Embed Size (px)
Citation preview

ATHABASCA UNIVERSITY
ASSOCIATIONS BETWEEN ESSENTIAL MEDICINE LISTINGS AND HEALTH
OUTCOMES FOR CARDIOVASCULAR DISEASE
BY
LIANE STEINER
A THESIS
SUBMITTED TO THE FACULTY OF GRADUATE STUDIES
IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF
MASTER OF HEALTH STUDIES
FACULTY OF HEALTH DISCIPLINES
ATHABASCA, ALBERTA
JULY, 2020
© LIANE STEINER

The future of learning.
1 University Drive, Athabasca, AB, T9S 3A3 Canada P: 780.675-6821 | Toll-free (CAN/U.S.) 1.800.788.9041 (6821)
[email protected] | fgs.athabascau.ca | athabascau.ca
Approval of Thesis
The undersigned certify that they have read the thesis entitled:
ASSOCIATIONS BETWEEN ESSENTIAL MEDICINE LISTINGS AND HEALTH OUTCOMES FOR
CARDIOVASCULAR DISEASE
Submitted by
Liane Steiner
In partial fulfillment of the requirements for the degree of
Master of Health Studies
The thesis examination committee certifies that the thesis
and the oral examination is approved
Co-Supervisors:
Dr. Shawn Fraser
Athabasca University
Dr. Navindra Persaud
University of Toronto
External Examiner:
Dr. F. Haider Alvi
Athabasca University
July 3, 2020

LISTING NEML MEDICINES ON HAQ SCORES
iii
Abstract
Context: National essential medicines lists are used to guide medicine selection, appropriate use,
medicine reimbursement and public sector medicine procurement for many countries therefore
medicine listings may impact health outcomes.
Methods: Countries’ national essential medicine lists were scored on whether they listed
medicines for ischemic heart disease, cerebrovascular disease and hypertensive heart disease was
synthesized. Linear regression was used to measure the association between countries’ medicine
coverage scores and healthcare access and quality scores.
Results: There was no association between medicine coverage scores and healthcare access and
quality scores when country characteristics were accounted for. However, there was an
association between health outcome scores and health expenditure for ischemic heart disease,
cerebrovascular disease and hypertensive heart disease.
Conclusion: Listing more medicines on national essential medicine lists may not improve health
access and quality scores; rather it may only be one factor in reducing mortality from
cardiovascular disease.
Keywords: cardiovascular disease, essential medicines, amenable mortality

LISTING NEML MEDICINES ON HAQ SCORES
iv
Table of Contents
Approval of Thesis .................................................................................................................... ii
Abstract .................................................................................................................................... iii
List of Abbreviations ............................................................................................................... vi
List of Tables .......................................................................................................................... vii
List of Figures ........................................................................................................................ viii
Chapter 1. Introduction ..............................................................................................................1 Background ............................................................................................................................1 Introduction to Key Terms .....................................................................................................2
Amenable Mortality ...........................................................................................................2
Essential Medicines ...........................................................................................................5
Research in Context ...............................................................................................................7
Building on Previous Research ..............................................................................................8
Identifying the Gap ..............................................................................................................10
Chapter 2. Methodology ..........................................................................................................12 Study Design ........................................................................................................................12
Inclusion Criteria .................................................................................................................12 Exclusion Criteria ................................................................................................................12
Defining a List of Medicines ...............................................................................................12 Guideline Description ..........................................................................................................12 Guideline Search Strategy....................................................................................................14
Medicines Abstraction .........................................................................................................15 Data Management ................................................................................................................15
Data Extraction ....................................................................................................................15 Data Sources ........................................................................................................................17
Variables for Analysis..........................................................................................................17 Data Analysis .......................................................................................................................21
Chapter 3. Manuscript and Additional Results ........................................................................24 Manuscript ...........................................................................................................................24
Dataset sources ................................................................................................................25 Inclusion Criteria .............................................................................................................26 Data collection .................................................................................................................26 Data extraction .................................................................................................................34 Data analysis ....................................................................................................................35
Results ..............................................................................................................................35
Ischemic heart disease .....................................................................................................36
Cerebrovascular disease ...................................................................................................39 Hypertensive heart disease ...............................................................................................41 Discussion ........................................................................................................................43 Strengths and Limitations ................................................................................................45 Future research .................................................................................................................46 Conclusion .......................................................................................................................46

LISTING NEML MEDICINES ON HAQ SCORES
v
Chapter 4. Additional Analysis ................................................................................................47
Additional Results ................................................................................................................47 Ischemic Heart Disease. ...................................................................................................47
Cerebrovascular Disease. .................................................................................................50 Hypertensive Heart Disease .............................................................................................52
Changes from Proposal ........................................................................................................54
Chapter 5. Discussion, Limitations and Conclusion ................................................................56 Discussion ............................................................................................................................56
Summary of Findings. ......................................................................................................56 Results in Context ................................................................................................................62 Limitations ...........................................................................................................................63
Underlying Data. ..............................................................................................................63 Methodology ....................................................................................................................64
Conclusion ...........................................................................................................................66
Future Research ...................................................................................................................66 Funding ................................................................................................................................66 Ethics....................................................................................................................................66
References ................................................................................................................................67
Appendix A: Medicines for Cardiovascular Disease ...............................................................77

LISTING NEML MEDICINES ON HAQ SCORES
vi
List of Abbreviations
ATC- Anatomical Therapeutic Chemical Classification System
CVD- Cardiovascular disease
GBD- Global Burden of Disease
GDP- Gross domestic product
HAQ- Healthcare access and quality
NCD- Non-communicable disease
NEML- National essential medicine list
SDI-Sociodemographic Index
WHO- World Health Organization
WHO Model List- The World Health Organization Model List of Essential Medicines

LISTING NEML MEDICINES ON HAQ SCORES
vii
List of Tables
Table 1. Data Sources …………………………………………………………….………......... 17
Table 2. Main Variables ……………………………………………..…………………………. 17
Table 3. Country Variables ………………………………...…….……………….……………. 18
Table 4. Country Characteristics ………………………………………………….………......... 28
Table 5. Ischemic Heart Disease: Medicine Coverage Score …………………….……………. 38
Table 6. Cerebrovascular Disease: Medicine Coverage Score……………………....…………. 40
Table 7. Hypertensive Heart Disease: Medicine Coverage Score…………………...……......... 42
Table 8. Ischemic Heart Disease: Class Coverage Score………………….…………...………. 49
Table 9. Cerebrovascular Disease: Class Coverage Score………………………………...……. 51
Table 10. Hypertensive Heart Disease: Class Coverage Score……………..……...………........ 53
Table 11. Medicines for Ischemic heart Disease…………………………..…………..…….…. 77
Table 12. Medicines for Cerebrovascular Disease……………………………….....….….......... 80
Table 13 Medicines for Hypertensive Heart Disease………………………………..…………. 83

LISTING NEML MEDICINES ON HAQ SCORES
viii
List of Figures
Figure 1. Conceptual Diagram……………………………… ……………...………………….. 20
Figure 2. Ischemic Heart Disease: Medicine Coverage Score ……………...………………….. 38
Figure 3. Cerebrovascular Disease: Medicine Coverage Score ………………………………... 40
Figure 4. Hypertensive Heart Disease: Medicine Coverage Score…………………….……….. 42
Figure 5. Ischemic Heart Disease: Class Coverage Score …………………………….……….. 49
Figure 6. Cerebrovascular Disease: Class Coverage Score ………………………..…………... 51
Figure 7. Hypertensive Heart Disease: Class Coverage Score……………………………...….. 53

LISTING NEML MEDICINES ON HAQ SCORES
1
Chapter 1. Introduction
Background
Ischemic heart disease and cerebrovascular disease (stroke) are the top two causes of
death worldwide and accounted for 15.2 million deaths in 2016; they have been the leading
causes of death worldwide for the past 15 years (The World Health Organization, 2018d).
According to the Global Burden of Disease (GBD) 2016 data ischemic heart disease accounted
for 17.3% of deaths worldwide, cerebrovascular disease accounted for 10.1% of deaths and
hypertensive heart disease accounted for 1.6% of deaths (“GBD Compare | IHME Viz Hub,”
2018).
Ischemic heart disease, cerebrovascular disease and hypertensive heart disease are all
cardiovascular diseases (CVD) under the larger category of non-communicable diseases (NCD).
NCD’s are diseases not passed from person to person, they have long duration with generally
slow progression (The World Health Organization, 2017a) and they are the result of a
combination of genetic, physiological, environmental and behaviours factors (The World Health
Organization, 2018c). Low- and middle-income countries are particularly vulnerable to NCDs
with over three-quarters of heart disease and stroke-related deaths occur in them (The World
Health Organization, 2018a). The burden of NCDs will be associated with “productivity loss and
catastrophic healthcare costs” (Bazargani, Ugurlu, de Boer, Leufkens, & Mantel-Teeuwisse,
2018) which has the potential to “significantly undermine national macroeconomic
development” (Abegunde, 2011). One explanation for increasing disease burden is the increasing
urbanization and socio-economic development in low- and middle-income countries which has
lead to increased exposure to tobacco smoking, unhealthy diets and reduced physical activity
(Bazargani et al., 2018) behaviours which increase risk of developing CVD (The Centers for

LISTING NEML MEDICINES ON HAQ SCORES
2
Disease Control and Prevention, 2015). Along with an aging population, these changes have lead
to an increased rate of CVD and other NCD’s (Bazargani et al., 2018). While some medicines to
treat chronic conditions are shown to be an effective intervention strategy, they remain largely
inaccessible in low- and middle-income countries (Abegunde, 2011; Mahmić-Kaknjo et al.,
2018).
This growing burden was recognized by the World Health Organization (WHO) and
following a 2011 United Nations meeting, the WHO released a briefing document that stated that
the burden of NCD’s can not be reduced without access to essential medicines (The World
Health Organization, 2011a). The WHO estimated that improving access to existing essential
medicines could save 10 million lives per year (The World Health Organization, 2004).
Introduction to Key Terms
Amenable Mortality. Ischemic heart disease, cerebrovascular disease and hypertensive
heart disease can be treated through proper medical interventions and therefore considered
amendable to healthcare (Fullman et al., 2018). Amenable mortality refers to deaths that should
not be fatal in the presence of effective medical care. National levels of personal health-care
access and quality can be approximated by amenable mortality (Barber et al., 2017). To decide
which conditions are amenable to healthcare, Noltes and McKee (2004) conducted a systematic
review of all studies that measured avoidable mortality and created a framework for assessing
mortality amendable to personal healthcare. This framework does not include all possible causes
of preventable death with adequate healthcare, however it does provide a set of causes for which
there is reasonable consensus, within the literature, that personal health care has a major effect
(Barber et al., 2017). This framework crested a list of causes of mortality for which there is
consensus that healthcare interventions can prevent deaths. The purpose of identifying causes is

LISTING NEML MEDICINES ON HAQ SCORES
3
to use them as “tracer conditions” whose health outcomes are monitored to study the responses
of healthcare systems for causes that should not be fatal when adequate care is received. Tracer
conditions can be easily measured over time to determine progress and evaluate health policies.
(Nolte & Mckee, 2004)
Amenable mortality is used as a surrogate marker for health access and quality under the
assumption that if a healthcare system is easily accessible and properly equipped deaths should
not occur. The purpose of measuring amenable mortality is to gain insight into health-system
delivery, effectiveness, and performance (16). Measuring healthcare access and quality using
amendable mortality is becoming an increasingly popular way to approximate national levels of
personal healthcare access and quality (Fullman et al., 2018) because mortality data is measured
in many countries and more easily accessed.
Fullman et al., (2018) created a Health Access and Quality (HAQ) Index comprised of 32
causes considered amenable to health care adapted from Nolte and McKee (2004). The study
represents a range of health service areas including vaccine-preventable disease; infectious
diseases; maternal and child health; non-communicable diseases including cancers,
cardiovascular and diabetes; and gastrointestinal conditions from which adequate healthcare can
easily avert death (Barber et al., 2017). HAQ score is a measure of amenable mortality and can
be used to “benchmark dimensions of health-system performance to identify untapped potential
for advancing personal health-care access and quality” (Barber et al., 2017, p. 232). The HAQ
score was calculated using data from the Global Burden of Disease (GBD) study, which is a
comprehensive worldwide observational epidemiological study that describes morbidity and
mortality from major disease, injuries and risk factors to health at national and regional levels
(Fullman et al., 2018).

LISTING NEML MEDICINES ON HAQ SCORES
4
Assigning a HAQ score to a country involved four major steps. The authors mapped the
previously identified causes amendable to personal healthcare (Nolte & Mckee, 2004) to a GBD
cause list based on corresponding International Classification of Disease (ICD) codes. Some
categories from previous research (Nolte & Mckee, 2004) were combined or excluded due to
conflict with the GBD cause list, an action supported by GBD (Barber et al., 2017). The variation
in death rates among countries could be attributed to differences in behavioural and
environmental risk exposure. To mitigate the variation when scoring countries, they risk
standardized cause specific mortality rates to remove variations in death rates not easily
addressed through personal health care (Barber et al., 2017). To construct the HAQ scores, they
computed a summary measure of personal health-care access and quality, on a scale from 0-100,
using principal component analysis. To better understand the maximum levels of personal
healthcare access and quality achievable, they assessed the highest recorded levels of healthcare
access and quality across the development spectrum and produced a frontier analysis model
based on the relationship between the HAQ Index and the Socio-Demographic Index (SDI)
(Barber et al., 2017). SDI is a summary measure of overall development based on average
income per capita, education attainment, and total fertility rates (Fullman et al., 2018).
After the GBD 2016 study results were released, the HAQ Index was updated. Similar
data abstraction and analysis procedures were employed, however a few improvements were
made since the previous iteration (Fullman et al., 2018). Improvements were possible because
researchers were able to access more data, including vital registration data, more cancer
registries, risk factors, and cause specific mortality modeling updates (Fullman et al., 2018). Due
to the increase in quantity and quality of cancer registries, risk standardization no longer needed
to be used and instead mortality to incidence ratios were used, which was found to more strongly

LISTING NEML MEDICINES ON HAQ SCORES
5
correlate with SDI. (Fullman et al., 2018)
Results show that HAQ scores ranged from more than 97 in Iceland to less than 20 in the
Central African Republic and Somalia. Total health spending per capita was strongly positively
correlated with HAQ Index performance in 2016 (Fullman et al., 2018); meaning that increases
in healthcare spending were associated with higher HAQ Index performance.
Essential Medicines. The WHO defines essential medicines as:
Medicines that satisfy the priority health care needs of the population. They are selected
with due regard to public health relevance, evidence on efficacy and safety, and
comparative cost-effectiveness. Essential medicines are intended to be available within
the context of functioning health systems at all times in adequate amounts, in the
appropriate dosage forms, with assured quality and adequate information, and at a price
the individual and the community can afford. The implementation of the concept of
essential medicines is intended to be flexible and adaptable to many different situations;
exactly which medicines are regarded as essential remains a national responsibility (The
World Health Organization, 2004).
Essential medicines lists are a policy tool to provide access to a basic list of medicines
aimed at mitigating health inequities, it is well recognized that health and illness are not
distributed randomly throughout society (The World Health Organization, n.d.-a). Inequalities in
access to essential medicines are part of inequalities in healthcare (Hogerzeil & Mirza, 2011).
The social determinants of health are primarily responsible for health inequities between and
within countries. (The World Health Organization, n.d.-a) Key social determinants of health
include the conditions that people are born into, grow, live, work and age in; the circumstances
are shaped by distributions of money, power and resources at multiple levels of governance. (The

