Embed Size (px)
Citation preview

Auditory Dys-Synchrony of Infancy:
Best Practices for Diagnosis, Monitoring and Guidance
Marilyn Neault, Ph.D., CCC-A
February 19, 2004
Thanks to the audiology and otolaryngology staff at Children’s Hospital Boston

What is auditory dys-synchrony?• Presence of cochlear hair cell activity
- cochlear microphonic in ABR- otoacoustic emissions (may disappear)
• Absence of auditory nerve response- no Wave I (no compound action potential)- no ABR waves
• Behavioral hearing discrepant from ABR- idiosyncratic, fluctuating responses- audiogram may range normal to profound

a.k.a. (also known as…)
• Auditory neuropathy• Primary auditory neuropathy (Shivashankar)• Auditory dys-synchrony• Auditory neuropathy “sensu stricto”
(Rapin and Gravel)• Peri-synaptic audiopathy• Persistent outer hair cell function(Not all the same – will break down into
categories as we learn more)• Your entry?

Why do children with auditory dys-synchrony drive audiologists crazy?
• Pure tone audiogram and ability to detect sounds in everyday life is often better than the absence of ABR would predict
• Word recognition ability is worse than the pure tone audiogram would predict
• Functional hearing ability fluctuates and may improve
• Expected benefit from hearing aids rarely realized

Possible sites of abnormality
• Inner hair cells• Synaptic junction between inner hair
cells and auditory neurons• Dendrites• Spiral ganglion cells• Axons
Heterogeneous disorder with different possible sites

Drawing from Takasaka (1993)

Other findings in auditory dys-synchrony
• Absent acoustic (stapedial) reflexes• OAE’s, if present, are not suppressed
by contralateral stimulation• Poor word recognition ability,
especially in noise• Poor temporal resolution• Poor low frequency discrimination• Limited or no benefit from hearing
aids

Concomitant conditions• Half of newborns have NICU histories• One-third of children (80% of adults) have other
neuropathies• Sural nerve biopsy may show abnormal
myelinization• Charcot-Marie-Tooth (hereditary sensorimotor
neuropathy)• Friedrich’s Ataxia• More than one child in family may have auditory
dys-synchrony with no concomitant conditions. Mutations in the otoferlin gene may be involved (Varga, J. Med Gen. 2003)

“Auditory Dys-Synchrony of Infancy” (“ADI”)
• Manifestation of cochlear activity in response to sounds without evidence of neural synchrony, in infancy
• Term implies neither etiology nor prognosis

Problems with ADI
#1. Some get better, some do not, no way (yet) to predict
outcome
#2. Newborns with auditory dys- synchrony pass OAE screen

Parent’s viewpoint• “What kind of a mother would take ‘I don’t know yet if your baby will be able to use his hearing to understand
speech’ for an answer?”• Why would they screen newborns with a method
that misses my baby’s problem?• Nebulous diagnosis with unknown cause and
unknown prognosis• Encourages shopping• Some audiologists not familiar with the condition• Conflicting opinions about use of hearing aids, FM
amplification

Incidence of auditory dys-synchrony?
From Sininger’s literature review:
3.1 / 1000 high risk infants
1/10 children with congenital hearing loss

Typical normal ABR tracings near threshold levels
L clicks 20dBHL
L 4000Hz 20dBHL
L 2000Hz 20dBHL
L 1000Hz 20dBHL
R clicks 20dBHL
R 4000Hz 20dBHL
R 2000Hz 20dBHL
R 1000Hz 20dBHL
15ms
20ms

Rarefaction clicks, 90 dBHL
Condensation clicks, 90 dBHL
9 month old former 25 week premie, passed newborn OAE screen but parents think she has a hearing loss

Rarefaction clicks, 90 dBHL
Condensation clicks, 90 dBHL

Responses to both polarities superimposed
Alternating polarity (CM not observable)
Rarefaction clicks, insert phone tubing pinchedto check for stimulus artifact
90 dBHL click stimuli

102 dBHL
90 dBHL
80 dBHL
70 dBHL
60 dBHL
(Note that the cochlear microphonic does not have a longer latency at lower intensities)

Audiogram by Visual Reinforcement Audiometrywith insert earphones, on the same day as the ABR.Tympanograms: normal, OAEs: absent bilaterally (though present at newborn screen).

