Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Axonal Damage in Relapsing MultipleSclerosis is Markedly Reduced
by Natalizumab
Martin Gunnarsson, MD, PhD,1 Clas Malmestrom, MD, PhD,2
Markus Axelsson, MD,2 Peter Sundstrom, MD, PhD,3 Charlotte Dahle, MD, PhD,4,5
Magnus Vrethem, MD, PhD,4 Tomas Olsson, MD, PhD,6 Fredrik Piehl, MD, PhD,6
Niklas Norgren, PhD,7 Lars Rosengren, MD, PhD,2 Anders Svenningsson, MD, PhD,3
and Jan Lycke, MD, PhD2
Objective: The impact of present disease-modifying treatments (DMTs) in multiple sclerosis (MS) on nerve injury andreactive astrogliosis is still unclear. Therefore, we studied the effect of natalizumab treatment on the release of 2brain-specific tissue damage markers into cerebrospinal fluid (CSF) in MS patients.Methods: CSF samples from 92 patients with relapsing forms of MS were collected in a prospective manner prior tonatalizumab treatment and after 6 or 12 months. In 86 cases, natalizumab was used as second-line DMT due tobreakthrough of disease activity. The levels of neurofilament light (NFL) and glial fibrillary acidic protein (GFAP) weredetermined using highly sensitive in-house developed enzyme-linked immunosorbent assays.Results: Natalizumab treatment led to a 3-fold reduction of NFL levels, from a mean value of 1,300 (standarddeviation [SD], 2,200) to 400 (SD, 270) ng/l (p < 0.001). The later value was not significantly different from thatfound in healthy control subjects (350ng/l; SD, 170; n ¼ 28). Subgroup analysis revealed a consistent effect on NFLrelease, regardless of previous DMT or whether patients had relapses or were in remission within 3 months prior tonatalizumab treatment. No differences between pre- and post-treatment levels of GFAP were detected.Interpretation: Our data demonstrate that natalizumab treatment reduces the accumulation of nerve injury inrelapsing forms of MS. It is anticipated that highly effective anti-inflammatory treatment can reduce axonal loss,thereby preventing development of permanent neurological disability.
ANN NEUROL 2011;69:83–89
Multiple sclerosis (MS) is a chronic inflammatory
demyelinating disease of the central nervous system
(CNS). Axonal damage occurs both within MS lesions and
in the normal-appearing white matter already at early
stages of the disease, as demonstrated by neuropathological
studies,1 magnetic resonance imaging (MRI) techniques,2–4
and by use of biomarkers.5–9 Numerous findings suggest
that axonal loss followed by astrogliosis is ultimately re-
sponsible for the development of irreversible neurological
deficits.8–18 The role of immune system-mediated mecha-
nisms in causing such processes, however, has not yet been
clarified. Disease-modifying treatments (DMTs) in MS
have so far been designed to modulate the immune system
and are almost exclusively effective in disease phases in
which the inflammatory component is prominent. Conse-
quently, DMTs in current use reduce the number of relap-
ses and appearance of T2 as well as gadolinium-enhanced
MRI lesions in relapsing-remitting MS (RRMS) patients.
Natalizumab, a monoclonal antibody preventing lympho-
cyte migration across the blood-brain barrier, is a highly
efficient agent in this respect.19–23 Whether early immuno-
modulatory intervention in fact retains axonal integrity and
View this article online at wileyonlinelibrary.com. DOI: 10.1002/ana.22247
Received May 13, 2010, and in revised form Jul 26, 2010. Accepted for publication Aug 20, 2010.
Address correspondence to Dr Svenningsson, Department of Neurology, Norrlands University Hospital, S-901 85 Umea, Sweden.
E-mail: [email protected]
From the 1Department of Neurology, Orebro University Hospital, Orebro; 2Department of Neurology, Sahlgrenska University Hospital, Goteborg;3Department of Neurology, Norrlands University Hospital, Umea; 4Department of Neurology and Neurophysiology, Linkoping University Hospital,
Linkoping; 5Clinical Immunology Unit, Department of Clinical and Experimental Medicine, Linkoping University, Linkoping; 6Neuroimmunology Unit, Center
for Molecular Medicine, Department of Clinical Neuroscience, Karolinska Institute, Stockholm; and 7UmanDiagnostics, Umea, Sweden.
