Embed Size (px)
Citation preview

www.elsevier.com/locate/braindev
Brain & Development 32 (2010) 299–304
Original article
Auditory processing disorder in perisylvian syndrome
Mirela Boscariol a, Vera Lucia Garcia b, Catarina Abraao Guimaraes a,Maria Augusta Montenegro a, Simone Rocha Vasconcelos Hage c, Fernando Cendes a,
Marilisa Mantovani Guerreiro a,*
a Department of Neurology, University of Campinas (UNICAMP), Campinas, Brazilb Interaction Between University Service and Community Program, State University of Sao Paulo (UNESP), Botucatu, Brazil
c Department of Speech Therapy, University of Sao Paulo (USP), Bauru, Brazil
Received 3 December 2008; received in revised form 24 March 2009; accepted 1 April 2009
Abstract
We hypothesized that the processing of auditory information by the perisylvian polymicrogyric cortex may be different from thenormal cortex. To characterize the auditory processing in bilateral perisylvian syndrome, we examined ten patients with perisylvianpolymicrogyria (Group I) and seven control children (Group II). Group I was composed by four children with bilateral perisylvianpolymicrogyria and six children with bilateral posterior perisylvian polymicrogyria. The evaluation included neurological and neu-roimaging investigation, intellectual quotient and audiological assessment (audiometry and behavior auditory tests). The resultsrevealed a statistically significant difference between the groups in the behavioral auditory tests, such as, digits dichotic test, non-verbal dichotic test (specifically in right attention), and random gap detection/random gap detection expanded tests. Our datashowed abnormalities in the auditory processing of children with perisylvian polymicrogyria, suggesting that perisylvian polymicro-gyric cortex is functionally abnormal. We also found a correlation between the severity of our auditory findings and the extent of thecortical abnormality.� 2009 Elsevier B.V. All rights reserved.
Keywords: Auditory cortex; Auditory perception; Dichotic listening; Perisylvian syndrome; Polymicrogyria
1. Introduction
Perisylvian syndrome comprises a variety of clinicalmanifestations due to lesions on the perisylvian or oper-cular regions [1]. Congenital malformations such aspolymicrogyria may be implicated as etiological factors.Bilateral perisylvian polymicrogyria is a malformationof cortical development characterized by excessivelysmall gyri seen around the Sylvian fissure on magneticresonance imaging [2,3].
0387-7604/$ - see front matter � 2009 Elsevier B.V. All rights reserved.
doi:10.1016/j.braindev.2009.04.002
* Corresponding author. Address: Department of Neurology – FCM– UNICAMP, P.O. Box 6111, 13083-970 Campinas, SP, Brazil. Tel.:+55 19 3521 7372; fax: +55 (19) 3521 7483.
E-mail address: [email protected] (M.M. Guerreiro).
Clinical features consist of pseudobulbar signs suchas drooling, poor swallowing and palatal dysfunctionin neurological examination, as well as dysarthria, epi-lepsy, specific language impairment and reading disabil-ities [4–7].
The severity of the clinical manifestations correlateswith the extent of the lesion. Therefore, the term bilat-eral perisylvian polymicrogyria is applied when the cor-tical malformation spreads around the entire extent ofthe sylvian fissure, and bilateral posterior perisylvianpolymicrogyria is applied when polymicrogyria occursonly in the posterior part of the parietooccipital regions.The latter appears to be associated with a genetic predis-position and softer clinical features (such as speechdelay) when compared to the bilateral perisylvian poly-

300 M. Boscariol et al. / Brain & Development 32 (2010) 299–304
microgyria (which often presents with pseudobulbarpalsy and epilepsy) [4,7].
Auditory processing is defined as the mechanismand process of the auditory system that enables locali-zation and sound lateralization, auditory discrimina-tion, pattern recognition, temporal processing andauditory performance in competitive speech ordegraded acoustic signals [8]. Temporal auditory pro-cessing is the perception of the temporal characteristicsof a sound or of a sound change within a restrictedtime interval. It is considered a fundamental abilityrequired for the auditory perception of verbal and non-verbal sounds [9]. This ability is important to identifythe sequence of phonemes in the speech. Problems withthis processing can interfere with temporal aspects ofspeech, such as perception and recognition of pho-nemes [10]. Children with auditory processing disordersmay have difficulties listening in background noise, fol-lowing oral instructions and understanding temporalaspects of speech in the presence of normal peripheralhearing [11].
