Embed Size (px)
Citation preview

Autosomal Recessive Distal Muscular Dystrophy: A Comparative Study
with Distal Myopathy with Rrmmed Vacuole Formation
Ikuya Nonaka, MD," Nobuhiko Sunohara, MD,* Eijiro Satoyoshi, MD," Kenjiro Terasawa, MD," and Kyozo Yonemoto, MD'F
~~~~~~~~ ~ ~ ~ ~ ~ ~ ~
To clarify the clinical and morphological characteristics of distal muscular dystrophy, clinical and pathological mate- rial from 4 affected persons was compared with similar studies in 4 patients with distal myopathy with rimmed vacuole formation. Although these two forms of autosomal recessive distal myopathy with onset in young adulthood were highly similar in their clinical symptoms, histochemical and electron microscopic findings of muscles subjected to biopsy were quite different. The muscle abnormalities in distal muscular dystrophy were almost the same as those in Duchenne muscular dystrophy, showing massive fiber necrosis followed by active fiber regeneration. In contrast, distal myopathy with rimmed vacuole formation showed a progressive muscle fiber atrophy and loss, rimmed vacuoles in the sarcoplasm, and no apparent fiber necrosis or regeneration.
Nonaka I, Sunohara N, Satoyoshi E, Terasawa K, Yonemoto K: Autosomal recessive distal muscular dystrophy: a comparative study with distal myopathy with rimmed vacuole formation.
Ann Neurol 17:51-59, 1985
A myopathy with a predilection for the distal ex- tremities, distal myopathy is prevalent in Sweden and is transmitted as an autosomal dominant trait [ l , 7, 10, 437. In affected patients muscle weakness usually ap- pears after the age of 40 years. Histological examina- tion of muscle shows myopathic changes and type 1 fiber atrophy, similar to the changes in myotonic dys- trophy [lo]. Non-Swedish forms of distal myopathy are probably heterogeneous and have various clinical and morphological features; the time of onset of the disease varies from infancy [2, 12, 18, 19, 401 to late adulthood 12 11, and muscle biopsies show myopathic changes, such as active fiber necrosis [8, 12, 19-21, 24, 35, 371, vacuolar formation {8, 13, 20, 21, 24, 28, 29, 31, 351, and an abnormal distribution of muscle fiber types, including hypotrophic type 1 fibers with type 1 fiber predominance 12, 401. Among non- Swedish patients two forms of distal myopathy with common clinical and pathological characteristics have recently been reported. The first 125-271 is character- ized by (1) transmission as an autosomal recessive trait; (2) onset usually in young adulthood; (3) early and preferential involvement of the gastrocnemius mus- cles; (4) highly elevated serum creatine kinase (CK)
levels; (5) relatively rapid progression leading to a nonambulant state usually within ten years of onset; and (6) dystrophic muscle abnormalities mimicking those of Duchenne muscular dystrophy (DMD). Be- cause of the well-established autosomal recessive in- heritance and characteristic clinical features, this disor- der has been regarded as a clinical entity by Miyoshi 127) who proposed the name autosomal recessive distal muscular dystrophy (DisMD). Two brothers 1161 and 3 sporadic cases 1241 with similar clinical and patho- logical features have been described recently; there- fore, DisMD is presumed to be fairly common.
The clinical features of the second form E14, 17, 22, 32, 38, 391 closely resemble those of DisMD, except for severe weakness and atrophy of peroneal muscles and only slightly elevated CK levels. The muscle ab- normalities are characterized by muscle fiber atrophy with rimmed vacuole formation in the sarcoplasm. The disease has been tentatively labeled familial distal my- opathy with rimmed vacuole formation (DMRV) [32}. To determine the differences in the pathophysiological mechanisms of muscle fiber degeneration and to at- tempt to confirm the clinical specificity in the de- scribed two forms of distal myopathy, a comparative
From the *National Center for Nervous, Mental and Muscular Dis- orders, Kodaira, Tokyo 187, Japan, and the tDepartmenr of Or- thopedics, Jikeikai University Medical School, Tokyo 105, Japan.
Received Jan 4 , 1984, and in revised form May 4. Accepted for publication May 6, 1984. Address reprint requests to Dr Nonaka.
5 1

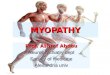
Fig I . A 29-year-old man with distal muscular dystrophy (Pa- tient l ) who had marked muscle weakness and atrophy in the lower legs. Note the markedly decreased muscle bulk in the gastro- cnemius and the relatively well-presemed thigh musclef .
histochemical and electron microscopic study was un- dertaken on muscle biopsy specimens. In addition, the results were compared with those in DMD.