VC 2011 American Neurological Association 83

prevents astrogliosis deserves further investigation. Detec-
tion of axonal and astroglial cytoskeletal proteins, such as
neurofilament light (NFL) and glial fibrillary acidic protein
(GFAP), in the cerebrospinal fluid (CSF) reflects these
processes in vivo.8,9 To study the effects of intense immune
modulation within the CNS on axonal damage and astro-
gliosis, we quantified NFL and GFAP in the CSF from 92
MS patients undergoing 6 to 12 months of treatment with
natalizumab.
Subjects and Methods
Patients and CSF CollectionFollowing acquisition of informed consent, 92 MS
patients (83 RRMS and 9 secondary progressive MS
with relapses [SPRMS]) were included consecutively
using a multicenter approach. Patients fulfilled the re-
vised McDonald criteria24 and were scheduled to start
treatment with 300mg natalizumab intravenously once
monthly according to Swedish guidelines. All patients
presented either a highly active disease course de novo or
breakthrough disease activity in terms of relapses in the
presence of other DMTs. The mean annual relapse rate
was 1.2 (standard deviation [SD], 1.1) during the year
prior to natalizumab treatment. Among the 92 patients
included, 6 were treatment naive, whereas 86 had been
using other DMTs, of which 67 were treated with inter-
feron-b, 4 with glatiramer acetate, 8 with mitoxantrone,
and 7 with other treatments. Thirty patients had experi-
enced a relapse within 3 months prior to natalizumab
treatment, whereas 62 patients were in remission during
this period. Patient demographics are shown in Table 1.
Medical history and additional clinical data such as
relapse count during the study period were recorded pro-
spectively in the medical record and in the Swedish MS
registry. CSF was collected consecutively by lumbar spi-
nal taps prior to treatment with natalizumab and after 6
(n ¼ 8) or 12 (n ¼ 84) months. Clinical examination
using the Expanded Disability Status Scale (EDSS)25 was
performed by trained neurologists no more than 1 week
apart from the lumbar puncture. Ten milliliters of CSF
was centrifuged at 1,300 to 1,800g for 10 minutes. Ali-
quots of supernatant (0.5–1.0ml) were immediately snap-
frozen to �80�C and not thawed until analysis. All
patients underwent routine CSF examinations including
cell counts, and protein electrophoresis and determina-
tion of immunoglobulin (Ig)G-index were performed in
59 patients. CSF samples from 28 healthy volunteers,
recruited among blood donors and university students,
were used as reference.
All NFL and GFAP analysis were performed simul-
taneously at the Section of Neurochemistry, Sahlgrenska
University Hospital, Molndal. CSF samples were blinded
for laboratory personnel during all stages of analysis. The
study was approved by the local ethics committee at
Uppsala University, Sweden.
NFL Enzyme-Linked ImmunoassayThe UmanDiagnostics NF-light enzyme-linked immuno-
assay (ELISA), developed by Norgren and coworkers,
detects 1 of the low molecular weight chains of neuronal
intracellular intermediate filaments.9 The assay is based
on 2 highly specific monoclonal antibodies and a biotin-
streptavidin horseradish peroxidase (HRP) system. Analy-
sis was performed at room temperature. Cerebrospinal
fluid samples were diluted 1:1 with sample dilution
buffer to a total volume of 100ll and incubated with
agitation (800rpm) for 1 hour in precoated anti-NFL
ELISA plates. Thereafter, a 100ll solution of tracer anti-
body (biotin anti-NFL) was added to each well and incu-
bated for 45 minutes. Washing cycles were performed af-
ter all incubations. Detection was performed using 100llstreptavidin-HRP incubated for 30 minutes, followed by
another incubation with 100ll 3,30,5,50-tetramethylben-
zidine for 15 minutes;. A volume of 50ll stop solution
(8% v/v sulphuric acid) was added to each well, and ab-
sorbance was read at k490nm. The sensitivity of the
NFL assay was 31ng/l.
GFAP ELISAMeasurements of GFAP were performed using the ELISA
procedure previously developed by Rosengren and co-
workers.17 In brief, ELISA plates were coated with hen
TABLE 1: Demographics of Multiple SclerosisPatients and HCs
Characteristic MS, n 5 92 HCs,n 5 28
Relapse,n 5 30a
Remission,n 5 62b
Gender,F/M
20/10 34/28 8/20
Age, yr 36 (19–59),p ¼ 0.020vs HCc
38 (14–56),p ¼ 0.034vs HCc
43(27–62)
MSduration,yr
9.0 (0.5–28) 10 (2–26) N/A
Values for age and MS duration are given as mean (range).aDenotes MS patients with relapses within 3 months priorto natalizumab treatment onset.bDenotes MS patients in remission during this period.ct test.MS ¼ multiple sclerosis; HC ¼ healthy control; N/A ¼not applicable.
