-
VITAMIN B12 -- COBALAMIN Known as CORRINOIDS -- corrin
structure
_________________ Other groups may attach to Co to form:
1. 5-deoxyadenosylcobalamin (5-deoxyadenosyl group)2.
Methylcobalamin (CH3 group)3. Cyanocobalamin (CN group)4.
Hydroxocobalamin (OH group)5. Aquocobalamin (H2O)6. Nitricobalamin
(NO2 group)
_____________are most active as coenzymesOthers can be easily
converted into the active forms
-
Fig. 9-35, p. 311
Structural formula of vitamin B12 (cyanocobalamin)
-
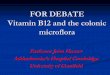
Absorption: Once released from foods by stomach pepsin, free
cobalamin: Attaches to R proteins (__________high affinity
for
cobalamin) and moves from stomach to small intestine The R
protein is hydrolyzed in ___________and free
cobalamin released Intrinsic Factor (IF) synthesized in stomach
and moved to
proximal small intestine binds to cobalamin (any form) The
complex travels to _______, where the receptors are
present
-
Stomach proteins R
Pyloric sphincter
Small intestine
Ileal receptor
IF
complex
IF
IF IF
IF R
B12
B12 + R
B12 R B12 R
B12
B12 IF
B12
B12
Fig. 9-36, p. 311
B12 IF
Vitamin B12 absorption.
-
VITAMIN B12 -- COBALAMIN (cont)
Transport: Following absorption, cobalamins bind to one of three
transport
proteins -- __________(TCI, TCII, TCIII) TCII is the main
carrier and it also helps vitamins uptake by the tissue
Storage: Although water soluble, it is stored in liver (60% of
body stores) and
muscle (30% of stores), primarily in the form of
adenosylcobalamin Due to the stored amount and bacterial production
in colon, it takes
several years for a deficiency to develop on a diet poor in B12
or low absorption
-
VITAMIN B12 -- COBALAMIN (cont)
Sources: Only in ______products -- originates from
microorganisms
About 70% of vitamin is ________with cooking Appreciable amounts
can be lost from milk by pasteurization (hence,
milk isnt a good source) B12 is synthesized by microorganisms
found in intestinal tract
If found in plants, its probably due to contamination DRI, 1998
(see your table)
It was raised to 2.4-2.6 g/day
-
VITAMIN B12 -- COBALAMIN (cont) Functions:
Serves as coenzyme for many enzymes: Metabolism of folate
(methionine synthetase) For DNA synthesis (deficiency causes
megaloblastic cells to be
released in circulation as macrocytes, but still with normal
hemoglobin, normochromic)
In nerve tissue Deficiency could cause impaired CHO metabolism
and glucose
utilization (methylmalonyl CoA to succinyl CoA) It is necessary
for myelin formation (needs methionine)
SEE TEXT, for folic acid, B12 and B6 interaction and
homocysteine accumulation
-
Fig. 9-33, p. 305
-
p. 312a
-
p. 312b
-
B12 deficiency Occurs in stages:
Low serum concentrations, as indicated by low TCII Low RBC
concentrations Leading to:
Decreased DNA synthesis Elevated serum homocysteine Anemia
Neuropathy (decreased methionine)
homocysteine methionine
Methyl THF methionine synthetase THF (active)
coenzyme-B12
__________________________-- severe deficiency Abnormal cell
division in bone marrow (megaloblastic cells) GI abnormalities
(diarrhea, constipation) Neurological ataxia Spastic reflexes
Paralysis of muscles and nerves
-
B12 deficiency risk factors: Poor diet -- rarely
About 5% deficiency caused by poor diet, rest by GI disorders or
poor absorption
Could be an issue among pure vegans, although takes long time to
develop
GI disorders: Lack of IF secretion (gastrectomy, impaired
gastric mucosa) Decreased absorptive surface (blind loop, ileal
resection,
celiac sprue, ileitis) Chronic pancreatitis
enzyme secretion impaired, for R protein synthesis Parasitic
infections (tapeworms)
Elderly (IF insufficiency), alcoholics, GI pts, infants
-
Assessing B12 status: Serum levels (normal 200-900 pg/mL)
Less than 100 pg/mL -- deficiency Holo TCII -- transcobalamin
with attached B12 (sensitive) TCII % saturation
Normally 20% of TCII is saturated with B12 Even early stages of
deficiency might show TCII saturation of 5%
Urinary homocysteine Not specific as it could originate from
folate deficiency
-
VITAMIN B6 -- ________________________
Structure Several vitamers which are interchangeable
Pyridoxine (alcohol) form in vegetables and has low
bioavailability Pyridoxal (aldehide) form in animal food --
unstable and destroyed by
cooking Pyridoxamine (amine) form in animal food -- also
unstable Pyridoxal-5-phosphate (PLP) -- generally considered the
active form
Therefore, the activity depends on the ability to metabolize
into PLP coenzyme
The synthetic vitamin is in a form of pyridoxine hydrochloride
-- stable
-
Fig. 9-38, p. 316 Vitamin B6 structures
-
Fig. 9-39, p. 316 Most of vitamin B6 metabolism occurs in the
liver
-
p. 317
Vitamin B6 metabolism is dependent on the normal
_________status
-
PLP functions: In about 60 reactions of amino acids
metabolism
Particularly important reactions of transamination, where both
PMP and PLP are involved as coenzymes
Also: Synthesis of heme Synthesis of niacin from tryptophan
Synthesis of histamine from histidine Synthesis of carnitine,
taurine, dopamine Cleavage of homocysteine Glycogen catabolism to
form glucose 1-phosphate Action on steroid hormone receptors
Prevents or interferes with hormone binding and by that mediates
hormone uptake
-
Fig. 9-42, p. 319
Cysteine synthesis from methionine requires vitamin B6 as
PLP
-
Sources: Meat (chicken, pork, fish), eggs
Low in dairy food Plant foods (whole grains, seeds, nuts)
Particularly high in the germ of the grain Easily destroyed by
processing, canning, heating,
freezing, milling DRI:
See table (about 2 and 1.6 mg/day for men and women) It depends
on protein intake. Formula by which the requirements
were calculated: 0.016 mg vitamin B6/1 g protein
-
Pyridoxine deficiency: Rare in US under normal conditions Takes
about 2 months to develop symptoms
Poor appetite, weakness, sleeplessness Microcytic hypochromic
anemia (impaired heme synthesis) Central and peripheral nervous
system disorders (impaired serotonin
synthesis) Hyperhomocysteinemia Glucose intolerance (especially
in pregnant women) Dermatological problems (glossitis, stomatitis)
Retarded growth, reproductive capacity
Pyridoxine toxicity -- doses from 300-500 mg/d Signs are similar
to deficiency, mostly ____________
-
At risk groups Infants born with low levels of B6 Elderly
Alcoholics (cant convert to PLP) People on high protein intake
Renal patients (from dialysis losses) Many drugs interfere with B6
metabolism
Anticonvulsants, corticosteroids, penicillamine Beneficial
effects of B6 supplementation (200 mg/day or more)
_________________ disease pts. on L-dopa Newborns or other pts.
with convulsions and seizures Alcoholics
-
Assessing pyridoxine status: Plasma PLP concentrations
When