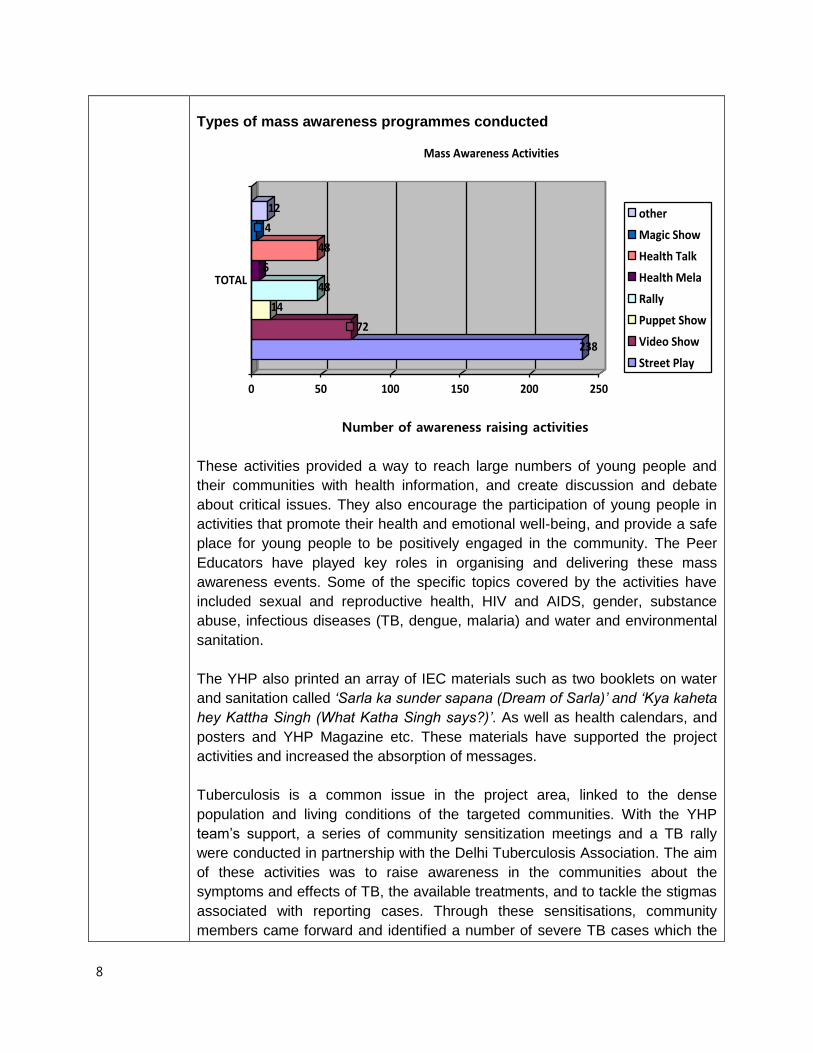
Types of mass awareness programmes conducted
238
72
14
48
6
48
4
12
0 50 100 150 200 250
TOTAL
Mass Awareness Activities
other
Magic Show
Health Talk
Health Mela
Rally
Puppet Show
Video Show
Street Play
Number of awareness raising activities
These activities provided a way to reach large numbers of young people and
their communities with health information, and create discussion and debate
about critical issues. They also encourage the participation of young people in
activities that promote their health and emotional well-being, and provide a safe
place for young people to be positively engaged in the community. The Peer
Educators have played key roles in organising and delivering these mass
awareness events. Some of the specific topics covered by the activities have
included sexual and reproductive health, HIV and AIDS, gender, substance
abuse, infectious diseases (TB, dengue, malaria) and water and environmental
sanitation.
The YHP also printed an array of IEC materials such as two booklets on water
and sanitation called ‘Sarla ka sunder sapana (Dream of Sarla)’ and ‘Kya kaheta
hey Kattha Singh (What Katha Singh says?)’. As well as health calendars, and
posters and YHP Magazine etc. These materials have supported the project
activities and increased the absorption of messages.
Tuberculosis is a common issue in the project area, linked to the dense
population and living conditions of the targeted communities. With the YHP
team’s support, a series of community sensitization meetings and a TB rally
were conducted in partnership with the Delhi Tuberculosis Association. The aim
of these activities was to raise awareness in the communities about the
symptoms and effects of TB, the available treatments, and to tackle the stigmas
associated with reporting cases. Through these sensitisations, community
members came forward and identified a number of severe TB cases which the
9
Peer Educators and YHP staff were able to then refer appropriately to the
nearest Directly Observed Treatment Short course centre (DOTS) which is a
specialist centre for diagnosis and treatment of TB.
Objective 3: Raising awareness and knowledge about access to available health care systems The YHP has initiated various advocacy activities with key decision makers for access and uptake of health services for the young people. The YHP has built strong links with government health bodies and in particular the departments relating to malaria and Women and Child Development (WCD). The YHP has conducted monthly convergence and coordination meetings with the WCD department to foster mutual support and coordination at all levels. A particular emphasis has been put on advocating for front line workers to mainstream and integrate the health of young people into their day to day business. The YHP has also supported the government department The Integrated Child Development Scheme (ICDS) through facilitating a number of ‘Sabla’ trainings which focusses on SRH for adolescent girls. Partners have approached the civic body, Municipal Corporation of Delhi (MCD) and briefed them on the project specifically around the focus on infectious diseases and SRH. Many of the issues that have been raised are related to water and sanitation including: lack of potable water, waste disposal and sewage maintenance. The latter two fuels infections by acting as a breeding ground for diseases such as malaria, dengue and water-borne illnesses. The YHP has highlighted how these issues could be mitigated through the cooperative efforts of communities and government and has continued to support the building of links between the two to facilitate this. Through the YHP, stakeholder sensitization and coordination meetings were organized for the five communities. The meetings brought together key stakeholders from communities and service providers including medical officers from the Health Department, malaria inspectors, TB officers from the DOTS department, Municipal Councillors, school principals and teachers, the Deputy Director from ICDS, Anganwadi supervisors (family health workers), presidents of Resident Welfare Association (RWAs) and partner staff. This forum provided a place for these stakeholders to discuss critical health-related issues affecting the community and identify potential actions to address them. These sensitization meetings also served the wider purposes of building links between government and communities, and to promote youth participation in health initiatives. For example one idea discussed was looking at how the pool of Peer Educators could be used to support government initiatives to raise community awareness of malaria and dengue during the next rainy season. Another was demonstrated in the participation of Anganwadi workers in supporting the organisation and delivery of the YHP sanitation rally. There was also a commitment from health professionals to support YHP activities through conducting information sessions on adolescent health issues in schools and HICs.
10
One of the biggest advocacy achievements of the YHP during the second year of the programme has been in influencing service providers to establish specific clinics for adolescents at the government run health units. The first such clinic was established by the Health Department in Mangolpuri, dedicating a special clinic time between 12-2 pm on Saturdays. This proved very successful and similar clinics were then established in each of the five project areas. The clinics have helped young people, especially adolescent girls, to feel much more comfortable and confident about access services in this space, which are dedicated solely to their needs. Additionally, our HIC and Peer Educators have been playing a critical role in
linking communities to services by making prompt referrals of young people to
health facilities where a need is identified. These referrals are reported on a
monthly basis, and to date have included issues such as SRH, TB, dengue, and
malaria. During the last year, Peer Educators and YHP project staff referred 398
cases to the health facility for appropriate medical help, and feedback from
doctors has confirmed this has resulted in an increase in the number of young
people accessing services and demonstrating health-seeking behaviour. The
YHP has additionally taken several groups of young girls to health centres for
medical check-ups and this is reflective of the level of trust that parents and
communities have in the programme.
Objective 4: Addressing the immediate needs of the community in issues related to health care, hygiene, and sanitation
In collaboration with the municipal corporation, the YHP carried out community
sanitation training for community members, leaders and Peer Educators, and
other stakeholders. This training focussed on topics such as degradable and
non-degradable waste, and solid waste management. Through a Participatory
Rural Appraisal (PRA) the participants developed their understanding on the
correlation between community sanitation and health. During the training
participants developed action plans on improving water and environmental
sanitation conditions in their own communities, for example reducing the use of
polythene bags, restricting what was thrown in drains to reduce clogging, and
campaigning against open defecation.
