Embed Size (px)
Citation preview
Atrial & Junctional Atrial & Junctional DysrhythmiasDysrhythmias
Atrial & Junctional DysrhythmiasAtrial & Junctional Dysrhythmias
AtrialAtrialPremature Atrial Premature Atrial ComplexComplexWandering Atrial Wandering Atrial PacemakerPacemakerAtrial Tachycardia Atrial Tachycardia (ectopic)(ectopic)Multifocal Atrial Multifocal Atrial TachycardiaTachycardiaAtrial FlutterAtrial FlutterAtrial FibrillationAtrial Fibrillation
JunctionalJunctionalJunctional Escape Junctional Escape RhythmRhythmPremature Junctional Premature Junctional ComplexComplexJunctional TachycardiaJunctional TachycardiaAccelerated Junctional Accelerated Junctional RhythmRhythmAV Nodal ReAV Nodal Re--entrant entrant Tachycardia (PSVT)Tachycardia (PSVT)
Atrial & Junctional vs. SA Node Atrial & Junctional vs. SA Node
Origin of the pacemaker site is at or above Origin of the pacemaker site is at or above the AV junction but is not the SA Nodethe AV junction but is not the SA Node
Single Atrial siteSingle Atrial siteMultiple atrial sitesMultiple atrial sitesAV JunctionAV Junction
Common CharacteristicsCommon CharacteristicsNarrow QRSNarrow QRSWithout regular, typical appearing, discernible P Without regular, typical appearing, discernible P waveswavesRegular or Irregular RhythmRegular or Irregular Rhythm
Premature Atrial Complex (PAC)Premature Atrial Complex (PAC)
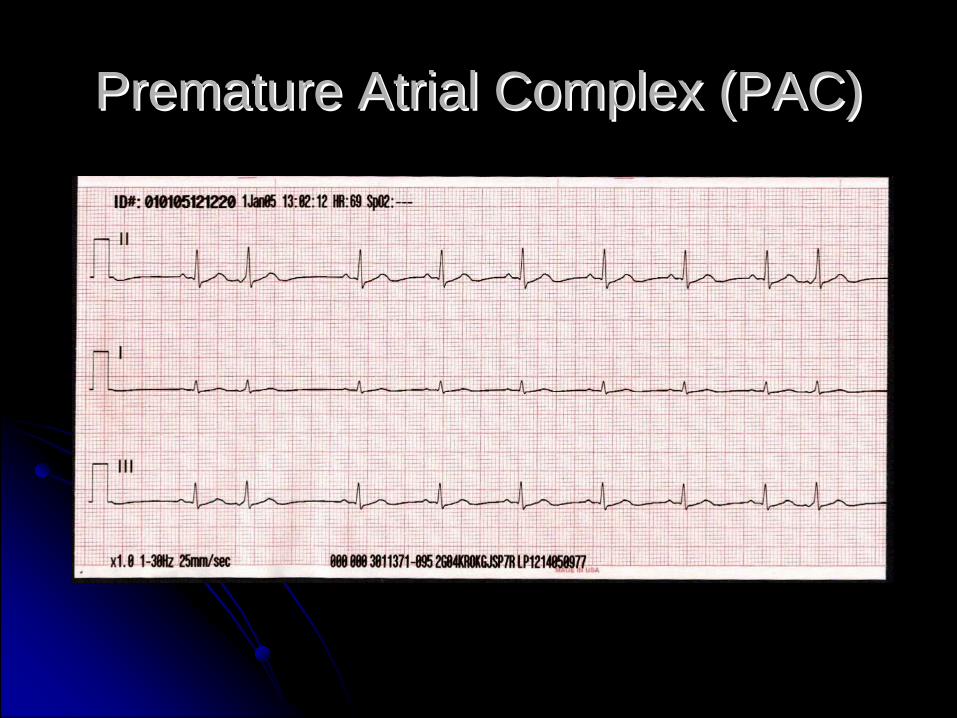
PAC PAC -- Ectopic beat from the AtriaEctopic beat from the Atriaearlier than expectedearlier than expected
ItIt’’s a complex, not a rhythm!s a complex, not a rhythm!Assess the underlying rhythm firstAssess the underlying rhythm first
Premature Atrial Complex (PAC)Premature Atrial Complex (PAC)
Premature Atrial Complex (PAC)Premature Atrial Complex (PAC)
CausesCausesIdiopathicIdiopathicCaffeine, tobacco, alcoholCaffeine, tobacco, alcoholStress, Emotion, InfectionStress, Emotion, InfectionDigitalis toxicityDigitalis toxicityHypoxiaHypoxiaCongestive failureCongestive failureIncreased sympathetic toneIncreased sympathetic tone
Premature Atrial Complex (PAC)Premature Atrial Complex (PAC)CharacteristicsCharacteristics
Heart Rate:Heart Rate: dependent on the underlying rhythmdependent on the underlying rhythmRhythmRhythm: irregular if PACs are present; underlying rhythm : irregular if PACs are present; underlying rhythm may be regularmay be regularPacemakerPacemaker SiteSite: ectopic site in the atria; underlying : ectopic site in the atria; underlying rhythm has its own pacemaker siterhythm has its own pacemaker siteP WavesP Waves: earlier than next expected P wave; positive in : earlier than next expected P wave; positive in lead II; may not look like other P waves presentlead II; may not look like other P waves presentPP--R IntervalR Interval: usually normal for the PAC: usually normal for the PACRR--R IntervalR Interval: unequal since PACs present: unequal since PACs presentQRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: usually one to one relationship: usually one to one relationship
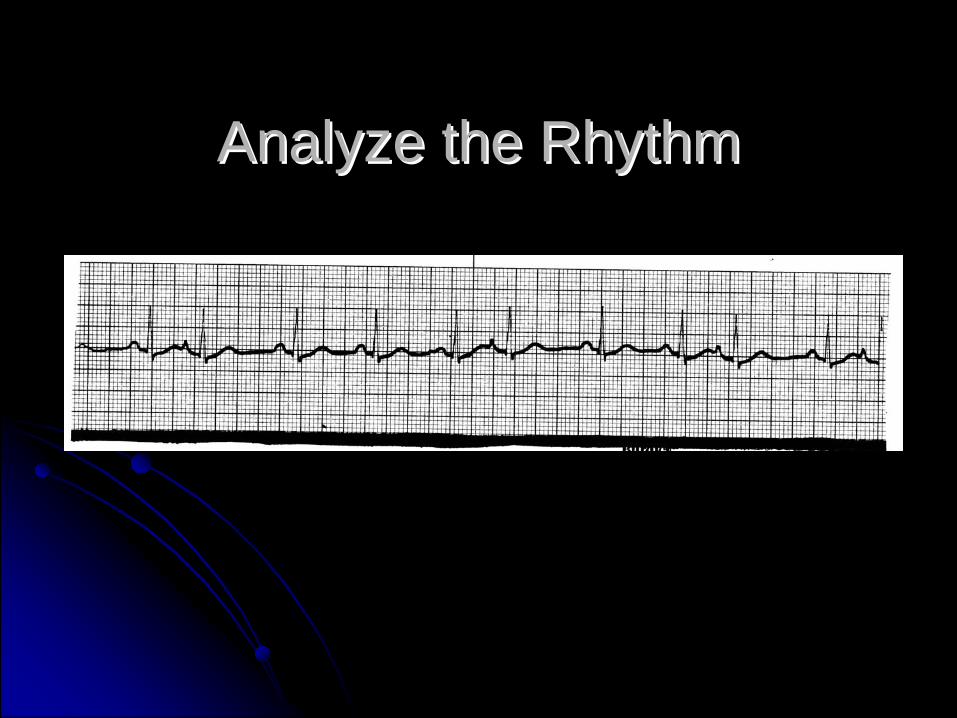
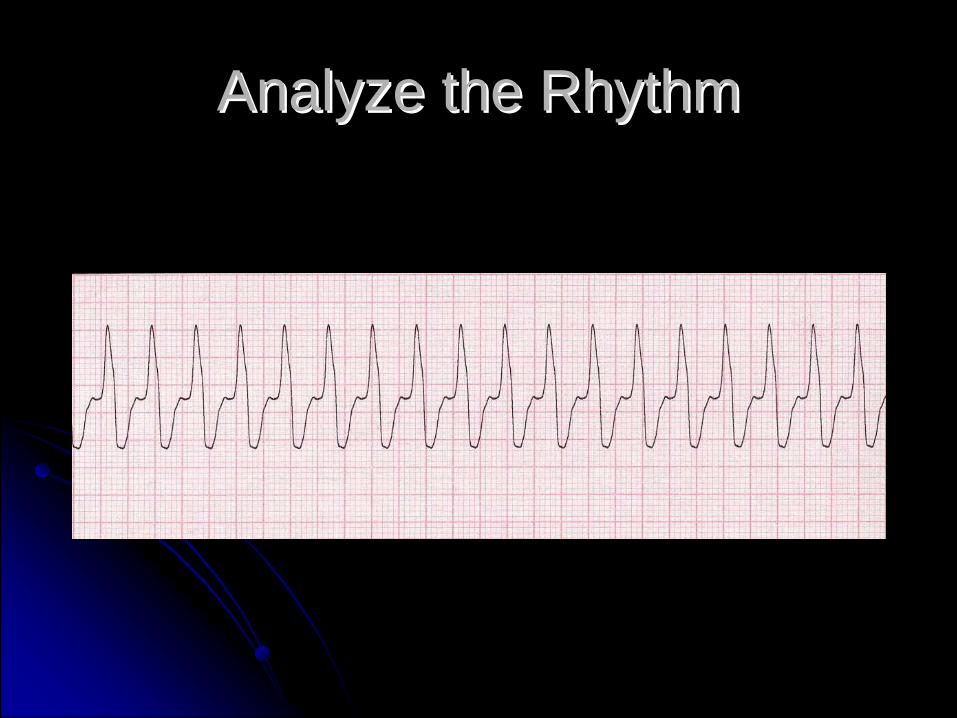
Analyze the RhythmAnalyze the Rhythm
Premature Atrial Complex (PAC)Premature Atrial Complex (PAC)
CharacteristicsCharacteristicsPaired Ectopic Beats referred to as coupletPaired Ectopic Beats referred to as coupletAlternating Ectopic Beat referred to as Bigeminy, Alternating Ectopic Beat referred to as Bigeminy, Trigeminy, or QuadrigeminyTrigeminy, or Quadrigeminy
e.g. Atrial Bigeminy or Ventricular Bigeminye.g. Atrial Bigeminy or Ventricular Bigeminy
May not always result in ventricular conductionMay not always result in ventricular conduction““Blocked PACBlocked PAC”” or or ““NonNon--conducted PACconducted PAC””
No compensatory pause in PACNo compensatory pause in PACCompensatory vs. Noncompensatory PauseCompensatory vs. Noncompensatory Pause
Compensatory vs Compensatory vs NoncompensatoryNoncompensatory PausePause
Compare the distance between 3 normal beatsCompare the distance between 3 normal beatsNoncompensatoryNoncompensatory
the normal beat following the premature complex occurs the normal beat following the premature complex occurs before it was expected (the distance not the same)before it was expected (the distance not the same)
CompensatoryCompensatorythe normal beat following the premature complex occurs the normal beat following the premature complex occurs when expected (the distance is the same)when expected (the distance is the same)

