Embed Size (px)
Citation preview

CLINICIAN’S CORNER
Atypical orthodontic extraction pattern managedby differential en-masse retraction againsta temporary skeletal anchorage devicein the treatment of bimaxillary protrusion
Kyu-Rhim Chung,a HyeRan Choo,b Jin-Hwa Lee,c and Seong-Hun Kimd
Suwon and Seoul, Korea, Philadelphia, Pa
aProfeMedicbDirecclinicaPhiladcPostgHee UdAssoHee UThe aproduReprinDenti130-7Subm0889-Copyrdoi:10
This report introduces an innovative treatment approach of selecting atypical and unconventional teeth for ortho-dontic extraction without compromising the quality of treatment outcomes by using temporary skeletal anchor-age devices in patients with bimaxillary protrusion. Both patients introduced in this report had solid Class Imolar relationships with bimaxillary anterior protrusion without facial or dental midline asymmetry. Their chiefconcerns were significant facial convexity, which conventionally requires the extraction of all 4 first premolars.However, 3 second premolars and 1 first premolar were removed in the first patient, and 2 second premolarsand 2 first premolars were removed in the second patient. All second premolars extracted had previously hadroot canal treatment and large prosthodontic restorations, which resulted in a compromised short lifespan ofthe teeth relative to the natural dentition. To manage these cases of asymmetric extraction space in a symmetricdental and skeletal environment, 2 mini-implants were placed in the posterior maxillary interradicular spaces, 1on each side. Despite the unusual asymmetric extraction of teeth, superimposition of the pretreatment and post-treatment cephalometric tracings shows excellent treatment outcomes of facial convexity reduction by asymetricmaximum retraction of the anterior teeth with no change in the molar relationships. (Am J Orthod DentofacialOrthop 2011;140:423-32)
Extraction of teeth has been an effective method ofcreating space in preparation for orthodontic den-tal alignment and for improving intermaxillary
relationships.1-3 The magnitude and vector of toothmovement as well as the biomechanical needs foranchorage preparation are primary factors to consider
ssor and chairman, Department of Orthodontics, Ajou University, School ofine, Suwon, Korea.tor of Craniofacial Orthodontics at The Children’s Hospital of Philadelphia;l associate, University of Pennsylvania Department of Orthodontics,elphia, Pa.raduate student, Department of Orthodontics, School of Dentistry, Kyungniversity, Seoul, Korea.ciate Professor, Department of Orthodontics, School of Dentistry, Kyungniversity, Seoul, Korea.uthors report no commercial, proprietary, or financial interest in thects or companies described in this article.t requests to: Seong-Hun Kim, Department of Orthodontics, School ofstry, Kyung Hee University #1 Hoegi-dong, Dongdaemun-gu, Seoul01, South Korea; e-mail, [email protected]; [email protected], revised and accepted, August 2009.5406/$36.00ight � 2011 by the American Association of Orthodontists..1016/j.ajodo.2009.08.036
in the selection of teeth for extraction in variousclinical situations.4-8
Traditionally, the premolars are most frequently se-lected for orthodontic extraction because they are lo-cated at a site that can strategically dictate the typesof anchorage preparation allowing the most efficientand effective treatment biomechanics to achieve thetreatment goals.5 Briefly, conventional anchorage valuesare determined by the number of teeth or the total rootsurface surrounded by the alveolar bone in 1 unit pullingagainst another unit. Its values relative to the extractionsite can affect the differential tooth movement duringactive orthodontic treatment, which determines thequality of the final treatment outcome. Therefore, thedecision for orthodontic extraction between the firstand second premolars can be critical in defining themost efficient biomechanics in conventional orthodon-tic treatment.6,7
For example, the maxillary and mandibular firstpremolars are commonly extracted to reduce facial con-vexity while maintaining Class I molar and canine rela-tionships in a Class I bimaxillary malocclusion. Unless
423

Fig 1. Schematic illustration of asymmetric extractiontreatment using biocreative therapy: A, initial stage oftreatment; B, after closure of extraction sites.
424 Chung et al
there are preexisting conditions, such as severe dentalmidline deviation or asymmetric molar relationships,asymmetric extraction of premolars is often discouragedto avoid complex orthodontic biomechanics that mightjeopardize the ideal treatment outcome in conventionalorthodontic treatment.9 Therefore, the conventional or-thodontic biomechanical concerns are often placed atthe top of the list, rather than the general health or ex-pected lifespan of the teeth when it comes to selection ofthe teeth to be extracted.