The training was followed by community meetings and a cleanliness drive was
planned where young people could set an example to others by collecting the
community garbage and cleaning up the environment. One block was identified
to be a “model block” after young people carried out the cleanliness drive and
distributed pamphlets and stickers to promote better sanitation in each area,
with the aim of encouraging other areas to follow suit. As part of the health in
Mangolpuri community, representatives from the MCD and Health departments
participated in talks to discuss the water and sanitation issues with the
community.
11
In Holambi Kalan the YHP has established six Slum, Health and Sanitation
Teams (SHASTs) consisting of 42 members of the community including
adolescents and community leaders. The SHASTs were formed to focus
specifically on issues of water, sanitation and hygiene. To date they have been
engaged in identifying the key problems in their communities and required
actions.
The programme also distributed sanitation kits and materials to Peer Educators
which included items such as soap, disinfectant, toothpaste, hand sanitiser and
sanitary pads for girls, to sensitize them about the importance of personal and
environmental hygiene and to encourage their peers as well. Kits were also
distributed to the Anganwadi centres with an aim to engage government
workers as similar role models of positive change.
A significant achievement of the YHP during year two was to engage some
schools in adolescent health issues. The programme organised sensitisation
workshops with principals and teachers on sanitation, health and hygiene,
career counselling and guidance for students in Holambi Kalan and Badarpur
areas. Subsequently, the schools authorities from seven schools allowed the
YHP to organise sessions in schools with students on the topics of water,
sanitation and hygiene, lifestyle choices and menstrual hygiene.
The YHP has supported all seven schools to establish or reactivate school
water and sanitation committees. Through these, selected students take a lead
in championing water and sanitation interventions in their schools, monitoring
the use of facilities, reporting if they become non-functional, and leading
Water and sanitation messages integrated into street plays on health and hygiene
Play one
- Clean your hands (six step process) before taking food or after using the toilet
- Always use a glass with a handle when taking water from a shared water jug, rather than dipping in a glass with your hand
- Avoid open defecation - Always clean vegetables and other foods with clean water - A toilet should be 20m away from a water source
Play two
- Keep sanitation and garbage areas clean and tidy - Always wear slippers (flipflops) when going to the toilet - In cases of diarrhoea, treat with oral rehydration salts - Clean water before drinking, through boiling, filtering or using
chlorine
12
awareness activities in the school. The YHP has also improved water and
sanitation facilities in four of the schools due to the needs identified. This
included the installation of two fresh water tanks, the repair of one water tank,
installation of one water pipe line, repair work to two toilet blocks and repair of a
water purifier. An additional public toilet block was repaired in Holambi Kalan
community where the need for access to services is particularly acute.
Utilising the strong links with the local government, during year two the YHP has
been able to influence the provision of services that have a direct impact on the
needs of communities in the target areas through:
o Influencing the MCD to reinstate a garbage collection service to Holambi
Kalan which had been experiencing a mass build up of rubbish due to
the lack of an active refuse collection.
o Highlighting issues of lack of access to clean water in Holambi Kalan to
the DJB (institution charged with supplying water to the State of Delhi)
which subsequently led to the establishment of a water tank van service
to the area to dispense fresh water. The DJB has also provided chlorine
tablets which the Peer Educators have distributed along with information
to the community on how they can be used to improve the water safety
before consumption.
o The Sanitation Inspector is now a frequent visitor to the project areas,
regularly identifying ways in which he can link with the Peer Educators to
disseminate information to the communities. One example of this was a
joint Dengue Spray initiative between Peer Educators and the Malaria
Inspector and Sanitation Inspectors who worked together to develop and
deliver a strategy to raise community awareness about dengue
protection before the onset of the rainy season.
Other additional benefits (unanticipated results)
Some of the additional or unanticipated results over year two included:
o Ten adolescent theatre groups were formed and trained by the YHP. Subsequently they were linked with a professional agency who supported them to develop scripts and start performing street plays in their communities. The plays focussed on issues relevant to the communities such as water and environmental sanitation, sexual and reproductive health and infectious diseases. In addition to supporting the YHP delivery, this also created a livelihood opportunity for the adolescents interested in street theatre as a profession.
o Dental camps were also organized in three YHP communities (Dwarka, Badarpur and Madanpur Khadar) to sensitize young people about oral hygiene.
o The young members of Mangolpuri area have formed an editorial committee comprising of six members (three boys and three girls) and have published a magazine which is exclusively based on the current scenario of youth, their thoughts, beliefs and dreams. One HIC also produced a comic book on alcohol abuse which was the creative idea of
13
the adolescents and was designed and produced by them. o After successful networking with the government organisation Centre for
Cultural Resources and Training (CCRT), a number of adolescents benefited from training on wall writing, role plays and other skills used to support the outreach activities of the YHP.
o In June 2012, a one day workshop on menstrual hygiene brought together YHP staff to revisit technical content of the topic and share learning from the YHP and a different Plan project on school menstrual hygiene that had just concluded in Uttar Pradesh.
o In addition to the YHP thematic topics, the HICs also carried out sessions on a diverse range of broader topics requested by young people such as: gender and violence, Independence movements, disaster management, nutrition, adolescence and their role models, and the Indian constitution and rights. The HICs have also started offering career counselling due to popular demand of the young people.
o Five girls who have had dropped out of school for different reasons were formally enrolled by YHP staff in the National Institute of Open School to resume their education and have continued to attend ever since.
o YHP project has experimented with income-generation activities such as handmade greeting cards, bags, photo frames, and artificial flowers with older girls with the aim of boosting their confidence, skills and independence.
Furthermore, the project also organised Rangoli (folk art) and a poem writing competition on YHP project issues on the eve of Diwali, and distributed awards to the winners and participants. The winning entries will be published in the YHP newsletter to showcase their work to a wider audience.
Progress against log frame indicators:
See Annex 1
Project activities:
See Annex 2
Project challenges:
During year two of the programme, there were a number of challenges experienced. These are outlined below:
o Due to the dense nature of the resettlement communities, there is very limited available space for public facilities such as the HICs. The HICs have established themselves in very small spaces (approximately 10x10ft on average) which puts significant limitations on the numbers of young people that can attend at the same time. The project has sought to respond to this issue by dividing the HIC activities into separate sessions for boys and girls, and by opening additional HICs (see below).
o The HICs have not only been extremely popular with adolescents but with families and community members too. YHP staff are often overwhelmed by the number of people who want to attend. Over the past year, four additional HICs have been established. Originally it was intended that five were created (one in each community) but now there are two in each community (with the exception of Badarpur). It is expected that a third will be established in each community over the third
14
year. However because of the level of activity each HIC engages in, additional staff will be needed to manage the additional HICs if the expansion is to go ahead. The YHP also plans to continue to rely on Peer Educators to support the delivery of activities, which not only is a resource for the HIC staff but also builds the skills and experience of the young people.
o The key factor that defines the success of the project will be effective supervision and monitoring. The YHP has been looking into opportunities to build on existing processes by developing a Management Information System (MIS) specifically for the YHP. This system would enable the YHP to more effectively track data to capture critical changes and impact as a result of the programme.
o Many young people growing up in the area do not have opportunities to live in a safe and healthy environment, learn essential life-skills, find meaningful work and participate in their culture and community. Without a strong connection to community, education, recreation and employment pathways, young people are both socially and economically marginalized. Although these are among the most vulnerable young people in the target areas, they are also among the most difficult to access as there are many that do not proactively engage with schools or the HICS. To reach out to these hard-to-reach adolescents, the YHP has increased its outreach through one to one interactions, family counselling and seeking the support of local community leaders to identify such youth. Through activities such as street plays, the YHP is also better able to engage with these young people.
o Lack of confidentiality and privacy have been identified as critical barriers in the poor uptake of health services by young people. In order to address this serious concern the YHP has successfully advocated for the creation of five special health clinics for adolescents by the government, and is continuing to encourage the further uptake of this model. The YHP is also encouraging doctors to participate in health talks at the HICs to build trust between them and the adolescents, especially girls.
o Poor community infrastructure creates further problems for carrying out training and awareness activities as there are limited spaces where training can take place due to poor electricity and water supplies. This means that training and events must be organised in far away locations at additional cost and inconvenience.
o Since the project deals with sensitive issues like SRH, some young people often feel inhibited to ask questions in public. Therefore, as a strategy, a question box has been installed at all HICs where girls and boys can anonymously drop in their queries, which are then addressed by the project staff during the group sessions on a daily basis or through specific Q&A sessions.
o Another challenge is to reach out to older adolescents (19-24 years) who do not access the HICs so frequently. Males in this age group are engaged in jobs so have limited time to access the HIC, whilst girls are at a marriageable age and are restricted to their homes due to traditional beliefs. In order to address this for girls, the YHP team is continuously involving parents and sensitizing them about adolescent health needs. Parents are also encouraged to visit HICs on Saturdays or days when
15
they are off work so that they can see through their own eyes how HIC/YHP is changing their sons/daughters lives. The YHP team is also providing career counselling to this age bracket and making the HIC library more useful for them by adding in competitions/entrance related books, and employment news for them.
