Embed Size (px)
Citation preview

Europace (2002) 4, 229–239doi:10.1053/eupc.2002.0251, available online at http://www.idealibrary.com on
ATRIAL FLUTTER
Atypical atrial flutters
P. Ricard, M. Imianitoff, K. Yaıci, J. M. Coutelour, M. Bergonzi, J. P. Rinaldi,N. Saoudi
Centre Hospitalier Princess Grace, Avenue Pasteur, 98012, Monaco
Manuscript submitted 11 April 2002, and accepted 16 April 2002.
Correspondence: Nadir Saoudi MD, Centre Hospitalier PrincesseGrace, Avenue Pasteur, 98012 Monaco (Principaute). Fax: 377 9798 96 90; E-mail: [email protected]
Typical atrial flutter is due to a counterclockwise macro-re-entry circuit localized in the right atrium with a surfaceECG pattern showing predominantly negative F waves inthe inferior leads and positive F waves in V1. Recently it hasbeen proposed to classify atrial flutter on the basis of itscavo-tricuspid isthmus dependence rather than on the ECGpattern. Therefore some atrial flutters are considered typi-cal even if the ECG does not exhibit a typical pattern. Thisis the case for reverse typical atrial flutter, lower loopre-entry and partial-isthmus-dependent short circuit flutter.The term atypical flutter refers to a non-isthmus dependent
1099–5129/02/030229+11 $35.00/0 � 2002 Published by Else
flutter. Usually these patients have had previous cardiacsurgery with a right or left atriotomy. Flutter involving aspontaneous right atrial scar is not uncommon.(Europace 2002; 4: 229–239)� 2002 Published by Elsevier Science Ltd on behalf ofThe European Society of Cardiology
Key Words: Atrial flutter, common atrial flutter, typicalatrial flutter, atypical atrial flutter, cavotricuspid isthmusre-entry arrhythmia, atrial scars.
orifices of the inferior and superior vena cava and theEustachian ridge as well as a functional barrier whichfor most (but not all) authors is the crista terminalis(Fig. 1)[4–6]. The direction of activation is usuallycounterclockwise, descending the anterior and lateralwalls and ascending the septal and posterior wall ofthe right atrium. Since the activation is dependent onthe cavotricuspid isthmus, radiofrequency ablation ofthis arrhythmia has been shown to be effective[7].However, it is of note that there is no perfect concor-dance between the ECG pattern, the mechanism of thearrhythmia and its dependence to the cavotricuspidisthmus as assessed by entrainment mapping tech-niques (Fig. 2)[5,8]. For instance, some flutters showinga typical ECG pattern may not be isthmus dependent(Fig. 3) and conversely an atypical ECG can be depen-dent on isthmus activation, for example during clockwisere-entry but also for various other reasons (Fig. 4). Thus,it has been recently proposed to classify flutters on thebasis of the mechanism of the arrhythmia and its isthmusdependence rather than on the ECG pattern. In theframe of this classification, are considered typical fluttersthat are dependent on the cavotricuspid isthmus regard-less of the ECG pattern[9]. Therefore the term atypicalrefers to a non-isthmus-dependent flutter. We would like
Atrial flutter is classically referred to as a regulartachycardia with a cycle length shorter than 250 ms andthe absence of an isoelectric baseline between atrialdeflections in at least one lead[1–3]. The previous classi-fication of atrial flutter was typically based only on theECG and did not take into account the mechanism ofthe arrhythmia. The first description of typical atrialflutter was presented by Sir Thomas Lewis in 1912[1].The ECG was characteristic of this arrhythmia showinga ‘saw tooth’ pattern in leads II, III, and/or aVF madeby a succession of downsloping straight segments, fol-lowed by a sharp negative deflection and by an upstrokeand a slight overshoot leading to the next cycle. In leadV1 a positive deflection is usually seen but a biphasicdeflection may also be detected. Later studies, mostly byPuech in the early sixties, showed that the mechanismof this arrhythmia is a large re-entrant right atrial circuitbounded anteriorly by the tricuspid annulus and pos-teriorly by several anatomical barriers such as the
vier Science Ltd on behalf of The European Society of Cardiology

230 P. Ricard et al.
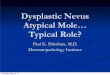
Figure 1 Typical counterclockwise atrial flutter. Left panel: mapping as depicted in theoriginal 1970 Paul Puech study4. Right panel: typical sawtooth atrial waveform patternwith at this moment 5:2 alternate Wenckebach AV conduction.
