Embed Size (px)
Citation preview

Sharma Mona et al / IJRAP 2011, 2 (1) 126-131
International Journal of Research in Ayurveda & Pharmacy, 2(1), Jan-Feb 2011 126-131
Review Article Available online through www.ijrap.net ISSN 2229-3566
NEW DRUG REGIMENS FOR OLD DISEASE TUBERCULOSIS: A REVIEW Gupta Sandeep, Sharma Mona*, Gupta Mahesh Kumar, Nagla Kapil, Gupta Raman
Kota College of Pharmacy, Sp-1, Riico Industrial Area, Ranpur, Kota, Rajasthan, India
Received on: 19/12/2010 Revised on: 21/01/2011 Accepted on: 30/01/2011
ABSTRACT Today ‘Tuberculosis (TB) is acknowledged as a global health threat. As resistant strains of Mycobacterium tuberculosis have emerged slowly and due to lack and treatment failure many countries have to adapt long term and costly treatment for the patients. Due to TB 1.8 million people die every year and 5000 every day. By this data we can analyze that there is an urgent need to improve its treatment by enhancing the activity of existing agents and introducing new agents. The new regimens should have better drug tolerability profile and longer duration of action and great patient acceptability. The new agents should be more effective against MDR/XDR TB and in HIV co infected patients and active against latent TB. This review presents the drug currently used and also the advanced drug undergoing clinical trials for the treatment of tuberculosis. A short description on their mechanism of action and inhibitors acting on related biochemical targets is also provided. The focus of this review is to consider the challenges in the development of new anti TB drugs and provide an up- to-date evaluation of current therapy status and progress of the developing new agents in the phase of clinical testing as one of the strategies for the improvement of TB treatment. KEY WORDS: Tuberculosis, new regimens, current drug. *Corresponding Author Mona Sharma, Student, M.Pharm. I year, Department of Pharmaceutical Chemistry, Kota College of Pharmacy, Kota, Rajasthan, India E-mail: [email protected] INTRODUCTION Given the global scale of tuberculosis as a major public health problem, research activity has been maintained in the area of TB drug development, despite inadequate funding and some preclinical successes have been reported. Tuberculosis is a common and often deadly infection caused mainly by strains of Mycobacterium tuberculosis, a slow growing pathogen with unusual propensity to shut down its metabolism in the face of adverse condition, such as starvation or immune stress, and to enter a persistent, or latent, phase in which it displays phenotypic resistance to some antibiotics1. The present review offers a critical overview of the current anti-TB drugs arsenal and of the contemporary trends in the development of new tuberculostatics capable to overcome the bacterial resistance, especially of new agents being in progress in the phase of clinical testing. Need of new drug regimen There are several major problems associated with currently available treatment of TB they are:
The duration and complexity often resulting in nonadherence and leading to emergence of resistance and continuous spread of the disease. Adverse events in response to anti tubercular drugs. Some drugs for drug-resistant TB are not available everywhere and are less effective, more toxic, and have longer use. Co-infection of TB and HIV, where their combined treatment involves a high pill count with associated adherence problems, overlapping toxicity profiles, drug interactions and risk of immune reconstitution syndrome. Prophylactic therapy of latent TB is also associated with problems. Due to above problems WHO developed a Directly Observed Therapy Short (DOTS) course, but due to its expensiveness and labor intensity it became a burden on public health programs running in developing countries2. Drug regimens used currently The currently applied drugs for treatment of TB include broad spectrum, narrow spectrum and different drug
Sharma Mona et al / IJRAP 2011, 2 (1) 126-131
International Journal of Research in Ayurveda & Pharmacy, 2(1), Jan-Feb 2011 126-131
combinations, which target different types of TB. They are categorized under two heads3:
1. First line drugs 2. Second line drug
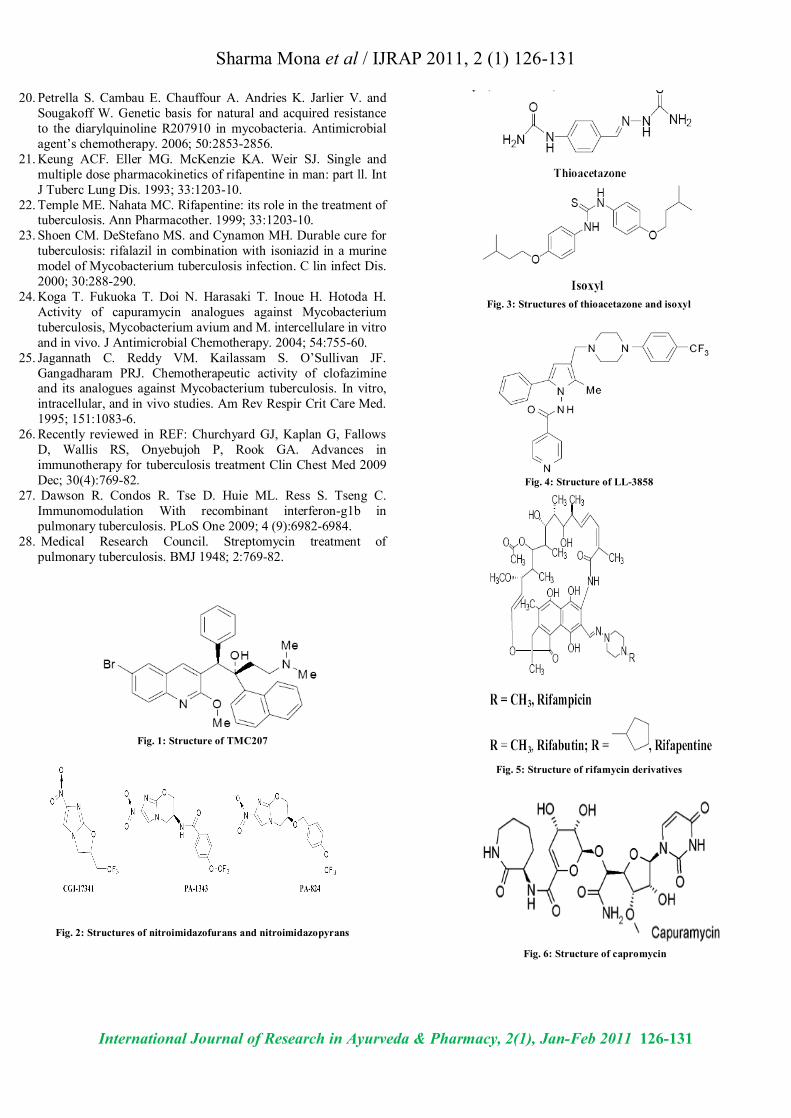
FIRST LINE DRUGS Streptomycin was the first antibiotic used to treat TB. Ii is an aminoglycoside antibiotic, the other agents of this category are: kanamycins, gentamycins tobramycin, dibecacin, sisomycin, netilmycin, pentisomycin. Other effective drugs were searched and are: erythromycin, clarithromycin, and rifampicin which were used in combination with isoniazid and ethambutol Isoniazid: It is a sulphonamide and act as a prodrug for TB. It acts by inhibition of mycolic acid biosynthesis by affecting enzyme mycolate synthetase in the bacilli. Ethambutol: it is a synthetic amino alcohol and act by inhibiting mycolate and glucose synthesis. Pyrazinamide: it is an analog of nicotinamide and active against semi dormant bacillus. And thought to act by sterilizing effect. SECOND LINE DRUGS The second line drugs used in the treatment of TB are: p-amino salicylic acid, ethionamide, protionamide, and cycloserine. p- Amino salicylic acid: its antibacterial activity was reported in 1946. But rarely used now in the treatment of TB. The hydrazide of PAS exhibit good activity. Ethionamide and Protionamide: these are two homologous compounds used as tuberculostatics due to their different mode of action. They are active against M. tuberculosis, M. bovis, M. smegmatis, and M. avium. Cycloserine: D-cycloserine is a structural analogue of D-alanine, it inhibit M. tuberculosis. Its major side effect CNS toxicity and also causes psychotic states with suicidal tendencies4. NEW REGIMENS UNDER DEVELOPMENT A number of new anti-TB drugs are in the stage of development with new mechanism of action that overcome the resistance caused by first line drugs and exhibit excellent activity against M. tuberculosis and reduce duration and dosing of the treatment. Diarylquinolines TMC207 It is a new anti TB agent with unique spectrum and specificity to mycobacteria. They are currently in phase2a clinical trials5. Nitroimidazofurans and Nitroimidazopyrans These posses in-vivo activity against TB. But due to mutagenic side effects it is not used clinically. The compounds are: PA-824, PA 1343, and OPC-67683.