The advent of temporary skeletal anchorage devices(TSADs) such as mini-implants and mini-screws has,however, significantly simplified orthodontic biome-chanics by providing independent absolute anchoragerather than the conventional active-reactive type of an-chorage between dental units.10-13 Consequently, theconcept of absolute anchorage has reduced the needfor symmetric orthodontic extractions primarily basedon the need to ease orthodontic tooth movements(Fig 1). Hence, clinicians now have the freedom to deter-mine extraction patterns not primarily based on the needfor orthodontic biomechanics but on the general heathof the teeth without compromising the quality of thefinal treatment outcome or complicating the biome-chanics during active treatment. Therefore, adverse pre-existing dental conditions such as periapical lesions, rootresorptions, abnormal tooth shapes, or poor periodontalconditions are important factors to consider in theselection of teeth for orthodontic extractions.
In this report, we present 2 patients with Class I bi-maxillary anterior protrusion with no dental and facialasymmetry who were successfully and efficiently treatedby asymmetric tooth extractions and asymmetric maxi-mum retraction of the anterior teeth by using TSADsto obtain symmetric Class I molar and canine relation-ships with optimal overjet and overbite as the final treat-ment outcomes.
PATIENT 1
A 23-year-old woman’s chief complaint was severefacial convexity. Her clinical and radiographic
September 2011 � Vol 140 � Issue 3 American
examinations showed that she had a solid Class I molarrelationship on both sides in a mild Class II skeletalpattern with no dental or facial asymmetry (Figs 2and 3). Not surprisingly, the primary treatment goalwas maximum retraction of the anterior teeth toreduce lip protrusion, which traditionally requiresorthodontic extraction of the 4 first premolars tocreate enough space for retraction of the anteriorteeth.
However, when a periapical radiolucency of themaxillary left second premolar raised a suspicionof a periapical lesion of the tooth (Fig 3, A), anendodontist was consulted, who confirmed a recur-rent periapical lesion of the tooth. Hence, we imme-diately adjusted the final treatment plan to extractthe 3 second premolars that had endodontic treat-ment and 1 maxillary right first premolar to achievebetter long-term stability of her general dentalhealth.
An orthodontic mini-implant (C-implant, Cimplant,Seoul, Korea) was placed on each side of the maxillaryposterior interradicular space, and the patient wassent for extraction of the teeth mentioned above. Ap-proximately 4 weeks after placement of the mini-implants, fixed orthodontic appliances were placedon all teeth except the maxillary molars to retainthe pretreatment Class I molar relationship. Initially,to relieve maxillary anterior crowding, the maxillaryright canine and left first premolar were retractedwith a sliding jig and intra-arch rubber bands againstthe skeletal anchorage derived from the C-implants(Fig 4, A-C). After leveling and aligning the maxillaryanterior teeth, all 7 maxillary anterior teeth wereretracted en-masse against the mini-implants (Fig 4,D-F).
As expected, the maxillary dental midline started toshift to the right side during the early stages of treat-ment. This was immediately and efficiently correctedby using differential strengths of retraction on eachside (Fig 4, G-I). The maxillary molars were engagedwith fixed orthodontic appliances only during the finalstage of the treatment to fine-tune the maxillomandib-ular molar relationship (Fig 4, J-L). Approximately 18months into active treatment, the patient’s facial profilehad significantly improved, and the dental occlusion wasmaintained as a symmetric Class I molar and canine re-lationship on both sides with optimal overjet and over-bite (Figs 5-7). Superimposition of the pretreatmentand posttreatment cephalometric tracings alsoconfirmed the maximum retraction of the anteriorteeth in a manner of controlled tipping with nopositional change of the maxillary molars in anydirection (Fig 8, Table).
