Embed Size (px)
Citation preview

CASE 1Case History and Clinical ExaminationA 13-year-old female neutered domestic shorthair catpresented to the referring veterinarian after the ownershad noticed blood on furniture and on the cat’s foodbowl. The cat had a history of excessive grooming thatwas attributed to flea allergy. The cat was being treatedevery three weeks with topical fipronil1. Ulcers on thehard palate were identified and the cat was referred to theValentine Charlton Cat Centre. Further physicalexamination findings were pale mucous membranes, aheart rate of 240 beats per minute, a grade IV/VI systolicheart murmur and alopecia over the ventral abdomen. Alinear ulcer (2 x 0.5cm) was present on the left side of the
hard palate midway between the midline and the dentalarcade (Fig 1a). A second, circular (0.8cm diameter)ulcer on the right side of the hard palate was noted caudalto the central incisors (Fig 1a).
Diagnostic TestsBlood tests revealed a mild elevation in glucose and aregenerative anaemia (Table 1). The cat was bloodtyped2 (blood type A) and a 50mL type A bloodtransfusion was given prior to surgery.
TreatmentAt surgery, the cat was placed in dorsal recumbency withthe jaws taped open for maximal exposure of the hard
6 — Aust Vet Practit 37(1) March 2007
CASE STUDIES
Use of a Bipedicle MucoperiostealFlap to Treat Arterial Haemorrhagefrom Palatine Ulcers in Three Cats
CJ Bailey, PLC Tisdalla, JA Beattyb, A Lingardb
and VR Barrsb
North Shore Veterinary Specialist Centre64 Atchison Street, Crows Nest, NSW 2065aVeterinary Specialist CentrePO Box 307, North Ryde, NSW 1670bValentine Charlton Cat CentreFaculty of Veterinary Science, University of Sydney, NSW 2006
Aust Vet Practit 37(1) March 2007 — 6
ABSTRACT
A novel surgical treatment for palatine arterial haemorrhage secondary to hardpalate ulceration is described in three cats. The owners first noticed externalhaemorrhage in all cases. Determination of the exact site of haemorrhage wasnot always possible on visual inspection because bleeding was intermittent.Severe anaemia was present in all cats and two cases required bloodtransfusion. Surgery was performed to ligate the palatine arteries and coverthe ulcerated regions of hard palate with sliding bipedicle mucoperiostealflaps. The flaps remained viable and stopped ongoing haemorrhage from theerosive lesions successfully in all cases. [Bailey CJ et al (2007) Aust VetPractit 37:6]
Ph: 02 9436 1213. Fax: 02 9906 5710Email: [email protected]
1Frontline, Merial2Rapid Vet-H Feline desk-top blood typing kits, Agrolab,Switzerland (Australian distributor IDEXX laboratories)

PALATINE ULCERS
palate. Both palatine arteries were ligated blindly at thecaudal extent of the hard palate with simple interrupted3/0 poliglecaprone 253 sutures (Fig 1b). An incision wasthen made along the lateral margin of the palatinemucosa immediately adjacent to the left dental arcade.The lateral edge of the ulcer was incised to enableelevation of the mucoperiosteum with a periostealelevator, leaving the caudal and rostral bases intact tocreate a bipedicle mucoperiosteal flap. This flap wastransposed over the linear ulcer deficit then sutured tothe incised medial edge of the ulcer using simpleinterrupted 4/0 poliglecaprone 25 sutures3 (Figs 1c &1d). The lateral palatine bone was left to granulate. Ashort unipedicle mucoperiosteal flap was elevated andtransposed to cover the circular ulcer on the right side(Fig 1e). Amoxycillin-clavulanic acid4 was administered(8.75 mg/kg sc) at the time of surgery followed by aseven-day course (12.5 mg/kg po bid). An Elizabethancollar was applied post-operatively to preventovergrooming. Excess salivation was noted in the first 24hours but no further haemorrhage was observed.Analgesia was provided with buprenorphine5 0.01mg/kgsc qid and soft food was introduced 24 hours aftersurgery. Two weeks after surgery the mucoperiosteal flapappeared intact and viable, the exposed hard palate had abed of granulation tissue and the PCV was 0.34L/L. In
addition to flea control, a food elimination diet wasrecommended to further investigate the overgrooming.Three months post-operatively the mouth hadcompletely healed.