We hypothesized that the processing of the auditoryinformation by the polymicrogyric cortex is different fromthe normal cortex. Therefore, the objective of this studywas to characterize the findings of the evaluation of theauditory processing in individuals with perisylviansyndrome.
2. Subjects and methods
This work was carried out in the Clinical Hospital ofthe University of Campinas (Unicamp), Campinas, SP,Brazil after being approved by the Ethics Committeeof the same university (protocol 196/2003). Parentsagreed to their children participating in this study, hav-ing read and signed the informed consent form. Thestudy was conducted from March 2007 to July 2008.
Inclusion criteria were the presence of either bilateralperisylvian polymicrogyria or bilateral posterior perisyl-vian polymicrogyria on magnetic resonance imaging,performance intelligence quotient >80 and specific lan-guage impairment. Specific language impairment refersto inadequate oral language acquisition in the absenceof sensory or intellectual deficits, pervasive developmen-tal disorders or severe environmental deprivation. Itoccurs at least 12 months behind chronological ageand nonverbal cognitive skills are usually normal. Thesechildren may present with school difficulties [4,5].
The assessment included: neurological examination,neuroimaging investigation, audiological assessmentand intellectual quotient score. We evaluated 10 childrenwith bilateral and symmetrical perisylvian polymicrogy-ria (Group I) and compared them with seven normalchildren (Group II). Ages ranged from eight to 16 years(mean = 11.6 years in Group I and mean = 11.4 years inGroup II).
In the neurological examination, four children inGroup I had pseudobulbar signs. They had abnormalhistory of drooling, choking, and sucking difficulty dur-ing the first years of life. There were no neurologicalchanges in the other children.
To obtain the intellectual quotient we utilized theWechsler intelligence scale for children III (WISC-III)[12]. For this study we included patients with perfor-mance intelligence quotient >80. Since language delaywas required for inclusion in the study, our patients fre-quently presented verbal intelligence quotient scoresinferior to performance intelligence quotient scores.Low verbal scores jeopardized full scale intelligencequotient scores, therefore we decided to include the per-formance intelligence quotient score as it better repre-sents the cognitive ability of this type of patient.
Neuroimaging investigation was performed in a 2.0 Tscanner (Elscint Prestige) with posterior multiplanarreconstruction and curvilinear reformatting in 3D mag-netic resonance imaging. Neuroimaging evaluationallowed a subdivision of Group I: four children hadbilateral perisylvian polymicrogyria and six childrenhad bilateral posterior perisylvian polymicrogyria.
The participants underwent pure tone audiometry.For the peripheral audiological evaluation an acousticcabin, AC-30 audiometer (Interacoustics) was used. Inchildren with normal peripheral hearing (threshold<25 dB), behavior tests of auditory processing wereapplied.
Taking into account age and auditory maturation,the behavior auditory tests were: the adapted digits dich-otic test with binaural integration [13], the nonverbaldichotic test [14], and the random gap detection test orrandom gap detection test expanded [10], with stimulithrough a two channel audiometer connected to a Phil-lips CD player. These were all conducted in an acousticcabin.
The digits dichotic test consists of 20 stimuli presen-tations (40 per ear). The test is presented at 50 dB basedon the average of pure tone thresholds at frequencies of500, 1000 and 2000 Hz. The patient hears two numberssimultaneously in each ear and repeats all of them. Thedigits list consists of the digits 4, 5, 7, 8 and 9, whichform dissyllable words in Portuguese. This test, in thebinaural integration task, evaluates the ability to com-bine components of the acoustic signal with competitivesounds and turn them into verbal terms. After 20 pre-sentations, the phones are reversed to avoid interferenceof the phones calibration [13].
