Embed Size (px)
Citation preview
AUGUST 2012 | PODIATRY MANAGEMENT | 91www.podiatrym.com
This article is written exclusivelyfor Podiatry Management by theAmerican College of Foot and AnkleSurgeons (ACFAS). Founded in 1942,ACFAS is a professional society ofmore than 6,300 foot and ankle sur-geons. The College promotes the artand science of foot, ankle and relatedlower extremity surgery, addresses theconcerns of foot and ankle surgeons,as well as advances and improves thestandards of education and surgicalskill to ensure the highest level of pa-tient care. For more information onACFAS, visit acfas.org or circle #152on the reader service card.
AbstractWhile the use of autologous
platelet preparations for the treatmentof musculoskeletal pathology has beenin vogue over the past decade, there isa surprising paucity of literature tojustify this, especially in regard to thefoot and ankle. A number of studiesare available for review; however, themajority are anecdotal case reports orcase series with no control group; andthose that do employ a more scientificapproach often have small samplesizes. While the rationale behind theuse of this technology has been thor-oughly examined, one must concludethat further evaluation is required be-
fore making a final judgment in regardto the efficacy for treatment of ten-donopathy in the foot and ankle. Theauthor will review the science behindplatelet concentrates, describe com-
mercially available systems, examineexisting literature, and provide a fewcase examples.
IntroductionThe field of orthobiologics has in-
creased seemingly exponentially overthe past few years, with more compa-nies offering bone substitutes, colla-gen matrices, dermal substitutes andautologous platelet preparations.Specifically of interest to this paper isthe advent and development ofplatelet concentrates, which havegone by a number names includingplatelet rich plasma (PRP), plateletrich concentrate, platelet releasate,platelet rich plasma-concentrate re-lease (PRCR), and autologous condi-tioned plasma (ACP). Regardless of
the name, the principle remains thesame: a patient’s whole blood is col-lected peripherally, then centrifugedto separate the individual compo-nents. Subsequently, the platelet rich
component is isolated, which can beadministered clinically to treat a vari-ety of conditions. The use of thisplatelet concentrate has been evaluat-ed in oral surgery, plastic/cosmeticsurgery, wound healing, orthopaedicsurgery (including bone fusion, frac-ture care, and tendon healing) as wellas multiple other areas. Some of thepopularity may be due to media cov-erage of professional athletes receiv-ing this as an alternative choice tosurgery or extended rehab and signifi-cant time away from their team.
Platelet PhysiologyIn addition to their role in clot-
ting, platelets have been shown to re-lease many proteins responsible for
BY ADAM M BUDNY, DPM
Continued on page 92
The goal in development of PRP productsis to achieve a concentration of platelets above the
baseline value for the subject.
SURGICAL INSIGHTS FROM ACFAS
AutologousPlatelets for Treatment
of Tendonopathyof the Foot and Ankle
www.podiatrym.com
SURGICAL INSIGHTS FROM ACFAS
TENDONOPATHY
92 | AUGUST 2012 | PODIATRY MANAGEMENT
enhancing tissue regen-eration and healingfrom intracellular alphagranules. These nativecytokines include trans-forming growth factorbeta (TGFbeta), vascu-lar endothelial growthfactor (VEGF), plateletderived growth factor(PDGF), insulin-likegrowth factor (IGF) andepithelial growth factor(EGF), among others.1-5
Based on the concentra-tion of these growthfactors, PRP is assumedto stimulate a “supra-physiologic” responsein an attempt to jump-start the healing process in chronicorthopaedic injuries.1
At a more basic level, blood con-tains three main components: plasma,red blood cells (RBC), and whiteblood cells (WBC). These are main-tained in healthy individuals at a rela-tively constant ratio of 93%:6%:1%(RBC, Plasma, WBC, respectively).6
The platelets component of blood ismanufactured in the bone marrow;they have a short lifespan of 7-10
days. They require thrombin to be ac-tivated (usually precipitated by an in-jury) which leads to aggregation, clot-ting, and subsequent release of thegrowth factors from the alpha gran-ules. These factors then play a varietyof roles in tissue healing (Table 1).1,3
