Embed Size (px)
Citation preview

American Journal of Medical Genetics 57:479-482 (1995)
Autosomal-Recessive Inheritance of Benign Recurrent Intrahepatic Cholestasis
Tom J. De Koning, Lodewijk A. Sandkuijl, Jan E.A.R. De Schryver, Eric A.M. Hennekam, Frits A. Beemer, and Roderick H.J. Houwen Department of Pediatric Gastroenterology, Wilhelmina Children’s Hospital (T.J.D.K., J.E.A.R.D.S., R.H.J.H.), Clinical Genetics Center (E.A.M.H., F.A.B.), Utrecht, and Institute of Clinical Genetics, Erasmus University (L.A.S.), Rotterdam, The Netherlands
Benign recurrent intrahepatic cholestasis (BRIC) is a rare disorder characterized by recurrent episodes of cholestasis without permanent liver damage. Familial and spo- radic cases have been described. Based on existing evidence, both autosomal-recessive and autosomal-dominant inheritance have been considered. We describe a large Dutch pedigree with 4 patients, strongly suggest- ing autosomal-recessive inheritance. 0 1995 Wiley-Liss, Inc.
KEY WORDS: benign recurrent intrahe- patic cholestasis, BRIC, auto- somal-recessive inheritance
INTRODUCTION Benign recurrent intrahepatic cholestasis (BRIC)
was first described by Summerskill and Walshe [1959]. This disease is characterized by multiple episodes of cholestasis without extrahepatic bile duct obstruction. At the onset of symptoms, serum bile acids are elevated and patients complain of severe pruritus and anorexia [Van Berge Henegouwen et al., 1974; Summerfield et al., 1981; Bijleveld et al., 1989al. This prodromal phase is generally followed by cholestatic jaundice. The attacks of jaundice can vary in duration from several weeks to months and resolve spontaneously. During an- icteric periods no biochemical abnormalities can be found in patients. The factors responsible for initiating jaundice attacks are unknown, but altered bile metab- olism may play a role [Bijleveld et a]., 1989bl. The dis- ease is benign in nature, without progression to chronic liver dysfunction [Putterman et al., 1987; Bijleveld et al., 1989al.
Received for publication June 13, 1994; revision received November 28, 1994.
Address reprint requests to Dr. R.H.J. Houwen, Department of Pediatric Gastroenterology, Wilhelmina Children’s Hospital, Postbox 18009,3501 CA Utrecht, The Netherlands.
0 1995 Wiley-Liss, Inc.
Familial cases were first described by Tygstrup [1960] and by Kuhn [1962]. In these and subsequent re- ports a total of 16 families with sibs affected by BRIC have been described [Kuhn, 1962; Da Silva and De Brito, 1966; Goldberg and Hendry, 1967; Rotthauwe et al., 1969; Rotthauwe and Rotthauwe, 1971; Lovisetto et al., 1990; Leiber et al., 1979; Minuk and Shaffer, 1987; Everson et al., 1989; Lau et al., 1989; Brenard et al., 1989; Bijleveld et al., 1989al. In addition, 2 affected males were reported where the great grandfathers were brothers [Tygstrup and Jensen, 19691, a family with affected first cousins [Biempica et al., 19671, and a family with 2 sets of sibs with BRIC in a large pedigree [De Pagter et al., 19761. Another family has been de- scribed with mother to son and daughter transmission [Lesser, 19731. Based on this information BRIC could be either an autosomal-recessive disease, or an auto- somal-dominant disorder with variable penetrance [Brenard et al., 19891.
Here we describe a large Dutch pedigree from an en- dogamous community with 4 BRIC patients, support- ing autosomal-recessive inheritance for this disease.
CLINICAL REPORTS Patient VII-1 (Fig. 1) is a girl born after an unevent-
ful pregnancy and delivery with a birth weight of 3,350 g. When she was 3 months old she started scratch- ing and subsequently became icteric. At physical exam- ination the liver was 3 cm below the costal margin. Laboratory studies showed a total serum bilirubin of 205 pmoM and a conjugated bilirubin of 130 pmol/l. The aspartate aminotransferase (ASAT) was 56 UA and the alanine aminotransferase (ALAT) was 25 UA. Needle biopsy of the liver showed no gross abnormalities. The cholestatic jaundice disappeared clinically and bio- chemically when the patient was 1 year old. Another attack started a t age 3 years. This time there was no hepatomegaly. Serum bile acids were 537 pmol/l, total serum bilirubin 475 pmol/l, conjugated bilirubin 403 pmol/l, ASAT 44 UA, and ALAT 36 UA. After 9 months the jaundice resolved, with concomitant nor- malization of the hyperbilirubinemia and the elevated bile acids. She is now 6 years old and well.