The most common cause for aThe most common cause for apause is a nonpause is a non--conducted PAC.conducted PAC.
Premature Atrial Complex (PAC)Premature Atrial Complex (PAC)
Premature Atrial Complex (PAC)Premature Atrial Complex (PAC)ManagementManagement
Usually not clinically significantUsually not clinically significanttreat underlying causetreat underlying cause
Frequent PACs may indicated enhanced Frequent PACs may indicated enhanced automaticity of atria or reentry mechanismautomaticity of atria or reentry mechanism
may warn of or initiate supraventricular arrhythmias may warn of or initiate supraventricular arrhythmias such as atrial tachycardia, atrial flutter, atrial such as atrial tachycardia, atrial flutter, atrial fibrillation or PSVTfibrillation or PSVTif nonconducted PACs are frequent and HR < 50, if nonconducted PACs are frequent and HR < 50, treat as bradycardiatreat as bradycardiaPACs may be wide (aberrant conduction) and must PACs may be wide (aberrant conduction) and must be differentiated form PVCsbe differentiated form PVCs
Wandering Atrial PacemakerWandering Atrial Pacemaker
PathophysiologyPathophysiologyshifting of pacemaker focus from one to another shifting of pacemaker focus from one to another within the atrial tissuewithin the atrial tissueMay be associated with ischemic disease involving May be associated with ischemic disease involving the sinus node or an inflammatory state (e.g. the sinus node or an inflammatory state (e.g. rheumatic fever)rheumatic fever)May occur without any finding of diseaseMay occur without any finding of disease
Wandering Atrial PacemakerWandering Atrial Pacemaker
CharacteristicsCharacteristicsHeart Rate:Heart Rate: usually 60usually 60--100 bpm100 bpmRhythmRhythm: irregularly irregular (one of three): irregularly irregular (one of three)PacemakerPacemaker SiteSite: variable, all within the atria : variable, all within the atria including SA nodeincluding SA nodeP WavesP Waves: variable including normal appearing P : variable including normal appearing P waveswavesPP--R IntervalR Interval: unequal, varies: unequal, variesRR--R IntervalR Interval: unequal, varies: unequal, variesQRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: usually one to one relationship: usually one to one relationship

Wandering Atrial PacemakerWandering Atrial Pacemaker
ManagementManagementECG rhythm generally does not require treatmentECG rhythm generally does not require treatmentUnderlying cause may require treatmentUnderlying cause may require treatment
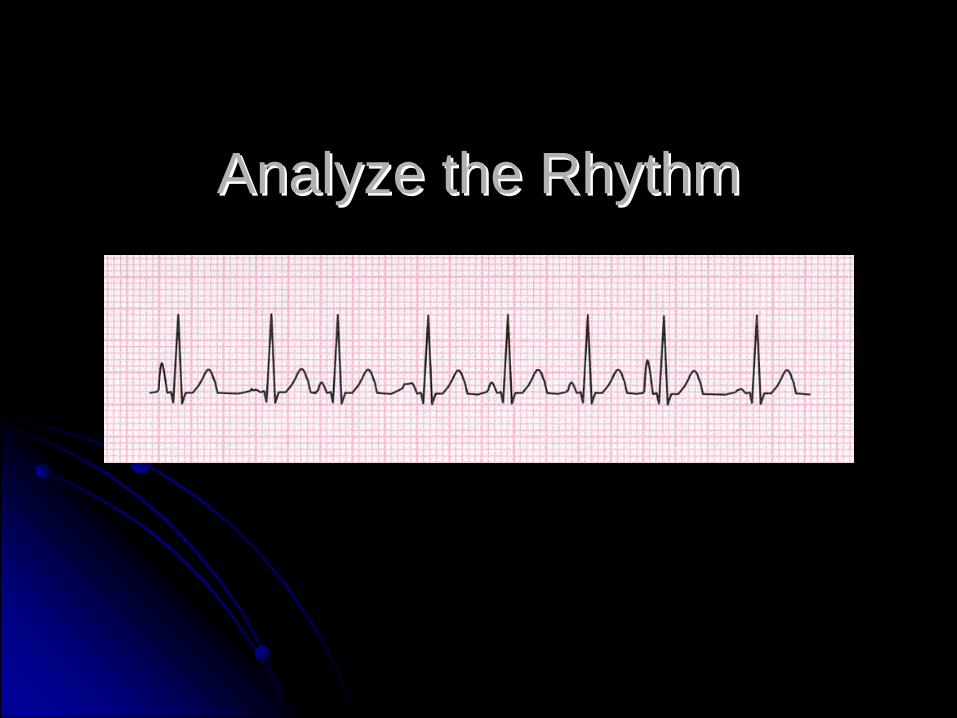
Analyze the RhythmAnalyze the Rhythm

Multifocal Atrial TachycardiaMultifocal Atrial Tachycardia
PathophysiologyPathophysiologySame as WAP just faster than 100 bpmSame as WAP just faster than 100 bpmAn uncommon ECG rhythmAn uncommon ECG rhythmUsually seen in someone with COPD or Usually seen in someone with COPD or severe systemic disease (e.g. sepsis, shock)severe systemic disease (e.g. sepsis, shock)
Multifocal Atrial TachycardiaMultifocal Atrial Tachycardia
CharacteristicsCharacteristicsHeart Rate:Heart Rate: >100 bpm>100 bpmRhythmRhythm: irregularly irregular (one of three): irregularly irregular (one of three)PacemakerPacemaker SiteSite: variable, all within the atria : variable, all within the atria including SA nodeincluding SA nodeP WavesP Waves: variable including normal appearing P : variable including normal appearing P waveswavesPP--R IntervalR Interval: unequal, varies: unequal, variesRR--R IntervalR Interval: unequal, varies: unequal, variesQRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: one to one relationship: one to one relationship

