Embed Size (px)
Citation preview

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/236077679
Preconceptiontoparenting:Motherhoodforwomenwithseverementalillness,asystematicreviewandmeta-synthesisofthe...
ArticleinArchivesofWomensMentalHealth·March2013
DOI:10.1007/s00737-013-0336-0·Source:PubMed
CITATIONS
37
READS
223
3authors:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
InfertilityandmentalhealthViewproject
ClareDolman
King'sCollegeLondon
7PUBLICATIONS72CITATIONS
SEEPROFILE
IanRichardJones
CardiffUniversity
387PUBLICATIONS19,993CITATIONS
SEEPROFILE
LouiseHoward
King'sCollegeLondon
267PUBLICATIONS3,896CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyClareDolmanon04September2014.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinblueareaddedtotheoriginaldocumentandarelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.

ORIGINAL ARTICLE
Pre-conception to parenting: a systematic review and meta-synthesisof the qualitative literature on motherhood for women with severemental illness
Clare Dolman & Ian Jones & Louise M. Howard
Received: 5 November 2012 /Accepted: 13 February 2013# Springer-Verlag Wien 2013
Abstract The majority of women with a severe mentalillness (SMI) become pregnant and have children. The aimof this systematic review and meta-synthesis was to examinethe qualitative research on the experiences of motherhood inwomen with SMI from preconception decision making tobeing a mother. The experiences of the health professionalstreating women with SMI were also reviewed. Eleven data-bases were searched for papers published up to April 25,2012, using keywords and mesh headings. A total of 23studies were identified that met the inclusion criteria on theviews of women with SMI, eight reported the views ofhealth professionals including one which reported both.The meta-synthesis of the 23 studies on women's viewsproduced two overarching themes Experiences ofMotherhood and Experiences of Services. Sub-themes in-cluded the following: Guilt, Coping with Dual Identities,Stigma, and Centrality of Motherhood. Four themesemerged from the synthesis of the eight papers reportingthe views of health professionals: Discomfort, Stigma, Needfor education, and Integration of services. An understandingof the experiences of pregnancy and motherhood for womenwith SMI can inform service development and provision toensure the needs of women and their families are met.
Keywords Pregnancy . Severe mental illness . Systematicreview . Qualitative research
Introduction
The majority of women with psychotic disorders aremothers (Howard et al. 2001; McGrath et al. 1999), butmost research in this area has either focused on thesubjects’ psychopathology and the potential harm to theirchildren (Murray et al. 2003) or on service provision(Howard and Hunt 2008). Although in the past thefertility of women with severe mental illness (SMI) wasconsidered to be lower than that of the general popula-tion (Howard et al. 2002), recent research has found it isincreasing (Vigod et al. 2012). Concurrently, there hasbeen a growing awareness internationally of the need toprovide gender sensitive mental health services, e.g.,Mainstreaming Gender and Women’s Mental Health(2003), and there is a developing literature on the expe-riences of mothers with SMI including their experiencesof health services. The literature on health professionals’perspectives on looking after mothers with SMI is limitedand has usually focused on prescribing and risk (Lesteret al. 2005) and less on their attitudes and experiences,including challenges and how to meet them. This is arelatively under-researched area of healthcare; hence, theNational Institute for Health and Clinical Excellence(NICE) antenatal and postnatal mental health guideline(CG45) calls for more research on patients’ access tospecified services and the quality of care, as well as dataon “staff views on the delivery of care” (NationalInstitute for Health and Clinical Excellence 2007).Qualitative methods are increasingly acknowledged as avaluable means of gaining a deeper insight into theexperiences of service users and health providers, andcan contribute to a greater understanding of the wayservices are used and might be improved (Walsh andDowne 2005; Rice 2008). To our knowledge, there havebeen no meta-syntheses of the qualitative literature on
C. Dolman (*) : L. M. HowardSection of Women’s Mental Health, Health Service and PopulationResearch Department, Box PO31 Institute of Psychiatry, King’sCollege London, De Crespigny Park, London SE5 8AF, UKe-mail: [email protected]
I. JonesDepartment of Psychological Medicine and Neurology, MRCCentre for Neuropsychiatric Genetics and Genomics, CardiffUniversity, Cardiff CF14 14XN, UK
Arch Womens Ment HealthDOI 10.1007/s00737-013-0336-0

pregnancy and childbirth (from preconception decision-making to views on being a mother with a mentalillness) from either the perspective of women with anSMI or the health professionals caring for them.
Meta-synthesis, deriving from theories developed byNoblit and Hare (1988), refers to “interpretive transla-tions produced from the integration or comparison offindings from qualitative studies” (Sandelowski et al.2006). The aim of this meta-synthesis was to bringtogether insights from qualitative studies that includedthe views of women with SMI on pregnancy and moth-erhood to give a fuller account of women’s perspectiveson the various aspects of the experience of havingchildren, and to explore the professionals’ experiencesof caring for these patients. It is hoped that byperforming a thematic synthesis of the relevant com-bined data, a more comprehensive account can be givenof these perspectives (Beck 2002).
We therefore aimed to:
(1) Synthesise the research literature on the experiencesof motherhood in women with SMI from pre-conception decision making to being a mother, in-cluding consideration of whether the experiences ofhaving children differed in women from differentdiagnostic groups.
(2) Synthesise the research literature on the experiencesof health professionals caring for mothers withSMI.
Methods
Studies were included if they satisfied the following inclu-sion criteria:
& Qualitative studies, using interviews, focus groups orboth, on the views of women with SMI or healthcareprofessionals caring for women with SMI on the subjectof having children.
& English-language papers published or in press inpeer-reviewed journals with a study population in-cluding women with serious mental illness (SMI)defined as female participants 18 years and olderwith a psychotic disorder (schizophrenia or bipolardisorder, with or without psychotic symptoms, andrelated disorders) or healthcare professionals caringfor them.
No demographic or geographic restriction was placedon sample participants or study setting. As it is goodpractice to be as inclusive as possible in a meta-synthesis(Walsh and Downe 2005), papers describing the concernsof women with SMI on genetic issues and how this
impacted on their views of pregnancy and motherhoodcould be included even if this was the only construct ofrelevance.
Exclusion criteria were:
(1) Studies only including participants under 18 years(2) Studies with no participants with SMI as defined above
(other than studies of health professionals)(3) Studies (randomised controlled trials, cohort studies,
case–control studies, cross-sectional studies, clinicalcase studies, surveys or dissertations/reports/bookchapters) with no qualitative component
Procedure
The following bibliographic databases were searched fromtheir respective start dates (given in parenthesis) to April 25,2012: PsycINFO (1806), Ovid MEDLINE(R) In-Process &Other Non-Indexed Citations and Ovid MEDLINE(R)(1946), EMBASE Classic + EMBASE (1947), Maternityand Infant Care (1971), British Nursing Index and Archive(1985), CINAHL (1982), Applied Social Services Index andAbstracts (1987), Social Service Abstracts (1979),Sociological Abstracts (1952), Social Policy and Practice(1890s).
For each of the databases, an inclusive search wasperformed using subject headings or mesh terms, textwords and keywords. Search terms included: bipolar dis-order, schizophrenia, SMI, postpartum psychosis; pregnan-cy, childbirth, perinatal, antenatal, puerperal, postnatal,primipara; mother, parent, maternal; qualitative, grounded
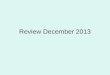
Papers identified throughDatabase searching:
n = 214
Papers identified by alternative means:
Hand searches: n=8Citation tracking: n=5
Papers after screening:n = 227
Full-text articles assessed for eligibility: n = 72
Papers excluded: n = 49
Reasons for exclusion:
Not reporting qualitative research: n = 32Study did not address issues around pregnancy or having children: n = 19Sample did not include women with SMI”s views: n = 11* papers could be excluded for more than 1 reason
Studies included in the review:n = 23
Fig. 1 Flow diagram of screened and included papers for women withSMI
C. Dolman et al.

theory, focus groups. Terms were combined using theBoolean “and” and “or” functions and single wordsearches were conducted as well as subject headings tocheck for omissions. Searches were complemented withcitation tracking and contact with ten researchers in thefield (Fig. 1). Using the same databases, a separatesearch was conducted to identify studies examining theexperience of health professionals caring for pregnantwomen or mothers with SMI. Additional search termsincluded: health professionals, medical professionals,clinicians, doctors, psychiatrist, nurses, midwives, peri-natal psychiatric workers, antenatal healthcare workers(Fig. 2).
Relevant data were extracted from all studies using astandardized data extraction form. This was to recordbasic information such as sample characteristics, setting,date and form of data collection, and analytical ap-proach. The papers were re-read to identify the first-order constructs (i.e., experiences of women as reportedin original studies) and second-order constructs (i.e.,original study author interpretations or conclusions),and checked to confirm that the authors’ interpretationswere supported by the data presented in the study. Atthis stage the comparison across and within studies toidentify and synthesize themes began.
The studies were methodically appraised by CDusing the previously validated Critical Appraisal SkillsProgramme CASP (Oxford 2010) as a guide and 20%of papers were independently assessed by a secondreviewer (KT); a consensus was reached on quality. TheCASP checklist was adapted to incorporate elements of theBMJ Qualitative Research Checklist (BMJ 2011) so that the
finalised version included items assessing study context,quality of analytical methods and service user involve-ment (see Appendix 1). Papers were scored out of atotal of 62, with an average of 42 achieved (scores arelisted in Table 1).
Analysing and synthesizing the selected studies
Appraising quality also gave another opportunity toexamine the studies and compare the constructs theyhad identified. Apparent contradictions and their possi-ble resolution were also re-examined at this stage,according to the principles of Noblit and Hare’s (1988)approach to synthesizing qualitative studies. Findingsare juxtaposed to both identify homogeneity of themesand note discordance. This “translation” of studiesserves to identify commonalities which, in the secondstage, can be synthesized to elucidate more refinedmeanings and concepts (Walsh and Downe 2005). Thestudies were independently analysed by LH and a con-sensus was reached on the content of the meta-synthesis, a procedure designed to enhance reliability(Mays and Pope 2000).
Results
A total of 227 papers on women with SMI were ini-tially identified; 23 studies met inclusion criteria for themeta-synthesis with a total of 355 women (see Fig. 1).These reflected an international perspective on the viewson pregnancy and motherhood of women with SMI,with papers from eight countries, including six eachfrom the US and UK (see Table 1). Eight papers (froman original search of 219) were located which reportedthe views of 143 health professionals on the pregnancyand motherhood issues affecting women with SMI (seeFig. 2). These figures include one paper, Nicholson etal. (1998), which reported results from both groups.Details of these papers are given in Table 4. Pleasenote that, in the following report of results, first-orderconstructs are quoted in italics, while second-order con-structs are in plain text with single quote marks.Information on excluded studies is available from authoron request.
Studies of women with SMI
Nine themes were identified: Stigma, Guilt, Custody loss,Concern over effect on the child, Isolation, Coping withdual identities, Centrality of motherhood, Problems withservice provision, Positive aspects of service provision.
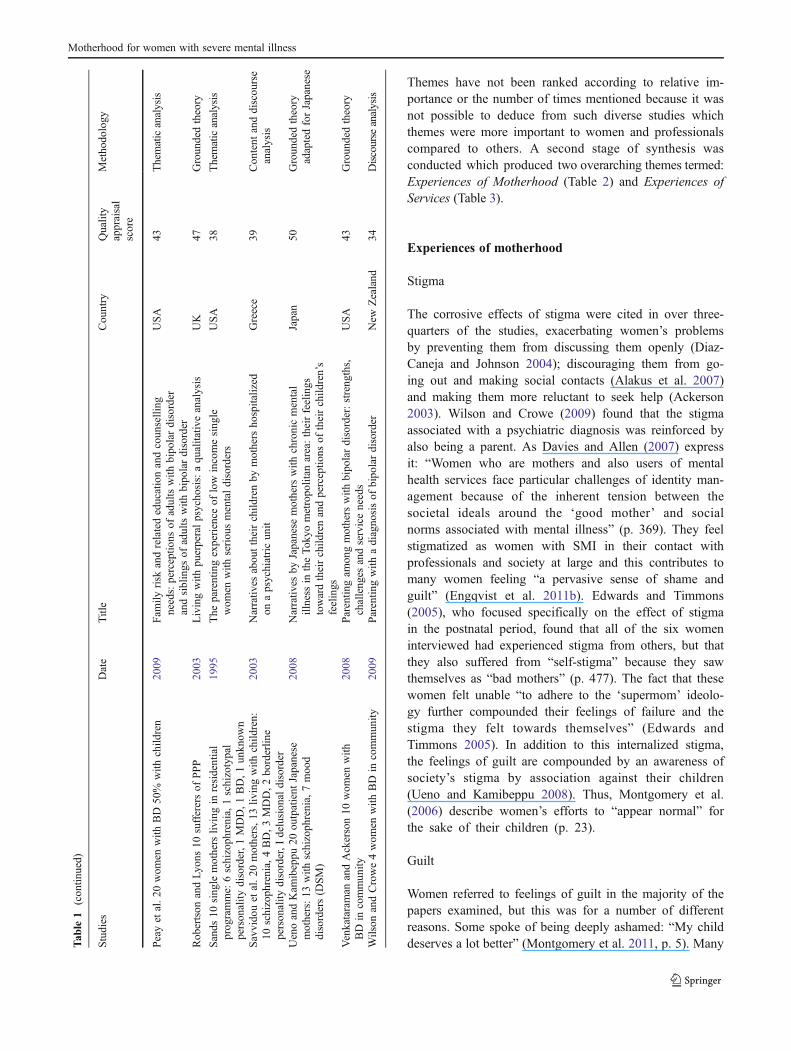
Papers identified throughDatabase searching:
n = 205
Papers identified by alternative means:
Hand searches: n=7Citation tracking: n=7
Inclusion criteria applied to 219
Full-text articles assessed for eligibility: n = 39
Studies included in the review: n = 8
Papers excluded: n = 31Reasons for exclusion:
Not reporting qualitative research: n = 15
Study did not address issues around pregnancy or having children: n = 21
* papers could be excluded for more than 1 reason
Fig. 2 Flow diagram of screened and included papers for healthprofessionals
Motherhood for women with severe mental illness