The nonverbal dichotic test consists of six differentnonverbal sounds, with three onomatopoeic soundsand three environmental sounds, combined in pairsand presented simultaneously in each ear in three stages.In the stage of free attention, the individual points onlyto a figure corresponding to one of the two sounds pre-sented. In the right and left attention, he points to the
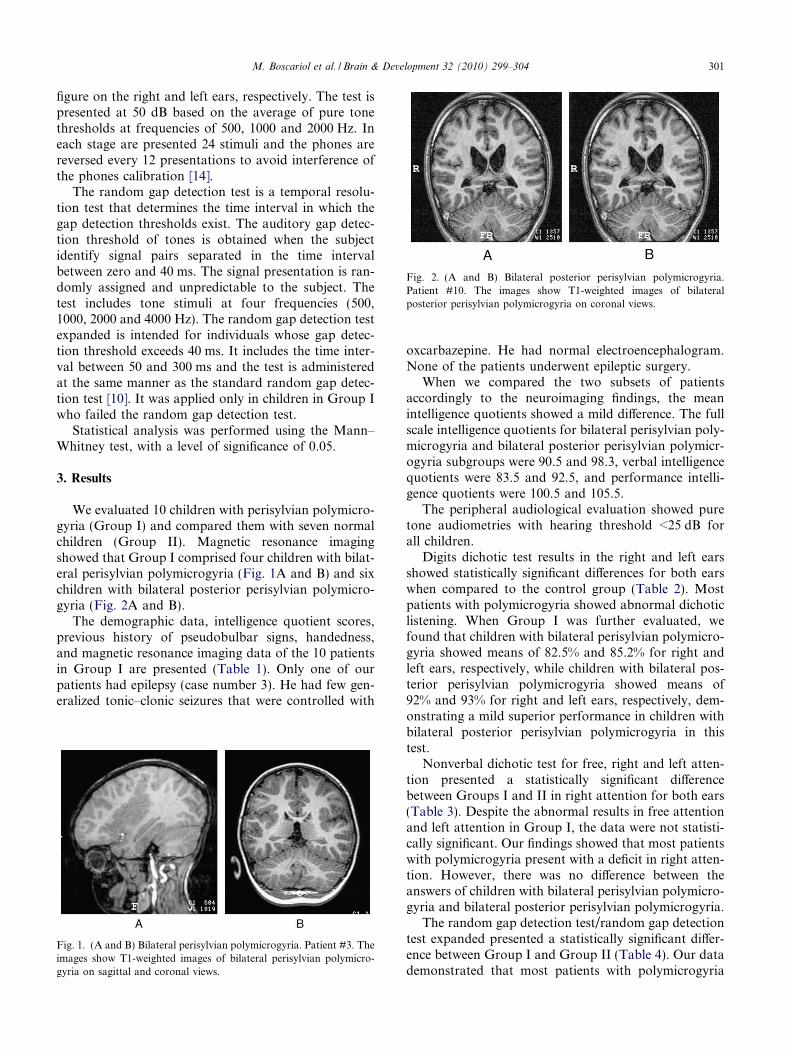
Fig. 2. (A and B) Bilateral posterior perisylvian polymicrogyria.Patient #10. The images show T1-weighted images of bilateralposterior perisylvian polymicrogyria on coronal views.
M. Boscariol et al. / Brain & Development 32 (2010) 299–304 301
figure on the right and left ears, respectively. The test ispresented at 50 dB based on the average of pure tonethresholds at frequencies of 500, 1000 and 2000 Hz. Ineach stage are presented 24 stimuli and the phones arereversed every 12 presentations to avoid interference ofthe phones calibration [14].
The random gap detection test is a temporal resolu-tion test that determines the time interval in which thegap detection thresholds exist. The auditory gap detec-tion threshold of tones is obtained when the subjectidentify signal pairs separated in the time intervalbetween zero and 40 ms. The signal presentation is ran-domly assigned and unpredictable to the subject. Thetest includes tone stimuli at four frequencies (500,1000, 2000 and 4000 Hz). The random gap detection testexpanded is intended for individuals whose gap detec-tion threshold exceeds 40 ms. It includes the time inter-val between 50 and 300 ms and the test is administeredat the same manner as the standard random gap detec-tion test [10]. It was applied only in children in Group Iwho failed the random gap detection test.
Statistical analysis was performed using the Mann–Whitney test, with a level of significance of 0.05.
3. Results
We evaluated 10 children with perisylvian polymicro-gyria (Group I) and compared them with seven normalchildren (Group II). Magnetic resonance imagingshowed that Group I comprised four children with bilat-eral perisylvian polymicrogyria (Fig. 1A and B) and sixchildren with bilateral posterior perisylvian polymicro-gyria (Fig. 2A and B).