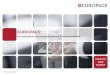
Figure 2 Transient entrainment mapping. Traces are those of a duodecapolar halocatheter, a catheter within the cavotricuspid isthmus and a decapolar coronary sinuscatheter. During a typical counterclockwise right atrial macro-re-entry at a cycle lengthof 240 ms, pacing is initiated within the cavotricuspid isthmus at a cycle length of 200 ms.Note that during pacing all electrograms are accelerated at the pacing rate without anydiscernible change in surface or intracardiac activation sequence or morphology. Thisconcealed form of entrainment is performed within the critical tachycardia isthmus as thereturn cycle length is identical to tachycardia cycle length. In this as in subsequent figures,H and the numbers are corresponding dipoles of the halo recording catheter.
Europace, Vol. 4, July 2002

Atypical atrial flutters 231
to review in this article some characteristics of bothtypical flutter but with unusual ECG patterns as well as‘true atypical’ types.
Typical atrial flutter with an unusualECG pattern
Reverse typical atrial flutter
In 10% of the cases, a reverse direction of rotation(clockwise re-entry) has been observed in atypical atrialflutter circuit[10,11]. This flutter exhibits the samere-entrant path and cavotricuspid isthmus dependenceas the typical flutter with counterclockwise activation.Reverse typical atrial flutter can be induced in the EPlaboratory in about 50% of the patients presenting onlyclinically counterclockwise flutter. Often (although notalways) the ECG pattern is different from that ofthe counterclockwise typical flutter showing a broader
positive deflection in the inferior leads and more impor-tantly a wide biphasic or negative deflection in V1 (Fig.5). An ECG pattern similar to the one observed duringthe counterclockwise typical flutter has been reported,but is less common. Because of its isthmus dependence,complete transection of the isthmus during radio-frequency ablation interrupts the arrhythmia andprevents its recurrence[10,12].
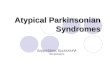
Figure 3 Pitfalls in the analysis of the surface ECG in typical atrial flutter. Left panel: surface ECG oftypical counterclockwise right atrial flutter. Right panel: transient entrainment in the isthmus at a pacing cyclelength of 220 ms revealed overt entrainment and complete reversal of right atrial activation. At pacing cessationa long local return cycle precedes reappearance of the previous recording of atrial activation with cycle lengthof 270 ms.
Other macro-re-entrant tachycardias of theright atrium
Some unusual macro-re-entrant tachycardias with amore complex mechanism but still dependent on thecavotricuspid isthmus have recently been described.
Lower loop re-entry tachycardia (LLR) was firstdescribed by Cheng et al.[13] LLR can alternate withtypical counterclockwise flutter. After passing throughthe cavotricuspid isthmus the activation goes up towardsthe inter-atrial septum, short circuits the crista terminalis
Europace, Vol. 4, July 2002

232 P. Ricard et al.
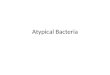
Figure 4 Bizarre ECG pattern of typical atrial flutter. Left panel: bizarre and certainlynon-localizable circuit on the surface ECG. Right panel: activation mapping shows counter-clockwise right atrial activation which proved to be isthmus dependent by entrainment mapping(not shown). The long flutter cycle length (300 ms) is due to the fact that previousradiofrequency pulses had been given in the isthmus yielding fractionation of the localelectrogram and prolongation of the isthmus conduction time.
Figure 5 Clockwise typical flutter. Left panel: surface ECG pattern relatively similar tothat of the regular (counterclockwise) typical flutter but for the presence of notches clearlyseen in the inferior leads, and the negativity of the F wave in V1. Right panel: transiententrainment proves the isthmus dependence.