Table 1 Summary of studies on views of women with severe mental illness
Studies Date Title Country Qualityappraisalscore
Methodology
Ackerson et al. 12 outpatient mothers withSMI, psychotic or severe mood disorder
2003 Coping with the dual demands of severe mentalillness and parenting
USA 42 Grounded theory +narrative history
Alakus et al. Focus groups of mothers withunder-5s, part of “Parents with Psychosis”project
2007 The needs of parents with a mental illness whohave young children: an Australian perspectiveon service delivery options
Australia 21 Thematic analysis
Bassett et al. 2 focus groups, 4 interviewswith women with SMI using communityrehabilitation services
1999 Parenting: experiences and feelings of parentswith a mental illness
Australia 43 Thematic analysis
Chernomas et al. 28 outpatients 18 withschizophrenia, 10 schizo-affective disorderin focus groups
2000 Perspectives of women living with schizophrenia Canada 37 Thematic analysis
Davies and Allen 11 outpatients with SMI andchildren, 3 with psychosis, 2 BD, 1 OCD,5 depression
2007 Integrating “mental illness” and “motherhood”:the positive use of surveillance by healthprofessionals. A qualitative study
UK 40 Interactionalframeworkanalysis
Diaz-Caneja and Johnson 22 outpatients, 8with schizophrenia, 10 BD, 4 MDD withpsychotic symptoms
2004 The views and experiences of severely mentallyill mothers: a qualitative study
UK 44 Thematic analysis
Doucet et al. 9 women who had beenhospitalized for PPP
2012 Postpartum psychosis: support needs of mothersand fathers
Canada 38 Content analysis
Edwards and Timmons 6 former MBU patients,3 PPP, 1 depressive psychosis, 2 severe PND
2005 A qualitative study of stigma among womensuffering from postnatal illness
UK 41 Grounded + feministtheory
Engqvist et al. 10 internet narratives of womenwith PPP
2011b Women’s experiences of postpartum psychoticepisodes — analyses of narratives from theinternet
Sweden 44 Content analysis
Heron et al. 5 women who experienced PPP 2012 Experiences of recovering from PP: a serviceuser/researcher collaboration
UK 43 Grounded analyticinduction approach
Khalifeh et al. 18 mothers: 2 with schizophrenia,6 BD, 10 MDD
2009 Home treatments as an alternative to hospitaladmission for mothers in a mental health crisis:a qualitative study
UK 53 Content analysis
Meiser et al. perceived genetic riskof BD: 10 euthymic Bipolar women
2005 Implications of genetic risk information in familieswith a high density of bipolar disorder: anexploratory study
Australia 48 Framework analysis
Montgomery et al. 20 outpatient mothers: 3 withschizophrenia, 4 BD, 9MDD, 4 unspecified
2006 Keeping close: mothering with serious mental illness Canada 50 Grounded theory
Montgomery et al. 32 mothers with SMI inpatientand in community, Canadian Ministry of Healthdefinition
2011 Mothers with serious mental illness: their experienceof “Hitting Bottom”
Canada 41 Thematic + narrativeanalysis
Mowbray et al. 24 mothers, 15 in community.SMI according to “agency records”
1995 Parenting and the significance of children for womenwith a serious mental illness
USA 43 Thematic analysis
Nicholson et al. Focus groups with 42 mothers incommunity: 23 affective disorder, 8 psychoticdisorder, 6 anxiety disorder, 5 other
1998 Focus on women: mothers with mental illness: 1 Thecompeting demands of parenting and living withmental illness
USA 51 Thematic analysis
C.D
olman
etal.
Themes have not been ranked according to relative im-portance or the number of times mentioned because it wasnot possible to deduce from such diverse studies whichthemes were more important to women and professionalscompared to others. A second stage of synthesis wasconducted which produced two overarching themes termed:Experiences of Motherhood (Table 2) and Experiences ofServices (Table 3).
Experiences of motherhood
Stigma
The corrosive effects of stigma were cited in over three-quarters of the studies, exacerbating women’s problemsby preventing them from discussing them openly (Diaz-Caneja and Johnson 2004); discouraging them from go-ing out and making social contacts (Alakus et al. 2007)and making them more reluctant to seek help (Ackerson2003). Wilson and Crowe (2009) found that the stigmaassociated with a psychiatric diagnosis was reinforced byalso being a parent. As Davies and Allen (2007) expressit: “Women who are mothers and also users of mentalhealth services face particular challenges of identity man-agement because of the inherent tension between thesocietal ideals around the ‘good mother’ and socialnorms associated with mental illness” (p. 369). They feelstigmatized as women with SMI in their contact withprofessionals and society at large and this contributes tomany women feeling “a pervasive sense of shame andguilt” (Engqvist et al. 2011b). Edwards and Timmons(2005), who focused specifically on the effect of stigmain the postnatal period, found that all of the six womeninterviewed had experienced stigma from others, but thatthey also suffered from “self-stigma” because they sawthemselves as “bad mothers” (p. 477). The fact that thesewomen felt unable “to adhere to the ‘supermom’ ideolo-gy further compounded their feelings of failure and thestigma they felt towards themselves” (Edwards andTimmons 2005). In addition to this internalized stigma,the feelings of guilt are compounded by an awareness ofsociety’s stigma by association against their children(Ueno and Kamibeppu 2008). Thus, Montgomery et al.(2006) describe women’s efforts to “appear normal” forthe sake of their children (p. 23).
Guilt
Women referred to feelings of guilt in the majority of thepapers examined, but this was for a number of differentreasons. Some spoke of being deeply ashamed: “My childdeserves a lot better” (Montgomery et al. 2011, p. 5). ManyT
able
1(con
tinued)
Stud
ies
Date
Title
Cou
ntry
Quality
appraisal
score
Metho
dology
Peay
etal.2
0wom
enwith
BD
50%
with
child
ren
2009
Family
risk
andrelatededucationandcoun
selling
needs:perceptio
nsof
adultswith
bipo
lardisorder
andsiblings
ofadultswith
bipo
lardisorder
USA
43Thematicanalysis
Rob
ertson
andLy
ons10
sufferersof
PPP
2003
Livingwith
puerperalpsycho
sis:aqu
alitativ
eanalysis
UK
47Groun
dedtheory
Sand
s10
sing
lemothers
livingin
residential
prog
ramme:
6schizoph
renia,1schizotypal
person
ality
disorder,1
MDD,1
BD,1
unkn
own
1995
The
parentingexperience
oflow
incomesing
lewom
enwith
seriou
smentald
isorders
USA
38Thematicanalysis
Savv
idou
etal.2
0mothers,1
3liv
ingwith
child
ren:
10schizoph
renia,4BD,3
MDD,2
borderlin
eperson
ality
disorder,I
delusion
aldisorder
2003
Narrativ
esabou
ttheirchild
renby
mothers
hospitalized
onapsychiatricun
itGreece
39Con
tent
anddiscou
rse
analysis
UenoandKam
ibeppu
20ou
tpatient
Japanese
mothers:13
with
schizoph
renia,7moo
ddisorders(D
SM)
2008
Narrativ
esby
Japanese
mothers
with
chronicmental
illness
intheTo
kyometropo
litan
area:theirfeelings
towardtheirchild
renandperceptio
nsof
theirchild
ren’s
feelings
Japan
50Groun
dedtheory
adaptedforJapanese
Venkataraman
andAckerson10
wom
enwith
BD
incommun
ity20
08Parentingam
ongmothers
with
bipo
lardisorder:streng
ths,
challeng
esandserviceneeds
USA
43Groun
dedtheory
Wilson
andCrowe4wom
enwith
BD
incommun
ity20
09Parentingwith
adiagno
sisof
bipo
lardisorder
New
Zealand
34Discourse
analysis
Motherhood for women with severe mental illness