Analyze the RhythmAnalyze the Rhythm

Multifocal Atrial TachycardiaMultifocal Atrial Tachycardia
ManagementManagementTreated like Supraventricular TachycardiaTreated like Supraventricular TachycardiaBe alert to signs of heart failureBe alert to signs of heart failure
Tachycardia Management Tachycardia Management OverviewOverview
If If Unstable Unstable : : Immediate Synchronized Immediate Synchronized CardioversionCardioversion
If Stable:If Stable:IV/OIV/O22/Monitor/12 lead ECG/Monitor/12 lead ECGIdentify Rhythm using 12 lead if necessaryIdentify Rhythm using 12 lead if necessaryDrug therapyDrug therapyIf drugs fail, then synchronized cardioversionIf drugs fail, then synchronized cardioversion
Tachycardia: Narrow ComplexTachycardia: Narrow Complex
Primary/Secondary ABCDPrimary/Secondary ABCDVagal maneuversVagal maneuversAdenosine 6 mg rapid IV push, with flushAdenosine 6 mg rapid IV push, with flush
Repeat with 12 mg rapid IV push with flushRepeat with 12 mg rapid IV push with flush
Other ConsiderationsOther Considerationsamiodarone 150 mg slow IV (15 mg/min)amiodarone 150 mg slow IV (15 mg/min)diltiazemdiltiazem 0.25 mg/kg slow IV 0.25 mg/kg slow IV synchronized cardioversionsynchronized cardioversion
Atrial FlutterAtrial FlutterSignatureSignature
““Saw toothSaw tooth”” baselinebaselineCommonly occurs in multiplesCommonly occurs in multiples
300, 300, 150150, 75, 75based on degree of AV blockbased on degree of AV block

Atrial FlutterAtrial Flutter
Atrial FlutterAtrial FlutterCausesCauses
Myocardial ischemiaMyocardial ischemiaHypoxiaHypoxiaCHFCHFCOPD (cor pulmonale)COPD (cor pulmonale)HyperthyroidismHyperthyroidismDigitalis toxicityDigitalis toxicity
Not a common dysrhythmiaNot a common dysrhythmia
Atrial FlutterAtrial FlutterCharacteristicsCharacteristics
Heart Rate:Heart Rate: usually multiples usually multiples -- 300, 150, 75300, 150, 75RhythmRhythm: usually regular except with variable AV : usually regular except with variable AV blockblockPacemakerPacemaker SiteSite: atrial site: atrial siteP WavesP Waves: No P waves; Flutter (F) waves: No P waves; Flutter (F) wavesPP--R IntervalR Interval: not applicable: not applicableRR--R IntervalR Interval: usually equal except with variable AV : usually equal except with variable AV blockblockQRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: not applicable: not applicable

Analyze the RhythmAnalyze the Rhythm

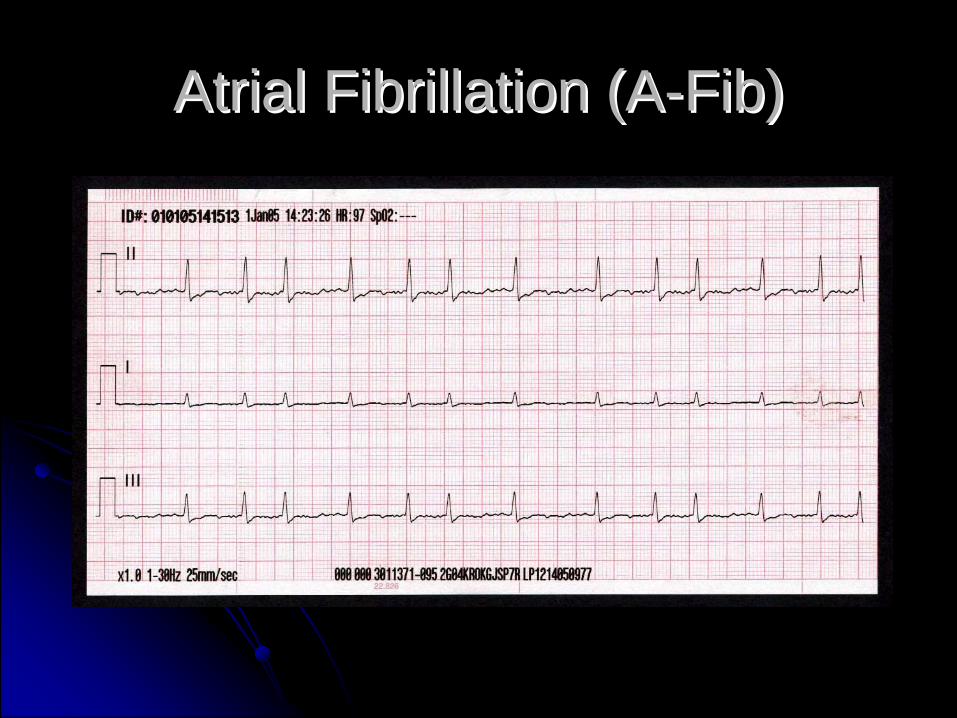
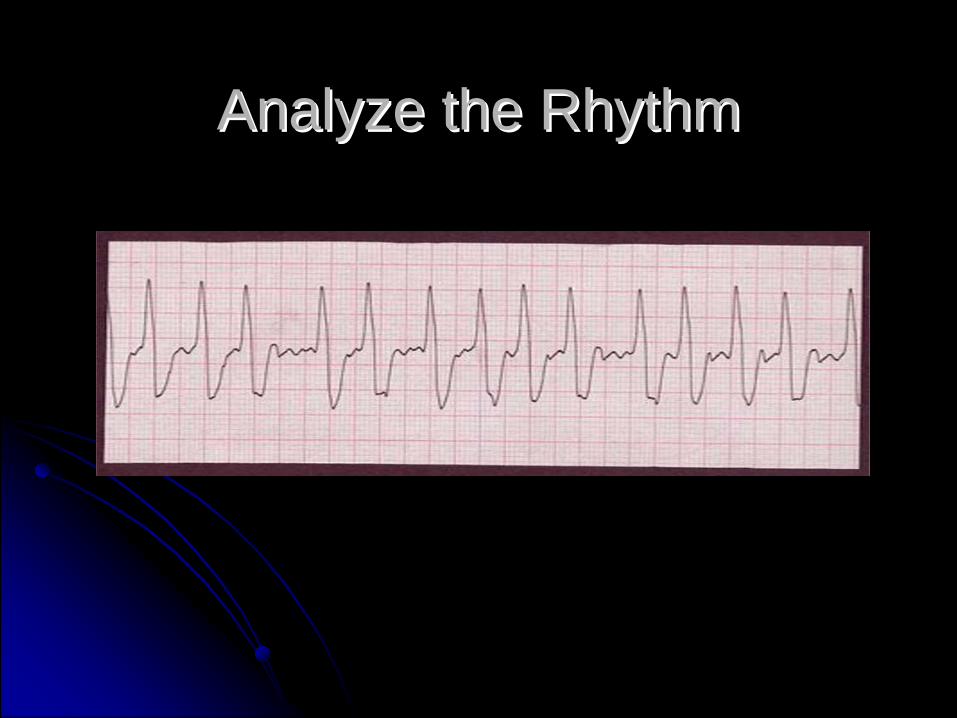
Atrial Fibrillation (AAtrial Fibrillation (A--Fib)Fib)
SignatureSignatureIrregularly irregularIrregularly irregularNo organized atrial activityNo organized atrial activity
TypesTypesAA--Fib with uncontrolled ventricular response Fib with uncontrolled ventricular response (rate > 100, usually 160(rate > 100, usually 160--180)180)AA--Fib with controlled ventricular responseFib with controlled ventricular response(rate < 100, usually 60(rate < 100, usually 60--70)70)
Atrial Fibrillation (AAtrial Fibrillation (A--Fib)Fib)
Atrial FibrillationAtrial FibrillationCharacteristicsCharacteristics
Heart Rate:Heart Rate: atrial rate may be very fast, avg of 400 atrial rate may be very fast, avg of 400 bpm; variable ventricular ratebpm; variable ventricular rateRhythmRhythm: irregularly irregular: irregularly irregularPacemakerPacemaker SiteSite: multiple atrial sites: multiple atrial sitesP WavesP Waves: No P waves; fibrillation (f) waves: No P waves; fibrillation (f) wavesPP--R IntervalR Interval: not applicable: not applicableRR--R IntervalR Interval: usually unequal : usually unequal QRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: not applicable: not applicable
Analyze the RhythmAnalyze the Rhythm
Atrial FibrillationAtrial FibrillationCausesCauses
Myocardial ischemiaMyocardial ischemiaHypoxiaHypoxiaCHFCHFCOPD (cor pulmonale)COPD (cor pulmonale)HyperthyroidismHyperthyroidismDigitalis toxicityDigitalis toxicityIdiopathicIdiopathic
Atrial FibrillationAtrial Fibrillation
PresentationPresentationParoxysmalParoxysmalAcuteAcuteChronicChronic
Atrial FibrillationAtrial Fibrillation
ComplicationsComplicationsLoss of atrial kickLoss of atrial kickThrombus formationThrombus formationEmboliEmboli
Tachycardia: A.fib/A. flutterTachycardia: A.fib/A. flutter
Primary/Secondary ABCDPrimary/Secondary ABCDAssess for WPW Assess for WPW –– Delta waveDelta wave
No WPWNo WPWCalcium channel blockersCalcium channel blockers
WPWWPWamiodarone 150 mg slow IV (15 mg/min)amiodarone 150 mg slow IV (15 mg/min)
Atrial Fib/Flutter TreatmentAtrial Fib/Flutter TreatmentRapid Response/Stable with SymptomsRapid Response/Stable with Symptoms
Oxygen, Monitor, IVOxygen, Monitor, IVVagal maneuvers (if needed as a diagnostic tool)Vagal maneuvers (if needed as a diagnostic tool)No WPWNo WPW
DiltiazemDiltiazem, 0.25 mg/kg slow IV over 2 min, may repeat i15 , 0.25 mg/kg slow IV over 2 min, may repeat i15 min at 0.35 mg/kg slow IV min at 0.35 mg/kg slow IV
WPWWPWamiodarone 150 mg slow IV (15 mg/min)amiodarone 150 mg slow IV (15 mg/min)