The goal in development of PRPproducts is to achieve a concentrationof platelets above the baseline valuefor the subject. There is not yet astandardization for the value of con-
centration that defines“platelet rich”, and themanufacturers of PRPsystems all achieve dif-ferent levels of plateletsand growth factors intheir centrifugation pro-cess (Table 2). The nor-mal concentration ofplatelets is 150,000/uLto 350,000/uL. Most re-search suggests at least1,000,000/uL is neededto promote an increasein healing.1,4
Most of the manu-facturers of PRP sys-tems achieve an in-crease of 3-5x inplatelets and will use
one or two centrifugation cycles toseparate the blood products). The sys-tem offered by Arthrex, AutologousConcentrated Plasma (ACP) (ArthrexInc, Naples, FL) is unique in thatWBCs and neutrophils are specificallynot included while the plasma con-centrate administered still contains asupra-physiologic amount of plateletsand associated cytokines.7 Previousliterature has suggested that the pres-ence of WBCs and neutrophils may bedeleterious to wound healing.8
Tendon Physiology and HealingTendon and ligament injuries can
fall into two broad categories of eitheracute or chronic. An acute injury im-plies that a tendon will go through thenormal three phases of healing: in-flammation, cellular proliferation, andremodeling.8,9 The tendon repair se-quence begins after formation of a clotand granuloma at the injury site, fol-lowed by fibroblasts forming collagen,mostly type 3.9 This gradually increas-es mechanical strength, and as thetendon is loaded through elastic defor-mation (i.e., muscle contracture/jointmovement), a gradual transition totype 1 collagen is made. When a ten-don injury becomes chronic, this nor-mal cycle is disrupted, and the tendonis frozen in the proliferative phase.This leads to a degenerative process oftendonopathy characterized by colla-gen fiber disruption, mucoid degener-ation, neo-vascularization, and an ab-
Continued on page 93
Growth Factor Function
TGF-beta Promotes formation of extracellular matrix andregulates bone metabolism
PDGF Stimulates angiogenesis, promotes cell proliferationand granulation
VEGF Angiogenesis
IGF Stimulates fibroblasts ad myoblasts
EGF Promotes cell differentiation and proliferation
TABLE 1
Growth Factors and TheirRespective Effects on Tissue
Platelet Concentration Increase in Platelets AboveSystem Baseline
Magellan* 2-14x
GPS III∞ Up to 9.3x
Symphony§ 3-6x
ACP ¤ 2x
* Arteriocyte Medical Systems, Cleveland, OH∞ BioMet Biologics Inc., Warsaw, IN§ Depuy Orthopaedics, Warsaw, IN¤ Arthrex Inc., Naples, FL
TABLE 2
Commercially AvailablePlatelet Concentration Systemsand the Relative Increasein Concentration of Platelets

AUGUST 2012 | PODIATRY MANAGEMENT | 93www.podiatrym.com
SURGICAL INSIGHTS FROM ACFAS
TENDONOPATHY
sence of inflammation.2,8 Tendons are,in general, relatively avascular struc-tures with a low basal metabolismthat contributes to the prolonged re-covery after injury.10 In vitro studieshave confirmed that application ofPRCR can lead to accelerated prolifer-ation of tenocytes, as well as Type 1and 3 collagen.9,10
Autologous platelet preparationshave the potential to interrupt chronictendonopathy in several ways. First ofall, this process is mediated by theadministration of supra-physiologicconcentrations of growth factors fromthe alpha granules contained in thePRP injection. As previously noted,this will introduce an increasedamount of cytokines that will subse-quently restart the cycle of tendon re-pair.3 This, combined with the me-chanical injury from injecting in theform of “micro-tenotomy” or “pepper-ing” techniques, will serve to createan inflammatory response to a stag-
nant healing environment and thusinitiate tendon repair.8
Literature ReviewWhen a systematic search for PRP
(or any of the aforementioned de-scriptors) is completed, a significantamount of literature can be found inregard to tendonopathy. The searchmust be narrowed, however, to re-main relevant to this article. Thenumber of prospective trials has sig-nificantly increased over the pastthree years to include research insports medicine, anterior cruciate lig-ament repair, rotator cuff repairs,Achilles tendonopathy, patellar ten-donopathy, lateral epicondylitis andplantar fasciosis.1, 3,8,10,12,14 Recently, thequality of this research has improvedto include prospective controlled tri-als; however, a number of case re-ports and series with retrospectivedata are available as well.