Tab
le2
Exp
eriencingmotherhoo
d
Studies
Guilt
Custody
loss
Concern
over
impact
onchild
ren
Isolation
Dualidentities
Stigma
Centrality
ofmotherhood
Ackerson(2003)
12outpatient
mothers
with
SMI,psychotic
orsevere
mooddisorder
Guilty
that
illness
affectingparenting,
sometim
esadanger
tochild
ren
Custody
concerns
“anongoingstressor”
forlargemajority
Worried
illness
affected
ability
toparent,especially
todisciplin
e,and
someconcerned
dangerousto
their
child
ren
Com
binedin
them
es“strainof
single
parenthood
”and
“chaotic
interpersonal
relatio
nships”
Independentsense
ofselfaffected
bydependence
onchild
ren,
sometim
esrolesreversed
Increasedreluctance
toseek
help,children
also
suffer
Greatly
valued
closeness
tochild
ren,
pridein
beingamother
Alakuset
al.(2007
)Fo
cus
groups
ofmothers
with
under–5s,p
artof
“Parents
with
Psychosis”
Fear
child
renwould
beremoved
Somediscriminated
againstby
child
protectio
n,+social
stigmakept
them
athome
Bassettet
al.(1999
)2focus
groups,4
interviewswith
wom
enwith
SMIusing
community
rehabilitation
services
Thisfear
“permeated
alltheyhadto
say”
Fear
theirchild
ren
will
developmental
illness
Mostsinglemothers
who
feltvery
isolated
Difficultto
beyourself
whenscared
of“saying
thewrong
thing”
incase
seen
asunfit
parent
Oncepeople
knew
,they'dbe
treated
differently
andpeople
would
avoidthem
Relationshipwith
child
renextrem
ely
important
Chernom
aset
al.(2000
)28
outpatients18
with
schizophrenia,10
schizoaffectivedisorder
infocusgroups
Guilty
atbehaviour
whenill
Haunted
by“deep
senseof
loss,g
rief”
whenlostcustody:
noreason
toliv
e
Feared
child
ren
would
develop
schizophrenia
Overw
helm
ing
lonelin
ess
andisolationvery
pervasivein
this
group
“Strugglingto
integrate
theirexperience
ofbeingjudged
anunfit
mother”
Keensensitivity
tostigma,feltrejected
Manybenefits:“love,
purpose,identity
andsupport”
DaviesandAllen(2007)
11outpatientswith
SMIand
child
ren,
3with
psychosis,
2BD,1
OCD,5
depression
Felthadfailedto
live
upto
imageof
“goodmother”
Feltcouldn
’tbe
honest
aboutworst
symptom
s;“crushed”whenchild
removed
“Dualidentity
”of
mentalpatient
and
mother;beinga
“good”
or“bad”
mother'
Mentalillness
'not
part
oftheidealisationof
motherhood,
“felt
stigmatized
byhealth
professionals”
Being
forced
torelin
quishrole
ofmother,feel
afailu
re,
lowersself–esteem
Diaz-CanejaandJohnson
(2004)
22outpatients,8
with
schizophrenia,10
BD,
4MDD
with
psychotic
symptom
s
Conscious
ofbeing
“aburden
tochild
ren”
Pervasivefear
oflosing
custody“I'd
losteverything
intheworld”
Mostfeared
child
ren
would
becomeill,
forgenetic
orenvironm
ental
reasons
Major
them
ewas
social
isolation
Haveto
care
forchild
andsimultaneously
look
aftertheirow
nmentalhealth
—very
difficult
Mostthoughtstigma
exacerbatedproblems,
preventedthem
from
talkingopenly
20wom
ensaid
child
ren
hadgiventhem
apurposein
life,andalso
increasedself–esteem
Doucete
tal.(2012)
9wom
enwho
hadbeen
hospitalized
forPP
P
Preferredsupportof
family
andpartneras
anxiousabout
strangers
Needed'affirmational'
supportthat
would
return
to'normal'
Mainproblemsdueto
ignoranceof
severity
ofPP
P:confused
with
PND
bymany
Somefeltdenial
ofrole
asmotherbecausebaby
takenaw
ayfrom
them
even
temporarily
Edw
ards
andTimmons
(2005)
6form
erMBU
patients,3PP
P,1
depressive
psychosis,
2severe
PND
Guilty
that
they
“couldn’tc
ope
asamother”
Halfdistraught
that
baby
would
beremoved
into
care
ofothers
Feltupsetthat
their
illness
leftthem
unable
tocare
for
child
properly
Thisgrouphadgood
family
support
Worried
was
abad
parent:upsetthat
didn
’tfeel
able
tocomfortchild
Allexperienced
stigma,
madethem
revise
their
ownstigmatizingview
s+
feelinga“bad
mother”
was
self-stigmatising
Inability
tobe
a“supermom
”made
them
feel
worse
Engqvistet
al.(2011b)
10internet
narratives
ofwom
enwith
PPP
8described
sham
eandguilt
atinfanticidal
thoughts
Feared
would
lose
thebaby
ifthey
shared
disturbing
thoughts
Feltwell-supportedby
family
andpartner
Pervasivesenseof
sham
eandguilt
self-stig
matising
as“failed”
mothers
2wom
enhadstrong
bondswith
baby,even
whenpsychotic,m
ost
feltdetached
Heron
etal.(in
press
2012
)5wom
enwho
experiencedPP
P
Allfeltguiltyat
beingapoor
mother,letting
child
,spouseand
family
down
2wom
enspokeof
worryingabout
“the
genetic
side
ofthings”
Allstressed
importance
offamily
support,
post-discharge
felt
isolated
Identityas
probable
good
mother
“devastated”,struggle
tocometo
term
swith
being“m
ental
patient”
Referredto
asaproblem,
partly
asso
differentto
PND;andforpartners
Hugeguilt
becauseso
wantedto
care
for
baby
—fulfillingrole
of“ideal
mother”
very
important
Khalifeh
etal.(2009
)18
mothers:2with
schizophrenia,6BD,
10MDD
Guiltat
“failin
gas
amother”
Reluctant
toseek
parentinghelp
dueto
fearsof
custodyloss
Awareunable
tocare
foranddisciplin
echild
ren,
also
worried
exposing
them
to
Appreciated
praise
from
staffasconcerned
a“bad”mother
Stigmatised
bypartners
aswella
scommunity
:“H
esaid
‘you
’remad,
wedon’tw
antyou’”
Didn’tw
antto
lose
child
renbutsom
eunhealthily
dependent:
“som
etim
esIam
the
C. Dolman et al.

Tab
le2
(con
tinued)
Studies
Guilt
Custody
loss
Concern
over
impact
onchild
ren
Isolation
Dualidentities
Stigma
Centrality
ofmotherhood
distressingbehaviour
andburdeningthem
child
,and
he’sthe
parent”
Meiseret
al.(2005
)perceivedgenetic
risk
ofBD:10
euthym
icBipolar
wom
en
Halfsaid
illness
affected
decision
tohave
child
ren
butm
ostwould
not
aborta
ffectedfetus
Majority
believedgenetic
explanationforBD
isde
stigmatism
forsufferers
butnotsocially
Montgom
eryet
al.(2006
)20
outpatient
mothers:3
with
schizophrenia,4BD,
9MDD,4
unspecified
Someashamed
bythoughtsof
hurtingtheir
child
rendespite
loving
them
“Masked”
illness
toauthorities
orfamily
dueto
fear
ofcustodyloss
Awareof
need
toprotect
child
from
theirillness,
“theirprim
ary
responsibility”
Felt“never
good
enough
”as
amother,
“intensifyingtheir
effortsto
appear
norm
al”
Pressure
to“appear
norm
al”—
anxietythat
not“ideal
mother”
stressful
Motherhoodgave
life
meaning,identity
of“m
other”
signified
norm
alcy
andsecurity
—“our
kids
areour
life”
Montgom
eryet
al.(2011)
32mothers
with
SMI
inpatient
andin
community,C
anadian
Ministryof
Health
definitio
n
Tremendous
guilt.
Manyspokeof
being
ashamed:“Mychild
deserves
alot
better”
Fear
ofcustody
loss
whenvery
depressed
Idon'tw
antthekids
toseemesuffer
and
worry
aboutwhat
effect
itwill
have'
Neededto
talk
through
experience
ofhitting
“bottom”,oftennot
able
toas
isolated
Storiesof
hitting
“bottom”illustrated
“sense
ofpowerlessness
asboth
aperson
and
mother”
Felt“isolated”
and
“embarrassed”
bytheirillness
Allspokeof
the
importance
andvalue
oftheirrole
asmothers.
Mow
bray
etal.(1995
)24
mothers,1
5in
community.S
MI
accordingto
“agency
records”
Guilty
that
had“let
theirchild
ren
down.”
“Not
themotherI
hadwantedto
be”
Halfwould
liketo
send
theirchild
toseeamentalhealth
professional
asconcernedhow
they
hadbeen
affected
Single
mothers
feltthey
needed
supportfrom
thechild
ren'sfathers
Over2/3feltchild
ren
“motivated
them
togrow
anddevelop”
Joyof
motherhood.
Most
said
having
achild
had
“motivated”them
tobe
responsible;
“Iwas
the
happiestperson
onthe
face
oftheearth”
Nicholson
etal.(1998
)Fo
cusgroups
with
42mothers
incommunity
:23
affectivedisorder,
8psychotic
disorder,6
anxietydisorder,5
other
Tryingto
balance
parentingdemands
andillness
ledto
stress
andguilt
Constantly
need
toprovethem
selves
orwill
lose
child
ren.
Pain
oflosing
achild
nevergoes
away:
“Myheartisin
chains”
Sometim
esmisinterpret
norm
alproblemsas
relatedto
theirillness:
“Because
Ihave
amentalillness,h
aveI
raised
herwrong?”
Pridein
beingaparent
“can
beapowerful
motivatingforce”,
butmanyconfront
“rolestrain
issues”
Undermined
bysocietal
stigma:
“People[think]
we're
goingto
abuse
ourchild
ren”
“Unm
itigatedenthusiasm
”fortalkingabouttheir
child
renshow
nin
focus
groups
Peay
etal.(2009
)20
wom
enwith
BD50%
with
child
ren
Large
majority
concerned
aboutchild
ren'srisk
ofinheritin
gpsychiatric
illness
Robertson
andLy
ons
(2003)0sufferersof
PPP
Guiltat
possible
effect
oninfants,
distress
tofamily,
guiltythat
“bad
mother”
Worried
illness
may
have
adetrim
entaleffect
onchild
'sdevelopm
ent
Wom
endescribed
feelings
ofisolation
andbeingscared
“Regaining
self”:
wom
enfeltthey
hadlosttheirminds
andidentity.To
oktim
eto
regain
self-
confidence
that
could
begood
mother
Stigmaandlack
ofunderstandingfrom
friends.Self-stig
matised
somoreisolated
Devastatedthat
hadnot
lived
upto
“Western
idealof
motherhood”
butmostfelthadmade
itup
tochild
renwhen
recovered
Sands(1995)
10single
mothers
livingin
residential
programme:
6schizophrenia,
1schizotypalpersonality
disorder,1
MDD,1
BD,
1unknow
n
Wom
ensensitive
abouttheirlosses
butn
eededto
resolvethem
Socially
isolated
butd
ependent
onrehabilitationservice
“Viewed
selves
aschild
ren”:feltthey
weretreated“likea
baby
”andsome
expected
child
ren
tolook
afterthem
whenolder
Saw
“ childbearingand
parenthood
aswaysto
affirm
theirnorm
alcy”
Forall,child
ren“central
totheirliv
es”,gave
them
“meaning
and
focus”.
Somereliedheavily
onchild
renforsupport:6
hopedthey'dtake
care
ofthem
Savvidou
etal.(2003
)20
mothers,1
3liv
ingwith
child
ren:
10schizophrenia,
Manywho
lostcustody
indivorcespokeof
theirgrief:“the
Imagined
child
renhaving
problemsdueto
their
mother's
illness
Someisolated
from
child
renby
ex-
partners.
Illnessmadeithard
tohave
amother/child
relatio
nship:
“when
Greek
cultu
resees
wom
enwith
SMIas
“incapable
mothers”.Hardto
maintain
Most“viewed
child
ren
asoffering
prim
aryjoy
totheirparents”
and
Motherhood for women with severe mental illness