Clinical Observations DisMD Group (Patients 1 through 4) None of the patients with DisMD had a family history of distal myopathy, although the parents of Patient 4 were cousins. All patients became aware of difficulty in climbing stairs or running, and developed atrophy of the calf muscles between 14 and 24 years of age (average, 18.5 years). The disease progressed rapidly in Patient 2; three years after the onset of disease, she walked alone but could not climb stairs without assistance. In the remaining 3 patients symptoms progressed steadily but at a slower rate.
O n physical examination all patients had conspicuous m u - cle atrophy and weakness in the calves, especially in the gastrocnemius muscles (Fig 1). Because of mild proximal muscle weakness, patients arose from the sitting position with Gowers’s maneuver. In Patients 3 and 4, the left leg was less severely affected than the right. There was mild muscle weakness in the hands and arms in Patients 1 and 2 but none in Patients 3 and 4 . Neck and facial muscles were spared.
Deep tendon reflexes were markedly diminished or absent in affected muscles. There were no muscle fasciculations.
CK levels were markedly elevated, as shown in Table 1. Lactic dehydrogenase, serum glutamic-oxaloacetic transami- nase and glutamic-pyruvic transaminase, and aldolase levels were also abnormally high. In all patients electromyography showed a myopathic pattern with no spontaneous discharges.
DMRV Group (Patients 5 throagh 8) The clinical and pathological features of Patients 5 through 7 have been described previously [32). A11 patients became aware of gait disturbance at the age of about 20 years with an initial symptom of foot drop or difficulty in standing on tip- toes, indicating the early preferential involvement of the lower legs. The disease progressed rapidly, later spreading to the thighs and arms. Mild weakness in the sternocleidomas- toid muscles developed in the advanced stage (Patients 5 , 7, and 8); the facial muscles were spared. O n physical examina- tion the peroneal muscles were found to be the most se- verely involved; patients could not stand on their toes or heels and showed marked weakness on dorsiflexion of an- kles. The gastrocnemius muscles were less severely affected. Deep tendon reflexes were diminished or absent in the af- fected muscles.
Serum CK levels were slightly elevated, ranging from 104 to 531 mU/ml (normal, less than 110 mU/ml). Serum aldol- ase, serum glutamic-oxaloacetic transaminase and glutamic- pyruvic transaminase, and lactic dehydrogenase levels were within normal limits except in Patient 6 , who had mildly elevated enzyme activities. Electromyography showed a my- opathic pattern in all patients that was associated with some spontaneous discharges in the form of positive sharp waves and fibrillation voltages (Patients 5 and 8).
Materials and Methods The muscle biopsy specimens were frozen in isopentane cooled by liquid nitrogen. Serial frozen sections were stained with H&E, modified Gomori trichrome, and a battery of histochemical methods [9]. For morphometric evaluation the muscle fibers were classified into type 1, 2A, 2B, and 2C fibers in adenosinetriphosphatase- (ATPase) stained sections [9] and their diameters were measured with a Kontron MOP2 semiautomatic image analyzer.
For electron microscopical examination small pieces of the biopsy specimens were fixed in cacodylate-buffered 2% glu- taraldehyde solution for two hours. After rinsing in the same buffer solution, they were postfixed for four hours in sym- collidine-buffered osmium tetroxide containing lanthanum nitrate. In addition to routine electron microscopical exami- nation, the population of satellite cells was determined in 200 cross-sectioned muscle fibers at a final magnification of X 3,000.
Results Muscle Histochemistry in DisM D In Patients 1 and 2 , the gastrocnemius muscle speci- mens studied were almost totally replaced by fibrous and adipose tissue. A few small-caliber fibers were em- bedded in dense connective tissue. Although the gas-
52 Annals of Neurology Vol 17 No 1 January 1985

Table I . Clinical Summary
Patient No., Age (yr),
Condition Sex
Distal muscular I . , 29, M dystrophy 2., 17, F
3., 28, F 4., 21, Mb
Distal myopathy 5., 25, F' with rimmed 6., 27, M' vacuole formation 7., 27, FC
8., 29, F
Age at Onset (yr)
24 14 20 16 22 24 20 26
Predominantly Affected Muscle
Motor Nerve CK Conduction (mU/mla Velocity ( d s )
Gastrocnemius Gastrocnemius Gastrocnemius Gastrocnemius Tibialis anterior Tibialis anterior Tibialis anterior Tibialis anterior
4,510 8,000
10,620 4,000
224 531 104 122
57.0 (tibial) 5 1.6 (peroneal) 46.5 (peroneal) 50.6 (tibial) 61.5 (median) 51.8 (median) 65.0 (median) 68.0 (median)
"Normal, less than 110 mU/ml bConsanguinity 'Positive family history.
