Embed Size (px)
Citation preview

At Issue: Vulnerability to Schizophrenia andLack of Common Sense
by Qiovanni Stanghellini
Abstract
This article explores the hypothesis that the relationaldeficit in schizophrenia is not a consequence of acutesymptoms and course but instead is a fundamentalaspect of schizophrenic vulnerability. This basic rela-tional deficit could be better understood as disconnect-edness from common sense. Common sense is a toolfor adaptation whose main scope is establishing cause-and-effect and motivational relationships in the physi-cal and social realms. The common sense deficitappears to involve a lack of intuitive attunement(impaired capacity to accurately typify the mentalstates of other persons because of the incapacity to beinvolved in their mental lives) and a damaged socialknowledge network (disorders of the background ofknowledge useful for organizing everyday experi-ences). Three dimensions of schizophrenic vulnerabil-ity can be distinguished: the sensory, conceptualiza-tion, and attitudinal dimensions. Sensory disorders areaberrations of self, body, and world perceptions.Conceptualization disorders are disturbances in theattribution of meanings and intentions. Attitudinal dis-orders consist of eccentricities in the individual'sstructure of values and beliefs, characterized by dis-trust toward conventional knowledge and attunement.This article describes the present state and possiblefuture directions of qualitative analyses and empiricalinvestigations relevant to assessing the interplaybetween vulnerability dimensions and disorders ofcommon sense.
Keywords: Common sense, attunement, relationaldeficit, schizophrenia, social knowledge, vulnerability.
Schizophrenia Bulletin, 26(4):775-787,2000.
Schizophrenia involves severe impairments in social func-tioning, typically in interpersonal relationships. Socialdysfunction is described in diagnostic manuals (AmericanPsychiatric Association 1994) as a consequence of acute
psychotic symptoms and a persistent feature in nonremit-ting psychoses. Several theoretical approaches considerimpairments of social functioning to be not just an out-come of psychotic syndromes but a fundamental phenom-enon of schizophrenic vulnerability. Vulnerability toschizophrenic psychoses seems to involve a basic rela-tional deficit (Maj 1998) that can be intuited but is diffi-cult to define reliably. Nonoperationalized but far-reach-ing concepts—such as the "schizoid-syntonic" distinction(Bleuler 1922; Kretschmer 1922; Minkowski 1927)—focus on the attitudes of people with psychosis towardtheir social environments. In this article, I will try to makethese concepts compatible with empirical testing.Schizophrenic vulnerability will be reinterpreted in rela-tion to the disconnection from common sense found inmany people with psychosis.
To describe situations characterized by detachmentfrom common sense, psychopathology adopts terms like"perplexity" in acute conditions and "autism" in chroniccases. People with or vulnerable to schizophrenia seem tobe especially prone to bracket common sense, especiallywhen compared to those with bipolar disorder (Kraus1982). They seem to lack, or sometimes to reject, com-mon sense categories that are normally used to typifyeveryday experiences. In short, people with schizophreniaare hypoconnected to common sense, while those withbipolar disorder are hyperconnected. Traditional vulnera-bility models (Zubin and Spring 1977; Nuechterlein andDawson 1984; Strauss et al. 1995) have generally ignoredthe issue of disconnectedness from common sense in peo-ple with schizophrenia. Little attention has been paid tothe common sense issue in schizotypal personality (Meehl1962; Raine et al. 1995; Claridge 1997). More attention tothe patients' attitudes toward common sense is paid byphenomenologically oriented psychopathological studieson schizophrenic vulnerability (Parnas and Bovet 1991).
Send reprint requests to Dr. G. Stanghellini, U.O. Sperimentale diPsichiatria, Dipartimento di Salute Mentale, Universita di Firenze, VialeMichelangiolo 41,1—50125 Firenze, Italy; e-mail: [email protected].
775
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

Schizophrenia Bulletin, Vol. 26, No. 4, 2000 G. Stanghellini
My thesis is that the common sense issue is crucial forunderstanding schizophrenic worlds, since the crisis ofcommon sense is probably the main root of the schizo-phrenia patient's vulnerable condition, and consequently,the origin of full-blown psychotic symptoms. The conceptof "crisis of common sense" (Blankenburg 1971) is prob-ably the most accurate way to characterize the prodromalchanges in thought process, as well as in awareness of andattitude toward both self and world, that are observed inpatients with psychosis. Persisting signs of withdrawaland positive symptoms can be interpreted as reactions todisordered emotional and cognitive attunement to theworld. The main purpose of this article is to redescribevulnerability to schizophrenic psychoses in the light of theconcept of common sense.
Vulnerability Revisited
In a revised vulnerability model, two main componentsmust be highlighted: (1) the clinical characteristics ofbasic disorders of experience that occur in the prodromalphases of schizophrenic episodes, that lead to full-blownpsychotic symptoms, and that last after remission of acutebreakdowns; and (2) the role of the patient in experienc-ing prepsychotic phenomena, coping with them, and con-stituting psychotic symptoms.
Basic Disorders of Experience. The recognition of sub-jective experience provides the basis for psychopathologi-cal research on psychoses (Schizophrenia Bulletin, 15[2],1989). Basic disorders of experience in prodromal phasesof schizophrenia have been described as depersonalizationand derealization phenomena (i.e., strange changes in selfand world awareness in which patients feel as if they, theexternal environment, or both are unreal). Huber andcoworkers and Chapman and coworkers were among thefirst who emphasized the importance of investigatingearly subjective complaints in people with schizophrenia.Table 1 summarizes their findings.
The Role of the Person in Dealing With BasicDisorders. The active role that the person with psychosiscan play in the shaping of psychotic syndromes has beenemphasized in phenomenological psychopathology(Stanghellini 1997b) and is implicit in Bleuler's (1911)distinction between primary symptoms—direct expres-sions of the schizophrenic illness process—and secondarysymptoms that result from psychoreactive coping strate-gies. Dialectic vulnerability models emphasize the activerole that patients have in interacting with their own dis-turbing experiences and suggest that this may be theprime factor in the development of psychotic symptomsand worldviews. Table 2 summarizes the main character-istics of these models.
Table 1. Basic disorders of experience
Area of StudyHuber:
basic symptomsChapman:
perceptive aberrations
Prepsychotic, subjective complaints (Huber 1966,1983)
Subjective side of schizophrenic vulnerability(Klosterkoetter 1988; Huber 1990)
Loss of control and automatism; impairments ofperception, language, thought, memory, and motricity;anhedonia and anxiety (Suellwold 1986)
Attenuated versions of schizophrenic experiences(Chapman 1966, Chapman et al. 1978)
Indicators of psychosis-proneness (Chapman etal. 1994, 1995)
Distortions in perceptions of one's body andexternal objects (Chapman et al. 1978)
Table 2. Dialectic vulnerability models
Author Disturbing experience Personal reaction
Bleuler(1911)Minkowski(1927)Wyrsch (1949)Janzarik(1959)Huber (1983)Mundt(1985)Strauss (1989)
Primary symptomsSchizophrenic evolutive factorSchizophrenic processIrruptive dynamicBasic symptomsIntentionality breakdownIllness
+ Psychological reaction+ Schizoid personality+ Person's position taking+ Stabilizing intentionality+ Psychoreactive coping+ Intentionality repair+ Coping
776
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

At Issue Schizophrenia Bulletin, Vol. 26, No. 4,2000
Two Main Shortcomings (and Possible Improvements)of the Vulnerability Paradigm. Although perceptual dis-orders and coping styles represent key features of psy-chotic vulnerability, other phenomena should be takeninto account.
The role of conceptualization disorders. The basic rela-tional deficit in psychosis involves at least two differentlevels of disturbed experience: (1) depersonalization andderealization phenomena that are mainly related to disor-ders of sensory experience, and (2) disorders of the con-ceptualization of experiences (Mundt 1991).