The demographic data, intelligence quotient scores,previous history of pseudobulbar signs, handedness,and magnetic resonance imaging data of the 10 patientsin Group I are presented (Table 1). Only one of ourpatients had epilepsy (case number 3). He had few gen-eralized tonic–clonic seizures that were controlled with
Fig. 1. (A and B) Bilateral perisylvian polymicrogyria. Patient #3. Theimages show T1-weighted images of bilateral perisylvian polymicro-gyria on sagittal and coronal views.
oxcarbazepine. He had normal electroencephalogram.None of the patients underwent epileptic surgery.
When we compared the two subsets of patientsaccordingly to the neuroimaging findings, the meanintelligence quotients showed a mild difference. The fullscale intelligence quotients for bilateral perisylvian poly-microgyria and bilateral posterior perisylvian polymicr-ogyria subgroups were 90.5 and 98.3, verbal intelligencequotients were 83.5 and 92.5, and performance intelli-gence quotients were 100.5 and 105.5.
The peripheral audiological evaluation showed puretone audiometries with hearing threshold <25 dB forall children.
Digits dichotic test results in the right and left earsshowed statistically significant differences for both earswhen compared to the control group (Table 2). Mostpatients with polymicrogyria showed abnormal dichoticlistening. When Group I was further evaluated, wefound that children with bilateral perisylvian polymicro-gyria showed means of 82.5% and 85.2% for right andleft ears, respectively, while children with bilateral pos-terior perisylvian polymicrogyria showed means of92% and 93% for right and left ears, respectively, dem-onstrating a mild superior performance in children withbilateral posterior perisylvian polymicrogyria in thistest.
Nonverbal dichotic test for free, right and left atten-tion presented a statistically significant differencebetween Groups I and II in right attention for both ears(Table 3). Despite the abnormal results in free attentionand left attention in Group I, the data were not statisti-cally significant. Our findings showed that most patientswith polymicrogyria present with a deficit in right atten-tion. However, there was no difference between theanswers of children with bilateral perisylvian polymicro-gyria and bilateral posterior perisylvian polymicrogyria.
The random gap detection test/random gap detectiontest expanded presented a statistically significant differ-ence between Group I and Group II (Table 4). Our datademonstrated that most patients with polymicrogyria
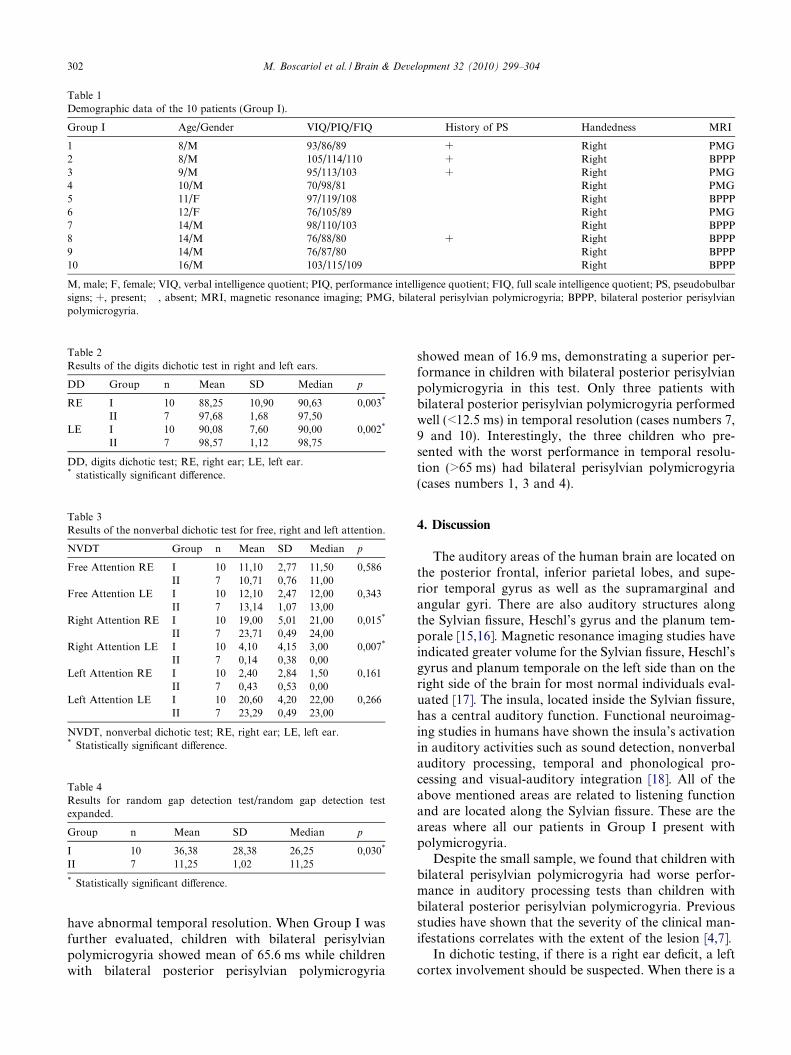
Table 1Demographic data of the 10 patients (Group I).