In 2011, Finoff, et al. wrote a two-
part paper. Part 1 was a retrospectivereview. Part 2 of their study was tobring patients back for a prospectivediagnostic ultrasound on patients un-dergoing percutaneous microtenoto-my and PRP injection for recalcitranttendonopathy.8 Their patients had avariety of involved tendons in boththe upper and lower extremities(n=10 (24.4%) and (n=31 (75.6%),respectively. Post-procedurally, theyfound that 83% of subjects were sat-isfied with the outcome. Althoughnone of their patients achieved asonographically normal tendon, therewere significant improvements inechotexture, resolution of intratendi-nous calcifications, and a decrease inintratendinous neovascularity.
The study was slightly differentfrom much of the available literatureas it did involve a percutaneous teno-tomy followed by PRP, while mostother trials simply describe three to
Continued on page 94

www.podiatrym.com
SURGICAL INSIGHTS FROM ACFAS
TENDONOPATHY
94 | AUGUST 2012 | PODIATRY MANAGEMENT
five injection sites for administrationof the PRP into the mid-substance ofthe tendon.
Another recent randomized con-trolled trial (RCT) evaluated the effi-cacy of PRP in arthroscopic rotatorcuff repair.10 This was an RCT of 53patients divided into a treatmentgroup (PRP) (n=26) and controlgroup (n=27), with healing verifiedvia validated scoring systems as wellas a follow-up MRI. All patients un-derwent rotator cuff repair, and thePRP group was found to have lowerpain scores at days 3, 7, 14, and 30days after surgery. Strength in exter-nal rotation was also higher at threemonths.
The follow-up MRI did notdemonstrate any significance in heal-ing rate; however, there were nine re-tears in the PRP group and 12 in thecontrol group, with an overall healingrate of 54% (in agreement with previ-ous literature). Their conclusion wasthat PRP could decrease pain and ac-celerate functional recovery. Thisgroup used the BioMet GPS systemfor platelet concentration, and thePRP was administered after comple-tion of the repair by injection into thejoint space.
In contrast to the study by Randel-li, another group was unable todemonstrate the same acceleratedhealing in rotator cuff repairs.5 Thiswas a cohort study of 42 patients,with 19 in the PRP treatment groupand 23 in the control. The authorsfound appreciable differences in pain,range of motion, strength, or function-al scores. Differences included the factthat they did not use a commerciallyavailable PRP system; instead, theyused an automated plateletpheresissystem, and they created a platelet gelwhich was then sutured between thetendon and bone. They do concedethat one of the greatest weaknessesbetween all studies about PRP is thelack of standardization of preparation,concentration, levels of WBCs in thegel, and platelet activation.
A recent paper on the applicationof PRP in ACL repair was also con-ducted to evaluate if there was a re-duction in anterior knee pain, kneel-ing pain, and donor site morbidityafter patellar tendon graft harvest-
ing.14 They also evaluated bone heal-ing at the final follow-up via MRI andconducted a clinical exam as well asvalidated (VISA) questionnaires.Forty athletes (all male) underwentACL reconstruction with an autolo-gous bone-patellar tendon-bone graft.They found a statistically significantincrease in VISA scores in the treat-ment group in regard to knee pain aswell as filling of the bone defect in85% (only 60% in the control group).The authors conclude that applicationof PRP can reduce pain in athleteswhich could otherwise be an obstacleto quick return to high-level sport.