Whereas perceptual aberrations often involve derealiza-tion feelings (vignette 1), disorders of conceptualizationinvolve impairments of the symbolic representation of per-ceptual stimuli. In the latter, the attribution of their functionto objects, of meanings to social situations, and of motiva-tions to other persons' behaviors are disordered (vignette 2).A special category within conceptualization disorders is thedisorders of social cognition (Perm et al. 1997), that is, dis-orders of relatedness to other persons (vignette 3).
Conceptualization disorders involving impairments insocial cognition are better accounted for by theories thatfocus on interpersonal awareness, such as phenomenolog-ical theories of schizophrenic vulnerability based on con-structs of disordered intentionality (Mundt 1985) and cri-sis of common sense (Blankenburg 1971; Wiggins et al.1990; Parnas and Bovet 1991), and by cognitiveapproaches such as the theory-of-mind deficit hypothesis,which is based on the model of child autism interpreted asthe failure to attribute mental states to other people(Baron-Cohen et al. 1994). Blankenburg (1971) arguedthat the fundamental source of relationship disturbancesoccurring in people with schizophrenia is the loss of nat-
Vignettei. Derealization feelings
F.B. is a 24-year-old man whose main psychopathologi-cal feature is disorganization. Especially at the sunsethour, he complains of paniclike attacks of psychoticseverity. During these attacks, which he calls "feelingsof vagueness," he sees colors more brightly and hearssounds more acutely than usual, and he undergoesexperiences of self and body transformation. He isaware that these are pathological experiences and can-not find any suitable explanation for them. He also seesother people as strange and unfamiliar. These experi-ences of derealization and depersonalization are some-what "naked" and not otherwise conceptualized.Although these phenomena of world and self transfor-mation are often accompanied by experiences of refer-ence, only sometimes do they become truly delusional,that is, changes in the outside world or in the facialexpressions of people are usually not interpretedaccording to a paranoid attributional style.
Vignette 2. Disordered attribution
C.D.B. is a 27-year-old insightful man with schizophre-nia. He says that nothing is obvious to him; everythingcan be uncanny. The world is complicated, difficult tounderstand: "Why does this happen? What does thatmean? How to explain these facts? Why?" Facts arenot self-evident. Only explanations can give a shape tohis experiences. He feels the need for a general theorythat makes the world understandable and his actionspossible. Each theory he builds up is short-lived; itneeds to be tested every time a new fact happens. Hedoes not experience sensory disorders but experiencessevere disorders of the conceptualization of reality.
Vignette 3. Impairment in social cognition
P.S. is a 42-year-old man who has been affected byparanoid schizophrenia since the age of 20. At theonset of his psychosis, he was trying in various ways tocompensate for his difficulties in getting in touch withother people. He had no secure ground to interpret theothers' intentions. He lacked the structure of the rulesof social life and systematically set about searching fora well-grounded and natural style of behavior. Forinstance, he was busy with an ethological study of the"biological" (i.e., not artificial) foundation of others'behaviors through a double observation of animal andhuman habits. The former was done through televisiondocumentaries, the latter via analyses of human inter-actions in public parks. An atrophy in his knowledge ofthe "rules of the game" led him to engage in intellectualinvestigations and to establish his own "know-how" forsocial interactions in a reflective way.
ural evidence of commonsensical everyday reality. This isthe core of schizophrenic vulnerability. People with schiz-ophrenia seem no longer able to typify their experiencesalong common sense categories; the at-homeness thataccompanies most of us in our everyday life is not there.
The role of eccentricity. A second shortcoming ofthe vulnerability paradigm is that the role of the personwith psychosis in the constitution of the syndrome ismainly conceived as involving coping strategies to try tocompensate for feelings of derealization and strangeness.This underestimates the individual's attitude toward ordi-nary perception and common sense categorizations of theworld. Persons vulnerable to schizophrenic psychosesmay hold opinions and convictions that are critical ofcommon sense conventions, and for this reason these peo-ple may attempt deliberately to situate themselves outsidethe constraints of shared beliefs and values. This is anactive self-positioning outside of commonsensical reality,not a passive or merely reactive response to experiencesof derealization and depersonalization.
777
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

Schizophrenia Bulletin, Vol. 26, No. 4, 2000 G. Stanghellini
Traditional vulnerability models stress derealizationand depersonalization as prime causes of overt symptomsand psychotic breakdowns, and they neglect eccentricity,i.e., active positioning at the margins of socially sharedworldviews (vignette 4) and the refusal of social norms(vignette 5). The structure of values and beliefs of the per-son who is vulnerable to schizophrenia is also of centralimportance. But whether it is a passive experience ofdeprivation of one's normal anchoring in the world (i.e.,disorders of perception and conceptualization) or anactive rejection of taken-for-granted assumptions aboutthe world itself (i.e., eccentricity), the crucial elementinvolves distortions in the experience of common sense.
Vignette 4. Active self-marginalization
V.V. is a 22-year-old university student of the humani-ties. She plans to get rid of what she herself calls "het-eronomia" (i.e., depending on the rules established byothers). She has recently started a course on Sumerianlanguage: "Since this was the first written language, Ithink that in it are expressed parts of the mind that wereworking by that age and are silent at present."Exploring parts of the human mind that were activeonce, and are no longer active now, could help her findthat original and eccentric view on the human conditionthat she is looking for. Her personal fight against therules established by others results in solitude and ahighly intellectualized style of living.
Vignette 5. Hyperawareness
E.B. is a 30-year-old man who says of himself "I am aparanoid schizophrenic. That's science's verdict. So let itbe." He is very religious and shows esoteric and meta-physical interests. During one hospitalization, he wasoften perplexed and found it very difficult to relate to otherpeople and in general to the external world. Almost everytime he perceived an object, the perception evoked inhim one concept or word, and that word was kindling anoverwhelming trend of word associations. It was like a'Hood of words" that made him lose his grasp on theactual situation. Therefore he could not engage in themost simple activities and participate in conversations.He explains that in the beginning it was a way "to exer-cise memory through perception. A way to enhance mymind. I was looking at one thing and I hadto put mystrength in order to evoke another thing, and so on. I wasfixed on potentiating my brain. It all started as a voluntaryaction that later turned into a passive experience."
What Is Common Sense?"Common sense" is not an easy concept to define. The18th-century Italian philosopher G.B. Vico (1744, Degnita12) gave the following sweeping definition: "It is a judge-
ment without any reflection, commonly felt by a wholeorder, a whole people, a whole nation or the whole humankind." The 18th-century Scottish philosopher T. Reid(Reid 1997) postulated that the human mind could harmo-nize with common sense because of an innate "instinct."In contrast to Vico's and Reid's praise for common sense,modem scientists and philosophers, with few but signifi-cant exceptions, more often have a critical attitude towardit (Koir6 1965). The major contributions to a positive"philosophy of common sense" are given by E. Husserl(1970) and his followers, and by L. Wittgenstein (1969),who affirmed that common sense is a set of rules of thegame that discipline human behaviors.
Common Sense as a Tool for Adaptation. Commonsense is a kind of understanding whose purpose is not the-oretical (knowing about something) but practical (doingsomething). It has its roots in evolution, and its purpose isan adaptive one, since it provides an image of reality builtup for the pragmatic aim of survival and adaptation(Horton 1982). Locke (1688) emphasized that commonsense consists of a set of empirical cause-and-effect rela-tionships useful for practical orientation in everydayactions. Modern psychologists argue that the fundamentalfeature of human thinking is its need to understand thecauses and motivations of behavior and everyday events(Heider 1958). Evolutionary psychologists state that "ourliteral survival depends upon a finely tuned knowledge ofthe causal texture of the world" (Plotkin 1997, p. 185).
Common Sense and Intersubjectivity. Not only theadjustment to and survival of individuals in their immedi-ate environments, but also the integrity of a whole societydepend on the possession of this "primary theory" of theworld that we call common sense. Common sense hasadaptive significance for both the natural environment andculture. It is mainly the latter aspect, (i.e., social adapta-tion based on an adequate degree of connectedness tocommon sense) that is of relevance in psychopathology.Social scientists and philosophers highlight the intersub-jective character of common sense and its implications formutual understanding (Schutz 1962). The main character-istic of common sense is its self-evidence for all membersof a given community—it comprises all that the membersof a given society are disposed to take as obvious andunproblematic (Husserl 1970).