480 De Koning et al.
I
II
111
IV
V
VI
VII
8
\ # \ #
3 4 5 10
I \ # \ # \ #
,,1 *2 -3 6 12
\ # \ #
1 3
1 3
I I
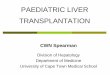
Fig. 1. Family pedigree. Affected individuals all presented before age 1 year.
Patient VII-4 was born after a normal gestation with a weight of 3,820 g. At age 2 months he started scratch- ing. Subsequently he developed jaundice. At physical examination he was icteric and had hepatomegaly with the liver 3 cm below the costal margin. Total serum bilirubin was 237 pmol/l, conjugated bilirubin 148 ,umol/l, serum bile acids 181 pmol/l, ALAT 20 U/L, and ASAT 34 U/L. A liver biopsy showed normal hepatic histology with bile plugs. The jaundice disappeared spontaneously. At age 13 months a second episode of jaundice started, which lasted for 2 months. At age 19 months he started scratching again and subsequently became icteric. This third episode lasted 6 months. At age 3 years he started scratching again. At that time bile acids were 605 pmol/l and total bilirubin 15 pmol/l. One month later icterus developed. At that time total bilirubin was 200 pmol/l and conjugated bilirubin 182 pmol/l. This attack lasted for 6 months. Two years later a short episode with scratching and high serum bile acids, but no visible icterus, occurred. A further cholestatic episode started a t age 6 years and is still continuing at the moment of writing.
Patient VII-5 is the younger sister of patient VII-4. She was born after an uneventful pregnancy and deliv- ery. At age 8 months the child started scratching. Two weeks later icterus developed. At that time serum bile acids were 324 pmol/l, total bilirubin 131 pmol/l, and conjugated bilirubin 114 pmoM, while transaminases were normal. Two months after the beginning of the attack she stopped itching and the serum bilirubin and bile acid levels became normal again. The patient is now 26 months old and no subsequent attacks have occurred.
Patient VII-6 was born at 40 weeks with a weight of 3,240 g after an uncomplicated pregnancy. At age 7 months he started scratching and shortly afterwards he became icteric. Physical examination showed jaun- dice, hepatomegaly, and multiple skin lesions due to scratching. Total serum bilirubin was 279 pmoV1, and conjugated bilirubin 213 pmolll, with normal transam- inases. A needle biopsy of the liver showed normal ar- chitecture with bile plugs. The cholestasis resolved spontaneously. When he was 11/2 years old a second at- tack started, beginning with a few days of pruritus, fol- lowed by visible jaundice. Laboratory investigations 4 weeks later showed a total bilirubin of 559 ,umol/l, conjugated bilirubin of 470 pmol/l, and a serum bile acid level of 180 pmol/l, with normal transaminases. Subsequently the bilirubin normalized, but bile acids remained elevated for 6 more months. The patient is now 3 years old and free of complaints.
GENEALOGICAL INVESTIGATIONS The family described here originated from a small
village, founded in the Middle Ages. The population of this community was fairly stable a t 1,000 inhabitants for many centuries. However, during the second half of the 19th century and the beginning of the 20th, popu- lation more than quadrupled, mainly under the influ- ence of the growing fishing industry. During this period the city was fairly isolated, with little immigration from outside. More than 90% of marriages were be- tween individuals already living in this community for some time [Putman and Burgman-Feenstra, 19831. The

Inheritance of BRIC 481
No effective treatment for BRIC exists so far. Treat- ment of cholestasis is symptomatic with cholestyra- mine. Ursodeoxycholic acid has been used to prevent cholestatic episodes, but not with conclusive results [Bircher, 1989; Bijleveld et al., 1989c; Crosignani et al., 19911. In every long-standing attack, supportive treat- ment with fat-soluble vitamins should be given. In ad- dition, patients should have an adequate caloric intake.
Most cases of BRIC reported in the literature are spo- radic. About one third of the cases have sibs or distant relatives with the disease [Brenard et al., 19891. Auto- somal-recessive inheritance has been suggested based on the occurrence of the disease in sib pairs and cousins. In addition, several patients with BRIC were described from small isolated communities [Tygstrup and Jensen, 1969; Biempica et al., 19671. However, in 1 family, transmission from a n affected mother to both her son and daughter was reported [Lesser, 19731, sug- gesting autosomal-dominant inheritance, but still com- patible with autosomal-recessive inheritance. The in- heritance of BRIC in the family described by De Pagter et al. [1976] is both consistent with autosomal- dominant inheritance with variable penetrance, and with autosomal-recessive inheritance with a high gene frequency in an endogamous community.