ANNALS of Neurology
84 Volume 69, No. 1

anti-GFAP IgG followed by incubation with CSF sam-
ples at room temperature for 2 hours. Rabbit anti-GFAP
IgG was added as secondary antibody and incubated for
1 hour at room temperature. Washing cycles were per-
formed after each incubation step. Detection was per-
formed with peroxidase-conjugated donkey antirabbit
IgG and 3,30,5,50-tetramethylbenzidine substrate. Absorb-
ance was read at k490 nm, and the sensitivity of the
GFAP assay was 16ng/l.
Statistical AnalysisWilcoxon signed ranks test and Mann-Whitney U test
were used for analysis of nonparametric data. Analysis of
parametric data, paired and unpaired, was performed using
t test. Test for age influence on the NFL levels in MS
patients as compared to healthy controls was done via lin-
ear regression analysis. Statistical calculations were per-
formed in SPSS 16.0 software (SPSS Inc., Chicago, IL).
Results
Clinical Data and CSF Inflammatory ParametersThe annual relapse rate during the natalizumab treatment
period was reduced from a mean value of 1.2 (SD, 1.1;
year prior to treatment) to 0.15 (SD, 0.36; p < 0.001).
The median pretreatment EDSS score was 4.0 (2.5–5.5,
25th–75th percentile) as compared to 3.5 (2.0–5.0,
25th–75th percentile) post-treatment (p < 0.001). More-
over, CSF inflammatory parameters were significantly
decreased in terms of cell count from a mean of 5.4
(SD, 6.9) to 1.6 (SD, 1.3) � 106 cells/l (p < 0.001) and
IgG-index from a mean of 1.1 (SD, 0.60) to 0.94 (SD,
FIGURE 1: Neurofilament light in cerebrospinal fluid (CSF)following natalizumab treatment. Intravenous infusions of300mg natalizumab were performed monthly in 92 multiplesclerosis patients. Neurofilament light (NFL) levels in theCSF were compared to levels obtained in 28 healthyindividuals. Pretreatment mean value was significantlydifferent from that obtained after treatment (p < 0.001) andin healthy controls (p < 0.001). No significant difference wasfound between mean values after treatment and in healthycontrols, respectively. SE 5 standard error.
TABLE 2: Clinical and Cerebrospinal Fluid Parameters following Natalizumab Treatment
Parameter Relapse, n 530a Remission, n 5 62b Statistics
Pretreatment After 6–12MonthsTreatment
Pretreatment After6–12 MonthsTreatment
Relapses/yr 2.0 (1.1)c 0.10 (0.31)c 0.84 (0.83)c 0.18 (0.39)c p < 0.001c
p < 0.001c
EDSS 3.5 (2.5–4.5)d 2.75(1.375–4.0)d
4.0 (2.25–6.0)d 4.0(2.375–5.625)d
p < 0.001d
p ¼ 0.023d
Cell count, 106 cells/l 5.8 (6.0)c 1.4 (1.2)c 5.2 (7.3)c 1.6 (1.4)c p < 0.001c
p < 0.001c
IgG index 0.93 (0.32)c,e 0.83 (0.29)c,e 1.1 (0.68)c,f 1.0 (0.56)c,f p ¼ 0.033c
p ¼ 0.001c
NFL, ng/l 2300 (3600)c 350 (170)c 860 (780)c 430 (310)c p < 0.005c
p < 0.001c
Values are given as mean (standard deviation) except for EDSS, which is presented as median (25th–75th percentile).aDenotes MS patients with relapses within 3 months prior to natalizumab treatment.bDenotes MS patients in remission during this period.cParied sample t test.dMann-Whitney U test.en¼ 17.fn ¼ 42.EDSS ¼ Expanded Disability Status Scale; IgG ¼ immunoglobulin G; NFL ¼ neurofilament light; MS ¼ multiple sclerosis.
Gunnarsson et al: Relapsing MS and Natalizumab
January 2011 85
0.50; p < 0.001). Stratification of the cohort into
patients with relapses within 3 months prior to natalizu-
mab treatment and patients in remission during this pe-
riod is shown in Table 2.