Journal of Orthodontics and Dentofacial Orthopedics
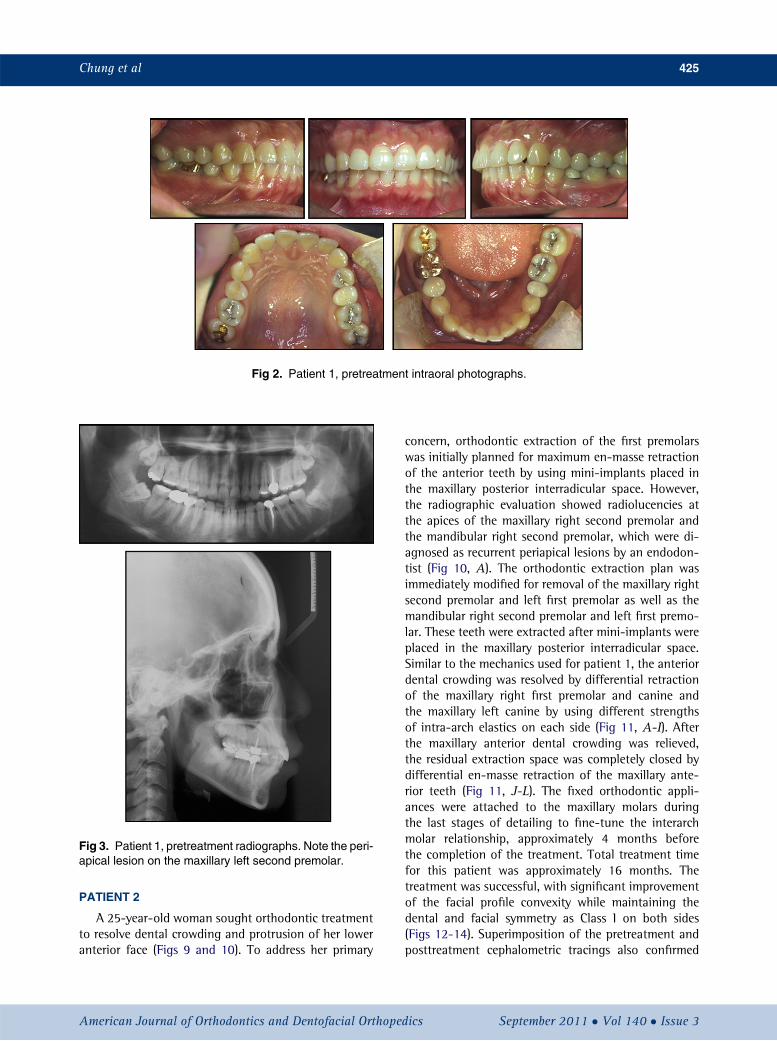
Fig 2. Patient 1, pretreatment intraoral photographs.
Fig 3. Patient 1, pretreatment radiographs. Note the peri-apical lesion on the maxillary left second premolar.
Chung et al 425
PATIENT 2
A 25-year-old woman sought orthodontic treatmentto resolve dental crowding and protrusion of her loweranterior face (Figs 9 and 10). To address her primary
American Journal of Orthodontics and Dentofacial Orthoped
concern, orthodontic extraction of the first premolarswas initially planned for maximum en-masse retractionof the anterior teeth by using mini-implants placed inthe maxillary posterior interradicular space. However,the radiographic evaluation showed radiolucencies atthe apices of the maxillary right second premolar andthe mandibular right second premolar, which were di-agnosed as recurrent periapical lesions by an endodon-tist (Fig 10, A). The orthodontic extraction plan wasimmediately modified for removal of the maxillary rightsecond premolar and left first premolar as well as themandibular right second premolar and left first premo-lar. These teeth were extracted after mini-implants wereplaced in the maxillary posterior interradicular space.Similar to the mechanics used for patient 1, the anteriordental crowding was resolved by differential retractionof the maxillary right first premolar and canine andthe maxillary left canine by using different strengthsof intra-arch elastics on each side (Fig 11, A-I). Afterthe maxillary anterior dental crowding was relieved,the residual extraction space was completely closed bydifferential en-masse retraction of the maxillary ante-rior teeth (Fig 11, J-L). The fixed orthodontic appli-ances were attached to the maxillary molars duringthe last stages of detailing to fine-tune the interarchmolar relationship, approximately 4 months beforethe completion of the treatment. Total treatment timefor this patient was approximately 16 months. Thetreatment was successful, with significant improvementof the facial profile convexity while maintaining thedental and facial symmetry as Class I on both sides(Figs 12-14). Superimposition of the pretreatment andposttreatment cephalometric tracings also confirmed
ics September 2011 � Vol 140 � Issue 3

Fig 4. Patient 1, progress intraoral photographs: A-C, the maxillary right canine and left first premolarwere retracted with a sliding jig and intra-arch rubber bands against the skeletal anchorage from theC-implants; D-F, after leveling and aligning, all 7 maxillary anterior teeth were retracted en-masseagainst the mini-implants; G-I, the maxillary dental midline started to shift to the right during the earlystages of treatment; J-L, the maxillary molars were engaged with fixed orthodontic appliances duringthe finishing stage. A 0.0173 0.025-in nickel-titanium reverse curve of Spee overlay archwire (Fores-tadentCo., Pforzheim,Germany) was applied to theC-implants hole for intrusion of the incisor segment.