They act by inhibiting replicating and latent phase of bacillus6, 7. Thiocarlide Thioacetazone and isoxyl. These are diacyl thioureas and act by inhibiting mycolic acid biosynthesis. Isoxyl is useful than toxic thioacetazone8,9. Tryptanthrin It is a novel potent indolo-quinazolinone alkaloid active against MDR-TB. But in-vivo data and in-vitro toxicity are needed before this structural prototype is applied10, 11. Oxazolidinones These are orally active synthetic antibacterial. Thiomorpholine analogue of U-100480 showing potent in-vitro activity against M. tuberculosis. Linezolid It is an oxazolidinone and act by inhibiting ribosomal protein synthesis by interfering with initiation complex formation. It is used in the treatment of MDR-TB and does not have any cross resistance with existing anti-TB agents12. Fluoroquinolones Novel fluoroquinolones have been considered of special interest for treating TB as they are far effective13. They are also preferred as they have minimum side effects and no cross-resistance. So they provide a better choice in the treatment of serious infections and mainly MDR-TB14. The new fluoroquinolones are: Moxifloxacin The in-vitro study of moxifloxacin shows to kill sub population of tubercle bacteria which was not shown by previous fluroquinolones and rifampicin. It is highly effective due to inhibition of effluxes out of bacteria and causing higher concentrations resulting in improved activity15. Gatifloxacin Gatifloxacin had showed greater activity than moxifloxacin but have a cross-resistance with it. Its clinical indications are found to be effective and have similar activity as moxifloxacin and isoniazid16. Gamifloxacin It is a drug which has shown activity in phase 3 trials but used for respiratory infections. Its in-vitro activity shows that at very high non-toxic dose also it not effective in treatment of TB17. Sitafloxacin It is in phase 3 trials and has outstanding activity and is highly effective than other fluroquinolones. It inhibits both DNA gyrase and topoisomerase 4 and its IC50 against these enzymes were lowest among the fluoroquinolones18.
Sharma Mona et al / IJRAP 2011, 2 (1) 126-131
International Journal of Research in Ayurveda & Pharmacy, 2(1), Jan-Feb 2011 126-131
Phenothiazines Phenothiazines are active against variety of bacteria, mycobacteria, viruses and protozoa. Chlorpromazine and thioridazine are the drugs having activity against mycobacteria of TB. These are methylene blue derivatives which render bacteria immobile. Its anti-TB activity is due to presence of calmodulin protein in bacteria. These act synergistically with other antimicrobial agents19. Pyrrole: LL-3858 It is a pyrrole derivative which showed antimycobacterial activity in preclinical studies. Its activity has showed good results in mice and dog and found to be well absorbed and showed better activity then isoniazid20. Information related to molecular mechanism is currently in phase 1 trials. Nitroimidazoles M. tubercle is an obligate aerobe which is capable of long-term persistence under conditions of low oxygen tension. Metronidazole is a drug which showed activity against dormant tubercle. It undergoes reduction at low redox potential in susceptible micro-organism to form nitro group which damages DNA and causes cell death. Shows synergistic activity in combination with first line drugs21. ATP Synthase Inhibitor FAS20013 (FASgene) It is a novel coumpound of sulphonylcarboxamides class. The coumpound is effective against mycobacterium and act by inhibiting ATP synthase. It is mainly effective in MDR-TB and superior to sterilize TB lesions and kill latent TB compared to other drugs22. It is 100% bioavailable on oral administration and no dose toxicity even on administration of 10 times the effective dose. InhA Inhibitors Isoniazid is first line drug in TB treatment it requires activation in which inheritant protective enzyme of mycobacteria-Kat G plays major role. InhA, the enoyl reductase enzyme from Mycobacterium tuberculosis, catalysis the last step in fatty acid biosynthesis pathway23. The main purpose is to bypass the activation step and directly inhibit InhA. Novel rifamycin derivatives Rifabutin It is 4 to 8 times more active than rifampin and favourable feature is it has good tissue penetration. Prime reason for it is that it can be co-administered with antiretroviral treatment. it is used in multi drug treatment with other drugs.