LISTING NEML MEDICINES ON HAQ SCORES
6
World Health Organization, n.d.-a) For example, health systems that rely on medicine supply
through out-of-pocket payments unfairly exclude the poor and vulnerable from accessing
medicines. (Hogerzeil & Mirza, 2011) Thus, medicines may be available, but access may be
limited to varying degrees within or between countries.
The WHO created a Model List of Essential Medicines (WHO Model List) in 1977 and
updates every two years based on scientific evidence for the comparative effectiveness, safety
and cost–effectiveness of the medicines (The World Health Organization Expert Committee,
2017). The WHO Model List, presents medicines and their common uses, along with an
appropriateness recommendation. The core list provides recommendations for minimum
medicine needs for a basic health-care system; particularly for priority conditions which are
“selected on the basis of current and estimated future public health relevance, and potential for
safe and cost-effective treatment” (The World Health Organization, 2017d). Essential medicine
selection depends on many factors, including the pattern of prevalent diseases, treatment
facilities, the training and experience of available personnel, financial resources, and genetic,
demographic and environmental factors (The World Health Organization, 2004).
A National Essential Medicines List (NEML) is an essential medicine list specific to a
country. NEML’s are created to address the health care priorities of individual countries
informed by the national burden of disease (Bazargani et al., 2018). “A country’s NEML reflects
a government’s commitment to ensuring that quality health commodities are available and
accessible to the population, and can serve an important tool for advocacy.”(Rashid, 2016)
Particularly in the public sector, essential medicines are more available than other medicines,
suggesting that there may be preferential attention from governments given to essential
medicines (Bazargani, Ewen, De Boer, Leufkens, & Mantel-Teeuwisse, 2014) therefore adopting

LISTING NEML MEDICINES ON HAQ SCORES
7
an NEML is the first step in ensuring equitable access to pharmaceutical treatments (Bazargani et
al., 2018). As recommended by the WHO, many countries have created or adapted their own
essential medicines list to meet the specific priority needs of their country. (The World Health
Organization, 2004)
The WHO hosts a repository of all countries’ NEML’s but not all countries have a
NEML. To address this gap, a team of researchers created a Global Essential Medicines (GEM)
database of all countries NEML’s .(Persaud, Jiang, Shaikh, Bali, Oronsaye, Woods, Drozdzal,
Rajakulasingam, Maraj, Wadhawan, Umali, Wang, McCall, Aronson, Plüddemann, Moja,
Magrini, et al., 2019) All medicines, with some exceptions, from countries’ NEML’s hosted in
the WHO’s National Essential Medicines Lists Repository were extracted and recorded in an
excel database. They identified NEMLs for 137, of 195 countries around the world. They listed
2182 medicines that appeared on at least one countries’ NEML, with a mean of 370 ± 175
medicines listed per country. The researchers concluded that country characteristics, including
WHO geographic region, population size, life expectancy, infant mortality, per capita gross
domestic product and health expenditure, only explained 33% of the differences in NEML’s and
the substantial NEML variations between countries suggest that it is unlikely that the differences
in priority health care needs of the population explain most of the variation (Persaud, Jiang,
Shaikh, Bali, Oronsaye, Woods, Drozdzal, Rajakulasingam, Maraj, Wadhawan, Umali, Wang,
McCall, Aronson, Plüddemann, Moja, Magrini, et al., 2019).
Research in Context
As previously mentioned, ischemic heart disease and cerebrovascular disease are the two
leading causes of death worldwide (The World Health Organization, 2018d). Although it’s not
one of the leading causes of death, hypertensive heart disease is also a global burden causing

LISTING NEML MEDICINES ON HAQ SCORES
8
1.6% of deaths worldwide (“GBD Compare | IHME Viz Hub,” 2018). Medicine availability and
accessibility plays and important role in addressing the burden of NCD’s (Abegunde, 2011) like
heart disease and hypertension as evident by a reduction in mortality and morbidity in many
countries since the implementation of essential medicines (Mahmić-Kaknjo et al., 2018).
Careful selection of essential medicines are thought to be a crucial first step to ensure
availability of medicines (The World Health Organization, 2004). Essential medicines listed on
countries’ NEML’s are supposed to be available at all times, in adequate amounts, and at a price
people can afford; therefore the coverage of the lists themselves becomes an important indication
of a countries’ ability to provide pharmaceutical interventions to reduce the burden of disease.
With this logic, listing medicines should lead to better health outcomes, particularly for causes of
disease and death considered amendable to healthcare.
It is important to evaluate whether NEML’s are adequately selected to maximize health
access and quality, and reduce the burden of CVD on the country. This study used the previously
created GEM database and HAQ scores to determine if listing medicines on a NEML was
associated with HAQ scores for ischemic heart disease, cerebrovascular disease and hypertensive
heart disease.
Building on Previous Research
There are several previous studies that this research built upon. The first looked at the
overlap in medicines between NEML’s and the 20th edition of the WHO Model List of Essential
Medicines. (Persaud, Jiang, Shaikh, Bali, Oronsaye, Woods, Drozdzal, Rajakulasingam, Maraj,
Wadhawan, Umali, Wang, McCall, Aronson, Plüddemann, Moja, Magrini, et al., 2019) This
research used their GEM database of NEML’s to compare a list of medicines used to manage
cardiovascular disease to countries’ NEML’s.

LISTING NEML MEDICINES ON HAQ SCORES
9
Previous research assessed countries’ NEMLs based on the number of differences from
the 20th edition of the WHO Model List of Essential Medicines. The WHO Model List was not
expected to be reproduced on countries NEML’s, rather due to differing needs, pharmaceutical
licensing and policies surrounding the production and sale of pharmaceuticals, it was meant to be
used as an evidence based guide to save costs and increase rational medicines’ availability and
prescribing (Mahmić-Kaknjo et al., 2018). Instead of only using the WHO Model List as the
reference, this study will create a list of medicines used to manage ischemic heart disease,
cerebrovascular disease and hypertensive heart disease.
This work built upon two previous studies, which looked at the quality of NEMLs by
either comparing them to the WHO Model List, or ensuring that they list medicines for all
therapeutic groups. The first measured the number and diversity of medicines used to treat CVD,
from 34 countries with operational NEML’s, across multiple low- and middle-income countries
(Bazargani et al., 2018). The researchers found that most medicine groups listed in international
guidelines appeared on countries’ NEML’s, with over 75% of NEML’s having adequate
treatment for most acute cardiovascular events as well as primary and secondary prevention of
CVD (Bazargani et al., 2018). However, they found that the coverage differed significantly
across income levels and regions. Because the main classes of medicines used in the treatment of
CVD were present, they concluded that selection will not be the limiting step in access to
medicines for CVD (Bazargani et al., 2018). Therefore, the study found that the quality of lists
assessed was overall adequate for cardiovascular disease. The second similar study compared
CVD medicines included in the WHO Model List of Essential Medicines to medicines listed in
19 Eastern Mediterranean countries (Mehrtash, Laing, & Wirtz, 2018). The study compared
both medicines listed on NEML’s and the dosage forms to the WHO Model List of Essential

LISTING NEML MEDICINES ON HAQ SCORES
10
Medicines. The researchers concluded that countries should improve their selection of essential
medicines for cardiovascular disease because the overall percent of WHO medicines was low in
some countries and others did not list medicines in certain therapeutic areas that are needed for
the treatment of CVD (Mehrtash et al., 2018). Therefore the study concluded that countries’
NEMLs need improvement to meet treatment needs.
Between the two similar studies both used different scoring techniques however, there
were 4 countries (Afghanistan, Jordan, Morocco, Pakistan) that were included in both studies.
Although some of the country level data overlapped between studies, they found mixed results
about the quality of NEMLs The discrepancy between studies may lie at a region level because
one explored multiple low- and middle- income countries across regions concluding that there
are regional differences while the other explored the Eastern Mediterranean only.
Identifying the Gap
No studies were identified that explored if listing CVD medicines, specifically for
ischemic heart disease, cerebrovascular disease and hypertensive heart disease, was associated
with measures of outcomes amenable to healthcare. We searched medline and embase using
“cardiovascular disease” or “ischemic heart disease” or “cerebrovascular disease” or
“hypertensive heart disease” (and their unique alternative names identified in the search scope
notes) in combination with “essential medicine” (and alternate names identified in the scope
notes).
Both the previous studies looking at NEMLs for cardiovascular disease assessed the
quality of included NEMLs. In contrast this study looked at the value that medicines add to
health outcomes related to cardiovascular disease.

LISTING NEML MEDICINES ON HAQ SCORES
11
This study built upon previous research studies by using a previously created database to
determine if there was a relationship between listing medicines on an NEML and HAQ scores in
countries. This study included more countries with a wider range of income then the previous
studies (Bazargani et al., 2018; Mehrtash et al., 2018) comparing CVD medicines across
countries with an NEML found in the GEM database. This additional country information will
allow for broad insight into the ability of countries to provide pharmaceutical interventions;
including a larger more diverse sample of countries will also allow us to better determine if
relationships exist within the variables.
Research question: Is there a relationship between listing medicines on a countries’
national essential medicines list (NEML) and their health access and quality (HAQ) index score
for three cardiovascular disease (CVD) causes of morbidity and mortality considered amenable
to healthcare.

LISTING NEML MEDICINES ON HAQ SCORES
12
Chapter 2. Methodology
Study Design
This study is cross sectional observational study that analyzes data at a specific point in time to
compare across countries.
Inclusion Criteria
Countries must have a NEML captured in the GEM database and a HAQ score for
ischemic heart disease, cerebrovascular disease and hypertensive heart disease.
Exclusion Criteria
Not all countries listed in GEM have an HAQ score, therefore they were excluded.
Defining a List of Medicines
Fullman et al., (2018) used 32 causes of mortality amenable to personal healthcare, that
were previously mapped by Barber et al., (2017) to the Nolte and Mckee (2004) cause list. This
only examined ischemic heart disease, cerebrovascular disease and hypertensive heart disease,
which are 3 of the 32 causes of mortality listed by Fullman et al. (2018). In order to identify
which medicines were associated with the three causes, we used the procedure described in the
manuscript to create a list of medicines.
Guideline Description
The primary guideline used for creation of a list of medicines was the Technical Package
for cardiovascular disease management in primary health care- evidence-based treatment
protocols. (The World Health Organization, 2016b) This guideline is put out by the World
Health Organization and endorsed by the Pan-American Health Organization, the World Heart
Federation, the World Stroke Organization, the International Society for Hypertension, the

LISTING NEML MEDICINES ON HAQ SCORES
13
World Hypertension League and the Centers for Disease Control and Prevention. (The World
Health Organization, 2016b) The package provides recommendations for cardiovascular disease
treatment in a primary care setting and is targeted for an international audience while being
mindful of fiscal resources. (The World Health Organization, 2016b) This guideline builds on
the WHO-PEN guideline with additional tools for CVD management. (The World Health
Organization, 2016b)
The second WHO guideline used was: Tackling NCDs: “Best Buys” and other
recommended interventions for the prevention and control of non-communicable diseases. (The
World Health Organization, 2017b) This guideline makes recommendation for a list of “Best
Buys” which are recommended cost effective and feasible interventions. (The World Health
Organization, 2017b) This guideline makes recommendations for CVD and other NCDs based
on global NCD targets. (The World Health Organization, 2017b) Although the focus of this
guideline is broad, including all NCD, there are specific recommendations for CVD.
The last two WHO guidelines are primarily used for diabetes treatment; both Prevention
and Control of Non-communicable Diseases: Guidelines for primary health care in low-resource
settings (The World Health Organization, 2012) and WHO Package of Essential Non
communicable (PEN) Diseases Interventions for Primary Health Care in Low-Resource Settings.
(The World Health Organization, 2010) These guidelines are for diabetes and not CVD
specifically therefore it may not be a comprehensive list of medicines used to treat CVD; also
these guidelines state that they are for low- resource settings therefore some countries may
question the applicability. (The World Health Organization, 2012) (The World Health
Organization, 2010) However, cardiovascular disease is commonly associated with diabetes
therefore we were able to identify some medicines used for CVD treatment from both guidelines.

LISTING NEML MEDICINES ON HAQ SCORES
14
Additional guidance was sought from the American Heart Association to ensure the list
of medicines was comprehensive. The American Heart Association is a not-for-profit association
that funds research and educates people about heart disease and stroke, based in the United States
of America with some international ties. (American Heart Association, n.d.)
Lastly, the WHO Model List of Essential Medicines was used to create a list of
medicines. The WHO Model List is update bi-annually by the WHO Expert Committee on the
Selection and Use of Essential Medicines (The World Health Organization, 2017c). The WHO
uses the following criteria for selecting essential medicines: medicines must have adequate
evidence of efficacy and safety, in a variety of settings, to be selected; relative cost-effectiveness
of both the medicines and treatment is considered and compared to efficacy when choosing
medicines in the same therapeutic category; In some cases, pharmacokinetic properties or local
considerations such as the availability of facilities for manufacture or storage may be considered;
medicines must be available in a form in which adequate quality, including bioavailability, can
be ensured; essential medicines should be formulated as single compounds, unless “the
combination has proven advantage in therapeutic effect, safety, adherence or in decreasing the
emergence of drug resistance in malaria, tuberculosis and HIV/AIDS” (The World Health
Organization, 2004) (The World Health Organization, 2017c).
Guideline Search Strategy
Identified guidelines and The WHO Model List of Essential Medicines 20th edition were
searched by using the ICD-10 diseases, conditions or cause of death and the overall HAQ cause
(either ischemic heart disease, cerebrovascular disease or hypertensive heart disease) category to
identify relevant medicines. For HAQ causes that were broad we looked at the WHO ICD-10
codes lookup (The World Health Organization, n.d.-b) to identify specific diseases conditions or

LISTING NEML MEDICINES ON HAQ SCORES
15
causes of death. Identified guidelines and The WHO Model List search was conducted based on
listed priority conditions and associated ICD-10 diseases and conditions.
Medicines Abstraction
The procedure for medication abstraction is described in the manuscript in Chapter 3.
Data Management
All data was extracted and stored in excel. There are no privacy concerns because all the
information is publicly available.
Data Extraction
For each of the 3 HAQ causes studied (ischemic heart disease, cerebrovascular disease
and hypertensive heart disease), all medicines identified were recorded in a table with duplicates
removed.
After creating three lists of medicines used to treat each of the HAQ causes, we
calculated how many medicines are listed on each countries’ NEML, giving each country a
medicine coverage score, described in the manuscript and below with additional details. The
medicines listed for each HAQ cause were coded into the GEM database, in an excel file. The
GEM database has listed medicines in the rows and countries in the columns; presence of a
medicine on a list was indicated using a “1” and absence was indicated using a “0”. (Persaud,
Jiang, Shaikh, Bali, Oronsaye, Woods, Drozdzal, Rajakulasingam, Maraj, Wadhawan, Umali,
Wang, McCall, Aronson, Plüddemann, Moja, Magrinic, et al., 2019) A formula was inputted
under each country that will include presence or absence of a medicine on an NEML multiplied
by the presence or absence on our list of medicines. The purpose is to indicating presence of a
medicines on both a country in the GEM database and our list of medicines used to treat or

LISTING NEML MEDICINES ON HAQ SCORES
16
manage diseases. Then the overall number of drugs that overlap on both lists were summed
creating a medicine coverage score for each country. The purpose of this score was to determine
if countries’ NEMLs list medicines that are used to treat or manage ischemic heart disease,
cerebrovascular disease and hypertensive heart disease; with higher scores indicating that more
medicines are listed on their NEML.
The NEML’s were scored in two different ways. The first method listed medicines
individually and compare them to medicines listed on countries NEML’s creating medicine
coverage scores for each country. The second method used the previously created list of
medicines, but medicines were grouped by therapeutic class to determine if the NEML included
any medicines within the class (Mehrtash et al., 2018). In order to determine which therapeutic
class of medicine a drug belongs to we used 2nd level ATC codes provided in the GEM database.
ATC codes are an internationally used code to identify active ingredients, they are classified
according to the main therapeutic use (WHO Collaborating Centre for Drug Statistics
Methodology, n.d.-b). ATC code were used because they are an internationally accepted system
of classification and the second level of codes outlines therapeutic subgroups, for the anatomical
main group, which in this case is, cardiovascular system. If medicines did not fall under
cardiovascular system, they were not included in this analysis. Medicines in a class are
therapeutically similar but because of trade deals, price, the political economy and complicated
inter country relationships some medicines in a class may be preferred in countries over others
therefore this score was included to provide a more fair evaluation of country NEML listings.
Further, it is not necessary to list many medicines per class; if they are considered
interchangeable, priority healthcare needs can be met without including an excessive number of
medicines. We calculated the total number of classes where countries listed at least one medicine