The only paper found whichspecifically addresses plantar fasciosiswas a pilot study by Barrett andErredge in 2004.12 This was a case se-ries of just nine patients undergoingPRP injection for recalcitrant plantar
fasciosis. The authors did comparepre- and post-procedural ultrasoundto evaluate the thickness of the fasciaand did find that there was a meanreduction of 2.30mm. Six of the ninehad complete resolution after twomonths, and one had dropped fromthe study after receiving a corticos-teroid injection. This was a very limit-ed study with no control group andvery small sample size, which wouldbe difficult to generalize to a largerpopulation. Also no statistical evalua-tion was performed.
At the most recent AmericanAcademy of Orthopaedic Surgeons(AAOS) meeting (February 2012), anabstract was presented by Monto.16 Inthis prospective, controlled trial, 36patients were randomized to an ultra-sound-guided corticosteroid or PRPinjection. All had failed extensiveconservative treatment for approxi-mately five months. The AOFAS scoreimproved from 52 (pre-injection) to81 at three months, but fell back to 58at twelve months, whereas in the PRPgroup, the scores improved from 37
pre-injection to 95 and 94, respective-ly. The author concluded that PRPwas more effective and durable fortreating recalcitrant plantar fasciitis.
Treatment of chronic Achilles ten-donopathy with PRP has been evalu-ated by a number of authors.8,13,15-17 Forthe most part, there have been favor-able results reported in regard to out-comes; however, the patient samplesize of all combined studies is stillvery small and difficult to apply to thegeneral population. Sanchez, et al.were the first to report the use of PRPin a retrospective case control seriesof Achilles tendonopathy in twelveathletes.16 The authors found betterfunctional outcomes and an earlier re-turn to training in the PRP group(n=6) with a 12 month follow-up.They also found a smaller cross-sec-tional area of the tendons on follow-
up MRI. Their series was, of course,limited by a small sample size andretrospective design. The same seniorauthor later reported outcomes associ-ated with two patients treated for re-vision Achilles surgery due to tissueloss.18 Both patients were athleteswho were able to return to their re-spective sports at 14 and 28 weeks.
Gaweda, et al. presented a caseseries of 14 patients (15 Achilles ten-dons) who had chronic Achilles ten-donopathy.15 Their treatment protocolwas 3mL of PRP administered withultrasound guidance, followed by sixweeks with crutches (six patients hadto undergo a second injection). Theyreported significant improvements inVISA and AOFAS foot and anklescores at 18 months. The AOFASscore increased from 55 to 96 at finalfollow-up. In addition, they found im-provements in the ultrasonic appear-ance of the tendons with decreasedthickness, reduction of interstitialtears, and hypo-echoic foci. Of note,they did report a transient increase in
Treatment of chronicAchilles tendonopathy with PRP has been evaluated
by a number of authors.
Continued on page 96

www.podiatrym.com
SURGICAL INSIGHTS FROM ACFAS
TENDONOPATHY
96 | AUGUST 2012 | PODIATRY MANAGEMENT
neovascularization for up tothree months.
DeVos, et al. performed alevel 1 RCT on chronic mid-sub-stance Achilles tendonopathy, inwhich one group received an ul-trasound guided PRP injectionvs. a saline injection controlgroup.13 The original paper re-ported 24 week outcomes for 54patients, and the same data wasused in a later paper reportingon a one year follow-up.17 Boththe PRP and the saline groupsdemonstrated statistically signifi-cant improvements in VISAscores (21.7 and 20.5 respective-ly). Both groups received whatcould be considered a variationof a micro-tenotomy, with 15 perfora-tions during administration of eitherthe PRP or saline. In addition, bothgroups were treated post-procedurallywith an eccentric training program.