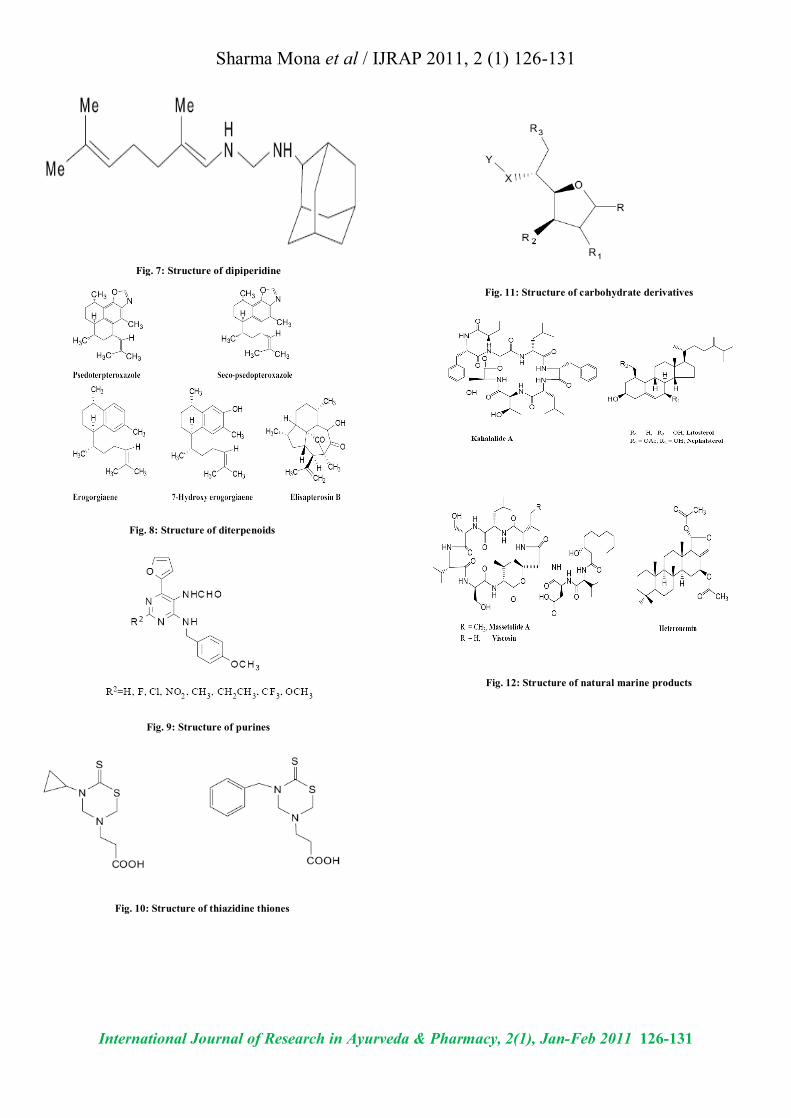
Rifapentine It is 2 to 4 times more active and has better pharmokinetic profile than RIF. It has longer duration of action and high serum peak levels which extend the dosing intervals in patients. Its adverse effects are very less and can be administered with indinavir24. Rifametane It is a novel semi-synthetic rifamycin having same spectrum and potency but with better pharmokinetic profile25. Rifalazil It is a new semi synthetic rifamycin, characterized by long half life and more active than rifampicin and rifabutin both in-vivo and in-vitro. Due to severe side effects its development have beenterminated26. Capuramycin analogs They posses antimycobacterial activity both in-vivo and in-vitro by inhibition of enzyme phospho-MurNAc-pentapeptide translocase and inturn inhibit the peptidoglycan assembly. Drugs are: RS-118641, RS-112997, and RS124922.They are used for MDR-TB treatment27. Pleuromutilins They inhibit the growth of bacteria and act by interfering with protein synthesis by binding to 23S r RNA and result in inhibition of peptide bond formation. It represents novel class of antibiotic and effective in MDR-TB28. Dipiperidine SQ-609 It is a novel coumpound and act by interfering with cell wall biosynthesis. The activity is shown in-vivo in mouse but is less effective than Isoniazid . Diterpenoids These are the compounds which are isolated from natural sources. They have been recently screened for anti-tuberculosis activity as it has many other activities also. It was found that benzooxazole is not necessary for the activity. Purines Substitutions at various positions of 9-benzyl purines like 2-,6- and 8- have shown high inhibitory activity against M. tuberculosis. Thiazidine thiones These compounds are derivatives of dithiocarbamic acid and have shown potent activity against M. tuberculosis. One of its compounds has activity in-vitro even in resistant strains of the bacteria. Carbohydrate derivatives These compounds were screened on the basis that sugars have property of inhibiting the enzyme activity
Sharma Mona et al / IJRAP 2011, 2 (1) 126-131
International Journal of Research in Ayurveda & Pharmacy, 2(1), Jan-Feb 2011 126-131
responsible for cell wall biosynthesis. On screening sugars simple monosaccharides showed potent activity against M. tuberculosis strains and used in MDR-TB. Natural Marine Products Cyclic depsipeptides were isolated from pseudomonans, a marine alga and a tune worm. These were tested against M. avium-intracellulare having MIC value 2.5-5 and 5-10 µg/ml respectively of massetolide A, viscosin B. other isolated from Sacoglossan mollusk Elysia rufescens named Kahalalides inhibited bacterial growth at 12 µg/ml. similarly litosterol and nephalsterol is isolated from red sea nephtheasp. Heteronemin sesqueterpine isolated from red sea sponge also show activity against M. tuberculosis. In addition to above classes other drugs classes on which work is continued for anti-tuberculosis activity are compiled as isoxazoles and cynopyridines, aminolupinanes, 1,3,5-tribenzimidazole pyrimidines, pyrazolines, thiosemicarbazones, hydantoins and hydrazones azetidinone, sydnones , pyrazinamine derivatives, hydrazinecarboxamides etc . CONCLUSION The current antitubercular drugs offer treatment which demands