women, notably those who had postpartum psychosis (PPP),felt they had failed their children by being separated fromthem for a time as infants: “I still have pangs of guilt that shewas in there [hospital] and cared for by members of staff andnot me” (Robertson and Lyons 2003, p. 423). Many wereashamed that they “couldn’t cope as a mother” (Edwardsand Timmons 2005) or that they hadn’t lived up to thesocietal “ideal of motherhood”: “I felt a failure, here wego again, I’m a failure as a mother” (Davies and Allen 2007,p. 369).
Of the studies addressing parenting, several quotedwomen who worried about the impact of their childrenseeing their illness: “I don’t want them to see me in a badway, as I saw my mother. Therefore I did not want thatburden put on them” (Diaz-Caneja and Johnson 2004, p.476). Some mothers regretted that their illness had forcedtheir children to take on too much responsibility in thehome: “My kids have had to come home and, you know,had to help with the housework” (Ackerson 2003, p. 115).Others felt guilt that their illness-driven behaviour wasbad for their children: “I feel guilty a lot of the timebecause I get irritable with them” (Wilson and Crowe2009, p. 880). Notably, Venkataraman and Ackerson’sstudy (2008) focusing on women with a diagnosis ofbipolar disorder highlighted participants’ guilt at “settinga bad example” when manic and overspending, gambling,etc. (p. 396).
Custody loss
Fear of custody loss was related to severe chronic ill-nesses, with most studies reporting it as a concern. InAckerson’s (2003) study, for example, 11 of the 12participants were worried about losing custody; this wasnot without reason as seven had lost custody of a childat some point. Bassett said this fear “permeated all theyhad to say” (Bassett et al. 1999). This fear of losing theirchild affected communication with care professionals,with some mothers saying they masked their symptomsbecause of it (Montgomery et al. 2006), while it madeothers reluctant to seek help (Khalifeh et al. 2009). InSands’ (1995) study, most interviewees struggled tomaintain custody and were traumatized by separation,and Savvidou et al. (2003) reported how traumatic mostwomen found this: “the greatest pain I’ve been through,drugs, prison, psychiatric clinics etc., was the loss of mychildren” (p. 397). For a number of the women withschizophrenia interviewed by Chernomas et al. (2000),the loss of a child was almost unbearable: “You start toget feelings for them, and then they’re gone, and youdon’t think you have a reason to live…” (p. 1519). Afew papers included the comments of women who hadpermanently lost custody (Diaz-Caneja and JohnsonT
able
2(con
tinued)
Studies
Guilt
Custody
loss
Concern
over
impact
onchild
ren
Isolation
Dualidentities
Stigma
Centrality
ofmotherhood
4BD,3
MDD,2
borderlin
epersonality
disorder,1
delusional
disorder
greatest
pain
I'vebeen
through
…was
loss
ofmy
child
ren”
Socially
ostracised,
reliedon
theirfamily
weneed
you,
you
arealwaysill…”
family
andsocial
relatio
nships
becauseof
stigma
said
mothering
was
importantto
them
.“I
wouldn'tbe
alive
with
outmychild
”.
UenoandKam
ibeppu
(2008)
20outpatient
Japanese
mothers:1
3with
schizophrenia,
7mooddisorders(D
SM)
Rem
orse
that
their
illness
affected
child
renand
madethem
sad.
Lessfear
ofcustody
loss,asow
nmothers
caredforthem
and
child
renwhenneeded
Feltsorryformaking
thechild
distressed,
forexposing
them
tosymptom
sandfor
stigmachild
faced
Lessisolated
astheir
mothers
steppedin
tohelp,b
utsocially
stigmatised
Feltneed
tobalance
“self-care”andcaring
forthechild
Someworried
child
would
bestigmatised:“M
ychild
hatesthat
Ihave
thisaw
ful
disorder”
Allexpressedgreatlove
fortheirchild
ren:
“Mychild
isthemost
importantthingin
mylife”
Venkataraman
and
Ackerson(2008)
10wom
enwith
BD
incommunity
Feltguiltyat
setting
abadexam
ple
whenmanic
and
overspending
etc.
Prepared
torenounce
alcoholism
orabusive
relatio
nships
tokeep
custody
Anger
anddepressive
behaviourhadnegativ
eim
pact
onchild
,and
ledto
poor
disciplin
e
Talked
abouttheir
“positive
personality
traitsas
strengthsin
parenting”
Alltalked
positiv
elyabout
beingamother:“T
here
isno
man
ontheface
oftheearthmoreim
portant
than
mygirls”
Wilson
&Crowe(2009
)4wom
enwith
BD
incommunity
Self-blame:
“Ifeel
guiltyalotof
the
timebecauseIget
irritablewith
them
”
Lackof
moderationcan
lead
toundisciplin
edandpoor
parenting,
feltshould
model
self-control
Veryaw
areof
need
tobe
“moderate”
and
monito
rtheir
emotions,
leadsto
“problem
atic
identityas
aparent”
Felt“judgedas
abadparent”
becauseof
theirdiagnosis.
Stigmaledto
“self-
surveillance”
SMIsevere
mentalillness,B
Dbipo
lardisorder,P
PPpo
stpartum
psycho
sis,MDD
major
depressive
disorder,M
BU
motherandbaby
C. Dolman et al.

Table 3 Pregnancy and motherhood for women with severe mental illness: experiences of services
Studies Problems with service provision Positive experiences ofservice provision
Ackerson (2003) 12 outpatientmothers with SMI
Delayed diagnosis, inconsistency of care,need for childcare in crises
Those accessing rehabilitationservices more likely to mentionprofessionals as supportive
Alakus et al. (2007) Focus groupsof SMI mothers with under–5s
Need for better inter–agency communication,more information on discharge, and supportgroups for preschool parents
Bassett et al. (1999) 2 focusgroups, 4 interviews with womenwith SMI in community
Upset at constantly changing staff, better accessto crisis help
Would benefit from contact withothers in same situation, onemother appreciated having aconstant case manager to talk to
Chernomas et al. (2000) 28outpatients with schizophreniain focus groups
Poor communication with professionals:reluctant to talk about parentingproblems as no time
Individual good experience: “I likehim as a doctor, he's very goodwith my schizophrenia”
Davies and Allen (2007) 11outpatients with SMI and 1or more children
Need to “manage identity” with clinicians,felt they failed to take women with SMIseriously as “expert” mothers
Individual health visitor praised fornoticing woman's needs as well asbaby's, and allowing time to talk
Diaz-Caneja and Johnson (2004)22 outpatients, 8 withschizophrenia, 10 BD, 4 MDD
unmet needs for consistent support in thecommunity, creches for doctor's appointments,parenting support and peer groups
Generally satisfied with treatment
Doucet et al. (2012) 9 women whohad been hospitalized for PP
Upset that put on general psychiatryward and not allowed to see their baby.Little community support
Edwards and Timmons (2005)6 former MBU patients
5 women said illness severity not recognisedso treatment delay
Diagnosis “label” found usefulby some women
Engqvist et al. (2011b) 10 internetnarratives of women with PPP
Most women angry and not listened to by staff,who were not well informed about PPP
Minority satisfied with inpatient care
Heron et al. (2012) 5 women whoexperienced PPP
All felt should be able to have baby with them.Shock at professionals' ignorance of PPP,wanted more information and support groups
Valued specialist care if in MBU
Khalifeh et al. (2009) 18 motherswith SMI treated at home in a crisis
Preferred home treatment but children preferredit if mothers hospitalised
Those treated in a Crisis House preferredit to hospital or home treatment
Meiser et al. (2005) The authorsperceived genetic risk of BD: 10euthymic Bipolar women
Ignorance of real risks of passing on BDshould be addressed
Majority satisfied that prenatal testingnot offered
Montgomery et al. (2006) 20 motherswith severe mental illness (outpatients)
Saw professionals as not fully understandingtheir desire to be good mothers: “your kidswill grow up fine without you”
Wanted help with parenting when ill– if available, felt they would copebetter
Montgomery et al. (2011) 32 motherswith SMI inpatient and in community
External stressors, esp. social services,exacerbated descent into severe depression
Mowbray et al. (1995) 24 motherswith SMI, 15 in community
Services often unaware they were mothers. Morehelp for children and practical support needed,parent support groups desirable
Nicholson et al. (1998) 42 motherswith SMI in focus groups
Lack of childcare provision if need to be hospitalized– may delay help seeking
Vast majority welcomed focusgroup disappointed not regular
Peay et al. (2009) 20 women withBD 50% with children
Wanted general information on genetic risk andcounselling
Robertson and Lyons (2003)10 sufferers of PPP
Some upset that treated in psychiatric unitnot MBU, and wanted more information onPPP for themselves, family and partners
Sands (1995) 10 single mothers living insupportive residential programme
Resentful of mental health programmes,including social rehabilitation
Appreciated stability of rehabilitationprogramme allowing them to keepcustody of children
Savvidou et al. (2003) 20 Greek motherswith SMI, 13 living with children
Tried to conceal illness to avoid custodyloss, most felt their opinion s ignored indecisions about the children
Social services helped them to keepin contact with children
Ueno and Kamibeppu (2008) 20 Japanesemothers with SMI
Need for parenting education
Motherhood for women with severe mental illness

2004; Savvidou et al. 2003), and the emotional toll thishad taken: “A deep sense of loss, grief and some angerhaunted the women who had lost children to child andfamily services. Years later, these women were still strug-gling to process and integrate their experience of beingjudged an unfit mother” (Chernomas et al. 2000).
Concern over the impact on the child
This consisted of three sub-themes:
& Genetic — that a child may have inherited her mentalillness. Although only two papers focused on geneticsexclusively (Meiser et al. 2005; Peay et al. 2009), thisfeatured as a concern in several other studies (Bassett et al.1999; Chernomas et al. 2000; Diaz-Caneja and Johnson2004; Heron et al. 2012; Mowbray et al. 1995). In Peay’sstudy on the perception of genetic risk among peoplewith bipolar disorder, a large majority were concernedabout their children’s risk, and Meiser’s interviewswith the same diagnostic group found that half thewomen said it had affected their decision whether ornot to have children. It is worth noting that in boththese studies, a significant proportion had a strongfamily history of mental illness (in Meiser’s study, allhad at least two affected relatives), so their awarenessof the condition’s heritability would have been greaterthan for many women with SMI.
& Environmental — for example, that a mother’s periodicinability to care properly for her child might causesignificant developmental damage (Mowbray et al.1995). Many were worried about the generally detrimen-tal effect of their illness on their children (Ackerson2003; Robertson and Lyons 2003; Ueno andKamibeppu 2008). Some women were worried about thepsychological impact of their child witnessing frighteningbehaviour (Diaz-Caneja and Johnson 2004), others by thelack of a “normal” childhood (Ackerson 2003) and theburden placed upon the child to care for their mother: “it’salmost like sometimes I am the child, and he’s the parent”(Khalifeh et al. 2009, p. 636).
& Secondary stigma — by the child’s association with a“mad mother”. For example, Ueno and Kamibeppu(2008) say their interviewees “worried that their childrenmay be stigmatized as ‘a child of a mother with a mentalillness’” and quote a woman saying “I think my childhates that I have this awful disorder” (p. 526). Oneparent described harassment and verbal abuse that herdaugh te r expe r i enced a t schoo l and in herneighbourhood, forcing them both to become reclusive(Ackerson 2003). Other studies concerned with parent-ing also noted the impact of stigma on children and thepossibility that others would reject them: “If othermothers knew I had a mental illness, they might notallow their children to play with mine” (Diaz-Canejaand Johnson 2004, p. 476).
Isolation
Women returned frequently to their feelings of isolation. Sub-themes related to the damage done to social and family re-lationships by their illness and the difficulties of raising chil-dren alone. Many had no one to talk to (Montgomery et al.2006), and felt very isolated (Bassett et al. 1999). “Pervasivein this group [28 women with schizophrenia] was an over-whelming sense of loneliness and isolation” (Chernomas et al.2000). Because of their illness, they often had poor socialnetworks and meager financial resources, and many spoke ofhow much more difficult it was to parent alone, especiallywhen they were ill (Khalifeh et al. 2009; Nicholson et al.1998; Sands 1995; Savvidou et al. 2003). These studies gen-erally involved women with the most severe enduring illness,including a high percentage of women with schizophrenia.This contrasted with the women who had PPP who reportedstrong family support networks (Doucet et al. 2012; Heron etal. 2012; Robertson and Lyons 2003).
Coping with dual identities
Combining the persona of “woman with mental illness” withthat of “mother” had both negative and positive effects on
Table 3 (continued)
Studies Problems with service provision Positive experiences ofservice provision
Venkataraman and Ackerson (2008)10 women with BD in community
Wanted more crisis help for themselvesand children, help with parenting andpeer support groups
Wilson and Crowe (2009) 4 womenwith BD in community
Felt professionals judging them as inadequateparents: “I felt like he was blaming me —that … I had deliberately ruined … this child”
SMI severe mental illness, BD bipolar disorder, PPP postpartum psychosis, MBU mother and baby unit
C. Dolman et al.