Challenge to audiologists:
• We need to test in such a way that we’ll see the auditory dys-synchrony of infancy (ADI)
• We need to recognize the signs of ADI when they are staring us in the face (a prolonged CM in response to clicks is not just a stimulus artifact!)
• We need not to overdiagnose ADI– CM followed by typical ABR waves is not
ADI ---we all have cochlear microphonics!– Recognize other reasons why a child might
have OAEs but act deaf

From an audiologist on a learning curve:
• “Because the ABR response did not show polarity inversion when ipsilaterally and contralaterally recorded tracings were superimposed, there is no evidence of auditory neuropathy.” (huh?)

From another audiologist on a learning curve:(well, aren’t we all…)
• “A polarity-inverting cochlear microphonic response was seen on superimposed rarefaction and condensation click tracings, indicating absence of auditory neuropathy.” (huh?)

N3 Potential in a toddler who is deafMay have vestibular originNot a cochlear microphonic; NOT dys-synchronyDoes not reverse polarity Does have a latency-intensity function

KNOW
THY
STIMULUS
ARTIFACT

Stimulus artifact generated by insert earphone and recorded by ABR electrodes

Overlaid ABR stimulus artifacts from 1000Hz tone bursts, recorded from joined electrodes (no head) and from a profoundly deaf infant.
1000Hz, 100dBHL, singlepolarity stimulus

Why did we not see auditory dys-synchrony pre-1990’s?
• We did -- we just didn’t know it• Reports of patients with ABR results poorer
than behavioral audiogram appeared by 1979• By mid-1990’s, widespread availability of
otoacoustic emissions equipment AND use of insert earphones for ABR testing (insert earphones allow observation of cochlear microphonic response in patients with absent ABR)

How do children with auditory dys-synchrony present to the audiology clinic?• Referred on newborn ABR hearing screen• Passed newborn OAE hearing screen but parents
suspect child is deaf• A few may have passed ABR screen but then
developed auditory dys-synchrony, or had a false negative result on their screen
• Toddler with delayed receptive language development seen for VRA (WE NEED TO TEST ACOUSTIC REFLEXES FOR THESE CHILDREN)
• Older hearing aid user with fluctuating hearing levels and limited hearing aid benefit for degree of loss

Joint Committee on Infant HearingYear 2000 Position Statement
Acknowledges that cases of auditory dys-synchrony may be missed by accepted screening protocols
Diagnostic audiology protocol includes ways to detect auditory dys-synchrony
Problem: auditory dys-synchrony cases may not reach diagnostic evaluation if screened by OAE

What should a UNHS program do
about auditory dys-synchrony?• Analyze the consequences of doing automated
ABR rather than either ABR or OAE for initial screening? (auditory dys-synchrony passes OAE screen at birth)
• Educate audiologists to look for it• Educate early intervention providers:
– Nature of parent experience– Typical behaviors of the children – Communication and therapy methods– Approach toward hearing aids and cochlear
implant issues

Audiological / Educational Management of Infants with Auditory Dys-synchrony
• Benefit from visual language system • Encourage speechreading (lipreading)• Some (about 50%) benefit from hearing aids;
perhaps in one ear• Beware of hair cell damage from hearing aid
amplification, at least while OAEs are present• Consider sound field FM amplification• Language stimulation in quiet background;
acoustic highlighting• Monitor behavioral audiogram and OAEs;
“hearing” may improve or decline

Try a hearing aid or not?
• Beware of hair cell damage if OAEs are still present. Presence of OAEs suggests normal cochlear amplifier function.
• If OAEs have disappeared, try testing speech perception in each ear separately at elevated intensities. If the child understands words better at a higher than conversational intensity, try a hearing aid in that ear (or ears).