We have described a large Dutch family with BRIC in which transmission is most likely autosomal-recessive. Review of all other familial cases of BRIC in the liter- ature is also consistent with autosomal-recessive in- heritance. Although it cannot be excluded that the transmission of BRIC in some families is due to other mechanisms, such as autosomal-dominant inheritance with variable penetrance, the observed transmission patterns in our family and in others makes it very likely that BRIC is an autosomal-recessive disease in the vast majority of patients.
The large family described here has also been used for the assignment of the BRIC gene to chromosome 18, thereby paving the way for the ultimate isolation of the gene by positional cloning [Houwen et al., 19941.
REFERENCES Arias IM, Che M, Gatmaitan 2, Leveille C, Nishida T, St. Pierre M
(1993): The biology of the bile canaliculus. Hepatology 17:318-329. Beaudoin M, Feldmann G, Erlinger S, Benhamou J P (1973): Benign
recurrent cholestasis. Digestion 9:4945. Biempica L, Gutstein S, Arias IM (1967): Morphological and biochem-
ical studies of benign recurrent cholestasis. Gastroenterology
Bijleveld CMA, Vonk RJ, Kuipers F, Havinga R, Fernandes J (1989a): Benign recurrent intrahepatic cholestasis: a long-term follow-up study of two patients. Hepatology 9532-537.
Bijleveld CMA, Vonk RJ, Kuipers F, Havinga R, Boverhof R, Koopman BJ, Wolthers BG, Fernandes J (198913): Benign recurrent intra- hepatic cholestasis: altered bile acid metabolism. Gastroenterology 97:427-432.
Bijleveld CMA, Vonk RJ, Kuipers F (1989~): Treatment of patients with benign recurrent intrahepatic cholestasis (reply). Hepatology 10:1031-1032.
Bircher J (1989): Treatment of patients with benign recurrent intra- hepatic cholestasis (letter to the editor). Hepatology 10:1030.
Brenard R, Geubel AF', Benhamou JP (1989): Benign recurrent intra- hepatic cholestasis: a report of 26 cases. J Clin Gastroenterol 11: 546-5151,
52:521-535.
ancestors of the BRIC patients lived in this city before and during this period of rapid population expansion.
Population growth continued during the last part of this century, the number of inhabitants now exceeding 20,000. The isolation, characteristic of this city in for- mer years, has diminished and people from other parts of the country have settled in this city. A rough esti- mate is that a t present 50% of the inhabitants are des- cendants from families already living in the city before the turn of the century. Among the descendants of this original population, presently estimated at approxi- mately 10,000 individuals, 4 patients were identified, which means that in this population the carrier fre- quency is quite high.
Genealogcal investigation showed that all BRIC patients were born to consanguineous relationships (Fig. 1). A large number of relationships between the 6 parents of the patients could be established, mostly via ancestors 5 generations ago. However, it was not possi- ble to identify a single common ancestor, responsible for introduction of the BRIC gene into this family. Since family connections between patients always included at least 1 unaffected male, X-linked inheritance could be excluded. None of the presumed carriers for the BRIC gene had experienced the characteristic signs of the disease. Therefore it is highly likely that BRIC has an autosomal-recessive inheritance.
DISCUSS I 0 N After the original description of BRIC by Summer-
skill and Walshe [ 19591, more than 100 cases have been published. The classical clinical picture consists of a prodromal phase with malaise, anorexia, and pruritus, which is usually most problematic a t night [Beaudoin et al., 19731. During this period there is a strong eleva- tion of serum bile acids, which is generally followed by cholestatic jaundice. The episodes vary considerably in length and frequency among patients. The symptoms can last from 2 weeks to 2 years and no prediction can be made as to their disappearance. Upper and lower respiratory tract infections and acute gastroenteritis are sometimes associated with the onset of symptoms [Bijleveld et al., 1989aI. The first episode of cholestasis in a patient can occur a t any age between the first year of life and adulthood. Not every prodromal phase of pruritus and malaise in a patient is followed by jaun- dice, as is clear from the fifth attack in case VII-4. Sim- ilarly, not every episode ofjaundice is preceded by a rec- ognizable prodromal phase. The disorder is benign in nature and there is no progression to chronic liver dys- function [Putterman et al., 19871.
The pathogenesis of bile acid accumulation and cholestasis is not clear. The basic defect could reside in the still-enigmatic canalicular bile acid transporter [Arias et al., 19931, resulting in the altered bile acid me- tabolism that has been observed in patients with BRIC [Bijleveld et al., 1989bl. Interestingly, biochemical dif- ferences in the uptake of the organic anion indocyanine green among BRIC patients have been described [Van Berge Henegouwen et al., 19781, suggesting genetic heterogeneity for BRIC, which could be either allelic, or due to the existence of more than one gene for BRIC.