LISTING NEML MEDICINES ON HAQ SCORES
17
and then divided it by the total number of classes that are appropriately used to treat that
condition.
Data Sources
Table 1: Data Sources
Data source Description Variables using this source
GEM Database The GEM Database (Persaud, Jiang, Shaikh, Bali,
Oronsaye, Woods, Drozdzal, Rajakulasingam,
Maraj, Wadhawan, Umali, Wang, McCall,
Aronson, Plüddemann, Moja, Magrinic, et al.,
2019) is a resource created by researches at St.
Michael’s Hospital in Toronto, Canada. This
resource is an excel database that lists all NEML’s
from countries’ whose NEML is listed in the WHO
repository. (Persaud, Jiang, Shaikh, Bali, Oronsaye,
Woods, Drozdzal, Rajakulasingam, Maraj,
Wadhawan, Umali, Wang, McCall, Aronson,
Plüddemann, Moja, Magrini, et al., 2019)
Medicine Coverage Score
Class Coverage Score
Health Access and Quality
Scores
This score was retrieved from a study by Fullaman
et al., (2018). The scores are a measure of amenable
mortality, as measured by age standardized
mortality rates.
HAQ Score
Global Health Observatory
(GHO)
Global Health Observatory is a repository of health
statistics data for 194 Member States. The aim is to
provide access to country data and statistics and to
monitor global regional and country situations and
trends (The World Health Organization, 2016c).
Geographic Region
Population Size
Health Expenditure
Life Expectancy
The World Bank The World Bank connects global financial
resources, knowledge, and innovative solutions to
meet the needs of developing countries (The World
Bank, n.d.). This resource contains information
about countries’ finances.
Income Level
Global Burden of Disease
Study
Prevalence
Variables for Analysis
Table 2: Main Variables
Variable Independe
nt or
Type Range Description Source Rationale

LISTING NEML MEDICINES ON HAQ SCORES
18
Table 3: Country Variables
Dependent
HAQ Score Dependent Continuous 0-100 This is a measure
of amenable
mortality created
using age-
standardized
death rates.
This score will
be pulled
directly from
Fullman et al.
(2018).
This variable represents a
score of amenable
mortality.
Medicine
Coverage
Score
Independent Continuous >0 This is a medicine
coverage score
with all medicines
separated. See
the data
extraction section
for how the score
was calculated.
This score was
calculated
using the
created list of
medicines and
the GEM
database.
The medicine coverage
score represents a
countries ability to
provide pharmaceutical
intervention to treat or
manage the diseases or
conditions
Class
Coverage
Score
Independent Continuous 0-10 This is a medicine
coverage score
with molecules
grouped by class
of medicine that
are considered
therapeutically
equivalent. See
the data
extraction section
for how the score
was calculated.
This score was
calculated
using the
created list of
medicines and
the GEM
database, then
grouping them
by 2nd level
ATC codes.
The class coverage score
represents a countries
ability to provide
pharmaceutical
intervention to treat or
manage the diseases or
conditions. The purpose
of grouping medicines is
to see if countries have
comprehensive medicine
coverage.
Variable Independen
t or
Dependent
Type Range Description Source Rationale
Health
Expenditur
e
Independent Continuous >0 Health spending
in current PPP per
capita (The World
Health
Organization,
2018e).
The
information
will be
retrieved from
the Global
Health
Observatory
created by the
WHO, for
2016 (The
World Health
Organization,
2018e).
Healthcare expenditure
may give insight into a
country’s ability to pay
for medicines and other
healthcare treatments.

LISTING NEML MEDICINES ON HAQ SCORES
19
Population
Size
Independent Continuous >0 The number of
people or
inhabitants in a
region or country
(Merriam-
Webster, n.d.).
The
information
will be
retrieved from
the Global
Health
Observatory
created by the
WHO, for
2016 (The
World Health
Organization,
2018e).
It is important to account
for variations in
population size to
determine if country
characteristics impact
health outcomes.
Life
Expectancy
Independent Continuous >0 Average number
of years that a
newborn is
expected to live if
current mortality
rates continue to
apply (The World
Health
Organization,
2006).
This
information
will be
retrieved from
the Global
Health
Observatory
created by the
WHO, for
2016 (The
World Health
Organization,
2016a)
It is important to account
for variations in life
expectancy because
cardiovascular disease is
more prevalent in certain
age groups (Goff et al.,
2014). Also, age is a
known risk factor for
CVD (Dhingra & Vasan,
2012).
Prevalence Independent Continuous >0 The number of
people with the
disease (Institute
for Health
Metrics and
Evaluation, 2017)
per 100, 000
people
This score will
be pulled
directly from
the Global
Health and
Data
Exchange, for
2017 (Global
Health and
Data
Exchange,
2018)
The addition of
prevalence can give
insight into quality of
care.

LISTING NEML MEDICINES ON HAQ SCORES
20
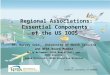
Figure 1. Conceptual diagram

LISTING NEML MEDICINES ON HAQ SCORES
21
Data Analysis
Due to the use of two different scoring techniques, two different analyses were run. Both
analyses use HAQ score as the dependent variable and alternated medicine coverage score and
class coverage score as the main independent variable. The purpose of including a second
analysis was to determine if each country lists at least one medicine for each class of
cardiovascular medicines, this information would not be included in the individual medicine
analysis. For both analyses the covariates are healthcare expenditure, GDP, life expectancy,
prevalence and population.
Data analysis was conducted using the 26th edition of SPSS (Laerd Statistics, 2018), and
a p-value ≤ 0.05 was considered significant. However bivariate and multivariate associations and
effect sizes were the focus of the analysis. The primary outcome of the analysis was to determine
if there is a positive relationship between listing medicines on a countries’ NEML and their HAQ
score. Assumption of a linear relationship, no significant outliers, independence of observations,
homoscedasticity and approximately normally distribution of errors, were checked using the
following procedure (Laerd Statistics, 2018).
Frequencies tables were created to examine the range of variables and ensure the data
was complete with no errors. Some values were missing however these were determined to be
true missing values not found in the data source, particularly health expenditure for some
countries.
Assumptions of linearity were checked by producing scatterplots with the independent
variable on the x-axis and the dependent variable on the y–axis with a line of best fit (Fields,

LISTING NEML MEDICINES ON HAQ SCORES
22
2018). We also examined partial plots to examine for any obvious and severe non-linearity. In
no case did we find any indications of a violation of the linearity assumption.
The data were checked for outliers. Outliers were detected using z-scores, which were
calculated for all data points. The decision criterion level chosen was 0.01, as it is often used
(Cousineau & Chartier, 2010). The sample size (number of countries) is approximately 130
therefore the degrees of freedom are approximately 129; after adjusting for the Bonferroni
correction to take into account sample size, with the chosen level of 0.01, a z-score of less than -
3.891 or greater than 3.891 was considered an outlier (Cousineau & Chartier, 2010).Using the
calculated z-score range of less than -3.891 or greater than 3.891, outliers were present
particularly for GDP, health expenditure and population. Next outliers were removed from these
variables to ensure that they are not to blame for the skewedness; even with outliers removed the
skewness pattern persisted. Outliers were kept because removal did not rectify the skewedness
and they are true values with no potential to be erroneous; eg: we know that China and India
have large populations.
Next we checked assumption of normality using the Shapiro-Wilk test along with histograms
with a bell curve added, box plots and Q-Q plots. Most variables were approximately normally
distributed with the exception of GDP, health expenditure and population.
To further look at the relationship between the variables, including those that appear to be not
normally distributed pairwise correlations were calculated using both the Pearson correlation and
Spearman’s rho correlation. Based on the histograms the variables were all skewed to the right
therefore Log 10 transformations were preformed (“Data transformations - Handbook of

LISTING NEML MEDICINES ON HAQ SCORES
23
Biological Statistics,” n.d.) on GDP, health expenditure and population to make them
approximately normally distributed.
Linearity, independence of observations and homoscedasticity were tested by graphing
the values of the residuals against the corresponding values of the outcomes predicted by the
model in a scatterplot. Visual inspection showed no clear or severe departures from normal
distribution and we concluded that the data met these assumptions. (44)
Parametric tests were chosen and two linear regression models were run; the first with
the log transformed independent variables for GDP, health expenditure and population, then with
the non-log transformed GDP, health expenditure and population. When looking at the R2 value,
the correlation value and the Beta value it appeared that they were similar meaning the log
transformation did not appear to affect the model. Therefore, it was decided that the non-
transformed variables would be used for the regression to aid in interpretation of the results.
Pearson correlation table suggested that GDP and health expenditure were significantly
related to each other and possibly colinear. To explore how this relationship was affecting the
model we removed GDP. We decided to remove GDP first because it had a lower Pearson
correlation value in relation to the dependent variable. We ran two models removing GDP then
added it back into the model; only a small impact to the R2 value was observed, therefore GDP
was not a significant contributor to the model. It was removed because health expenditure is
theoretically a more important variable because it is expected to more directly impact mortality
outcomes, also there was slightly less missing data.

LISTING NEML MEDICINES ON HAQ SCORES
24
Chapter 3. Manuscript and Additional Results
Manuscript
The manuscript is a summary of they key findings of this original research.
Approximately 29% of deaths worldwide are from cardiovascular disease specifically,
ischemic heart disease, stroke and hypertensive heart disease. (“GBD Compare | IHME Viz
Hub,” 2018) The burden of these and other non-communicable diseases (NCD) will be
associated with productivity loss and catastrophic healthcare costs (Bazargani et al., 2018) which
has the potential to significantly undermine national macroeconomic development (Abegunde,
2011). Deaths from cardiovascular disease are amenable to healthcare, meaning adequate
healthcare can prevent them (i.e. amenable mortality) (Fullman et al., 2018).
Following a 2011 United Nations meeting, the World Health Organization (WHO)
released a briefing document which stated that the burden of NCD’s cannot be reduced without
access to essential medicines. (The World Health Organization, 2011b) Essential medicines are
those that satisfy the priority health care needs of the population. (The World Health
Organization, 2004) The purpose of an essential medicines list is to ensure quality medicines are
available in a functioning health system, in appropriate forms, at affordable prices for both the
individual and the community. (The World Health Organization, 2004)The WHO created a
Model List of Essential Medicines (WHO Model List) which provides recommendations for
minimum medicine needs for a basic health-care system. Many countries have embraced the idea
of essential medicines and adapted their own national essential medicines list (NEML) to address
their health care priorities informed by their national burden of disease. (Bazargani et al., 2018)
NEML’s are used to guide appropriate use of medicines, as well as medicine selection,
reimbursement and public sector procurement (The World Health Organization, 2016b, 2018b).

LISTING NEML MEDICINES ON HAQ SCORES
25
In the public sector, essential medicines are more available than other medicines, suggesting that
there may be preferential attention from governments given to them, therefore carefully selecting
and adopting an NEML is the first step in ensuring equitable access to pharmaceutical treatment
(Bazargani et al., 2018).
Medication availability and accessibility plays and important role in addressing the
burden of NCD’s (Abegunde, 2011) as evident by a reduction in mortality and morbidity in
many countries since the implementation of essential medicines (Mahmić-Kaknjo et al., 2018).
The purpose of this study is to determine if there is an association between listing
medicines used to treat ischemic heart disease, stroke and hypertensive heart disease and
amenable mortality related to these conditions measured by the healthcare access and quality
(HAQ) score. (Fullman et al., 2018)
Methods
Dataset sources
All medications, with some exceptions, from countries’ NEML’s hosted in the WHO’s
National Essential Medicines Lists Repository were extracted and recorded in an excel database
(Persaud, Jiang, Shaikh, Bali, Oronsaye, Woods, Drozdzal, Rajakulasingam, Maraj, Wadhawan,
Umali, Wang, McCall, Aronson, Plüddemann, Moja, Magrini, et al., 2019). NEMLs for 137
countries were identified. They listed 2182 medicines that appeared on at least one countries’
NEML, with a mean of 370 ± 175 medications listed on NEMLs (Persaud, Jiang, Shaikh, Bali,
Oronsaye, Woods, Drozdzal, Rajakulasingam, Maraj, Wadhawan, Umali, Wang, McCall,
Aronson, Plüddemann, Moja, Magrini, et al., 2019).

LISTING NEML MEDICINES ON HAQ SCORES
26
Countries received an amenable mortality score, calculated by measuring age
standardized mortality rates, for ischemic heart disease, cerebrovascular disease and hypertensive
heart disease. (Fullman et al., 2018) HAQ score was part of a larger study that combined 32
causes to create a composite, HAQ Index for 195 countries.
Inclusion Criteria
Countries were included if they had a NEML captured by GEM database and a HAQ
score for ischemic heart disease, cerebrovascular disease and hypertensive heart disease.
Data collection
In order to identify which medications were relevant to the three causes of interest
(ischemic heart disease, cerebrovascular disease and hypertensive heart disease), we used the
following procedure. Guidelines for ischemic heart disease, cerebrovascular disease and
hypertensive heart disease were searched for on the WHO website in June 2019. Four
international guidelines distributed by the WHO, an internationally recognized health authority,
were selected: Prevention and Control of Non-communicable Diseases: Guidelines for primary
health care in low-resource settings (The World Health Organization, 2012), WHO Package of
Essential Non communicable (PEN) Diseases Interventions for Primary Health Care in Low-
Resource Settings (The World Health Organization, 2010), Technical Package for cardiovascular
disease management in primary health care- evidence-based treatment protocols (The World
Health Organization, 2016b), Tackling NCDs: “Best Buys” and other recommended
interventions for the prevention and control of non-communicable diseases (The World Health
Organization, 2017b). Although it is not an internationally recognized guideline, additional
guidance from the American Heart Association’s website was used to ensure all relevant
medicines were captured (American Heart Association, 2019). These guidelines along with the

LISTING NEML MEDICINES ON HAQ SCORES
27
WHO Model List of Essential Medicines 20th edition (The World Health Organization, 2017d)
were used to identify medicines used for treatment of ischemic heart disease, cerebrovascular
disease and hypertensive heart disease. Guidelines were searched using the causes and associated
ICD-10 codes provided. (Fullman et al., 2018)
Population size, health expenditure and life expectancy were retrieved from the Global
Health Observatory (GHO)(The World Health Organization, 2018e); prevalence for ischemic
heart disease, cerebrovascular disease and hypertensive heart disease was retrieved from the
Global Burden of Disease Study (“GBD Compare | IHME Viz Hub,” 2018). Most data was for
the year 2016; if 2016 data was not available, data from the closest year to 2016 was retrieved.
Country characteristics can be found in Table 4.