Fig 5. Patient 1, posttreatment intraoral photographs.
426 Chung et al
September 2011 � Vol 140 � Issue 3 American Journal of Orthodontics and Dentofacial Orthopedics
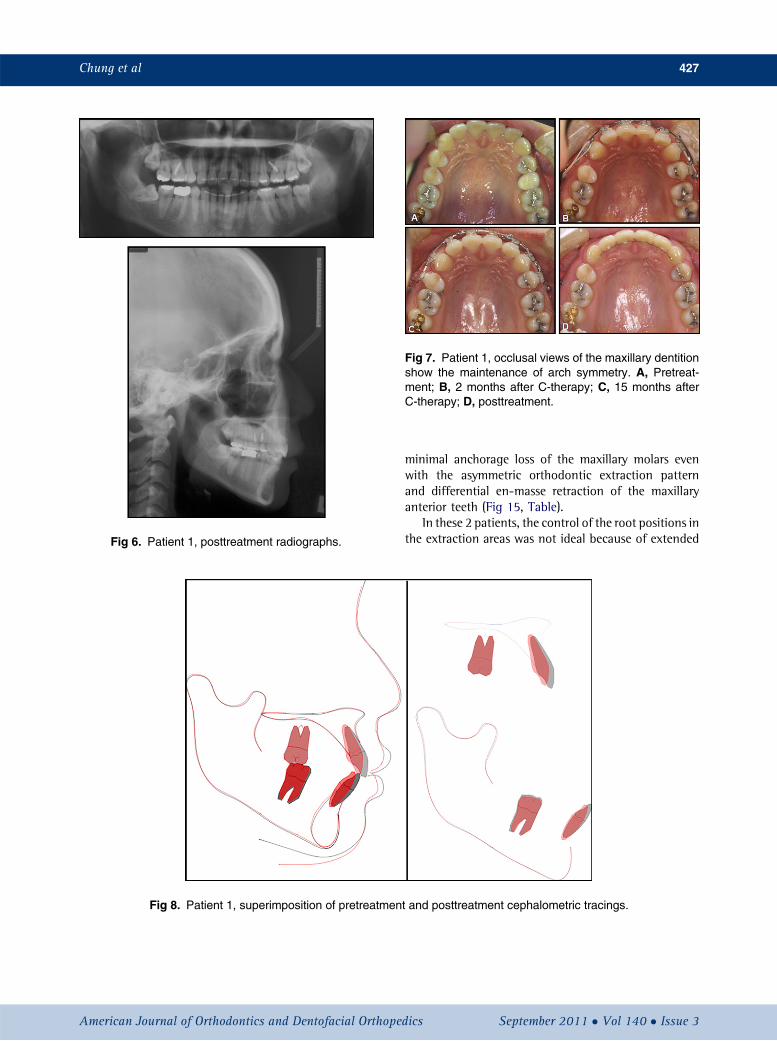
Fig 6. Patient 1, posttreatment radiographs.
Fig 7. Patient 1, occlusal views of the maxillary dentitionshow the maintenance of arch symmetry. A, Pretreat-ment; B, 2 months after C-therapy; C, 15 months afterC-therapy; D, posttreatment.
Fig 8. Patient 1, superimposition of pretreatmen
Chung et al 427
American Journal of Orthodontics and Dentofacial Orthoped
minimal anchorage loss of the maxillary molars evenwith the asymmetric orthodontic extraction patternand differential en-masse retraction of the maxillaryanterior teeth (Fig 15, Table).
