Embed Size (px)
Citation preview

Asymmetric Distribution of Arteriovenous Crossings in the Normal Retina
David V. Weinberg, MD/ Kathleen M. Egan, MPH/ Johanna M. Seddon, MD2
Background: Recently, there has been renewed interest in the orientation of the crossing retinal vessels at arteriovenous intersections, particularly as it relates to the risk of branch vein occlusion. Little is known about the distribution of the two types of crossings in the normal retina.
Methods: The authors studied standard fundus photographs of 51 subjects without retinal disease. Arteriovenous crossings were analyzed for fundus location and relative orientation of the crossing vessels (vein-posterior or vein-anterior).
Findings: In the superotemporal quadrant, crossings were distributed closer to the optic disc (P < 0.001 ), and a greater proportion of crossings were vein-posterior (P = 0.01) than in the inferotemporal quadrant. As a result, within a 3-disc diameter (DD) radius of the optic disc, there were significantly more vein-posterior crossings in the superotemporal than in the inferotemporal quadrant (P < 0.001 ).
Conclusion: These findings further define normal retinal vascular anatomy and may explain the predilection for branch retinal vein occlusions to occur in the superotemporal quadrant. Ophthalmology 1 993; 100:31-36
The retinal blood vessels exit the optic disc and branch in a complex pattern to serve the metabolic need of the inner retina. As the vessels traverse the retina, the arteries and veins frequently cross one another. Branch retinal vein occlusions (BRVOs) occur at arteriovenous crossings. At crossing points, the vein most frequently crosses under (posterior to) the artery. In 19 36, Jensen 1 published a monograph on BRVO in which he observed that BRVOs rarely occur at crossings where the vein crosses over the artery. In the eyes of visually normal patients, he counted a greater number of arteriovenous crossings in the superotemporal quadrant than in the inferotemporal quad-
Originally received: April 7, 1992.
Revision accepted: August 10, 1992. 1 Department of Ophthalmology, Northwestern University Medical School, Chicago. 2 Retina Service, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston.
Presented in part at the Association for Research in Vision and Ophthalmology Annual Meeting, Sarasota, May 1992.
Reprint requests to David Weinberg, MD, Northwestern University Medical School, Ward 2-186, 303 East Chicago Ave, Chicago, IL 60611.
rant. The proportion of vein-posterior crossings was slightly higher in the superotemporal than in the inferotemporal quadrant. Jensen speculated that the predominance of superotemporal BRVO was due to the greater number of arteriovenous crossings, particularly vein-posterior crossings, in the superotemporal quadrant.
Jensen's observation that BRVO rarely occurs at veinanterior crossings has recently been confirmed by two studies that found that 2.4% or less of BRVOs occur at vein-anterior crossings, a rate much lower than the proportion of vein-anterior crossings in the fundus. 2
•3 The
data demonstrate that each vein-posterior crossing carries a much greater risk of BRVO than each vein-anterior crossing. This investigation was designed to systematically study the distribution of the two types of arteriovenous crossings in the eyes of visually normal subjects.
In general, previous studies have used terminology that referred to the vessel that was located most anteriorly at the crossing point. For the purposes of this report, we chose to refer to the position of the vein relative to the artery, either vein-anterior or vein-posterior. We chose this terminology because it seemed simpler, and because our principal conclusions were relevant to BRVO.
31

Ophthalmology Volume 100, Number 1, January 1993
Patients and Methods
Patients were recruited from the outpatient clinics of the Massachusetts Eye and Ear Infirmary. Patients were included if they met the following entry criteria: age 60 years of age or younger, with no history of retinal disease, and ocular media of sufficient clarity to obtain high-quality fundus photographs. Stereoscopic 30° photographs of both eyes were taken with a fundus camera (Zeiss, Germany) using color transparency film. Standard fields centered on the disc (field 1) and centered on the macula (field 2) were taken of each eye.