CK = serum creatine kinase.
trocnemius muscle in Patient 4 was relatively well pre- served, it showed advanced myopathic changes when compared with the proximal portion of the rectus femoris. Even in less affected proximal rectus femoris (Patients 1, 3, and 4 ) and biceps brachii (Patient 2) muscles, there was a marked variation in fiber size, with
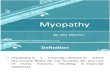
Fig 2. Minute structure of muscle in Patient 2 with distal mus- cular dystrophy. Whereas the gastrocnemius muscle is almost to- tally replaced by connective and adipose tissue, the less severely af- fected proximal muscle of the biceps brachii shows moderate variability offiber size and numerous necrotic fibers with occa- sionalphagocytosis (asterish). (H&E; X 300.)
a number of necrotic fibers throughout the sections that were occasionally invaded by acid phosphatase- positive macrophages (Fig 2). Regenerating fibers, with basophilic cytoplasm, vesicular nuclei, and staining for alkaline phosphatase, were increased in number. None of the fibers had rimmed vacuoles. Hypercontracted (opaque) fibers were scattered throughout, most of which were stained by glyoxal-bis(2-hydroxyanil), dem- onstrating ionic calcium. O n ATPase staining both type 1 and 2 fibers were seen to be distributed in a normal mosaic pattern, although undifferentiated type 2C fibers showed an increase in number (Fig 3 ; Table 2). In the gastrocnemius muscle in Patient 4, type 1
Nonaka et al: Autosomal Recessive Distal MD 53

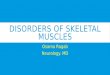
F i g 3. Histochemical study of rectus femoris muscle in Patient 1 with distal muscular dystrophy. In addition to well-differ- entiated type 1 (I) , 2A (A), and 28 (Blfibers in a normal mo- saic pattern, numerous undzJferentiated type 2C ( C ) fibers are scattered throughout the section, rejecting an active regenerative process. (a, H 6 E ; 6, routine ATPase; c, ATPase with preincu- bation at pH 4.6; d, the same as cat pH 4.2; a-d, x 120.)
Table 2. Fiber Tybe Distribution and Fiber Diameter
Condition
No. of Fiber Type Distribution Mean Fiber Diameter (p) Patient Examined Fibers No. Muscles Examined 1 2 A 2B 2 c 1 2 A 2B 2C
Distal muscular 1 RF 308 19.5% 15.9% 46.1% 18.59% 44.3 62.0 47.9 35.1 dystrophy G C . . .
2 BB 562 24.0 13.2 32.9 29.9 40.9 31.6 31.8 29.2 GC . I .
3 RF 639 48.9 27.9 1.1 22.1 64.6 64.9 84.9 54.9 GC N E
4 RF 519 23.3 28.9 32.8 15.0 56.3 51.6 45.9 45.5 G C 568 11.6 41.2 0 47.2 63.4 15.6 . . . 42.9
Distal myopathy 5 VM 490 81.2 9.0 0 9.8 38.2 20.5 . . . 15.9 with rimmed vacuole 6 VM 34 3 47.5 36.4 15.2 0.9 52.1 58.4 59.4 60.7 formation TA 320 69.7 22.5 0.9 6.9 46.8 61.6 62.7 28.0
7 BB 435 65.3 20.7 8.3 5.7 32.9 44.8 62.0 18.8 8 BB 396 27.5 38.6 33.6 0.3 47.1 43.6 41.3 41.2
TA 484 57.9 32.2 1.9 8.0 48.4 25.9 22.6 23.5
a
a
"Mostly fibrous and adipose tissue. RF = rectus fernoris; GC = gastrocnemius; BB = biceps brachii; VM = vastus medialis; TA = tibialis anterior; NE = nor examined.