Audiological / Educational Management of Infants with Auditory Dys-synchrony, continued
• Let parents know that a cochlear implant may help, if hearing does not improve and hearing aids don’t help
• Help connect parents with other parents of children with the same condition

Auditory Neuropathy Information Homepage(with links including parent listserv)
http://auditoryneuropathy.com

Why might a CI help a child with auditory dys-synchrony?
• The child’s auditory nerve cells do not fire in tempo with incoming sounds.
• The cochlear implant may act as a drill sergeant for auditory nerve fibers, stimulating them to fire in synchrony and to keep tempo with incoming sounds.

“Problem solving is an important skill in any professional, yet it can be counter-productive if applied too early in a goal-setting endeavor, especially if done for the family rather than with them.”
D. Bailey

Typical candidacy to benefit from a cochlear implant
• Age 12 months and up with profound bilateral hearing loss
• OR age 25 months and up with severe or profound hearing loss and poor ability to recognize words through hearing aids
“profound” means average hearing thresholds >90dBHL at 500, 1000 and 2000Hz, unaided;
“severe” means 70-90dBHL, unaided; “poor” means no more than 30% correct
repetition of one-syllable word list without clues at 57dBHL, with terrific hearing aids

Cochlear implant candidacy for a child with auditory dys-synchrony
• Same as “typical” candidacy EXCEPT: – Allow enough time to know whether hearing
will improve or even recover– Pure tone hearing levels are not the
determining factor; a child may show a mild-moderate loss on the audiogram but may still benefit from a cochlear implant, if the child can not learn to recognize words without looking
– Assess the reason for the condition, to assess the risk that the auditory nerve is truly “patholo-gical” or may deteriorate in function over time

Is anything different about the CI candidacy workup for a child with auditory dys-synchrony?
• Should have MRI of the inner ears / auditory nerve (not just a CT scan). Consider MRI of the whole brain as well.
• Should be evaluated by a neurologist for other peripheral neuropathies
• Should monitor functional use of hearing in case ADI is resolving
• Should have ABR, OAE, acoustic reflex tests repeated just prior to surgery
• Consider Auditory Steady State Response (ASSR) to assist in ear determination
• As for any CI candidate, parents should accept that outcomes are variable and not always predictable.

What do you have to lose?(by implanting a child with auditory dys-synchrony)
• Ability to hear in the implanted ear when not using the speech processor
• Ability to determine the extent to which hearing may improve or resolve on its own
• Any ability the child might have had to localize the direction of a sound source

What do you have to gain?(by implanting a child with auditory dys-synchrony)
• Likelihood of auditory synchrony on one side
• Likelihood of stable hearing• Potential to learn to recognize
spoken words and sentences in quiet without looking
• Byproducts of better hearing: better speech and better language

Why might someone with auditory dys-synchrony have a particularly good CI outcome?• Language base in visual language system
prior to CI; may not have been severely language-deprived prior to implant.
• Has had and will have intense therapy and vigilant attention to communication.
• Most have had some auditory experience prior to implant.
• ?? May have cellular or neural elements in the cochlea in better supply than in some types of sensorineural hearing loss??

Why might someone with auditory dys-synchrony have a particularly limited CI outcome?
• Cochlear implant may not succeed in driving the auditory nerve fibers to fire in synchrony.
• If a degenerative nerve condition is present, such as in some mitochondrial disoders, performance with the CI could decline over time.
• Child may have other challenges which would have made it difficult for him to learn to understand speech and to speak, even if he had had normal hearing.

Before and after CI with auditory dys-synchronyBEFOREPure tone
audiogram mild to profound, fluctuating, moderately severe most common.
No nerve action potential (Wave I).
No ABR response.No acoustic reflexes.
AFTER
Sound field pure tone audiogram predictable at about 30dBHL, 250-6000Hz.
Nerve action potential seen on neural response telemetry.
EABR response +Acoustic reflex
stimulable using cochlear implant.