In these 2 patients, the control of the root positions inthe extraction areas was not ideal because of extended
t and posttreatment cephalometric tracings.
ics September 2011 � Vol 140 � Issue 3
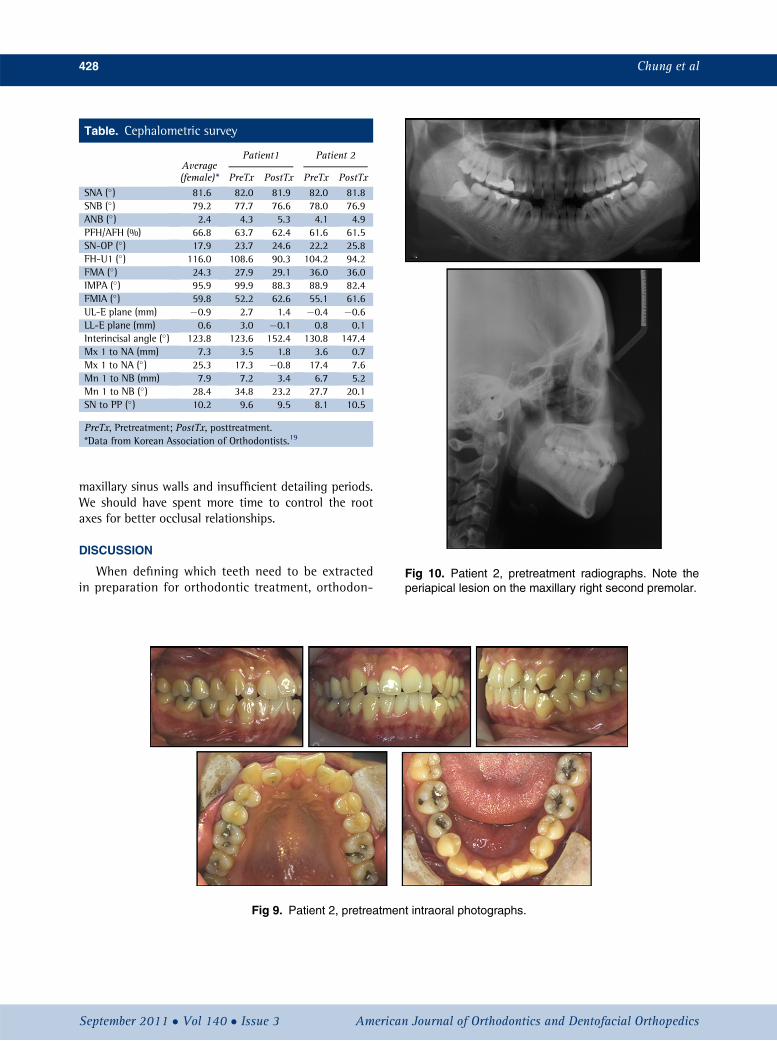
Table. Cephalometric survey
Average(female)*
Patient1 Patient 2
PreTx PostTx PreTx PostTxSNA (�) 81.6 82.0 81.9 82.0 81.8SNB (�) 79.2 77.7 76.6 78.0 76.9ANB (�) 2.4 4.3 5.3 4.1 4.9PFH/AFH (%) 66.8 63.7 62.4 61.6 61.5SN-OP (�) 17.9 23.7 24.6 22.2 25.8FH-U1 (�) 116.0 108.6 90.3 104.2 94.2FMA (�) 24.3 27.9 29.1 36.0 36.0IMPA (�) 95.9 99.9 88.3 88.9 82.4FMIA (�) 59.8 52.2 62.6 55.1 61.6UL-E plane (mm) �0.9 2.7 1.4 �0.4 �0.6LL-E plane (mm) 0.6 3.0 �0.1 0.8 0.1Interincisal angle (�) 123.8 123.6 152.4 130.8 147.4Mx 1 to NA (mm) 7.3 3.5 1.8 3.6 0.7Mx 1 to NA (�) 25.3 17.3 �0.8 17.4 7.6Mn 1 to NB (mm) 7.9 7.2 3.4 6.7 5.2Mn 1 to NB (�) 28.4 34.8 23.2 27.7 20.1SN to PP (�) 10.2 9.6 9.5 8.1 10.5
PreTx, Pretreatment; PostTx, posttreatment.*Data from Korean Association of Orthodontists.19
Fig 10. Patient 2, pretreatment radiographs. Note theperiapical lesion on the maxillary right second premolar.
428 Chung et al
maxillary sinus walls and insufficient detailing periods.We should have spent more time to control the rootaxes for better occlusal relationships.
DISCUSSION
When defining which teeth need to be extractedin preparation for orthodontic treatment, orthodon-
Fig 9. Patient 2, pretreatment intraoral photographs.
September 2011 � Vol 140 � Issue 3 American Journal of Orthodontics and Dentofacial Orthopedics

Fig 11. Patient 2, progress intraoral photographs: A-I, differential retraction of the maxillary right firstpremolar and canine and the maxillary left canine with different strengths of intra-arch elastics oneach side; J-L, finishing stages.