NFLPrior to natalizumab treatment, the mean NFL concen-
tration in CSF from the 92 MS patients studied was
1,300ng/l (SD, 2200), whereas healthy controls displayed
a mean value of 350ng/l (SD, 170; p < 0.001; Fig 1).
After treatment, however, the mean NFL level was signif-
icantly reduced to 400 (SD, 270) ng/l (p < 0.001).
Notably, the post-treatment value did not differ signifi-
cantly from that found in healthy control subjects.
We have previously shown that NFL levels are
increased in the 3-month period after a relapse.7–9 There-
fore, we made a separate analysis of the groups of
patients having a relapse versus being in remission during
this time period before lumbar puncture. Thus, the
mean NFL concentration in CSF was determined as
2,300ng/l (SD, 3,600) in MS patients with relapses (n ¼30), as compared to 860ng/l (SD, 780) in patients dis-
playing clinical remission for at least 3 months (n ¼ 62)
(p < 0.038; equal variance not assumed). When exclu-
sively analyzing MS patients in remission, NFL levels
were still significantly reduced following natalizumab
treatment (p < 0.001; see Table 2). Both patients with
and those without ongoing relapses during the 3-month
period prior to natalizumab treatment displayed post-
treatment NFL levels not significantly different from
those obtained in healthy controls (mean, 350ng/l; SD,
170; see Table 2).
Pretreatment levels of NFL in treatment-naive MS
patients (n ¼ 6) were higher (3,300ng/l; SD, 6,600) but
not significantly different from those obtained in patients
subjected to DMTs prior to natalizumab (1,200ng/l; SD,
1,600; n ¼ 86). An adequate comparison regarding dif-
ferent types of immune modulation was not possible due
to different treatment regimes and uneven patient distri-
bution. After being on natalizumab treatment for 6 to 12
months, both treatment-naive MS patients and those
who had previously undergone immune modulation pre-
sented NFL levels similar to values obtained in healthy
controls (data not shown).
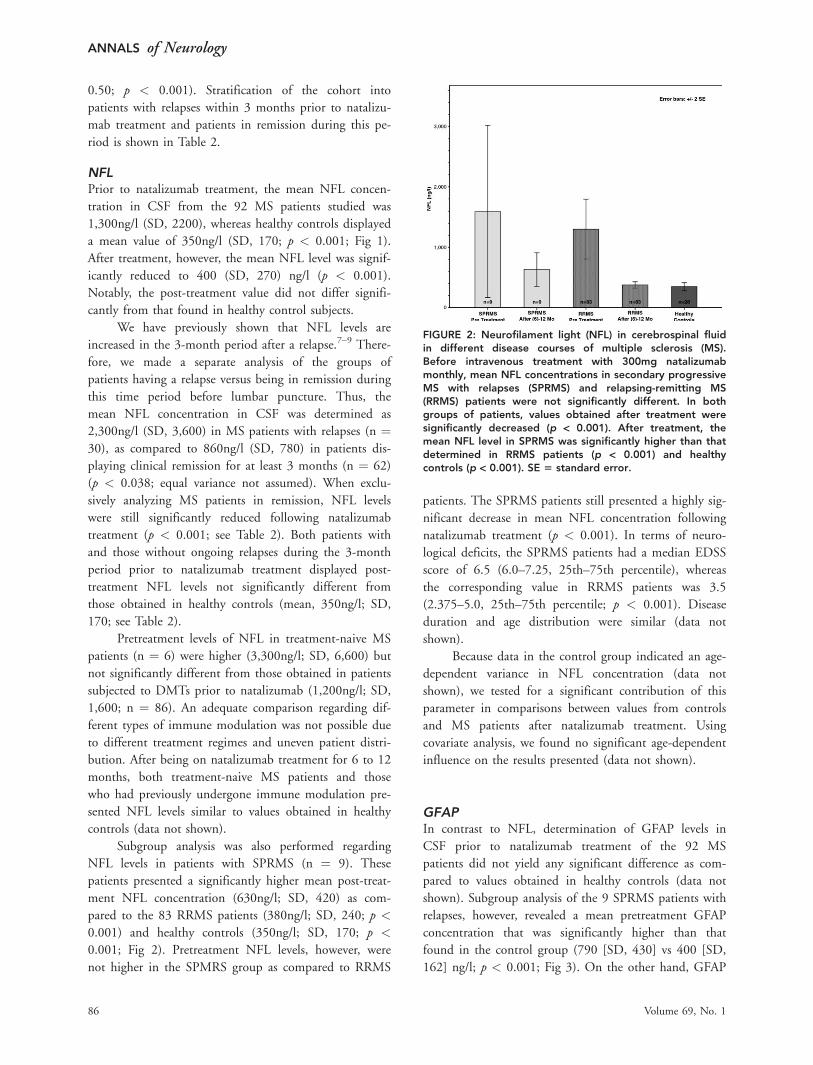
Subgroup analysis was also performed regarding
NFL levels in patients with SPRMS (n ¼ 9). These
patients presented a significantly higher mean post-treat-
ment NFL concentration (630ng/l; SD, 420) as com-
pared to the 83 RRMS patients (380ng/l; SD, 240; p <
0.001) and healthy controls (350ng/l; SD, 170; p <
0.001; Fig 2). Pretreatment NFL levels, however, were
not higher in the SPMRS group as compared to RRMS
patients. The SPRMS patients still presented a highly sig-
nificant decrease in mean NFL concentration following
natalizumab treatment (p < 0.001). In terms of neuro-
logical deficits, the SPRMS patients had a median EDSS
score of 6.5 (6.0–7.25, 25th–75th percentile), whereas
the corresponding value in RRMS patients was 3.5
(2.375–5.0, 25th–75th percentile; p < 0.001). Disease