LISTING NEML MEDICINES ON HAQ SCORES
28
Table 4. Country Characteristics
Country
ISO
Code Geographic Region
Income
Group
Health
Expenditure
for 2015
(per capita
in PPP
intl$)
Population
for 2016
(in
thousands)
Life
Expectancy
for 2016 (in
years)
Year of
NEML
Publication
Afghanistan AFG
Eastern
Mediterranean Low 183.9 34656 62.7 2014
Albania ALB Europe Upper middle 773.7 2926 76.4 2011
Algeria DZA Africa Upper middle 1031.2 40606 76.4 2016
Angola AGO Africa Lower middle 195.5 28813 62.6 2007
Antigua and
Barbuda ATG The Americas High 1105.1 101 75 2008
Argentina ARG The Americas High 1389.8 43847 76.9 2011
Armenia ARM Europe Upper middle 883.2 2925 74.8 2010
Bahrain (Kingdom
of) BHR
Eastern
Mediterranean High 2453.2 1425 79.1 2015
Bangladesh BGD South-East Asia Lower middle 88 162952 72.7 2008
Barbados BRB The Americas High 1233.6 285 75.6 2011
Belarus BLR Europe Upper middle 1084.6 9480 74.2 2012
Belize BLZ The Americas Upper middle 523.7 367 70.5 2008
Bhutan BTN South-East Asia Lower middle 287.1 798 70.6 2016
Bolivia BOL The Americas Lower middle 445.8 10888 71.5 2011
Bosnia and
Herzegovina BIH Europe Upper middle 1101.8 3517 77.3 2009
Brazil BRA The Americas Upper middle 1391.5 207653 75.1 2014
Botswana BWA Africa Upper middle 970 2250 66.1 2012
Bulgaria BGR Europe Upper middle 1491.9 7131 74.8 2011
Burkina Faso BFA Africa Low 96.1 18646 60.3 2014
Burundi BDI Africa Low 63.7 10524 60.1 2012
Cabo (Cape) Verde CPV Africa Lower middle 310.4 540 73.2 2009

LISTING NEML MEDICINES ON HAQ SCORES
29
Cambodia KHM South-East Asia Lower middle 209.6 15762 69.4 2003
Cameroon CMR Africa Lower middle 162.8 23439 58.1 2010
Central African
Republic CAF Africa Low 31.9 4595 53 2009
Chad TCD Africa Low 99.8 14453 54.3 2007
Chile CHL The Americas High 1903.1 17910 79.5 2005
China CHN Western Pacific Upper middle 762.2 1411415 76.4 2012
Colombia COL The Americas Upper middle 852.8 48653 75.1 2011
Congo COG Africa Lower middle 202.7 5126 64.3 2013
Costa Rica CRI The Americas Upper middle 1286.5 4857 79.6 2014
Côte d'Ivoire CIV Africa Lower middle 189.6 23696 54.6 2014
Croatia HRV Europe High 1656.4 4213 78.3 2010
Cuba CUB The Americas Upper middle 2478.8 11476 79 2012
Czech Republic CZE Europe High 2469.9 10611 79.2 2012
Democratic Peoples
Republic of Korea PRK South-East Asia Low
25369 71.9 2012
Democratic Republic
of Congo COD Africa Low 34 78736 60.5 2010
Djibouti DJI
Eastern
Mediterranean Lower middle 146.7 942 63.8 2007
Dominica DMA The Americas Upper middle 585.7 74
2007
Dominican Republic DOM The Americas Upper middle 873.1 10649 73.5 2015
Ecuador ECU The Americas Upper middle 980.2 16385 76.5 2013
Egypt EGY
Eastern
Mediterranean Lower middle 495.2 95689 70.5 2012
El Salvador SLV The Americas Lower middle 578.5 6345 73.7 2009
Eritrea ERI Africa Low 56.2 4955 65 2010
Estonia EST Europe High 1886.8 1312 77.8 2012
Ethiopia ETH Africa Low 65.6 102403 65.5 2014
Fiji FJI Western Pacific Upper middle 331.4 899 69.9 2015
Gambia GMB Africa Low 114.1 2039 61.9 2001
Georgia GEO Europe Lower middle 717.7 3925 72.6 2007
Ghana GHA Africa Lower middle 249.3 28207 63.4 2010

LISTING NEML MEDICINES ON HAQ SCORES
30
Grenada GRD The Americas Upper middle 677.5 107 73.4 2007
Guinea GIN Africa Low 57.2 12396 59.8 2012
Guyana GUY The Americas Upper middle 336.1 773 66.2 2010
Haiti HTI The Americas Low 120.1 10847 63.5 2012
Honduras HND The Americas Lower middle 353.4 9113 75.2 2009
India IND South-East Asia Lower middle 237.7 1324171 68.8 2015
Indonesia IDN South-East Asia Lower middle 369.3 261115 69.3 2011
Iran (Islamic
Republic of) IRN
Eastern
Mediterranean Upper middle 1261.7 80277 75.7 2014
Iraq IRQ
Eastern
Mediterranean Upper middle 481 37203 69.8 2010
Jamaica JAM The Americas Upper middle 511.4 2881 76 2012
Jordan JOR
Eastern
Mediterranean Upper middle 568.1 9456 74.3 2011
Kenya KEN Africa Lower middle 157.2 48462 66.7 2016
Kiribati KIR Western Pacific Lower middle 151.8 114 66.1 2009
Kyrgyzstan KGZ Europe Lower middle 286.6 5956 71.4 2009
Latvia LVA Europe High 1429.3 1971 75 2012
Lebanon LBN
Eastern
Mediterranean Upper middle 1117.3 6007 76.3 2014
Lesotho LSO Africa Lower middle 251.1 2204 52.9 2005
Liberia LBR Africa Low 127.8 4614 62.9 2011
Lithuania LTU Europe High 1874.6 2908 75 2012
Madagascar MDG Africa Low 76.7 24895 66.1 2008
Malawi MWI Africa Low 108.2 18092 64.2 2015
Malaysia MYS Western Pacific Upper middle 1063.9 31187 75.3 2014
Maldives MDV South-East Asia Upper middle 1513.9 428 78.4 2011
Mali MLI Africa Low 118.5 17995 58 2012
Malta MLT Europe High 3470.9 429 81.5 2008
Marshall Islands MHL Western Pacific Upper middle 862.8 53
2007
Mauritania MRT Africa Lower middle 177.1 4301 63.9 2008
Mexico MEX The Americas Upper middle 1008.7 127540 76.6 2011
Mongolia MNG South-East Asia Lower middle 469.6 3027 69.8 2009

LISTING NEML MEDICINES ON HAQ SCORES
31
Montenegro MNE Europe Upper middle 957 629 76.8 2011
Morocco MAR
Eastern
Mediterranean Lower middle 435.3 35277 76 2012
Mozambique MOZ Africa Low 63.7 28829 60.1 2016
Myanmar (Burma) MMR South-East Asia Lower middle 267.2 52885 66.8 2010
Namibia NAM Africa Upper middle 942.5 2480 63.7 2016
Nepal NPL South-East Asia Low 150.6 28983 70.2 2011
Nicaragua NIC The Americas Lower middle 406 6150 75.5 2011
Nigeria NGA Africa Lower middle 215.2 185990 55.2 2010
Oman OMN
Eastern
Mediterranean High 1635.9 4425 77 2009
Pakistan PAK
Eastern
Mediterranean Lower middle 134.4 193203 66.5 2016
Papua New Guinea PNG Western Pacific Lower middle 98.6 8085 65.9 2012
Paraguay PRY The Americas Upper middle 724.3 6725 74.2 2009
Peru PER The Americas Upper middle 671 31774 75.9 2012
Philippines PHL Western Pacific Lower middle 322.8 103320 69.3 2008
Poland POL Europe High 1704.2 38224 77.8 2017
Portugal PRT Europe High 2661.4 10372 81.5 2011
Republic of
Moldova MDA Europe Lower middle 515.3 4060 71.5 2011
Romania ROU Europe Upper middle 1090.4 19778 75.2 2012
Russian Federation RUS Europe Upper middle 1414 143965 71.9 2014
Rwanda RWA Africa Low 143.2 11918 68 2010
Saint Lucia LCA The Americas Upper middle 681.4 178 75.6 2007
Saint Vincent and
the Grenadines VCT The Americas Upper middle 469.5 110 72 2010
Senegal SEN Africa Low 97.1 195 75.1 2013
Serbia SRB Europe Upper middle 1323.7 8820 76.3 2010
Seychelles SYC Africa High 867.3 94 73.3 2010
Slovakia SVK Europe High 2062 5444 77.4 2012
Slovenia SVN Europe High 2733.8 2078 80.9 2017
Solomon Islands SLB Western Pacific Lower middle 173 599 71.1 2017

LISTING NEML MEDICINES ON HAQ SCORES
32
Somalia SOM Africa Low
14318 55.4 2006
South Africa ZAF Africa Upper middle 1086.4 56015 63.6 2014
Sri Lanka LKA South-East Asia Lower middle 353.1 20798 75.3 2013
Sudan SDN Africa Lower middle 277 39579 65.1 2014
Suriname SUR The Americas Upper middle 1016.9 558 71.8 2014
Sweden SWE Europe High 5298.6 9838 82.4 2016
Syrian Arab
Republic SYR
Eastern
Mediterranean Low
18430 63.8 2008
Tajikistan TJK Europe Low 192.7 8735 70.8 2009
Thailand THA South-East Asia Upper middle 610.2 68864 75.5 2013
The former
Yugoslav Republic
of Macedonia MKD Europe Upper middle 857.1 2081 75.9 2008
Timor-Leste TLS South-East Asia Lower middle 141.3 1269 68.6 2015
Togo TGO Africa Low 95.6 7606 60.6 2012
Tonga TON Western Pacific Upper middle 323.8 107 73.4 2007
Trinidad & Tobago TTO The Americas High 2204.1 1365 71.8 2010
Tunisia TUN
Eastern
Mediterranean Lower middle 774.1 11403 76 2012
Uganda UGA Africa Low 138.5 41488 62.5 2012
Ukraine UKR Europe Lower middle 469.4 44439 72.5 2009
United Republic of
Tanzania TZA Africa Low 96.5 55572 63.9 2013
Uruguay URY The Americas High 1747.8 3444 77.1 2011
Vanuatu VUT Western Pacific Lower middle 106.1 270 72 2006
Venezuela
(Bolivarian Republic
of) VEN The Americas Upper middle 579.4 31568 74.1 2004
Viet Nam VNM Western Pacific Lower middle 334.3 94569 76.3 2008
Yemen YEM
Eastern
Mediterranean Low 144.5 27584 65.3 2009
Zambia ZMB Africa Lower middle 203 16591 62.3 2013
Zimbabwe ZWE Africa Low 182.3 16150 61.4 2011

LISTING NEML MEDICINES ON HAQ SCORES
33
ISO: The International Organization for Standardization

LISTING NEML MEDICINES ON HAQ SCORES
34
Data extraction
Using the identified guidelines for ischemic heart disease, cerebrovascular disease and
hypertensive heart disease, medications used to treat these conditions were abstracted using the
following procedure: If a guideline indicated a therapeutic class of medications, that class was
fully expanded to include all medicines because medicines within the same chemical subgroup
may be considered therapeutically similar. The WHO Model List recognizes interchangeability
of certain medicines on their list for others within the same therapeutic class. (The World Health
Organization, 2017d) Using this principle, 4th level Anatomical Therapeutic Chemical
Classification (ATC) codes (WHO Collaborating Centre for Drug Statistics Methodology, n.d.-a)
were used to guide which medicines are in the same therapeutic class. If a therapeutic class was
mentioned and specific alternatives were stated, only those medicines were included (no
therapeutic class expansion was done).
Medicines listed on the WHO Model List or those from guidelines appearing on the
WHO Model List (in a form that is usable for the conditions or cause), with a square box symbol,
were fully expanded based on the 4th level, chemical subgroup of the ATC code to include all
medicines within that therapeutic class. If the medicine is not denoted with a square box it was
not expanded. If specific medicines considered equivalent were stated, only those medicines
were included.
An exception to these rules were made for streptokinase, it is not denoted with a square
box on the WHO Model List however, it was expanded. Two clinicians (NP, DM) agreed that it
was worth expanding because all medicines in the therapeutic class were felt to be equivalent

LISTING NEML MEDICINES ON HAQ SCORES
35
and widely used. We felt that it would be unfair to exclude streptokinase alternatives because
they are equally valid from a clinical perspective.
All medicines identified in the guidelines were combined into one list per HAQ cause, for
each list medicines were de-duplicated (Appendix 1). A medicine coverage score was created by
summing the number of medicines on a country’s NEML that were also listed on our list of
medicines used to treat each HAQ cause.
Data analysis
Data was analyzed using IBM SPSS Statistics version 26 (IBM Corp., 2018), and a p-
value ≤ 0.05 was considered significant. An ordinary least squares linear regression model was
used to test the hypothesis that there would be a positive relationship between listing medicines
(medicine coverage score) and HAQ scores. HAQ score was used as the dependent variable and
the previously calculated medicine coverage score was used as the independent variable. Linear
regression results are reported for both unadjusted and adjusted with health expenditure,
population, life expectancy and prevalence as covariates. For the regression, assumptions were
checked including assumptions of normality. Two variables (population and healthcare
expenditure) were not normally distributed so they were logged; however in the regression little
difference was observed between models with logged and not logged variables therefore for
interpretation purposes we kept the unlogged variables in the regression.
Results
In total, 131 countries were included in the analysis having both a NEML and HAQ score
(Table 4). WHO regions represented by countries were the Eastern Mediterranean (14 countries),
Europe (26 countries), Africa (38 countries), the Americas (29 countries), South-East Asia (13

LISTING NEML MEDICINES ON HAQ SCORES
36
countries) and the Western Pacific (11 countries) (The World Health Organization, 2018e).
Using the World Bank categorization, included countries represented a range of income levels
with 28 low income countries, 40 lower-middle income countries, 43 upper middle countries and
20 high income countries (The World Bank, n.d.). Three countries (Democratic Peoples Republic
of Korea, Somalia and Syrian Arab Republic) were excluded from the regression analysis
because they were missing values for healthcare expenditure.
The total number of medicines identified through guideline searches for each cause; 103
medicines for ischemic heart disease, 96 medicines for cerebrovascular disease and 73 medicines
for hypertensive heart disease (see appendix for list of medicines).
Ischemic heart disease
For ischemic heart disease, medicine coverage scores ranged from 2 to 73 (median: 28,
IQR: 23 to 37). Table 5 reports the results of the unadjusted linear regression model showing
that listing ischemic heart disease medicines only explained 0.5% of the variability in the HAQ
scores across countries included in the analysis (R2= 0.005). Figure 2 shows the unadjusted
relationship between variables by regions, with the size of the bubbles representing per capita
health expenditure. Table 5 reports the results after adjusting for population size, health
expenditure, life expectancy and prevalence, which showed that approximately 18% of
differences in the HAQ score for ischemic heart disease (R2= 0.176) were explained by medicine
coverage score for ischemic heart disease along with the four covariates; therefore the addition of
covariates improved the fit of the model. The small correlation between HAQ and medicine
coverage (r= 0.069) confirmed little relationship between these variables for ischemic heart
disease, however other variables in the adjusted analysis showed an association with HAQ
scores. Health expenditure was associated with a 0.011 point increase in HAQ score for each

LISTING NEML MEDICINES ON HAQ SCORES
37
additional per capita dollar (p<0.001) and prevalence of ischemic heart disease was associated
with a 0.007 point decrease in HAQ score for each additional 100, 000 people diagnosed with
ischemic heart disease (p<0.001).

LISTING NEML MEDICINES ON HAQ SCORES
38
Table 5. Ischemic Heart Disease: Medicine Coverage Score
Variable B
95% CI
lower bound
95% CI
upper bound Beta P-value
Pearson
correlation
Unadjusted Medicine Coverage Score 0.109 -0.164 0.382 0.69 0.43 0.069
Adjusted Medicine Coverage Score 0.194 -0.14 0.528 0.123 0.252 0.108
Health Expenditure 0.011 0.005 0.017 0.467 <0.001 0.232
Population -1.056E-7 0 0 0.001 0.991 -0.008
Life Expectancy 0.058 -0.636 0.752 0.02 0.869 0.093
Prevalence -0.007 -0.01 -0.004 -0.49 <0.001 -0.108
Note: R2unadjussted = 0.005 (F = 0.626, (df: 130), p =0.43). R2
adjussted = 0.176 (F = 5.131, (df: 125), p < 0.001)
Figure 2. Ischemic Heart Disease: Medicine Coverage Score
0
20
40
60
80
100
0 10 20 30 40 50 60 70 80
HA
Q S
core
Medicine Coverage Score
Ischemic Heart Disease
Africa
Eastern Mediterranean
Europe
South-East Asia
The Americas
Western Pacific

LISTING NEML MEDICINES ON HAQ SCORES
39
Cerebrovascular disease
For cerebrovascular disease, medicine coverage scores ranged from 1 to 67 (median: 21,
IQR: 17 to 31). Table 6 reports the results of the unadjusted linear regression model showing that
listing cerebrovascular disease medicines explained approximately 15% of the variation in the
HAQ scores (R2= 0.153). Figure 3 shows the unadjusted relationship between variables by
regions, with the size of the bubbles representing per capita health expenditure. Table 6 reports
the results of the adjusted analysis, which showed that approximately 44% of differences in the
HAQ score for cerebrovascular disease (R2= 0.443) were explained by medicine coverage score
for cerebrovascular disease along with the four covariates, again the addition of covariates
improved the fit of the model. The correlation (r=0.391) confirms an association between
medicine coverage score and HAQ score for cerebrovascular disease however the multivariate
relationship was not present when covariates were included. Similar to ischemic heart disease,
other variables in the adjusted analysis showed a significant association with HAQ scores. Health
expenditure was associated with a 0.014 point increase in HAQ score for each additional per
capita dollar (p<0.001), life expectancy was associated with a 0.557 point increase with each
additional year of life (p=0.042) and prevalence of cerebrovascular disease was associated with a
0.008 point decrease in HAQ score for each additional 100, 000 people diagnosed with
cerebrovascular disease (p=0.001).