The Social Imprinting of Common Sense. Our knowl-edge of the world we live in derives only in part from ourfirsthand experience; to a much greater extent, it issocially derived—handed down by reports and teachingsof others (Schutz 1962). The common sense world is anold inheritance. We learn it as children who faithfully
778
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

At Issue Schizophrenia Bulletin, Vol. 26, No. 4, 2000
accept the teachings of adults at a stage of psychologicalgrowth that is prior to doubts and uncertainties. In short:we are imprinted with it.
Preservation of Common Sense. The common senseworld enjoys relative stability and consistency amongindividuals who belong to the same group. The remark-able stability of common sense is due to the tendency toassimilate the unusual into the usual. As a rule, experi-ences that fit common sense typifications are felt as morereal than those that are idiosyncratic. If an experiencedoes not fit common sense schemata, it is usually not theschemata that are called into question; rather, the newcharacter of the experience is ruled out and normalized.
What Is Common Sense About? Two main categories offacts are dealt with by common sense—physical statesand psychological ones. Common sense represents aguideline for orientation in both realms. The 18th-centuryScottish philosopher D. Hume (1739-1740) held that thehuman mind's main purpose was to detect cause-and-effect relationships. Modern psychology seems to confirmHume's theory (Sperber et al. 1995) in arguing that every-one is a natural physicist and a natural psychologist(Plotkin 1997). While physical causation deals with therelationships between material objects (e.g., "If I touchfire, then my hand will burn"), psychological causation isconcerned with interpretation of others' mental statesthrough the attunement with and observation of others'behaviors (actions, facial expressions, etc.; e.g., "If shesmiles, she is happy"). This property of detecting theintentions and motivations behind somebody's behaviorsis called "mind reading" (Baron-Cohen et al. 1994).Social cognition (Perm et al. 1997) is especially relevantto the issue of psychotic vulnerability, since disorders ofthe capacity to attribute meanings to social situations are 'involved in psychotic syndromes. Children with autismseem to have an incapacity to make sense of others'behaviors (Baron-Cohen et al. 1994). In people withschizophrenia, the ability to attribute mental states is alsoimpaired (Frith 1992) and delusions can be seen as theeffect of the "exclusion of casualness" (Berner 1982).
Common Sense as Social Knowledge. One may askwhether common sense is a set of "commonplaces"involving particular beliefs or whether it is more ade-quately represented as a "sense" useful for attuning withwhat is "common." Is common sense a network of knowl-edge relevant to ordinary life situations shared by themembers of a given society? Or is it more of a psychicfunction aimed at understanding current social situationsand at harmonizing with them? Or both? The construct ofcommon sense has two aspects. The first aspect can be
conceptualized as a stock of knowledge useful at the levelof everyday life. Common sense is a set of rules of infer-ence that is the medium for organizing the everyday expe-riences of individuals and social groups (Flick 1998). It isthe foundation of people's expectations and of meaningattributions (Moscovici and Hewstone 1983). This processof inference is mainly automatic in nature—motivationsand meanings are attributed prereflectively.
Common Sense as Intuitive Attunement. Phenome-nological definitions (Merleau-Ponty 1945; Husserl 1970)emphasize the second aspect of common sense: theimportance of preconceptual perceptive attunementbetween the subject and the outer world that is rooted inintuition, corporeality, and the affective or emotional life.Bovet and Parnas (1993, p. 583) write, "Common sensereflects our preconceptual attunement to the world. Itreveals not so much what is evident but how it is evident,the constantly present and tacit frame of experience . . . .The defect in common sense can manifest itself in . . . alack of the sense for the 'rules of the game' of humanbehavior." However, the concept of attunement is rathervague. What sort of psychological process is involved?What is it that a person is (or is not) attuned with?
In everyday experience, we feel familiarly related tothe environment and to current social situations. At a per-ceptual level, objects in the world and persons appearfamiliar (i.e., as we expect them to be according to ourpast experience). In social situations, the movements,expressions, and utterances of others also appear typicaland understandable. There is a break with ordinary experi-ence when objects or persons disagree perceptually withexpectancies (e.g., when colors are too bright or detailsmagnified—perceptive aberrations). But one can alsohave this feeling of strangeness without any change on theperceptual level, that is, when the meanings of objects inthe world (e.g., "What is this chair for?") and of theactions of others (e.g., "Why is he laughing?") appearuncanny. The attunement concept refers mainly to thissecond level of experience, which involves the intuitiveattribution of meanings to objects and situations, and ofintentions to other people. Phenomenological research inpsychopathology has been mainly concerned with whatthe philosopher J.R. Searle (1995) calls "social reality,"whose main components may be considered "mentalfacts" and "social facts," as opposed to brute physicalfacts (e.g., "There is snow on Mt. Everest"). The conceptof intuitive attunement—reshaped within the frameworkof the theory-of-mind (Baron-Cohen et al. 1994)—mayhelp to explain some aspects of the phenomena that hap-pen in the social space and involve social cognition inattributing mental states to partners. Social attunementinvolves the ability to intuit (from Latin intuire, intus +
779
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

Schizophrenia Bulletin, Vol. 26, No. 4, 2000 G. Stanghellini
ire, "to go inside") what is going on in somebody else'smind. I can attune with a given social situation when I amable to comprehend thoughts and feelings of others byobserving their behavior and to explain others' behaviorin terms of intentional (e.g., "He is looking for anaspirin") or nonintentional (e.g., "He has a headache")mental facts. Social cognition is based on a fundamentalfeature of the human mind, the urge to establish motiva-tional relationships, and understanding other minds proba-bly depends on coordinating one's own movement andfacial expressions with those of others—a capacityalready present in newborn babies (Butterworth 1999).
Schizophrenic Vulnerability as a Disorderof Common Sense Typification
Studies on premorbid adjustment of people with schizo-phrenia (Malmberg et al. 1998) and high-risk studies(Dworkin et al. 1993; Dworkin et al. 1994; Olin et al.1998; Hodges et al. 1999) demonstrate that early prob-lems in interpersonal relationships are strongly associatedwith schizophrenia. Boys who will develop schizophre-nia show disruptive behaviors and social anxiety, andthey suffer from rejection by peers; girls are often ner-vous and withdrawn. Severe impairments in social com-petence such as social isolation, sensitivity, odd behavior,and odd speech are common features in people withschizotypal personality (Kendler et al. 1989). A basicrelational deficit is supposed to be a core phenomenon ofthe schizophrenic condition (Maj 1998). In this section,the global deficit involved in schizophrenic vulnerabilitywill be conceptualized as a disconnection from commonsense. Two main areas of this construct are at issue: com-mon sense as social knowledge, and common sense asintuitive attunement. Since the concept of "typification"(Schutz 1962) includes both these aspects, I will adoptthis term to designate that feature of human thinkingthrough which we make sense of the world by attributingmeanings, causes, and intentions to objects, situations,and other persons. In the case of schizophrenic vulnera-bility, we may speak of hypotypification. Deficits of com-mon sense typification can be described as a deficit in theknowledge of commonsensical beliefs or rules—what canbe termed the damaged social knowledge networkhypothesis. It is also possible that abnormalities in com-mon sense typification are a consequence of an individ-ual's distrust toward social knowledge and criticismtoward its conventionality. Deficits in common sense typ-ification can also be interpreted as consequences of a lackof intuitive attunement, or alternatively as an attitude ofdistrust toward intuition (and an emphasis on rationality,for instance).