duration and age distribution were similar (data not
shown).
Because data in the control group indicated an age-
dependent variance in NFL concentration (data not
shown), we tested for a significant contribution of this
parameter in comparisons between values from controls
and MS patients after natalizumab treatment. Using
covariate analysis, we found no significant age-dependent
influence on the results presented (data not shown).
GFAPIn contrast to NFL, determination of GFAP levels in
CSF prior to natalizumab treatment of the 92 MS
patients did not yield any significant difference as com-
pared to values obtained in healthy controls (data not
shown). Subgroup analysis of the 9 SPRMS patients with
relapses, however, revealed a mean pretreatment GFAP
concentration that was significantly higher than that
found in the control group (790 [SD, 430] vs 400 [SD,
162] ng/l; p < 0.001; Fig 3). On the other hand, GFAP
FIGURE 2: Neurofilament light (NFL) in cerebrospinal fluidin different disease courses of multiple sclerosis (MS).Before intravenous treatment with 300mg natalizumabmonthly, mean NFL concentrations in secondary progressiveMS with relapses (SPRMS) and relapsing-remitting MS(RRMS) patients were not significantly different. In bothgroups of patients, values obtained after treatment weresignificantly decreased (p < 0.001). After treatment, themean NFL level in SPRMS was significantly higher than thatdetermined in RRMS patients (p < 0.001) and healthycontrols (p < 0.001). SE 5 standard error.
ANNALS of Neurology
86 Volume 69, No. 1

levels were similar in healthy controls and RRMS
patients (mean, 510ng/l; SD, 460; n ¼ 83).
Natalizumab treatment for 6 to 12 months had no
significant influence on the GFAP levels in CSF, neither
in the entire 92 MS patient population nor in cases of
subgroup analysis (see Fig 3).
Discussion
Irreversible neurological deficits in MS likely emerge as a
consequence of accumulating nerve injury starting al-
ready in early phases of the disease.8–18 Due to the long
lag phase before clinical disability can be detected and a
lack of reliable biomarkers, the effect of current immuno-
modulatory treatments on tissue damage has been diffi-
cult to assess. Previously, we have characterized NFL as a
marker of ongoing axonal damage.7–9 In this study, we
demonstrate that elevated NFL levels in CSF from 92
patients with relapsing forms of MS are markedly
decreased following natalizumab treatment for 6 to 12
months. Post-treatment NFL levels were not significantly
different from values obtained in healthy individuals.
Moreover, the effect was consistent regardless of whether
the patients were treated with first-line DMT at the time
of natalizumab treatment onset or not.
The natalizumab mechanism of action and its CNS
anti-inflammatory potential has been well characterized.