54 Annals of Neurology Vol 17 No 1 January 1985

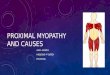
Fig 4. Representative muscle structure in Patient 8 with distal myopathy with rimmed vacuole formution. There is marked vari- ability in muscle fiber size, with mild endomysial fibrosis. Numerous vacuoles rimmed by granular materials (rimmed vacuoles) (arrowheads) are present in relatively small-caliber fibers. (Modzjied Gomori trichrome stain; x 2JO.)
fibers were hypertrophic and type 2 fibers tended to be atrophic and occasionally clustered in small groups.
Muscle Histocbemisty in D M R V The histological and histochemical findings in Patients 5 through 7 have been described in a previous report C321. In Patients 6 and 8, both proximal and distal muscles were subjected to biopsy at the same time, and the findings confirmed the preferential involve- ment of distal muscles.
In all patients there was marked variation in fiber size. Although small-caliber fibers tended to aggregate in small groups, there was no grouped atrophy, as is typical in a neuropathic process. Except for Patient 6, who had one necrotic fiber with phagocytosis, the mus- cles showed no apparent fiber necrosis. Regenerating fibers characterized by basophilic cytoplasm, vesicular nuclei, and prominent nucleoli were not recognizable. There was mild to moderate endomysial fibrosis and mild adipose tissue replacement. In addition to the nonspecific myopathic changes, the predominant find- ing was the presence of numerous vacuoles rimmed by
finely granular material that was basophilic on H&E and purple-red on modified Gomori trichrome staining (Fig 4). Most vacuoles showed acid phosphatase activ- ity. Fiber type analysis (see Table 2) disclosed that both type 1 and type 2 fibers were affected, although type 1 fibers tended to predominate and type 2B fibers de- creased as the disease progressed. Type 2C and al- kaline phosphatase-positive fibers were slightly in- creased in number. The vacuoles did not stain positively with periodic acid-Schiff or oil red 0.
Electron Microscopy in DisMD On electron microscopy examination a number of fibers were found to be necrotic. Degenerated fibers were frequently filled with fragmented myofibrils and were invaded by numerous phagocytes. Even fibers showing early structural changes, such as focal myofibrillar disorganization and hypercontraction, were surrounded by phagocytes, which occasionally in- vaded the sarcoplasm. Scattered throughout were re- generating fibers containing poorly organized myo- fibrils and increased numbers of ribosomes. Twin, triple, or multiple satellite cells, probably resulting from recent cell division, were increased in number (Fig 5) . Such satellite cells occasionally showed “ac- tivated” characteristics, including an increased number of organelles, markedly proliferated caveolae forming tubular structures, and large nuclei with distinctive in- dentation. An increase in the number of satellite cells
Nonaka et al: Autosomal Recessive Distal MD 5 5

was confirmed by statistical analysis: 16.0 to 18.6% of the nuclei belonged to satellite cells in Patients 1 through 3 (controls, mean * SD, 4.4 t 1.8% 1361 (Table 3).
Electron Microscopy in DMRV The outstanding ultrastructural features in the DMRV group were numerous myeloid (lamellar) bodies, and vacuoles that contained cytoplasmic debris and gly- cogen particles (Fig 6). These inclusions were sur- rounded not by membranes but, rather, usually by myofibrils with occasional focal disorganization and Z
Table 3 . Quantitative Analysis of Satellite Cell Populations
Fig 5 . Electron micrograph of Patient 2 with distal muscular dystrophy. Multiple satellite cells probabi$ resulting from recent cell division are present in a mildly degeneratedfiber. A phago- ryte (p) is present in the endomysium. (Lanthanum nitrate stain; x 6,900.)
streaming. Glycogen particles were slightly increased in number in subsarcolemmal areas. Even in and around fibers containing such inclusions, phagocytes were not recognizable. Satellite cells were quiescent and not morphologically altered. A quantitative analy- sis of satellite cell populations demonstrated no in-
Condition
~
Patient Examined No. of No. of No. of SNlMF SNiMN -I- SN No. Muscle MF MN SN (5%) (5%)
Distal muscular dystrophy
Distal myopathy with rimmed vacuole formation
Duchenne muscular
Controls' dystrophyb
1 2 3 4" 5 6 7 8
RF 200 22 1 42 21 16.0 BB 200 186 39 20 17.3 RF 200 192 44 22 18.6
VM 200 196 6 3 2.9 TA 200 292 22 11 7.5 BB 200 181 14 7 7.1 TA 200 2 16 5 3 2.3
23 % 10" 14.9 5 3.2d
4.4 * 1 .8d
"No electron microscopic specimen available. bW&ayama and Schotland 1421. 'Schmalbruch and Hallhammer 1361. Subjects 25 to 35 years old. "Mean ? SD. MF = muscle fibers; MN = myonuclei; SN = satellite cell nuclei; RF = rectus femoris; BB = biceps brachii; VM = vascus medialis: TA = tibialis anterior.