LISTING NEML MEDICINES ON HAQ SCORES
40
Table 6. Cerebrovascular Disease: Medicine Coverage Score
Variable B
95% CI
lower
bound
95% CI
upper bound Beta P-value
Pearson
correlation
Unadjusted Medicine Coverage Score 0.565 0.333 0.796 0.391 <0.001 0.391
Adjusted Medicine Coverage Score 0.173 -0.089 0.435 0.117 0.194 0.393
Health Expenditure 0.014 0.009 0.018 0.587 <0.001 0.609
Population -3.977E-06 0 0 -0.037 0.596 -0.092
Life Expectancy 0.557 0.1 1.095 0.2 0.042 0.476
Prevalence -0.008 -0.013 -0.004 -0.319 0.001 0.185
Note: R2unadjussted = 0.153 (F = 23.225, (df: 130), p <0.001). R2
adjussted = 0.443 (F = 19.071, (df: 125), p <0.001)
Figure 3. Cerebrovascular Disease: Medicine Coverage Score
0
20
40
60
80
100
0 10 20 30 40 50 60 70 80
HA
Q S
core
Medicine Coverage Score
Cerebrovascular Disease
Africa
Eastern Mediterranean
Europe
South-East Asia
The Americas
Western Pacific

LISTING NEML MEDICINES ON HAQ SCORES
41
Hypertensive heart disease
For hypertensive heart disease, medication coverage scores ranged from 0 to 54 (median: 17,
IQR 13 to 25). Table 7 reports the results of the unadjusted linear regression model showing that
listing hypertensive heart disease medicines explained approximately 11% of the variation in the
HAQ score (R2= 0.109). Figure 4 shows the unadjusted relationship between variables by
regions, with the size of the bubbles representing per capita health expenditure. Table 7 reports
the results of the adjusted analysis, which showed that approximately 45% of differences in the
HAQ score for hypertensive heart disease (R2= 0.454) were explained by listing medicines for
hypertensive heart disease along with the four covariates. Similar to cerebrovascular disease, the
correlation (r= 0.331) confirms the association between medicine coverage score and the HAQ
score for hypertensive heart disease, however the multivariate relationship was not present when
covariates were included. Other variables in the adjusted analysis showed a significant
association with HAQ scores. Health expenditure was associated with a 0.008 point increase in
HAQ score for each additional per capita dollar (p<0.001), life expectancy was associated with a
1.371 point increase with each additional year of life ( p<0.001) and prevalence of hypertensive
heart disease was associated with a 0.044 point decrease in HAQ score for each additional 100,
000 people diagnosed with hypertensive heart disease (p<0.001).

LISTING NEML MEDICINES ON HAQ SCORES
42
Table 7. Hypertensive Heart Disease: Medicine Coverage Score
Variable B
95% CI
lower bound
95% CI
upper bound Beta P-value
Pearson
correlation
Unadjusted Medicine Coverage Score 0.621 0.312 0.929 0.331 <0.001 0.331
Adjusted Medicine Coverage Score 0.204 -0.116 0.524 0.11 0.209 0.324
Health Expenditure 0.008 0.004 0.013 0.346 <0.001 0.533
Population 2.073E-06 0 0 0.019 0.782 -0.009
Life Expectancy 1.371 0.829 1.913 0.484 <0.001 0.554
Prevalence -0.044 -0.063 -0.026 -0.402 <0.001 0.084
Note: R2unadjussted = 0.109 (F = 15.846, (df: 130), p <0.001). R2
adjussted = 0.454 (F = 19.963, (df: 125), p <0.001)
Figure 4. Hypertensive Heart Disease: Medicine Coverage Score
0
20
40
60
80
100
0 10 20 30 40 50 60
HA
Q S
core
Medicine Coverage Score
Hypertensive Heart Disease
Africa
Eastern Mediterranean
Europe
South-East Asia
The Americas
Western Pacific

LISTING NEML MEDICINES ON HAQ SCORES
43
Discussion
The number of medications used to treat ischemic heart disease, cerebrovascular disease
and hypertensive heart disease included in national essential medicines lists was associated with
amenable mortality but the association was not present when country characteristics such as
health spending were accounted for.
Our research suggests that increases in a country’s health expenditure may improve HAQ
scores for cardiovascular disease. Fullman et al., (2018) found that health spending per capita
was strongly correlated with HAQ Index performance, however there was a large variation in
score within similar levels of spending (Fullman et al., 2018). Government spending as a fraction
of total health spending was also positively correlated with HAQ Index performance (Fullman et
al., 2018). Per-capita health expenditure is inadequate to pay for basic healthcare interventions in
some low-income countries (Backman et al., 2008; Mendis & Banerjee, 2010). For the countries
included in this study, 62 countries’ (of the 131 total countries; one country had no data) per-
capita government expenditure on health was less than the minimum required for basic effective
public-health system (Backman et al., 2008). A modest increase in public spending, efficient
resource use and an investment in prevention programs is necessary for addressing inequity in
healthcare (Mendis & Banerjee, 2010). It is also possible that higher healthcare spending would
allow countries to purchase a better selection of medicines which may, in turn, lead to better
health outcomes.
We found that prevalence of cardiovascular disease was significantly associated with
HAQ score in all of the adjusted regression models. This finding indicates that higher prevalence
of cardiovascular disease was associated with a lower HAQ score for each cause. Life
expectancy was also significantly associated with HAQ score for cerebrovascular disease and

LISTING NEML MEDICINES ON HAQ SCORES
44
hypertensive heart disease in the multivariate regression models. Life expectancy and prevalence
have similar individual and societal level risk factors underpinning them, including the social
determinants of health. The social determinants of health can impact both prevalence and life
expectancy but they may also be independently related to HAQ score, however we were unable
to find a measure of the social determinants of health that could be tested in the regression.
Many studies have linked cardiovascular disease to the social determinants of health (Havranek
et al., 2015; Jeemon & Reddy, 2010; Martínez-García et al., 2018; Mendis & Banerjee, 2010).
An individual’s social status including income, education and literacy, housing and living
conditions, employment, social exclusion and access to other health care services can influence
behavioural risk factors for the development of cardiovascular disease and subsequent outcomes
related to cardiovascular disease (Mendis & Banerjee, 2010). We suspect that barriers within the
healthcare system, driven by the social determinants of health, are particularly important for
cardiovascular health. For example, inequity exist within the implementation of cost-effective
interventions and the provision of care for cardiovascular disease predominantly in low-income
countries where health systems are may not be adequately equipped for providing chronic
disease care (Mendis & Banerjee, 2010).
Other factors, such as quality of care, may impact mortality from cardiovascular disease. A study
of 137 low- and middle-income countries found that amenable mortality outcomes were
predominantly due to poor quality healthcare (84% of cardiovascular deaths amenable to
healthcare), while the remaining 16% was due to non-utilization of healthcare (Kruk et al.,
2018). This study shows that cardiovascular deaths for people entering the healthcare system are
predominantly driven by poor quality of care. Therefore, quality of care, may account for some

LISTING NEML MEDICINES ON HAQ SCORES
45
of the observed differences in amendable mortality and this would attenuate any real relationship
between medicine selection and health outcomes.
Strengths and Limitations
This was the first study we are aware of to compare NEML medications listings for
cardiovascular diseases on a large scale.
As a cross-sectional associational study, it would inappropriate to draw causal
conclusions about a relationship between medicine coverage scores and HAQ scores. Studying
these associations over time may help solidify the conclusions drawn in this cross-sectional
study.
Applying a global medicine coverage score calculation represents a number of
challenges. The score does not account for medications that are therapeutically interchangeable
within a class; therefore, only one medication in the class needs to be present for treatment, and
the others are redundant. In the medicine coverage score calculations we did not take into
account equivalence therefore countries that listed multiple equivalent medicines in a class
would have received additional points for each drug listed. However, listing more than one
medicine in a class can be beneficial in certain circumstances, for example in the case of drug
recalls or shortages. In addition, there are no guidelines for the number of medicines needed in a
class for proper coverage so we opted to include any that were listed in the country score.
Although there are limitations to creating a medicine coverage score, this approach allowed for
an overall score that could be compared across many countries.
For the HAQ Index it is possible that misclassifications of disease codes and causes of
death occurred. Also the database does not capture substantial inequalities in personal healthcare

LISTING NEML MEDICINES ON HAQ SCORES
46
access and quality across geographic regions or socioeconomic status. Further details about
limitations for the HAQ score calculations can be found in the article by Fullman et al., (2018).
The GEM database captured the most recent NEMLs in the WHO repository however, it is
possible that a more recent NEML existed, and data extraction was liable to errors; further details
can be found in the article by Persaud et al., (2019).
Future research
Future research could study the associations over time to better quantify the association
between tested variables. In addition, future research may also consider how the social
determinants of health perpetuate cycles of inequity within the health system and better measure
them.
Conclusion
The number of medicines relevant to cardiovascular disease included in NEMLs is associated
with amenable cardiovascular mortality but this association is not present when accounting for
country attributes such as national healthcare spending. Other country attributes appear to be
more related to cardiovascular deaths amenable to healthcare.

LISTING NEML MEDICINES ON HAQ SCORES
47
Chapter 4. Additional Analysis
Additional Results
In addition to the results in the manuscript, a medicine class score was calculated for the
thesis to determine if countries listed at least one medication per therapeutic class. Medicines
from several therapeutic classes were present in the list of medicines used to treat ischemic heart
disease, cerebrovascular disease and hypertensive heart disease. For all causes, therapeutic
classes present were: cardiac therapy, antihypertensives, diuretics, beta blocking agents, calcium
channel blockers, agents acting on the renin-angiotensin system and lipid modifying agents. For
ischemic heart there was one additional class: vasoprotectives. Three countries (Democratic
Peoples Republic of Korea, Somalia and Syrian Arab Republic) were excluded from the
regression analysis because they were missing values for healthcare expenditure.
Ischemic Heart Disease.
Medicine class analysis. For ischemic heart disease, class coverage scores ranged from 12.5%
to 100%. Table 8 reports the results of the unadjusted linear regression model showing that
listing therapeutic classes for ischemic heart disease only explained 0.1% of the variation in the
HAQ score (R2= 0.001). Figure 5 shows the unadjusted relationship between variables by
regions, with the size of the bubbles representing per capita health expenditure. An adjusted
linear regression model showed that approximately 17% of differences in the HAQ score for
ischemic heart disease (R2= 0.173) were explained by listing therapeutic classes for ischemic
heart disease along with the four covariates (Table 8). The small correlation between HAQ score
and class coverage score (r= -0.032) confirms little relationship between these variables for
ischemic heart disease, however other variables in the adjusted analysis showed an association
with HAQ scores. Other variables in the adjusted analysis showed a significant association with

LISTING NEML MEDICINES ON HAQ SCORES
48
HAQ scores. Health expenditure was associated with a 0.012 point increase in HAQ score for
each additional per capita dollar (p<0.001) and prevalence of ischemic heart disease was
associated with a 0.007 point decrease in HAQ score for each additional 100, 000 people
diagnosed with ischemic heart disease (p<0.001).

LISTING NEML MEDICINES ON HAQ SCORES
49
Table 8. Ischemic Heart Disease: Class Coverage Score
Variable B
95% CI lower
bound
95% CI upper
bound Beta P-value
Pearson
correlation
Unadjusted Class Coverage Score -5.328 -34.614 23.958 -0.032 0.719 -0.032
Adjusted Class Coverage Score -13.843 -44.150 16.464 -0.081 0.368 -0.016
Health Expenditure 0.012 0.006 0.018 0.493 <0.001 0.232
Population 1.211E-06 0 0 0.011 0.9 -0.008
Life Expectancy 0.226 -0.498 0.95 0.077 0.537 0.093
Prevalence -0.007 -0.01 -0.003 -0.464 <0.001 -0.108
Note: R2unadjussted = 0.001 (F = 0.130, (df: 130), p =0.719). R2
adjussted = 0.173 (F = 5.009, (df: 125), p <0.001)
Figure 5. Ischemic Heart Disease: Class Coverage Score
0
20
40
60
80
100
0% 20% 40% 60% 80% 100%
HA
Q S
core
Class Coverage Score
Ischemic Heart Disease
Africa
Eastern Mediterranean
Europe
South-East Asia
The Americas
Western Pacific

LISTING NEML MEDICINES ON HAQ SCORES
50
Cerebrovascular Disease.
Medicine class analysis. For cerebrovascular disease, class coverage scores ranged from 0% to
100%. Table 9 reports the results of the unadjusted linear regression model showing that listing
therapeutic classes for cerebrovascular disease explained approximately 2% of the variation in
the HAQ score (R2= 0.023). Figure 6 shows the unadjusted relationship between variables by
regions, with the size of the bubbles representing per capita health expenditure. An adjusted
linear regression model showed that approximately 44% of differences in the HAQ score for
cerebrovascular disease (R2= 0.435) were explained by listing therapeutic classes for
cerebrovascular disease along with the four covariates (Table 9). The small correlation (r=
0.152) between HAQ score and class coverage score confirms little relationship between these
variables for cerebrovascular disease, however other variables in the adjusted analysis showed a
significant association with HAQ scores. Health expenditure was associated with a 0.015 point
increase in HAQ score for each additional per capita dollar (p<0.001), life expectancy was
associated with a 0.64 point increase with each additional year of life (p=0.026) and prevalence
of cerebrovascular disease was associated with a 0.008 point decrease in HAQ score for each
additional 100, 000 people diagnosed with cerebrovascular disease (p=0.001).

LISTING NEML MEDICINES ON HAQ SCORES
51
Table 9. Cerebrovascular Disease: Class Coverage Score
Variable B
95% CI
lower bound
95% CI
upper bound Beta P-value
Pearson
correlation
Unadjusted Class Coverage Score 20.692 -2.671 44.055 0.152 0.082 0.152
Adjusted Class Coverage Score -2.051 -23.162 18.16 -0.018 0.811 0.141
Health Expenditure 0.015 0.01 0.019 0.622 <0.001 0.609
Population -4.017E-06 0 0 -0.037 0.597 -0.092
Life Expectancy 0.64 0.079 1.201 0.229 0.026 0.476
Prevalence -0.008 -0.012 -0.003 -0.29 0.001 0.185
Note: R2unadjussted = 0.023 (F = 3.071, (df: 130), p =0.082). R2
adjussted = 0.435 (F = 18.487, (df: 125), p <0.001)
Figure 6. Cerebrovascular Disease: Class Coverage Score
0
20
40
60
80
100
0% 20% 40% 60% 80% 100%
HA
Q S
core
Class Coverage Score
Cerebrovascular Disease
Africa
Eastern Mediterranean
Europe
South-East Asia
The Americas
Western Pacific

LISTING NEML MEDICINES ON HAQ SCORES
52
Hypertensive Heart Disease
Medicine class analysis. For hypertensive heart disease, medicine coverage scores
ranged from 0% to 100%. Table 10 reports the results of the unadjusted linear regression model
showing that listing therapeutic classes for hypertensive heart disease explained approximately
0.7% of the variation in the HAQ score (R2= 0.007). Figure 7 shows the unadjusted relationship
between variables by regions, with the size of the bubbles representing per capita health
expenditure. The results of the adjusted analysis showed that approximately 45% of differences
in the HAQ score for hypertensive heart disease (R2= 0.44.8) were explained by listing
therapeutic classes for hypertensive heart disease along with the four covariates (Table 10). The
small correlation between HAQ score and class coverage score (r = 0.084) confirms little
relationship between these variables for hypertensive heart disease, however other variables in
the adjusted analysis showed a significant association with HAQ scores. Health expenditure was
associated with a 0.009 point increase in HAQ score for each additional per capita dollar
(p<0.001), life expectancy was associated with a 1.429 point increase with each additional year
of life (p<0.001) and prevalence of hypertensive heart disease was associated with a 0.041 point
decrease in HAQ score for each additional 100, 000 people diagnosed with hypertensive heart
disease (p<0.001).