Atrial Fib/Flutter TreatmentAtrial Fib/Flutter TreatmentRapid Response/UnstableRapid Response/Unstable
Oxygen, Monitor, IVOxygen, Monitor, IVSedateSedateCardioversionCardioversionConsider anticoagulation firstConsider anticoagulation first
Atrial Fib/Flutter TreatmentAtrial Fib/Flutter Treatment
Slow Response/Unstable (usually occurs in Slow Response/Unstable (usually occurs in AA--Flutter)Flutter)
Oxygen, Monitor, IVOxygen, Monitor, IVAtropineAtropinePacemakerPacemakerDopamine or epinephrine infusionDopamine or epinephrine infusion

Atrial Fib/Flutter TreatmentAtrial Fib/Flutter Treatment
Normal (controlled) RateNormal (controlled) RateOxygen, Monitor, IVOxygen, Monitor, IVEvaluate, treat underlying problemsEvaluate, treat underlying problems
Patient may have CHF with pulmonary Patient may have CHF with pulmonary edema or Acute MIedema or Acute MI
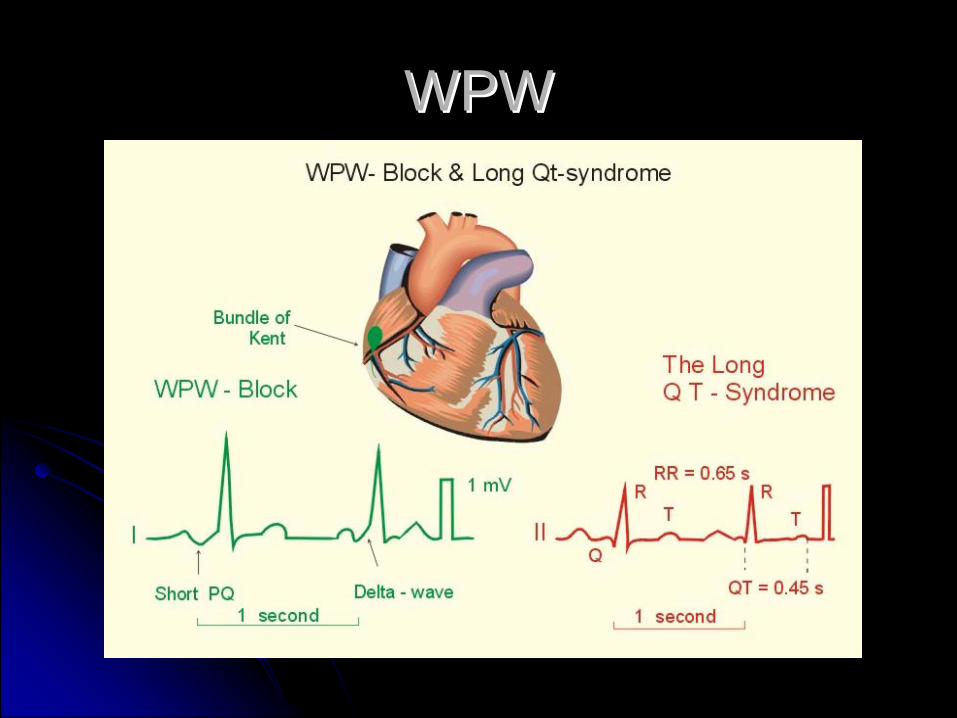
WPWWPW
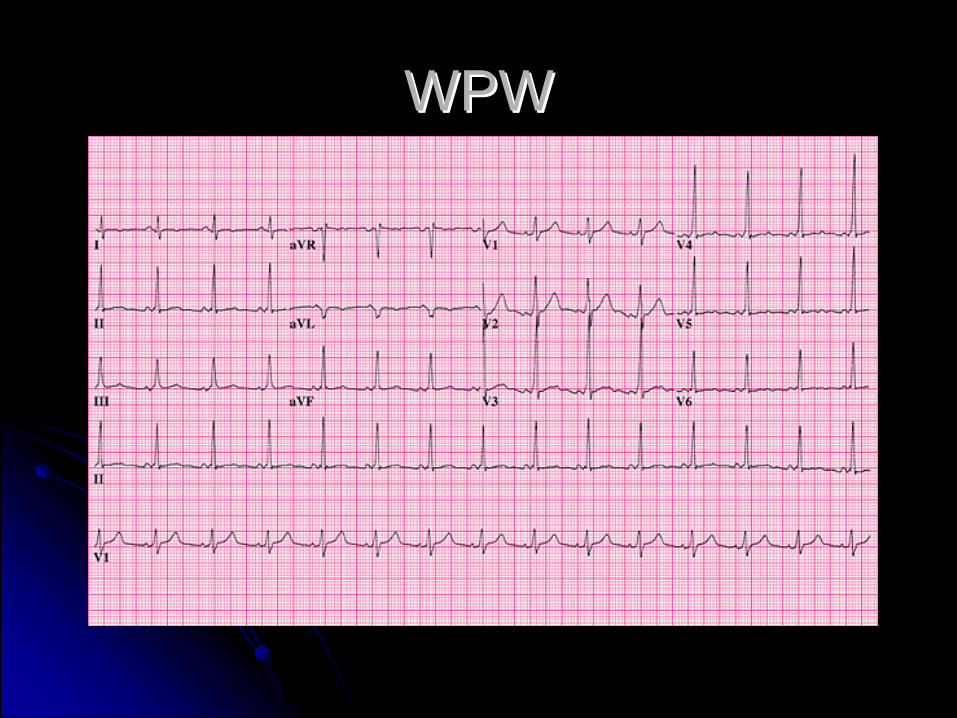
WPWWPW
Supraventricular Tachycardia (SVT)Supraventricular Tachycardia (SVT)
Supraventricular origin that is:Supraventricular origin that is:NotNot a sinus rhythma sinus rhythmNotNot atrial fibrillation or flutteratrial fibrillation or flutterNotNot WAP or MATWAP or MAToften segregated intooften segregated into
Nonparoxysmal Atrial Tachycardia (ectopic)Nonparoxysmal Atrial Tachycardia (ectopic)Paroxysmal Supraventricular Tachycardia (reentry)Paroxysmal Supraventricular Tachycardia (reentry)