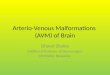
A 127 X 102 em transparent grid overlay was constructed and hung in front of a white projection surface. Major horizontal and vertical grid marks were placed at 12-cm intervals. Minor grid marks were placed at 2.4-cm intervals. A circle 12 em in diameter was drawn in the center of the grid (Fig 1 ). An Ektagraphic III slide projector (Eastman Kodak) equipped with an Ektanar f:3.5, 4-6-inch zoom lens (Eastman Kodak) was used to project the transparencies onto the screen. To avoid distortion of the image, the projector was aligned horizontally and vertically with the center of the screen. For each eye, field 1 was first projected onto the screen. The optic disc was focused, centered in the circle, and the zoom adjusted so that the horizontal diameter of the optic disc just filled the circle. The paths of the retinal vessels were drawn on the grid with an erasable pen, marking the position of each arteriovenous intersection. Field 2 of the same eye was then projected. The optic disc was centered in the circle using the same projection distance and zoom setting used for field 1. The positions of any arteriovenous crossings that had not been seen in field 1 were marked on the screen.
Photographs were read by a single reader (DVW). The transparencies were viewed on a light table using stereo-
4
3
2
r \ \.._ ~
0
·1
·2
·3
-4 ·5 -4 -3 -2 -1 0 2 3 4 5
Figure 1. A scale representation of the grid used to determine the positions of the arteriovenous crossings. In the actual grid, the diameter of the circle and the spacing of the major grid marks were 12 em. The images were projected onto the screen and the magnification was adjusted so that the horizontal disc diameter just filled the circle. Horizontal and vertical distances were read in disc diameters.
32
scopic viewers specially modified for 7X magnification. Each arteriovenous intersection was examined to determine the relative positions of the crossing artery and vein, which were either vein crossing posterior to the artery or vein crossing anterior to the artery. For intersections for which this relationship could be ascertained, the type of crossing was recorded. The horizontal and vertical distances from the center of the disc were determined from the grid and recorded to the nearest 0.1 disc diameter (DD). For horizontal measurements, distances temporal to the disc were considered positive, and distances nasal to the disc were considered negative. For vertical measurements, distances superior to the disc were considered positive, and those inferior to the disc were considered negative. This convention was used for both right and left eyes. For each crossing, the direct distance from the center of the optic disc was calculated as the square root of the sum of the squares of the measured horizontal and vertical distances (Pythagorean theorem).
The quadrant in which the crossing was found was recorded. In general, the quadrant to which a crossing was assigned (superotemporal, inferotemporal, superonasal, or inferonasal) was based on position relative to horizontal and vertical lines passing through the center of the disc. Because the retinal vessels tend to exit from the nasal side of the disc, the first-order crossings of the vessels supplying the temporal retina sometimes occurred nasal to the center of the disc. Crossings of this type were assigned to the temporal quadrants based on their major distribution.
Comparisons of the superotemporal and inferotemporal quadrants were based on averaged counts of the left and right eyes of each patient with n = 51. The average value of the left and right eye also was used in analysis of patterns by gender and age. The paired t test was used to evaluate differences in mean values within eyes, and Student's t test was used to evaluate differences between groups. Nonparametric tests were used for comparison of proportions.
Findings
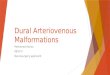
Composite diagrams display the positions of all observed vein-posterior crossings (Fig 2) and vein-anterior crossings (Fig 3) in the 102 eyes. A summary of the crossing configuration and fundus position of all arteriovenous crossings is presented in Table 1. A total of 933 crossings was counted in 102 eyes of 51 patients (9.1 crossings per eye). The vein crossed posterior to the artery at 672 crossings (72%) and anterior to the artery at 261 crossings (28% ). The average distance of crossings from the center of the disc was 2 DD. Vein-posterior crossings occurred closer to the optic disc than did vein-anterior crossings (mean distances, 1. 7 and 2.1 DD, respectively; P < 0.001 ).