LISTING NEML MEDICINES ON HAQ SCORES
53
Table 10. Hypertensive Heart Disease: Class Coverage Score
Variable B
95% CI
lower bound
95% CI
upper bound Beta P-value
Pearson
correlation
Unadjusted Class Coverage Score 13.277 -14.112 40.667 0.084 0.339 0.084
Adjusted Class Coverage Score -4.736 -26.334 16.862 -0.03 0.665 0.077
Health Expenditure 0.009 0.005 0.013 0.378 <0.001 0.535
Population 1.965E-06 0 0 0.018 0.795 -0.01
Life Expectancy 1.429 0.881 1.977 0.505 <0.001 0.548
Prevalence -0.041 -0.058 -0.023 -0.367 <0.001 0.071
Note: R2unadjussted = 0.007 (F = 0.92, (df: 130), p =0.339). R2
adjussted = 0.448 (F = 19.455, (df: 125), p <0.001)
Figure 7. Hypertensive Heart Disease: Class Coverage Score
0
20
40
60
80
100
0% 20% 40% 60% 80% 100%
HA
Q S
core
Class Coverage Score
Hypertensive Heart Disease
Africa
Eastern Mediterranean
Europe
South-East Asia
The Americas
Western Pacific

LISTING NEML MEDICINES ON HAQ SCORES
54
Changes from Proposal
In the original proposal, three databases were used to derive the list of medicines used to
treat ischemic heart disease, cerebrovascular disease and hypertensive heart disease. However we
were unable to find internationally recognized guidelines that dictate which medicines should be
used for these conditions; it was felt that guidelines endorsed by the WHO (Prevention and
Control of Non-communicable Diseases: Guidelines for primary health care in low-resource
settings, WHO Package of Essential Non communicable (PEN) Diseases Interventions for
Primary Health Care in Low-Resource Settings, Technical Package for cardiovascular disease
management in primary health care- evidence-based treatment protocols and Tackling NCDs:
“Best Buys” and other recommended interventions for the prevention and control of non-
communicable diseases) were a more reliable and rigorously composed source of information, so
they were used instead.
Some covariates were added or removed from the original proposal. The original
proposal included NEML year, geographic region, SDI, GDP, health expenditure, population
size, age distribution, sex distribution, and life expectancy. Prevalence, separated by cause
(ischemic heart disease, cerebrovascular disease and hypertensive heart disease), per 100,000
was added as a covariate to the final regression because prevalence is a measure of disease
burden and it was felt that prevalence may give us an idea of availability and quality of
cardiovascular care in a country.
Age and sex distribution were removed because the data was grouped and we were
unable to separate it for the analysis. NEML year was removed because countries are responsible
for updating their NEML on a regular basis therefore, they should be held to the standard of the

LISTING NEML MEDICINES ON HAQ SCORES
55
most recent guidelines for treatment of cardiovascular disease. SDI and GDP both measured
income; SDI was chosen for removal because it also measured education and infant mortality,
which were not likely related to cardiovascular disease outcomes. GDP and healthcare
expenditure were also highly correlated; we could not include both for fear that the colinearity
may influence the regression model. We ran both GDP and healthcare expenditure in the
regression model and there was not much difference between them; following the lead of
Fullman et al., (2018) we chose to include health expenditure.

LISTING NEML MEDICINES ON HAQ SCORES
56
Chapter 5. Discussion, Limitations and Conclusion
Discussion
Summary of Findings. In the unadjusted analysis listing medicines used to treat
cerebrovascular disease and hypertensive heart disease was associated with HAQ scores. In the
adjusted analysis, listing medicines used to treat ischemic heart disease, cerebrovascular disease
and hypertensive heart disease was not associated with HAQ scores when accounting for country
characteristics. Disease prevalence and health expenditure were significantly associated with
HAQ scores for all causes (ischemic heart disease, cerebrovascular disease and hypertensive
heart disease). In the medicine class analysis most countries listed medicines in each of the
researched medicine classes. In the adjusted analysis we were able to explain 45% at most of the
dependent variable, HAQ score, therefore variables such as the social determinants of health
likely contribute to amenable mortality outcomes.
Social Determinants of Health. Many studies have linked cardiovascular disease to the
social determinants of health (Havranek et al., 2015; Jeemon & Reddy, 2010; Martínez-García et
al., 2018; Mendis & Banerjee, 2010). Risk factors for cardiovascular disease are tobacco
consumption, high blood pressure, high cholesterol and diabetes (Mendis & Banerjee, 2010;
Yusuf, Reddy, Ôunpuu, & Anand, 2001), yet other factors can increase the risk of cardiovascular
disease including, low socioeconomic status, diet, physical inactivity, obesity, age, sex, family
history and insulin resistance. (Mendis & Banerjee, 2010) An individual’s social status including
income, education and literacy, housing and living conditions, employment, social exclusion and
other health care services can influence behavioural risk factors, the development of
cardiovascular disease and subsequent outcomes, including mortality, related to cardiovascular
disease (Mendis & Banerjee, 2010). The social determinants of health can impact cardiovascular

LISTING NEML MEDICINES ON HAQ SCORES
57
mortality based on both individual and societal factors; these factors can also impact life
expectancy and the prevalence of cardiovascular disease.
Socioeconomic status. Socioeconomic status encompasses wealth and income, education,
employment and other factors. (Havranek et al., 2015) Like many other diseases, there is a social
gradient for cardiovascular disease with people who are of low socioeconomic status
experiencing more incidence and mortality of cardiovascular disease particularly in high income
countries. (Mendis & Banerjee, 2010) They also experience worse health outcomes after
cardiovascular events such as stroke or myocardial infarction (Kapral, Wang, Mamdani, & Tu,
2002; Salomaa et al., 2001). Having a stroke or myocardial infarction leads to a diagnosis of
cerebrovascular disease or ischemic heart disease.
There are several interconnected reasons people of low socioeconomic status experience worse
health outcomes. Education is one of the most important predictors of cardiovascular disease
outcomes (Rosengren et al., 2019; Winkleby, Jatulis, Frank, & Fortmann, 1992). People who are
less educated are more likely to exhibit negative health behaviors like smoking, which accounted
for the widening of an existing social difference in cardiovascular risk (Osler et al., 2000). It is
important that people are in a position to receive preventative advice, understand it and act upon
it; this can be accomplished when people receive at least a primary education (Mendis &
Banerjee, 2010). Education is interconnected with other factors of socioeconomic status, for
example education can lead to better employment and thus more financial stability (Hahn &
Truman, 2015) There are many different factors acting on individual’s ability to achieve greater
education, for example government policies about the provision of education, or ability to pay.

LISTING NEML MEDICINES ON HAQ SCORES
58
Employment is an important contributor to cardiovascular health, however it can contribute both
positively and negatively depending on the type of employment. Employment can lead to higher
income which leads to better health (The World Health Organization, n.d.-a) because income
provides access to resources such as healthier foods, safe environments and healthcare. (Hahn &
Truman, 2015) Unemployment can contribute to poor health by increasing risk profiles for
cardiovascular disease (P. Zagozdzon, Parszuto, Wrotkowska, & Dydjow-Bendek, 2014); it was
also found to double the risk of cardiovascular mortality (Pawel Zagozdzon, Zaborski, &
Ejsmont, 2009). Employment can also be a source of stress, which is associated with
cardiovascular disease (Kivimäki & Kawachi, 2015). In addition, physically hazardous working
conditions along with low job control were the driving factors behind an association between
occupational class and less than good perceived general health. (Schrijvers, Dike Van De Mheen,
Stronks, & Mackenbach, 1998)
Income level is important for health both directly through being able to afford shelter and
healthy food, and indirectly by reducing stress etc. Specifically, cost of care can prevent people
of low socioeconomic status from accessing healthcare (Kapral et al., 2002; Kristiansson et al.,
2009). In 2015, 1.4 billion people incurred catastrophic health spending, which is defined as out-
of-pocket spending that exceeds 10% of the household budget, which pushed 371.7 million
people below the poverty line. (The World Health Organization & The World Bank, 2019) Out
of pocket spending is a source of socioeconomic inequality because healthcare spending leads to
service delivery only if the individual can pay. (The World Health Organization & The World
Bank, 2019) Research shows that wealthier populations are more likely to seek healthcare when
they need it (Makinen et al., 2000); inability to seek care can lead to worse health outcomes.
Poor health outcomes can perpetuate the cycle of poverty because paying medical bills can

LISTING NEML MEDICINES ON HAQ SCORES
59
increase the risk of impoverishment and illness may result in productivity loss and loss of
income (Mendis & Banerjee, 2010; The World Health Organization & The World Bank, 2019).
We know that socioeconomic status can impact health outcomes between and within
countries. Areas where there are many people of low socioeconomic status may experience
worse health outcomes for the reasons listed above. Socioeconomic status may act as a
confounder that neither the HAQ score or our regression model was able to account for due to
the lack of a standardized measure for included countries.
Health system barriers. Equity gaps exist within the implementation of cost-effective
interventions and the provision of care for cardiovascular disease. They are particularly relevant
for low-income countries where health systems are improperly equipped for providing chronic
disease care. (Mendis & Banerjee, 2010) A study of 137 low- and middle-income countries and
classified cardiovascular deaths amenable to healthcare into two categories, deaths due to poor
quality of care and those related to non-utilization of healthcare. (Kruk et al., 2018) To
differentiate poor quality care they assumed that once users seek care correct management and
retention in care is the system’s responsibility. They found that amenable mortality outcomes
were predominantly due to poor quality healthcare. Specifically, for cardiovascular disease, 84%
of mortality was due to poor quality care, while the remaining 16% of amenable deaths was due
to non-utilization of healthcare, (Kruk et al., 2018) suggesting that quality of care is the biggest
driver of mortality for causes amenable to healthcare. For example in Kenya, cardiovascular
medicines can only be prescribed by physicians, (Vedanthan et al., 2016) however it can be
difficult for patients to access physicians due to a lack of effective referral networks (Mercer et
al., 2019) and a shortage of physicians making it difficult to contend with the disease burden.

LISTING NEML MEDICINES ON HAQ SCORES
60
(Vedanthan et al., 2016) Therefore, patients may be entering the healthcare system but not
receiving proper cardiovascular care.
In many countries the per-capita expenditure is inadequate to pay for basic healthcare
interventions; the poor suffer the most from the high cost of diagnostics, drugs and
inaccessibility of healthcare and thus have worse health outcomes. (Mendis & Banerjee, 2010)
For the countries included in this study 60 countries’ (one country had no data) per capita
government expenditure on health was less than the minimum required for basic effective public-
health system. (Backman et al., 2008) In our research, we found that health expenditure was
related to cardiovascular deaths that are amenable to healthcare. Possible explanations for this
observation are healthcare spending may directly relate to medicine listing because medicines
can be costly, particularly newer and patented medicines, therefore countries that spend more
money on medicines may list more medicines and higher cost medicines; or perhaps this trend is
explained by countries inability to spend on other basic healthcare interventions. Fullman et al.,
(2018) also found that for the overall HAQ Index score, encompassing all 32 causes of amenable
mortality, healthcare expenditure was related to better performance. Our research suggests that
increases in a country’s health expenditure may improve healthcare access and quality scores for
cardiovascular disease, which is consistent with the previous research (Fullman et al., 2018;
Mendis & Banerjee, 2010)
In order to address equity gaps in low income countries, a modest increase in public
spending, efficient resource use and an investment in prevention programs is necessary. (Mendis
& Banerjee, 2010) Increasing health expenditure is not necessarily feasible because resources are
finite. In our statistical analysis, health expenditure and GDP were associated with each other, so
much so that GDP had to be removed from the regression. This relationship shows that a

LISTING NEML MEDICINES ON HAQ SCORES
61
country’s ability to spend on healthcare is related to their overall country income. However, this
is a general trend, and HAQ index performance showed a large variation in score within similar
levels of spending (Fullman et al., 2018). Perhaps variations within similar levels of spending are
caused by the implementation of cost-effective interventions and although countries can not
increase spending they could organize healthcare more efficiently. Healthcare dollars spent in
areas other than medicine provision may be more important investments for preventing
cardiovascular deaths considering the relationship between health expenditure and HAQ score.
Medicine access. From previous research findings, medicine access is effected by both
the quality of healthcare and non-utilization of healthcare. (Kruk et al., 2018) People may not
receive prescription medicine as required due to either not being appropriately prescribed or not
being able to access medicines because of cost or other systematic barriers. A previous study
echoed this sentiment with their finding that medicine selection was not the limiting step in
access because most countries listed medicines in each therapeutic categories. (Bazargani et al.,
2018)
The purpose of listing medicines on NEMLs is to ensure the population it serves has
reasonable access to listed medicines and although countries may have adequate coverage of
cardiovascular medicines on their NEML, listing medicines does not necessarily guarantee
access. Research found that essential medicines remain largely inaccessible particularly in low-
and middle-income countries (Abegunde, 2011; Vialle-Valentin, Serumaga, Wagner, & Ross-
Degnan, 2015). Access to essential medicines has been recognized by many as part of the right to
health, and it has been added as an indicator to measure the “progress in progressive realization
of the right to health”. (Hogerzeil & Mirza, 2011) The concept underpinning essential medicines
of equity, solidarity and social justice are in line with the principles of human rights (Hogerzeil

LISTING NEML MEDICINES ON HAQ SCORES
62
& Mirza, 2011). However, NEMLs are not necessarily enforceable in court, meaning there is not
necessarily a legal right to access NEML listed medicines; there is a move towards making them
enforceable in order to guarantee people access to the listed medicines (Hogerzeil & Mirza,
2011). Unfortunately, we were unable to find a reliable measure of medicine access measured
globally that we could test in our regression analysis, we had to assume that if a medicine was
listed on an NEML, people were able to access them as per the definition of an essential
medicine (The World Health Organization, 2004).
From our results, we believe that simply having access to medicines may not be enough
to overcome the negative impact of the social determinants of health on cardiovascular
outcomes. Our research findings are consistent with health expenditure (and related social
spending) both directly affecting medicine listing and cardiovascular outcomes; and indirectly
affecting cardiovascular outcomes via the social determinants of health. We were unable to
include the social determinants of health as a covariate because the data is not available for a
large number of countries. Health expenditure and the size of the economy (measured by GDP)
could also similarly indirectly affect amenable mortality through other factors.
Results in Context
This was the first study we could find to compare NEML medicines listings for
cardiovascular diseases on a large scale. Previous research focused on the content of the lists to
determine if included NEMLs met minimum standards for treatment of cardiovascular disease
using both the WHO Model List and international guidelines (Bazargani et al., 2018; Mehrtash et
al., 2018). The authors found mixed results; the first study found that countries’ NEML met
coverage standards for cardiovascular disease treatment (Bazargani et al., 2018) and the other
found that they did not. (Mehrtash et al., 2018) These studies looked at different groupings of

LISTING NEML MEDICINES ON HAQ SCORES
63
countries and used different benchmarks for coverage standards therefore mixed results can be
explained.
Our research built upon this work by assessing the value of listing cardiovascular
diseases medicines on amenable mortality outcomes. Our research found an association between
listing cardiovascular disease medicines and HAQ scores (measure of amenable mortality) in an
unadjusted linear regression model however we did not find an association when covariates were
added to the regression model. However we did find a relationship between healthcare
expenditure and HAQ scores for cardiovascular disease, therefore the association is likely more
complicated.
Limitations
Underlying Data. The study has several limitations particularly due to the source of
information gathered. The HAQ Index score as a measure of amenable mortality was subject to
several key limitations. First, the risk-standardization procedure may not represent all possible
risk-outcome pairs, for example, they did not look at determinants of neonatal disorders. Second,
there are limitations within the GBD cause of death estimation, which is used to calculate HAQ
scores. However GBD updates their data annually and aims to improve their comparative risk
assessment, which will then improve future HAQ score calculations. Third, the HAQ score does
not directly capture causes amenable to healthcare without substantial mortality rates (eg:
depression); therefore the measure could be improved by calculating the effects of healthcare
access and quality for non-fatal health outcomes. Fourth, it is possible that misclassifications of
disease codes and causes of death occurred; this can affect the results because it may influence
the total number of deaths that are included for each cause of death. Lastly, the database does not
capture substantial inequalities in personal healthcare access and quality across geographic

LISTING NEML MEDICINES ON HAQ SCORES
64
regions or socioeconomic status. Despite the limitations the Fullman et al., (2018) have stated
that the HAQ scores are a more robust indicator of overall healthcare access and quality than
previous measures. Previous research in this area focused on specific countries or regions
therefore their research was able to provide a comparison between countries on a much larger
scale, which can help countries prioritize healthcare reform and monitor overall progress. With
each iteration the measure is updated and methods are improved and although the HAQ score is
not a perfect measure, it provides a basis for comparison between countries and over time.
The second data set used was the GEM Database, which contains NEMLs that were
found in the WHO essential medicine list repository. The authors used the most up to date
NEML’s listed in the WHO repository at the time of extraction (2017), but it is possible that the
NEML lists in the repository were not the most recent NEML for a country because it is the
country’s responsibility to update the repository. Finally, the database was liable to errors
because country documents were extracted by hand, documents in the repository had to be
translated, medicine names were not standardized, and judgments had to be made in ambiguous
cases. To attempt to mitigate as many errors as possible, data was abstracted by two individuals
to reduce the likelihood of errors. Now that the database is publically available, future updated
can be carried out be countries themselves to reduce potential errors.
Methodology. In the process of HAQ score creation, researchers risk and age standardized
death rates (Fullman et al., 2018). It is possible that population and prevalence are related to the
dependent variable because they were factored into the HAQ calculation; however the equation
standardized these variables, therefore we added them back in as covariates to see if difference in
these variables were associated with HAQ score performance.