Very often cannot distinguish between the twoVery often cannot distinguish between the two
Supraventricular TachycardiaSupraventricular Tachycardia
Nonparoxysmal Atrial TachNonparoxysmal Atrial TachEnhanced automaticityEnhanced automaticityPatient cannot pinpoint onsetPatient cannot pinpoint onsetOften caused by digitalis toxicityOften caused by digitalis toxicity
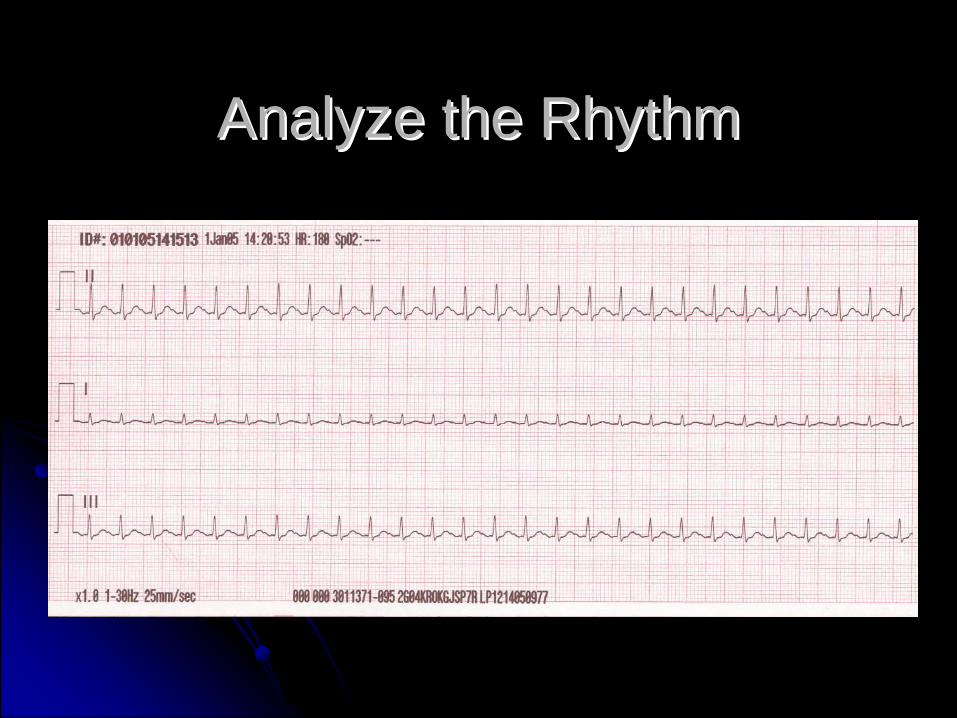
Analyze the RhythmAnalyze the Rhythm
Analyze the RhythmAnalyze the Rhythm
Analyze the RhythmAnalyze the Rhythm
Analyze the RhythmAnalyze the Rhythm
Supraventricular TachycardiaSupraventricular Tachycardia
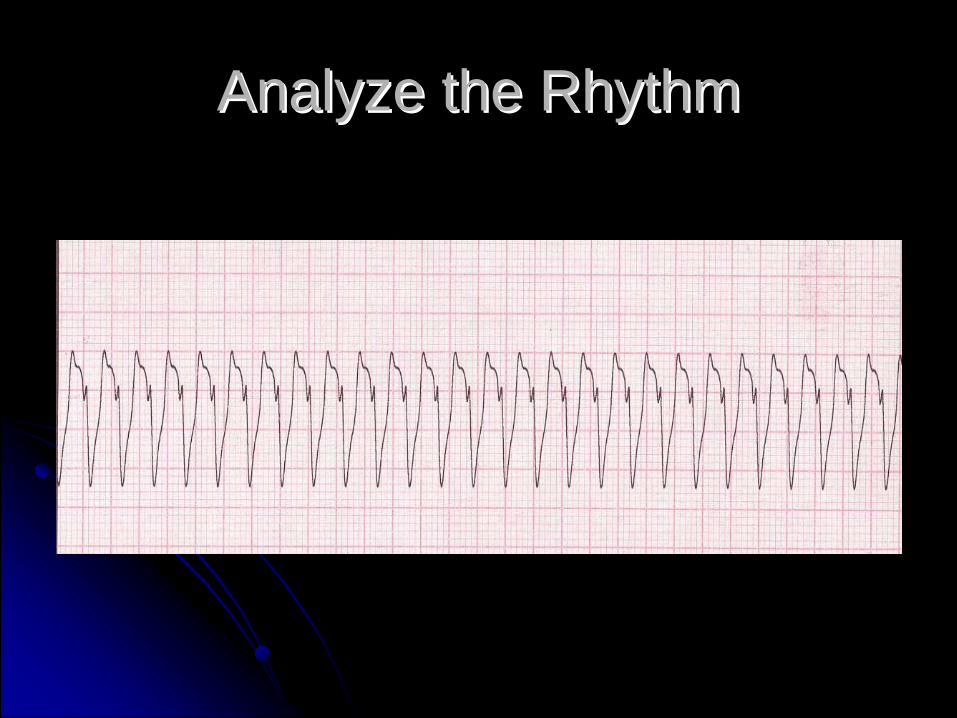
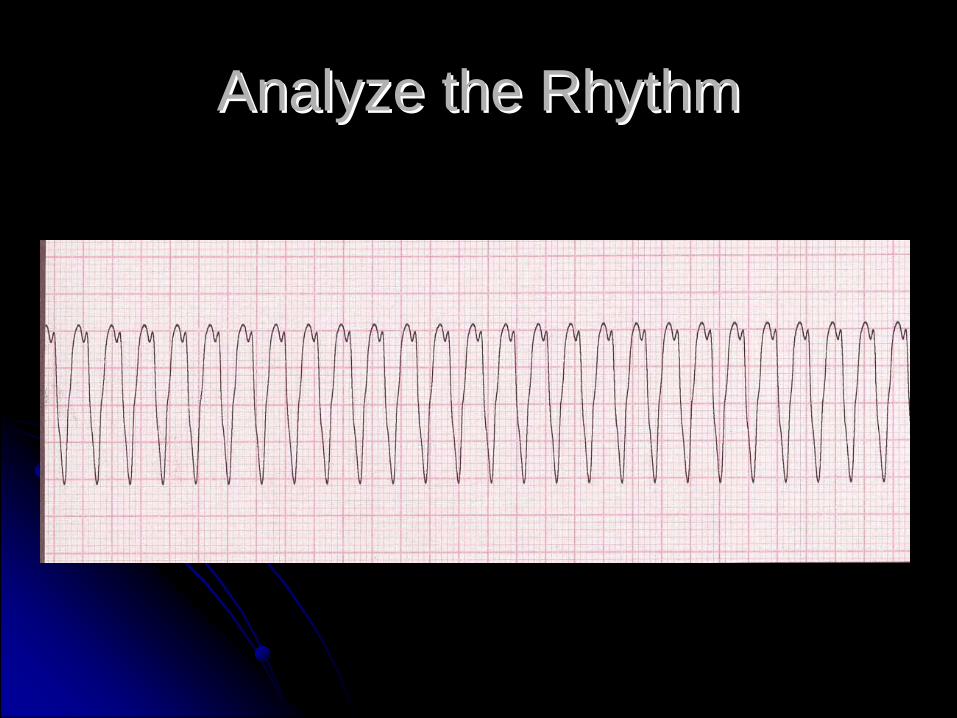
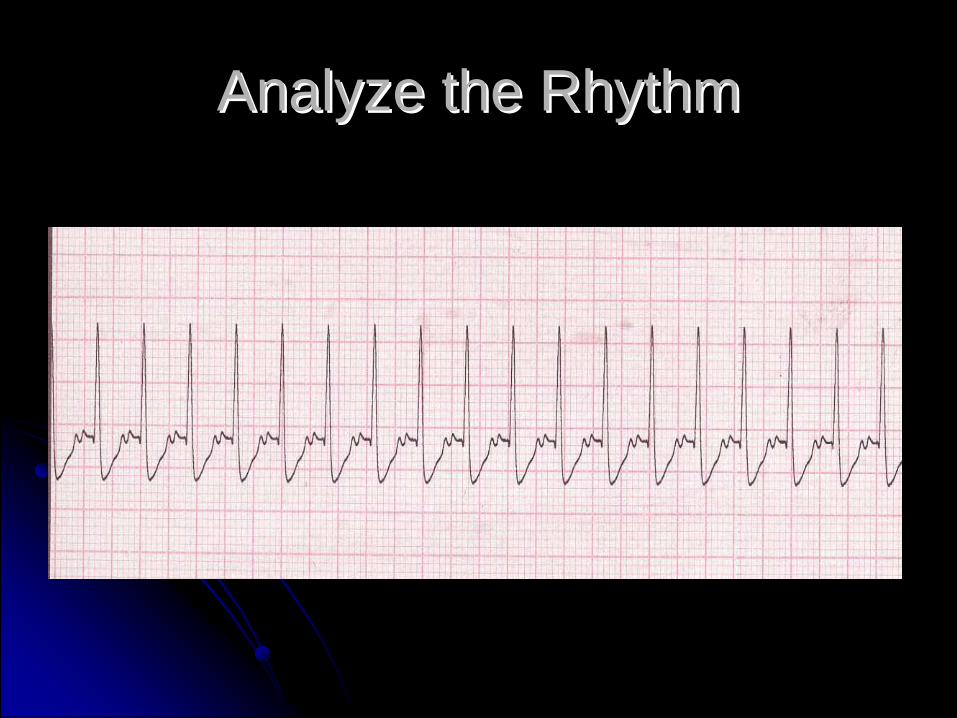
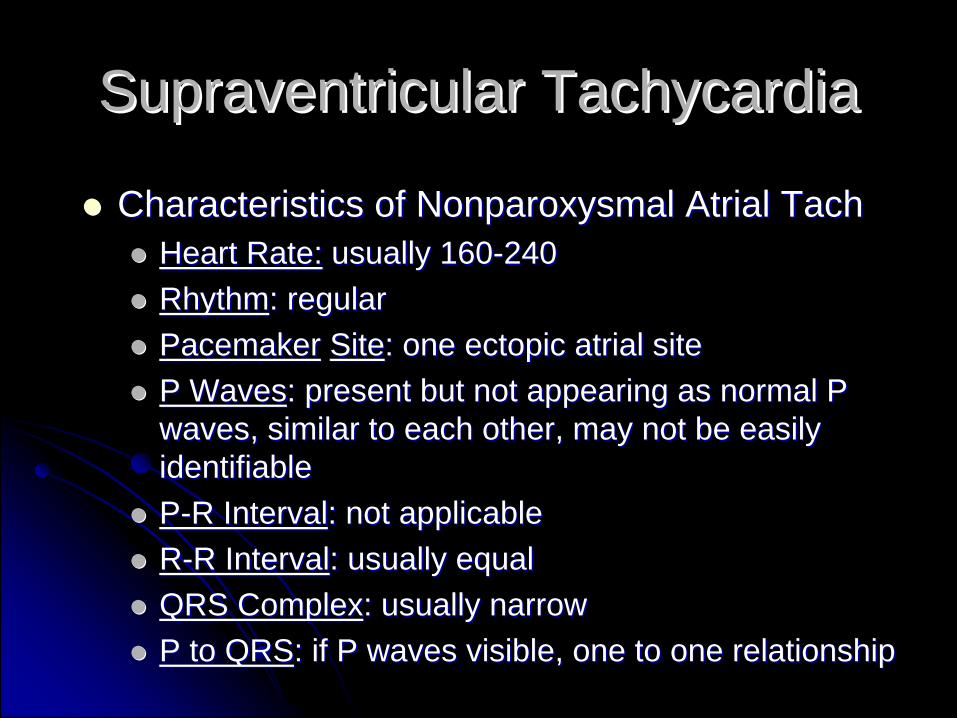
Characteristics of Nonparoxysmal Atrial TachCharacteristics of Nonparoxysmal Atrial TachHeart Rate:Heart Rate: usually 160usually 160--240240RhythmRhythm: regular: regularPacemakerPacemaker SiteSite: one ectopic atrial site: one ectopic atrial siteP WavesP Waves: present but not appearing as normal P : present but not appearing as normal P waves, similar to each other, may not be easily waves, similar to each other, may not be easily identifiableidentifiablePP--R IntervalR Interval: not applicable: not applicableRR--R IntervalR Interval: usually equal : usually equal QRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: if P waves visible, one to one relationship: if P waves visible, one to one relationship
Analyze the RhythmAnalyze the Rhythm