482 De Koning et al.
Crosignani A, Podda M, Bertolini E, Battezzati PM, Zuin M, Setchell KDR (1991): Failure of ursodeoxycholic acid to prevent a cholestatic episode in a patient with benign recurrent intrahepatic cholestasis: a study of bile acid metabolism. Hepatology 13:10761083.
Da Silva LC, De Brito T (1966): Benign recurrent intrahepatic cholestasis in two brothers: a clinical, light, and electron mi- croscopy study. Ann Intern Med 65:330-341.
De Pagter AGF, Van Berge Henegouwen GP, Ten Bokkel Huinink JA, Brandt KH (1976): Familial benign recurrent intrahepatic cholestasis: interrelation with intrahepatic cholestasis of preg- nancy and from oral contraceptives? Gastroenterology 71:202-207.
Everson GT, Ahnen D, Harper PC, Krawitt EL (1989): Benign recur- rent intrahepatic cholestasis: treatment with s-adenosylmethio- nine. Gastroenterology 96:1354-1357.
Goldberg DM, Hendry EB (1967): Familial form of benign idiopathic recurrent cholestasis. Arch Intern Med 120:556-564.
Houwen RHJ, Baharloo S, Blankenship K, Raeymakers P, Juyn J , Sandkuijl LA, Freimer NB (1994): Genome screening by searching for shared segments: mapping of a gene for benign recurrent in- trahepatic cholestasis. Nat Genet 8:380-386.
Kiihn HA (1962): Ikterus durch intrahepatische Cholestase bei Briidern. Acta Hepato-Splen 9:229-245.
Lau JYN, Lok ASF, Lai CL, Wu PC, Lin H J (1989): Benign recurrent intrahepatic cholestasis in a Chinese girl. J Gastroenterol Hepatol 4581-583.
Leiber DU, Lagenstein I, Griittner R (1979): Benigne rezidivierende familiare intrahepatische Cholestase bei eineiigen Zwillingen. Monatsschr Kinderheilkd 127:48-51.
Lesser PB (1973): Benign familial recurrent intrahepatic cholestasis. Dig Dis 18:259-264.
Lovisetto P, Raviolo P, Rizetto M, Marchi L, Actis GC, Verme G (1990): Benign recurrent intrahepatic cholestasis. A clinico-pathologic study. Res Clin Lab 20:19-27.
Minuk GY, Shaffer EA (1987): Benign recurrent intrahepatic cholestasis: evidence for an intrinsic abnormality in hepatocyte secretion. Gastroenterology 93:1187-1193.
Putman JHM, Burgman-Feenstra HA (1983): “Van wee bin jie d’r Ben.” Bunschoten-Spakenburg: De Bunschoter BV, pp 24-36.
Putterman C, Keidar S, Brook JG (1987): Benign recurrent intrahep- atic cholestasis: 25 years follow-up. Postgrad Med J 63:295-296.
Rotthauwe HW, Rotthauwe I (1971): Familiare rekurrierende intra- hepatische Cholestase seit dem fruhen Kindesalter. Z Kinderheilkd 110:292-316.
Rotthauwe HW, Beseler WD, Kowalewski S (1969): Benigne rekurri- erende intrahepatische Cholestase. Klin Wochenschr 47: 140-149.
Summerfield JA, Kirk AP, Chitranukroh A, Billing BH (1981): A dis- tinctive pattern of serum bile acid and bilirubin concentrations in benign recurrent intrahepatic cholestasis. Hepatogastroenterol- ogy 28:139-142.
Summerskill WHJ, Walshe JM (1959): Benign recurrent intrahepatic obstructive jaundice. Lancet II:686-690.
Tygstrup N (1960): Intermittent possibly intrahepatic cholestatic jaundice. Lancet I: 1171-1172.
Tygstrup N, Jensen B (1969): Intermittent intrahepatic cholestasis of unknown etiology in five young males from the Faroe Islands. Acta Med Scand 185523-530.
Van Berge Henegouwen GP, Brandt KH, De Pagter AGF (1974): Is an acute disturbance in hepatic transport of bile-acids the primary cause of cholestasis in benign recurrent intrahepatic cholestasis? Lancet I:1249-1251.
Van Berge Henegouwen GP, Ferguson DR, Hofmann AF, De Pagter AGF (1978): Familial and nonfamilial benign recurrent cholestasis distinguished by plasma disappearance of indocyanine green but not cholylglycine. Gut 19:345-349.