Sustainability
The YHP aims to achieve long-lasting impact on the health of adolescents in the project areas, that is driven and owned by the beneficiaries for whom it is delivering. For this purpose, a range of strategies are built into the design and delivery of the programme. Peer-led behaviour change Peer Educators are a key vehicle of the programme, acting as community- based social messengers and agents of positive and healthy behaviour change. Adolescents are trained, motivated and supported to take the positive messages forward to other young people and their communities, with the intention that they will be able to continue in this way even beyond the conclusion of the project. Strategic skills development Through the Peer Education and on-going support in delivering outreach activities, adolescents have built their capacity not only in awareness of key health information and behaviours, but also in wider basic competencies that will assist them in their future paths, such as skills in presentations, debating, written communications and influencing. In addition, YHP has provided technical training in specific areas such as street theatre and income-generation. Providing such skills development is crucial for the retention and engagement of young people, particularly the older adolescents.
Community stakeholder groups Working with and through Community Stakeholder group’s aims to engage men, women, elders and families in the YHP activities and strengthen communities to take responsibilities and ownership of key health issues in their environments. Linking with government institutions The programme aims to connect adolescents and communities with the service providers and policy makers through various activities including bringing young people into direct contact with health professionals. The YHP engages with government through a number of relevant departments and levels through networking, joint planning and delivery of activities.
Health Information Centres (HICs) Each of the HICs has now established a committee composed of parents, young people and local leaders. The committees meet on a monthly basis and play a lead role in planning, monitoring and taking decisions about the HIC activities and practices.
AstraZeneca involvement:
Regular calls (once a month) with AZ Global and AZ India to discuss updates and upcoming events.
Visit of Plan personnel to the AZ office in Delhi in September 2012 to review the progress of the YHP.
Visit by the AZ India Director of Sales to see first-hand the impact of the
16
YHP. This includes visiting a Health Information Centre (HIC) to see a health-focused street play being performed and meet with adolescent beneficiaries.
Two ‘town hall’ meetings during the year in which Plan met with AZ staff to update them on key achievements, success and learning’s from the project. This included the participation of Peer Educators who presented directly to 80 AZ employees in Delhi on their experiences under the YHP.
AZ employees invited to judge a poster competition of entries from young people who had designed posters based on health and lifestyles messages.
Project management, monitoring and evaluation:
The project is delivered through Project Coordinators (PCs) and Project Managers (PMs) at the partners’ level. The PCs are responsible for the day to day project activities and their work plan and deliverables are monitored by the PM. At the same time Plan India has a dedicated Project Coordinator for overall project monitoring and implementation through regular support and field visits. Regular meetings and communication are maintained between Plan and the partners to ensure a close working relationship. Plan India also facilitates regular project review and sharing meetings to bring all partners together, and exchange field experiences, challenges, learning and best practice. Project activities are monitored on a weekly and monthly basis. A database has been developed to record the details of HIC visitors, registered members, Peer Educators and the parents and this tracks comprehensive information on all the adolescents utilizing the HICs. The project team plans and reviews micro and macro level activities on a monthly basis. Peer Educators are the crucial component of the project acting as community- based social messengers and the agents for change. They are involved in every stage of the programme including design, delivery, and monitoring and reporting to ensure project ownership and effectiveness. They use a template report to collect information, monitor progress of activities and assess performance with support from the YHP staff.
Budget:
See Annex 3 Financial
Quotes and photos:
Quotes “I learnt how we can prevent disease by keeping ourselves clean, use safe drinking water and practice hand washing and other forms of personal hygiene.” Kamlesh, girl aged 14 “My parent did not enroll me in the school because I had to take care of my father...it was hard because my father was sick and he needed me at that
17
moment, but thanks to the YHP team that they helped me to catch up with my studies as I could get the books from HIC to read them at my home.” Rajesh, boy aged 16 “We, the adolescent girls, are working for the holistic development of youths in the age group (10-24 years) by generating awareness about adolescent health, water and sanitation, reproductive health and encouraging parents and grandparents to fulfil their roles as care givers. We employ street plays as a methodology to sensitize the community. We are happy for what we are doing for ourselves, our peers and the community.” Arati, girl aged 14 “This programme has enhanced my knowledge on health and well-being, life skill education, reproductive health, menstrual hygiene, water and sanitation. Now I realize how incomplete my knowledge was, I am imparting awareness and sensitising my peers in our area. Today I am confident and feel free to discuss all the matters with our elders without any inhibitions.” Laxmi, girl aged 16 “We, the children in the Health Information Centre are participating in Peer Educator training sessions and street play workshops. Now I confidently participate in family and social events in my area” Pooja, girl aged 18 “Today our Peer Educators are confident enough to take formal sessions with young people, and they are also referring other young peoples to avail health care services.” YHP Staff - Badarpur “This gives me an opportunity to follow my dream, I wish HIC/YHP could open in other areas as well so that other communities youth get an opportunity of changing their personalities, enjoying better health and take informed decisions of their lives.” Kavita, girl 17 years “After I return from school I immediately rush to HIC where I like spending time and get to learn and access the library.” Geeta, girl 16 years “Before coming here (to the HIC) my daughter was nervous and having less confidence in whatever she does, but now it is heartening to see tremendous change in her personality and confidence. It is amazing.” Mother of a HIC attendee, Dwaraka “It is envisioned that the youth and communities will be actively and effectively involved and enabled to increase their responsibility towards environment to improve their own health status. The intention, therefore, is to build the capacity of communities to access, analyse, plan, implement and manage health and health related development issues”

18
Local leader, Dwarka Photos:
Picture 1 (June 2012): This poster designed by the Peer Educator on the left,
was selected to be presented at the World Environment Summit held in Brazil (a conference on child rights and ecology). The concept of the poster is the impact
of water, sanitation and pollution on young people.