CASE 2Case History and Clinical ExaminationA 14-year-old female neutered domestic shorthair catwas presented to the referring veterinarian because theowners noticed profuse bleeding from the cat’s mouth. Apalatine ulcer was identified extending longitudinally for2cm on the right side of the hard palate and crossing themidline at the rostral aspect (Fig 2). Haemorrhageappeared to originate from the linear part of the ulcer. Atinitial presentation blood tests (Table 1) revealed mildanaemia and pre-renal azotaemia (urine specific gravity>1.055). Twenty-four hours later the PCV had decreasedto 0.19L/L and the cat was referred to the VeterinarySpecialist Centre, North Ryde. Abnormalities noted onphysical examination were the ulcer, a grade II/VIsystolic heart murmur and the presence of flea dirt in thecoat.
Aust Vet Practit 37(1) March 2007 — 77 — Aust Vet Practit 37(1) March 2007
HAEMATOLOGY AND BIOCHEMISTRYParameter Case 1 Case 2 Case 3 Reference Range
Haematocrit (L/L) 0.15 0.27→0.19 0.10 0.30-0.45
Total Plasma Protein (g/L) 71 74 84 59-78
Red Cell Count (x1012/L) 3.55 n/a 2.60 6.0-10.0
Hb (g/L) 50 n/a 27 80-140
MCV (fl) 42.3 n/a 38.5 40-45
MCH (pg) 14.1 n/a 10.4 13-17
MCHC (g/L) 333 n/a 270 310-350
Platelets (x109/L) n/a 478 634 200-700
Uncorrected Reticulocytes % 3.6 n/a 9 0-1.0
Absolute reticulocyte count (x109/L) 128 n/a 234 50
White Blood Cell count (x109/L) 18.2 n/a 12.2 8.0-14.0
Neutrophils (x109/L) 9.65 n/a 11.71 3.76-10.8
Lymphocytes (x109/L) 6.01 n/a 0.24 1.6-7.0
Monocytes (x109/L) 0.18 n/a 0.24 0.08-0.56
Eosinophils (x109/L) 1.82 n/a 0.00 0.16-1.4
Basophils (x109/L) 0.36 n/a 0.00 0-0.14
Bands (x109/L) 0.18 n/a 0.00 0-0.42
Urea (mmol/L) 6.92 37 13.7 7.2-10.7
Creatinine (µmol/L) 126 167 214 90-180
Glucose (mmol/L) 10.4 9.4 8.90 3.6-6.6
ALT (IU/L) 25 43 47 <60
ALP (IU/L) 23 37 76 <50
FIV status n/a n/a Negative –
TABLE 1: Haematology and biochemistry. n/a = not available.
3Monocryl, Ethicon4Clavulox, Pfizer5Temgesic, Reckitt Benckiser

PALATINE ULCERS
Aust Vet Practit 37(1) March 2007 — 88 — Aust Vet Practit 37(1) March 2007
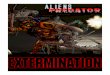
FIGURE 1b: Ligation of the left and right major palatinearteries in the region where they exit the palatine foraminaof the hard palate.
FIGURE 1a: Erosive lesions on hard palate of Case 1.L=left, R=right. Arrow points to smaller lesion.
FIGURE 1c: Elevation of a bipediclemucosal flap.
FIGURE 1d: Mucosal flap transposedmedially and sutured to cover thepalatine ulcer.
FIGURE 1e: Short unipedicle mu-cosal flap covering smaller ulcer.Arrows point to exposed areas left togranulate.
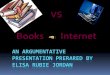
FIGURE 2: Erosive lesions on hardpalate of Case 2, appearing as mirrorimage of Case 1.
FIGURE 3a: Erosive lesions on hardpalate of Case 3, similar to Case 2.
FIGURE 3b: Healed mucosal flap inCase 3, 11 months post-operatively.