Supraventricular TachycardiaSupraventricular Tachycardia
Nonparoxysmal Atrial TachNonparoxysmal Atrial TachManagementManagement
Correct underlying cause if possibleCorrect underlying cause if possibleIf hemodynamically unstable:If hemodynamically unstable:
consider immediate cardioversionconsider immediate cardioversion
If hemodynamically If hemodynamically stablestable, consider:, consider:Diltiazem, 0.25 mg/kg slow IV over 2 min, may Diltiazem, 0.25 mg/kg slow IV over 2 min, may repeat in 15 mins at 0.35 mg/kg slow IVrepeat in 15 mins at 0.35 mg/kg slow IVMetoprolol, 5 mg slow IV over 2Metoprolol, 5 mg slow IV over 2--5 mins, may repeat 5 mins, may repeat in 5 minin 5 minAmiodarone, 150 mg IV infusion over 10 minsAmiodarone, 150 mg IV infusion over 10 mins
Supraventricular TachycardiaSupraventricular TachycardiaParoxysmal Supraventricular Tachycardia Paroxysmal Supraventricular Tachycardia (PSVT)(PSVT)
CausesCausesreentry mechanism at AV junction with or without an reentry mechanism at AV junction with or without an accessory pathwayaccessory pathwayonset may occur due toonset may occur due to
increased sympathetic toneincreased sympathetic tonestimulant usestimulant useelectrolyte abnormalitieselectrolyte abnormalitiesanxiety/emotional stressanxiety/emotional stress
Clinical significance dependent on rate and Clinical significance dependent on rate and underlying cardiac functionunderlying cardiac function

Supraventricular TachycardiaSupraventricular TachycardiaParoxysmal Supraventricular Tachycardia Paroxysmal Supraventricular Tachycardia (PSVT)(PSVT)
Episodes begin/end suddenlyEpisodes begin/end suddenlyHealthy patients c/o palpitationsHealthy patients c/o palpitationsPatients with heart disease c/oPatients with heart disease c/o
WeaknessWeaknessDizzinessDizzinessShortness of breathShortness of breathChest painChest painPulmonary edemaPulmonary edema

Supraventricular TachycardiaSupraventricular Tachycardia
Characteristics of Paroxysmal SVTCharacteristics of Paroxysmal SVTHeart Rate:Heart Rate: usually 160usually 160--240240RhythmRhythm: regular: regularPacemakerPacemaker SiteSite: one ectopic atrial site: one ectopic atrial siteP WavesP Waves: usually not identifiable: usually not identifiablePP--R IntervalR Interval: not applicable: not applicableRR--R IntervalR Interval: usually equal : usually equal QRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: not applicable: not applicable
Supraventricular TachycardiaSupraventricular TachycardiaManagementManagementOxygen, Monitor, IVOxygen, Monitor, IVAssess for Stable vs UnstableAssess for Stable vs Unstable
If UnstableIf UnstableImmediately cardiovertImmediately cardiovert
Supraventricular TachycardiaSupraventricular TachycardiaAssess for Stable vs Unstable (cont)Assess for Stable vs Unstable (cont)
If StableIf StableVagal maneuversVagal maneuvers
Avoid in digitalis toxicityAvoid in digitalis toxicityMay produce AV blocks or asystoleMay produce AV blocks or asystole
AdenosineAdenosine6 mg RAPID IV push, may repeat in 16 mg RAPID IV push, may repeat in 1--2 minutes at 12 mg 2 minutes at 12 mg RAPID IV push, then 12 mg RAPID IV pushRAPID IV push, then 12 mg RAPID IV pushfollow each dose follow each dose immediatelyimmediately with a 10with a 10--20 cc flush20 cc flushBlocks conduction through AV nodeBlocks conduction through AV nodeMay produce transient aystoleMay produce transient aystoleShort halfShort half--life (<6 seconds)life (<6 seconds)Drug InteractionsDrug Interactions

Supraventricular TachycardiaSupraventricular TachycardiaAssess for Stable vs Unstable (cont)Assess for Stable vs Unstable (cont)
If Stable PSVT remains after Adenosine and vagal If Stable PSVT remains after Adenosine and vagal maneuver, may consider:maneuver, may consider:
Beta blockerBeta blockerMetoprolol, 5 mg slow IV over 2Metoprolol, 5 mg slow IV over 2--5 mins, may repeat in 5 5 mins, may repeat in 5 minminONLYONLY if NO history of heart disease or CHFif NO history of heart disease or CHF
DiltiazemDiltiazem0.25 mg/kg slow IV over 2 min, may repeat in 15 mins at 0.25 mg/kg slow IV over 2 min, may repeat in 15 mins at 0.35 mg/kg slow IV0.35 mg/kg slow IV
AmiodaroneAmiodarone150 mg IV infusion over 10 mins150 mg IV infusion over 10 mins
Synchronized CardioversionSynchronized Cardioversion
Sedate, if possibleSedate, if possibleValium 5 to 10 mg IV orValium 5 to 10 mg IV orVersed 2.5 Versed 2.5 -- 5 mg IV5 mg IVAdminister slowlyAdminister slowly
may cause hypotension and/or respiratory may cause hypotension and/or respiratory depressiondepression
Administer to produce amnestic effectAdminister to produce amnestic effectPrepare for Synchronized cardioversionPrepare for Synchronized cardioversion
Synchronized CardioversionSynchronized Cardioversion
Energy SettingsEnergy Settings50 J (PSVT/Atrial Flutter)50 J (PSVT/Atrial Flutter)100J100J200J200J300J300J360J360J
Digitalis Toxicity: CAUTION!Digitalis Toxicity: CAUTION!Cardioversion may produce VFCardioversion may produce VF
Vagal ManeuversVagal ManeuversIncrease parasympathetic toneIncrease parasympathetic toneSlow heart rateSlow heart rateSlow conduction through AV nodeSlow conduction through AV nodeManeuversManeuvers
Valsalva maneuverValsalva maneuverHave patient hold breath, bear downHave patient hold breath, bear down““Bear down as if having a bowel movementBear down as if having a bowel movement””