continuous administration of drugs for 6 months. Newer drugs are needed to shorten the total duration of treatment and significantly reduce the number of doses need to be taken under DOTS. There are mainly two sources of new chemical entities, the first one is provided from natural product extraction, evaluation, and characterization and second deals with the original compounds made more accessible by design of new synthetic transformations. The new regimens have exceptional safety profiles and avoid the drug-drug interactions presently conforming the TB and HIV therapy. The “road ahead” i.e. the search of new regimens for TB treatment is full of challenges and success depends on the necessary resources and innovative ideas flourishment. Finally, the registration of novel drugs represents the necessary and sufficient conditions of success in improving the treatment of TB patients and impacting the epidemic globally. REFERENCES 1. Pratt RJ. Extensively drug-resistant (XDR) tuberculosis. British
Journal of Infection Control. 2007; 8:20-22. 2. Orme I. Search for new drugs for treatment of Tuberculosis.
Antimicrobial agents and chemotherapy. 2000; 45:1943-1946. 3. Dooley K. Flexner C. Hackman J. Peloquin CA. Nuermberger E.
Chaisson RE. Repeated administration of high-dose intermittent rifapentine reduces rifapentine and moxifloxacin plasma concentrations. Antimicrob Agents Chemotherapy 2008; 52:4037-42.
4. Upshar R. Singhb J. Ford N. Bull World Health Organ. 2009; 87:481-483.
5. Brennan PJ. Young DB. Tuberculosis. 2008; 88:85-170. 6. Lounis NN. Veziris A. Truffot-Pernot CC. Andries K and Jarlier
V. Combinations of R207910 with drugs used to treat multidrug resistance tuberculosis have the potential to shorten treatment duration. Antimicrob. Agents Chemother. 2006; 50:3543-3547.
7. Stover CK. Warrener P. VanDevanter DR. Sherman DR. Arain TM. Langhorne MH. A small molecule nitroimidazopyran drug candidate for treatment of tuberculosis. Nature. 2000; 405:962-966.
8. Iona E. Giannoni F. Pardini M. Brunori L. Orefici G. and Fattorini L. Metronidazole plus rifampin sterilize long-term dormant mycobacterium tuberculosis antimicrobial agents and chemotherapy. Antimicrobial Agents and Chemotherapy. 2007; 51; 1537-1540.
9. I-Nae Park. Sang-Bum Hong. Yeon-Mok Oh. Mi-Na Kim. Efficacy and tolerability of daily–half dose linezolid in patients with interactable MDR-TB. Journal of Antimicrobial chemotherapy. 2006; 50:701.
10. Hu Y. Coates ARM. and Mitchison DA. Sterilizing Activities of Fluoroquinolones against Rifampin-tolerant population of mycobacterium tuberculosis. Antimicrobial agents and chemotherapy. 2003; 47:653-657.
11. Lu T and Drlica K. In vitro activity of C-8-methoxy fluoroquinolones against mycobacteria when combined with anti-tuberculosis agents. Journal of antimicrobial chemotherapy. 2003; 52:1025-1028.
12. Miyazaki E. Miyazaki M. Chen JM. Chaisson RE. and Bishai WR. Moxifloxacin , a new 8-methoxyquinolone, is active in a mouse model of tuberculosis. Antimicrobial agents chemotherapy. 1999; 43:85-89.
13. Daporta MT. Bellido MJL. Guirao GY. Hernandez MS. and Garcia-Rodriguez JA. In vitro activity of older and newer fluoroquinolones against efflux mediated high level ciprofloxacin resistant Streptococcus pneumonia. Int J antimicrob agents. 2004; 24:185-7.