Europace, Vol. 4, July 2002

Atypical atrial flutters 233
and descends along the lower part of the right lateralwall while simultaneously activating the rest of thelateral wall in an ascending direction. This results in ashorter cycle length because the size of the circuit issmaller. In the study of Yang et al.[14] the site of the earlybreakthrough was found in the low lateral right and highright atrium (RA) in 13 out of 24 and in 11 out of 24episodes, respectively. In the same study, it has also beenshown, in some cases, the presence of early break-throughs with multiple collision sites in 38% of the cases.For example some patients can have a breakthrough atboth high and low right atrium. The ECG pattern ismost of the time very close to that seen in the typicalflutter, showing negative atrial complexes in the inferiorleads. The presence of concealed entrainment at theisthmus, the termination of the tachycardia duringradiofrequency ablation applied to the isthmus and theabsence of recurrence when bidirectional block isachieved, demonstrate that this atrial flutter was isthmusdependent. Partially isthmus-dependent short circuits(PIDSC) flutter have been found in 14% of the patientsin these series. A counterclockwise atrial flutter can beobserved with premature activation of the coronarysinus ostium and impulse collision at the isthmus of the
counterclockwise wavefront as well as another clockwisefront emerging from the coronary sinus ostium area.This activation results in a short circuit around theEustachian ridge barrier. The same patient may there-fore display both typical counterclockwise flutter andpartial isthmus-dependent flutter. Radiofrequency abla-tion applied to the isthmus, stretching from the coronarysinus ostium to the orifice of the inferior vena cava hasbeen successful in preventing recurrence of PIDSCflutter. We also observed appearance of such PIDSCunmasked by ablation of the cavotriscupid isthmussuggesting an epicardial short circuit which was a by-stander during ongoing typical counterclockwise flutter,it became overt after isthmus ablation (Fig. 6). Howeverablation at cavotriscupid isthmus is still required to treatcounterclockwise typical flutter that is often associatedwith this arrhythmia.
Figure 6 Epicardial short circuit allowing flutter to persist after isthmus ablation. Clear double spikes (A B) areseen within the isthmus during ongoing atrial flutter suggesting the presence of isthmus block and of bystanderisthmus activation by daughter waves. The electrogram recorded within the proximal coronary sinus (CS 9–10) isexactly temporally located between the double spikes and ablation at that site was successful.
Atypical atrial flutters
As previously mentioned the term atypical is used forflutters that are independent of the cavotriscuspidisthmus and independent of the ECG pattern[9].
Europace, Vol. 4, July 2002

234 P. Ricard et al.
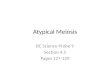
Figure 7 Left atriotomy as shown by a non-contact mapping system. Six consecutive snapshots of the leftatrium in the left anterior oblique projection are shown. The most anterior portion has been electronically erasedto allow visualization of the posterior wall. During sinus rhythm, the impulse depolarizes the left atrium firstfrom the Bachman bundle and proceeds anteriorly and inferiorly (from 1 to 3). The atriotomy prohibits furtherlateral wavefront progression and impulse is forced to turn around it to activate the rest of the left atrium (4to 6).
Lesion macro-re-entrant atrial tachycardia
In this kind of tachycardia the central obstacle is ascar. It might be the result of a previous atriotomy,a septal prosthetic patch, a suture line or a blocksecondary to radiofrequency ablation[15–17]. Othernatural obstacles such as the superior and the inferiorvena cava can be part of the circuit. Usually mappingshows an area of low voltage electrograms or ofalmost complete electrical silence. Double potentialscan be recorded along lines of block. The locationof the scars and associated anatomic barriers deter-mines the size and the properties of the re-entrantcircuits. Some of them are very complex especiallyafter placement of an intraatrial baffle (Senning,Mustard), after maze surgery or after Fontan pro-cedure with a dilated right atrium[16,18,19]. The aim of
Europace, Vol. 4, July 2002
mapping will then be to localize the entire circuit andits relations with surrounding inexcitable barriers. Forthis purpose, entrainment mapping is an essentialtool in order to allow identification of an isthmuswhere concealed entrainment can be demonstrated[20].Although often not really mandatory, the use ofcomputerized mapping, such as three-dimensionalelectro-anatomic mapping or non-contact mappinghas been of great help to localize ongoing circuitsaround scars even in the absence of inducible tachy-cardias (Fig. 7)[21–23].