Electrically evoked Auditory Brainstem Responsestimulated through the cochlear implant in theoperating room
Vv

Electrically elicited acoustic reflex stimulated by presenting a signal through the cochlear implant

Models of auditory dys-synchrony
• Temporal bones of expired premies with outer hair cells but no inner hair cells (Amatuzzi et al., Arch. Oto. HNS 2001)
• Carboplatin causes selective loss of inner hair cells (but have acoustic reflexes)
• Mouse strain with no inner hair cells• Mouse strain with early degeneration of
cells that support the spiral ganglion cells

Research questions:
• Need better way to differentiate which cases will improve or resolve– Catalog and monitor our series
• Serial test measures • Infant auditory development scales
– Additional electrophysiological measures?• Some patients have ASSR and some have
cortical auditory evoked potentials, despite absence of ABR

Research questions
• Can people with auditory dys-synchrony localize sound?
• Does ABR or ASSR improve as pure tone audiogram and functional use of hearing improve?
• Is true resolution possible? (study “resolved” cases for acoustic reflexes, gap detection, discrimination in noise)
• Performance with cochlear implants• What happens to the unimplanted ear over
time?

Neault and Kenna (study in progress,2004) Subjects:
• 50 children with ADI whose hearing loss was evident during the first few months of life, seen at Children’s Hospital Boston
• Excluded: later onset auditory dys-synchrony

Unilateral vs. Bilateral
Of 50 children with ADI as of 2/04,40 (80%) with bilateral ADI (14 of these
now have cochlear implants)
8 (16%) with one ear ADI, one ear normal hearing
2 (4%) with one ear ADI, one ear typical sensorineural hearing loss (one now has a cochlear implant)

How They Came to Us (N = 50)• 30: Followup for newborn ABR screen referral• 6: Passed newborn OAE but parents
suspected deafness (dx’d at 6-27 months)• 3: Passed newborn ABR screen but
suspected deaf within first few months of life (two a real pass, ? one bogus)
• 6: Not screened; parents suspected hearing loss
• 5: Newborn screening data not confirmed

Characteristics of 50 Children with ADI
• Of 23 who had CT and/or MRI of inner ears so far, 5 showed abnormalities of cochlea or nerve (2 have normal cochlear turns, stenotic IAC, no cochlear nerve)
• 1 has optic nerve hypoplasia• 9 have abnomalities on MRI of
brain

What Happened to the 50 Children So Far • 14 with bilateral ADI now have cochlear
implant• 1 with unilateral ADI, unilateral typical
SNHL now has a cochlear implant • 6 with bilateral ADI resolved to normal
hearing findings• 29 “other” (some still very young, some
planning implantation, some developing usable but not normal hearing, all receiving habilitation, nearly all have at least somevisual language support)

Cochlear Implant Group (the first 11 of those implanted)
• Preoperative hearing levels: ranged from moderately severe to profound; poorer ear implanted
• Age at implantation:Median 22 monthsMean 30 monthsRange 14 to 62 months

Cochlear Implant Group (N = 11)
• Progress typical of children with cochlear implants
• Progress commensurate with their developmental abilities
• Those who are developmentally able to demonstrate open set speech recognition have done so

Cochlear Implant Group: What Happened to the Unimplanted Ear? • One improved from very profound to severe
by age 42 months• Two dropped from severe to profound range,
one at age 2 years and one at age 4 years• One uses hearing aid consistently in
unimplanted ear• One uses hearing aid sporadically in
unimplanted ear• None have word recognition ability beyond
pattern perception in the unimplanted ear

Caveat Implantor
• Does the child have a cochlear nerve?
( One child with unilateral and one child with bilateral ADI in our series showed absence of cochlear nerves )

Caveat Implantor
• Six of 50 children with ADI in our series resolved to NORMAL behavioral and/or electrophysiological measures of hearing
• All six showed signs that their hearing was improving (behaviorally or electrophysiologically) by 12 months of age, but you had to look for it

Resolved ADI
• 2 sisters with no other conditions• 1 boy with hyperbilirubinemia (to 44)• 1 boy whose mother had viral meningitis
during pregnancy• 1 boy whose mother had Lyme disease and had Bell’s Palsy 4 days before
delivery; baby negative for Lyme• 1 boy who was a 35 week premie, HIFI
vent• All had maintained robust OAEs