Fig 12. Patient 2, posttreatment intraoral photographs.
Chung et al 429
American Journal of Orthodontics and Dentofacial Orthopedics September 2011 � Vol 140 � Issue 3
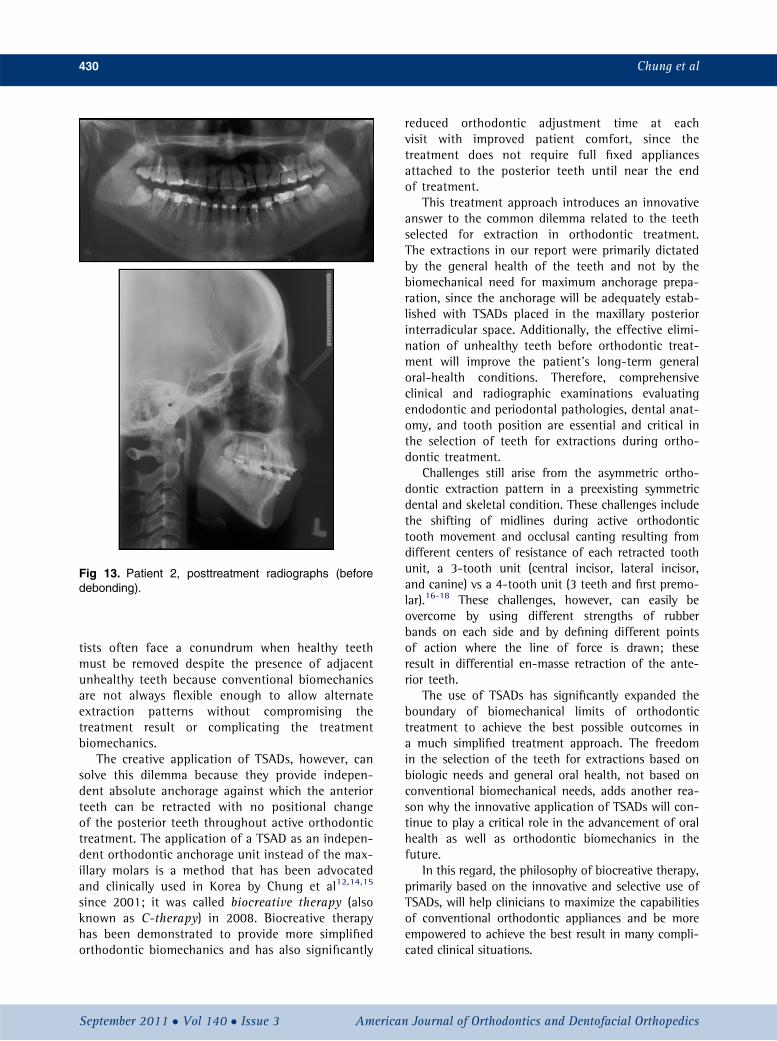
Fig 13. Patient 2, posttreatment radiographs (beforedebonding).
430 Chung et al
tists often face a conundrum when healthy teethmust be removed despite the presence of adjacentunhealthy teeth because conventional biomechanicsare not always flexible enough to allow alternateextraction patterns without compromising thetreatment result or complicating the treatmentbiomechanics.
The creative application of TSADs, however, cansolve this dilemma because they provide indepen-dent absolute anchorage against which the anteriorteeth can be retracted with no positional changeof the posterior teeth throughout active orthodontictreatment. The application of a TSAD as an indepen-dent orthodontic anchorage unit instead of the max-illary molars is a method that has been advocatedand clinically used in Korea by Chung et al12,14,15
since 2001; it was called biocreative therapy (alsoknown as C-therapy) in 2008. Biocreative therapyhas been demonstrated to provide more simplifiedorthodontic biomechanics and has also significantly
September 2011 � Vol 140 � Issue 3 American
reduced orthodontic adjustment time at eachvisit with improved patient comfort, since thetreatment does not require full fixed appliancesattached to the posterior teeth until near the endof treatment.
This treatment approach introduces an innovativeanswer to the common dilemma related to the teethselected for extraction in orthodontic treatment.The extractions in our report were primarily dictatedby the general health of the teeth and not by thebiomechanical need for maximum anchorage prepa-ration, since the anchorage will be adequately estab-lished with TSADs placed in the maxillary posteriorinterradicular space. Additionally, the effective elimi-nation of unhealthy teeth before orthodontic treat-ment will improve the patient’s long-term generaloral-health conditions. Therefore, comprehensiveclinical and radiographic examinations evaluatingendodontic and periodontal pathologies, dental anat-omy, and tooth position are essential and critical inthe selection of teeth for extractions during ortho-dontic treatment.