Periatriotomy re-entrant tachycardia has beenextensively studied in the right atrium and is wellcharacterized. During tachycardia, activation rotatesaround the scar which is usually located in the anteriorright atrial free wall which is activated descendingly as intypical flutter. But clockwise activation is also possible.

Atypical atrial flutters 235
Figure 8 Lesion macro-re-entrant tachycardia. In this right anterior oblique projection a rightatriotomy has been electronically drawn to show impulse rotation around it. In each panel the first fourupper electrograms are recorded from the halo catheter and show a descending wavefront. The fifth lineshows recordings made in position A, B and C on the atriotomy line. The inferior vena cava is shown bythe oval. Double electrograms (a and b) are recorded at each site reflecting the activation wavefront onboth sides of the atriotomy. They are widely separated in its middle part (A) and progressively join (B)when approaching its lowest portion (C) where impulse returns.
Entrainment mapping is thus an essential tool to analysethe circuit. Participation of the anterior right atrial freewall can be demonstrated when concealed entrainment isobtained during pacing at this site. In contrast pacing atthe septum or flutter isthmus will result in a longerreturn cycle length than that of baseline suggesting thatthese sites are not actually part of the circuit (Fig. 2). Aline of double potentials is recorded along the scar in thelateral right atrium and extends towards the inferiorvena cava (Fig. 8). Isthmuses in the circuit can be foundbetween the SVC and the superior end of the scar, theIVC and the inferior end of the scar, the atriotomy scarand the tricuspid annulus or even within the scaritself [26–27]. Wide fractionated electrograms can berecorded from these isthmuses. Ablation is ofteneffective to cure this type of tachycardia. The narrowestisthmus can be chosen if not too close to the sino-atrialnode or the AV node. It is worth noting that typicalflutter is also often associated with RA atriotomy tachy-cardia. Therefore it seems logical that ablation be alsodelivered at the cavotricuspid isthmus during the same
procedure. There is no ECG pattern typical of thetachycardia and it may very well resemble that of themost common typical atrial flutter or even to an atrialtachycardia such as the classical sino-atrial re-entranttachycardia[28].
If most of the time the impulse rotates around theatriotomy, several other re-entry circuits can be found.In a series[29] of 21 patients suffering from 30 tachycar-dias after surgical closure of an atrial septal defect, thelocations of the tachycardia circuit were multiple. Themost frequent was peritricuspid in 11 patients followedby periatriotomy in 9 patients, more complex circuitswith double loop re-entry involving both the tricuspidannulus and the scar or the scar alone, in 10 patients. Itis interesting to note that during the same procedure theflutter loop may switch from one to another when afterlesion creates block in one path thereby forcing theimpulse to follow another (Fig. 9). Factors pre-disposing to periatriotomy re-entry are related to theatriotomy properties. A long vertical line, incomplete atthe inferior vena cava end and anteriorly placed is more
Europace, Vol. 4, July 2002

236 P. Ricard et al.
frequently seen in this arrhythmia. Factors predisposingto peritricuspid re-entry are a posterior atriotomy, atransverse or short atriotomy, a low location of theatriotomy reaching the inferior vena cava.
Non-incisional atypical right atrialflutter
Upper loop re-entry tachycardia (ULR) is a non-cavotricuspid isthmus dependent tachycardia involvingthe upper portion of the RA and characterized by aclockwise rotation of activation[14]. An isthmus wasidentified between the superior vena cava and thefossa ovalis where concealed entrainment was found.Another type of non-iatrogenic lesion macro-re-entrant tachycardia has recently been described[30]. Inthese cases the impulses rotate around areas of lowvoltages most frequently in the anteroinferolateral por-tion of the right atrial wall. We have encountered onlyone such case in which the low-voltage area seemed to
Europace, Vol. 4, July 2002
be the late consequence of a traumatic pericardialeffusion.