identity: “I felt 100% female, I felt complete, a woman”(Diaz-Caneja and Johnson 2004, p. 475). Some studiesreported the added pressure to be a “perfect” mother: “Ihad this vision of, picture of how I would be as a motherand I didn’t live up to that expectation, so it made mefeel quite bad” (Edwards and Timmons 2005, p. 477).Sometimes this is viewed positively: Nicholson et al.(1998) quotes a woman saying “I think sometimes wemake the better parents because it is so hard to be likethis and we have to try twice as hard” (p. 638). Othersreported that motherhood “motivated them to grow anddevelop” (Mowbray et al. 1995; Nicholson et al. 1998).Having interviewed and observed ten chronically mentallyill mothers in a supported residential programme, Sands(1995) suggested that they “saw childbearing and parent-hood as ways to affirm their normalcy [as] parenthood isa pervasive human activity that connects one with thecommunity” (p. 94).
Altogether, identity issues were referred to in themajority of papers, and it was a particular problem forwomen whose first experience of SMI came immediate-ly after childbirth. Heron et al. (2012) described theshocking experience of suffering a PPP, especially withno history of mental illness, as “an affront” to one’ssense of personal and social identity (p. 9). Womeninterviewed by Robertson and Lyons (2003) describeda theme of “regaining self” as they gradually recovered(p. 423).
Centrality of motherhood
Eighteen of 23 studies highlighted the importance of being amother to women with SMI. This had negative implicationswhen women were forced to relinquish their mothering roledue to illness as it led to feelings of failure and lowered self-esteem (Edwards and Timmons 2005; Heron et al. 2012;Montgomery et al. 2011). This differed somewhat betweenwomen with a disabling chronic psychotic illness andwomen with an episode of PPP — a severe episodetriggered by childbirth from which they had recovered.The former group often experienced a lifelong struggle tocope with parenting, often alone and impoverished(Chernomas et al. 2000; Diaz-Caneja and Johnson 2004).The PPP group, in contrast, reported much better familyand social support. Many in this group were upset thatbecoming a mother had not been the “perfect” experiencethey had expected: “My sisters had babies and nothing’sgone wrong, it was just me…” (Robertson and Lyons2003, p. 420).
The vast majority of studies conveyed the positive effectof becoming a mother. The studies with the most severely illsamples, such as Chernomas et al. (2000) — 28 outpatientswith schizophrenia — and Sands (1995) — ten single
mothers with SMI in a residential programme —contained particularly positive affirmations of the centralrole children played in these women’s lives. Indeed, thelatter study, which used a comparison group of wellmothers attending a day-care centre, found that thewomen with SMI regarded being a mother as the mostimportant thing in their lives: “in contrast with … theday-care mothers [who] expressed more ambivalenceabout being a parent. […] One way or another, all thementally ill mothers said that being a mother was cen-tral to their existence, that it gave meaning and focus totheir lives” (Sands 1995, p. 90).
Experiences of services
The two themes which have been combined under thisheading are: (a) Problems with service provision and (b)Positive experiences of services (Table 3).
Problems with service provision
Twenty two out of 23 studies reported problems withthe provision of services, ranging from difficulties withinteracting with medical staff (Wilson and Crowe 2009;Engqvist et al. 2011b; Davies and Allen 2007) to feel-ing upset by the frequent changes in personnel (Bassettet al. 1999). This theme also included the differenttreatment needs of women with PPP, who complainedof treatment delay due to misdiagnosis (Edwards andTimmons 2005) and not being able to have their babywith them in hospital (Robertson and Lyons 2003). Twostudies cited drug side effects as impairments to parent-ing which were not fully recognized by professionals(Mowbray et al. 1995) and (Savvidou et al. 2003), andsome reported the need for more practical help during acrisis, such as childcare provision (Diaz-Caneja andJohnson 2004; Nicholson et al. 1998; Venkataramanand Ackerson 2008).
A major sub-theme in the negative experiences ofservice provision was the unmet need that many womenidentified for both information and peer support groups.The majority of researchers asked women what they feltwould improve their lives in relation to becoming par-ents, and many suggested well-written information ondischarge, especially on parenting issues (Heron et al.2012). Mothers who had suffered PPP were keen formedical professionals to receive better training about thecondition (Edwards and Timmons 2005; Engqvist et al.2011b).These mothers also wanted peer support groupsas they felt isolated, even from the larger group ofmothers who had suffered from postnatal depression, forwhom there was felt to be more support (Heron et al. 2012).
Motherhood for women with severe mental illness

Generally mothers with SMI were enthusiastic about peersupport (Alakus et al. 2007; Mowbray et al. 1995;Venkataraman and Ackerson 2008). This would give themthe opportunity to “share their experiences and obtain guid-ance about coping with parenting” (Diaz-Caneja and Johnson2004), and so could be viewed as an informal method ofparenting education, which was also a popular request(Ueno and Kamibeppu 2008; Venkataraman and Ackerson2008). Some expressed a preference for diagnosis-specificgroups (e.g., women with bipolar disorder interviewed byVenkataraman and Ackerson 2008).
Positive experiences of services
Many studies gave examples of positive experienceswith services but these were usually at the level ofindividual healthcare professionals rather than thehealthcare system (Bassett et al. 1999; Chernomas etal. 2000; Davies and Allen 2007; Savvidou et al.2003). An emergent sub-theme was the desire to talkregularly to someone sympathetic; when this was avail-able it was appreciated: “To have someone you can talkto and trust like I can with my case manager … thatmakes me stable” (Bassett et al. 1999, p. 601). Where special-ist services were available, for example a Mother and BabyUnit (Heron et al. 2012), rehabilitation service (Ackerson2003) or Women’s Crisis House (Khalifeh et al. 2009), wom-en were appreciative. Of the 42 women included in focusgroups by Nicholson et al. (1998), the vast majority welcomedthe opportunity to discuss issues with other mothers with SMI,and were disappointed that it was not a regular part of recov-ery programmes.
The views of health professionals on the pregnancyand childbirth issues of women with severe mental illness
Using the same databases as above, a second search wasperformed (Fig. 2). We identified eight papers whichinvestigated health professionals’ perspectives (Table 4).Of note however, is that four of these papers were byEngqvist and colleagues in Sweden focusing on healthprofessionals caring for women with PPP. Two of thesestudies used the same dataset to describe the experiencesof psychiatric nurses and the later two used anotherdataset to describe the experiences of psychiatrists. Oneof the three UK papers described perinatal psychiatricand antenatal workers (see Table 4) caring for womenwith SMI (Wan et al. 2008), and the other addressed theattitudes of mental health nurses towards severe perinatalmental illness (McConachie and Whitford 2009) andtowards caring for psychiatric patients who were alsoparents (Maddocks et al. 2010). The American paper
reported on focus groups with psychiatric case managersas well as groups of mothers with SMI, described earlier(Nicholson et al. 1998). Table 5 displays the four themeswhich emerged from a synthesis of these papers:Discomfort (comprising Anxiety and Additional responsi-bility), Stigma, Need for education, and Integration ofservices. These were further synthesized into two super-ordinate themes: Experience of professionals, comprisingDiscomfort and Stigma, and Views on service provision,combining the latter two.
Experience of professionals
Discomfort
Two themes that emerged under the heading of “experience”were Anxiety and Additional Responsibility, whichoverlapped to the extent that they have been combinedunder the superordinate theme of Discomfort.
Anxiety
McConachie and Whitford (2009) found that generalpsychiatric nurses “had little experience and felt uneasyworking with women who had an SMI in the perinatalperiod” and were “frightened” of looking after a baby. “Ithink it is stressful … I feel responsible … my worriesand anxieties go up right away” (Community nurse, p.871). Similarly, Wan et al. (2008) revealed the anxiety ofmidwives when dealing with women with schizophreniaas they felt inadequately trained for the task: “Whensomebody says schizophrenia, especially in midwifery,people get frightened because they think they’re symp-tomatic …. I think we need more awareness sessions formidwifery” (registered mental nurse working in the ante-natal clinic, p. 179). The psychiatrists interviewed byEngqvist et al. (2011a) felt burdened by a feeling of“great responsibility” for both mother and child whenmaking decisions. The psychiatric nurses in the 2009Swedish study spoke of the “strong emotions” they felttreating women with PPP, including “sadness, sympathy,empathy, compassion, discomfort, anger, anxiety and hap-piness”. One nurse said: “often the women have a veryextroverted chaotic behavior, hard to work with, creatingmuch anxiety in both me and others” (Engqvist et al.2009, p. 27). Several were anxious about the responsi-bility of keeping the women and their babies safe, andtwo nurses described being angry with a mother whodrowned her baby. Engqvist and colleagues suggest edu-cators should address this problem as these negativelycharged emotions “could interfere with providing com-passionate and effective nursing care”.
C. Dolman et al.