The remainder of the analyses were confined to observations about the temporal quadrants. Table 2 shows results stratified by eye, gender, and age. There were significantly more crossings in the left eyes than in the right. However, the proportion of crossing types was statistically

Weinberg et al · Arteriovenous Crossings in the Normal Retina
VEIN-POSTERIOR CROSSINGS
2
-2
4+---~---r--~--~--~----r---~--,---~--~ -4 -2
Figure 2. A composite drawing of the positions of all vein-posterior crossings in 102 eyes. The axes are labeled in disc diameters and intersect at the center of the optic disc. The lateral orientation of the right eyes is reversed so that right and left eyes can be superimposed.
similar by eye. Males and females were similar both in number of crossings and the proportion of crossing types. The average age of patients was 39 years (range, 20 to 60 years). Patients younger than 40 years had approximately 2 more crossings counted per eye, on average, compared with older patients, but the composition of crossing types did not vary by age.
The superotemporal and inferotemporal quadrants were compared with respect to the number, composition, and position of crossings (Table 3). In the temporal quadrants, a total of 668 crossings were counted, of which 489 (72%) were vein-posterior and 179 (28%) were vein-anterior. The proportion of vein-posterior crossings in the superotemporal quadrant (78%) was greater than in the inferotemporal quadrant (68%) (P = 0.01).
The mean number of crossings was similar in the superotemporal (3.2 per eye) and inferotemporal (3.3 per eye) quadrants (P = 0.62). In the superotemporal quadrant, however, crossings were distributed nearer to the disc (Fig 4 ). The mean distance of crossings from the center of the optic disc was 2.1 DD in the superotemporal quadrant and 2.5 DD in the inferotemporal quadrant (P < 0.001 ). The number of crossings within a 3-DD radius of the center of the disc was greater in the superotemporal than the inferotemporal quadrant (P = 0.03). The combined effects of the distribution of crossings closer to the disc and the greater proportion of vein-posterior crossings in the superotemporal quadrant resulted in a greater number of vein-posterior crossings within 3 DD of the disc in the superotemporal quadrant than the inferotemporal quadrant ( 1.9 and 1.3 crossings per eye, respectively; P < 0.001 ). In contrast, vein-anterior crossings were more numerous in the inferotemporal than the superotemporal quadrant
VEIN-ANTERIOR CROSSINGS
.- .· . '• : : =.~~:: .
~;, . • ·:-:- ;+ • : . •: .. · .: .. .·
': . · . .: .. -2 . :·: ..
·.:
-4+---~---r-------+--------r---~--~--~--4 -4 -2
Figure 3. A composite drawing of the positions of all vein-anterior crossings in 102 eyes. The axes are labeled in disc diameters and intersect at the center of the optic disc. The lateral orientation of the right eyes is reversed so that right and left eyes can be superimposed.
To show regional differences, the numbers and types of crossings in the two temporal quadrants were calculated for concentric 0.5-DD zones around the optic disc. These data are graphically displayed in Figure 4. The proportions of vein-posterior crossings in each concentric zone are displayed in Figure 5.
Discussion
We found no significant difference in the number or proportion of crossing types by gender. Left eyes had a slightly greater number of arteriovenous crossings than right eyes. Although the difference was statistically significant, the clinical significance is unclear. Except for the series reported by Blankenship and Okun,4 in which 64% of BR VOs were in the left eye, there seems to be no predilection for BR VOs to occur in left eyes.
Numerous clinical series have documented that BRVO most commonly occurs in the superotemporal quadrant. The second most common location is inferotemporaL BR VO is uncommon in the nasal quadrants. In 407 cases of temporal BRVO pooled from 6 clinical series of 40 or more cases each, 62% of temporal BR VOs were superotemporal and 38% were inferotemporaL 1•
3-
7 Nearly all BRVOs observed clinically occur within 3 DD of the optic disc.4 For this reason, we evaluated crossings within 3 DD of the optic disc in a separate analysis.