Group I Age/Gender VIQ/PIQ/FIQ History of PS Handedness MRI
1 8/M 93/86/89 + Right PMG2 8/M 105/114/110 + Right BPPP3 9/M 95/113/103 + Right PMG4 10/M 70/98/81 � Right PMG5 11/F 97/119/108 � Right BPPP6 12/F 76/105/89 � Right PMG7 14/M 98/110/103 � Right BPPP8 14/M 76/88/80 + Right BPPP9 14/M 76/87/80 � Right BPPP10 16/M 103/115/109 � Right BPPP
M, male; F, female; VIQ, verbal intelligence quotient; PIQ, performance intelligence quotient; FIQ, full scale intelligence quotient; PS, pseudobulbarsigns; +, present; �, absent; MRI, magnetic resonance imaging; PMG, bilateral perisylvian polymicrogyria; BPPP, bilateral posterior perisylvianpolymicrogyria.
Table 2Results of the digits dichotic test in right and left ears.
DD Group n Mean SD Median p
RE I 10 88,25 10,90 90,63 0,003*
II 7 97,68 1,68 97,50LE I 10 90,08 7,60 90,00 0,002*
II 7 98,57 1,12 98,75
DD, digits dichotic test; RE, right ear; LE, left ear.* statistically significant difference.
Table 3Results of the nonverbal dichotic test for free, right and left attention.
NVDT Group n Mean SD Median p
Free Attention RE I 10 11,10 2,77 11,50 0,586II 7 10,71 0,76 11,00
Free Attention LE I 10 12,10 2,47 12,00 0,343II 7 13,14 1,07 13,00
Right Attention RE I 10 19,00 5,01 21,00 0,015*
II 7 23,71 0,49 24,00Right Attention LE I 10 4,10 4,15 3,00 0,007*
II 7 0,14 0,38 0,00Left Attention RE I 10 2,40 2,84 1,50 0,161
II 7 0,43 0,53 0,00Left Attention LE I 10 20,60 4,20 22,00 0,266
II 7 23,29 0,49 23,00
NVDT, nonverbal dichotic test; RE, right ear; LE, left ear.* Statistically significant difference.
Table 4Results for random gap detection test/random gap detection testexpanded.
Group n Mean SD Median p
I 10 36,38 28,38 26,25 0,030*
II 7 11,25 1,02 11,25
* Statistically significant difference.
302 M. Boscariol et al. / Brain & Development 32 (2010) 299–304
have abnormal temporal resolution. When Group I wasfurther evaluated, children with bilateral perisylvianpolymicrogyria showed mean of 65.6 ms while childrenwith bilateral posterior perisylvian polymicrogyria
showed mean of 16.9 ms, demonstrating a superior per-formance in children with bilateral posterior perisylvianpolymicrogyria in this test. Only three patients withbilateral posterior perisylvian polymicrogyria performedwell (<12.5 ms) in temporal resolution (cases numbers 7,9 and 10). Interestingly, the three children who pre-sented with the worst performance in temporal resolu-tion (>65 ms) had bilateral perisylvian polymicrogyria(cases numbers 1, 3 and 4).