In the pivotal natalizumab trial, a highly significant
reduction in relapse rate and MRI lesion formation was
obtained.19 These results have been confirmed in open
follow-up studies of patients with treatment failure on
first-line DMTs and in highly active MS.20,21 The anti-
inflammatory effect is likely to be achieved by interfer-
ence with lymphocyte migration into the CNS, reflected
among others by a reduced expression of proinflamma-
tory cytokines and chemokines in the CSF compart-
ment.26–28 In the present investigation, both clinical pa-
rameters, that is, relapse rate and EDSS score, and CSF
inflammatory markers in terms of inflammatory cell
counts in CSF and IgG-index were decreased following
natalizumab treatment. These data are well in line with
the results presented in the pivotal natalizumab trial and
several other studies.19–23 Therefore, it is of certain inter-
est that we concomitantly demonstrate a normalization
of NFL levels in CSF from this cohort of MS patients.
In contrast to the marked effect on NFL release, no
changes in astrogliosis, as determined by GFAP quantifi-
cation, were seen following natalizumab treatment. This
may be due to the characteristics of the patient cohort,
because earlier data suggest that GFAP is elevated in sec-
ondary progressive but not RRMS.8,9,12,17 Such a notion
is supported by the fact that increased GFAP levels, as
compared to healthy controls, were found exclusively in
patients presenting an underlying progressive disease
course and more pronounced neurological deficits in
terms of EDSS score.
Accurate identification of MS patients with insuffi-
cient treatment effect and at high risk for development of
future neurological disability is becoming increasingly im-
portant. Immune modulation in MS partly prevents devel-
opment of sustained disability if initiated during the relaps-
ing phase of the disease, but the evidence for long-term
treatment efficacy has not yet been clarified. Furthermore,
the risk-benefit profiles of current DMTs differ consider-
ably, and difficulties in accurate assessment of treatment ef-
ficacy at the individual level in a short time perspective
present a clinical dilemma. Except for MRI parameters
reflecting CNS inflammation, there are presently no surro-
gate markers of disease activity in practical use. The Uman-
Diagnostics NF-light ELISA is based on 2 monoclonal
antibodies highly specific and sensitive for detection of
NFL in body fluids.9 By use of this assay and other immu-
nochemical setups, it has been shown that neurofilament
levels are increased in CSF during MS exacerbations.7–9,29
Moreover, high NFL levels determined at diagnostic lum-
bar punctures, especially in the presence of relapses, corre-
late with a worse prognosis as determined using EDSS and
multiple sclerosis severity score (MSSS) at clinical follow-
ups after 5 and 14 years, respectively.9,18 Notably, we have
earlier demonstrated significantly higher NFL levels also in
phases of clinical remission as compared to control sub-
jects.8,9 This likely reflects an ongoing clinically silent
FIGURE 3: Glial fibrillary acidic protein (GFAP) incerebrospinal fluid in different disease courses of multiplesclerosis (MS). The mean pre-treatment GFAP concentrationwas significantly higher in secondary progressive MS withrelapses (SPRMS) but not relapsing-remitting MS (RRMS)patients as compared to healthy controls (p < 0.001). Nosignificant differences were found after intravenoustreatment with 300 mg natalizumab monthly. SE 5 standarderror.
Gunnarsson et al: Relapsing MS and Natalizumab
January 2011 87

axonal damage that, according to data presented here, is
amendable to more intense immunomodulatory treatment.
NFL levels in this study were considerably increased, in both
the presence and absence of relapses. Furthermore, treat-
ment-naive patients as well as patients previously subjected
to first-line DMTs displayed increased NFL levels in CSF.
These results further strengthen the rationale for NFL deter-
mination as a measure of subclinical disease activity related
to ongoing nerve injury. We believe that our data also sup-
port NFL quantification in CSF as a putative outcome pa-
rameter in clinical trials of new drugs in MS. GFAP on the
other hand, does not seem to be a useful biomarker in this
aspect, at least not in relapsing-remitting phases of the dis-
ease. Further studies focused on correlations between levels
of NFL in CSF and atrophy measurements by emerging
MRI techniques may provide valuable additional data.
In conclusion, our data support the notion that
inflammatory activity in RRMS is associated with axonal
damage. Effective immunomodulatory treatment is likely
to be of utmost importance in preventing axonal loss
and development of irreversible CNS injury. It is antici-
pated that highly active control of CNS inflammation in
MS may have profound effects on the long-term course
of the disease, although this remains to be shown in
future studies. In this context, analysis of NFL levels in
the CSF have the potential to provide vital information
regarding treatment efficacy in the short-term perspective
and to facilitate treatment decisions.
