Embed Size (px)
Citation preview

i
August 2016
IVIG and SCIG Utilization in the Atlantic Provinces in FY 2015/16

ii
Report Prepared by: Marina Hamilton, Program Manager Data Analysis by: Tanja Keselj, Senior System Analyst Erica Paolone, Data Analyst Mark Daine, Database Coordinator Graham Wile, Senior System Analyst Nova Scotia Provincial Blood Coordinating Program Room 2123 1673 Bedford Row Halifax, Nova Scotia B3J 1T1 Phone: (902) 487-0516

1Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Table of Contents 1 Executive Summary ..................................................................................................... 2
2 Introduction .................................................................................................................. 3
3 International and National Perspective ........................................................................ 4
4 Provincial Distribution Trends ....................................................................................... 7
5 Utilization Data ............................................................................................................ 11
5.1 Data Collection .................................................................................................. 12
5.2 Data Quality ....................................................................................................... 12
6 Prevalence and Incidence of the Use of IVIG and SCIG in the Atlantic Provinces .. 14
6.1 Incidence ............................................................................................................. 14
6.2 Prevalence ............................................................................................................ 15
7 Disease Categories and Indications ............................................................................. 16
8 Request Approval Process ............................................................................................ 18
9 Appropriateness of Use ............................................................................................... 20
9.1 Appropriateness of Indications ......................................................................... 20
9.2 IgG Levels for Immune Deficiencies ................................................................ 23
10 Discards ...................................................................................................................... 25
11 Dosing Intravenous Immune Globulin (IVIG) Based on Dosing Body Weight ...... 26
12 Subcutaneous Immunoglobulin .................................................................................. 27
12.1 Atlantic Guidelines ............................................................................................ 27
13 Recommendations ...................................................................................................... 30
Appendix A per Capita Utilization of IVIG/SCIG for Most Common Indications ........ 31
Appendix B Year to Year New and Chronic Patients on IVIG and SCIG ...................... 36

2Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
1 Executive Summary This report provides an overview of the distribution and utilization of intravenous immunoglobulin (IVIG) and subcutaneous immunoglobulin (SCIG) in the Atlantic Provinces for the 2015/16 fiscal year. When compared with many other developed countries, Canada has the highest per capita consumption of IVIG and SCIG; the distribution of these immune globulins in Canada has continued to rise over the last ten years by 5 to 10% each year. In the 2015/16 fiscal year, Canada had a rise in the distribution by 9% from what it was in the previous year. Atlantic Canada demonstrated a 6% increase in the distribution of IVIG and SCIG in 2015/16 from what it was in 2014/15. Although New Brunswick was the only Atlantic province to exhibit a decrease in the distribution of IVIG and SCIG in 2014/15, they did exhibit a growth of 6% in 2015/16. The growth rate in distribution for Newfoundland and Labrador was 3.4 %, a decrease from 7% in 2014/15. Nova Scotia exhibited a growth of 3.9% while Prince Edward Island’s growth for this fiscal year was 33.3%. This increase may be attributed to a rise in the new cases treated with IVIG/SCIG. During 2015/16 the use of IVIG/ SCIG increased in Neurology, Hematology and Dermatology while Immunology and Rheumatology decreased compared to last year. The top three uses of IVIG and SCIG in Atlantic Canada are for the treatment of Primary Immune Deficiency (PID), Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP), and Immune Thrombocytopenia Purpura (ITP). The Atlantic use of IG decreased for Immune Thrombocytopenia Purpura (ITP), Multifocal Motor Neuropathy (MMN) and Guillian Barré Syndrome (GBS); while it increased for Primary Immune Deficiency (PID), Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP), Myasthenia Gravis (MG), Secondary immune deficiency (SID) and Stiff Person syndrome in Atlantic Canada. In Atlantic Canada this year, 3% of the total IVIG administered, was given for Unlabeled conditions (UL-N) for which there is no evidence to support the use of IVIG; where as 97% of the use was for appropriate indications.
Monitoring patient serum IgG levels every 3-6 months is recommended for PID to ensure that patients using IVIG and SCIG are being dosed appropriately. This fiscal year, 77% of patients in Atlantic Canada had their serum IgG levels monitored, a slight decrease from last year. The target range for IgG levels is between 7 and 10 g/L. For those PID patients whose IgG levels are 10g/L or above, there is the potential to reduce the amount of product they are receiving while still experiencing clinically beneficial outcomes. These patients are identified in all Atlantic provinces and their information is shared in their respective province specific report to explore the opportunity for dose adjustment.
The dosing of IVIG, based on dosing body weight rather than actual body weight, was introduced by the Nova Scotia Provincial Blood Coordinating Program (NSPBCP) in 2010/11. It is applicable to all patients excluding patients with Guillian Barré Syndrome, solid organ transplant and those who are shorter than 5 feet in height. In 2015/16, the analysis of 1109 Atlantic patients revealed that 89% of those eligible were dosed according to their dosing body weight. There was an estimated cost avoidance of $3,189,975 for 62,207 grams.

3Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
The combined total of IVIG discards in the Atlantic Provinces decreased from 1,098 grams in 2014/15 to 720 grams in 2015/16. This year’s discards are 0.001% of the total distribution.
In conclusion, The Atlantic distribution of 172g/1000 population of IVIG is less than the Canadian distribution of 190g/1000 population in 20154/16. IVIG and SCIG distribution increased in the Atlantic Provinces by 6% during the 2015/16 fiscal year, which is a 4% increase from last year. Among Canadian Provinces New Brunswick at 134g/1000 population is ranked second best in per capita distribution of IVIG/SCIG after the Territories, while Nova Scotia and Newfoundland and Labrador have a growth rate of 4% and 3% respectively. While the majority of the IVIG and SCIG transfused in Atlantic Canada have been appropriate, 3% was utilized in patients with conditions for which there are little or no evidence to support its use. The NSPBCP continues to be effective in monitoring the use of IVIG and determining the indications and appropriateness of its use. The data generated through the Atlantic Collaborative allows the development of strategies for optimizing the use of IVIG with the end goal being to ensure that patients are dosed appropriately, clinical benefit is achieved, adverse reactions are avoided, and product wastage is minimized. It is recommended that all eligible future patients of IVIG and SCIG be dosed based on the dosing body weight. It is also recommended that all primary immune deficiency patients be consulted with immunologists. And for patients with the serum IgG levels that are above the target range, the Blood Transfusion Medical Directors should have a discussion with the respective prescribing physicians for dose adjustment.
2 Introduction This report is a summary of the utilization of IVIG and SCIG in the Atlantic Provinces for the fiscal year 2015/16. The purpose of this report is to describe the use of IVIG and SCIG in the Atlantic Provinces, to identify recommendations for improvement in data quality, and to identify strategies for optimizing appropriate use of these products to minimize product wastage. In this report the NSPBCP continues to publish the comparison of IVIG and SCIG distribution data with the rest of Canada, as this serves as a benchmark for the Atlantic Provinces. The Atlantic Provinces and the rest of Canada are examined separately in this report. The data analysis for this report was conducted on a subset of the data that was reported to NSPBCP on or before May 18, 2016. Any data submitted after this date is not included in this report’s analysis but will impact on next year’s analysis.

4Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
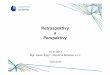
3 International and National Perspective Figure 1 shows an international comparison of per capita IVIG and SCIG consumption for 2011 to 2013 in select countries of the world. Canada was the second highest user of IVIG and SCIG in 2012. The IVIG and SCIG consumption was 118g/1000 population in Canada for 2009 which increased to 168.5g/1000 population in 2012. The United States and Canada are using two to three times more than other countries. Source: Market Research Bureau (via Canadian Blood Services)
Figure 1

5Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
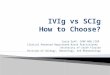
Figure 2 shows the annual combined distribution of IVIG and SCIG across Canada (including Quebec) for the last five fiscal years. Since 2011, Canada’s IVIG and SCIG distribution rates have consistently increased by 6 to 9%, with a 9% increase in 2015/16.
5.155.48
5.886.23
6.78
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
2011-2012 2012-2013 2013-2014 2014-2015 2015-2016
IVIG
an
d S
CIG
(1,
000,
000s
of g
ram
s)
National Ig Distribution and Growth Rate(includes Quebec)
9%
6%
7%
6%
Figure 2

6Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure 3 shows Atlantic Canada’s combined annual distribution of IVIG and SCIG for the last thirteen years. Distribution rates were relatively unchanged from 2002 through to 2006, as demonstrated by this graph; the last eight fiscal years show steady increases to the distribution rate. Atlantic Canada saw a 6% distribution increase in 2015/16 from the previous fiscal year.
6%
-7% 7%
17%
13% 0%9%
6%7%
5%8%
4%
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
IVIG
an
d S
CIG
(1,
000,
000s
of
gram
s)
IVIG and SCIG Distribution and Growth Rate in Atlantic Canada
Figure 3

7Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
4 Provincial Distribution Trends This section summarizes the total amounts of IVIG and SCIG distributed to facilities in the Atlantic Provinces in recent fiscal years. While different from the amount of IVIG and SCIG utilized, it provides a reference for monitoring year-to-year trends. Figure 4 demonstrates the total grams of IVIG and SCIG distributed by CBS to New Brunswick and Newfoundland and Labrador from the 2006/07 fiscal year until 2015/16.
Although New Brunswick was the only Atlantic province to exhibit a decrease in the distribution of IVIG and SCIG in 2014/15, they did exhibit a growth of 6% in 2015/16. The growth rate in distribution for Newfoundland and Labrador was 3.4 %, a decrease from 7% in 2014/15. Nova Scotia (Figure 5) exhibited a growth of 3.9% while Prince Edward Island’s growth for this fiscal year was 33.3%.
64055
68370
76001
86640
95568
99953
99643
100770
93330
97802.5
67800
71407
66179
81650
82115
83813
79868
94965
101670
102175
00
115
346
651774 1120 2065
20103408
00
77
282 803 1058656
837
8403909
0
20000
40000
60000
80000
100000
120000
NB NL
Total Grams of Ig Distributed in NB and NL
SCIG(g)
IVIG (g)
Figure 4

8Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure 5 demonstrates the total grams of IVIG and SCIG distributed by CBS to Nova Scotia and Prince Edward Island from the 2006/07 fiscal year until 2015/16.
Nova Scotia has shown an increasing trend in IVIG and SCIG distribution in the past five years. The growth has slowed to 4% in 2015/16 from 7% in 2014/15 and 12.3% in 2013/14. The increasing growth rate is attributable to the number of new cases treated with IVIG/SCIG; 216 in 2015/16 and 215 in 2014/15. Prince Edward Island demonstrated a 33.3% increase in the distribution of IVIG and SCIG in 2015/16 after an increase of 30.5% in 2014/15. This increase may be attributed to a rise in the new cases treated with IVIG/SCIG in PEI. There were 29 new cases in 2015/16 and 30 new cases in 2014/15. The use of IVIG/SCIG increased in Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP), Secondary Immune Deficiency (SID), and Refractory Autoimmune Scleritis in PEI during 2015/16. There was a decrease in the grams utilized for Multifocal Motor Neuropathy (MMN).
88108
105479
104502
102148
98745
115355
130797
140143
147978
150305
1101015235
1399512255
21355
18960
23245
18455
24255
32695
0
0 403 1205 3359
3867
4169
11393
1410218231
00 0 0
0 0770
558566
464
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
NS PE
Total Grams of Ig Distributed in NS and PE
SCIG(g)
IVIG (g)
Figure 5

9Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Table 1 highlights the actual cost of IVIG/SCIG distributed in Atlantic Canada; both in the current and for the past 5 fiscal years. Table 1: Total Grams and Cost of Ig Distributed to the Atlantic Provinces by Fiscal Year
The price of IVIG/SCIG per gram increased by $3.43 in 2015/16. All Atlantic provinces saw the overall cost of Ig increase from last fiscal year due to the rise in the amount distributed. The variation and impact of the IVIG costs per gram demonstrates how continued appropriate utilization is essential to ensuring that this expensive product is available to those who most need it. Figure 6 below compares the amount of IVIG and SCIG distributed, per thousand population, among the Canadian provinces and territories for the last three fiscal years.
Fiscal Year
Avg. Price per
gram
New Brunswick Nova Scotia Prince Edward
Island Newfoundland &
Labrador
Grams Cost Grams Cost Grams Cost Grams Cost
2010-2011 $62.90 96219 $6,052,345 102104 $6,422,546 21355 $1,343,266 82918 $5,215,717
2011-2012 $58.97 100727 $5,940,309 119222 $7,031,042 18960 $1,118,155 84870 $5,005,162
2012-2013 $55.29 100763 $5,571,253 134967 $7,462,434 24015 $1,327,812 80524 $4,452,220
2013-2014 $48.74 102835 $5,011,807 151536 $7,385,297 19013 $926,626 95802 $4,669,051
2014-2015 $47.85 95340 $4,561,917 162080 $7,755,341 24821 $1,187,659 102510 $4,904,995
2015-2016 $51.28 101211 $5,189,482 168536 $8,642,809 33159 $1,700,446 106084 $5,440,152

10Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
All Canadian Provinces and Territories exhibited a rise in the per capita distribution of IVIG/SCIG. At the distribution of 134 per thousand population this year, New Brunswick is the lowest in distribution (per 1000 population) in the country, behind the territories. Figure 7 below compares the amount of IVIG and SCIG distributed, per thousand population, among the Atlantic provinces, Atlantic region and rest of the Canadian provinces and territories excluding Atlantic Canada for the last three fiscal years.
QC MN PEI AB NL NS SK BC ON NBYT/NT/
NU2013-2014 230 202 131 188 182 161 156 143 132 136 592014-2015 231 220 170 200 195 172 163 147 144 126 472015-2016 242 230 226 222 201 179 173 162 158 134 64
0
50
100
150
200
250
300
gram
s per
100
0 p
opu
lati
on
National IVIG and SCIG Distribution per 1000 Population
Figure 6

11Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure 7
All Atlantic Provinces exhibited a rise in the per capita distribution of IVIG/SCIG. At the distribution of 134 per thousand population this year, New Brunswick is the lowest in distribution (per 1000 population) among the Atlantic Provinces. All Atlantic provinces, collectively, also show an increase in distribution per thousand population. At the distribution of 172 per thousand population this year, the Atlantic Region continues to be lower than Rest of the country in distribution per 1000 population.
5 Utilization Data The information presented in the remainder of this report is derived from the Intravenous Immunoglobulin Network (IVIN) database housed at the NSPBCP. The following sections provide information regarding the data used to create the graphs and tables and should be considered in the interpretation of the utilization information in this report.
NB NL NS PEI Atlantic Rest of Canada2013-2014 136 182 161 131 156 1682014-2015 126 195 172 170 162 1772015-2016 134 201 179 226 172 190
0
50
100
150
200
250
gram
s per
100
0 p
opu
lati
on
Atlantic IVIG and SCIG Distribution per 1000 Population

12Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
5.1 Data Collection By gathering and storing data for this report through the Intravenous Immunoglobulin Network (IVIN) system, we are ensuring that it remains current and reproducible. On occasion, revisions, corrections and additions may be identified following the publication of the annual report. In the event that this occurs, the data in the database is adjusted and the amendments are documented. When conducting analyses on past years the amended data is used. This is a consideration when noting differences in numbers between previous reports and the current report. The NSPBCP continues to successfully liaise with one of the Zones in Nova Scotia and the Lab Information System manager to obtain a quarterly data extract from the Zone’s Laboratory Information System (LIS). This approach has decreased human resource dependence as well as eliminated manual data entry errors. It is recommended that in order to minimize the human error, jurisdictions consider the option of exploring extracts of data from Laboratory Information System (LIS) into IVIN. The NSPBCP implemented a new strategy for SCIG log sheets that resulted in marked improvement in the reporting and monitoring of SCIG data during 2014/15. Until last fiscal year the clinics received the log sheets from the patients, verified content and then forward it to the Blood Transfusion Laboratory. A slight lack of compliance at any step resulted in a poor capture of the utilization data. In order to improve this, the NSPBCP implemented the strategy where the log sheets (or their copy) are required to be returned to the dispensing BTS by the patient in order to receive more product. The BTS then enter the information into IVIN. In case of non compliance, the product dispensed is limited to a week’s supply. Routine dispense amounts can be resumed anytime upon submission of the previous log sheets. The population of reference for this report is all patients who received doses of IVIG and/or SCIG for any indication.
5.2 Data Quality
The NSPBCP strives to continuously improve the quality of data obtained for analysis. To this end, the program reviews all of the submitted data for inconsistencies and to identify any incomplete data entry fields. Most of these checks are now completed using automated integrity queries. Any inconsistencies discovered by the queries are investigated and resolved. All cases with indications marked as “insufficient” or as “other” are identified on a quarterly basis so that the correct information pertaining to the diagnosis may be sought. This is done to minimize ambiguity in the categorization of disease indications; the appropriateness of IVIG and SCIG use is based on this information. Clinical experts are consulted electronically to assign an appropriateness category (L, UL-I, UL-N) whenever IVIG is used for any new indication. As previously mentioned, this report includes data received by the NSPBCP for the fiscal year 2015/16 as of May 18, 2016. The data is extracted from the database and that is the source used for generating the report. Data for fiscal year 2015/16 can continue to be entered into the database but it will not be part of the extract used for generating the report. However for previous fiscal years, an updated or live database is used for a true reflection of the revisions, corrections and submissions on data that were completed after the generation of previous

13Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
annual reports. This may reflect as a variation in the indications, utilized IVIG grams and overall appropriateness of use of IVIG from what was presented in the previous annual reports. Data submissions were reviewed for missing data on a quarterly period which contributed to quality improvement of the Atlantic IVIG/SCIG Utilization report and must be continued. Percent capture of the distribution data for the Atlantic Provinces during the time period of this report was greater than 95%. This is based on the amount of IVIG or SCIG reported as utilized (transfused + discarded) divided by the total amount of IVIG or SCIG distributed.
Province Percent Capture
2013-2014 Percent Capture
2014-2015 Percent Capture
2015-2016 New Brunswick 96.5 99.0 99.0 Nova Scotia 99.6 100.5 99.9 Prince Edward Island 100.1 101.9 96.0 Newfoundland and Labrador 99.6 99.0 97.7
Percent capture of the IVIG distribution data for the Atlantic Provinces during the time period of this report decreased slightly from the previous year. However; the high percent capture of IVIG supports the fact that the utilization data in this report is representative of the actual overall utilization and a result of a continuous evaluation, reminders, support and mutual effort between the NSPBCP and the data submitters throughout the Atlantic Provinces. Table 3 shows an improved percent capture of the SCIG distribution data for New Brunswick only. The remaining Atlantic Provinces exhibit a decrease during the time period of this report from what it was in 2014/15.
Table 3: Percent Capture for SCIG
Province Percent Capture
2013-2014 Percent Capture
2014-2015 Percent Capture
2015-2016 New Brunswick 73.7 88.8 95.2 Nova Scotia 38.0 97.4 84.9 Prince Edward Island 98.6 91.2 79.7 Newfoundland and Labrador 92.1 92.4 68.4
Table 2: Percent Capture for IVIG

14Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
6 Prevalence and Incidence of the Use of IVIG and SCIG in the Atlantic Provinces
The study of prevalence and incidence of cases using IVIG and SCIG is used to understand the variation in the trends of IVIG and SCIG distribution over a period of time. Population data used to calculate prevalence and incidence was taken from the website of Statistics Canada.
6.1 Incidence
Incidence refers to the rate at which new cases of a disease occur in a population during a specified period. It is also calculated per 100,000 population to avoid display in decimals. Figure 8 shows yearly provincial comparison of the incidence rates of patients requiring either IVIG or SCIG treatment in the Atlantic provinces over the last three fiscal years. The incidence of cases requiring IVIG/SCIG increased in New Brunswick from 18 new cases per 100,000 last year to 24 new cases this year. The incidence rate remained the same for Nova Scotia at 23/100,000 population for the past 3 fiscal years. Newfoundland and Labrador saw a rise from 20/100,000 in 2014/15 to 23/100,000 population in 2015/16. Prince Edward Island was the only Atlantic province to exhibite a decrease in the incidence from 21/100,000 population in 2014/15 to 20/100,000 population in 2015/16.
Figure 8
1918
2423 23 23
16
2120 20 20
23
NB NS PE NL
Incidence of Cases on IVIG and SCIG (per 100,000 pop)

15Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
38 37
46 4546
48
34
38 38
4144
47
NB NS PE NL
Prevalence of Cases on IVIG and SCIG (per 100,000 pop)
6.2 Prevalence Prevalence is broadly defined as the proportion of individuals in a population having a disease. In this case, prevalence refers to the proportion of individuals (calculated per 100,000 population) that are receiving IVIG and/or SCIG. Figure 9 shows that the prevalence rate for individuals requiring either IVIG or SCIG increased for all Atlantic provinces except Prince Edward Island where it remained the same as 2014/15.
Figure 9

16Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
7 Disease Categories and Indications
When IVIG was first introduced in the early 1980s, it was used exclusively for immune deficiencies. Since that time the number of indications for its use has expanded across a wide range of specialties. Figure 10 shows the total grams of Atlantic IVIG and SCIG used by major disease categories in the last two fiscal years. It is important to consider that the disease category is based on the categorization of the indication for use and does not necessarily reflect the specialty of the ordering physician.
There was a rise in use of IVIG and SCIG for neurological conditions by 3%, hematological conditions by 4% and dermatological conditions by 22% in 2015/16 of what it was in 2014/15. Immunological conditions saw a decrease of 242 grams exhibiting a decline by 0.3% of what it was in the previous year. Rheumatological conditions also exhibited a decrease of 1,614 grams, a decline of 4.8%. All other disease categories are analyzed as a combined category named ‘other’, the use increased in this category by 129% in 2015/16. This is an increase of 6,179 grams from 2014/15.
Neurological Immunological Hematological Rheumatological Dermatological Other
2014-2015 169547 84526 74869 33922 14475 4795
2015-2016 175737 84284 78041 32308 17660 10975
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
200000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
IVIG and SCIG (g) Use By Disease Category in the Atlantic Provinces
Figure 10

17Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure 11 shows the total IVIG and SCIG used in each of the most common indications in the Atlantic Provinces in the last three fiscal years.
The highest use was for Primary Immune Deficiency (PID) and Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP). In 2015/16 the use of IVIG/SCIG increased in Primary Immune Deficiency, Chronic Inflammatory Demyelinating Polyradiculoneuropathy, Secondary Immune Deficiency (SID), Myasthenia Gravis (MG), Stiff Person Syndrome (SPS) and Multiple Sclerosis (MS). The use decreased for Immune Throbocytopenic Purpura (ITP), Multifocal Motor Neuropathy (MMN) and Guillain-Barre Syndrome (GBS). Graphs showing provincial utilization of IVIG and SCIG for all nine most common indications for IVIG/SCIG use can be found in Appendix A.
PID CIDP ITP SID MG MMN GB SPS MS2014-2015 83890 71607 39705 28970 29670 29980 14038 9535 4302015-2016 84027 74925 39130 36564 33854 27910 11673 9655 965
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
IVIG and SCIG Use by Indication in the Atlantic Provinces
Figure 11

18Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Table 4 shows the comparison of the top five indications by usage of IVIG and SCIG (g) in each Atlantic province during 2015/16. While not all provinces have the same top three indications for use, they do all share commonalities in their lists.
NB NS PE NL
Indication g Indication g Indication g Indication g
SID 18414 PID 51422 CIDP 12260 CIDP 19365
PID 17325 CIDP 26865 PID 3835 MG 12900
CIDP 16435 ITP 14018 SPS 3000 ITP 11593
ITP 11919 MMN 12815 SID 2160 PID 11445
MG 8205 MG 12034 RAS 2120 SLE 9755
In 2015/16 the highest amount of IVIG/SCIG was used for Primary immune deficiency in Nova Scotia. This was the second ranked indication by amount of IVIG/SCIG use in both New Brunswick and Prince Edward Island. Use of IVIG for Chronic Inflammatory Demyelinating Polyradiculoneuropathy (CIDP) was ranked highest in Newfoundland and Labrador and Prince Edward, second and third in Nova Scotia and New Brunswick respectively. High use of IVIG and SCIG for PID reinforces the importance of regularly monitoring IgG levels to ensure dosing is appropriate.
8 Request Approval Process In an effort to optimize the appropriate use of IVIG, the Atlantic Blood Utilization Strategy (ABUS) Working Group developed an Atlantic-wide IVIG request approval system. Through this process, requests for IVIG are reviewed to determine if the indication, as well as the dosing, frequency and duration of treatment, meet the guidelines for use. In the event of a discrepancy, the ordering physician is contacted and discussion ensues regarding the variation. If the ordering physician continues to feel that a given case merits a change from the guidelines, he or she is asked to discuss the case with a consultant with the relevant clinical expertise. The pathway thus taken by the request is allocated a number representing the route it took for its approval. These pathway numbers are recorded and submitted for each and every new request of IVIG. A detailed guide of the request approval pathway numbers is attached as Appendix C at the end of the report. The distribution of the Atlantic request approval pathways taken by new IVIG orders during 2015/16 is as follows: 1,302 requests passed through the approval process. There were 1,211 (93%) requests
Table 4: Top Indications

19Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
that met the guidelines upon initial submission. Out of the remaining 91, 42 (46%) were for indications not listed in the guidelines (non neurology, non immunology and non hematology patients). Of the remaining 49, consultation occurred between Blood Transfusion Services staff and the clinical expert in 43 (88%) of the cases. Where a consult happened, 25 (51%) were revised to meet the guideline after consultation with Blood Transfusion Services staff or clinical expert, 16 were dispensed as requested despite consultation with a clinical expert, 1 request was withdrawn after the ordering MD consulted with the clinical expert and 6 were dispensed as requested without a clinical expert consultation.
Table 5: Request Approval Pathways
Pathway Description NB NS PEI NL Atlantic
1 Request was for an indication not listed in the guidelines
27 7 7 1 42
2 Request met the guidelines upon initial submission
298 473 54 386 1211
3 Request was revised to meet the guidelines after discussion with BTS staff
2 7 0 5 14
4 Request was withdrawn after discussion with BTS staff
0 1 0 0 1
5 Request was revised to meet the guidelines after the ordering MD consulted with the clinical expert
1 0 3 7 11
6 Request was withdrawn after the ordering MD consulted with the clinical expert
0 0 1 0 1
7 The original request was granted even after the ordering MD consulted with the clinical expert
0 0 6 10 16
8 Consultation with the clinical expert was required but did not occur
1 1 2 2 6
Total 329 489 73 411 1302

20Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
9 Appropriateness of Use
9.1 Appropriateness of Indications
When IVIG utilization data is received by the NSPBCP, the indications for the use of IVIG are categorized based on their appropriateness for use with this product. The following describes the categories used:
Category Explanation L (labeled/licensed) The manufacturer can advertise the use of
IVIG for these conditions. UL-I (unlabeled, indicated) The manufacturer cannot advertise the use of
IVIG for these conditions, but there is some evidence to support its use.
UL-N (unlabeled, not indicated) There is no evidence to support the use of IVIG for these conditions.
II (insufficient information) The NSPBCP was unable to obtain sufficient information. In most cases the indication provided is only a symptom or overly general diagnosis rather than the specific indication for the use of IVIG. This category is addressed in the Data Collection section of this report.

21Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure 12 shows the proportion of IVIG used for Unlabelled, not indicated (UL-N) conditions in the Atlantic Provinces.
This year, Atlantic use of IVIG for UL-N indications remained steady at 3% of the total use. This is an increase in New Brunswick of 2% during 2015/16, Newfoundland and Labrador and Prince Edward Island while Nova Scotia exhibited a slight decrease.
NB NS PE NL Atlantic2012-2013 3.0% 1.2% 0.0% 2.6% 2.0%2013-2014 2.3% 2.3% 0.0% 2.2% 2.1%2014-2015 0.5% 2.6% 1.0% 2.5% 1.9%2015-2016 2.5% 2.4% 4.6% 3.6% 3.0%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
5.0%
UL
-N U
sage
(%
)
Proportion of IVIG used for UL-N Indications
Figure 12

22Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Table 6 lists the Atlantic UL-N indications for IVIG during 2015/16 fiscal year by total grams utilized.
Table 6: UL-N Indications
Indication
IVIG(grams)
1. Chronic Urticaria 3870
2. Rapid-Onset Obesity with Hypothalamic Dysfunction, Hypoventilation and Autonomic Dysregulation (ROHHAD)
1750
3. Vasculitis Neuropathy 1674
4. Transverse Myelitis 940
5. Lichen Planus 750
6. CMV pneumonia 330
7. Polyarthritis/polychondritis/lytic bone lesions 270
8. Scleroderma 240
9. Cellulitis 225
10. Thrombotic thrombocytopenic purpura 215
11. Acute Hemolytic Anemia 170
12. Necrotizing Fasciitis due to Group B Streptococci 140
13. Myelitis 125
14. Neutrophilic Panniculitis 120
15. Axonal Polyneuropathy 120
16. Lymphoma 100
17. Seizures 60
18. Leukemia 20
19. Tuberous Sclerosis 10
Total 11129
Because the price per gram varies depending on both availability and U.S. dollar exchange rates, it is imperative that IVIG be utilized appropriately with the goal being to reduce the amount used for conditions where it is not likely to be of clinical benefit (UL-N indications) to as close to zero grams as possible. Approximately $570,695 was spent for UL-N indications in Atlantic Canada this year.

23Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
9.2 IgG Levels for Immune Deficiencies
When patients are receiving IVIG or SCIG for the treatment of immune deficiencies, it is recommended that serum IgG levels be measured on a regular basis and the dose of IVIG and SCIG be adjusted to keep the IgG level between the target range of 7 and 10g/L. Figure 13 shows the proportion of patients with PID who had their IgG levels monitored. The frequency of monitoring cannot be inferred from this graph.
In 2015/16, 77% of Atlantic patients with primary immune deficiencies had their serum IgG levels monitored and reported. This is a 2% decrease from last year. Improvement in monitoring and reporting of serum IgG levels was observed in New Brunswick with an increase to 67% of cases this year. In Prince Edward Island, 100% of their Primary Immune
NB NS PE NL Atlantic2013-2014 57% 73% 55% 79% 70%2014-2015 46% 86% 100% 95% 79%2015-2016 67% 77% 100% 89% 77%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Per
cen
t of
mon
itor
ed p
atie
nts
Proportion of Primary Immunodeficiency cases with monitored serum IgG levels
Figure 13

24Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Deficiency patients had their serum IgG levels monitored. Nova Scotia and Newfoundland and Labrador exhibited a decline in the monitoring and reporting of serum IgG levels.
Figure 14
Figure 14 shows the total number of individuals (both pediatric and adult) with Primary Immune Deficiency, in each of the 4 provinces, who had their serum IgG levels monitored. This monitoring helps identify those patients whose serum levels are above the target range of 7 to 10g/L and who may achieve the same clinical benefit with decreased dosing. In Nova Scotia, 43% of those monitored had their serum IgG level above 10g/L; likewise 41% in New Brunswick; 10% in Prince Edward Island and 32% in Newfoundland and Labrador had higher than target serum IgG levels. The NSPBCP has included the details of all the patients with serum IgG levels above the target range in the province specific reports.
31% 32%41%
13% 12% 8%0%
10% 10%
30%41%
19%
42%32% 19%
49%44% 49% 67%
70%80%
53%41%
48%
27%36% 41% 39%
45% 43%33%
20%10%
17% 19%32%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NB NS PEI NL
Proportion of serum IgG by the target levels
>10g/L
7-10g/L
< 7g/L

25Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
10 Discards One goal of the NSPBCP is to optimize appropriate use as well as to minimize wastage. Figure 15 shows a summary of the discarded IVIG during this past fiscal year in the Atlantic Provinces.
The total discards decreased from 1098g in 2014/15 to 720g in 20145/16. Decreases in discards were seen in all Atlantic provinces. The cause of the majority of wastage of IVIG in this fiscal year was breakage and in lab temperature/visually unacceptable.
NB NS PEI NL Atlantic2012-2013 275 285 25 555 11402013-2014 135 420 40 263 8582014-2015 115 385 40 568 11082015-2016 103 378 30 210 720
IVIG
(g)
Atlantic IVIG(g) discards
Figure 15

26Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Table 7 summarizes the reasons given for the amount (g) of discarded product discussed above.
Reasons NB NS PEI NL Atlantic Broken 40 187.5 20 175 422.5Expired 50 0 0 0 50Incorrectly reconstituted 10 0 0 0 10Pooled, not used 3.2 0 0 0 3.2Product failed to reconstitute properly 0 0 10 0 10Research/Validation 0 55 0 0 55Returned to lab temperature/visually unacceptable 0 135 0 0 135Spiked not transfused/Sterility/integrity of product compromised 0 0 0 34.5 34.5Total 103.2 377.5 30 209.5 720.2
It is recommended that the data on discards continue to be collected and monitored. In order to minimize the discards, continuous education regarding the care for and the use of IVIG and early return of the unused products to the laboratory if not transfused should be emphasized. As IVIG is safely stored at room temperature (between 2˚C-25˚C) according to the manufacturers’ inserts, the NSPBCP recommended in 2014/15 that product be stored at room temperature when possible to reduce wastage of product that has been returned to the lab more than 30 minutes after it was dispensed, and to reduce slippery condensation build up which has been anecdotally identified as a reason for breakage. Again in 2015/16, broken is the number one reason for discards increasing from 340g in 2014/15 to 422.5 in 2015/16.
11 Dosing Intravenous Immune Globulin (IVIG) Based on Dosing Body Weight (DBW)
Adverse reactions like hemolysis are substantially more likely to happen when a high dose of IVIG is infused. Some Canadian jurisdictions have made recommendations to use adjusted weight based dosing instead of actual patient weight. Dosing weight, an intermediate between ideal body weight and actual body weight, was developed to more accurately dose IVIG. With most of the IVIG being used for appropriate indications and dosing, dosing IVIG based on an adjusted body weight rather than on actual weight may add to safety from hemolysis and may decrease the use of IVIG in patients with a high deviation from ideal body weight. Actual body weight (which includes the weight of adipose tissue of the patient) is used for calculating the dose of fat soluble drugs. As intravenous immunoglobulin is not lipid soluble, an adjusted body weight is appropriate to use for dosing.
Table 7: Reasons for IVIG discards

27Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Patients with Gillian Barré Syndrome and Solid Organ Transplant are excluded from dosing body weight. Also patients less than 5ft in height and those having a lack of expected clinical response are also excluded. These four categories are not included in the calculations of savings. Figure 16 reveals the total grams saved of IVIG for this fiscal year and the number of patients dosed according to DBW.
In 2015/2016, 1,099 Atlantic patients received immunoglobulin. Of the 770 patients eligible, 689 (89%) were dosed based on adjusted body weight resulting in an avoidance of 62,207 grams worth $3,189,975.
12 Subcutaneous Immunoglobulin
12.1 Atlantic Guidelines
In 2012, Atlantic guidelines for Subcutaneous Immunoglobulin Home Administration Programs were approved and disseminated after stakeholder feedback and a pilot implementation. The guidelines included appropriate indications, dosing, and the patient education material for push and pump methods of self administration. At this time the only labeled use of SCIG is for PID.
14130
23191
7182
17704
62207
200241
47
201
689
0
100
200
300
400
500
600
700
800
0
10000
20000
30000
40000
50000
60000
70000
NB NS PEI NL Combined
IVIG
(g)
Savings Using Dosing Based on Adjusted Body Weight (DBW)
IVIG (g) saved by DBW
Number of patients
Figure 16

28Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
In total there were 96 patients on SCIG in the Atlantic Provinces this year, up from 59 in 2014/15. There were 5 new patients on SCIG in Nova Scotia bringing a total to 59 cases. New Brunswick had 2 new patients bringing their total to 18 patients, Newfoundland and Labrador and Prince Edward Island did not have any new cases, keeping the total of patients at 18 and 1 respectively. In 2015/16, SCIG was used for indications other than Primary immune deficiencies. 1,596 grams of SCIG was used for 9 patients with Secondary Immuned Deficiency in the Atlantic Provinces. Prince Edward Island did not have any UL-N indications for SCIG in the previous three fiscal years. Home administration of SCIG has successfully helped transition patients from depending on hospital administration of this product to administering in the comfort of their own home. We expect this program to continue to grow in Atlantic Canada as patients and practitioners are becoming more aware of the health benefits and cost savings associated with home administration. A 2013 Transfusion Medicine article estimated that SCIG treatment, rather than IVIG treatment, reduced cost to the healthcare system per patient of $5,736 over 3 years, principally due to less use of hospital personnel.

29Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure 17 shows that there were 26,004 grams of SCIG distributed in 2015/16, an increase from 17,518g in 2014/15.
Table 8: Number of SCIG Patients
Fiscal Year Province # Patients Receiving
SCIG
2014-2015
NB 8 NS 47 PE 2 NL 3 Atlantic 60
2015-2016
NB 18 NS 59 PE 1 NL 18 Atlantic 96
NB NS PEI NL Atlantic2013-2014 2065 11393 558 837 148532014-2015 2010 14102 566 840 175182015-2016 3406 18229 462 3907 26004
Distribution of SCIG (g) in the Atlantic Provinces
Figure 17

30Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
13 Recommendations
During the June 24, 2016 Atlantic Blood Utilization Stategy (ABUS) working group meeting, the following recommendations were made:
1. Develop a policy directive for the Atlantic Deputy Ministers to support. Each province will be responsible for implementation of the directive. The policy directive will apply to the distribution and use of IVIG by all medical professionals and will include the following:
a. Screening of approved medical conditions by the Health Authority, b. Screening of Neurology conditions by Neurology experts, c. Screening of all other conditions, d. Dosing through adjusted body weight calculation, e. Evaluating clinical outcomes, f. Outdating of product, g. Reporting.
2. Revitalize the Request Approval Process to support the policy directive: a. Develop a list of approved medical conditions based on Ontario’s list of approved indications.
Incorporate expectations to review orders prior to dispense to ensure: i. consultants are engaged for non-approved conditions
ii. the dose, frequency and duration are appropriate iii. pre-requisites have been met iv. dosing through adjusted body weight calculations
b. Engage Neurologists and implement a Neurology review process similar to Ontario’s and British Columbia’s where requests for neurology patients outside the approved indications will be approved for a three month period and will require an outcome questionnaire be submitted prior to the patient receiving any further Ig.
c. Develop criteria and process for evlauating clinical outcomes d. Develop an algorithm/work aids for laboratory use.
3. Separate the pre-printed order forms for Hematology, Neurology and create a miscellanous form.
4. Develop a policy for patients travelling out of province with Ig.
5. Explore the possibility of adding C1 Esterase and possibly other products to ABUS.

31Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Appendix A per Capita Utilization of IVIG/SCIG for Most Common Indications Figure A1
NB NS PE NL Atlantic2013-2014 16829 40988 3460 12886 741622014-2015 18404 49273 3691 12522 838902015-2016 17325 51422 3835 11445 84027
(46)
(132)
(11)
(38)
(227)
(54)
(141)
(10)
(39)
(244)
(55)
(146)
(10)
(35)
(246)
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for Primary Immune Dificiency(# of Patients)

32Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure A2
Figure A3
NB NS PE NL Atlantic
2013-2014 14093 4285 1640 7027 27045
2014-2015 16275 5019 1140 6536 28970
2015-2016 18414 7466 2160 8524 36564
(58)
(20)
(7)
(26)
(111)
(67)
(26)
(8)
(30)
(131)
(81)
(32)
(11)
(39)
(163)
0
5000
10000
15000
20000
25000
30000
35000
40000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for Secondary Immune Deficiency(# of Patients)
NB NS PE NL Atlantic2013-2014 15855 20960 4590 17835 592402014-2015 15659 28593 8680 18675 716072015-2016 16435 26865 12260 19365 74925
(24)
(31)
(6)
(22)
(83)
(20)
(37)
(7)
(23)
(87)
(23)
(38)
(5)
(22)
(88)
0
10000
20000
30000
40000
50000
60000
70000
80000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for CIDP(# of Patients)

33Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure A4
Figure A5
NB NS PE NL Atlantic
2013-2014 14622 18641 935 9035 43233
2014-2015 13898 15157 1460 9190 39705
2015-2016 11919 14018 1600 11593 39130
(58)
(60)
(8)
(42)
(168)
(53)(51)
(7)
(45)
(156)
(78)
(55)
(8)
(45)
(186)
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for ITP(# of Patients)
NB NS PE NL Atlantic
2013-2014 13391 8530 4450 8470 34841
2014-2015 6875 9650 4310 9145 29980
2015-2016 5880 12815 1880 7335 27910
(12)
(13)
(3)
(5)
(33)
(11)
(14)
(3)
(6)
(34)
(11)
(14)
(3)
(6)
(34)
0
5000
10000
15000
20000
25000
30000
35000
40000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for Multifocal Motor Neuropathy(# of Patients)

34Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure A6
Figure A7
NB NS PE NL Atlantic
2013-2014 5717 4655 300 2825 13496
2014-2015 6086 4188 355 3410 14038
2015-2016 5964 3081 395 2233 11673
(24)
(27)
(1)
(13)
(65)
(21)
(24)
(3)
(14)
(62)
(23)
(16)
(2)
(14)
(55)
0
2000
4000
6000
8000
10000
12000
14000
16000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for Guillain-Barre Syndrome(# of Patients)
NB NS PE NL Atlantic
2013-2014 4988 11065 1060 11142 28255
2014-2015 5438 11645 300 12288 29670
2015-2016 8205 12034 715 12900 33854
(16)
(26)
(4)
(23)
(69)
(18)
(24)
(3)
(22)
(67)
(21)
(31)
(4)
(28)
(84)
0
5000
10000
15000
20000
25000
30000
35000
40000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for Myasthenia Gravis(# of Patients)

35Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Figure A8
Figure A9
NB NS PE NL Atlantic
2013-2014 305 4915 1220 2410 8850
2014-2015 0 5340 2120 2075 9535
2015-2016 435 4940 3000 1280 9655
(2)
(4)
(1)
(1)
(8)
(5)
(2) (1)
(8)
(1)
(6)
(2)
(1)
(10)
0
2000
4000
6000
8000
10000
12000
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for Stiff Person Syndrome(# of Patients)
NB NS PE NL Atlantic
2013-2014 0 890 0 0 890
2014-2015 0 430 0 0 430
2015-2016 100 865 0 0 965
(0)
(3)
(0) (0)
(3)
(0)
(2)
(0) (0)
(2)
(1)
(4)
(0) (0)
(5)
0
200
400
600
800
1000
1200
Tot
al g
ram
s IV
Ig a
nd
SC
Ig
Total Ig Use for Multiple Sclerosis(# of Patients)

36Atlantic IVIG/SCIG Utilization Report 2015/16 approved by ABUS WG August 2016
Appendix B Year to Year New and Chronic Patients on IVIG and SCIG Figure B1 below shows the distribution of new and chronic patients (both Adult and Pediatric) in each Atlantic province from 2013/14 to 2015/16.
Figure B1
145 144 165208 222 234
26 25 26
110 125 127
146 137
179
213 215 216
23 30 29
107 106 123
0
50
100
150
200
250
300
350
400
450
500
NB NS PEI NL
Comparison of New and Chronic Cases
New cases
Chronic cases