Figure 9 Flutter transformation during radiofrequency ablation. Left panel: during typical counter-clockwise flutter isthmus radiofrequency delivery, the ECG is suddenly modified and a new tachycardiaemerges best seen in the right panel. This is due to isthmus block which does not alow the baseline circuitto be active, but allows emergence of impulse rotation around the atriotomy.
Atypical left atrial flutter
Left atrial flutter has recently been described and onlylittle information is available on both the incidenceand mechanism of the arrhythmia[31,32]. On the sur-face ECG, the F waves are flat or positive in V1 andmost of the time positive in inferior leads but negativeF waves can also be seen. In our experience voltagesare higher in the presence of a cavotricuspid isthmusblock, which in the case of typical flutter resemblancemay further add to the confusion[33]. There are sev-eral ways to distinguish left from right atrial flutter.Coronary sinus activation is often inverse and pro-ceeds from the distal or mid part of the coronarysinus to the proximal part. Entrainment mappingshows that during right atrial stimulation the post-pacing interval is long and that the shortest returninterval is found in the coronary sinus. When left

Atypical atrial flutters 237
atrial stimulation is possible, through a patent fora-men ovale or after a transeptal puncture, the returncycle does not exceed the cycle length by 20 ms. Thetime of activation is a simple way to identify leftatrial flutter. During sequential conventional map-ping, with more than 8 RA sites, the RA activationtime accounts for <50% of the arrhythmia cyclelength (Fig. 10). It has also been suggested thatisolated variations of the right atrial cycle was pre-dictive of a left flutter (spontaneous variations of>100 ms in the RA with concomitant variationsof <20 ms in the LA). Three dimensional electro-anatomic mapping system (CARTO, BiosenseWebster) is a very useful tool here to locate thecircuit. In the study of Jaıs et al.[31] complete mapswere achieved in 17 patients. Most of the patients hadstructural heart disease, frequently mitral valvedisease. Only 4 patients had previous cardiac surgery.One to three loop circuits rotating around the mitralannulus or the pulmonary veins and a zone of blockor silent area may be encountered. Linear ablation ofthe most accessible part of the circuit was successfulin 73% of the patients.
Recently a form of macro-re-entry has also beendescribed for which one limb was the coronary sinuswall and the other the left atrial wall[34]. Thisrare form of tachycardia is certainly rendered possibleby the fact that the electrical activity of both struc-tures, though most of the time synchronous, can bedissociated[35].
Figure 10 Left atrial flutter. Left panel: atypical ECG with sawtooth in the inferior leads and positive F wave inV1 but low voltage. Right panel: coronary sinus and halo recordings show inverse (lateral to septal) left atrialactivation and dual wavefront in the right atrium covering less than 50% of the cycle.
Conclusion
Atypical atrial flutter represents a large variety ofsupraventricular tachycardias and refers to any non-cavotricuspid isthmus-dependent tachycardia that has apermanently undulating pattern in at least one lead. Theunderlying circuit(s) can be located in either the right orleft atrium. Some of these arrhythmias are well charac-terized and are amenable to catheter ablation with asuccess rate that is comparable with other types ofsupraventricular tachycardia. But for many others theuse of sophisticated mapping tools is of prime impor-tance and treatment of these tachycardias necessitatesa large electrophysiological experience and should be
Europace, Vol. 4, July 2002

238 P. Ricard et al.
reserved for specialized centres. Finally the number offlutters, their stability, their alternation with atrialfibrillation and factors such as the size of the atria areimportant determinants of long-term prevention whenusing ablative techniques.
References
[1] Lewis T, Feil HS, Strupd WD. Observations upon a curiousand not uncommon form of extreme acceleration of theauricles. Heart 1912; 4: 171.
[2] Schamroth L. In: The Disorders of Cardiac Rhythm.Victoria, Australia: Blackwell Scientific Publications 1980:49–57.
[3] Puech P. L’Activite electrique auriculaire normale etpathologique. Paris: Masson & Cie 1956.
[4] Puech P, Latour H, Grolleau R. Le flutter et ses limites. ArchMal Coeur 1970; 63: 116–44.