Although a level-one RCT, a fewquestions remain. First of all, was itthe micro-tenotomy that caused theimprovement in both groups? Second-ly, since both groups underwent aneccentric strengthening regimen afterthe treatment, does this trial simplyshow that the ideal treatment forAchilles tendonopathy is physicaltherapy alone? Investigations have in-deed shown that both micro-tenotomyand eccentric training are effective formid-portion Achilles tendonopathy.8
Case ExamplesThe author has used the Autolo-
gous Concentrated Plasma system(Arthrex Inc., Naples, FL (Figure 1)for approximately one year for bothchronic plantar fasciosis and mid-portion Achilles tendonopathy. In allcases, patients have undergone ex-tensive conservative treatments fortheir respective conditions, includingstretching, strengthening, bracing,orthotics, physical therapy, etc. If thepatients fail to respond to the conser-vative measures, and their next stepwould be to make a decision forsurgery, they are given the option toattempt an ultrasound-guided injec-tion of ACP. The authors preferred
technique includesadministration of apre-emptive infiltra-tion with 0.5%bupivicaine proxi-mal to the site ofpathology. Subse-quently the ACP isinjected with a“peppering” tech-nique (approximate-ly 5-10 individualdepots) into the ten-don or fascia. Post-procedurally, theyare to abstain fromNSAIDs for at leasttwo weeks, and usetramadol or hy-drocodone with ac-etaminophen and
ice for pain. In both scenarios, theyare protected with a removable frac-ture boot and crutches. Gradual tran-sition to shoes and limited activity isallowed at two weeks with an appro-priate home exercise program. Re-turn to low-impact aerobic activi-ty/exercise is allowed after four tosix weeks.
Plantar FasciosisA 48-year-old female had been
treated for plantar fasciitis for sixmonths with no relief. This includedplantar fascia-specific stretching, or-thotics, NSAIDs, and night splinting.ACP was offered to her as an alterna-tive to surgical fasciotomy. Injectionwas administered under ultrasoundguidance (Figure 2) followed by twoweeks in a protective fracture boot.At one month, she was pain free andtransitioned to accommodative shoesand activities without limitation.
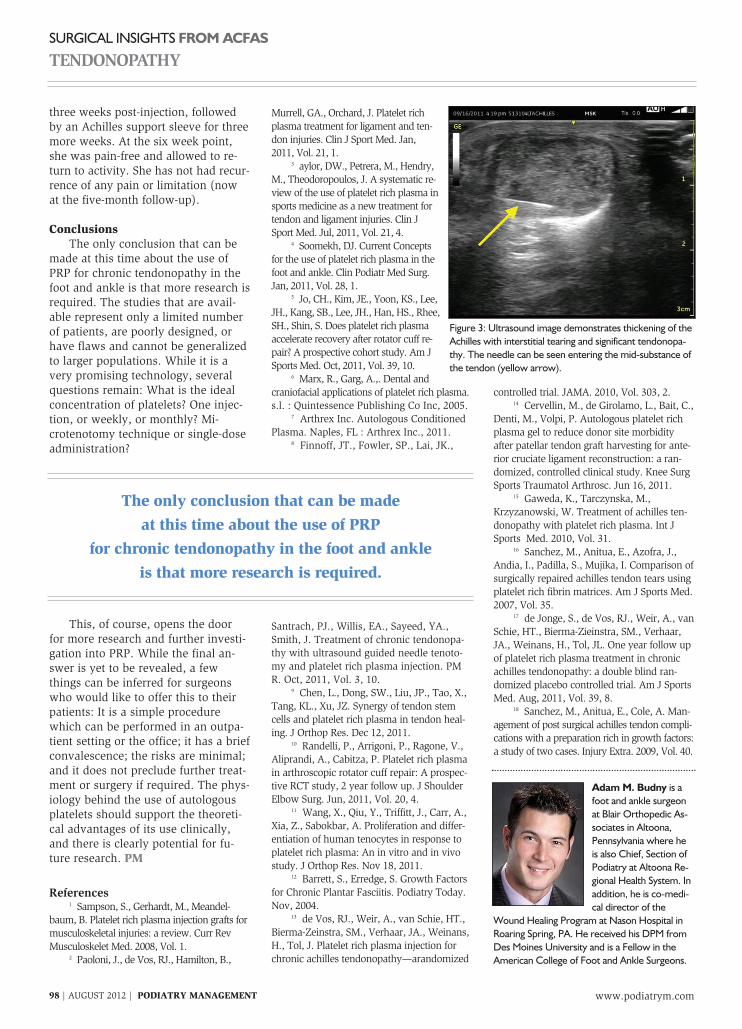
Achilles TendonopathyA 53-year-old female presented
with a two-year history of Achillespain. She had been treated by anotherprovider unsuccessfully and had per-sistent pain in the left Achilles tendon.After she had gone through physicaltherapy as well as bracing without fur-ther relief, an ACP injection was of-fered as a last resort prior to surgicalintervention. Using the technique pre-viously described, she underwent in-jection therapy (Figure 3). She wasimmobilized in a fracture boot for
Continued on page 98Figure 1: Arthrex ACP centrifuge system(a) and syringe(b).