These different dimensions of schizophrenic vulnera-bility can be outlined as follows:
1. Sensory-level disorders (perception of self, body,and world)
2. Conceptualization-level disorders (attribution ofmeaning and intention)2.1 Damaged social knowledge network
2.1.1 Atrophy of social knowledge network2.1.2 Hypertrophy of social knowledge
network2.2 Lack of intuitive attunement
3. Attitudinal-level disorders (eccentric structure ofvalues and beliefs): distrust toward conventionalknowledge and intuitiveness3.1 Skepticism3.2 Hypertolerance of ambiguity
Sensory-Level Disorders. Sensory-level disorders areaberrations in the perception of self, body, and world.Strictly speaking, these are not disorders of commonsense. I mention this category of disorders, however,because they are involved in the pathogenesis of schizo-phrenic psychoses and are presumably related to the dis-orders of conceptualization of reality. These disorders ofsubjective experience occur very early in the course ofschizophrenia (Huber 1983) and are relevant for thedevelopment of full-blown psychoses (Chapman et al.1978; Klosterkoetter 1988).
Conceptualization-Level DisordersDamaged social knowledge network. Conceptual-
ization disorders involve impairments in the attribution ofmeanings and intentions that can be related either to anatrophy or to a hypertrophy of the background of knowl-
. edge useful for typifying everyday experiences.Atrophy. In the case of atrophy, there is a lack of
available knowledge of socially shared categories to typ-ify the actions of both others and oneself. People withschizophrenia, relative to those with neuroses or bipolardisorder (Cutting and Murphy 1988, 1990) are markedlydeficient in "real-world knowledge"—the majority of peo-ple with schizophrenia seem to have deficient knowledgeconcerning events and behaviors in the world aroundthem. Those with hebephrenia especially are impaired intheir knowledge of how other people might behave in acertain situation (see also vignette 3). According to thesefindings, Cutting and Murphy argue that incompetentsocial judgment is an intrinsic feature of schizophrenia(especially of hebephrenia) and not a consequence ofenvironmental factors or actual illness. These findingsconfirm classic phenomenological hypotheses about thepathogenetical role of lack of common sense in schizo-
780
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022
At Issue Schizophrenia Bulletin, Vol. 26, No. 4, 2000
phrenia, in which the pragmatic use of things is affected(Minkowski 1927).
Hypertrophy. Disorders of conceptualization can alsobe due to a hypertrophied background of knowledge-at-hand. The phenomenon of "automatic consciousness"experienced by E.B. (vignette 5) is a well-known andfundamental feature of psychotic thinking. Complexassociations are passively triggered by a single word orperceptual detail. This stream of consciousness generatesthe emergence of meanings that would usually remainimplicit in normal experience. The emergence of theexplicit from the implicit is responsible for an "expansionof the horizon of meanings" (Schwartz et al. 1997, p.178). An enlarged horizon of meanings may reflect ahypertrophied network of knowledge-at-hand and a lackof inhibition in the associations between semanticallyrelated concepts. The phenomenon of automatic con-sciousness shows that disentanglement from commonsense can occur not only through a defective state (atro-phy of social knowledge network), but also vice-versavia a positive condition. Indeed, these free-associationvariations may lead to a condition of hyper awareness inwhich all possible meanings linked to a given situationemerge. A hyperextended network of semantic associa-tion stored in the data base is actualized by a single expe-rience. Relevant meanings are no longer selected fromthe set of all possible meanings. There is a failure of apurpose-at-hand device that can no longer select justthose meanings that are relevant to a given situation.These abnormalities in the conceptualization of experi-ence are studied according to the experimental paradigmsof cortical maps and semantic priming (Evans 1997;Schwartz et al. 1997), which generate hypotheses of neu-robiological relationships that can be empirically tested(Spitzer et al. 1993).
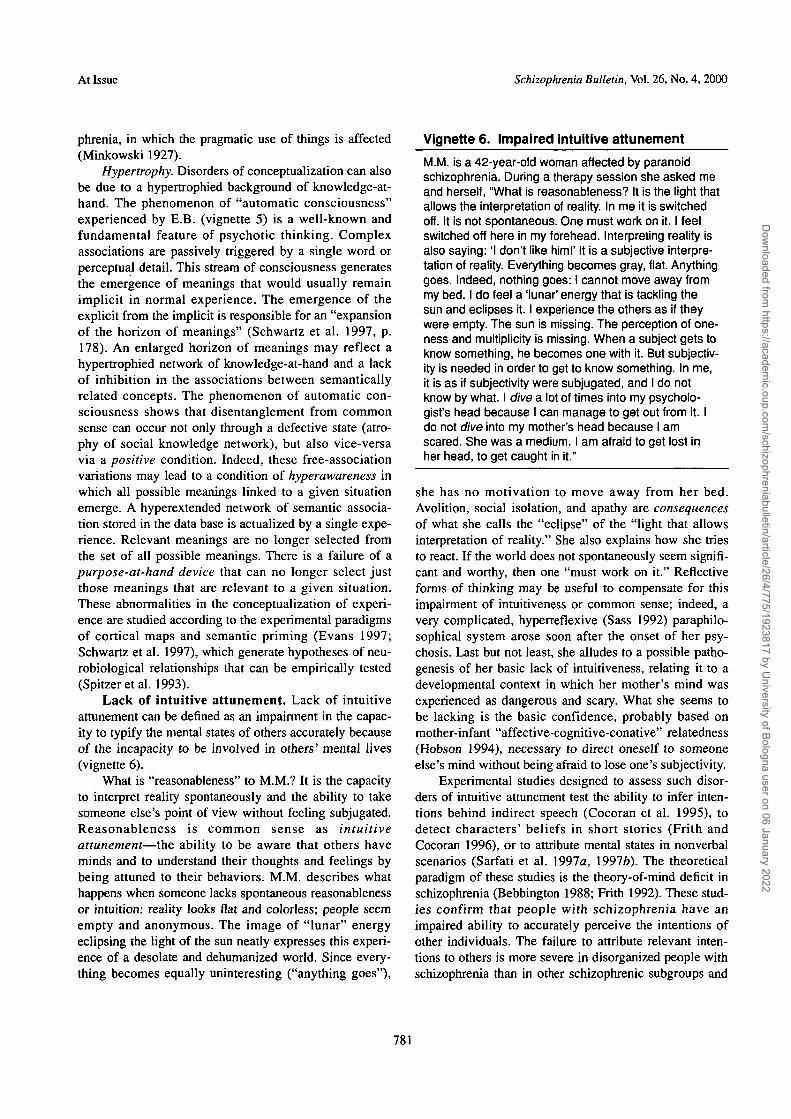
Lack of intuitive attunement. Lack of intuitiveattunement can be defined as an impairment in the capac-ity to typify the mental states of others accurately becauseof the incapacity to be involved in others' mental lives(vignette 6).
What is "reasonableness" to M.M.? It is the capacityto interpret reality spontaneously and the ability to takesomeone else's point of view without feeling subjugated.Reasonableness is common sense as intuitiveattunement—the ability to be aware that others haveminds and to understand their thoughts and feelings bybeing attuned to their behaviors. M.M. describes whathappens when someone lacks spontaneous reasonablenessor intuition: reality looks flat and colorless; people seemempty and anonymous. The image of "lunar" energyeclipsing the light of the sun neatly expresses this experi-ence of a desolate and dehumanized world. Since every-thing becomes equally uninteresting ("anything goes"),
Vignette 6. Impaired intuitive attunement
M.M. is a 42-year-old woman affected by paranoidschizophrenia. During a therapy session she asked meand herself, "What is reasonableness? It is the light thatallows the interpretation of reality. In me it is switchedoff. It is not spontaneous. One must work on it. I feelswitched off here in my forehead. Interpreting reality isalso saying: 'I don't like him!' It is a subjective interpre-tation of reality. Everything becomes gray, flat. Anythinggoes. Indeed, nothing goes: I cannot move away frommy bed. I do feel a 'lunar' energy that is tackling thesun and eclipses it. I experience the others as if theywere empty. The sun is missing. The perception of one-ness and multiplicity is missing. When a subject gets toknow something, he becomes one with it. But subjectiv-ity is needed in order to get to know something. In me,it is as if subjectivity were subjugated, and I do notknow by what. I dive a lot of times into my psycholo-gist's head because I can manage to get out from it. Ido not dive into my mother's head because I amscared. She was a medium. I am afraid to get lost inher head, to get caught in it."
she has no motivation to move away from her bed.Avolition, social isolation, and apathy are consequencesof what she calls the "eclipse" of the "light that allowsinterpretation of reality." She also explains how she triesto react. If the world does not spontaneously seem signifi-cant and worthy, then one "must work on it." Reflectiveforms of thinking may be useful to compensate for thisimpairment of intuitiveness or common sense; indeed, avery complicated, hyperreflexive (Sass 1992) paraphilo-sophical system arose soon after the onset of her psy-chosis. Last but not least, she alludes to a possible patho-genesis of her basic lack of intuitiveness, relating it to adevelopmental context in which her mother's mind wasexperienced as dangerous and scary. What she seems tobe lacking is the basic confidence, probably based onmother-infant "affective-cognitive-conative" relatedness(Hobson 1994), necessary to direct oneself to someoneelse's mind without being afraid to lose one's subjectivity.