LISTING NEML MEDICINES ON HAQ SCORES
65
The WHO states that an essential medicine list should consist of a limited number of medicines.
(The World Health Organization, 2004) The purpose of this recommendation is to ensure that
countries have enough medicines to meet their national priority conditions, while not including
an excessive number of medicines, to ensure reasonable supply and access to listed medicines.
We did not consider the length of the NEMLs in the analysis; the first analysis calculated a
medicine coverage score based on the number of medicines listed on a countries’ NEML. If the
total number of medicines on the list was included in the medicine coverage score calculations,
we could take into account the WHO recommendations of limited number of medicines and
reward countries, within the scoring technique, for maintaining a limited list length.
Another critique of the scoring calculation used, is that it does not account for medicines
that are therapeutically interchangeable within a class; therefore, only one medicine in the class
needs to be present for treatment, and the others are redundant. This idea was taken from the
WHO Model List where only one drug in a class was listed and they stated that other in the class
can be used alternatively, therefore countries may only need to list one medicine in a class for
sufficient coverage. In the medicine coverage score calculations we did not take into account
equivalence therefore countries that listed multiple equivalent medicines in a class would have
received additional points for each drug listed. We tried to counteract this limitation by
calculating a class coverage score to determine if countries listed at least one medicine per class.
Although it is important to consider overall number of medicines listed on NEMLs, there is no
recommended number of medicines that should be listed, therefore we could not compare
countries by this metric. Future work may improve these methods by collapsing medicine classes
only when indicated as therapeutically equivalent by a guideline (the current method grouped
them by ATC code), where countries would receive a point for listing one of the medicines.

LISTING NEML MEDICINES ON HAQ SCORES
66
Conclusion
Listing more medicines was associated with HAQ score in a univariate linear regression
however the relationship was no longer significant after accounting for country attributes such as
healthcare expenditure. However, some country attributes were significantly related to HAQ
score. Approximately half of the variation in HAQ score was explained by the tested variables
therefore, there are other drivers of cardiovascular deaths amenable to healthcare that we were
unable to explore because they are unknown or not currently measured globally.
Future Research
This research was based on the assumption that listing cardiovascular medicines meant
that the medicine was available in the listing country, however we know that this is not always
the case, therefore more robust measures of essential medicine access should be measured
globally. Also, cardiovascular disease mortality rates were used as a surrogate marker for
healthcare access and quality; future research could measure healthcare access or quality using
other metrics such as affordability of care or treatment follow-up in order to better determine
targets for health system improvements. Finally, future research may also consider how the
social determinants of health perpetuate cycles of inequity within the health system.
Funding
No funding was required. All data sources are publically available at no charge.
Ethics
Ethics approval was not needed for this project because the information is publically
available.

LISTING NEML MEDICINES ON HAQ SCORES
67
References
Abegunde, D. (2011). Essential Medicines for Non-Communicable Diseases (NCDs), 1–31.
American Heart Association. (n.d.). To be a relentless force for a world of longer, healthier lives.
Retrieved October 15, 2019, from https://www.heart.org/
American Heart Association. (2019). Cardiac Medications. Retrieved October 5, 2019, from
https://www.heart.org/en/health-topics/heart-attack/treatment-of-a-heart-attack/cardiac-
medications
Backman, G., Hunt, P., Khosla, R., Jaramillo-Strouss, C., Fikre, B. M., Rumble, C., … Vladescu,
C. (2008). Health systems and the right to health: an assessment of 194 countries. The
Lancet. https://doi.org/10.1016/S0140-6736(08)61781-X
Barber, R. M., Fullman, N., D Sorensen, R. J., Bollyky, T., McKee, M., Nolte, E., …
Collaborators, Q. (2017). Healthcare Access and Quality Index based on mortality from
causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel
analysis from the Global Burden of Disease Study 2015. Lancet, 390, 231–266.
https://doi.org/10.1016/S0140-6736(17)30818-8
Bazargani, Ewen, M., De Boer, A., Leufkens, H. G. M., & Mantel-Teeuwisse, A. K. (2014).
Essential medicines are more available than other medicines around the globe. PLoS ONE,
9(2), 1–7. https://doi.org/10.1371/journal.pone.0087576
Bazargani, Ugurlu, M., de Boer, A., Leufkens, H. G. M., & Mantel-Teeuwisse, A. K. (2018).
Selection of essential medicines for the prevention and treatment of cardiovascular diseases
in low and middle income countries. BMC Cardiovascular Disorders, 18, 126.

LISTING NEML MEDICINES ON HAQ SCORES
68
https://doi.org/10.1186/s12872-018-0858-5
Cousineau, D., & Chartier, S. (2010). Outliers detection and treatment: a review. International
Journal of Psychological Research, 3(1), 58. https://doi.org/10.21500/20112084.844
Data transformations - Handbook of Biological Statistics. (n.d.). Retrieved October 17, 2019,
from http://www.biostathandbook.com/transformation.html
Dhingra, R., & Vasan, R. S. (2012). Age as a Cardiovascular Risk Factor. Medical Clinics of
North America. https://doi.org/10.1016/j.mcna.2011.11.003
Fields, A. (2018). Discovering Statistics using IBM SPSS Statistics (5th ed.). Thousand Oaks,
California: SAGE Publications.
Fullman, N., Yearwood, J., Abay, S. M., Abbafati, C., Abd-Allah, F., Abdela, J., …
Collaborators, Q. (2018). Measuring performance on the Healthcare Access and Quality
Index for 195 countries and territories and selected subnational locations: a systematic
analysis from the Global Burden of Disease Study 2016. Lancet, 391, 2236–2271.
https://doi.org/10.1016/S0140-6736(18)30994-2
GBD Compare | IHME Viz Hub. (2018). Retrieved September 27, 2018, from
https://vizhub.healthdata.org/gbd-compare/
Global Health and Data Exchange. (2018). Global Burden of Disease Study 2015 (GBD 2015)
Socio-Demographic Index (SDI) 1980–2015 | GHDx. Retrieved December 2, 2018, from
http://ghdx.healthdata.org/record/global-burden-disease-study-2015-gbd-2015-socio-
demographic-index-sdi-1980–2015
Goff, D. C., Lloyd-Jones, D., Bennett, G., Coady, S., D’Agostino, R., Gibbons, R., … Tomaselli,

LISTING NEML MEDICINES ON HAQ SCORES
69
G. (2014). 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report
of the American College of Cardiology/American Heart Association Task Force on Practice
Guidelines. Journal of the American College of Cardiology, 63(25).
https://doi.org/10.1016/j.jacc.2013.11.005
Hahn, R. A., & Truman, B. I. (2015). Education improves public health and promotes health
equity. International Journal of Health Services.
https://doi.org/10.1177/0020731415585986
Havranek, E. P., Mujahid, M. S., Barr, D. A., Blair, I. V., Cohen, M. S., Cruz-Flores, S., …
Yancy, C. W. (2015). Social Determinants of Risk and Outcomes for Cardiovascular
Disease. Circulation. https://doi.org/10.1161/cir.0000000000000228
Hogerzeil, H. V, & Mirza, Z. (2011). The World Medicines Situation 2011: Access to essential
Medicines as Part of the Right to Health. Geneva. Retrieved from
http://apps.who.int/medicinedocs/documents/s18772en/s18772en.pdf
Institute for Health Metrics and Evaluation. (2017). GBD Compare | IHME Viz Hub. Retrieved
December 3, 2018, from https://vizhub.healthdata.org/gbd-compare/
Jeemon, P., & Reddy, K. S. (2010). Social determinants of cardiovascular disease outcomes in
Indians. Indian Journal of Medical Research. https://doi.org/10.4103/0971-5916.73415
Kapral, M. K., Wang, H., Mamdani, M., & Tu, J. V. (2002). Effect of socioeconomic status on
treatment and mortality after stroke. Stroke. https://doi.org/10.1161/hs0102.101169
Kivimäki, M., & Kawachi, I. (2015). Work Stress as a Risk Factor for Cardiovascular Disease.
Current Cardiology Reports. https://doi.org/10.1007/s11886-015-0630-8

LISTING NEML MEDICINES ON HAQ SCORES
70
Kristiansson, C., Gotuzzo, E., Rodriguez, H., Bartoloni, A., Strohmeyer, M., Tomson, G., &
Hartvig, P. (2009). Access to health care in relation to socioeconomic status in the
Amazonian area of Peru. International Journal for Equity in Health.
https://doi.org/10.1186/1475-9276-8-11
Kruk, M. E., Gage, A. D., Joseph, N. T., Danaei, G., García-Saisó, S., & Salomon, J. A. (2018).
Mortality due to low-quality health systems in the universal health coverage era: a
systematic analysis of amenable deaths in 137 countries. The Lancet.
https://doi.org/10.1016/S0140-6736(18)31668-4
Laerd Statistics. (2018). Linear Regression Analysis in SPSS Statistics - Procedure, assumptions
and reporting the output. Retrieved December 8, 2018, from
https://statistics.laerd.com/spss-tutorials/linear-regression-using-spss-statistics.php
Mahmić-Kaknjo, M., Jeličić-Kadić, A., Utrobičić, A., Chan, K., Bero, L., & Marušić, A. (2018).
Essential medicines availability is still suboptimal in many countries: a scoping review.
Journal of Clinical Epidemiology, 98, 41–52. https://doi.org/10.1016/j.jclinepi.2018.02.006
Makinen, M., Waters, H., Rauch, M., Almagambetova, N., Bitran, R., Gilson, L., … Ram, S.
(2000). Inequalities in health care use and expenditures: Empirical data from eight
developing countries and countries in transition. Bulletin of the World Health Organization.
https://doi.org/10.1590/S0042-96862000000100006
Martínez-García, M., Salinas-Ortega, M., Estrada-Arriaga, I., Hernández-Lemus, E., García-
Herrera, R., & Vallejo, M. (2018). A systematic approach to analyze the social determinants
of cardiovascular disease. PLoS ONE. https://doi.org/10.1371/journal.pone.0190960

LISTING NEML MEDICINES ON HAQ SCORES
71
Mehrtash, H., Laing, R., & Wirtz, V. J. (2018). Comparative analysis of essential medicines for
cardiovascular diseases in countries of the WHO Eastern Mediterranean Region. Eastern
Mediterranean Health Journal, 24(5), 427–434. https://doi.org/10.26719/2018.24.5.427
Mendis, S., & Banerjee, A. (2010). Equity, social determinants and public health programmes. In
E. Blas & S. Kurup (Eds.) (pp. 31–48). The World Health Organization. Retrieved from
https://apps.who.int/iris/bitstream/handle/10665/44289/9789241563970_eng.pdf?sequence=
1&isAllowed=y
Mercer, T., Njuguna, B., Bloomfield, G. S., Dick, J., Finkelstein, E., Kamano, J., … Akwanalo,
C. (2019). Strengthening referral networks for management of hypertension across the
health system (STRENGTHS) in western Kenya: A study protocol of a cluster randomized
trial. Trials. https://doi.org/10.1186/s13063-019-3661-4
Merriam-Webster. (n.d.). Population | Definition of Population by Merriam-Webster. Retrieved
December 3, 2018, from https://www.merriam-webster.com/dictionary/population
Nolte, E., & Mckee, M. (2004). Does Health Care Save Lives? Avoidable Mortality Revisited.
The Nuffeld Trust, 139. Retrieved from www.nuffieldtrust.org.uk
Osler, M., Gerdes, L. U., Davidsen, M., Bønnum-Hansen, H., Madsen, M., Jørgensen, T., &
Schroll, M. (2000). Socioeconomic status and trends in risk factors for cardiovascular
diseases in the Danish MONICA population, 1982-1992. Journal of Epidemiology and
Community Health. https://doi.org/10.1136/jech.54.2.108
Persaud, N., Jiang, M., Shaikh, R., Bali, A., Oronsaye, E., Woods, H., … Heneghan, C. (2019).
Comparison of essential medicines lists in 137 countries. Bulletin of the World Health

LISTING NEML MEDICINES ON HAQ SCORES
72
Organization. https://doi.org/10.2471/BLT.18.222448
Persaud, N., Jiang, M., Shaikh, R., Bali, A., Oronsaye, E., Woods, H., … Heneghan, C. (2019).
Global Essential Medicines. Retrieved November 29, 2019, from
https://figshare.com/articles/GlobalEssentialMedicinesDatabase_xlsx/7814246/1
Rashid, S. (2016). Updating National Essential Medicine Lists A Step-by-Step Advocacy Guide
Updating National Essential Medicine Lists: A Step-by-Step Advocacy Guide. Retrieved
from http://apps.who.int/medicinedocs/documents/s23536en/s23536en.pdf
Rosengren, A., Smyth, A., Rangarajan, S., Ramasundarahettige, C., Bangdiwala, S. I., AlHabib,
K. F., … Yusuf, S. (2019). Socioeconomic status and risk of cardiovascular disease in 20
low-income, middle-income, and high-income countries: the Prospective Urban Rural
Epidemiologic (PURE) study. The Lancet Global Health. https://doi.org/10.1016/S2214-
109X(19)30045-2
Salomaa, V., Palomäki, P., Mustaniemi, H., Kaarsalo, E., Arstila, M., Torppa, J., … Koskinen, S.
(2001). Relation of socioeconomic position to the case fatality, prognosis and treatment of
myocardial infarction events; the FINMONICA MI Register Study. Journal of
Epidemiology and Community Health. https://doi.org/10.1136/jech.55.7.475
Schrijvers, C. T. M., Dike Van De Mheen, H., Stronks, K., & Mackenbach, J. P. (1998).
Socioeconomic inequalities in health in the working population: The contribution of
working conditions. International Journal of Epidemiology.
https://doi.org/10.1093/ije/27.6.1011
The Centers for Disease Control and Prevention. (2015). Behaviors That Increase Risk for Heart