Picture 2:Wall painting workshop by CCRT (Centre for Cultural Resources and Training) Delhi, September 2012
19
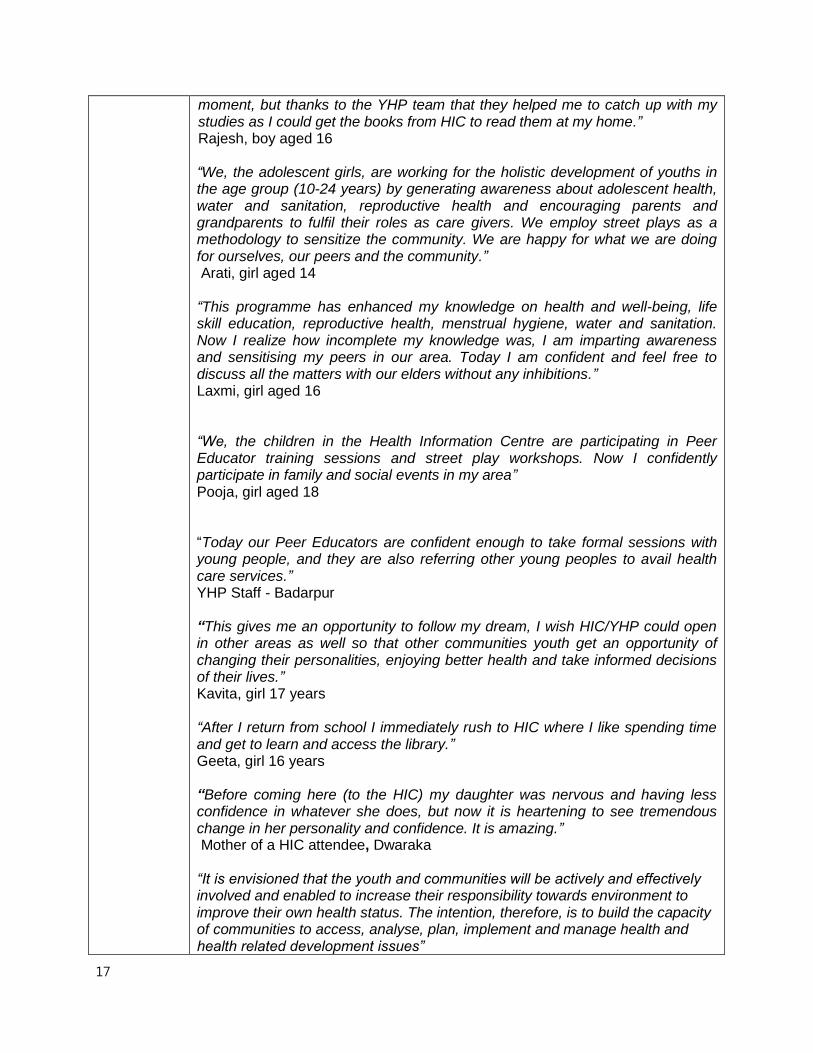
Picture 3:Adolescent visit to the Natural Museum of Natural Sciences where
they focused on the human biology exhibition, October 2012
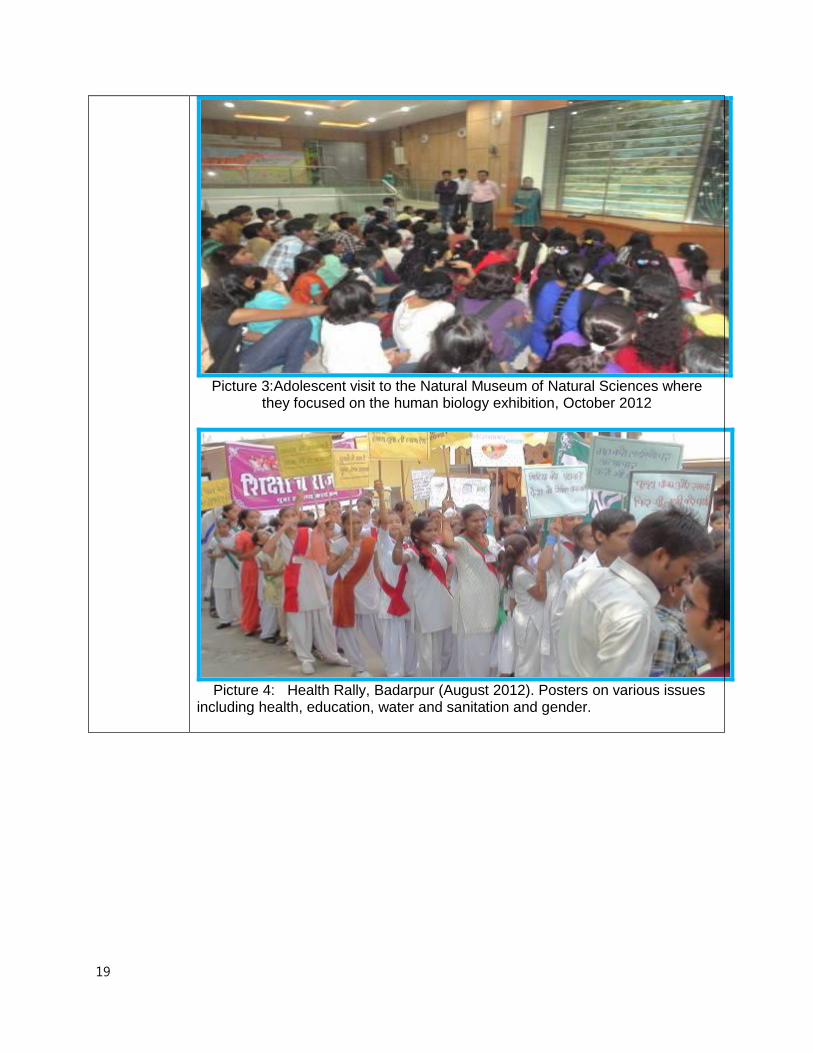
Picture 4: Health Rally, Badarpur (August 2012). Posters on various issues including health, education, water and sanitation and gender.

20
Picture 5: School Sanitation Training in Progress, Holambi Kalan (August 2012)
Picture 6: Water tank installation supported by the project, Holambi Kalan (July
2012)
21
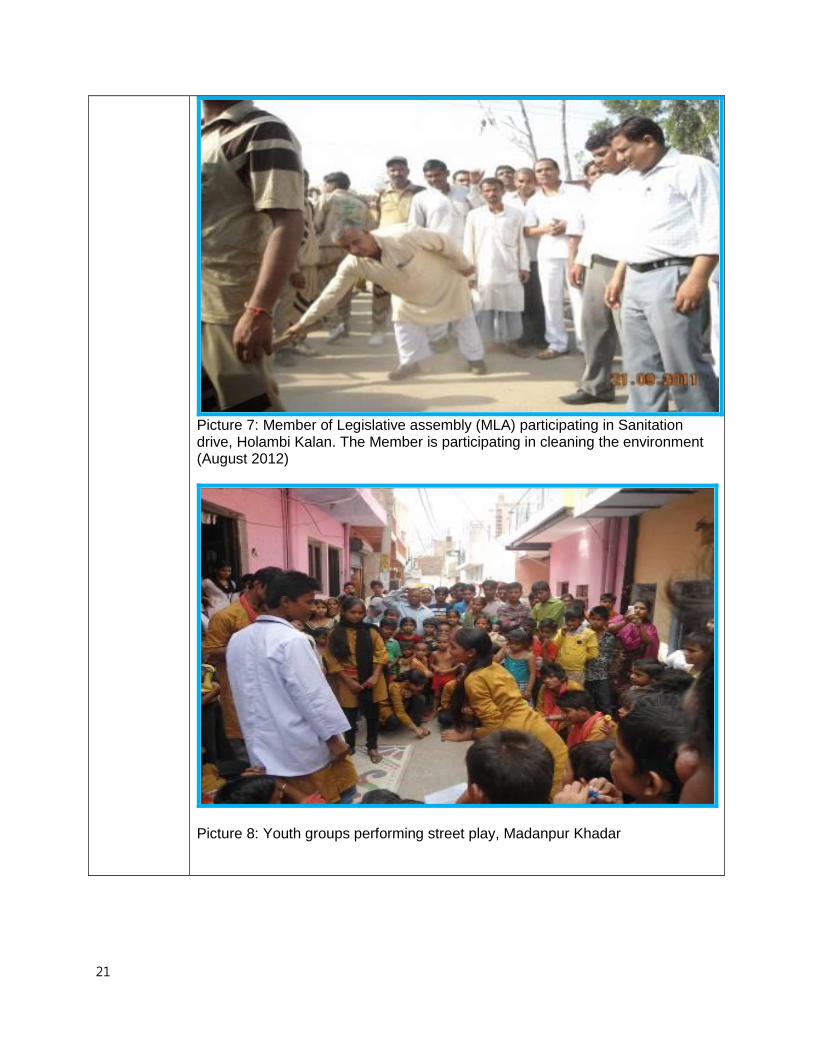
Picture 7: Member of Legislative assembly (MLA) participating in Sanitation drive, Holambi Kalan. The Member is participating in cleaning the environment (August 2012)
Picture 8: Youth groups performing street play, Madanpur Khadar
22
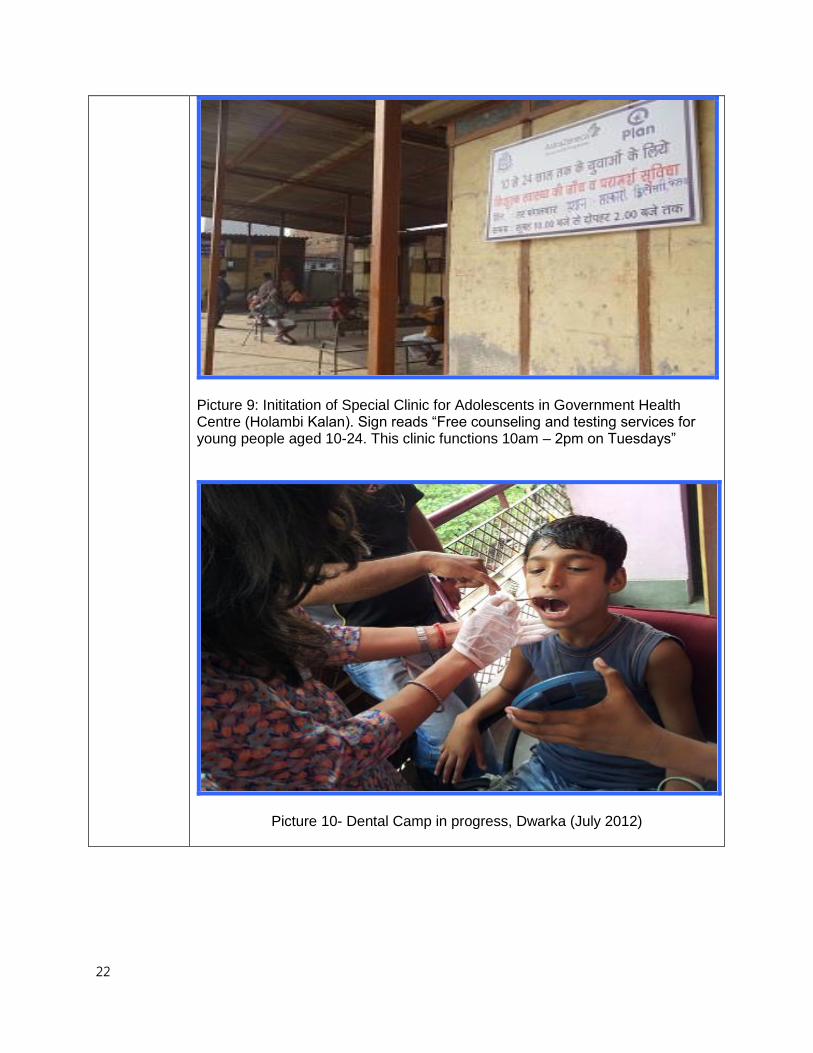
Picture 9: Inititation of Special Clinic for Adolescents in Government Health Centre (Holambi Kalan). Sign reads “Free counseling and testing services for young people aged 10-24. This clinic functions 10am – 2pm on Tuesdays”
Picture 10- Dental Camp in progress, Dwarka (July 2012)
23
Picture 11- Sanitation kit (including toothpaste, antiseptic and a manual) that Peer Educators are given.
24
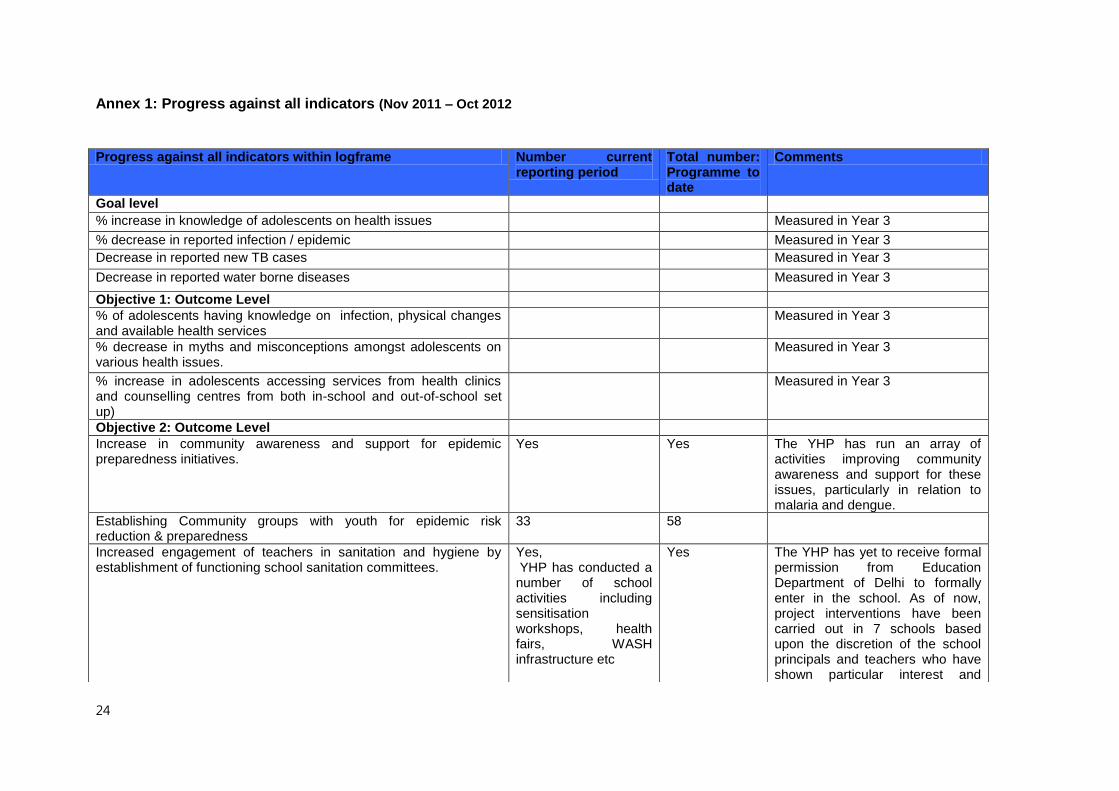
Annex 1: Progress against all indicators (Nov 2011 – Oct 2012
Progress against all indicators within logframe Number current reporting period
Total number: Programme to date
Comments
Goal level
% increase in knowledge of adolescents on health issues Measured in Year 3
% decrease in reported infection / epidemic Measured in Year 3
Decrease in reported new TB cases Measured in Year 3
Decrease in reported water borne diseases Measured in Year 3
Objective 1: Outcome Level
% of adolescents having knowledge on infection, physical changes and available health services
Measured in Year 3
% decrease in myths and misconceptions amongst adolescents on various health issues.
Measured in Year 3
% increase in adolescents accessing services from health clinics and counselling centres from both in-school and out-of-school set up)
Measured in Year 3
Objective 2: Outcome Level
Increase in community awareness and support for epidemic preparedness initiatives.
Yes Yes The YHP has run an array of activities improving community awareness and support for these issues, particularly in relation to malaria and dengue.
Establishing Community groups with youth for epidemic risk reduction & preparedness
33 58
Increased engagement of teachers in sanitation and hygiene by establishment of functioning school sanitation committees.
Yes, YHP has conducted a number of school activities including sensitisation workshops, health fairs, WASH infrastructure etc
Yes The YHP has yet to receive formal permission from Education Department of Delhi to formally enter in the school. As of now, project interventions have been carried out in 7 schools based upon the discretion of the school principals and teachers who have shown particular interest and
25
support.