14. Ruiz-Serrano MJ. In vitro activities of six fluoroquinolones against 250 clinical isolates of mycobacterium tuberculosis susceptible or resistant to first-line anti-tuberculosis drugs. Antimicrobial agents chemotherapy. 2000; 44:2567-2568.
15. Milatovic D. In vitro activity of sitafloxacin and six other fluoroquinolones against 8,796 clinical bacterial isolates. Antimicrobial agents chemotherapy. 2000; 44:1102-1107.
16. Amarala L. Kristiansenb JE. Viveirosa M and Atouguiac J. Activity of phenothiazines against antibiotic resistant Mycobacterium tuberculosi: a review supporting further studies that may elucidate the potential use of thioridazine as anti-tuberculosis therapy. Journal of antimicrobial chemotherapy. 2001; 47:505-511.
17. Anheim CA. Abstract n. 63 submitted to the American Chemical Society Meeting. 2004.
18. Iona E. Giannoni F. Pardini M. Brunori L. Orefici G. and Fattorini L. Metronidazole plus rifampin Sterilizes Long-Term Dormant Mycobacterium tuberculosis antimicrobial agents and chemotherapy. 2007; 51:1537-1540.
19. Long KS. Poehlsgaard J. Kehrenberg C. Schwarz S and Vester B. The Cfr r-RNA methyltransferase confers resistance to Phenicols, Lincosamides, Oxazolidinones, Pleuromutilins. Antimicrobial agents and chemotherapy.
Sharma Mona et al / IJRAP 2011, 2 (1) 126-131
International Journal of Research in Ayurveda & Pharmacy, 2(1), Jan-Feb 2011 126-131
20. Petrella S. Cambau E. Chauffour A. Andries K. Jarlier V. and Sougakoff W. Genetic basis for natural and acquired resistance to the diarylquinoline R207910 in mycobacteria. Antimicrobial agent’s chemotherapy. 2006; 50:2853-2856.
21. Keung ACF. Eller MG. McKenzie KA. Weir SJ. Single and multiple dose pharmacokinetics of rifapentine in man: part ll. Int J Tuberc Lung Dis. 1993; 33:1203-10.
22. Temple ME. Nahata MC. Rifapentine: its role in the treatment of tuberculosis. Ann Pharmacother. 1999; 33:1203-10.
23. Shoen CM. DeStefano MS. and Cynamon MH. Durable cure for tuberculosis: rifalazil in combination with isoniazid in a murine model of Mycobacterium tuberculosis infection. C lin infect Dis. 2000; 30:288-290.
24. Koga T. Fukuoka T. Doi N. Harasaki T. Inoue H. Hotoda H. Activity of capuramycin analogues against Mycobacterium tuberculosis, Mycobacterium avium and M. intercellulare in vitro and in vivo. J Antimicrobial Chemotherapy. 2004; 54:755-60.
25. Jagannath C. Reddy VM. Kailassam S. O’Sullivan JF. Gangadharam PRJ. Chemotherapeutic activity of clofazimine and its analogues against Mycobacterium tuberculosis. In vitro, intracellular, and in vivo studies. Am Rev Respir Crit Care Med. 1995; 151:1083-6.
26. Recently reviewed in REF: Churchyard GJ, Kaplan G, Fallows D, Wallis RS, Onyebujoh P, Rook GA. Advances in immunotherapy for tuberculosis treatment Clin Chest Med 2009 Dec; 30(4):769-82.
27. Dawson R. Condos R. Tse D. Huie ML. Ress S. Tseng C. Immunomodulation With recombinant interferon-g1b in pulmonary tuberculosis. PLoS One 2009; 4 (9):6982-6984.
28. Medical Research Council. Streptomycin treatment of pulmonary tuberculosis. BMJ 1948; 2:769-82.
Fig. 1: Structure of TMC207
Fig. 2: Structures of nitroimidazofurans and nitroimidazopyrans
Fig. 3: Structures of thioacetazone and isoxyl
Fig. 4: Structure of LL-3858
Fig. 5: Structure of rifamycin derivatives
Fig. 6: Structure of capromycin
Sharma Mona et al / IJRAP 2011, 2 (1) 126-131
International Journal of Research in Ayurveda & Pharmacy, 2(1), Jan-Feb 2011 126-131
Fig. 7: Structure of dipiperidine
Fig. 8: Structure of diterpenoids
Fig. 9: Structure of purines
Fig. 10: Structure of thiazidine thiones
Fig. 11: Structure of carbohydrate derivatives
Fig. 12: Structure of natural marine products