Jensen, 1 using direct ophthalmoscopy, counted the number of arteriovenous intersections in the eyes of 50 patients. He found a greater number of crossings in the superotemporal quadrant than in the inferotemporal quadrant. This asymmetry has been used to explain the greater number of BRVOs occurring in the superotem-
33

Ophthalmology Volume 100, Number 1, January 1993
Table 1. Crossing Configuration in all Four Quadrants and in the Temporal Quadrants
All Vein-posterior V ein·anterior Crossings Crossings Crossings
All Quadrants Total number (%) 933 672 (72) 261 (28)
Mean per eye (range) 9.1 (5-16) 6.6 (3-13) 2.6 (0-6)
Mean distance from disc in DD (range) 2.0 (0.3-5.4) 2.1 (0.3-5.2) 1.7 (0.3-5.6)
Temporal Quadrants Total number (%) 668 489 (73) 179 (27)
Mean per eye (range) 6.5 (3-14) 4.8 (2.5-9.5) 1.7 (0-4.5)
DD =disc diameters.
poral quadrant. 8 In contrast to Jensen, we found no difference in the overall number of crossings in the superotemporal and inferotemporal quadrants. However, the crossings were distributed differently, with a greater density of crossings closer to the disc in the superotemporal quadrant, as demonstrated in Figure 4. Because of this difference in distribution, within a 3-DD radius of the center of the disc there were significantly more crossings in the superotemporal quadrant. The limitations of direct ophthalmoscopy may have biased Jensen's observations to crossings nearer to the optic disc.
Our finding that the vein crossed anterior to the artery at 28% of all arteriovenous crossings is consistent with previous reports. 1
•3 Due to factors that are unclear, vein
anterior crossings are relatively protected from occlusion, accounting for 2.4% or less of all BRVOs?·3 On the average, vein-anterior crossings occurred closer to the disc than vein-posterior crossings and were more common in the inferotemporal than the superotemporal quadrant.
Table 2. Comparison of Temporal Arteriovenous Crossing by Eye, Gender, and Age
Eye OD OS
Gender Male Female
Age <40 yrs ~40 yrs
Number
51 51
30 21
29 22
Mean Number of Crossings (Range)
6.1 (3.0-11.0) 7.0* (3.0-14.0)
6.5 (3.5-11.5) 6.6 (4.0-10.0)
7.4 (3.5-11.5) 5.5* (4.0-8.0)
OD = right eye; OS = left eye.
• p < 0.05.
34
Percent V ein•posterior
Crossings (Range)
73 (25-100) 74 (25-100)
72 (45-100) 75 (40-93)
74 (55-93) 72 (40-100)
Figure 5 shows the relative proportions of vein-posterior crossings in the two quadrants. In each zone within 3 DO of the disc, the proportion of vein-posterior crossings in the superotemporal quadrant was greater than or equal to the proportion in the corresponding zone of the inferotemporal quadrant.
The findings of this study are relevant in interpreting previous reports. We found that arteriovenous crossings are not randomly distributed with respect to distance from the optic disc or quadrant. Thus, when making comparisons regarding arteriovenous crossings in the superotemporal and inferotemporal quadrants, it is important that standard documentation be used, which equally represents equivalent regions of the two quadrants.
Weinberg and associates3 found a greater proportion of vein-posterior crossings in eyes with BR YO compared with uninvolved fellow eyes or controls. Because standard photographic fields were not used, the photographs of the BRVO eyes almost certainly over-represented the quadrant containing the BRVO (most frequently the superotemporal quadrant). Photographs of the fellow eyes or controls would not be expected to be biased by quadrant. This sampling difference could explain the reported differences between the groups. The greater proportion of vein-posterior crossings in the BRVO eyes may have been due to the over-representation of the superotemporal quadrant, where we have shown the proportion of veinposterior crossings to be highest.