Additional responsibility
For five of the studies analysed, the difference for staffwas the need to care for an infant as well as an adultpatient; however, the converse applied for the midwives inthe study of Wan et al. (2008), who found it challengingto care for a new mother who was also mentally ill. Forexample, asked to recommend an intervention for motherswith schizophrenia, a midwife responded: “I don’t knowenough about mental health…. I think generally peopleare more sympathetic to people that have a physicalillness … as opposed to mental illness” (p. 181). In thetwo Swedish papers analysing interviews with nurses ex-perienced in caring for women with PPP, the nurses foundthat “they need to address the relationship between thewoman and her child… [the nurse] becomes a model forthe patient of how to care for her baby… ‘and by sodoing I try to encourage this type of contact’” (Engqvistet al. 2007, p. 1337). The psychiatrists (Engqvist et al.2011a) describe being more involved with these womencompared with other patients “because there is so much atstake. It is not just a woman with psychosis but also herchild and its earliest experiences which are so extremely
important” (p. 77). Nicholson et al. (1998) reported thatcase managers “expressed a great deal of concern for thechildren” of mothers with SMI, and felt that the womendid not have enough resources to help them cope. Thiswas echoed by psychiatric nurses in the Maddocks study(2010): “I used to find it quite difficult because … youwant to support them but you have to think about thechild, you have to think about their safety, their future andtheir emotional needs as well” (p. 678). Psychiatric nursesquestioned on their feelings about caring for women withSMI in the perinatal period (McConachie and Whitford(2009) saw this as very challenging. They were “fright-ened about looking after babies” and felt insufficientlytrained: “No, I don’t do mothers and babies, no seriouslyI know my limitations, I would not take that on. I wouldfeel very uncomfortable” (p. 870).
Stigma
All studies referred to stigma as an issue. Wan et al.(2008) described “perceived ignorance and social stigmaattached to mental illness” as one of two overarchingthemes that recurred across topics and across the range
Table 4 The views of health professionals caring for women with severe mental illness: summary of papers
Author Date Title Qualityappraisalscore
Number of participants Method
Engqvist et al.(Sweden)
2007 Strategies in caring for women withpostpartum psychosis — an interviewstudy with psychiatric nurses
42 10 psychiatric nurses Interviews
Engqvist et al.(Sweden)
2009 Psychiatric nurses’ descriptions of womenwith psychosis occurring postpartum andthe nurses’ responses — an exploratorystudy in Sweden
40 10 psychiatric nurses Interviews
Engqvist et al.(Sweden)
2010 Nurses — psychiatrists’ main collaboratorswhen treating women with postpartumpsychosis
52 9 psychiatrists Interviews
Engqvist et al.(Sweden)
2011a Comprehensive Treatment of Women withPostpartum Psychosis across Health CareSystems from Swedish Psychiatrists’Perspectives
51 9 psychiatrists Interviews
Maddockset al. (UK)
2010 A phenomenological exploration of the livedexperience of mental health nurses who carefor clients with enduring mental healthproblems who are parents
45 6 psychiatric nurses Interviews
McConachie adWhitford (UK)
2009 Mental health nurses’ attitudes towardssevere perinatal mental illness
48 16 psychiatric nurses 3 focus groups
Nicholsonet al. (USA)
1998 Focus on women: mothers with mentalillness: The competing demands ofparenting and living with mental illness
51 55 Mental HealthCase Managers
5 focus groups
Wan et al. (UK) 2008 The service needs of mothers withschizophrenia: a qualitative study ofperinatal psychiatric and antenatal workers
48 28:15 midwives, 7Reg. Mental Nurses,3 MBU nursery nurses,1 antenatal manager, 1obstetrician, 1 psychiatrist
Interviews
Motherhood for women with severe mental illness

Tab
le5
The
view
sof
health
profession
alscaring
forwom
enwith
SMI
Stud
ies
Exp
erienceof
profession
als
Viewson
serviceprov
ision
Discomfort
Anx
iety
Add
edrespon
sibility
Stigma
Needforeducation
Integrationof
services
Eng
qviste
tal.(20
07)
10psychiatricnu
rses
interviewed
(9female
1male)
Needtocareforbaby
too+provide'amodel'
form
other,+educate
family
aboutpostpartum
psychosis
Who
letreatm
entteam
needsto
co–op
erate.Nurse
actsas
link,
coordinatin
gafter–care
Eng
qviste
tal.(20
09)
9psychiatricnu
rses
interviewed
(8female
1male)
8describ
edhaving
“stro
ngresponses”
including
“discomfort,
angerand
anxiety”
Needto
foster
mother's
relatio
nshipwith
baby,
manywom
en“disconn
ected”
from
child
.Feel'terrific
burden
andsenseof
respon
sibility'
Nurse
educationneeded
toaddressnegativ
efeelings
towards
motherswith
SMI,help
them
develop
strategies
tocope
Eng
qviste
tal.
(201
0)9psychiatrists
interviewed
(5male
4female)
Psychiatrists'ex
pressed
doubtsconcerning
their
ownpractice,andinsecurity
aboutm
akingthebest
treatmentd
ecisions'
Believednu
rses
needed
tobe
able
toassess
interaction
betweenmotherandherchild
“Thisisno
troutine
care”nu
rses
need
good
know
ledg
ebase
ofPP
P
Outpatient
clinic
team
follo
wup
for6–
12mon
ths+collabo
rate
with
child
care
centre.
Recog
nise
theim
portance
ofinvo
lving
family
Eng
qviste
tal.(20
11a)
9psychiatrists
interviewed
(5male
4female)
Moreinvolved:focused
on'protectingwom
enwith
PPPfrom
suicide
andinfanticide'
Con
cern
forbaby
'ssafety
+risk
ofsuicide—
feel
very
respon
sibleas
“somuch
atstake”
Keento
give
accurate
diagno
sis“asthis
diagno
siscanbe
stigmatizing”
Services
should
consider
providingsupportand/or
peer
supervisionfor
professionalsin
thisfield
Und
erscored
impo
rtance
ofinclud
ingfamily
intreatm
ent
plan
anddischargeplanning
process
Maddo
ckset
al.(20
10)
6psychiatricnu
rses
interviewed
(genderun
specified)
Unsurehowinvolved
with
patientsas
parents:“Ithink
alotofnursesarefrightened
ofit”
Awareof
child
protection
responsibilities:“you
have
tothinkabout[thechild's]
safety”
Worriedabouttheirlack
ofknow
ledgeandtraining
regardingchildren:“I'm
notconfid
entatitbecause
I'mnottrained
init”
Num
erou
sreferences
madeto
theim
portance
ofliasing
with
otheragencies:“W
eneed
closer
working
relatio
nships
with
social
services”
McC
onachieandWhitford
(200
9)16
psychiatric
nurses
in3focusgrou
ps(14female2male)
Manyfeltvery
uneasy
working
with
wom
enin
theperin
atalperio
d;“they
werefrightened
about
lookingafterb
abies”
Needmoretraining
,better
integrationof
services:
frustrated
atlack
ofcollabo
ratio
nwith
otherservices
The
stigmatizationof
amentalh
ealth
referral
was
discussedin
all
grou
pswom
enmight
manipulateEPD
Sscore
toavoidlosing
custod
ybecauseview
edas
“poo
rmother”
Feltneeded
more
specialised
training,
especiallytocareforb
aby:
“Assessing
howsheis
carin
gforthechild
…we're
notq
ualifiedfor
that”
Identifiedprob
lemsof
accoun
tabilityandsharing
respon
sibility:
frustrated
at“lackof
commun
icationfrom
otherprofession
als”
C. Dolman et al.

of participant occupations (p. 182). Nicholson et al.(1998) quote a case manager saying: “It is always thestigma of being mentally ill. When [the mothers] go tothe hospital to give birth, people immediately assumethey cannot care for the child.” This stigmatizing atti-tude extended to healthcare workers and “sometimes ledto negative preconceptions among workers concerningthe abilities of mothers with SMI to be ‘good’ mothers,and to their negative treatment by workers”. Similarly,all three focus groups reported by McConachie andWhitford (2009) discussed the stigmatization of a men-tal health referral. They also raised the problem ofwomen manipulating their scores on the EdinburghPostnatal Depression Scale to avoid being seen as a“bad mother” and losing custody. Psychiatrists inEngqvist et al.’s (2011a) study felt extra pressure whendeciding on a diagnosis of PPP “as this disorder can bestigmatizing”. Thus medical professionals are aware ofthe stigmatization suffered by mothers with SMI, andare also aware of it occurring among health workers:“When somebody say schizophrenia, especially in mid-wifery, people get frightened because they think they’resymptomatic…. I think we need more awareness ses-sions for midwifery” (psychiatric nurse quoted in Wanet al. p179 (2008).
Views on service provision
Need for education
As may be seen from the quote above, some healthprofessionals saw a need for education as a means oftackling stigma, but other studies emphasised the otherareas training could address. The psychiatric nurses inMcConachie and Whitford’s 2009 study felt they neededmore specialized training to deal with mothers andbabies: “Caring for the women is alright – it is thebabies I don’t like (lots of laughter) it certainly poses achallenge. Assessing how she is caring for the child …we’re not qualified for that” (p. 870). The nursesinterviewed by Maddocks et al. (2010) felt ill-equippedto assess their clients’ parenting capacity: “I wouldn’tknow what to look for” (p. 679). The focus groups inWan et al. (2008) called for more psychiatric training formidwives as well as parenting education for patients, anda psychiatrist quoted in Engqvist et al. (2010) empha-sized that nurses caring for women with PPP needed tobe knowledgeable about the disorder: “This is not routinecare, the nurses must give top care to these patients” (p.498). Two other Swedish studies (Engqvist et al. 2009,2011a) brought out the theme of education as a means ofaddressing the anxiety suffered by professionals treatingT
able
5(con
tinued)
Stud
ies
Exp
erienceof
profession
als
Viewson
serviceprov
ision
Discomfort
Anx
iety
Add
edrespon
sibility
Stigma
Needforeducation
Integrationof
services
Nicho
lson
etal.(19
98)
55MentalH
ealth
Case
Managersin
5focus
grou
ps
Casemanagers“strug
gled”
with
clients'multip
leprob
lems+“exp
ressed
agreatdeal
ofconcern”
forthechild
renof
mothers
with
SMI
Managersspok
eof
additio
nal
concernforchild
reninvo
lved
andof
thelack
ofresources
tohelp
thewom
encope
Casemanager:“Itisalways
thestigmaof
beingmentally
ill.W
hen[the
mothers]go
totheho
spitalto
give
birth,
peop
leim
mediately
assume
they
cann
otcare
forthe
child
”
Somesugg
estedthey
them
selves
needed
moresupp
ort,requ
ested
training
sessions
Needform
oresupportservices:
“I'veseen
alotofm
othersgo
intocrisis,needing
hospitalizations
anddebating
which
shouldcomefirst,their
mentalhealth
orchild
care,
becausethey
hadno
oneinthe
community
thatcouldhelpthem
”
Wan
etal.(20
08)28
:15
midwives,7
Reg.
MentalNurses,3MBU
nurserynu
rses,1
antenatal
manager,1
obstetrician,
1psychiatrist
Midwives
anxiou
sthat
not
trainedto
recogn
iseor
nursepsychiatricpatients
Awareof
need
tomonitor
patients'mentalhealth
constantly:“Ithinkwefail
them
postnatally
…because
Ithink
theem
phasisdoes
goon
thebaby”
Perceivedignoranceand
stigmaattached
tomental
illness,including
among
healthcareworkers,identified
asmajor
reason
forp
oor
postpartu
mcare
Morepsychiatriceducation
formidwives
requ
ested
bymidwives
them
selves
andneed
forparenting
training
forpatients
Need“integratio
nof
services
andcontinuity
ofsupp
ort”,
mostfeltwom
enwith
schizoph
reniareceived
“insufficientpostnatalsupport”
SMIsevere
mentalilln
ess,MBU
motherbaby
unit,
EPDSEdinb
urgh
PostnatalD
epressionScale2
Motherhood for women with severe mental illness