PALATINE ULCERS
Diagnostic Tests and TreatmentThe cat was blood typed on admission (blood type A).The PCV had increased to 0.24L/L before surgery (TPP76g/L). Since the cat was clinically stable, bloodtransfusion was not performed. At surgery, a biopsy wastaken from the cranial edge of the linear ulcer andsubmitted for histopathology. A similar surgicaltechnique to that used in Case 1 was performed:horizontal mattress sutures using 4/0 polydioxanone6
were placed at the caudal aspect of the ulcer to ligate theright palatine artery. The bipedicle mucoperiosteal flapwas transposed over the linear ulcer deficit on the rightside and sutured to the incised medial edge of the ulcer,using simple interrupted 4/0 polydioxanone sutures.Post-operative care, including analgesia, antimicrobialtherapy, feeding and provision of an Elizabethan collar,was similar to Case 1. Monthly topical flea control withfipronil was prescribed.
On histopathology the biopsy tissue was composed ofhyperplastic stratified squamous oral epithelium withunderlying dense connective tissue. Within theconnective tissue there was interspersed granulationtissue. There was no evidence of a neoplastic process,haemosiderosis or an ischaemic cause such as athrombosed vessel.
The cat re-presented four days after discharge becausethe owner had noticed bleeding from the mouth. Themucoperiosteal flap was intact and viable with noevidence of haemorrhage from that site. However, asmall focal point of haemorrhage appeared to originatefrom a small ulcer on the left side of the rostral hardpalate. Blood tests revealed a PCV of 0.26L/L and TPPof 76g/L. Surgery was performed to ligate the leftpalatine artery and appose the ulcer edges with 4/0polydioxanone horizontal mattress sutures. Atexamination four weeks later, the mouth had completelyhealed. No recurrence of the ulcer occurred. The catdeveloped an invasive mandibular lesion two years laterand was euthanased.
CASE 3Case History and Clinical ExaminationA seven-year-old male domestic short hair cat presentedfor lethargy and inappetence. The owner had noticed asmall amount of blood on the cat’s lips and firm blackfaeces had been observed. Physical examinationrevealed a heavy flea burden, very pale mucousmembranes and ulceration of the hard palate in anL-shape (3 x 0.5cm on right side of hard palate with ashort narrow extension across to the left side at therostral margin; Fig 3a).
Diagnostic TestsSevere regenerative anaemia was identified onhaematology with results consistent with iron deficiencyanaemia secondary to chronic blood loss (Table 1).
TreatmentThe cat was typed, treated with fipronil and given a50mL type A blood transfusion before surgery. Bothpalatine arteries were ligated and the linear ulcer wascovered with a sliding bipedicle mucoperiosteal flap asdescribed for the previous cases. The short narrow ulceron the right side was small enough to have the edges
apposed using horizontal mattress sutures withoutcreating excessive tension. Post-operative care was thesame as for Case 1 with the addition of ferrous sulphate81.5mg po sid and topical imidocloprid7 every fourweeks. The PCV 10 days post surgery was 0.26L/L andthe mouth was healing well. Eleven months post-operatively there had been no recurrences of palatineulceration but the residual healed areas were still visible(Fig 3b).
DISCUSSIONPalatine arterial haemorrhage in the cat was first reportedin 1990 (Wildgoose 1990). In that case, a small erosionwas located on the hard palate level with the anterioraspect of the second premolar tooth, 4 to 5mm from themidline. Profuse haemorrhage was identified from theerosion which overlaid the right major palatine artery.Haemorrhage was controlled with electrocautery(Wildgoose 1990). Menrath & Miller (1995)subsequently reported a cat with a bleeding palatineerosive lesion that resulted in severe blood loss anaemia.They postulated that the pathogenesis of these lesionswas excessive licking/grooming as a result of a pruriticskin condition. The cat was given a blood transfusionand horizontal mattress sutures were placed across thewidth of the erosion (Menrath & Miller 1995).