Challenges still arise from the asymmetric ortho-dontic extraction pattern in a preexisting symmetricdental and skeletal condition. These challenges includethe shifting of midlines during active orthodontictooth movement and occlusal canting resulting fromdifferent centers of resistance of each retracted toothunit, a 3-tooth unit (central incisor, lateral incisor,and canine) vs a 4-tooth unit (3 teeth and first premo-lar).16-18 These challenges, however, can easily beovercome by using different strengths of rubberbands on each side and by defining different pointsof action where the line of force is drawn; theseresult in differential en-masse retraction of the ante-rior teeth.
The use of TSADs has significantly expanded theboundary of biomechanical limits of orthodontictreatment to achieve the best possible outcomes ina much simplified treatment approach. The freedomin the selection of the teeth for extractions based onbiologic needs and general oral health, not based onconventional biomechanical needs, adds another rea-son why the innovative application of TSADs will con-tinue to play a critical role in the advancement of oralhealth as well as orthodontic biomechanics in thefuture.
In this regard, the philosophy of biocreative therapy,primarily based on the innovative and selective use ofTSADs, will help clinicians to maximize the capabilitiesof conventional orthodontic appliances and be moreempowered to achieve the best result in many compli-cated clinical situations.
Journal of Orthodontics and Dentofacial Orthopedics
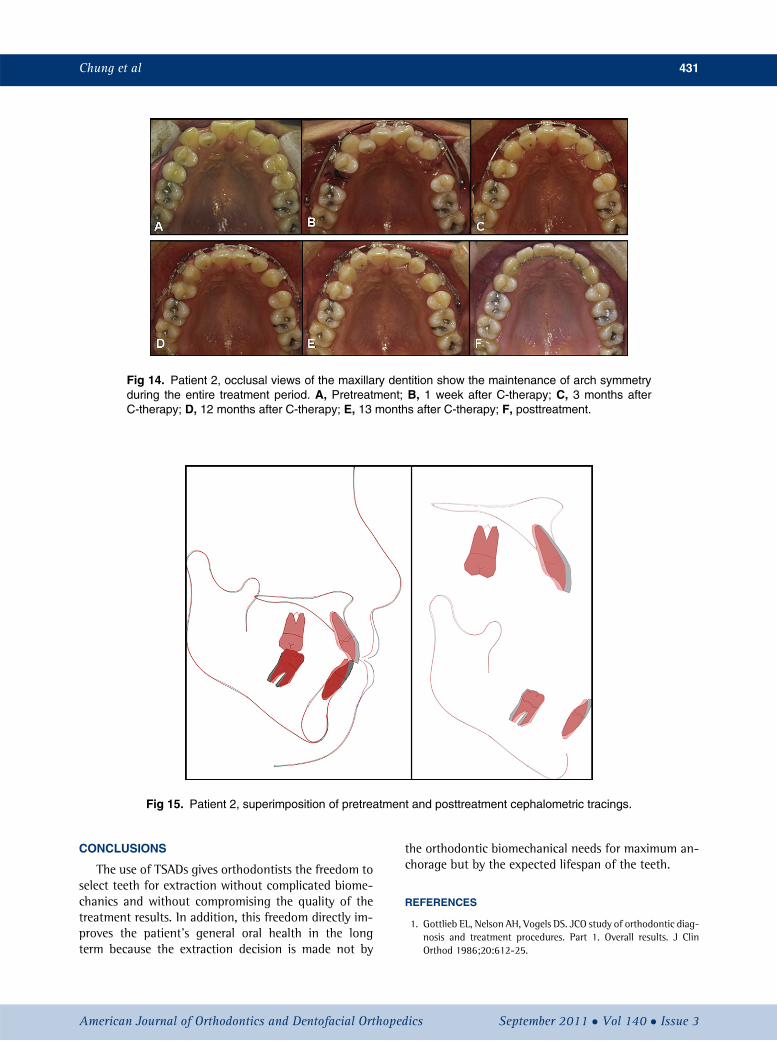
Fig 14. Patient 2, occlusal views of the maxillary dentition show the maintenance of arch symmetryduring the entire treatment period. A, Pretreatment; B, 1 week after C-therapy; C, 3 months afterC-therapy; D, 12 months after C-therapy; E, 13 months after C-therapy; F, posttreatment.