Acknowledgment
Research performed in this project was supported by
grants from Orebro Society of Medicine (M.G.), Swedish
Society of the Neurologically Disabled (J.L.), Gothen-
burg Multiple Sclerosis Society (J.L.), Edith Jacobsson
Foundation (J.L.), Swedish Reasearch Council (T.O.),
Bibbi and Niels Jensen Foundation (T.O.), Soderbergs
Foundation (T.O.), Montell Williams Foundation, EU
fp6 (T.O.), Neuropromise (LSHM-CT-2005-018637)
(T.O.), and Biogen Idec (J.L.).
We thank S. Fridlund for skillful technical assistance.
Authorship
M.G. and C.M. contributed equally.
Potential Conflicts of Interest
M.G. has served on educational boards for Biogen Idec,
BayerScheringPharma, and Merck; has received speakers
honoraria from Biogen Idec, Merck, BayerScheringPharma,
and SanofiAventis; has received payment for development of
educational presentations from Biogen Idec; and has had
travel expenses reimbursed by Biogen Idec and Merck. C.M.
has received lecture honoraria from Biogen, and has had
travel expenses partially reimbursed by Biogen Idec. M.A. has
had travel expenses reimbursed by Biogen Idec and
MerckSerono. P.S. has served on an advisory board for
Novartis; has received lecture fees from Biogen Idec; and has
had travel expenses reimbursed by Biogen Idec. C.D. has
received personal compensation for activities with Biogen
Idec, Merck, BayerScheringPharma, and SanofiAventis as a
speaker and consultant. M.V. has a grant pending from
Biogen Idec and has received lecture honoraria from Biogen
Idec and Merck Serono. F.P. has a grant pending from Biogen
Idec; has received payment for development of educational
presentations from Biogen Idec, Novartis, and MerckSerono;
and has had travel expenses reimbursed by Biogen Idec and
Novartis. N.N. is employed by UmanDiagnostics AB.A.S.
has served on an advisory board for MerckSerono; has
received lecture honoraria from Biogen Idec and Baxter; and
has had travel expenses partially reimbursed by Biogen Idec,
MerckSerono, and Baxter. J.L. has served on advisory boards
for Biogen Idec and Merck Serono; has a grant pending from
Biogen Idec; has received speakers honoraria from Biogen
Idec and Merck Serono; and has had travel expenses
reimbursed by Biogen Idec. T.O. has received consultancy
fees from Biogen Idec, SanofiAventis, Merck, and Novartis;
and has grants pending from Biogen Idec, Merck,
SanofiAventis, and Bayer.
References1. Trapp BD, Peterson J, Ransohoff RM, et al. Axonal transection in
the lesions of multiple sclerosis. N Engl J Med 1998;338:278–285.
2. Pascual AM, Martinez-Bisbal MC, Bosca I, et al. Axonal loss is pro-gressive and partly dissociated from lesion load in early multiplesclerosis. Neurology 2007;69:63–67.
3. Filippi M, Bozzali M, Rovaris M, et al. Evidence for widespreadaxonal damage at the earliest clinical stage of multiple sclerosis.Brain 2003;126:433–437.
4. De Stefano N, Narayanan S, Francis SJ, et al. Diffuse axonaland tissue injury in patients with multiple sclerosis with low cere-bral lesion load and no disability. Arch Neurol 2002;59:1565–1571.
5. Teunissen CE, Iacobaeus E, Khademi M, et al. Combination ofCSF N-acetylaspartate and neurofilaments in multiple sclerosis.Neurology 2009;72:1322–1329.
6. Brettschneider J, Petzold A, Junker A, Tumani H. Axonal damagemarkers in the cerebrospinal fluid of patients with clinically iso-lated syndrome improve predicting conversion to definite multiplesclerosis. Mult Scler 2006;12:143–148.
7. Lycke JN, Karlsson JE, Andersen O, Rosengren LE. Neurofilamentprotein in cerebrospinal fluid: a potential marker of activity in mul-tiple sclerosis. J Neurol Neurosurg Psychiatry 1998;64:402–404.
8. Malmestrom C, Haghighi S, Rosengren L, et al. Neurofilamentlight protein and glial fibrillary acidic protein as biological markersin MS. Neurology 2003;61:1720–1725.
9. Norgren N, Sundstrom P, Svenningsson A, et al. Neurofilamentand glial fibrillary acidic protein in multiple sclerosis. Neurology2004;63:1586–1590.