Many aetiologies can cause ulcerative lesions in the oralcavity of the cat but, typically, these do not result insignificant oral haemorrhage. Aetiologies of oralulcerative lesions in the cat include eosinophilicgranuloma complex (Frost & Williams 1986, vonTscharner & Bigler 1989, Pedersen 1992), Calicivirusinfection (Hoover & Kahn 1975, Pedersen 1992),neoplasia such as squamous cell carcinoma (Frost &Williams 1986, Pedersen 1992), immune-mediateddiseases such as pemphigus vulgaris and systemic lupuserythematosus (Manning et al 1982, Pedersen 1992),ingestion of caustic substances and trauma (Pedersen1992).
The three cases in the current series all presented withevidence of bleeding from the mouth that was detectedby the owners. However, if the cat has been repeatedlyswallowing the blood, external haemorrhage may not beapparent and the extent of blood loss anaemia may beprofound by the time the cat is presented to theveterinarian. Therefore, lethargy, inappetence and/ormelaena may be the main presenting signs and a fullphysical examination should be performed on all cases todetect ulcerative lesions of the hard palate and theinitiating cause of pruritis.
The clinical appearance of all three lesions was similar,demonstrating longer linear erosions with defined edgeson one side of the hard palate and smaller, short erosionsat the rostral aspect on the opposite side. Case 2demonstrated that haemorrhage was not limited to thelarger lesion, as a second procedure was required tocover the smaller erosion. This highlights the difficultyassociated with identification of the exact site ofhaemorrhage. Also, at the time of presentation many ofthese cases do not display active haemorrhage.
Aust Vet Practit 37(1) March 2007 — 1010 — Aust Vet Practit 37(1) March 2007
6PDS II, Ethicon7Advantage, Bayer

PALATINE ULCERS
Therefore, diagnosis is often made by pattern-recognition, in which cats presented with a regenerativeanaemia and a palatine ulcer are assumed to be bleedingfrom the ulcer. The consistent finding was that theerosions overlay the major palatine arteries in the hardpalate. The right and left major palatine arteries, whichare branches of the maxillary arteries, are the main bloodsupply to the hard palate (Evans & Christensen 1979).They exit the palatine foramina of the hard palate at thelevel of and medial to the distal cusp of the upper fourthpremolar (Orsini & Hennet 1992) and course forward inthe palatine sulcus just medial to midway between thedental arcade and the midline (Bezuidenhout 2003).They become more superficial as they course rostrally tolie closely under the oral mucosa. A small branch passesthrough the oval palatine fissure between the canineteeth before the artery travels to the back of the incisorteeth where the vessel anastomoses with its fellow(Evans & Christensen 1979).
An understanding of the regional anatomy was importantfor performing the surgical procedure, especiallybecause the major palatine arteries are not directlyvisible. Ligation of the bases of the major palatinearteries was attempted with the dual aim of reducingintra-operative haemorrhage whilst elevating themucoperiosteal flap and to stop ongoing haemorrhagefrom the palatine erosions. The mucosa of the hard palateremained viable and healed in all three cases indicatingthat sufficient collateral circulation exists after ligationof the major palatine arteries.
A bipedicle mucoperiosteal flap was transposed over thelarger ulcerated regions to provide a robust coverage ofthe ulcerated area. Electrocautery had been previouslydescribed in the treatment of palatine arterialhaemorrhage (Wildgoose 1990) but that case involvedonly a small lesion and the extensive use ofelectrocautery in the oral cavity can be detrimental towound healing (Fossum 2002). The use of tightly-approximated broad horizontal mattress sutures placedacross the width of the erosion has also been describedfor the treatment of this condition (Menrath & Miller1995). However, for larger lesions, it is not possible toappose the mucosal edges with sutures as the mucosa isnot compliant and undue tension may result in wounddehiscence (Fossum 2002). The mucoperiosteal flapused in the current study for the closure of the longerlinear erosive lesions was bipedicle because it supplied abetter blood supply than that which would be providedfrom a narrow single base. The flap needed to beundermined sufficiently to allow enough mobility to betransposed medially without tension. The principles ofatraumatic tissue handling were adhered to reduce thechance of dehiscence (Fossum 2002). The exposed areaof the hard palate immediately adjacent to the dentalarcade was left to heal with granulation tissue.