Experimental studies designed to assess such disor-ders of intuitive attunement test the ability to infer inten-tions behind indirect speech (Cocoran et al. 1995), todetect characters' beliefs in short stories (Frith andCocoran 1996), or to attribute mental states in nonverbalscenarios (Sarfati et al. 1997a, 19976). The theoreticalparadigm of these studies is the theory-of-mind deficit inschizophrenia (Bebbington 1988; Frith 1992). These stud-ies confirm that people with schizophrenia have animpaired ability to accurately perceive the intentions ofother individuals. The failure to attribute relevant inten-tions to others is more severe in disorganized people withschizophrenia than in other schizophrenic subgroups and
781
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022
Schizophrenia Bulletin, Vol. 26, No. 4, 2000 G. Stanghellini
normal controls (Sarfati et al. 1997a, 1997b). Thought,language, and communication disorders are especiallyhighly correlated with this inability. People with schizo-phrenia who fail to appreciate other people's mental statesdo not seem to rely on what is specifically relevant to thecontext, but on two competing strategies of decoding:either they choose the prevailing meaning of an ambigu-ous stimulus (e.g., a word), thus relying on their back-ground knowledge (Swiney 1984), or else they showfacilitation for word recognition by semantic categoriza-tion (Koh and Peterson 1978; Traupman 1980).
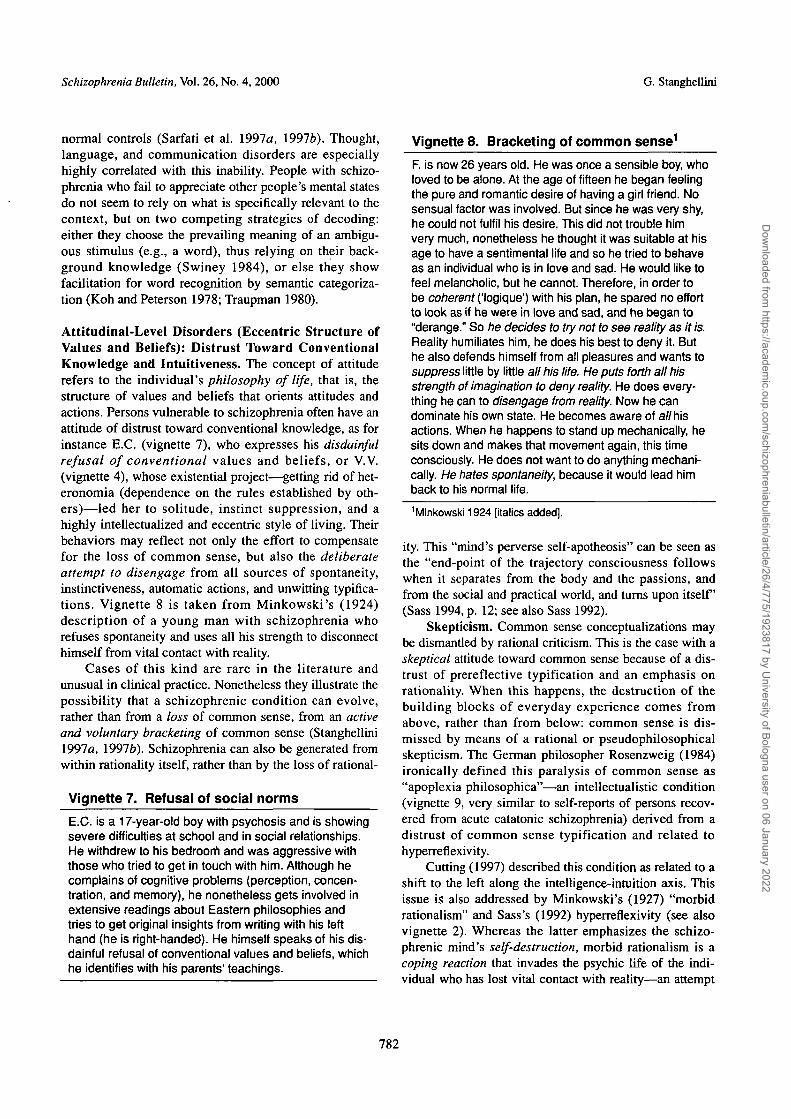
Attitudinal-Level Disorders (Eccentric Structure ofValues and Beliefs): Distrust Toward ConventionalKnowledge and Intuitiveness. The concept of attituderefers to the individual's philosophy of life, that is, thestructure of values and beliefs that orients attitudes andactions. Persons vulnerable to schizophrenia often have anattitude of distrust toward conventional knowledge, as forinstance E.C. (vignette 7), who expresses his disdainfulrefusal of conventional values and beliefs, or V.V.(vignette 4), whose existential project—getting rid of het-eronomia (dependence on the rules established by oth-ers)—led her to solitude, instinct suppression, and ahighly intellectualized and eccentric style of living. Theirbehaviors may reflect not only the effort to compensatefor the loss of common sense, but also the deliberateattempt to disengage from all sources of spontaneity,instinctiveness, automatic actions, and unwitting typifica-tions. Vignette 8 is taken from Minkowski's (1924)description of a young man with schizophrenia whorefuses spontaneity and uses all his strength to disconnecthimself from vital contact with reality.
Cases of this kind are rare in the literature andunusual in clinical practice. Nonetheless they illustrate thepossibility that a schizophrenic condition can evolve,rather than from a loss of common sense, from an active
and voluntary bracketing of common sense (Stanghellini1997a, 19976). Schizophrenia can also be generated fromwithin rationality itself, rather than by the loss of rational-
Vignette 7. Refusal of social normsE.C. is a 17-year-old boy with psychosis and is showingsevere difficulties at school and in social relationships.He withdrew to his bedroom and was aggressive withthose who tried to get in touch with him. Although hecomplains of cognitive problems (perception, concen-tration, and memory), he nonetheless gets involved inextensive readings about Eastern philosophies andtries to get original insights from writing with his lefthand (he is right-handed). He himself speaks of his dis-dainful refusal of conventional values and beliefs, whichhe identifies with his parents' teachings.
Vignette 8. Bracketing of common sense1
F. is now 26 years old. He was once a sensible boy, wholoved to be alone. At the age of fifteen he began feelingthe pure and romantic desire of having a girl friend. Nosensual factor was involved. But since he was very shy,he could not fulfil his desire. This did not trouble himvery much, nonetheless he thought it was suitable at hisage to have a sentimental life and so he tried to behaveas an individual who is in love and sad. He would like tofeel melancholic, but he cannot. Therefore, in order tobe coherent ('logique') with his plan, he spared no effortto look as if he were in love and sad, and he began to"derange." So he decides to try not to see reality as it is.Reality humiliates him, he does his best to deny it. Buthe also defends himself from all pleasures and wants tosuppress little by little all his life. He puts forth all hisstrength of imagination to deny reality. He does every-thing he can to disengage from reality. Now he candominate his own state. He becomes aware of all hisactions. When he happens to stand up mechanically, hesits down and makes that movement again, this timeconsciously. He does not want to do anything mechani-cally. He hates spontaneity, because it would lead himback to his normal life.