56 Annals of Neurology Vol 17 N o 1 January 1985

Fig 6. Electron micrograph of Patient 7 with distal myopathy Table 4. Summavy of Histological Findings with rimmed vacuole formution. Despite the presence of numerous autophagic vacuoles and myeloid bodies in the muscle fibers, the satellite cell (arrow) as in the quiescent state. No phagocytes are seen in or around the degenerative jiber. (Lanthanum nitrate stain; X 3,600.)
crease in satellite nuclei compared with the amount in age-matched controls (see Table 3). The morpholog- ical characteristics of DisMD, DMRV, and DMD are summarized in Table 4.
Discussion The inheritance and symptoms of DisMD resemble those of DMRV. The preferential involvement of the gastrocnemius rather than peroneal muscles and the high CK levels in DisMD are probably the clinical findings crucial to differential diagnosis. The muscle abnormalities are strikingly different in the two forms of distal myopathy: in DisMD, active fiber necrosis followed by regeneration resembles that in DMD 13, 4, 301. Although myopathic changes with muscle fiber necrosis can be found in a number of autosomal domi- nant and sporadic distal myopathies, Miyoshi and col- leagues 125-271 in a study of 17 patients in eight families confirmed that DisMD is transmitted as an autosomal recessive trait. Although none of the pres- ent 4 patients had a positive family history, the clinical and pathological features were identical to those of DisMD.
The most outstanding morphological features in DMRV are myopathic change and rimmed vacuole formation. The rimmed vacuole per se is not a finding
Finding DisMD DMRV DMD
Degeneration - + Rimmed vacuoles -
Necrosis with + ? + Opaque fibers + Basophilia + Alkaline phosphatase- + 5 + Type 2C fibers on t t t t t t t
No. of satellite cells t t t --t t t t
phagocytosis + -
Regeneration + -
positive fibers
ATPase staining
- + Small fibers in groups -
Fiber type predominance ? 1 1 Fiber type involvement 1 + 2 1 + 2 1 + 2
in advanced stage
DisMD = distal muscular dystrophy; DMRV = distal myopathy with rimmed vacuole formation; DMD = Duchenne’s muscular dys- trophy; - = none; + = marked; ? = mild;? ? t = markedly increased; +- ? = normal to mildly increased.
specific to this disorder, for such vacuoles can be seen in various neuropathic and myopathic processes 19, 1 1, 151. Because there is no histological evidence suggest- ing a neuropathic or dystrophic process, vacuole for- mation in this state is assumed to play an important role in inducing muscle fiber atrophy and fiber loss. Focal myofibrillar degeneration, probably due to diges- tion by a certain proteolytic enzyme, is assumed to initiate lysosomal activation of enzymes such as cathep- sins, which probably induce an antophagic phenome- non [ 3 2 } . The phagocytized myofibrils and cytoplasmic
Nonaka et al: Autosomal Recessive Distal MD 57

organelles are then degraded in the lysosomes, with subsequent formation of the myeloid bodies recog- nized on electron microscopy and the rimmed vacu- oles noted histochemically.
The repair process taking place after muscle fiber degeneration is also different in the two forms of my- opathy. Statistical analysis of undifferentiated type 2C fibers, which stain darkly on ATPase staining with both alkaline and acid preincubation, showed a re- markable increase in the number of these fibers in DisMD and only a slight increase in DMRV. Because the regenerating fibers in dystrophic muscles behave as do type 2C fibers on ATPase staining C9, 331, the increased number of these fibers in DisMD indicates active regeneration after degeneration.