Figure 2: Ultrasound image demonstrates thickening of the plantar fascia (green arrow) with concomitant heelspur. The needle is perpendicular to the long axis of the ultrasound probe (yellow arrow).
www.podiatrym.com
SURGICAL INSIGHTS FROM ACFAS
TENDONOPATHY
98 | AUGUST 2012 | PODIATRY MANAGEMENT
three weeks post-injection, followedby an Achilles support sleeve for threemore weeks. At the six week point,she was pain-free and allowed to re-turn to activity. She has not had recur-rence of any pain or limitation (nowat the five-month follow-up).
ConclusionsThe only conclusion that can be
made at this time about the use ofPRP for chronic tendonopathy in thefoot and ankle is that more research isrequired. The studies that are avail-able represent only a limited numberof patients, are poorly designed, orhave flaws and cannot be generalizedto larger populations. While it is avery promising technology, severalquestions remain: What is the idealconcentration of platelets? One injec-tion, or weekly, or monthly? Mi-crotenotomy technique or single-doseadministration?
This, of course, opens the doorfor more research and further investi-gation into PRP. While the final an-swer is yet to be revealed, a fewthings can be inferred for surgeonswho would like to offer this to theirpatients: It is a simple procedurewhich can be performed in an outpa-tient setting or the office; it has a briefconvalescence; the risks are minimal;and it does not preclude further treat-ment or surgery if required. The phys-iology behind the use of autologousplatelets should support the theoreti-cal advantages of its use clinically,and there is clearly potential for fu-ture research. PM
References1 Sampson, S., Gerhardt, M., Meandel-
baum, B. Platelet rich plasma injection grafts formusculoskeletal injuries: a review. Curr RevMusculoskelet Med. 2008, Vol. 1.
2 Paoloni, J., de Vos, RJ., Hamilton, B.,
Murrell, GA., Orchard, J. Platelet richplasma treatment for ligament and ten-don injuries. Clin J Sport Med. Jan,2011, Vol. 21, 1.
3 aylor, DW., Petrera, M., Hendry,M., Theodoropoulos, J. A systematic re-view of the use of platelet rich plasma insports medicine as a new treatment fortendon and ligament injuries. Clin JSport Med. Jul, 2011, Vol. 21, 4.
4 Soomekh, DJ. Current Conceptsfor the use of platelet rich plasma in thefoot and ankle. Clin Podiatr Med Surg.Jan, 2011, Vol. 28, 1.
5 Jo, CH., Kim, JE., Yoon, KS., Lee,JH., Kang, SB., Lee, JH., Han, HS., Rhee,SH., Shin, S. Does platelet rich plasmaaccelerate recovery after rotator cuff re-pair? A prospective cohort study. Am JSports Med. Oct, 2011, Vol. 39, 10.