Histopathology was performed on Case 2. Themicroscopic appearance of the tissue was consistent withthe previously proposed pathogenesis of repetitivetrauma from excessive licking/grooming in thisparticular case (Menrath & Miller 1995). The felinetongue has numerous well-developed harsh conicalpapillae that provide an effective rasping action forgrooming and prehension (Dyce et al 1987, Menrath &
Miller 1995). In the process of licking/grooming, thetongue is thought to repeatedly impinge on the hardpalate in a backward rasp-like fashion with the cross-sectional shape of the tongue preferentially contactingeither side of the midline over the regions of the majorpalatine arteries (Menrath & Miller 1995). The continualabrasion of the epithelium may result in the eventualerosion into the major palatine arteries and causesubstantial haemorrhage (Menrath & Miller 1995). Apossible explanation for the asymmetrical appearance ofthe lesions is the cat’s preferentially grooming to the leftor right. It is unclear as to why so few feline cases withpruritis or overgrooming develop bleeding palatineulcers and why the condition was not recognised in theliterature prior to 1990 (Wildgoose 1990). Affected catsmay be those that overgroom constantly. Anotherpossible explanation for the disease pathogenesis isextension of the inflammatory process secondary totrauma-induced mucosal ulceration to involve thepalatine arteries and surrounding tissues, resulting inarteritis or periarteritis of the palatine arteries. Thehistopathology for Case 2 was consistent with repetitivetrauma rather than arteritis/periarteritis but histo-pathological anlayisis of biopsies from a larger numberof cases would be useful.
The haemorrhage from the palatine ulcers may be severeenough to warrant a blood transfusion as in two of thepresent cases. Whilst a definitive pathogenesis is notproven for these three cases, the surgical techniquedescribed proved effective in arresting ongoinghaemorrhage in cats with significant anaemia. Thepresence of fleas or flea dirt and/or the history ofovergrooming in the present case series were consistentwith the previously proposed pathogenesis of repetitiveabrasion from the tongue. Therefore, the authorsrecommend that subsequent to the surgery, anElizabethan collar is applied to stop overgrooming in theshort-term. Cats should be treated with effective fleaparasiticides and other causes of pruritic skin diseaseshould be investigated (e.g. dietary elimination trials andintradermal allergen skin testing).
REFERENCES BEZUIDENHOUT, AJ (2003) Textbook of Small Animal Surgery, Ed
Slatter, 3rd edn, pp2630-2627, Saunders, PhiladelphiaDYCE, KM, SACK, WO & WENSING, CJG (1987) Textbook of
Veterinary Anatomy, 1st edn, pp100-101, Saunders,Philadelphia
EVANS, HE & CHRISTENSEN, GC (1979) Miller’s Anatomy of theDog, 2nd edn, pp141-675, Saunders, Philadelphia
FOSSUM, TW (2002) Small Animal Surgery, 2nd edn, p275,Mosby, St. Louis
FROST, P & WILLIAMS, CA (1986) Feline dental disease, Vet ClinNth Am Small Anim Pract 16:851
HOOVER, EA & KAHN, DE (1975) Experimentally induced felinecalicivirus infection: clinical signs and lesions, J Am Vet MedAssoc 166:463
MANNING, TO, SCOTT, DW, SMITH, CA & LEWIS, RM (1982)Pemphigus diseases in the feline: seven case reports, J AmAnim Hosp Assoc 18:433
MENRATH, VH & MILLER, R (1995) The repair and prevention ofbleeding palatine erosive lesions in the cat, Aust Vet Practit25:202
ORSINI, P & HENNET, P (1992) Anatomy of the mouth and teethof the cat, Vet Clin Nth Am Small Anim Pract 22:1265
PEDERSEN, NC (1992) Inflammatory oral cavity diseases of thecat, Vet Clin Nth Am Small Anim Pract 22:1323
VON TSCHARNER, C & BIGLER, B (1989) The eosinophilicgranuloma complex, J Small Anim Pract 30:228
WILDGOOSE, WH (1990) Palatine arterial haemorrhage in a cat,Vet Rec 126:273
Aust Vet Practit 37(1) March 2007 — 1111 — Aust Vet Practit 37(1) March 2007