women with PPP: “It is important to address these issuesin nursing education and in clinical practice” (Engqvistet al. 2009). For the psychiatrists interviewed in the 2011study, peer supervision or support was suggested, andsome American case managers “suggested they them-selves were not provided with adequate support for deal-ing with these issues” and were keen to join with theirpeers in a focus group discussion (Nicholson et al. 1998p. 41).
Integration of services
This theme echoes some of the comments about discon-nected services made by women with SMI under thetheme Problems with service provision: “It’s good net-working that we require with the services – primarycare, the GP and if there’s been a CPN involved andthe health visitor and the midwife” (antenatal managerquoted in Wan et al. 2008, p. 180). Psychiatric nurses(McConachie and Whitford 2009) also identified problemswith sharing responsibility: “There isn’t any information shar-ing … unless they’re looking for us to do something” (com-munity nurse, p. 871). This was echoed in Maddocks et al.(2010): “social workers for children might not necessarilyhave that great an understanding of adult mental health andvice versa. There needs to be common ground” (p. 679). TheSwedish studies also emphasized the need for the wholetreatment team to collaborate: “I think that it is possible tocooperate for a patient’s sake with all the different staff and thevaried areas of expertise” (Engqvist et al. 2007, p. 1337). Theyalso underscored the importance of including the family in thetreatment plan and discharge planning process (Engqvist et al.2011a).
Discussion
Main findings
We found that, despite the heterogeneity of samples andmethods in these studies, it was clear that the experi-ence of motherhood evokes powerful emotions forwomen with SMI regardless of diagnosis or socio-cultural context. Indeed there is some evidence (Sands1995) that women with SMI valued motherhood morehighly than other women, perhaps because they hadlittle else positive in their lives, or because the fear ofhaving them taken away made them appreciate them allthe more. Thus although no studies reported data relatedspecifically to pregnancy, the vast majority of studies(19 of 23) emphasized the importance women attachedto becoming mothers, both in terms of their own self-esteem, and in the way that their children were central
to their existence, conferring benefits such as “love, pur-pose, identity and support” (Chernomas et al. 2000).However, we also found that for many women, being aparent with a major mental illness is associated with stigma,guilt, isolation and concerns over the impact of illness ontheir children or the possibility of custody loss: a pervasiveanxiety for many women in these studies. Consultationswith health professionals for pre-conception advice, ante-natal care or mental healthcare while parenting may there-fore be influenced by these underlying concerns even ifthey are not disclosed during interviews (Davies andAllen 2007).
Stigma was a particularly prominent theme whichmay impact on access to healthcare. The stigma associ-ated with mental illness was exacerbated by becoming aparent (Wilson and Crowe 2009) as women felt doublystigmatized — by some health professionals as well associety generally — because their capacity to be “agood mother” was automatically doubted (Chernomaset al. 2000; Davies and Allen 2007; Edwards andTimmons 2005; Khalifeh et al. 2009; Wilson andCrowe 2009). This concurs with a recent quantitativesurvey which found that people with a mental illnessrated “being seen as a bad parent” as the second mostimportant barrier to seeking psychiatric care (Clement etal. 2012). This recurring theme overlapped with theconsciousness of having “dual identities” as a mentallyill woman who was socially stigmatized and in need ofthe State’s help, while at the same time trying to fulfilthe idealized role of extremely competent, nurturing andselfless mother.
Within the overarching theme of Experiences ofServices, prominent sub-themes were the lack of conti-nuity of care and the need for childcare provision,especially in a crisis, confirming earlier findings fromsurveys (Howard and Hunt 2008; Howard et al. 2001).An unmet need for information was also evident as inother types of studies (Howard and Hunt 2008), and aneed for peer support, which might prove particularlyhelpful to this population, isolated by both the stigma ofmental illness and the need to care for an infant fulltime. Unfortunately, there is a scarcity of good qualityresearch on whether such support could improve socialnetworks and childcare.
The singular experience of women suffering fromPPP was evident in several themes. For women whohad never experienced mental illness before and hadanticipated a “perfect” birth, the chasm between expec-tation and reality was especially hard to bear. Thuscomments on Guilt, the Centrality of Motherhood andCoping with Dual Identities were plentiful from thisgroup of women, whereas they were far less likely totalk about suffering from isolation as they generally
C. Dolman et al.

reported strong family support (Doucet et al. 2012;Heron et al. 2012).
Health professionals’ views overlapped with women’sviews in terms of their consciousness of stigma. Non-psychiatrically trained groups, particularly midwives, ac-knowledged that ignorance and stigma affected the poor post-partum care given to women with SMI (Wan et al. 2008).They concluded the best way to tackle this problem would beto provide more education in mental health. Parenting supportwas suggested by both women with SMI and professionalscaring for them, which supports the quantitative literature onthis subject (Miller 1997; Nicholson and Blanch 1994). It haspotential as an intervention, though more research needs to bedone on the efficacy of such interventions for women withSMI (David et al. 2011).
The challenges of treating severely ill women togetherwith newborns, and the safety issues that presents, camethrough strongly in the health professional theme ofDiscomfort as well as in some professionals’ requests forextra training to help them cope more effectively (Engqvistet al. 2011a; McConachie and Whitford 2009). Other sug-gestions from professionals included peer support and su-pervision for perinatal psychiatrists, and more psychiatriceducation for midwives (Wan et al. 2008) and socialworkers (Maddocks et al. 2010). This desire for more spe-cialist training for the professionals was echoed in some ofthe patients’ interviews (Engqvist et al. 2011b; Heron et al.2012). This is pertinent to the current international debateover whether perinatal mental health services should bespecialist and whether women should be treated inspecialised mother and baby units as occurs, albeit spo-radically, in the UK. The results of this review supportthe assertion of The National Institute for Health andClinical Excellence that staff should receive training onmental disorders and women with SMI should normallybe admitted to a specialist mother and baby unit (NICE2007, p. 14). Internationally there is an increasing aware-ness of the special needs of women with mental illnessin the perinatal period, as evidenced by recent guidelineson the subject such as SIGN in Scotland (ScottishIntercollegiate Guidelines Network 2012) and “BeyondBlue” in Australia (beyondblue 2011).
Evidence gaps
This review highlights notable gaps in the literature, forexample, the absence of research on preconception viewson motherhood among women with SMI, and how men-tally ill women who lose their children can be supportedby services (Stanley and Penhale 1999). Some researchhas been done on the characteristics of women with SMIwho lose custody (Hollingsworth 2004) but little has beendone on women’s own experience of separation from their
children, the effect it might have on their illness (Dippleet al. 2002) and how professionals should acknowledgethis and respond appropriately (Sands 2004). The efficacyof parenting interventions for women with SMI and theusefulness of peer support for this group would alsobenefit from more exploration (Nicholson et al. 1993).
Limitations of review
The studies reviewed were heterogenous in samples, meth-odologies and context. As is usual in qualitative research,many of the studies have small sample sizes and several didnot interview a representative mix of women. The majorityof studies did not differentiate between diagnoses whenreporting results, so it was not possible to distinguish be-tween the views of women with different conditions.However the two papers exclusively about bipolar disorderand parenting revealed the development of a heightenedawareness of the need to self-monitor moods (Wilson andCrowe 2009); and the possible advantages of hypomanicenergy when parenting (Venkataraman and Ackerson 2008).More research is needed to determine whether specific di-agnoses present particular problems in the perinatal periodand early years of motherhood.
Conclusion and implications
The particular needs of women with SMI when they havechildren has tended to be overlooked by professionals(Howard 2006; Krumm and Becker 2006), but there isnow a growing literature on their views which is synthesizedhere. This is the first systematic review to give an overviewof the qualitative literature in the area of women’s mentalillness in relation to having children from pre-conception toparenting. Despite the heterogeneity of the studies includedhere, this review highlights the complexity of the challengesfacing women with SMI when they have children and theways in which issues such as stigma and fear of custody lossmitigate against the establishment of a meaningful therapeu-tic relationship with health professionals. Research intopossible interventions such as preconception counselling,parenting programmes and peer support is needed. The re-sults emphasize the central importance women with SMIassign to motherhood (David et al. 2011; Dipple et al. 2002),a fact that should not be underestimated when caring for thispopulation. This review also highlights the level of anxietyhealth professionals from different disciplines experiencewhen caring for women with SMI in the perinatal period,and some of the interventions, such as improved specialisttraining and workplace peer support, which might address it.
Acknowledgments The authors thank Kylee Trevillion (KT) for herhelp with quality appraisal.
Motherhood for women with severe mental illness

Appendix
Quality Appraisal Form
Review ID:
Author Name:
Paper title:
Reviewer ID: CD
APPRAISAL
Please grade the answers to each question by ticking 0, 1 or 2. Unless otherwise specified, questions should be scored as follows: 0 – study does not meet criteria/answer question 1 – study partially meets criteria/gives a partially satisfactory answer to the question 2 – study fully meets criteria/gives a fully satisfactory answer to the question If a question is not applicable to a particular study, please mark “n/a” in the adjacent comments section.
1. The research presents clearly stated aims
Question Comments Score0 1 2
Is the study question focused in terms of the population studied?
Is the study question focused in terms of the outcomes considered?
Q1 Subtotal ………………..
2. A qualitative methodology is appropriate for this research (e.g., does the research seek to interpret or illuminate the actions and/or subjective experiences of research participants?)
Question Comments Score0 1 2
Was a qualitative methodology appropriate?
Q2 Subtotal ………………..
C. Dolman et al.

Continue only if score on each of questions 1 and 2 is one or more
3. The context of the research was clearly described
erocSstnemmoCnoitseuQ0 1 2
Was the context of the research clearly described?
Q3 Subtotal ………………..
4. The research design was appropriate to meet the aims of the research
Question Comments Score0 1 2
Was the research design appropriate to address the aims of the research?
Q4 Subtotal ……………….
5. Was the recruitment/sampling strategy appropriate to the aims of the research?
Q5 Subtotal ………………..
erocSstnemmoCnoitseuQ0 1 2
Does the study have clear inclusion criteria? Does the study have clear exclusion criteria? Was the sampling strategy appropriate for the aims of the research?Were the subjects appropriate for the aims of the research? Was the study sample representative of the research setting? Does the study report on the level of non-participation?
Motherhood for women with severe mental illness

6. Was the data collected in a way that addressed the research issue?
erocSstnemmoCnoitseuQ0 1 2
Is the study setting appropriate to the aims of the research? Is the method of data collection clear? Is the method of data collection appropriate to the aims of the research?Is the process of data collection clear? Were study instruments piloted? Is data saturation discussed?
Q6 Subtotal ………………..
7.
Comments Score0 1 2
Is the data verifiable? N.B. Data is audio or video taped (=2), researcher makes notes during data collection (=1).
C. Dolman et al.

Q7 Subtotal ………………..
8. Were ethical considerations appropriately considered?
Question Comments Score0 1 2
Did researchers obtain informed consent from all participants? Was data collected in a private setting?
Was data sufficiently aggregated during presentation to ensure anonymity?
Q8 Subtotal ………………..
Motherhood for women with severe mental illness

9. Was data analysis sufficiently rigorous?
erocSstnemmoCnoitseuQ0 1 2
Is the analytical process described in detail? Were steps taken to identify data that was contrary to the main findings and hypotheses of the study? Were multiple analysts used to increase the rigour of the research? Does the study report on level of inter-rater reliability?
Q9 Subtotal ………………..
10. Was there a clear statement of findings?
erocSstnemmoCnoitseuQ0 1 2
Does the study clearly report its findings?
Q10 Subtotal ………………..
11. How valuable was the research?
erocSstnemmoCnoitseuQ0 1 2
Were service users, providers or advocates involved in the development of the study? Were study participants invited to receive feedback on the research? Were the study findings disseminated beyond the academic community?
C. Dolman et al.