The asymmetry in the distribution of numbers and types of crossings predicts a greater frequency of BRVO in the superotemporal quadrant. If all crossings in the temporal quadrants are assumed to have an equal risk of BRVO, then based on the mean number of crossings in each quadrant, our data predict that 49% of temporal BRVOs should occur in the superotemporal quadrant. As previously stated, nearly all BR VOs occur within 3 DO ofthe optic disc.4 If all crossings within 3 DO ofthe disc are considered, the predicted incidence of BRVO in the superotemporal quadrant increases to 54%. An additional factor to be considered is the difference in relative risk of BRVO at vein-anterior and vein-posterior crossings . Weinberg and associates3 found 97.6% of all BRVOs at

Weinberg et al · Arteriovenous Crossings in the Normal Retina
Table 3. Comparison of Crossing Patterns in the Superotemporal and Inferotemporal Quadrants
Superotemporal lnferotemporal P Value
Mean distance from disc in DD (range) 2.1 (0.4-5.2) 2.5 (0.4-5.4) < 0.001 Mean number of all crossings
Overall (range) 3.2 (1.5-6.5) 3.3 (1.0-6.0) 0.62 Within 3 DD (range) 2.4 (1.0-5.0) 2.0 (0.5-4.0) 0.03
Mean number ofV-P crossings Overall (range) 2.5 (1.0-5.0) 2.3 (0-5.0) 0.26 Within 3 DD (range) 1.9 (0.5-4.5) 1.3 (0-3.0) < 0.001
Mean number of V-A crossings Overall (range) 0.72 (0-2.0) 1.0 (0-3.5) 0.01 Within 3 DD (range) 0.55 (0-1.5) 0.70 (0-2.0) 0.14
Mean percent ofV-P crossings Overall (range) 78 (33-100) 68 (0-100) 0.01 Within 3 DD (range) 77 (33-100) 65 (0-100) 0.06
DD ~ distance from the center of the optic disc in disc diameters; V-P ~vein-posterior; V-A~ vein-anterior.
vein-posterior crossings. Only 77.7% of crossings in the same eyes were vein-posterior crossings. Calculating from these data, the risk ofBRVO at each vein-posterior crossings is approximately 12 times higher than each vein-anterior crossing. The data in this report show that veinposterior crossings occur with greater frequency in the superotemporal quadrant. Computing based on the mean
If) (!) z iii If)
0 a: ()
u. 0 a: w ID ~ ;;) z
0·0 5 5· 1 1· 1.5 I 5·2 2·2.5 2 5·3 3·3.5 3.5·4 4·4.5 4 5·5 5·5 5
DISTANCE FROM DISC
Figure 4. A representation of the numbers of arteriovenous crossings in the superotemporal and inferotemporal quadrants by crossing type and distance from the disc. Each division on the horizontal axis represents a concentric 0.5-DD zone measured from the center of the optic disc. The vertical axes represent the number of crossings in the 102 eyes. Solid bars represent vein-posterior crossings and shaded bars represent veinanterior crossings. Notice that crossings in the superotemporal quadrant tend to be found closer to the disc than in the inferotemporal quadrant.
numbers of crossings within 3 DO and the relative risk of BR VO for the two crossing types predicts that 59% of temporal BR VOs should occur in the superotemporal quadrant. This is similar to the previously mentioned figure of 62%, which was the percentage of superotemporal BR VOs calculated from the pooled data of several large series. 1•
3-
7
Our methods involved examining standard fundus photographs of visually normal subjects. In our experi-
100
"' 80 Cl z iii
"' 0 a: ()
60
a: 0 a: UJ 40 .... "' 0 Q.
2: w 20 > ....