ANNALS of Neurology
88 Volume 69, No. 1

10. Lim ET, Sellebjerg F, Jensen CV, et al. Acute axonal damage pre-dicts clinical outcome in patients with multiple sclerosis. Mult Scler2005;11:532–536.
11. Petzold A, Eikelenboom MJ, Keir G, et al. Axonal damage accu-mulates in the progressive phase of multiple sclerosis: three yearfollow up study. J Neurol Neurosurg Psychiatry 2005;76:206–211.
12. Petzold A, Eikelenboom MJ, Gveric D, et al. Markers for differentglial cell responses in multiple sclerosis: clinical and pathologicalcorrelations. Brain 2002;125:1462–1473.
13. Semra YK, Seidi OA, Sharief MK. Heightened intrathecal releaseof axonal cytoskeletal proteins in multiple sclerosis is associatedwith progressive disease and clinical disability. J Neuroimmunol2002;122:132–139.
14. De Stefano N, Narayanan S, Francis GS, et al. Evidence of axonaldamage in the early stages of multiple sclerosis and its relevanceto disability. Arch Neurol 2001;58:65–70.
15. Bjartmar C, Kidd G, Mork S, et al. Neurological disability corre-lates with spinal cord axonal loss and reduced N-acetyl aspartatein chronic multiple sclerosis patients. Ann Neurol 2000;48:893–901.
16. De Stefano N, Matthews PM, Fu L, et al. Axonal damage corre-lates with disability in patients with relapsing-remitting multiplesclerosis. Results of a longitudinal magnetic resonance spectros-copy study. Brain 1998;121(pt 8):1469–1477.
17. Rosengren LE, Lycke J, Andersen O. Glial fibrillary acidic proteinin CSF of multiple sclerosis patients: relation to neurological defi-cit. J Neurol Sci 1995;133:61–65.
18. Salzer J, Svenningsson A, Sundstrom P. Neurofilament light as aprognostic marker in multiple sclerosis. Mult Scler 2010;16:287–292.
19. Polman CH, O’Connor PW, Havrdova E, et al. A randomized, pla-cebo-controlled trial of natalizumab for relapsing multiple sclero-sis. N Engl J Med 2006;354:899–910.
20. Putzki N, Yaldizli O, Buhler R, et al. Natalizumab reduces clinicaland MRI activity in multiple sclerosis patients with high disease ac-tivity: results from a multicenter study in Switzerland. Eur Neurol2010;63:101–106.
21. Putzki N, Kollia K, Woods S, et al. Natalizumab is effective as sec-ond line therapy in the treatment of relapsing remitting multiplesclerosis. Eur J Neurol 2009;16:424–426.
22. Havrdova E, Galetta S, Hutchinson M, et al. Effect of natalizumabon clinical and radiological disease activity in multiple sclerosis: aretrospective analysis of the Natalizumab Safety and Efficacy inRelapsing-Remitting Multiple Sclerosis (AFFIRM) study. LancetNeurol 2009;8:254–260.
23. Miller DH, Soon D, Fernando KT, et al. MRI outcomes in a pla-cebo-controlled trial of natalizumab in relapsing MS. Neurology2007;68:1390–1401.
24. Polman CH, Reingold SC, Edan G, et al. Diagnostic criteria formultiple sclerosis: 2005 revisions to the ‘‘McDonald Criteria.’’ AnnNeurol 2005;58:840–846.
25. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: anexpanded disability status scale (EDSS). Neurology 1983;33:1444–1452.
26. Mellergard J, Edstrom M, Vrethem M, et al. Natalizumab treat-ment in multiple sclerosis: marked decline of chemokines andcytokines in cerebrospinal fluid. Mult Scler 2010;16:208–217.
27. Sellebjerg F, Bornsen L, Khademi M, et al. Increased cerebrospi-nal fluid concentrations of the chemokine CXCL13 in active MS.Neurology 2009;73:2003–2010.
28. Khademi M, Bornsen L, Rafatnia F, et al. The effects of natalizu-mab on inflammatory mediators in multiple sclerosis: prospectsfor treatment-sensitive biomarkers. Eur J Neurol 2009;16:528–536.
29. Rejdak K, Petzold A, Stelmasiak Z, Giovannoni G. Cerebrospinalfluid brain specific proteins in relation to nitric oxide metabolitesduring relapse of multiple sclerosis. Mult Scler 2008;14:59–66.
Gunnarsson et al: Relapsing MS and Natalizumab
January 2011 89