1Minkowski 1924 [italics added].
ity. This "mind's perverse self-apotheosis" can be seen asthe "end-point of the trajectory consciousness followswhen it separates from the body and the passions, andfrom the social and practical world, and turns upon itself(Sass 1994, p. 12; see also Sass 1992).
Skepticism. Common sense conceptualizations maybe dismantled by rational criticism. This is the case with askeptical attitude toward common sense because of a dis-trust of prereflective typification and an emphasis onrationality. When this happens, the destruction of thebuilding blocks of everyday experience comes fromabove, rather than from below: common sense is dis-missed by means of a rational or pseudophilosophicalskepticism. The German philosopher Rosenzweig (1984)ironically defined this paralysis of common sense as"apoplexia philosophica"—an intellectualistic condition(vignette 9, very similar to self-reports of persons recov-ered from acute catatonic schizophrenia) derived from adistrust of common sense typification and related tohyperreflexivity.
Cutting (1997) described this condition as related to ashift to the left along the intelligence-intuition axis. Thisissue is also addressed by Minkowski's (1927) "morbidrationalism" and Sass's (1992) hyperreflexivity (see alsovignette 2). Whereas the latter emphasizes the schizo-phrenic mind's self-destruction, morbid rationalism is acoping reaction that invades the psychic life of the indi-vidual who has lost vital contact with reality—an attempt
782
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

At Issue Schizophrenia Bulletin, Vol. 26, No. 4, 2000
Vignette 9. Apoplexia philosophies1
"We moved to the patient's bedside. The patient had toconfine himself to his bed; he was no longer able toperform any of the essential daily actions. He felt para-lyzed. The rigidity of his stupor had taken control overhim. His hands could no longer grasp, for who was itthat gave them the right to take things? His feet couldno longer walk, for who could ensure ground for theirsteps? His eyes could no longer look, for who couldprove to him that no dream was fooling them? Thesame was true for his ears that could no longer listen,for was it really worthwhile to pull something out of thevoid?"1 Rosenzweig 1984.
to re-establish new rules for typification when life can nolonger be lived but only thought of (Minkowski 1947).Both pathways, active bracketing and passive loss ofcommon sense, would seem to be possible.
Hypertolerance of ambiguity. Hypotypification,whose source can be traced back to the vulnerable individ-ual's set of values and beliefs, can also originate from ahypertolerance of ambiguity (Frenkel-Brunswik 1949). Asin the case of skepticism, this can also be a deliberate epis-temological attitude, related to a concern for the complex-ity of reality, to a realization that facts-in-the-world, withtheir infinite profiles, cannot be caught by a single concep-tualization or reduced to a unidimensional form of under-standing. Such an attitude of intolerance toward therestricted horizon of common sense typifications is alsopartly reflected in the case of the patient E.B. (vignette 5),who does all he can to enhance his mind's capacity tounderstand. He uses all his power to connect the percep-tion of the meaning of one object with a trend of associ-ated meanings. An enlarged horizon of meanings may notsimply reflect an automatic train of more or less relevantassociations. It may also reflect a deliberate attempt toenlarge one's own mental capacity for conceptualization.The philosophical paragon of this attitude is the "art ofmemory," a mental exercise to improve memory throughthe activation of fluid semantic associations (Yates 1966;Rossi 1983). The art of memory is also an esoterichermeneutic instrument to break through the innermostsecrets of nature. In fact, E.B.'s mnemonics evolve towardovert psychopathology in two ways. There is a shift fromactivity to passivity: he begins with a voluntary attempt toenlarge his mental capacities and ends up by being discon-nected from common sense typifications. There is a secondshift from using the art of memory as a mnemonic deviceto using it as a tool to interpret the complex symbolism ofreality. In short, a skeptical attitude toward common sensetypifications can generate a metaphysical move (asking forthe proper meaning of something), leading to hyperreflex-
ivity and the tendency to reify abstractions. It is also possi-ble for an attitude based on the hypertolerance of ambigu-ity to generate the refusal of conventional common sensetypifications that do not reflect enough of the complexityof reality and to promote the search for idiosyncratic andesoteric cues to interpret reality itself.
Conclusions
The basic assumption of this article is that the relationaldeficit observed in patients with schizophrenia is not aconsequence of acute symptoms or a social or institutionalartifact but a fundamental aspect of schizophrenic vulner-ability. Phenomenological psychopathology has attemptedto describe this basic relational deficit as disconnected-ness from common sense. The first aim of this study wasto gather philosophical cues and empirical evidence(mainly from developmental psychology) to stipulate adefinition of common sense. In my view, common senseis a tool for adaptation that is generally shared by themembers of a given community, derived from a process ofsocial imprinting, and preserved by assimilation of theunusual into the usual. Its main purpose is the discerningof cause-and-effect relationships in the physical realm andmotivational ones in the social world. The latter are espe-cially relevant in psychopathology. There is considerableempirical evidence that the schizophrenic condition ischaracterized by loss of common sense of two kinds: lackof intuitive attunement (i.e., impairment in the capacity toaccurately typify the mental states of others because of anincapacity to be involved in their mental lives) and a dam-aged network of social knowledge (i.e., of the backgroundknowledge useful for organizing everyday experiences).In the proposed model of schizophrenic vulnerability, Idistinguish three dimensions: sensory disorders, conceptu-alization disorders, and attitudinal disorders. Althoughsensory disorders (aberrations of self, body, and worldperceptions) are not common sense disorders in a strictsense, they are tightly interconnected with common-sensedisorders. Conceptualization disorders (disturbances inthe attribution of meanings and intentions) are relatedeither to a damaged social knowledge network or to a lackof intuitiveness. Conceptualization disorders includesocial knowledge network disorders and disorders of intu-itive attunement. Social knowledge network disorders caninvolve either atrophy of the social knowledge data baseor a kind of hypertrophy because of a hyperextended net-work of semantic associations between the conceptsstored in the data base. Both atrophy and hypertrophy leadto deficits in social functioning. Disorders of intuitiveattunement are manifest as a defective ability to attributemental states in short stories or nonverbal scenarios. Thisapproach to disorders of intuitive attunement relies on the
783
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

Schizophrenia Bulletin, Vol. 26, No. 4, 2000 G. Stanghellini
theory-of-mind deficit paradigm. Attitudinal disorders(eccentric structures of values and beliefs) are character-ized by distrust toward common sense (i.e., conventionalknowledge and intuitiveness). They include a skepticalattitude toward common sense and a hypertolerance ofambiguity, reflecting a refusal to conceptualize the worldthrough the simplifying views given by common sense.
Further empirical investigations are needed to verifythe basic hypothesis that disorders of common sense areprimary phenomena of schizophrenic vulnerability and notside effects of schizophrenic symptoms and course. Thiscould be done in longitudinal studies, especially with high-risk subjects, by assessing conceptualization disordersbefore the onset of overt schizophrenic symptoms and bylooking for their possible correlation with disorders ofsocial competence in people who subsequently developschizophrenia. The relationship between attitudinal-leveldisorders and social competence should also be investi-gated in high-risk subjects before the onset of psychoticsymptoms. Interview-based research instruments should bedeveloped to assess the patterns of values and beliefs ofpeople at risk for schizophrenia in order to test the hypoth-esis that, in some cases, an eccentric attitudinal orientationcan be involved in the pathogenesis of the schizophrenicrelational deficit. Also, the interplay between the three dif-ferent dimensions of schizophrenic vulnerability needsmore investigation. It is still unclear how the differentcomponents of each dimension interact with each other(i.e., how disorders of the social knowledge data base andof intuitiveness are related to each other). It is also unclearhow different dimensions affect each other (i.e., how a dis-order in one dimension can affect a nondisordered one, orhow a nondisordered dimension may prevent a schizo-phrenic breakdown when other dimensions are affected).In the model I propose, the three dimensions are relativelyindependent of each other, that is, one can be disorderedindependently from the other two (vignettes 1 and 2). Butit can also happen that a disorder in one dimension mayaffect another (vignette 5). It is tempting to hypothesizethat at least two dimensions must be affected to imply aschizophrenic syndrome in the full clinical sense.