4. Discussion
The auditory areas of the human brain are located onthe posterior frontal, inferior parietal lobes, and supe-rior temporal gyrus as well as the supramarginal andangular gyri. There are also auditory structures alongthe Sylvian fissure, Heschl’s gyrus and the planum tem-porale [15,16]. Magnetic resonance imaging studies haveindicated greater volume for the Sylvian fissure, Heschl’sgyrus and planum temporale on the left side than on theright side of the brain for most normal individuals eval-uated [17]. The insula, located inside the Sylvian fissure,has a central auditory function. Functional neuroimag-ing studies in humans have shown the insula’s activationin auditory activities such as sound detection, nonverbalauditory processing, temporal and phonological pro-cessing and visual-auditory integration [18]. All of theabove mentioned areas are related to listening functionand are located along the Sylvian fissure. These are theareas where all our patients in Group I present withpolymicrogyria.
Despite the small sample, we found that children withbilateral perisylvian polymicrogyria had worse perfor-mance in auditory processing tests than children withbilateral posterior perisylvian polymicrogyria. Previousstudies have shown that the severity of the clinical man-ifestations correlates with the extent of the lesion [4,7].
In dichotic testing, if there is a right ear deficit, a leftcortex involvement should be suspected. When there is a

M. Boscariol et al. / Brain & Development 32 (2010) 299–304 303
left ear deficit on dichotic tests the corpus callosum maybe involved, but this finding could also mean a righthemisphere involvement [19]. These findings are in keep-ing with our study because our patients, all of whomhave bilateral polymicrogyria, demonstrated both rightand left ear deficits, suggesting bilateral cortex dysfunc-tion. In digits dichotic test, patients have to recognizetwo stimuli presented to each ear at the same time andrepeat both, requiring the ability to group componentsof the acoustic signal against background noise [13].The Group I children had a worse performance thanthe Group II children. The nonverbal dichotic testabnormality may indicate poor performance in process-ing of nonlinguistic sounds such as tonal, melodic stim-uli and speech intonation [14]. The results of thenonverbal dichotic test indicated a deficit in the atten-tion mechanisms for right attention. However, therewas no statistically significant difference for free atten-tion or left attention. The failure of unilateral selectiveattention was previously found in dyslexic children,when the authors found a deficit in right attention fornonverbal sounds [20,21]. Our data suggest that the non-dominant cerebral hemisphere is probably more impor-tant in nonverbal tasks.
The auditory ability of temporal resolution is one ofthe aspects of temporal processing [8]. Temporal resolu-tion can be defined as the individual’s capacity to per-ceive the minimum detectable gap in a tone or soundburst. The random gap detection test and random gapdetection test expanded results in Group I led to the cor-relation between auditory processing disorders and spe-cific language impairment. Disorders in temporalresolution are an indication that the individual is unableto perceive fast changes in frequencies of ongoingspeech. Therefore, they may miss subtle details of thespeech and this difficulty may jeopardize the schoolperformance.
A deficit in temporal processing was confirmed in ourpatients in Group I. This can cause alterations in phono-logical processing, auditory discrimination, receptivelanguage and reading [10]. In our study, only threepatients performed well in temporal resolution. Thesethree individuals presented with bilateral posterior peri-sylvian polymicrogyria while patients with the worstperformance had bilateral perisylvian polymicrogyria.
Furthermore, we also found a possible correlationbetween intelligence quotients and the extent of the cor-tical abnormality, as our results showed worse scores inpatients with bilateral perisylvian polymicrogyria andbetter scores in patients with bilateral posterior perisyl-vian polymicrogyria. These features may result from themore severely disturbed auditory processing in bilateralperisylvian polymicrogyria group, or otherwise may bedue to the involvement of the areas that are responsiblefor higher language function in bilateral perisylvianpolymicrogyria. Again, our data support the statement
that the extent of cortical maldevelopment correlateswith clinical findings [4,7].
In conclusion, our data showed auditory processingabnormalities in patients with polymicrogyria. It hasbeen questioned whether dysplastic neural tissue har-bors function. Functionality has been shown in polymi-crogyric areas [22]. Our study adds more information tothis matter, suggesting that perisylvian polymicrogyriccortex is functionally abnormal.
Acknowledgements
Mirela Boscariol received a scholarship from CNPq(Grant Number # 132461/2007-2) and FAPESP (GrantNumber # 07/00806-4). Catarina A. Guimaraes receiveda scholarship from FAPESP (Grant Number # 06/56257-6).