The paucity of a regenerative process in DMRV and the active regeneration in DisMD were also confirmed by electron microscopical examination with statistical analysis of satellite cell populations. The satellite cell is a mononucleated cell, located between the basal lam- ina and plasma membrane of the muscle fiber 1231, that plays an important role in muscle regeneration as a source of myoblastic cells E5, 61. When cross sections of normal muscle were examined by electron micros- copy, the proportion of satellite cell nuclei in the total number of nuclei within the basal laminae of the mus- cle fibers (the satellite nuclei plus myonuclei) was found to be 4.4 t 1.8% in middle-aged adults 1361 and 8.2 k 1.8% in infants less than 3 years of age 1341. They are present at high frequency in diseased muscles, especially in those diseases with an active re- generative process, such as DMD [42}, and with histo- logical characteristics of muscle fiber immaturity, includ- ing Werdnig-Hoffmann disease [4 11 and congenital nonprogressive m yoparhy 1 341. Therefore, a normal incidence of satellite cells in DMRV reflects a paucity of muscle regeneration. In contrast, the markedly in- creased number of satellite cells with occasional elec- tron microscopic features of “activation” in DisMD strongly suggests the presence of active fiber regenera- tion.
Because the disease in the present patients differs from the Swedish form in the clinical and pathological findings, we conclude that there are at least two addi- tional distinct forms of distal myopathy, autosomal re- cessive DisMD and DMRV, that can be recognized in the wide spectrum of distal myopathies.
The authors thank Dr Paul Neumann (Department of Neuropathol- ogy, Albert Einstein College of Medicine) for his suggestions and advice.
References 1. Barrows HM, Duemler LP: Late distal myopathy: report of a
2. Bautista J, Rafel E, Castilla JM, Alberca R: Hereditary distal case. Neurology (Minneap) 12:547-550, 1962
myopathy with onset in early infancy: observation of a family. J Neurol Sci 37:149-158, 1978
3. Bodensteiner JB, Engel AG: Intracellular calcium accumulation in Duchenne dystrophy and other myopathies: a study of 567,000 muscle fibers in 114 biopsies. Neurology (Minneap) 28:439-446, 1978
4. Bradley WG, Fulthorpe JJ: Studies of sarcolemmal integrity in myopathic muscle. Neurology (Minneap) 28:670-677, 1978
5. Carlson BM: The regeneration of skeletal muscle: a review. Am J Anat 137:119-150, 1973
6. Chou SM, Nonaka I: Satellite cells and muscle regeneration in diseased human skeletal muscles. J Neurol Sci 34:131-145, 1977
7. Dahlgaard E: Myopathia distalis tarda hereditaria (distal late he- reditary myopathy). Acta Psychiatr Neurol Scand 35:440-447, 1960
8. DeVisser M: Computed tomographic findings of the skeletal musculature in sporadic distal myopathy with early adult onset. J Neurol Sci 59:331-339, 1983
9. Dubowitz V, Brooke MH: Muscle Biopsy: A Modern Ap- proach. London, Philadelphia, Toronto, Saunders, 1973
10. Edstrom L Histochemical and histopathological changes in skel- etal muscle in late-onset hereditary distal myopathy (Welander). J Neurol Sci 26:147-157, 1975
11. Fukuhara N , Kumamoto T, Tsubaki T: Rimmed vacuoles. Acta Neuropathol (Berl) 5 1:229-235, 1980
12. Heyck H , Liiders CJ, Wolrer M: Uber eine kongenitale distale Muskeldystrophie mit benigner Progredienz. Nervenarzt 39:549-552, 1968
13. Ideta T, Shikai T, Uchino M, et al: Distal myopathy: report of fourcasesintwofamilies. ClinNeurol(Tokyo) 13:579-586,1973
14. Kira J, Fujii N, Ishimoto S, et al: Distal myopathy with promi- nent vacuolar change in muscle: clinicopathological study of 6 cases. Clin Neurol (Tokyo) 22:594-601, 1982
15. Kratz R, Brooke MH: Distal myopathy. In Vinken PJ, Bruyn GW (eds): Handbook of Clinical Neurology, Vol 40. Amster- dam, ElsevierlNorth Holland Biomed, 1979, pp 47 1-483
16. Kuhn E, Schrijder JM: A new type of distal myopathy in two brothers. J Neurol 226:181-185, 1981