Resolving auditory dys-synchrony

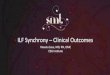
Sibling of girl with resolved ADIAge 3 weeks: no ABR waves, robust OAEsMother: “She acts deaf the way her sister did.”Age 3 months: Wave V present 80dB +, no reflexesAge 14 months: Normal behavioral audiogramAge 30 months: Normal audiogram, reflexes present AU, 92% PBK score in each ear

AC (AIR)
UNMASKED
MASKED
BC (BONE)
UNMASKED
MASKED
125 250 500 1000 2000 4000 8000750 1500 3000 6000
0
10
20
30
40
50
-10
60
70
80
90
100
110
120
FREQUENCY IN HERTZ (Hz)
HE
AR
ING
LE
VE
L (H
L) IN
DE
CIB
ELS
(dB
)
KEY
R L
SOUNDFIELD
S
SPEECH AUDIOMETRY
SDT
SRT
SPEECHDISCRIM.(WORDRECOG.)
R L
DPOAE: robust AU
Tympanograms: normal
Ipsilateral acoustic reflexes: normal AD, absent AS
92% inSF (ESPMonosyl.)
X X XX
20 20
Age 26 months
X

One month old boy with peak bilirubin 44.By five months, he had ABR waves down to 30dB left and 20dB right, only at slow stim.rate. By 14 months, ABR waves down to 20dBin each ear; morphology best at slow rate.

LEFT RIGHT
Clicks 20dBHL Clicks 20dBHL
4000Hz 20dBHL 4000Hz 20dBHL
2000Hz 20dBHL 2000Hz 20dBHL
1000Hz 20dBHL 1000Hz 20dBHL
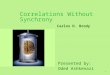
Resolved ADI. ABR of 17 month old boy who had no ABRwaves at birth. Still has some difficulty localizing sound.

Same 17 month old with resolving ADI; cochlear microphonic remains unusually large.
LEFT RIGHT
Clicks 90dBHL Clicks 90dBHL
Clicks 20dBHL Clicks 20dBHL

What about children whose ADI does not “resolve” but they do develop usable hearing?

25 week premie; still no ABR waves at 2 yrs. 8 months
Speaks in clear 4-word sentences. Uses MicroEar BTE FMin mainstreamed preschool; comprehends speech well.

Some typical things that partially hearing toddlers and preschoolers with auditory dys-synchrony do
• Respond to intonation• Talker-specific understanding• Localize sounds poorly• Develop articulation out of the usual order
for sensorineural hearing loss– Vowel distortions (poor low freq discrimination)– May have unvoiced plosives in their speech
and be able to imitate them
• May benefit inconsistently from hearing aids

How can a child with no ABR synchrony develop “hearing?”
Perhaps …
“…The brain ingeniously builds an accurate clock from an enormous number of sloppy ones….”
--Steven Strogatz (2003)SYNC: The Emerging Science of Spontaneous Order

(Strogatz, 2003)
“ ….Left to their own devices, this motley bunch of neural oscillators would fire off impulses at disparate rates, producing an electrical racket akin to the sound of an orchestra tuning up before a performance. To work together as an accurate clock, these hypothetical oscillators would need to cooperate, to sense one another’s electrical rhythms so as to stay in step.”

Conclusions Regarding Auditory Dys-Synchrony of Infancy (ADI)
• Infants with ADI are not always good implant candidates– 2/50 had no cochlear nerve– 6/50 resolved– A few will develop enough usable hearing that
CI surgery may not be necessary
– Those who prove to be good candidates benefit greatly from cochlear implantation, in a manner typical of other deaf children with the same cognitive abilities and pre-implant language base

Conclusions Regarding Auditory Dys-Synchrony of Infancy (ADI)
• Those who are going to resolve start developing ABR waves by 12 months
• BUT you have to look for it; may need to slow the stimulus repetition rate
• Repeat ABR and monitor functional hearing again just before early CI surgery for a child with auditory dys-synchrony

Additional Thoughts
• Children with “resolved” ADI missed out on a few months of good hearing and should not be cut off from early intervention
• Parents may have much invested in acceptance of hearing disorder
• Children may still have subtle auditory disorders and should be watched