References
Ackerson BJ (2003) Coping with the dual demands of severe mentalillness and parenting: the parents' perspective. Fam Soc84(1):109–118
Alakus C, Conwell R, Gilbert M, Buist A, Castle D (2007) The needsof parents with a mental illness who have young children: anAustralian perspective on service delivery options. InternationalJournal of Social Psychiatry 53(4):333–339
Antenatal and Postnatal Mental Health Clinical Management and Ser-vice Guideline, National Institute for Health and Clinical Excel-lence (2007) http://www.nice.org.uk.
Bassett J, Lampe C, Lloyd H (1999) Parenting: experiences and feel-ings of parents with a mental illness. J Ment Heal 8(6):597–604
Beck CT (2002) Postpartum depression: a metasynthesis. Qual HealRes 12(4):453–472
BMJ (2011) Consolidated criteria for reporting qualitative researchhttp://bmjopen.bmj.com/content/suppl/2011/02/21/bmjopen-2010000017.DC1/bmjopen_research_checklist_000017.pdf
CASP: Critical Appraisal Skills Programme (2010) http://www.casp-uk.net/wp-content/uploads/2011/11/CASP_Qualitative_Appraisal_Checklist_. Accessed 11/2011
Chernomas WM, Clarke DE, Chisholm FA (2000) Perspectives of wom-en living with schizophrenia. Psychiatr Serv 51(12):1517–1521
Clement S, Brohan E, Jeffery D, Henderson C, Hatch S, Thornicroft G(2012) Development and psychometric properties of the barriers toaccess to care evaluation scale (BACE) related to people with mentalill health. BMC Psychiatry 12(1):36 http://www.biomedcentral.com/1471-244X/12/36
David DH, Styron T, Davidson L (2011) Supported parenting to meet theneeds and concerns of mothers with severe mental illness. Am JPsychiatr Rehabil 14(2):137–153. doi:10.1080/15487768.2011.569668
Davies B, Allen D (2007) Integrating 'mental illness' and 'motherhood':the positive use of surveillance by health professionals. A quali-tative study. Int J Nurs Stud 44(3):365–376
Dept of Health HG, UK (2003) Mainstreaming gender and women'smental health implementation guidance. London
Diaz-Caneja A, Johnson S (2004) The views and experiences ofseverely mentally ill mothers—a qualitative study. Social Psychi-atry & Psychiatric Epidemiology 39(6):472–482
Dipple H, Smith S, Andrews H, Evans B (2002) The experience ofmotherhood in women with severe and enduring mental illness.Social Psychiatry and Psychiatric Epidemiology 37(7):336–340.doi:10.1007/s00127-002-0559-2
Doucet S, Letourneau N, Blackmore ER (2012) Support needs ofmothers who experience postpartum psychosis and their partners.Journal of Obstetric, Gynecologic, & Neonatal Nursing
Edwards E, Timmons S (2005) A qualitative study of stigma amongwomen suffering postnatal illness. J Ment Heal 14(5):471–481.doi:10.1080/09638230500271097
Engqvist I, Ahlin A, Ferszt G, Nilsson K (2010) Nurses – psychiatrists'main collaborators when treating women with postpartum psy-chosis. J Psychiatr Ment Heal Nurs 17(6):494–502. doi:10.1111/j.1365-2850.2010.01549.x
Engqvist I, Ahlin A, Ferszt G, Nilsson K (2011a) Comprehensivetreatment of women with postpartum psychosis across health caresystems from swedish psychiatrists' perspectives. The QualitativeReport 16(1):66–83
Engqvist I, Ferszt G, Ahlin A, Nilsson K (2009) Psychiatric nurses'descriptions of women with postpartum psychosis and nurses'responses: An exploratory study in Sweden. Issues in MentalHealth Nursing 30(1):23–30. doi:10.1080/01612840802498268
Engqvist I, Ferszt G, Åhlin A, Nilsson K (2011b) Women's experienceof postpartum psychotic episodes—analyses of narratives fromthe Internet. Arch Psychiatr Nurs 25(5):376–387. doi:10.1016/j.apnu.2010.12.003
Engqvist I, Nilsson A, Nilsson K, Sjöström B (2007) Strategies in caringfor women with postpartum psychosis – an interview study withpsychiatric nurses. J Clin Nurs 16(7):1333–1342. doi:10.1111/j.1365-2702.2007.01717.x
Heron J, Gilbert N, Dolman C, Shah S, Beare I, Dearden S, MuckelroyN, Jones I, Ives J (2012) Information and support needs duringrecovery from postpartum psychosis. Archives of Women's Men-tal Health:1–11
Hollingsworth L (2004) Child custody loss among women withpersistent severe mental illness. Soc Work Res 28(4):199–209
Howard LM (2006) Pregnancy in women with psychotic disorders.Clin Eff Nurs 9(2):201–211
Howard LM, Hunt K (2008) The needs of mothers with severe mentalillness: a comparison of assessments of needs by staff and pa-tients. Archives of Women’s Mental Health 11(2):131–136.doi:10.1007/s00737-008-0006-9
Howard LM, Kumar C, Leese M, Thornicroft G (2002) The generalfertility rate in women with psychotic disorders. Am J Psychiatry159(6):991–997
Howard LM, Kumar R, Thornicroft G (2001) Psychosocial character-istics and needs of mothers with psychotic disorders. Br J Psychi-atry 178(5):427–432. doi:10.1192/bjp.178.5.427
Khalifeh H, Murgatroyd C, Freeman MP, Johnson S (2009) Hometreatment as an alternative to hospital admission for mothersin a mental health crisis: a qualitative study. Psychiatr Serv60(5):634–639
Krumm S, Becker T (2006) Subjective views of motherhood in womenwith mental illness-a sociological perspective. J Ment Heal15(4):449–460
Did the study articulate clear recommendations for future policy and/or practice? Did the study articulate clear recommendations for future research?
Q11 Subtotal ………………..
Total Score (out of a maximum of 62 points) ….....................
Motherhood for women with severe mental illness

Lester H, Tritter JQ, Sorohan H (2005) Patients' and health profes-sionals' views on primary care for people with serious mentalillness: focus group study. BMJ 330(7500):1122
Maddocks S, Johnson S, Wright N, Stickley T (2010) A phenomeno-logical exploration of the lived experience of mental health nurseswho care for clients with enduring mental health problems whoare parents. J Psychiatr Ment Heal Nurs 17(8):674–682.doi:10.1111/j.1365-2850.2010.01582.x
Mays N, Pope C (2000) Assessing quality in qualitative research. BMJ320(7226):50–52. doi:10.1136/bmj.320.7226.50
McConachie S, Whitford H (2009) Mental health nurses’ attitudestowards severe perinatal mental illness. J Adv Nurs 65(4):867–876. doi:10.1111/j.1365-2648.2008.04952.x
McGrath JJ, Hearle J, Jenner L, Plant K, Drummond A, Barkla J(1999) The fertility and fecundity of patients with psychoses.Acta Psychiatr Scand 99(6):441–446
Meiser B, Mitchell PB, McGirr H (2005) Implications of geneticrisk information in families with a high density of bipolardisorder: an exploratory study. Social Science & Medicine60(1):109–118
Miller LJ (1997) Sexuality, reproduction, and family planning in wom-en with schizophrenia. Schizophr Bull 23(4):623–635
Montgomery P, Mossey S, Bailey P, Forchuk C (2011) Mothers withserious mental illness: their experience of "hitting bottom". ISRNnursing 2011:708318
Montgomery P, Tompkins C, Forchuk C, French S (2006) Keepingclose: Mothering with serious mental illness. J Adv Nurs54(1):20–28
Mowbray CT, Oyserman D, Ross S (1995) Parenting and the signifi-cance of children for women with a serious mental illness. Journalof Mental Health Administration 22(2):189–200
Murray L, Cooper P, Hipwell A (2003) Mental health of parents caringfor infants. Archives of Women's Mental Health 6:71–77
Nicholson J, Blanch A (1994) Rehabilitation for parenting roles forpeople with serious mental illness. Psychosocial RehabilitationJournal
Nicholson J, Geller JL, Fisher WH, Dion GL (1993) State policies andprograms that address the needs of mentally ill mothers in thepublic sector. Hospital and Community Psychiatry 44:484–484
Nicholson J, Sweeney EM, Geller JL (1998) Focus on women:Mothers with mental illness: II. Family relationships and thecontext of parenting. Psychiatr Serv 49(5):643–649
Noblit GW, Hare RD (1988) Meta-ethnography: Synthesizing qualita-tive studies, vol 11. Sage Publications.
Peay HL, Hooker GW, Kassem L, Biesecker BB (2009) Family riskand related education and counseling needs: perceptions of adults
with bipolar disorder and siblings of adults with bipolar disorder.American Journal of Medical Genetics Part A 149A(3):364–371.doi:10.1002/ajmg.a.32696
Rice MJ (2008) Evidence-based practice in psychiatric and mentalhealth nursing: qualitative meta-synthesis. Journal of the Ameri-can Psychiatric Nurses Association 14(5):382–385
Robertson E, Lyons A (2003) Living with puerperal psychosis: aqualitative analysis. Psychol Psychother Theory Res Pract 76(Pt4):411–431
Sandelowski M, Trimble F, Woodard EK, Barroso J (2006) Fromsynthesis to script: transforming qualitative research findings foruse in practice. Qual Heal Res 16(10):1350–1370
Sands RG (1995) The parenting experience of low-income singlewomen with serious mental disorders. Fam Soc 76(2):86–96
Sands RG (2004) Maternal custody status and living arrangements ofchildren of women with severe mental illness. Heal Soc Work29:317–325
Savvidou I, Bozikas VP, Hatzigeleki S, Karavatos A (2003) Narrativesabout their children by mothers hospitalized on a psychiatric unit.Fam Process 42(3):391–402
Scottish Intercollegiate Guidelines Network: Management of perinatalmood disorders: a national clinical guideline (2012) http://www.sign.ac.uk/pdf/sign127.pdf.
Stanley N, Penhale B (1999) The mental health problems of mothersexperiencing the child protection system. Identifying needs andappropriate responses. Child Abuse Review 8:34–35
Ueno R, Kamibeppu K (2008) Narratives by Japanese mothers withchronic mental illness in the Tokyo metropolitan area: their feel-ings toward their children and perceptions of their children'sfeelings. J Nerv Ment Dis 196(7):522–530
Venkataraman M, Ackerson BJ (2008) Parenting among mothers withbipolar disorder: strengths, challenges, and service needs. J FamSoc Work 11(4):389–408. doi:10.1080/10522150802441825
Vigod SN, Seeman MV, Ray JG, Anderson GM, Dennis CL,Grigoriadis S, Gruneir A, Kurdyak PA, Rochon PA (2012) Tem-poral trends in general and age-specific fertility rates amongwomen with schizophrenia (1996–2009): a population-basedstudy in Ontario, Canada. Schizophrenia Research
Walsh D, Downe S (2005) Meta-synthesis method for qualitativeresearch: a literature review. J Adv Nurs 50(2):204–211
Wan MW, Moulton S, Abel KM (2008) The service needs ofmothers with schizophrenia: a qualitative study of perinatalpsychiatric and antenatal workers. General hospital psychiatry30(2):177–184
Wilson L, Crowe M (2009) Parenting with a diagnosis bipolar disorder.J Adv Nurs 65(4):877–884
C. Dolman et al.
View publication statsView publication stats


![Review of Maritime Transport 2013 [Arabic]Review of Maritime Transport 2013 [Arabic] ... 2013](https://img.pdfslide.net/doc/110x75/5e31b798be917c48d84af07a/review-of-maritime-transport-2013-arabic-review-of-maritime-transport-2013-arabic.jpg)