17. Kumamoto T, Fukuhara N , Nagashima M, et al: Distal my- opathy: histochemical and ultrastructural studies. Arch Neurol 39:367-371, 1982
18. Lapresle J, Fardeau M, Godet-Guillain MJ: Myopathie distale et congenitale, avec hypertrophie des mollets. J Neurol Sci 1737- 102, 1972
19. Magee KR, DeJong RN: Hereditary distal myopathy with onset in infancy. Arch Neurol 13:387-390, 1965
20. Markesbery WR, Griggs RC, Herr B: Distal myopathy: electron microscopic and histochemical studies. Neurology (Minneap) 27:727-735, 1977
21. Markesbery WR, Griggs RC, Leach RP, Lapham LW: Late onset hereditary distal myopathy. Neurology (Minneap) 23: 127- 134, 1974
22. Matsubara S, Tanabe H: Hereditary distal myopathy with filamentous inclusions. Acra Neurol Scand 65:363-368, 1982
23. Mauro A: Satellite cell of skeletal muscle fibers. J Biophys Biochem Cytol 9493-495, 1961
24. Miller RG, Blank NK, Layzer RB: Sporadic distal myopathy with early adult onset. Ann Neurol 5:220-227, 1979
25. Miyoshi K, Iwasa M, Kawai H: Autosomal recessive distal mus- cular dystrophy: a new genetico-clinical entity of progressive muscular dystrophy. In Ebashi S (ed): Muscular Dystrophy. To- kyo, University of Tokyo, 1982, pp 471-483
26. Miyoshi K, Iwasa M, Kawai H, et al: Autosomal recessive distal muscular dystrophy. Nippon Rinsho 35:3922--3928, 1977
27. Miyoshi K, Tada Y, Iwasa M, et al: Geneticoclinical features of distal myopathy: results with 14 of our own cases from 7
58 Annals of Neurology Vol 17 No 1 January 1985

pedigrees and other cases from Japanese literame. Clin Neurol (Tokyo) 14:963, 1974
28. Miyoshi S, Santa T, Ohta M, Araki S: A case report of sporadic distal myopathy, with special reference to vacuolar degeneration and rod-like body in muscle fibers. Clin Neurol (Tokyo)
29. Mitusawa H, Nakano I, Inoue K, et al: Distal myopathy: a variety characterized by prominent vacuolar degeneration of muscle. Neurol Med (Tokyo) 12:40-47, 1980
30. Mokri B, Engel AG: Duchenne dystrophy: electron micro- scopic findings pointing to a basic or early abnormality in the plasma membrane of the muscle fiber. Neurology (Minneap)
3 1. Murone I, Sat0 T, Shirakawa K, et al: Distal myopathy: a case of nonhereditary distal myopathy. Clin Neurol (Tokyo) 3:387- 393, 1963
32. Nonaka I, Sunohara N, Ishiura S, Satoyoshi E: Familial distal myopathy with rimmed vacuole and lamellar (myeloid) body formation. J Neurol Sci 51:141-155, 1981
33. Nonaka 1, Takagi A, Sugita H: The significance of type 2C muscle fibers in Duchenne muscular dystrophy. Muscle Nerve 4:326-333, 1981
34. Nonaka I, Tojo M, Sugita H: Fetal muscle charactetistics in nemaline myopathy. Neuropediatrics 14:47-52, 1983
10:lll-120, 1970
25:1111-1120, 1975
35. Sasaki K, Mori H, Takahashi K, Nakamura H: Distal rny- opathy: report of four cases. Clin Neurol (Tokyo) 9627-637, 1969
36. Schmalbruch H, Hallhammer U: The number of satellite cells in normal human muscle. Anat Rec 185:279-288, 1976
37. Sumner D, Crawfurd M, Harriman D G F Distal muscular dys- trophy in an English family. Brain 94:51-60, 1971
38. Toyokura Y, Kurisaki H, Takatsu M: Muscle pathology of distal myopathy. In Miyoshi K (ed): Current Research in Muscular Dystrophy. Japan. Tokyo, The Ministry of Health and Welfare (Japan), 1981, pp 42-43
39. Vaccario ML, Scopetta C, Bracaglia R, Uncini A: Sporadic distal myopathy. J Neurol224:291-295, 1981
40. Van der Does de Willebois AEM, Bethlem J, Meyer AEFH, Simons AJR: Distal rnyopathy with onset in early infancy. Neu- rology (Minneap) 18:383-390, 1968
41. Van Haelst U: An electron microscopic study of muscle in Werdnig-Hoffmann disease. Virchows Arch Pathol Anat
42. Wakayama Y, Schotland D L Muscle satellite cell populations in Duchenne muscular dystrophy. In Mauro A (ed): Muscle Re- generation. New York, Raven, 1979, pp 121-129
43. Welander L: Myopathia distalis tarda hereditaria. Acta Med
3511291-305, 1970
Scad 14l (s~ppl 265):l-24, 1951
Nonaka et al: Autosomal Recessive Distal MD 59