0· 0.5 .5 · 1 1· 1.5 1.5· 2 2· 2. 5 2.5 · 3 3· 3 .5 3. 5· • • . • . 5 • . 5 · 5
DISTANCE FROM DISC
Figure 5. The percentage of crossings that are vein-posterior crossings displayed by quadrant and by distance from the disc. Each division on the horizontal axis represents a concentric 0.5-DD zone measured from the center of the optic disc. The solid bars represent the percent of veinposterior crossings within each zone in the superotemporal quadrant. The shaded bars represent the percent of vein-posterior crossings within each zone in the inferotemporal quadrant. Notice that except for the 3-to 3.5-DD zone, the percent of crossings that are vein-posterior in the superotemporal quadrant is always greater than or equal to the percent of vein-posterior crossings in the corresponding zone of the inferotemporal quadrant.
35

Ophthalmology Volume 100, Number 1, January 1993
ence, even under optimal conditions, it is impossible to determine from photographs the anatomy of every arteriovenous crossing. We selected patients with excellent media clarity to allow the classification of a maximum number of crossings, assuming that the counted crossings were a representative sample of all crossings (counted and uncounted). Although we chose patients with excellent media clarity, younger patients inevitably had slightly clearer media, and, as a result, more crossings were counted in the younger than the older patients (7 .4 and 5.5 per eye, respectively; P < 0.001). However, there is no evidence that one crossing type was systematically overor under-counted. If the proportion of crossing types was biased by number of crossings counted, we should have seen a difference in proportion of crossing types between the younger and older patients. Such a difference was not seen (74% versus 72% vein-posterior, respectively; P = 0. 71 ). In addition, our findings of the overall proportions of the two crossing configurations are consistent with previous reports, which used a variety of counting techniques.1-3
Most of our analyses compared findings in the superotemporal and inferotemporal quadrants. We specifically designed our study using standard photographs equally representing the two quadrants to avoid any over- or under-counting of crossings in one quadrant relative to the other. If there was a small systematic over-representation of one crossing type, relative comparisons of the superotemporal and inferotemporal quadrants are still valid since they were studied under the same conditions.
We have shown that our data predict, on a statistical basis, the observed predilection for BRVO to occur in the superotemporal quadrant. Other factors not addressed by this study may also contribute to regional differences in the occurrence ofBR VO. Hemodynamic or anatomic differences between the vessels in the two quadrants may
36
exist. Such differences could account for a difference in the incidence of occlusion by quadrant, or for a tendency for occlusions in one quadrant or the other to be symptomatic.
Limited inferences can be made from the study of visually normal eyes. It is possible that eyes that develop BRVO differ from healthy eyes with respect to arteriovenous crossing patterns. However, these data expand our knowledge of normal retinal vascular anatomy and provide a plausible explanation for the clinically observed predilection for superotemporal BRVO.
References
I. Jensen VA. Clinical studies of tributary thrombosis in the central retinal vein. Acta Ophthalmol Suppl 1936;10.
2. Duker JS, Brown GC. Anterior location of the crossing artery in branch retinal vein occlusion. Arch Ophthalmol 1989;107:998-1000.
3. Weinberg D, Dodwell DG, Fern SA. Anatomy of arteriovenous crossings in branch retinal vein occlusion. Am J Ophthalmol 1990; 109:298-302.
4. Blankenship GW, Okun E. Retinal tributary vein occlusion: history and management by photocoagulation. Arch Ophthalmol 1973;89:363-8.
5. Sedney SC. Photocoagulation in retinal vein occlusion [thesis]. Doc Ophthalmol 1976;40:1-24.
6. Michels RG, Gass JDM. The natural course of retinal branch vein obstruction. Trans Am Acad Ophthalmol Otolaryngol 1974;78:0P166-77.
7. Gutman FA, Zegarra H. The natural course of temporal retinal branch vein occlusion. Trans Am Acad Ophthalmol Otolaryngol 1974;78:0P178-94.
8. Orth DH, Patz A. Retinal branch vein occlusion. Surv Ophthalmol 1978;22:357 -76.