6 Marx, R., Garg, A.,. Dental andcraniofacial applications of platelet rich plasma.s.l. : Quintessence Publishing Co Inc, 2005.
7 Arthrex Inc. Autologous ConditionedPlasma. Naples, FL : Arthrex Inc., 2011.
8 Finnoff, JT., Fowler, SP., Lai, JK.,
Santrach, PJ., Willis, EA., Sayeed, YA.,Smith, J. Treatment of chronic tendonopa-thy with ultrasound guided needle tenoto-my and platelet rich plasma injection. PMR. Oct, 2011, Vol. 3, 10.
9 Chen, L., Dong, SW., Liu, JP., Tao, X.,Tang, KL., Xu, JZ. Synergy of tendon stemcells and platelet rich plasma in tendon heal-ing. J Orthop Res. Dec 12, 2011.
10 Randelli, P., Arrigoni, P., Ragone, V.,Aliprandi, A., Cabitza, P. Platelet rich plasmain arthroscopic rotator cuff repair: A prospec-tive RCT study, 2 year follow up. J ShoulderElbow Surg. Jun, 2011, Vol. 20, 4.
11 Wang, X., Qiu, Y., Triffitt, J., Carr, A.,Xia, Z., Sabokbar, A. Proliferation and differ-entiation of human tenocytes in response toplatelet rich plasma: An in vitro and in vivostudy. J Orthop Res. Nov 18, 2011.
12 Barrett, S., Erredge, S. Growth Factorsfor Chronic Plantar Fasciitis. Podiatry Today.Nov, 2004.
13 de Vos, RJ., Weir, A., van Schie, HT.,Bierma-Zeinstra, SM., Verhaar, JA., Weinans,H., Tol, J. Platelet rich plasma injection forchronic achilles tendonopathy—arandomized
controlled trial. JAMA. 2010, Vol. 303, 2.14 Cervellin, M., de Girolamo, L., Bait, C.,
Denti, M., Volpi, P. Autologous platelet richplasma gel to reduce donor site morbidityafter patellar tendon graft harvesting for ante-rior cruciate ligament reconstruction: a ran-domized, controlled clinical study. Knee SurgSports Traumatol Arthrosc. Jun 16, 2011.
15 Gaweda, K., Tarczynska, M.,Krzyzanowski, W. Treatment of achilles ten-donopathy with platelet rich plasma. Int JSports Med. 2010, Vol. 31.
16 Sanchez, M., Anitua, E., Azofra, J.,Andia, I., Padilla, S., Mujika, I. Comparison ofsurgically repaired achilles tendon tears usingplatelet rich fibrin matrices. Am J Sports Med.2007, Vol. 35.
17 de Jonge, S., de Vos, RJ., Weir, A., vanSchie, HT., Bierma-Zieinstra, SM., Verhaar,JA., Weinans, H., Tol, JL. One year follow upof platelet rich plasma treatment in chronicachilles tendonopathy: a double blind ran-domized placebo controlled trial. Am J SportsMed. Aug, 2011, Vol. 39, 8.
18 Sanchez, M., Anitua, E., Cole, A. Man-agement of post surgical achilles tendon compli-cations with a preparation rich in growth factors:a study of two cases. Injury Extra. 2009, Vol. 40.
Adam M. Budny is afoot and ankle surgeonat Blair Orthopedic As-sociates in Altoona,Pennsylvania where heis also Chief, Section ofPodiatry at Altoona Re-gional Health System. Inaddition, he is co-medi-cal director of the
Wound Healing Program at Nason Hospital inRoaring Spring, PA. He received his DPM fromDes Moines University and is a Fellow in theAmerican College of Foot and Ankle Surgeons.
Figure 3: Ultrasound image demonstrates thickening of theAchilles with interstitial tearing and significant tendonopa-thy. The needle can be seen entering the mid-substance ofthe tendon (yellow arrow).
The only conclusion that can be madeat this time about the use of PRP
for chronic tendonopathy in the foot and ankleis that more research is required.