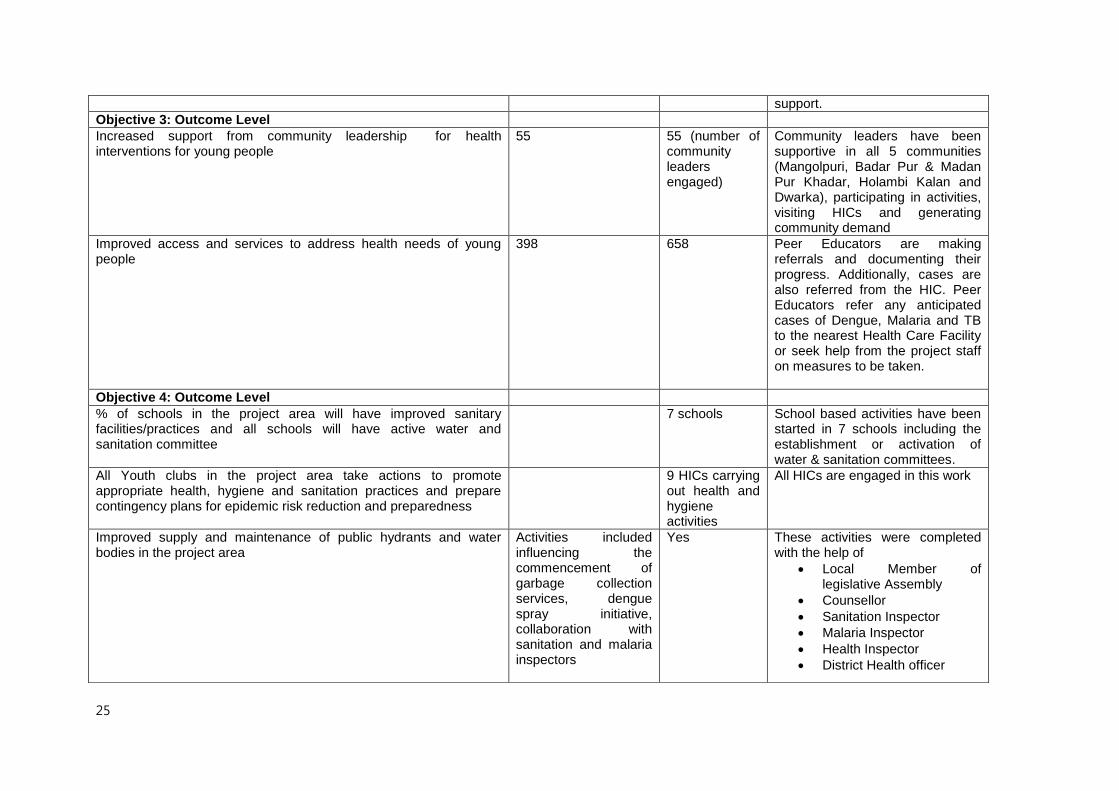
Objective 3: Outcome Level
Increased support from community leadership for health interventions for young people
55 55 (number of community leaders engaged)
Community leaders have been supportive in all 5 communities (Mangolpuri, Badar Pur & Madan Pur Khadar, Holambi Kalan and Dwarka), participating in activities, visiting HICs and generating community demand
Improved access and services to address health needs of young people
398 658 Peer Educators are making referrals and documenting their progress. Additionally, cases are also referred from the HIC. Peer Educators refer any anticipated cases of Dengue, Malaria and TB to the nearest Health Care Facility or seek help from the project staff on measures to be taken.
Objective 4: Outcome Level
% of schools in the project area will have improved sanitary facilities/practices and all schools will have active water and sanitation committee
7 schools School based activities have been started in 7 schools including the establishment or activation of water & sanitation committees.
All Youth clubs in the project area take actions to promote appropriate health, hygiene and sanitation practices and prepare contingency plans for epidemic risk reduction and preparedness
9 HICs carrying out health and hygiene activities
All HICs are engaged in this work
Improved supply and maintenance of public hydrants and water bodies in the project area
Activities included influencing the commencement of garbage collection services, dengue spray initiative, collaboration with sanitation and malaria inspectors
Yes These activities were completed with the help of
Local Member of legislative Assembly
Counsellor
Sanitation Inspector
Malaria Inspector
Health Inspector
District Health officer
26
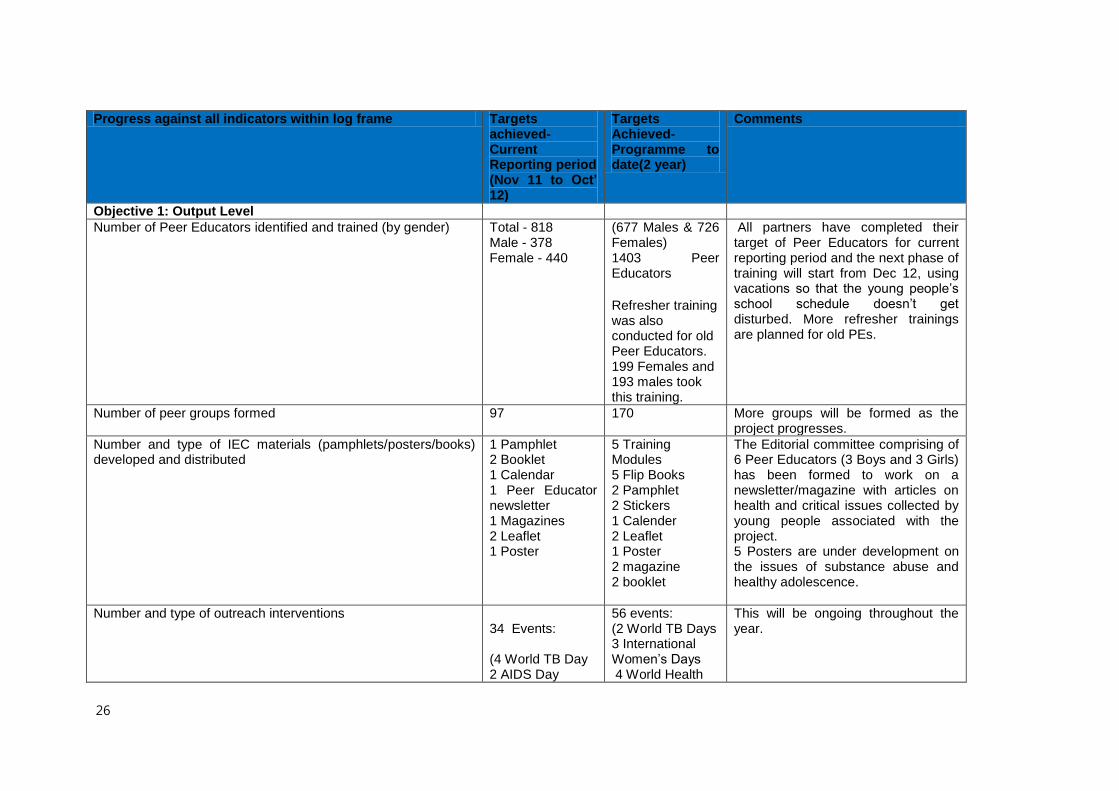
Progress against all indicators within log frame Targets achieved-Current Reporting period (Nov 11 to Oct’ 12)
Targets Achieved-Programme to date(2 year)
Comments
Objective 1: Output Level
Number of Peer Educators identified and trained (by gender) Total - 818 Male - 378 Female - 440
(677 Males & 726 Females) 1403 Peer Educators Refresher training was also conducted for old Peer Educators. 199 Females and 193 males took this training.
All partners have completed their target of Peer Educators for current reporting period and the next phase of training will start from Dec 12, using vacations so that the young people’s school schedule doesn’t get disturbed. More refresher trainings are planned for old PEs.
Number of peer groups formed 97 170 More groups will be formed as the project progresses.
Number and type of IEC materials (pamphlets/posters/books) developed and distributed
1 Pamphlet 2 Booklet 1 Calendar 1 Peer Educator newsletter 1 Magazines 2 Leaflet 1 Poster
5 Training Modules 5 Flip Books 2 Pamphlet 2 Stickers 1 Calender 2 Leaflet 1 Poster 2 magazine 2 booklet
The Editorial committee comprising of 6 Peer Educators (3 Boys and 3 Girls) has been formed to work on a newsletter/magazine with articles on health and critical issues collected by young people associated with the project. 5 Posters are under development on the issues of substance abuse and healthy adolescence.
Number and type of outreach interventions 34 Events: (4 World TB Day 2 AIDS Day
56 events: (2 World TB Days 3 International Women’s Days 4 World Health
This will be ongoing throughout the year.
27
Celebration 3(Cultural events- Diwali celebration Day, cricket match-sports day) 3 Women’s Day 2 Water Day) 1 Environment day 1 Drugs Abuse Rally 1 Hand Wash Day 1 Cultural Day 1 Disaster Management day 1 World Food Day 1 World Population Day 1 Independence Day 1 Teacher Day
Days 1 Water Day 1 International Youth Day 1 World Environment Day 1 Malaria Day 1 Cleanliness Drive 2 Hand Washing Days 2 Girl Child Weeks 1 Breast Feeding week 2 Cultural Events 1 Disaster Management Day
Estimated number of community members reached through outreach
38,465 60,988 Community members reached out through mass awareness activities like-(Street play, Puppet Show, Rally, Camps, and Community Meetings, Health Mela etc.)
Number of adolescents informed/reached by Peer Education mobilization activities
35,250 65,250 This figure indicates the number of young people reached through trained peer educators, HIC attendees, group meeting and mass awareness activities.