[5] Olgin JE, Kalman JM, Fitzpatrick AP, Lesh MD. Role ofright atrial structures as barriers to conduction during humantype I atrial flutter. Activation and entrainment mappingguided by intracardiac echocardiography. Circulation 1995;92: 1839–48.
[6] Friedman PA, Luria D, Fenton AM, Munger TM, JahangirA, Shen WK, Rea RF, Stanton MS, Hammill SC, Packer DL.Global and right atrial mapping of human atrial flutter:The presence of posteral-medial (sinus venosa region)double block and double potentials. Circulation 2000; 101:1568–77.
[7] Saoudi N, Poty H, Nair M, Abdelazziz, M, Anselme F,Letac B. In: Saoudi N, Schoels P, El Sheriff N, eds. Radio-frequency Catheter Ablation for the Common Type of AtrialFlutter. New York, New York: Futura Publishing Co 1998.
[8] Cosio FG, Lopez Gil M, Arribas F, et al. The mechan-isms of entrainment of human common flutter studiedwith multiple endocardial recordings. Circulation 1994; 89:2117–26.
[9] Saoudi N, Cosio F, Waldo A, Chen SA, Iesaka Y, LeshM, Saksena S, Salerno J, Schoels W. A classification ofatrial flutter and regular atrial tachycardia according toelectrophysiological mechanisms and anatomical bases.A Statement from a Joint Expert Group from theWorking Group of Arrhythmias of the European Societyof Cardiology and the North American Society ofPacing and Electrophysiology. Eur Heart J 2001 Jul; 22:1162–82.
[10] Saoudi N, Nair M, Abdelazziz A, Poty H, Daou A, AnselmeF, Letac B. Electrocardiographic patterns and results ofradiofrequecy catheter ablation of clockwise type I atrialflutter. J Cardiovasc Electrophysiol 1996; 7: 931–42.
[11] Cosio FG, Lopez Gil M, Arribas F, Gonzalez HD. Mech-anisms of induction of typical and reversed atrial flutter.J Cardiovasc Electrophys 1998; 9: 281–91.
[12] Tai C-T, Chen S-A, Chiang C-E, Lee S-H, Ueng K-C, WenZ-C, Chen Y-J, Yu W-C, Huang J-L, Chiou C-W, ChangM-S. Electrophysiologic characteristics and radiofrequencycatheter ablation in patients with clockwise atrial flutter.J Cardiovasc Electrophysiol 1996; 8: 24–34.
[13] Cheng J, Cabeen WR, Scheinman MM. Right atrial flutterdue to lower loop reentry. Mechanism and anatomicsubstrate. Circulation 1999; 99: 1700–5.
[14] Yang Y, Cheng J, Bochoeyer A, Hamdam H, Kowal RC,Page R, Lee RJ, Steiner PR, Saxon LA, Lesh MD, ModinGW, Scheinman MM. Atypical right atrial flutter patterns.Circulation 2001; 103: 3092–8.
[15] Triedman JK, Saul JP, Weindling SN, Walsh EP. Radio-frequency ablation of intra-atrial reentrant tachycardia aftersurgical palliation of congenital heart disease. Circulation1995; 91: 707–14.
Europace, Vol. 4, July 2002
[16] Cronin CS, Nitta T, Mitsuno M, Isobe F, Schuessler RB,Boineau JP, Cox JL. Characterization and surgicalablation of acute atrial flutter following the Mustardprocedure. A canine model. Circulation 1993; 88(Suppl2): 461–71.
[17] Baker BM, Cain ME, et al. Catheter ablation of clinicalintraatrial reentrant tachycardias resulting from previousatrial surgery: localizing and transecting the critical isthmus.J Am Coll Cardiol 1996; 28: 411–17.
[18] Van Hare GF, Lesh MD, Ross BA, Perry JC, Dorostkar.Mapping and radiofrequency ablation of intraatrial reentranttachycardia after the Senning or Mustard procedure fortransposition of the great arteries. Am J Cardiol 1996; 77:985–91.