LISTING NEML MEDICINES ON HAQ SCORES
73
Disease. Retrieved October 9, 2018, from https://www.cdc.gov/heartdisease/behavior.htm
The World Bank. (n.d.). GDP (current US$) | Data. Retrieved December 2, 2018, from
https://data.worldbank.org/indicator/NY.GDP.MKTP.CD
The World Health Organization. (n.d.-a). About social determinants of health. Retrieved
December 9, 2019, from https://www.who.int/social_determinants/sdh_definition/en/
The World Health Organization. (n.d.-b). International Statistical Classification of Diseases and
Related Health Problems 10th Revision (ICD-10)-WHO Version for 2016. Retrieved
December 1, 2018, from http://apps.who.int/classifications/icd10/browse/2016/en#/I
The World Health Organization. (2004). WHO Policy Perspectives on Medicines-Equitable
access to essential medicines: a framework for collective action WHO Policy Perspectives
on Medicines Equitable access to essential medicines: a framework for collective action 8.
Retrieved from http://apps.who.int/medicinedocs/pdf/s4962e/s4962e.pdf
The World Health Organization. (2006). Definitions and Metadata. Retrieved from
https://www.who.int/whosis/whostat2006DefinitionsAndMetadata.pdf
The World Health Organization. (2010). Package of Essential Noncommunicable (PEN) Disease
Interventions for Primary Health Care in Low-Resource Settings. Retrieved from
http://www.who.int/cardiovascular_diseases
The World Health Organization. (2011a). Briefing Document: Essential Medicines for Non-
Communicable Diseases ( NCDs ). https://doi.org/10.1371/journal.pmed.1000333
The World Health Organization. (2011b). Briefing Document: Essential Medicines for Non-
Communicable Diseases ( NCDs ). https://doi.org/10.1371/journal.pmed.1000333

LISTING NEML MEDICINES ON HAQ SCORES
74
The World Health Organization. (2012). Prevention and control of noncommunicable diseases :
guidelines for primary health care in low resource settings., 68.
The World Health Organization. (2016a). GHO | By category | Life expectancy and Healthy life
expecancy - Data by country. WHO. Retrieved from
http://apps.who.int/gho/data/node.main.688?lang=en
The World Health Organization. (2016b). HEARTS Technical Package for Cardiovascular
disease management in primary health care. Retrieved from
https://apps.who.int/iris/bitstream/handle/10665/252661/9789241511377-
eng.pdf;jsessionid=A6EF6593B92AE82AEB8C4AD28DE606EA?sequence=1
The World Health Organization. (2016c). WHO | About the GHO. WHO. Retrieved from
https://www.who.int/gho/about/en/
The World Health Organization. (2017a). Noncommunicable Diseases | WHO | Regional Office
for Africa. Retrieved October 3, 2018, from https://afro.who.int/health-
topics/noncommunicable-diseases
The World Health Organization. (2017b). Tackling NCDS - Best Buys. Retrieved from
https://apps.who.int/iris/bitstream/handle/10665/259232/WHO-NMH-NVI-17.9-
eng.pdf;jsessionid=8BC070A284E32E92FA7273189F82E9DD?sequence=1
The World Health Organization. (2017c). The Selection and Use of Essential Medicines :
Executive Summary. WHO Technical Report Series, 2015(March), 1–15.
The World Health Organization. (2017d). WHO Model List of Essential Medicines 20th Edition.
Retrieved from

LISTING NEML MEDICINES ON HAQ SCORES
75
http://www.who.int/medicines/publications/essentialmedicines/20th_EML2017.pdf
The World Health Organization. (2018a). Access to essential medicines and technology.
Retrieved from http://apps.who.int/iris/bitstream/handle/10665/260420/WHO-NMH-NVI-
18.3-eng.pdf?sequence=1
The World Health Organization. (2018b). Essential Medicines and Health Products Information
Portal. Retrieved May 22, 2019, from
http://apps.who.int/medicinedocs/static/PublicSubcollections/National-Essential-Medicines-
Lists-NEMLs-Repository/
The World Health Organization. (2018c). Noncommunicable diseases. Retrieved October 3,
2018, from http://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
The World Health Organization. (2018d). The top 10 causes of death. Retrieved September 26,
2018, from http://www.who.int/en/news-room/fact-sheets/detail/the-top-10-causes-of-death
The World Health Organization. (2018e). WHO | Global Health Observatory (GHO) data.
Retrieved December 2, 2018, from http://www.who.int/gho/en/
The World Health Organization Expert Committee. (2017). The Selection and Use of essential
medicines. (Vol. 1006). Retrieved from
http://apps.who.int/iris/bitstream/10665/42620/1/WHO_TRS_914_eng.pdf
The World Health Organization, & The World Bank. (2019). Global Monitoring Report on
Financial Protection in Health 2019. Retrieved from
https://www.who.int/healthinfo/universal_health_coverage/report/fp_gmr_2019.pdf?ua=1
Vedanthan, R., Tuikong, N., Kofler, C., Blank, E., Kamano, J. H., Naanyu, V., … Fuster, V.

LISTING NEML MEDICINES ON HAQ SCORES
76
(2016). Barriers and facilitators to nurse management of hypertension: A qualitative
analysis from western Kenya. Ethnicity and Disease. https://doi.org/10.18865/ed.26.3.315
Vialle-Valentin, C. E., Serumaga, B., Wagner, A. K., & Ross-Degnan, D. (2015). Evidence on
access to medicines for chronic diseases from household surveys in five low- and middle-
income countries. Health Policy and Planning. https://doi.org/10.1093/heapol/czu107
WHO Collaborating Centre for Drug Statistics Methodology. (n.d.-a). ATC/DDD Index 2018.
WHO Collaborating Centre for Drug Statistics Methodology. (n.d.-b). WHOCC - Structure and
principles. Retrieved December 7, 2018, from
https://www.whocc.no/atc/structure_and_principles/
Winkleby, M. A., Jatulis, D. E., Frank, E., & Fortmann, S. P. (1992). Socioeconomic status and
health: How education, income, and occupation contribute to risk factors for cardiovascular
disease. American Journal of Public Health. https://doi.org/10.2105/AJPH.82.6.816
Yusuf, S., Reddy, S., Ôunpuu, S., & Anand, S. (2001). Global burden of cardiovascular diseases.
Part I: General considerations, the epidemiologic transition, risk factors, and impact of
urbanization. Circulation. https://doi.org/10.1161/hc4601.099487
Zagozdzon, P., Parszuto, J., Wrotkowska, M., & Dydjow-Bendek, D. (2014). Effect of
unemployment on cardiovascular risk factors and mental health. Occupational Medicine.
https://doi.org/10.1093/occmed/kqu044
Zagozdzon, Pawel, Zaborski, L., & Ejsmont, J. (2009). Survival and cause-specific mortality
among unemployed individuals in Poland during economic transition. Journal of Public
Health. https://doi.org/10.1093/pubmed/fdn061

LISTING NEML MEDICINES ON HAQ SCORES
77
Appendix A: Medicines for Cardiovascular Disease
Table 11. Medicines for Ischemic heart Disease
Medicine Name Primary ATC Code
Acebutolol C07AB04
Acenocoumarol B01AA07
Acetylsalicylic acid B01AC06
Alteplase B01AD02
Amiodarone C01BD01
Amlodipine C08CA01
Atenolol C07AB03
Atorvastatin C10AA05
Benazepril C09AA07
Bendrofluazide (Bendroflumethiazide) C03AA01
Betaxolol C07AB05
Bevantolol C07AB06
Bisoprolol C07AB07
Bumetanide C03CA02
Candesartan C09CA06
Captopril C09AA01
Carvedilol C07AG02
Celiprolol C07AB08
Chlorothiazide C03AA04
Chlortalidone (Chlorthalidone) C03BA04
Cilazapril C09AA08
Cilnidipine C08CA14
Clopidogrel B01AC04
Cyclopenthiazide C03AA07
Dalteparin B01AB04
Delapril C09AA12
Digoxin C01AA05
Dopamine C01CA04
Drotrecogin alfa B01AD10
Enalapril C09AA02
Enoxaparin B01AB05
Epanolol C07AB10
Epinephrine (Adrenaline) C01CA24
Eplerenone C03DA04
Eprosartan C09CA02
Esmolol C07AB09

LISTING NEML MEDICINES ON HAQ SCORES
78
Ethyl biscoumacetate B01AA08
Felodipine C08CA02
Fibrinolysin B01AD05
Fluindione B01AA12
Fluvastatin C10AA04
Fosinopril C09AA09
Furosemide C03CA01
Heparin B01AB01
Hydrochlorothiazide C03AA03
Hydromorphone N02AA03
Imidapril C09AA16
Indapamide C03BA11
Irbesartan C09CA04
Isosorbide C01DA
Isosorbide dinitrate C01DA08
Isosorbide mononitrate C01DA14
Isradipine C08CA03
Lacidipine C08CA09
Landiolol C07AB14
Lercanidipine C08CA13
Lidocaine (Lignocaine, Xylocaine) C05AD01
Lisinopril C09AA03
Losartan C09CA01
Lovastatin C10AA02
Manidipine C08CA11
Methylchlorothiazide C03AA
Metoprolol C07AB02
Moexipril C09AA13
Morphine N02AA01
Nadroparin B01AB06
Nebivolol C07AB12
Nicardipine C08CA04
Nifedipine C08CA05
Nilvadipine C08CA10
Nimodipine C08CA06
Nisoldipine C08CA07
Nitrendipine C08CA08
Nitroglycerin (Glyceryl trinitrate) C01DA02
Nitroprusside C02DD01
Olmesartan C09CA
Oxygen V03AN01
Pentaerythritol tetranitrate C01DA05
Perindopril C09AA04

LISTING NEML MEDICINES ON HAQ SCORES
79
Phenprocoumon B01AA04
Plasminogen activator B01AD
Polythiazide C03AA05
Practolol C07AB01
Pravastatin C10AA03
Prourokinase B01AD
Quinapril C09AA06
Ramipril C09AA05
Reteplase B01AD07
Rosuvastatin C10AA07
Simvastatin C10AA01
Spirapril C09AA11
Spironolactone C03DA01
Streptokinase B01AD01
Talinolol C07AB13
Telmisartan C09CA07
Tenecteplase B01AD11
Torsemide C03CA04
Trandolapril C09AA10
Urokinase B01AD04
Valsartan C09CA03
Verapamil C08DA01
Warfarin B01AA03
Zofenopril C09AA15

LISTING NEML MEDICINES ON HAQ SCORES
80
Table 12. Medicines for Cerebrovascular Disease
Medicine Name
Primary ATC
Code
Acebutolol C07AB04
Acenocoumarol B01AA07
Acetylsalicylic acid B01AC06
Alteplase B01AD02
Amiodarone C01BD01
Amlodipine C08CA01
Apixaban B01AF02
Atenolol C07AB03
Atorvastatin C10AA05
Benazepril C09AA07
Bendrofluazide
(Bendroflumethiazide) C03AA01
Betaxolol C07AB05
Bevantolol C07AB06
Bisoprolol C07AB07
Bumetanide C03CA02
Candesartan C09CA06
Captopril C09AA01
Carvedilol C07AG02
Celiprolol C07AB08
Chlorothiazide C03AA04
Chlortalidone (Chlorthalidone) C03BA04
Cilazapril C09AA08
Cilnidipine C08CA14
Clopidogrel B01AC04
Cyclopenthiazide C03AA07
Dabigatran B01AE07
Dalteparin B01AB04
Delapril C09AA12
Digoxin C01AA05
Dipyridamole B01AC07
Drotrecogin alfa B01AD10
Enalapril C09AA02
Enoxaparin B01AB05
Epanolol C07AB10
Eplerenone C03DA04
Eprosartan C09CA02
Esmolol C07AB09
Ethyl biscoumacetate B01AA08

LISTING NEML MEDICINES ON HAQ SCORES
81
Felodipine C08CA02
Fibrinolysin B01AD05
Fluindione B01AA12
Fluvastatin C10AA04
Fosinopril C09AA09
Furosemide C03CA01
Heparin B01AB01
Hydrochlorothiazide C03AA03
Imidapril C09AA16
Indapamide C03BA11
Irbesartan C09CA04
Isradipine C08CA03
Lacidipine C08CA09
Landiolol C07AB14
Lercanidipine C08CA13
Lisinopril C09AA03
Losartan C09CA01
Lovastatin C10AA02
Manidipine C08CA11
Methylchlorothiazide C03AA
Metoprolol C07AB02
Moexipril C09AA13
Nadroparin B01AB06
Nebivolol C07AB12
Nicardipine C08CA04
Nifedipine C08CA05
Nilvadipine C08CA10
Nimodipine C08CA06
Nisoldipine C08CA07
Nitrendipine C08CA08
Nitroprusside C02DD01
Olmesartan C09CA
Perindopril C09AA04
Phenprocoumon B01AA04
Plasminogen activator B01AD
Polythiazide C03AA05
Practolol C07AB01
Pravastatin C10AA03
Prourokinase B01AD
Quinapril C09AA06
Ramipril C09AA05
Reteplase B01AD07
Rivaroxaban B01AF01

LISTING NEML MEDICINES ON HAQ SCORES
82
Rosuvastatin C10AA07
Simvastatin C10AA01
Spirapril C09AA11
Spironolactone C03DA01
Streptokinase B01AD01
Talinolol C07AB13
Telmisartan C09CA07
Tenecteplase B01AD11
Torsemide C03CA04
Trandolapril C09AA10
Urokinase B01AD04
Valsartan C09CA03
Verapamil C08DA01
Warfarin B01AA03
Zofenopril C09AA15

LISTING NEML MEDICINES ON HAQ SCORES
83
Table 13. Medicines for Hypertensive Heart Disease
Medicine Name Primary ATC Code
Acebutolol C07AB04
Amlodipine C08CA01
Atenolol C07AB03
Atorvastatin C10AA05
Benazepril C09AA07
Bendrofluazide (Bendroflumethiazide) C03AA01
Betaxolol C07AB05
Bevantolol C07AB06
Bisoprolol C07AB07
Bumetanide C03CA02
Candesartan C09CA06
Captopril C09AA01
Carvedilol C07AG02
Celiprolol C07AB08
Chlorothiazide C03AA04
Chlortalidone (Chlorthalidone) C03BA04
Cilazapril C09AA08
Cilnidipine C08CA14
Cyclopenthiazide C03AA07
Delapril C09AA12
Digoxin C01AA05
Dopamine C01CA04
Enalapril C09AA02
Epanolol C07AB10
Eplerenone C03DA04
Eprosartan C09CA02
Esmolol C07AB09
Felodipine C08CA02
Fluvastatin C10AA04
Fosinopril C09AA09
Furosemide C03CA01
Hydralazine C02DB02
Hydrochlorothiazide C03AA03
Imidapril C09AA16
Indapamide C03BA11
Irbesartan C09CA04
Isradipine C08CA03
Lacidipine C08CA09
Landiolol C07AB14
Lercanidipine C08CA13

LISTING NEML MEDICINES ON HAQ SCORES
84
Lisinopril C09AA03
Losartan C09CA01
Lovastatin C10AA02
Manidipine C08CA11
Methylchlorothiazide C03AA
Methyldopa C02AB
Metoprolol C07AB02
Moexipril C09AA13
Nebivolol C07AB12
Nicardipine C08CA04
Nifedipine C08CA05
Nilvadipine C08CA10
Nimodipine C08CA06
Nisoldipine C08CA07
Nitrendipine C08CA08
Nitroprusside C02DD01
Olmesartan C09CA
Perindopril C09AA04
Polythiazide C03AA05
Practolol C07AB01
Pravastatin C10AA03
Quinapril C09AA06
Ramipril C09AA05
Rosuvastatin C10AA07
Simvastatin C10AA01
Spirapril C09AA11
Spironolactone C03DA01
Talinolol C07AB13
Telmisartan C09CA07
Torsemide C03CA04
Trandolapril C09AA10
Valsartan C09CA03
Zofenopril C09AA15