Number of HIC established 4 9 6 more planned to be opened in year three.
Number of referrals made by HIC and peer educators 398 658 Through the monthly reporting format used by PEs and HICs.
28
Objective 2: Output Level
Formation of active Community Stakeholder Groups in each community
36 59 59 Groups have been formed to promote young people’s health. Additionally, 9 HIC committees have also been formed whose role is to ensure that HIC functions effectively.
Number of referrals made through community based referral system
68 68 This will be ongoing throughout the entire programme.
Number of community meetings carried out 237 551 In the meetings, the discussions were around familiarizing the community with the project, health issues and, misconceptions associated and how to dispel them all.
Number and type of IEC materials (pamphlets/posters/books) developed and distributed
1 Pamphlet 1 Poster 2 Booklet 1 Magazine
2 Pamphlet 1 Poster 2 Booklet
This pamphlet was developed by 14 year old Peer Educator from Mangolpuri area. On water, environment and sanitation issues.
Number of Melas/ Thematic camps/ street plays/ video shows on sanitation, hygiene, infection prevention, debates held
115 Street Play 41 Film Show 5 Rallies 33 Health Talks 11 Puppet Show 2 Health Mela 4 Magic Shows 12 Others
238 Street Plays 72 Video Shows 14 Rallies 48 Health Talks 39 Puppet Shows 6 Health Melas 4 Magic shows 12 Others
This is an effective communication medium to increase community awareness as also endorsed by the community.
Number of community members sensitized 38,465 (Nov11-Oct12)
60,988 (Nov10-Oct12)
It is gradually increasing through various communication strategies (One to one meetings, group meetings, meeting at the HICs, and various mass awareness activities).
Objective 3: Output Level
Number of health providers trained on adolescent health & counselling skills imparted
295 586 This includes Medical Officers (MOs), Auxiliary Nurse Midwives (ANMs), Accredited Social Health Activists (ASHA) workers and Anganwadi workers.
Number of legislators leaders, media persons, police) supportive of health initiatives attending workshops.
2 MLA 2 MC
6 MLAs 9 MCs
More will be sensitized as the project progresses. (Member of Legislative
29
11 RWA 6 Counselor 4 Local Leaders
14 RWA Presidents 6 Counselors 4 Local Leaders
Assembly (MLA); Municipal Councillor (MC) and Resident Welfare Association (RWA).
Objective 4: Output Level
Number of schools participating in sanitation activities 1.Conducted
Sanitation programme with adolescent-distribution of sanitation kits 2.Teachers sensitization meeting on thematic issues – like – water & sanitation, Health and social issues
1.Conducted
Sanitation programme with adolescent-distribution of sanitation kits 2.Teachers sensitization meeting on thematic issues – like – water & sanitation, Health and social issues
This is underway in 7 schools.
Number of Youth clubs involved in sanitation work in the community
9 9 All HICs are supporting work in sanitation.
Number of sessions facilitated by Peer Educators under the supervision of teachers
NA NA This will take place after the permission is granted by the Education Dept, Govt of Delhi.
Number of referral/counselling done by trained teachers Male – 35 Female - 21
Male – 35 Female - 21
A small number of teachers and principals from 7 schools reached.
Number of Community action groups taking part in maintaining public hydrants
0 0 This will take place in the next six months.
30
Annex 2 Progress against Activity Plan (Nov 2010 – Oct 2012)
Activity Description Variance/Deviation Comment
Start-up workshop
A workshop was organized in Delhi, which was attended by AZ and partner staff. The project was reviewed and revised accordingly. A brief overview of the baseline was provided and the expectations and requirements of the project were discussed.
Completed
Partners developed work plans following this workshop. Partners gained clarity on the project.
Finalizing the baseline report
The baseline report was finalized, after incorporating comments by the programme and technical team.
Completed
The results of the baseline (and specific area-characteristics) were incorporated into the work plan of various partners.
Developing work plans
All the four partner organizations developed a detailed annual work plan for their project including a budget.
Completed Also Year 3 planning completed
Recruitment of Staff
Project Managers (4) and Project Coordinators (12) were recruited by the partners.
On schedule Partners recruited the project staff on time.
Orientation of Staff
Newly recruited Project Managers and Project Coordinators were oriented on the project (goal, objectives, strategies, milestones etc.)
Completed All partners got the orientation training and capacity building training. Training 1-‘Training on 5 Project Thematic Areas’ Training 2-Communication and Facilitation skills
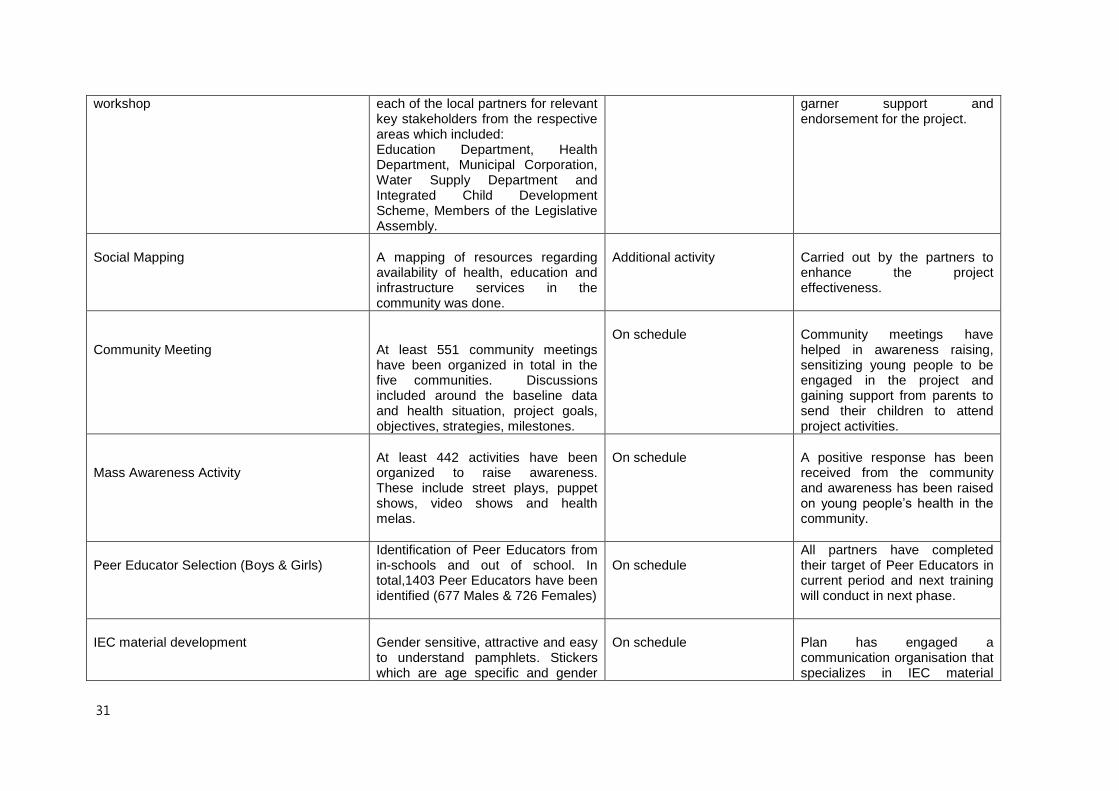
Stakeholder sensitization and coordination
Five workshops were organised by
On schedule
Workshops were organized to
31
workshop
each of the local partners for relevant key stakeholders from the respective areas which included: Education Department, Health Department, Municipal Corporation, Water Supply Department and Integrated Child Development Scheme, Members of the Legislative Assembly.
garner support and endorsement for the project.
Social Mapping
A mapping of resources regarding availability of health, education and infrastructure services in the community was done.
Additional activity
Carried out by the partners to enhance the project effectiveness.
Community Meeting
At least 551 community meetings have been organized in total in the five communities. Discussions included around the baseline data and health situation, project goals, objectives, strategies, milestones.
On schedule
Community meetings have helped in awareness raising, sensitizing young people to be engaged in the project and gaining support from parents to send their children to attend project activities.
Mass Awareness Activity
At least 442 activities have been organized to raise awareness. These include street plays, puppet shows, video shows and health melas.
On schedule
A positive response has been received from the community and awareness has been raised on young people’s health in the community.