Fig 15. Patient 2, superimposition of pretreatment and posttreatment cephalometric tracings.
Chung et al 431
CONCLUSIONS
The use of TSADs gives orthodontists the freedom toselect teeth for extraction without complicated biome-chanics and without compromising the quality of thetreatment results. In addition, this freedom directly im-proves the patient’s general oral health in the longterm because the extraction decision is made not by
American Journal of Orthodontics and Dentofacial Orthoped
the orthodontic biomechanical needs for maximum an-chorage but by the expected lifespan of the teeth.
REFERENCES
1. Gottlieb EL, Nelson AH, Vogels DS. JCO study of orthodontic diag-nosis and treatment procedures. Part 1. Overall results. J ClinOrthod 1986;20:612-25.
ics September 2011 � Vol 140 � Issue 3

432 Chung et al
2. Gottlieb EL, Nelson AH, Vogels DS. JCO study of orthodontic diag-nosis and treatment procedures. Part 1. Results and trends. J ClinOrthod 1996;30:615-29.
3. Crossman IG, Reed RT. Long term results of premolar extractions inorthodontic treatment. Br J Orthod 1978;5:61-6.
4. Williams R, Hosila FJ. The effect of different extraction sites uponincisor retraction. Am J Orthod 1976;69:388-410.
5. Proffit WR, Fields HW, Sarver DM. Contemporary orthodontics. 4thed. St Louis: Mosby Elsevier; 2007. p. 283.
6. Kim HJ, Chun YS, Jung SH. Spatial changes of the upper dentitionfollowing en-masse space closure: a comparison between first andsecond premolar extraction. Korean J Orthod 2005;35:371-80.
7. Ong HB, Woods MG. An occlusal and cephalometric analysis ofmandibular first and second premolar extraction effects. AngleOrthod 2001;71:90-102.
8. Lim HJ, Ko KT, Hwang HS. Esthetic impact of premolar extractionand nonextraction treatments on Korean borderline patients. AmJ Orthod Dentofacial Orthop 2008;133:524-31.
9. Tayer BH. The asymmetric extraction decision. Angle Orthod 1992;62:291-7.
10. Kim MJ, Park SH, Kim HS, Mo SS, Sung SJ, Jang GW, et al. Effectsof orthodontic mini-implant position in the dragon helix applianceon tooth displacement and stress distribution: a three-dimensionalfinite element analysis. Korean J Orthod 2011;41:191-9.
11. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Development oforthodontic micro-implants for intraoral anchorage. J Clin Orthod2003;37:321-8.
September 2011 � Vol 140 � Issue 3 American
12. Chung KR, Kim YS, Linton JL, Lee YJ. The miniplate withthe tube for skeletal anchorage. J Clin Orthod 2002;36:407-12.
13. Chung KR, Jeong DM, Park HJ, Kim SH, Nelson G. Severebidentoalveolar protrusion treated with lingual Biocreativetherapy using palatal miniplate. Korean J Orthod 2010;40:276-87.
14. Chung KR, Kim SH, Kook YA, Son JH. Anterior torque control usingpartial osseointegrated mini-implants: biocreative therapy type Itechnique. World J Orthod 2008;9:95-104.
15. Chung KR, Kim SH, Kook YA, Choo H. Anterior torquecontrol using partial osseointegrated mini-implants: bio-creative therapy type II technique. World J Orthod 2008;9:105-13.
16. Sia A, Koga Y, Yoshida N. Determining the center of resistance ofmaxillary anterior teeth subjected to retraction forces in slidingmechanics. Angle Orthod 2007;77:999-1003.
17. Jeong GM, Sung SJ, Lee KJ, Chun YS, Mo SS. Finite-element inves-tigation of the center of resistance of the maxillary dentition.Korean J Orthod 2009;39:83-94.
18. Sung SJ, Kim IT, Kook YA, Chun YS, Kim SH, Mo SS.Finite-element analysis of the shift in center of resistanceof the maxillary dentition in relation to alveolar bone loss.Korean J Orthod 2009;39:278-88.
19. Korean Association of Orthodontists. Cephalometric norm ofKorean adults with normal occlusion. Korea: Ji-Sung PublishingCo; 1998. p. 589-95.
Journal of Orthodontics and Dentofacial Orthopedics