References
American Psychiatric Association. DSM—IV: Diagnosticand Statistical Manual of Mental Disorders. 4th ed.Washington, DC: APA, 1994.
Baron-Cohen, S.; Tager-Flushberg, H.; and Cohen, D.J.Understanding Other Minds: Perspectives from Autism.Oxford, U.K.: Oxford Medical Publications, 1994.
Bebbington, P., ed. Social Psychiatry: Theory, Methodology,and Practice. New Brunswick, NJ: Transactions, 1988.
Berner, P. Psychiatrische Systematik. Bern-Stuttgart-Wien, Germany: Huber, 1982.
Blankenburg, W. Der Verlust der natuerlichenSelbstvertaendlichkeit: Ein Beitrag zur PsychopathologieSymptomarmer Schizophrenien. Stuttgart, Germany:Enke, 1971.
Bleuler, E. Dementia praecox oder Gruppe derSchizophrenien. Leipzig, Germany: Deutike, 1911.
Bleuler, E. Die Probleme der Schizoidie und der Syntonie.Zeitschrift fuer die Gesamte Neurologie und Psychiatrie,78:373-399, 1922.
Bovet, P., and Parnas, J. Schizophrenic delusions: A phe-nomenological approach. Schizophrenia Bulletin,19(3):579-597,1993.
Butterworth, G. A developmental-ecological perspectiveon Strawson's "The Self." In: Gallagher, S., and Shear, J.,eds. Models of the Self. Thorverton, U.K.: ImprintAcademic, 1999. pp. 203-211.
Chapman, J. The early symptoms of schizophrenia.British Journal of Psychiatry, 121:225-263, 1966.
Chapman, L.J.; Chapman, J.P.; and Kwapil, T.R. Scales forthe measurement of schizotypy. In: Raine, A.; Lencz, T; andMednick, S.A., eds. Schizotypal Personality. Cambridge,NY: Cambridge University Press, 1995. pp. 79-106.
Chapman, L.J.; Chapman, J.P.; Kwapil, T.R.; Eckbald,M; and Zinser, M.C. Putatively psychosis prone subjectsten years later. Journal of Abnormal Psychology,103:171-183,1994.
Chapman, L.J.; Chapman, J.P.; and Raulin, M.L. Bodyimage aberrations in schizophrenia. Journal of AbnormalPsychology, 87:339-347, 1978.
Claridge, G., ed. Schizotypy: Implications for Illness andHealth. Oxford, U.K.: Oxford University Press, 1997.
Cocoran, R.; Mercer, G.; and Frith, CD. Schizophrenia,symptomatology and social inference: Investigating the"theory of mind" in people with schizophrenia.Schizophrenia Research, 17:5-13, 1995.
Cutting, J. Principles of Psychopathology: Two Worlds—Two Minds—Two Hemispheres. Oxford, U.K.: OxfordUniversity Press, 1997.
Cutting, J., and Murphy, D. Schizophrenic thought disor-der: A psychological and organic interpretation. BritishJournal of Psychiatry, 152:310-319, 1988.
Cutting, J., and Murphy, D. Impaired ability of schizo-phrenics, relative to manics or depressives, to appreciatesocial knowledge about their culture. British Journal ofPsychiatry, 157:355-358, 1990.
Dworkin, R.H.; Cornblatt, B.A.; Friedman, R.;Kaplansky, L.M.; Lewis, S.A.; Rinaldi, A.; Shilliday, C ;
784
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022
At Issue Schizophrenia Bulletin, Vol. 26, No. 4, 2000
and Erlenmeyer-Kimling, L. Childhood precursors of affec-tive vs. social deficits in adolescents at risk for schizophre-nia. Schizophrenia Bulletin, 19(3):563-577,1993.
Dworkin, R.H.; Lewis, J.A.; Cornblatt, B.A.; andErlenmeyer-Kimling, L. Social competence deficits in ado-lescents at risk of schizophrenia. Journal of Nervous andMental Disease, 182:103-108,1994.
Evans, J.L. Semantic activation and preconscious process-ing in schizophrenia and schizotypy. In: Claridge, G., ed.Schizotypy: Implications for Illness and Health. Oxford,U.K.: Oxford University Press, 1997. pp. 80-97.
Flick, U. Everyday knowledge in social psychology. In:Flick, U., ed. The Psychology of the Social. Cambridge, NY:Cambridge University Press, 1998. pp. 1-12.
Frenkel-Brunswik, E. Intolerance of ambiguity as an emo-tional and perceptual personality variable. Journal ofPersonality, 18:108-143,1949.
Frith, CD. The Cognitive Neuropsychology of Schizophre-nia. Hove, U.K.: Lawrence Erlbaum Associates, 1992.
Frith, CD., and Cocoran, R. Exploring "theory of mind" inpeople with schizophrenia. Psychological Medicine,26:521-530,1996.
Heider, F. The Psychology of Interpersonal Relations. NewYork, NY: Wiley, 1958.
Hobson, R.P. Understanding persons: The role of affect.In: Baron-Cohen, S.; Tager-Flushberg, H.; and Cohen,D.J., eds. Understanding Other Minds: Perspectives FromAutism. Oxford, U.K.: Oxford Medical Publications,1994. pp. 204-227.
Hodges, A.; Byrne, M.; Grant, E.; and Johnstone, E. Peopleat risk of schizophrenia: Sample characteristics of the first100 cases in the Edinburgh High-Risk Study. BritishJournal of Psychiatry, 174:547-553,1999.
Horton, R. Tradition and modernity revisited. In: Hollis, M.,and Lukes, S. eds. Rationality and Relativism. Oxford,U.K.: Basil Blackwell, 1982. pp. 201-260.
Huber, G. Reine Defektsyndrome und Basisstadien endo-gener Psychosen. Fortschritte fuer Neurologie undPsychiatrie, 34:409-426, 1966.
Huber, G. Das Konzept substratnaher Basissymptome undseine Bedeutung fuer Theorie und Therapie schizophrenerErkrankungen. Nervenarzt, 54:23-32,1983.
Huber, G., ed. Idiopatische Psychosen: Psychopatho-logie—Neurobiologie—Therapie. Stuttgart, Germany:Schattauer, 1990.
Hume, D. A Treatise of Human Nature. (1739-1740)Oxford, U.K.: Clarendon Press, 1955.
Husserl, E. The Crisis of the European Sciences andTranscendental Phenomenology: An Introduction to
Phenomenological Philosophy. Husserliana VII.Evanston, IL: The Northwestern University Press, 1970.
Janzarik, W. Dynamische Grundkonstellationen in endo-genen Psychosen. Berlin, Germany: Springer, 1959.
Kendler, K.S.; Lieberman, J.A.; and Walsh, D. TheStructured Interview for Schizotypy (SIS): A preliminaryreport. Schizophrenia Bulletin, 15(4):559-571, 1989.
Klosterkoetter, J. Basissymptome un Endphaenomene derSchizophrenic. Berlin, Germany: Springer, 1988.
Koh, S.D., and Peterson, R.A. Encoding orientation andthe remembering of schizophrenic young adults. Journalof Abnormal Psychology, 87:303-313, 1978.
Koire\ A. Newtonian Studies. Cambridge, MA: HarvardUniversity Press, 1965.
Kraus, A. Identity and psychosis of the manic-depressive.In: De Koning, A.J.J., and Jenner, F.A., eds. Phenom-enology and Psychiatry. London, U.K.: Academic Press,1982. pp. 201-216.
Kretschmer, E. Koerperbau und Charakter. Berlin-Goettingen-Heidelberg, Germany: Springer, 1922.
Locke, J. An Essay Concerning Human Understanding.(1688) Edited by A.C. Frazer. Oxford, U.K.: OxfordUniversity Press, 1979.
Maj, M. Critique of the DSM-FV operational diagnosticcriteria for schizophrenia. British Journal of Psychiatry,172:458-460, 1998.
Malmberg, A.; Lewis, G.; David, A.; and Allebeck, P.Premorbid adjustment and personality in people withschizophrenia. British Journal of Psychiatry,172:308-313, 1998.