Vagal ManeuversVagal ManeuversCarotid sinus massageCarotid sinus massage
USE with extreme caution USE with extreme caution IFIF at all!at all!ContraindicationsContraindications
Patient >50Patient >50History of CVA or heart diseaseHistory of CVA or heart diseaseCarotid bruitCarotid bruitUnequal carotidsUnequal carotids
ProcedureProcedureBegin with right carotidBegin with right carotidMassage 15 to 20 secondsMassage 15 to 20 secondsWait 2 to 3 minutes, go to left carotidWait 2 to 3 minutes, go to left carotidOnly one carotid at a timeOnly one carotid at a time
Vagal ManeuversVagal Maneuvers
Divers ReflexDivers ReflexHold breath, immerse face in cold waterHold breath, immerse face in cold waterCan be combined with Valsalva maneuverCan be combined with Valsalva maneuverContraindicated in ischemic heart diseaseContraindicated in ischemic heart diseaseUsually performed in young childrenUsually performed in young children

Junctional RhythmsJunctional Rhythms
Premature Junctional ComplexPremature Junctional Complex
PathophysiologyPathophysiologyEarly complex originating from the AV nodeEarly complex originating from the AV nodeCausesCauses
Digitalis toxicity (most common cause)Digitalis toxicity (most common cause)Increased vagal toneIncreased vagal toneHypoxiaHypoxiaCAD usually following AMICAD usually following AMI
A premature complex, NOT an ECG rhythmA premature complex, NOT an ECG rhythm

Premature Junctional ComplexPremature Junctional Complex
Premature Junctional ComplexPremature Junctional Complex
CharacteristicsCharacteristicsHeart Rate:Heart Rate: dependent on underlying rhythmdependent on underlying rhythmRhythmRhythm: irregular due to PJC: irregular due to PJCPacemakerPacemaker SiteSite: dependent on underlying rhythm: dependent on underlying rhythmP WavesP Waves: dependent on underlying rhythm; P wave may : dependent on underlying rhythm; P wave may be inverted, buried in QRS, absent or after QRSbe inverted, buried in QRS, absent or after QRSPP--R IntervalR Interval: dependent on underlying rhythm: dependent on underlying rhythmRR--R IntervalR Interval: dependent on underlying rhythm: dependent on underlying rhythmQRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: not applicable: not applicable
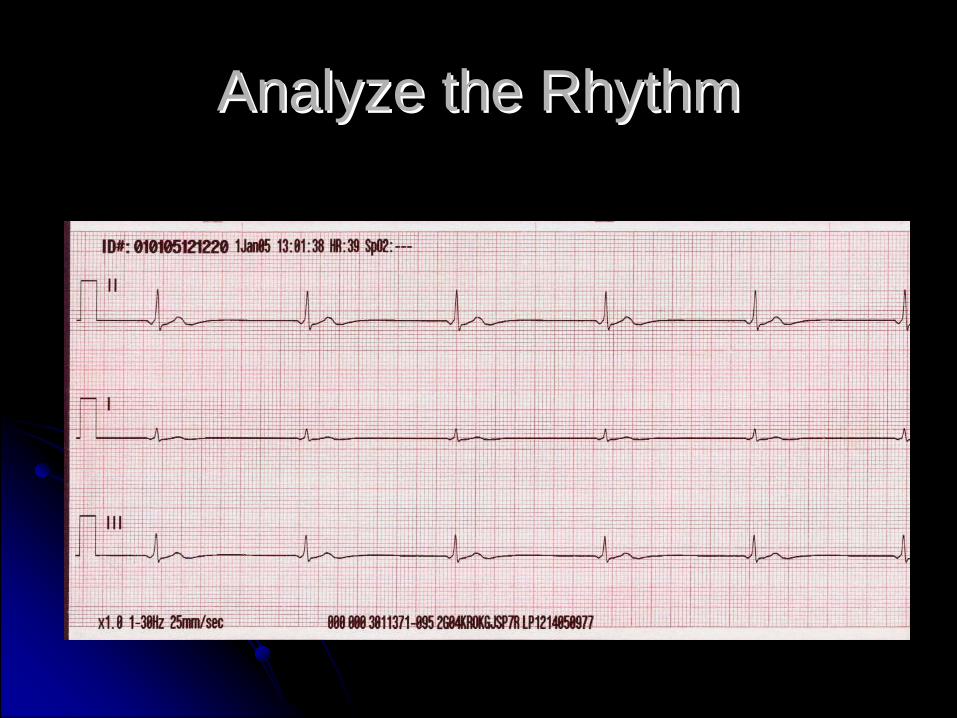
Analyze the RhythmAnalyze the Rhythm
PJCsPJCs
ManagementManagementGenerally No TreatmentGenerally No TreatmentAssess Underlying CauseAssess Underlying CauseQuinidine, Procainamide may be consideredQuinidine, Procainamide may be considered
Analyze the RhythmAnalyze the Rhythm