Peer Educator Selection (Boys & Girls)
Identification of Peer Educators from in-schools and out of school. In total,1403 Peer Educators have been identified (677 Males & 726 Females)
On schedule
All partners have completed their target of Peer Educators in current period and next training will conduct in next phase.
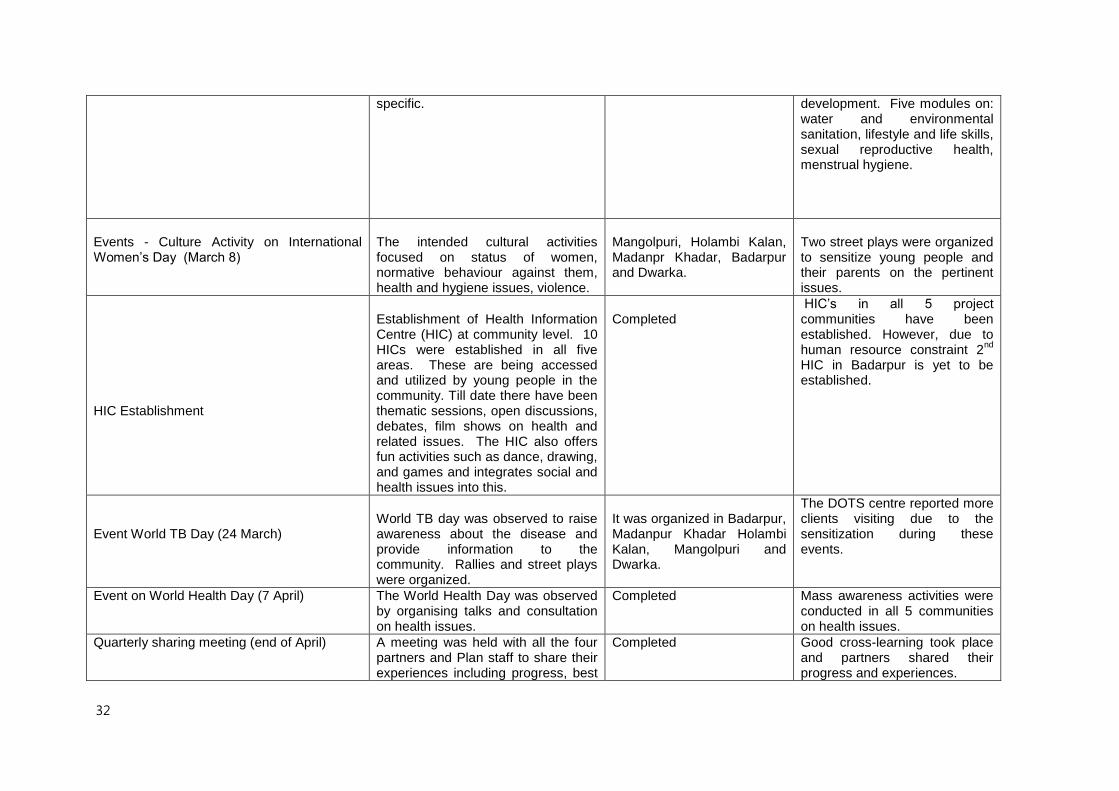
IEC material development
Gender sensitive, attractive and easy to understand pamphlets. Stickers which are age specific and gender
On schedule
Plan has engaged a communication organisation that specializes in IEC material
32
specific. development. Five modules on: water and environmental sanitation, lifestyle and life skills, sexual reproductive health, menstrual hygiene.
Events - Culture Activity on International Women’s Day (March 8)
The intended cultural activities focused on status of women, normative behaviour against them, health and hygiene issues, violence.
Mangolpuri, Holambi Kalan, Madanpr Khadar, Badarpur and Dwarka.
Two street plays were organized to sensitize young people and their parents on the pertinent issues.
HIC Establishment
Establishment of Health Information Centre (HIC) at community level. 10 HICs were established in all five areas. These are being accessed and utilized by young people in the community. Till date there have been thematic sessions, open discussions, debates, film shows on health and related issues. The HIC also offers fun activities such as dance, drawing, and games and integrates social and health issues into this.
Completed
HIC’s in all 5 project communities have been established. However, due to human resource constraint 2
nd
HIC in Badarpur is yet to be established.
Event World TB Day (24 March)
World TB day was observed to raise awareness about the disease and provide information to the community. Rallies and street plays were organized.
It was organized in Badarpur, Madanpur Khadar Holambi Kalan, Mangolpuri and Dwarka.
The DOTS centre reported more clients visiting due to the sensitization during these events.
Event on World Health Day (7 April)
The World Health Day was observed by organising talks and consultation on health issues.
Completed Mass awareness activities were conducted in all 5 communities on health issues.
Quarterly sharing meeting (end of April)
A meeting was held with all the four partners and Plan staff to share their experiences including progress, best
Completed Good cross-learning took place and partners shared their progress and experiences.
33
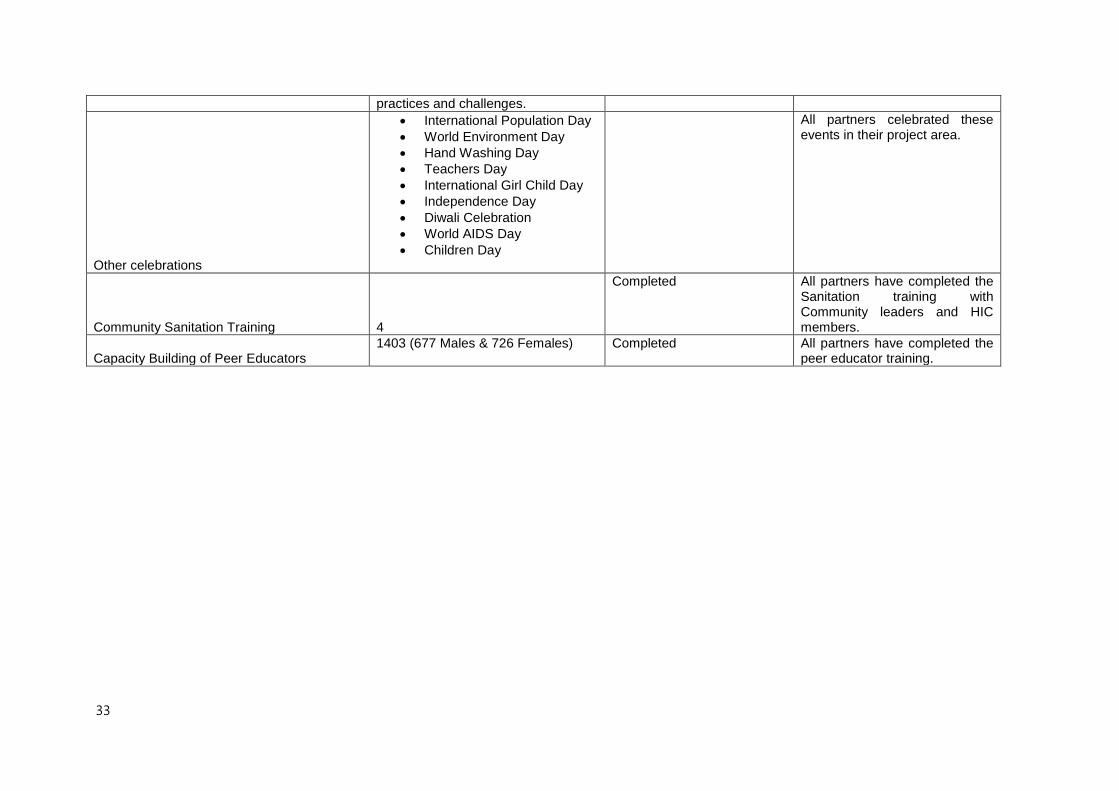
practices and challenges.
Other celebrations
International Population Day
World Environment Day
Hand Washing Day
Teachers Day
International Girl Child Day
Independence Day
Diwali Celebration
World AIDS Day
Children Day
All partners celebrated these events in their project area.
Community Sanitation Training 4
Completed All partners have completed the Sanitation training with Community leaders and HIC members.
Capacity Building of Peer Educators 1403 (677 Males & 726 Females)
Completed All partners have completed the
peer educator training.





