Meehl, P.E. Schizotaxia, schizotypy, schizophrenia.American Psychologist, 17:827-838,1962.
Merleau-Ponty, M. Phenomenologie de la Perception.Paris, France: Gallimard, 1945.
Minkowski, E. Psychiatrie et me'taphysique: A larecherche de l'humain et du vecu. Revue de Metaphysiqueet de Morale, 52:3-A, 33-358, 1947.
Minkowski, E. La Schizophrenic: Psychopathologie desSchizoides et des Schizophrenes. (1927) 2nd ed. Paris,France: Payot, 1953.
Minkowski, E. Les schizophrenes peints par eux-memes.{Medicine, 5, 1924.) Reprinted in: Postel, J., ed. LaPsychiatrie. Paris, France: Larousse, 1994.
Moscovici, S., and Hewstone, M. Social representationsand social explanations: From the "naive" to the "ama-teur" scientist. In: Hewstone, M., ed. Attribution Theory:Social and Functional Extensions. Oxford, U.K.: BasilBlackwell, 1983. pp. 98-125.
785
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022
Schizophrenia Bulletin, Vol. 26, No. 4, 2000 G. Stanghellini
Mundt, C. Das Apathiesyndrom der Schizophrenen. Einepsychopathologische und computertomographischeUntersuchung. Berlin, Germany: Springer, 1985.
Mundt, C. Constituting reality—its decline and repair in thelong-term course of schizophrenic psychoses: The intention-ality model. In: Marneros, A.; Andreasen, N.C.; and Tsuang,M.T., eds. Negative Versus Positive Schizophrenia. Berlin,Germany: Springer, 1991. pp. 96-108.
Nuechterlein, K.H., and Dawson, M.E. A heuristic vulner-ability/stress model of schizophrenic episodes.Schizophrenia Bulletin, 10(2):300-312, 1984.
Olin, S.C.; Mednick, S.A.; Cannon, T.; Jacobsen, B.; Parnas,J.; Schulsinger, R; and Schulsinger, H. School teacher rat-ings predictive of psychiatric outcome 25 years later. BritishJournal of Psychiatry, 172(Suppl 33):7-13,1998.
Parnas, J., and Bovet, P. Autism in schizophrenia revis-ited. Comprehensive Psychiatry, 32:7-21, 1991.
Penn, D.L.; Corrigan P.W.; Bentall, R.P.; Racenstein,J.M.; and Newman, L. Social cognition and schizophre-nia. Psychological Bulletin, 121:114-132, 1997.
Plotkin, H. Evolution in Mind. London, U.K.: Penguin,1997.
Raine, A.; Lencz, T.; and Mednick, S.A., eds. SchizotypalPersonality. Cambridge, NY: Cambridge UniversityPress, 1995.
Reid, T. Inquiry Into the Human Mind: On the Principlesof Common Sense. Edinburgh, Scotland: Brookes, 1997.
Rosenzweig, F. Das Buechlein vom gesunden und krankenMenschverstand. Konigstein, Germany: Athenaum,Jiidischer Verlag, 1984.
Rossi, P. Clavis Universalis: Arti Delia Memoria e LogicaCombinatoria da Lullo a Leibniz. Bologna, Italy: IIMulino, 1983.
Sarfati, Y.; Hardy-Baile\ M.C.; Besch, C ; andWidloecher, D. Attributions of intentions to others in peo-ple with schizophrenia: A non-verbal exploration withcomic strips. Schizophrenia Research, 25:199-209,1997a.
Sarfati, Y; Hardy-Baile\ M.C.; Nadel, J.; Chevalier, J.F.;and Widloecher, D. Attribution of mental states to othersby schizophrenic patients. Cognitive Neuropsychiatry,2:1-17, 19976.
Sass, L.A. Madness and Modernism: Insanity in the Lightof Modern Art, Literature, and Thought. Cambridge, MA:Harvard University Press, 1992.
Sass, L.A. The Paradoxes of Delusions. Ithaca, NY:Cornell University Press, 1994.
Schutz, A. Common sense and scientific interpretation ofhuman action. In: Natanson, M., ed. Collected Papers: I.The Problem of Social Reality. The Hague, the
Netherlands: Nijhoff, 1962. pp. 3-27.
Schwartz, M.A.; Wiggins, O.P.; and Spitzer, M. Psychoticexperience and disordered thinking: A reappraisal fromnew perspectives. Journal of Nervous and MentalDisease, 185:176-187, 1997.
Searle, J.R. The Construction of Social Reality. NewYork, NY: Free Press, 1995.
Sperber, D.; Premack, D.; and Premack, A.J., eds. CausalCognition. Oxford, U.K.: The Clarendon Press, 1995.
Spitzer, M.; Braun, U.; Hermle, L.; and Maier, S.Associative semantic network dysfunctions in thought-disordered schizophrenic patients: Direct evidence fromindirect semantic priming. Biological Psychiatry,34:864-877, 1993.
Stanghellini, G. Antropologia della Vulnerabilita. Milan,Italy: Feltrinelli, 1997a.
Stanghellini, G. For an anthropology of vulnerability.Psychopathology, 30:1-11, 19976.Strauss, J.S. Mediating processes in schizophrenia:Towards a new dynamic psychiatry. British Journal ofPsychiatry, 155(Suppl 5):22-28, 1989.
Strauss, J.S.; Hafez, H.; Lieberman, P.; Harding, CM. Thecourse of psychiatric disorder: HI. Longitudinal principles.American Journal of Psychiatry, 142:289-296, 1985.
Suellwold, L., and Huber, G. Schizophrene Basisstoerun-gen. Berlin, Germany: Springer, 1986.
Swiney, D.A. Theoretical and methodological issues incognitive science: A psycholinguistic perspective. In:Kintsch, W; Miller, J.R; and Poltson, P.G., eds. Methodsand Tactics in Cognitive Science. Hillsdale, NJ: LawrenceErlbaum, 1984. pp. 121-158.
Traupman, K.L. Encoding process memory for categori-cally related words by schizophrenic patients. Journal ofAbnormal Psychology, 89:704-713,1980.
Vico, G.B. La Scienza Nuova. (1744) Milan, Italy:Rizzoli, 1998.
Wiggins, O.P.; Schwartz, M.A.; and Northoff, G. Toward aHusserlian phenomenology of initial stages of schizophrenia.In: Spitzer, M., and Maher, B.A., eds. Philosophy andPsychopathology. New York, NY: Springer, 1990. pp. 21-34.
Wittgenstein, L. On Certainty. Oxford, U.K.: BasilBlackwell, 1969.
Wyrsch, J. Die Person des Schizophrenen: Studien zurKlinik, Psychologie, Daseinsweise. Bern, Germany:Haupt, 1949.
Yates, F.A. The Art of Memory. London, U.K.: Routledgeand Kegan Paul, 1966.
Zubin, J., and Spring, B. Vulnerability: A new view onschizophrenia. Journal of Abnormal Psychology,86:103-126, 1977.
786
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022

At Issue Schizophrenia Bulletin, Vol. 26, No. 4, 2000
Acknowledgments
I wish to thank Prof. M. Maj and Prof. L.A. Sass for theirhelpful comments on earlier versions of this manuscript.
The Author
Giovanni Stanghellini is Psychiatrist, FlorenceDepartment of Mental Health, Florence, Italy; Secretary,World Psychiatric Association Clinical PsychopathologySection and Italian Society for Psychopathology; andProfessor of Social Psychopathology, Postgraduate Schoolof Psychiatry, University of Florence, Florence, Italy.
787
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/26/4/775/1923817 by U
niversity of Bologna user on 06 January 2022






![Evidence for Hydraulic Vulnerability Segmentation and · Evidence for Hydraulic Vulnerability Segmentation and Lack of Xylem Refilling under Tension1[OPEN] Guillaume Charrier2*,](https://img.pdfslide.net/doc/110x75/5c8bb38009d3f2a66a8bde42/evidence-for-hydraulic-vulnerability-segmentation-evidence-for-hydraulic-vulnerability.jpg)