Junctional Escape RhythmJunctional Escape Rhythm
CausesCausesSA Node DiseaseSA Node DiseaseIncreased Vagal ToneIncreased Vagal ToneDigitalisDigitalisInferior Wall MIInferior Wall MINormal on Temporary BasisNormal on Temporary Basis
Junctional Escape RhythmJunctional Escape RhythmCharacteristicsCharacteristics
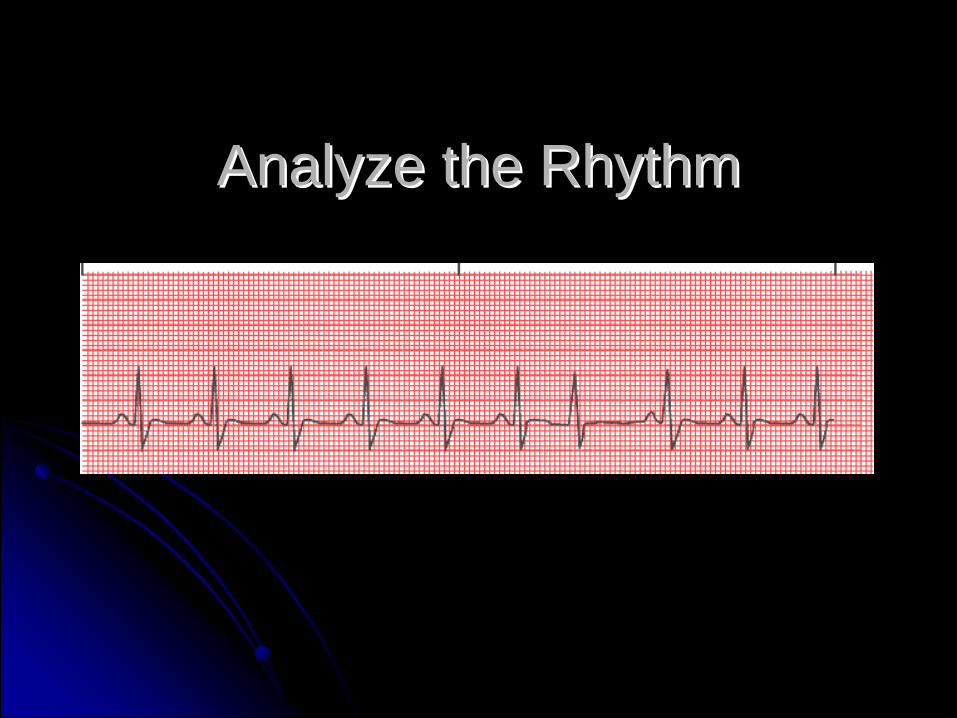
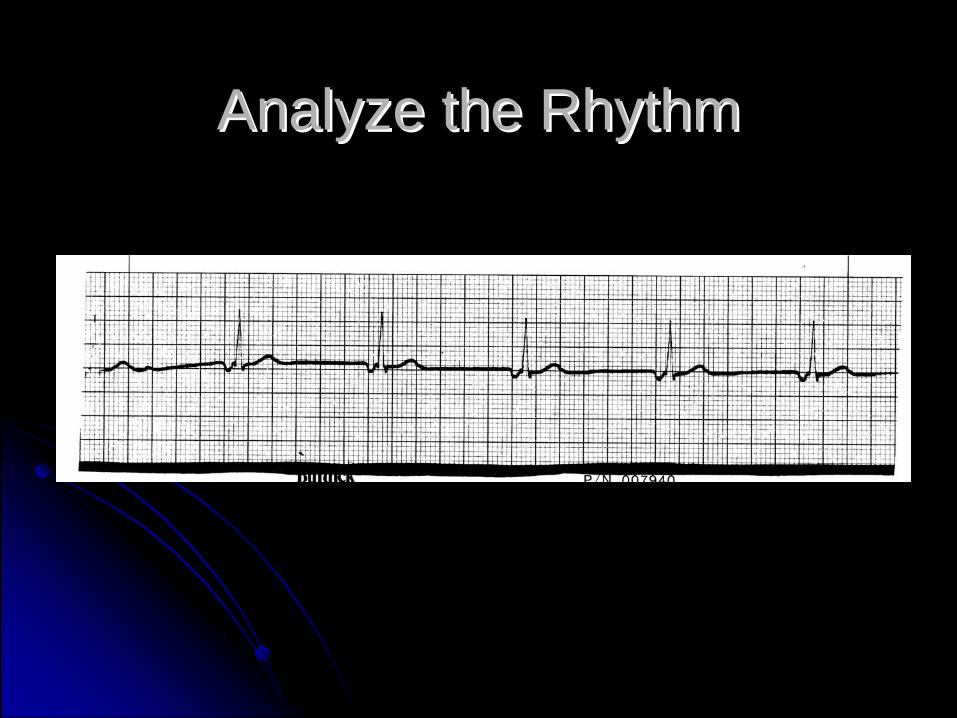
Heart Rate:Heart Rate: usually 40usually 40--60 bpm60 bpmRhythmRhythm: ventricular rhythm is regular: ventricular rhythm is regularPacemakerPacemaker SiteSite: escape pacemaker in the AV junction: escape pacemaker in the AV junctionP WavesP Waves: may or may not be present; may precede, be : may or may not be present; may precede, be buried in or follow QRS; abnormal appearingburied in or follow QRS; abnormal appearingPP--R IntervalR Interval: usually abnormally short: usually abnormally shortRR--R IntervalR Interval: usually regular: usually regularQRS ComplexQRS Complex: usually narrow: usually narrowP to QRSP to QRS: may not be applicable: may not be applicable
Analyze the RhythmAnalyze the Rhythm
Junctional Escape RhythmJunctional Escape Rhythm
ManagementManagementTreat Only if UnstableTreat Only if UnstableManage as Unstable BradycardiaManage as Unstable Bradycardia
Accelerated Junctional RhythmAccelerated Junctional Rhythm
CausesCausesEnhanced AV junction automaticityEnhanced AV junction automaticityUsually digitalis toxicityUsually digitalis toxicity
CharacteristicsCharacteristicsSame as Junctional Escape Rhythm except Same as Junctional Escape Rhythm except HR > 60 but < 100 bpmHR > 60 but < 100 bpm
ManagementManagementOxygen, monitor, IVOxygen, monitor, IVTreat the underlying causeTreat the underlying causeObserve for other arrhythmiasObserve for other arrhythmias
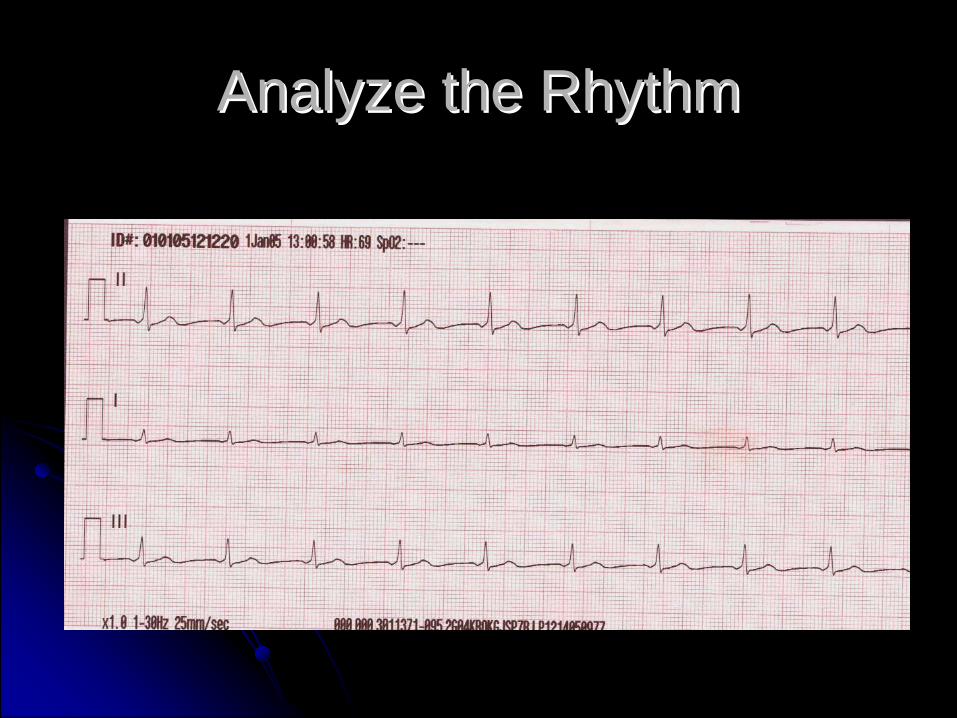
Analyze the RhythmAnalyze the Rhythm
Junctional TachycardiaJunctional TachycardiaCausesCauses
Myocardial ischemiaMyocardial ischemiaStimulantsStimulantsDigitalis toxicityDigitalis toxicity
CharacteristicsCharacteristicsSame as Junctional Escape Rhythm exceptSame as Junctional Escape Rhythm exceptHR > 100HR > 100
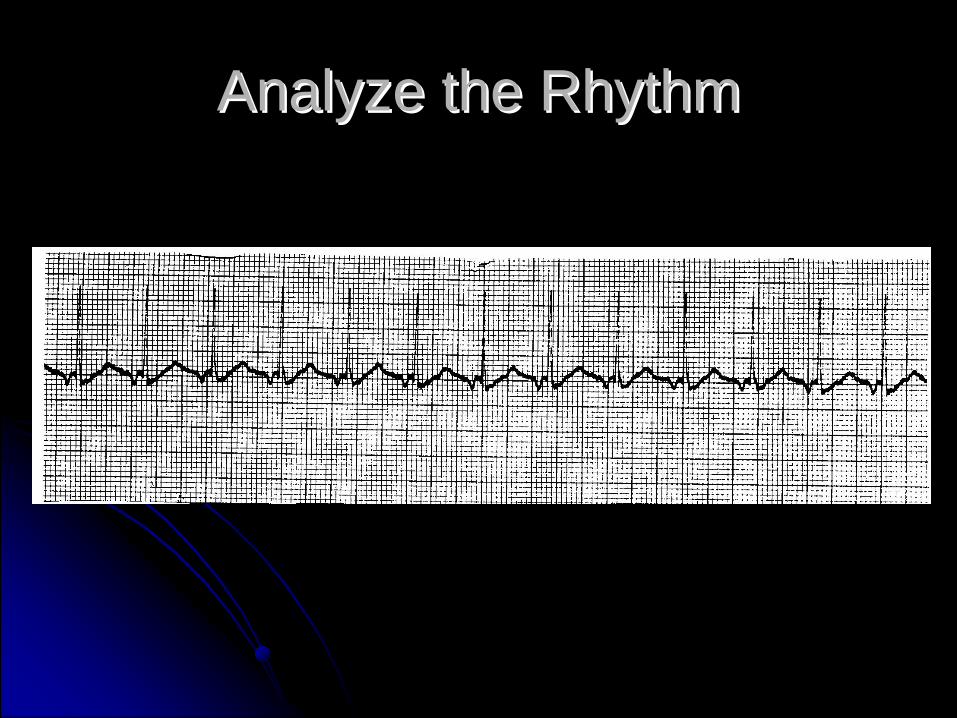
Analyze the RhythmAnalyze the Rhythm
Junctional TachycardiaJunctional Tachycardia
ManagementManagementConsider the possibility of Digitalis ToxicityConsider the possibility of Digitalis ToxicityStableStable
Oxygen, Monitor, IVOxygen, Monitor, IVVagal ManeuversVagal ManeuversDiltiazem or VerapamilDiltiazem or Verapamil
Junctional TachycardiaJunctional Tachycardia
ManagementManagementUnstableUnstable
Oxygen, Monitor, IVOxygen, Monitor, IVSedateSedateCardiovertCardiovert
Questions?Questions?













![Dysrhythmias (002) [Read-Only] - Aventri · Atrial AV node Ventricular Classification of Rhythm Abnormalities Supraventricular Atrial origin Atrial fibrillation Atrial flutter Atrial](https://img.pdfslide.net/doc/110x75/5f024baa7e708231d4038f22/dysrhythmias-002-read-only-aventri-atrial-av-node-ventricular-classification.jpg)