References
[1] Kuzniecky R, Andermann F, Guerrini R. Congenital bilateralperisylvian syndrome: study of 31 patients. Lancet1993;341:608–12.
[2] Guerreiro MM, Andermann E, Guerrini R, Dobyns WB,Kuzniecky R, Silver K, et al. Familial perisylvian polymicrogyria:a new familial syndrome of cortical maldevelopment. Ann Neurol2000;48:39–48.
[3] Barkovich AJ, Kuzniecky RI, Jackson GD, Guerrini R, DobynsWB. A developmental and genetic classification for malforma-tions of cortical development. Neurology 2005;65:1873–87.
[4] Guerreiro MM, Hage SR, Guimaraes CA, Abramides DV,Fernandes W, Pacheco PS, et al. Developmental language disorderassociated with polymicrogyria. Neurology 2002;59:245–50.
[5] Hage SR, Cendes F, Montenegro MA, Abramides DV, Gui-maraes CA, Guerreiro MM. Specific language impairment:linguistic and neurobiological aspects. Arq Neuropsiquiatr2006;64(2-A):173–80.
[6] Kuzniecky R, Andermann F. CBPS study group – the congenitalbilateral perisylvian syndrome: imaging findings in a multicenterstudy. AJNR 1994;15:139–44.
[7] Brandao-Almeida IL, Hage SRV, Oliveira EPM, Guimaraes CA,Teixeira KCS, Abramides DVM, et al. Congenital bilateralperisylvian syndrome: familial occurrence, clinical and psycholin-guistic aspects correlated with MRI. Neuropediatrics2008;39(3):139–45.
[8] American Speech-Language-Hearing Association – ASHA. Cen-tral Auditory processing: current status of research and implica-tions for clinical practice. Rockville, ASHA; 2005.
[9] Musiek FE, Shinn JB, Jirsa R, Bamiou DE, Baran JA, Zaidan E.GIN (gaps in noise) test performance in subjects with confirmedcentral auditory nervous system involvement. Ear Hear2005;26:608–18.
[10] Keith RW. Random Gap Detection Test. Saint Louis, Auditec;2000.
[11] Jerger J, Musiek F. Report of the consensus conference on thediagnosis of the auditory processing disorders in school-agedchildren. J Am Acad Audiol 2000;11:372–83.
[12] Wechsler D. Escala de inteligencia para crianc�as. 3a ed. SaoPaulo: Casa do Psicologo; 2002.
[13] Santos MFC, Pereira LD. Escuta com dıgitos. In: Pereira LD,Schochat E, editors. Processamento auditivo central: manual deavaliac�ao. Sao Paulo: Lovise; 1997. p. 147–9.

304 M. Boscariol et al. / Brain & Development 32 (2010) 299–304
[14] Ortiz KZ, Pereira LD. Nao-verbal de escuta direcionada. In:Pereira LD, Schochat E, editors. Processamento auditivo central:manual de avaliac�ao. Sao Paulo: Lovise; 1997. p. 151–5.
[15] Celesia GG, Puletti F. Auditory cortical areas of man. Neurology1969;19(3):211–20.
[16] Galaburda N, Sanides F. Cytoarchitetonic organization of thehuman auditory cortex. J Comp Neurol 1980;190:597–610.
[17] Musiek FE, Reeves A. Asymmetries of the auditory areas of thecerebrum. J Am Acad Audiol 1990;1:240–5.
[18] Bamiou DE, Musiek FE, Luxon LM. The insula (Island of Reil)and its role in auditory processing. Literature review. Brain ResRev 2003;42(2):143–54.
[19] Musiek FE, Baran JA, Pinheiro ML. Neuroaudiology: casestudies. San Diego: Singular; 1994.
[20] Smith K, Griffths P. Defective lateralized attention for nonverbalsounds in developmental dyslexia. Neuropsychology1987;25(1B):259–68.
[21] Sauer L, Pereira LD, Ciasca SM, Pestun M, Guerreiro MM.Dichotic listening and SPECT in dyslexic children. Arq Neuro-psiquiatr 2006;64(1):10–1.
[22] Araujo D, de Araujo DB, Pontes-Neto OM, Escorsi-Rosset S,Simao GN, Wichert-Ana L, et al. Language and motor FMRIactivation in polymicrogyric cortex. Epilepsia 2006;47(3):589–92.