[19] Deal BJ, Mavroudis C, Backer CL, Johnsrude CL, RocchiniAP. Impact of arrhythmia circuit cryoablation during Fontanconversion for refractory atrial tachycardia. Am J Cardiol1999; 83: 563–9.
[20] Saoudi N, Anselme F, Poty H, Criber A, Castellanos A.Entrainment of supraventricular tachycardias: A review.PACE 1998; 21(11): 2105–25.
[21] Schilling RJ, Kadish AH, Peters NS, Goldberger J, DaviesDW. Endocardial mapping of atrial fibrillation in the humanright atrium using a non contact catheter. Eur Heart J 2000;21: 550–64.
[22] Shpun S, Gepstein L, Hayam G, Ben-Haim SA. Guidance ofradiofrequency endocardial ablation with real-time three-dimensional magnetic navigation system. Circulation 1997;96: 2016–21.
[23] Shah D, Jaıs P, Haıssaguerre M, Chouairi S, Hocini M,Garrigue S, Clementy J. Three-dimensional mapping of thecommon atrial flutter circuit in the right atrium. Circulation1997; 96: 3904–12.
[24] Kalman JM, van Hare GF, Olgin J, Saxon LA, Stark SI, LeshMD. Ablation of ‘incisional’ reentrant atrial tachycardiacomplicating surgery for congenital heart disease: use ofentrainment to define a critical isthmus of conduction.Circulation 1996; 93: 502–12.
[25] Baker BM, Cain ME, et al. Catheter ablation of clinicalintraatrial reentrant tachycardias resulting from previousatrial surgery: localizing and transecting the critical isthmus.J Am Coll Cardiol 1996; 28: 411–17.
[26] Cosıo FG, Arribas F, Lopez Gil M, Gonzalez D. Atrialflutter mapping and ablation II. Radiofrequency ablation ofatrial flutter circuits. Pacing Clin Electrophysiol 1996; 19:965–75.
[27] Saoudi N, Redonnet M, Anselme F, Poty H, Cribier A.Catheter ablation of atrioatrial conduction as a cure for atrialarrhythmia after orthotopic heart transplantation. J Am CollCardiol 1998; 32: 1048–55.
[28] Kasal A, Anselme F, Cribier A, Saoudi N. Post operativetachycardia with a P wave identical to that of sinusrhythm. What is the tachycardia mechanism? J CardiovascElectrophysiol 2000; 11: 823–4.
[29] Shah DC, Jaıs P, Hocini M. Catheter ablation of atypical rightatrial flutter. In: Haissaguerre M, Zipes DP, eds. CatheterAblation of Arrhythmias, 2nd Edition. Armonk, NY: FuturaPublishing Co., Inc 2002.
[30] Kall JG, Rubenstein DS, Kopp DE, Burke MC, Verdino RJ,Lin AC, Johnson T, Cooke PA, Wang ZG, Fumo M, WilberD. Atypical atrial flutter originating in the right atrial freewall. Circulation 2000; 101: 270–9.
[31] Jaıs P, Shah DC, Haıssaguerre M, Hocini M, Peng JT,Takahashi A, Garrigue S, Le Metayer P, Clementy J.Mapping and ablation of left atrial flutters. Circulation 2000;101: 2928–34.
[32] Jaıs P, Shah DC, Macle L. Catheter ablation of atypical leftatrial flutter. In: Haïssaguerre M, Zipes JP, eds CatheterAblation of Arrhythmias, 2nd Edition. Armonk, NY: FuturaPublishing Co., Inc 2002.
[33] Saoudi N. Les flutters atypiques. Arch Mal Coeur Vaiss 2001;94: 59–70.

Atypical atrial flutters 239
[34] Olgin JE, Jayachandran JV, Engelstein E, Groh W,Zipes DP. Atrial macroreentry involving the coronary sinus.J Cardiovasc Electrophysiol 1998; 10: 1094–9.
[35] Kasai A, Anselme F, Saoudi N. Myocardial connectionsbetween left atrial myocardium and coronary sinus muscu-lature in man. J Cardiovasc Electrophysiol 2001.12; 9: 981–5.
Europace, Vol. 4, July 2002